
Resuscitation and thoracic trauma
45
RESUSCITATION & THORACIC TRAUMA PRESENTERS: DR UMAR & DR MARYAM SUPERVISOR: DR FAIZUL
-
Upload
hidayat-shariff -
Category
Health & Medicine
-
view
20 -
download
3
Transcript of Resuscitation and thoracic trauma
RESUSCITATION & THORACIC
TRAUMA
PRESENTERS: DR UMAR & DR MARYAMSUPERVISOR: DR FAIZUL
OUTLINE
• INTRODUCTION
•LIFE THREATENING THORACIC INJURY
•COMMON CONDITION OF THORACIC INJURY
• TAKE HOME MESSAGES
INTRODUCTION• Trauma causes 100,000 deaths and more than 9 million disability
injury annually in worldwide (6th leading cause of death).
• Chest injuries are responsible for 20-25% of all trauma death.
•The World Health Ranking 2011 has ranked Malaysia at number 20 with the most deaths caused by road accidents.
•An average of 18 people were killed on Malaysian roads daily.
* Malaysian Institute of Road Safety (MIROS)
CLASIFICATION
•Anatomy•Lungs, pleura and ribs•Cardiac injury•Trachea , oesophagus & major vessels•Diaphragm
•Mechanism of injury•Blunt•Penetrating•Shearing / acceleration-decelaration injury
•Cause / Aetiology•MVA / trauma•Fall from height•Gunshot / sharp or blunt object

LIF
E T
HR
EA
TEN
ING
C
ON
DIT
ION
TENSION PNEUMOTHORAX
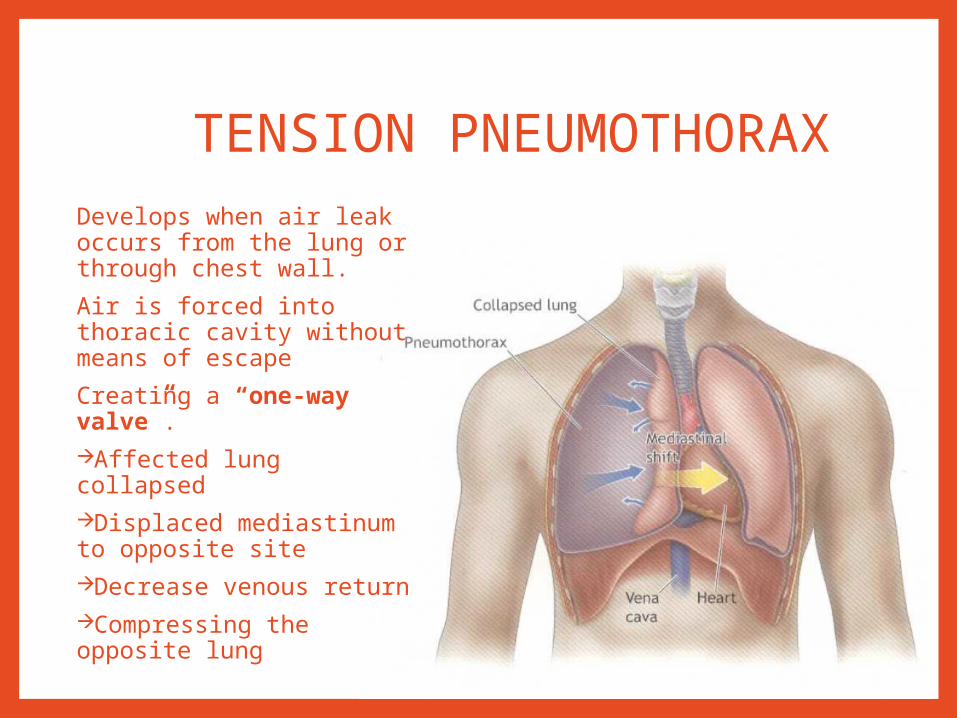
TENSION PNEUMOTHORAXDevelops when air leak occurs from the lung or through chest wall.
Air is forced into thoracic cavity without means of escape
Creating a “one-way valve”.Affected lung collapsedDisplaced mediastinum to opposite siteDecrease venous returnCompressing the opposite lung
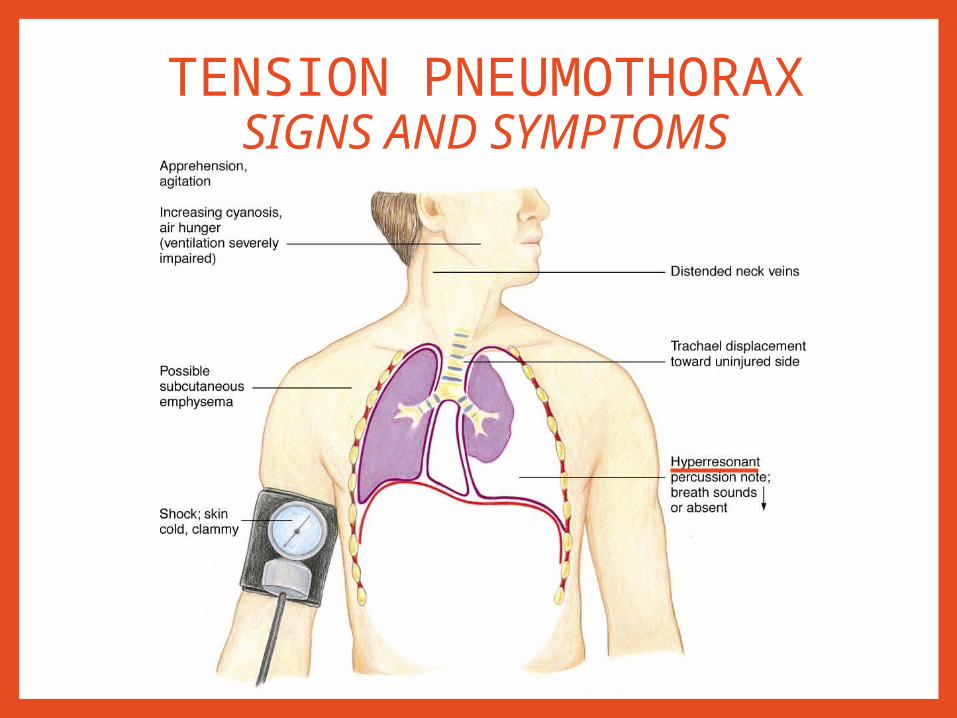
TENSION PNEUMOTHORAXSIGNS AND SYMPTOMS
TENSION PNEUMOTHORAX
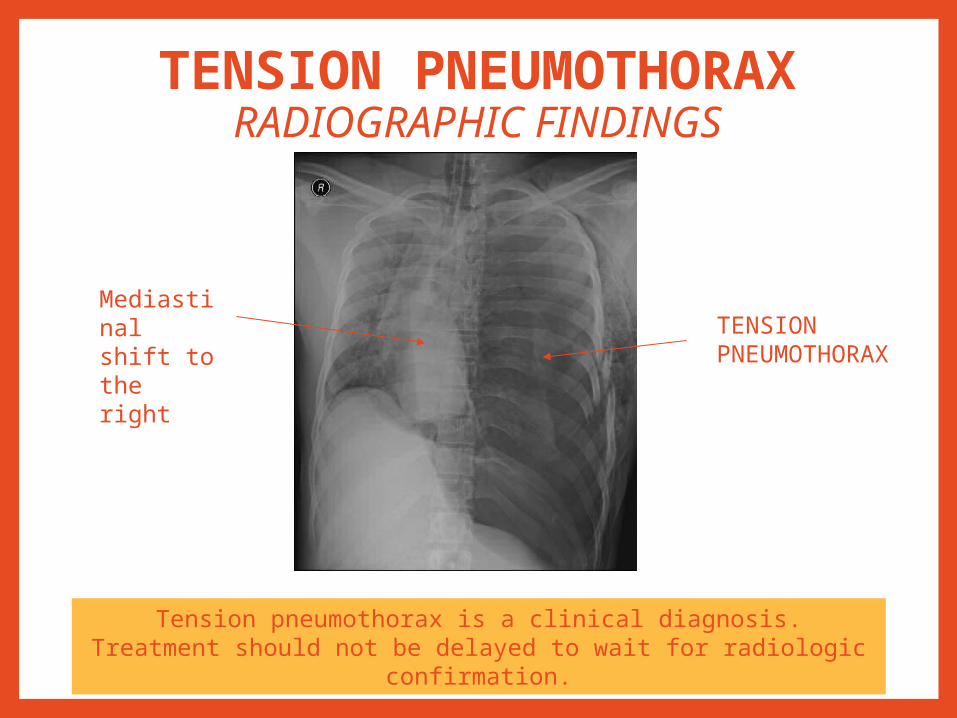
RADIOGRAPHIC FINDINGS
Mediastinal shift to the right
TENSIONPNEUMOTHORAX
Tension pneumothorax is a clinical diagnosis.Treatment should not be delayed to wait for radiologic confirmation.
TENSION PNEUMOTHORAX
Management1. Initial Management: needle thoracostomy
- convert the injury to simple pneumothorax.
2. Definitive management: chest tube insertion
3. Supportive management:
- Analgesia
- Ventilatory support
- CXR monitoring
- Chest phyisotherapy
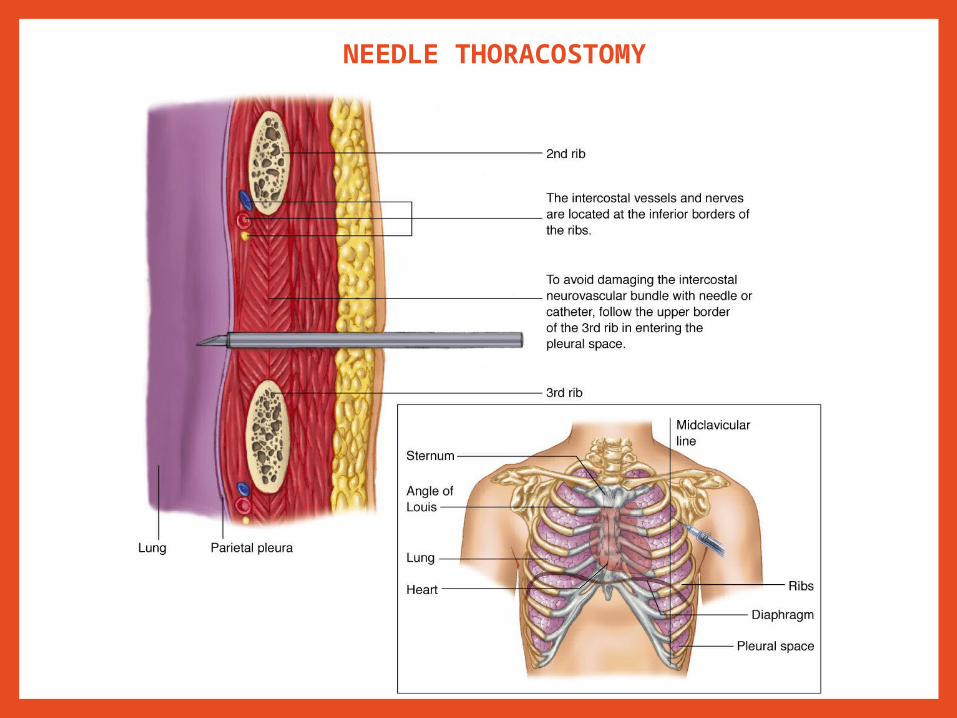
NEEDLE THORACOSTOMY
OPEN PNEUMOTHORAX

OPEN PNEUMOTHORAX:Pathophysiology
•Known as “sucking chest wound.”
•Air allowed to enter pleural space from the outside.
•Ineffective ventilation because air goes in and out from the chest wound, rather than from trachea.
•Leading to hypoxia and hypercarbia.
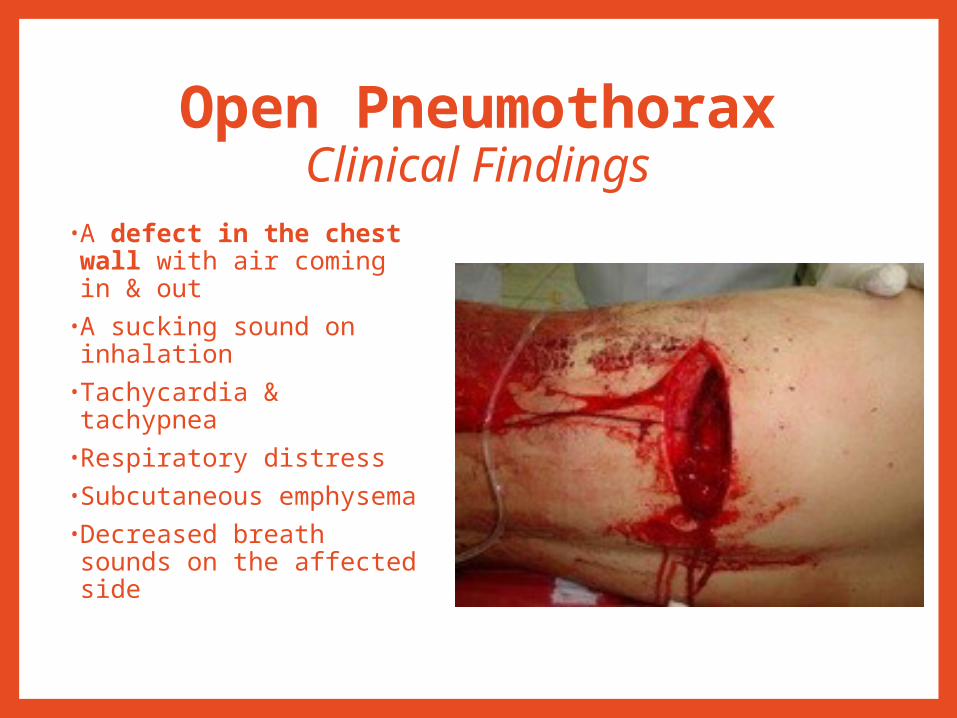
Open PneumothoraxClinical Findings
•A defect in the chest wall with air coming in & out
•A sucking sound on inhalation
•Tachycardia & tachypnea•Respiratory distress•Subcutaneous emphysema
•Decreased breath sounds on the affected side
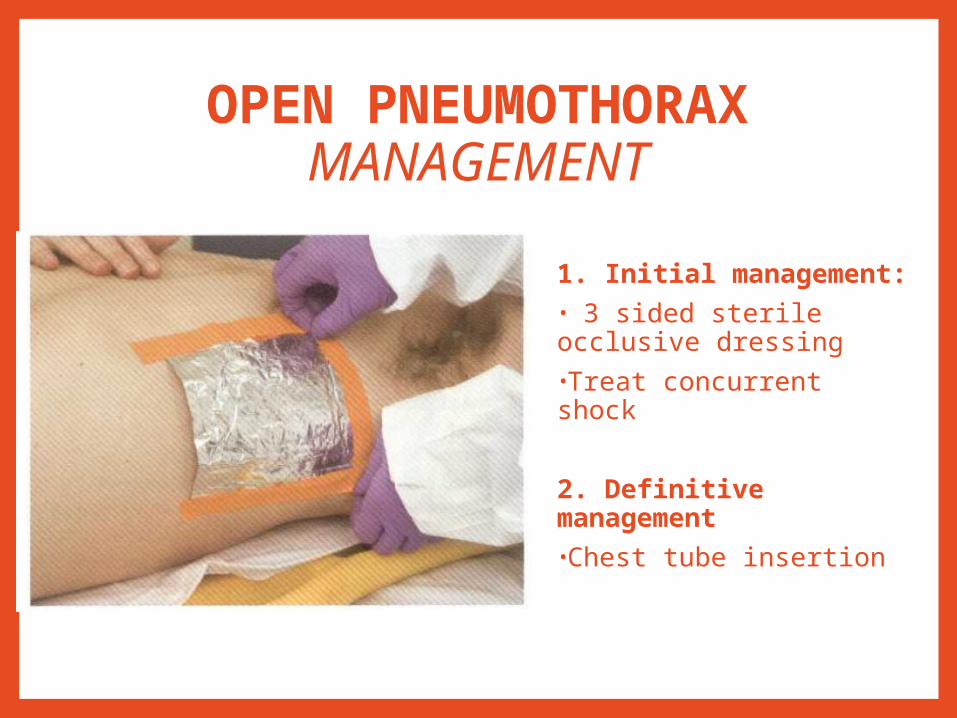
OPEN PNEUMOTHORAXMANAGEMENT
1. Initial management:• 3 sided sterile occlusive dressing•Treat concurrent shock
2. Definitive management•Chest tube insertion
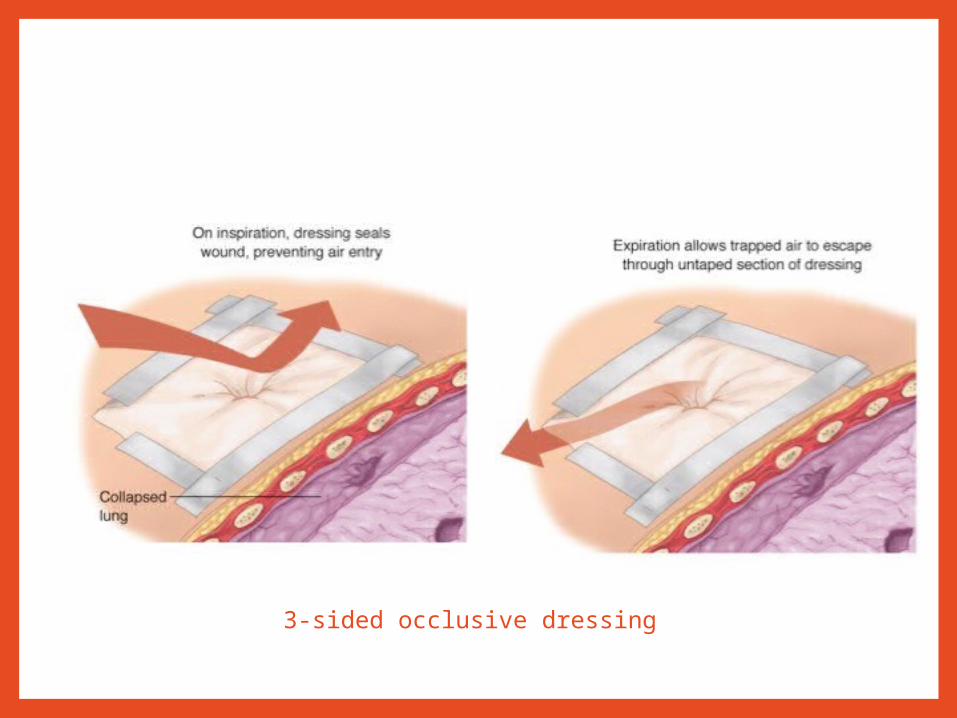
3-sided occlusive dressing
FLAIL CHEST & PULMONARY
CONTUSION
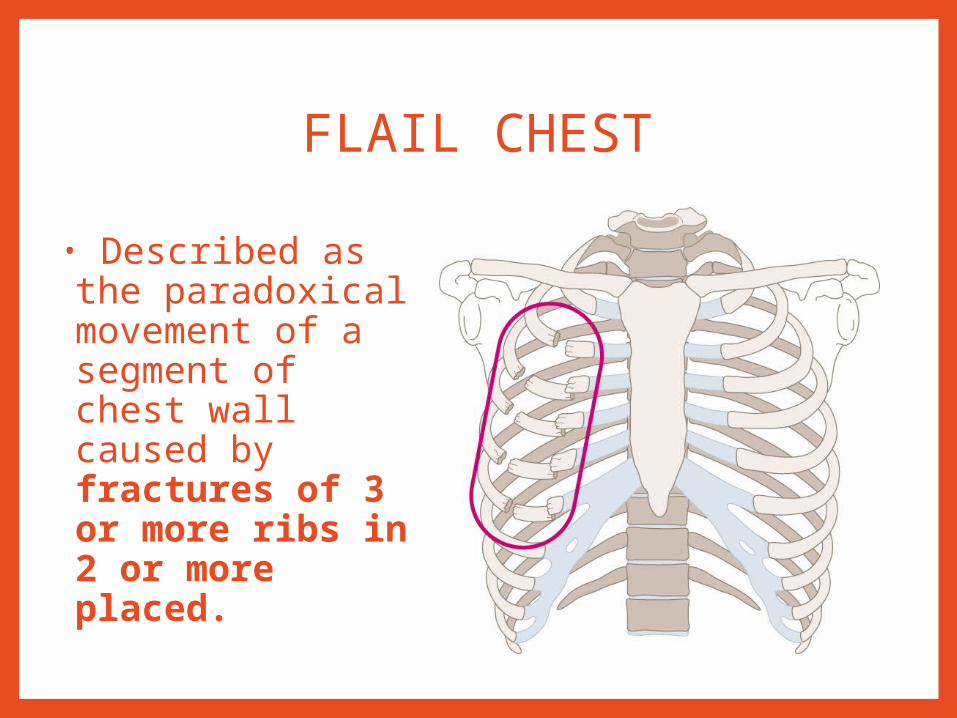
FLAIL CHEST
• Described as the paradoxical movement of a segment of chest wall caused by fractures of 3 or more ribs in 2 or more placed.

FLAIL CHEST
Severe hypoxia resulting from: •The underlying lung injury disturbance of ventilation & perfusion •Restricted chest wall movement associated with pain impaired ventilation

FLAIL CHESTClinical findings
INSPECTION-Chest wall contusion-Paradoxical chest wall movement-Respiratory distress
Palpation-Crepitation of rib
FLAIL CHEST
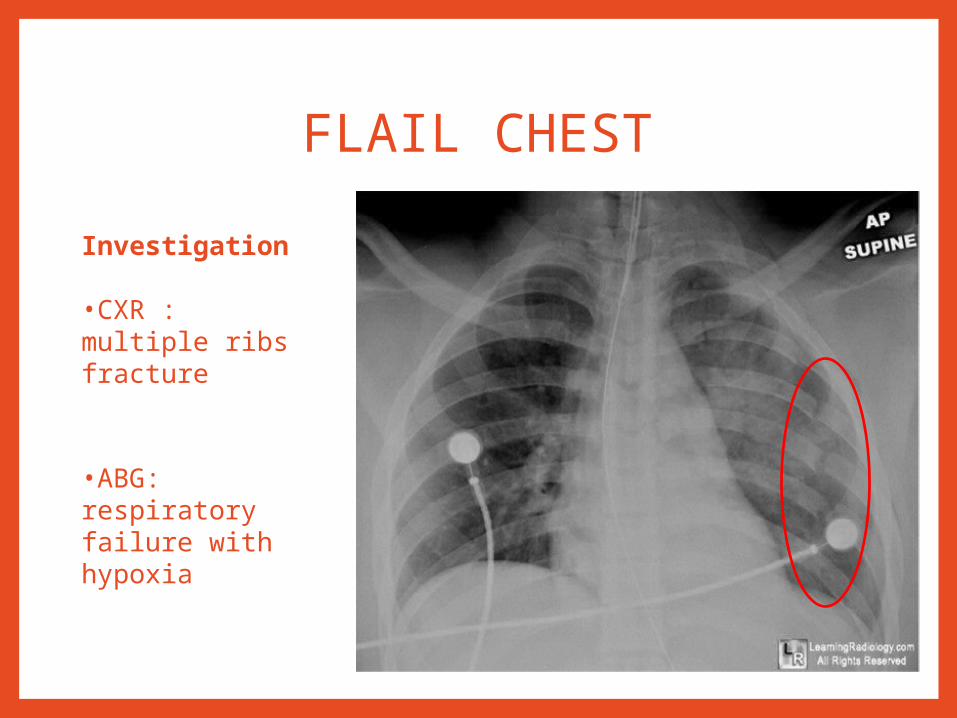
Investigation
•CXR : multiple ribs fracture
•ABG: respiratory failure with hypoxia

FLAIL CHESTManagement
1. Initial management:- adequate ventilationfluid resuscitation
In absence of systemic hypotension, fluid resuscitation should be carefully controlled to prevent overhydration.
FLAIL CHESTManagement
2. Definitive management
Positive-pressure ventilation may be needed.•Reverses the mechanism of paradoxical chest wall movement•Restores the tidal volume
Adequate analgesic•Reduces the pain of chest wall movement
Assess for the development of a pneumothorax•May need chest tube insertion

MASSIVE HEMOTHORAX
MASSIVE HEMOTHORAX
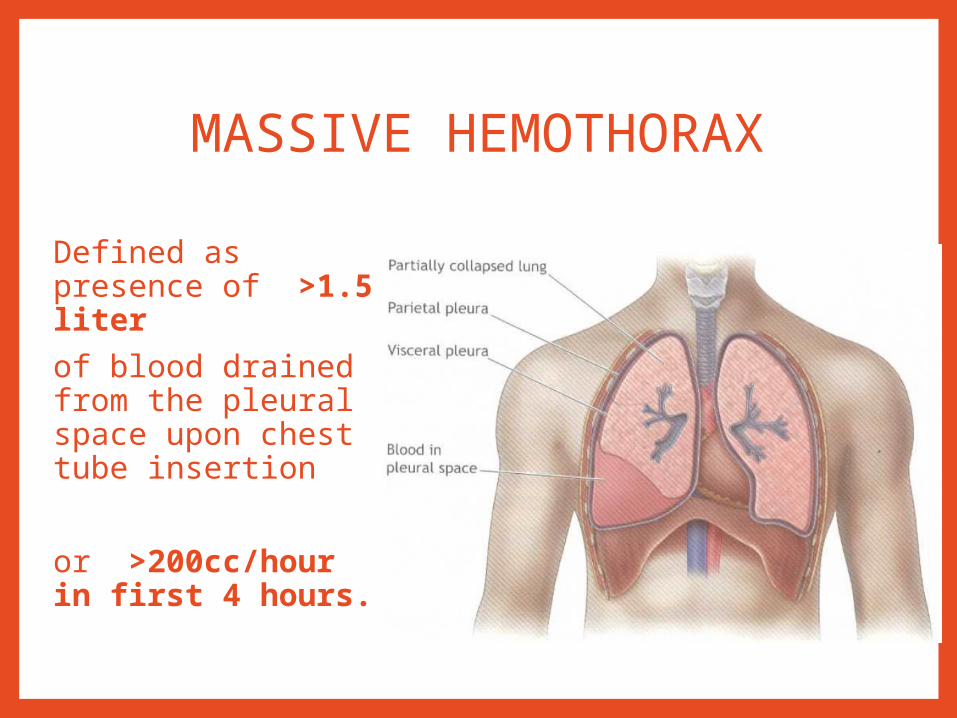
Defined as presence of >1.5 liter of blood drained from the pleural space upon chest tube insertion
or >200cc/hour in first 4 hours.
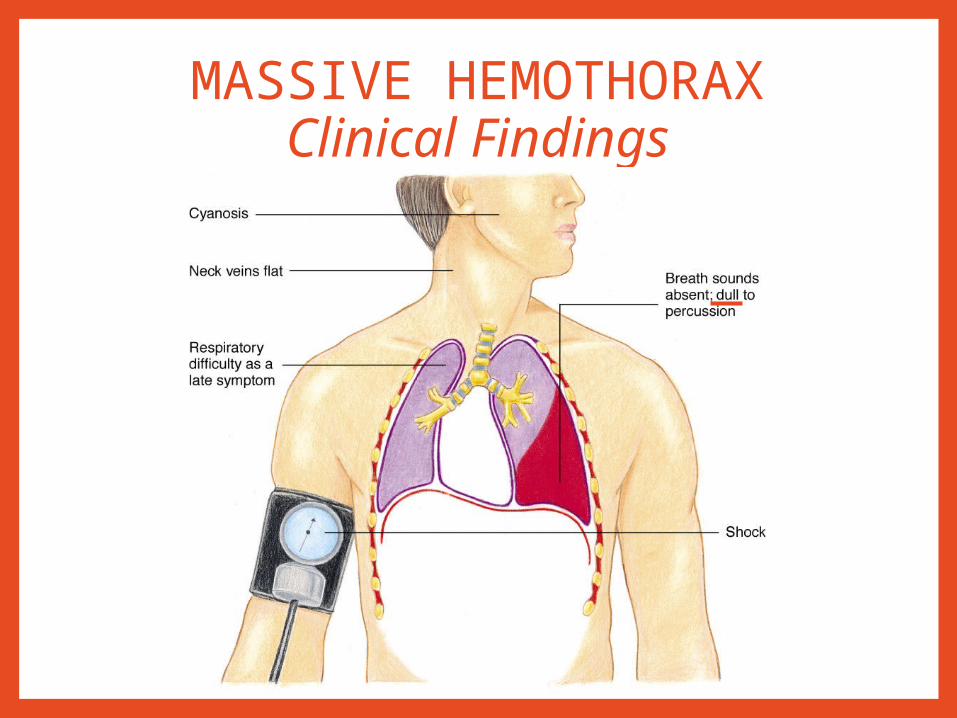
MASSIVE HEMOTHORAXClinical Findings
MASSIVE HEMOTHORAXManagement
Large caliber IV linesCrystalloid infusionBlood transfusion
Chest tube insertionConsider for thoracotomy

MASSIVE HEMOTHORAX
Chest tube insertion
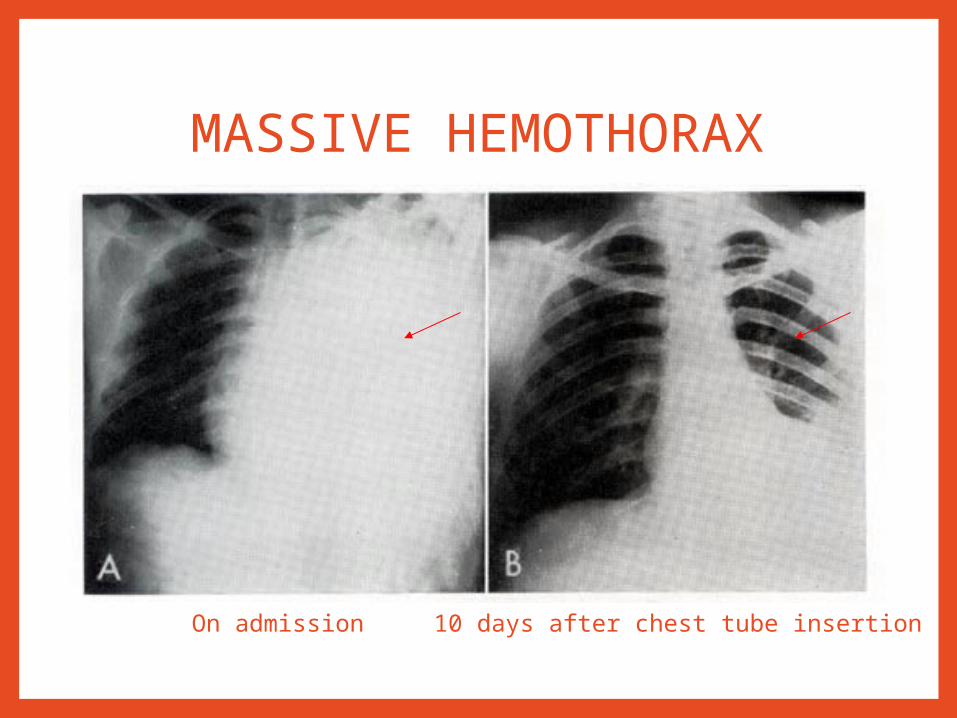
MASSIVE HEMOTHORAX
10 days after chest tube insertionOn admission

CARDIAC TAMPONADE
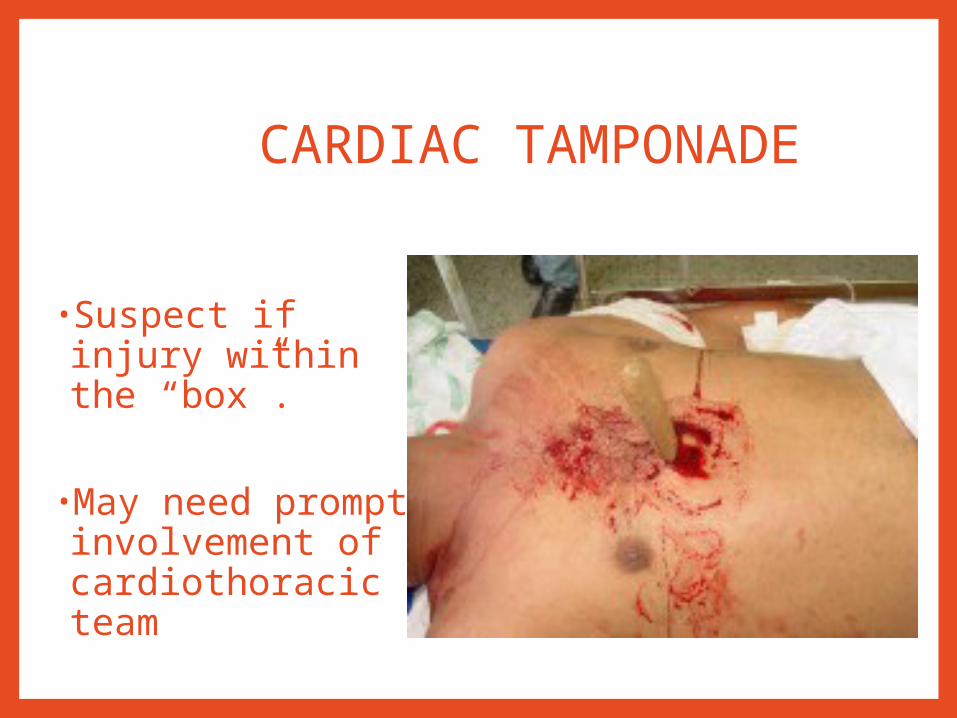
CARDIAC TAMPONADE
•Suspect if injury within the “box”.
•May need prompt involvement of cardiothoracic team
CARDIAC TAMPONADE
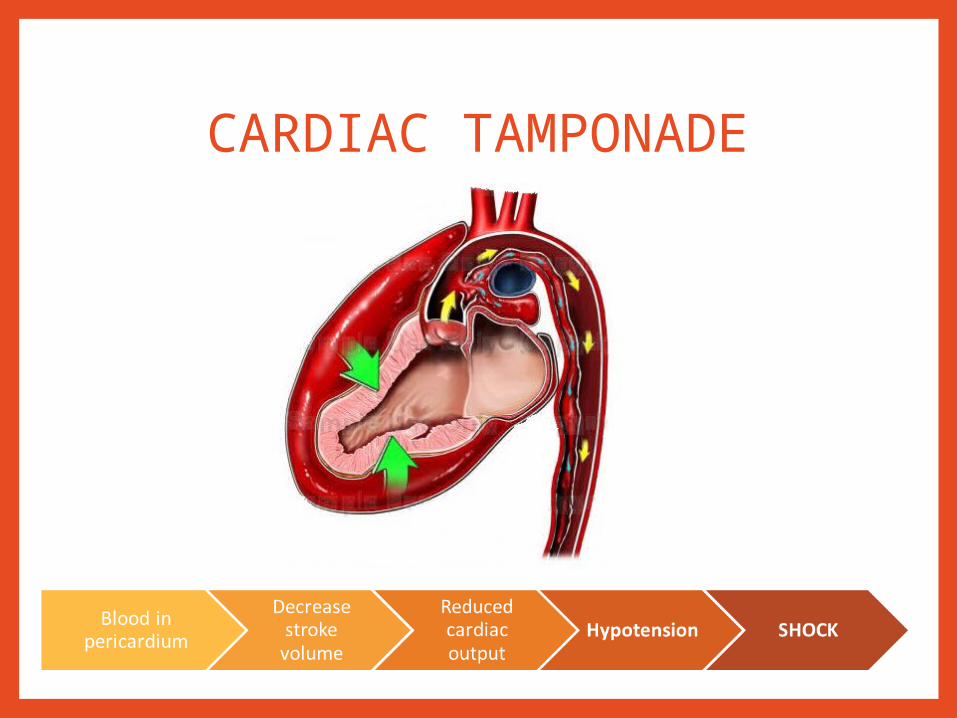
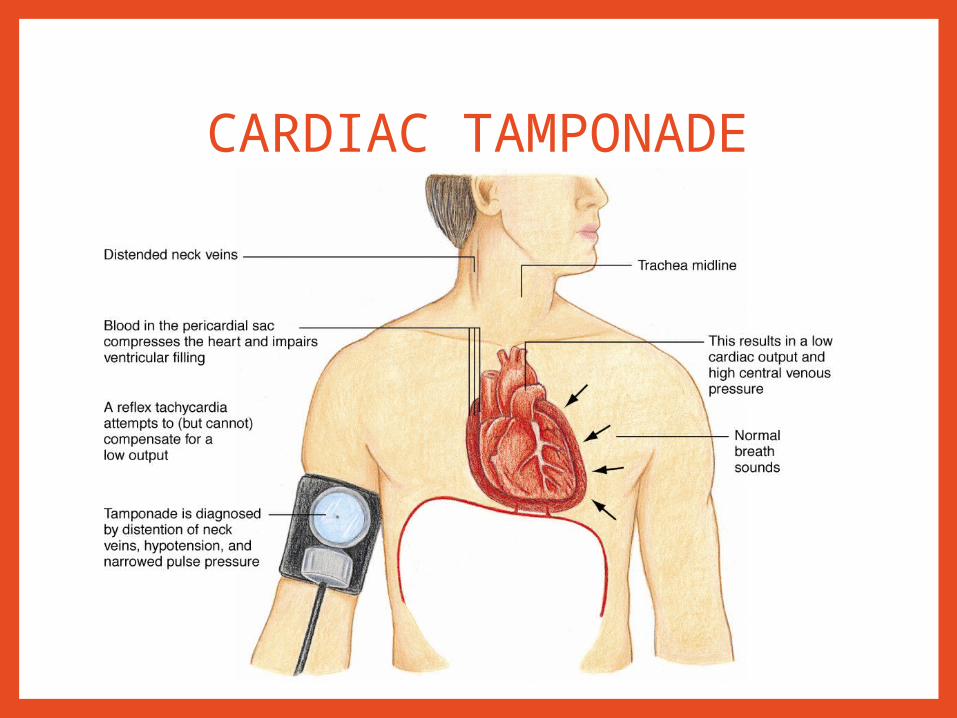
Pathophysiology •A blunt or penetrating trauma may cause tears in the myocardial walls, allowing blood to leak from the heart.
If 150 to 200 mL of blood enters the pericardial space acutely, pericardial tamponade can develops
CARDIAC TAMPONADE
CARDIAC TAMPONADE
CARDIAC TAMPONADE
Cardiac Tamponade Management•Airway and ventilation •Circulation—IV fluid challenge•Pericardiocentesis•Prompt involvement of cardiothoracic team.•Do not take out the penetrating object

CARDIAC TAMPONADE
Pericardocentesis
OTHER CHEST INJURIES
1. RIB FRACTURE2. SIMPLE PNEUMOTHORAX3. HEMOTHORAX4. PULMONARY CONTUSION5. TRACHEOBRONCHIAL TREE INJURIES6. CARDIAC CONTUSION7. TRAUMATIC MAJOR VESSEL DISRUPTION8. DIAPHRAGMATIC INJURIES
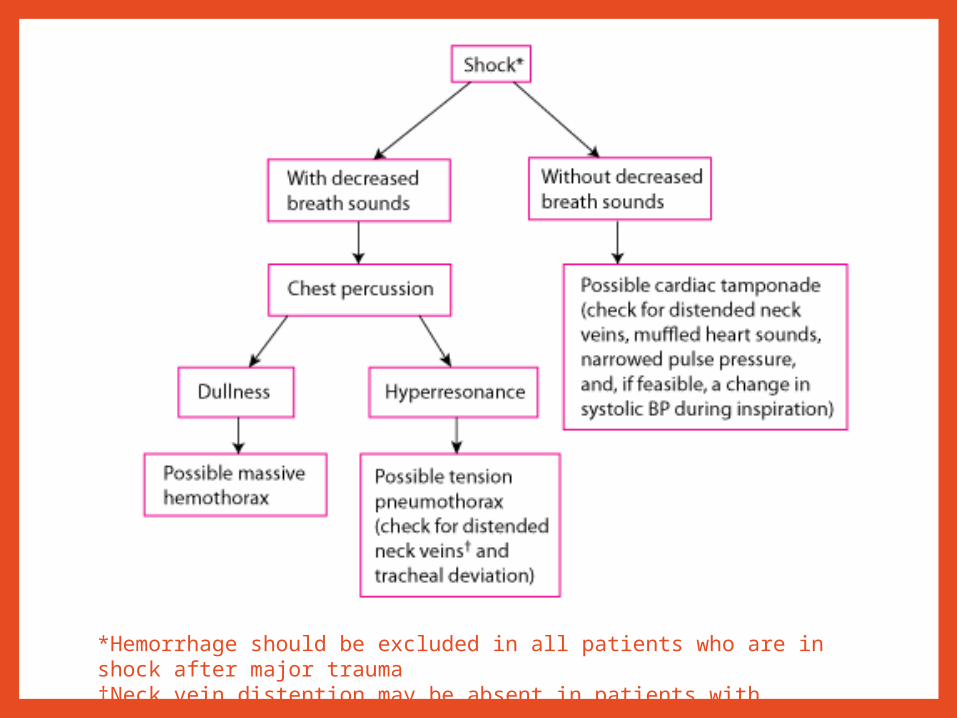
*Hemorrhage should be excluded in all patients who are in shock after major trauma†Neck vein distention may be absent in patients with hypovolemic shock.

GENERAL MANAGEMENT•Primary & secondary survey•Serial clinical assessment & SPO2 monitoring•Adequate analgesia (pain control CPG)•Oxygen therapy tailored to oxygenation status•Chest tube insertion•Intensive & vigorous chest physiotherapy, deep breathing exercise & incentive spirometry
•Mucolytic & nebulizer•Early referral to appropriate team (i.e. anaest, CTC)•± Assisted ventilation or intubation•± Thoracotomy / thorachoscopy and proceed
TAKE HOME MESSAGES1. Life threatening condition in thoracic injury are
• Tension pneumothorax
• Open pneumothorax
• Massive hemothorax
• Flail chest
• Cardiac temponade.
2. Tension pneumothorax required emergent needle thoracotomy without waiting for CXR if highly suspected clinically
3. Do not remove the object causing the penetrating thoracic injury
4. Open pneumothorax is managed with flutter-valve dressing or three sided dressing
TAKE HOME MESSAGES
5. Flail chest is defined as segmental fractures in 2 or more places of 3 or more consecutive ribs.
6. Massive hemothorax happen when
• more than 1.5 liters blood drained upon chest tube insertion
• Or more than 200cc/hour in 4 hours
7. All symptomatic traumatic pneumo/hemothorax require chest tube insertion
8. Cardiac tamponade is recognized by presence of Beck’s Triad which are
• Muffled heart sound
• Hypotension
• Distended neck veins
TAKE HOME MESSAGES
9. Key management in thoracic injury include
• Identifying the life threatening condition
• Resuscitation and oxygen therapy
• Chest tube insertion
• Adequate pain control and aggressive chest physiotherapy
• Ventilation and early associate team referral
REFERENCES
• ATLS for Doctors, 8th Edition• Bailey & Love Short Practice of Surgery, 25th
Editions• Emergency Medicine Clinics of North America
- Volume 30, Issue 2 (May 2012)• SRB’s Manual of Surgery 4th edition


















