
Respiratory Anatomy and Physiology
13
Respiratory Anatomy and Physiology
-
Upload
indigo-cherry -
Category
Documents
-
view
25 -
download
0
description
Respiratory Anatomy and Physiology. THORACIC CAVITY. 3 sections Mediastinum 2 Lung Chambers * because each lung is in a separate chamber the unaffected lung will remain expanded Right lung has ___ lobes Left lung has ___ lobes - PowerPoint PPT Presentation
Transcript of Respiratory Anatomy and Physiology

Respiratory Anatomy and Physiology

(Riddell, 2000)
THORACIC CAVITY3 sections
Mediastinum
2 Lung Chambers
* because each lung is in a separate chamber the unaffected lung will remain expanded
Right lung has ___ lobesLeft lung has ___ lobesLower lobes or bases are positioned ___________.

(Riddell, 2000)
Surfactant Functions of
surfactant
I. Keeps surface tension lower
II. Allows for Alveolar expansion
III. Prevents collapse of alveoli

(Riddell, 2000)
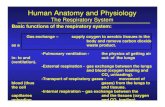
Processes of RespirationGas exchange occurs in 4 steps:
Ventilation
Diffusion
Perfusion
Diffusion

(Riddell, 2000)
Ventilation
The respiratory control center is located in the ____and ____ of the brain stem (respiratory center).
Autonomic regulation -controlled by ____________
-there are 2 groups of chemoreceptors
1.Central chemoreceptors -sense changes in _________
2. Peripheral chemoreceptors - sense changes in ________

(Riddell, 2000)
Hypoxia
Causes:
Hypoxemic hypoxia
Stagnant or ischemic hypoxia
Anemic hypoxia
Histotoxic hypoxia

(Riddell, 2000)
Signs and Symptoms of HypoxiaAcute Hypoxia Increase in ventilation (Chemoreceptor mediated) Decreases in judgement and motor proficiency Dyspnea, fatigue, headache, nausea, vomiting,
decreased visual acuity Cyanosis of lips and nail beds if adequate
hemoglobin Insomnia and cheyne stokes breathing Disorientation, hallucinations, convulsions with
extreme hypoxia
Chronic Hypoxia Dyspnea, fatigue, cyanosis Pulmonary hypertension (d/t alveolar hypoxia and
vasoconstriction) and polycythemia Body adapts to hypoxia with increased ventilation,
pulmonary vasoconstriction, and increased production of RBC’s

(Ignativicius & workman, 2002)
Adventitious Sounds
additional breath sounds superimposed on normal sounds
indicate changes in the tracheobronchial tree
vary in pitch, intensity, duration, and the phase of the respiratory cycle
Examples: crackle, wheeze, rhonchus, pleural friction rub

(Ignatavicius & Workman, 2002)
Voice Sounds-vocal resonance is increased when the sound must travel through a ________________
(i.e. consolidated area of the lung, pneumonia, atelectasis, pleural effusion, tumor, or abscess)
Bronchophony - assess by having client repeat
the __________ while auscultatingWhispered Pectoriloquy
-perceived by having the client whisper ____________Egophony
- assess by having client repeat the letter __-listen for an _______

(Riddell, 2000)
Abnormal Rates and Rhythms
Bradypnea
Tachypnea
Hypoventilation
Hyperventilation
Cheyne Stokes
Ataxic Sighing
Obstructive

(Riddell, 2000)
Arterial Blood Gases
NormalpH pO2pCO2 HCO3Base excess 0
(+2 alkalosis, -2 acidosis)SaO2
Respiratory Acidosis (pH<7.35, pCO2>50mmHg)
Respiratory Alkalosis (pH>7.45, pCO2<35mmHg)
Metabolic Acidosis
Metabolic Alkalosis

(Riddell, 2000)
Interpreting ABGsAsk yourself these questions…1. pH—acidotic or alkalotic?2. PaCO2—low or high?-respiratory3. Normal & HCO3 low or high with a
normal PaCO2?--metabollic • pH is low (acidosis)• pH is normal or high (alkalosis)• PaCO2 is low (alveolar hyperventilation)• PaCO2 is normal or high (alveolar
hypoventilation)• pH is low and PaCO2 is normal-
consider metabolic causes—low pH and HCO3 less than 22-metabolic acidosis
• pH is high and PaCO2 is normal-consider metabolic causes
• high pH and HCO3 greater than 26-metabolic alkalosis

(Riddell, 2000)
References
Ignatavicius, D. D. & Workman, M. L. (2002). Medical-surgical nursing: Critical thinking for collaborative care. Saunders: PA
Riddell, K. (2000). Windsor Regional Hospital.

















![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System.](https://static.fdocuments.us/doc/165x107/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)