Result of Endoureterotomy in the Management of Primary Obstructive Megaureter in the First Year of...
5
Result of Endoureterotomy in the Management of Primary Obstructive Megaureter in the First Year of Life: Preliminary Report Mehdi Shirazi, MD, Mohammad Natami, MD, Pooya Hekmati, MD, and Mohamadreza Farsiani, MD Abstract Purpose: The present study aimed to investigate the efficacy of endoureterotomy in patients who were less than 1-year-old with primary obstructive megaureter (POMU). Patients and Methods: Three of 10 patients with POMU aged between 2 and 12 months for whom conservative management was not applicable had recurrent urinary tract infection (UTI) and urosepsis, while the rest had decreased renal function. After obtaining the clinical history and performing physical examinations and imaging studies (ultrasonography, voiding cystourethrography (VCUG), radionuclide renal scan), the patients under- went endoureterotomy using a neonatal ureteroscope (4.5F) and Bugbee electrode with pure cutting current at the 6 o’clock position. A Double-J stent was inserted and removed 1 week later. This was followed by serial physical examination, renal function test, urine analysis, urine culture, and imaging studies in the 1st month and every 3 months after Double-J stent removal. Results: Hydroureteronephrosis was significantly decreased in nine patients. Postoperative VCUG revealed no sign of iatrogenic vesicoureteral reflux. In addition, a follow-up renal scan showed remarkable improvement in the renal function in the patients who had decreased renal function, except for one patient in whom uncontrolled urosepsis developed in the follow-up; the patient underwent cutaneous ureterostomy. No UTI was detected in the group who presented with recurrent UTI and urosepsis. Conclusion: According to the results of our study, endoureterotomy may be an alternative in management of POMU. Of course, further studies with longer follow-up periods are needed to confirm the applicability of this method in patients younger than 1 year. Introduction U reteral diameter more than 5 mm in association with a group of anomalies is labeled as megaureter. 1,2 Several hypotheses have been made concerning the pathophysiology of primary obstructive megaureter (POMU), such as alter- ation in the muscularis layers of the distal part of the ureter by absent longitudinal muscle fiber and hypertrophied circular muscle or increase in the connective tissue deposition. 3,4 Males are more commonly involved, with dominancy at the left side. 5 Patients with POMU may present with variable symptoms, such as urinary tract infection (UTI), urosepsis, failure to thrive, and abdominal mass. Multiple management strategies are available for children less than 1 year old, and the therapeutic modality is quite difficult to select. In pa- tients with mild obstruction, conservative management by symptoms monitoring, periodic radiologic imaging study, and prophylactic antibiotic therapy is an acceptable modal- ity. 6–9 On the other hand, progressive renal damage is an indication for operative management, regardless of the pa- tient’s age. 10–12 The ultimate goal of surgical intervention is preserving renal function and its development by relieving the obstruction of the collecting system without creation of iatrogenic reflux. To date, ureteroneocystostomy is an ac- ceptable open surgical intervention for correction of ob- structing megaureter in symptomatic patients. It has its own complications, however, especially when a dilated ureter is reimplanted into the small bladder, which may interfere with the functional development of the lower urinary tract because the trigone will be manipulated. It may create iat- rogenic vesicoureteral reflux (VUR), as well. 12,13 Re- implantation of an obstructed megaureter should be avoided in the first year of life. because it has a higher failure rate as well as a greater risk of morbidity and reoperation. 10,14 Some researchers have recommended cutaneous ureter- ostomy 15,16 or temporary Double-J stent insertion 17 to pre- serve the function of the kidney. These procedures have Department of Urology, Shiraz Medical School, Shiraz, Fars, Iran. JOURNAL OF ENDOUROLOGY Volume 28, Number 1, January 2014 ª Mary Ann Liebert, Inc. Pp. 79–83 DOI: 10.1089/end.2013.0098 79
-
Upload
mohamadreza -
Category
Documents
-
view
213 -
download
0
Transcript of Result of Endoureterotomy in the Management of Primary Obstructive Megaureter in the First Year of...

Result of Endoureterotomy in the Management of PrimaryObstructive Megaureter in the First Year of Life:
Preliminary Report
Mehdi Shirazi, MD, Mohammad Natami, MD, Pooya Hekmati, MD, and Mohamadreza Farsiani, MD
Abstract
Purpose: The present study aimed to investigate the efficacy of endoureterotomy in patients who were less than1-year-old with primary obstructive megaureter (POMU).Patients and Methods: Three of 10 patients with POMU aged between 2 and 12 months for whom conservativemanagement was not applicable had recurrent urinary tract infection (UTI) and urosepsis, while the rest haddecreased renal function. After obtaining the clinical history and performing physical examinations and imagingstudies (ultrasonography, voiding cystourethrography (VCUG), radionuclide renal scan), the patients under-went endoureterotomy using a neonatal ureteroscope (4.5F) and Bugbee electrode with pure cutting current atthe 6 o’clock position. A Double-J stent was inserted and removed 1 week later. This was followed by serialphysical examination, renal function test, urine analysis, urine culture, and imaging studies in the 1st month andevery 3 months after Double-J stent removal.Results: Hydroureteronephrosis was significantly decreased in nine patients. Postoperative VCUG revealed nosign of iatrogenic vesicoureteral reflux. In addition, a follow-up renal scan showed remarkable improvement inthe renal function in the patients who had decreased renal function, except for one patient in whom uncontrolledurosepsis developed in the follow-up; the patient underwent cutaneous ureterostomy. No UTI was detected inthe group who presented with recurrent UTI and urosepsis.Conclusion: According to the results of our study, endoureterotomy may be an alternative in management ofPOMU. Of course, further studies with longer follow-up periods are needed to confirm the applicability of thismethod in patients younger than 1 year.
Introduction
Ureteral diameter more than 5 mm in association witha group of anomalies is labeled as megaureter.1,2 Several
hypotheses have been made concerning the pathophysiologyof primary obstructive megaureter (POMU), such as alter-ation in the muscularis layers of the distal part of the ureter byabsent longitudinal muscle fiber and hypertrophied circularmuscle or increase in the connective tissue deposition.3,4
Males are more commonly involved, with dominancy at theleft side.5 Patients with POMU may present with variablesymptoms, such as urinary tract infection (UTI), urosepsis,failure to thrive, and abdominal mass. Multiple managementstrategies are available for children less than 1 year old, andthe therapeutic modality is quite difficult to select. In pa-tients with mild obstruction, conservative management bysymptoms monitoring, periodic radiologic imaging study,and prophylactic antibiotic therapy is an acceptable modal-ity.6–9 On the other hand, progressive renal damage is an
indication for operative management, regardless of the pa-tient’s age.10–12
The ultimate goal of surgical intervention is preservingrenal function and its development by relieving theobstruction of the collecting system without creation ofiatrogenic reflux. To date, ureteroneocystostomy is an ac-ceptable open surgical intervention for correction of ob-structing megaureter in symptomatic patients. It has its owncomplications, however, especially when a dilated ureter isreimplanted into the small bladder, which may interferewith the functional development of the lower urinary tractbecause the trigone will be manipulated. It may create iat-rogenic vesicoureteral reflux (VUR), as well.12,13 Re-implantation of an obstructed megaureter should be avoidedin the first year of life. because it has a higher failure rateas well as a greater risk of morbidity and reoperation.10,14
Some researchers have recommended cutaneous ureter-ostomy15,16 or temporary Double-J stent insertion17 to pre-serve the function of the kidney. These procedures have
Department of Urology, Shiraz Medical School, Shiraz, Fars, Iran.
JOURNAL OF ENDOUROLOGYVolume 28, Number 1, January 2014ª Mary Ann Liebert, Inc.Pp. 79–83DOI: 10.1089/end.2013.0098
79

several complications, however, including encrustation, stentmigration, UTI, stone formation, and stomal stenosis.18–20
In this study, we aim to report our preliminary experienceof endoureterotomy for treatment of primary obstructedmegaureter in children less than 1 year old.
Patients and Methods
The present study was performed between January 2010and January 2011, and the patients were followed by serialphysical examination, renal function test, urine analysis, urineculture, and imaging studies in the 1st month and every3 months after Double-J stent removal. The study was con-ducted in 10 patients younger than 1 year who were selectedfrom different centers. The patients were followed up indifferent manners regarding the timing of renal isotope scanand ultrasonography in the conservative management pe-riod. All the enrolled patients with impaired renal functionhad below 40% differential functions on the last preopera-tive isotope scan. All patients underwent renal ultrasonog-raphy, revealing a ureteral diameter of more than 15 mm.Moreover, voiding cystourethrography (VCUG) and diureticrenography were performed for all the patients to selectthose without reflux and obtain their baseline renal function.After confirming the diagnosis, urine analysis and urineculture were obtained and then prophylactic antibioticswere started.
Our inclusion criteria for surgical intervention were im-paired differential function on the last preoperative assess-ment (differential function less than 40%), distal ureteraldiameter more than 15 mm at ultrasonography, and recurrentUTI after a period of antibiotic prophylaxis or urosepsis.Based on the inclusion criteria, the patients were classifiedinto two groups: (1) patients with decreased renal function,and (2) patients who presented with recurrent UTI or ur-osepsis (cases 5, 6, and 8) with acceptable renal function on thelast preoperative renal scan (more than 40%).
The study and the procedure were reviewed and approvedby the research and ethics committee of Shiraz University ofMedical Sciences, Shiraz, Iran. All the patients’ legal guard-ians were informed about the options that existed formanagement of this problem and informed consents fortaking part in the study were obtained from them. Our pro-cedure was started under general anesthesia. Before endo-ureterotomy, cystoscopy was performed to rule out posteriorurethral valve and ectopic ureter. Then, a 0.018-inch guide-wire was applied to access the affected ureter by ureteroscope(4.5F neonatal ureteroscope [Richard Wolf GmbH, Knittlin-
gen, Germany]). In stenotic cases in which the ureteroscopewas not advanced through the ureterovesical junction (UVJ), azebra guidewire was used along with the safety guidewire tobypass it using a railroad maneuver. After passing throughthe UVJ, there was a stenotic ring a few millimeters behind theUVJ. After insertion of the safety wire and passing it throughthe stenotic ring, a retrograde incision was made at the 6o’clock position longitudinally using a Bugbee electrode withpure cutting current (25W). The ureteroscope was advancedsimultaneously when we made the incision. The stenotic ringwas passed by the ureteroscope, and the adequacy and depthof the incision were rechecked while we were pulling off theureteroscope from the ureter. After completion of the proce-dure, a 3F Double-J stent was inserted into the affected ureter.The stent was removed 1 week after the procedure, and an-tibiotic therapy (first generation cephalosporin) was contin-ued during this time.
The patients were followed up for about 18 months, andurine culture and serial ultrasonography were obtained at thefirst month and every 3 months after ureteral stent removal. Inaddition, VCUG was performed at the sixth month of thefollow-up to rule out iatrogenic VUR. Moreover, a radionu-clide renal scan was obtained from the patients at 3, 6, and 18months of the follow-up period. In this study, the operativegoals were defined as reduction in the degree of hydro-ureteronephrosis, improvement in or stabilization of renalfunction, and elimination of the UTI episodes.
Results
The present study was conducted in 10 patients (7 boys and3 girls) aged between 2 months and 12 months (mean7.1 mos). The mean follow-up period was 18 months (range6–24 mos). Left-side involvement was detected in all the pa-tients, except for one whose problem was at the right side.Also, seven patients presented with decreased renal function(group 1), while three (group 2) were referred with recurrentUTI and urosepsis that was unresponsive to prophylacticantibiotic therapy. One of the patients was febrile because ofUTI. In addition, four of the seven male patients were cir-cumcised when they were referred to us.
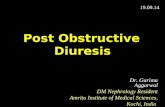
The endoureterotomy procedure lasted for 25 up to 40minutes. No significant intraoperative or postoperative com-plications were notable. The hospitalization time was 24 to 48hours. At the 18th month of the follow-up, 6 of the 10 patientshad complete resolution in the degree of hydroureterone-phrosis (Fig. 1), and 3 patients showed reduction from severeto mild (Table 1). Except for one (case 9), all the patients in
FIG. 1. (A) Preoperation ultra-songraphy and (B) postoperativeultrasonography. BL = bladder;LU = left ureter; UBL = urinarybladder.
80 SHIRAZI ET AL.

group 1 (cases No. 1, 2, 3, 4, 7, 9, and 10) showed significantimprovement in renal function postoperatively. Although thedegree of hydronephrosis in case 9 diminished from severe tomoderate, urosepsis developed in that patient during theperiod of follow-up visits with reduction in kidney functionon renal isotope scan; therefore, loop cutaneous ureterostomywas performed for this patient.
In group 2 (cases No. 5, 6, and 8), although renal functionhad not changed significantly, all the patients were infec-tion free postoperatively, and distal ureteral diameters weredecreased.
Discussion
POMU refers to the condition in which the patient presentswith intrinsic ureteral obstruction in the distal end of the ureter.This condition can be explained by various pathophysiologiccauses, including ureteral muscularis layer involvement bydiminished longitudinal fibers and hypertrophic change ofcircular muscle fibers,4 changes in the innervation pattern ofthe muscularis layer,21 and deposition of collagen material inthe abnormal matter.3 According to several pathophysiologicissues existing in the background of this condition, varioustreatment options are advised for management of POMU. Inspite of these several methods of treatment, the management ofthis condition remains inconclusive, especially in children lessthan 1 year old.
Nonoperative conservative treatment was investigated bysome researchers but had a failure rate of about 84%.22 Inother studies, spontaneous resolution of POMU without im-pairment in the renal function was reported.6,23–26 POMU inassociation with progressive renal damage, symptoms such asfever and flank pain, and increasing dilatation, is indicated foroperative management. Arena and coworkers30 reported thathydroureteronephrosis resolved spontaneously in 55.6% oftheir patients when the retrovesical ureteral diameter wasbetween 11 and 15 mm.27 They also mentioned that sponta-neous resolution was less likely when ureteral diameter wasmore than 15 mm.
Peters and colleagues10 conducted a study in which 89% ofthe patients were less than 8 months old and reported a re-markable reoperation rate. Similar to the plication method orexcisional tapering technique, open surgery has its owncomplications, the most common of which being ureteralstricture.28 In addition, an open surgical procedure is associ-ated with technical difficulties regarding reimplantation ofthe dilated ureter into a small bladder. Consequently, someresearchers have recommended cutaneous ureterostomy15,16
or temporary Double-J stent insertion.17 Cutaneous ureter-ostomy is associated with many complications, such as is-chemia of the distal ureter, stomal stenosis, and difficulty inother future surgeries.19,20 Temporary Double-J stent place-ment is also accompanied by several complications, includingstent migration, encrustation, UTI, and stone formation.18
Bladder dysfunction is another complication of open surgeryin this age group.14,29
The need for intervention for the aforementioned groupand the remarkable complications of the open surgical tech-niques have led to emergence of minimally invasive methodsthat preserve renal function with acceptable postoperativeresults and minimal postoperative complications. There is apaucity of data, however, regarding the endoscopic man-agement of POMU in the literature.
Yttrium-aluminum-garnet (YAG) laser endoureterotomyhas also been described in the literature. This technique wasused for ureteral stricture in two studies, one of which re-ported an acceptable success rate,30 while the other reported alower one.31 YAG laser was also used for correction of con-genital megaureter in adults with symptomatic and radiologicimprovement of all patients at 30.5 months.32
Endoscopic balloon dilation is suggested by some cliniciansas a minimally invasive therapy in patients less than 1 year oldwho have POMU.13,33 This procedure, however, is not with-out its complications. As Garcia-Aparicio and associates33
pointed out, 3 of 13 patients needed ureteral reimplantationbecause of persistent hydroureteronephrosis and VUR. Fur-thermore, the balloon is not available worldwide, and there islimited experience with this technique. Kajbafzadeh and
Table 1. Characteristics of Patients at 6 and 18 Months of Follow-Up
Creatinine DTPA scan Distal ureteral diameter (mm) Degree of hydroureteronephrosis
No. SexAge
(mos)
Postop Postop Postop Postop
Preop 6 18 Preop 6 18 Preop 6 18 Preop 6 18
1 M 2 0.4 0.2 0.3 25% Lt 36% Lt 49% Lt 25 14 5 Severe No No2 M 6 0.5 0.4 0.5 35% Lt 42% Lt 45% Lt 16 10 4 Moderate No No3 M 12 0.5 0.6 0.5 29% Lt 40% Lt 40% Lt 25 14 8 Severe Mild Mild4 M 7 0.4 0.4 0.4 9.2% Lt 32% Lt 37% Lt 17 10 3 Severe No No5 M 8 0.4 0.5 0.5 50% Rt 48% Rt 49% Rt 20 14 7 Severe Mild Mild6 F 5 0.6 0.4 0.5 50% Lt 50% Lt 49% Lt 22 20 11 Severe Mild Mild7 M 9 0.5 0.5 0.5 29% Lt 49% Lt 48% Lt 21 14 5 Severe No No8 F 5 0.5 0.4 0.4 45% Lt 47% Lt 45% Lt 25 14 8 Severe No No
*9 F 6 0.5 0.5 0.4 10.5% Lt 8% Lt — 18 12 — Severe Moderate —10 M 11 0.7 0.5 0.4 24% Lt 41% Lt 45% Lt 22 12 5 Severe No No
*Case 9 was not included at 18 months of follow-up because of urosepsis and deteriorated renal function; she underwent cutaneousureterostomy at 12 months of age.
All patients had no vesicoureteral reflux on preoperative and postoperative voiding cystourethrography.Cases 5 and 6 presented with recurrent urinary tract infection, case 8 presented with urosepsis, and all others had decreased renal function.DTPA = diethylenetriaminepentaacetic acid; preop = preoperative; postop = postoperative.
ENDOURETEROTOMY IN PRIMARY OBSTRUCTING MEGAURETER 81

colleagues12 demonstrated the long-term safety of endo-ureterotomy in patients more than 1 year old.
Endoscopic ureteral incision for POMU in children morethan 1 year old was first described by Kajbafzadeh and co-workers12 with a postoperative success rate of about 90%.
The high rate of postoperative open surgery morbidity,creation of VUR, and its cost are diminished when using theendoscopic approach. The endoscopic technique also pre-vents damage to the vasculature of the distal end of the ureter.As reported by Defoor and associates,34 open surgery wouldcompromise it and result in ureteral stricture in the future.
In practice, an endoscopic ureteral incision could be madeby several methods, such as cold knife, electrosurgical probes,and the holmium:YAG laser. In the present study, the re-searchers made use of the electrocautery method, because itprovides precise control of the incision width and length withgood ability to provide local hemostasis.12
A Double-J stent was inserted for all the patients for 1 weekafter the operation to promote ureteral healing. It may preventrestricturing or urine extravasation, as well. On the otherhand, long-lasting ureteral stent placement can cause in-flammation, leading to impairment in the healing process aswell as scar tissue formation.35
Kajbafzadeh and coworkers12 performed endoureterotomyafter at least 12 months of conservative management. In ourstudy, all patients underwent endoureterotomy when theywere less than 1 year old.
We used a Double-J stent for 1 week to reduce the risk ofrestricturing. The diameter of the distal ureteral part and thekidney function were improved in all the study patients, ex-cept for one who underwent cutaneous ureterostomy becauseof deterioration in her renal function and urosepsis in thefollow-up (case 9). No new onset of UTI was observed inour patients postoperatively, however. The prophylacticantibiotic was discontinued after performing the renal scan toconfirm obstruction resolution. Overall, the results of thecurrent study suggest that endoureterotomy is practicable forchildren less than 1 year old with POMU. Of course, furtherstudies with longer follow-up periods are needed on a largernumber of patients to confirm the obtained results.
Conclusion
In this study, we tried a new method for management ofPOMU in patients less than 1 year old. There is controversy inthe management of this problem. Minimally invasive proce-dures result in a high success rate and are not accompanied bythe complications associated with other methods, especiallyconventional open surgery. The findings of the present studyrevealed a remarkable success rate in patients undergoingendoureterotomy. According to the preliminary results of ourstudy, endoureterotomy may be an alternative in manage-ment of POMU. Of course, further studies with longer follow-up periods are needed to confirm the applicability of thismethod in patients less than 1 year old.
Acknowledgments
The present article was extracted from the thesis written byMr. Mohammad Natami in Urology approved by ShirazUniversity of Medical Sciences (Proposal No. 90-01-01-4087).
The authors would like to thank the Research ImprovementCenter of Shiraz University of Medical Sciences, Shiraz, Iran,
and Ms. A. Keivanshekouh for improving the use of English inthe manuscript.
Disclosure Statement
No competing financial interests exist.
References
1. Cussen LJ. The morphology of congenital dilatation of theureter: Intrinsic ureteral lesions. Aust N Z J Surg 1971;41:185–194.
2. Hellstrom M, Hjalmas K, Jacobsson B, Jodal U. Ureteral di-ameter in low-risk vesicoureteral reflux in infancy andchildhood. Acta Radiol Diagn (Stockh) 1986;27:77–83.
3. Lee BR, Silver RI, Partin AW, et al. A quantitative histologicanalysis of collagen subtypes: The primary obstructed andrefluxing megaureter of childhood. Urology 1998;51:820–823.
4. Shokeir AA, Nijman RJ. Primary megaureter: Current trendsin diagnosis and treatment. BJU Int 2000;86:861–868.
5. Antoine K, Darius J. Reflux and megaureter. In: Wein AJ,Kavoussi LR, Novick AC, Partin AW, Peters CA, eds.Campbell-Walsh Urology. 9th ed. Philadelphia: Saunders,2007, pp 3467–3481.
6. Keating MA, Escala J, Snyder HM III, et al. Changing con-cepts in management of primary obstructive megaureter. JUrol 1989;142:636–640.
7. McLellan DL, Retik AB, Bauer SB, et al. Rate and predictorsof spontaneous resolution of prenatally diagnosed primarynonrefluxing megaureter. J Urol 2002;168:2177–2180.
8. Williams DI, Hulme-Moir I. Primary obstructive mega-ureter. Br J Urol 1970;42:140–149.
9. Shukla AR, Cooper J, Patel RP, et al. Prenatally detectedprimary megaureter: A role for extended followup. J Urol2005;173:1353–1356.
10. Peters CA, Mandell J, Lebowitz RL, et al. Congenital ob-structed megaureters in early infancy: Diagnosis and treat-ment. J Urol 1989;142:641–645.
11. Stehr M, Metzger R, Schuster T, et al. Management of theprimary obstructed megaureter (POM) and indication foroperative treatment. Eur J Pediatr Surg 2002;12:32–37.
12. Kajbafzadeh AM, Payabvash S, Salmasi AH, et al. En-doureterotomy for treatment of primary obstructive mega-ureter in children. J Endourol 2007:21:743–749.
13. Torino G, Collura G, Mele E, et al. Severe primary obstruc-tive megaureter in the first year of life: Preliminary experi-ence with endoscopic balloon dilation. J Endourol 2011:26:325–329.
14. Lipski BA, Mitchell ME, Burns MW. Voiding dysfunctionafter bilateral extravesical ureteral reimplantation. J Urol1998;159:1019–1021.
15. Hendren WH. Operative repair of megaureter in children.J Urol 1969;101:491–507.
16. Hendren WH. Technical aspects of megaureter repair. BirthDefects Orig Artic Ser 1977;13:21–33.
17. Ransley PG, Dhillon HK, Gordon I, et al. The postnatalmanagement of hydronephrosis diagnosed by prenatal ul-trasound. J Urol 1990;144:584–587.
18. Farrugia MK, Steinbrecher HA, Malone PS. The utilization ofstents in the management of primary obstructive mega-ureters requiring intervention before 1 year of age. J PediatrUrol 2011;7:198–202.
19. Rickwood AM. Genitourinary surgery. In: Rob C, Smith R,Baron; Dudley H, Carter DC, Russell RC, Whitfield HN, eds.
82 SHIRAZI ET AL.

Rob & Smith’s Operative Surgery. London: Butterworth-Heinemann, 1986, p 831.
20. Koo HP, Bloom DA. Temporary urinary diversion (ureter-ostomy & vesicostomy) In: Frank JD, Gearhart JP, SnyderHM, eds. Operative Pediatric Urology. New York: ChurchillLivingstone, 2002, p 45.
21. Dixon JS, Jen PYP, Yeung CK, Gosling JA. The vesico-ureteric junction in three cases of primary obstructivemegaureter associated with ectopic ureteric insertion. Br JUrol 1998;81:580–584.
22. Sheu JC, Chang PY, Wang NL, et al. Is surgery necessary forprimary non-refluxing megaureter? Pediatr Surg Int1998;13:501–503.
23. Liu HY, Dhillon HK, Yeung CK, et al. Clinical outcome andmanagement of prenatally diagnosed primary megaureters.J Urol 1994;152: 614–617.
24. Arena F, Baldari S, Proietto F, et al. Conservative treatmentin primary neonatal megaureter. Eur J Pediatr Surg 1998;8:347–351.
25. Baskin LS, Zderic SA, Snyder HM, Duckett JW. Primarydilated megaureter: Long-term followup. J Urol 1994;152:618–621.
26. Hemal AK, Ansari MS, Doddamani D, Gupta NP. Sympto-matic and complicated adult and adolescent primary ob-structive megaureter—indications for surgery: Analysis,outcome, and follow-up. Urology 2003;61:703–707.
27. Arena S, Magno C, Montalto AS, et al. Long-term follow-upof neonatally diagnosed primary megaureter: Rate andpredictors of spontaneous resolution. Scand J Urol Nephrol2012;46:201–207.
28. Ossandon F, Romanini MV, Torre M. A modified techniqueof ureteroplasty for megaureter in children. J Urol 2005;174:1417–1420.
29. Fung LC, McLorie GA, Jain U, et al. Voiding efficiency afterureteral reimplantation: A comparison of extravesical andintravesical techniques. J Urol 1995;153:1972–1975.
30. Hibi H, Ohori T, Taki T, et al. Long-term results of en-doureterotomy using a holmium laser. Int J Urol 2007;14:872–874.
31. Singal RK, Denstedt JD, Razvi HA, Chun SS. Holmium:YAGlaser endoureterotomy for treatment of ureteral stricture.Urology 1997;50:875–880.
32. Biyani CS, Powell CS. Congenital megaureter in adults: En-doscopic management with holmium:YAG laser—preliminaryexperience. J Endourol 2001;15:797–799.
33. Garcia-Aparicio L, Rodo J, Krauel L, et al. High pressureballoon dilation of the ureterovesical junction—first lineapproach to treat primary obstructive megaureter? J Urol2012;187:1834–1838.
34. DeFoor W, Minevich E, Reddy P, et al. Results of taperedureteral reimplantation for primary megaureter: Extra-vesical versus intravesical approach. J Urol 2004;172:1640–1643.
35. Hafez KS, Wolf JS Jr. Update on minimally invasivemanagement of ureteral strictures. J Endourol 2003;17:453–464.
Address correspondence to:Mehdi Shirazi, MD
Department of UrologyShiraz Medical School
Zand AvenueShiraz, Fars7134844119
Iran
E-mail: [email protected]
Abbreviations UsedPOMU¼primary obstructive megaureter
UTI¼urinary tract infectionUVJ¼ureterovesical junction
VCUG¼voiding cystourethrographyVUR¼vesicoureteral refluxYAG¼ yttrium-aluminum-garnet
ENDOURETEROTOMY IN PRIMARY OBSTRUCTING MEGAURETER 83