Release of DSM-5 DSM-IV versus DSM-5. Release of DSM-5 DSM-IV versus DSM-5.


Contents
Event Information................................3
Introduction to Neurotalks...................... 3
Acknowledgements................................ 3
Event Schedule...................................... 3
Information Manual...............................4 - 10
Introduction to Mental Illness.................. 4
Some Valuable Vocabulary..................... 4
Quick Facts............................................. 4
Making a Diagnosis……………………… 5
What Takes Place……………………....... 5
Differences between the ICD and DSM………………................................... 5
Conceptualizing Mental Illness………..… 5
Culture and Religion……………………... 5
Language………………………………….. 5 - 6
Present-day Application………………….. 6
Forms of Bias……………………………… 6
Making “Trendy” Diagnoses…….............. 6 - 7
Research Funding…………………….…… 7
Sex and mental Illness.............................. 7 - 8
Information Manual (continued)………….. 10 - 18
Mental Illness and the Economy: Fast Facts……………………….............................. 8
Neurobiology of the Brain............................... 8
General Anatomy........................................... 8 - 9
Anatomy and Mental Illness..........................10
Cellular Anatomy........................................... 11
Chemical/Electrical Messengers...................11
Common Neurotransmitter Types.................11 - 12
Neurotransmitters and Mental Illness............13
Categories of Mental Illness .........................14
Suicide........................................................... 14
Quick Facts................................................... 14 - 15
Risk Factors for Suicide................................15
Protective Factors against Suicideand other Mental Health Problems.............................................15
Treatment Options.......................................... 16
Cultural Considerations................................... 16
Psychopharmaceuticals................................. 16
Types……………………………………..…….. 16 - 17
How do they work........................................... 17
Psychotherapy................................................ 17 - 18
Resources...................................................... 19
Neurotalks Symposium 2016 2

Event Information
IntroductionThank-you for participating in the 2016 Let's Talk Science Neurotalks High SchoolSymposium! This marks the second symposium that Let's Talk Science hosts at the University of Manitoba.
High school students from all over Winnipeg came to the Fort Garry campus to learn about mental health and illness. We approached this topic from a holistic perspective. Students listened to two speakers, watched a Ted Talk, participated in round-table discussions, and engaged in several hands-on activities.
By participating in Neurotalks, students connected with like-minded peers, faculty members, leading researchers, and other professionals in the community. Together, we learned about this complex issue by looking at scientific research, as well as some of its psychological, social, and medical implications.
It is the aim of Let’s Talk Science (LTS) and the Neurotalks coordinating team to empower our young people and help them develop into conscientious community members as well as future professionals.
AcknowledgementsWe would like to give special thanks to:
The Neurotalks Coordinators Amy Tieu, Kyle Castrojeres, Affan Ali Sher, Joseph Asimanew, Andrew Samuel, and Karina Fagerstrom-Castro for their tireless efforts in planning the Let's Talk Science Neurotalks Symposium.
Our sponsors Let's Talk Science National, Lindt, and the Science Students Association at the University of Manitoba for their generous contributions to help
make this event a reality.
Our guest speakers Dr Krystyna Kockzandi, Dr Brian Cox, and Dr Don Stewart for helping to welcome the students and for sharing their perspectives on mental health and illness.
Thehigh school students and educators who took time out of their week to join us and learn more about this nuanced topic.
The Let's Talk Science volunteers who helped tremendously with set up and clean up; who took on the role of group leaders; who helped facilitate round-table discussions; and who led workshops.
Schedule8:30-9:00Sign in and light snacks
9:00-9:20Opening Ceremonies
9:25-11:07Presentations and round-table discussions:
9:25 am - 9:39 am - Keynote presentation #1 9:39 am - 9:57 am - Round-table discussion topic #19:57 am - 10:02 am - (gifts to speaker, questions)10:02 am - 10:17 am - Ted Talk 10:17 am - 10:37 am - RT discussion #2 10:37 am - 11:07 am - Jeopardy Game Show
11:07-11:17 Intro for lunch
11:17-12:02Lunch
12:02-12:12Afternoon instructions
12:12-2:28Activities (3 total)*
2:28-2:48Final speaker
2:48 - 2:58 Gift to speaker, questions
2:58-3:18Closing remarks + feedback sheet
*Afternoon Activities (each 35 minutes):
Pig Brain Anatomy demonstration Stress and Self-care Neurotransmitters + Action Potentials
Neurotalks Symposium 2016 3

Information Manual*Please note that Let's Talk Science does not claim ownership of any of this material. The NeuroTalks coordinating team compiled a list of topics related to mental health and illnessthat we believeare of interest to students and educators. If you are interested in learning more about any of these topics, please refer to the references boxes for source information.
IntroductionMental illnesses are health issues that impact the way a person interacts with the world around them. Mental illnesses affect the way a person thinks about themselves and others because they impact one’s feelings, behaviours, and thoughts1.
Despite how common mental illness is in our community, the strong stigma attached to mental illness often prevents people from reaching out and obtaining the supports they need.
In fact, the stigma and discrimination that comes with being labeled as having a mental illness often adds to the person's suffering and it can negatively impact their self-esteem. This can further disrupt a person’s relationships and limit their ability and willingness to find work, obtain housing, and complete their education2.
Some valuable vocabularyMental illnesses* are different from neurological disorders.Mental illnessesareof major focus in psychiatry and mainly describe abnormalities in the way a person thinks, feels, or behaves, and how these impairments lead to distress or impairments in day-to-day functioning3.
Right now, there are 297 diagnosable illnesses in the diagnostic manual healthcare workers use when performing diagnoses4. This manual is called the DSM.
Neurological disorders* are part of neurology and describe physical diseases ofthe Central Nervous System (CNS) and Peripheral Nervous System (PNS).
Examples of neurological disorders include: Alzheimer’s disease (AD), Autism Spectrum Disorders (ASD), and Fetal Alcohol Spectrum Disorder (FASD).
*Despite these definitions, It is not always clear where to draw the line between neurology and psychiatry.
The Mind refers to a person’s understanding of things, their thought process, and consciousness. The mind is not composed of matter, so it cannot be studied directly5.
The Brain refers to the organ found inside our skulls composed of cells, molecules, blood vessels, etc. The brain coordinates movements, thoughts, and feelings5. The brain is made of matter and can be studied directly.
Prevalence describes the proportion of a population who will experience a mental illness in their life time.
Incidence describes the number of new cases reported in a population at any given time period.
In the case of mental illness, social stigma is when people have prejudiced attitudes and discriminate against people with mental illness. The consequences of bias and discrimination show up in a variety of ways, including bullying and being denied work.
Quick FactsThe likelihood of a Canadian developing a mental illness in their life time (i.e.: prevalence) is 20% (1 in 5 Canadians)6.
At any given time, 10.4% of Canadians will have a mental illness (i.e.: incidence)6.
From 2009-2014, about 25% of the Manitoban population aged 10 and older received medical help for at least one of the following mental illnesses7:
Anxiety Substance abuse Personality disorder Depression Schizophrenia
Canadians in the lowest income bracket are 3-4 times more likely than Canadians in the highest income bracket to describe their mental health as ‘poor or fair’8.
Across Canada, 23-67% of those experiencing homelessness report having a mental illness8.
Neurotalks Symposium 2016 4

References:1http://www.cmha.ca/mental_health/mental-illness/2http://www.minddisorders.com/Del-Fi/Diagnosis.html3World health organization4http://www.slate.com/articles/health_and_science/medical_examiner/2013/04/diagnostic_and_statistical_manual_fifth_edition_why_will_half_the_u_s_population.html5http://www.differencebetween.net/science/health/difference-between-mind-and-brain/6http://www.mooddisorderscanada.ca/documents/Media%20Room/Quick%20Facts%203rd%20Edition%20Referenced%20Plain%20Text.pdf7Annual Statistics 2013-2014: http://www.gov.mb.ca/health/annstats/as1314.pdf8http://www.camh.ca/en/hospital/about_camh/newsroom/for_reporters/Pages/addictionmentalhealthstatistics.aspx
Diagnosing Mental IllnessDiagnosis is the identification and classification of a disease based on the patient’s signs and symptoms.
Mental illness diagnoses are made by mental health clinicians (i.e.: psychiatrists, psychologists, and psychiatric nurse practitioners) using the Diagnosis and Statistical Manual of Mental Disorders (DSM)1.
What TakesPlace?Whena person seeks a mental health clinician’s help, the clinician will first interview the patient (and, if appropriate, the patient’s family). During this interview, they conduct a medical history and may ask the patient to complete psychological evaluations (i.e. tests or checklists). The clinician will form a diagnosis based on the patient’s symptoms using the DSM.
Differences between the ICD and the DSM
Throughout the years, the ICD and DSM have become similar. However,three main differences include the fact that2:
The ICD is created by a global health agency (World Health Organization, WHO) whose mission is to improve public health. The DSM is created by a single national (American) private association: the American Psychological Association (APA).
The ICD is regulated by World Health Assembly which is made up of all of the health ministers from each of the 193 WHO member countries (including Canada). The DSM is regulated by the assembly of the APA.
The ICD is given out at a very low cost and is handed out as broadly as possible. Low-income countries receive significant discounts on the ICD. It
is also available for free on the internet. The DSM, on the other hand, produces a significant portion of the APA’s revenue. Revenue from the DSM comes not only from the sale of the book, but also from selling related material as well as copyright permissions to be published in articles and books.
References:1http://www.minddisorders.com/Del-Fi/Diagnosis.html2http://www.apa.org/monitor/2009/10/icd-dsm.aspx
Conceptualizing Mental IllnessThe language we use, our culture, religion, and biochemistry are only some factors that play a role in how mental illness is diagnosed and treated.
These social and biochemical factors also impact how we, as individuals, understand mental health.These factors can impact the views and assumptions we develop about mental health and those afflicted with related illnesses.
Culture and ReligionThe way mental health is defined varies between groups, societies, cultures, and institutions1. These various groups have different methods of determining: What is mentally healthy Understanding the causes and symptoms of mental
illness Coming up with appropriate interventions.
Each person comes from different cultural, political, religious, and class backgrounds. Mental health professionals can also be influenced by their own personal values, and this can affect the diagnosis and methodology they use during treatment.
With that said, mental health professionals are beginning to understand the importance of being knowledgeable and respectful of religious and spiritual beliefs that are different from their own.
Although the APA states that religion needs to be respected when making diagnoses, the APA has received criticism about their ethnocentric (i.e.: primarily Euro-American) perspective2. For example: several non-Western mental illnesses are left out of
the DSM Non-Western mental illnesses that are included in
the DSM are often misinterpreted.
Language
Neurotalks Symposium 2016 5

Language is powerful and our choice of words influences the way we view the world. One major concern about the DSM is that it relies heavily on labeling to make sense of a particular illness. Placing labels like a mental health diagnosis on a person can cause others to erases that person’s other qualities and form opinions of them based exclusively on their diagnosis1. Efforts have been made in more recent editions of the DSM to try and minimize this risk.
Present-Day ApplicationWe can help fight this stigma by making simple changes in our own day-to-day vocabulary.
For example, switching from"_________ is schizophrenic/anorexic" to, "_______ has schizophrenia/anorexia" is a subtle yet powerful way of emphasizing that a person is not defined solely based on their illness.
Another way we can remove bias from our everyday language lies in our use of the words,"And"/"but". For example, saying, "She has depression and she has lots of friends" is more empowering to the person mentioned than saying, "She has depression, but she has lots of friends". In this example, replacing "but" with "and", helps remove the suggestion that people with depression don't typically have many friends.
In regards to suicide, saying that someone, “Attempted suicide” or, “Completed suicide” comes naturally to most people. However, this has the negative connotation that suicide survivors have failed, and those who die are successful. One thing we can say to help remove this negative connotation is to say, “Die by suicide” instead.
Changing our language can be challenging because it requires self-awareness and some practice. With time, though, these changes will start feeling more natural.
References:1http://www.minddisorders.com/Del-Fi/Diagnosis.html#ixzz477GutGFX2http://www.apa.org/monitor/2009/10/icd-dsm.aspx
Forms of BiasThe DSM is often criticized for adding to the social stigma that already exists against people who have mental illness.
Social stigma leads to bias, which is an unfair belief or opinionagainst those with mental illness formed without reason or knowledge. Unfortunately, bias can also lead society to treat people with mental illness differently, and this impairs their quality of life.
Within research, who the funders are and their interests can bias the results researchers obtain from their studies. Pop culture and even sex/gender can impact the diagnoses mental health workers make about patients seeking help.
Making"Trendy" DiagnosesWhen researchers step back and take a look at the number of people diagnosed with a mental illness in any given year, these numbers usually fluctuate.
This means that in a population, some mental illnesses become less common, while others become more common.
Some explanations for these patterns include: 1. People are more familiar with the illness and
clinicians are also more aware of the symptoms associated with that mental illness.
2. Stigma against mental illness is less powerful, so people are seeking help out more frequently.
3. Environmental factors (e.g.: civil war, oppression, etc.) influence people and make them less/more likely to develop a particular mental illness.
4. Mental health clinicians are like us in that they, too, can be swayed by trends and popular opinions*. (Example: Dissociative Identity Disorder, DID).
5. Since clinicians are in a position of power, they may influence their clients to behave in a way that fits a particular description*. (Example: Dissociative Identity Disorder, DID).
*One example involves Dissociative Identity Disorder (DID)2(previously known as Multiple Personality Disorders (MPD). Between 1890 and 1920, there were 77 reported cases of DID. These numbers declined sharply until 1970, and then increased sharply again.
In the 90's, the likelihood that someone would be diagnosed with DID rose from 1 in 1,000,000 to 1.4% in Winnipeg and 0.4% in Turkey2.
In the 1970’s, a book titled Sybil was published. After its publishing, the public became very interested in DID because the main character in this book had DID. After Sybil, characters with DID became more common and were frequently glamourized2.
The number of people diagnosed with DID jumped around this time. It is possible clinicians were already seeing DID symptoms in their patients, but only recently began to diagnose patients with DID because interest in this disorder grew.
Given that DID is a rare disorder, the prospect of diagnosing someone with DID may have become appealing to mental health workers. Mental health
Neurotalks Symposium 2016 6

workers may have influenced their clients into acting a certain way that fit with this disorder.
The change in prevalence of DID is one example of how mental health workers can be influenced by trends, or popular/mainstream culture.
More recently, researchers have noticed a sharp increase in the number of people diagnosed with Attention Deficit/Hyperactivity Disorder (ADHD). A series of factors, including the five mentioned above, likely play a role in explaining this trend.
Research FundingPharmaceutical companies are always creating new products. It is important to make sure that these drugs are safe for use so studies must be conducted to know how effective a particular drug. These studies also help researchers understand the benefits and risks of using a particular drug, both in the long and short term.
Research costs money, and this money can come from various sources including public sources (government) or private sources (companies, individuals, etc.)
As consumers, we must always consider the agendas behind private companies or individuals who fund studies.
Something that many people find controversial is that illness, both physical and psychological, are profitable for pharmaceutical companies because of the drugs used as part of treatment programs.
Funding bias, or sponsorship bias, can occur, meaning that a study agrees with the interests of the study's financial provider1.
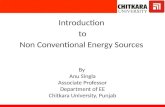
Figure 1: Annual Statistics 2013-2014: http://www.gov.mb.ca/health/annstats/as1314.pdf. Page 31When private companies fund research, funding biasis a risk and research about tobacco, pharmaceutical drugs, and chemical toxicity is often linked to funding bias.Possible causes of funding bias include:
Human nature: People often feel obligated to return favours (sometimes called reciprocity). Researchers may not be consciously aware they are affected by this human tendency2.
Conclusion is chosen before the study begins: The results of studies might be specifically destroyed or chosen if it agrees with a particular conclusion3. Funders may fund several studies and may only publicize studies whose results support the conclusions they are hoping for. Sometimes researchers are made to sign agreements that say they are not allowed to release any of the study's results themselves and that the only people they can submit those results to are the funders.
Bias in participant selection:Researchers may impact the outcome of a study by being biased in: who they allow to participate in the study; which variables they look at in a study, and how many people they choose to participate in the study4.
Misconduct: some researchers may change the data to fit a particular outcome5.
Sex and Mental IllnessFigure 1(page 7) shows the percentage of 10+ year old Manitobans receiving medical care for at least one of the following mental illnesses (anxiety disorders, substance abuse, schizophrenia, depression, or personality disorder) based on age and sex6. From this figure, we see that females are consistently affected by mental illness more frequently than are males.
Neurotalks Symposium 2016 7

Why might this be?Females often face challenges that males do not encounter as frequently, including7:
Being a victim of sexism, which means that they face discrimination and prejudice because of their sex or gender.
Experiencing domestic violence Being a single parent Being at a socioeconomic disadvantage
Females also experience social pressure that promote certain qualities including looking a certain way and being nurturing. On the other hand, social pressures may discourage certain traits in females, like assertiveness. These challenges and expectations can be psychologically damaging and are risk factors for developing mental health issues.
Mental Illness and the Economy:Fast Facts
People living with a mental illness are less likely to be employed than are individuals without a mental illness1.
70-90% of people with severe mental illness (like chronic schizophrenia) are unemployed1.
In any week, about 500,000 (almost 2% of the Canadian Population) cannot work because of mental health-related problems1.
In Canada, the economic burden of mental illness in Canada is about $51 billion annually. This includes healthcare costs, and productivity loss at work1.
In Ontario alone, about $5 billion dollars are put towards alcohol-related law enforcement, health care, lost productivity, and other alcohol-related issues1.
Money that companies put towards creating aworkenvironmentin which employees feel comfortable talking about their mental illness, prevention, and early intervention is beneficial in the long run. This trend is seen in various countries1.
References:1http://www.camh.ca/en/hospital/about_camh/newsroom/for_reporters/Pages/addictionmentalhealthstatistics.aspx2Abnormal Psychology, Fifth Canadian Edition, Wileyhttp://www.gov.mb.ca/health/annstats/as1314.pdf
Neurobiology of the brain
We can split the brain up into several sections based on function and structure. Tying in biology and chemistry when we talk about mental illness has helped de-stigmatize these conditions.
Using animals and comparing the brains of healthy individuals to the brains of people with mental illness helps researchers figure out if and how disordered brains differ from healthy brains.
General Anatomy
Figure 2: cybersurgeon.net
Lobe PurposeOccipital processes visual signalsParietal processes sense of touchTemporal auditory signalsFrontal controls motor/voluntary movement
(like that of muscles)planningattentionorganizationthinkinglong-term memory formation.
Neurotalks Symposium 2016 8
References:1Sheldon Krimsky, "Do Financial Conflicts of Interest Bias Research? An Inquiry into the "Funding Effect" Hypothesis," Science, Technology & Human Values, 38(4), July 2013, doi:10.1177/01622439124562712Cialdini, Robert B (2008-08-08). Influence: Science and Practice (5th ed). Prentice Hall. ISBN 978-0-205-60999-4.3Wilmshurst, Peter. "Dishonesty in Medical Research" (PDF)4Lexchin, Joel; Bero, Lisa A; Djulbegovic, Benjamin; Clark, Otavio (2003-05-31). "Pharmaceutical industry sponsorship and research outcome and quality: systematic review". BMJ 326 (7400): 1167–1170.doi:10.1136/bmj.326.7400.1167. PMC 156458. PMID 127756145David Michaels (2008-07-15). "It's Not the Answers That Are Biased, It's the Questions". The Washington Post.6Annual Statistics 2013-2014: http://www.gov.mb.ca/health/annstats/as1314.pdf7http://www.who.int/mental_health/prevention/genderwomen/en/

Figure 3:http://www.proprofs.com/flashcards/story.php?title=intro-mind-and-brain--topic-2-foundation-brains
Forebrain
Telencephalon Diencephalon
cerebral cortex (cerebrum)
Sensing, thinking, learning, emotion, consciousness, voluntary movement
ThalamusInformation about our environment that we acquire through our senses (touch, hearing, sight, and taste1) is processed here and sent to the part of the brain that "decodes" that kind of information.
basal gangliaInvolved mostly in motor control
HypothalamusRegulates basic biological needs like hunger, thirst, and temperature control. The hypothalamus also regulates hormone release, meaning it is also involved in our fight or flight response, our biological rhythms (example: sleep), and sexual behaviour.
limbic systemInvolved in emotional regulation as well as learning and memory, emotional memories, and recognizing emotions in others.
1The exception is smell.
midbrain
Mesencephalon
tectum tegmentum
Hindbrain
Metencephalon Myelencephalon
Cerebellum (“little brain”)
Coordinates fine muscles and balance
Medulla oblongataRegulates largely unconscious functions including reflexes, breathing, circulation, the sleep-wake cycle, and arousal.Pons ("bridge")
Connects cortex and cerebellum
Figure 4: http://corpusoptima.com/wp-content/upLoads/2012/09/CorpusCallosum222.jpg
Corpus CallosumFibers that connect and relay information between the two cerebral hemispheres
Neurotalks Symposium 2016 9

Figure 5:http://www.proprofs.com/flashcards/story.php?title=intro-mind-and-brain--topic-2-foundation-brains
Ventricle Locationcerebral aqueduct2 midbrain
Lateral forebrainthird forebrain
2where the CSF is produced.
Anatomy and Mental IllnessResearchers have attempted to understand mental illness from a biological perspective. Doing a quick Google search will bring up hundreds of papers about this area of research!
Research is important within psychiatry because it helps us understand mental health and illness more clearly. This knowledge can help us figure out what causes mental illness, what mental illness looks like, how to prevent it, and (hopefully) how to cure it.
Participants are humans who agree to participate in research studies to be tested on.
Sometimes, participants with mental illness will show differences in their brain structure when compared to people who do not have that mental illness (i.e.: healthy controls).
The affected areas in the brain can help researchers understand why people with a particular mental illness show certain impairments.
For example:Research on people with schizophrenia often show noticeable differences when their brains are compared to brains of people without schizophrenia:
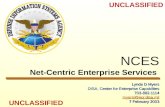
Figure 6: Harvard University Schizophrenia Project
The images pictured above (figure 6, page 10)show a magnetic resonance (MR) image of a healthy brain on the left and a schizphrenic brain to the right. Placing the two images side be side emphasizes the different ventricle sizes beteen the healthy brain and the schizophrenic brain.
The larger ventricle size in the schizophrenic brain (right) suggests that brain cell (AKA neuronal) death has occured1.
Figure 6 also shows that the schizophrenic brain has more Cerebrospinal Fluid (CSF) in the part of the brain containing the amygdala and hippocampus compared to the healthy brain.
The hippocampus and amygdala are located in the two bulb-like portions found at the bottom of the brain. The hippocampus and amygdala are important for memory formation and learning. Individuals with schizophrenia tend to show deficits in learning and memory formation2.
This helps illustrate how differences in anatomy could help explain some of the deficits observed in behaviour.
Neurotalks Symposium 2016 10

Figure 7: Prof. Philip Ward, NISAD Cognitive Neuroscience Research Panel.
In figure 7 (page 10), a different imaging technique called functional magnetic resonance imagining (fMRI) shows differences in brain activity between a healthy control (N) and schizophrenia participants (S). These participants were placed in an MRI scanner as they were performing a task that tested their executive functioning skills3.
Executive functioning skills are the set of mental skills that help you get things done. Examples of tasks that require executive functioning skills includes: time management, paying attention, switching focus, and making sure you don't say the wrong thing.
Can clinicians use these findings to make diagnoses? In short, no. Although researchers have found promising trends, not all patients will show the same abnormalities. Some patients might even show no abnormalities when compared to healthy controls.
Since structural differences can vary among people with the same mental disorder,mental health workers are not yet able to rely on structural differences to figure out a patient's diagnosis.
References: 1http://www.schizophrenia.com/family/disease.htm2Saykin, A. J., Gur, R. C., Gur, R. E., Mozley, P. D., Mozley, L. H., Resnick, S. M... Stafiniak, P. ( 1991). Neuropsychological function in schizophrenia: Selective impairment in memory and learning. Arch Gen Psychiatry. 48(7), 618-624. doi:10.1001/archpsyc.1991.01810310036007.3http://www.schizophrenia.com/research/NISAD.research.htm
Cellular AnatomyGlial cells are support cells in the nervous system important for keeping the brain healthy. Glial cells are also an important part the brain's response to injury and disease.
Neurons are cells that receive, decode, and sendoff information within the brain and other parts of the body.
Figure 8: http://slideplayer.com/slide/6431520/
Part of Neuron FunctionDendrites receives information from other
neurons
Soma (Cell Body) contains the cell’s nucleus and chemical machinery
Axons long, thin fiber that transmits signals to other neurons, muscles,
OR glands
Myelin Sheath insulating material (from glial cells), that surrounds some axons
Axon Terminals at the end of axons that secretes neurotransmitters
Synapse junction where information is transmitted between neurons
Synaptic Cleft microscopic gap between neurons
Chemical/Electrical MessengersThe brain makes use of electrical and chemical signaling to send messages from one part of the brain to another, and from the brain to the rest of the body.
Figure 9: www.scistyle.comHow are messages sent?
1. Electrical signal travel down axon.
2. Signal tells the neuron to release neurotransmitters (signal molecules usually stored in the axon terminal)
Neurotalks Symposium 2016 11

3. Neurotransmitters released into tiny space between neurons called the “synaptic cleft”
4. Neuron binds with a receptor (like a lock and key) on the “postsynaptic neuron”
5. Signal continues until it reaches its target.
Common neurotransmitter typesNeurotransmitters are brain chemicals that help relay information throughout the brain and body. These tiny molecules allow signals to be passed on between our brain cells (i.e.: neurons) by binding to receptors.
Receptors are places on the surface or interior of a cell that binds specific substances including hormones, neurotransmitters, and drugs2. Receptors tend to be very specific and bind to only one type of substance or very similar substances.
Neurotransmitters allow the brain to give organs and other tissues instructions on how to function. Neurotransmitters can also impact our ability to focus, our sleep patterns, and our mood1.
There are several types of neurotransmitters, and each one is responsible for one or more functions in the brain. Some common neurotransmitters are:
1. Dopamine2. Norepinephrine (AKA noradrenalin)3. Epinephrine (AKA adrenalin)4. GABA (gamma-aminobutyric acid)5. Serotonin6. Glutamate
Dopamine
Dopamine helps regulate emotional responses. This neurotransmitter also helps control the brain's reward and pleasure centres. Dopamine lets us to not only to see rewards, but it also allows us to take action to move toward these rewards.
Low Dopamine levels in the brain increases our risk for developing an addiction.Further, since dopamine is important for movement, low dopamine levelscan lead to Parkinson-like symptoms. This includes stiffness in the muscles, jerking movements, and a slowing of movement3.
Norepinephrine (AKA noradrenalin)
Norepinephrine helps regulate: Sleep Wakefulness Eating Aggression
Too much noradrenalin causes anxiety
Too little noradrenalin leads to low energy, decreased focus, and problems with one's sleep cycle.
Epinephrine (AKA adrenalin)
Adrenalin is involved in the flight-or-flight response. When released into the body, adrenalin: Increase blood flow to muscles Increases output of the heart Causes pupil dilation Tells the body to release sugar stores so that tissue
(like leg muscle) can use this for energy.
Long term stress or insomnia (lack of sleep) can decrease one’s epinephrine levels.
GABA (gamma-aminobutyric acid)
GABA's main function is to reduce the activity of the brain cells (neurons) it binds to.
Researchers believe that GABA is mainly responsible for controlling the symptoms of fear or anxiety experienced when neurons are overexcited4.
Neurotalks Symposium 2016 12

Serotonin
Adequate amounts of serotonin are necessary for a stable mood. Serotonin also helps regulate:
Carbohydrate (sugar) cravings Sleep cycle Pain perception Proper digestion
Low serotonin levels are linked to poorer immune system functioning, meaning that the body's ability to fight off disease and infection is impaired.
We can deplete our serotonin levels by using stimulant medications or caffeine on a daily basis.
Stimulants are substances which excite physical and/or mental functioning. Specifically, stimulants can impact alertness, attention, energy levels, and can also increase blood pressure, heart rate, and breathing rate. Caffeine is an example of a stimulant: it helps increase arousal, improve focus, decrease sleep, and increase heart rate, among other functions3. ADHD(attention deficit/ hyperactivity disorder) medications are another example of a stimulant4.
Glutamate
Glutamate is important for learning and memory formation, but glutamate can also be damaging to the brain:
1. If there is too much glutamate present, nerve cells can over stimulated.
2. Receptors for glutamate can also become very sensitive and need a much smaller amount of glutamate to be activated.
In both scenarios, neurons are being over stimulated; this can lead to cell damage and even cell death5.
Neurotransmitters and Mental Illness
Our brains need a specific balance of neurotransmitters to work properly and adverse symptoms appear when neurotransmitters are out of balance1.
Small changes in neurotransmitter levels (“keys”), the number of receptors (“locks”), and even how sensitive these “locks” are to “keys” can have BIGeffects on our functioning and overall well-being.
It is not clear what might case these shifts, but there is evidence that the following may play a role: Stress Poor diet Neurotoxins Genetic predisposition Drugs (prescription and recreational) Alcohol Caffeine
Researchers have found clear links between shifts in neurotransmitter levels and some mental illnesses, including: Schizophrenia Depression Bipolar disorder (AKA BPD or manic depression)
Example: SchizophreniaDopamine is strongly linked to symptoms of Schizophrenia.
Two types of receptors important in Schizophrenia are the D1 and D2 dopamine receptors: D2 dopamine receptors:In the striatum (a brain region involved in the reward system6), levels of D2 dopamine receptors are high. D2 receptors in the striatum are linked to positive symptoms like hallucinations and delusions. D1 dopamine receptors:Low levels of D1 dopamine receptors triggers negative symptoms like a lack of emotions (AKA flat emotionality).
Example: DepressionLinked to serotonin, norepinephrine (AKA noradrenalin), and dopamine:
Serotonin:Low levels of serotonin in the brain can trigger symptoms of depression and can also lead to suicidal thoughts.
Norepinephrine:Although norepinephrine levels do not directly cause depression, there is a link between stress and depression.Individuals who experience chronic stress have higher than normal norepinephrine levels. People who are chronically stressed are at greater risk for developing depression.
Dopamine:When people have depression, they are more likely to show lower than normal levels of dopamine.
Neurotalks Symposium 2016 13

Dopamine is involved in the pleasure and reward system of the brain. People with depression are less likely to engage in activities they previously enjoyed. Lower than normal dopamine levels can help explain whydepressed people find less joy in their hobbies.
Example: Bipolar disorder (AKA BPD or Manic Depression)Linked to Serotonin, Dopamine, GABA, and Glutamate:
Serotonin:Individuals with BPD tend to show lower serotonin levels in the brain.
Dopamine:Dopamine may influence the shift between mania and depression, such that:
Elevated dopamine levels are linked to manic episodes, and lower dopamine levels are linked to depressive episodes.
GABA:GABA's main function is to reduce the activity of the brain cells (neurons) it binds to.
This role appears weakened among people with BPD compared to people without BPD.
Glutamate:Glutamate is found in higher than normal levels in certain parts of the brain.
Too much glutamate in the brain can lead to overstimulation of neurons and this can lead to cell damage and even cell death.
References:1https://www.neurogistics.com/TheScience/WhatareNeurotransmi09CE.asp2http://www.dictionary.com/browse/receptor3http://www.mayoclinic.org/diseases-conditions/parkinsons-disease/basics/definition/con-200284884https://www.drugabuse.gov/publications/research-reports/prescription-drugs/stimulants/what-are-stimulants5http://thebrain.mcgill.ca/flash/d/d_04/d_04_m/d_04_m_peu/d_04_m_peu.html6http://web.stanford.edu/group/hopes/cgi-bin/hopes_test/about-glutamate-toxicity/7http://www.schizophreniaforum.org/for/curr/AbiDargham/
Categories of mental disordersA person is said to have a mental disorder when they show problems in their "cognition, emotional regulation, or behaviours" that reflects a problem with psychological, biological, or developmental processes important for one's mental functioning.1
Mental disorders are often linked to difficulty meeting social demands, work-related responsibilities, and other important activities.
The DSM uses categories to classify the many mental disorders2. Among these categories, 6of the most well known are3:
1. Mood disorders (AKA affective disorders)2. Anxiety disorders3. Psychotic disorders4. Substance related and addictive disorders 5. Personality disorders6. Eating disorders
Mood disorders (AKA affective disorders): These disorders describe issues with how a person feels. Sufferers experience persistent extremes in their feelings, meaning some people experience extreme sadness, others experience excessive happiness, while some experience a fluctuation between the two3.Examples: Depression, mania and bipolar disorder (BPD) 2.
Anxiety disorders: The main issue for people suffering with this type of disorder is irrational and overblown fear.Examples: Generalized anxiety disorder (GAD), post-traumatic stress disorder (PTSD), obsessive-compulsive disorder (OCD), panic disorder.
Psychotic disorders: People with this type of disorder have extreme distortions in their sense of reality and how they think. People with psychotic disorders often experience delusions, which is when they believe something is true even when told it isn't3.Examples: schizophrenia
Substance related and addictive disorders: People are diagnosed with this disorder when their consumption of some substance or activityhas changed their behaviour to such an extent that they can't meet social and work-related expectations.
A person may not be able to stop their use of this substance. Substance abuse can lead to the development of other mental disorders like anxiety or mood disorders.Some substances/activities people may abuse are:gambling, setting fire to things, opiates, alcohol, amphetamines, and prescription drugs. Personality disorders: People with this type of disorder show long-lasting, maladaptive, and inflexible patterns in their thinking and behaviour. These qualities impact their social, school, and/or work-related lives and are distressing either to the person with the disorder or to others around them2.3.Examples: antisocial personality disorder (APD), obsessive-compulsive personality disorder2.
Neurotalks Symposium 2016 14

Eating disorders:Individuals who suffer from eating disorders experience an intensepreoccupation with food and weight gain. Their preoccupation impacts their emotions, behaviours, and attitudes3.Examples: Bulimia, Anorexia Nervosa, binge eating disorder.
If you seek complete information about the many mentaldisorders and other categories that exist, you can refer to: ICM (found online for free if you perform a quick
Google search), DSM (check your local library to see if they offer it) Any textbook containing information about abnormal
psychology.
SuicideSuicide means that a person wishes to intentionally end their life. To some people, ending their life seems like the only way they can cope with a tough situation or with difficult feelings.However, many who think about suicide do not actually want to end their life1.
Quick FactsApproximately 4000 Canadians die by suicide every year1.
Suicide accounts for: 24% of all deaths among Canadians aged 15 – 24 16% of all deaths for the age group 25 – 44.
Approximately 181 cases of suicide were reported each year between 2008 and 2012 in Manitoba2.
Between 2008 and 2012, the rate of suicide between the ages of 15 to 65+ in Manitoba was higher among men than it was among women. 10-14 year old boys and girls show similar rates of suicide.
People from oppressed groups who face discrimination and prejudice based on factors like race, sex, sexual orientation, age, and physical or mental ability are more at risk for suicide than their more privileged counterparts.
In Canada, the First Nations and Inuit people are several times more likely to die by suicide than are non-indigenous people3.
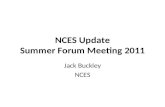
As we can see from figure 10 (page 12), The Inuit community is 6-11 times more likely to die by suicide than the rest of the Canadian population.
Suicide rates among First Nations people are 2 times more likely to die by suicide than the rest of the Canadian population (also on figure 10, page 12).
Figure 10: http://www.heretohelp.bc.ca/visions/aboriginal-people-vol5/aboriginal-mental-health-the-statistical-reality. A graph showing rates of suicide among Inuit, First Nations, and non-indigenous (here, represented by "All Canadians").
Since 1999, 27% of all deaths in Nunavut have been due to suicide3. This rate continues to rise, especially among youth.
Suicide rates vary between First Nations communities, and some First Nations communities are much more at risk for suicide than other communities3. One community recently brought to media attention was a Cree community in Ottawa called Attawapiskat. In early April of 2016, officials declared a state of emergency in this community. In just one day, there were 11 reported suicide attempts and in March, officials recorded 28 suicide attempts4. .
Risk Factors for SuicideTons of factors exist which can lead a person to consider suicide. Some well-known risk-factors are1:
Neurotalks Symposium 2016 15
References:1American Psychiatric Association, 2013, page 202Abnormal Psychology, Fifth Canadian Edition, Wiley, pages 120-1253http://www.epigee.org/6-most-common-types-of-mental-illness.html

History of mental illness History of suicide attempts Family or loved one died by suicide Significant loss (recently fired, death of a loved one,
separation from a partner, etc.) History of trauma Isolation Substance use (like drugs or alcohol) Access to fire arms.
Protective Factors against Suicide (and other mental health problems)
People going through difficult situations or who experience difficult emotions can have a hard time coping with their problems. People can resort to temporary fixes (e.g.: substance use, alcohol, over-exercising, binge-eating, and even sex) to help them avoid dealing with their circumstances or emotions.
These people are often aware that these temporary fixes are harmful, but stopping may be hard anyway because it helps them meet a particular need (example: control, security, physical relief, comfort, etc.)
Although these fixes can make them feel good for a short time, these temporary fixes can add to their problems in the long-run and can even worsen their emotional health5.
This is why it is important for people to findstrategies that revolve around maintaining one’s overall well-being1:
Building social supports:Finding people that you can turn to when you are feeling down will help you get through difficult circumstances.
These are people you can speak to about what you are going through. These are also people who help remind you of your accomplishments, that you are valued, that you are loved, and that the present moment is temporary. These could even be people willing to sit with you in silence to keep you company.Examplesinclude: friends, family, educators, counselors,and spiritual leaders.
Finding positive coping strategiesCoping strategies can help make person’s experience of stress and conflict tolerable6. Coping skills can also help a person solve their problems.Examplesinclude:painting, colouring, spending time with pets, exercising, writing, and going bird-watching.
Seeking support and treatmentIn the treatment options section (pages 16 -18), we will go into some detail about treatment options.
References:1http://www.cmha.ca/mental_health/preventing-suicide/2https://www.gov.mb.ca/health/annstats/as1213.pdf3http://www.heretohelp.bc.ca/visions/aboriginal-people-vol5/aboriginal-mental-health-the-statistical-reality4http://www.rcinet.ca/eye-on-the-arctic/2016/04/13/canadian-parliament-held-emergency-debate-on-suicides-in-indigenous-community/5Report on mental illness in Canada (2002). Retrieved from: http://www.phac-aspc.gc.ca/publicat/miic-mmac/index.html6https://en.wikipedia.org/wiki/Coping_(psychology)#cite_note-3
Treatment Options:Cultural Considerations
Approaches to mental health treatment can vary based on one's culture. Western medical systems tend to understand mental health using a biomedical model1. This approach focuses on biological factors that make a person unhealthy, and do not take into account psychological, social, or environmental influences2.
Traditional indigenous practice, on the other hand, values a holistic approach to mental wellness3.
Traditionally, this approach focuses on culture and spirituality as a form of treatment. The main goal is to help the person regain a state of balance with one's family, community, and the rest of the environment. Thus, one's family and the rest of the community play an important role in helping the sufferer regain their sense of balance3.
Depending on a person's values and needs, the main stream approach to treatment may not always be the best approach. Culture can play an important role in coming up with an effective treatment plan.
PsychopharmaceuticalsPsychopharmaceuticals are prescription drugs which are manufactured to alter the chemistry of the brain. These drugs can be classified based on their function and can be used to treat certain mental disorders.
TypesPsychiatric drugs fall into one of the following categories5:
1. Antipsychotics2. Antianxiety drugs (AKA Anxiolytics)3. Antidepressants4. Stimulants5. Mood stabilizers (AKA antimanic agents)
Neurotalks Symposium 2016 16

AntipsychoticsThese drugs help treat psychosis.
Psychosis describes when a person loses touch with reality and can include delusions and hallucinations.
Psychosis and can be a symptom of mental disorders including: bipolar disorder (BPD), severe depression (AKA psychotic depression), and schizophrenia5.
Antipsychotics are also frequently prescribed in combination with other drugs to help treat mental disorders including5: Generalized Anxiety Disorder (GAD) Severe Depression Post-traumatic stress disorder (PTSD) Attention Deficit Hyperactivity Disorder (ADHD)
Antipsychotics do not cure mental health disorders, but they do help decrease the severity of symptoms so that the user can enjoy a better quality of life.
Antianxiety drugs (AKA Anxiolytics)These types of medication help reduce feelings of anxiety including fear, worry, and anxiety attacks.
Beta blockersare a form of anxiolytic drug, but they are used for short term anxiety symptoms. Beta blockers help reduce the physical symptoms of anxiety like rapid heart rate, sweating, and trembling5.
People can use this medication “as needed”, to help them deal with the short-term physical symptoms of anxiety.
AntidepressantsAntidepressant medications are usually used to help treat depression. This type of medication helps improve depression symptoms and helps prevent these symptoms from returning5.
There are several forms of antidepressants and some people respond better to some types than others. No one quite knows why this is!
StimulantsThese medications increase attention, focus, energy levels, blood pressure,breathing rate, and heart rate. Some users report this medication also has a calming effect4.
Generally, stimulants are prescribed to people diagnosed with Attention Deficit/Hyperactivity Disorder (ADHD).
Mood stabilizers (AKA antimanic agents)These drugs help minimize abnormal brain activity. These drugs are primarily used to “treat bipolar disorder (BPD), mood swings linked to other mental disorders.
Sometimes, they are also used to increase the effect of medications used to treat depression”5
Anticonvulsants, which were originally manufactured to help treat seizures, also have the ability to control unstable moods.
Supervision is important! Mental health workers always weigh the pros and cons of prescribing medications because of the possible complications and side effects that come with use5.
It is very important to receive supervision from a healthcare professional when changing drugs, stopping treatment, or increasing dose because they can help keep an eye out for possible complications.
References:1http://www.pimatisiwin.com/online/wp-content/uploads/2011/08/04VukicGregory.pdf2https://en.wikipedia.org/wiki/Biomedical_model3http://www.heretohelp.bc.ca/visions/aboriginal-people-vol5/aboriginal-mental-health-the-statistical-reality4http://whatmeds.stanford.edu/medications/categories.html5http://www.nimh.nih.gov/health/topics/mental-health-medications/index.shtml#part_149867
How do PsychopharmaceuticalsWork?
Psychiatric medications work by impacting neurotransmitter levels in the brain. Psychiatric medications can do this through one of two ways:
1. Increase effect of neurotransmitterThese types of drugs decrease how quickly neurotransmitters are “reabsorbed" by neurons (brain cells). These drugs do this by preventing enzymes from breaking down neurotransmitters.Enzymes are a special type of protein that helps increase the speed at which a reaction takes place. In the brain, certain enzymes break down neurotransmitters to stop their activity.Example: Anti-depressants like SSRI’s:
One of the major neurotransmitters involved in the onset of depression is serotonin. People with depression have lower levels of serotonin in their brains, and it is believed these low levels of serotonin contribute to symptoms of depression.
SSRI's (selective serotonin reuptake inhibitors) prevent the ability of neurons to reabsorb serotonin. This allows serotonin levels to build up in the brain so that they reach a more normal level.
Neurotalks Symposium 2016 17

By normalizing serotonin levels, depressive symptoms should improve or disappear altogether.2. Decrease effects of neurotransmitterThese dugs interfere with neurotransmitter receptors on a receiving cell. By interfering with the receptor, the neurotransmitter (key) cannot combine with the receptor (lock). If they cannot bind to each other, the message that this neurotransmitter brings can't occur.
Example: Antipsychotics (typical and atypical)These drugs typically affect dopamine levels in the brain.
People with schizophrenia have higher than normal levels of dopamine in their brains. These high dopamine levels contribute to positive symptoms of schizophrenia like delusions.
Antipsychotics help decrease the brain's sensitivity to dopamine by blocking receptors that bind to dopamine. In doing so, these drugs help alleviate some of the disordered thought typical of schizophrenia.
PsychotherapyAlso known as talk therapy, this treatment option connects sufferers with mental health workers like psychiatrists and psychologists to help them with their mental health issues.
This form of treatment allows a person to learn about their condition, moods, thoughts, behaviours, and feelings1. In doing so, talk therapy helps teach the person how to take control of their life and how to cope with difficult situation using positive coping strategies.
Several types of talk therapy exist. A person's situation and needs will help determine which type of therapy will work best for them.Some popular forms of talk therapy showing promising results are:
Psychodynamic therapyThe therapist helps the clientbecome aware oftheir unconscious thoughts and behaviours.
The therapist helps the client gain new understanding about their reasons for acting or thinking in a certain way so the sufferer can fix their issues1.
Interpersonal therapyThe therapist focuses on issues their client has with their relationships. This form of therapy helps clients develop their social skills with others (like friends, peers, and family) 1.
Supportive psychotherapyThe therapist focuses on their client’s healthy patterns of thought and behaviours.
By encouraging these behaviours and thoughts, therapists help clients resolve some of the internal conflict they feel.
The therapist is fully engaged, empathic, encouraging, and supportive to the client.
Clients get better outcomes from this form of therapy when there is a strong sense of trust between the therapist and the client. 2.
Cognitive behaviour therapy (CBT)Therapists help the client pinpoint unhealthy behaviours and thought patterns so that the client can replace them with healthy alternatives1.
Dialectical behaviour therapy (DBT)This is a branch of cognitive behaviour therapy (CBT),
Psychologists have discovered that some peoples’ emotional levels can escalate much more quickly than the average person’s in emotionally charged situations.
Emotionally charged situations are more likely to occur with family, friends, or within romantic relationships3.
DBT focuses on how the client interacts with people in different environments so that they can respond in a more constructive manner.
Acceptance and commitment therapy (ACT)ACT’s two core values are:
1. “Accept what is out of one’s control”4
Client developsmindfulness skills to deal with difficult thoughts and emotions so that they no longer have the same effect on them.
Mindfulness is when a person is mentally aware and focused. This mental state lets the person fully engage in what they are doing at the moment.
In this state, thoughts and feelings that are normally difficult for the client are much less influential over the person4. Examples of mindfulness skills: deep-breathing and meditation
2. “Commit to actions that improve and enrich one’s life”4
The therapist helps you pinpoint your values so the client can use this knowledge to guide and motivate them toadjusttheir life “for the better”4
Neurotalks Symposium 2016 18
References: 1http://www.mayoclinic.org/tests-procedures/psychotherapy/home/ovc-201971882https://en.wikipedia.org/wiki/Supportive_psychotherapy3http://psychcentral.com/lib/whats-the-difference-between-cbt-and-dbt/4http://www.actmindfully.com.au/acceptance_&_commitment_therapy

ResourcesKlinic Community Health Centre:
WEBSITE: www.klinic.mb.ca PHONE: (204) 784-4090 ADDRESS: 870 Portage Avenue
Klinic drop-in counselling:
PHONE: (204) 784-4067 EMAIL: [email protected]
ADDRESS: Central/Downtown:545 Broadway Avenue
Schedule*:Day Time
Mondays & Wednesdays Noon - 7:00 pmTuesdays, Fridays &
SaturdaysNoon - 4:00 pm
ADDRESS: Transcona/River East/Elmwood/ Access Transcona: 845 Regent Avenue West
Schedule*:Day Time
Tuesdays Noon - 7:00 pm
*Times may change. Klinic recommends arriving at least 2 hours before closing time to help ensure you are seen on the day you visit.
24-hour Telephone Services:
Manitoba Suicide Line: 1-877-435-7170
Crisis Line: (204)-786-8686
Toll Free: 1-888-322-3019
Sexual Assault Crisis Line: (204)-786-8631
Toll Free: 1-888-292-7565
Neurotalks Symposium 2016 19

For rural and northern Manitobans:
WEBSITE: www.supportline.ca PHONE: 1-866-367-3276
Schedule:Day Time
Mondays to Fridays 10:00 AM- 9:00 PM
Seneca House:
WEBSITE: http://www.sararielinc.com/community_mental_health_support.php
GENERAL PHONE: (204) 237 9263 ADDRESS: 66 Moore Avenue, Winnipeg SENECA WARMLINE SUPPORT : 204-942-9276 SENECA WARMLINE SCHEDULE: 7:00 PM - 10:00
PM
Disorders Association of Manitoba:
WEBSITE: http://www.mooddisordersmanitoba.ca/ AND http://www.mooddisordersmanitoba.ca/our-services/
ADDRESS: 100 - 4 Fort Street, Winnipeg Peer Support Line PHONE: (204) 786-0987; Toll
Free: 1-800-263-1460 Support E-mail: [email protected] GENERAL EMAIL: [email protected]
Macdonald Youth Services:
WEBSITE: www.mys.ca/AND http://www.mys.ca/programs.php
PHONE: (204) 477-1722 EMAIL:[email protected]
Youth Crisis Stabilization System (YCSS):
PHONE: (204) 949-4777 TOLL-FREE: 1-888-383-2776 YCSS SCHEDULE: 24/7
Mobile Crisis centre:
ADDRESS: 817 Bannatyne MOBILE CRISIS SERVICEPHONE:(204) 940-1781 SCHEDULE: 24/7
Neurotalks Symposium 2016 20
Schedule:Day Time
Mondays to Fridays 9:00 AM - 4:00 PM