Review Alcohol and Diabetes - Diabetes Care
9
Review A lcohol and Diabetes JANET MCDONALD Newer concepts regarding the management of diabetes favor a diet that is more liberal in carbohydrate content and more personalized for the patient. Ideally, the end result will be improved glycemic control and fewer complications. Allowing more flexibility in the diet is a way of fostering better patient compli- ance. Alcohol, for example, which is frequently disallowed, can safely be included in the diet of many diabetic patients who desire a drink with meals, provided that certain guidelines are followed. Dietary substitutions can be made with relative ease. Although there are contraindications to its use by certain people, alcohol in moderation does not appear to compromise carbohydrate homeostasis in most indi- viduals and, if early studies are confirmed, could possibly have some beneficial side-effects. More open discussion of alcohol use with patients is needed to give them the know-how to alter their diets and to inform them of the necessary precautions, DIABETES CARE 3. 629-637, SEPTEMBER-OCTOBER 1980. P hysicians in the United States tend to be reluctant about permitting the use of alcoholic beverages in the diets of their diabetic patients. 1 In contrast, many clinicians in Europe consider alcoholic bever- ages, particularly dry wine, an integral part of the diabetic diet. 2 The reason for this difference in attitude may be that in wine-drinking countries of Europe, unlike the United States, wine is accepted as an important constituent of the daily diet. With the burgeoning interest in wine in this country, the subject of alcohol in the diabetic diet needs to be addressed. CURRENT CONCEPTS IN DIABETIC DIET THERAPY The principal manifestation of diabetes mellitus is hypergly- cemia, control of which is the major objective of treatment. The importance of diet in achieving this goal has long been recognized. 3 Although dietary control continues to be an es- sential part of the management of diabetes, the actual com- position of the ideal diet remains a subject of controversy. 4 ' 5 Before 1971, dietary management of diabetes emphasized the restriction of carbohydrate to 40-45% of the total kilocal- ories (kcal), necessitating rather large fat intakes. In recent years, a new approach to diet therapy has evolved in an effort to reduce the risk of atherosclerosis. 6 Liberalization of carbo- hydrate in the diet allows for a reduction in fat intake which, in turn, may result in a lowering of blood lipids. As long as the total caloric intake does not exceed that necessary to at- tain or maintain ideal body weight, the consensus of opinion is that increasing the amount of unrefined complex carbohy- drate in the diet is not detrimental to most diabetic pa- tients. 3 In 1976, the American Diabetes Association and the American Dietetic Association published a revision of the original ADA Exchange Lists in accordance with the new concepts regarding the diabetic diet. 7 A guide for profes- sionals to aid in using the Exchange Lists was also made available. 8 In the chapter on Special Needs, alcohol is briefly discussed. It is hoped that the following more comprehensive discussion will answer some questions that the physician, di- etitian, and ultimately the patient might have. METABOLISM OF ALCOHOL AND ITS EFFECT ON CARBOHYDRATE HOMEOSTASIS Pure alcohol is rapidly absorbed and contains approximately 7 kcal/g, although the calories actually available to the body for energy may be slightly less. 9 Various types of alcoholic beverages are absorbed at different rates depending on their composition. In general, distilled spirits are absorbed most rapidly, followed by wine, and then beer. 10 Absorption is slowed further in the presence of food. Alcohol is metabolized primarily in the liver, and its end products are carbon dioxide and water. Alcohol does not re- quire insulin for its oxidation, but it can affect carbohydrate metabolism in various ways. Effects of alcohol differ accord- ing to the species, dose, whether it is given in the fasted or fed state and by the oral or intravenous route, and whether it is administered acutely or chronically. The subject of alcohol and carbohydrate metabolism has been reviewed recently in some detail by Marks. x The following brief discussion will focus on the known effects of alcohol in human beings, espe- cially those with diabetes. DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 629 Downloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022
Transcript of Review Alcohol and Diabetes - Diabetes Care

Review
Alcohol and DiabetesJANET MCDONALD
Newer concepts regarding the management of diabetes favor a diet that is more liberal in carbohydratecontent and more personalized for the patient. Ideally, the end result will be improved glycemic controland fewer complications. Allowing more flexibility in the diet is a way of fostering better patient compli-ance. Alcohol, for example, which is frequently disallowed, can safely be included in the diet of manydiabetic patients who desire a drink with meals, provided that certain guidelines are followed. Dietarysubstitutions can be made with relative ease. Although there are contraindications to its use by certainpeople, alcohol in moderation does not appear to compromise carbohydrate homeostasis in most indi-viduals and, if early studies are confirmed, could possibly have some beneficial side-effects. More opendiscussion of alcohol use with patients is needed to give them the know-how to alter their diets and toinform them of the necessary precautions, DIABETES CARE 3. 629-637, SEPTEMBER-OCTOBER 1980.
Physicians in the United States tend to be reluctantabout permitting the use of alcoholic beverages inthe diets of their diabetic patients.1 In contrast,many clinicians in Europe consider alcoholic bever-
ages, particularly dry wine, an integral part of the diabeticdiet.2 The reason for this difference in attitude may be thatin wine-drinking countries of Europe, unlike the UnitedStates, wine is accepted as an important constituent of thedaily diet. With the burgeoning interest in wine in thiscountry, the subject of alcohol in the diabetic diet needs tobe addressed.
CURRENT CONCEPTS IN DIABETIC DIET THERAPY
The principal manifestation of diabetes mellitus is hypergly-cemia, control of which is the major objective of treatment.The importance of diet in achieving this goal has long beenrecognized.3 Although dietary control continues to be an es-sential part of the management of diabetes, the actual com-position of the ideal diet remains a subject of controversy.4'5
Before 1971, dietary management of diabetes emphasized therestriction of carbohydrate to 40-45% of the total kilocal-ories (kcal), necessitating rather large fat intakes. In recentyears, a new approach to diet therapy has evolved in an effortto reduce the risk of atherosclerosis.6 Liberalization of carbo-hydrate in the diet allows for a reduction in fat intake which,in turn, may result in a lowering of blood lipids. As long asthe total caloric intake does not exceed that necessary to at-tain or maintain ideal body weight, the consensus of opinionis that increasing the amount of unrefined complex carbohy-drate in the diet is not detrimental to most diabetic pa-tients.3
In 1976, the American Diabetes Association and theAmerican Dietetic Association published a revision of theoriginal ADA Exchange Lists in accordance with the newconcepts regarding the diabetic diet.7 A guide for profes-sionals to aid in using the Exchange Lists was also madeavailable.8 In the chapter on Special Needs, alcohol is brieflydiscussed. It is hoped that the following more comprehensivediscussion will answer some questions that the physician, di-etitian, and ultimately the patient might have.
METABOLISM OF ALCOHOL AND ITS EFFECT ONCARBOHYDRATE HOMEOSTASIS
Pure alcohol is rapidly absorbed and contains approximately7 kcal/g, although the calories actually available to the bodyfor energy may be slightly less.9 Various types of alcoholicbeverages are absorbed at different rates depending on theircomposition. In general, distilled spirits are absorbed mostrapidly, followed by wine, and then beer.10 Absorption isslowed further in the presence of food.
Alcohol is metabolized primarily in the liver, and its endproducts are carbon dioxide and water. Alcohol does not re-quire insulin for its oxidation, but it can affect carbohydratemetabolism in various ways. Effects of alcohol differ accord-ing to the species, dose, whether it is given in the fasted orfed state and by the oral or intravenous route, and whether itis administered acutely or chronically. The subject of alcoholand carbohydrate metabolism has been reviewed recently insome detail by Marks.x The following brief discussion willfocus on the known effects of alcohol in human beings, espe-cially those with diabetes.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 629
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022

ALCOHOL AND DIABETES/JANET McDONALD
Hyperglycemia. In the nonfasting state, blood glucoselevels tend to rise after alcohol administration.11 The eleva-tion is due primarily to glycogenolysis in the liver mediatedat least in part by the adrenal medulla-sympathetic nervoussystem.11 The extent of the increase depends mostly on thedose of ethanol and the magnitude and availability of hepaticglycogen stores.n Alcohol in very large amounts has been re-ported to induce gross glucose intolerance in some people.12
This problem is more commonly associated with alcohol-ism13 and may result from liver damage and/or sympathetico-adrenal activation consequent to alcohol intoxication in ge-netically susceptible individuals.1 The glucose intol-erance often disappears when alcohol is withdrawn from thediet.1-12-
Hypoglycemia. Ingestion of alcohol also can produce hypo-glycemia under several different circumstances. The mostwell-known type of alcohol-induced hypoglycemia occurs inpersons who have fasted for some time and have depleted he-patic glycogen reserves; it is believed to be due to the inhibi-tion of gluconeogenesis by alcohol.14 Individuals with diabe-tes are more vulnerable to this effect of alcohol14 as areadrenocortical-deficient or thyrotoxic subjects,15 normal per-sons regularly consuming a low carbohydrate diet, and chil-dren.16 Obese individuals, however, are unusually resist-ant.15
Alcohol by itself does not stimulate insulin secretion.However, several investigators have reported that whengiven in moderate amounts orally or intravenously to nonal-coholics, alcohol enhances the plasma insulin response to anoral or intravenous glucose load.17"23 Although the mecha-nism is not known, this effect of alcohol has been observedin both normal17"23 and mildly diabetic18'20'21 individuals. Ingeneral, alcohol tends to enhance intravenous glucose toler-ance, but results pertaining to oral glucose tolerance are con-flicting. Oral glucose tolerance has been reported to be un-changed,20 improved,21 and impaired23 by moderate amountsof alcohol. Differences in experimental conditions may ex-plain the discrepancy. In a study designed to more closely ap-proximate the usual mode of alcohol and food intake,McMonagle and Felig21 found a dampened blood glucose risewith alcohol in both normal and mildly diabetic subjects.They concluded that moderate alcohol intake (60 ml of ab-solute alcohol) by individuals with mild diabetes is withoutacute deleterious effects on blood glucose. A similar conclu-sion was reached by Walsh and O'Sullivan24 in acute experi-ments involving 20 diabetic subjects who were given 35 mlof ethanol 2Vi h postprandially. Mean plasma glucose valuesafter alcohol, although lower, were not significantly differentfrom the control period (no drink). Two of the insulin-de-pendent subjects in this study developed severe hypoglyce-mia after alcohol ingestion. However, the authors were un-certain as to whether alcohol was the cause, since plasmaglucose levels were not measured before alcohol consump-tion. Alcohol, however, does appear to augment the glu-cose-lowering action of insulin or other hypoglycemicagents.25'26 Arky et al.25 reported five cases involving insu-lin-treated diabetic individuals who developed extremely se-
vere hypoglycemia after excessive alcohol ingestion; three ofthe patients suffered permanent neurologic damage and theother two died. All these patients were alcoholics. However,studies in normal healthy subjects have shown that a moder-ate quantity of alcohol (equivalent to a "shot" of whiskey)infused in the fasting state can delay recovery from hypogly-cemia produced by intravenously administered insulin, indi-cating that alcohol interferes with counterregulation.25
Schlierf and his associates27 compared the effect of ethanoland dry wine in amounts up to about 800 kcal/day on bloodglucose, ketones, and other parameters of diabetic and non-diabetic subjects fed a high fat (ketogenic) formula diet.There was no consistent effect of either beverage on bloodglucose. Ethanol produced an increase in blood ketones,which appeared to be greater in diabetic than in nondiabeticsubjects. Equivalent doses of the dry wine had a lesser hyper-ketonemic effect. Although it has been documented that al-cohol by itself suppresses ketogenesis,28 hyperketonemia fol-lowing alcohol in combination with a fat-rich diet has beenreported by others.29 The explanation of Schlierf et al.27 forusing a ketogenic diet was to permit evaluation of the effectof added alcoholic beverage ingestion on already elevatedblood ketone levels. The effects of alcohol on glycemic andketone status while on a ketogenic diet, however, may notcorrespond to its effects when on a more conventional dietwith liberal carbohydrate.
Lolli and his co-workers30 found that moderate amounts ofdry wine had no adverse effect on blood sugar levels of 30diabetic patients when consumed either with meals or on anempty stomach and may have contributed to the mainte-nance of reasonably low blood sugar levels. The only un-toward effects were observed in some of the patients whowere treated with tolbutamide (Orinase) and given wine onan empty stomach. These patients experienced mild hotflashes, dizziness, and feelings of warmth (similar to an alco-hol-disulfiram reaction). These symptoms were almost unde-tectable when wine was taken with a mixed meal. Similarreactions have been noted when alcohol in any form is com-bined with sulfonyl compounds.2'26
To investigate the combined and separate effects of alco-hol and glucose on the production of reactive hypoglycemia,O'Keefe and Marks,22 on three separate occasions, gave 10healthy volunteers (5 h after breakfast) the equivalent ofthree gin and tonics containing 50 g of ethyl alcohol and 60g of sucrose, gin and "Slimline" tonic containing 50 g of al-cohol and 0.5.g of sucrose, or tonic alone containing 60 g ofsucrose. Gin and "Slimline" tonic had no significant effecton plasma insulin or blood glucose. The sugar-rich tonic pro-duced a reactive hyperinsulinemia and hypoglycemia, whichwere even more pronounced when gin was added. The hypo-glycemia induced by gin and tonic was severe enough tocause neuroglycopenic symptoms in three subjects. A com-parable hypoglycemic reaction would be expected to occurwith like amounts of other alcoholic beverages and high-car-bohydrate mixers. Data from a similar experiment,23 how-ever, contradict those of O'Keefe and Marks.22 Dornhorstand Ouyang23 found that a glucose and alcohol solution pro-
630 DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022

ALCOHOL AND DIABETES/JANET McDONALD
voked a significantly higher serum glucose level in sixhealthy subjects than either a glucose or alcohol solutionalone. Although both groups of investigators observedhigher insulin levels after alcohol and carbohydrate, the rea-son for the discrepant results regarding blood glucose is notclear.
There are no reports in the literature on the long-term ef-fects of regular alcohol consumption (in moderate amounts)on carbohydrate homeostasis. Nikkila and Taskinen20 re-ported that after 1 wk of daily use of ethanol in amounts pro-viding 25% of the total caloric intake, normal subjects hadan impairment of both intravenous and oral glucose toler-ance with no change in plasma insulin response. They attri-buted the decreased glucose tolerance to insulin resistance ofthe tissues, perhaps secondary to a decline in liver function.Contrary to these results, Carey et al.31 found a slight de-crease in fasting blood glucose levels but no change in glu-cose tolerance curves of 12 normal subjects who consumed20% of their daily caloric requirement as ethanol for 12 days.Although unlikely, it is possible that the slightly greateramount of alcohol employed by Nikkila and Taskinen20
could account for the differences in results. It should bepointed out that the amounts of alcohol used in these studiesare more than one would recommend for regular daily con-sumption.
Although the long-term effect of daily ethanol ingestionon glycemic status of diabetic patients needs to be studiedfurther, on the basis of what is presently known, it seems safeto say that moderate alcohol intake by individuals with milddiabetes does not have acute deleterious effects on carbohy-drate homeostatis in normal mixed-meal situations. Diabeticpatients should be cautioned both against excessive con-sumption of alcohol and against normal food intake immedi-ately before drinking alcoholic beverages (advice that isequally prudent for nondiabetic individuals). A diabetic per-son who becomes hypoglycemic for any reason after alcoholingestion may be thought to be intoxicated and consequentlynot treated appropriately.
HYPERLIPIDEMIC EFFECT OF ALCOHOL
Individuals with diabetes have a two- to threefold in-creased risk of cardiovascular disease and an increasedmortality from coronary heart disease.32 Hyperlipemia,particularly hypertriglyceridemia, is more common in
diabetic than in nondiabetic individuals and is presumed tobe a determinant in the development of atherosclerotic dis-ease.33 Although recent evidence has deemphasized elevatedtriglycerides as an. independent risk factor in the general pop-ulation,34 there is no consensus of opinion on this matter.35
Hypertriglyceridemia, however, may play a greater role inthe etiology of cardiovascular disease in diabetic than innondiabetic individuals.33>36~38
The ability of alcohol to influence lipid metabolism andlipid transport is well documented.39 Unfortunately, most ofthe published studies deal with healthy individuals or ani-mals given large quantities of alcohol or with chronic alco-
holics. There are only limited data on the administration ofmoderate doses of alcohol to normal individuals or to dia-betic patients. Previous investigations have shown that somesubjects respond to alcohol ingestion by an elevation inplasma triglycerides while others do not.
In a study of both diabetic and nondiabetic subjects bySchlierf et al.,27 neither ethanol nor dry wine had any con-sistent effect on free fatty acids or triglycerides. Cholesteroland phospholipid levels also remained unchanged when thesource of fat in the diet was of the unsaturated type, but be-came markedly elevated in some subjects (all of whom werediabetic) during intake of saturated fat.27 Whether the re-sults would have been the same had a more conventional(rather than ketogenic) diet been employed is not known. Ithas been shown, however, that the simultaneous ingestion ofethanol and fat produces a significantly greater lipemic re-sponse than the sum of the individual changes due to ethanoland fat given alone; the magnitude of the response correlateswith the initial fasting triglyceride concentration.40 In agree-ment with this finding, Ginsberg and his associates41 ob-served a significant increase in fasting plasma triglyceridesafter moderate doses (87 g/day) of ethanol for 7 days in hy-pertriglyceridemic persons but not in normal subjects. In fourhypertriglyceridemic subjects who were studied an additional4 days, fasting triglyceride levels did not return to control-period levels for at least 36 h after cessation of alcohol.Plasma total cholesterol levels, on the other hand, increasedmodestly but significantly in the normal subjects but wereunchanged in the hypertriglyceridemic subjects, althoughcholestrol fractionation showed a consistent reciprocalchange in low density and very low density lipoprotein cho-lesterol levels in the latter group (fractionation, unfortu-nately, was not done in the normal group). There were nosignificant changes in fasting or postprandial plasma glucoseand insulin or in the fasting level of free fatty acids with alco-hol ingestion. This study and others42'43 show that the effectof alcohol in inducing hypertriglyceridemia is independent ofany alcohol effect on glucose tolerance. However, morestudies of diabetic subjects in this regard are sorely needed.44
In contrast to the findings of Ginsberg et al. ,41 Friedmanand associates45 reported no significant effect of acute moder-ate alcohol (60 g) ingestion on serum lipid levels in eithernormo- or hyperlipemic subjects. Differences in subject pop-ulation and experimental design may account for the discrep-ancy in results of these two groups of investigators. Carey etal.31 also found no significant changes in serum cholesterol,triglyceride, or phospholipid levels after moderate (20% oftotal kcal) alcohol intake for 12 days by normal subjects. Thediet was not controlled in this experiment, however, and nospecific data regarding lipid parameters were included in thepublished report.
In a longer-term study of eight apparently healthy volun-teers, Berg and Johansson46 gave ethanol daily (as light beer)in amounts corresponding to about 16% of the total caloricintake for 5 wk. The alcohol period was preceded and fol-lowed by 2-wk control periods with no alcohol. Blood sam-pling was done in the morning after an overnight fast.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 631
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022

ALCOHOL AND DIABETES/JANET McDONALD
Plasma triglycerides increased in every subject during thefirst week of the alcohol period but subsequently showed noconsistent trend. One of the subjects, however, had amarked progressive increase in plasma triglycerides until 15days after alcohol was begun. This was followed by a declinein plasma triglycerides, although they did not revert to theinitial control level even after 2 wk of an alcohol-free diet.This subject also had abnormally high cholesterol and low-density-lipoprotein (LDL) levels during the first control pe-riod. There were no consistent changes among subjects inplasma total cholesterol or LDL levels, but high-density-lipo-protein (HDL) levels showed a slight but significant increaseduring the ethanol period and returned toward control valueswhen alcohol was withdrawn.
Unfortunately, few of the studies cited above were per-formed in diabetic subjects. Moreover, the results of variousinvestigations were not always consistent, probably becauseof differences in subject population and/or in experimentaldesign. Whether information gathered from short-term alco-hol studies can be generalized to long-term moderate alcoholconsumption is unknown. It is apparent, however, that thereis more than one effect of alcohol on triglyceride metabo-lism, as recently reviewed by Janus and Lewis.47 Briefly, ali-mentary lipemia tends to be greater if alcohol is includedwith a meal; alcohol may cause a slight transient rise inplasma triglycerides in fasting individuals; in some patientswith hypertriglyceridemia, even moderate doses of alcoholcan cause further elevation of lipid levels, which may persistfor some time after cessation of alcohol; in other hypertri-glyceridemic persons who chronically overindulge in alco-hol, triglyceride levels may become normal when alcohol iswithdrawn. In summary, alcohol ingestion raises triglyceridelevels in susceptible individuals and should be strongly dis-couraged for persons with preexisting hypertriglyceridemia,whether they are diabetic or not.
ALCOHOL AND CORONARY HEART DISEASE
The literature on the relationship of specific alco-holic beverages and cardiovascular disease issparse. Experiments in animals indicate that winemay exert a hypocholesterolemic effect.48'49 The
polyphenols in wine have been noted to have a cholesterol-lowering ability.50 Henze et al.51 reported that use of wine inamounts less than 0.5 L/day had little correlation with serumcholesterol and other cardiovascular risk factors; greateramounts, however, showed a positive correlation with serumcholesterol. There is also some evidence that coronary dis-ease is lower in cultures where the diet regularly includes
wine.52-54
Several reports in the past few years indicate a negativeassociation between moderate consumption of alcohol ingeneral and coronary heart disease.55"62 Because a good criti-cal review of the literature on this topic is included in therecent article by LaPorte et al.,62 no attempt at a thoroughdiscussion will be made here. Most of the published reportsto date have been based on either retrospective or prospec-
tive epidemiologic research. As LaPorte et al.62 point out,few studies, if any, are beyond criticism for possible biases.Alcohol consumption, for example, can be associated withother known risk factors (e.g., smoking56) that contribute tothe development of coronary artery disease. Many of the in-vestigations have been controlled for certain confoundingrisk factors to the extent possible, but some have not. De-spite the criticisms of individual studies, which are diverse innature, there tends to be a common finding: moderate drink-ing (the equivalent of about 2 oz of pure alcohol per day onthe average) seems to be associated with a lower rate of heartdisease than either heavy drinking or nondrinking.
In the study of Klatsky et al.,56 a convincing protective ef-fect of alcohol on coronary heart disease was observed onlyamong nonsmokers. Other investigators have found no asso-ciation between alcohol and heart disease.63"65 These studiesare difficult to evaluate, however, because two of them63'64
did not control for usual risk factors, and the third, reportedin a brief abstract,65 contains too little information.
A possible explanation for the negative relationshipbetween alcohol and coronary heart disease may be thatmoderate alcohol ingestion raises HDL-cholesterol le-vels.46'60'61'66"67 In the Cooperative Lipoprotein PhenotypingStudy,66 for example, alcohol intake was moderately asso-ciated with increases of plasma triglycerides, moderately tostrongly correlated with decreases of LDL-cholesterol, andstrongly correlated with increases of HDL-cholesterol. HDL-cholesterol is believed to confer protection against cardiovas-cular disease,68 although the nature of this relationship is notwell understood. For example, there are subfractions ofHDL, not all of which are thought to be protective.69
Human studies in which diet and other risk factors are con-trolled need to be performed to test the effect of various typesof alcoholic beverages on subfractions of HDL-cholesterol.
To put the above discussion into perspective, it should bepointed out that none of the published reports on alcoholand coronary artery disease or alcohol and HDL-cholesterolhave focused on persons with diabetes. It cannot be assumedthat the apparent protective effect of alcohol would be thesame for diabetic individuals as for the population-at-large. Itis possible, for example, that alcohol-induced rises in HDLinvolve different subfractions in diabetic than in nondiabeticsubjects. More research clearly needs to be done. Consid-ering what is presently known, however, there certainly ap-pears to be no good reason to restrict moderate alcohol con-sumption by either diabetic or nondiabetic individuals toprevent coronary disease unless there are other complicatingfactors, e.g., a preexisting lipid disorder.
NUTRIENT COMPOSITION OF ALCOHOLIC BEVERAGES
Beer and wine contain small amounts of B vitamins as well ascertain required minerals such as calcium, magnesium, andiron. Distilled spirits are devoid of any essential nutrients.Except for calories, consumption of commercially availablealcoholic beverages in small to moderate amounts contrib-utes little to normal daily nutrient requirements.
632 DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022
ALCOHOL AND DIABETES/JANET McDONALD
Of interest is the fact that most alcoholic beverages arelow in sodium (Na). Wine and beer also have a relativelyhigh potassium (K) content, creating a favorable K:Naratio. These beverages, therefore, can generally be recom-mended in moderation to many patients for whom a low so-dium diet and/or diuretics have been prescribed. It is advis-able, however, that individuals on sodium-restricted dietscheck the sodium content of any wines they plan to drink.This information can be obtained from the respective win-eries. Some wines are treated with ion-exchange resins (apractice that is on the decline in this country) and may haveunacceptably high sodium levels.
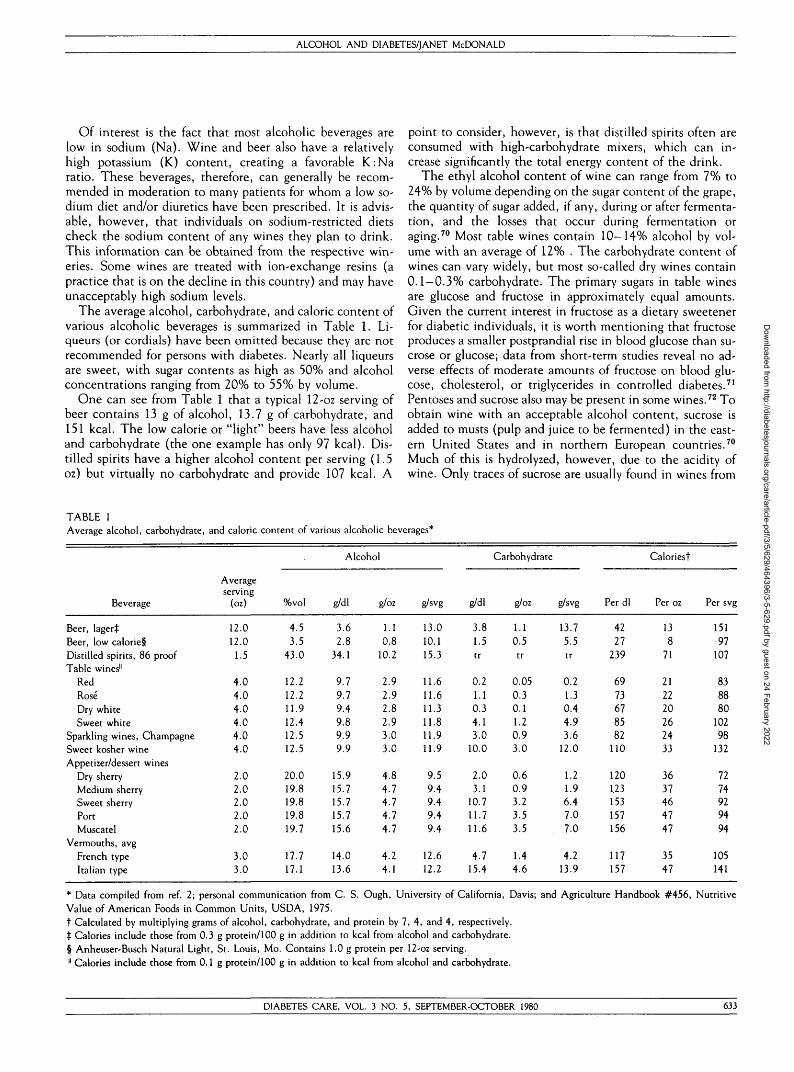
The average alcohol, carbohydrate, and caloric content ofvarious alcoholic beverages is summarized in Table 1. Li-queurs (or cordials) have been omitted because they are notrecommended for persons with diabetes. Nearly all liqueursare sweet, with sugar contents as high as 50% and alcoholconcentrations ranging from 20% to 55% by volume.
One can see from Table 1 that a typical 12-oz serving ofbeer contains 13 g of alcohol, 13.7 g of carbohydrate, and151 kcal. The low calorie or "light" beers have less alcoholand carbohydrate (the one example has only 97 kcal). Dis-tilled spirits have a higher alcohol content per serving (1.5oz) but virtually no carbohydrate and provide 107 kcal. A
point to consider, however, is that distilled spirits often areconsumed with high-carbohydrate mixers, which can in-crease significantly the total energy content of the drink.
The ethyl alcohol content of wine can range from 7% to24% by volume depending on the sugar content of the grape,the quantity of sugar added, if any, during or after fermenta-tion, and the losses that occur during fermentation oraging.70 Most table wines contain 10-14% alcohol by vol-ume with an average of 12% . The carbohydrate content ofwines can vary widely, but most so-called dry wines contain0.1-0.3% carbohydrate. The primary sugars in table winesare glucose and fructose in approximately equal amounts.Given the current interest in fructose as a dietary sweetenerfor diabetic individuals, it is worth mentioning that fructoseproduces a smaller postprandial rise in blood glucose than su-crose or glucose; data from short-term studies reveal no ad-verse effects of moderate amounts of fructose on blood glu-cose, cholesterol, or triglycerides in controlled diabetes.71
Pentoses and sucrose also may be present in some wines.72 Toobtain wine with an acceptable alcohol content, sucrose isadded to musts (pulp and juice to be fermented) in the east-ern United States and in northern European countries.70
Much of this is hydrolyzed, however, due to the acidity ofwine. Only traces of sucrose are usually found in wines from
TABLE 1Average alcohol, carbohydrate, and caloric content of various alcoholic beverages*
Beverage
Beer, lagerlBeer, low calorie§Distilled spirits, 86 proofTable wines"
RedRoseDry whiteSweet white
Sparkling wines, ChampagneSweet kosher wineAppetizer/dessert wines
Dry sherryMedium sherrySweet sherryPortMuscatel
Vermouths, avgFrench typeItalian type
Averageserving
(oz)
12.012.0
1.5
4.04.04.04.04.04.0
2.02.02.02.02.0
3.03.0
%vol
4.53.5
43.0
12.212.211.912.412.512.5
20.019.819.819.819.7
17.717.1
Alcohol
g/dl
3.62.8
34.1
9.79.79.49.89.99.9
15.915.715.715.715.6
14.013.6
g/oz
1.10.8
10.2
2.92.92.82.93.03.0
4.84.74.74.74.7
4.24.1
g/svg
13.010.115.3
11.611.611.311.811.911.9
9.59.49.49.49.4
12.612.2
g/dl
3.81.5tr
0.21.10.34.13.0
10.0
2.03.1
10.711.711.6
4.715.4
Carbohydrate
g/oz
1.10.5tr
0.050.30.11.20.93.0
0.60.93.23.53.5
1.44.6
g/svg
13.75.5tr
0.21.30.44.93.6
12.0
1.21.96.47.07.0
4.213.9
Perdl
4227
239
6973678582
110
120123153157156
117157
Caloriest
Per oz
138
71
212220262433
3637464747
3547
Per svg
15197
107
838880
10298
132
7274929494
105141
* Data compiled from ref. 2; personal communication from C. S. Ough, University of California, Davis; and Agriculture Handbook #456, NutritiveValue of American Foods in Common Units, USDA, 1975.t Calculated by multiplying grams of alcohol, carbohydrate, and protein by 7, 4, and 4, respectively.t Calories include those from 0.3 g protein/100 g in addition to kcal from alcohol and carbohydrate.§ Anheuser-Busch Natural Light, St. Louis, Mo. Contains 1.0 g protein per 12-oz serving." Calories include those from 0.1 g protein/100 g in addition to kcal from alcohol and carbohydrate.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 633
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022

ALCOHOL AND DIABETES/JANET McDONALD
Vitis vinifera varieties of grapes, of which most Californiawines are made.
Returning to Table 1, it can be seen that a typical servingof dry table wine is 4 oz, has slightly less alcohol than beer,considerably less carbohydrate (usually less than 1 g), andcontains 85 kcal. Sweet white wines have a higher sugar con-tent, and sweet kosher wines can approach 15% or more ofcarbohydrate. It should be mentioned that dry kosher winesare available now in this country and are similar in contentto the nonkosher dry wines. Dry sherries are quite low in car-bohydrate (less than 2 g) whereas sweet sherries, port, andmuscatel contain 6 - 7 g of carbohydrate per 2 oz serving. Afinal point of interest is the marked difference in carbohy-drate between French and Italian vermouth, 4-2 versus13.9 g per 3-oz serving, respectively.
USE OF ALCOHOL IN THE DIABETIC DIET
Once it has been determined that alcohol is permis-sible in the diet of a particular patient, the pa-tient then needs to know how much and whatkinds of alcoholic beverages are acceptable. It
has been suggested that alcohol contribute not more than6% of the total calories per day.73 For a 70-kg man on a nor-mal-calorie diet, this would amount to approximately 160kcal/day or two 4-oz glasses of dry wine. The alcohol allow-ance should be stated in fluid ounces of a particular beverage.
Types of beverages to include. Many alcoholic beverages,such as beer, ale, and certain wines, contain appreciable car-bohydrate, which must be considered in diet calculations.Even though the carbohydrate content of diabetic diets hasbeen liberalized, simple sugars should still be limited. There-fore, sweet or dessert wines and liqueurs are not recom-mended for routine use. Distilled spirits, such as whiskey,gin, vodka, and rum, contain no carbohydrate and are per-fectly acceptable. Drink mixers, if used, should be preferablylow in carbohydrate or carbohydrate-free.
In general, dry table wines are well suited for the diabeticdiet because of their low carbohydrate content. Some winesin this category are listed in Table 2. The carbohydrate con-tribution of these wines can, in fact, be ignored in mostcases. A conservative rule of thumb would be to disregard
TABLE 2Some wines with low carbohydrate content*
Red White Other
BurgundyCabernet SauvignonClaretGamay BeaujolaisMerlotPetite SirahPinot NoirZinfandel
ChablisChardonnayDry Chenin BlancFrench ColombardDry GewurztraminerDry RieslingDry SauterneDry Sauvignon BlancWhite Burgundy
Dry RoseDry ChampagneDry Sherry
* Low carbohydrate considered to be less than 2% reducing sugars.
the residual sugar in wine if it amounts to 2% or less butmake necessary caloric adjustments for amounts above that.
Calculating alcoholic beverages into the diet. Alcohol is bestsubstituted for fat exchanges (preferably saturated fat) be-cause it is metabolized to 2-carbon fragments and handled bythe body as fat.8 However, to achieve greater flexibility inthe diet, there is no reason why alcohol cannot be substi-tuted for carbohydrate or protein calories if this is more con-venient for a given individual and is consistent with his/hertherapeutic goals.
The following formula can be used to determine the num-ber of kcal from alcohol:74
0.8 X proof X ounces = kcal
The number 0.8 is a constant derived from several calcula-tions. Proof is twice the percentage of alcohol by volume.Therefore, when the alcohol content is expressed as a per-centage, such as in wines and beers, one can double the per-centage and apply the same formula.
Example: One 4-oz glass of dry table wine con-taining 12% alcohol will provide:
0.8 x 24 x 4 = 77 kcal
Any carbohydrate kcal in the alcoholic beverage should beadded to those from alcohol to obtain the approximate num-ber of total kcal; the number is approximate because beer andwine contain small amounts of protein. If mixers containingsignificant kcal are used, e.g., orange juice or cream, thensubstitutions are best made from the appropriate exchangelist, e.g., fruit or fat.
Sources of information about alcoholic beverages. Nutritionallabeling requirements do not apply to alcoholic beverages.Most wine labels bear the alcohol content. A few wineriesvoluntarily supply the residual sugar content as well. Labelsfor distilled spirits indicate the proof, 50% of which is thealcohol content. In general, beer labels do not reveal eitheralcohol or carbohydrate content, but these are fairly standardwithin a narrow range among various brands of beer. Labelsfor low-calorie or "light" beers indicate the caloric content,and some brands include other nutritional information.
As a general guide, one could use the data in Table 1 tomake estimates of the alcohol, carbohydrate, and caloriccontent of various beverages. For wine, it is desirable to havemore specific information, particularly if wine is to be in-cluded in the diet on a regular basis. While table wines aregenerally thought of as dry, there can be considerable varia-tion in the same varietal from different wineries. Further-more, because of the complexity of wine, tasting is not al-ways a valid indicator of sugar content. Wines with littlegrape sugar which also are deficient in fruit acid can tastesweeter than wines that have twice as much sugar but suffi-cient acid to balance it.75 The ability to perceive sweetnessalso can vary between individuals.
There are several ways to obtain information about thesugar content of wines. First, one should find a knowledge-able wine merchant who can give general information about
634 DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022

ALCOHOL AND DIABETES/JANET McDONALD
the dryness or sweetness of specific wines. Second, one canwrite to the quality control laboratories of the wineries to in-quire about the residual or reducing sugar content of certainwines. Finally, one can use the reducing sugar tablets (e.g.,Clinitest) to determine the sugar concentration of the wine.This method, however, necessitates buying the wine andopening it first. Although Clinitest tablets are intended totest for reducing sugars in the urine of diabetic individuals,they have been found to be quite reliable for determiningglucose and fructose in wine as well.76 One merely needs tofollow the same instructions as for urine and read the sugarpercentage on the accompanying color chart. One shortcom-ing of this procedure, however, is that highly colored redwines can mask the indicator color changes.77 The tabletdoes not react with sucrose because sucrose is not a reducingsugar, but as mentioned previously, few wines contain su-crose. [It should be emphasized that test methods that mea-sure only glucose (glucose oxidase-catalase system) are notsatisfactory for wine because wine also contains fructose andsmall quantities of other reducing sugars.]
Use of alcoholic beverages in cooking. Alcohol evaporatesat 172.4°F, a relatively low temperature that is below thesimmering stage. Therefore, when alcoholic beverages areused in cooking either over direct heat or in the oven, thealcohol vaporizes, leaving only the flavor of the beverageto enhance the food. The loss of alcohol results in a sig-nificant reduction of calories. If the beverage contains sugars,the carbohydrate calories will be retained unless the cookingperiod is sufficiently long for caramelization to take place(more than 1 h in a 300°F oven). In this case, the car-amelized sugars will not be utilized by the body. Usually,the quantity of alcoholic beverage used in cooking doesnot exceed one or two tablespoons per serving. Hence,this is an excellent means of flavoring foods and, in mostinstances, does not have to be calculated into the diet whenused in this manner.
Precautions and contraindications. Diabetic individualsshould include alcohol in their diet only with the knowledgeand consent of their physician and only when the diabetes iswell controlled. Alcoholic beverages are devoid of any signif-icant nutritional value except for calories and, therefore,should not displace foods that provide essential nutrients.This is particularly important in the case of the obese personwith diabetes who is on a low-calorie diet.
In the diabetic patient, as discussed earlier, alcohol maybe more likely to precipitate a hypoglycemic reaction, whichmay not be recognized because the symptoms are similar tointoxication. Necessary treatment may therefore be delayed.For this reason, it is important that alcohol be consumedwith food or at least taken shortly before or after a meal.
A number of situations warrant the avoidance of alcohol.Alcoholic beverages are contraindicated when certain con-comitant conditions exist, e.g., hypertriglyceridemia (whichis more prevalent in diabetes), gastritis, pancreatitis, andcertain types of renal and cardiac disease. Alcohol, further-more, may react synergistically or antagonistically with somemedications. Certain patients taking sulfonyl derivatives (in-
cluding oral hypoglycemic sulfonylureas), for example, mayexperience the distressing disulfiram-like reaction describedearlier when they consume alcohol. Alcohol also interactswith barbiturates, tranquilizers, and a number of otheragents.78 When such drugs are prescribed, alcoholic bever-ages must be used with extreme caution, if at all. Finally, al-cohol should never be permitted for patients who have aproven or suspected tendency to become dependent on it.These contraindications, incidentally, apply to all drinkers,not just those with diabetes.
CONCLUSION
The problem of noncompliance by patients in following theirdiabetic diet is a major one.79 There are many reasons forthis, one of which is the failure to adapt the diet to fit thespecific needs, life-style, and personal preferences of the pa-tient. Health professionals are realizing that a majority ofpeople with diabetes can manage well without strict adher-ence to complex dietary rules.3 Greater flexibility and indi-vidualization of the nutritional care plan will improve pa-tient cooperation and reduce needless anxiety about thepossible deleterious effects of occasional dietary indiscre-tions.
A basic principle of diet therapy is education, and dietaryinstruction for the diabetic person should include a discus-sion of alcohol. It is better that a patient have a clear under-standing of what is permitted than to be left wondering andfeeling guilty every time he/she takes a drink. One of themajor contributions of a beverage such as wine, for example,is that it adds interest and palatability to a diet that other-wise can be rather monotonous and dull. Furthermore,allowing alcohol in the diet of a diabetic patient who hascustomarily enjoyed a drink with meals has a psychologicalbenefit as well in that the eating pattern is not completelydisrupted. Thus, a common-sense approach that stressesmoderation in drinking should please the patient and hope-fully engender better dietary compliance.
Presented in part at the 62nd Annual Meeting of the AmericanDietetic Association, Las Vegas, Nevada, October 22-26, 1979.
Address reprint requests to Janet McDonald, U.S. PublicHealth Service Hospital, 15th Avenue and Lake Street, San Fran-cisco, California 94118.
REFERENCES1 Marks, V.: Alcohol and carbohydrate metabolism. Clin. Endo-
crinol. Metab. 7: 333-49, 1978.2 Leake, C. D., and Silverman, M.: Alcoholic Beverages in Clin-
ical Medicine. Chicago, Year Book Medical Publishers, Inc., 1966,p. 81.
3 Wood, F. C , and Bierman, E. L.: New concepts in diabetic di-etetics. Nutr. Today 7: 4-12, 1972.
4 Leading Article: Diet and the diabetic. Br. Med. ) . 2: 780,1976.
5 Dorchy, H., Loeb, H., and Ernould, C : Diet and the diabetic(letter). Br. Med. J. 2: 1447, 1976.
6 Bierman, E. L., Albrink, M. J., Arky, R. A., et al.: Special
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 635
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022
ALCOHOL AND DIABETES/JANET McDONALD
Reports: Principles of nutrition and dietary recommmendations forpatients with diabetes mellitus: 1971. Diabetes 20: 633-34, 1971.
7 American Diabetes Association and American Dietetic Asso-ciation: Exchange Lists for Meal Planning, 1976.
8 American Diabetes Association and American Dietetic Asso-ciation: A Guide for Professionals: The Effective Application of"Exchange Lists for Meal Planning," 1977.
9 McDonald, J. B.: Not by alcohol alone. Nutr. Today 14: 14-19, 1979.
10 Newman, H. W., and Abramson, M.: Absorption of variousalcoholic beverages. Science 96: 43-44, 1942.
11 Wallgren, H., and Barry, H.: Actions of Alcohol, Vol. 1. Am-sterdam, Elsevier Publishing Co., 1970, pp. 110-11.
12 Phillips, G. B., and Safrit, H. F.: Alcoholic diabetes. Induc-tion of glucose intolerance with alcohol. JAMA 217: 1513-19,1971.
13 Lieber, C. S.: Metabolic effects produced by alcohol in theliver and other tissues. Adv. Intern. Med. 14: 151-99, 1968.
14 Freinkel, N., Arky, R. A., Singer, D. L., et al.: Alcohol hypo-glycemia. IV. Current concepts of its pathogenesis. Diabetes 14:350-61, 1965.
15 Arky, R. A., and Freinkel, N.: Alcohol hypoglycemia. V. Al-cohol infusion to test gluconeogenesis in starvation, with specialreference to obesity. N. Engl. J. Med. 274: 426-33, 1966.
16 McLaughlan, J. M., Noel, F. J., and Moodie, C. A.: Hypogly-cemia in humans induced by alcohol and a low carbohydrate diet.Nutr. Rep. Int. 5: 331-36, 1973.
17 Metz, R., Berger, S., and Mako, M.: Potentiation of theplasma insulin response to glucose by prior administration of alco-hol. Diabetes 18: 517-22, 1969.
18 Friedenberg, R., Metz, R., Mako, M., and Surmaczynska, B.:Differential plasma insulin response to glucose and glucagon stimu-lation following ethanol priming. Diabetes 20: 397-403, 1971.
19 Kuhl, C., and Andersen, M. D.: Glucose- and tolbutamide-mediated insulin response after preinfusion with ethanol. Diabetes23: 821-26, 1974.
20 Nikkila, E. A., and Taskinen, M.-R.: Ethanol-induced altera-tions of glucose tolerance, postglucose hypoglycemia, and insulinsecretion in normal, obese, and diabetic subjects. Diabetes 25: 933—43, 1975.
21 McMonagle, J., and Felig, P.: Effects of ethanol ingestion onglucose tolerance and insulin secretion in normal and diabetic sub-jects. Metabolism 24: 625-32, 1975.
22 O'Keefe, S. J. D., and Marks, V.: Lunchtime gin and tonic acause of reactive hypoglycemia. Lancet J: 1286-88, 1977.
23 Dornhorst, A., and Ouyang, A.: Effect of alcohol on glucosetolerance. Lancet 2: 957-59, 1971.
24 Walsh , C . H . , and O'Sul l ivan, D. J.: Effect of moderate alco-hol intake on control of diabetes. Diabetes 2 3 : 4 4 0 - 4 2 , 1974-
25 Arky, R. A . , Veverbrants , E., and Abramson , E. A . : Irrevers-ible hypoglycemia: a complicat ion of alcohol and insulin. J A M A206: 575-78, 1968.
26 Seltzer, H . S.: Drug-induced hypoglycemia: a review based on473 cases. Diabetes 2 1 : 9 5 5 - 6 6 , 1972.
27 Schlierf, G . , G u n n i n g , B. , Uzawa, H . , and Kinsell, L. W . :T h e effects of calorically equivalent amounts of e thanol and drywine on plasma lipids, ketones, and blood sugar in diabetic andnondiabetic subjects. Am. J. Clin. Nutr. 15: 85-89, 1964.
28 Arky, R. A . , and Freinkel, N . : Alcohol hypoglycemia. Effectsof ethanol on plasma: III. Glucose, ketones, and free fatty acids in"juvenile" diabetics: a model for "non-ketotic diabetic acidosis"?Arch. Intern. Med. 114: 501 -507 , 1964.
29 Lefevre, A . , Adler, H . , and Lieber, C . S.: Effect of ethanol onketone metabolism. J. Clin. Invest. 49: 1775-82 , 1970.
30 Lolli, G. , Balboni, C , Ballatore, C , et al.: Wine in the dietsof diabetic patients. Q. J. Stud. Alcohol 24: 4 1 2 - 1 6 , 1963.
31 Carey, M. A. , Jones, J. D., and Gastineau, C. F.: Effect ofmoderate alcohol intake on blood chemistry values. JAMA 216:1766-69 , 1971.
32 Kannel, W. B., and McGee, D. L.: Diabetes and cardiovascu-lar disease. J A M A 241: 2035-38 , 1979.
33 Santen, R. J., Willis, P. W. , and Fajans, S. S.: Atheroscle-rosis in diabetes mellitus. Correlations with serum lipid levels, adi-posity, and serum insulin level. Arch. Intern. Med. 130: 8 3 3 - 4 2 ,1972.
34 Kannel, W. B.: Status of coronary heart disease risk factors. J.Nutr. Educ. 10: 1 0 - 1 3 , 1978.
35 Tzagournis, M.: Triglycerides in clinical medicine. A review.Am. J. Clin. Nutr. 31: 1437-52 , 1978.
36 Reinheimer, W. , Bliffen, G. , McCoy, J., et al.: Weight gain,serum lipids and vascular disease in diabetics. Am. J. Clin. Nutr.20: 9 8 6 - 9 6 , 1967.
37 Tzagournis, M., Chiles, R., Ryan, J. M., andSkil lman, T. G.:Interrelationships of hyperinsulinism and hypertriglyceridemia inyoung patients with coronary heart disease. Circulation 38: 1156-63, 1968.
38 Garcia, M. J., McNamara, P. M., Gordon, T . , and Kannel,W. B.: Morbidity and mortality in diabetics in the Framinghampopulation. Sixteen-year follow-up study. Diabetes 23: 1 0 5 - 1 1 ,1974.
39 Jones, D. P. , Perman, E. S., and Lieber, C. S.: Free fatty acidturnover and triglyceride metabolism after ethanol ingestion inman. J. Lab. Clin. Med. 66: 8 0 4 - 1 3 , 1965.
40 Wilson, D. E.( Schreibman, P. H . , Brewster, A . C , andArky, R. A. : T h e enhancement of alimentary lipemia by ethanol inman. J. Lab. Cl in . Med. 75: 2 6 4 - 7 4 , 1970.
41 Ginsberg, H . , Olefsky, J., Farquhar, J. W . , and Reaven, G.M.: Moderate e thanol ingestion and plasma triglyceride levels. Astudy in normal and hypertriglyceridemic persons. A n n . Intern.Med. 80: 1 4 3 - 4 9 , 1974.
42 Ostrander , L. D . , Lamphiear, D. E., Block, W . D . , et al.: Re-lationship of serum lipid concent ra t ions to alcohol consumption.Arch. Intern. Med. 134: 451-56, 1974.
43 Lifton, L., and Scheig, R.: E thano l - induced hypertriglyceride-mia. Prevalence and cont r ibu t ing factors. A m . J. C l in . Nut r . 31:614-18, 1978.
44 Albr ink , M. J.: Dietary and drug t r e a t m e n t of hyperl ipidemiain diabetes . Diabetes 23: 91 .3 -18 , 1974.
45 Fr iedman, M . , R o s e n m a n n , R. H . , and Byers, S. O . : Effect ofmodera te ingest ion of a lcohol upon serum triglyceride responses ofn o r m o - and hyper l ipemic subjects. Proc . Soc . Exp. Biol. Med. 120:696-98, 1965.
46 Berg, B . , and Johansson, B. G . : Effects on parameters of liverfunction, plasma lipid concentra t ions and lipoprotein parameters.In Prolonged Adminis t ra t ion of Ethanol to Young, Heal thy Volun-teers: Effects o n Biochemical , Morphological and Neurophysiologi-cal Parameters. Belfrage, B . , et al . , Eds. Ac ta Med. Scand. Suppl.552, 1973, pp. 7-18.
47 Janus , E. D . , and Lewis, B. : A lcoho l and abnormal i t ies of lipidmetabolism. Clin. Endocrinol. Metab. 7: 321-32, 1978.
48 Morgan , A . F. , Brinner , L. , Plaa, C . B . , and S tone , M. M . :Uti l izat ion of calories from alcohol and wines and their effects oncholesterol metabolism. A m . J. Physiol. 189: 2 9 0 - 9 6 , 1957.
49 G o t o , Y., Kikuchi , K.( Abe , K., et al . : T h e effect of e thanol
636 DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022
ALCOHOL AND DIABETES/JANET McDONALD
on the onset of experimental atherosclerosis. Tohoku J. Exp. Med.114: 3 5 - 4 3 , 1974.
50 Masquelier, J.: Les constituants de vin presentant une actionhypocholesterolemiante. Proc. Cong. Med. Int. Etude Sci. VinRaisin, Bordeaux, 1961, pp. 137-42.
51 Henze, K., Bucci, A. , Signoretti, P., et al.: Alcohol intakeand coronary risk factors in a population group in Rome. Nutr.Metab. 21 (Suppl. 1): 157-59, 1977.
52 Nussbaum, L.: Is wine good therapy for heart disease? JAMA186: 27, 1963.
53 Stout, C , Morrow, J., Brandt, E. N . , Jr., and Wolf, S.: Un-usually low incidence of death from myocardial infarction. Study ofan Italian-American community in Pennsylvania. JAMA J88:8 4 5 - 4 9 , 1964.
54 St. Leger, A. S., Cochrane, A. L., and Moore, F.: Factorsassociated with cardiac mortality in developed countries with par-ticular reference to the consumption of wine. Lancet J: 1017—20, 1979.
55 Keller, M. (Ed.): Alcohol and Health. Second Special Reportto the U.S . Congress. Washington, D.C. , U .S . Government Print-ing Office, 1974, pp. 6 8 - 7 2 .
56 Klatsky, A. L., Friedman, G. D., and Siegelaub, A. B.: Alco-hol consumption before myocardial infarction: results from the Kai-ser-Permanente epidemiologic study of myocardial infarction. Ann.Intern. Med. 8J : 294 -301 , 1974.
57 Stason, W . B. , Neff, R. K., Miet t inen, O . S., et al.: Alcoholconsumption and non-fatal myocardial infarction. A m . J. Epide-miol. 104: 6 0 3 - 6 0 8 , 1976.
58 Barboriak, J. J., Rimm, A. A . , Anderson, A. J., et al.: Coro-nary artery occlusion and alcohol intake. Br. Heart J. 39: 2 8 9 - 9 3 ,1977.
59 Yano, K., Rhoads, G. G. , and Kagan, A . : Coffee, alcohol andrisk of coronary heart disease among Japanese men living in Hawaii.N . Engl. J. Med. 297: 4 0 5 - 4 0 9 , 1977.
60 Hennekens , C . H. , Rosner, B., and Cole, D. S.: Daily alcoholconsumption and fatal coronary heart disease. A m . J. Epidemiol.107: 196-200, 1978.
61 Hennekens, C. H., Willett, W., Rosner, B., et al.: Effects ofbeer, wine, and liquor in coronary deaths. JAMA 242: 1973-74,1979.
62 LaPor te , R. E. , Cresan ta , J. L , and Kuller, L. H . : T h e rela-
tionship of alcohol consumption to atherosclerotic heart disease.Prev. Med. 9: 2 2 - 4 0 , 1980.
63 Paul, O . , Lepper, M. H. , Phelan, W . H . , et al.: A longitudi-nal study of coronary heart disease. Circulation 28: 2 0 - 3 1 , 1963.
64 U . S . Nat ional Heart Institute: T h e Framingham Heart Study:Habits and Coronary Heart Disease. PHS Publ. No . 1515. Wash-ington, D . C . , U . S . Government Printing Office, 1966.
65 Kannel , W . B., and Woosley, P.: Alcohol and cardiovascularrisk. Circulation 52(Suppl. II): 200, 1975.
66 Castelli, W . P. , Doyle, J. T . , Gordon, T . , et al.: Alcohol andblood lipids. T h e Cooperative Lipoprotein Phenotyping Study. Lan-cet 2: 153-55, 1977.
67 Barboriak, J. J., Anderson, A. J., and Hoffman, R. G. : Inter-relationship between coronary artery occlusion, high-density lipo-protein cholesterol, and alcohol intake. J. Lab. Cl in . Med. 94:348-53, 1979.
68 Gordon, T . , Castelli, W . P. , Hjortland, M. C , et al.: Highdensity lipoprotein as a protective factor against coronary heart dis-ease. T h e Framingham Study. Am. J. Med. 62: 7 0 7 - 1 4 , 1977.
69 Marx, J. L.: T h e HDL: the good cholesterol carriers? Science205: 677-79, 1979.
70 Amer ine , M. A . : Composition of Wines. I. Organic Const i tu-ents. Adv . Food Res., Vol. V. New York, Academic Press, Inc. ,1954, pp. 353-430.
71 Koivisto, V. A.: Fructose as a dietary sweetner in diabetes mel-litus. Diabetes Care I: 241-46, 1978.
72 A m e r i n e , M. A . : W i n e . Sci. A m . 211: 4 6 - 5 5 , 1964.73 Wes t , K. M . : Diabetes mell i tus. In Nut r i t iona l Suppor t of
Medical Practice. Schneider, H. A., Anderson, C. E., and Cour-sin, D. B., Eds. Hagerstown, Md., Harper &. Row, 1977, pp. 278-96.
74 Gastineau, C. F.: Nutrition note. Alcohol and calories. MayoClinic Proc. 5/: 88, 1976.
75 Rubin , H . : Dry wines for diabetics? In Winemas t e r c o l u m n ,San Francisco C h r o n i c l e , July 27 , 1977.
76 Ough, C. S., and Cooke, G. M.: A rapid semi-quantitative re-ducing sugar test for dry wines. Wines Vines 47: 27-29, 1966.
77 Ough, C. S.: Sugar test (letter). Wines Vines 47: 32, 1966.78 Alcohol-Drug Interactions. FDA Drug Bull. 9: 10-12, 1979.7 9 W e s t , K. M . : Diet therapy of d iabe tes : a n analysis of failure.
Ann. Intern. Med. 79: 425-34, 1973.
DIABETES CARE, VOL. 3 NO. 5, SEPTEMBER-OCTOBER 1980 637
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/3/5/629/464396/3-5-629.pdf by guest on 24 February 2022