
Respiratory System
52
HINF 2502 (Clinical Processes and Decision Making) © Hadi Kharrazi, Dalhousie University 1 Lecture #5 HINF 2502 (Clinical Processes and Decision Making) [email protected] http://flame.cs.dal.ca/~kharrazi/ Respiratory System
-
Upload
guest2379201 -
Category
Health & Medicine
-
view
4.081 -
download
1
Transcript of Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 1
Lecture #5HINF 2502 (Clinical Processes and Decision Making)
[email protected]://flame.cs.dal.ca/~kharrazi/
Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 2
Lecture in a Nutshell
1. Structure and Function of the Normal Respiratory System2. Evaluation of the Patient with Respiratory Disease 3. Diagnostic Tests and Procedures in the Patient with Respiratory
Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 3
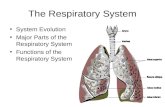
1. Structure and Function of the Normal Respiratory System
Gross Anatomy • The primary function of the lungs is gas exchange. The entire
cardiac output goes through the lungs, where oxygen is absorbed and carbon dioxide is removed from blood. Gas exchange requires adequate cardiac output, alveolar ventilation, alveolar-capillary surface area, and regional matching of blood flow to ventilation. In the normal lung, alveolar-capillary surface can double from 50 m2 to 100 m2 by recruiting closed capillaries and alveoli. Lung disease can affect ventilation, pulmonary blood flow, or alveolar-capillary surface area and usually reduces the ability of the lung to match pulmonary blood flow with ventilation. These changes compromise the lungs' ability to meet the body's demand for gas exchange.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 4
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 5
The Airway• Inspired air travels through the nose and pharynx, where it
is heated, humidified, and filtered of particles greater than 10 μm in diameter and soluble gases are removed. Entrance to the trachea is through the larynx, which is open during ventilation and closed and covered by the epiglottis during swallowing and Valsalva maneuvers.
• The trachea, which is 10 to 12 mm in diameter, is held open by anterior, U-shaped, incomplete, cartilage rings. The trachea divides into the two mainstem bronchi at the level of the sternomanubrial junction. The right mainstem bronchus takes off at a less acute angle than the left, and therefore foreign bodies are more commonly aspirated into the right lung.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 6
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 7
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 8
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 9
• The large airways are supported by circumferential cartilage rings and continue to branch, with the cartilage disappearing in the smaller airways. These bronchial branches are conducting airways and do not participate in gas exchange.
• At about the 18th branch, the airways become respiratory bronchioles and contain increasing numbers of alveolar sacs. They continue to branch, becoming alveolar ducts, which ultimately terminate in alveoli.
• Gas exchange takes place in the branches from the respiratory bronchioles to the alveoli, called the respiratory zone. After the tenth branch, the total cross-sectional area of the airways increases rapidly and resistance to air flow decreases.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 10
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 11
• Airflow is laminar proximal to the respiratory zone, where turbulent flow begins and diffusion becomes the dominant mechanism of gas movement.
• The alveolar lining cells are predominantly flat, type I pneumocytes, which rest on a very thin basement membrane and allow rapid diffusion of gases to and from the adjacent capillary blood.
• Type II pneumocytes, about 5% of the alveolar lining cells, are round and secrete surfactant, a complex lipoprotein that coats the alveolar surface and decreases surface tension, thus stabilizing alveoli against collapse at low volumes. Type II cells are capable of regeneration and repair and are also the precursors of type I cells.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 12
• The lungs have a dual circulation:
1. The bronchial circulation originates from the aorta and, under systemic pressure, supplies nutrient flow to lung structures proximal to alveoli. One-third of the venous outflow from the bronchial circulation returns through bronchial veins to the right side of the heart, similar to other organs perfused by systemic blood. The remainder of the bronchial circulation drains into the pulmonary veins, which empty into the left atrium, forming part of the normal anatomic right-to-left shunt.
2. The pulmonary circulation is a low-resistance circuit that receives the entire output of the right cardiac ventricle. Pulmonary artery pressure and pulmonary vascular resistance are about one-tenth those of the systemic circulation. Pulmonary arteries and arterioles are thin walled and have much less smooth muscle than systemic arteries. At the level of the alveolar ducts, the pulmonary arterioles terminate in a meshwork of capillaries, which form a sheet of blood surrounding the alveoli and create the large surface area necessary for gas exchange. Blood returns to the heart through pulmonary veins that course between lung lobules, coalesce into four main pulmonary veins, and empty into the left atrium.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 13
Ventilation is the movement of air in and out of the lungs. The volume of air in the lungs is determined by the balance between the outward elastic force of the thoracic cage and the inward elastic recoil of the lungs.
• During inspiration, active contraction of the respiratory muscles increases intrathoracic volume and creates subatmospheric pressure in the pleural space and alveoli. Air enters the lung down the pressure gradient between atmospheric and intrathoracic pressure.
• Exhalation is passive in normal lungs and begins when inspiratory muscles relax. Intrinsic elastic recoil passively returns the lungs to their resting volume, where alveolar pressure and ambient pressure are equal. In disease states such as emphysema, when the elastic recoil of the lung is greatly diminished, active contraction of the expiratory muscles is required to empty enough air from the lungs to permit ventilation.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 14
• The primary respiratory muscle is the diaphragm. The so-called accessory muscles of respiration-the intercostal, sternocleido-mastoid, scalene, and abdominal muscles-normally contribute little. At rest, the diaphragm is dome shaped, curving into the thoracic cavity. During contraction it flattens, increasing the thoracic volume and distending the abdominal wall.
• If the lungs are hyperinflated because of trapped gas from emphysema or asthma (obstructive lung diseases), the diaphragm is flat or inverted at end expiration and its contraction will not produce an appreciable change in thoracic volume. In this situation the accessory muscles of respiration, the scalenes and sternocleidomastoids, contract and elevate the anterior chest wall.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 15
• Respiratory muscles must overcome both elastic and resistive forces. The opposing elastic forces of the chest wall (outward force) and lungs (inward force) determine the resting lung volume at the end of passive expiration, called the functional residual capacity (FRC). The FRC should be less than 50% of the total lung capacity (TLC), which is the total amount of air that the lung can contain.
• Elasticity is usually measured as its inverse function, compliance. Compliance is the change in lung volume produced by a given change in transpulmonary pressure. In normal lungs at FRC, it takes about 1 cm H2O pressure to inflate the lungs 200 mL. Compliance then would be 200 mL/cm H2O, decreasing as lung volume increases toward TLC. Compliance is decreased in diseases such as pulmonary fibrosis or pulmonary edema, which restrict lung volume expansion. Compliance is increased in emphysema because of the loss of elastic recoil
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 16
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 17
• When compliance is decreased, the work of breathing is increased, because of the increased pressure required to inflate the lungs.
• In diseases such as emphysema in which compliance is increased, the work of breathing is also increased during inspiration as a result of the loss of mechanical advantage from hyperinflation and flattened diaphragms, and during expiration because decreased lung elastic recoil requires active muscle contraction to empty the lungs in preparation for the next inspiration.
• In patients with severe obstructive or restrictive lung disease, the work of breathing may be a major contributor to the resting metabolic rate. In extreme cases, this increase in energy expenditure can result in weight loss known as pulmonary cachexia. With normal lungs, the work of breathing uses only 4% to 5% of the total calories burned, but in severe lung disease up to 30% of the total-body oxygen consumption can be consumed by the work of breathing.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 18
• Airway resistance is inversely related to the total cross-sectional area of the airways. Normal resistance is in the range of 1 to 2 cm H2O/L/sec. Although the peripheral airways are narrow, their total cross-sectional area is large, so that resistance to air flow at that level of the tracheobronchial tree is low. Airway resistance decreases as lung volume increases because of an increase in airway diameter resulting from tethering of airway walls to lung tissue.
• Causes of increased airway resistance include airway obstruction by intrinsic mass or mucus plug, airway smooth muscle contraction (bronchospasm), and the dynamic compression of a forced exhalation.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 19
• Not all air entering the lungs is in contact with gas-exchanging units. The portion of an inhaled breath that fills the respiratory zone is the alveolar volume (Va), and the portion remaining in the conducting airways is the dead space volume (Vd). At end expiration, Vd contains exhaled alveolar gas that has equilibrated with pulmonary capillary blood; thus, on the next breath, the amount of fresh air reaching the alveoli is the Va minus the Vd.
• Slow, deep breathing results in greater alveolar volume and therefore greater gas exchange than rapid shallow breathing at the same volume of air per minute, or minute ventilation.
• The distribution of ventilation in the lungs is unequal, with greater ventilation in the base and less at the apex in the upright position. The same is true for lung perfusion. This matching of ventilation and perfusion optimizes gas exchange.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 20
• Ventilation is the primary short-term homeostatic mechanism for maintaining normal blood pH, the strongest factor controlling ventilation. This is accomplished through elimination or retention of CO2. The partial pressure of carbon dioxide (Pco2) in blood is inversely proportional to the minute ventilation. Hypoxia is the second strongest drive to ventilation. Maintaining pH and adequate oxygenation is accomplished through the respiratory control system, which consists of neurologic respiratory control centers, respiratory sensors, and respiratory effectors.
• Respiratory Control Centers Neuronal control of autonomic respiration resides in the brain stem, primarily the medullary reticular formation. The medulla receives input from the pons, which may modify or fine-tune the rhythm of breathing. Voluntary ventilation originates in the cerebral cortex and can override autonomic ventilatory control.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 21
• Respiratory Effectors The muscles of respiration include the diaphragm and accessory muscles, as previously discussed. For effective ventilation, these muscles must be coordinated by the respiratory control center through the phrenic, intercostal, cranial, and cervical nerves.
• Respiratory Sensors There are two types of respiratory receptors: chemoreceptors and mechanoreceptors.
Central and peripheral chemoreceptors detect changes in pH, Pco2, and partial pressure of oxygen (Po2). Central chemoreceptors located in the medulla respond rapidly to changes in hydrogen ion concentration and Pco2 by stimulating or inhibiting ventilation to maintain blood pH within the normal range. The peripheral chemoreceptors also respond to hydrogen ion concentration and Paco2 but are most sensitive to changes in partial pressure of arterial oxygen (Pao2).
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 22
• In contrast to the linear response of ventilation to Paco2, the response to changes in Pao2 are minimal until the Pao2 drops below 60 mm Hg. Below that threshold there is a steep relationship between Pao2 and ventilation.
The Pao2 versus ventilation curve is a mirror image of the oxygen dissociation curve for hemoglobin.
• Mechanoreceptors in the chest wall and airways modulate rate and depth of breathing in response to stretch. J receptors located in juxtacapillary regions in the lung periphery stimulate ventilation in response to pulmonary vascular engorgement. There are also airway irritant receptors that respond to physical and chemical stimuli.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 23
Ctn. Structure and Function of the Normal Respiratory System
CO2 suffocation (?)
O2 suffocation (?)

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 24
Perfusion The pulmonary vascular bed receives the entire output of the right ventricle. Because the pulmonary circulation is a low-pressure system, it is affected by gravity, with the greatest blood flow going to the dependent portions of the lungs. The hydrostatic pressure increases from the top to the bottom of the lungs. Alveolar pressure, assuming open airways, is relatively constant throughout the lung. It is the relationship between alveolar and pulmonary vascular pressure that largely determines blood flow in the normal lung.
• In 1964, West devised a model of blood flow within the lungs that divides the lung into three zones, determined by the relationship between pulmonary vascular and alveolar pressures.
Zone 1 is defined as an area of the lungs in which alveolar pressure exceeds pulmonary artery pressure, thus inhibiting perfusion. This ventilated but unperfused area of the lung is called alveolar or physiologic dead.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 25
Zone 2 conditions exist when pulmonary arterial pressure is higher than alveolar pressure but alveolar pressure is higher than pulmonary venous pressure. In zone 2, the hydrostatic pressure driving blood flow is the difference between pulmonary artery pressure and alveolar pressure.
In zone 3, pulmonary venous pressure exceeds alveolar pressure and blood flow is determined by the arterial-venous pressure difference.
In states of increased oxygen demand, cardiac output rises and pulmonary vascular resistance actually falls through recruitment of previously unperfused vessels, increasing the total vascular cross-sectional area. This allows blood flow to increase dramatically with relatively small increases in pulmonary artery pressure.
The relationship between lung volume and pulmonary vascular resistance is U-shaped. At low volumes, vascular resistance decreases with increasing volume because of tethering of vessels to lung tissue, but, at high lung volumes, resistance rises again, with compression of capillaries by increasing alveolar volume.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 26
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 27
Gas TransferOxygen and carbon dioxide are easily dissolved in plasma. Other atmospheric gases are much less soluble and are not significantly exchanged across the alveolar-capillary interface. The solubility of O2 and CO2 allows complete equilibration between alveolar and plasma concentrations during each respiratory cycle.
The majority of O2 contained in the blood is bound to hemoglobin, with a small fraction dissolved measured as the Pao2. Each molecule of hemoglobin is capable of carrying four molecules of oxygen. Under normal conditions, at a Pao2 of 150 mm Hg, hemoglobin is completely saturated, and further increases in Pao2 have little effect on the oxygen content of blood. The oxygen-hemoglobin dissociation curve is a graph of the relationship between Pao2 and hemoglobin saturation. Its shape reflects the cooperative binding of oxygen to hemoglobin.
Decreased blood pH, increased temperature, increased 2,3-diphosphoglycerate, and increased Paco2 all act to decrease the affinity of hemoglobin for oxygen, which facilitates unloading of oxygen into tissues.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 28
• Carbon monoxide binds hemoglobin with 240 times greater affinity than does oxygen at the same sites and also induces cooperative binding. Binding of hemoglobin by carbon monoxide decreases the oxygen content of blood by decreasing the amount of oxygen bound to hemoglobin but has no effect on partial pressure of alveolar oxygen (Pao2). It simultaneously decreases the off-loading of oxygen into tissues by increasing the affinity of hemoglobin for oxygen.
• Carbon dioxide is also bound to hemoglobin but does not exhibit cooperative binding; thus the shape of the CO2 dissociation curve is more linear than that of O2 and is determined by mass effect of Pao2. In the lung, O2 displaces CO2 from hemoglobin, and, in tissues, the release of O2 allows on-loading of CO2.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 29
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 30
Abnormalities of Pulmonary Gas Exchange Partial pressures of oxygen and carbon dioxide in arterial blood are determined by the degree of equilibration between the alveolar gas and capillary blood. The degree of equilibration depends on four main factors:
1. Ventilation/Perfusion Inequality (Mismatch) The lung is composed of units with varying ratios of ventilation to perfusion ([Vdot]/[Qdot]). In normal lungs, the range of [Vdot]/[Qdot] ratios is narrow, from about 0.5 to 3.0. As lung disease develops, the range widens, so that [Vdot] and [Qdot] are matched in fewer lung units. This mismatch without compensation will cause the Pao2 to fall and the Paco2 to rise.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 31
2. Hypoventilation Hypoventilation is defined as ventilation inadequate to keep Paco2 from increasing above normal. In this situation, hypoxia may occur when increased CO2 in alveoli displaces sufficient O2. Partial pressure of alveolar carbon dioxide (Paco2) is directly proportional to minute ventilation. The alveolar gas equation describes the reciprocal relationship between Paco2 and Pao2:
3. ShuntShunt is the portion of the blood that goes from the right side of the heart to the left without an opportunity for exchange of oxygen and carbon dioxide. Anatomic shunt occurs across intracardiac septal defects, via pulmonary arteriovenous malformations, and from the very small percentage of venous return from cardiac and bronchial circulations that empties directly into the left atrium. Physiologic shunt occurs when pulmonary capillary blood traverses unventilated lung units and is actually one extreme of [Vdot]/[Qdot] mismatch. Shunt is the most potent source of hypoxemia because the oxygen content of shunted blood cannot be affected by increases in the fraction of inspired oxygen.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 32
4. Diffusion Impairment With normal cardiopulmonary function, blood spends an average of 0.75 second in the pulmonary capillaries at rest. During vigorous exercise, this time may be decreased to 0.25 second. Because it takes only 0.25 second for blood and alveolar oxygen to equilibrate across the thin alveolar capillary membrane, even under these conditions there is no fall in the end-capillary oxygen concentration. Increased diffusing distance resulting from alveolar capillary membrane thickening requires more time for oxygen to equilibrate between alveolar gas and capillary blood, resulting in a decrease in Pao2 first with exercise and in extreme cases at rest. Hypoxemia is rarely caused solely by diffusion impairment.
Aging: The lung grows by alveolar multiplication up to 8 years of age, after which it continues to grow by increasing alveolar diameter until about age 20. Thereafter, both total alveolar surface area and elastic recoil decrease progressively with age. By age 80, alveolar surface area is reduced by about 30%. In aging, small airways and alveoli in the lower lung zones tend to collapse during expiration, increasing [Vdot]/[Qdot] mismatch and contributing to the progressive increase in the alveolar-arterial oxygen difference found in the normal lung with age.
Ctn. Structure and Function of the Normal Respiratory System

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 33
2. Evaluation of the Patient with Resipratory Disease
History • Common symptoms of respiratory disease, such as dyspnea or
cough, are common to diseases of other organ systems as well. For example, dyspnea is also a cardinal symptom of heart disease, and cough may be caused by gastroesophageal reflux or chronic sinusitis. An organized approach to the patient, starting with a careful history and a detailed physical examination, will focus further investigation to determine the etiology of the symptom and usually lead to the correct diagnosis.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 34
Common Presenting Complaints
• Dyspnea (shortness of breath) is a common complaint of patients with pulmonary disease. Timing and acuity of onset, exacerbating and alleviating factors, and degree of functional impairment are key elements of the history.
If dyspnea is recent, of sudden onset, and accompanied by chest pain, diseases such as pneumothorax, pulmonary embolism, and pulmonary edema should come to mind. If the dyspnea is long standing and is slowly progressive, chronic conditions such as chronic obstructive pulmonary disease, pulmonary fibrosis, and neuromuscular disease are in the differential diagnosis. The progression of chronic dyspnea may be insidious. It is important to ask specific questions to quantify changes in functional status over time.
Ctn. Evaluation of the Patient with Resipratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 35
• Orthopnea is defined as dyspnea that occurs in the supine position as a result of a decrease in vital capacity caused by abdominal contents exerting force against the diaphragm.
• Paroxysmal nocturnal dyspnea is dyspnea that occurs one to several hours after lying down and is associated with congestive heart failure. It is caused by increased venous return to the heart resulting in mild pulmonary edema. Asthma can also be associated with nocturnal dyspnea, in part because adrenal cortisol secretion is lowest at about 4:00 am. Exercise-induced asthma causes dyspnea out of proportion to the degree of exertion, with dyspnea often being most severe in the 15 to 30 minutes after cessation of exercise.
Ctn. Evaluation of the Patient with Resipratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 36
• Wheezing, although associated with asthma, has many causes. The absence of wheezing does not rule out asthma in any setting, and the presence of wheezing does not establish the diagnosis. Other conditions that cause wheezing are congestive heart failure; endobronchial obstruction by tumor, foreign body, or mucus; vocal cord abnormalities; and acute bronchitis.
• Cough is a frustrating symptom for both the patient and the physician. The three most common causes of chronic cough are asthma, postnasal drip, and gastroesophageal reflux disease. Cough may be mild and infrequent or it may be severe enough to induce emesis or syncope. Cough may be dry or may produce sputum or blood (hemoptysis). A common cause of a dry, hacking cough is the use of angiotensin-converting enzyme inhibitors. The symptom may begin months or longer after initiation of the drug. Although possible, it occurs less often in patients taking angiotensin II receptor antagonists. Bordetella pertussis infection (whooping cough) and viral lower respiratory infections can produce a cough that may last for 3 months or longer. Patients with asthma often have cough, and on occasion it is their only symptom, a condition referred to as cough-variant asthma.
Ctn. Evaluation of the Patient with Resipratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 37
• Sputum: More than occasional production of sputum is abnormal and should be characterized by quantity, color, presence or absence of blood, and timing. The physician should ask the patient to estimate the frequency and volume of sputum produced in 24 hours as well as any diurnal variation. Chronic bronchitis is defined as a persistent cough resulting in sputum production for more than 3 months in each of the last 3 years. Patients with asthma often have a productive cough resulting from excess mucus production. The color of sputum does not signify an infection but is influenced by the concentration of cellular debris, predominantly white cells, present in any inflammatory process.
• Hemoptysis is a frightening symptom. The volume of blood may be scant or large enough to cause asphyxiation or exsanguination. The most common cause worldwide is pulmonary tuberculosis. Most cases of hemoptysis are small in volume and self-limited and resolve with treatment of the underlying process. Massive hemoptysis, defined as more than 500 mL of blood in 24 hours, is rare, but is a medical emergency when it occurs. The physician should distinguish among hemoptysis, epistaxis, and hematemesis.
Ctn. Evaluation of the Patient with Resipratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 38
• Substance Abuse: An accurate history of tobacco use as well as other toxic and environmental exposures is essential in patients with respiratory complaints. Tobacco smoke is the most prevalent environmental toxin causing lung disease. Patients may be anxious about other inhaled toxins or irritants and yet may continue to smoke without concern.
• Environmental Factors: A history of exposure to other inhaled toxins, irritants, or allergens should be elicited. A careful occupational history often uncovers exposure to inorganic dust or fibers such as asbestos, silica, or coal dust. Organic dusts may cause hypersensitivity pneumonitis and interstitial lung disease. Solvents and corrosive gases are also causes of pulmonary disease. The presence of household pets should be documented. A travel history is important in evaluating infectious causes of pulmonary disease. Travel to developing countries increases the risk of exposure to tuberculosis. A family history is important in assessing the risk of genetic lung diseases such as cystic fibrosis and alpha1-antitrypsin deficiency as well as the susceptibility to asthma, emphysema, or lung cancer.
Ctn. Evaluation of the Patient with Resipratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 39
Physical Examination
• Inspection: The first steps in the physical examination of the patient with pulmonary disease are observation and inspection, which must be done when the patient's chest is bare. The physician should watch the patient breathe and should note the effort required for breathing. An increased respiratory rate, use of accessory muscles of respiration, pursed-lip breathing, and paradoxical abdominal movement all indicate increased work of breathing.
The shape of the thoracic cage should be noted. Increased anteroposterior diameter is seen in obstructive lung disease. Severe kyphoscoliosis, pectus excavatum, ankylosing spondylitis, and morbid obesity all can produce restrictive ventilatory disease as a consequence of distortion and restriction of the volume of the thoracic cavity.
Ctn. Evaluation of the Patient with Respiratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 40
• Palpation: The physician should place both hands on the lower half of the patient's posterior thorax with thumbs touching and fingers spread and should keep the hands in place while the patient takes several deep inspirations. The physician's thumbs should separate slightly and the hands should move symmetrically apart during the patient's inspiration. Fremitus is a faint vibration felt best with the edge of the hand against the patient's chest wall while the patient speaks. Fremitus is increased in patients with underlying consolidation, and it is decreased over a pleural effusion.
• Percussion: Next, the patient's chest should be percussed. The level of the diaphragms on each side should be noted. The percussion note should be compared on the two sides starting at the apex and moving down, including the posterior, anterior, and lateral aspects. A pleural effusion, consolidation, a mass, or an elevated diaphragm can cause dullness to percussion; hyperresonance can be caused by a pneumothorax or by hyperinflation.
Ctn. Evaluation of the Patient with Respiratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 41
• Auscultation: Auscultation of the lungs is performed to evaluate the quality of the breath sounds and to detect the presence of extra (adventitious) sounds not heard in normal lungs. Normal breath sounds have two qualities, vesicular and bronchial. Bronchial breath sounds are heard over the central airways and are louder and coarser than vesicular breath sounds, which are heard at the periphery and the base of the lungs. Bronchovesicular sounds are a combination of the two and are heard over medium-sized airways.
Bronchial breath sounds and bronchovesicular breath sounds at the periphery of the lungs are abnormal and may be caused by underlying consolidation. In the presence of consolidation, there is increased transmission of vocal sounds, called whispered pectoriloquy, as well as egophony, in which the spoken letter "e" sounds like an "a" over the area of consolidation (and is sometimes compared to the bleating of a goat).
Ctn. Evaluation of the Patient with Respiratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 42
• Abnormal or extra pulmonary sounds are crackles, wheezes, and rubs.
Crackles can be coarse rattles or fine, Velcro-like sounds. Coarse crackles are often caused by mucus in the airways or by the opening of large and medium-sized airways. Fine crackles, produced on inspiration by the opening of collapsed alveoli, are most common at the bases and are heard in pulmonary edema and interstitial fibrosis.
Wheezing is a higher pitched sound and, when heard locally, suggests large airway obstruction. The wheezing of patients with asthma or congestive heart failure is lower in pitch and is heard diffusely over all lung fields. Localized wheezing can also be heard in conditions such as pulmonary embolism, obstruction of a bronchus by a tumor, and foreign body aspiration.
Rub is a pleural sound caused by inflamed pleural surfaces rubbing together. It has been described as the sound of pieces of leather rubbing against each other. Rubs are often evanescent and depend on the amount of fluid in the pleural space.
Ctn. Evaluation of the Patient with Respiratory Disease

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 43
Ctn. Evaluation of the Patient with Respiratory Disease
Inspection
Observation: anxiety, distress, malnutrition, somnolence
Chest wall shape, deformity
Respiratory rate, depth, pattern
Paradoxical respiratory motion of chest and abdomen
Retractions
Use of accessory muscles
Pursed-lip breathing
Cyanosis
Palpation
Tracheal deviation
Chest expansion
Vocal fremitus
Lymphadenopathy
Subcutaneous emphysema
Percussion
Normal, dull, or hyperresonant
Auscultation
Breath sounds: normal vesicular over periphery and bronchial centrally
Pleural rub
Added sounds: wheezes, crackles
Stridor

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 44
Ctn. Evaluation of the Patient with Respiratory Disease
DisorderMediastinal
DisplacementChest Wall Movement
Vocal Fremitus
Percussion Note
Breath Sounds
Added Sounds
Voice Sounds
Pleural effusion
Heart displaced to opposite side
Reduced over affected area
Absent or markedly decreased
Dull
Absent over fluid; bronchial
at upper border
Absent; pleural rub may be found above
effusion
Absent over effusion;
increased with egophony at upper border
Consolidation NoneReduced over affected area
Increased or normal
Dull Bronchial Crackles
Increased with egobronchoph
ony and whispered
pectoriloquy
Pneumothorax
Tracheal deviation to
opposite side if under tension
Decreased over affected
areaAbsent Resonant
Absent or decreased
Absent Absent
Atelectasis Ipsilateral shiftDecreased
over affected area
Variable DullAbsent or
diminishedCrackles may
be heardAbsent
Bronchospasm
NoneDecreased
symmetricallyNormal or decreased
Normal or decreased
Bronchovesicular
WheezeNormal or decreased
Interstitial fibrosis
NoneDecreased
symmetricallyNormal or increased
NormalBronchovesicul
ar
End-inspiratory crackles
unaffected by cough or posture
Normal

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 45
3. Diagnostic Tests and Procedures
Chest Radiography
• Chest radiography is the most common and usually initial imaging procedure used to evaluate chest disease. The standard radiographic views are the posteroanterior and left lateral projections. These radiographs, called "plain films," can reveal abnormalities of bone, mediastinal structures, lung parenchyma, airways, and pleura. The plain radiograph in combination with the history and physical examination is often sufficient to diagnose chest disease. In many circumstances, however, additional imaging techniques are necessary to define the disease process more clearly.
• Computed tomography provides more information than the plain film by improving resolution, locating abnormalities in three dimensions, and, with use of intravascular contrast dye, distinguishing vascular from other structures. The spiral computed tomographic scan is an additional improvement in the technique that is faster, permits the radiologist to define the thickness of the sections depending on the goal of the scan.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 46
Ctn. Diagnostic Tests and Procedures
Chest X-Ray

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 47
Ctn. Diagnostic Tests and Procedures
Chest CT Scan / Multiple cuts

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 48
• MRI: Magnetic resonance imaging is not commonly used in the evaluation of pulmonary disease; however, there are special situations in which it can add important information. Magnetic resonance imaging is the imaging procedure of choice to evaluate neurologic and vertebral involvement in patients with superior sulcus tumors of the lung. It is also used to diagnose and evaluate vascular compromise in patients with mediastinal fibrosis, an uncommon but often fatal disease.
Ctn. Diagnostic Tests and Procedures

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 49
Pulmonary Function Testing Routine pulmonary function testing evaluates four areas of lung function: air flow (spirometry), lung volumes, gas exchange (ABG or diffusing capacity), and lung mechanics. Accurate interpretation of pulmonary function tests requires appropriate reference standards. Variables that affect the standard values include age, sex, height, race, and hemoglobin concentration.
Ctn. Diagnostic Tests and Procedures
• Spriometry: Measurement of airflow is the most commonly performed pulmonary function test because of its value in the diagnosis and management of obstructive lung disease.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 50
Ctn. Diagnostic Tests and Procedures
Spirometry
Spirometry in a normal subject and in a patient with obstructive lung disease. FEV1 represents the forced expired volume in 1 second, and FVC represents the forced vital capacity. The slope of the line connecting the points at 25% and 75% of the FVC represents the forced expired flow, FEF25-75, or maximum midexpiratory flow (MMEF).
A, The maximum expired flow/volume curve in a normal subject. The peak expiratory flow (PEF) and forced expiratory flows at 50% and 75% of the exhaled vital capacity (FEF50 and FEF75) are indicated. PIF = peak inspiratory flow. B, In obstructive lung disease (OLD), hyperinflation pushes the position of the curve to the left, and there is characteristic scalloping on expiration. In restrictive lung disease (RLD), lung volumes are reduced, but flow for any point in volume is normal. The flow/volume curve displays different patterns with various forms of upper airway obstruction (UAO), with reduction in respiratory flow if the obstruction is outside the thoracic cavity and, in addition, in expiratory flow if the obstruction is caused by a fixed deformity.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 51
Ctn. Diagnostic Tests and Procedures
• Gas Exchange: The cornerstone in the evaluation of gas exchange is measurement of arterial blood gases. Arterial blood samples are analyzed for pH, the partial pressure of arterial oxygen (Pao2), and the partial pressure of arterial carbon dioxide (Paco2). The percent hemoglobin saturation is routinely calculated from the Pao2 and is an accurate estimate of hemoglobin saturation except in the case of carbon monoxide poisoning. If carbon monoxide poisoning is suspected, hemoglobin oxygen saturation must be directly measured. The Paco2 reflects ventilation, and the Pao2 reflects the adequacy of gas exchange. A calculation of the alveolar-arterial oxygen difference, sometimes called the A-a gradient, is used to evaluate the presence of impaired gas exchange as well as the severity of the impairment.

HINF 2502 (Clinical Processes and Decision Making)
© Hadi Kharrazi, Dalhousie University 52
Summary
1. Structure and Function of the Normal Respiratory System2. Evaluation of the Patient with Respiratory Disease 3. Diagnostic Tests and Procedures in the Patient with Respiratory
Disease








![Respiratory System [โหมดความเข้ากันได้] · PATHOLOGY OF RESPIRATORY SYSTEM นพ. อรรณพ นาคะป ท Respiratory system U it](https://static.fdocuments.us/doc/165x107/5fa578efd4e80f055f6b3401/respiratory-system-aaaaaaaaaaaaaaaaaa-pathology.jpg)
![Respiratory system roadmap.pptx [Repaired] - Loginanatomical-sciences.health.wits.ac.za/roadmaps/Respiratory system... · DIVISION OF THE RESPIRATORY SYSTEM CONDUCTING PORTION Nasal](https://static.fdocuments.us/doc/165x107/5a78c3d87f8b9ae6228c9db0/respiratory-system-repaired-loginanatomical-scienceshealthwitsaczaroadmapsrespiratory.jpg)




![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System.](https://static.fdocuments.us/doc/165x107/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)

