Response of Charité total disc replacement under physiologic loads: prosthesis component motion...
10
2005 Outstanding Paper Award: Surgical Science Response of Charite ´ total disc replacement under physiologic loads: prosthesis component motion patterns Patrick O’Leary, MD a,b , Michael Nicolakis, MD c , Mark A. Lorenz, MD a,b , Leonard I. Voronov, MD a,b , Michael R. Zindrick, MD a,b , Alexander Ghanayem, MD a,b , Robert M. Havey, BS a,b , Gerard Carandang, MS a , Mark Sartori, BS a,b , Ioannis N. Gaitanis, MD a,b , Stanley Fronczak, MD a , Avinash G. Patwardhan, PhD a,b, * a Musculoskeletal Biomechanics Laboratory, Department of Veterans Affairs, Edward Hines Jr. VA Hospital, 5th Ave. and Roosevelt Rd., Hines, IL 60141, USA b Department of Orthopaedic Surgery and Rehabilitation, Loyola University Medical Center, 2160 S. First Ave., Maywood, IL 60153, USA c Evangelisches Krankenhaus Wien, Hans-Sach-Gasse 10–12, A-1180 Vienna, Austria Received 11 January 2005; accepted 15 June 2005 Abstract BACKGROUND CONTEXT: Total disc replacement (TDR) has been recommended to reduce pain of presumed discogenic origin while preserving spinal motion. The floating core of Charite ´ TDR is professed to allow the replication of the kinematics of a healthy disc under physiologic loads. While segmental motion after Charite ´ TDR has been measured, little is known about the effects of a physi- ologic compressive preload on vertebral motion and the motion of prosthesis components after TDR. PURPOSE: (1) Does Charite ´ TDR allow restoration of normal load-displacement behavior of a lumbar motion segment under physiologic loads? (2) How do the prosthesis components move relative to each other under physiologic loads when implanted in a lumbar motion segment? STUDY DESIGN: A biomechanical study using human lumbar spines (L1-sacrum). METHODS: Five lumbar spines (age: 5269.3) were used. Specimens were tested under flexion (8 Nm) and extension (6 Nm) moments with compressive follower preloads of 0 N and 400 N in the following sequence: (i) intact, (ii) Charite ´ TDR at L5-S1, (iii) simulated healed fusion at L5-S1 with Charite ´ TDR at L4-L5. Segmental motion was measured optoelectronically. Motions between pros- thesis end plates and core were visually assessed using sequential digital video-fluoroscopy over the full range of motion. Here we report on kinematics of 10 Charite ´ TDRs: 5 at L5-S1 and 5 at L4-L5. RESULTS: Charite ´ TDR increased the flexion-extension range of motion of lumbar segments (p ! .05). At 400 N preload, the range of motion increased from intact values of 6.864.4 to 10.062.4 degrees at L5-S1 and from 7.062.6 to 10.862.9 degrees at L4-L5. Charite ´ TDR increased segmental lordosis by 8.166.9 degrees at L5-S1 (p ! .05) and 5.463.5 degrees at L4-L5 (p !.05). Four patterns of prosthesis component motion were noted: (1) angular motion only between the upper end plate and core, with little or no visual evidence of core translation (9 of 10 TDRs at 0 N preload and 5 of 10 TDRs at 400 N preload); (2) lift-off of upper prosthesis end plate from core or of core from lower end plate (observed in extension in 9 of 10 TDRs under 0 N preload only); (3) core entrapment, resulting in a locked core over a portion of the range of motion (observed in extension in 8 of 10 TDRs under 400 N preload); (4) angular motion between both the upper and lower end plates and core, with visual evidence of core translation (1 of 10 TDRs at 0 N preload, 5 of 10 TDRs at 400 N preload). The pattern of load-displacement curves was substantially changed under a physiologic preload in 8 of 10 TDRs; instead of a relatively gradual change in angle with changing moment application as seen for an intact segment, the TDR displayed regions of both relatively small and relatively large angular changes with gradual moment application. CONCLUSIONS: Charite ´ TDR restored near normal quantity of flexion-extension range of motion under a constant physiologic preload; however, the quality of segmental motion differed FDA device/drug status: approved for this indication (Charite ´ Artificial Disc). Nothing of value received from a commercial entity related to this manuscript. * Corresponding author. Department of Orthopaedic Surgery and Rehabilitation, Loyola University Medical Center, 2160 S. First Avenue, Maywood, Illinois 60153. Tel.: (708) 202-5804; fax: (708) 202-7938. E-mail address: [email protected] (A.G. Patwardhan) 1529-9430/05/$ – see front matter Ó 2005 Elsevier Inc. All rights reserved. doi:10.1016/j.spinee.2005.06.015 The Spine Journal 5 (2005) 590–599
-
Upload
patrick-oleary -
Category
Documents
-
view
214 -
download
1
Transcript of Response of Charité total disc replacement under physiologic loads: prosthesis component motion...

The Spine Journal 5 (2005) 590–599
2005 Outstanding Paper Award: Surgical Science
Response of Charite total disc replacement under physiologic loads:prosthesis component motion patterns
Patrick O’Leary, MDa,b, Michael Nicolakis, MDc, Mark A. Lorenz, MDa,b,Leonard I. Voronov, MDa,b, Michael R. Zindrick, MDa,b, Alexander Ghanayem, MDa,b,
Robert M. Havey, BSa,b, Gerard Carandang, MSa, Mark Sartori, BSa,b,Ioannis N. Gaitanis, MDa,b, Stanley Fronczak, MDa, Avinash G. Patwardhan, PhDa,b,*
aMusculoskeletal Biomechanics Laboratory, Department of Veterans Affairs, Edward Hines Jr. VA Hospital,
5th Ave. and Roosevelt Rd., Hines, IL 60141, USAbDepartment of Orthopaedic Surgery and Rehabilitation, Loyola University Medical Center, 2160 S. First Ave., Maywood, IL 60153, USA
cEvangelisches Krankenhaus Wien, Hans-Sach-Gasse 10–12, A-1180 Vienna, Austria
Received 11 January 2005; accepted 15 June 2005
Abstract BACKGROUND CONTEXT: Total disc replacement (TDR) has been recommended to reduce painof presumed discogenic origin while preserving spinal motion. The floating core of Charite TDR isprofessed to allow the replication of the kinematics of a healthy disc under physiologic loads. Whilesegmental motion after Charite TDR has been measured, little is known about the effects of a physi-ologic compressive preload on vertebral motion and the motion of prosthesis components after TDR.PURPOSE: (1) Does Charite TDR allow restoration of normal load-displacement behavior ofa lumbar motion segment under physiologic loads? (2) How do the prosthesis components moverelative to each other under physiologic loads when implanted in a lumbar motion segment?STUDY DESIGN: A biomechanical study using human lumbar spines (L1-sacrum).METHODS: Five lumbar spines (age: 5269.3) were used. Specimens were tested under flexion (8Nm) and extension (6 Nm) moments with compressive follower preloads of 0 N and 400 N in thefollowing sequence: (i) intact, (ii) Charite TDR at L5-S1, (iii) simulated healed fusion at L5-S1 withCharite TDR at L4-L5. Segmental motion was measured optoelectronically. Motions between pros-thesis end plates and core were visually assessed using sequential digital video-fluoroscopy over thefull range of motion. Here we report on kinematics of 10 Charite TDRs: 5 at L5-S1 and 5 at L4-L5.RESULTS: Charite TDR increased the flexion-extension range of motion of lumbar segments(p!.05). At 400 N preload, the range of motion increased from intact values of 6.864.4 to10.062.4 degrees at L5-S1 and from 7.062.6 to 10.862.9 degrees at L4-L5. Charite TDR increasedsegmental lordosis by 8.166.9 degrees at L5-S1 (p!.05) and 5.463.5 degrees at L4-L5 (p!.05). Fourpatterns of prosthesis component motion were noted: (1) angular motion only between the upper endplate and core, with little or no visual evidence of core translation (9 of 10 TDRs at 0 N preload and 5of 10 TDRs at 400 N preload); (2) lift-off of upper prosthesis end plate from core or of core from lowerend plate (observed in extension in 9 of 10 TDRs under 0 N preload only); (3) core entrapment,resulting in a locked core over a portion of the range of motion (observed in extension in 8 of 10 TDRsunder 400 N preload); (4) angular motion between both the upper and lower end plates and core, withvisual evidence of core translation (1 of 10 TDRs at 0 N preload, 5 of 10 TDRs at 400 N preload). Thepattern of load-displacement curves was substantially changed under a physiologic preload in 8 of 10TDRs; instead of a relatively gradual change in angle with changing moment application as seen foran intact segment, the TDR displayed regions of both relatively small and relatively large angularchanges with gradual moment application.CONCLUSIONS: Charite TDR restored near normal quantity of flexion-extension range ofmotion under a constant physiologic preload; however, the quality of segmental motion differed
FDA device/drug status: approved for this indication (Charite Artificial
Disc).
Nothing of value received from a commercial entity related to this
manuscript.
1529-9430/05/$ – see front matter � 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.spinee.2005.06.015
* Corresponding author. Department of Orthopaedic Surgery and
Rehabilitation, Loyola University Medical Center, 2160 S. First Avenue,
Maywood, Illinois 60153. Tel.: (708) 202-5804; fax: (708) 202-7938.
E-mail address: [email protected] (A.G. Patwardhan)

591P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
from the intact case over the flexion-extension range. Whereas some TDRs showed visual evidenceof core translation, the predominant angular motion within the prosthesis occurred between the up-per end plate and the polyethylene core. Likely factors affecting the function of the Charite TDRinclude implant placement and orientation, intraoperative change in lordosis, and magnitude ofphysiologic compressive preload. Further work is needed to assess the effects of the prosthesis mo-tion patterns identified in the study on the load sharing at the implanted level and polyethylene corewear. � 2005 Elsevier Inc. All rights reserved.
Keywords: Total disc replacement; Lumbar spine; Biomechanics; Kinematics; Follower preload
Introduction
Total disc replacement (TDR) has been recommended toreduce pain of presumed discogenic origin while preservingspinal motion to reduce the likelihood of accelerated adja-cent level degeneration that has been reported after lumbararthrodesis surgery. One of the objectives of TDR im-planted for degenerative disc disease is to allow replicationof the natural biomechanics of a healthy intervertebral discunder physiologic loads. The design of a TDR, its im-planted position within the disc space, and the presenceand quality of the bony, soft tissue, and muscular structuresare among the factors that determine how well the naturalbiomechanics are replicated.
The design of the Charite prosthesis consists of two co-balt-chrome end plates and a mobile ultrahigh-molecular-weight polyethylene core [1,2]. The three-componentprosthesis with unconstrained sliding core was designedto allow replication of the normal kinematics of lumbarsegments under physiologic loads [2].
Previous studies have measured segmental motions afterCharite TDR [3]. However, little is known about the effectsof a physiologic compressive preload on segmental motionand the motion of prosthesis components after TDR. Theprosthesis component motion patterns may have implica-tions to polyethylene core wear under in vivo physiologicloads and load sharing within the implanted and adjacentlevels. Failure to provide normal load sharing may resultin instability, which may in turn cause hypertrophic boneformation or accelerated facet degeneration. If the core issubject to wear either from shear, compression, or a combi-nation of these forces, or if motion patterns are abnormal,the goal of saving adjacent levels may not be realized.
We asked two questions:
(1) Does Charite TDR allow restoration of normal load-displacement behavior of a lumbar motion segmentunder physiologic loads?
(2) How do the prosthesis components move relative toeach other under physiologic loads when implantedin a lumbar motion segment?
Materials and methods
Specimens
Five human cadaveric lumbar spine specimens (L1-sacrum) were tested. The specimens were from four males
and one female, with a mean age of 52 years (SD: 9.3)(Table 1). The specimens had no radiographic signs ofmetastatic disease or bridging osteophytes. The age rangeof this study sample is comparable to that of specimensused in previous biomechanical studies of lumbar discprostheses [3], and to that of patients treated with lumbardisc prostheses [4–6].
Plain radiographs were taken; T2-weighted magneticresonance imaging scans and discography were performedto assess the extent of degenerative changes at the appropri-ate intervertebral levels; 3 of 5 L5-S1 levels had moderatedegeneration, and 2 of 5 L5-S1 levels had moderate-severedegeneration. One of the five L4-L5 levels had moderatedegeneration, whereas 4 of 5 L4-L5 levels had mild degen-eration (Table 2).
Experimental setup
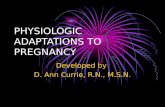
The L1 vertebra and sacrum were anchored in cups us-ing polymethylmethacrylate and pins. The specimen wasfixed to the apparatus at the caudal end and was free tomove in any plane at the proximal end (Fig. 1). A momentwas applied by controlling the flow of water into bags at-tached to loading arms fixed to the L1 vertebra. The appa-ratus allowed continuous cycling of the specimen betweenspecified maximum moment endpoints in flexion andextension.
The motion of the L1, L2, L3, L4, and L5 vertebrae rel-ative to sacrum was measured using an optoelectronic mo-tion measurement system (Model 3020, Optotrak; NorthernDigital, Waterloo, Ontario). In addition, bi-axial angle sen-sors (Model 902-45; Applied Geomechanics, Santa Cruz,CA) were mounted on each vertebra to allow real-timefeedback for the optimization of the preload path. A six-component load cell (Model MC3A-6-250, AMTI Multi-component transducers; AMTI Inc., Newton, MA) was
Table 1
Specimen demographics
Specimen Age (years) Sex Cause of death
1 59 Male Melanoma
2 46 Male Cardiomyopathy
3 60 Male Severe blood loss
4 57 Male Renal failure
5 39 Female Pneumonia, sepsis
Mean 52
SD 9.3

592 P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
placed under the specimen to measure the applied compres-sive preload and moments. Fluoroscopic imaging (GE OEC9800 Plus digital fluoroscopy machine) was used duringflexion and extension in order to monitor motions between
Table 2
Specimen degeneration based on X-ray, MRI, and discography
Specimen L5-S1 L4-L5 Facet joints
1 50% loss of
height; anterior
osteophytes
Minimal height
loss; intact disc
No hypertrophy
2 20% loss of
height; black
disc
Black disc Mild hypertrophy
3 20% loss of
height; intact
disc
Annular
disruption;
black disc
No hypertrophy
4 20% loss of
height; annular
disruption;
black disc
Annular
disruption;
black disc
No hypertrophy
5 O50% loss of
height; anterior
osteophytes;
annular
disruption
20% loss of disc
height; anterior
osteophytes;
annular
disruption
Mild hypertrophy
L5-S1 facets
prosthesis end plates and core, as well as between the im-plant and vertebral end plates. Sequential digital video-fluoroscopy images were obtained over the full range offlexion-extension motion.
The compressive preload was applied along a path thatfollowed the lordotic curve of the lumbar spine, calledthe follower load path [7,8]. By applying a compressiveload along the follower load path, the segmental bendingmoments and shear forces resulting from the preload appli-cation were minimized [9,10]. This allowed the lumbarspine to support physiologic compressive preloads withoutdamage or instability.
The preload was applied using bilateral loading cablesthat were attached to the cup holding the L1 vertebra.The cables passed freely through guides anchored to eachvertebra and were connected to a loading hanger under thespecimen (Fig. 1). The cable guide mounts allowed anterior-posterior adjustments of the follower load path within arange of about 10 mm. The alignment (optimization) ofthe preload path was performed by adjusting the cableguides to minimize changes in lumbar lordosis when thecompressive load up to 400 N was applied to the speci-men. Our previous studies demonstrated that optimizationof the follower preload path minimizes the effects of
Fig. 1. Experimental setup showing a lumbar spine specimen subjected to a follower preload. The preload was applied using bilateral loading cables that
were attached to the cup holding the L1 vertebra. Segmental motion was measured using optoelectronic markers attached to the spinous processes and
bi-axial angle sensors attached to vertebrae anteriorly. Prosthesis component motion was monitored using a digital videofluoroscopy machine.

593P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
experimental artifacts (moment and shear force induced bypreload application) on the range of motion of the spine inflexion-extension [8].
Experimental protocol
Test conditionsSpecimens were tested in the following sequence: (i) in-
tact, (ii) Charite TDR at L5-S1, and (iii) simulated healedfusion at L5-S1 with Charite TDR at L4-L5. We simulateda healed fusion at L5-S1 so that we could assess the effectsof a single level arthroplasty at L4-L5, although it shouldbe noted that the final testing sequence is an ‘‘off-label’’(non-FDA-approved) use of the Charite TDR adjacent toa fusion.
In each condition, the specimens were subjected to flex-ion (8 Nm) and extension (6 Nm) moments with compres-sive follower preloads of 0 N and 400 N. These momentvalues are within the range of moments used in previousbiomechanical studies of human lumbar spine segments[8]. A compressive follower load of 400 N was used to sim-ulate the physiologic load on the lumbar spine produced bymuscle activity during activities of daily living [11,12].
Baseline measurementsFirst, the baseline range of motion of the intact specimen
was determined in flexion-extension under 0 N externalpreload. The load-displacement data were collected untiltwo reproducible load-displacement loops were obtained.This required a maximum of three loading cycles. After op-timization of the preload path, the range of motion test onthe intact spine was repeated in flexion-extension for 400 Ncompressive follower preload.
Total disc replacementAfter testing the intact spine, a Charite TDR was per-
formed by experienced spine surgeons using standard tech-niques described previously [13]. The midline of thevertebral body was marked after careful measurement withdigital calipers. A longitudinal incision was made throughthe anterior longitudinal ligament and annulus fibrosus inthe exact location of the measured midline. A near-completediscectomy was then performed. The lateral portions of theannulus were preserved in each specimen. The cartilaginousportions of the end plates were removed, being careful topreserve the bony end plate architecture. After discectomy,the disc space was gradually distracted using the centralspreader and other distractors. In each case, the posteriorlongitudinal ligament was released as has been described[13] to achieve ligament balancing and proper positioningof the disc prosthesis. Trial sizes were used to estimate thesize of the disc footprint. These sizes were verified usingfluoroscopy and a preoperative template. The implant wassized to the largest possible end plate that would reasonablyfit onto the bony end plate. In certain cases, an osteotomewas used to remove a lip of bone from either the native
superior or inferior end plates to ensure parallel alignmentof the prosthetic end plates. Next, a Charite disc prosthesiswas implanted at L5-S1 using the appropriate insertion for-ceps in the exact location of the demarcated midline (Table3). Proper anteroposterior and sagittal placement was con-firmed both by direct visualization and by fluoroscopy. Op-timal position was regarded as the middle of the prosthesissitting 2 mm posterior to the mid-sagittal line of the verte-bral body [13]. The end plates were distracted and a coresize was selected after trials (Table 3). The core was im-planted and after distraction was removed, fluoroscopywas again used to confirm optimal positioning. The speci-men was then tested in flexion-extension as describedabove.
After testing of the TDR at L5-S1, a healed fusion at thatlevel was simulated. This was accomplished by removingthe TDR and using interbody fusion cages, facet screws,and polymethylmethacrylate with screws to act like an an-terior tension band (subsequent mechanical testing showedevidence of less than 1–2 degrees of motion at the L5-S1level under flexion-extension moments). Next, an anteriordiscectomy was performed at L4-L5 and a Charite discprosthesis was implanted as described previously (Table3). The specimen was then tested in flexion-extension.The specimen was wrapped in saline soaked towels to pre-vent dehydration of the tissue throughout the test protocol.All tests were performed at room temperature.
After completion of the mechanical test protocol, theL2-L3 segment was separated from the lumbar spine. Todetermine the bone mineral density of the specimen, theL2 body was scanned with use of a peripheral computed to-mography bone-mineral densitometry instrument (XCTResearch SA; Norland Medical Systems, White Plains,NY). Trabecular bone mineral density was measured forthe L2 vertebra in the scan made approximately in the mid-point of the vertebral end plates. None of the five specimenswas classified as osteoporotic, and all were thus included inthe subsequent data analysis.
Data analysis
Analysis of segmental motionThe load-displacement curves were analyzed to deter-
mine the total angular range of motion in flexion-extensionat the L5-S1 and L4-L5 segments in the intact spine and af-ter TDR. The angular motion data before and after each
Table 3
Summary of disc prostheses sizes
L5-S1 L4-L5
Specimen End plates Core End plates Core
1 # 4 (0, 7.5 �) # 4 (8.5 mm) # 4 (0, 5 �) # 4 (8.5 mm)
2 # 3 (0, 7.5 �) # 3 (8.5 mm) # 3 (0, 0 �) # 3 (8.5 mm)
3 # 3 (0, 5 �) # 3 (8.5 mm) # 3 (0, 0 �) # 3 (8.5 mm)
4 # 4 (0, 7.5 �) # 4 (8.5 mm) # 4 (0, 0 �) # 4 (8.5 mm)
5 # 3 (0, 5 �) # 3 (8.5 mm) # 3 (0, 0 �) # 3 (7.5 mm)

594 P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
disc replacement were analyzed using a repeated-measuresanalysis of variance. The level of significance was set atp!.05.
Analysis of segmental lordosisSegmental lordosis angles at L5-S1 and L4-L5 were cal-
culated from digital video-fluoroscopic images by three in-dependent observers for the intact specimen in neutralposture. These same independent observers then calculatedthe segmental lordosis angles after L5-S1 arthroplasty forboth 0 N and 400 N preload conditions. The segmental lor-dosis data before and after each disc replacement were an-alyzed using a repeated-measures analysis of variance. Thelevel of significance was set at p!.05. The same analysis ofsegmental lordosis was repeated after the TDR was insertedat L4-L5.
Analysis of prosthesis component motionsThe motions between the prosthesis components were
visually assessed using the sequential video-fluoroscopicimages obtained during the flexion-extension range of mo-tion. This assessment was performed by three independentobservers. Each observer assessed whether there was angu-lar motion at each of the two end plate-core joints andwhether or not there was visible core translation. In addi-tion, any ‘‘lift-off’’ of the prosthesis end plates from coreand/or separation at the vertebral end plate and prosthesiswere also noted.
To assess whether the frequency distribution of thesemotion patterns depended on the segmental level (L5-S1vs. L4-L5) or on the compressive preload (0 N vs. 400N), statistical analysis for contingency tables was per-formed. All statistical data analyses were performed usingthe Systat 10.2 software (Systat Software Inc., Richmond,CA).
Results
Segmental motion
Charite TDR increased the flexion-extension range ofmotion of lumbar segments. Under 0 N preload, the angularmotion increased from 7.864.8 to 13.462.3 degrees atL5-S1 (p!.05), and from 7.463.0 to 13.063.8 degrees atL4-L5 (p!.05) (Table 4). At 400 N preload, the range of mo-tion increased from intact values of 6.864.4 to 10.062.4degrees at L5-S1 (p!.05) and 7.062.6 to 10.862.9 degreesat L4-L5 (p!.05) (Table 5).
The TDR procedure significantly increased segmentallordosis at both levels (Table 6). Under a compressive pre-load of 400 N, the segmental lordosis at L5-S1 increasedfrom 12.662.7 to 20.768.3 degrees, an increase of8.166.9 degrees (p!.05). At L4-L5, the segmental lordosisincreased from 6.462.6 to 11.861.2 degrees, an increase of5.463.5 degrees (p!.05).
Prosthesis component motion
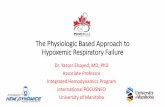
Four prosthesis component motion patterns (PCMPs)were noted (Fig. 2):
PCMP1: angular motion predominantly between theupper end plate and core, with little or no visible coretranslation (Fig. 2A);PCMP2: lift-off of upper prosthesis end plate from coreor of core from lower end plate (Fig. 2B);PCMP3: core entrapment, resulting in a locked coreover a portion of the range of motion (Fig. 2C); andPCMP4: angular motion between both the upper andlower end plates and core, with visible core translation(Fig. 2D).
The incidence rates of these movement patterns asa function of the segmental level and the magnitude ofcompressive preload are shown in Table 7. It should be not-ed that motion patterns PCMP1 and PCMP4 are mutuallyexclusive; hence their frequencies at a given segment addup to the total number of TDRs tested for that segment(ie, 5). On the other hand, motion patterns PCMP2 andPCMP3 (lift-off and core entrapment/locking) could coexistwith other observed patterns because lift-off or core entrap-ment/locking occurred during a portion of the flexion-extension motion.
In our sample, the motion pattern PCMP4 (angular mo-tion between both the upper and lower end plates and core,
Table 4
Total flexion-extension range of motion (deg) under 0 N preload
L5-S1 L4-L5
Specimen Intact TDR* Intact TDR*
1 5.7 10.0 8.7 14.9
2 15.6 15.8 10.8 14.0
3 3.6 12.6 2.9 17.7
4 5.1 13.3 6.3 10.4
5 8.8 15.3 8.3 8.1
Mean 7.8 13.4 7.4 13.0
SD 4.8 2.3 3.0 3.8
TDR5total disc replacement.
* Significantly larger than the corresponding intact value, p!.05.
Table 5
Total flexion–extension range of motion (deg) under 400 N preload
L5-S1 L4-L5
Specimen Intact TDR* Intact TDR*
1 4.0 8.1 7.6 13.0
2 14.0 12.5 10.4 11.9
3 3.6 9.6 3.6 13.6
4 4.4 7.4 5.3 8.7
5 7.9 12.6 8.0 6.9
Mean 6.8 10.0 7.0 10.8
SD 4.4 2.4 2.6 2.9
TDR5total disc replacement.
* Significantly larger than the corresponding intact value, p!.05.

595P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
with visible core translation) occurred more frequentlyunder a physiologic preload as compared with withouta preload (5 of 10 TDRs at 400 N vs. 1 of 10 at 0 N; Pear-son chi-square test: one-tailed p5.05) (Table 7). An exam-ination of motion patterns over both preloads showed thatthe prosthesis motion pattern with visible core translation(PCMP4) occurred more frequently at L4-L5 as comparedwith at the L5-S1 level; however, this trend was not statis-tically significant (Pearson chi-square test: one-tailedp5.21).
Lift-off of upper prosthetic end plate from core or ofcore from lower end plate (PCMP2) was observed onlyunder the conditions of 0 N external compressive preload(Table 7), whereas the entrapment/locking of the core(PCMP3) was seen more frequently under a physiologicpreload (8 of 10 TDRs) than without a preload (1 of 10TDRs). The predominant angular motion within the pros-thesis occurred at the articulation between the upper endplate and the core in all TDRs once the prosthesis compo-nents rearticulated after lift-off or entrapment of the corewere released.
Discussion
The Charite III was designed as an unconstrained totallumbar disc prosthesis [4]. Several biomechanical studieshave supported the efficacy of the Charite prosthesis. Ah-rens et al. [14] demonstrated an increase in range of motionat implanted segments versus intact segments. The averagerange of motion for flexion of the L4-L5 segment was 7.7degrees in intact segments and 9.8 degrees in a Charite im-planted segment. Extension range of motion was 3.5 and3.3 degrees, respectively. Cunningham [3] concluded thatthe Charite total disc prosthesis recreated the physiologicbehavior of the intervertebral disc with respect to the in-stantaneous center of rotation. Clinical outcome studiesgenerally report short-term results that are comparable tofusion [1].
However, there have been reported complications. Clin-ical reports show instances of core fracture [15], prosthesismigration or dislocation [15,16], and nonmovement of
Table 6
Effect of TDR on segmental lordosis (deg) under 400 N preload
L5-S1 L4-L5
Specimen Intact TDR* Intact TDR*
1 9.5 22.9 10.4 9.9
2 14.8 27.2 6.8 12.3
3 9.8 6.6 5.0 11.8
4 14.5 26.0 6.6 13.1
5 14.5 20.8 3.4 11.9
Mean 12.6 20.7 6.4 11.8
SD 2.7 8.3 2.6 1.2
TDR5total disc replacement.
* Significantly larger than the corresponding intact value, p!.05.
prosthesis [17]. Although it may be argued that the physio-logical environment in the spine cannot be directly com-pared with total joints, enough similarities exist betweenthe Charite prosthesis and the total joint implants that usemetal on polyethylene articulations [18]. The total joint ex-perience in wear and survivorship of implants suggests thatcareful assessment of component motions under in vivoloading may give important information to surgeons andmanufacturers to decrease implant-related long-term com-plications (such as wear, disintegration, fracture, dislodge-ment, loosening, or nonmovement).
Clinical measurement of vertebral motion using flexionand extension films is commonly performed to assess thefunction of TDR. However, this may not be adequate be-cause this measurement demonstrates end points only. Itdoes not allow the clinician to visualize prosthesis compo-nent motion throughout a given motion cycle. To ourknowledge, in clinical cases that are reported, careful as-sessment of core movement and movements between endplates and core are not performed. Sequential imaging dem-onstrating the pattern of motion is needed to assess thequality of motion that may affect the survivorship of theimplant components and long-term results.
In the absence of a compressive preload, we observeda lift-off of the upper prosthesis end plate from the coreor of the core from lower end plate in 9 of the 10 TDRs(4 of 5 L5-S1 and 5 of 5 L4-L5 TDRs). This phenomenonwas absent (0 of 10 TDRs) when a physiological preloadwas applied. This demonstrates the importance of muscleloading in maintaining TDR function for an unconstraineddevice such as the Charite. Because the Charite prosthesisis designed with two articulating surfaces, angulation be-tween the upper and lower end plates can be the result ofangulation between the upper end plate and the core, angu-lation between the lower end plate and the core, or angula-tion between both end plates and the core. In 5 of 10 TDRsunder a physiologic preload we observed angular motionbetween both prosthesis end plates and core, with transla-tion of the core estimable by our assessment technique.In the remaining 5 of 10 TDRs, the amount of core trans-lation was below the threshold of estimation from the fluo-roscopic images. The predominant angular motion withinthe prosthesis was seen at the articulation between the up-per end plate and the core in all TDRs when full contact ofall three components was reached.
The pattern of intervertebral load-displacement curvesfor implanted segments was different from the intact casein 8 of 10 TDRs; instead of a gradually changing motionpattern of a normal lumbar segment, the TDR displayed re-gions of both relatively small and relatively large changesin angle with gradual moment application (Fig. 3). The mo-tion response of an intact segment to applied moments isgoverned by bony and soft-tissue constraints. The disrup-tion of some of these structures, most notably the anteriorlongitudinal ligament and the anterior annulus, during theinsertion of the Charite TDR decreases this constraint. As

596 P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
Fig. 2. Prosthesis component motion patterns (PCMPs). (A) Angular motion predominantly between the upper end plate and core, with little or no visible
core translation (PCMP1). (B) Lift-off of upper prosthesis end plate from core or of core from lower end plate (PCMP2). (C) Core entrapment, resulting in
a locked core over a portion of the range of motion (PCMP3). (D) Angular motion between both the upper and lower end plates and core, with visible core
translation (PCMP4).
a result, a larger angular travel was seen in the absence ofphysiologic compressive preload for the same applied mo-ment for the TDR case (through lift-off at end plate/core in-terface in extension) when compared with the intact case.Under a compressive preload, we observed entrapmentand locking of the polyethylene core over a portion of thesagittal plane motion. This phenomenon is reflected in therelatively flat portion of the load-displacement curves in
the presence of a preload (Fig. 3). Once the core was re-leased, a large angular change was noted, reflected in thesharp rise of the load-displacement curves. The effect thatthese intervertebral and prosthesis component motion pat-terns will have on the long-term outcome is not known,but nonuniform motion could influence the wear behaviorof the implant. Other observed movement patterns (pre-dominant angular motion at one articulation with only

597P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
a small amount of core translation) may also influence theload-sharing within the implanted segment and at adjacentlevels.
The TDR seemed to function differently depending onthe segment level (L5-S1 vs. L4-L5). While the resultantflexion-extension range of motion was similar at the twolevels (Tables 4 and 5), there was a trend (although not sta-tistically significant) for a difference between the L4-L5and L5-S1 levels in terms of the frequencies of prosthesiscomponent motion patterns (Table 7). A likely explanationfor this may be the natural morphologic differences be-tween the two disc spaces. The final segmental lordosis af-ter TDR was significantly larger at L5-S1 than at L4-L5(Table 6). This may have placed the prosthesis in subopti-mal angular alignment (‘‘lordosing’’ of the implant). Inour laboratory experience, it appeared that in order to getangular motion between both the upper and lower endplates and core with core translation, the end plates mustcross the parallel point and go into flexion. This is less like-ly to occur if the prosthesis end plates are substantially ex-tended relative to each other in the unloaded position of thesegment. Physiologic variations in sacral inclinations andlordosis at the L5-S1 level may make it impossible toachieve parallel end plates despite the currently availableoptions of prosthesis end plate angles.
Likely factors affecting the function of the prosthesis in-clude implant placement, segmental lordosis, intraoperativechange in lordosis, and magnitude of physiologic compres-sive preload on the implant. We found that restoring theposterior disc height by resecting enough of the posteriortethers to make the end plates parallel during the distractionphase of the implantation is vital. However, the selection ofthe end plate lordosis angle and its relationship to coreheight are issues that need further investigation. The choiceof end plate angles and the resulting lordosis under loadwill affect the angular orientation of the prosthesis relativeto the load-bearing line, and may result in nonoptimum mo-tion. In an effort to restore lordosis to the lumbar spine,‘‘lordosing’’ the implant must be avoided. This puts the
Table 7
Frequency distribution of prosthesis component motion patterns
Prosthesis component
motion pattern
Spine Segment PCMP1 PCMP2 PCMP3 PCMP4
L5-S1 (0 N) 5/5 4/5 1/5 0/5
L4-L5 (0 N) 4/5 5/5 0/5 1/5
L5-S1 (400 N) 3/5 0/5 4/5 2/5
L4-L5 (400 N) 2/5 0/5 3/5 3/5
PCMP5prosthesis component motion pattern.
PCMP1: angular motion predominantly between the upper end plate
and core, with little or no visible core translation (Fig. 2A); PCMP2:
lift-off of upper prosthesis end plate from core or of core from lower
end plate (Fig. 2B); PCMP3: core entrapment, resulting in a locked core
over a portion of the rang of motion (Fig. 2C); PCMP4: angular motion
between both the upper and lower end plates and core, with visible core
translation (Fig. 2D).
segment in maximum extension in the neutral standing pos-ture, causing it to lock and yield nonoptimum motion pat-terns. The effect of increased lordosis of the implantedsegment, observed in the majority of specimens in our lab-oratory experiment, is consistent with the clinical experi-ence of others [16,19]. Although the patient’s overallsagittal alignment and balance may be preserved in theshort term [19], this will produce a decrease of lordosisin the adjacent segments. The increase in segmental lordo-sis after Charite TDR and alteration in the alignment of ad-jacent segments may influence long-term outcome [19].
It is important that the two end plates must not be offsetwith respect to each other in the anterior-posterior directionin the sagittal plane. This might occur when the end platesare impacted deeper separately at final seating or during re-moval of insertion forceps. This occurred in one of our testspecimens (L5-S1, specimen 5) and resulted in the core be-ing trapped and locked in a tilted position, perhaps as a re-sult of shear loading of the implant. Interestingly, this didnot adversely affect the range of motion of that segment(Tables 4 and 5), but led to the motion taking place only be-tween the upper end plate and the core without core trans-lation. We would recommend that careful attention be paidto the final placement and orientation of the end plates andcore.
In the present study, the sample size of 5 per level al-lowed us to detect a statistically significant effect of TDRson the flexion-extension range of motion of lumbar seg-ments. However, power analysis showed that a larger sam-ple size (n57–10) may be needed to reach conclusions with80% power when comparing the frequencies of prosthesiscomponent motion patterns as a function of segmentallevel.
Careful attention should be paid to the alignment of thepreload path in the experimental setup in order to minimizethe moments and shear forces induced by the preload alongthe mid-plane of the discs, thereby decreasing the effect ofsuch experimental artifact loads on the specimen’s range ofmotion [8]. In the present study, it was possible to align thepreload path such that an average angular change in thespecimen’s lordosis of less than 2 degrees resulted whena 400 N preload was applied in the neutral posture. The ef-fect of preload on range of motion might be different fromthat reported in the present study depending on how wellthe follower preload path was optimized.
A compressive preload applied along a follower loadpath that is not properly aligned (optimized) has the poten-tial to force the specimen towards its extension or flexionlimits, thereby artificially constraining the specimen’s mo-tion. A large increase in the segmental lordosis after TDRcan place the preload path posterior to the implant. We in-vestigated the effect of realigning the preload path on themotion response of the Charite disc. In two specimens,the preload cables were moved anteriorly such that whena preload of 400 N was applied, the specimen’s sagittalalignment (lordosis) approximated that of the intact spine

598 P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
Fig. 3. Load versus angular displacement graphs. (A) An L5-S1 motion segment. (B) An L4-L5 motion segment.

599P. O’Leary et al. / The Spine Journal 5 (2005) 590–599
under 400 N preload. This was an attempt to simulate an invivo situation where the patient may have a righting reflexor other muscle compensatory mechanisms that allow him/her to maintain a balanced postoperative spinal alignment[19]. The range of motion results indicated that realignmentof the preload path increased the range of motion at L4-L5by at most 1–2 degrees. Interestingly, the prosthetic compo-nent motion patterns at the L5-S1 and L4-L5 levels wereunchanged after realignment of the preload path. Thus,the results of prosthesis motion appear to be unaffectedby any experimental artifact that may be caused by themethod of applying a follower preload.
The study addressed only the immediate response of themotion segment after disc prosthesis insertion. The amountof preload produced by annular pre-tensioning after inser-tion of the implant is not known. No assumption was madein the present study regarding the magnitude of the preloadon the implant caused by disc space distraction. The pre-load caused by annular pre-tensioning served as the ‘‘base-line control’’ in our experiment. That is, testing the TDRunder 0 N external preload corresponded to testing theTDR under the preload resulting from annular pre-tension-ing alone. The tension in the annulus may decrease overtime as has been observed in previous studies [20,21]. Thisstudy did not account for the possible effect of long-termrelaxation of the annulus on the response of the TDR. Otherfactors that may influence its motion response in the longterm include settling of the implant into the vertebra overtime, heterotrophic ossification, postoperative fibrosis, andcore wear and deformation over time.
Conclusions
Charite TDR restored near normal quantity of flexion-extension range of motion under a constant physiologicpreload; however, the quality of segmental motion differedfrom the intact case over the flexion-extension range. Al-though some TDRs showed visual evidence of core transla-tion, the predominant angular motion within the prosthesisoccurred between the upper end plate and the polyethylenecore. Likely factors affecting the function of the ChariteTDR include implant placement and orientation, intraoper-ative change in lordosis, and magnitude of physiologiccompressive preload. Further work is needed to assess theeffects of the prosthesis motion patterns identified in thestudy on the load sharing at the implanted level and poly-ethylene core wear.
References
[1] McAfee PC, Fedder IL, Saiedy S, Shucosky EM, Cunningham BW.
Experimental design of total disc replacement: experience with
a prospective randomized study of the SB Charite. Spine 2003;
28(20):S153–62.
[2] Link HD. History, design and biomechanics of the LINK SB Charite
artificial disc. Eur Spine J 2002;11:S98–S105.
[3] Cunningham BW. Basic scientific considerations in total disc arthro-
plasty. Spine J 2004;4:219S–30S.
[4] Geisler FH, Blumenthal SL, Guyer RD, et al. Neurological complica-
tions of lumbar artificial disc replacement and comparison of clinical
results with those related to lumbar arthrodesis in the literature: re-
sults of a multicenter, prospective, randomized investigational device
exemption study of the Charite intervertebral disc. J Neurosurg Spine
2004;1(2):143–54.
[5] Griffith SL, Shelokov AP, Buttner-Janz K, LeMaire JP, Zeegers WS.
A multicenter retrospective study of the clinical results of the LINK
SB Charite intervertebral prosthesis: the initial European experience.
Spine 1994;19(16):1842–9.
[6] Guyer RD, McAfee PC, Hochschuler SH, et al. Prospective random-
ized study of the Charite artificial disc: data from two investigational
centers. Spine J 2004;4:252S–9S.
[7] Patwardhan AG, Havey RM, Meade KP, Lee B, Dunlap B. A follower
load increases the load-carrying capacity of the lumbar spine in com-
pression. Spine 1999;4(10):1003–9.
[8] Patwardhan AG, Havey RM, Carandang G, et al. Effect of compres-
sive follower preload on the flexion-extension response of the human
lumbar spine. J Orthop Res 2003;21:540–6.
[9] Patwardhan AG, Lee B, Meade KP. Frontal plane response of the
lumbar spine subjected to a follower loaddrole of muscles. J. Bio-
mech Engin 2001;123:212–7.
[10] Shirazi-Adl A, Parnianpour M. Load-bearing and stress analysis of
the human spine under a novel wrapping compression loading. Clin
Biomech 2000;15:718–25.
[11] Schultz A. Loads on the lumbar spine. In: Jayson MIV, editor. The lum-
bar spine and back pain. Edinburgh: Churchill Livingstone, 1987:
204–14.
[12] Nachemson A. Lumbar intradiscal pressure. In: Jayson MIV, editor.
The lumbar spine and back pain. Edinburgh: Churchill Livingstone,
1987:191–203.
[13] Zeegers WS. LINK lumbar artificial discdoperative technique. In:
Buttner-Janz K, Hochschuler SH, McAfee PC, editors. The artificial
disc. New York, NY: Springer, 2003:115–38.
[14] Ahrens J, Shelokov AP, Carver JL. Normal joint mobilities main-
tained with an artificial disc prosthesis. Brussels: International Soci-
ety for the Study of the Lumbar Spine, 1998.
[15] Taksali S, Grauer JN, Vaccaro AR. Material considerations for inter-
vertebral disc replacement implants. Spine J 2004;4:231S–8S.
[16] van Ooij A, Oner FC, Verbout AJ. Complications of artificial disc re-
placement: a report of 27 patients with the SB Charite disc. J Spinal
Disord Tech 2003;16:369–83.
[17] Cinotti G, David T, Postacchini F. Results of disc prosthesis after
a minimum follow-up period of 2 years. Spine 1996;21(8):995–1000.
[18] Santos EG, Polly DW, Mehbod AA, Saleh KJ. Disc arthroplasty: les-
sons learned from total joint arthroplasty. Spine J 2004;4:182S–9S.
[19] Cakir B, Richter M, Kafer W, Puhl W, Schmidt R. The impact of total
lumbar disc replacement on segmental and total lumbar lordosis. Clin
Biomech 2005;20(4):357–64.
[20] Woo SLY, Gomez MA, Woo YK, Akeson WH. Mechanical properties
of tendons and ligaments. I. Quasi-static and nonlinear viscoelastic
properties. Biorheology 1982;19:385–96.
[21] Havey RM, Voronov LI, Gaitanis I, et al. Relaxation response of lum-
bar spine segments undergoing annular distraction: implications to
anterior lumbar interbody implant stability. Orthopedic Research So-
ciety, San Francisco, CA, March 7–10, 2004.