Revista Mexicana de...
106
www.revmexneuroci.com / ISSN 1665-5044 Revista Mexicana de Neurociencia Publicación oficial de la Academia Mexicana de Neurología A.C. Órgano Oficial de Difusión de la AMN Academia Mexicana de Neurología, A.C. Rev Mex Neuroci ahora en CONACyT Vol. 18, núm. 5 (septiembre-octubre de 2017) Revista Mexicana de Neurociencia; 18,5 (2017):1-101
-
Upload
truongngoc -
Category
Documents
-
view
213 -
download
0
Transcript of Revista Mexicana de...
www.revmexneuroci.com / ISSN 1665-5044
Revista Mexicana de
NeurocienciaPublicación oficial de la Academia Mexicana de Neurología A.C.
Órgano Oficial de Difusión de la AMN
AcademiaMexicana deNeurología, A.C.
Rev Mex Neuroci ahora en CONACyT
Vol. 18, núm. 5 (septiembre-octubre de 2017)
Rev
ista
Mex
ican
a d
e N
euro
cien
cia;
18
,5 (2
01
7):
1-1
01

Editorial committee 2017Chief editor: Dr. C. Ildefonso Rodríguez Leyva [email protected]: M.C. Carolina León Jimenez M.C. Antonio Arauz Góngora [email protected] editor: Dra. Lilia Núñez OrozcoEmeritus editor: Dr. C. Carlos Cantú Brito
International editorial comitee
National editorial comitee
Dr. Anthony Amato Dr. José BillerDr. Andre KannerDra. Farrah MateenDr. José Merino
Dr. Sergio de Jesús Aguilar Castillo Dr. Marco Antonio Alegría LoyolaDra. Alma Yolanda Alvarado GutierrezDr. Carlos Gabriel Ascanio RodríguezDra. Catherine Boll WoehrlenDr. Antonio Bravo OroDr. Jorge Burgos CentenoDra. Graciela Cárdenas HernándezDr. Paul Carrillo MoraDra. Teresa Corona VázquezDra. Beatriz ChavezDr. Bruno Estañol VidalDra. Agnes FleuryDr. José Flores RiveraDra. Silvia GarcíaDr. Fernando Góngora RiveraDra. Margarita González CruzDra. Alejandra González-DuarteDr. Oscar González-Vargas
Dr. Rubén Haro Silva Dr. Juan Calixto Hernández AguilarDr. Héctor Gerardo Hernández RodríguezDr. Jesús Higuera CallejaDr. Javier Jaramillo de la TorreDr. Humberto Juárez JiménezDr. Rubén Martínez HernándezDra. Iris E. Martínez JuárezDra. Adriana Martínez MayorgaDr. Francisco Mena-BarrancoDra. Roxana Millán CepedaDra. Rebeca Millán GuerreroDr. Alberto Mimenza AlvaradoDra. Leticia Munive BaezDr. Luis Manuel Murillo BonillaDr. Alfredo Ponce de LeónDr. Guillermo Punzo BravoDra. Sandra Quiñones AguilarDra. María Teresa Reyes
Héctor Gerardo Hernández RodríguezMaestro Alejandro GarcíaRebeca BarrosoDesign Cortex
Statistical AdvisorStyle corrector
TranslatorDesign
Dra. Mayela Rodríguez ViolanteDr. Leopoldo Rivera CastañoDr. Ulises Rodríguez OrtizDr. Francisco Rogel OrtizDr. Luis Ángel Ruano Calderón Dra. Angélica Ruiz-FrancoDr. José Luis Ruiz-SandovalDr. José Manuel Sandoval RiveraDr. Daniel San JuanDr. Horacio Sentíes MadridDra. Mónica Sierra del RioDra. Ana Luisa Sosa Ortiz Dr. José Luis Soto-HernándezDr. Gersain Trujillo AlonsoDr. Steven Vargas CañasDr. Rubén Darío Vargas GarcíaDra. Karina Vélez JiménezDr. Marco Zenteno Castellanos
Dr. José Obeso Dr. Julio PascualDr. Marc Patterson Dr. Eduardo TolosaDr. Samuel Wiebe

Contenidos ContentsCONTRIBUCIONES ORIGINALES• Perfil neuropsicológico de un grupo de
adultos mayores diagnosticados con deterioro cognitivo leve
• Caracterización fractal de ventrículos cerebrales normales en imágenes de resonancia Magnética ponderadas en T2
• Relación entre la enfermedad ateroesclerótica y hernia discal en pacientes con manejo conservador integral.
REVISIONES • Revisión del trastorno del espectro autista:
Actualización del diagnóstico y tratamiento • Fisiopatología del trauma raquimedular • ¿Dónde estamos y a dónde vamos? Nuevas
estrategias integrales en el manejo de hernia de disco.
• Consideraciones y reconceptualización de teorias del dolor crónico asociado a disfunciones musculoesqueleticas y su implicancia en la plasticidad y reorganización cerebral: una revisión de la literatura.
• Celulas madres: una nueva alternativa en el manejo de la paralisis cerebral
REPORTES DE CASO• Evaluación neuropsicológica de la pragmática
de la comunicación en un paciente con daño cerebral adquirido
• Tratamiento endovascular de pseudoaneurismas gigantes de la arteria carótida interna cervical: a propósito de un caso y revisión de la literatura
EDITORIAL• Carta editorial por Dr. Miguel Osorno Guerra
ORIGINAL CONTRIBUTIONS• Neuropsychological profile of a group of
older adults diagnosed with mild cognitive impairment
• Fractal characterization of normal cerebral ventricles in t2-wheigthed magnetic resonance imaging
• Relationship between atherosclerotic disease and disc herniation in patients with integral conservative management.
REVIEWS• Autism spectrum disorder review: diagnosis
and treatment update• Pathophysiology of spinal trauma• Where are we and where are we going?
Review of strategies and new integral proposals in the management of herniated disc.
• Considerations and reconceptualization of theories of chronic pain associated with musculoskeletal dysfunctions and its implication in plasticity and cerebral reorganization: a review of the literatura.
• Stem cells: an alternative for the treatment of cerebral palsy
CASE REPORTS• Neuropsychological evaluation of pragmatics
in a patient with acquired brain injury • Endovascular treatment of giant
pseudoaneurysms of the cervical internal carotid artery: Case report and Review of literature.acquired brain injury
EDITORIAL• Editorial letter by Dr. Miguel Osorno Guerra
Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
2
Neuropsychological profile of a group of older adults diagnosed with mild cognitive impairment
Neuropsychological profile of a group of older adults diagnosed with mild cognitive impairment
Original contribution
Ríos-Gallardo Ángela Magnolia,1 Muñoz-Bernal Luisa Fernanda,2 Aldana-Camacho Laura Victoria,3 Santamaría-Íñiguez María Fernanda,4 Villanueva-Bonilla Cristian5
1 PhD. Neurociencia Cognitiva. Grupo de Investigación Dneuropsy. Vicerrectora Investigación y Proyección Social Universidad Surcolombiana.2 Esp. Evaluación Clínica y Tratamiento de Trastornos Emocionales y Afectivos. Fundación Universitaria Konrad Lorenz.3 Psicóloga Universidad Surcolombiana. Grupo de Investigación Dneuropsy.4 Mg. Psicología Clínica. Fundación Universitaria Konrad Lorenz.5 Psicólogo Universidad Surcolombiana. Joven Investigador Colciencias. Grupo de Investigación Dneuropsy.
Abstract
INTRODUCTION: Mild cognitive impairment (MCI) is a clinical condition between normal aging and a probable dementia process such as Alzheimer’s disease (AD), which manifests itself as a loss of memory greater than expected for age, without meeting the diagnostic criteria Established for AD. This disease occurs in people with advanced ages. It is expected that by 2050 life expectancy in Colombia will exceed 79 years and with more than 20% of the population over 60 years.
OBJECTIVE: To describe the neuropsychological profile of a group of older adults with MCI.
METHODS: The sample consisted of 69 elderly adults with an average age of 71.79 years. Mini-Mental State Examination and Neuropsychological Assessment (Grover and Buschke Verbal Memory and Cognitive Cerad) were used.
RESULTS: In all, 49% of older adults assessed had a predominance of MCI-type amnestic multiple domains, 35% had non-amnestic MCI multiple domains and 8% met criteria for MCI-type amnestic single domain and non-amnesic single domain.
CONCLUSION: When comparing the results of other investigations and taking into account that the present study does not estimate prevalence, it is necessary to recognize the similarity in the results and the usefulness of the case study to make more accurate diagnoses.
Keywordsmild cognitive impairment, dementia, executive functions, attention, memory.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
3
ResumenINTRODUCCIÓN: El deterioro cognitivo leve (DCL) es una condición clínica entre el envejecimiento normal y un probable proceso demencial como la enfermedad de Alzheimer (EA), que se manifiesta por pérdida de memoria mayor a la esperada para la edad, sin cumplir con los criterios diagnósticos establecidos para la EA. Dicha enfermedad se presenta en personas con edades avanzadas. Se espera que para el 2050 la esperanza de vida en Colombia sea superior a 79 años y con más del 20% de la población por encima de los 60 años.
OBJETIVO: Describir el perfil neuropsicológico de un grupo de adultos mayores con DCL.
MÉTODOS: La muestra fue conformada por 69 adultos mayores con una edad promedio de 71.79 años. Se utilizaron instrumentos de tamizaje (Mini-Mental State Examination, Escalas de memoria, depresión y actividades de la vida diaria) y de evaluación neuropsicológica (Memoria Verbal de Grober and Buschke y el Cerad Cognitivo).
RESULTADOS: El 49% de los adultos mayores valorados presenta un predominio de DCL tipo amnésico múltiples dominios, el 35% presenta DCL tipo no amnésico múltiples dominios y el 8% cumple los criterios para DCL tipo amnésico único dominio y no amnésico único dominio.
CONCLUSIONES: Al comparar los resultados de otras investigaciones y teniendo en cuenta que en el presente estudio no se estima prevalencia, es necesario reconocer la similitud en los resultados arrojados y la utilidad que presenta el estudio de caso para realizar diagnósticos más acertados.
Palabras clavedeterioro cognitivo leve, demencia, funciones ejecutivas, atención, memoria.
Corresponding author:Ps. Cristian Villanueva-Bonilla. Facultad de Salud de la Universidad Surcolombiana, contiguo Hospital Universitario Hernando Moncaleano. Calle 9 carrero 4. Neiva, Huila, Colombia. Phone.: (57) (8) 8718310. Ext. 3137. Email: [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
4
Introduction
Methods
Mild cognitive impairment (MCI) is a clinical condition between normal aging and Alzheimer’s disease (AD), which is manifested by memory loss greater than expected for the age, without complying with the diagnostic criteria established for AD.1 MCI is associated with an increased risk of developing dementia; additionally, neuropsychological deficits are more common and clinically important in intervention and rehabilitation processes.2
The increase in life expectancy represents one of the most relevant aspects of our current society, resulting from a series of factors such as disease control, better nutritional conditions, hygiene, birth control, and decrease of mortality. According to the last census performed in Colombia, 6.3% of the population is over 65 years of age, corresponding to 2,612,508 inhabitants. The general population increased by an average of 1.9% per year (in the period 1990-2003), while the population aged over 80 grew at a rate of 4%.3
It is expected that by 2050, life expectancy in Colombia will exceed 79 years, and more than 20% of the population will be over 60 years old.4 These figures suggest that, as the population ages, diseases of this age such as dementia will also increase. Taking into account that senescence involves a series of changes, especially at the cognitive level, it is necessary to analyze these changes because not all of them are particular to old age. When it comes to alterations in cognitive functions with a predominance of important changes in memory, language, perception, and attention, some are due to the appearance of dementia.5,6 However, there is interindividual variability due to external factors such as educational level, gender, socioeconomic status, and eating habits.7
Considering the aforementioned, and due to the lack of clarity about recognizing a pre-dementia process that begins with MCI, Petersen et al.8
proposed diagnostic criteria to identify cognitive impairments that do not affect daily life activities
Participants
The sample consisted of 69 older adults with an average age of 71.79 years (SD=7.88) and 2.76 years of schooling (SD=1.04). The group consisted of 78% females and 22% males. Out of these participants, 74% presented medical history of risk of arterial hypertension (54%), diabetes (11%), cardiopathies (7%), and cerebrovascular disease (1%), and a family medical history of dementia (18%), Parkinson’s disease (7%), psychiatric background (3%), and other neurodegenerative conditions (2%). This sample of patients arises from the diagnostic process performed on 573 elderly people, of which 48% (275) did not present cognitive impairment, and 52% (298) were assessed in depth due to the suspicion of dementia in process. Of this remaining population (298), 23% were diagnosed with MCI according to the classification proposed by Petersen et al.8 The research protocol and
and suggest that MCI should be designated as a transition state between normal aging and dementia.9-12
This article presents the neuropsychological profile of a group of older adults with MCI at the Memory Clinic of the city of Neiva, Colombia. The objective of this clinic is to develop integral rehabilitation programs in mental health and offer a complementary treatment to the pharmacological, within the framework of investigative processes, led by a group at the Surcolombiana University. This approach includes the recovery or optimization of cognitive, occupational, social, and physical abilities, and is aimed at patients with cognitive disorders secondary to neurodegenerative diseases, vascular diseases, or sequelae of cranioencephalic trauma, and their families.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
5
active search strategies for information and word production from an established category.
Sustained attention. Search and visual tracking from the Trail Making Test (TMT) Part A, which allows to obtain the number of correct sequences in a maximum execution time of 120 seconds.21
Constructional apraxia and visual-spatial skills. Determined by the Rey-Osterrieth Complex Figure Test,22 which allows to evaluate the execution and to assess the capacity to generate planning strategies and imitative capacity.
Executive functions. Categorization, conceptualization, planning, organization, and abstraction are evaluated with tests such as the Wisconsin, Raven, and WAIS (Wechsler Adult Intelligence Scale) subtests.
Procedures
A screening process was initially performed to obtain the participants’ cognitive processes baseline. Once this was completed, if there was a suspected cognitive impairment in a participant (value less than 2 ± SD in each of the tests), we proceeded to a complementary neuropsychological evaluation with a protocol standardized by the Neuroscience group of the University of Antioquia,23 which was used in a study of the prevalence of dementia in Neiva’s population over 60 years of age.24
After the complementary neuropsychological assessment, all the cases were submitted to study by an interdisciplinary team (neurologist, psychiatrist, and neuropsychologist), whose purpose was to establish a diagnosis with the support of MCI international criteria.25
informed consent were approved by the Research Ethics Committee of the Faculty of Health of the Surcolombiana University.
InstrumentsScreening Instruments
Mini-Mental State Examination (MMSE).13 A cut-off point between 23 and 24 was used, with a sensitivity and specificity of 87% and 82%, respectively.
Subjective Memory Complaints Questionnaire.14 It is applied to one of the relatives and/or caregiver (who must be in permanent contact with the participant). The cut-off point is 19 and the maximum score is 45.
Lawton and Brody Scale. It evaluates the subject’s ability to lead an independent life, and studies the patient’s performance in order to correlate it with the cognitive skills he uses to access the context in which he is developing.15
Yesavage Geriatric Depression Scale. Allows a differential diagnosis with pseudodementia.16
Complementary neuropsychological evaluation tests
Grober-Buschke Test. Test of explicit verbal memory with controlled coding that allows to register free recall and cued recall, phonological and semantic, in the short and long term.17
Cognitive CERAD.18 Standardized in the Colombian population by the Neuroscience Research Group at the University of Antioquia.19 It evaluates the following cognitive domains:
Language. It utilizes the 64 figures of the Boston Naming Test.20 The subject must name objects, and the errors are classified into six categories: visual, semantic, visual-semantic, phonological, descriptive, and others.
Semantic fluency. It explores the generation of

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
6
Results
First, the sociodemographic characteristics of the participants are described. Next, the scores obtained in the neuropsychological tests are evaluated, and the performance of the subjects is established with respect to the MCI subtype in which they are located. Finally, an inter- and intra-group comparison is performed for MCI subtypes in order to establish significant differences in the performance of the cognitive spheres evaluated.
Neuropsychological profile
To determine the state of the cognitive functions of the participants, a descriptive analysis was performed for each of the cognitive domains evaluated.
The classification of optimal and low performance was based on a conversion of the gross scores in each of the tests that constitute the protocol used, taking into consideration the age, schooling, and the standardized scales for the Colombian population proposed by the research group of the University of Antioquia.19 The direct scores that were below average for the age and schooling were considered low performance, and those that were above the mean were considered optimal performance. Table 1 presents the performance of the participants in the cognitive domains.
Language
It was found that 56.8% of the evaluated subjects exhibited low performance in the tasks of denomination, semantic fluency, and phonological fluency, with only 43.2% presenting optimal performance.
Memory In the memory of constructional praxis, 64.9% of the evaluated subjects presented low performance; likewise, 70.3% obtained low performance in the Rey complex figure test. Meanwhile, 97.3%
displayed optimal performance in the recognition of a list of words.
Attention
In the Trail Making Test (TMT), 62.2% of those evaluated had low performance, and 86.5% used more time than expected for their age and schooling in the execution of the task, just as 78.4% did in the visual execution test.
Constructional abilities
Though 62.2% had an optimal performance, the time spent for the execution of the test in the majority of the subjects was high, which is to say, there is a slowing down in this process.
Executive functions
The 78.4% of the subjects obtained low performance in tests of calculation (WAIS) and the Wisconsin (64.9%); similarly, 62.2% of the population did not reach the number of categories indicated for age and schooling, and 59.5% had a low performance in the initial category index.
Functional status assessment
The results of the functional status scales complement the diagnostic criteria for MCI proposed by Petersen et al.8 Participants must be totally independent in their basic activities of daily living.
In the functional status assessment, 81.1% of the population shows no signs of depression, 64.9% of those evaluated are at level two of the functional state, and in relation to the other tests it is evident that the basic functions of daily life are not altered (100% of the population presents absence of disability), which is why they’re considered MCI.
Typifying the subtypes of MCI
Taking into consideration the analysis of the cognitive domains and the description of the

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
7
sample studied, participants were classified into subtypes of MCI. This was done through a rigorous review of the case and the standardized scales for the Colombian population, in order to verify the correspondence in 1.5 standard deviations of the expected mean for age and schooling in each of the tests, placing each subject in one of the sub-types to carry out an intragroup characterization with respect to age, schooling, origin, and gender. The distribution of the participants according to the classification of the subtypes of MCI is presented in Figure 1.
According to the classification with respect to MCI subtypes, we found in the evaluated sample a predominance of amnestic multiple domains with 49% belonging to this sub-type; the percentage for non-amnestic multiple domains was 35%, and 8% met the criteria for amnestic single domain as well as non-amnestic single domain.
In the amnestic single domain group, the most common age was that of 66.7% of participants, which were older than 70 years, and the remainder of the group’s age range was from 60 to 69 years old; the participants included in the amnestic multiple domains sub-type were 55.6% aged between 60 and 69 years, and 44.4% were over 70 years; within the non-amnestic single domain group, 33.3% were aged 60 to 69 years and 66.7% older than 70; with regards to non-amnestic multiple domains, the majority of the participants (76.69%) were over 70 years and the minority (23.1%) were in the range of 60 to 69 years of age.
One hundred percent of the participants in the amnestic single domain group had basic primary schooling. In the group for amnestic multiple domains, 88.9% had basic primary schooling and 11.1% had some middle school. In the non-amnestic single domain group, the whole group had basic primary schooling. In the non-amnestic multiple domains group, 69.2% had basic primary and 30.8% had some middle school.
Intra- and inter-group comparison of neuropsychological characteristics (MCI subtypes)The statistical calculation was performed to know
the compliance with normality parameters; the calculated p value was p> 0.05 according to the Shapiro-Wilk and the ANOVA statistic was applied. Table 2 shows the comparison of intragroup neuropsychological characteristics.
The ANOVA shows that there is a statistically significant difference between the groups in the tests that evaluate the field of visual execution and praxis; with p=0.001 in the recollection of constructional praxis, p=0.016 in the execution of constructional praxis, and p=0.027 in the execution of the Rey figure test, the significant difference clearly shows that the dependent variable is directly related to the independent variables in the study. With respect to the remaining tests, there are no significant differences between groups.
DiscussionThe human being, from the perspective of the life cycle, transits through different stages. In later adulthood, there are changes that relate to these stages, among which is the slowing down of cognitive processes such as attention, memory, visuoconstruction abilities, and executive functions. These changes can become significant and generate cognitive alterations that affect the older adult’s general performance. Experts in the subject have named these subtle changes MCI, which is characterized by a clinical picture consisting of the decrease of one or more cognitive functions without affectation in the activities of daily living.26
Petersen et al.8 propose as criteria for MCI diagnosis that there should be a cognitive concern on the part of the patient or an informant, a decline in cognitive functions, intact daily life activities, and no pathological, neurological, or psychiatric alteration to explain the deterioration. Furthermore, they classify MCI into four sub-types taking into consideration the cognitive domain: amnestic single domain MCI, amnestic multiple

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
8
Test applied Denomination
Semantic Fluency
Phonological Fluency
Memory of a list of words
Total Intrusions of the Word Listing
Recognition of the correct words list
Recognition of the incorrect words list
Recollection of constructional praxis
Rey–Osterrieth complex figure test (Total score)
Trail Making Test (Correct Answers)
Trail Making Test (Time)
Visual Execution Test (Correct Answers)
Visual Execution Test (Omissions)
Visual Execution Test (Time)
Constructional Praxis
Rey–Osterrieth complex figure test (Time)
Rey–Osterrieth complex figure test (Total score)
PerformanceLow
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Percentage 56.80%
43.20%
56.80%
43.20%
56.80%
43.20%
40.50%
59.50%
48.60%
51.40%
35.10%
64.90%
2.70%
97.30%
64.90%
35.10%
70.30%
29.70%
62.20%
37.80%
86.50%
13.50%
32.40%
67.60%
32.40%
67.60%
78.40%
21.60%
37.80%
62.20%
64.90%
35.10%
32.40%
67.60%
Lang
uage
Mem
ory
Atte
ntio
nV
isuo
cons
truc
tion
abili
ties
Table 1. Cognitive profile.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
9
Test applied Raven-A
WAIS Arithmetic
Wisconsin correct hits
Wisconsin errors
Wisconsin categories
Wisconsin perseverative responses
Wisconsin Initial Conceptualization Index
Wisconsin Total Attempts
PerformanceLow
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Low
Optimal
Complete
Incomplete
Percentage 40.50%
59.50%
78.40%
21.60%
64.90%
35.10%
45.90%
54.10%
62.20%
37.80%
32.40%
67.60%
59.50%
40.50%
83.80%
16.20%
Exec
utiv
e Fu
nctio
ns
TestMini-Mental
Denomination
Memory of list of words
Constructional Praxis
Recollection of list of words
Recollection of constructional praxis
Trail Making Test (Time)
Visual Execution Test (Time)
Rey–Osterrieth complex figure test (Time)
Rey–Osterrieth complex figure test (Total score)
Semantic Fluency
Phonological Fluency
Raven-A
WAIS Arithmetic
Wisconsin correct hits
Wisconsin errors
Wisconsin perseverative responses
F0.571
2.019
1.373
3.97
0.467
7.461
0.973
2.445
0.356
3.46
0.451
1.232
1.399
1.478
2.431
1.626
0.811
Sig.0.638
0.13
0.268
0.016
0.707
0.001
0.417
0.081
0.785
0.027
0.719
0.314
0.26
0.238
0.083
0.202
0.497
Table 2. ANOVA statistical values for the comparison of neuropsychological characteristics between the groups (MCI subtypes).
F = Statistical ValueSig. = Statistical Significance

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
10
domains MCI, non-amnestic single domain MCI, and non-amnestic multiple domains MCI.27
The participants classified in the non-amnestic single domain MCI group had low grades in tests of denomination, semantic fluency, phonological fluency, and visuoconstruction execution, evidencing predominantly cognitive affectation of language. The group classified in the subtype non-amnestic multiple domains presented low performance in denomination tests, sustained attention, executive functions, and visuoconstruction execution, which indicate more than one altered cognitive sphere.
In the analysis performed with ANOVA at the inter- and intra-group level, we verified significant differences between the groups in the execution of constructional praxis tests as much in memory as in copying, and in the elaboration of the complex Rey figure; this shows that the dependent variable meets the criterion of being directly influenced by the independent variables present in the study. This verifies that the initial classification, product of case studies, gives an important value to the clinical findings and helps establish a clear diagnostic criterion.28
In Colombia, research has shown how, over the years, cognitive processes deteriorate and may become clinically significant.29,30 In these studies, the cognitive profile of a group of older adults was established and it was concluded that, at an older age, performance declines in attention, language, memory, and executive functions; similarly, the neuropsychological evaluation showed that the participants presented a decline in cognitive spheres, such as language, with low performance in the denomination, phonological fluency, and semantics tests.
With regards to memory, the remarkably inferior performance was presented at the recollection of constructional praxis and the complex Rey figure; as for attention, low results were found in the performance of the trail making test, the visual execution test (time), and the complex Rey figure test. With respect to the executive functions, a low
performance was evident in the WAIS arithmetic and the Wisconsin card classification tests.
In different studies, it was found that patients with amnestic MCI had poor performance in memory tests (episodic predominance), while non-amnestic multiple domains had more difficulty with language tasks.31-33 These findings are similar to the present study because the evaluated subjects exhibited low performance in tests related with semantic and phonological fluency; in the amnestic multiple domains group, they had low performance in language, memory, and attention.
Regarding schooling as a variable to be analyzed regarding cognitive decline, many studies show that the higher the schooling, the lower the impairment in cognitive performance.11,33,34 This is corroborated in the present investigation because the range of schooling is low, having been considered a risk factor and a trigger of this clinical picture.
The affected areas in the participants in multiple domains MCI show decline in memory, attention, language, and visuoconstructional abilities, among others. These processes are also affected in the amnestic multiple domains MCI with a greater decline in amnestic processes. When comparing the aforementioned figures, and taking into account that the present study does not estimate prevalence, it is necessary to recognize the similarity in the results obtained and the usefulness of the case study to make more accurate diagnoses.28

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
11
Conflict of interest statementThe authors declare there are no relevant conflicts of interest in this study.
FundingThere was no particular source of funding for this scientific report.
Figure 1. Population distribution according to the classification of the MCI subtypes.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
12
1. Petersen R, Doody R, Kurz A, Mohs R, Morris J, Rabins P, et al. Current concepts in mild cognitive impairment. Arch Neurol. 2001; 58: 1985-1992.
2. Yanhong O, Chandra M, Venkatesh D, Mild cognitive impairment in adult: A neuropsychological review. Ann Indian Acad Neurol. 2013; 16: 310-318.
3. Ministerio de Salud y Protección Social. Diagnóstico preliminar sobre personas mayores, dependencia y servicios sociales en Colombia. 2008; Available from: https://www.minsalud.gov.co/proteccionsocial/Documents/Situacion%20Actual%20de%20las%20Personas%20adultas%20mayores.pdf.
4. Velásquez V, López L, López H, Cataño N, Muñoz. Efecto de un programa educativo para cuidadores de personas ancianas: una perspectiva cultural. Rev Salud Publica. 2011; 13: 610-619.
5. Bocanegra Y, Trujillo-Orrego N, Pineda D. Demencia y deterioro cognitivo leve en la enfermedad de Parkinson: una revisión. Rev Neurol. 2014; 59: 555-569.
6. Gainotti G, Quaranta D, Vita M, Marra C. Neuropsychological predictors of conversion from mild cognitive impairment to Alzheimer’s disease. J Alzheimers Dis. 2014; 38: 481-495.
7. Cooper C, Sommerlad A, Lyketsos C, Livingston G. Modifiable predictors of dementia in mild cognitive impairment: A systematic review and meta-analysis. Am J Psychiatry. 2015; 172: 323-334.
8. Petersen R, Smith G, Waring S, Ivnik R, Tangalos E, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. 1999; 56: 303-308.
9. Casanova-Sotolongo P, Casanova-Carrillo P, Casanova-Carrillo C. Deterioro cognitivo en la tercera edad. Rev Cubana Med Gen Integr. 2004; 20(5-6): 0-0.
10. Figuera L, Mulet B, Sánchez-Casas R, Estragó M, Cardús M, Alquézar A. Deterioro cognitivo anterior a la enfermedad de Alzheimer: tipologías y evolución. Psicothema. 2005; 17: 250-256.
11. Rodríguez N, Juncos-Rabadán O, Mayo D. Discriminación mediante marcadores cognitivos del deterioro cognitivo leve frente a envejecimiento normal. Rev Esp Geriatr Gerontol. 2008; 43: 291-298.
12. Valls-Pedret C, Molinuevo J, Rami L, Diagnóstico precoz de la enfermedad de Alzheimer: fase prodrómica y preclínica. Rev Neurol. 2010; 51: 471-480.
13. Folstein M, Folstein S, McHugh P. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12: 189-198.
14. Moreno A, Montañés P, Cano C, Plata S, Gámez A. Comparación de perfiles neuropsicológicos del Viejo-Joven (VJ) y el Viejo-Viejo (VV): envejecimiento normal y enfermedad de Alzheimer. Rev Asoc Colomb Gerontol Geriatr. 2005; 19: 776-796.
15. Lawton M, Moss M, Fulcomer M, Kleban M. A research and service oriented multilevel assessment instrument. J Gerontol. 1982; 37: 91-99.
16. Yesavage J, Sheikh J. 9/Geriatric Depression Scale (GDS) recent evidence and development of a shorter violence. Clin Gerontol. 1986; 5: 165-173.
17. Grober E, Merling A, Heimlich T, Lipton R. Free and cued selective reminding and selective reminding in the elderly. J Clin Exp Neuropsychol.1997; 19: 643-654.
18. Morris J, Heyman A, Mohs R, Hughes J, Van Belle G, Fillenbaum G, et al. The consortium to establish a registry for Alzheimer’s disease (CERAD): I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology. 1989; 39: 1159-1165
19. Aguirre-Acevedo D, Gómez R, Moreno S, Henao-Arboleda E, Motta M, Muñoz C, et al. Validez y fiabilidad de la batería neuropsicológica CERAD-Col. Rev Neurol. 2007; 46: 655-660.
20. García-Albea J, Del Viso S, Bernardos M. Test de Boston para el diagnóstico de la afasia: adaptación española. Bogotá: Editorial Medica Panamericana; 1996.
21. Kortte K, Horner M, Windham W, The trail making test, part B: cognitive flexibility or ability to maintain set? Appl Neuropsychol Adult. 2002; 9: 106-109.
22. Osterrieth P. The test of copying a complex figure: A contribution to the study of perception and memory. Arch Psychol. 1944; 30: 206-356.
23. Henao-Arboleda E, Aguirre-Acevedo D, Muñoz C, Pineda D, Lopera F. Prevalencia de deterioro cognitivo leve de tipo amnésico en una población colombiana. Rev Neurol. 2008; 46: 709-713.
24. Goodling M, Amaya E, Parra M, Ríos A. Prevalencia de las demencias en el municipio de Neiva 2003-2005. Acta Neurol Colomb 2006; 22: 243-248.
References
Revista Mexicana de Neurociencia September-October, 2017; 18(5):1-13
Original contributionMild cognitive impairment
13
25. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan E. Clinical diagnosis of Alzheimer’s disease Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984; 34: 939-939.
26. Henao-Arboleda E, Moreno-Carrillo C, Ramos V, Aguirre-Acevedo D, Pineda D, Lopera F. Caracterización de síntomas neuropsiquiátricos en pacientes con DCL de tipo amnésico en una población colombiana. Revista Chilena de Neuropsicología. 2010; 5: 153-159.
27. Albert M, DeKosky S, Dickson D, Dubois B, Feldman H, Fox N, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011; 7: 270-279.
28. Fisk J, Merry H, Rockwood K. Variations in case definition affect prevalence but not outcomes of mild cognitive impairment. Neurology. 2003; 61: 1179-1184.
29. Montañés P, Cano C, Pedraza O, Peñalosa M, Rubiano L, Gamez A. Demencia no Alzheimer: variante frontal de la demencia fronto-temporal. Revista de la Asociación Colombiana de Gerontología y Geriatría. 2003; 17: 539-583.
30. Hernández L, Montañés P, Gámez A, Cano C, Núñez E. Neuropsicología del envejecimiento normal. Revista de la Asociación Colombiana de Gerontología y Geriatría. 2007; 21: 992-1004.
31. Frutos-Alegría M, Moltó-Jordà J, Morera-Guitart J, Sánchez-Pérez A, Ferrer-Navajas M. Perfil neuropsicológico del deterioro cognitivo leve con afectación de múltiples áreas cognitivas. Importancia de la amnesia en la distinción de dos subtipos de pacientes. Rev Neurol. 2007; 44: 455-459.
32. López O. Clasificación del deterioro cognitivo leve en un estudio poblacional. Rev Neurol. 2003; 37: 140-144.
33. Migliacci, M., D. Scharovsky, and S. Gonorazky, Deterioro cognitivo leve: características neuropsicológicas de los distintos subtipos. Rev Neurol. 2009; 48: 237-241.
34. Mías C, Sassi M, Masih M, Querejeta A, Krawchik R. Deterioro cognitivo leve: estudio de prevalencia y factores sociodemográficos en la ciudad de Córdoba, Argentina. Rev Neurol. 2007; 44: 733-738.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
14
Fractal characterization of normal cerebral ventricles in t2-wheigthed magnetic resonance imaging
Caracterización fractal de ventrículos cerebrales normales en imágenes de resonancia magnética ponderadas en T2
Original contribution
Alejandro Velasco,1 Javier O Rodríguez,2 Edgar G Ordonez-Rubiano,3 Signed E Prieto,4 Catalina S Correa,4 Germán Forero,5 Laura Mendez,1 Hebert Bernal,1 Laura P Valero,1 Natalia Hoyos.1
1 Faculty of Medicine – Universidad Militar Nueva Granada. Bogotá, D.C. Colombia.2Faculty of Medicine – Universidad Militar Nueva Granada, Centro de Investigaciones Clínica del Country. Bogotá, D.C. Colombia.3 Fundación Universitaria de Ciencias de la Salud (FUCS) – Hospital de San José, Hospital Infantil Universitario de San José. Bogotá, D.C. Colombia.4 Universidad Militar Nueva Granada, Centro de Investigaciones Clínica del Country. Bogotá, D.C. Colombia.5 Universidad Militar Nueva Granada. Bogotá, D.C. Colombia.
Abstract
Introduction: The fractal geometry describes adequately the irregularity of the natural objects such as the cerebral ventricles, which are irregular structures that can be characterized through the Box-Counting method.
Objective: This research aims to develop a new methodology of geometric characterization of the cerebral ventricles, based on the fractal geometry for the analysis of normal cerebral ventricles.
Methods: Based on the Box-Counting method, the fractal dimensions of the both lateral ventricles of a normal adult were obtained. Sequential cephalic-caudal 4mm axial slices were acquired on T2-WI, and the differences and similarities of the lateral ventricles were established using the Ventricular Intrinsic Mathematical Harmony.
Results: The fractal dimension of the left lateral ventricle had values between 1.0641 and 1.3599, and in the right lateral ventricle had values between 0.8931 and 1.3219.
Conclusion: A new morphometric measure of the cerebral ventricles was developed based on the fractal geometry for its use as an objective and reproducible measure.
Keywordsbrain, cerebral ventricle, fractal, fractal geometry, lateral ventricles.
Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
15
ResumenIntroducción: Las dimensiones fractales permiten caracterizar matemáticamente la irregularidad de las formas naturales como los son las estructuras cerebrales. Los ventrículos cerebrales son objetos irregulares que pueden ser estudiados mediante esta geometría.
Objetivo: La investigación pretende desarrollar una caracterización en el espacio fractal de Box-Counting del ventrículo cerebral normal del adulto.
Métodos: Con fundamento en el método Box-Counting, se analizó la estructura geométrica de las imágenes obtenidas mediante TAC de un sujeto normal. Para ello se tomaron las imágenes de cortes cada 4mm y se midieron las dimensiones fractales de los ventrículos cerebrales, determinando además la Armonía Matemática Intrínseca Ventricular entre las imágenes consecutivas de cada ventrículo.
Resultados: Las dimensiones fractales presentaron valores entre 0.8931 y 1.3599, con valores de AMIV entre 0 y 2, mostrando la capacidad de la metodología de caracterizar la estructura irregular de los ventrículos cerebrales.
Conclusiones: : Los resultados constituyen una nueva medida morfométrica para los ventrículos cerebrales, que permitió establecer medidas características de normalidad de utilidad como referencia para determinar la presencia de alteraciones ventriculares.
Palabras clavecerebro, ventrículo cerebral, fractal, geometría fractal, ventrículos laterales.
Corresponding author: Edgar G Ordóñez-RubianoPhone: (+57)-300-643-9837, (+57)-(1)-287-0087Fax: (+57)-(1)-287-5878E-mail: [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
16
IntroductionDue to an impossibility to perform trustable Euclidian measures that could be associated with structures with complex and irregular shapes in different scales,1,2 Benoit Mandelbrot in 1975 developed the fractal geometry, geometry that allows characterization of the irregular objects. This advance allowed him to work in a measure of the irregularity of objects, denominated as Fractal Dimension (FD). For non-mathematical fractals, characterized by superposition between its parts, considered as wild fractals, the FD is calculated with the Box-Counting method.3,4
There are different examples of application of fractal geometry in medicine, including laboratory and clinical sets: evaluation of diagnosis, follow-ups, and results of any therapeutic intervention.5–9
Even though, in many cases, determining the FD by itself is not enough to establish differences for clinical practice, making it necessary to establish mathematical concepts for its evaluation. For example, like it was in an experimental model of coronary re-stenosis, where the morphometric of histology was evaluated, based on the processing of the FDs of the arterial layers, using the term of Arterial Intrinsic Mathematical Harmony (AIMH),10 that can differentiate healthy versus sick arteries, with an accuracy of 10^30. This made place to a generalization of all possible fractal arterial structures, from the normal lumen to the total occlusion of the arterial lumen.11 In other clinical project, the fractal dimension of the branching of the left coronary artery from diastole to systole in angiography was evaluated, differentiating patients with and without severe arterial occlusive disease.12 Likewise, different diagnoses of the left cardiac ventricle in ventriculogram13 and echocardiography14 have been established, relating its FDs. Different authors have also shown its clinical applications in erythrocytary diagnosis,15 cervical uterine paraneoplastic lesions,16 and cardiac hemodynamics.17 Fractal geometry has been applied to the measurement of cerebral structures, analysis of electroencephalograms,
and functional Magnetic Resonance Imaging (MRI) as well.18,19 Thus, demonstrating that the fractal geometry is a complementary important tool able to characterize states of normality and disease.20,21
The cerebral ventricles are evaluated with MRI for clinical practice through the use of lines for determining lengths and using Euclidian formulas for establishing volumes or approximated areas. Clinical MRI is based on the electromagnetic activity of spins of active atomic nuclei of hydrogen (protons and neutrons). Voxel-based MRI, by the way, could be very accurate for establishing measures, based on three-dimensional occupation of matter.22
However, these measurements do not take into account completely the irregularity of cerebral structures, thus some important information can be ignored that could be determinant for clinical decisions and are based on statistic probabilistic significance. There is no other published work regarding the fractal characterization of the cerebral ventricles. This paper aims to develop a new objective and reproducible histological morphometric measurement for the characterization of the cerebral ventricles with the application of the fractal geometry.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
17
Methods and Materials
DefinitionsFractal: Irregular object, from the Latin “fractus”: irregular, fractioned.
Fractal dimension: A not-dimensional numeric measurement that determines the degree of the irregularity of a fractal.
For this work, it was used the definition for FD of Box-Counting:
Where N (2-k) is a function of the grade of partition of the k grid, and corresponds to the number of squares occupied by the object in the grid with partition 2-k.
Procedure
Sequential cephalic-caudal 4mm axial slices of a T2-WI sequence of a non-contrast MRI of the head were acquired from a healthy patient with a General Electric SIGNA HD.XT. 1.5 Tesla. All images were processed in software developed by previous researches for the calculation of FDs with the Box Counting method.12,11 The borders of the both lateral ventricles were delineated. Posteriorly, the number of squares occupied by the ventricles in the different slices was established. Based on these values the FD of the Box-Counting was obtained for each ventricle in the different slices using the equation D (see definitions). Finally, the Ventricular Intrinsic Mathematical Harmony (VIMH) was calculated, mathematically defined as the degree of similarity or difference between two FDs when comparing the two units and its significant digits. Two FDs present a VIMH of 0 if they have differences between the units. For example with 0,786 and 1,234: there is a VIMH of 1 if they have an equal value between the units
)2()2(
222)2()2( )1(
1
)1(
k
k
kk
KK
NN
LogLogLogNLogN LogD
Results
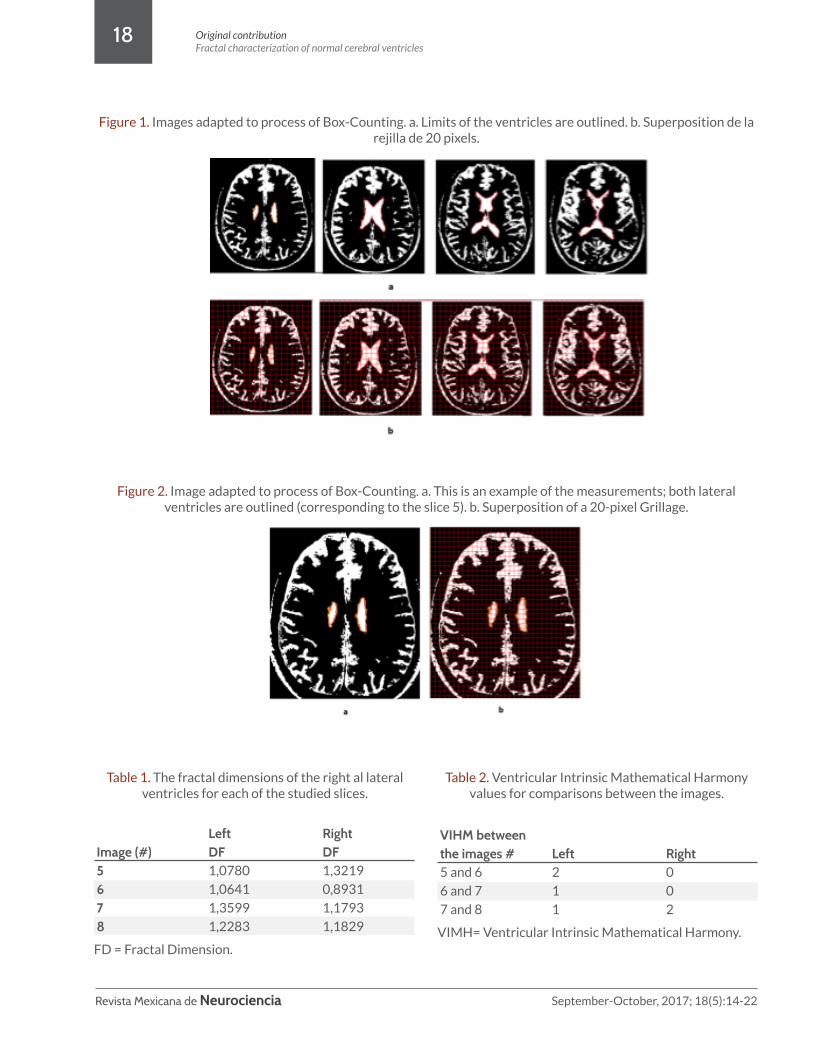
It was found that the cerebral lateral ventricles were observed in 4 out of 8 the adapted MRI slices. (Figure 1) For the both lateral ventricles of each 4 images the FD was obtained. The FD presented variations between 0,8931 and 1,3598. For the right lateral ventricles FDs ranged between 0,8931 and 1,3219 (Table 1), while the values of the degree of irregularity of the left ventricles were between 1.0641 and 1.3598. The degree of similarity between the parts of the ventricles were obtained when finding the VIMH for each ventricle in the different slices, as each image is a section of a three dimensional object. The values of the VIMH (Table 2) were higher for the lateral left ventricle on two of the three comparisons, showing that there is a greater degree of similarity between the parties to the left ventricle compared with the right. Additionally, the comparison of the images of the right ventricle of the slices 7 and 8 showed a greater self-organization than those of the left ventricle of the same slice, but in the other two comparisons the left ventricles had greater VIHM values.
but differentiate between each other in the first significant digit, as it is with 1,242 and 1,433; therefore, an IVMH of 2 will correspond to equal values to the unit and the first significant digit, as it is the case of 1,563 and 1,543, and then in the same way sequentially.
Bioethical considerations
This work meets the standards of medical ethics committees of the sponsoring institution of research and with the Helsinki Declaration of 1975, updated in 2000. It complies with the scientific, technical and administrative standards for health research, based on the resolution No. 008430 of 1993, and specifically title 11 concerning research on human beings, to be classified in the category of research without risk, as mathematical calculations on results of tests are done made a voluntary without coercion, not affecting the patient and respect their integrity and anonymity.23
Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
18
Figure 1. Images adapted to process of Box-Counting. a. Limits of the ventricles are outlined. b. Superposition de la rejilla de 20 pixels.
Figure 2. Image adapted to process of Box-Counting. a. This is an example of the measurements; both lateral ventricles are outlined (corresponding to the slice 5). b. Superposition of a 20-pixel Grillage.
Table 1. The fractal dimensions of the right al lateral ventricles for each of the studied slices.
Table 2. Ventricular Intrinsic Mathematical Harmony values for comparisons between the images.
Image (#)5678
LeftDF1,0780
1,0641
1,3599
1,2283
RightDF1,3219
0,8931
1,1793
1,1829
FD = Fractal Dimension.
VIHM between the images #5 and 6
6 and 7
7 and 8
Left2
1
1
Right0
0
2
VIMH= Ventricular Intrinsic Mathematical Harmony.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
19
DiscussionThis is the first work where the Box-Counting method was applied for quantification of the degree of irregularity of the cerebral ventricles. This can be useful as a new reference for future studies of measuring of ventricles in patients with different diseases. Therewith, a new measurement for evaluation of the self-organization between the measures of the same ventricle in different slices was performed. This can also be a reference of normality in the future, for detecting the presence of ventricular alterations. However, this measure should be performed in larger series of healthy individuals to increase accuracy.
The measures conventionally used in a clinical fashion, especially in the Emergency Room, are based on Euclidean measurements and on the use of formulas to make approximations regarding the volume or size of specific structures. Even though, because of the irregularity of the structures, there is potentially important clinical information that can be lost by using Euclidean geometry on irregular objects. Additionally, the objectivity and the reproducibility of the measurements are difficult, which may involve variations in inter- and intra-observer interpretation.In contrast, the measurements obtained by fractal geometry are an objective and reproducible method suited to the characteristics of brain structures, which provides clinical information that can be useful not only to assess the initial state of a patient but also for the purpose of monitoring their changes over time.
Fractal geometry has been successfully used for the objective characterization of different cellular and histological structures in medicine. For example, Hayano et al. 6, 24 performed fractal measures over Computed Tomography Angiography images of the liver, and made direct correlations with the degree of heterogeneity of tumors, for the evaluation of anti-angiogenic treatment, and for the survival of patients with hepatocellular carcinoma. In the same way, Fiz et al.7 used fractal measures of ultrasound images of pulmonary nodules, differentiating benign and malignant nodules. Meanwhile, Talu
performed fractal measures that could differentiate the microvasculature of the retina of patients with diabetic macular edema, which allowed making an earlier diagnosis of the disease.9 Other comparisons between fractal dimensions of parts of a structure, or the whole structure, or its dynamics have been studied in other experimental and clinical phenomena.10, 12-14, 25
In the brain, the fractal characterization was performed with MRI, obtaining important information regarding normal changes that occur during aging.26 Reishofer et al.27 also observed differences between FDs of cerebral structures in MRI of healthy patients and patients with arteriovenous malformations, giving information about the clinical behavior of these lesions. Besides, Wang et al. made fractal analysis of electroencephalograms of ictal and inter-ictal states, achieving a characterization of each one, with a high sensibility (>90%), demonstrating that it can be used for the automatic identification of seizures.28
In this paper, we present a fractal characterization of cerebral lateral ventricles. Furthermore, the concept of VIMH is implemented, whereby variations of fractal auto-organization of the cerebral ventricles can be observed in different slices. In further studies, there should be an implementation of this methodological analysis of different neurological diseases and cerebral lesions demonstrating changes in geometry of cerebral structures, in order to develop diagnostic and therapeutic clinical applications.
This work is based on a form of physical-mathematical non-causal thinking, which seeks to establish the underlying laws of the different phenomena within the cerebral ventricles. This research perspective has established diagnoses and predictions in areas such as immunology,29 molecular biology,30 infectology,31,32 neonatal and adult cardiology,33,34
and predicting epidemics,35 obtaining results of clinical, experimental and public health utility. Further studies are needed to implement the fractal characterization of the cerebral ventricles and VIMH in the clinical context of patients with diseases of the central nervous system.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
20
Conflict of interest The authors declare no conflict of interest.
Funding SourceProduct of MED-1344, project funded by the Research Vice-Rector of the Military University Nueva Granada. Validity 2014. Bogotá, Colombia.
Conclusions
Aknowledgements
This research is based on physical and mathematical theories that provide a new tool for clinical practice for a future adequate evaluation of the irregularity of the cerebral ventricles using the Box-Counting method and the VIMH.
Thanks to the Asociación Colombiana de Neurocirugía.
Thanks to the Universidad Militar Nueva Granada. Special thanks to Elsa Cardenas, Vice President of Research, Dr. Yanneth Méndez Academic Vice Chancellor, Dr. Jorge Luque, dean of the Faculty of Medicine and to Nydia Rojas, director of the Research Center of the Faculty of Medicine for his constant support and cooperation in our research.
We also thank the Research Center of the Clínica del Country, especially to Doctors Tito Tulio Roa, Director of Medical Education, Jorge Ospina, Medical Director, Alfonso Correa, Director of the Research Center, and Dr. Adriana Lizbeth, epidemiologist. To Sandra Rodriguez, nurse, and Silvia Ortiz, Head Nurse research Center, for their constant support to our research.
In dedication to our children. In dedication to Laura Rivera-Osorio.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
21
1. Mandelbrot B. ¿Cuánto Mide la Costa de Gran Bretaña? Los Objetos Fractales. Barcelona: Tusquets Editores; 1987. 27–50.
2. Mandelbrot B. The Fractal Geometry of Nature. Barcelona: Tusquets Editores; 2000. 3. Peitgen H-O, Jürgens H, Saupe D. Limits And Self Similarity. Chaos and Fractals. New York: Springer-
Verlag; 1992. 135–82. 4. Peitgen H, Jürgens H, Saupe D. Length, Area and Dimension: Measuring Complexity and Scaling
Properties. In: Peitgen H, Jürgens H, Saupe D, eds. Chaos and Fractals. New York: Springer-Verlag; 1992. 183–228.
5. Al-Kadi OS. A multiresolution clinical decision support system based on fractal model design for classification of histological brain tumours. Comput Med Imaging Graph. 2015;41:67-79.
6. Hayano K, Yoshida H, Zhu AX, Sahani D V. Fractal analysis of contrast-enhanced CT images to predict survival of patients with hepatocellular carcinoma treated with sunitinib. Dig Dis Sci. 2014;59(8):1996–2003.
7. Fiz JA, Monte-Moreno E, Andreo F, et al. Fractal dimension analysis of malignant and benign endobronchial ultrasound nodes. BMC Med Imaging. 2014;14:22.
8. Metze K. Fractal dimension of chromatin: potential molecular diagnostic applications for cancer prognosis. Expert Rev Mol Diagn. 2013;13(7):719-735.
9. Tălu S. Multifractal geometry in analysis and processing of digital retinal photographs for early diagnosis of human diabetic macular edema. Curr Eye Res. 2013;38(7):781–792.
10. Rodriguez J, Mariño M, Avilan N, et al. Medidas fractales de arterias coronarias en un modelo experimental de reestenosis. Armonía matemática intrínseca de la estructura arterial. Rev Colomb Cardiol. 2002;10:65–72.
11. Rodríguez J, Prieto S, Correa C, et al. Theoretical generalization of normal and sick coronary arteries with fractal dimensions and the arterial intrinsic mathematical harmony. BMC Med Phys. 2010;10(1):1–6.
12. Rodríguez J, Prieto S, Correa C, et al. Fractal diagnosis of severe cardiac dysfunction Fractal dynamic of the left coronary branching. Rev Colomb Cardiol. 2012;19(5):225–32.
13. Rodríguez J, Prieto S, Correa C, et al. Fractal diagnosis of left heart ventriculograms Fractal geometry of ventriculogram during cardiac dynamics. Rev Colomb Cardiol. 2011;19(1):18–24.
14. Rodríguez J, Prieto S, Ortiz L, et al. Mathematical diagnosis of pediatric echocardiograms with fractal dimension measures evaluated through intrinsic mathematical harmony. Rev Colomb Cardiol. 2010;17(2):79–86.
15. Correa C, Rodríguez J, Prieto S, et al. Geometric diagnosis of erythrocyte morphophysiology. Int J Med Med Sci. 2012;3(11):715–720.
16. Prieto S, Rodríguez J, Correa C, et al. Diagnosis of cervical cells based on fractal and Euclidian geometrical measurements: Intrinsic Geometric Cellular Organization. BMC Med Phys. 2014;14(1):2.
17. Rodríguez J, Correa C, Melo M, et al. Chaotic cardiac law : Developing predictions of clinical application. Int J Med Med Sci. 2013;4(2):79–84.
18. Spasic S, Culic M, Grbic G, et al. Spectral and fractal analysis of cerebellar activity after single and repeated brain injury. Bull Math Biol. 2008;70(4):1235–1249.
19. Lahmiri S, Boukadoum M. Alzheimer’s disease detection in brain magnetic resonance images using multiscale fractal analysis. ISRN Radiol. 2013;2013:627303.
20. Di Ieva A, Grizzi F, Jelinek H, et al. Fractals in the Neurosciences, Part I: General Principles and Basic Neurosciences. Neuroscientist. 2013;20(4):403–417.
21. Di Ieva A, Esteban FJ, Grizzi F, et al. Fractals in the Neurosciences, Part II: Clinical Applications and Future Perspectives. Neuroscientist. 2015;21(1):30–43.
22. Bitar R, Leung G, Perng R, et al. MR Pulse Sequences : What Every Radiologist Wants to Know but Is Afraid to Ask. Radio Graphics. 2006;26(2):513–538.
23. Ministerio de Salud de Colombia. Resolución número 8430 DE 1993. 1–19.24. Hayano K, Lee SH, Yoshida H, et al. Fractal analysis of CT perfusion images for evaluation of
antiangiogenic treatment and survival in hepatocellular carcinoma. Acad Radiol. 2014;21(5):654–660.
25. Rodríguez J. New diagnosis aid method with fractal geometry for pre-neoplasic cervical epithelial cells. Rev UDCA Actual y Divulg Científica. 2011;1(14):15–22.
Bibliography

Revista Mexicana de Neurociencia September-October, 2017; 18(5):14-22
Original contributionFractal characterization of normal cerebral ventricles
22
26. Liu JZ, Zhang LD, Yue GH. Fractal dimension in human cerebellum measured by magnetic resonance imaging. Biophys J. 2003;85(6):4041–4016.
27. Reishofer G, Koschutnig K, Enzinger C, et al. Fractal dimension and vessel complexity in patients with cerebral arteriovenous malformations. PLoS One. 2012;7(7):e4114–4118.
28. Wang Y, Zhou W, Yuan Q, et al. Comparison of ictal and interictal EEG signals using fractal features. Int J Neural Syst. 2013;23(6):1350028.
29. Rodríguez J, Bernal P, Álvarez L, et al. Plasmodium falciparum MSP-1 and EBA-140 peptides prediction of binding to HLA class II probability, combinatory and entropy applied to peptide sequences. Inmunología. 2010;29(3):91–9.
30. Rodríguez J, Bernal P, Prieto S, et al. Theory of malaria peptides with high-affinity binding to red blood cells. Theoretical predictions of new binding peptides and predictive mutations of critical amino acids. Inmunología. 2010;29(1):7–19.
31. Rodríguez J, Prieto S, Correa C, et al. Predictions of CD4 lymphocytes’ count in HIV patients from complete blood count. BMC Med Phys. 2013;13(1):3.
32. Rodríguez J, Prieto S, Correa C, et al. Teoría de conjuntos aplicada al recuento de linfocitos y leucocitos: predicción de linfocitos T CD4 de pacientes con virus de la inmunodeficiencia humana/sida. Inmunología. 2013;32(2):50–56.
33. Rodríguez J, Prieto S, Domínguez D, et al. Mathematical-physical prediction of cardiac dynamics using the proportional entropy of dynamic systems. Int J Med Med Sci. 2013;4(9):370–381.
34. Rodríguez J, Prieto S, Flórez M, et al. Physical-mathematical diagnosis of cardiac dynamic on neonatal sepsis : predictions of clinical application. Int J Med Med Sci. 2014;5(5):102–108.
35. Rodríguez J. A method for forecasting the seasonal dynamic of malaria in the municipalities of Colombia. Rev Panam Salud Pública. 2010;27(3):211–218.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
23
Relationship between atherosclerotic disease and disc herniation in patients with integral conservative management
Relación entre la enfermedad ateroesclerótica y hernia discal en pacientes con manejo conservador integral
Original contribution
Jorge Rendón-Félix,1* Diana Paola Urias-Valdez,1 David Gustavo Rodriguez-Cisneros,1 Eloy Ovando-Sanders.1
1 Centro de la Columna Vertebral. Zapopan, Jalisco, México.
Abstract
Introduction: Atherosclerosis is the leading cause of general mortality and hospital morbidity. The prevalence of lumbar intervertebral disc degeneration related to atherothrombotic pathology has been increasing, and the incidence of low back pain reaches its peak after 45 years. A relationship between the decrease in apolipoprotein A1 and hypertriglyceridemia as related factors, as well as hypertension, elevated LDL levels and a high Framingham score, but it has yet to be seen if the treatment is compromised in that aspect.
Methods: Retrospective observational study in patients with herniated disc treated with combined conservative therapy, comparing their effectiveness depending on the cardiovascular risk presented.
Results: A total of 171 patients were analyzed. 25.7% presented adequate weight, 41.5% overweight and 32.8%, obesity. In all, 42.7% had hypertension, 19.3% diabetes mellitus, 15.3% smoked, no patients had physical activity and 24% had a high or very high cardiovascular risk. There was no difference between the results presented with the combined conservative treatment.
Conclusion: In addition to the physical components that cause disc herniation, there is a compromised circulatory component, which was not affected after the combined conservative treatment, which is why it is recommended the timely treatment of the herniated disk and its risk factors.
Keywordsatherosclerosis, herniated disk, conservative treatment.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
24
Corresponding Author: Jorge Rendón-Félix.Centro de la Columna Vertebral.Av. San Ignacio 123, Col. Jardines de San Ignacio.Zapopan, Jalisco. C.P. 45040 México.e-mail: [email protected]
Resumen
Introducción: La aterosclerosis constituye la primera causa de mortalidad general y morbilidad hospitalaria. La prevalencia de la degeneración del disco intervertebral lumbar relacionada a la patología aterotrombótica ha ido creciendo, y la incidencia de dolor lumbar alcanza su pico después de los 45 años. Se ha encontrado una relación entre la disminución de la apolipoproteína A1 y la hipertrigliceridemia como factores relacionados, así como la hipertensión, niveles elevados de LDL y un puntaje elevado en el Score Framingham, pero no se ha visto si el tratamiento está comprometido en ese aspecto.
Métodos: Estudio observacional retrospectivo en pacientes con hernia discal tratados con terapia conservadora combinada, comparando su efectividad dependiendo del riesgo cardiovascular que presentaran.
Resultados: Un total de 171 pacientes fueron analizados. 25.7% presentaban peso adecuado, 41.5% sobrepeso y 32.8%, obesidad. Un 42.7% tenían hipertensión arterial, 19.3% diabetes mellitus, 15.3% tabaquismo, ningún paciente realizaba actividad física y 24% tuvieron un riesgo cardiovascular alto o muy alto. No hubo diferencia entre los resultados presentados con el tratamiento conservador combinado.
Conclusión: Además de los componentes físicos que causan hernia discal, se aprecia un componente circulatorio comprometido, el cual no se vio afectado tras el tratamiento conservador combinado, por lo que se recomienda el tratamiento oportuno de la patología y de los factores de riesgo.
Palabras claveaterosclerosi, hernia discal, tratamiento conservador.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
25
IntroductionAtherosclerosis is the leading cause of general mortality and hospital morbidity. It is a disease of the metabolism that responds to the persistent aggression and exponential intensity that affects the connective tissue of the arterial wall, in which a series of physical, hemodynamic, biochemical, metabolic, humoral, inflammatory, and coagulation alterations finally end up damaging the arterial wall with a scar, which is the atherosclerotic lesion.1
Since this ischemic injury is capable of causing pain and degeneration of the structures involved, atherothrombotic disease of the arteries that irrigate the spine has received increased consideration as one of the possible underlying factors for both lower back pain and herniated discs. Atheromatous plaques begin to appear in the abdominal aorta in adulthood, and 20 years later, 10% of the population in developed countries will have advanced lesions in the abdominal aorta. The prevalence of lumbar intervertebral disc degeneration (IDD) related to atherothrombotic pathology has been increasing steadily in early adulthood, and the incidence of lumbar pain (LP) increases linearly to reach its highest prevalence after the age of 45. Although IDD and LP are fairly common, one can develop without the other.
The most rapid increase in the number of complications (necrosis, ulcerations, thrombi, calcifications) occurs between the ages of 44-64 years old.2,3 These lesions tend to accumulate at the bifurcation and around the orifices of the branched arteries. The lumbar spine, supplied by these branched arteries, may be affected if the arteries become clogged. The segmental lumbar arteries supply the first to the fourth lumbar segments. The fifth lumbar segment is supplied by branches of the middle sacra, and by tributaries of the iliolumbar arteries. In addition to the lumbar vertebrae, these arteries also irrigate surrounding structures such as intervertebral discs, nerve roots, and paraspinal muscles. The spinal cord is less dependent on these arteries because its main supply of blood does not come from the lumbar
spine.4 In contrast, the intervertebral disc,5 as the largest avascular structure in the body, relies on the passive diffusion of the peripheral arteries for nourishment. Therefore, the disc may be a risk zone for anyone with atherosclerotic disease. Computed tomography angiography (CTA) offers better spatial resolution to visualize the atherosclerotic narrowing of small arteries, such as the lumbar artery.
After the preliminary findings of a necropsy study in 1993,5,6 suggesting an association between decreased blood supply to the lumbar spine and lower back pain, atherosclerosis and cardiovascular risk factors have received increased consideration as possible underlying factors for back disorders.
Lifestyle factors, such as smoking or diet, may play a significant role in spinal problems as they promote vascular disease and play an underlying role in degenerative changes and pain.
Other cardiovascular risk factors have been studied concerning lumbar intervertebral disc degeneration and lower back pain’s relationship with atherosclerosis. Hemingway7 found a considerable decrease in Apolipoprotein A1 (Apo 1, the major protein component of high-density lipoproteins (HDL) which is responsible for the activation of the lecithin-cholesterol acyltransferase (LCAT) which binds to the HDL receptor to stimulate inverse cholesterol transport and to intervene in the structure) in a sample of 4,886 office workers between 35 and 55 years old, in both genders; and in men an important hypertriglyceridemia associated with incapacity for work due to a disease secondary to back pain. Leino-Arjas8-10 found an association between elevated triglycerides and lower back pain in three separate studies.
In addition, high blood pressure, high cholesterol, elevated LDL, and increased carotid intima and middle layers have been found to be significantly associated with lower back pain.
An increase in the investigation of modifiable and non-modifiable risk factors in patients

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
26
with cardiovascular risk leads to a reduction in morbidity and mortality. This risk assessment uses the Framingham model, tables, and SCORE, which can easily be adapted to the conditions, resources, and priorities of different countries, and take into account the heterogeneity in cardiovascular disease mortality, as can be seen in Figure 1.11
In an effort to seek a more rapid and effective recovery for patients, the combined conservative strategies achieve an accelerated recovery of patients in a more effective and less invasive way (through anti-inflammatory drugs, ozone therapy, and targeted rehabilitation),12-15 leaving surgery as a last resort and obtaining good results in the majority of patients with herniated disc.
Due to the tendency for combined conservative treatment of the herniated disc and to the relationship of the disease with vascular diseases, it was decided to seek a relationship between both and to seek benefits through conservative combined treatment of disc herniation.
Material and methods Ethical considerationsA retrospective observational study was performed in patients with herniated disc undergoing conservative combined treatment at the Spine Center in 2015, with the objective of comparing the effectiveness of the technique used in different groups of patients depending on cardiovascular risk and presented comorbidities.
Inclusion criteria were: 18-65 years old patients with clinical and imaging diagnosis of herniated disc, who completed a minimum of 15 sessions of combined treatment of parenteral therapy, rehabilitation, and ozone therapy in the Spine Center. Additionally, they duly signed an informed consent to an anonymous review of their progress with this therapeutic modality.
Patients outside this age range or with a different
diagnosis were excluded, as well as patients who did not complete the 15 combination treatment induction sessions or who have been inconstant, patients who presented an inconvenience or an adverse event in their treatment or in their condition, patients with incomplete records or who did not authorize the review of their clinical file through the informed consent. Response variables were assessed after administration of 15 sessions of conservative combined treatment using an visual analogue scale for pain (VAS; 0 = no pain and 10 = most severe pain) and the search for a relationship between weight, body mass index (BMI), and risk of cardiovascular event related to the present symptomatology.
All patients were standardized in each session with intravenous medications (analgesics, anti-inflammatories, multivitamins and homotoxicology), ozone therapy and physical therapy sessions (electrotherapy, local ultrasound, massage therapy, thermotherapy, hydrotherapy, traction, Williams exercises, and neuromuscular bandaging).
The study was conducted in accordance with the principles of the 1989 Declaration of Helsinki, with all its modifications, and under the norms and guidelines of Mexico’s General Health Law. As this was a retrospective observational study, it did not require a review by the Institution’s Ethics Committee. All the patients gave their informed consent duly signed.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
27
Figure 1. Cardiovascular risk using Framingham Score.11
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
AGESCOREMan-1
0
1
2
3
4
5
6
7
Woman-9
-4
0
3
6
7
8
8
8
Points0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
<17
Men2%
2%
3%
4%
5%
6%
7%
9%
13%
16%
20%
25%
30%
45%
>45%
>45%
>45%
<45%
Women1%
1%
2%
2%
2%
2%
2%
3%
3%
3%
4%
7%
8%
11%
13%
15%
18%
>20%
STEP 1
Hard CHD Risk
NO
YES
DIABETESSCOREMan0
2
Woman0
4
STEP 2
NO
YES
SMOKERSCOREMan0
2
Woman0
2
STEP 3
<160
160-99
200-239
240-279
>280
Total CholesterolSCOREMan-3
0
1
2
3
Woman-2
0
1
1
3
STEP 4
<35
35-44
45-49
50-59
>60
Systolic
<120
120-129
130-139
140-159
>160
Diastolic<80 80-84 85-89 90-99 >100
HDL CHOLESTEROLSCOREMan2
1
0
0
-2
Woman5
2
1
0
-3
STEP 5
Table for the quantification of the
risk in function of the score
When the systolic and diastolic blood pressure throw different scores, the higher value is used.
Risk of serious cardiovascular
event or “hard” event (10 years)
BLOOD PRESSURE MEN
STEP 6
0 Points
0 Points
1 Point
2 Points
3 Points
Systolic
<120
120-129
130-139
140-159
>160
Diastolic<80 80-84 85-89 90-99 >100
BLOOD PRESSURE WOMEN
-3 Points
0 Points
0 Points
2 Points
3 Points

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
28
Results
Out of 593 patients treated in 2015, 171 met the inclusion criteria. The average age of the patients was 59.7 ± 13.7 years, their weight 75.7 ± 15.9 kg, the pain (measured by VAS) at the beginning was of 7.3 ± 1.9, and 2.4 ± 2 at the end, and there was no discernible difference related to the risk factors. Cholesterol levels were 193.4 ± 40.8, LDL levels of 116.2 ± 81.8, HDL levels of 52.4 ± 13, and the average risk of cardiovascular event was 14.8 ± 13.3.
Out of the 171 patients, 25.7% presented an
Figure 2. Comorbidities in the study group.
DM: diabetes mellitus.
adequate weight, 41.5% were overweight, and the remaining 32.8% had some degree of obesity (22.2% obesity type I, 5.8% obesity type II and 4.7% obesity type III). It should be mentioned that 42.7% of the patients suffered arterial hypertension, 19.3% had diabetes mellitus, 15.3% used tobacco, no patient performed any physical activity prior to the radiculopathy, and 24% presented a high or very high cardiovascular risk (Framingham score >20). These results are better illustrated in Figure 2.
Comorbidity (%)
45
40
35
30
25
20
15
10
5
0
Normal w
eight
Overweight
Obesity
Hypertensio
n
DM type 2
Tobacc
o use
Activity

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
29
Conflict of interest statementThe authors of this manuscript declare no conflict of interest with the subjects mentioned here.
FundingThe authors of this manuscript declare that they have received no funding whatsoever that could interfere with the subjects mentioned herein.
ConclusionIt can be observed that the herniated disc, in addition to the physical factors that cause it, has an important circulatory component, which was not so affected when comparing the results after the combined conservative treatment. Adequate recognition of symptoms caused by disc herniation, together with a correct diagnosis, timely treatment, and control of comorbidities, is indispensable for a favorable prognosis; therefore, a timely and adequate diagnosis and comprehensive treatment of the patient’s condition and its underlying circulatory diseases, is highly recommended.
Discussion
It is increasingly common to hear the term “herniated disc” and the increase in the incidence of cases with this pathology is alarming because the onset of symptoms is occurring at an earlier age and the patient seeks treatment until the disease worsens, which makes its handling much more complicated.
Simultaneously, atherosclerosis has become one of the great epidemics of the 21st century. Twenty-five years ago, when the International Conference on Primary Care was held by the World Health Organization (WHO), a list of eight essential elements was drawn up, where no reference was made to the treatment or prevention of conditions such as heart disease or stroke. At the time, cardiovascular diseases and other non-communicable diseases were considered characteristic of industrialized countries (in fact, they were called “diseases of the rich”) were attributable to ways of life radically different from those prevailing in most parts of Africa, Asia and many other places of the developing world, but the reality is quite different: cardiovascular diseases have not only appeared in practically all countries but have also spread remarkably; this increasing burden poses a real threat of hindering social and economic development. Risk factors serve as indicators of future health status, and five out of ten of the main global threats are related to non-communicable diseases such as arterial hypertension, tobacco use, alcohol use, hypercholesterolemia, obesity, or overweight.16
Results show there is a correlation between atherosclerosis, metabolic syndrome, and
microcirculation ailments such as herniated discs. The fact that more prevalence of arterial hypertension has been observed (42.7%) than that of diabetes mellitus (19.3%), and the fact that the patients respond to intravenous treatment indicates that the circulation of the intervertebral disc can be more compromised by atherosclerosis than by ischemia (without ruling out the latter), but more circulation studies have to be done to confirm it and to be able to regulate approaches to future treatments.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):23-30
Original contributionAtherosclerosis and herniated disc
30
1. Santana-López, S., Montero-Díaz, R., Sánchez-Fuentes, A.L., Valdés-Vento, A.C, Vidal Vega, I. Caracterización de los factores de riesgo de la aterosclerosis. Rev. Ciencias Médicas de Pinar del Río. Enero-febrero, 2016; vol 20 (1):136-141
2. Vihert AM. Atherosclerosis of the aorta in five towns. Bull World Health Organ. 1976;53:501e8. 3. Zhdanov VS, Sternby NH, Vikhert AM, Galakhov IE. Development of atherosclerosis over a 25 year
period: an epidemiological autopsy study in males of 11 towns. Int J Cardiol. 1999;68:95e106.4. Chiras J, Morvan G, Merland JJ. The angiographic appearances of the normal intercostal and
lumbar arteries. Analysis and the anatomic correlation of the lateral branches. J Neuroradiol. 1979;6:169e96.
5. Beckworth WJ, Holbrook JF, Ward L, Welle JR, Foster LG. (2016). Atherosclerotic Diseaseand Its Relationship to Lumbar Degenerative Disc Disease, Facet Arthritis and Stenosis Using CT Angiography. 05/12/2016, de EMORY University School of Medicine Sitio web: http://www.painmed.org/2016posters/poster101.pdf
6. Kauppila LI, Tallroth K. Postmortem angiographic findings for arteries supplying the lumbar spine: their relationship to lowback symptoms. J Spinal Disord. 1993;6:124e9.
7. Hemingway H, Shipley M, Stansfeld S, Shannon H, Frank J, Brunner E, et al. Are risk factors for atherothrombotic disease associated with back pain sickness absence? The whitehall II study. J Epidemiol Community Health. 1999;53:197e203.
8. Leino-Arjas P, Kaila-Kangas L, Solovieva S, Riihima¨ki H, Kirjonen J, Reunanen A. Serum lipids and low back pain: an association? A follow-up study of a working population sample. Spine. 2006;31:1032e7.
9. Leino-Arjas P, Solovieva S, Kirjonen J, Reunanen A, Riihima¨ki H. Cardiovascular risk factors and low-back pain in a long-term follow-up of industrial employees. Scand J Work Environ Health. 2006;32:12e9.
10. Leino-Arjas P, Kauppila L, Kaila-Kangas L, Shiri R, Heistaro S, Helio¨vaara M. Serum lipids in relation to sciatica among Finns. Atherosclerosis. 2008;197:43e9.
11. Guía de Práctica clínica: Detección y estratificación de factores de riesgo cardiovascular. México: Secretaria de Salud; 2009.
12. Ernst E1, Schmidt K. Homotoxicology--a review of randomised clinical trials. Eur J Clin Pharmacol. 2004 Jul;60(5):299-306.
13. Andreula CF, Simonetti L, de Santis F, Agati R, Ricci R, Leonardi M. Minimally Invasive Oxygen-Ozone Therapy for Lumbar Disk Herniation. AJNR Am J Neuroradiol. 2003;24:996-1000.
14. Zhang Y, Ma Y, Jiang J, Ding T, Wang J. Treatment of the lumbar disc herniation with intradiscal and intraforaminal injection of oxygen-ozone. J Back Musculoskelet Rehabil. 2013;26(3):317-22.
15. Ovando-Sanders E, Salazar-García JL, Ortiz-Watson LA. Reporte de 147 casos de éxito en el Centro de la Columna Vertebral a base de colchicina homeopática, ozono y terapia física. Rev Mex Med Fis Rehab. 2014;26(1):24-37.
16. Yusuf S. Global burden of cardiovascular diseases. Circulation. 2001, 104:2746-53.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
31
Autism spectrum disorder review: diagnosis and treatment update
Revisión del trastorno del espectro autista: Actualización del diagnóstico y tratamiento
Revision
Lucía Lisseth Vázquez-Villagrán,1 Carlos Daniel Moo-Rivas,1 Elisael Meléndez-Bautista,1 Juan Sebastián Magriñá-Lizama,1 Nina Isabel Méndez-Domínguez.2
1 Estudiante de Medicina. Campus ciencias de la salud. Universidad Marista de Mérida. 2 Médico Cirujano, Maestra de ciencias de Ecología Humana, Dra. En Ciencias de la Salud Investigadora Posdoctorante en Centro de investigación y de Estudios Avanzados del IPN. Profesora Titular, Universidad Marista de Mérida, Campus de Ciencias de la Salud.
Abstract
Autism spectrum disorder (ASD) is considered a multifactorial etiology during child’s neurodevelopmental process covering the following clinical groups including: a) autistic disorder b) Rett´s Syndrome c) childhood disintegrative and d) widespread development. Affects 1 to 2/1000 people and is characterized by impaired in: a) social behavior b) deficit verbal and nonverbal c) restricted interests and repetitive behaviors, and d) changes in the scope of activities. The TEA persists lifelong and shows heterogeneity, ranging from mild personality changes to severe disability. The importance of this review is to provide a timely diagnosis in order to obtain a more favorable prognosis for the patient. The sections to treat are the symptoms, diagnosis and treatment. The relevance of this review is to provide and update information about ASD, so that it could guide the reader to fully understand the characteristics of this disease and the advances that have been developed to take appropriate treatment and improve the quality of patient’s life.
KeywordsASD, Autism spectrum disorder, Review, Diagnosis, Treatment.
Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
32
Corresponding author: Nina Isabel Méndez Domínguez.Antigua carretera a Progreso Km 6, Cordemex, 97310 Mérida, Yucatán, México. Phone: +52 (999) 942-9400.E-mail: [email protected]
Resumen
El Trastorno del Espectro Autista (TEA) es considerado una etiología multifactorial del neurodesarrollo infantil que abarca los siguientes grupos clínicos entre ellos: a) el trastorno autista b) los trastornos de Rett c) desintegrativo infantil y d) generalizado del desarrollo. Afecta entre 1 a 2/1000 personas y se caracteriza por alteración en: a) comportamiento social b) déficit verbal y no verbal c) intereses restrictivos y conductas repetitivas, así como d) alteraciones en el margen de actividades.
El TEA persiste toda la vida y muestra una gran heterogeneidad, que varía desde modificaciones leves de la personalidad hasta discapacidad grave. La importancia de la siguiente revisión es procurar un diagnóstico oportuno con el fin de obtener un pronóstico más favorable para el paciente. Las secciones a tratar serán la sintomatología, diagnóstico y tratamiento.
La relevancia del presente artículo radica en proporcionar al lector información ampliada y actualizada sobre el TEA, de manera que sirva como una herramienta para que el lector comprenda en su totalidad las características de esta patología y los avances que se han desarrollado para poder llevar un tratamiento adecuado y mejorar la calidad de vida del paciente.
Palabras claveTEA, Trastornos del espectro autista, Revisión, Diagnóstico, Tratamiento.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
33
IntroductionAutistic spectrum disorder (ASD) affects one in every 700 to 1000 people; one in every 1000 presents classic autism symptomatology, generally affecting three to four boys per each girl at a global level. Autism disorder is a neurodevelopmental disorder under whose autism spectrum disorder umbrella encompasses five clinical groups including Rett syndrome, Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorder; it affects cognitive, emotional, and social skills and competency. The specific etiologies and neural bases of autism remain largely unknown; it has been proposed that alterations in multiple genes in combination with environmental factors constitute the cause for the development of the autism phenotype.1,2,3
Its manifestations are mainly cognitive and behavioral of variable severity, characterized by early dysfunction in communication and social interactions, presenting with repetitive, restrictive, stereotyped patterns of behavior and loss of interest in diverse activities. Additionally, it is frequently accompanied by impairments in adaptive functioning, sensory processing disorder, aggression, or self-injury. It is generally diagnosed clinically with the presence of central symptoms based on the criteria established by the DSM-V. Treatment of ASD must be individualized and there has been growing interest in the role of various pharmacological treatments.4,5,6,7
The importance of early detection and diagnosis by primary care physicians is that they know the disease and, should there be clinical suspicion, to refer the patient to a specialist or be treated, aside from supporting the adaptation of the patient with ASD to their environment. The social impact of timely intervention of patients has a positive effect on their environment and community when receiving the necessary support; the prognosis is very variable. It has been observed that patients with autism and their families have a lower quality of life directly related to higher traits of autism and deficits of executive functions.8,9,10
Definition Autism spectrum disorder occurs in the early years of life. It is considered a multifactorial origin etiology, where genetics play an important role. Included in the category of ASD, based on the update of the DSM-V, are all generalized developmental disorders under the same diagnosis. These include autism disorder or Kanner syndrome, Rett syndrome, childhood disintegrative disorder, Asperger syndrome, and pervasive developmental disorder not otherwise specified / atypical autism.8,9,11
The ASD comprise a heterogeneous group of clinical expressions, whose main cause is unknown. Autism’s clinical manifestations include social interaction and communication deficiencies with persistent deterioration, restricted and repetitive patterns of behavior, as well as deficiencies in social-emotional reciprocity, deficits in nonverbal communicative behaviors, and in the ability to develop, maintain, and understand relationships. Intellectual disability is frequent, with or without affecting of the cognitive competence and skills. It should be noted that the manifestations of ASD vary according to the severity of the autistic condition, level of development, and chronological age.12,13,2
ClassificationBased on the classification of ICD.10 and the new update of the DSM-V regarding the types of autism (see Table 1), the ASD encompasses all generalized developmental disorders under a single diagnosis (except for Asperger disorder, which has been excluded from ASD in the DSM-V) that varies in age of onset, as well as in clinical presentation considering variations in cognitive, linguistic, behavioral and social skills.13 (See Table 2)
The heterogeneity of the autistic disorder is due to different etiologies or combination of factors believed, according to the DSM-V, to be associated with known medical or genetic conditions, environmental factors, or other neurodevelopmental, mental or behavioral disorders. Primary autism is considered to be likely caused by an indeterminate genetic factor, and
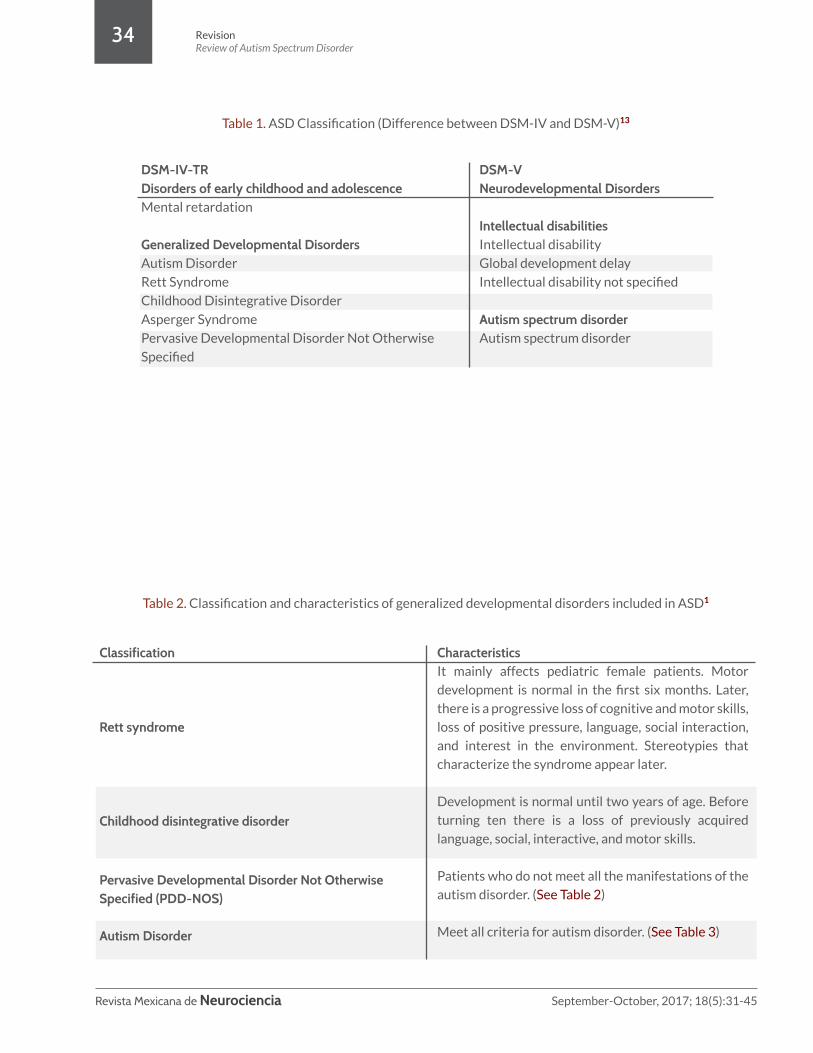
Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
34
Table 1. ASD Classification (Difference between DSM-IV and DSM-V)13
Table 2. Classification and characteristics of generalized developmental disorders included in ASD1
DSM-IV-TRDisorders of early childhood and adolescenceMental retardation
Generalized Developmental DisordersAutism Disorder
Rett Syndrome
Childhood Disintegrative Disorder
Asperger Syndrome
Pervasive Developmental Disorder Not Otherwise
Specified
DSM-VNeurodevelopmental Disorders
Intellectual disabilitiesIntellectual disability
Global development delay
Intellectual disability not specified
Autism spectrum disorderAutism spectrum disorder
Classification
Rett syndrome
Childhood disintegrative disorder
Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS)
Autism Disorder
CharacteristicsIt mainly affects pediatric female patients. Motor
development is normal in the first six months. Later,
there is a progressive loss of cognitive and motor skills,
loss of positive pressure, language, social interaction,
and interest in the environment. Stereotypies that
characterize the syndrome appear later.
Development is normal until two years of age. Before
turning ten there is a loss of previously acquired
language, social, interactive, and motor skills.
Patients who do not meet all the manifestations of the
autism disorder. (See Table 2)
Meet all criteria for autism disorder. (See Table 3)

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
35
secondary autism associated with known genetic alterations.13
PrevalenceIt has been observed that the male-to-female ratio of incidence of this disorder is of 4:1, regardless of social or cultural classes. In Spain, during the seventies, autism was considered a disorder of low prevalence; however, it has since increased to 60/10,000 inhabitants suffering from ASD. American sources mention this number has increased from 1/1000 in 1998 to a 2002 accepted prevalence of 1/150-1/200 patient with ASD.14,15
Clinical manifestationsThe clinical manifestations of patients with ASD are divided into three areas: a) deterioration in social interactions, b) verbal and nonverbal communication, and c) behavioral patterns and restricted and repetitive interests.16 (See Table 3)
The clinical manifestations of autism are usually present between the year and a half and two years of age that remain stable during the preschool and school years. Typically, the average interval from the time parents begin to worry until they ask for help can be more than a year. During the first year the most consistent behavior in children with autism is: not responding to their name and not looking at faces or doing so rarely. During the second year, there is absence of interest in sharing experiences and inability to pay attention. The following are considered precocious signs: a) frequent tantrums and low tolerance to change; b) absence of babbling at nine months old; c) no signaling or gesticulation at one year of age, unresponsive when called by name; d) won’t utter single words at sixteen months of age; e) absence of symbolic play at a year and a half; f) absence of two-word phrases at two years old. Any of the aforementioned findings should motivate a thorough investigation, considering
Manifestations
Deterioration in social interactions
Deterioration in communication
Deterioration in patterns of behavior, and restricted and repetitive interests
Characteristics• Patients may or may not show affection when inter-acting socially.• Older pediatric patients often do not point things out, instead, use eye contact. • They present lack of social interest, with an absence of friends, according to their age, or prefer to play alone.• In early childhood, some children do not babble and cannot compensate for this language deficit with facial expressions or gestures.• Immediate or delayed echolalia.• Concern about specific parts of toys.• Behavior is restricted, repetitive, with stereotyped interests (child does not change toys or objects).• They can demonstrate atypical and impulsive behav-ior such as with objects, through unusual gestures, or with self-harming actions.• They repeat the same question several times, regard-less of having received an answer, or participate in repetitive games.• They are concerned about their family, school environment, or routines.
Table 3. Manifestations of autism.16

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
36
autism one of the possible diagnoses. In a third of cases, the development is normal between the first and second year, and may later experience a gradual or unexpected regression, backtracking on previous development. Symptoms may also not be apparent to parents or teachers until four or six years of age.17
Patients may have cognitive abilities with moderate, severe, or profound mental retardation in IQ tests. With normal intellectual ability, the cognitive and language skills are often preserved; characteristically, they tend to misunderstand nonverbal messages, show difficulty in interpersonal relationships, especially when in a group, and possess few manipulative skills, are expressionless, speak with an abnormal tone, and focus on repetitive conversation topics that are interesting only to them.17
DiagnosisAutistic spectrum disorder can be reliably diagnosed in children from the age of two years, with early intervention being beneficial for these patients. However, the average age for diagnosis is between three and six years. It has been postulated that one of the causes of this delay has to do with the great difficulty inherent in diagnosing these disorders at very early ages. Several factors contribute to this: a) symptom presentation is very variable and changes with age, b) social deficits and language delays may not be identified until the child begins to relate to peers in preschool.6,16
It is evident that the early detection of this disorder is crucial to aid the prognosis, the child’s subsequent development, and the family’s ability to adequately handle the difficulties that arise from this situation. We currently consider that around the year of life, and even earlier, the red flags for this disorder can already be identified. These signs are: little or no interest in visual contact, absence of orientation response when the child is named, absence of pointing, and absence of showing objects. This is fundamental because the earlier the diagnosis is made, the faster the child and his family can be given adequate help in order to promote an increase of achievements in
functional abilities, communication, and intellectual processes.2,18
In early care, the diagnostic process of ASD should be based on the child’s evolutionary history information, for which interviews will be conducted with parents, educators, and significant people in the child’s life. Information will be collected regarding the child’s neurobiological development, communicative, social, and motor developmental milestones, and on the appearance of the first autistic symptoms, as well as on their environment, their relationship style, behavior patterns, interactions with adults and children of the same age, level of participation in structured group dynamics, and their adaptation in the nursery or pre-school.18
The American Academy of Neurology (AAN) in their report on identification and diagnosis of ASD, emphasize that a double approach is required. (See Algorithm 1) The first level deals with the strict monitoring of the neurodevelopment of children to discover any change or deviation from normal, for which it is desirable that doctors remain alert from the birth of the child. The second level in the diagnosis is to define the clinical characteristics of the child and then carry out three phases of evaluation.19
Phase 1, Identification of possible cases: the objective is to recognize the manifestations or to verify the observations of the parents regarding their child’s communication, behavior, and social interaction.19
Phase 2, Global evaluation: seeks to observe the consistency and the significance of the child’s neurological and behavioral manifestations, and to confirm the observations and concerns of the parents or physicians who referred the child to the specialist.19
Phase 3, Specific diagnosis: establishes the definitive diagnosis of ASD and defines its type. For this purpose the information provided by the parents and the specialists who have seen the patient is contrasted, applying the necessary tests

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
37
Level 1Routine developmental review (pediatric follow-up)
Absolute indication for immediate evaluation:
• No babbling, no signaling or other gestures at 12 months;
• No unique word utterances at 16 months.
• No use of spontaneous 2-word phrases (no echolalia) at 24 months.
• Any loss of language or social skills at any age.
Level 2. Diagnosis and evaluation of autismFormal diagnostic procedures.
Interview tools: GARS, PIA, PDDST-stage3, ADI-R.
Observation instruments: CARS, STAT, ADOS-G.
Clinical diagnosis: DSM-V.
Extended medical and neurological evaluation.
Specific evaluations to determine the development profil.e
Speech-language-communication, cognitive and adaptive behavior, occupational therapy,
evaluation of family resources, and neuropsychological, behavioral, and academic evaluation.
Extended laboratory evaluation (only if indicated).
Pruebas metabólicas y genéticas, electrofisiología, imágenes neurológicas.
Reevaluate at next consult
Refer to level 2, as indicatedRefer to early intervention or to the local school
district. Proceed to level 2
Level 1. Lab InvestigationAudiologist final assessment
Lead detection (if there are signs of pica)
Specific evaluation to detect autism
(E.g. CHAT, PDDST-stage1, Australian scale, etc.)
Algorithm 1. Diagnostic Levels for Autism.1

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
38
to correlate the data with the criteria of the DSM-V diagnostic manual.19
Caution is advised in the diagnosis of ASD due to nonspecific manifestations in different age groups. Early non-specific signs in infancy or small children include irritability, passivity, and difficulty sleeping and eating.16
Since autism does not have a diagnostic biological marker the judgment is strictly clinical, based on the behavioral manifestations given by the criteria of the DSM-V (see Table 4). The DSM-V manual mentions that the main features of autistic spectrum disorder are the persistent deterioration of social and reciprocal communication and social interaction (criteria A), and the behavioral patterns, interests, or restrictive and repetitive activities (criteria B). These symptoms are present since early childhood and limit or impede daily functioning (criteria C and D). The stage in which functional deterioration is obvious will vary according to the characteristics of the individual and his/her environment. The manifestations of the disorder also vary greatly depending on the severity of the autistic condition, the level of development, and the chronological age.13, 20
There is a wide variety of instruments for the diagnosis of autism spectrum disorder. The three most prominent are: a) The Modified Checklist for Autism in Toddlers (M-CHAT) is best applied in pediatric primary care during the recognition of the healthy child at a year and a half of age, the moment at which the symptoms become measurable and remain stable until preschool age between 16 and 30 months. It is a questionnaire addressed entirely to the parents consisting of 23 questions (see Table 5). b) The Autism Observation Scale for Infants (AOSI) studies children who have an older sibling with autism. c) The Childhood Autism Spectrum Test (CAST), for children between four and six years of age, is also a diagnostic tool.17
For definitive diagnostic confirmation there is a broad consensus on the use of validated tools such as The Autism Diagnostic Interview-Revised (ADI-R) and The Autism Diagnostic Observation Schedule (ADOS).17
Complementary testsLaboratory. Laboratory tests almost never provide data for diagnosis, but in many cases are performed to rule out the symptomatic forms of autism, especially if there is an associated history of lethargy, cyclic vomiting, early epileptic seizures, dysmorphic features, and mental retardation.1
Neurophysiology. The electroencephalogram (EEG) tends to be normal in autistic children who do not have convulsions or clinical evidence of concomitant cerebral pathology.17
Neuroimaging. In idiopathic forms of autism, neuroimaging is usually normal; in some cases it observes hypoplasia of the posterior vermis and cerebellar hemispheres, reduction of the volume of the cerebral parietal lobes, and thinning of the corpus callosum.1
Genetic testing is not a routine study method for autism, and neither is metabolic screening, because less than 5% of patients will have an underlying metabolic disorder.8
Differential diagnosisWhen a patient has some of the symptoms, a differential diagnosis should be made to rule out pathologies that may present similar symptoms, such as sensory anomalies, genetic or physical illnesses, since certain disorders or diseases may be accompanied by symptoms of autism and may require specific treatments. Among the most common are mental retardation / developmental delay, language developmental disorders, learning disabilities, hearing disorders, Landau-Kleffner syndrome, anxiety, and obsessive-compulsive disorder.16
TreatmentThe objectives to keep in mind, in order to correctly treat children with autism spectrum disorder, should include: the patient’s functional independence and quality of life, seeking to reduce the negative consequences of the disorder itself, facilitate development and learning of the individual, promote socialization, reduce disruptive

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
39
Table 4. DSM-V Diagnostic criteria.13
A. Persistent deficits in social communication and social interaction across multiple contexts, as manifested in the following symptoms, whether current or past (examples are illustrative, not exhaustive):1. Deficiencies in social-emotional reciprocity vary, for example, from an abnormal social approach and failure of normal conversation in both directions, to a decrease in shared interests, emotions, or affections, to failure to initiate or respond to social interactions.2. Deficiencies in nonverbal communicative behavior used in social interaction vary, for example, from poorly integrated verbal and non-verbal communication, to anomalies of visual contact and body language, or deficiencies in the understanding and use of gestures, to a total lack of facial expression and non-verbal communication.3. Deficiencies in the development, maintenance, and understanding of a relationship range from, for instance, difficulties adjusting behavior in various social contexts, to difficulties sharing imaginative games, the ability to make friends, or even a lack of interest in other people.Specify current severity:Magnitude is based on impairments of social communication and repetitive and restricted behaviors.
B. Repetitive and restricted patterns of behaviors, activities, and interests, manifested in at least two of the following symptoms, whether current or past (examples are illustrative, not exhaustive):1. Motor movements, stereotyped or repetitive use of objects or speech (e.g., simple stereotyped motor movements, aligning objects, spinning objects, echolalia, idiosyncratic phrases).2. Insistence on sameness, inflexible adherence to routines or patterns of verbal and non-verbal ritualized behavior (e.g., extreme discomfort in the face of small changes, difficulties with transitions, rigid thought patterns, greeting rituals, need to always follow the same path, or eat always the same thing).3. Highly restricted, obsessive interests that are abnormal because of their intensity or focus (e.g., excessive attachment or preoccupation with unusual objects, overly circumscribed or persevering interests). 4. Sensory hyper or hypo-reactivity or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain or temperature, adverse response to sounds or specific textures, excessive smelling or touching of objects, fascination with lights or rotating objects).Specify current severity: Magnitude is based on social and communicative disturbances and on the presence of repetitive and restricted patterns of behavior.
C. Symptoms must be present in the early developmental period (although they may not fully manifest until the demands of the environment exceed the child's abilities, or can be dissimulated in later life through learned skills).
D. Symptoms cause clinically significant changes in social, occupational, or other important areas of current functioning.
E. These alterations are not best explained by the presence of an intellectual disability (intellectual development disorder) or a global developmental delay. Intellectual disability and autism spectrum disorder often co-occur; to make a diagnosis of comorbidity of autism spectrum disorder and intellectual disability, social communication must be below expectations as a function of the general level of development.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
40
Note: Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger syndrome, or pervasive developmental disorder not otherwise specified should be diagnosed with autism spectrum disorder. Individuals who have marked deficits in social communication but whose symptoms do not meet the criteria for autism spectrum disorder should be evaluated for social (pragmatic) communication disorder.Specify if:
It is accompanied or not by intellectual disability. It is accompanied or not by a language disorder.It is associated with a medical or genetic condition or with a known environmental factor (coding note: use an additional code to identify the medical or genetic condition).It is associated with another mental or behavioral neurodevelopmental disorder (coding note: use additional code(s) to identify the associated mental or behavioral neurodevelopmental disorder).With catatonia (coding note: use additional code 293.89 [F06.1] catatonia associated with autism spectrum disorder to indicate the presence of concurrent catatonia).
behaviors, and educate relatives and teachers to have an active participation in these during the intervention.21
It is necessary, in order to carry out the treatment, the participation of a multidisciplinary team that includes specialists with knowledge of diagnosis and treatment of autistic spectrum disorders, relatives, teachers, and people who maintain direct contact with the child that generate some influence through interactions.21
Intervention-based practices include clinical-educational strategies based on research of relevant interest groups, which can be taken into consideration while planning appropriate treatment for the patient.22 (See Table 6).
There are global models of treatment that have shown positive results when applied; however, each of these models differ in terms such as the age of onset in which to start the application, the influence of the environment, actions regarding the answers obtained, individualization of the child, and reinforcements to apply. It is necessary to evaluate all variables that influence the way the treatment will be handled to be able to choose an adequate model to apply in order to achieve an adequate interaction of the child with its environment, developing as well the language and socialization skills.22
Appropriate pharmacological treatment for children with autism spectrum disorder should take into consideration the general basic care that any pediatric patient receives, such as prevention and immunization campaigns. Recommendations directed to a specific pharmacological treatment are based only on case studies and literature, which can be taken into consideration during the selection of the appropriate drug in each case.21
The main symptoms to be treated in patients with autism spectrum disorder are: epilepsy, aggression, hyperactivity, irritability, attention deficit, poor social interaction, obsessions, and anxiety. Individual treatment should take into account factors such as: to start with monotherapy to avoid the occurrence of any adverse drug reaction; administer low doses and adjust them according to the effect it produces in the patient; follow-up; take into consideration the pharmacokinetic and pharmacodynamic factors of each drug.23
A pharmacological treatment administering oxytocin, a neuropeptide related to social attachment and the development of bonding via a single intranasal dose, was linked to facilitation in the processing and retention of social information and recognition of emotion in relation with language intonation; however, this type of therapy is still subject to investigation and hasn’t produced sufficient data to verify its effectiveness and to consider it an adequate treatment.24

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
41
1. Does your child enjoy being rocked, bounced on your knees, etc.? 2. Is your child interested in other children? * 3. Does your child like to climb to places, such as to the top of the stairs? 4. Does your child enjoy playing peekaboo, hide-and-seek, or other similar games? 5. Does your child pretend to, for example, serve a cup of tea or simulate other things? * 6. Does your child use the index finger to signal, to ask for something? 7. Does your child use the index finger to point, to show interest in something? * 8. Does your child know how to play with small toys (such as cars or blocks) and not just put them in their mouth, touch them, or throw them away? 9. Has your child ever brought an object to show you something? * 10. Does your child look into your eyes for more than a second or two? 11. Has your child shown hypersensitivity to noise (for instance, covering the ears)? 12. Does your child laugh in response to your face or your smile? 13. Does your child imitate you (for example, when you make a face)? 14. Does your child answer to his/her name when called? * 15. If you point to a toy in the room, does your child look at it? * 16. Does your child walk? 17. Does your child make strange movements with the fingers close to his/her face? 18. Does your child look at the things you’re looking at? 19. Does your child try to call attention towards his/her own activities? 20. Have you ever wondered if your child is deaf? 21. Does your child understand what people say? 22. Does your child sometimes stare ahead or wander aimlessly? 23. Does your child look at your face to check your reaction when finding something unfamiliar?
* These are the critical questions, the most indicative of the existence of autistic features.
Table 5. M-CHAT. 6
Table 6. Intervention Practices.22
Preventive behavioral
Behavioral interventionMoldingJoint attention
Natural contextParental interventionPeer learningPivotal behaviors
Strategies for autonomyWork systemsVisual support
Give different types of visual, physical and verbal
stimuli to achieve the desired response.
Look for alternatives to reduce behavioral problems.
Reinforce the desired behavior by imitating it.
Increase the response to the perceived behavior of
other people.
Teaching of daily activities.
Family participation.
Interactions with other children.
Motivation, spontaneous initiation, response to
multiple signals, and autonomy.
Favor the child’s independence.
Organize areas for play and other activities.
Use visual cues to maintain a behavior or ability.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
42
Another treatment of interest is secretin, which is a gastrointestinal polypeptide involved in digestion, and that in intravenous infusion therapies has been associated with an improvement in socialization, cognitive, and communication skills thanks to its intervention as a neurotransmitter; however, like other hormonal therapies, there isn’t enough evidence to be able to demonstrate its true therapeutic value. On the other hand, melatonin is a neurotransmitter whose main therapeutic function is the induction of sleep in patients with insomnia problems. Specific effects of its application in autism have not been demonstrated, its use is based on simply treating sleep disorders in children with autism to produce a sedative effect, but its excessive use can cause adverse effects such as dizziness, lethargy, and headache.25
Among the main drugs used in the treatment of autism are typical antipsychotics such as haloperidol, thioridazine, chlorpromazine and the atypical risperidone, olanzapine and clozapine, whose use is more common. These are used with the objective to treat the child’s behavioral problems by blocking the D2 dopaminergic channels, causing a diminished reaction to stimuli known as “neuroleptic syndrome,” observed as calm and quiet behavior in the child. In turn, some atypical antipsychotics also exhibit an antagonism of type 2A receptors for serotonin, aside from their effect on the D2 channels. It is important to individualize the patient when these drugs are administered, since there are no pre-established criteria for dosing and could present extrapyramidal adverse effects such as tremors, sialorrhea, sedation, impaired liver function, etc. This therapy should be suspended if no changes are perceived in the patient’s behavior within six weeks.23,25
Risperidone is now considered the safest and most effective antipsychotic in the short-term treatment of autism, although it has been linked to a significant increase in weight of about two kilograms when used in 12-week trials. The effects of haloperidol have also been shown to be as effective as those produced by risperidone. Caution should be exercised when using clozapine in treatment because of the high risk of granulocytosis as an
adverse effect; olanzapine is useful to treat children and adults but with minor adverse effects such as increased appetite and weight gain. Even with limitations in its study, intramuscular application of paliperidone has shown improvements in suppressing irritability and aggression in patients with autism, and its only adverse effect is the increase in appetite. Treatment with aripiprazole can be extended up to one year due to its safety and good tolerance in children and adolescents with autism.25,26
Olanzapine also produces an improvement in the treatment of irritability and hyperactivity in autism with lesser effects than risperidone, but with more marked adverse effects such as weight gain, so its use is recommended more for the treatment of adolescents rather than of children.25
Attempts have been made to test the efficacy of a placebo treatment for autism in order to avoid some of the adverse effects of drugs such as haloperidol and risperidone; however, placebos have not shown any favorable outcome against any other type of pharmacological therapy.25
Serotonin reuptake inhibitors such as fluoxetine, paroxetine and sertraline are given to children with autism because they have been found to increase 25% of serotonin levels in platelets and serum. This treatment is based on suppressing symptoms such as anxiety, depression, obsessive-compulsive disorders, and self-injurious behavior.23
Clomipramine has shown favorable results in reducing symptoms such as repetitive behaviors in children with autism with effectiveness similar to haloperidol; however, the intensity of the effect varies with each patient and the doses have to be individualized to avoid adverse effects such as dry mouth, constipation, lethargy, depression, and sleep and behavior problems. Fluvoxamine is effective in treating repetitive and aggressive behavior, but the percentage of effectiveness in patients is very low and very poorly tolerated leading to anxiety, irritability, lack of concentration, and aggressive behavior, among other adverse effects.27

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
43
The effects of fluoxetine are more effective during adolescence than at any other age. Sertraline has been shown to be well tolerated and moderately effective in treating repetitive and aggressive behavior with a minimum amount of adverse effects such as weight gain and anxiety. The use of citalopram brings a wide range of adverse effects such as hyperactivity, impulsivity, insomnia, diarrhea, and dry skin, and is merely used to treat symptoms secondary to behavioral problems. Effective therapy in children for hyperactivity may require the use of multiple drugs such as venlafaxine with serotonin and noradrenaline receptor inhibitors. Mirtazapine is a tricyclic antidepressant which antagonizes serotonin receptors and α-2 adrenergic receptors, showing a very low incidence of adverse effects during its use to treat anxiety, irritability, and hyperactivity.27
A series of indistinguishable behaviors may be associated with variable epileptic seizures in children with autism. The administration of antiepileptic drugs such as sodium valproate, carbamazepine, lamotrigine and topiramate, among others have action mechanisms focusing on blocking sodium and calcium channels, reducing excitatory glutamatergic activity, and increasing inhibition by GABA. The administration of these drugs is directed towards the resolution of these crises without taking into consideration the presence of autism in children. Electroencephalogram studies may associate the presence of autism with the manifestations of seizures by finding temporary unilateral or bilateral paroxysms in the temporal lobes.23,25
Studies have investigated a possible increase in the permeability of the intestinal barrier, so specific diets have been considered for children with autism. Such diets involve the elimination of products such as gluten or casein, found in products such as wheat and milk, since their activity has been linked to opioid effects. The ketogenic diet includes a high fat content and a low amount of carbohydrates that leads to the formation of ketone bodies by the liver and these are linked to a lower incidence of epileptic seizures.
The proposal to include supplements in this type of diets such as magnesium and vitamin B6 has also been evaluated, but there is no evidence that any specific diet plan has beneficial effects in children with autism.25
PrognosisIn general, patients’ prognoses are variable, they depend on the early attention given and also on the severity of the underlying etiologies. The best prognoses belong to patients who have access to different treatments and with socio-familial conditions that favor their development. Some factors are associated with better prognoses: the development of some communicative language before the age of six, presence of slight or no mental retardation in nonverbal intelligence tests, and psychotherapeutic intervention as early and as intensive as possible. The cooperation between specialists such as neurologists, psychiatrists, neuroscientists, psychologists, speech therapists, occupational therapists, and educators is crucial to continue to promote understanding and allow a more adequate approach to patients.28,8,29
Quality of lifeIn studies evaluating IQ, early language development, daily executive functions, and their influence on quality of life, children with ASD were found to have a lower quality of life than children with normal development. This inferior quality of life is related to higher levels of autistic features and deficits of executive functions. It is recorded that, in addition to the patient, the family has a significant reduction in the quality of life affecting different domains (economic, social, educational, and psychological). It is recommended to work with the aggravating factors in autism and the deficits of executive functions that are more associated to an inferior quality of life. The intention is to improve the interventions and, together with the individualized treatments, to improve the quality of life in patients and their families and, in turn, become a useful tool for evaluating treatment outcomes.10,30

Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
44
ConclusionThe present article analyzed the main tools available with the objective of providing information for the early diagnosis and intervention for patients with ASD. It is essential to recognize its main and early clinical manifestations in the first years of life, so that the physician is able to offer the optimal clinical-educational and pharmacological treatment to improve the patients’ prognosis and quality of life.
Conflict of interestThere are no conflicts of interest for any of the authors in this scientific report.
FundingThe authors have not declared any funding source for this scientific report.
Revista Mexicana de Neurociencia September-October, 2017; 18(5):31-45
RevisionReview of Autism Spectrum Disorder
45
1. Camino-León R, López-Laso E. El espectro autista. Vox pediátrica. 2006; 14, 2: 7-152. Millá MG, Mulas F. Atención temprana y programas de intervención específica en el trastorno del espectro autista. Rev
Neurol. 2009; 48 (Supl 2): S47-S523. Oviedo N, Manuel-Apollinar L, De la Chesnaye E, Guerra-Araiza C. Aspectos genéticos y neuroendocrinos en el trastorno
del espectro autista. Bol Med Hosp Infant Mex. 2015; 72 (1): 5-144. Yoo H. Genetics of Autism Spectrum Disorder: Current Status and Possible Clinical Applications. Exp Neurobiol. 2015; 4:
257-272.5. Kong MYF. Diagnosis and history taking in children with autism spectrum disorder: dealing with the challenges. Front.
Pediatr. 2015; 3:55.6. Caretti-Giangaspro E, Alcamí-Pertejo M. Instrumentos para la detección precoz de los trastornos del espectro autista. Rev
Pediatr Aten Primaria. 2007;9: 301-157. Hye-Ran P, Jae-Meen L, Hyo-Eun M, Dong-Soo L, Bung-Nyun K, Jinhyun K, et al. A short review on the current
understanding of autism spectrum disorders. Exp Neurobiol. 2016; 25(1):1-13.8. Rogel-Ortiz F. Autismo. Gac Méd Méx. 2005; 141 (2): 143-147.9. Díez-Cuervo A, Muñoz-Yunta J, Fuentes-Biggic J, Canal-Bedia R, Idiazábal-Aletxae M, Ferrari-Arroyo M, et al. Guía de
buena práctica para el tratamiento de los trastornos del espectro autista. Rev Neurol. 2006; 43(7), 425-38.10. De Vries M, Geurts H. Influence of autism traits and executive functioning on quality of life in children with an autism
spectrum disorder. Journal of autism and developmental disorders. 2015; 45(9), 2734-2743.11. Lopez-Gómez S, Cajal-Cernuda C. Curso y pronóstico del trastorno autista12. Balbuena F. Etiología del autismo: el continuo idiopático- sindrómico como tentativa explicativa. Rev chil neuro-psiquiatr.
2015; 53(4): 269- 27613. Blazer-Dan G, Burke-Jack D. Carpenter William, T. Xavier Castellanos, F. Dimsdale Joel, E. et al. Trastorno del espectro
autista. Manual diagnóstico y estadístico de los trastornos mentales. España 2014. P. 50-5914. Ministerio de sanidad y política social. Guía de prática clínica para el manejo de pacientes con trastornos del espectro
autista en atención primaria. Ministerio de ciencia e innovación. España 2009.p.13-31.15. Geschwind D. Advances in autism. NIH Annu Rev Med. 2009; 60: 367-38016. Sung-Koo Kim. Recent update of autism spectrum disorders. Korean J pediatr. 2015; 58(1): 8-1417. Ruiz-Lázaro P, Posada de la Paz M, Hijano-Bandera F. Trastornos del espectro autista. Detección precoz, herramientas de
cribado. Rev Pediatr Aten Primaria. 2009; 11 (17): 381-s39718. Sampedro-Tobón ME, González-González M, Vélez-Vieira S, Lemos-Hoyos M. Detección temprana en trastornos del
espectro autista: una decisión responsable para un mejor pronóstico. Bol Med Hosp Infant Mex. 2013;70(6): 456-46619. Álvarez-Alcántara E. Trastornos del espectro autista. Rev Mex Pediatr. 2007;74(6); 269-27620. Cabrera D. Generalidades sobre el autismo. Rev Colomb Psiquiat. 2007; vol. 36 (1) 208-220s21. Moyano MB, Alonso M, Aspitarte A, Brío MC, Cleffi V, Cukier S, et al. Guía para el tratamiento de los trastornos del
espectro autista. CAP y N. 2013.22. Salvadó-Salvadó B, Palau-Baduell M, Clofent-Torrentó M, Montero-Camacho M, Hernández-Latorre M. A. Modelos de
intervención global en personas con trastorno del espectro autista. Revista de Neurología. 2012; 54 (Supl 1) S63-71.23. Morant A, Mulas F, Hernandez S. Abordaje farmacológico en el espectro autista. Rev Neurol. 2002; 34 (Supl 1) S64-S67.24. Ruggieri VL., Arberas CL. Abordajes terapéuticos en los trastornos del espectro autista. Revista de Neurología. 2015; 60
(Supl. 1) S45-S49.25. The British Psycological Society and The Royal College of Psychiatrist. Recognition, referral, diagnosis and management of
adults on the autism spectrum. Great Britain. National Collaborating Centre for Mental Health. 201226. Fuentes-Biggi J, Ferrari-Arroyo MJ, Boada-Muñoz L, Touriño-Aguilera E, Artigas-Pallarés J, Belinchón-Carmona M, et al.
Guía de buena práctica para el tratamiento de los trastornos del espectro autista. Rev Neurol. 2006; 43(7) 425-38.27. Doyle CA, McDougle CJ. Pharmacologic treatments for the behavioral symptoms associated with autism spectrum
disorders across the lifespan. Dialogues Clin Neurosci. 2012; 14(3), 263-279.28. Soto-Calderón R. El síndrome autista: un acercamiento a sus características y generalidades. Revista Educación. 2002;
26(1): 47-61.29. Gadia C, Tuchman R. Manejo de los niños con trastornos del espectro autista. Rev Neurol. 2003; 36 (2): 166-173.30. Dietert R, Dietert J, DeWitt J. Environmental risk factors for autism. Emerging Health Threats Journal. 2011; Vol. 4, 1-11.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
46
Pathophysiology of spinal trauma
Fisiopatología del trauma raquimedular
Revision
Huber Padilla-Zambrano,1 YanCarlos Ramos-Villegas,2 Hernando Raphael Alvis-Miranda,3 Andrei F. Joaquin. MD,4 Luis Rafael Moscote-Salazar5
Abstract
Spinal trauma (TRM) includes traumatic lesions characterized by fractures of the spine and may also have deficits in motor and / or sensory functions due to complete or partial involvement of the spinal cord. Pathophysiologically, it occurs by two mechanisms: primary spinal cord injury and secondary spinal cord injury; The first involves the initial mechanical injury due to local deformation and energy transformation, while the second involves a cascade of biochemical and cellular processes. The evolution of these processes has been divided into 5 phases: Immediate, Acute, Subacute, Intermediate and Chronic; The study of these phases is important because it allows the selection of interventions that may possibly improve the patient’s neurological prognosis.
1 Facultad de Medicina, Universidad de Cartagena, Cartagena de Indias, Colombia.2 Facultad de Medicina, Universidad de Cartagena, Cartagena de Indias, Colombia.3 Residente de Neurocirugia, Universidad de Cartagena, Cartagena de Indias, Colombia.4 Department of Neurology, Neurosurgery Division, State University of Campinas, Campinas-Sao Paulo, Brazil. 5 Neurocirujano, Universidad de Cartagena, Cartagena de Indias, Colombia.
Resumen
El Trauma Raquimedular (TRM) engloba las lesiones de origen traumático que se caracterizan por fracturas de la columna vertebral y pueden tener también déficits de las funciones motoras y/ o sensoriales por la afectación completa o parcial de la medula espinal. Fisiopatológicamente, se produce por dos mecanismos: lesión medular primaria y lesión medular secundaria; la primera implica en la lesión mecánica inicial debido a la deformación local y la transformación de energía, mientras que la segunda abarca una cascada de procesos bioquímicos y celulares. La evolución de estos procesos se ha dividido en 5 fases: Inmediata, Aguda, Subaguda, Intermedia y Crónica. El estudio de esas fases es importante pues permite la selección de las intervenciones que pueden posiblemente mejorar el pronóstico neurológico del paciente.
KeywordsSpinal cord injury, spinal cord injury, primary spinal cord injury, pathophysiology, neurogenic shock, spinal shock.
Corresponding author: Dr. Luis Rafael Moscote Universidad de Cartagena , Cartagena de Indias, Colombia e-mail: [email protected]
Palabras clavetrauma raquimedular, lesión medular secundaria, lesión medular primaria, fisiopatología, shock neurogénico, shock espinal.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
47
Introduction
Descriptions of traumatic injury to the spine and its treatment were reported between 3000-2500 BC on a parchment written by Edwin Smith, who mentioned 48 cases of traumatic lesions affecting the Central Nervous System (CNS), of which 12.5% corresponded to spinal injuries. Writings by Hippocrates were later found, reporting traumatic and non-traumatic lesions of the spine. And in the second century AD, Galen was among the first to experiment with animals and report the changes observed by affecting a part of the spinal cord.1
Spinal Cord Injuries (SCI) include injuries of traumatic origin affecting the bony, cartilaginous, muscular, vascular, meningeal, radicular, and medullary structures of the spine -in a joint or isolated way- at any of its levels.1-3 Medullary Lesions (ML) are a devastating neurological problem characterized by the deficit of motor, sensory, and anatomical functions due to a complete or partial involvement of the spinal cord, mainly caused by trauma, occurring in about 15 to 25% of SCI.4,5
SCI present mainly due to traffic or work accidents, accompanied by multiple traumatic injuries such as cranial, thoracic and pelvic. Additionally, they can also be related to injuries by firearm, falling from heights, and by an explosion, among others.1 This medullary traumatic pathology affects mostly men at a male: female-and-young-people ratio of 4:1,3 and has become a public health problem because it involves long-term treatment, high costs in care, and leads to a negative affectation in the patient and his family. The majority of patients affected with SCI cannot recover lost functions because the CNS, unlike the Peripheral Nervous System (PNS) once affected presents irreversible changes that hinder nerve regeneration.2,5
This article intends to describe a review of the pathophysiological considerations found in the scientific literature, which are developed in patients with SCI.
PhysiopathologyTo describe the pathophysiology of SCI, the types of lesions that the spinal cord can undergo must be known, classified as follows: solid cord injury, contusion, laceration, and massive compression; with contusion being the most common SCI representing between 25% and 40% of the cases. In the majority of these, the anatomic severity of the damage does not correlate with the degree of loss of functional abilities presented by the patient.6,7
SCI are a two-step process involving primary and secondary mechanisms, the latter being first described by Allen in 1911.8 The primary process includes the initial mechanical trauma due to the observed displacement of the structures of the vertebral column caused by direct energy, which causes axonal disruption, vascular damage, and cellular apoptosis. In the secondary process, progressive vascular changes are observed; these are caused by the initial trauma leading to the presence of edema and ischemia, accompanied by the liberation of free radicals and ionic alterations, with excitotoxicity as consequence.8,9
The evolution of SCI undergo a series of changes divided into phases: immediate, acute, subacute, intermediate, and chronic.9
Primary injury There are four mechanisms of primary injury: 1) impact with transient compression, 2) laceration-transection, 3) distraction, and 4) impact plus persistent compression; the last being the most common presentation.10
The first mechanism presents in patients with degenerative disease of the cervical spine suffering from hyperextension trauma. The laceration-transection may be due to firearm shot, displaced fracture, or stabbing wound. Distraction is the forced stretching of the spinal cord secondary to flexion, extension, rotation, or dislocation; it is more frequent in people with degenerative disease

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
48
of the cervical spine. Finally, the mechanism of impact plus persistent compression is observed in fractures with burst of vertebral body and retropulsion of bone fragments that exert compression in the spinal cord.10
Initial mechanical trauma includes tension and compression forces, causing penetrating injuries, strains, or tears in neural tissues and vascular structures.5 The initial impact results in the development of a hemorrhage that alters the blood flow, producing local infarcts due to hypoxia and ischemia, which harms the gray matter due to its metabolic requirements and differences in irrigation.5,10 The neurons located in the affected area suffer structural alterations and the myelin sheath diminishes, this, additional to the edema and the macrophages present in the area, are the factors that lead to the deterioration of the nervous transmission.5
Secondary injuryTheories about the secondary mechanisms have evolved in the last 30 years. In the 70s, the free radical hypothesis was crucial to the injury process as Demopoulos et al. stated. Later, in the 80s, they centered on the importance of calcium and lipid peroxidation. Presently, however, we’re exploring the involvement of apoptosis, inhibition of intracellular protein synthesis, and glutaminergic mechanisms in the injury process.8
In 1911, Allen et al. observed there was a harmful agent present in the hemorrhagic fluid that could be causing damage to the spinal cord. This aroused the interest of different authors, which postulated physiological and biochemical mechanisms to explain the post-traumatic damage of the spinal cord tissue, such as: vascular changes, free radical formation, ionic imbalance, apoptosis, and inflammatory responses, among others.8,11
Secondary spinal cord injury begins immediately, or minutes after injury, and can be extended for several days and even weeks.6,12 The tissue damage increases progressively, affecting the different levels of the spinal cord. In addition, endothelial damage leads to increased permeability and the
presence of intracellular edema, an important factor for the extravasation of the cells of the immune system.6
Trauma triggers a series of pathophysiological processes that induce secondary spinal cord injury. To achieve an adequate understanding, this process has been divided into phases taking into account the events that occur in each one of them.13
Immediate phase This phase occurs within the first two hours. It begins at the time of trauma with detectable changes such as general inflammation in the spinal cord followed by hemorrhage in the central gray matter. The cells present necrosis by the mechanical disruption of the membranes and, in turn, ischemia due to vascular disruption. Sudden microvascular disruption causes bleeding in the white matter, aggravating the lesion due to the fact that it can spread and affect the adjacent or distal segments.13
Acute phase This phase happens within 2 to 48 hours. In the acute phase the primary damage occurs as a direct result of trauma, and once the structural thresholds are overcome, immediate cellular and biochemical alterations begin to happen.12,13 This phase is marked by systemic and local alterations such as alterations of the vascular mechanisms, ionic imbalance, and immune system response, among others, which will be described next.12,13
Free radicals The production of radicals from the lipid peroxidation of the cell membrane in the lesions of the central nervous system causes enzymatic deterioration dependent on phospholipids, alterations in the ionic gradients, and even lysis of the membranes.8 In addition, they play an important role in post-traumatic hypoperfusion since there is a reduction of the blood flow of the spinal cord leading to the appearance of edema and an inflammatory response.11 Oxidative stress disables key mitochondrial enzymes in processes such as the respiratory chain,8 production of DNA-associated-proteins due to their nitration,6 and
Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
49
inhibition of Na+ /K+ -ATPase inducing a metabolic collapse and, therefore, the necrotic or apoptotic death of the cell.14
The use of high doses of methylprednisolone within the first eight hours has been found to improve spinal cord blood flow and microvascular perfusion, contributing to clinical neurological recovery.8 In this way, their routine use in clinical practice is still questionable. On the other hand, the cytoprotection through inhibitors of lipid peroxidation facilitates the maintenance of neuronal excitability and inhibits the vasoconstrictor effect produced by prostaglandins.8,11
Vascular mechanismsThe injury causes a reduction of the blood flow, and therefore progressive ischemia, during the first hours, possibly associated to the vasospasm induced by mechanical damage.8,10 White matter perfusion decreases the first five minutes, re-establishing at approximately 15 minutes; however, in the gray matter there are multiple hemorrhages and intravascular thrombosis absenting flow during the first hour, and maintaining this the first 24 hours.12
The systemic hypotension resulting from the loss of hemodynamic self-regulation of the microvasculature may cause additional decreases in the blood flow of the spinal cord with induced hypertension that does not necessarily reverse ischemia but produces marked hyperemia at adjacent sites.10,14
After the ischemic period, the medulla can present a period of reperfusion, which can exacerbate the injury due to the generation of free radicals and other toxic products that contribute to oxidative stress.10,14
Ionic imbalanceUnregulated ion flow is detrimental to cell function and survival since the permeability of the cell membrane is compromised by the activation of the protease.12 In addition, high concentrations of intracellular Ca+ cause mitochondrial damage, enzymatic activation, changes in gene expression,
and apoptosis secondary to the activation of caspases, calpain, phospholipase A2, lipoxygenase, and cyclooxygenase.10–12
The failure of the Na+/ K+ -ATPase bombs, the activation of voltage-dependent Na+ channels, and the massive depolarization impede the mobilization of intracellular Na+ to extracellular space, producing, as a result, an activation of NMDA, AMPA, and Kainate glutamate receptors generating an excitotoxicity that damages oligodendrocytes and axons.6,14
The increase of the extracellular potassium produces an excessive depolarization of the neurons, which affects the nervous conduction, being an important factor in the spinal shock. On the other hand, the decrease in magnesium affects metabolic processes such as glycolysis, oxidative phosphorylation, and protein synthesis.10
Lipid peroxidationAfter the increase in levels of intracellular Ca+, the mitochondrial dysfunction, the degradation of arachidonic acid, and the activation of inducible nitric oxide synthase, the formation of reactive species of oxygen and nitrogen is produced, causing the peroxidation of lipids, damage of proteins and nucleic acids, inducing alterations in the cytoskeleton and organelles that lead to lysis and, therefore, to neuronal loss.12
Inflammatory responseAfter the trauma, the microglia cells induce leukocyte extravasation, which begins to release cytokines (such as tumor necrosis factor α, interleukin-6, and interleukin-1β) complement and reactive species of the oxygen, allowing a greater extravasation and greater tissue damage.6,11,12,14
These cytokines induce cyclooxygenase-2 expression by promoting the degradation of arachidonic acid in prostaglandins, prostacyclin, and thromboxanes that mediate permeability, vascular resistance, and platelet aggregation and adhesion. Excess cytoplasmic Ca+ activates the phospholipases so that they can produce arachidonic acid from the lipids of the cell membrane.6,14

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
50
The inflammatory response is important for the elimination of cell debris, which may be vital in the regeneration of surviving neurons; however, an exaggerated response damages healthy tissue and exacerbates the lesion.12
Microglial cells, neutrophils, and macrophages offer innate immunity, and lymphocytes offer adaptive immunity. Neutrophils enter the damaged spinal cord immediately after the injury and peaks at six hours. Macrophages remain elevated within two to seven days and persist for up to two weeks after the injury.6
ApoptosisApoptosis is a form of programmed cell death characterized by cellular shrinkage, chromatin aggregation, and nuclear pyknosis, mediated by the activation of enzymes called caspases.14 During the acute phase the process of cellular inflammation and then rupture of the cell membrane lead to cell death by necrosis immediately; after several hours the caspase cascade is activated in neurons, oligodendrocytes, microglia, and astrocytes.10,12
In trauma, apoptosis occurs at the epicenter of the lesion and areas of Wallerian degeneration in the white matter, even after several weeks, contributing to post-injury demyelination.8,11,14
Inhibition of protein synthesis with cycloheximide has been found to inhibit apoptosis, reduce secondary damage, and improve functional outcome after spinal cord injury, which demonstrates the requirement for the cell to actively contribute to its own apoptotic disappearance stemming from the synthesis of new proteins.14
Subacute phaseThe phase lasts approximately from two days to two weeks, in which the phagocytic response increases in order to achieve a removal of the débrided tissue in the area of the lesion, allowing a possible axonal regeneration.15 In addition, the astrocytic response occurs late due to hyperplasia and hypertrophy of the astrocyte population around the lesion, which will form the glial scar, which represents the physical and chemical barrier to axonal regeneration and promotes the restoration of ionic maintenance.16
Intermediate phaseThis phase lasts approximately from two weeks to six months, characterized by the maturation of the glial scar produced by the late astrocytic response. In addition, this reaction of the astrocytes allows the possible regeneration of the affected axons to continue, but is insufficient for recovery in severe lesions.17
Chronic phase The degenerative process continues and extends to the areas surrounding the lesion, which present depressed electrical and functional activity evolving to what is known as secondary injury and thus a subsequent loss of neuronal function. The trauma -in addition to producing neuronal death- provokes lysis of glial cells, destruction of blood vessels, and lesions in axonal tracts that, when unable to regenerate, cause the alterations to be permanent.18
The process of demyelination begins 24 hours after injury, increasing two weeks later due to the effect of inflammatory cells entering a second phase of migration.19 At the third week, some fibers present Wallerian degeneration and loss of axonal diameter. The immature forms of healthy oligodendrocytes are able to re-myelinate some axons; additionally, the Schwann cells release trophic factors that collaborate with this process.18,20
Neurogenic shockIt is defined as a systolic blood pressure <100 mmHg associated with a heart rate <80 bpm in the context of medullary trauma, with sudden loss of autonomic tone resulting from the injury due to damage in the sympathetic nervous system (cervical or high thoracic SCI).21,22 It manifests clinically with hypotension, bradycardia, circulatory collapse due to decreased peripheral vascular resistance, and compromise of cardiac output.6,10
The mechanical trauma produces a direct compression of the CNS and peripheral elements by the osteoligamentous structures; additionally, there is damage to vessels, axons, and rupture of nerve cells’ membranes. Secondary to the

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
51
triggered inflammatory process, ischemia of the spinal cord is presented; later, the regulation of the blood flow of the tissue ceases leading to systemic hypotension, exacerbating the ischemia and the progression of the spinal injury.22 Hypotension and neurogenic shock after acute spinal injury is a distributive process resulting from loss of peripheral vasoconstrictor tone in the arterioles and accumulation of blood within the peripheral vasculature.12
Spinal shock It is a post-trauma neurophysiological condition generated by neuronal hyperpolarization, making them insensitive to the brain stimuli, showing as lost function and reflex activity below the level of the injury.6,19 The clinical picture is characterized by the presence of flaccid paralysis, areflexia, loss of sympathetic tone producing bradycardia, hypotension and absence of the cavernous bulb reflex.6 These symptoms will remain until the reflex arcs below the level of the injury resume their functionality.3 Spinal shock can be divided into four phases: areflexia/hyporeflexia; initial reflex return; early hyperreflexia; and late hyperreflexia.6
FundingThe authors have not declared any funding source for this scientific report.
Conflict of interestThere are no conflicts of interest for any of the authors in this scientific report.
Conclusion
In the pathophysiology of SCI, a series of events such as free radical production, vascular alteration, ionic imbalance, lipid peroxidation, immune system response and apoptotic induction are present, chronologically distributed in the phases described above. Other hemodynamic alterations can present, such as neurogenic and spinal shock, affecting the prognosis of these patients.
Knowing the phases of the spinal cord injury gives the physician an idea of the physiological events that are possibly occurring, which allow him to make an adequate selection of the interventions that could possibly improve the neurological prognosis of the patient.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):46-52
RevisionSpinal cord trauma
52
1. Moreno García S. Trauma raquimedular. Morfolia. 2015;7(1):48–54. 2. Lavanderos F J, Muñoz G S, Vilches A L, Delgado M M, Cárcamo H K, Passalaqua H S, et al.
Traumatismo raquimedular. Cuad Cir. 2008;22:82–90. 3. Sandiumenge A, Villavicencio C. Fluido terapia en el traumatismo medular. INFOCOLLOIDS.
2008;(17):1–23. 4. Galeiras Vázquez R, Ferreiro Velasco ME, Mourelo Fariña M, Montoto Marqués A, Salvador de la
Barrera S. Actualización en lesión medular aguda postraumática. Parte 1. Med Intensiva. 2017.
5. Yılmaz T, Turan Y, Keleş A. Pathophysiology of the spinal cord injury. Journal of Clinical and Experimental Investigations. 2014;5(1):131–6.
6. Mataliotakis GI, Tsirikos AI. Spinal cord trauma: pathophysiology, classification of spinal cord injury syndromes, treatment principles and controversies. Orthopaedics and Trauma. 2016;30(5):440–9.
7. Lee J, Thumbikat P. Pathophysiology, presentation and management of spinal cord injury. Surgery. 2015;33(6):238–47.
8. Sekhon H.S. L, G. Fehlings M. Epidemiology, demographics, and pathophysiology of acute spinal cord injury. Spine. 2001;26(24S):S2–12.
9. Baador A M, Cruz T S, Villalón F J. Actualización en la fisiopatología y manejo de traumatismo raquimedular. Revisión bibliográfica. Rev Chil Neurocirugía. 2016;42:144–50.
10. Acevedo González JC, Varón LF, Berbeo Calderón ME, Feo Lee O, Díaz Orduz R. Avances fisiopatológicos para el entendimiento de la lesión medular traumática . Revisión bibliográfica. Rev Col Or Tra. 2015;22(4):272–81.
11. Silva NA, Sousa N, Reis RL, Salgado AJ. From basics to clinical: A comprehensive review on spinal cord injury. Prog Neurobiol. 2013;
12. Oyinbo CA. Secondary injury mechanisms in traumatic spinal cord injury: A nugget of this multiply cascade. Acta Neurobiol Exp. 2011;71:281–99.
13. Ballestero Plaza V, Marré Pacheco B, Martínez Aguilar C, Fleiderman Valenzuela J, Zamorano Pérez JJ. Lesión de la médula espinal. actualización bibliográfica: fisiopatología y tratamiento inicial. Coluna/ Columna. 2012;11(1):73–6.
14. Kwon BK, Tetzlaff W, Grauer JN, Beiner J, Vaccaro AR. Pathophysiology and pharmacologic treatment of acute spinal cord injury. The spine journal. 2004;4:451–64.
15. Donnelly DJ, Popovich PG. Inflammation and its role in neuroprotection, axonal regeneration and functional recovery after spinal cord injury. Experimental Neurology. 2008;209:378–88.
16. Herrmann JE, Imura T, Song B, Qi J, Ao Y, Nguyen TK, et al. STAT3 is a critical regulator of astrogliosis and scar formation after spinal cord injury. The Journal of neuroscience. 2008;28(28):7231–43.
17. Hill CE, Beattie MS, Bresnahan JC. Degeneration and Sprouting of Identified Descending Supraspinal Axons after Contusive Spinal Cord Injury in the Rat. Experimental Neurology. 2001;171:153–69.
18. Nieto-sampedro M. literatura Pathophysiology of spinal cord injury . A review Artículos de revisión Fisiopatología de la lesión medular . Revisión de literatura. 2017;(March).
19. Lovesio C. Traumatismos raquimedulares. In: Medicina Intensiva. Buenos aires: El ateneo; 2006. 20. Li Y, Raisman G. Schwann cells induce sprouting in motor and sensory axons in the adult rat spinal
cord. The Journal of neuroscience. 1994;14(7):4050–63. 21. Santacruz LF, Herrera P. ÁM. Trauma raquimedular. Trauma Raquimedular. 2012;257–71. 22. Duarte Misol DR, Rubiano AM, Moscote-Salazar LR. Choque neurogénico : Fisiopatología ,
diagnóstico y tratamiento. Rev Traum Amér Lat. 2016;6(1):27–30.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
53
Where are we, and where are we going? Review of strategies and new integral proposals in the management of herniated disc
¿Dónde estamos y a dónde vamos? Nuevas estrategias integrales en el manejo de hernia de disco
Revision
Eloy Ovando-Sanders,1 Diana Paola Urias-Valdez,1 Jorge Rendón-Félix,1* Héctor Echevarría-Requeijo,1 David Gustavo Rodríguez-Cisneros.1
Abstract
At some point in their lives, 66% of adults suffer low back pain, of which 85% have at least one herniated disc. This disease is the leading cause of disability, reduced working hours and high costs due to persistent pain. Historically, the mainstay of treatment has been based on drugs, leaving imaging studies and invasive treatments as a last resort when there was no observed improvement with the conservative treatment.
The main justification for surgery is an accelerated pain relief compared to conservative therapy (reason of its high practice) but, besides not having a standardized management, there has been no difference in long-term benefits or lower costs. Similarly, there is not a consensus to establish a specific drug, dose or precise exact rehabilitation sessions for the proper management of the condition, so that each case must be individualized.
In recent years, there have been new management strategies based on anti-inflammatories, ozone therapy and proper rehabilitation, with promising results (pain remission in up to 95% of patients) in early stages, but wider dissemination is needed in order to establish them as therapeutic alternatives.
1 Centro de la Columna Vertebral. Zapopan, Jalisco, México.
Keywordsherniated disk; radiculopathy; integrated conservative treatment.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
54
Resumen
En algún momento de su vida, 66% de los adultos padecerán dolor de espalda baja, de los cuales 85% tendrán al menos una hernia discal. Esta enfermedad es la causa principal de incapacidad, disminución de horas laborales y elevados costos debido a la persistencia del dolor. Históricamente, el pilar de su tratamiento ha sido a base de medicamentos, dejando los estudios de imagen y tratamientos invasivos como última opción cuando no hubo mejoría con el tratamiento conservador.
La principal justificación de la cirugía es un alivio acelerado del dolor en relación al tratamiento conservador (razón de su alta práctica) pero, además de no contar con un estándar quirúrgico, no hay diferencias en beneficios a largo plazo o disminución de costos. De la misma manera, aunque existe un consenso donde se establece que tipo de medicamento, dosis exactas o sesiones precisas de rehabilitación para la adecuada recuperación del padecimiento, cada caso debe ser individualizado.
Las nuevas estrategias de manejo integral, combinando terapias a base de antiinflamatorios, ozono y adecuada rehabilitación, han tenido resultados prometedores (remisión del dolor hasta en el 95% de los pacientes) en fases iniciales, pero falta mayor difusión para poder establecerlas como alternativas terapéuticas.
Palabras clavehernia discal; hernia lumbar; radiculopatía; manejo integral conservador.
Correspondencia: Jorge Rendón-Félix.Centro de la Columna Vertebral.Av. San Ignacio 123, Col. Jardines de San Ignacio. Zapopan, Jalisco. C.P. 45040 México.E-mail: [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
55
Introduction
Alterations of the intervertebral disc, especially degeneration, reduce the quality of life and are well short of effective therapies. This is a very common condition. It is excessively silent, or it is tolerated because of its chronicity, but has alarming consequences - incapacitating, especially.1
In the last three months, approximately 10% of the adult population of the United States (the most studied in this disease due to the condition’s implications in its workforce) has reported back pain irradiating to the lower limbs, better known as “sciatica”, due to the L4, L5, S1, and S2 nerve roots, which join together in the lumbosacral plexus to form the tibial and peroneal nerves, exiting the pelvis in a single trunk as the sciatic nerve.2,3
Once trauma is ruled out as the pain’s origin, the cause of vertebral fractures, spondylolisthesis, or lumbar stenosis, 85% of adult radicular-type back pain will be secondary to a herniation of one or more intervertebral discs.3
It is well known that intervertebral disc herniation by itself is not a direct cause of root pain, considering its prevalence increases with age, and it is not uncommon to see magnetic resonances finding herniation either asymptomatic or with minimal symptomatology.4 However, this predisposes the contact of the nucleus pulposus with a nerve root, triggering an inflammatory phenomenon that causes the mechanical effect of compression and referred pain.5
Contrary to popular opinion, surgical intervention is not the first (or the main) option in cases of disc herniation, since several studies and reviews have postulated that patients with this condition improved substantially with conservative treatment (up to 87% of cases) in a period of three months after the onset of pain6 and, even in adequately performed studies of patients with persistent radiculopathy, it is well established that the condition did not improve after surgery.7,8
Generally, the natural history of lumbar hernias is favorable, and patients who begin with radiculopathy exhibit decreased symptomatology within a period of six weeks after diagnosis (treated conservatively and through physical rehabilitation). The international guidelines (translated and adapted for our country) establish the recommendation to defer any imaging, invasive procedures, or surgical interventions in patients with lumbar radiculopathy during that time period in the absence of trauma or signs of surgical urgency such as cauda equina syndrome. If there are no improvements in the symptoms during that period, imaging studies should be performed to establish the exact cause and regulate the procedures to follow.10
Unfortunately, this rule is not always followed. Under the justification of faster pain relief (compared to conservative therapy), surgery is suggested as the first option for most patients who request it, or who urgently seek a solution to their condition. This is done without considering risk factors specific to the surgical intervention, or the minimal (or zero) advantage it has compared to the magnitude of long-term pain recovery, plus an increased rate of complications characteristic of the intervention, and longer overall disability time.7,11,12
Similarly, due to the prevalence and high costs of the disease in an adult population at the height of productivity (diagnostic costs, specific therapy, work compensation, days of work absence, and lack of productivity), and insufficient evidence regarding the most adequate approach, we continue to work with different combinations of treatments and complementary therapies to improve the quality of life of the patients and to reduce the costs and times of incapacity.13
Considering all of the above, we made a systematic review of the current literature in the UpToDate database, the Cochrane Library, and the American and Mexican guidelines concerning the treatments for lumbar intervertebral disc hernia radiculopathy currently available, taking into consideration the levels of evidence in the studies, and the recommendations secondary to these. A

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
56
review was also made of the different alternative approaches that have historically been carried out and of the new comprehensive strategies offered to treat them correctly with high expectations of remission and symptom relief.
Treatment of the herniated discOver the years, and with the advent of new drugs or therapeutic interventions (whether surgical or intrathecal/intradiscal procedures), multiple studies have been performed comparing them with traditional therapies (as well as comparing conservative and surgical treatments), and the vast majority did not show a significant difference in final results at one year and at four years of follow-up regardless of the medications or surgical techniques used.7,8,14,15
Similarly, in the surgical field, they continue to make comparisons between different surgical techniques in order to find the most effective one with fewer adverse effects, but no particular procedure has demonstrated enough of an advantage in all areas to be called “the gold standard.” Although there is doubt about which surgical procedure to follow (both discectomy and microdiscectomy have the same post-surgical results in medium and long term), minimally-invasive procedures have boomed recently, though they still fail to show significant advantages over traditional procedures, on top of which there is a requirement for trained staff and centers with capabilities to perform them, resulting in higher costs that do not justify the benefits obtained.16
Regarding the eternal dilemma between surgery or conservative therapy, the two therapeutic modalities have been compared. Irrespective of the surgical technique chosen, the results do not show much more of an advantage against the conservative treatment in terms of pain relief and improvement in function three months after treatment,17 or in the long-term follow-up of four years,18 or eight years19 (without taking into consideration surgical risks, need for reinterventions, or complications typical of the procedure).
For almost 10 years, Peul et al. have shown that,
although the recovery rate is higher with surgery (4 weeks v. 12 with conservative treatment), 5% of the patients in both groups continued to experience pain and lack of recovery after one-year follow-up, regardless of the treatment they received.7
Likewise, there is no exact consensus on the use of rehabilitation devices such as spinal traction to control the disease, having to individualize them for each patient based on their symptomatology, with no change in the natural evolution of the disease, and with little evidence of benefits.20
There is insufficient evidence, as well, to support a quantifiable improvement of symptoms with the use of nonsteroidal anti-inflammatory drugs (NSAIDs) or the use of epidural steroid injections. Results that vary from patient to patient and there is no change in the natural history of the disease, but there are different reports of adverse effects.21,22
And, on another note, the use of opioid analgesics should be restricted and limited to patients with severe lower-back pain followed by strict supervision. A higher rate of fractures of the hip, humerus, or wrist, has been reported secondary to falls caused by overdosage (voluntary and involuntary) due to the use and abuse of this family of medications because of the profound suppression of pain and anesthesia they provide, as well as their toxicity after a prolonged use.23
Adequate rehabilitation with supervised exercises (which may include physiotherapy and chiropractic treatment) has been shown to prevent weakness, improve mobility, and alleviate the symptomatology.24
Controlling risk factors to improve adherence to the treatment (such as smoking cessation, weight loss, and regular exercise), as well as an adequate following of the therapies, and a clear understanding of their condition, have proven to be of enormous importance in patient recovery. Similarly, attacking the underlying inflammatory component of the root disease (with a targeted therapy) has been linked to better results, but

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
57
the little evidence found in the literature is observational and inconclusive.25
Conservative alternatives used historicallyThis is a condition in constant study. Whenever new health therapies arise, it is inevitable to test their effectiveness in conditions where the patient can benefit, and lumbar hernias are no exception. The results are variable (most of them range from regular to good) in different well-studied approaches in clinical trials or meta-analysis to determine their benefits. The techniques are listed below:
Glucosamine, herbal therapies, and biological agents The use of glucosamine has been extensively studied in inflammatory joint disorders, being particularly useful in knee and hip problems. However, data about its use for lumbar radiculopathy is scarce, and no differentiations were found either in pain or quality of life changes in patients using glucosamine versus placebo, so their use is limited to joints with wide range of motion.26
Regarding the use of herbal therapies, several systematic reviews of clinical trials with different compounds (mainly Capsicum frutescens –chili pepper–, Harpagophytum procumbens –devil’s claw–, Salix alba –white willow bark–, Symphytum officinale –comfrey root extract–, and lavender oil) resulted in short-term improvement of the symptoms in the follow-up. With no ability to determine medium- or long-term benefits due to the limitations of the studies, they cannot be compared directly against the traditional drugs and can only be recommended as therapeutic adjuvants.27
Since the advent of the use of biological agents to control various conditions of rheumatic and autoimmune origin, and knowing there is an inflammatory component in disc herniation radiculopathies, the use of anti-TNF-alpha drugs (particularly infliximab, either parenteral or intradiscal) has not been shown to be superior to placebo in terms of pain management when
followed-up at three months and at one year; therefore, its use is not recommended in the modality described.28,29
Rapid relief with physical therapies: chiropractic stimulation, acupuncture, and massageChiropractic spinal stimulation involves the movement of a joint beyond its usual range of motion but without exceeding its anatomical limit (the so-called “para-physiological” zone), with low- or high-intensity lever movements. The effectiveness of this type of therapy has been seen mainly in the short term. It modestly improves root pain in the initial 12-week period but, without showing differences in the annual follow-up, its use should be seen as a merely adjuvant therapy.30
As for acupuncture, the westernization of this millenary practice has sought to standardize its use (either as an integral therapy or as adjuvant in the treatment of various ailments), obtaining similar results as those of spinal stimulation (moderate improvement in symptomatology and function during the first three months). The meta-analysis could not determine, however, whether the benefit was due to the activity exerted by the inserted needles or merely by the placebo effect. So, the indication is that its use may be more beneficial in people who hold a high expectation of obtaining a benefit from this treatment in a short period of time.31
Similar to acupuncture, massages exert a therapeutic effect in the short term by relaxing muscle fibers and improving mobility. Due to the various massage techniques used, there has been no clear benefit in the medium or long term (there was improvement the first 10 weeks with massage sessions, but it decreased as time progressed and there was no improvement at one-year follow-up), so it is recommended as a relaxing therapy with short-term benefits.32
Physical modalities: interference therapy, diathermy, low-level laser, ultrasound, and nerve stimulationThe patient plays an important factor in the use of these types of stimulation therapies. They can have rapid benefits, but their use must be individualized

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
58
and combined with other treatments for greater patient benefit.
Inferential therapy consists of the application of an alternating current of medium frequency, modulated to produce frequencies up to 150 Hz to stimulate nerve roots. It may help a very select group of patients, but it has not been possible to standardize it for a general benefit.33
A similar treatment with comparable results is the application of short-band diathermy, which consists of raising the temperature of the deep tissues by electromagnetic radiation applied in a range of 10 to 100 MHz, but, unlike the previous one, a clear benefit in pain improvement has not been found.34
In regards to low-level lasers, they consist of the application of a light with a wavelength of 632 to 904 nm, directed at the pain area. The trials showed a superior improvement of pain at the year of follow-up, but this decreased in patients who exercised, so a greater benefit can be found in patients who are incapacitated by their condition.35
Although widely used for musculoskeletal pain syndromes, the use of ultrasound has not been well evaluated for disc radiculopathy. As for deep tissue heating, it is usually used in combination with other physical therapy modalities, so it has not been possible to establish a clear benefit as a single therapy and is not recommended as such.36
Nerve stimulation (both transcutaneously and with the insertion of percutaneous needles into the dermatomes of the nerve root) involves the application of electrical stimuli by means of electrodes, with the aim of improving the symptoms by modifying the perception of pain. Although both types of stimulation may offer benefits, a marked superiority has been seen with the use of percutaneous stimulation, though there has been no long-term follow-up of the symptomatology.37
Combined treatments: optimizing resultsThere are no trials that evaluate an optimal sequencing of therapies, so the decision to choose
one therapy over another relies upon the treating doctor and the patient’s expectations, seeking practicality, and taking into consideration costs, convenience, and the availability of the resources and trained personnel required for each specific therapy.
New comprehensive strategiesIn an effort to find a faster, more effective, and less costly recovery option for patients and companies (in terms of decreasing times of incapacity and absenteeism), the new conservative strategies obtained an accelerated recovery of patients in a more effective and less invasive way. Each has promising results, but with the inconvenience of not having controlled clinical studies to compare them with other drugs or surgery due to patients’ perception and favoritism of a particular type of treatment. This can delay the establishment of these therapies as part of the integral treatment of herniated disks in order to displace the traditional therapies.
These treatments cover therapeutic routes and drugs that, on paper, have a superior effectiveness over traditional therapies, but have not secured a follow-up of their patients or made their own comparative structured studies.
Anti-inflammatories in measured doses: the principle of homotoxicologyA treatment strategy that had a great boom in the late twentieth century was the use of high-potency anti-inflammatory drugs in minimal therapeutic doses or diluted administration to control the inflammatory component of the disease while avoiding the toxicity of those drugs.
All the studies in this area searched for the right drug in the exact dose to treat the various events derived from an inflammatory component, giving way to the advent of homotoxicology as a way to apply drugs in carefully measured doses based on simple dilutions and serial and supervised administrations of the medication (without becoming doses or principles of homeopathy), based on the different toxic substances released by the body during the various stages of the inflammatory process,

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
59
obtaining a therapeutic effect in a select group of diseases as well as minimizing the toxicity with the use of this group of anti-inflammatories.38
Unfortunately, the way in which homotoxicology studies were done was based on tests with different dosages of the medicines to achieve an effective and safe dose, which is why their studies were not comprehensive due to the adverse effects that the patients could have, and their use had been limited to drugs whose effectiveness had already been proven and which were currently allowed by the different regulatory agencies of each country.
Local ozone therapy and its effectivenessWith the advent at the beginning of this century of different therapies based on hyperbaric oxygen and ozone for the recovery of different inflammatory or surgical conditions, another type of local therapy with paravertebral oxygen-ozone has been studied since 2003.39 The results were quite encouraging in terms of patient recovery and the reduction of pain and radiographic changes characteristic of disc hernias (assessed with imaging studies and the analog visual scale of pain), so its use is now considered as an excellent individual therapy and, better still, as adjuvant in the different conservative treatments of herniated disc, with minimum to zero
adverse effects, excellent patient tolerance, and reduced costs of operation, so, to date, comparison studies continue based on this component with different combinations.40
Combination of therapeutic alternatives: are we getting closer to the treatment of the future?It has been observed that by using our previous knowledge in combination with different treatments available, a high rate of remission in patients has been achieved by a synergy of anti-inflammatory drugs in homotoxicological doses, with the adjuvant use of ozone-based therapy and adequate rehabilitation (including thermotherapy, electro-stimulation, hydrotherapy, and ultrasound) at the same time, reducing the amount of pain and increasing functionality for patients undergoing these therapeutic combinations (with a rate of improvement of over 95% of patients), which heralds a new outlook in the recovery of herniated disc radiculopathy benefitting patients, employers, and the health sector. At the same time, there is still a need for more diffusion, and for comparisons with the currently established treatments in the international guides in order to regulate them either as a complement or a substitution of the traditional treatments (whether conservative or surgical).41
Conclusion
The treatment of lumbar hernias is a field in constant study and growth, where new methods are sought to treat them with greater effectiveness and lower costs, establishing new strategies that aim at the improvement of the treatment while clarifying its study. The daily search for ways to grow as an integral therapy in the treatment of the herniated disc has been sought in both the surgical and conservative areas. Conservative treatments show a tangible superiority in regards to remission of pain, duration of treatment, diminished invasion, and reduction of costs and times of recovery, so it seems that the traditional treatment of the herniated disc as we’ve known it is about to change in the not too distant future.
FundingThe authors have not declared any funding source for this scientific report.
Conflict of interestThere are no conflicts of interest for any of the authors in this scientific report.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
60
1. Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58:26-35.
2. Andersson G, Watkins-Casatillo SI. Low back pain. In: The burden of musculoskeletal diseases in the United States, third edition. Rosemont, IL: Bone and Joint Initiative, 2014 (http://www .boneandjointburden.org).
3. Ropper AH, Zafonte RD. Sciatica. N Engl J Med. 2015;372:1240-8.4. Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, et al. Systematic literature
review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36:811-6.
5. Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the herniated lumbar disc: controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-80.
6. Vroomen PCAJ, de Krom MCTFM, Wilmink JT, Kester ADM, Knottnerus JA. Lack of effectiveness of bed rest for sciatica. N Engl J Med. 1999;340:418-23.
7. Peul WC, van Houwelingen HC, van den Hout WB, Brand R, Eekhof JA, Tans JT, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356:2245-56.
8. Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Hanscom B, Skinner JS, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a randomized trial. JAMA. 2006;296:2441- 50.
9. Vroomen PCAJ, de Krom MCTFM, Knottnerus JA. Predicting the outcome of sciatica at short-term follow-up. Br J Gen Pract. 2002;52:119-23.
10. Kreiner DS, Hwang SW, Easa JE, Resnick DK, Baisden JL, Bess S, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014 Jan;14(1):180-91.
11. Bush K, Cowan N, Katz DE, Gishen P. The natural history of sciatica associated with disc pathology: a prospective study with clinical and independent radiologic follow-up. Spine. 1992;17:1205-12.
12. Kreiner DS, Hwang SW, Easa JE, Resnick DK, Baisden JL, Bess S, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014;14:180-91.
13. Chou R, Loeser JD, Owens DK, Rosenquist RW, Atlas SJ, Baisden J, et al. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: an evidence-based clinical practice guideline from the American Pain Society. Spine. (Phila Pa 1976) 2009;34:1066- 77.
14. Weber H. Lumbar disc herniation: a controlled, prospective study with ten years of observation. Spine. (Phila Pa 1976) 1983;8:131-40.
15. Osterman H, Seitsalo S, Karppinen J, Malmivaara A. Effectiveness of microdiscectomy for lumbar disc herniation: a randomized controlled trial with 2 years of follow-up. Spine. 2006;31:2409-14.
16. Arts MP, Brand R, van den Akker ME, Koes BW, Bartels RH, Peul WC, et al. Tubular diskectomy vs conventional microdiskectomy for sciatica: a randomized controlled trial. JAMA. 2009;302(2):149.
17. Oliphant D. Safety of spinal manipulation in the treatment of lumbar disk herniations: a systematic review and risk assessment. J Manipulative Physiol Ther. 2004;27:197-210.
18. Weinstein JN, Lurie JD, Tosteson TD, Tosteson AN, Blood EA, Abdu WA, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine. (Phila Pa 1976). 2008;33(25):2789.
19. Lurie JD, Tosteson TD, Tosteson AN, Zhao W, Morgan TS, Abdu WA, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine. (Phila Pa 1976). 2014 Jan;39(1):3-16.
20. Wegner I, Widyahening IS, van Tulder MW, Blomberg SE, de Vet HC, Brønfort G, et al. Traction for low-back pain with or without sciatica. Cochrane Database Syst Rev. 2013;8:CD003010.
21. Friedly JL, Comstock BA, Turner JA, Heagerty PJ, Deyo RA, Sullivan SD, et al. A randomized trial of epidural glucocorticoid injections for spinal stenosis. N Engl J Med. 2014;371:11-21.
22. Al-Shoha A, Rao DS, Schilling J, Peterson E, Mandel S. Effect of epidural steroid injection on bone mineral density and markers of bone turnover in post-menopausal women. Spine. 2012;37(25): E1567-71.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):53-61
RevisionReview and new proposals in the management of herniated disc
61
23. Chou R, Turner JA, Devine EB, Hansen RN, Sullivan SD, Blazina I, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015;162:276-86.
24. Fernandez M, Hartvigsen J, Ferreira ML, Refshauge KM, Machado AF, Lemes ÍR, et al. Advice to stay active or structured exercise in the management of sciatica: a systematic review and meta-analysis. Spine. (Phila Pa 1976) 2015;40: 1457-66.
25. Cohen SP, White RL, Kurihara C, Larkin TM, Chang A, Griffith SR, et al. Epidural steroids, etanercept, or saline in subacute sciatica: a multicenter, randomized trial. Ann Intern Med. 2012;156:551- 9.
26. Wilkens P, Scheel IB, Grundnes O, Hellum C, Storheim K. Effect of glucosamine on pain-related disability in patients with chronic low back pain and degenerative lumbar osteoarthritis: a randomized controlled trial. JAMA. 2010;304(1):45.
27. Oltean H, Robbins C, van Tulder MW, Berman BM, Bombardier C, Gagnier JJ. Herbal medicine for low-back pain. Cochrane Database Syst Rev. 2014; :CD004504.
28. Korhonen T, Karppinen J, Paimela L, Malmivaara A, Lindgren KA, Järvinen S, et al. The treatment of disc herniation-induced sciatica with infliximab: results of a randomized, controlled, 3-month follow-up study. Spine. (Phila Pa 1976). 2005;30(24):2724.
29. Korhonen T, Karppinen J, Paimela L, Malmivaara A, Lindgren KA, Bowman C, et al. The treatment of disc-herniation-induced sciatica with infliximab: one-year follow-up results of FIRST II, a randomized controlled trial. Spine. (Phila Pa 1976). 2006;31(24):2759.
30. Bronfort G, Hondras MA, Schulz CA, Evans RL, Long CR, Grimm R. Spinal manipulation and home exercise with advice for subacute and chronic back-related leg pain: a trial with adaptive allocation. Ann Intern Med. 2014 Sep;161(6):381-91.
31. Kalauokalani D, Cherkin DC, Sherman KJ, Koepsell TD, Deyo RA. Lessons from a trial of acupuncture and massage for low back pain: patient expectations and treatment effects. Spine. (Phila Pa 1976). 2001;26(13):1418.
32. Cherkin DC, Sherman KJ, Kahn J, Wellman R, Cook AJ, Johnson E, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized, controlled trial. Ann Intern Med. 2011;155(1):1.
33. Hurley DA, McDonough SM, Dempster M, Moore AP, Baxter GD. A randomized clinical trial of manipulative therapy and interferential therapy for acute low back pain. Spine (Phila Pa 1976). 2004;29(20):2207.
34. Gibson T, Grahame R, Harkness J, Woo P, Blagrave P, Hills R. Controlled comparison of short-wave diathermy treatment with osteopathic treatment in non-specific low back pain. Lancet. 1985;1(8440):1258.
35. Klein RG, Eek BC. Low-energy laser treatment and exercise for chronic low back pain: double-blind controlled trial. Arch Phys Med Rehabil. 1990;71(1):34.
36. Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Phys Ther. 2001;81(10):1641.
37. Ghoname EA, White PF, Ahmed HE, Hamza MA, Craig WF, Noe CE. Percutaneous electrical nerve stimulation: an alternative to TENS in the management of sciatica. Pain. 1999;83(2):193.
38. Ernst E1, Schmidt K. Homotoxicology--a review of randomised clinical trials. Eur J Clin Pharmacol. 2004 Jul;60(5):299-306.
39. Andreula CF, Simonetti L, de Santis F, Agati R, Ricci R, Leonardi M. Minimally Invasive Oxygen-Ozone Therapy for Lumbar Disk Herniation. AJNR Am J Neuroradiol. 2003;24:996-1000.
40. Zhang Y, Ma Y, Jiang J, Ding T, Wang J. Treatment of the lumbar disc herniation with intradiscal and intraforaminal injection of oxygen-ozone. J Back Musculoskelet Rehabil. 2013;26(3):317-22.
41. Ovando-Sanders E, Salazar-García JL, Ortiz-Watson LA. Reporte de 147 casos de éxito en el Centro de la Columna Vertebral a base de colchicina homeopática, ozono y terapia física. Rev Mex Med Fis Rehab. 2014;26(1):24-37.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
62
Consideraciones y reconceptualización de teorias del dolor crónico asociado a disfunciones musculoesqueleticas y su implicancia en la plasticidad y reorganización cerebral: una revisión de la literatura
Considerations and reconceptualization of theories of chronic pain associated with musculoskeletal dysfunctions and its implication in plasticity and cerebral reorganization: a review of the literatura.
Revisión
Sebastián Pinto Concha,2,3 Felipe Araya Quintanilla,1,2
Héctor Gutiérrez Espinoza.1,4
1 Facultad de Ciencias de la Salud, Escuela de Kinesiología. Universidad de Las Américas, Chile.2 Escuela de Kinesiología, Facultad de Ciencias de la Salud. Universidad Gabriela Mistral. Santiago, Chile. 3 Centro de medicina del deporte, Clínica Las Condes, Chile. 4 Centro de diagnóstico y tratamiento (CDT) Hospital Clínico San Borja Arriaran, Santiago, Chile.
ResumenLos modelos explicativos actuales de los trastornos de dolor musculoesqueletico crónico hacen referencia a los mecanismos nociceptivos periféricos e impulsados de manera secundaria a una anomalía estructural y/o post-traumática. A la luz de varias limitaciones presentes en la literatura y en la evidencia disponible, se hace necesario generar una síntesis de conceptos bajo un marco actual de conocimiento, acerca del re conceptualización del dolor y sus procesos a nivel del sistema nervioso central. Actualmente nuestro entendimiento acerca del dolor y la neuroplasticidad en los trastornos musculoesqueleticos crónicos, en esta última década, la neurociencia moderna está en constante crecimiento. Es por esto que los modelos propuestos y teorías continuamente crecen y evolucionan bajo un requerimiento de una nueva información creciente. Al considerar que naturalmente, las teorías o conceptos que hasta ahora tenemos se podrían considerar equivocadas en el sentido más simplista, pero en un sentido especifico e incluso sutil, sólo necesitan ser consideradas como incompletas en una necesidad de re conceptualizar. Es por esto, que nuestra revisión tiene como objetivo describir y contextualizar las nuevas teorías adaptativas del dolor crónico y ver sus implicancias en la plasticidad y reorganización cortical en disfunciones musculoesqueleticas. Cabe mencionar que las nuevas teorías adaptativas del dolor y los nuevos conocimientos, sugieren y obligan a generar nuevas estrategias que integren todos los sistemas y veamos como piedra angular el trabajo en estructura corticales y subcorticales.
Palabras clavedolor musculoesqueletico, neuroplasticidad, dolor.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
63
Abstract
Current explanatory models of chronic musculoskeletal pain disorders refer to peripheral nociceptive mechanisms and are driven secondary to the structural and post-traumatic anomaly. Considering several limitations present in the literature and available evidence, it is necessary to generate a synthesis of concepts under a current framework of knowledge about the conceptualization of pain and its processes at the level of the central nervous system. Currently our understanding of pain and neuroplasticity in chronic musculoskeletal disorders, in this last decade, modern neuroscience is constantly growing. That is why the proposed models and theories continually grow and evolve under a requirement of new and growing information. Whereas, Naturally, the theories or concepts that we have so far could be mistaken in the simplistic sense, but in a specific and even subtle sense, they only need to be considered as incomplete in need to re-conceptualize. Therefore, our review aims to describe and contextualize the new adaptive theories of chronic pain and to see their implications in plasticity and cortical reorganization in musculoskeletal dysfunctions. It is worth mentioning that the new adaptive theories of pain and new knowledge suggest and force to generate new strategies that integrate all the systems and see as a cornerstone the work in the cortical and subcortical structures.
Keywordsmusculoskeletal pain, neuroplasticity, pain.
Correspondencia: Facultad de Ciencias de la Salud, Universidad de Las Américas, Sede Providencia, Manuel Montt 948, Santiago, Chile.Correo electrónico: [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
64
IntroducciónEl trastorno de dolor musculoesqueletico, es una condición de ámbito clínico como experimental,1 que abarcan factores difusos y complejos para poder explicar la condición de dolor crónico persistente en este tipo de sujetos. Hoy en día, la baja adherencia y adaptación a los tratamientos de rehabilitación convencionales basados simplemente en enfoques biológicos y mecánicos,2 hacen que el escenario clínico sea más complejo aun, ya que los enfoques de intervención, solo consideran la lesión estructural articular, mecánica y/o tisular ser la fuente real, unica e inicial de un evento doloroso. Sin embargo, esta es, potencialmente la generadora del dolor al inicio de quienes presentan esta condición, con una menor consideración acerca de la sensibilización central y la alteración del procesamiento del dolor3 y con ello, los cambios neuroplasticos y de reorganización cortical mediado por estos trastornos crónicos.4-6
Paralelamente hoy se evidencia un re conceptualización acerca de la moderna neurofisiologia del dolor y la disfunción del movimiento, como dos aspectos de un sistema integrado que han ido incrementándose en la literatura en lo que respecta a nuestro entendimiento clínico y obliga a una constante evolución para replantear nuestra propuesta de tratamiento e intervención.1,7,8,9,11 Sin embargo, la re conceptualización permanece incompleta hasta que se integre el comportamiento cortical cerebral y su plasticidad, asociada a una alteracion en el procesamiento del dolor.3 En efecto, el dolor, la sensibilización central, el movimiento con un desempeño motor diferenciado y la plasticidad cerebral son aristas complejas y son componentes de un sistema específico y amplio integrado de redes neuronales diferenciadas a un comportamiento de dolor crónico.12
Una comprensión contemporánea, sugiere que puede haber mecanismos paralelos existentes involucrados en el dolor crónico asociado a los trastornos musculoesqueleticos y que estos podrían simultáneamente
actuar con los mecanismos biomecánicos de sobrecargas de tejidos localizados, implicando una continua actividad de estructuras cerebrales prefrontales y meso límbicas, áreas relacionadas con la cognición y aspectos emocionales.6,12,13 Esto se asocia a la idea de que el estado real de los tejidos no proporciona una medida adecuada y precisa del dolor, que ya está siendo reconocida respecto a varios síndromes de dolor musculoesqueletico crónico.4,6,9 Sin embargo, aún se utilizan predominantemente modelos mecánicos y existen paradigmas sobre el dolor basados en el comportamiento del tejido, biomecánica de una articulación y la carga de éstas para explicar el dolor5 sin tomar en cuenta aspectos de la sensibilizacion central3 y plasticidad cortical del sistema motor.1,7,16 Estos modelos biomecánicos estructurales continúan siendo desarrollados,5,13,14 pero no reconocen adecuadamente el papel que integra el sistema nervioso central en la experiencia del dolor musculoesqueletico. Esta omisión descuida todo un marco actual de la literatura, que ofrece una explicación más detallada y completa en cuanto al porqué los intentos de relacionar los síntomas del dolor a la patología estructural y/o periférica siguen cayendo de forma limitada.6,9,12,15 En este contexto, es difícil definir un punto de tiempo definitivo mediante el cual podamos afirmar que la recuperación de los tejidos periféricos se ha completado en términos de las etapas tanto inflamatoria como proliferativa. En la práctica, tal vez sea más importante considerar otros factores además de la evolución temporal de los síntomas, el considerar si los mecanismos del dolor éstan influenciados ya sea por el tejido local estructural o por un predominio de un procesamiento del sistema nervioso central alterado por el dolor.16 El propósito de esta revisión de la literatura, es generar un marco teórico contundente y describir las nuevas teorías adaptativas del dolor crónico y ver sus implicancias en la plasticidad y reorganización cortical en disfunciones musculoesqueleticas.
Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
65
Objetivo
Métodos
Describir y contextualizar las nuevas teorías adaptativas del dolor crónico y ver sus implicancias en la plasticidad y reorganización cortical en disfunciones musculoesqueleticas.
Se realizó una búsqueda especifica electrónica en las bases de datos; Medline, PEDro (especializada en fisioterapia), Central y SportDiscus, los términos de búsqueda utilizados fueron; Musculoskeletal pain, Neuronal plasticity, neuroplasticity, Chronic Pain. Se seleccionaron artículos publicados en inglés y español hasta el 31 de diciembre del 2016. Además, se realizaron búsquedas manuales y seguimientos de referencias en las siguientes revistas: Revista de Neurologia de Barcelona, España, Journal of Pain and Symptom Management, Hong Kong Physiotherapy Journal, Acute pain.
Reconceptualizacion y nueva teoria del dolor
La neuromatriz fue un concepto desarrollado porque había sido imposible para los investigadores encontrar determinadas regiones corticales espacialmente segregadas dedicadas a la percepción del dolor.20 Sin embargo, en su estado inicial fue significativamente diferente de lo que la actual teoría de la matriz del dolor se ha convertido.21 Puede suponerse que la teoría actual disponible del dolor no es necesariamente correcta en su totalidad, en el futuro será modificada, especificada y reconceptualizada para reflejar nuevos conocimientos. Pero es significativamente menos equivocada de lo que era antiguamente. Ultimamente se han hecho mejoras progresivas a la teoría de la neuromatriz del dolor. Una definición muy útil del dolor es que corresponde a un correlato consiente de la percepción implícita de amenaza al tejido u organismo que está en peligro.9 Sin
entender lo que es el dolor, es difícil avanzar y discutir las intervenciones. Existe una multitud de diferentes enfoques que se pueden tomar cuando se habla de la neurobiología del dolor y los numerosos aspectos importantes para considerarlo. Existen diversos puntos reportados que son fundamentales para una comprensión mas extendida del dolor actual. Uno de ellos es que el dolor no nos da una medida del estado actual del tejido. Esto ha sido demostrado a través de algunos estudios tanto en animales y seres humanos. Dichos datos han demostrado que, en el dolor, la actividad de los nociceptores y el estado del tejido no están isomórficamente relacionados en absoluto, pero son moduladas por una variedad de factores, planteando además la escasa relación vista anteriormente entre el daño estructural de un tejido y con el estado real del dolor de los sujetos, lo cual no existen una relación directamente proporcional.5,22 Es importante considerar que la nocicepción no es suficiente para la experiencia del dolor, a pesar de que éste es el conductor más común en la experiencia del dolor,23 y que es modulado por un número de diferentes factores, incluyendo los dominios de tipo somáticos, psicológicos, emocionales y sociales.9
Los factores que influyen en el dolor son variados y parecen depender en gran medida del contexto en el que el estímulo nocivo se evalúa. Algunas de las áreas que han sido demostradas para modular el dolor de manera de exacerbarlo o atenuarlo; incluyen a los mediadores inflamatorios, la temperatura del tejido, el flujo de sanguineo, la excesiva atención e hipervigilancia, la ansiedad, el miedo, el catastrofismo, la angustia, la expectativa del paciente, el grado de credibilidad, el contexto social, aprehensión, entre otras.6,12,13,16 Por ende, se puede apreciar que los componentes nociceptivos para genera un proceso de dolor van más allá del estado de un tejido o estructura.
La conceptualización del dolor antes mencionada se ve vinculada al sistema motor y hasta ahora solo ha sido teorizada, manejada y estudiada simplemente como un síntoma de la patología, una lesión, y/o solamente como un fenómeno

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
66
de tipo sensorial. La disfunción del movimiento, la afección de tipo psicosocial y emocional fueron considerados entonces una consecuencia de aquel problema de tipo sensorial asociado al problema doloroso.21 Las actuales investigaciones realizadas1,7,12 durante ésta última década han demostrado que el dolor no es sólo un síntoma, sino que puede persistir y convertirse en una condición fisiopatológica del sistema.3,24 La disfunción del movimiento podria plantearse no sólo como una consecuencia y minimizar al dolor reactivamente, sino ser el componente motor de un problema más amplio que converge también con factores intrínsecos mencionados, a su vez, los factores sociales y medioambientales que continuamente moderan la percepción y el componente conductual del dolor crónico, como una compleja construcción multidimensional del sistema.9,12,23,25
Las nuevas propuestas de las teorías del dolor, abordan a que cuando el dolor persiste, la relación entre la percepción del dolor y el estado del tejido se vuelven aún más imprecisos. En parte, la teoría de la neuromatriz se ajusta a nuestro conocimiento actual de la biología y la neurociencia, que es lo suficientemente flexible para crecer y desprender dos componentes muy importantes en ésta teoría.
El primer paso es considerar al dolor como una de las diversas salidas que dispone el sistema nervioso central en respuesta a la amenaza que se percibe y que esta percepción de amenaza, es la que impulsa salidas del sistema, implicando el desarrollo inherente de manifestaciones específicas a nivel motor y del movimiento, tales como la rigidez tipo espasmo, cambios en la actividad neuromuscular en los multiples niveles del SNC, con una redistribución de ésta actividad dentro y entre de los músculos y cambios en la cinematica o en el sentido de posición y movimiento.1,10,26 Aspectos que generalmente son considerados de manera errónea, como consecuencias de un proceso doloroso.
El segundo paso es entender que estos cambios en el corto plazo son beneficiosos para la
supervivencia y como mecanismo de respuesta, pero tendrían implicancias en el largo plazo, descritas como plasticidad adaptada a nivel cerebral, esto en base a una continua percepcion de miedos o amenazas de lesión o reinjuria, escaza variabilidad motora, que implica utilizar las mismas estrategias y sinergias musculares provocando un patrón motor de movimiento aberrante y generando un espasmo reactivo, con la presencia de bajos umbrales de dolor en estímulos mecánicos, térmicos y químicos relacionados a los estados de la sensibilización central del sistema.1,3,12,27,28,29 Clínicamente estos cambios se pueden manifestar como hiperalgesia secundaria generalizada y/o alodinia no sólo en relación a los estímulos táctiles y térmicos, sino que también con un patrón de movimiento.8
Otra teoría es la propuesta en el trabajo de Puentedura 201225 reconocida como la “Teoría del Neurotag” (muy similar a la neuromatriz), en donde explica el conjunto de redes y diversas áreas del cerebro, comúnmente asociadas al desarrollo de dolor neural. Esta teoría menciona el mapeo cerebral que existe y sus conexiones como se ven alteradas en el proceso de dolor. Se aprecia y explican distintas áreas corticales y subcorticales invadidas por el proceso de dolor, como la amígdala, hipotálamo y cerebelo. Estructuras encargadas del miedo, respuestas autónomas y equilibrio y coordinación propiamente tal. Síntomas que se pueden apreciar clínicamente en pacientes con dolor crónico. Todo esto sugiere, que el procesamiento del dolor, no depende de ningún tejido especifico asociado a una nocicepcion periférica como puede pasar en la degeneración discal o ruptura de un tendón,17,18 sino más bien de un proceso inminente y otros factores emocionales. Cabe destacar, que autores sugieren que el tejido anatómico no siempre cicatriza desde una perspectiva estructural tisular, incluso después de intentar reparar quirúrgicamente el tejido dañado, sino que posee el potencial de un cambio morfológico adaptativo y biológicamente degenerativo y adaptado a las demandas funcionales y de carga del sujeto.17, 19 Es posible que este punto sea altamente individualizado y
Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
67
agravado por los factores específicos del tejido y del propio individuo, como por ejemplo los fenómenos de hipovascularización relativa del tejido, la reinervación de terminales nerviosos con marcadores neurales en tendones y discos intervertebrales, lo que hace entender el sentido de individualismo a nivel estructural.19
Es importante mencionar que esta neuromatriz o redes neuronales, son altamente especificas e individuales en cada sujeto. Por eso se cree que el dolor es propio, único y complejo. El individualismo en este sentido, puede ser una puerta a nuestros trabajos terapéuticos, considerando una modulación del mapeo cerebral con los componentes afectados mencionados anteriormente.
Dolor y neuroplascitidad en disfunciones musculoesqueleticas
La neuroplasticidad, es un concepto clave para entender el proceso del dolor y su implicandia en el movimiento. Cuando el dolor es persistente, puede dar lugar a cambios en la representación propioceptiva de la parte del cuerpo afectada, específicamente en la corteza sensorial primaria, secundaria, motora y otras áreas influyentes.1,7,15 Se reporta que ésto tendría implicancias para el sistema motor, puesto que se sabe que la alteración tanto experimental y clinica de estos mapas cerebrales resultan en una planificación de ejecución motora interrumpida, aberrante e ineficaz.30
Existe gran cantidad de evidencia informando de que estos cambios pueden llegar a ser parte de un tema más global.1,7,15,27 Está surgiendo evidencia de que el sistema nervioso central también se reorganiza en respuesta a la disfunción musculoesquelética,8,10,12 lo que sustentaría las afirmaciones mencionadas anteriormente. El término denominado neuroplasticidad, es una propiedad intrínseca del sistema nervioso que le permite adaptarse a los cambios ambientales, modificaciones fisiológicas y experiencias.31 La neuroplasticidad puede ser adaptativa o mal adaptiva en la
presencia de dolor o disfunción y los mismos procesos provocan la reorganización del sistema nervioso central, pudiendo potencialmente ser aprovechados también para revertir los cambios centrales y conducir a resultados positivos en los pacientes.32 Sin embargo, los clínicos quienes abordan pacientes que se presentan con disfunción musculoesquelética y dolor crónico convencionalmente evalúan el desempeño de movimientos de regiones específicas o prescriben ejercicios de control motor sin tener en cuenta el potencial de la plasticidad en el sistema nervioso central.33 En contraste, los clínicos que trabajan con pacientes con disfunción neurológica consideran comúnmente el efecto de la disfunción cortical en el rendimiento del paciente, involucrando al cerebro y su afección cortical por ser la fuente del problema.
Reconocer y abordar la neuroplasticidad como un componente del control motor en pacientes con disfunción musculoesquelética es sumamente importante, ya que que puede conducir a una mayor comprensión de los mecanismos neurales que sustentan la disfunción motora; y el alcance de abordar a la organización neural mal adaptiva a través de la neuroplasticidad, la cual posiblemente puede mejorar la efectividad de los tratamientos dirigidos al comportamiento motor, tales como la habilidad del movimiento e incluso la fuerza muscular.
Recientes reportes de los procesos neuroplasticos corticales mencionan que influyen en los aspectos de la rehabilitación musculoesquelética. Sin embargo, los enfoques fisioterapeuticos musculoesqueléticos actuales utilizan rutinariamente la prescripción del ejercicio que está influenciada principalmente por protocolos de ejercicios investigados en estudios clínicos, con escaso énfasis en los procesos centrales del cerebro asociados con la neuroplasticidad.33, 34 Un enfoque para mejorar el rendimiento o desempeño motor a través de la neuroplasticidad es la imaginería motora, donde el movimiento real es deliberadamente mejorado o sustituido mediante el ensayo mental de una tarea.35 Se utiliza ampliamente

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
68
en un contexto deportivo y en algunos casos de rehabilitación y dolor en síndromes neurológicos, su uso en la rehabilitación musculoesquelética es relativamente poco desarrollado.35,36 El entrenamiento de tareas específicas bajo un concepto de aprendizaje motor es otro enfoque que ha demostrado ser eficaz en mejorar la fuerza, activación y el rendimiento motor, acompañado de cambios en áreas del cerebro involucradas en la ejecución de las tareas.37,38 Por lo tanto, es sorprendente que las estrategias que abordan la neuroplasticidad, tales como las imágenes mentales y el entrenamiento específico con el aprendizaje de una tarea motora, no se han adoptado más ampliamente en la rehabilitación músculeesquelética.37 Sin embargo, este tema es tremendamente amplio y es necesario abordarlo en otra posible publicación.
Actualmente, se reportan numerosos cambios centrales que se producen como consecuencia del dolor y que desarrollan alteraciones del movimiento, una reducción en la variabilidad con el movimiento y la percepción alterada del cuerpo en el espacio.1,39,40 Con respecto a esto último, los pacientes con dolor lumbar crónico han demostrado un déficit en la propiocepción, asociado a un pobre desempeño en el juicio del movimiento, poca agudeza táctil, mayores dificultades para identificar las letras trazadas en su zona lumbar y escasa disociación lumbar.15
La interacción entre la percepción corporal y el repertorio de movimientos de una persona es tan estrecha que aún persiste en amputados cuando hacen frente a los movimientos del miembro fantasma. Un modelo integrado del dolor, la plasticidad, y el movimiento, es argumentado por O`Sullivan, 2013,41 quien propone el uso de un modelo conceptual biopsico-motor, que propone la existencia de tres aspectos de comportamiento distintos del movimiento relacionados con el dolor: los comportamientos de protección, comportamiento comunicativo y el comportamiento social. Está claro que estas tres características del comportamiento involucran la actividad cerebral a un nivel consciente o inconsciente. Como tal, la existencia
de un modelo conceptual proporciona un marco útil sobre lo que temporalmente sucede y evalua la integridad de las hipótesis relevantes al dolor, el cerebro y el movimiento.
Aunque la relación causal entre el dolor y la reorganización cortical no se ha establecido definitivamente con los trastornos musculoesqueleticos, reportes actuales sugieren que el dolor es un conductor de la reorganización cortical. Existen condiciones en donde la reorganización en la corteza somatosensorial primaria está presente y además existe una normalización con la atenuación del dolor.42,43
Sin embargo, el dolor por si solo no es necesario ni suficiente para impulsar los cambios neuroplásticos. En condiciones como la distonía y el sindorme de túnel carpiano son ambas condiciones en que investigaciones, han demostrado cambios neuroplásticos en la corteza motora y somatosensorial primaria en la ausencia de dolor. La distonía focal de la mano implica una pérdida del control individual de la dígitación de la mano que resulta de las rápidas acciones motoras repetitivas de los dedos. Estos movimientos dan lugar a una confusión en la representación de los dígitación con la pérdida de la segregación espacial.47,48
Los sujetos con dolor lumbar recurrente continúan demostrando un control motor anormal en la ausencia de dolor, posiblemente reflejando una continua reorganización de las propiedades neuronales y de organización en la corteza motora primaria.49,50 Sin embargo, se ha evidenciado algunos de los cambios morfológicos en el volumen de la sustancia gris del cuerpo estriado y ganglios basales, estructuras relacionadas con la modulación del movimiento, control postular y aprendizaje de tareas, esto asociado a los cambios en el retorno somatotopico cortical.44,45,46 Entendiendo esto como un proceso de cronificacion de dolor crónico e incluso cambios estructurales profundos a nivel cortical, que no son reversibles con nuestras herramientas terapéuticas actuales, enfocadas en los comportamientos periféricos.
Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
69
Aunque el dolor proporciona un impulso para los cambios neuroplásticos en el SNC, otras formas de estímulos, procesos cognitivos y conductas pueden inducir cambios plásticos. Según Keim et.al en el 2008 menciono que en estudios de animales, humanos sanos y sujetos comprometidos neurológicamente han demostrado que la prominente repetición y la atención son factores importantes que inducen cambios neuroplásticos en las cortezas somatosensorial y motora primaria.51 Las estructuras límbicas y prefrontales son las áreas corticales responsables de estos aspectos del comportamiento y emociones, y los resultados han demostrado cambios importantes en estas áreas en los estados de dolor crónico, incluyendo algunos trastornos de dolor musculoesqueletico crónico.52,53
Hoy en día es necesario discutir la evidencia que apoya la sensibilización central del sistema nervioso en los trastornos musculoesqueléticos crónicos, asociado a la alteracion en el procesamiento central del dolor con actividad de reorganizacion en zonas corticales bajo el concepto de la neurofisiología del dolor en el campo de la neurociencia, relacionando el potencial papel de la neuroplasticidad en los trastornos de dolor crónico musculoesquelético y sus implicancias en el sistema motor.
Discusión
La presente revisión pretende facilitar sinergias de conocimiento y proporcionar un entendimiento de los complejos sistemas de integración del cuerpo, además de describir y contextualizar las nuevas teorías adaptativas del dolor crónico y ver sus implicancias en la plasticidad y reorganización cortical en disfunciones musculoesqueleticas.
El razonamiento final, es plantear un marco conceptual abordando un modelo biopsico-motor enfocado en la neurociencia, que reúna de manera óptima los cambios corticales asociados al dolor y la plasticidad cerebral en las disfunciones del movimiento en el sistema motor.
Un punto clave de éste trabajo es establecer un modelo de alcance hacia el nuevo concepto de la neurofisiologia del dolor y la relacion a los trastornos de los movimientos, los cuales deben ser manejados de una manera multidimensional, integrada; abordando tanto sistema aferente, eferente, la integración y procesamiento del sistema nervioso central. Así mismo, considerar la investigación y la información científica, que avanza de forma imperativa entregando nuevas ideas, percepciones, modelos y evidencia sobre el procesamiento del dolor.
Es importante mencionar que el dolor es un proceso complejo y amplio que involucra factores intrínsecos y extrínsecos, que aborda todo tipo de redes neuronales y se procesa, modula y crea completamente en el cerebro. Desde ahí, se generan consecuencias a nivel periférico que corresponden a las manifestaciones clínicas y sintomatológicas que se pueden apreciar en la práctica clínica. Al entender estos procesos, mecanismos y reconceptualizaciones, se hará más sencillo comprender y establecer nuevas estrategias de tratamiento que integren todos los sistemas y veamos como piedra angular el estructuras corticales y subcortciales.
Conflicto de interesesNo existen conflictos de interés para ninguno de los autores, en este informe científico.
Fuentes de financiamientoNo hay fuentes de financiamiento.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
70
1. Hodges PW, Tucker K. Moving differently in pain: a new theory to explain the adaptation to pain. Pain. 2011;152:90–98.2. O`Sullivan P. Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control
impairments as underlying mechanism. Manual Therapy. 2005, 10 (4) :242-2553. Nijs J, Van Houdenhove B, Oostendorp R. Recognition of central sensitization in patients with musculoskeletal pain:
Application of pain neurophysiology in manual therapy practice. Manual Therapy. (2010); 15: 135–1414. Henry D, Chiodo A, Yang W. Central Nervous System Reorganization in a Variety of Chronic Pain States: A Review. PM&R.
(2011); 3:1116-1125.5. Liu P, Maffulli N, Rolf C, Smith R. What are the validated models for tendinopathy?. Scand J Med Sci Sports. (2011); 21(1):
3-17.6. Pelletier R, Higgins J, Bourbonnais D. Is neuroplasticity in the central nervous system the missing link to our
understanding of chronic musculoskeletal disorders?. BMC Musculoskeletal Disorders (2015): 16-257. Cote J, Hoeger Bement M. Update on the Relation Between Pain and Movement: Consequences for Clinical Practice. Clin J
Pain. (2010); 26 (9):754-762.8. Simmonds M, Moseley L, Vlaeyen J. Pain, Mind, and Movement An Expanded, Updated, and Integrated Conceptualization
Clin J Pain. (2008); 24 (4):279–2809. Moseley GL. Reconceptualising pain according to modern pain science. Physical Therapy Reviews. (2007); 12 (3) :169-178.10. Hodges PW. Pain and motor control: From the laboratory to rehabilitation. Journal of Electromyography and Kinesiology.
(2011); (21): 220–228.11. Hodges PW, Smeets R. Interaction Between Pain, Movement, and Physical Activity. Short-term Benefits, Long-term
Consequences, and Targets for Treatment. Clin J Pain. (2015); 31:97–10712. Moseley GL, Flor H. Targeting cortical representations in the treatment of chronic pain a review. Neurorehabil Neural
Repair. (2012); 26: 646–5213. Littlewood C, Malliaras P, Bateman M, Stace R, May S, Walters S. The central nervous system e an additional consideration
in rotator cuff tendinopathy and a potential basis for understanding response to loaded therapeutic exercise. Manual Therapy. (2013); 18(6):468-72.
14. Cook J, Purdam C. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. (2009);43: 409-416
15. Wand B, Parkitny L, O’Connell N, Luomajoki H, McAuley J, Thacker M, et al. Cortical changes in chronic low back pain: current state of the art and implications for clinical practice. Manual Therapy. (2011); 16:15-20.
16. Gifford, L. Pain, the tissues and the nervous system: a conceptual model. Physiotherapy. (1998); 84 (1), 27-36.17. Adams M, Roughley P. What is Intervertebral Disc Degeneration, and What Causes It?. Spine. (2006); 31: 2151–2161.18. Seitz A, McClure P, Finucane S, Boardman D, Michener L. Mechanisms of rotator cuff tendinopathy: Intrinsic, extrinsic, or
both?. Clinical Biomechanics. (2011); 26: 1–1219. Rees JD1, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology.
2006;45(5):508-2120. Iannetti GD, Mouraux A. From the neuromatrix to the pain matrix (and back). Exp Brain Res. 2010;205(1):1-1221. Melzack R. Phantom limbs and the concept of a neuromatrix. Trends Neurosci. (1990);13:88-92.22. Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA.Systematic literature review of imaging features
of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811-623. Butler D., Moseley L. Explain pain. Physiotherapy Research International. 2004.9;4185–18724. Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH, et.al. Sensitization in patients with painful
knee osteoarthritis. Pain. 2010;149(3):573-8125. Puentedura EJ, Louw A. A neuroscience approach to managing athletes with low back pain. Phys Ther Sport.
2012;13(3):123-3326. Hodges PW, Smeets RJ. Interaction between pain, movement, and physical activity: short-term benefits, long-term
consequences, and targets for treatment. Clin J Pain. 2015;31(2):97-107.27. Madeleine P, Mathiassen SE, Arendt-Nielsen L. Changes in the degree of motor variability associated with experimental
and chronic neck-shoulder pain during a standardised repetitive arm movement. Exp Brain Res. (2008);185:689–69828. Farina D, Leclerc F, Arendt-Nielsen L, et al. The change in spatial distribution of upper trapezius muscle activity is
correlated to contraction duration. J Electromyogr Kinesiol. (2008);18:16–2529. Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional Endogenous Analgesia During Exercise in Patients with
Chronic Pain: To Exercise or Not to Exercise? Pain Physician. (2012); 15:ES205-ES213 30. Tsao H, Galea MP, Hodges PW. Reorganization of the motor cortex is associated with postural control deficits in recurrent
low back pain. Brain. 2008;131: 2161-71
Referencias
Revista Mexicana de Neurociencia September-October, 2017; 18(5):62-71
RevisiónDolor crónico asociado a disfunciones musculoesqueléticas
71
31. Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastic human brain cortex. Annu Rev Neuroscience. 2005;28:377-401.32. Flor H. Painful memories. Can we train chronic pain patients to ‘forget’ their pain? EMBO Rep. (2002);3(4):288-91.33. Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent, nonspecific low back pain: a
systematic review. Phys Ther. (2009);89(1):9-2534. Bystrom MG, Rasmussen-Barr E, Grooten WJ. Motor control exercises reduces pain and disability in chronic and
recurrent low back pain: a meta-analysis. Spine. (2013); 38(6):350-835. Guillot A, Collet C. Construction of the Motor Imagery Integrative Model in Sport: a review and theoretical investigation
of motor imagery use. Int Rev Sport Exerc Psychol. (2008);1(1):31-44.36. Mulder T. Motor imagery and action observation: cognitive tools for rehabilitation. J Neural Transm. (2007);114(10):1265-
78.37. Tsao H, Galea MP, Hodges PW. Driving plasticity in the motor cortex in recurrent low back pain. Eur J Pain.
(2010);14(8):832-9.38. Carey JR, Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey L, Rundquist P, et al. Analysis of fMRI and finger tracking training
in subjects with chronic stroke. Brain. (2002);125(Pt 4):773-88.39. Madeleine P, Vedsted P, Blangsted A K, Sjøgaard G, Søgaard K. Effects of electromyographic and mechanomyographic
biofeedback on upper trapezius muscle activity during standardized computer work. Ergonomics. (2006); (49): 921-933.40. Madeleine P, Leclerc F, Arendt-Nielsen L, Ravier P, Farina D. Experimental muscle pain changes the spatial distribution of
upper trapezius muscle activity during sustained contraction. Clin Neurophysiol. (2006); (117): 2436-2445.41. Vibe K, O Sullivan P, Skouen J, Smith A, Kvale A. Efficacy of classification-based cognitive functional therapy in patients
with non-specific chronic low back pain: A randomized controlled trial. Eur J Pain. 2013 J;17(6):916-2842. Birbaumer N, Lutzenberger W, Montoya P, Larbig W, Unertl K, Topfner S, et al. Effects of regional anesthesia on phantom
limb pain are mirrored in changes in cortical reorganization. J Neurosci. (1997);17:5503–8.43. Huse E, Larbig W, Flor H, Birbaumer N. The effect of opioids on phantom limb pain and cortical reorganization. Pain.
(2001);90:47–55.44. Rodriguez-Raecke R, Niemeier A, Ihle K, Ruether W, May A. Brain gray matter decrease in chronic pain is the consequence
and not the cause of pain. J Neurosci. (2009);29:13746-1375045. Seminowicz DA, Wideman TH, Naso L, Hatami-Khoroushahi Z, Fallatah S, Ware MA, et al. Effective treatment of chronic
low back pain in humans reverses abnormal brain anatomy and function. J Neurosci. (2011);31(20):7540-5046. Baliki M, Petre B, Torbey S. Corticostriatal functional connectivity predicts transition to chronic back pain. Nature
Neuroscience. 2012.15:1117-112147. Byl NN, McKenzie A, Nagarajan SS. Differences in somatosensory hand organization in a healthy flutist and a flutist with
focal hand dystonia: a case report. J Hand Ther. 2000;13(4):302-948. Byl NN, Nagarajan SS, Merzenich MM, Roberts T, McKenzie A. Correlation of clinical neuromusculoskeletal and central
somatosensory performance: variability in controls and patients with severe and mild focal hand dystonia. Neural Plast. 2002;9(3):177-203
49. D’hooge R, Hodges P, Tsao H, Hall L, MacDonald D, Danneels L. Altered trunk muscle coordination during rapid trunk flexion in people in remission of recurrent low back pain. J Electromyogr Kinesiol. (2013);23:173–81.
50. Brumagne S, Janssens L, Knapen S, Claeys K, Suuden-Johanson E. Persons with recurrent low back pain exhibit a rigid postural control strategy. Eur Spine J. (2008);17:1177–84.
51. Keim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res. (2008);51:225–39
52. Apkarian AV, Baliki MN, Geha PY. Towards a theory of chronic pain. Prog Neurobiol. (2009);87:81–97.53. Mansour A, Farmer M, Baliki M, Apkarian AV. Chronic pain: the role of learning and brain plasticity. Restor Neurol Neurosci.
(2014);32:129–39.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
72
Stem cells: an alternative for the treatment of cerebral palsy
Células madres: una nueva alternativa en el manejo de la parálisis cerebral
Revision
Ángela María Sánchez,1 Luz Mabel Ávila Portillo,2 Eugenia Espinoza.3
Abstract
Cerebral palsy it’s a high impact pathology in general population, generating big costs for the public health system. With an increase of its prevalence resulting in a high incidence rate of premature low weight new born. Presently, there has been in an increasing interest in producing basic and clinical research with the aim on therapeutic value from transplant using pluripotent, particularly in children affect by cerebral palsy. This paper describes a comprehensive review from 13 informative papers that covers the mayor attributes on this newly developed technic.
1 Facultad de Medicina Universidad de la Sabana. Colombia2 Hospital Militar Central, Stem Medicina Regenerativa, CryoHoldco de Latinoamerica3 Universidad Militar Nueva Granada, Hospital Militar Central, Instituto Roosevelt. Colombia
ResumenLa Parálisis Cerebral (PC) es una patología de alto impacto en la población general, generando grandes gastos en el sistema de salud. Con un aumento de su incidencia en los últimos años por el nacimiento de prematuros de muy bajo peso. Actualmente se está desarrollando investigación en ciencias tanto básica como clínica con el fin de evaluar el potencial terapéutico de las células madre en la funcionalidad y calidad de vida de niños con PC. En este estudio se revisaron 13 artículos con el fin de evidenciar la seguridad y eficacia de esta terapia, e implementar en el futuro el uso de células madre en el tratamiento de pacientes con PC.
Keywordscerebral palsy, stem cells, therapy, GMFCS cerebral palsy, stem cells, therapy, GMFCS
Corresponding author: Ávila Portillo Luz Mabel.Hospital Militar central. Tv. 3 #49-00Bogotá, Colombia
Palabras claveparálisis cerebral, células madre, terapéutica, GMFCS, reparación cerebral

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
73
Introduction
In context with Cerebral PalsyCerebral Palsy (CP) affects one in 500 school-age children. In recent years, it has been defined as a non-progressive motor syndrome with clinical manifestations that change with age, causing a limitation of motor activity. Associated with injury or malformation during fetal brain development or in childhood, it affects muscle control, coordination, tone, and reflexes, as well as body movement and balance.1,2,18 It can also affect fine and gross motor skills, as well as oral motor functioning.2,18
CP is caused by brain injury or malformation during the period of brain development in the prenatal or perinatal stage, or immediately after birth.1-3
Risk factors and potential etiologies of CP depend on the time of injury (prenatal, perinatal, or postnatal) and on biological, temperamental-psychological, familial, and social factors.1
The following risk situations may intervene in the different ages of the child: fetal intrinsic factors such as fetal genetics, infections, and endocrine factors; placental factors such as placental size, structural and functional abnormalities, environmental factors, and infections; and extrinsic factors which may include maternal nutritional status, maternal age, education, multiple gestation, cigarette consumption, alcohol, medications, and history of prematurity.1
There are multiple etiologies for CP, so the most important thing is early detection of neurodevelopmental problems. Some of the main issues associated with prematurity are hypoxia and ischemia, intraventricular hemorrhage, and auditory and visual dysfunction. Postnatal problems involve infections, cranioencephalic trauma, cerebrovascular disease, and bronchopulmonary dysplasia.1
There are various classifications for CP, including pathophysiological classifications (type of tension: dystonia, chorea, ballism, rigidity, ataxic, and
mixed types) and topographic classifications (quadriplegia, diplegia, hemiplegia, and double hemiplegia).1
For practical applications of this article, however, it is important to know the gross motor function classification system (GMFCS). This universal classification system evaluates the degree of functionality or limitation of the patient and is divided into five domains:4
GMFCS Level I: walks without limitations.
GMFCS Level II: walks with limitations.
GMFCS Level III: walks aided by mobility devices.
GMFCS Level IV: self-mobility with the use of motorized help. Limited self-mobility, wheelchair use probable.
GMFCS Level V: severe limitations in the head and trunk. Requires extensive use of assistive technology and physical assistance; transported in a wheelchair.
The current therapeutic measures are observation, facilitation of neurodevelopment, feeding, sleep, development of skills and manual dexterity, improvement of positions and basic postures of development, general mobility, communication and language, leisure time use, and abilities and attitudes for their development, all of which are implemented through physiotherapy, language therapy, and occupational therapy. The current medical management consists of oral antispastic, baclofen bomb, selective dorsal rhizotomy, benzodiazepine, and botulinum toxin.1
In context with Stem CellsStem cells are currently of great interest in the area of scientific research. They have great therapeutic potential in multiple hematopoietic, osteoarticular, cardiovascular, and neurological pathologies due to their characteristics of self-renewal, differentiation, and derivation to a mature cell. Stem cells are divided according to their origin in embryonic and adult, and according to

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
74
their potential of differentiation into pluripotent, multipotent, and totipotent.5
Types of stem cells (SC)* Bone marrow SC: generate hematopoietic, blood system, and mesenchymal cells.5
* Umbilical cord blood, placenta, and Wharton’s jelly SC: generate heterogeneous populations with pluripotent potential. 5
* Neural SC: capable to differentiate into glia and astrocytes.5
* Adipose tissue SC: heterogeneous cell population including mesenchymal and endothelial progenitors.5
* Skin SC: generate dermis, epidermis and subcutaneous cellular tissue.5
Stem cells’ restorative potential for the brain in patients with CPStem cells have been studied in multiple brain pathologies such as stroke, hypoxic-ischemic encephalopathy, autism, neurodegenerative diseases, and cerebral palsy, due to their great potential for proliferation and tissue restoration.
Several clinical and preclinical studies investigate the brain repair mechanisms as well as the safety and efficacy of stem cell therapy in patients with CP.
Although the exact mechanism of brain tissue repair is still being studied, it is considered that SC influence the repair by means of paracrine and trophic effects such as increased synaptogenesis, stimulation of endogenous mechanisms of repair, stimulation of angiogenesis, neovascularization, cellular migration, and stimulation of the proliferation of endogenous stem cells; these have, in a smaller way, the capacity of proliferation, differentiation, and integration of SC to brain tissue, which results in the replacement of neurons and glia and we thus obtain remyelination, with subsequent increase of neuronal plasticity and improvement in motor function.6
Stem Cells and Cerebral Palsy - Animal ModelsBrain injury causes motor and cognitive development deficit, which incurs great costs for the healthcare system due to the children’s requirements. At present, the incidence of cerebral palsy is eight per 1000 live births. This has grown in recent years due to the increased survival of very low birth weight preterm infants and patients with brain damage secondary to hypoxic-ischemic encephalopathy.6 In spite of this, the therapeutic strategies used for CP have not shown significant improvements in the functionality or in the repair of the brain, for which the therapeutic potential of SC for the regeneration of brain tissue and subsequent functional rehabilitation has been investigated.6 Different studies in animal models obtained successful results and identified some of the brain repair mechanisms.
In 2006, Meier et al. studied 36 rats to evaluate the therapeutic potential of stem cells derived from umbilical cord blood (UCB). Following brain injury due to hypoxic-ischemic encephalopathy caused by ligation of the left carotid artery at seven days of age, they subsequently gave intraperitoneal transplantation of cells derived from human UCB stem cells. The results indicated the presence of human HLA-specific antigens in the lesion area, suggesting cellular migration, and also identified a significant improvement in locomotor functionality (p=0.001) with a significant decrease in spastic paresis (P=0.001). 7 (See table 1.1).
In 2012, Sang-Hun Bae, et al. studied 60 rats in which the left carotid artery was ligated with subsequent brain injury. They treated them by intravenous transfusion of UCB-derived stem cells at doses of 1x107 cells. They evaluated human immunoreactivity, 3-phosphate dehydrogenase levels, PCR to identify human RNA, and cytokine measurements. The results showed presence of SC in the ipsilateral and contralateral regions of the lesion suggesting neuroprotection of uninjured tissue, in addition to immunomodulation, neovascularization, increased cell proliferation and microglia.8 (See table 1.2).
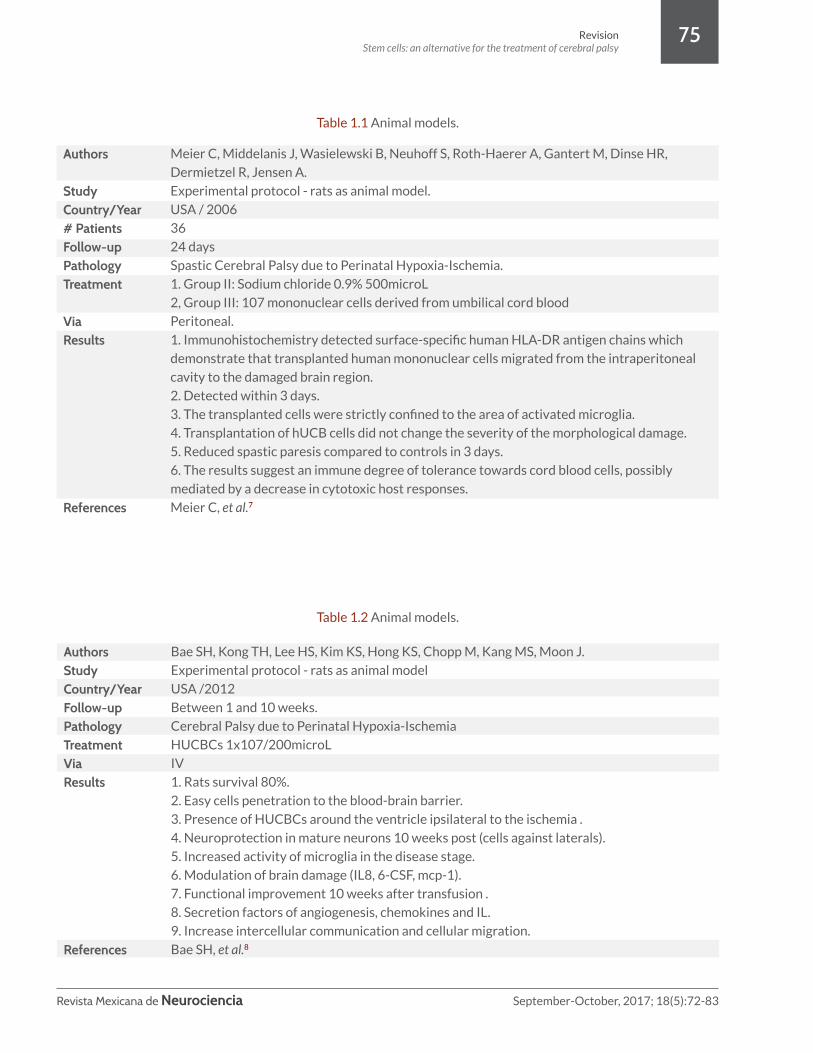
Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
75
Authors
StudyCountry/Year# PatientsFollow-up PathologyTreatment
ViaResults
References
Meier C, Middelanis J, Wasielewski B, Neuhoff S, Roth-Haerer A, Gantert M, Dinse HR,
Dermietzel R, Jensen A.
Experimental protocol - rats as animal model.
USA / 2006
36
24 days
Spastic Cerebral Palsy due to Perinatal Hypoxia-Ischemia.
1. Group II: Sodium chloride 0.9% 500microL
2, Group III: 107 mononuclear cells derived from umbilical cord blood
Peritoneal.
1. Immunohistochemistry detected surface-specific human HLA-DR antigen chains which
demonstrate that transplanted human mononuclear cells migrated from the intraperitoneal
cavity to the damaged brain region.
2. Detected within 3 days.
3. The transplanted cells were strictly confined to the area of activated microglia.
4. Transplantation of hUCB cells did not change the severity of the morphological damage.
5. Reduced spastic paresis compared to controls in 3 days.
6. The results suggest an immune degree of tolerance towards cord blood cells, possibly
mediated by a decrease in cytotoxic host responses.
Meier C, et al.7
Table 1.1 Animal models.
Table 1.2 Animal models.
AuthorsStudyCountry/YearFollow-up PathologyTreatment ViaResults
References
Bae SH, Kong TH, Lee HS, Kim KS, Hong KS, Chopp M, Kang MS, Moon J.
Experimental protocol - rats as animal model
USA /2012
Between 1 and 10 weeks.
Cerebral Palsy due to Perinatal Hypoxia-Ischemia
HUCBCs 1x107/200microL
IV
1. Rats survival 80%.
2. Easy cells penetration to the blood-brain barrier.
3. Presence of HUCBCs around the ventricle ipsilateral to the ischemia .
4. Neuroprotection in mature neurons 10 weeks post (cells against laterals).
5. Increased activity of microglia in the disease stage.
6. Modulation of brain damage (IL8, 6-CSF, mcp-1).
7. Functional improvement 10 weeks after transfusion .
8. Secretion factors of angiogenesis, chemokines and IL.
9. Increase intercellular communication and cellular migration.
Bae SH, et al.8
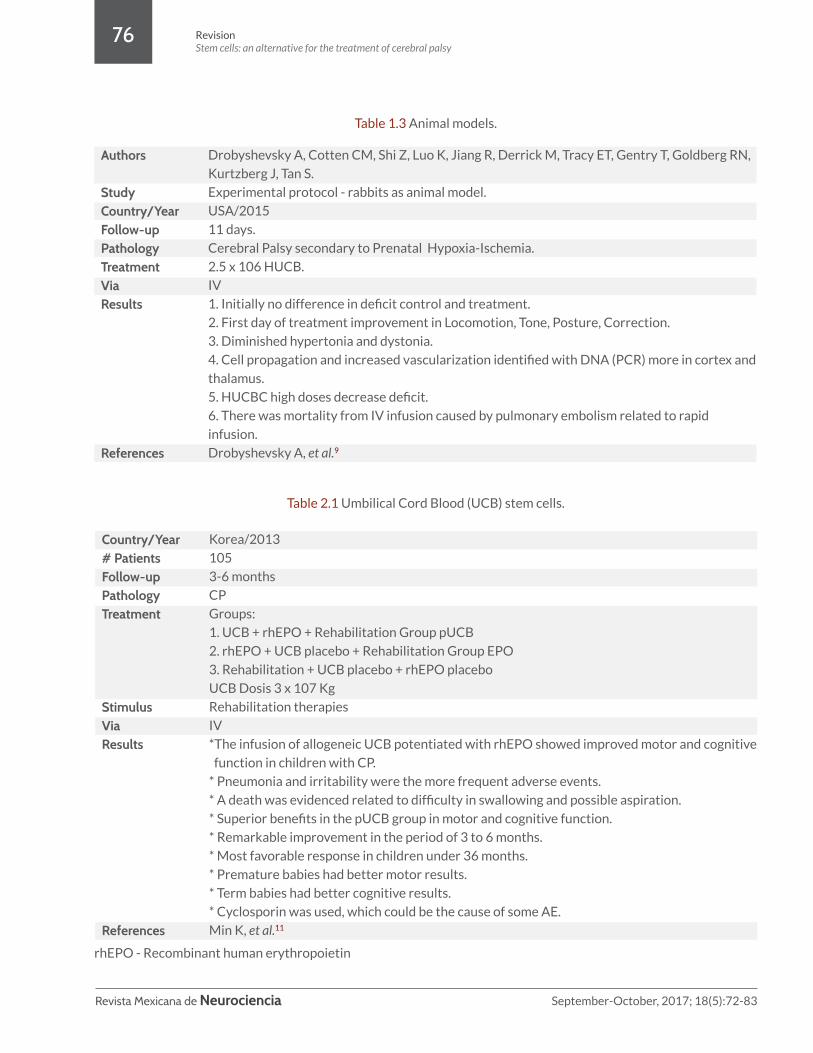
Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
76
Authors
StudyCountry/YearFollow-up PathologyTreatment ViaResults
References
Drobyshevsky A, Cotten CM, Shi Z, Luo K, Jiang R, Derrick M, Tracy ET, Gentry T, Goldberg RN,
Kurtzberg J, Tan S.
Experimental protocol - rabbits as animal model.
USA/2015
11 days.
Cerebral Palsy secondary to Prenatal Hypoxia-Ischemia.
2.5 x 106 HUCB.
IV
1. Initially no difference in deficit control and treatment.
2. First day of treatment improvement in Locomotion, Tone, Posture, Correction.
3. Diminished hypertonia and dystonia.
4. Cell propagation and increased vascularization identified with DNA (PCR) more in cortex and
thalamus.
5. HUCBC high doses decrease deficit.
6. There was mortality from IV infusion caused by pulmonary embolism related to rapid
infusion.
Drobyshevsky A, et al.9
Table 1.3 Animal models.
Table 2.1 Umbilical Cord Blood (UCB) stem cells.
Country/Year# PatientsFollow-up PathologyTreatment
StimulusViaResults
References
Korea/2013
105
3-6 months
CP
Groups:
1. UCB + rhEPO + Rehabilitation Group pUCB
2. rhEPO + UCB placebo + Rehabilitation Group EPO
3. Rehabilitation + UCB placebo + rhEPO placebo
UCB Dosis 3 x 107 Kg
Rehabilitation therapies
IV
*The infusion of allogeneic UCB potentiated with rhEPO showed improved motor and cognitive
function in children with CP.
* Pneumonia and irritability were the more frequent adverse events.
* A death was evidenced related to difficulty in swallowing and possible aspiration.
* Superior benefits in the pUCB group in motor and cognitive function.
* Remarkable improvement in the period of 3 to 6 months.
* Most favorable response in children under 36 months.
* Premature babies had better motor results.
* Term babies had better cognitive results.
* Cyclosporin was used, which could be the cause of some AE.
Min K, et al.11
rhEPO - Recombinant human erythropoietin

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
77
A 2015 Duke University study by Drobyshevsky et al. was performed on rabbits with prenatal ischemia induced by occlusion of the uterine artery at 22 days of gestation and subsequent reperfusion until birth (31.5 days). This was followed by intravenous transfusion of 5x106 UCB-derived stem cells. When the results were analyzed there was a significant improvement (p<0.05) at five days in posture, at five and 11 days in locomotion, and at five and 11 days in tone and dystonia, which was correlated with an increase in cellular concentration. There was significant improvement (p<0.05) in all domains at five and 11 days with low doses.9 (See table 1.3)
Stem Cells and Cerebral Palsy - Clinical TrialsAt www.clinicaltrials.gov there are 24 clinical trials of SC treatment in patients with CP, of which the following have shown results:10
Studies with UCB-derived SCA double-blind, randomized, placebo-controlled study was undertaken in 2013 by Min, et al. They studied the therapeutic potential of UCB-derived SC with erythropoietin (rhEPO) and rehabilitation in 105 children with a three to six months follow-up. The results showed that the infusion of allogeneic UCBSCs enhanced with rhEPO achieved a superior response than the placebo groups in terms of motor and cognitive function in children with CP, and the response in patients younger than 36 months was better. Some adverse events were reported, related to the use of cyclosporine. Failure in the group with single transplantation does not allow the conclusion to be drawn as to whether the improvement in functionality was due to SC or the use of cells enhanced with rhEPO.11 (Table 2.1)
A study conducted in 2014 by Cotten, et al. treated 23 patients with hypoxic-ischemic encephalopathy with intravenous transfusion of UCB-derived cell analogs in doses of 1-5 x 107 cells, with a 12-month follow-up. The study did not show any adverse events (there were two deaths unrelated to the therapy, due to the severity of the comorbidities) and resulted in improvement of at least three of the six domains evaluated: 1. Level of consciousness, 2. Spontaneous activity, 3. Tone, 4. Posture, 5.
Primitive reflexes, and 6. Autonomous functions.12
(Table 2.2)
In 2015, the study conducted by Feng, et al. evaluated the safety of umbilical cord-derived allogeneic SC therapy in 47 patients with CP. The transplanted doses of 2-3 x 107 were given in four to eight injections, the first intravenous and the remaining intrathecal. The paraclinical evaluation, signs, symptoms, and vital signs measurements resulted in normal pre- and post-infusion paraclinicals (<0.05), with no evidence of adverse events from the initial IV infusion. The intrathecal infusion, however, did report adverse events such as 42.6% fever, 21.2% vomiting, three convulsions, three headaches, two respiratory infections, two incidences of dermatitis, one abdominal pain and constipation. An age of ≤10 years old at onset of treatment was identified as a significant risk factor (=0.036) to develop AE.13 (Table 2.3)
The study conducted in 2015 at Duke University by Romanov, et al. included 80 patients who received intravenous infusion of 3-3.5 x 108 UCBSC and follow-ups from 3 to 36 months. No adverse events were reported. Significant improvement in the tone of the limbs was evident (p=0.0002-0.0004), upper extremity strength (p=0.025), reduction of the epileptic paroxysm, and improvement in the mental sphere (memory, attention, intellectual and emotional development). The results obtained referred to the ability to sit without support (Level IV), walk with support (Level III) or walk without support (Level II). The authors suggest that the therapy was more effective in patients two to six years of age, with a greater number of infusions, and a lesser degree in the severity of the disease.14
(Table 2.4)
Studies with bone marrow-derived SC A study conducted in 2013 by Chen, et al. evaluated the efficacy of bone marrow-derived stem cell therapy in 60 patients with CP, with GMFCS levels III-V. They were administered an intrathecal dose of 1-2 x 107 bone marrow-derived SC with a six-month follow-up. The results show a significant improvement in the GMFM scale score (P=0.011 and 0.001) at three and six months post-transplant,

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
78
compared to the baseline and control group. There was no significant language improvement in any of the groups at one month, three months, and six months (p=0.751, 0.522, and 0.304 respectively). No adverse events were reported.15 (Table 3.1)
Another study was conducted in 2015 by Sharma, et al. They evaluated the safety, viability, and efficacy of intrathecal transplantation of autologous stem cells derived from bone marrow in 40 patients with all types of CP with an intrathecal dose of 10.23 x 106 cells and immunosuppression with prednisolone IV, followed up for six months. The evaluation was performed in different domains, in which significant improvement was found in seated balance (p=0.00443), standing balance (p=0.00443), walking balance (p=0.00443), movement of the extremities (p=0.02334) and nonsignificant improvement in upper extremities tone (p=0.13361), lower extremities tone (p=0.073), and trunk muscles tone (p=0.13361) in the diplegia group. In the quadriplegia group, significant improvement was found in all domains (p<0.05) including oral motor functions (p=0.0015), cephalic support (p=0.00443), and cognition (p=0.0015). SPECT performed at the beginning
of treatment and at six months post-treatment showed increased metabolism in the frontal, temporal, parietal, basal ganglia, thalamus, and cerebellum areas. No severe adverse events were reported.16 (See table 3.2)
Studies with embryonic SCIn 2014, a study by Shroff, et al. reported on the efficacy of therapy with human embryonic stem cells (hESC) in 101 patients <18 years old with CP. There were four phases in which different doses were used, administered subcutaneously, intravascularly, and intrathecally, in addition to the administration of ophthalmic, oral, and otic drops in children with neurosensorial depression. This study reports significant improvement (p<0.05) in all GMFCS levels: 42 patients started on level V, 21 were on level IV, 15 on level III, 12 on II, and one on I. At the end of the study, no patients remained on levels V or IV, 12 patients got to level III, 50 patients to level II, and 29 patients finished on level I. SPECT also showed improvement in perfusion after receiving hESC therapy. In children with hearing impairment there was improvement in hearing closely. Non-severe adverse events were reported only in the early stages of treatment.17 (Table 4)
Country/Year# PatientsFollow-up PathologyTreatment ViaResults
References
USA/2014
23
12 months
Hypoxic-ischemic encephalopathy.
1-5 x 107 UCB cells.
IV
* There was no evidence of adverse events from the infusion.
* No significant changes in the first two infusions (AF, AT, nor O2SAT).
* O2SAT decreased after the third and fourth infusion.
* A patient of 35 weeks gestation with cord pH of 6.72 (stop).
* A patient with E. coli received ampicillin/cefotaxime for 21 days (stop).
* Significant improvement in at least 3 areas.
* Two patients died at 14 months. The first, diagnosed with chromosome 17p12 deletion as well
as Wolff-Parkinson-White (WPW) syndrome, died due to respiratory syncytial virus pneumo
nia. The second with encephalopathy due to severe cystic encephalomalacia, diagnosed with
cytomegalovirus infection during his 5th postnatal week, died of acute gastroenteritis with
hypovolemic shock.
Cotten C M, et al.12
Table 2.2 Umbilical Cord Blood (UCB) stem cells.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
79
Table 2.3 Umbilical Cord Blood (UCB) stem cells.
Table 2.4 Umbilical Cord Blood (UCB) stem cells.
Country/Year# PatientsPathologyTreatment ViaResults
References
China/2015
47
CP
2-3 x 107 UCB cells in 4 to 8 injections.
First infusion IV, rest of infusions intrathecal.
* Normal paraclinical evaluations pre-and post- transfusion.
* No AE in initial IV infusion.
* Adverse events on intrathecal infusion: Fever 42.6%, Vomiting 21.2%, 3 Seizures, 3 Head
aches, 2 Respiratory infections, 2 Dermatitis, 1 Abdominal pain and constipation. All of them
improved with symptomatic treatment at 72 hours.
* More adverse events in children under 10 years.
* Increased motor function.
* Less risk of leukemia, tumors, and infections.
* Safe Therapy.
Feng M, et al.13
Country/Year# PatientsFollow-upPathologyTreatment StimulusViaResults
References
Russia/2015
80
3 to 36 months
CP and related complications.
3-3.5 x 108 UCB cells.
Rehabilitation therapies.
IV
* Neurological improvement (diminished muscle and tone pathology, improved tone of the
limbs, increased muscle strength, reduced paroxysmal epilepsy).
* Improvement in the mental sphere (memory, attention, and intellectual and emotional
development).
* 23 children showed progress in physical and mental areas.
* 17 patients showed no improvement.
* 18 patients showed significative progress in motor activities.
* No adverse events.
* More effective in patients aged 2-6.
* Other predictors of the success of the therapy are the amount of infusion of cells and the
severity of the disease.
* The group of patients who did not respond to the therapy was related to the severity level of
their CP and these patients received no more than two doses.
Romanov YA, et al.14

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
80
Country/Year# PatientsFollow-upPathologyTreatment StimulusViaResults
References
China/2013
60
6 months
CP
1-2 x 107 stem cells derived from bone marrow.
Rehabilitation therapies.
IV
* 1, 3, 6 months after the transfusion were evaluated.
* The two groups increased function in 6 months.
* Control group had no significative changes.
* Treatment group did show significative changes at 3 and 6 months.
* No evidence of adverse events.
* No improvement in language.
Chen G, et al. 15
Table 3.1 Bone marrow stem cells.
Table 3.2 Bone marrow stem cells.
Country/Year# PatientsFollow-upPathologyTreatment StimulusViaResults
References
India/2015
40
6 months
CP
10.23 x 106 stem cells derived from bone marrow.
Rehabilitation therapies.
Intrathecal.
* Diplegia group
100% improvement in sitting balance, 90.91% in gait balance, 90% in movement of upper
extremities, 83.3% in oromotor activities, 80% in cognition, 70% in movement of lower
extremities, 66.6% in language, 50% in ambulation, 45.45% in muscle tone in the lower
extremities, 44.44% in lifting activities, 40% in the trunk’s muscle tone, 36.36% in muscle tone
in the upper limbs.
* Quadriplegia group
83.33% showed improvement controlling the neck, 78.95% in sitting balance, 63.16% in
cognition, 60% in oromotor skills, 54.55% in ambulation, 52.38% in muscle tone in the lower
extremities, 50% in muscle tone in the upper limbs, 45.45% in speech, 45% in the trunk’s
muscle tone, 36.36% in standing balance, 31.58% in walking balance.
* Mixed group
83.33% improvement in speech and foot balance, 66.67% in walking balance, 60% in oromotor
skills, 50% in sitting balance and muscle tone in the lower extremities and trunk, 33.33% in
muscle tone in the upper extremities. The dystonia patients improved.
* 7.5% no improvement.
*17.5% minor improvement.
*50% moderate improvement.
*25% major improvement.
Sharma A, et al.16

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
81
Table 4. Human embryonic stem cells (hesc).
Country/Year# PatientsFollow-upPathologyTreatment StimulusViaResults
References
India/2014
101
12 months.
CP
hESC
Rehabilitation therapies.
SC IV Intrathecal, ophthalmic, otic, and oral drops.
* 69% cognitive improvement.
* 80.3% recognition/sensitization.
* 78.9% aggressiveness.
* 74.5% following commands.
* 29 patients ended in GMFCS-E&R 1.
* 50 patients ended in GMFCS-E&R 2.
* 12 patients ended in GMFCS-E&R 3.
*No patients ended in GMFCS-E&R 4 and 5.
Patients' SPECT showed improvement in perfusion after receiving stem cell therapy.
Shroff G, et al. 17
Every day, children around the world suffer from prenatal, perinatal, or postnatal brain damage, resulting in death, or in some cases PC, and the main cause is typically hypoxic-ischemic encephalopathy. Improved health care strategies in recent years have helped reduce perinatal mortality, but these survivals have resulted in an elevated CP incidence. Current therapeutic strategies, however, have not achieved significant improvement in motor functions or brain repair.
For approximately 20 years, the therapeutic potential of stem cells has been studied in multiple brain pathologies such as stroke, hypoxic-ischemic encephalopathy, autism, CP, and degenerative diseases.6 Nevertheless, current clinical trials in CP are limited.
Although the studies about this therapy are in phases I and II of scientific investigation at the
Discussionmoment, we can consider, thanks to some animal models and clinical trials, that the analog or autologous stem cell therapies are a promising alternative for the treatment of children with CP.6
Stem cells are a great opportunity in CP because by many paracrine and trophic factors they generate brain repair and, later, functional rehabilitation.6 In animal models, there has been evidence of improved motor function following the transfusion of stem cells derived from umbilical cord by multiple mechanisms - such as cell migration from the site of injection to the lesion site, and even to the contralateral site of the lesion, which is related to a neuroprotective effect. In addition, other effects found in these studies include the evidence of the presence of human stem cells in the animal brain identified through immunohistochemistry of human HLA.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
82
Conclusion
Stem cells have a great potential for brain repair and functional rehabilitation with minimal adverse events; however, more controlled and more specific clinical trials are required to demonstrate the long-term efficacy and safety of patients.
FundingThe authors have not declared any funding source for this scientific report.
Conflict of interestThere are no conflicts of interest for any of the authors in this scientific report.
The clinical trials analyzed in this document demonstrate stem cell safety and suggest efficacy in the rehabilitation of children with CP. The mechanisms by which the brain repair is developed are not clear; however, in animal models, we can see changes such as cellular migration, neovascularization, and production of endogenous stem cells with posterior remyelination, which produce an improvement in the motor and cognitive functions. In spite of the significant findings from these studies, there is a lack of data for the exact evaluation of the improvement in the patients studied, such as the specific progress of each CP level according to the GMFCS scale. All studies demonstrate the safety of this therapy as there are no reports of severe post-transfusion adverse events. All investigations have evaluated the patients in a period ranging from three months to a maximum of 36 months, making it difficult to assess the adverse effects and long-term functionality of the individuals studied.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):72-83
RevisionStem cells: an alternative for the treatment of cerebral palsy
83
1. Eugenia Espinosa. (2007). Parálisis Cerebral. Neuropediatría. (175 - 184). Bogotá (Colombia): ASCONI.
2. Definition. (s.f). (Recuperado el 27 febrero de 2016, de http://www.cerebralpalsy.org/about-cerebral-palsy/definition)
3. Cause of Cerebral Palsy. (Recuperado el 27 febrero de 2016, de http://www.cerebralpalsy.org/about-cerebral-palsy/cause)
4. Types of Cerebral Palsy, (Recuperado el 27 febrero de 2016, de http://www.cerebralpalsy.org/about-cerebral-palsy/types-and-forms)
5. LM Ávila Portillo, et al. (2012). “Las células madre, piedra angular de rejuvenecimiento”. Aclarando conceptos. MED, DOI:10.4464/MD.2012.40.1.5002, 8. 22/02/2016
6. Jessica M. Sun & Joanne Kurtzberg. (2015). Cord blood for brain injury. Cytotherapy, 17: 775-785, 11. 03/02/2016, De Pubmed Base de datos.
7. Meier, C, Middelanis, J, et al, “Spastic Paresis After Perinatal Brain Damage in Rats is Reduced by Human Cord Blood Mononuclear Cells”. 2006 International Pediatric Research Foundation. Inc.2006;59:
8. Sang-Hun Bae, Tae-Ho Kong, et al. “Long-Lasting Paracrine Effects of Human Cord Blood Cells on Damaged Neocortex in an Animal Model of Cerebral Palsy” College of Life Science, Department of Applied Bioscience, CHA University, Seoul, South Korea. Cell Transplantation. Vol. 21, pp. 2497–2515, 2012.
9. Drobyshevsky, A, Cotton, M, et al, “Human Umbilical Cord Blood Cells Ameliorate Motor Deficits in Rabbits in a Cerebral Palsy Model”. a Department of Pediatrics, NorthShore University HealthSystem, Evanston, Ill. , and b Department of Pediatrics and c Robertson Cell and Translational Therapy Program, Duke University, Durham, N.C. , USA. March 17, 2015
10. 24 studies found for: STEM CELL AND CEREBRAL PALSY. (s.f). (Recuperado el 24 febrero de 2016, de https://clinicaltrials.gov/ct2/results/map? term=STEM+CELL +AND+CEREBRAL+PALSY).
11. Min, Kyunghoon et al. “Umbilical Cord Blood Therapy Potentiated with Erythropoietin for Children with Cerebral Palsy: A Double-Blind, Randomized, Placebo-Controlled Trial.” Stem Cells. (Dayton, Ohio) 31.3 (2013): 581–591. PMC. Web. 19 Feb. 2016.
12. Cotten, C. Michael et al. “Feasibility of Autologous Cord Blood Cells for Infants with Hypoxic-Ischemic Encephalopathy.” The Journal of pediatrics. 164.5 (2014): 973– 979.e1. PMC. Web. 20 Feb. 2016.
13. Feng, Mei et al. “Safety of Allogeneic Umbilical Cord Blood Stem Cells Therapy in Patients with Severe Cerebral Palsy: A Retrospective Study.” Stem Cells International. 2015 (2015): 325652. PMC. Web. 29 Feb. 2016.
14. Romanov, Y, Tarakonov, O, et al, Human allogeneic AB0/Rh-identical umbilical cord blood cells in the treatment of juvenile patients with cerebral palsy.Rusia. 2015; 17: 969e978
15. Chen, Guojun et al. “Neural Stem Cell-like Cells Derived from Autologous Bone Mesenchymal Stem Cells for the Treatment of Patients with Cerebral Palsy.” Journal of Translational Medicine. 11 (2013): 21. PMC. Web. 19 Feb. 2016.
16. Sharma, Alok et al. “A Clinical Study of Autologous Bone Marrow Mononuclear Cells for Cerebral Palsy Patients: A New Frontier.” Stem Cells International. 2015 (2015): 905874. PMC. Web. 29 Feb. 2016.
17. Shroff, Geeta, Anupama Gupta, and Jitender Kumar Barthakur. “Therapeutic Potential of Human Embryonic Stem Cell Transplantation in Patients with Cerebral Palsy.” Journal of Translational Medicine. 12 (2014): 318. PMC. Web. 29 Feb. 2016.
18. Armstrong, R. W. (2007), Definition and classification of cerebral palsy. Developmental Medicine & Child Neurology, 49: 166. doi: 10.1111/j.1469-8749.2007.00166.
References
Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
84
Neuropsychological evaluation of pragmatics in a patient with acquired brain injury
Evaluación neuropsicológica de la pragmática de la comunicación en un paciente con daño cerebral adquirido
Case report
Nekane Galparsoro-Izagirre,1,2 Ignacio Sánchez-Cubillo,3 Malen Migueles,4 Daniel Adrover-Roig.5
1Red Menni de Daño Cerebral, Hospital Aita Menni, Bilbao, 2Basque Center on Cognition, Brain and Language, 3Red Menni de Daño Cerebral, Hospital Aita Menni, Donostia, 4Universidad del País Vasco, 5Universitat de les Illes Balears
AbstractStudies in patients with brain injury have provided to clinical practice a wide range of valuable language assessment tools and rehabilitation strategies. In contrast, the ability to make a proper use of language adapted to a specific social and cultural context has been scarcely explored in brain-damaged patients. Therefore, clinicians still lack specific assessment batteries to diagnose pragmatic difficulties in these patients. Given the importance of such disorders on their social and professional reinsertion, we aimed at studying the usefulness of the Montréal Protocol for the Evaluation of Communication (MEC) in order to detect abnormal pragmatic capacities in a patient with a brain injury, as compared to a control participant. In addition, we explored the role of other cognitive processes, such as executive functions and social cognition on pragmatics. Results revealed that the MEC is a useful protocol to structure and guide the evaluation process of pragmatics, and it is sensitive to most of the symptoms observed at baseline. A partial dissociation between executive control and pragmatics was evident in the presented case, along with an impaired ability to recognize facial emotions, a difficulty that might explain some of the symptoms observed at the pragmatic level.
Keywordscommunication, brain injury, assessment

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
85
Resumen
El lenguaje y sus alteraciones en pacientes con lesiones cerebrales han sido extensamente estudiados, y han aportado a la práctica clínica valiosos instrumentos de evaluación y diversas estrategias de rehabilitación. En contraposición, la habilidad para realizar un correcto uso del lenguaje adaptado a un contexto social y cultural, ha sido muy poco explorada en pacientes con lesiones cerebrales. Por ello, hasta la fecha, los clínicos carecen de baterías de evaluación específicas para diagnosticar las dificultades pragmáticas en pacientes con daño cerebral. Dada la importancia que este tipo de alteraciones tienen sobre la reinserción social y laboral, nos planteamos estudiar la utilidad del Protocolo para la Evaluación de la Comunicación de Montréal (MEC) para la detección de las alteraciones de la pragmática en un paciente con una lesión cerebral en comparación con un sujeto control. Además, exploramos el papel de otros procesos cognitivos, como las funciones ejecutivas y la cognición social en la pragmática de la comunicación. Los resultados revelaron que el Protocolo MEC es útil para estructurar y guiar la exploración y es sensible a la mayor parte de la sintomatología observada al inicio. Se aprecian signos de disociación entre ciertos aspectos ejecutivos y la pragmática de la comunicación junto con una alteración en la capacidad de reconocimiento facial de emociones. Este aspecto podría explicar parte de la sintomatología observada a nivel pragmático en el paciente.
Palabras clavecomunicación, daño cerebral, evaluación
Correspondence: Daniel Adrover RoigCtra. de Valldemossa, Km. 7.5. Edificio Beatriu de Pinós #20Phone: +34 971 17 24 26E-mail: [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
86
Introduction Case reportLanguage and aphasia have been studied extensively1 but that’s not the case with communication, which requires interaction among several interlocutors and is governed by rules and conventions determined by the socio-cultural context. Pragmatics is of special importance in dialogue: the way in which interlocutors make use of the language in a given context. The respect for taking turns in conversation, an adequate understanding and expression of prosody, the ability to follow social rules, grasp intentionality and understand indirect language are fundamental skills for effective communication.The alteration of these features has a significant impact on the social and work life of the affected individual.2
Communication is a complex social behavior with an underlying diversity of social and cognitive variables.3 Traditionally, the focus has been placed on the executive functions such as variables that explain the alterations in social behavior,4 whose recent development opens the door to recognition of facial expressions5 or Theory of Mind6 as new hypotheses. However, clinicians do not possess sufficient instruments to evaluate in a systematic and standardized way all these aspects in adults with acquired brain injuries.
The following is the case of a patient with trouble maintaining an adequate communicative interaction due to important pragmatic deficits, and an evaluation protocol is proposed to try to collect information in a structured way of all the variables involved in the communication process. These instruments are administered to a control participant to compare the performance on tests that have no scales.
L.S. is a 38-year-old male, with no relevant medical history. On 10/8/2011 he suffered severe cranioencephalic trauma. He scored 7/15 on the Glasgow Coma Scale (GCS) and on TAC presented multiple bilateral temporoparietal subcortical contusions, a right temporoparietal subdural hematoma and a longitudinal fracture of the right petrous part. It required a bifrontal decompressive craniotomy. He remained in an induced coma for 12 days and the post-traumatic amnesia lasted five weeks. Three months after the injury he started outpatient rehabilitation treatment. At that moment he had overcome the state of post-traumatic confusion, was able to saunter, and was self-sufficient in his daily life activities.
However, he presented a significant verbal disinhibition, hasty speech, and frequent articulation errors (altering the sounds /l/, /r/, /z/, /d/ and consonant groups such as /tl/ or /dr/). He presented a slightly monotonous prosody and expressive blocks caused by difficulty in accessing vocabulary, difficulty with social skills and infantilism, showing a partial awareness of the deficit (5 points over 7). In contact with his social environment, he had difficulty adjusting the conversation topic to his interlocutor, as well as the amount of information transmitted. He tended to interrupt and to not cede the conversation turn, tending towards monolog, giving extensive replies that were imprecise. He showed behavior inappropriate for the context and gave advice to strangers. Furthermore, the family noticed a change in his facial expression. Considering his good progress, the absence of significant motor, cognitive, and language problems, and his personal autonomy, the issues related to his social interaction became fundamental. Henceforth, the recovery of social and conversational skills became one of the main objectives, for they would determine his social reintegration. For contrast, a 41-year-old control participant was selected with equivalent educational level and social environment.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
87
The following tests were administered to the patient and to the control subject.
- The Montreal Protocol for the Evaluation of Communication (MEC): 7 evaluates alterations in communication, including the discursive, prosodic, lexical-semantic, and pragmatic components. Faces test:8 evaluates the ability to comprehend basic mental states16 (happiness, sadness, anger, surprise, fear, and disgust) and complex ones (desire, interest, preoccupation, suspicion) through facial expressions. Eyes test – revised:9 evaluates the comprehension of complex mental states observing the eyes. Faux Pas Recognition Test:5 measures the comprehension of social situations and the capacity to infer mental states through short stories describing different social situations with and without inadequate commentaries to detect. Other instruments: The Wisconsin Card Sorting Test (WCST),10 the Tower of London (TOL),11 and the Trail Making Test (TMT-A y TMT-B)12 were administered to evaluate executive functions.
The results obtained in the MEC (Figure 1) show difficulty in the ability to comprehend and express emotion through voice inflection, using the same
melody to express happiness, sadness, and anger. It is below the average and the control in the interpretation of indirect speech acts (Figure 2), in which he should decipher non-literal messages based on the context (‘I have a headache’ implying to lower the music volume). In the interpretation of metaphors (‘My son is a saint’) and idiomatic expressions (‘He made a decent woman out of her’), he situated in the normal, though showing a marked tendency to add unnecessary information and to use inappropriate arguments. In narrative discourse, there are major difficulties to handle information as it is broadened (Figure 2). Does not perform an adequate selection of relevant information and adds, omits, and modifies details, resulting in an unclear discourse with no conductive thread. In the assignment to give a title to the text, there was no inference in the two given opportunities. In the analysis of conversational discourse there is a marked tendency to logorrhea, constantly using crutches (‘no worries’, ‘phenomenal’), repeats content and makes sudden changes in the conversation topics, continuously bringing them back to his focus of interest: his present situation. He does not cede and even ‘steals’ the conversation turn.
20
18
16
14
12
10
8
6
4
2
0
MEC - Prosody -
*
*
*
*
Dire
ct s
core
s in
the
MEC
Comprehension
Linguistic prosody
Control L.S. Cut-off point
Emotional prosody
Repetition Comprehension Repetition Production
Figure 1. Scores in linguistic and emotional prosody (MEC).
Note: * Process altered, according to the cut-off point established by scales.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
88
50
45
40
35
30
25
20
15
10
5
0
MEC - Metaphors/Acts/Discourse -
**
*
**
*
*
Dire
ct s
core
s in
the
MEC
Explanations
Metaphors Speech acts
Answerchoice
Explanations Questionnaire InferenceAnswerchoice
Partialmemory
Full memory
Conversationaldiscourse
Narrative discourse
Control L.S. Cut-off point
Figure 2. Scores for metaphors, speech acts, and narrative discourse (MEC).
Figure 3. Scores in social cognition tests.
Note: * Process altered, according to the cut-off point established by scales.
Control L.S. Max.
**
*
40
35
30
25
20
15
10
5
0
Num
ber o
f cor
rect
ans
wer
s
Social cognition
Eyes test Faces test
Eyes/Faces
Slip detection Slipcomprehension
Mental statuscomprehension
Slip absencedetection
Comprehensionof text without
a slipFaux Pas
In the facial recognition tests (Figure 3) L.S. made four mistakes out of 20 in the faces test, three of them in the complex mental states items (bored, interested, and arrogant), while the control subject made no mistakes. In the eyes test, he made twice as many
mistakes as the control and is below average according to the scale.13 In the Faux Pas test, he gets 9 out of 10 situations right, though he has difficulty understanding the mental state of the characters and recognizing the emotions of the victims of the slip (Figure 3).

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
89
Table 1. Results of the executive functions tests.
a: Formula for calculation: [n (total cards) – (n categories x cards/category + random mistakes)]; b : Score obtained in function of the number of movements performed to carry out the test; t = time; PC= percentile; *: Low scores regarding the scale and/or the control subject to clinical judgement.
The Wisconsin Card Sorting Test
Tower of London
Trail Making Test
L.S.6 categories
106 cards*
(40 perseverative mistakesa)*
34/36b
TMT A t=30"
TMT B t=69"
TMT B-A T=39"
Control6 categories
69 cards
(3 perseverative mistakes)
33/36
TMT A T=34"
TMT B T=67"
TMT B-A T=33"
In the WCST he shows a number of perseverative errors far above the control and as for the TMT, according to scale14 a slight slowing down is observed.
The TMT B-A tool that evaluates alternating attention was in normal ranges (Table 1). His TOL results are adequate.
The MEC protocol has been sensitive to the majority of L.S.’s clinical symptomatology and picks up on difficulties that were not revealed in observation, such as the alteration of the ability to express and comprehend emotional prosody. The protocol allows a finer evaluation than simple observation since it makes a distinction between linguistic and emotional prosody. Along this line, it’s been found that brain injury patients with inappropriate social behaviors have as much difficulty recognizing emotional expressions correctly as for recognizing prosody.15 However, L.S.’s clinical symptomatology revealed other problems which the MEC did not detect, such as the difficulties in the interpretation of non-literal language. The results showed difficulty only in the comprehension of indirect speech acts, but not of metaphoric or idiomatic expressions. These difficulties could explain his uncertainty, which leads to a continuous search for explanations for every arising comment. The MEC has not been sensitive to the problems adapting to the context and interlocutor in regards to the
Discussion
choice of what and how much to say, as well as to whom. There is a preservation of the abilities related to planning (TOL) and alternating attention, but not in regards to cognitive flexibility (WCST). Therefore, there is a relative dissociation between the pragmatic processes and some of the executive processes in this patient. These results support previous studies that showed that the abilities encompassed in the term ‘social cognition’ can be relatively independent of the ones related to the executive control.16
The results in the Faces Test, the Eyes Test, and the Faux Pas show his difficulties identifying the emotions of his interlocutors. Therefore, he is unable to tune the content and length of discourse according to the interest of his interlocutor leading him to lead the conversations. All these aspects highlight the complexity of the analysis of communication and social behaviors, as well as the importance of a fine-tuning of these tests to the cultural characteristics of the evaluated subject.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
90
Conflict of interestThere are no potential conflicts of interest for any of the authors in this scientific report.
FundingThere is no funding for this scientific report.
Conclusion
The MEC Protocol and other evaluation instruments have provided relevant information about this patient’s pragmatic abilities, objectifying part of his clinical symptomatology and expanding the information to that obtained in the interview. The alteration in the pragmatics presents with a high frequency of perseverative behaviors. It is recommended to adapt the MEC Protocol to the Spanish-speaking population and design situations closer to quotidian life to value the pragmatics in patients with acquired brain damage.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):84-91
Case reportPragmatics in brain injury
91
1. Tippett DC, Niparko JK, Hillis AE. Aphasia: Current concepts in theory and practice. J Neurol Transl Neurosci. 2014; 2: 1042.
2. Muñoz-Céspedes JM, Melle N. Alteraciones de la pragmática de la comunicación después de un traumatismo craneoencefálico. Rev Neurol. 2010; 38: 852-859.
3. Milders M, Fuchs S, Crawford JR. Neuropsychological Impairments and changes in emotional and social behaviour following severe traumatic brain injury. J Clin Exp Neuropsychol. 2003; 25: 157-172.
4. Ubukata S, Tanemura R, Yoshizumi M, Sugihara G, Murai T, Ueda K. Social cognition and its relationship to functional outcomes in patients with sustained acquired brain injury. Neuropsychiatr Dis Treat. 2014; 10: 2061-2068.
5. Ruffman T, Slade L, Rowlandson K, Rumsey C, Garnham A. How language relates to belief, desire and emotion understanding. Cognitive Development. 2003; 18: 139-158.
6. Tate RL. Executive dysfunction and characterological changes after traumatic brain injury: Two sides of the same coin? Cortex. 1999; 35: 39-55.
7. Ferreres A, Abusamra V, Cuitiño M, Côté, H, Ska B, & Joanette Y. Protocolo MEC. Protocolo para la evaluación de la comunicación de Montreal. Buenos Aires: Neuropsi Ediciones; 2007.
8. Baron-Cohen S, Wheelwright S, Jolliffe T. Is there a ‘language of the eyes’? Evidence from normal adults and adults with autism or Asperger syndrome. Vis Cogn. 1997; 4: 311-331.
9. Baron-Cohen S, Wheelwright S, Hill J, Raste Y, Plumb I. The ‘Reading the Mind in the Eyes’ Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiat. 2001; 42: 241-251.
10. Heaton RK, Cheleune GJ, Talley JL, Kay GG, Curtis G. Wisconsin Card Sorting Test (WCST): Manual revised and expanded. Odessa: Psychological Assessment Resources; 1993.
11. Shallice T. Specific impairments in planning. Philosophical Transcripts of the Royal Society of London 1982; 298: 199-209.
12. Reitan RM. Trail Making Test: Manual for administration and scoring. Tucson, AZ: Reitan Neuropsychology Laboratory; 1958.
13. Román F, Rojas G, Román N, Iturry M, Blanco R, Leis A, et al. Baremos del Test de la mirada en español en adultos noramles de Buenos Aires. Rev Neuropsicología Latinoamericana. 2012; 4: 1-5.
14. Periáñez JA, Ríos-Lago M, Rodríguez-Sánchez JM, Adrover-Roig D, Sánchez-Cubillo I, Crespo-Facorro B, et al. Trail Making Test in traumatic brain injury, schizophrenia, and normal ageing: sample comparisons and normative data. Arch Clin Neuropsychol. 2007; 22: 433-447.
15. Guranski K, Podemski R. Emotional prosody expression in acoustic analysis in patients with right hemisphere ischemic stroke. Neurol Neurochir Pol. 2015; 49:113-120.
16. Lough S, Gregory C, Hodges JR. Dissociation of social cognition and executive function in frontal variant frontotemporal dementia. Neurocase. 200; 7: 123-130.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
92
Endovascular treatment of giant pseudoaneurysms of the cervical internal carotid artery: case report and review of the literature
Tratamiento endovascular de pseudoaneurismas gigantes de la arteria carótida interna cervical: a propósito de un caso y revisión de la literatura
Case report
Gustavo Melo-Guzmán,1 Víctor Hugo Escobar-de la Garma,1 Omar Antonio Pérez-Morales,1 Felipe Padilla-Vázquez,1 Jorge del Bosque Méndez,2 Rafael Mendizábal-Guerra.1
1 Servicio de Neurocirugía del Hospital Juárez de México. Ciudad de México.2 Servicio de Cirugía de Cabeza y Cuello del Hospital Juárez de México. Ciudad de México.
Abstract
Introduction. Cervical internal carotid pseudoaneurysms are vascular lesions with high morbidity due to embolism and rupture. Surgery of these lesions is technically difficult, with low success rates. Nowadays, endovascular therapy has allowed favorable results with the use of covered-stents allowing vessel reconstruction.
Case report. A 45-year male with a past history of right blunt cervical trauma three years ago was admitted for study of a pulsatile right cervical mass. He reported headache 6 months before admission and progressive dysphagia with a protruding non-painful pulsatile mass in the right cervical region, causing dysphonia. A contrast-enhanced cervical computed tomography scan and the angiogram revealed a giant pseudoaneurysmal lesion in the cervical segment of the right internal carotid artery. The first endovascular procedure in which “stent in stent” technique was performed achieved 70% embolization of the aneurysm one year later. New angioplasty with a covered stent inside the previous ones achieved 90% embolization of the pseudoaneurysm. Eleven months later a new angiogram revealed definite embolization of the aneurysm.
Conclusion. The use of stents may be now a feasible and safe way of treating selected cases of giant pseudoaneurysms of the cervical internal carotid artery.
Keywordspseudoaneurysm, endovascular therapy, internal carotid artery, stent in stent, covered stent.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
93
Resumen
Introducción. Los pseudoaneurismas de la arteria carótida interna cervical son lesiones vasculares con alta morbilidad por su elevado riesgo de embolismo y ruptura. La cirugía de estas lesiones es técnicamente difícil, con tasas de éxito no siempre favorables. Actualmente la terapia endovascular ha demostrado resultados exitosos con baja morbimortalidad.
Reporte de caso: Paciente masculino de 45 años con el antecedente de trauma cervical contuso tres años atrás estudiado por masa cervical pulsátil derecha. Reportó cefalea frontal progresiva y disfagia insidiosa con la aparición de masa no dolorosa y pulsátil en la region cervical derecha condicionando disfonía. La angiotomografía computada cervical y angiografía reveló una lesión aneurismática gigante originada de la arteria carótida interna cervical derecha. Se realizó técnica de “stent in stent” obteniendo reconstruccion del vaso y trombosis inicial del 70% un año después. Nueva angioplastía con stent cubierto obtuvo embolización del 90%, lograndose trombosis y oclusion del 100% en el control angiográfico 11 meses después.
Conclusión. El uso de stents cubiertos puede ser una manera feasible y segura de tratar casos seleccionados de pseudoaneurismas gigantes en la arteria carótida interna cervical.
Palabras clavepseudoaneurisma, terapia endovascular, arteria carótida interna, stent in stent, stent cubierto.
Corresponding author:Víctor Hugo Escobar-de la GarmaAv. Instituto Politécnico Nacional 5160, Del. Gustavo A. Madero,Col. Magdalena de las Salinas CP 07760. Ciudad de México, México.Phone: (01) 55 5747 7560E-mail: [email protected], [email protected]

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
94
Introduction
Case report
Carotid and vertebral pseudoaneurysms are rare vascular lesions which may occur due to disruption of the arterial wall after trauma, invasion by tumor, radiation necrosis or mycotic infection.1-3
Surgery to treat these lesions has fallen into disuse due to the great technical requirements involved, the significant morbidity and mortality associated with the procedure, and the low success rate.4
Endovascular therapy has substituted open procedures by being minimally invasive and presenting minimum morbidity as well as high technical success rates.4 The embolization with coils and balloons has fallen into disuse and been substituted by covered stent placements, which allow to reconstruct the geometry of the parent vessels, recover their permeability, and achieve the subsequent regression of the pseudoaneurysm wall.5
The goal of this report is to describe the complex and progressive treatment of giant cervical pseudoaneurysms by endovascular approach and to review the literature.
A 45-year-old man was admitted to our hospital with a history of blunt trauma in the right cervical region five years before. An onset of insidious intermittent dry cough began in that period. Subsequently, it was accompanied by an intermittent oppressive frontal holocranial headache of progressively high intensity, partially attenuated with conventional analgesics. Months prior to visiting our hospital, he presented an increase in volume in the right pharyngeal region that produced changes in voice and limited swallowing, for which he consulted with an otorhinolaryngologist who, in turn, referred him to our institution.
In the physical examination we found a rounded
mass, pulsatile and ill-defined, palpable in the right lateral region of the neck, non-painful, attached to deeper structures, of soft consistency, measuring approximately five centimeters in its wider diameter, extending to the oral cavity and the posterolateral oropharyngeal wall, obliterating 60% of it, making swallowing difficult.
Contrast-enhanced computer tomography of the cervical area (Figure 1) revealed obliteration of the right parapharyngeal space by a rounded mass of thick wall that captured contrast medium homogeneously and extended to the posterolateral oropharynx wall, connecting to the right internal carotid artery, and displacing the internal jugular vein dorsally and laterally. In sagittal and coronal reconstructions it was confirmed that the dilation depended on the right internal carotid artery in its cervical portion.
The initial cerebral pan-angiography revealed the existence of a giant saccular pseudoaneurysm of 40 x 50 mm in its diameters, rostrocaudal and mediolateral respectively, in the middle and upper third of the cervical segment of the right internal carotid artery, accompanied by the phenomenon of stealing from the right anterior cerebral artery. (Figure 2) Two months later, carotid angioplasty was performed using two stents (WallstentTM
Endoprosthesis, Boston Scientific, Natick, MA, USA) telescoped (stent in stent) at the point of the pseudoaneurysm (Figure 3) and a year later an angiographic control revealed thrombosis of 70% of the lesion and improvement of the blood flow of the anterior cerebral circulation. It was decided to undertake a new angioplasty with ePTFE (Expanded Polytetrafluoroethylene) covered stent of 8 mm x 8 cm (FLUENCY® plus Vascular Stent Graft, BARDpv Crawley, West Sussex, England) inside both Carotid Wallstents with immediate angiographic thrombosis result of 90% of the pseudoaneurysm and total reconstruction of the artery two years after the initial procedure (Figure 4).

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
95
Figure 1. Axial (a), coronal (b) and sagittal (c) contrast-enhanced CT of the cervical skull junction demonstrating the right parapharyngeal space blocked by a hyperdense round mass dependent on the ipsilateral cervical internal
carotid artery with a thrombosed area at its medial and rostral periphery (white arrows).
Figure 2. Cerebral angiography of the right internal and external carotid artery in lateral projection demonstrating an irregular giant pseudoaneurysm (40 x 50 mm) originating from the middle and upper third of the cervical
segment of the right internal carotid artery stealing from the anterior cerebral circulation ipsilateral (black arrows).
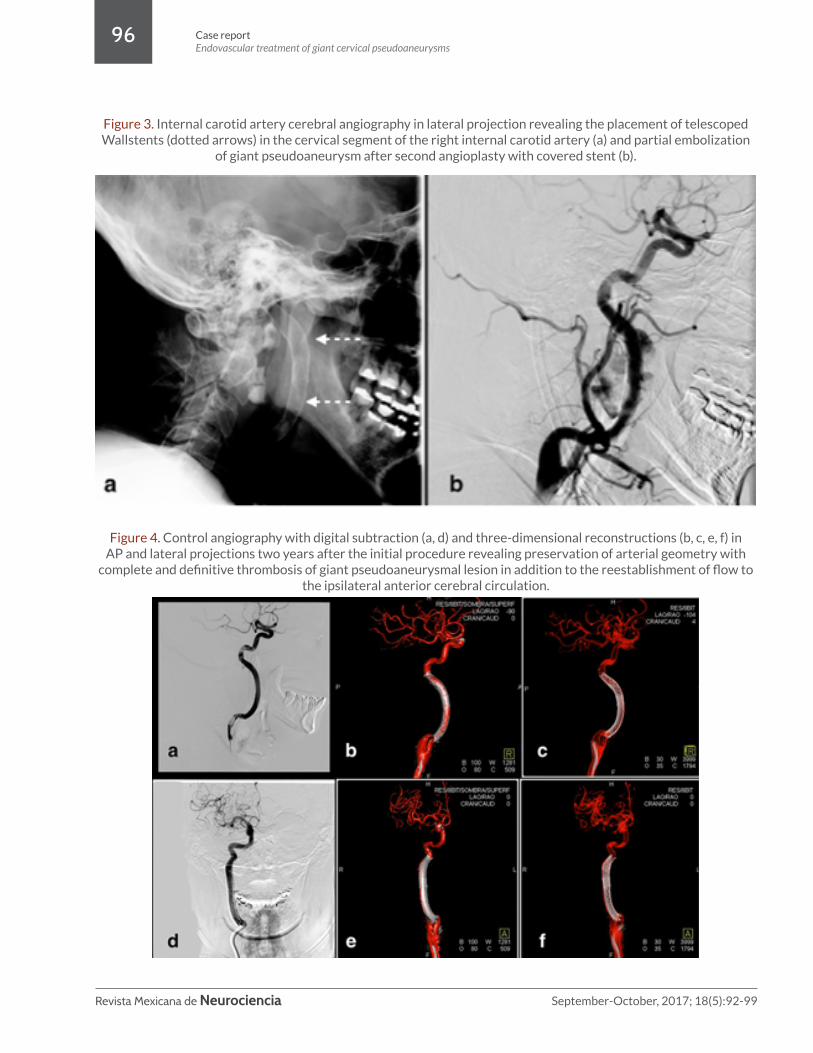
Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
96
Figure 3. Internal carotid artery cerebral angiography in lateral projection revealing the placement of telescoped Wallstents (dotted arrows) in the cervical segment of the right internal carotid artery (a) and partial embolization
of giant pseudoaneurysm after second angioplasty with covered stent (b).
Figure 4. Control angiography with digital subtraction (a, d) and three-dimensional reconstructions (b, c, e, f) in AP and lateral projections two years after the initial procedure revealing preservation of arterial geometry with
complete and definitive thrombosis of giant pseudoaneurysmal lesion in addition to the reestablishment of flow to the ipsilateral anterior cerebral circulation.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
97
Pseudoaneurysms are considered “false aneurysm lesions” because they consist of a single layer of fibrous tissue that envelops a sac of turbulent blood flow surrounded by a hematoma; these lesions differ from true aneurysms, which involve all three layers of the normal arterial vessel.2 The sac of the pseudoaneurysm communicates directly with the arterial lumen. The true lumen of the parent vessel may be ruptured through dissection of the subintimal or subadventitial space.6
Usually, these lesions originate from a disruption of the arterial wall. Commonly, arterial dissections can lead to pseudoaneurysms by tearing the intima with extravasation of blood in the arterial wall. If the hematoma dissects the vessel between the intima and the media, the false lumen may occlude the true light of the parent vessel; if the dissection is between the media and the adventitia, the development of pseudoaneurysms is possible.6
The incidence of carotid pseudoaneurysms is 0.33%.7 The frequency of these lesions is on the rise as result of increased detection by better imaging techniques.
The etiology of the trauma - whether it is contusive or penetrating - is the most frequent origin of these lesions.8,9 Pseudoaneurysms will be found in a third of all cervical trauma injuries.9 Carotid lesions are found in 3% of traumatic arterial lesions.10 Among non-penetrating injuries, we can find lesions due to hyperextension, cervical rotation, direct contusion to neck injury, and intraoral trauma. Chaer et al. described in 2008 that 29% of arterial dissections result in pseudoaneurysms.9
Iatrogenic etiology has an incidence of 7.7%. It’s been said that up to 1% of all diagnostic angiographies and 8% of endovascular therapeutic procedures can end the development of a pseudoaneurysm.2
Infectious etiology of the arterial wall is more frequently found to be due to Gram positive bacteria, currently assigning 22% to Staphylococcus aureus, 17% to Salmonella
Discussion sp., 11% to Streptococcus sp., and 11% to Enterococcus sp. infections.2
Other less frequent causes are vasculitis (transmural inflammation with subsequent rupture), invasion of the arterial wall by neoplasms, drug abuse, and genetic disorders of connective tissue.2
Clinically these lesions can be silent, their clinical expression may be conditioned by secondary local factors secondary to the mass effect in giant lesions (dysphonia, cough, difficulty swallowing, and dysphagia in those with a parapharyngeal location) or epistaxis in lesions contiguous to the sphenoid sinus.3 They can manifest systemically when there are complications derived from the pseudoaneurysm per se, such as rupture and massive hemorrhage, distal ischemia due to thromboembolism, sepsis in infectious cases, and occlusion of the parent vessel. The morbidity of carotid pseudoaneurysms is 80%.7
The first line diagnostic study in cervical lesions is the Doppler ultrasound with sensitivity of 94% and specificity of 97%.2 The “Ying-Yang” sign suggests turbulent flow of blood inside the aneurysmal sac. This mode of treatment can detect the width of the neck of the lesion and the size of the hematoma surrounding the pseudoaneurysmal lesion.2
An angiotomography has a sensitivity of 95% and a specificity of 98.7%. Its main benefit is it differentiates between true aneurysmal lesions and pseudoaneurysms of intracranial location.2
Digital subtraction angiography is the second line image in these lesions. The information it provides is vital for the treatment to be established such as the size of the sac, the diameter of the neck, the affected vascular territory, and the final or distal artery affected.2
In 1999, Biff et al. designed the following scale of carotid lesions:11
I- Intimal lesions without hemodynamic relevance.
II- Dissections and hematomas with potential hemodynamic compromise.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
98
Conflict of interestThe authors state there are no conflicts of interest related to the writing of this article.
FundingThe authors state no funding was received from any person or company to create this article.
Conclusion
The endovascular treatment of giant pseudoaneurysms of the internal carotid artery with cervical stents can be an effective and safe method these days. Reconstruction of the parent vessel lumen may require the use of uncovered telescoping stents to provide the support and structure required to prevent eventual bending of the covered stent.
III- Pseudoaneurysms.
IV- Arterial occlusions.
V – Complete section of vessel.
This scale is related to the prognosis and the appropriate treatment choice. The aggressive management of these lesions aims to prevent fatal hemorrhaging and thromboembolic events.11
Surgery of these lesions has always been characterized as technically very demanding. The different techniques include revascularization with bypass (internal carotid to middle cerebral via superficial temporal), direct repair of the arterial defect, and clipping. Clipping is high risk if the endothelialized fibrous sac is not found, as well as in lesions without a well-defined neck.1,4,10
Total occlusion of the parent vessel is a commonly performed treatment with apparently good results; however, it has been associated with ischemic events in 5 to 22% post-occlusion even while securing anterior communicating artery collateral flow.12 This surgery’s mortality is 1.44%.10
The advantages of endovascular therapy as a minimally invasive method make it a very attractive therapeutic strategy to treat these lesions effectively and safely. It was initially described as coil embolization,13 but
this technique has fallen into disuse because the devices may be subject to intra-aneurysmal migration and their effectiveness in broad-neck lesions is limited.12-14 The use of stents has some advantages. It is a relatively simple and rapid procedure compared to surgery: the procedure, per se, is not in the aneurysmal sac, it preserves permeability in the parental vessel, promotes late thrombosis, and has a reduced mass effect compared with the use of coils.4 The technical success rate is 98.2% with use of stents, and the complications include 9.1% of embolism and 1.8% of arterial dissections.4
The use of covered stents shares many of the advantages of other stents; however, some of the disadvantages are poor navigation due to their rigidity, higher risk of vascular perforations, intimal hyperplasia or subacute thrombosis, and secondary stenosis. The ideal covered stent would be flexible, very elastic, with high adherence to the vascular wall, and self-expanding (because of the potential of collapse under the internal carotid’s high pressure in those expandable by balloon).1,4,6,10,15
Non-covered stents promote late thrombosis which is sometimes incomplete; however, in this specific case, we used the telescoping technique, whose objective is the reconstruction of the artery’s geometry to provide the necessary support to prevent the possible bending of a single covered stent.

Revista Mexicana de Neurociencia September-October, 2017; 18(5):92-99
Case reportEndovascular treatment of giant cervical pseudoaneurysms
99
1. Yi AC, Palmer E, Luh GY, Jacobson JP, Smith DC. Endovascular treatment of carotid and vertebral pseudoaneurysms with covered stents. AJNR Am J Neuroradiol. 2008; 29(5):983-7.
2. Keeling AN, McGrath FP, Lee MJ. Interventional radiology in the diagnosis, management, and follow-up of pseudoaneurysms. Cardiovasc Intervent Radiol. 2009; 32(1):2-18.
3. Gupta V, Niranjan K, Rawat L, Gupta AK. Stent-graft repair of a large cervical internal carotid artery pseudoaneurysm causing dysphagia. Cardiovasc Intervent Radiol. 2009; 32(3):558-62.
4. Alaraj A, Wallace A, Amin-Hanjani S, Charbel FT, Aletich V. Endovascular implantation of covered stents in the extracranial carotid and vertebral arteries: Case series and review of the literature. Surg Neurol Int. 2011;2:67.
5. Lim J, Suh SH, Lee KY, Hong CK, Park SW. Endovascular treatment of iatrogenic intracranial pseudoaneurysm following stent angioplasty. J Neuroimaging. 2012; 22(2):194-6.
6. Scavee V, De Wispelaere JF, Mormont E, Coulier B, Trigaux JP, Schoevaerdts JC. Pseudoaneurysm of the internal carotid artery: treatment with a covered stent. Cardiovasc Intervent Radiol. 2001; 24(4):283-5.
7. Fusonie GE, Edwards JD, Reed AB. Covered stent exclusion of blunt traumatic carotid artery pseudoaneurysm: case report and review of the literature. Ann Vasc Surg. 2004; 18(3):376-9.
8. Zhou B, Zhou T, Arous EJ, Liu W. A giant common carotid artery pseudoaneurysm after penetrating injury. J Vasc Surg. 2012; 55(1):240-1.
9. Chaer RA, Derubertis B, Kent KC, McKinsey JF. Endovascular treatment of traumatic carotid pseudoaneurysm with stenting and coil embolization. Ann Vasc Surg. 2008; 22(4):564-7.
10. Yeh CH, Lin MS, Chiu MC, Chen CH, Pai YL. Endovascular treatment of a huge cervical carotid artery pseudoaneurysm with Wallgraft prosthesis. Ann Vasc Surg. 2011; 25(2):265 e1-3.
11. Biffl WL, Moore EE, Offner PJ, Brega KE, Franciose RJ, Burch JM. Blunt carotid arterial injuries: implications of a new grading scale. J Trauma. 1999; 47(5):845-53.
12. Lv X, Jiang C, Li Y, Lv M, Zhang J, Wu Z. Intracranial pseudoaneurysms, fusiform aneurysms and carotid-cavernous fistulas. Repair with percutaneous implantation of endovascular covered stents. Interv Neuroradiol. 2008; 14(4):435-40.
13. Maras D, Lioupis C, Magoufis G, Tsamopoulos N, Moulakakis K, Andrikopoulos V. Covered stent-graft treatment of traumatic internal carotid artery pseudoaneurysms: a review. Cardiovasc Intervent Radiol. 2006; 29(6):958-68.
14. Li MH, Li YD, Gao BL, Fang C, Luo QY, Cheng YS, et al. A new covered stent designed for intracranial vasculature: application in the management of pseudoaneurysms of the cranial internal carotid artery. AJNR Am J Neuroradiol. 2007; 28(8):1579-85.
15. Riesenman PJ, Mendes RR, Mauro MA, Farber MA. Endovascular exclusion of an external carotid artery pseudoaneurysm using a covered stent. Cardiovasc Intervent Radiol. 2007; 30(5):1025-8.
References

Revista Mexicana de Neurociencia September-October, 2017; 18(5):100-101
Editorial100
MEXICAN JOURNAL OF NEUROSCIENCESEPTEMBER 2017
Dear reader:
This phrase is frequently referenced in multiple events and in reflections. And I think it’s correct, for change is perennial as it is inevitable. Change by itself, however, is meaningless. What is truly transcendental is the change that results in evolution.
The Mexican Journal of Neuroscience has been the official publication of the Mexican Academy of Neurology for 17 years—the first issue was July/August 2000. As every living entity, it has undergone several phases. First, it overcame the difficult stage of its birth, and survived—the vast majority of publications die in the first 2 to 5 years of their founding. During its growth period, the primary objective became to acquire more readers and authors, so we made design changes in order to adapt it to the modern environment and make it more attractive to read. Later, we considered it necessary to change it to a digital format. This increased its diffusion as it was included in the Open Access platform, which earned it the recognition of the CONACyT.
After 17 years, however, it has not yet achieved our most desired goal: to be indexed. This is why we have undertaken a series of modifications in the structure of the journal—transformations that, as mentioned before, seek not only to change it, but to help it evolve. For this reason, a new editorial committee was appointed. It is diverse, with great academic prestige, and representative of the main institutions of Mexican Neurology. In this committee, you will also find international members of the highest level, with wide experience in editorial work. Suffice it to mention Dr. José Obeso (Movement disorders), Dr. José Biller (Frontiers), and Dr. José Merino (BMJ).
Editorial
“Change is the only constant.”– Heraclitus of Ephesus

Revista Mexicana de Neurociencia September-October, 2017; 18(5):100-101
Editorial 101
Having an editorial committee with these characteristics, while indispensable, would not be enough to achieve the evolution we seek, which is to help the journal reach maturity. In this quest, we are endowing it with a copy editor (Mr. Alejandro García), a statistical reviewer (Dr. Héctor Gerardo Hernández Rodríguez), and as you will notice in this issue, a professional translator (Ms. Rebeca Barroso).
The current issue represents a milestone in this process. You will see that each article will now appear in both Spanish and English, and the full text will also be published in OVID in XML format. We hope to achieve a better, wider distribution so it can soon be read and cited by a greater number of readers and authors. The exposure could yield citations in MedLine, and hopefully, in the near future, an indexed journal.
As an aside, I would like to thank each and every person involved in this task. Their work, passion, generosity, and professional and academic abilities drive us in our efforts to fulfill the dream of our Academy, the dream born 17 years ago.
Finally, I would like to emphasize that the Mexican Journal of Neuroscience belongs to the Mexican Academy of Neurology—that is, it belongs to all its members—which is why I invite you to read it, quote it, share it, collaborate in it, and with it. With everybody’s participation, I am convinced that it will be a source of pride, not only for all members of the Academy but for Mexican Neuroscience.
SINCERELY
Dr. Miguel Osorno GuerraPresident of the Mexican Academy of Neurology

Revista Mexicana de Neurociencia
Estimado Académico:
Por medio de la presente, es un gusto saludarle y extenderle la más cordial invitación a colaborar con la publicación de artículos de investigación original; básica, tradicional o aplicada, casos clínicos o artículos de revisión en la Revista Mexicana de Neurociencia, órgano oficial de difusión científica de la Academia Mexicana de Neurología.
Esta Revista ha sido incluida recientemente en el índice de revistas de CONACyT, y estamos trabajando para que pronto esté disponible en las plataformas OVID y SciELO, especialmente en PubMed.
Estamos seguros que su trayectoria académica le permitirá participar e invitar a colaborar a sus distinguidos colegas, que con su participación enriquecerán nuestra revista.
El Comité Editorial está formado por investigadores de diversas instituciones de nuestro país y del extranjero, que cuentan con reconocida calidad académica.
Esperamos que usted y cada integrante de la Academia Mexicana de Neurología se sientan parte y sumamente orgullosos de la Revista Mexicana de Neurociencia.
Reciba un cordial saludo.Atentamente,
Dra. Carolina LeónCo-Editor
Dr. Ildefonso RodríguezEditor
Dr. Antonio ArauzCo-Editor
Revista Mexicana de Neurociencia
San francisco 1384 Torre B 7, Col. Del Valle, Ciudad de México, C.P. 03100Teléfonos: +52 (55) 5559 9833 / +52 (55) 5575 9312
www.neurologia.org.mx www.revmexneuroci.com
Revista Mexicana de
NeurocienciaPublicación oficial de la Academia Mexicana de Neurología A.C.


Revista Mexicana de Neurociencia, 2017; 18(5): 1-101
www.revmexneuroci.com






![VSOSA SCHOOL SOSA SOSA 300,000fT-J / 100 150,000P] 200 ... · —)VSOSA SCHOOL SOSA SOSA 300,000fT-J / 100 150,000P] 200,OOOP3 5 sosa : L : FAX : 03-3364-6324 U R L :](https://static.fdocuments.us/doc/165x107/6112f77e3c5dea35443ffef5/vsosa-school-sosa-sosa-300000ft-j-100-150000p-200-avsosa-school-sosa.jpg)