Retinoblastoma
82
Case presentation Dr Tariq Masood TMO Radiology Department, HMC
Transcript of Retinoblastoma

Case presentation
Dr Tariq Masood TMO Radiology Department, HMC


Case 2 year old male child Mother had noticed some white spot in the
window of his left eye since early childhoodAnd gradual protrusion of the eye


Clinical differentials?

Leucocoria• TUMOR
– Retinoblastoma (most common cause--58%)– Retinal astrocytic hamartoma (3%):– Medulloepithelioma (rare)
• DEVELOPMENTAL– Persistent hyperplastic primary vitreous
• (2nd most common cause--28%)– Coats disease (16%)– Retrolental fibroplasia (3--5%)– Coloboma of choroid / optic disc

• INFECTION– Uveitis– Larval granulomatosis (16%)
• DEGENERATIVE– Posterior cataract
• TRAUMA– Retinopathy of prematurity (5%)– Organized vitreous hemorrhage– Long-standing retinal detachment

• Leukocoria in Normal-sized Eye• CALCIFIED MASS
– Retinoblastoma– Retinal astrocytoma
• NONCALCIFIED MASS– Toxocaral endophthalmitis– Coats disease
• Leukocoria with Microphthalmia• UNILATERAL
– Persistent hyperplastic primary vitreous (PHPV)• BILATERAL
– Retinopathy of prematurity– Bilateral PHPV



Diagnosis?

RETINOBLASTOMA

History/Overview• In 1597 it starts with a man named Pieter Pauw and
his autopsy findings of cancerous tumor originating in
a 3 year-old eye. The results of the autopsy were
later found by Edwin B. Dunphy who suggested
Retinoblastoma.

In 1872 a Brazilian ophthalmologist called Hilário de Gouvêa treated a boy with retinoblastoma. Later in life, the boy had two daughters that also had retinoblastoma. This proposed perhaps the disease was genetic.

In 1986 Dr. Knudson discovered the retinoblastoma gene and then a year later he isolated the gene making it the first ever tumor suppressor to be identified.

In one of Knudson’s cases he found that one family had a genetic past of the disease and found that the gene causing the disorder is located in chromosome 13 that has been mutated.

Retinoblastoma
Rare malignant congenital intraocular tumor arising from primitive photoreceptor cells of retina (included in primitive neuroectodermal tumor group)
AKA neuroepithelioma of the retina

Cause of Retinoblastoma1. Mutations Mutations in the RB1 gene are responsible
for most cases of retinoblastoma. RB1 is a tumor suppressor gene, which means that it normally regulates cell growth and keeps cells from dividing too rapidly or in an uncontrolled way.

2.Chromosomal anomaly– A small percentage of retinoblastomas are
caused by deletions in the region of chromosome 13 that contains the RB1 gene. Because these chromosomal changes involve several genes in addition to RB1, affected children usually also have;microcephaly, ear changes, facial dysmorphism, mental retardation, finger + toe abnormalities, malformation of genitalia.

TYPES A.Non-Heritable form
B.Heritable form

A.Non-Heritable form(60%)RB1 mutations occur only in the eye and cannot be
passed to the next generation.typically only one eye is affected and there is no
family history of the disease.Affected individuals are born with two normal
copies of the RB1 gene. Then, usually in early childhood, both copies of the
RB1 gene in retinal cells acquire mutations or are lost
Mean age at presentation--23 months

B.Heritable form(40%) RB1 mutations occur in all of the body's cells,
including reproductive cells (sperm or eggs). People with germinal retinoblastoma may have a
family history of the disease, and they are at risk of passing on the mutated RB1 gene to the next generation.
Mutations in the RB1 gene appear to be inherited in an autosomal dominant pattern.

Autosomal dominant inheritance suggests that one copy of the altered gene in each cell is sufficient to increase cancer risk.
A person with germinal retinoblastoma may inherit an altered copy of the gene from one parent, or the altered gene may be the result of a new mutation that occurs in an egg or sperm cell or just after fertilization.

For retinoblastoma to develop, a mutation involving the other copy of the RB1 gene must occur in retinal cells during the person's lifetime.
This second mutation usually occurs in childhood, typically leading to the development of retinoblastoma in both eyes.

B.Heritable form
1.Heritable sporadic form2.Familial retinoblastoma

1.Heritable sporadic form (20-25%)-- sporadic germinal mutation (50% chance to occur in subsequent generations)
Mean age at presentation:12 months--bilateral retinoblastomas in 66%

2.Familial retinoblastoma (5-10%)autosomal dominant with abnormality
in chromosome 13 Mean age at presentation: 8 monthsusually 3 to 5 ocular tumors per eyebilateral tumors in 66%Risk of secondary nonocular
malignancy:Osteo, chondro, fibrosarcoma,
malignant fibrous histiocytoma

Trilateral retinoblastoma (rare variant) bilateral retinoblastomas + neuroectodermal pineal tumor (pineoblastoma)
Quadrilateral retinoblastoma trilateral retinoblastoma + 4th focus in suprasellar cistern

Incidence1:15,000 to 30,000 livebirths Most common intraocular neoplasm in childhood
1% of all pediatric malignancies

Mean age at presentation is 18 months
98% in children <5 years of ageM:F = 1:1

Patterns of growth Endophytic Growth occurs inwards into the vitreous ±
anterior chamber Cell clusters may detach and float in the
vitreous (vitreous seeding)

Exophytic Growth occurs outwardsProliferation into subretinal space with non-
rhegmatogeneous retinal detachment + invasion of vascular choroid (hematogenous spread)

Combined Endophytic and Exophytic

LocationPosterolateral wall of globe (most commonly)60% unilateral 40% bilateral + frequently
synchronous (90% bilateral in inherited forms)
Normal ocular size/Enlarged

• Leukocoria - 60% • Strabismus - 20% • Secondary glaucoma
• Anterior segment invasion • Orbital inflammation • Orbital invasion
Presentations of retinoblastoma

PROPTOSIS

Imaging of RBUltrasound
CT scan
MRI

Imaging is crucial for timely management and survival of patients with retinoblastoma.
Cross-sectional imaging are done to exclude ;
Other retrobulbar tumours with globe invasion,
Optic nerve invasion by the retinoblastomaIntracranial metastases

USHeterogeneous hyperechoic solid intraocular
massCystic appearance upon tumor necrosisSecondary retinal detachment in all casesAcoustic shadowing (in 75%)Vitreous hemorrhage frequent


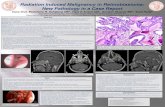
Figure 7e. Retinoblastoma in a 7-year-old girl who complained of blurry vision in her right eye.

Figure 7d. Retinoblastoma in a 7-year-old girl who complained of blurry vision in her right eye.
Chung E M et al. Radiographics 2007;27:1159-1186

CT ScanCT is sensitive to calcification. Clumped or punctate calcification (in 95 per
cent of cases) in the posterior part of the globe extending into the vitreous
Minimal enhancement.

CT Scan• Calcification in an intra-ocular mass in a child
(3 yrs, retinoblastoma until proven otherwise. Absence of calcification means this diagnosis is unlikely, since it is rare in other causes of leukocoria.
• Retinoblastoma is the most common cause of orbital calcifications!

CT ScanSolid smoothly marginated lobulated
retrolental hyperdense mass in endophytic type
Exophytic type grows subretinally causing retinal detachment
Partial punctate / nodular calcification

Dense vitreous (common)Extraocular extension (in 25%): optic nerve
enlargement, abnormal soft tissue in orbit, intracranial extension
± Macrophthalmia


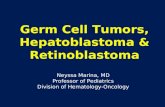
CT diagnosis of retinoblastoma
Calcification



Figure 8a. Trilateral retinoblastoma in a child of unknown age.

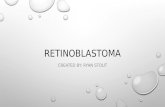
MRIMRI is the modality of choice for pre-
treatment staging on retinoblastomaT1 : Intermediate signal intensity,
hyperintense c.f. vitreous T2 : Hypointense c.f. vitreous
subretinal exudate usually hyperintense on T1WI + T2WI (proteinaceous fluid)




T1 C+ (Gd)The mass usually enhances relatively
homogeneously when smallLarger tumours often have areas of necrosis,
rendering it heterogeneous



Linear enhancement of the choroid beyond the margins of the tumour should raise the possibility of choroidal involvement, although inflammation may lead to similar appearance

Enhancement of the anterior chamber need not represent tumour involvement, with hyperaemia, uveitis and iris neovascularisation all leading to asymmetric enhancement


Careful assessment of the optic disc and optic nerve should be carried out to assess for involvement


Extra-ocular extension through the sclera will be visible as interruption of the otherwise hypointense non-enhancing sclera by enhancing tumour

PROGNOSISSpontaneous regression in 1%;

Poor prognostic signs
Contrast enhancement
Optic nerve involvement
Choroidal invasionLarge tumor
Anterior locationsPoor cellular
differentiationOlder children

COMPLICATIONS (1) Metastases to: meninges (via
subarachnoid space), bone marrow, lung, liver, lymph nodes
(2) Radiation-induced sarcomas develop in 15-20%

MortalityChoroidal invasion:
65% if significant, 24% if slightOptic nerve invasion:
<10% if not invaded15% if through lamina cribrosa44% if significantly posterior to lamina
cribrosaMargin of resection not free of tumor: >65%

Differential diagnosisRetinal Astrocytic hamartomaRetrolental fibroplasiaCoat’s diseasePeristent hypertrophic primary vitreousToxocaral infestationNorrie’s disease

DDxRetinal astrocytic hamartoma.May occur in association with TS or NF or an
isolated abnormality.May be bilateral multiple small retinal masses. calcification may occur in the older child

• Coats disease• Coats’ disease is a primary congenital, non-familial
idiopathic vascular anomaly of the retina. It is characterised by telangiectatic, leaky retinal vessels thatlead to progressive retinal exudates. It usually occursin young males (70%) with an incidence peak at age 6–8years. It is mostly unilateral (90%). Patients present withleukocoria, strabismus or painfulglaucoma..

Calcification is rare,allowing differentiation from RB.
CT shows homogeneous increased density within the vitreous chamber,retinal detachment and lack of enhancement after contrast administration.
The MRI findings are retinal detachmentwithout intraocular mass and high signal subretinal effusion on both T1W and T2W MRI

Retrolental fibroplasia Retinopathy of prematurity causes retro-
lental fibroplasia with the development of retrolental membranes.
Present usually with bilateral leucocorea at the age of 7-10weeks with a history of prematurity and oxygen therapy.
No Calcification.Microphthalmia.

Persistent hyperplastic primary vitreous is caused by the failure of the embryonic
hyaloid vascular system to regress normally and extensive proliferation of embryonic connective tissue It is characterised by a leukocoria in a microphthalmic eye.
Small irregular lens with shallow anterior chamber.
If bilateral,PHPV may be part of the diagnosis of Norrie’s disease.

On CTNo calcification.Increased attenuation of vitreous with
enhancement of abnormal intravitreal tissue.Triangular retrolental density with its apex
on the posterior lens and base on the posterior globe.

Toxocara canis infectionSclerosing endophthalmitis is a granulomatous
chorioretinitis uveitis that develops secondary to a Toxocara canis infestation, in more than 5 yrs age
Present with leucocorea----often bilateral.It differs from RB by its central position, the fact
that it is hyperintense to vitreous on T2 weighted images, the patient age and a positive serologic enzyme-linked immunosorbent assay (ELISA).

CT demonstrate a hyperdense vitreous cavity,sometimes with retinal detachment.No enhancement is seen.

Norrie diseaseRare X-linked recessive syndrome consisting
of retinal malformation, deafness and mental retardation. Female carriers are completely healthy. The ocular changes in male patients include retinal detachments and vitreo-retinal haemorrhage

Treatment• Depends on tumour size and the stage of
disease and involves one or more modalities:• Conservative external-beam radiation therapy
cryotherapylaser photocoagulationradioactive plaque therapythermochemotherapytumour reduction chemotherapy
• Surgical enucleationen bloc resection

TreatmentAdvantages Disadvantages
Photocoagulation (Laser Therapy) The laser beam focuses on the cancerous tumor, cuts off blood supply to the tumor and shrinks it.
Depending on the size of the tumor, chemotherapy may be needed for larger tumors that cannot be shrunk by just laser.
Cryotherapy (Freezing Treatment) The tumor is frozen and thawed a several times by a cold gas and it deflates the tumor with no signs of a tumor at all.
The tumor will leave a pigmented scar and the eye lid will swell for a couple of days.
Chemotherapy After the extensive cycles of chemo, the cancer cells are reduced, therefore, shrinking of the tumor.
There are several cycles, and there is a port necessary to draw blood, and insert the drugs.
Enucleation This is removal of the eyeball and the tumor is extracted when no other option is possible due to the size of the tumor.
The whole eyeball is removed and it causes permanent eye damage because there is no way of an eye transplant.

WE HATE RETINOBLASTOMA

THANKS