RESPIRATORY SYSTEM
87
RESPIRATORY SYSTEM dr. Sri Lestari Sulistyo Rini, MSc
-
Upload
gay-calhoun -
Category
Documents
-
view
22 -
download
3
description
RESPIRATORY SYSTEM. dr. Sri Lestari Sulistyo Rini, MSc. Respiratory System. Functions of the Respiratory System. Exchange O 2 Air to blood Blood to cells Exchange CO 2 Cells to blood Blood to air Regulate blood pH Vocalizations Protect alveoli. Function of the Nose. - PowerPoint PPT Presentation
Transcript of RESPIRATORY SYSTEM

RESPIRATORY SYSTEM
dr. Sri Lestari Sulistyo Rini, MSc

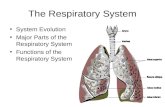
Respiratory System

Functions of the Respiratory System
Exchange O2
Air to blood Blood to cells
Exchange CO2 Cells to blood Blood to air
Regulate blood pH
Vocalizations Protect alveoli

Function of the Nose
The only externally visible part of the respiratory system that functions by: Providing an airway for respiration Moistening and warming the entering air Filtering inspired air and cleaning it of
foreign matter Serving as a resonating chamber for
speech Housing the olfactory receptors

Conducting Zone: Bronchi
The carina of the last tracheal cartilage marks the end of the trachea and the beginning of the right and left bronchi
Air reaching the bronchi is: Warm and cleansed of impurities Saturated with water vapor
Bronchi subdivide into secondary bronchi, each supplying a lobe of the lungs
Air passages undergo 23 orders of branching in the lungs


Respiratory Zone
Defined by the presence of alveoli; begins as terminal bronchioles feed into respiratory bronchioles
Respiratory bronchioles lead to alveolar ducts, then to terminal clusters of alveolar sacs composed of alveoli
Approximately 300 million alveoli: Account for most of the lungs’ volume Provide tremendous surface area for gas
exchange


Breathing (ventilation): air in to and out of lungs
External respiration: gas exchange between air and blood
Internal respiration: gas exchange between blood and tissues
Cellular respiration: oxygen use to produce ATP, carbon dioxide as waste
Four Respiration Processes

Lung Volumes: Spirometer Measurements


PULMONARY VOLUMES, CAPACITIES, AND RATES
SPIROGRAM
Volumes tidal volume (500 ml)
anatomical dead space (150 ml)alveolar ventilation (350 ml)physiological dead space
inspiratory reserve volume (3000 ml)expiratory reserve volume (1200 ml)residual volume (1300 ml)
Capacities total lung capacity (TV+IRV+ERV+RV)vital capacity (TV+IRV+ERV) (4700 ml)inspiratory capacity (TV+IRV)functional residual capacity (RV+ERV)
Ratesmaximum voluntary ventilation = TV x breaths/minutealveolar ventilation rate = alveolar ventilation x breaths/minute
IRV
ERV
TV
RVmaximum expiration
VC TLC
6000 ml
5000 ml
4000 ml
3000 ml
2000 ml
1000 ml
maximum inspiration

Lung Volumes: Spirometer Measurements

PHYSIOLOGY OF RESPIRATION
Concepts related to pulmonary ventilation (breathing)
- inspiration (inhalation) vs. expiration (exhalation)- atmospheric pressure- intrapulmonic pressure- pressure gradient

Boyle’s Law
Boyle’s law – the relationship between the pressure and volume of gases
P1V1 = P2V2
P = pressure of a gas in mm Hg V = volume of a gas in cubic millimeters Subscripts 1 and 2 represent the initial
and resulting conditions, respectively

Pressure Relationships in the Thoracic Cavity
Respiratory pressure is always described relative to atmospheric pressure
Atmospheric pressure (Patm) Pressure exerted by the air surrounding the
body Negative respiratory pressure is less than Patm Positive respiratory pressure is greater than Patm

Pressure Relationships in the Thoracic Cavity
Intrapulmonary pressure (Ppul) – pressure within the alveoli
Intrapleural pressure (Pip) – pressure within the pleural cavity

Pressures
Atmospheric pressure – 760 mm Hg, 630 mm Hg here
Intrapleural pressure – 756 mm Hg – pressure between pleural layers
Intrapulmonary pressure – varies, pressure inside lungs


Alveolar Pressure Changes


Inspiration
Begins with the contraction of the diaphragm and the external intercostals
This causes thoracic volume to Which causes lung volume to Which causes lung pressure to Now Palv is <Patm so air will flow
down its pressure gradient and enter the lungs.
Inspiration ends when Palv=Patm

Inspiration
The diaphragm and external intercostal muscles (inspiratory muscles) contract and the rib cage rises
The lungs are stretched and intrapulmonary volume increases
Intrapulmonary pressure drops below atmospheric pressure (1 mm Hg)
Air flows into the lungs, down its pressure gradient, until intrapleural pressure = atmospheric pressure


Pressure – Volume Relationships
As vol. , pressure As vol. , pressure This is given by Boyle’s
Law which says: P1V1 = P2V2
Why does this occur? Remember, pressure
equals force/areaP = Force/Area
So, in this equation as A gets larger P must get smaller

Active processBoyle’s Law
INSPIRATION
air molecule
decrease volume increase pressure
increase volume decrease pressure
FORCED INSPIRATIONRESTING INSPIRATION
external intercostals(11 pairs)
diaphragm
sternocleidomastoidscalenes
Inspiratory musclesPhrenic nerves (C3-5)Thoracic nerves (T1 – T11)
thoracic volume pleural volume intrapleural pressure lung volume intrapulmonic pressureair flow into the lungs
760 mmHg
760 mmHg
760 mmHg
758 mmHg
BEFORE INSPIRATION DURING INSPIRATION
Process

Expiration
Inspiratory muscles relax and the rib cage descends due to gravity
Thoracic cavity volume decreases Elastic lungs recoil passively and
intrapulmonary volume decreases Intrapulmonary pressure rises above
atmospheric pressure (+1 mm Hg) Gases flow out of the lungs down the
pressure gradient until intrapulmonary pressure is 0

Expiration
Quiet expiration is a passive process that is due to the elasticity of the lungs. What pressure and volume
changes occur during quiet expiration?
Forced expiration is an active process due to contraction of oblique and transverse abdominus muscles, internal intercostals, and the latissimus dorsi.

Passive process at rest
EXPIRATION
internal intercostals(11 pairs)
internal intercostals (11 pairs)rectus abdominisabdominal obliquestransversus abdominis
Forced expiration
thoracic volume pleural volume intrapleural pressure lung volume intrapulmonic pressureair flow of the lungs
Process
external abdominal oblique
internal abdominal oblique
transversus abdominis
rectus abdominis
760 mmHg
762 mmHg
elastic recoilsurface tension

Factors that influence pulmonary air flow
F = P/R Diameter of airways, esp.
bronchioles Sympathetic & Parasympathetic NS

Factors Affecting Ventilation Airway Resistance Diameter Mucous blockage Bronchoconstrictio
n Bronchodilation Alveolar
compliance Surfactants Surface tension
Alveolar elasticity

Airway Resistance
Due primarily to diameter of the conducting tubes.
How increased parasympathetic affect tube diameter? How would it affect airway resistance?
Histamine causes massive bronchoconstriction.
When might one experience massive histamine release? Why treat it with epinephrine?
Local accumulations of mucus, infectious materials or solid tumors are also sources of airway resistance.

DEAD SPACE Tidal volume NOT used in gas exchange Anatomical: conducting pathways
(150mls) Alveolar: gas reach alveoli, not enough blood supply due to: - Pulmonary embolism - Non vascular air space
Physiological dead space= anatomical + alveolar

Types of Dead Space
Anatomic dead space That contained in the conducting airways
Alveolar dead space That contained in the respiratory portion
of the lung Physiologic dead space
The anatomic dead space plus alveolar dead space

Efficiency of Breathing: Normal & High Demand
Total Pulmonary Ventilation(rate X tidal vol about 6 L/min)
Alveolar ventilation(– dead air space – 4.5 L/min)
Little variation [O2] & [CO2] Exercise- High Demand
Depth of breathing Use inspiratory reserve

Matching Ventilation with Alveolar Blood Flow (Perfusion)
Mostly local regulation Low [O2] in alveoli vasoconstriction of
arteriole Reduced blood flow at rest
(lung apex ) saves energy
High blood [CO2] bronchodilation

VENTILATON-PERFUSION MATCHING
Alveolar gas
V
Q Capillary flow

Matching Ventilation and Perfusion
Required for exchange of gases between the air in the alveoli and the blood in pulmonary capillaries
Two factors interfere with the process: Dead air space and shunt
The blood oxygen level reflects the mixing of blood from alveolar dead space and physiologic shunting areas as it moves into the pulmonary veins

Efficiency of Breathing: Normal & High Demand
Figure 17-2 g: Anatomy Summary

FICK’S LAW Rate of transfer of a gas through a
sheet of tissue is proportional to tissue area difference in gas partial pressure diffusion constant
inversely proportional to tissue thickness
ΔPjaringan tebal
kL.gasV
difusioefperm ..

Respiratory Membrane
This air-blood barrier is composed of: Alveolar and capillary walls Their fused basal laminas
Alveolar walls: Are a single layer of type I epithelial cells Permit gas exchange by simple diffusion Secrete angiotensin converting enzyme
(ACE) Type II cells secrete surfactant

Composition of the Alveolar Structures
Type I alveolar cells Flat squamous epithelial cells across
which gas exchange takes place Type II alveolar cells
Produce surfactant, a lipoprotein substance that decreases the surface tension in the alveoli and allows for greater ease of lung inflation

Respiratory Membrane

Factors Affecting Alveolar-Capillary Gas Exchange
Surface area available for diffusion Thickness of the alveolar-capacity
membrane Partial pressure of alveolar gases Solubility and molecular weight of
the gas

Lung Compliance
The ease with which lungs can be expanded
Specifically, the measure of the change in lung volume that occurs with a given change in transpulmonary pressure
Determined by two main factors Distensibility of the lung tissue and
surrounding thoracic cage Surface tension of the alveoli

Lung Compliance
Lung compliance (C) = (ΔV)/(ΔP) The change in lung volume (ΔV)
that can be accomplished with a given change in respiratory pressure (ΔP)

Compliance is the ease with which the lungs and thoracic wall can be expanded during inspiration.
COMPLIANCE
elasticitysurface tension
Related to two factors:
destroys lung tissue (emphysema)fills lungs with fluid (pneumonia)produces surfactant deficiency (premature birth, near-drowning)interferes with lung expansion (pneumothorax)
Compliance is decreased with any condition that:

Alveolar Surface Tension
Surface tension – the attraction of liquid molecules to one another at a liquid-gas interface
The liquid coating the alveolar surface is always acting to reduce the alveoli to the smallest possible size
Surfactant, a detergent-like complex, reduces surface tension and helps keep the alveoli from collapsing

Factors That Diminish Lung Compliance
Scar tissue or fibrosis that reduces the natural resilience of the lungs
Blockage of the smaller respiratory passages with mucus or fluid
Reduced production of surfactant Decreased flexibility of the thoracic
cage or its decreased ability to expand


Pons centers Influence and modify activity of the
medullary centers Smooth out inspiration and expiration
transitions and vice versa Pneumotaxic center – continuously
inhibits the inspiration center Apneustic center – continuously
stimulates the medullary inspiration center
Control of Respiration: Pons Respiratory Centers


Respiration Regulation In the pons, there are 2 more respiratory
centers: the pneumotaxic and the apneustic centers.
The apneustic center acts to prolong inspiration or cause breath holding in the inspiratory phase.
The pneumotaxic center inhibits the apneustic center and promotes exhalation
They both act to smooth the transition btwn inspiration and expiration.

Control of Breathing
Automatic regulation of ventilation Controlled by input from two types of
sensors or receptors: Chemoreceptors: monitor blood levels of
oxygen, carbon dioxide and adjust ventilation to meet the changing metabolic needs of the body
Lung receptors: monitor breathing patterns and lung function

What factors affect breathing?
Respiratory control centers are sensitive tocarbon dioxide and hydrogen levels
If those rise (in blood), breathing rate increasesLow blood oxygen can also be detected
Hyperventilation lowers blood carbon dioxidelevels; can lead to blood alkalosis(slows breathing rate)


Respiratory Reflexes Respiratory center activity is modified by:1. Chemoreceptors sensitive to the Pco2, pH,
or Po2 of the blood or CSF2. BP changes detected in the carotid or
aortic sinuses3. Lung stretch receptors (Hering-Breuer
Reflex)4. Irritating physical or chemical stimuli in
the respiratory tract5. Other sensations (pain, emotions)

Herring-Breuer Reflex
Limits the degree of inspiration and prevents overinflation of the lungs Infants
Reflex plays a role in regulating basic rhythm of breathing and preventing overinflation of lungs
Adults Reflex important only when tidal volume
large as in exercise

Respiration Regulation
There’s reciprocal inhibition btwn the inspiratory neurons and the expiratory neurons
During quiet respiration, the DRG is active for about 2 seconds (inspiration) and then is inactive for 3 seconds (expiration)

Respiration Regulation
During forced respiration, the level of DRG activity increases to where it activates VRG neurons.
Thus, we’ll have our normal inspiratory muscles plus our accessory inspiratory muscles activated.
At the end of the active inspiration, the VRG expiratory neurons initiate active expiration.

Depth and Rate of Breathing
Inspiratory depth is determined by how actively the respiratory center stimulates the respiratory muscles
Rate of respiration is determined by how long the inspiratory center is active
Respiratory centers in the pons and medulla are sensitive to both excitatory and inhibitory stimuli

Control of Respiration: Medullary Respiratory Centers

Depth and Rate of Breathing: Reflexes
Pulmonary irritant reflexes – irritants promote reflexive constriction of air passages
Inflation reflex (Hering-Breuer) – stretch receptors in the lungs are stimulated by lung inflation
Upon inflation, inhibitory signals are sent to the medullary inspiration center to end inhalation and allow expiration

Depth and Rate of Breathing: PCO2
Changing PCO2 levels are monitored by chemoreceptors of the brain stem
Carbon dioxide in the blood diffuses into the cerebrospinal fluid where it is hydrated

Depth and Rate of Breathing: PCO2
Resulting carbonic acid dissociates, releasing hydrogen ions
PCO2 levels rise (hypercapnia) resulting in increased depth and rate of breathing

Factors Affecting Breathing

Depth and Rate of Breathing: Higher Brain Centers
Hypothalamic controls – act through the limbic system to modify rate and depth of respiration Example: breath holding that occurs in anger
A rise in body temperature acts to increase respiratory rate
Cortical controls – direct signals from the cerebral motor cortex that bypass medullary controls Examples: voluntary breath holding, taking a
deep breath

NEGATIVE FEEDBACK CONTROL
CONTROLLED CONDITIONA stimulus or stress disrupts
homeostasis by causing a decrease in arterial oxygen or an increase in carbon
dioxide and/or hydrogen ions
RECEPTORChemosensitive neurons in medulla and
chemoreceptors in aortic and carotid bodies respond to changes and direct nerve impulses to the control center
CONTROL CENTERInspiratory neurons of medulla interpret
sensory input and generate nerve impulses that pass ultimately to effectors
EFFECTORSMuscles of inspiration contract more often
and more forcefully (hyperventilation)
RETURN TO HOMEOSTASISHyperventilation results in increase in
arterial oxygen and/or pH, and/or decrease in arterial carbon dioxide



Modifying Respiration

Depth and Rate of Breathing: PCO2
Hyperventilation – increased depth and rate of breathing that: Quickly flushes carbon dioxide from the blood Occurs in response to hypercapnia
Though a rise in CO2 acts as the original stimulus, control of breathing at rest is regulated by the hydrogen ion concentration in the brain
Hypoventilation – slow and shallow breathing due to abnormally low PCO2 levels Apnea (breathing cessation) may occur until
PCO2 levels rise

Pco2, Po2, and pH
Central and peripheral chemoreceptors The central are located on the medulla The peripheral are located in the carotid
sinus and aortic arch. The central respond to pH (indirectly to
CO2) and are the most important. There are peripheral receptors for pH,
Pco2 and Po2. Of these pH and Pco2 are more important (but
still less so than the central chemoreceptors)

High Pco2 = Hypercapnia
When Pco2 rises, it will activate peripheral Pco2 receptors, peripheral pH receptors, and central pH receptors.
All will respond by increasing respiration rate and depth.
Decrease in plasma pH independent of Pco2 changes will activate peripheral pH receptors but not central ones. Why?

CARBON DIOXIDE IN THE LUNGS
H+ + HCO3- H2CO3 H20 + CO2
carbonic anhydrase
HCO3-
CO2Cl-
CAPILLARY ENDOTHELIUM
4O2-HbH-HbO2
ALVEOLUS
diffusion
diffusion
1.5% O2
dissolved in plasma
98.5% O2
goes to Hb
CO2
Total7% from plasma23% from globin
70% from bicarbonate



Depth and Rate of Breathing: Arterial pH
Changes in arterial pH can modify respiratory rate even if carbon dioxide and oxygen levels are normal
Increased ventilation in response to falling pH is mediated by peripheral chemoreceptors
Acidosis may reflect: Carbon dioxide retention Accumulation of lactic acid Excess fatty acids in patients with diabetes
mellitus Respiratory system controls will attempt to raise
the pH by increasing respiratory rate and depth

Respiratory Adjustments: Exercise
As exercise begins: Ventilation increases abruptly, rises slowly,
and reaches a steady state When exercise stops:
Ventilation declines suddenly, then gradually decreases to normal
Neural factors bring about the above changes, including: Psychic stimuli Cortical motor activation Excitatory impulses from proprioceptors in
muscles

Diffusion Through Respiratory Membrane
Gases are exchanged between alveolar air and capillary blood because of differences in partial pressure

Oxygen-HemoglobinDissociation Curve at
Rest

Bohr effect:


Shifting the Curve


Regulation of Blood pH and Gases

TERIMA KASIH


![Respiratory System [โหมดความเข้ากันได้] · PATHOLOGY OF RESPIRATORY SYSTEM นพ. อรรณพ นาคะป ท Respiratory system U it](https://static.fdocuments.us/doc/165x107/5fa578efd4e80f055f6b3401/respiratory-system-aaaaaaaaaaaaaaaaaa-pathology.jpg)