Severe coagulopathy and transient hypertension following a ...

of 13
Upload
sonia-martinCategory
view
215download
07/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
1/13
Reversal of Coagulopathy in Critically Ill Patients WithTraumatic Brain Injury: Recombinant Factor VIIa is More
Cost-Effective Than PlasmaDeborah M. Stein, MD, MPH, Richard P. Dutton, MD, MBA, Mary E. Kramer, RN,and Thomas M. Scalea, MD
Background: Traumatic brain injury(TBI) is the leading cause of death and dis-
ability after trauma. Coagulopathy is com-
mon in this patient population and requires
rapid reversal to allow for safe neurosurgi-
cal intervention and prevent worsening of
the primary injury. Typically reversal of co-
agulopathy is accomplished with the use of
plasma. Recombinant factor VIIa (rFVIIa;NovoSeven, Novo Nordisk, Bagsvaerd,
Denmark) has become increasingly used
off-label in patients with neurosurgical
emergencies to rapidly reverse coagulopa-
thy. We hypothesized that the use of rFVIIa
in this patient population would prove to
be cost-effective as well as demonstrate
clinical benefit.
Methods: The trauma registry at theR Adams Cowley Shock Trauma Center
was used to identify all coagulopatic trauma
patients admitted between January 2002
and December 2007 with relatively isolated
TBI (head Abbreviated Injury Scale score
of>4). The medical records of patients were
reviewed and demographics, injury-specific
data, medications administered, laboratory
values, blood product utilization, neurosur-
gical procedures, length of stay (LOS), dis-
charge disposition, and outcome data were
abstracted. Patients who received rFVIIa
for reversal of coagulopathy were com-
pared against those who did not receive
rFVIIa. t Tests were used to compare dif-
ferences between continuous variables,
and 2 analysis was used to compare cat-
egorical variables. A p value of
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
2/13
ber of patients may be taking preinjury anticoagulants such as
warfarin. Use of these medications is associated with a markedly
higher mortality rate in injured patients.12 Even in the absence of
these other factors, coagulopathy can occur as a direct result of
brain injury. This is thought to be because of the release of tissue
thromboplastin and activation of systemic fibrinolysis.4,68
Coagulopathy in patients with TBI precludes safe neurosur-gical intervention and may result in worsening of the primary
injury if left untreated. Coagulopathy in this patient population is
typically reversed with the use of fresh frozen or thawed fresh
plasma and vitamin K. This therapy may result in slow correc-
tion times and a delay in vital therapy. The volume of plasma
required to normalize coagulation is variable and unpredictable,
and simple replacement of clotting factors with plasma may not
achieve normal coagulation in patients with significant physio-
logic dysfunction. In addition, not only can large volumes of
plasma precipitate pulmonary edema in patients with cardiac
dysfunction, a number of studies have also documented worse
outcomes in patients who required large volume transfusions ofplasma during acute care hospitalizations.1316
Recombinant activated factor VII (rFVIIa; NovoSeven,
Novo Nordisk, Bagsvaerd, Denmark) is a drug developed for
treatment of hemophiliacs with inhibitors to factors VIII and
IX.9,17 Recombinant factor VIIa has become increasingly
used off-label in patients for both traumatic and nontrau-
matic neurosurgical emergencies.1836 However, to date, no
randomized prospective trial has been published describing
efficacy in this patient population. A number of case series
and retrospective studies have demonstrated effective use in
coagulopathic patients with TBI.18,21,30,31,33,36 Recombinant
activated factor VII is expensive, however, costing approxi-mately US $1.00 per microgram. Complete reversal of co-
agulopathy with rFVIIa can thus cost up to US $10,000.
Given the lack of high-quality evidence describing clinical
effectiveness of this therapy, significant questions have been
raised about the cost-effectiveness of the use of rFVIIa in
these off-label clinical scenarios, especially in light of the
frequency of its use in many hospitals.20,30,32,3742
At the R Adams Shock Trauma Center (STC), we have
used rFVIIa on an off-label basis since 2001. We began using
this therapy initially for acute traumatic hemorrhage and ex-
tended our use to patients with coagulopathy and TBI. Given the
results of recent work from our institution demonstrating adecreased time to neurosurgical intervention in coagulopathic
patients with severe TBI and a trend toward a decreased length
of stay (LOS),30 we hypothesized that the use of rFVIIa in this
patient population would prove to be cost-effective as well as
demonstrate clinical benefit.
MATERIALS AND METHODSAfter approval by the University of Maryland Institutional
Review Board, the trauma registry at the R Adams Cowley STC
was used to identify all trauma patients admitted between Jan-
uary 2002 and December 2007 with an anatomic TBI (head
Abbreviated Injury Scale, AIS score of4). Patients with any
other body region AIS score of3 were then excluded to limit
the effect of hemorrhage and coagulopathy from significant
concomitant injuries on the decision to use rFVIIa. All patients
who were coagulopathic at admission (International normalized
ratio, INR 1.4) were identified. This definition of coagulopa-
thy was chosen because this is the clinical value at which our
neurosurgeons request normalization in patients with TBI. Weare unaware of any data that support this practice, but given the
retrospective nature of this work, utilization of the clinical trig-
ger for reversal of coagulopathy at our institution was chosen for
the definition of coagulopathy for the purposes of this study. The
medical records of patients were reviewed. Patients who died
within 24 hours of admission and those that were deemed non-
survivable at the time of neurosurgical consultation, and there-
fore no reversal of coagulopathy was attempted, were excluded.
During the study period, the neurosurgical management of
all patients was done by a single neurosurgical group and ac-
cording to an institutional protocol based on the Brain Trauma
Foundation Guidelines.43
Administration of rFVIIa for all pa-tients at STC is requested by the attending surgeon, intensivist,
or anesthesiologist, and requires approval from an institutional
gatekeeper. Request for the use of rFVIIa for reversal of coagu-
lopathy in patients with TBI was entirely at the discretion of the
treating physician and was nonprotocolized. The gatekeepers
monitor usage and recommend dosing based on the clinical
status of the patient.
The medical records of all study subjects were reviewed
and demographics, injury-specific data, medications ad-
ministered, laboratory values, blood product utilization,
LOS, discharge disposition, and outcome data were ab-
stracted. Neurosurgical procedures, including craniotomy, in-traventricular catheter placement, fiberoptic pressure monitor
placement, or subdural drain placement, were also recorded.
Financial data were obtained from the Finance Office at the
STC. Patients who met inclusion criteria for the study who
received rFVIIa for reversal of coagulopathy were identified
and compared against those who met inclusion criteria but did
not receive rFVIIa. t Tests were used to compare differences
between continuous variables, and 2 analysis was used to
compare categorical variables. A p value of0.05 was con-
sidered significant for all statistical tests.
RESULTSDuring a 6-year period, there were 36,624 injured patientsadmitted to the R Adams Cowley STC, 2,997 with an anatomic
severe TBI (head AIS score of4). Of these patients, 1,671
were identified with a relatively isolated TBI (no other body
region AIS score of3). Of these, 302 were found to be
coagulopathic at admission (INR 1.4). Upon review of the
patients records, 76 patients with a LOS 24 hours were
excluded, as were 47 patients in whom no attempt at reversal of
coagulopathy was attempted because of nonsurvivability. One
hundred seventy-nine patients were subsequently included for
further analysis. One hundred eleven (62.0%) were treated with
conventional therapy alone whereas 68 (38.0%) received rFVIIa
The Journal ofTRAUMA Injury, Infection, and Critical Care
64 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
3/13
for reversal of their coagulopathy (Fig. 1). Doses of rFVIIa
administered ranged from 5.9 g/kg to 115 g/kg (mean
41.9 35.5, median 25.1).
Baseline characteristics between the two groups were com-
pared. There were no differences in age, predicted survival
(Trauma Score Injury Severity Score), admission revised trauma
score, or admission Glasgow Coma Scale (GCS) in the two
groups, whereas Injury Severity Score and admission INR were
significantly higher in the rFVIIa group. There was no differencein sex distribution or mechanism of injury between the groups,
but the rFVIIa group had a higher percentage of patients with
head AIS score of 5 injuries (as compared with AIS score equal
to 4), a greater frequency of patients who underwent neurosur-
gical procedures and a higher percentage of patients with pre-
injury warfarin use as the cause of their coagulopathy. Table 1
depicts the characteristics of these two groups.
There was no significant difference in total hospital
charges or costs between the two groups (Fig. 2). When
stratified by cost center, pharmacy charges and costs were
significantly higher in the group that received rFVIIa (Fig. 3,
A and B). Outcome measures were also evaluated. Outcome
data for the two groups are detailed in Table 2. LOS and
intensive care unit LOS (ICU-LOS) were the same in the two
groups, but functional outcome measures for survivors, such
as discharge GCS and Rancho Los Amigos Cognitive Scale
(RLAS), were higher in the conventionally treated patients.
There was no difference in mortality rates (18.9% in the no rFVIIa
group vs. 26.5% in the rFVIIa group, p 0.5) or thromboembolic
complication rates (16.2% vs. 19.1%, p 0.6). Thromboem-
bolic complications in the conventionally treated group in-
cluded two territorial cerebral infarctions (CI), one CI sec-
ondary to brain herniation, two suspected CIs, one cardiac
Fig. 1. Study population.
Table 1 Baseline Characteristics of All Patients
No rFVIIa (n 111) rFVIIa (n 68)p
Mean Mean
Age (yr) 57.4 23.2 61.4 24.9 0.273ISS 24.0 7.2 26.7 8.0 0.024Predicted survival
(TRISS)0.77 0.25 0.75 0.23 0.586
RTS 6.56 1.67 6.60 1.50 0.858Admission GCS 10.6 4.9 10.2 4.4 0.574Admission INR 1.9 0.7 2.5 0.7 0.001
n % n % p
Male 71 64.0 43 63.2 0.914Blunt injury 106 95.5 65 95.6 0.975Head AIS
4 75 67.6 32 47.1 0.0075 36 32.4 36 52.9 0.007
Neurosurgicalintervention
41 36.9 48 70.6 0.001
Cause ofcoagulopathy
Warfarin 54 48.6 45 66.2 0.028TBI alone 46 41.4 21 30.9 0.161Cirrhosis 9 8.1 3 4.4 0.338
ISS, Injury Severity Score; TRISS, Trauma Score, Injury SeverityScore; RTS, Revised Trauma Score; GCS, Glasgow Coma Scale; PT,prothrombin time; INR, International normalized ratio; AIS, Abbrevi-ated Injury Scale; TBI, traumatic brain injury.
Reversal of Coagulopathy in TBI Patients
Volume 66 Number 1 65
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
4/13
thrombus, four myocardial infarctions, three patients with
myocardial ischemia manifested by elevated cardiac en-
zymes, two deep venous thromboses, and five pulmonary
emboli. In the 68 patients in the rFVIIa group, there were one
territorial CI, three CIs secondary to brain herniation, two
suspected CIs, one cardiac thrombus, three myocardial in-
farctions, one patient with myocardial ischemia, two deep
venous thromboses, one pulmonary emboli, and one patient
with a sagittal sinus thrombosis.
When the patient populations included for analysis were
examined in detail, it was realized that there were a large
percentage of patients who had a head AIS score of 4 or 5
injury on CT, but were not physiologically or neurologically
compromised. These patients had markedly different baseline
characteristics and outcomes than patients who required ICU
admission (Table 3). Therefore, to better evaluate the effective-
ness and potential cost benefit in patients who had significant
neurologic or physiologic sequelae of their injuries, patients who
required admission to the ICU were analyzed separately.
There were 110 patients (61.4%) who required ICU
admission. Fifty-five (50%) received conventional therapy
alone and 55 received rFVIIa. Baseline characteristics of
these two groups are shown in Table 4. The group that
received rFVIIa had a higher mean admission INR, a
higher percentage of AIS score of 5 head injuries, more
neurosurgical interventions, and was more likely to have
preinjury warfarin use as the primary cause of their co-
agulopathy. Admission Injury Severity Score, predicted
survival, revised trauma score, and admission GCS were
no different between the two groups.
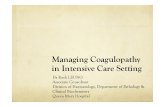
For patients requiring ICU admission, total mean
charges and costs were significantly lower in the group
that received rFVIIa (Fig. 4). When analyzed by cost
center, hospital (bed), laboratory, blood bank, respira-
tory service and rehabilitation service charges, and costs
were less in the group that received rFVIIa (Fig. 5, A and
B). When outcome measures were evaluated, total days of
mechanical ventilation and LOS were significantly lower
in the rFVIIa group (Table 5). Charges and costs per day
of hospitalization were analyzed to determine the effect of
LOS on total charges and costs. A nonsignificant increase
in charges and cost per day of admission was noted in the
group that received rFVIIa (Fig. 6). When charges and
costs per day were stratified by cost center, pharmacy
charges and costs were significantly higher in the rFVIIa
Fig. 2. Total charges and costs for all patients.
Fig. 3. (A) Charges for all patients. (B) Costs for all patients.
Table 2 Outcomes of All Patients
No rFVIIa(n 111)
rFVIIa(n 68)
p
Mean Mean
LOS (d) 11.7 13.9 11.8 10.1 0.976
ICU-LOS (d) 8.5 14.2 10 10.2 0.465Discharge GCS 13.2 2.6 11.9 2.6 0.006Discharge RLAS 5.9 2.0 5.2 2.0 0.036
n % n % p
Mortality 21* 18.9 18 26.5 0.517Thromboembolic complications 18 16.2 13 19.1 0.233
* Withdrawal of care in 13 of 21 patients. Withdrawal of care in 16 of 18 patients.LOS, length of stay; ICU, Intensive Care Unit; GCS, Glasgow
Coma Scale; RLAS, Rancho Los Amigos Cognitive Scale.
The Journal ofTRAUMA Injury, Infection, and Critical Care
66 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
5/13
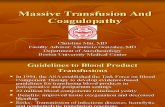
group (Fig. 7, A and B). In addition, blood product utili-
zation was examined for the groups who required ICU
admission. There were significant differences in total units
of red blood cells (RBC) and platelets administered during
hospitalization between the two groups as well as signifi-
cant differences in the number of units of plasma trans-
fused in the first 24 hours of admission, as well as during
the entire hospitalization (Fig. 8). Functional outcome mea-
sures for survivors recorded at discharge were no different in the
two groups. Similarly, mortality and thromboembolic compli-
cation rates were not statistically different between the pa-tients that received rFVIIa and those that were treated with
conventional therapy alone (Table 5).
The group that did not require ICU admission was similarly
analyzed. Fifty-six patients (81.1%) were treated with conven-
tional therapy alone and 13 were treated with rFVIIa. Baseline
characteristics were no different in the group that received con-
ventional therapy and the group that was treated with rFVIIa
(Table 6). Total mean charges and costs were not signifi-
cantly different between the groups (Fig. 9), but pharmacy
charges and costs were significantly higher in the rFVIIa
group (Fig. 10, A and B). In terms of outcome variables, no
differences were noted between the two groups (Table 7).
DISCUSSION
Coagulopathy occurs commonly in patients with TBI
and must be addressed rapidly to allow for safe neurosur-
gical intervention and prevent worsening of the primary
injury from ongoing hemorrhage. Recombinant factor VIIa
has been used in hemorrhaging trauma patients for many
years.18,4448 Numerous reports exist in the literature de-
scribing the successful use of rFVIIa in patients requiring
neurosurgical intervention2123,30,31,33,35 and for the pre-
vention of progression of injury in patients with nonsurgical
intracranial bleeds.10,27,28,33,34 Recombinant activated factorVII has also been successfully used as an effective reversal
agent in patients with neurosurgical emergencies who were
taking preadmission warfarin.19,25,26,30,33 However, no pro-
spective, randomized trial examining the effectiveness of
rFVIIa in patients with TBI has been conducted.
Reversal of coagulopathy with conventional therapy
takes time and may delay neurosurgical intervention.30 In
one study, it was demonstrated that the rate of correction
of the INR with plasma and vitamin K is only 0.18
INR/h.49 Recent data from our institution demonstrated
that coagulopathic patients with severe TBI treated with
Table 3 Comparison of Patients Requiring ICU Admission and Those Who Did Not
ICU (n 110) No ICU (n 69)p
Mean Mean
Age (yr) 55.8 23.9 63.9 23.0 0.027ISS 26.8 7.9 22.2 6.1 0.001
Predicted survival (TRISS) 0.70 0.26 0.86 0.18 0.001RTS 6.13 1.63 7.29 1.26 0.001
Admission GCS 8.8 4.6 13.1 3.8 0.001Admission INR 2.2 1.1 2.1 0.7 0.545LOS (d) 16.6 13.9 4.1 2.7 0.001Discharge GCS 11.2 2.8 14.6 1.0 0.001Discharge RLAS 4.5 1.8 7.1 1.2 0.001Total charges (US $) 92,814 76,944 19,161 14,074 0.001Total costs (US $) 65,274 54,205 13,025 9,308 0.001
n % n % p
Male 72 65.4 41 59.4 0.419Blunt injury 103 93.6 67 97.1 0.299Head AIS
4 56 50.9 51 73.9 0.003
5 54 49.1 18 26.1 0.003Neurosurgical intervention 77 70.0 12 17.4 0.001Cause of coagulopathy
Warfarin 52 47.3 47 68.1 0.007TBI alone 51 46.4 16 23.2 0.002Cirrhosis 6 5.4 5 8.7 0.390
Received rFVIIa 55 50.0 13 18.8 0.001Mortality 31* 28.2 8 13.0 0.001Thromboembolic complications 24 21.8 8 11.6 0.085
* Withdrawal of care in 22 of 31 patients. Withdrawal of care in 7 of 8 patients.ISS, Injury Severity Score; TRISS, Trauma Score Injury Severity Score; RTS, Revised Trauma Score; GCS, Glasgow Coma Scale; PT,
prothrombin time; INR, International normalized ratio; AIS, Abbreviated Injury Scale; TBI, traumatic brain injury; LOS, length of stay; GCS,Glasgow Coma Scale; RLAS, Rancho Los Amigos Cognitive Scale.
Reversal of Coagulopathy in TBI Patients
Volume 66 Number 1 67
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
6/13
conventional therapy alone took, on average, three times
longer to receive neurosurgical intervention.30 Despite the
potential benefit of rFVIIa in achieving quicker interven-
tion times, no statistically significant outcome differences
were appreciated in this small group of patients.
Cost-effectiveness of rFVIIa in patients with neuro-
surgical emergencies remains a topic of considerable
debate.23,30,32,39,50,51 Several reports have been published
attempting to address the issue of cost-effectiveness in
patients treated both on-label and off-label with
rFVIIa.38,39,40,50,52,53 Generally, these studies have dem-
onstrated a cost benefit for patients treated with rFVIIa. In
this study, we were able to demonstrate a significant eco-
nomic benefit of the use of rFVIIa for reversal of coagu-
lopathy in severely injured patients with TBI.
Fig. 4. Total charges and costs for patients admitted to the ICU.
Fig. 5. (A) Charges for patients admitted to the ICU. (B) Costs for
patients admitted to the ICU.
Table 4 Baseline Characteristics of Patients Admittedto the ICU
No rFVIIa(n 55)
rFVIIa(n 55)
p
Mean Mean
Age (yr) 51.7 22.3 59.7 25.1 0.078ISS 26.3 8.1 27.1 7.7 0.595Predicted survival
(TRISS)0.68 0.27 0.74 0.23 0.216
RTS 6.49 1.50 6.69 1.40 0.554Admission GCS 8.2 4.8 9.7 4.3 0.080Admission INR 1.9 0.8 2.5 1.3 0.004
n % n % p
Male 36 65.5 36 65.5 1.000Blunt injury 52 94.5 51 92.7 0.700Head AIS
4 34 61.8 22 40.0 0.0245 21 38.2 33 60.0 0.024
Neurosurgical
intervention
33 60.0 44 80.0 0.024
Cause ofcoagulopathy
Warfarin 17 30.9 35 63.6 0.001TBI alone 32 58.2 19 34.5 0.014Cirrhosis 5 9.1 1 1.8 0.095
ISS, Injury Severity Score; TRISS, Trauma Score Injury SeverityScore; RTS, Revised Trauma Score; GCS, Glasgow Coma Scale; PT,prothrombin time; INR, International normalized ratio; AIS, Abbrevi-ated Injury Scale; TBI, traumatic brain injury.
Table 5 Outcomes for Patients Admitted to the ICU
No rFVIIa(n 55)
rFVIIa(n 55)
p
Mean Mean
Ventilator days 15.4 14.7 8.8 8.0 0.004LOS (d) 19.4 16.3 13.7 10.2 0.029ICU-LOS (d) 17.2 16 12.3 9.9 0.057Discharge GCS 11.5 2.9 11.0 2.7 0.454Discharge RLAS 4.6 1.9 4.5 1.8 0.909
n % n % p
Mortality 15* 27.3 16 29.1 0.834Thromboembolic complications 11 20.0 12 21.8 0.817
* Withdrawal of care in 8 of 15 patients. Withdrawal of care in 14 of 16 patients.LOS, length of stay; ICU, Intensive Care Unit; GCS, Glasgow
Coma Scale; RLAS, Rancho Los Amigos Cognitive Scale.
The Journal ofTRAUMA Injury, Infection, and Critical Care
68 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
7/13
Not all patients with coagulopathy and an anatomic brain
injury will necessarily benefit from rFVIIa administration,
but we have clearly shown that in patients who are neurolog-
ically or physiologically compromised, using rFVIIa to re-
verse coagulopathy significantly decreases total charges and
costs of hospitalization. This was found to be true even
though the patients who received rFVIIa had a higher AIS
grade of brain injury and were more likely to require neuro-
surgical intervention than patients who had reversal of their
coagulopathy with plasma alone. This decrease in overall cost
is directly attributable to the clinically and statistically sig-
nificant decrease in LOS, as charges and costs per day were
comparable in the two groups. The increase in pharmacy
costs with the use of rFVIIa is directly offset by the decrease
in LOS. In addition, the utilization of fewer blood products
contributes to the cost savings as well. At our institution, the
cost of a single 1.2-mg vial, the smallest dose-vial of Novo-
Seven available, is US $1,100.35. This is equivalent to ap-
Fig. 6. Total charge and cost per day for patients admitted to the
ICU.
Fig. 7. (A) Charge per day for patients admitted to the ICU. (B)
Cost per day for patients admitted to the ICU.
Fig. 8. Blood product use in patients admitted to the ICU.
Table 6 Baseline Characteristics of Patients NotRequiring ICU Admission
No rFVIIa(n 56) rFVIIa(n 13)p
Mean Mean
Age (yr) 62.9 22.9 68.5 23.6 0.438ISS 21.8 5.4 24.6 9.3 0.142Predicted survival
(TRISS)0.86 0.18 0.81 0.24 0.374
RTS 7.28 1.23 7.12 1.57 0.697Admission GCS 13.0 3.8 12.4 4.5 0.604Admission INR 2.0 0.6 2.4 0.9 0.050
n % n % p
Male 35 62.5 6 46.1 0.282Blunt injury 54 96.4 13 100.0 0.490Head AIS
4 41 73.2 10 76.9 0.7855 15 26.7 3 23.1 0.791
Neurosurgicalintervention
8 14.2 4 30.7 0.161
Cause ofcoagulopathy
Warfarin 37 66.1 10 76.9 0.454TBI alone 14 25.0 2 15.4 0.463Cirrhosis 4 7.1 1 7.7 0.940
ISS, Injury Severity Score; TRISS, Trauma Score Injury SeverityScore; RTS, revised trauma score; GCS, Glasgow Coma Scale; PT,prothrombin time; INR, International normalized ratio; AIS, Abbrevi-ated Injury Scale; TBI, traumatic brain injury.
Reversal of Coagulopathy in TBI Patients
Volume 66 Number 1 69
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
8/13
proximately 9 units of administered plasma. Even if the cost
of rFVIIa is not directly offset by the savings in units of
plasma administered, the reduction in ventilator days and
LOS clearly compensates for the cost of the drug.
The direct cause of the decrease in LOS and subsequent
charges and costs in the population of patients who required
ICU admission and received rFVIIa cannot be analyzed in
this retrospective study, but hypotheses can be generated. It
has been well known for years that administration of red
blood cells is associated with worse outcomes because of an
increased risk of infections, organ dysfunction, and respira-
tory failure.13,5457 There is an increasing body of literature
that describes worse outcomes in patients who receive plasmaas well.1316 Many of these studies describe an increase in
respiratory failure and acute lung injury or acute respiratory
distress syndrome (ARDS) with the administration of plasma.
At least one publication of subgroup analysis from two ran-
domized trials describes that the use of rFVIIa and the atten-
dant decrease in transfusion requirements were associated
with a lower rate of organ failure and ARDS.58 In this current
study, the number of units of plasma transfused in both the
first 24 hours as well as throughout the hospitalization was
significantly lower in the rFVIIa group. Perhaps, this directly
resulted in a decrease in the need for days of mechanical
ventilation because of a lower incidence of respiratory dys-function. The total number of units of packed RBC and
platelets transfused were not different in the first 24 hours of
hospitalization, but were lower for the entire LOS. Whether
the decrease in the number of packed RBC and platelets
transfused in the rFVIIa group is a cause or an effect of a
shorter LOS is unknown. Whatever the cause, the use of
rFVIIa for reversal of coagulopathy in patients with TBI who
required ICU admission was clearly associated with fewer
days of mechanical ventilation, a shorter hospital LOS, and a
decrease in overall charges and costs of hospitalization.
In addition to the economic benefit demonstrated here,
there may be a benefit in functional outcome as well. Al-though there was no difference in functional outcome mea-
sures between the two groups that required ICU admission,
these measures were evaluated at hospital discharge. The fact
that LOS was shorter in the rFVIIa means that these measures
were recorded days earlier in the rFVIIa groups. As func-
tional outcome is an exquisitely time-sensitive measure, it
may be expected that if measured at the same time points
after injury, patients who received rFVIIa for reversal of their
coagulopathy might have better functional outcome scores
than those who were treated with conventional therapy
alone. Alternatively, because of the frequency of plateaus
in functional recovery after TBI, perhaps the group treated
Fig. 9. Total charges and costs for patients not requiring ICU
admission.
Fig. 10. (A) Charges for patients not requiring ICU admission. (B)Costs for patients not requiring ICU admission.
Table 7 Outcomes for Patients Not Requiring ICUAdmission
No rFVIIa(n 56)
rFVIIa(n 13)
p
Mean Mean
LOS (d) 4.1 2.8 3.7 2.2 0.610Discharge GCS 14.5 1.0 14.7 0.5 0.545Discharge RLAS 7.0 1.3 7.4 0.9 0.395
n % n % p
Mortality 6* 10.7 2 15.3 0.788Thromboembolic complications 7 12.5 1 7.8 0.642
Withdrawal of care in 5 of 6 patients. Withdrawal of care in 2 of 2 patients.LOS, length of stay; ICU, Intensive Care Unit; GCS, Glasgow
Coma Scale; RLAS, Rancho Los Amigos Cognitive Scale.
The Journal ofTRAUMA Injury, Infection, and Critical Care
70 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
9/13
with rFVIIa simply recovered functional status sooner than
those patients treated with plasma. However, the retrospec-
tive nature of this work severely limits conclusions concern-
ing functional outcome.
Importantly, there was no difference in mortality in the
groups evaluated in this study, despite the fact that patients in
the rFVIIa group had more severe anatomic injury and were
more likely to require neurosurgical intervention. Demon-
strating a mortality benefit with the use of rFVIIa in severely
injured patients with TBI is likely to require hundreds of
patients and is impractical in a retrospective study of this size.
The baseline rate of thromboembolic complications was high
in the severely injured patients presented in this study. De-
spite consistent concerns in the literature about the risk of
thromboembolic complications in patients treated with
rFVIIa,28,5961 no increase in the risk of thromboembolic
complications was demonstrated in this study.
As important as determining which patients with TBI ben-efit from the use of rFVIIa is determining which subset of
patients do not benefit. In our institution, admission to the ICU
is dictated by the need for intracranial pressure monitoring, the
need for mechanical ventilation, or the need for vasoactive
medication infusion. Other patients who simply need close mon-
itoring with serial neurologic examinations for their TBI are
often admitted to our Neurotrauma Intermediate Care Unit.
In the group not requiring ICU admission, patients were
typically administered plasma or rFVIIa and admitted to
the Intermediate Care Unit and discharged to home within
a few days. Use of rFVIIa in these patients demonstrated
no clear benefit, but also did not demonstrate any evidenceof worse outcome or increase in cost. Low numbers of
patients in this subset may have limited our ability to draw
conclusions about the use of rFVIIa.
There are several important and obvious limitations to
this study. First, the retrospective design does not allow for
the determination of cause and effect but rather only sug-
gests the identification of associations. In this retrospective
study, there is clearly a selection bias in who receives rFVIIa
and who gets treated with conventional therapy based on the
patients degree of coagulopathy, the perceived urgency of
reversal, and the patients clinical status. The study design
also limits the type of clinical information that could becompared between the two groups because of the consistency
of documented information.
Despite its limitations, this study has clearly demonstrated
that in coagulopathic patients with TBI who require ICU admis-
sion, patients selected to receive rFVIIa demonstrated greater
cost-effectiveness of care, decreases in ventilator days, and a
shorter hospital LOS. In addition, we have provided an addi-
tional evidence that rFVIIa is safe in this patient population.
Prospective studies in this patient population are sorely needed
to confirm these findings and to establish clinical effectiveness
to ultimately improve outcome in patients with severe TBI.
REFERENCES1. Shackford SR, Mackersie RC, Holbrook TL, et al. The epidemiology of
traumatic death. A population-based analysis. Arch Surg. 1993;128:571
575.
2. Langlois JA, Rutland-Brown W, Thomas KE. Traumatic Brain Injury in
the United States: Emergency Department Visits, Hospitalizations, and
Deaths. Atlanta, GA: Centers for Disease Control and Prevention, Nation
Center for Injury Prevention and Control; 2006.
3. Thurman D, Alverson C, Dunn K, Guerrero J, Sniezek JE.
Traumatic brain injury in the United States: a public health
perspective. J Head Trauma Rehabil. 1999;14:602615.
4. Cortiana M, Zagara G, Fava S, Seveso M. Coagulation abnormalities
in patients with head injury. J Neurosurg. 1986;30:133138.
5. Zehtabchi S, Soghoian S, Carmody K, et al. The association of
coagulopathy and traumatic brain injury in patients with isolated
head injury. Resuscitation. 2008;76:5256.
6. Stein SC, Smith DH. Coagulopathy in traumatic brain injury.
Neurocrit Care. 2004;1:479488.
7. Zygun DA, Kortbeek JB, Fick GH, Laupland KB, Doig CJ. Non-
neurologic organ dysfunction in severe traumatic brain injury. Crit
Care Med. 2005;33:654660.
8. Hulka F, Mullins R, Frank E. Blunt brain injury activates thecoagulation process. Arch Surg. 1996;131:923928.
9. Powner DJ, Hartwell EA, Hoots WK. Counteracting the effects of
anticoagulants and antiplatelet agents during neurosurgical
emergencies. Neurosurgery. 2005;57:823831.
10. May AK, Young JS, Butler K, Bassam D, Brady W. Coagulopathy in
severe closed head injury: is empiric therapy warranted? Am Surg. 1997;
63:233237.
11. Carrick MM, Tyroch AH, Youens CA, Handley T. Subsequent
development of thrombocytopenia and coagulopathy in moderate and
severe head injury: support for serial laboratory examination.
J Trauma. 2005;58:725730.
12. Cohen DB, Rinker C, Wilberger JE. Traumatic brain injury in
anticoagulated patients. J Trauma. 2006;60:553557.
13. Bochicchio GV, Napolitano L, Joshi M, Bochicchio K, Meyer W,
Scalea TM. Outcome analysis of blood product transfusion in
trauma patients: a prospective, risk-adjusted study. World J Surg.
2008;32:21852189.
14. Dara SI, Rana R, Afessa B, Moore SB, Gajic O. Fresh frozen
plasma transfusion in critically ill medical patients with
coagulopathy. Crit Care Med. 2005;33:26672671.
15. Etemadrezaie H, Baharvahdat H, Shariati Z, Lari SM, Shakeri
MT, Ganjeifar B. The effect of fresh frozen plasma in severe
closed head injury. Clin Neurol Neurosurg. 2007;109:166171.
16. Khan H, Belsher J, Yilmaz M, et al. Fresh-frozen plasma and
platelet transfusions are associated with development of acute lung
injury in critically ill medical patients. Chest.
2007;131:13081314.
17. Hedner U. Mechanism of action of factor VIIa in the treatment of
coagulopathies. Semin Thromb Hemost (Suppl). 2006;32:S77S85.18. Dutton RP, McCunn M, Hyder M, et al. Factor VIIa for correction
of traumatic coagulopathy. J Trauma. 2004;57:709719.
19. Srensen B, Johansen P, Nielsen GL, Srensen JC, Ingerslev J.
Reversal of the international normalized ratio with recombinant
activated factor VII in central nervous system bleeding during
warfarin thromboprophylaxis: clinical and biochemical aspects.
Blood Coagul Fibrinolysis. 2003;14:469477.
20. Roitberg B, Emechebe-Kennedy O, Amin-Hanjani S, Mucksavage J,
Tesoro E. Human recombinant factor VII for emergency reversal of
coagulopathy in neurosurgical patients: a retrospective comparative
study. Neurosurgery. 2005;57:832836.
21. Park P, Fewel ME, Garton HJ, Thompson BG, Hoff JT. Recombinant
activated factor VII for the rapid correction of coagulopathy in
nonhemophilic neurosurgical patients. Neurosurgery. 2003;53:3439.
Reversal of Coagulopathy in TBI Patients
Volume 66 Number 1 71
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
10/13
22. Karadimov D, Binev K, Nachkov Y, Platikanov V. Use of activated
recombinant factor VII (Novoseven) during neurosurgery.
J Neurosurg Anesthesiol. 2003;15:330332.
23. Yusim Y, Perel A, Berkenstadt H, Attia M, Knoller N, Sidi A. The use of
recombinant factor VIIa (NovoSeven) for treatment of active or impending
bleeding in brain injury: broadening the indications. J Clin
Anesth. 2006;18:545551.
24. Freeman WD, Brott TG, Barrett KM, et al. Recombinant factor VIIafor rapid reversal of warfarin anticoagulation in acute intracranial
hemorrhage. Mayo Clin Proc. 2004;79:14955000.
25. Lin J, Hanigan WC, Tarantino M, Wang J. The use of recombinant
activated factor VII to reverse warfarin-induced anticoagulation in
patients with hemorrhages in the central nervous system: preliminary
findings. J Neurosurg. 2003;98:73740.
26. Brody DL, Aiyagari V, Shackleford AM, Diringer MN. Use of
recombinant factor VIIa in patients with warfarin-associated
intracranial hemorrhage. Neurocrit Care. 2005;2:263267.
27. White CE, Schrank AE, Baskin TW, Holcomb JB. Effects of
recombinant activated factor VII in traumatic nonsurgical intracranial
hemorrhage. Curr Surg. 2006;63:310317.
28. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII
for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777785.29. Mayer SA, Brun NC, Begtrup K, et al. Efficacy and safety of
recombinant activated factor VII for acute intracerebral hemorrhage.
N Engl J Med. 2008;358:21272137.
30. Stein DM, Dutton RP, Kramer ME, Handley C, Scalea TM. Recombinant
factor VIIa: decreasing time to neurosurgical intervention in patients with
severe traumatic brain injury. J Trauma. 2008;64:620628.
31. Bartal C, Freedman J, Bowman K, Cusimano M. Coagulopathic
patients with traumatic intracranial bleeding: defining the role of
recombinant factor VIIa. J Trauma. 2007;63:725732.
32. Hawryluk GW, Cusimano MD. The role of recombinant activated
factor VII in neurosurgery: hope or hype? J Neurosurg. 2006;
105:859868.
33. Stein DM, Dutton RP, Hess JR, Scalea TM. Low-dose recombinant
factor VIIa for trauma patients with coagulopathy. Injury. 2008;
39:10541061.34. Steiner T, Diringer MN, Schneider D, et al. Dynamics of
intraventricular hemorrhage in patients with spontaneous
intracerebral hemorrhage: risk factors, clinical impact, and effect of
hemostatic therapy with recombinant activated factor VII.
Neurosurgery. 2006;59:76774.
35. Uhrig L, Blanot S, Baugnon T, Orliaguet G, Carli PA, Meyer PG.
Use of recombinant activated factor VII in intractable bleeding
during pediatric neurosurgical procedures. Pediatr Crit Care Med.
2007;8:576579.
36. Zaaroor M, Soustiel JF, Brenner B, Bar-Lavie Y, Martinowitz U,
Levi L. Administration off label of recombinant factor-VIIa (rFVIIa)
to patients with blunt or penetrating brain injury without
coagulopathy. Acta Neurochir (Wein). 2008;150:663668.
37. Ganguly S, Spengel K, Tilzer LL, Oneal B, Simpson SQ.Recombinant factor VIIa: unregulated continuous use in patients
with bleeding and coagulopathy does not alter mortality and
outcome. Clin Lab Haematol. 2006;28:309312.
38. Loudon B, Smith MP. Recombinant factor VIIa as an adjunctive
therapy for patients requiring large volume transfusion: a
pharmacoeconomic evaluation. Intern Med J. 2005;35:463467.
39. Kissela BM, Eckman MH. Cost effectiveness of recombinant factor VIIa
for treatment of intracerebral hemorrhage. BMC Neurology. 2008;8:17.
40. Morris S, Ridley S, Munro V, Christensen MC. Cost effectiveness of
recombinant activated factor VII for the control of bleeding in patients with
severe blunt trauma injuries in the United Kingdom. Anaesthesia. 2007;
62:4352.
41. Rudisill CN, Hockman RH, DeGregory KA, Mutnick AH, Macik
BG. Implementing guidelines for the institutional use of factor VIIa
(recombinant): a multidisciplinary approach. Am J Health Syst
Pharm. 2006;63:16411646.
42. Ranucci M, Isgro G, Soro G, Conti D, De Toffol B. Efficacy and
safety of recombinant activated factor VII in major surgical
procedures. Arch Surg. 2008;143:296304.
43. Brain Trauma Foundation and AANS/CNS Joint Section on
Neurotrauma and Critical Care. Guidelines for the management of
severe traumatic brain injury. J Neurotrauma (Suppl). 2007;24:S1S106.44. Kenet G, Walden R, Eldad A, Martinowitz U. Treatment of traumatic
bleeding with recombinant factor VIIa. Lancet 1999;354:1879.
45. Harrison TD, Laskosky J, Jazaeri O, Pasquale MD, Cipolle M. Low-dose
recombinant activated factor VII results in less blood and blood product use
in traumatic hemorrhage. J Trauma. 2005;59:150154.
46. Boffard KD, Riou B, Warren B, et al. Recombinant factor VIIa as
adjunctive therapy for bleeding control in severely injured trauma
patients: two parallel randomized, placebo-controlled, double-
blind clinical trials. J Trauma. 2005;59:815.
47. Rizoli SB, Nascimento B, Osman F, et al. Recombinant activated
coagulation factor VII and bleeding trauma patients. J Trauma.
2006;61:14191425.
48. Perkins JG, Schreiber MA, Wade CE, Holcomb JB. Early versus late
recombinant factor VIIa in combat trauma patients requiring massivetransfusion. J Trauma. 2007;62:10951101.
49. Boulis N, Bobek M, Schmaier A, Hoff JT. Use of factor IX complex in
warfarin related intracranial hemorrhage. Neurosurgery. 1999;45:1113
1119.
50. Earnshaw SR, Joshi AV, Wilson MR, Rosand J. Cost-effectiveness
of recombinant activated factor VII in the treatment of intracerebral
hemorrhage. Stroke. 2006;37:27512758.
51. Traynor K. Budget-busting drug gets institutional oversight. Am J
Health-Syst Pharm. 2004;61:866867.
52. Galanaud JP, Pelletier-Fleury N, Logerot-Lebrun H, Lambert T.
Determinants of drug costs in the hospitalized patients with
haemophilia: impact of recombinant activated factor VII.
Pharmacoeconomics. 2003;21:699707.
53. Lyseng-Williamson KA, Plosker GL. Recombinant factor VIIa(Eptacog Alfa): a pharmacoeconomic review of its use in
haemophilia in patients with inhibitors to clotting factors VIII and
IX. Pharmacoeconomics. 2007;25:10071029.
54. Bulger EM, Jurkovich GJ, Nathens AB, et al. Hypertonic
resuscitation of hypovolemic shock after blunt trauma: a randomized
controlled trial. Arch Surg. 2008;143:139148.
55. Dellinger RP, Levy MM, Carlet JM, et al. Surviving sepsis
campaign: international guidelines for management of severe sepsis
and septic shock: 2008. Crit Care Med. 2008;36:296327.
56. Vincent JL, Baron JF, Reinhart K, et al. Anemia and blood transfusion in
critically ill patients. JAMA. 2002;288:
14991507.
57. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT study: anemia
and blood transfusions in the critically ill current clinical practicein the United States. Crit Care Med. 2004;32:3952.
58. Rizoli SB, Boffard KD, Riou B, et al. Recombinant activated factor
VII as an adjunctive therapy for bleeding control in severe trauma
patients with coagulopathy: subgroup analysis from two randomized
trials. Crit Care. 2006;10:R178.
59. Tawil I, Stein DM, Mirvis SE, Scalea TA. Post traumatic cerebral
infarction: incidence, outcome, and risk factors. J Trauma. 2008;64:849
853.
60. Thomas GO, Dutton RP, Hemlock B, et al. Thromboembolic
complications associated with factor VIIa administration. J Trauma.
2007;62:564569.
61. Narayan RK, Maas AIR, Marshall LF, Servadei F, Skolnick BE, Tillinger
MN. Recombinant factor VIIa in traumatic intracerebral hemorrhage: results
of a dose escalation trial. Neurosurgery. 2008;62:776788.
The Journal ofTRAUMA Injury, Infection, and Critical Care
72 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
11/13
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
12/13
the things that VIIa are supposed to do so why not show that
outcome data?
Dr. Lonnie Frei (Jackson, Mississippi): Im a big pro-
ponent of VIIa. Ive used it many times in the past. But it is
without a doubt without problems, including its cost.
One of the things that I found interesting was the INR that
you picked to choose and stratify your patients which was anINR of greater than 1.4. Yet your patient population who re-
ceived Factor VIIa on average had an INR that was 2.4.
Would it be advantageous to take a look at the amount of
FFP that would be required to treat these patients who have
INRs just slightly above 1.4 as opposed to those patients who
have the higher INR and would there, would the cost advan-
tage persist?
Secondarily, one of the things that is not explained is the
fact that those patients who received Factor VIIa had a de-
creased length of stay and ventilator days.
I think Factor VIIa is a great product for coagulation.
Does it have other properties that we dont know about or and I realize that thats probably not the case but in fact to
what do you attribute the decreased length of stay and the
decreased ventilator days in that patient population?
Dr. Carl J. Hauser (Boston, Massachusetts): I shouldsay up front that I am a consultant for Novo Nordisk and that
I co-chair the Steering Committee of the current Factor VIIa
trauma trial, although I hope it doesnt color my comments.
I thought this was a very nice study and I congratulate the
authors. This is an area where there is a lot of smoke and not
much light.
There are a couple of difficulties with interpreting the
clinical data, as the authors know very well. First, decreasedINR values per se dont necessarily reflect reversal of anti-
coagulation after Factor VIIa use. They simply reflect the
presence of VIIa in the plasma. Second, fresh frozen plasma
per se cannot correct an INR of 1.4. In fact, an INR of up
to 1.5 is considered normal by just about everyone except
neurosurgeons. Third, FFP can only correct a truly elevated
INR down to about 1.6 or 1.7. Treating past that with FP is of
no proven value, wasteful and potentially dangerous. There
was a great article on this by Holland and Brooks in the
American Journal of Clinical Pathology in 2006 that anyone
who thinks otherwise should read.
That said, I think the key issue from a pharmeco-economic point of view is the dose of Factor VIIa you use. If
the correction of anti-coagulation sought consists of achiev-
ing a normal INR I refer to this and the euboxia ap-
proach it can be done with very, very small amounts of
Factor VIIa. You dont need to use the 90 micrograms per
kilogram dose, a half or a third of that will do just fine. Thats
usually $1,200 or $2,400 worth which, as the authors point
out, is probably a bargain. The VIIa stroke trials suggest
higher doses may be marginally more effective but at some-
what higher risk of complications.
So Id like to know what dose the authors used or what
the range of doses that the group of users in their institution
used were. Also, were you able to track differences in com-
plications at different doses?
Dr. Bryan A. Cotton (Nashville, Tennessee): First of
all, Dr. Stein, fantastic study. Congratulations on your work.
Two quick questions.
One, did you look at the time to death in two different
groups to see if there were: 1, different causes and 2, howquickly they were dying?
And on that same note did you consider looking at
actually ventilator-free days versus just straight ventilator
days, looking more, again, as a better surrogate for time on
the ventilator?
Dr. Bijan S. Kheirabadi (San Antonio, Texas): I would
just like to know in this patient, was the fibrinogen level was
also decreased or whether giving Factor VIIa actually can
reverse in that situation?
Dr. Deborah M. Stein (Baltimore, Maryland): First of
all, let me thank you very much for your comments and
questions and, Dr. Valadka, for spending some time with me
this morning.
Let me address the issues of our definition of coagulopa-
thy that a couple of people have asked about. The reason we
chose an INR of less than or equal to 1.4 is simply because
thats what our neurosurgeons insist that we correct to. They
want it below 1.4. Where that comes from, nobody knows.
Nobody can explain it to me but thats what they want. And,
you know, for the purpose of a retrospective study using a
level that we clinically treat is what we felt was most appro-
priate. Certainly there are much better physiologic markers of
coagulopathy such as thromboelastography.
As far as concern about the short half-life of Recombi-
nant Factor VIIa, we do typically concomitantly administer
some plasma in these patients. But typically, if you want to
acutely reverse their coagulopathy in order to normalize
them, for example reverse their coagulopathy associated with
Coumadin use, typically one dose is all thats really needed.
And we do see consistently lower INRs thereafter.
In terms of Dr. Valadkas comments about not waiting to
correct their coagulopathy and taking the patient right to the
operating room, I could not agree with him more. I think that
may be the real benefit of the use of Recombinant Factor
VIIa. At our institution it takes about an hour for us to get
plasma from the time the patient gets typed. Typically this
drug can be given, a simple syringe, en route to the operating
room and I think that that actually is one of the real benefits
of the use of this approach.
In terms of Dr. Jurkovichs question about indiscriminate
use of Recombinant Factor VIIa, this was non-protocolized.
The decision to administer Recombinant Factor VIIa is left to
the discretion of the attending trauma surgeon or anesthesi-
ologist with gatekeeper approval. I do agree that it would be
nice to have a protocol. We dont have one currently and its
certainly not based on any manufacturer or label recommen-
dation as this is an entirely off-label indication.
The Journal ofTRAUMA Injury, Infection, and Critical Care
74 January 2009
7/27/2019 Reversal of Coagulopathy in Critically Ill Patients With Traumatic Brain Injury
13/13
We did not look at changes in imaging or reversal of
coagulopathy in terms of the INR for the purposes of this study
we did do that in our previous work because in this study we
really wanted to focus on the cost, potential cost-effectiveness.
In terms of Dr. Freis question about stratifying the
patients by their initial INR. I think thats a wonderful idea.
It certainly is something Im very happy to go back and takea look at our data and do.
Why the length of stay was lower, why ventilator days
were lower? I think its not necessarily the benefit of Factor
VII but really what youre doing is reducing the amount of
plasma. The one thing I want to make very clear is I dont
think that Recombinant Factor VIIa is a silver bullet to treat
traumatic brain injury. What I think it allows us to do is use
less plasma which I think is intrinsically bad for patients with
traumatic brain injury.
In reference to Dr. Cottons question about timing of death.
There was no difference in timing of death in those patients.
We didnt look at ventilator free days because at our
institution once the patients are off the ventilator, they
typically leave the hospital within 48 hours. That really
doesnt allow us to do much of a comparison of ventilator-
free days because even though they are recently off of
the ventilator, they tend to stay within our system to one
of our local rehabilitation centers that can accommodatethem.
And to address Dr. Hausers question, typically the dos-
ing regimen that we use for simple reversal of coagulopathy
for patients with traumatic brain injury is usually a single 1.2
milligram dose. That costs about $1,200.
I dont off-hand remember the upper limit of the range of
dosing in this study, but the mean dose was 60 micrograms
per kilogram.
And in terms of the last question we did not evaluate
fibrinogen levels for the purposes of this study but it would be
an interesting question to go back and look at.
Reversal of Coagulopathy in TBI Patients
Volume 66 Number 1 75