Resilience by Design: Improving Hospital Functionality ...
1
Resilience by Design: Improving Hospital Functionality Following Earthquake Megan Boston University of Waikato DESIGN HAZARD ANALYSIS t Displacement STRUCTURAL ANALYSIS DAMAGE EDP Probablity REPAIRS Floor t OPERABILITY RESILIENCE t Functionality RESILIENCE BASED EARTHQUAKE ENGINEERING (RBEE) 0 10 20 30 40 50 60 70 80 90 100 Stairs Wall Partitions Wall Finishings Elevators Sanitary Piping Chiller Large Capacity Cooling Tower Compressor Fire Sprinkler Piping Suspended Ceilings Small Area Suspended Ceilings Large Area Cold/Potable Water Piping Cold/Potable Water Pipe Bracing Hot Water Piping Small Hot Water Pipe Bracing Small Hot Water Piping Large Hot Water Pipe Bracing Large Sanitary Pipe Bracing Chilled Piping Small Chilled Pipe Bracing Small Chilled Piping Large Chilled Pipe Bracing Large Steam Piping Small Steam Pipe Bracing Small Steam Piping Large Steam Pipe Bracing Large HVAC Ducts Small Fire Sprinkler Drops No Repairs Required Repairs Required for Full Recovery Repairs Required for Functional Recovery Repairs Required for Re-occuapncy 0 10 20 30 40 50 60 70 80 90 100 Moment Frame Base Isolated Lighting Percentage of times component is damaged to a hinder functionality Percentage of times component is damaged to a hinder functionality Hospital Component Damage 0 0.2 0.4 0.6 0.8 1.0 Functionality Days Base Isolated 10% Percentile 50% Percentile 90% Percentile 4 8 12 16 0 10% Percentile 50% Percentile 90% Percentile Moment Frame 4 8 12 16 0 Days 0 0.2 0.4 0.6 0.8 1.0 Functionality Resilience Curves Administration Blood Bank Dialysis Emergency Dept ICU 1 ICU 2 Inpatient 1 Inpatient 2 Inpatient 3 Laboratory Maternity Pediatrics Radiology Sterilization Surgery NICU Pharmacy Moment Frame 4 8 12 16 0 Days Administration Blood Bank Dialysis Emergency Dept ICU 1 ICU 2 Inpatient 1 Inpatient 2 Inpatient 3 Laboratory Maternity Pediatrics Radiology Sterilization Surgery NICU Pharmacy Days Base Isolated 4 8 12 16 0 Hospital Service Operability Inoperable Operable Partition Wall Damage No access to Exterior Exits Large Leaks in Piping Ceiling Tile Damage Physical Damage Transformer Damaged Elevators Damaged Stairs Damaged Compressor Damaged Chiller Damaged Boiler Damaged HVAC Piping Damaged Fire Sprinkler Drops Damaged Fire Sprinkler Piping Damage Motor Control Damaged Low Voltage Switchgear Damaged Cooling Tower Damaged HVAC Ducting Damaged Egress Mech/Elec Equipment Fire Sprinklers HVAC Distribution HVAC Equipment HVAC/ Climate Control Nonstructural Damage Effecting Service Area Access to Service Area AND OR OR OR OR OR OR OR OR Introduction Fault Tree Analysis Hospitals are a critical component to community resilience following disasters. Hospitals need to be able to provide needed medical assistance to people injured during the earthquake and continued care to those already in the hospital. Recent policies and guidelines have emphasized the need for hospitals to remain operational following a major disaster. To remain functional, it is critical to understand what types of physical damage contribute to losses of specific hospital services and the loss of the hospital as a whole. In addition to structural damage, damage to nonstructural components such as suspended ceilings, partition walls, and piping, can severely hinder the hospital’s ability to continue providing life saving treatment. The necessity of hospitals to continue to operate and function following an earthquake highlight the need to move beyond code design and beyond performance-based design. Performance-based design moves beyond code-based design by considering the potential damage and downtime of the building. However, it does not provide needed information on the ability of critical facilities, such as hospitals, to continue to operate in the presence of minor to moderate nonstructural damage. Thus, a further level of understanding and analysis is required to accurately predict realistic functionality of a hospital immediately after an earthquake and during the recovery period. Resilience-based design add an additional level of analysis that maps physical damage to actual hospital services and operations to provide a depiction of what real time functionality of a hospital will actually be. Resilience-based design with fault tree analysis can be used: • in scenarios to predict loss-of-service to one or more hospital services given a set of damage • in probabilistic assessments of building performance following a performance-based design analysis • for rapid real time analysis of a hospital’s current state of operability following an event • for developing emergency planning scenarios • to inform decisions on placement of critical equipment, hospital services, and general hospital layout to improve services the hospital can render following an earthquake Conclusions Results For this method of resilience-based design, fault trees are used to map estimated physical damage and downtime (determined following a P-58 PACT assessment) to clinical and non-clinical hospital service. A fault tree is created for each service considered in the hospital. Fault tree consider the phys- ical damage to the service area as well as nonlocalized damage that could also impact the operability of the hospital service. Damaged components feed into the basic events of the fault tree. By following the binary logic up through the tree, it is possible to determine whether a service will be operable or not. Using the downtime estimations for repairs, the fault tree analysis is rerun at each point in time to provide a re- silience curve that shows the change in functionality over time. Changes to the design of the hospital will change the damage and downtime, which will also change the functionality of the hospital. Resil- ience-based design should be an iterative process where changes to the hospital design are made until the build reaches a desired performance and resilience objective. Figure 2. Sample fault tree for checking for nonstructural damage that will effect a service area. Figure 1. Diagram showing the iterative process for resilience-based earthquake engineering. It is a seven-step process that changes the structural and non-structural design of the hospital to meet performance, operability, and resilience objectives. 1. Design the structural and nonstructural components, also consider the building layout, placement of hospital services, and traffic flow through the building. 2. Perform a hazard analysis for the site location. 3. Perform a structural analysis of the building. 4. Estimate damage to structural and non-structural components. 5. Create a repair schedule based on estimated downtimes, mobilization needs, and ambient factors. 6. Use the damage and downtime estimates to determine the operability of individual hospital services. 7. Combine the operability of all hospital services to estimate the functionality of the hospital at any time during the recovery timeframe. Plot the change in functionality over time. Make adjustments to the design until all requirements are meet. Figure 3. Example of damage distribution for two designs of a hospital building. The one on the left is a steel moment frame design with a long period. The one on the right is the same hospital with added base-isolation. The results show the percentage of times a component is damaged to a certain level. Each hospital design was analyzed for 2000 realizations. The colors indicate the level of damage in terms of functionality: no repairs require, repairs required before the building can be re-occupied, repairs required before the building can be used for its intended function (functional Recovery), and repairs required to restore building to the pre-earthquake state (full recovery). Changing the design from a moment frame to a base isolated frame decreases the amount and severity of damage in the hospital. Figure 4. For each realization of the damage and downtime analysis, the results can be fed into the fault trees to determine what hospital services are inoperable or operable immediately after the earthquake and during the recovery. The results above are for the realization that had the median amount of downtime for all the results. Hospital components that were damaged and required repairs to meet re-occupancy and functional recovery were used as inputs to the fault tree analysis. Based on the layout of the hospital, the location of physical damage, and the fault tree logic, each hospital service is analyzed to determine if it is operable. Due to the decrease of damaged components in the base isolated building, there is a lower loss of operability in the hospital as a whole compared to the regular moment frame hospital. Figure 5. The operability of each service can be combined to estimate the overall functionality of the hospital over time. The graphs above show the resilience curve for the two hospital models. Resilience is shown as the functionality of the hospital over time. Due to more severe and distributed damage in the moment frame model, this model experiences a longer period of reduced services and restoration of functionality. It has lower resilience to the earthquake than the base isolated model which has a rapid recovery and functionality restoration after an earthquake. Future Work This resilience-based design framework can be expand to: • different building occupancy types • multi-hazard analysis • city wide resilience analysis
Transcript of Resilience by Design: Improving Hospital Functionality ...

Resilience by Design:Improving Hospital Functionality Following Earthquake
Megan BostonUniversity of Waikato
DESIGN
HAZARD ANALYSIS
t
Dis
plac
emen
t
STRUCTURAL ANALYSIS
DAMAGE
EDP
Prob
ablit
y
REPAIRS
Floo
r
t
OPERABILITY
RESILIENCE
t
Func
tiona
lity
RESILIENCE BASED
EARTHQUAKE ENGINEERING
(RBEE)
0 10 20 30 40 50 60 70 80 90 100
StairsWall Partitions
Wall Finishings
Elevators
Sanitary Piping
Chiller Large CapacityCooling Tower
Compressor
Fire Sprinkler Piping
Suspended Ceilings Small AreaSuspended Ceilings Large Area
Cold/Potable Water PipingCold/Potable Water Pipe Bracing
Hot Water Piping SmallHot Water Pipe Bracing Small
Hot Water Piping LargeHot Water Pipe Bracing Large
Sanitary Pipe BracingChilled Piping Small
Chilled Pipe Bracing SmallChilled Piping Large
Chilled Pipe Bracing LargeSteam Piping Small
Steam Pipe Bracing SmallSteam Piping Large
Steam Pipe Bracing Large
HVAC Ducts Small
Fire Sprinkler Drops
No RepairsRequired
Repairs Requiredfor Full Recovery
Repairs Requiredfor Functional Recovery
Repairs Requiredfor Re-occuapncy
0 10 20 30 40 50 60 70 80 90 100
Moment Frame Base Isolated
Lighting
Percentage of times component is damaged to a hinder functionality Percentage of times component is damaged to a hinder functionality
Hospital Component Damage
0
0.2
0.4
0.6
0.8
1.0
Func
tiona
lity
Days
Base Isolated
10% Percentile
50% Percentile
90% Percentile
4 8 12 160
10% Percentile
50% Percentile
90% Percentile
Moment Frame
4 8 12 160Days
0
0.2
0.4
0.6
0.8
1.0
Func
tiona
lity
Resilience Curves
AdministrationBlood Bank
DialysisEmergency Dept
ICU 1ICU 2
Inpatient 1Inpatient 2Inpatient 3Laboratory
Maternity
Pediatrics
RadiologySterilization
Surgery
NICU
Pharmacy
Moment Frame
4 8 12 160Days
AdministrationBlood Bank
DialysisEmergency Dept
ICU 1ICU 2
Inpatient 1Inpatient 2Inpatient 3Laboratory
Maternity
Pediatrics
RadiologySterilization
Surgery
NICU
Pharmacy
Days
Base Isolated
4 8 12 160
Hospital Service Operability
Inoperable Operable
Partition Wall
Damage
No access to Exterior
Exits
Large Leaks in Piping
Ceiling Tile
Damage
Physical Damage
Transformer Damaged
Elevators Damaged
Stairs Damaged
Compressor Damaged
Chiller Damaged
Boiler Damaged
HVAC Piping
Damaged
Fire Sprinkler
Drops Damaged
Fire Sprinkler
Piping Damage
Motor Control
Damaged
Low Voltage
Switchgear Damaged
Cooling Tower
Damaged
HVAC Ducting
Damaged
Egress Mech/Elec Equipment
Fire Sprinklers HVAC Distribution
HVAC Equipment
HVAC/ Climate Control
Nonstructural Damage Effecting Service Area
Access to Service Area
ANDOR
OR
OROROROR
OR
OR
Introduction
Fault Tree Analysis
Hospitals are a critical component to community resilience following disasters. Hospitals need to be able to provide needed medical assistance to people injured during the earthquake and continued care to those already in the hospital. Recent policies and guidelines have emphasized the need for hospitals to remain operational following a major disaster. To remain functional, it is critical to understand what types of physical damage contribute to losses of specific hospital services and the loss of the hospital as a whole. In addition to structural damage, damage to nonstructural components such as suspended ceilings, partition walls, and piping, can severely hinder the hospital’s ability to continue providing life saving treatment.
The necessity of hospitals to continue to operate and function following an earthquake highlight the need to move beyond code design and beyond performance-based design. Performance-based design moves beyond code-based design by considering the potential damage and downtime of the building. However, it does not provide needed information on the ability of critical facilities, such as hospitals, to continue to operate in the presence of minor to moderate nonstructural damage. Thus, a further level of understanding and analysis is required to accurately predict realistic functionality of a hospital immediately after an earthquake and during the recovery period. Resilience-based design add an additional level of analysis that maps physical damage to actual hospital services and operations to provide a depiction of what real time functionality of a hospital will actually be.
Resilience-based design with fault tree analysis can be used: • in scenarios to predict loss-of-service to one or more hospital services given a set of damage • in probabilistic assessments of building performance following a performance-based design analysis• for rapid real time analysis of a hospital’s current state of operability following an event• for developing emergency planning scenarios• to inform decisions on placement of critical equipment, hospital services, and general hospital layout to improve services the hospital can render following an earthquake
Conclusions
Results
For this method of resilience-based design, fault trees are used to map estimated physical damage and downtime (determined following a P-58 PACT assessment) to clinical and non-clinical hospital service. A fault tree is created for each service considered in the hospital. Fault tree consider the phys-ical damage to the service area as well as nonlocalized damage that could also impact the operability of the hospital service.
Damaged components feed into the basic events of the fault tree. By following the binary logic up through the tree, it is possible to determine whether a service will be operable or not. Using the downtime estimations for repairs, the fault tree analysis is rerun at each point in time to provide a re-silience curve that shows the change in functionality over time. Changes to the design of the hospital will change the damage and downtime, which will also change the functionality of the hospital. Resil-ience-based design should be an iterative process where changes to the hospital design are made until the build reaches a desired performance and resilience objective.
Figure 2. Sample fault tree for checking for nonstructural damage that will effect a service area.
Figure 1. Diagram showing the iterative process for resilience-based earthquake engineering. It is a seven-step process that changes the structural and non-structural design of the hospital to meet performance, operability, and resilience objectives. 1. Design the structural and nonstructural components, also consider the building layout, placement of hospital services, and traffic flow through the building. 2. Perform a hazard analysis for the site location. 3. Perform a structural analysis of the building. 4. Estimate damage to structural and non-structural components. 5. Create a repair schedule based on estimated downtimes, mobilization needs, and ambient factors. 6. Use the damage and downtime estimates to determine the operability of individual hospital services. 7. Combine the operability of all hospital services to estimate the functionality of the hospital at any time during the recovery timeframe. Plot the change in functionality over time. Make adjustments to the design until all requirements are meet.
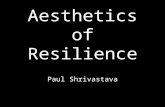
Figure 3. Example of damage distribution for two designs of a hospital building. The one on the left is a steel moment frame design with a long period. The one on the right is the same hospital with added base-isolation. The results show the percentage of times a component is damaged to a certain level. Each hospital design was analyzed for 2000 realizations. The colors indicate the level of damage in terms of functionality: no repairs require, repairs required before the building can be re-occupied, repairs required before the building can be used for its intended function (functional Recovery), and repairs required to restore building to the pre-earthquake state (full recovery). Changing the design from a moment frame to a base isolated frame decreases the amount and severity of damage in the hospital.
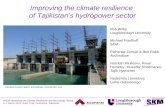
Figure 4. For each realization of the damage and downtime analysis, the results can be fed into the fault trees to determine what hospital services are inoperable or operable immediately after the earthquake and during the recovery. The results above are for the realization that had the median amount of downtime for all the results. Hospital components that were damaged and required repairs to meet re-occupancy and functional recovery were used as inputs to the fault tree analysis. Based on the layout of the hospital, the location of physical damage, and the fault tree logic, each hospital service is analyzed to determine if it is operable. Due to the decrease of damaged components in the base isolated building, there is a lower loss of operability in the hospital as a whole compared to the regular moment frame hospital.
Figure 5. The operability of each service can be combined to estimate the overall functionality of the hospital over time. The graphs above show the resilience curve for the two hospital models. Resilience is shown as the functionality of the hospital over time. Due to more severe and distributed damage in the moment frame model, this model experiences a longer period of reduced services and restoration of functionality. It has lower resilience to the earthquake than the base isolated model which has a rapid recovery and functionality restoration after an earthquake.
Future WorkThis resilience-based design framework can be expand to:• different building occupancy types• multi-hazard analysis• city wide resilience analysis