Resistance Training for the Client With Metabolic Syndrome
42
Resistance Training for the Client with Metabolic Syndrome By Brad Schoenfeld, MSc, CSCS, CSPS, NSCA-CPT
-
Upload
pooja-manoj -
Category
Documents
-
view
69 -
download
3
description
Resistance training for client with metabolic syndrome.
Transcript of Resistance Training for the Client With Metabolic Syndrome

Resistance Training for the Client with Metabolic Syndrome
By Brad Schoenfeld, MSc, CSCS, CSPS, NSCA-CPT

About the NSCA
The National Strength and Conditioning Association (NSCA) is an
educational nonprofit association committed to supporting and
disseminating research-based knowledge and its practical application to
improve athletic performance and fitness.
The NSCA offers four credentials of distinction:
Certified Strength and Conditioning Specialist® (CSCS®)
NSCA-Certified Personal Trainer® (NSCA-CPT®)
Certified Special Population Specialist™ (CSPS™)
Tactical Strength and Conditioning Facilitator™ (TSAC-F™)
Any webinar questions can be directed to [email protected].

Webinar Quiz
• Available at www.nsca.com/Continuing-
Education/Quizzes-and-Assessments/CEU-Quizzes/
• You must be logged in to purchase quiz
• All webinar quizzes are $20 and are worth 0.2 CEUs
with a passing score of 70% or better.

September 2012
Resistance Training for the Client with Metabolic Syndrome
By Brad Schoenfeld, MSc, CSCS, CSPS, NSCA-CPT

What is Metabolic Syndrome
• Lifestyle disease directly linked
to obesity.
• Primary clinical outcome is
cardiovascular disease.
• Predisposes to other conditions
including polycystic ovary
syndrome, fatty liver, cholesterol
gallstones, asthma, sleep
disturbances, and some forms
of cancer.

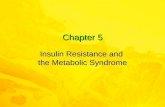
Metabolic Syndrome Stats
• Approximately 25% of
adults in the U.S. have
metabolic syndrome
• Approximately 43% of
those over 60 years of age
have metabolic syndrome
25
43
% Total Population % Over 60
% Afflicted

Then vs. Now…
• In early-hunter gatherer populations,
men hunted 1-4 nonconsecutive days
per week and women gathered food
every 2-3 days (Eaton et al. 2002)
▫ Estimated steps per day: 20,000
• Present Westernized society has
decreased caloric expenditure by
approximately 1200 calories
compared with early 20th century
hunter-gatherer societies (Cordain et
al. 1998)

Effects of Lifestyle on Health
• The prevalence of Type 2 diabetes in
present hunter-gatherer, rudimentary
horticultural, simple agricultural, and
pastoral societies is 1.1% (Diamond,
2003).
• An estimated 32.8% to 38.5% of
female and male Americans,
respectively, born in 2000 who will
contract diabetes during their lifetime
(Narayan et al. 2003)


Clinical identification of metabolic syndrome. Diagnosis is made when at least 3
of the 5 characteristics are present (some say that insulin resistance must be
present for diagnosis).
Risk Factor Defining Level
Abdominal Obesity (by waist circumference
Men
Women
>102 cm (>40 in)
>88 cm (>35 in)
Triglycerides ≥150 mg/dL
HDL Cholesterol
Men
Women
<40 mg/dL
<50 mg/dL
Blood Pressure ≥130/≥85 mm Hg
Fasting Glucose ≥110 mg/dL

Predisposing Factors • Age
• Hispanic or South
Asian descent.
• Family history of type
II diabetes.

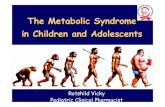
Metabolic Syndrome Flowchart
Genetics Inactivity Diet Obesity
Regular
Exercise
Reduced
Calorie Diet
High Blood
Pressure
Insulin
Resistance Dyslipidemia
Pro
Inflammatory
State
Pro
Thrombotic
State

Metabolic Syndrome and CVD Risk
• The Kuopio Ischaemic Heart Disease Risk Factor
Study of 1209 Finnish men (aged 42 to 60 years) found
that metabolic syndrome increased the risk of
cardiovascular mortality by ~3-4 times after adjustment
of other risk factors (Lakka et al. 2002)
• The Framingham Heart Study showed that metabolic
syndrome alone predicted ≈25% of all new-onset cases
of CVD (Grundy et al. 2004)

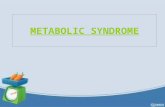
Metabolic Syndrome and Life Expectancy
• Metabolic syndrome is
associated with a ~twofold
increase in all-cause
mortality (Lakka et al. 2002)
▫ Can reduce average life
expectancy by ~5 years
• Even greater effect on
quality of life!
78.2
73.3
70
71
72
73
74
75
76
77
78
79
Normal Life Expectancy Life Expectancy Metabolic Syndrome

The Importance of Exercise
• Physical activity serves as a
key physiological regulator of
thrifty genes to inhibit
unhealthy adiposity (Sinha et
al. 2002)

Metabolic Syndrome and Strength
• Muscular strength is inversely
associated with prevalence of
the metabolic syndrome
▫ Effects are independent of
aerobic fitness as well as age
and smoking

Fitness-Based Intervention
• Weight loss should be the primary target for
intervention in those with metabolic syndrome
• Proper diet and caloric restriction is essential to
achieving weight loss
• A combination of cardiovascular exercise and
resistance training can enhance weight loss, facilitate
weight management, as well as directly improving
measures of cardiovascular risk

Key Point! www.workout911.com
18
• Combined resistance training
and aerobic training is more
effective in combating
metabolic syndrome than either
alone

Exercise Training and Obesity
• Exercise increases energy
expenditure both during and after
training
• Exercise is associated in a
preferential reduction in belly fat
(Hunter et al. 2010)

Exercise Training and Insulin Sensitivity
• Significant improvements in
insulin sensitivity and
glucose uptake
▫ Increased muscle mass
increases uptake capacity
▫ Enhanced GLUT4 response

GLUT4 Translocation Illustrated
Glucose
Plasma Membrane

Time Course of Exercise-Induced Effects
• The effects of exercise on insulin resistance are fairly
short-lived.
▫ Insulin sensitivity in rodents reverted back to baseline
approximately 29–53 hours after exercise (Kump et al.
2005).
▫ Insulin sensitivity declines after 2 weeks of reduced
physical activity in untrained humans (2010).

Key Point! www.workout911.com
23
• Exercise consistency is
paramount to maintaining
insulin sensitivity!

Exercise Training and Lipids
• Lowered triglyceride
concentrations
• Reduced postprandial lipemia
• Decreased concentrations of
small LDL particles
• Increased HDL-C concentrations
• Increased lipoprotein enzyme
activity

Exercise Training and Hypertension
• Reduced BP response to maximal exercise
• Improved HR recovery • Smaller elevations in BP when
performing activities that require muscular effort
• Helps manage co-morbidities (e.g., diabetes)
• Modest reductions in resting BP (~2-4%)

Resistance Training vs. Aerobics
• Potteiger et al. (2012) evaluated the effects of
resistance training vs. aerobic training on
physically inactive overweight males (age 27–
48 years).
▫ Equated training frequency and exercise session
duration combined with energy restriction
▫ Calculated a MetSyn z score from the total of
risk factors (triglycerides, HDL cholesterol,
fasting glucose, waist circumference, and MAP)
▫ Both resistance training and aerobic produced
similar reductions in clinical risk factors for
metabolic syndrome

Exercise Considerations • Medical clearance should be obtained before training the client with
metabolic syndrome.
▫ Consult with physician with respect to any medications
• Monitor BP before and after exercise
▫ Routine check of BP between sets
▫ Uncontrolled hypertension is an absolute contraindication for RT
(>180/110 mm/Hg)
▫ Hypertension of >160/>100 mm/Hg is a relative contraindication for RT
• Avoid holding breath / straining (Valsalva Maneuver)
▫ Exhale during concentric, inhale during eccentric
• Avoid excessive tight gripping (pressor response)
• Be aware for signs of hypoglycemia

Exercise Intervention Program
• Modified super-circuit
training employing a
combination of resistance
and aerobic exercise
• Perform 3, non-consecutive
days per week (e.g. M, W, F)
• Additional moderate intensity
cardio can be performed on
alternate days

Training Protocol Template
• 5-minute warm-up
• Upper body resistance circuit
• 5-10 minutes aerobic exercise
• Lower body resistance circuit
• 5-10 minutes aerobic exercise
• Cool-down

Resistance Training Variables
• Exercise selection
• Intensity
• Sets
• Rest interval
• Tempo

Exercise Selection
• Focus on large muscle groups using
multi-joint movements
▫ The metabolic cost of an exercise is
directly related to the amount of
muscle worked (Elliot et al. 1992)
▫ Greater EPOC (Farinatti et al. 2011)
▫ Enhanced insulin sensitivity of all
major muscle groups
▫ Reduced pressor response

Intensity
• Load should allow for 12-15 sub maximal repetitions • Lower rep ranges (8-10) may
be needed depending on BP response
• Initial loads should equal ~40% 1-RM for upper body and ~50% 1-RM for hips/legs
▫ RPE of 3-4 (“moderate” to
“somewhat hard”)
• Gradually increase intensity
over time
Rating Description
0 Complete rest
1 Very light
2 Fairly light
3 Moderate
4 Somewhat hard
5 Hard
6
7 Very hard
8
9
10 Maximal exertion

Key Point! www.workout911.com
33
• Hypertension is the primary
moderator of resistance
exercise intensity!

Sets
• Begin with a single set in untrained individuals
▫ Acclimation
▫ Single set routines have similar effects on EPOC as
multi-set routines (Heden et al. 2011)
• Progress to 3 sets per exercise
▫ Greater exercise duration heightens energy expenditure
during the workout (Heden et al. 2011)
▫ Increased muscle contractions has greater effect on
glucose uptake

Rest Intervals
• Aim to move as quickly as possible between sets
(<10 seconds)
• Limiting rest intervals between sets (< 30 seconds)
significantly increases caloric expenditure (Haltom et al.,
1999 ).
• Consider acute BP response: longer rest periods (90
seconds) may be required for some to allow blood
pressure to return to baseline, thus requiring a
conventional RT programming

Tempo
• Repetition speed should be fast but controlled (i.e. 1-
0-1)
▫ High-velocity concentric actions increase total energy
expenditure during exercise (Mazzetti et al. 2007)
▫ Faster repetitions reduces the pressor response

Aerobic Exercise Protocol
• Initially, steady state exercise at 40-70%
HRR is best
▫ Higher-intensity interval exercise can be
employed over time to facilitate greater
weight loss and reductions in fasting
insulin concentrations (Trapp et al.
2008).
• Avoid exercises with high ground
reaction forces (e.g. running, step
aerobics, jumping rope)

Measuring Progress
• Skinfold testing generally not
accurate in this population
• Girth measurements are
preferred

Acknowledgements
• A special thanks to my friend and colleague, Paul
Sorace, for his assistance and guidance in
developing this presentation.

Question/Answer
Thank you for coming!
I can be reached through my blog:
www.workout911.com

References • Cordain L, Gotshall RW, Eaton SB, and Eaton SB III. Physical activity, energy expenditure and
fitness: an evolutionary perspective. Int J Sports Med 19: 328-335, 1998.
• Eaton SB, Strassman BI, Nesse RM, Neel JV, Ewald PW, Williams GC, Weder AB, Eaton SB 3rd,
Lindeberg S, Konner MJ, Mysterud I, Cordain L. Evolutionary health promotion. Prev Med. 2002
Feb;34(2):109-18
• Farinatti PT, Castinheiras Neto AG. The effect of between-set rest intervals on the oxygen uptake
during and after resistance exercise sessions performed with large- and small-muscle mass. J
Strength Cond Res. 2011 Nov;25(11):31
• Grundy SM, Brewer HB Jr, Cleeman JI, Smith SC Jr, Lenfant C; American Heart Association;
National Heart, Lung, and Blood Institute. Definition of metabolic syndrome: Report of the
National Heart, Lung, and Blood Institute/American Heart Association conference on scientific
issues related to definition. Circulation. 2004 Jan 27;109(3):433-8
• Harris KA, Holly RG. Physiological response to circuit weight training in borderline hypertensive
subjects. Med Sci Sports Exerc. Jun;19(3):246-52, 1987.
• Hunter GR, Brock DW, Byrne NM, Chandler-Laney PC, Del Corral P, Gower BA. Exercise training
prevents regain of visceral fat for 1 year following weight loss. Obesity (Silver Spring). 2010
Apr;18(4):690-5

References
• Jurca, R., Lamonte, M.J., Church, T. S. et al. Associations of muscle strength and aerobic fitness with metabolic syndrome in
• men. Med. Sci. Sports Exerc. 36:1301–1307, 2004.
• Krough-Madsen R, Thyfault JP, Broholm C, Mortensen OH, Olsen RH, Mounier R, Plomgaard P, Van Hall G, Booth FW, and Pedersen BK. A 2-wk reduction of ambulatory activity attenuates peripheral insulin sensitivity. J Appl Physiol 108: 829–838, 2010.
• Kump D and BoothFW. Alterations in insulin receptor signalling in the rat epitrochlearis muscle upon cessation of voluntary exercise. J Physiol 562: 829–838, 2005.
• Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA. 2002; 288: 2709–2716
• Mazzetti S, Douglass M, Yocum A, Harber M. Effect of explosive versus slow contractions and exercise intensity on energy expenditure. Med Sci Sports Exerc. 2007 Aug;39(8):1291-301.
• Potteiger JA, Claytor RP, Hulver MW, Hughes MR, Carper MJ, Richmond S, Thyfault JP. Resistance exercise and aerobic exercise when paired with dietary energy restriction both reduce the clinical components of metabolic syndrome in previously physically inactive males. Eur J Appl Physiol. 2012 Jun;112(6):2035-44
• Trapp E, Chisholm D, Freund J, and Boutcher S. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int J Obes 32: 1–8, 2008.