REVALIDATION AND PUBLIC HEALTH PROFESSIONAL APPRAISAL
42
REVALIDATION AND PUBLIC HEALTH PROFESSIONAL APPRAISAL
description
REVALIDATION AND PUBLIC HEALTH PROFESSIONAL APPRAISAL. INTRODUCTION. Purpose of Revalidation/Professional A ppraisal Revalidation/ORSA standards RO/Designated Bodies Appraisal standards/ supporting information Recent RO guidance East Midlands approach. The Purpose of Revalidation. - PowerPoint PPT Presentation
Transcript of REVALIDATION AND PUBLIC HEALTH PROFESSIONAL APPRAISAL

REVALIDATION AND PUBLIC HEALTH
PROFESSIONAL APPRAISAL

INTRODUCTION
• Purpose of Revalidation/Professional Appraisal
• Revalidation/ORSA standards• RO/Designated Bodies• Appraisal standards/ supporting
information• Recent RO guidance• East Midlands approach

The Purpose of Revalidation
• To provide patients, public, employers and other health care professionals with the assurance that licensed doctors (RST) are up to date and fit to practise

The Purpose of Medical/Professional Appraisal• Enable doctors to discuss their practice
and demonstrate they continue to meet GMP/GPH practice and inform RO’s recommendation to GMC
• Enable doctors to improve their quality of work and PDP
• Consider their own needs for PDP• In line with employers priorities

GMC or UKPHR?
• Revalidation is not a FPH process
• It is a process of the GMC and UKPHR for people who want to retain their license to practise

Revalidation Process
• GMC requires local systems of professional appraisal and clinical governance to effectively and fairly distinguish between satisfactory and poor performance
• Responsible officers (RO) appointed for employers (Designated Bodies) to oversee local systems and make recommendations to GMC on whether each doctor should continue to practise

Revalidation Process cont.
• Doctors to be revalidated every 5 years and provide a portfolio of supporting information at annual professional appraisal
• Launch nationally in late 2012

ORSA – Organisational Readiness Self-Assessment
• New standards are identified by ORSA
• ORSA – developed by the DH Revalidation Support Team (RST)
• Standards apply to Designated Bodies• New systems to be set up during
2011/12 and 2012/13 and functioning (with evidence) by March 2013

Who is my RO? - GMC
• Laid down in law – no choice (prescribed connection)
• Usually Medical Director of employer• GMC will write to you but find out
now… • GMC on-line account (GMC
homepage – click on “GMC online for doctors”)

Designated Bodies1. Primary Care Trusts2. Local Health Boards3. National Health Service Trusts4. NHS Foundation Trusts5. Strategic Health Authorities6. Health Boards7. The Department of Health8. The Scottish Ministers9. The Welsh Ministers10. Postgraduate medical deaneries in England and Wales11.Any Scottish training governance body12.The Royal Navy13. The regular army within the meaning of section 374 of the
Armed Forces Act 200614. The Royal Air Force

Designated Bodies15. Special Health Boards16. Special Health Authorities17. The Common Services Agency for the Scottish Health Service18. Bodies which provide independent health care services within the meaning of section 2(5) of the Regulation of Care (Scotland) Act 2001(2) A Government department or any executive agency of a Government department19. The following locum agencies: (a) limited companies with shares owned wholly by the Secretary of State for Health, which are concerned with the contracting of locum doctors(3); and (b) locum agencies in England and Wales which are participants in the NHS Purchasing and Supply Agency’s national framework agreement for the supply of medical locums(4)20. A non-departmental public body21. Any body whose principal office is located in the United Kingdom and whose President or Dean is a member of the Academy of Medical Royal Colleges (e.g. FPH)

Overall Aim of UKPHR To ensure a system of revalidation that is •rigorous •timely •effective •affordable •appropriate to its multidisciplinary and multi-professional membership •equivalent where possible to those in public health being revalidated by other, mainly statutory, regulators, such as the GMC

UKPHR Key Issues• Many of the definitions can be adapted
and used• Aim is for the majority of registrants to be
revalidated through their employer with recommendation to UKPHR
• RO system is likely to be implemented – need to consider the options
• Ambition is to have the system starting end of December
• Need public health specialists to be trained as appraisers

Employed by a Local Authority?• Many PH consultants in England will be employed by local
authorities
• DH has proposed that local authorities in England will be ‘designated bodies’ (results of consultation due in Autumn)
• Arrangements for academics with honorary PCT contracts and CCGs tbc as above

Dual Specialties
• ‘Work in progress’ - being pursued nationally
• You only have one RO, who must make a recommendation to the GMC about the totality of your work
• One session per week of GP (on a 'performers list') trumps a further nine sessions in public health (discuss with your RO)

What if I can’t be bothered?
Failure to engage
Fitness to practise
Will affect
and RO recommendation

Fitness to Practise
Issues that will impact on fitness to practise include:•Patient safety concerns•Failure to engage in revalidation•Undermine confidence in the profession•Conduct (which includes fraud and dishonesty among many other factors)•Performance •Health

ORSA New Appraisal Standards
• Formal Professional Appraisal Policy agreed by relevant organisations
• Appraisal Lead in place• Accredited training for appraisers (and
appraisees)• Appraiser Support Network ( at least
annual)

ORSA New Appraisal Standards
• New eligibility criteria for appraisers• Been through at least 3 appraisal
cycles as appraisee• Received accredited appraiser training
• Academic colleagues covered by organisation holding honorary contract

• Increased quality assurance process• Consultant database - centralised• Central Storage of appraisal papers
meeting information governance standards
• Formal appraiser feedback via appraisee questionnaires and aggregation of appraiser development needs
• 3 yearly appraisal of appraisers• Complaints process
ORSA New Appraisal Standards

• Managed exemption process• Exception audit (for appraisals not
completed within 28 days)• Annual report and Action plan• Aggregation of regional CPD needs via
Summary Appraisal (Form 4) and PDP audit
ORSA New Appraisal Standards

Confidential appraisal
discussion
Post-appraisal sign-off by doctor
and appraiser
The Process of Medical AppraisalAppraisal covers the whole of the doctor’s practice

What’s New about Appraisal for Revalidation - Processes
• Includes whole scope of work• RO will use
• Appraisal outcome• Plus other information (clinical governance)
• Appraiser/Appraisee:• Sign off statements• Engagement• Portfolio/supporting information• Progress since last appraisal• Health/probity• New Summary and PDP


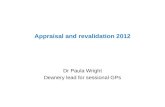
Revalidation: a five year cycle

Levels of supporting information• R
eval
idati
onO
rgan
isat
ion
al a
nd
in
div
idu
al
info
rmat
ion
Supporting information that promotes reflection , may be about the current working environment or areas for future growth and development
GMC guidance is the essential basis for all revalidation decisions
Supporting information defined by the General Medical Council
(Fitness to practise)
Supporting information defined by the employing organisation or specialist body
(Fitness for purpose)
Professional development
Personal
Aspirations
Mandatory requirements may be made contractually by the employing organisation

Good Medical/Public Health Practise – GMC Domains/Attributes
Supporting Information
1. Knowledge, skills and performance 2. Safety and Quality
Attribute 1Maintain your professional developmentAttribute 2Apply knowledge and experience to practiseAttribute 3Keep clear, accurate and legible records
Attribute 1Systems to protect patients and improve careAttribute 2Respond to risks to patient safetyAttribute 3Protect patients from risks posed by your health
3. Communication, partnership and teamwork
4. Maintaining Trust
Attribute 1Communication skillsAttribute 2Work constructively with colleagues and delegationAttribute 3Establish and maintain partnerships with patients
Attribute 1Show respect for patientsAttribute 2Treat patients fairly and without discriminationAttribute 3Act with honesty and integrity

Summary of GMC supporting information requirements
There are six types of supporting information:
1. Continuing professional development2. Quality improvement activity3. Significant events4. Feedback from colleagues5. Feedback from patients (where applicable)6. Review of complaints and compliments

So:-
• Keep up to date• Review and improve your practise• Demonstrate learning/reflection• PH Audit• Get feedback• MSF/360° Appraisal

Public Health Audit
• FPH has developed examples of audit and case review (see Faculty website)
Examples :• DPH annual report• Commissioning reports and impact• Screening annual reports• Health Equality Impact Assessments• Case Review/Reflection• SUI involvement

Feedback
• Colleague• Supervision / training feedback• Formal Complaints• Patient feedback only required for those
who have direct patient contact
• Multi source feedback– At least once in the revalidation cycle– What tool to use? – RO decision

GMC Timeline
July 12 GMC/ROs confirm their doctors
Sept 12 GMC/ROs confirm doctors recommendation dates
Sept – Nov 12 GMC confirms submission dates
Dec 12 GMC issue first notices todoctors and ROs (9 months
notice)

Implementation Years
Year Dates Who0 April 12 – March 13 RO’s, ? Doctors
in leadership1 April 13 – March 14 20% all doctors2 April 14 – March 15 60% all doctors3 April 15 – March 16 100% all
doctors

Year 1 – Selection Process
• Random selectionorLocal criteria
• RO decision

RO Recommendations
• Positive recommendation – continue to license
• Deferral request
• Notification of non-engagement

Deferral Request• Engaged but insufficient evidence, gaps
identified, anticipate able to make informed recommendation once collected
• Engaged, but participating in on-going process (HR, remediation, investigation) anticipate able to make informed recommendation once concluded
• Length of deferral:– 3-6 months– 6-9 months– 9-12 months– More than 12 months

Notification of Non-Engagement
• Not engaged• Does not meet deferral criteria• Doctor had sufficient opportunity and
support• All local processes exhausted

Current East Midlands PH Appraisal System
• In place since 2002/03• Recognised by Faculty of PH as example of
good practise• Includes all PH Consultants – regardless of
background• Includes those on UKPHR but not in
consultant post• Covers PCTs, SHA, Universities• HPA has own system• Co-ordinated annually Sept-Mar

• Systematic /structured/QA approach• Meets all ORSA standards• QA central database• Appraiser training/network• Allocation/choice of appraiser• MDS – submissions/RO link• Evaluation/Feedback
East Midlands Approach/Framework

• National guidance• Local guidance/policies/processes• Portfolio checklist• Structured Line Manager letter• Outline agenda for appraisal interview• Handling difficult appraisal guidance• MDS for central database
East Midlands Framework – Resource Pack

SUMMARY
Revalidation
•GMC/UKPHR process•5 year cycle•Find your RO•RO uses appraisal plus other information

SUMMARY
Appraisal
•Do engage annual enhanced appraisal by approved appraiser•Systematic/QA’d process•Quality supporting information/portfolio is paramount•Demonstrate learning/reflection•Sensible PDP