
RESIDENT / HUMANITARIAN COORDINATOR REPORT ON … · Cox‟s Bazar and the inter-agency forum for...
41
Resident / Humanitarian Coordinator Report on the use of CERF funds RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS BANGLADESH RAPID RESPONSE DISPLACEMENT 2016 RESIDENT/HUMANITARIAN COORDINATOR Robert Watkins
Transcript of RESIDENT / HUMANITARIAN COORDINATOR REPORT ON … · Cox‟s Bazar and the inter-agency forum for...

Resident / Humanitarian Coordinator
Report on the use of CERF funds
RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS
BANGLADESH RAPID RESPONSE
DISPLACEMENT 2016
RESIDENT/HUMANITARIAN COORDINATOR Robert Watkins

2
REPORTING PROCESS AND CONSULTATION SUMMARY
a. Please indicate when the After Action Review (AAR) was conducted and who participated.
The After-Action Review took place on 23 July 2017. All Agencies concerned by the CERF RR allocation participated to the review.
b. Please confirm that the Resident Coordinator and/or Humanitarian Coordinator (RC/HC) Report was discussed in the Humanitarian and/or UN Country Team and by cluster/sector coordinators as outlined in the guidelines.
YES NO
c. Was the final version of the RC/HC Report shared for review with in-country stakeholders as recommended in the guidelines (i.e. the CERF recipient agencies and their implementing partners, cluster/sector coordinators and members and relevant government counterparts)?
YES NO
Following its review by the CERF Secretariat, the final version of the RC/HC Report will be shared with in-country stakeholders as recommended in the guidelines.

3
I. HUMANITARIAN CONTEXT
TABLE 1: EMERGENCY ALLOCATION OVERVIEW (US$)
Total amount required for the humanitarian response: 41,000,000
Breakdown of total response funding received by source
Source Amount
CERF 3,090,269
COUNTRY-BASED POOL FUND (if applicable)
OTHER (bilateral/multilateral) 4,215,538
TOTAL 7,305,807
TABLE 2: CERF EMERGENCY FUNDING BY ALLOCATION AND PROJECT (US$)
Allocation 1 – date of official submission: 22/12/2016
Agency Project code Cluster/Sector Amount
IOM 16-RR-IOM-042 Water, Sanitation and Hygiene 236,149
IOM 16-RR-IOM-043 Health 187,093
IOM 16-RR-IOM-044 Shelter 980,591
UNFPA 16-RR-FPA-055 Health 399,999
UNFPA 16-RR-FPA-054 Sexual and/or Gender-Based Violence 203,895
UNICEF 16-RR-CEF-129 Child Protection 107,873
UNICEF 16-RR-CEF-130 Nutrition 282,667
WFP 16-RR-WFP-072 Food Aid 692,002
TOTAL 3,090,269
TABLE 3: BREAKDOWN OF CERF FUNDS BY TYPE OF IMPLEMENTATION MODALITY (US$)
Type of implementation modality Amount
Direct UN agencies/IOM implementation 2,528,715
Funds forwarded to NGOs and Red Cross / Red Crescent for implementation 561,554
Funds forwarded to government partners
TOTAL 3,090,269

4
HUMANITARIAN NEEDS In November 2016, a surge of population comprising mainly of rural families with cultural and ethnic similarities with the bordering communities in south eastern Bangladesh crossed the border from the northern part of Rakhine State into Bangladesh. The majority of the mass influx has been into Cox‟s Bazar district through different entry points in land border or marine channel. Teknaf (Leda Makeshift Settlement, Shamlapur) and Ukhia (Kutupalong Makeshift Settlement) Upazilas, which were already hosting a large number of both registered refugees and undocumented Myanmar nationals (UMNs) recorded the highest influx. On 26 November 2016, the United Nations in Bangladesh released a Joint Humanitarian Contingency Plan to define preparedness and response actions to cope with the influx of Rohingya refugees from Rakhine State, Myanmar into Cox‟s Bazar, Bangladesh. The plan considered lessons learned and needs identified from previous responses to cross-border displacements in order to ensure that the humanitarian community was able to deliver an effective and timely integrated response. The Joint Humanitarian Contingency Plan concerned a caseload of 50,000 people (60% women, 40% men) including 25,000 children. At that time, the specific number of the new arrivals was difficult to ascertain accurately due to the sensitivity of the matter and the fact that the new refugees were on-the-move and thus were staying in assessed locations for a limited period of time while seeking refuge and livelihood opportunities in other areas. As of 03 December 2016, the United Nations in Bangladesh indicated that at least 22,000 people (10,229 men, 11,771 women including 12,102 children) had already arrived into Cox‟s Bazar. Eventually, from ISCG Needs and Population Reports, we know that 75,000 Rohingya people arrived in Bangladesh since the outbreak of violence in 2016 in North Rakhine in the first months of implementation of the CERF-funded projects. In August 2017, this number of newly arrived Rohingya population continues to increase and has reached more than 87,000 persons. According to the Multi-Sector Initial Rapid Assessment (MIRA) report conducted from 24 November to 1 December 2016, the new arrivals came from more than 50 villages in Rakhine state, Myanmar. The duration of their journey to Cox‟s Bazar district in Bangladesh varied between 7 to 30 days. New Rohingya refugees included unaccompanied children, pregnant and lactating women, people with disabilities, victims of torture, abuse or exploitation (before undertaking or during their journey to Bangladesh) including sexual violence notably rape. Rohingya in Rakhine were already considered very vulnerable, suffering from poverty, high levels of food insecurity, and high rates of malnutrition in young children. The vast majority of them have reached Bangladesh without any personal belongings. The sudden influx in south eastern Bangladesh has increased the number of highly vulnerable Rohingya refugees, exceeding the absorption capacity of the on-going and critically underfunded assistance provided in the underdeveloped district of Cox‟s Bazar. As a result, there has been a sudden and marked deterioration of the humanitarian situation, including an alarming level of malnutrition in the camps, high levels of psycho-social stress due to low birth spacing, large family sizes and cramped living conditions; poor sanitation and hygiene practices; inadequate access to safe drinking water. In the context of the new influx and the sudden deterioration of the humanitarian situation, women‟s and girls‟ vulnerability to Sexual and Gender Based Violence (SGBV) increased. Triggering factors included: heightened level of stress, restricted mobility and privacy, disrupted services and weakened protection. The stressful overcrowded living conditions and scarce resources led to negative coping mechanisms including begging, survival sex work and sex for food. Latrines and bathing facilities were a key source of concern as they were not sufficient in number, not well lit, and not sufficiently sex-segregated. The large majority of new arrivals were impoverished, irregular day labourers, many of whom were already reliant on WFP assistance in in Myanmar. The food security situation of the new arrivals and their hosts steadily worsened in Bangladesh. Adults were managing with only one meal per day. Female-headed households were especially vulnerable. 48 percent of under 5 children were malnourished. The prevalence of acute malnutrition in Teknaf and Ukhiya Upazilas was serious (12.5 percent. In 2014 already, the Kutupalong official camp recorded a moderate acute malnutrition (MAM) rate of 11 per cent and a severe acute malnutrition (SAM) rate of 2 per cent in the Nayapara official camp, the MAM rate was 13 per cent, and the SAM rate was 1 per cent. Due to the poor pre-crisis nutrition status as well as the aggravating factors, the nutritional situation of the population was rapidly deteriorating. The arrival of UMNs created a strain to the existing water and sanitation infrastructure within the registered refugee camps, makeshift settlements of Leda, Kutupalong and Shamlapur and in villages of Ukhia and Teknaf Upazilas. There were insufficient sanitation facilities (toilets, bathrooms) in the settlements to serve the increasing number of users. To minimize the risk of disease outbreaks due to poor sanitation and improper hygiene practices, the provision of sanitation facilities as well as hygiene promotion were urgently needed. About 45 per cent of the new arrivals did not have access to adequate water supply while only 2 per cent had access to their relatives‟ latrines and as high as 95 per cent were practicing open defecation. The level of hygiene practices was very poor as about 94 per cent of the
5
new arrivals were not practicing handwashing due to lack of soap and 91 per cent of adolescent girls and women faced challenges during menstruation. The influx of the new arrivals exacerbated existing gaps in supporting the provision of primary and secondary health services, including emergency services, in both the makeshift settlements as well as Government facilities in Ukhiya Upazila. Key triggers of the deterioration of the health situation included: increased size of the community trying to access basic health care services; insufficient health care personnel, especially female doctors and paramedics, equipment and drugs; lack of regular medical supplies including family planning commodities, which threatens population health and well-being. Furthermore, the number of people staying in one room was extremely high in some cases, as almost 8 per cent of the households in the MIRA sample (n=584) reported that more than 17 people were sharing one room. As the winter months were bringing additional health risks to population without adequate shelter.
II. FOCUS AREAS AND PRIORITIZATION
At the time of the CERF RR application, humanitarian partners in Bangladesh were developing a Humanitarian Response Plan (HRP) that took into consideration the planning assumptions of the Joint Humanitarian Contingency Plan developed at inter-agency level and released on 26 November 2017. The 6-month HRP plan (valued US$ 41 million) articulated the shared vision of the international community on how to respond to the assessed and expressed needs of the estimated caseload of 50,000 new Rohingya directly affected by the crisis. Building on the existing Joint Humanitarian Contingency Plan, the HRP focused on the following strategic objectives:
1. Advocacy efforts with relevant authorities for the respect of humanitarian principles and the creation of a conducive environment that allows humanitarian access to the new Rohingya refugees and enables people in need of life-saving services to access basic services;
2. Protection services to restore safety and dignity of the new arrivals, including effective response to and prevention of SGBV cases and abuse (incl. survival sex work, food for sex); equitable access to SGBV service providers; access for vulnerable children to child protection services and other basic services, protection monitoring/assessments; equitable access to psychosocial support;
3. Immediate life-saving assistance, including strengthening of current humanitarian assistance programmes in health, food security/nutrition, wash.
Out of these overarching HRP strategic objectives (SO), the Resident Coordinator (RC), in consultation with the UNCT Sub-Group for Cox‟s Bazar and the inter-agency forum for humanitarian assistance in Cox‟s Bazar (NGOs, UN representatives, Development Partners) determined that the CERF proposal would focus on SO2 and SO3 “Protection services to restore safety and dignity of the new arrivals” and “Immediate life-saving assistance”. The CERF-supported response targeted 22,000 new arrivals in Cox‟s bazar out of the total caseload of 50,000 individuals directly affected by the current crisis, as indicated in the overall Joint Humanitarian Contingency Plan. The geographical location of the individuals targeted with CERF funding were the two official settlements located in Nayapara (Teknaf) and Kutupalong (Ukhiya), as well as the makeshift settlements (particularly in and around the Teknaf and Ukhiya Upazilas (sub-districts), and the host communities. The CERF allocation aimed to address the most critical and life-saving humanitarian needs in the following key sectors of this humanitarian response: Protection, Food, Nutrition, Wash, Health and Shelter. The prioritization of the geographical and sectoral focus of the CERF request was also informed by the Multi-Cluster/Sectoral Initial Rapid Assessment (MIRA) conducted from 24 November to 1 December 2016 by the Inter-Agency Emergency Coordination Team in Cox‟s Bazar to support the identification of acute humanitarian needs of the new arrivals.
III. CERF PROCESS
The following needs assessments informed the CERF prioritization process: i) available secondary data related to the Rohingya population; ii) Initial Multi-Cluster Rapid Needs Assessment – MIRA, conducted by national and international humanitarian partners from 24 November to 1 December 2016. Throughout the prioritization process, consultations at operational level took place between agencies and the RCO. At a more strategic level, the RC maintained a constant dialogue with the Ministry of Disaster Management and Relief (MoDMR), the Ministry of Foreign Affairs (MoFA) and the Prime Minister‟s Office (PMO).

6
The following sectors were highlighted as key priorities where immediate and life-saving support was required: Protection, Food Security/Nutrition, Wash, Health. A CERF prioritisation meeting was convened by the RCO on 7 December 2016, with the participation of representatives from agencies of the prioritised sectors. During the meeting, agencies discussed the assessment initial findings and agreed on the overall strategic parameters for the CERF-supported response. The discussion focused on the following elements: i) agreement on the key priority sectors for the immediate response (Protection, Food, Nutrition, Wash, Health); ii) validation of the geographic areas to focus the life-saving interventions (Cox‟s Bazar – registered refugee camps, host communities, makeshift camps); iii) determination of the caseload for the CERF-supported response and prioritization of the beneficiary groups. The key criteria and parameters to select projects for inclusion in the CERF submission were also discussed during the CERF prioritization meeting held on 7 December. Key criteria and parameters followed to prioritise projects for CERF support included the following: • Directly related to the Rohingya influx response. • Adhere to „life-saving‟ criteria and centre around the most (not all) essential humanitarian needs. • For humanitarian projects. • Based on partnerships/complementarity of interventions. • Be informed by a larger response strategy. • Complemented by other funding sources. • Direct assistance to be implemented within 4 months (6 months to complete all project activities and deplete the funds) • Access, discreet and low-profile interventions, building on existing basic services (as requested by the Government) Based on the endorsed guidance and overarching priorities established, sectors identified priority projects/activities for CERF funding. Projects/activities were selected based on the following jointly agreed criteria: i) available needs assessments data; ii) funding situation; iii) compliance with the CERF life-saving criteria; iv) agencies‟ operational capacity to implement the activities within up to the first six months of the response; Agencies prepared CERF grant proposals for prioritized projects. In most cases, agencies consulted with respective regional or headquarters emergency/CERF Focal Points during this drafting stage. Most UN agencies took into consideration gender equality issues in their respective projects, underpinned, where possible, by gender analysis. Where more than one project was to be submitted within a sector, the principle of complementarity between the projects was implemented. The RC, with support from the Resident Coordinator Office (RCO) and the OCHA Regional Office for Asia and the Pacific (ROAP), ensured that drafted proposals met the necessary requirements. The RC also validated the specific amount requested by each proposal and agency. This included an appraisal of pledges or contributions received. The RCO/OCHA team consolidated the application package and completed Parts I and II of the application template.
IV. CERF RESULTS AND ADDED VALUE
TABLE 4: AFFECTED INDIVIDUALS AND REACHED DIRECT BENEFICIARIES BY SECTOR1
Total number of individuals affected by the crisis: 50,000
Cluster/Sector
Female Male Total
Girls
(< 18)
Women
(≥ 18) Total Boys
(< 18)
Men
(≥ 18) Total
Children
(< 18)
Adults
(≥ 18) Total
Child Protection 4,459 4,459 4,194 4,194 8,653 8,653
Food Aid 10,726 7,836 18,562 9,581 5,883 15,464 20,307 13,719 34,026
Health 9,852 17,960 27,812 7,376 6,649 14,025 17,228 24,609 41,837
7
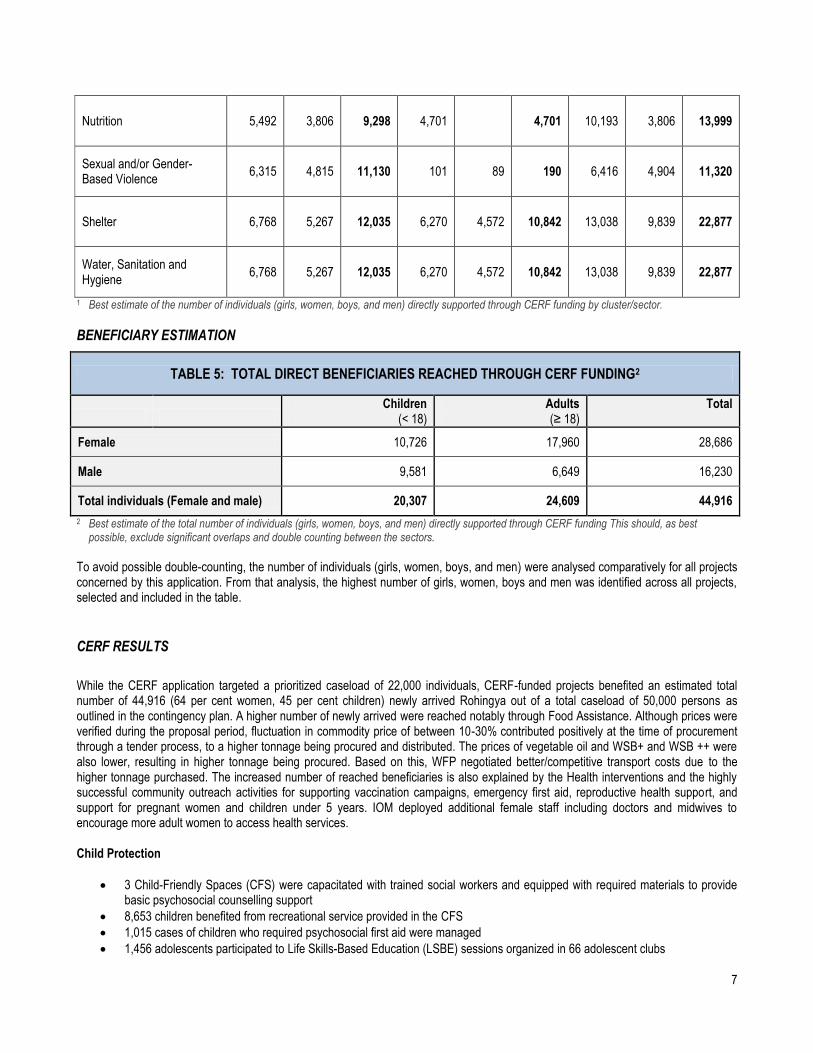
Nutrition 5,492 3,806 9,298 4,701 4,701 10,193 3,806 13,999
Sexual and/or Gender-Based Violence
6,315 4,815 11,130 101 89 190 6,416 4,904 11,320
Shelter 6,768 5,267 12,035 6,270 4,572 10,842 13,038 9,839 22,877
Water, Sanitation and Hygiene
6,768 5,267 12,035 6,270 4,572 10,842 13,038 9,839 22,877
1 Best estimate of the number of individuals (girls, women, boys, and men) directly supported through CERF funding by cluster/sector.
BENEFICIARY ESTIMATION
TABLE 5: TOTAL DIRECT BENEFICIARIES REACHED THROUGH CERF FUNDING2
Children
(< 18) Adults (≥ 18)
Total
Female 10,726 17,960 28,686
Male 9,581 6,649 16,230
Total individuals (Female and male) 20,307 24,609 44,916
2 Best estimate of the total number of individuals (girls, women, boys, and men) directly supported through CERF funding This should, as best possible, exclude significant overlaps and double counting between the sectors.
To avoid possible double-counting, the number of individuals (girls, women, boys, and men) were analysed comparatively for all projects concerned by this application. From that analysis, the highest number of girls, women, boys and men was identified across all projects, selected and included in the table.
CERF RESULTS
While the CERF application targeted a prioritized caseload of 22,000 individuals, CERF-funded projects benefited an estimated total number of 44,916 (64 per cent women, 45 per cent children) newly arrived Rohingya out of a total caseload of 50,000 persons as outlined in the contingency plan. A higher number of newly arrived were reached notably through Food Assistance. Although prices were verified during the proposal period, fluctuation in commodity price of between 10-30% contributed positively at the time of procurement through a tender process, to a higher tonnage being procured and distributed. The prices of vegetable oil and WSB+ and WSB ++ were also lower, resulting in higher tonnage being procured. Based on this, WFP negotiated better/competitive transport costs due to the higher tonnage purchased. The increased number of reached beneficiaries is also explained by the Health interventions and the highly successful community outreach activities for supporting vaccination campaigns, emergency first aid, reproductive health support, and support for pregnant women and children under 5 years. IOM deployed additional female staff including doctors and midwives to encourage more adult women to access health services. Child Protection
3 Child-Friendly Spaces (CFS) were capacitated with trained social workers and equipped with required materials to provide basic psychosocial counselling support
8,653 children benefited from recreational service provided in the CFS
1,015 cases of children who required psychosocial first aid were managed
1,456 adolescents participated to Life Skills-Based Education (LSBE) sessions organized in 66 adolescent clubs

8
492 adolescents completed 11 LSBE sessions
528 interactive sessions were conducted by the adolescent groups
6 adolescents Interactive Popular Theatre (IPT) groups and performances were organized
25 Community Based Child Protection Committees (CBCPCs) were made fully functional and organized public debates and discussions on issues related to child marriage, child labour and corporal punishment
1,015 cases of children in the need of protection were referred by CBCPC‟s social workers and managed by relevant service providers
184 unaccompanied and separated children were identified, among them 27 children reunited with their families during project period
Food Aid
34,026 new arrivals received food assistance
731 MT of rice was procured and distributed
6,811 households received planned general food distributions in time
3,633 children, PLWs and TB patients receiving food assistance
Messaging and counselling on specialized nutritious foods, Infant & Young Child Feeding (IYCF) practices, maternal care and nutrition were implemented effectively
Health
26,914 new arrivals had access to primary health care
8,127 new arrivals received first aid emergency assistance
3,225 patients received medical assistance in eight IOM health facilities provided with essential medicines and equipped
8 vaccination centres were established to provide access to vaccination services to children under five
422 deliveries were safely conducted in all targeted facilities
230 ante-natal care cases were safely managed
84 obstetric emergencies managed in Ukhiya Upazila health complex
1,000 pregnant women provided with Safe Delivery Kits
100% health facilities equipped with Rape Treatment Kits to provide treatment for rape survivors
Immediate access to GBV related information and clinical services made available
5,000 condoms were distributed at health facilities
3, 006 patients were provided with emergency transportation through a voucher distribution programme Nutrition
6,122 children under 5 were screened for malnutrition
750 children under 5 referred and treated for Severe Acute Malnutrition (SAM)
94 community nutrition workers and volunteers as well as 114 governmental health service providers were trained on Infant Young Child Feeding in emergency (IYCF-E) practices
3,806 Pregnant and Lactating Women (PLW) were counselled on IYCF practices
2,632 children of 6 to 23-month-old received Micronutrient Powder (MNP) supplementation
9,352 children under 5 and adolescent received deworming treatment Sexual and/or Gender-Based Violence
11,320 women‟s and girls were supported for responding to their GBV-related psychological needs
8 psycho-social counsellors were hired and deployed to conduct 180 psycho-social counselling sessions
3 Women Friendly Spaces were established to provide safe space for women and girls, psycho-social counselling service and functioning referral for GBV survivors
3,600 Dignity Kits including garments, sanitary napkins, safety whistles, torch and personal hygiene products were distributed
7,200 women and girls of reproductive age received Dignity Kits and blankets to restore their sense of dignity

9
Shelter
22,877 new arrivals benefited from emergency shelter assistance
A total of 4,620 of the most vulnerable newly arrived UMNs were provided with shelter materials and essential basic supplies (general NFI kits) that included items such as mosquito net, utensils, basic clothing articles, and a bag to carry the items.
17,196 plastic tarps and 4,982 canvas tarps were distributed Water, Sanitation and Hygiene
22,877 new arrivals had access to 15 litres of safe water per person per day
Access to safe water was facilitated to ensure a total water collection time of 30 minutes maximum for a round trip including queuing for all targeted persons
6,450 hygiene kits were distributed
3 ring wells were connected by gutters and one rainwater pond connected to roof catchment by gutters and PVC pipes
An existing rain water pond was also maintained throughout the project and connected to the roof catchments to harvest rainwater
20 Deep tube-wells were installed; and 5 community latrines were constructed
60 household latrines built; 30 bathing cubicles constructed; formed 6 groups of adolescent girls with 134 participants and conducted menstrual hygiene sessions; all 5 community latrines had hand washing devices installed.
CERF’s ADDED VALUE
a) Did CERF funds lead to a fast delivery of assistance to beneficiaries? YES PARTIALLY NO CERF funds led to a fast delivery of assistance to beneficiaries for all CERF funded projects. For instance, emergency latrines were constructed in 48 hours and the mass vaccination campaign for Measles Rubella-Oral Polio Vaccine (MR-OPV) was undertaken swiftly. Moreover, CERF funds brought life-saving reproductive health services closer to the beneficiaries, reducing significantly travel time for the provision of emergency care. The establishment of 24/7 referral pathways eliminated the time and distance inconvenience for referral. The delivery of Clean Delivery Kits ensured timely, sage and clean deliveries. Moreover, the distribution of Dignity Kits within the three weeks was made possible by the CERF. It provided women and girls with means for safe mobility in the settlement areas to access information, services and peer support networks. The fast delivery of assistance was achieved despite challenging unfavourable weather conditions (heavy monsoon rain).
b) Did CERF funds help respond to time critical needs1? YES PARTIALLY NO CERF funds helped respond to time-critical needs of highly vulnerable and destitute persons as planned in all concerned projects. For instance, CERF funding allowed the timely critical response to disease outbreaks. It also contributed to the delivery of psychological first aid and emergency service referral for unaccompanied women and children exposed to acute forms of violence including witnessing extra-judicial murders, experiencing sexual violence and undergoing physical torture. CERF funds were of paramount importance to prevent further loss of lives by providing life-saving assistance to an extremely vulnerable population in all sectors concerned by this report.
c) Did CERF funds help improve resource mobilization from other sources? YES PARTIALLY NO CERF funds helped to improve resource mobilization from other sources, notably on Child Protection, Health, SGBV, WASH and Shelter emergency response interventions. Complementary funding was mobilized from the Canadian Humanitarian Assistance Fund (CHAF), Denmark, United Kingdom‟s Department for International Development (DFID), and the US Bureau of Population, Refugees and Migration (BPRM). In addition, internal emergency staff were deployed to cover for the increased needs and to fill
1 Time-critical response refers to necessary, rapid and time-limited actions and resources required to minimize additional loss of lives and
damage to social and economic assets (e.g. emergency vaccination campaigns, locust control, etc.).

10
capacity gaps for the overall response (e.g. SURGE). Out of the US$ 7.3 million mobilized for this emergency, 58 per cent of those were mobilized from sources other than the CERF.
d) Did CERF improve coordination amongst the humanitarian community?
YES PARTIALLY NO CERF funding was allocated at a time when a new humanitarian coordination structure was being established in Cox‟s Bazar to respond to the aggravated protracted refugee crisis. The Inter Sectoral Coordination Group (ISCG) led to improving communication, coordination and standard information sharing between partners. CERF funding combined with a more predictable coordination platform led to a significantly enhanced coordination amongst the humanitarian community. For instance, IOM and UNFPA jointly implemented the CERF health project and this contributed to strengthened coordination between the Agencies. The use of limited resources was maximized and duplication avoided. For the first time, a multi-sectoral service provision for GBV survivors was coordinated outside the registered refugee camps. Site selection of vaccination posts was also decided in a coordinated manner among the humanitarian community.
e) If applicable, please highlight other ways in which CERF has added value to the humanitarian response
CERF added value to the humanitarian response by enabling joint and timely life-saving GBV and health interventions. It led to a strong interaction of GBV and sexual and reproductive health programming to ensure that medical care for sexual assault survivors was supported by trained staff in appropriately equipped and accessible facilities. CERF funded projects notably Health, WASH and Shelter interventions allowed to maintain the physical environment of the makeshift settlements relatively safe and secure. Purchasing price of commodities allowed to increase bulk procurement and consequently, added value for money to the CERF RR interventions.
V. LESSONS LEARNED
TABLE 6: OBSERVATIONS FOR THE CERF SECRETARIAT
Lessons learned Suggestion for follow-up/improvement Responsible entity
NA NA NA
TABLE 7: OBSERVATIONS FOR COUNTRY TEAMS
Lessons learned Suggestion for follow-up/improvement Responsible entity
Information sharing across sectors to be further
strengthened
Findings from distribution monitoring reports for Dignity Kits should be shared across sectors to ensure that WASH
sector/cluster‟s and GBV sector/cluster‟s distributions are well coordinated and that products (e.g. menstrual hygiene products)
are culturally appropriate.
WASH and GBV sectors/clusters
GBV preparedness measures to be strenghtened
First responders across sectors should receive information regarding GBV referral pathways and guiding principles for communicating with survivors. Integrated psychological and
health interventions should support GBV first response.
GBV sector/cluster; ISCG
Advocacy for increased access to basic social services to be
continued
Access to child protection services should be expanded for refugee children/adolescents and their familiies including
unaccompangied and separated children in camps and host community settings.
National authorities and humanitarian partners
Community messaging to be aligned across humanitarian
actors
Community messaging on issues such as GBV services availability and access by humanitarian actors should be aligned
to facilitate dissemination and outreach of the information. ISCG
Emergency hot line numbers to The establishment of one single hot line number with dispatch ISCG
11
be centralized system should be considered to facilitate information sharing and referral
12
VI. PROJECT RESULTS
2 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 3 This should include both funding received from CERF and from other donors.
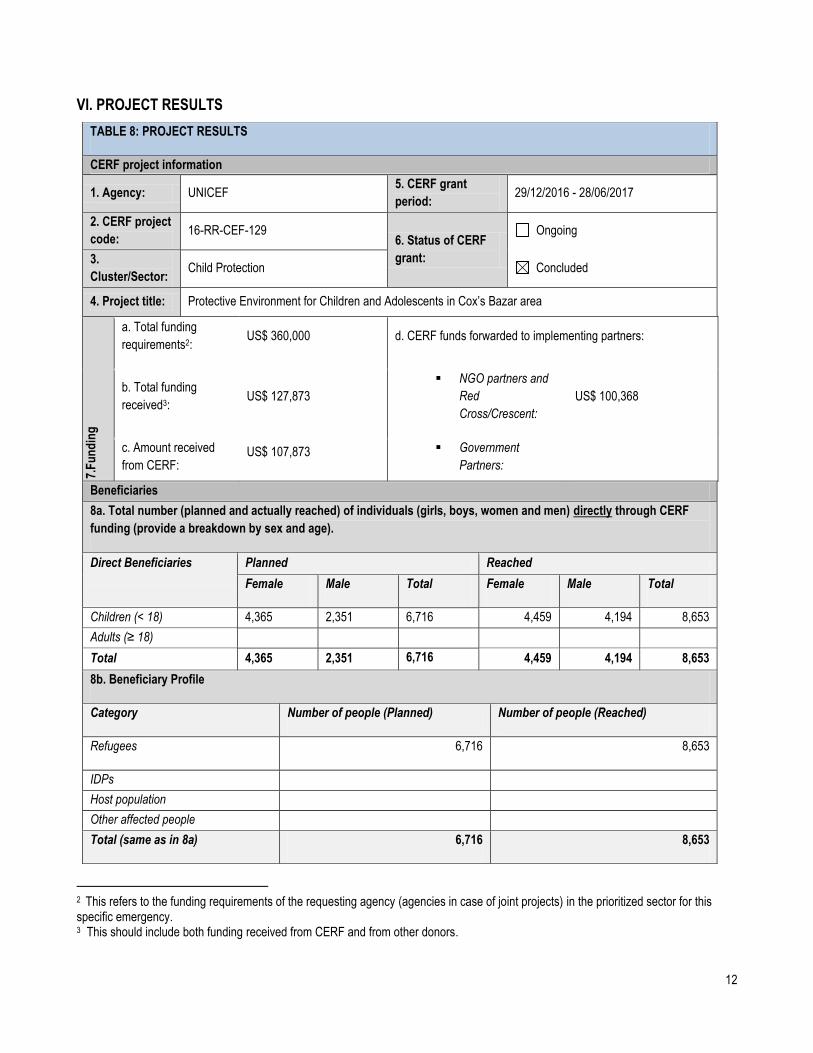
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: UNICEF 5. CERF grant
period: 29/12/2016 - 28/06/2017
2. CERF project
code: 16-RR-CEF-129
6. Status of CERF
grant:
Ongoing
3.
Cluster/Sector: Child Protection Concluded
4. Project title: Protective Environment for Children and Adolescents in Cox‟s Bazar area
7.F
un
din
g
a. Total funding
requirements2: US$ 360,000 d. CERF funds forwarded to implementing partners:
b. Total funding
received3: US$ 127,873
NGO partners and
Red
Cross/Crescent:
US$ 100,368
c. Amount received
from CERF:
US$ 107,873 Government
Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF
funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 4,365 2,351 6,716 4,459 4,194 8,653
Adults (≥ 18)
Total 4,365 2,351 6,716 4,459 4,194 8,653
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 6,716 8,653
IDPs
Host population
Other affected people
Total (same as in 8a) 6,716 8,653
13
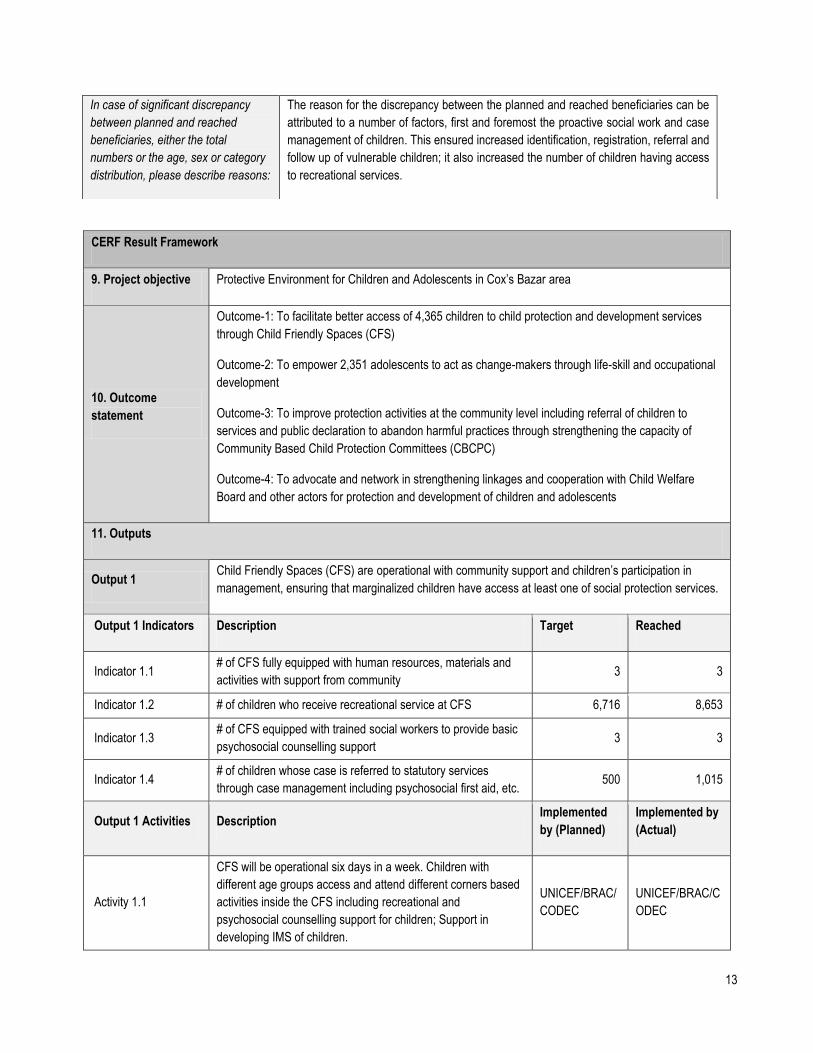
CERF Result Framework
9. Project objective Protective Environment for Children and Adolescents in Cox‟s Bazar area
10. Outcome
statement
Outcome-1: To facilitate better access of 4,365 children to child protection and development services
through Child Friendly Spaces (CFS)
Outcome-2: To empower 2,351 adolescents to act as change-makers through life-skill and occupational
development
Outcome-3: To improve protection activities at the community level including referral of children to
services and public declaration to abandon harmful practices through strengthening the capacity of
Community Based Child Protection Committees (CBCPC)
Outcome-4: To advocate and network in strengthening linkages and cooperation with Child Welfare
Board and other actors for protection and development of children and adolescents
11. Outputs
Output 1 Child Friendly Spaces (CFS) are operational with community support and children‟s participation in
management, ensuring that marginalized children have access at least one of social protection services.
Output 1 Indicators Description Target Reached
Indicator 1.1 # of CFS fully equipped with human resources, materials and
activities with support from community 3 3
Indicator 1.2 # of children who receive recreational service at CFS 6,716 8,653
Indicator 1.3 # of CFS equipped with trained social workers to provide basic
psychosocial counselling support 3 3
Indicator 1.4 # of children whose case is referred to statutory services
through case management including psychosocial first aid, etc. 500 1,015
Output 1 Activities Description Implemented
by (Planned)
Implemented by
(Actual)
Activity 1.1
CFS will be operational six days in a week. Children with
different age groups access and attend different corners based
activities inside the CFS including recreational and
psychosocial counselling support for children; Support in
developing IMS of children.
UNICEF/BRAC/
CODEC
UNICEF/BRAC/C
ODEC
In case of significant discrepancy
between planned and reached
beneficiaries, either the total
numbers or the age, sex or category
distribution, please describe reasons:
The reason for the discrepancy between the planned and reached beneficiaries can be
attributed to a number of factors, first and foremost the proactive social work and case
management of children. This ensured increased identification, registration, referral and
follow up of vulnerable children; it also increased the number of children having access
to recreational services.

14
Activity 1.2
Linkage development of CFS with the service provider
agencies through organizing meeting and dialogue. Visit of
local government and civil society to the CFS program regularly
and Involvement of local government and like-minded
organizations with CFS‟s special events.
UNICEF/BRAC/
CODEC
UNICEF/BRAC/C
ODEC
Activity 1.3
Formation and function of CBCPC, Peer Groups, Parents
Groups to practice and ensure the child protection. Training of
Peer Leaders on Life skills modules, Child Development
Module, Sports for Development.
UNICEF/CODE
C
UNICEF/BRAC/C
ODEC
Activity 1.4 Refresher on case management guideline for social workers UNICEF/CODE
C UNICEF/CODEC
Activity 1.5 Linkage development of CFS with the local service provider
agencies through organizing meeting and dialogue.
UNICEF/BRAC/
CODEC
UNICEF/BRAC/C
ODEC
Activity 1.6 Introduce child protection policy at CFS; Support in developing
IMS of children UNICEF UNICEF
Output 2 Adolescent clubs are active in ensuring that adolescent girls and boys have access to resources
required for their development.
Output 2 Indicators Description Target Reached
Indicator 2.1 # of adolescents for whom LSBE made available who attend
one LSBE session at adolescent club
2351
1,456
Indicator 2.2 # of adolescents completed 11 LSBE sessions who are
engaged in civic engagement
1645 492
Indicator 2.3 # of interactive sessions conducted by the adolescent groups 1000 sessions 528
Indicator 2.4 # of adolescent Interactive Popular Theatre (IPT) groups and
performances 6 IPT groups 6 IPT groups
Output 2 Activities Description Implemented
by (Planned)
Implemented by
(Actual)
Activity 2.1
Organize and facilitate the life skill sessions with effective
guidelines through active participation and regular attendance
of the adolescents.
UNICEF/BRAC UNICEF/BRAC/C
ODEC
Activity 2.2 Introduce Life Skills Based Education (LSBE) sessions for
adolescents; UNICEF/BRAC UNICEF/BRAC
Activity 2.3
Facilitate formation of CBCPCs at community level; Support in
strengthened the network among all CBCPCs supporting to
ensure the life skill training for adolescents.
UNICEF/BRAC UNICEF/BRAC
Activity 2.4 Facilitate linkages between adolescent‟s members of the
Adolescents Clubs with members at the CFS. UNICEF/BRAC
UNICEF/BRAC/C
ODEC
Activity 2.5 Adolescents IPT group formation and performance by
adolescents groups UNICEF/BRAC UNICEF/BRAC
Activity 2.6 Sports for development team formation and play by adolescent UNICEF/BRAC UNICEF/BRAC

15
groups
Output 3 CBCPCs are functional to ensure that marginalized children are provided with family support and
statutory services
Output 3 Indicators Description Target Reached
Indicator 3.1 # of CBCPCs which are provided with child development and
CRC and fully functional with community contribution 25 25
Indicator 3.2
# of targeted communities, which hold public debate and
discussion on e.g. child marriage, child labour, corporal
punishment
25 25
Indicator 3.3
# of cases of children referred per CBCPC per year to service
providers and/ or Child Welfare Board at Upazilla or district
level
500 1,015
Output 3 Activities Description Implemented
by (Planned)
Implemented by
(Actual)
Activity 3.1
Establishment of CBCPCs; CBCPC members, parents trained
on child development. CBCPCs will prepare a Child Protection
Action Plan based on their identification of problems and
issues. CBCPCs will be provided with support to implement
their action plan.
UNICEF/CODE
C
UNICEF/BRAC/
CODEC
Activity 3.2
CBCPCs will enhance the rapport building and accelerate the
referral linkage with child protection networks / service
providers consists of Social Welfare, Health, Women & Child
Affairs Department, NGO etc.
UNICEF/CODE
C UNICEF/CODEC
Activity 3.3
Child rights and child protection issues will be discussed in
interactive dialogue manner deliberately at the meetings of
different committees and forums of communities where parents,
and other community members.
UNICEF/CODE
C
UNICEF/BRAC/
CODEC
Output 4 Strengthened coordination between service providers at union, upazilla and district levels ensuring that
children are provided with services in a timely manner
Output 4 Indicators Description Target Reached
Indicator 4.1 # of follow up actions decided by Child Welfare Boards in
Ukhiya and Teknaf fully undertaken by social service officials 5 0
Output 4 Activities Description Implemented
by (Planned)
Implemented by
(Actual)
Activity 4.1
Build linkages with CBCPC, DSS at district and Upazilla level
and other actors for protection and development of children and
adolescents
UNICEF/CODE
C
UNICEF/BRAC/
CODEC
Activity 4.2 Coordinate activities so that DWA can lead CPiE south east
coast sub cluster UNICEF UNICEF
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy

16
between planned and actual outcomes, outputs and activities, please describe reasons:
Due to the conservative beliefs and practices prevailing among Rohingya communities, community members and parents were
not very supportive of adolescents' (especially girls‟) participation at the beginning of the project. Adolescents were almost
"invisible" within the makeshift settlement and to ensure their participation in the club-based activities (e.g. attending Life skills
sessions, sports, IPT etc.), the project organized consultations and sessions with community members and parents to outline the
purpose and objectives of the adolescents‟ clubs and activities. These consultations helped to gain the support of community
members and parents for carrying out the activities for children. This has gradually enabled to create a supportive environment
for the adolescents to incrementally attend the clubs based activities which have an impact on developing their self- esteem, and
other life skills to cope with this adverse situation and, to know their rights and responsibilities. To reach the UMN children the
project has facilitated mobile CFSs to ensure outreach work of the social workers and facilitate children access to CFS based
activities. It is to be noted that the absence of an agreed legal status of the UMN children creates a major challenge in their
access to governmental social protection services. It should also be noted that, coordination among child-centred care and
protection service providers and implementation of case management for children at risk have resulted in referral and
accessibility to relevant service providers.
The number of cases of children referred to service providers and/ or Child Welfare Board at Upazila or district level was higher
than planned. The reasons are the increased capacities of the CBCPC. All the members of the CBCPCs participated to the Child
Development and Child rights perspective module which enabled them to have increased knowledge and understanding of the
protection risks in the context and also the need for referral and accessibilities of social services. It also enhanced the sense of
responsibilities and accountabilities of the duty bearers towards the protection of the children by the laws of the land. In addition,
social workers developed their skills to conduct the case management of the children by participating in case management
trainings. This increased the number of children they could cover during the same time frame.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design,
implementation and monitoring:
A sector based coordination structure has been established for Rohingya response in Cox‟s Bazar underpinned by the principles
of the cluster approach, allowing for more effective sectoral coordination and response. The formation of sectoral standards,
needs assessments and analysis, other relevant technical issues played a vital improvement in the Rohingya response strategy
and enabled to monitor needs and gaps in the provision of humanitarian assistance for ensuring protection of Rohingya children.
Moreover, a strong coordination mechanism inter-sector coordination group (ISCG) also developed to mirror the HCTT to the
extent possible and CCC sector also participate actively in the group to complement and supplement response activities. At sub-
national level, UNICEF continues to lead sectoral coordination in the Child Protection sector in Cox‟s Bazar. The Child Protection
Sector‟s name was changed, as per the request of Ministry of Foreign Affairs to the “Child centred Care Sector”. Under the Child
Protection Sector (Child Centred Care Sector) in Cox‟s Bazar, a technical working group was formed with representation of
UNHCR, Bangladesh Red Crescent Society, and Save the Children, and National Organizations (BRAC and CODEC). The
technical working group is closely working on the case management procedure and referral pathways and to review the case
management tools/forms that have been used by the Social workers (SWs) to cater this dimension of the situation. Child
Protection Sector (Child Centered Care Sector) has reviewed sector indicators and set targets for 2017 and 4Ws of the Sector
was also updated with participation from sector members.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT

17
Routine monitoring on the project has been conducted to review progress across all levels.
Field visits have been undertaken to monitor and support smooth implementation.
Discussions with children, adolescents, members of Community based child protection
committee (CBCPC) as well parents‟ groups have taken place to understand the impact of
the project. Implementing partners have ensured routine reporting on the project. Joint
visits of the project have also been facilitated between UNHCR, UNICEF and IOM through
coordination, sharing of progresses and facilitation visit to the Child Friendly Spaces (CFS)
and Adolescents clubs. Also, the Upazila Social Services Officer (USSO) of Department of
Social Services (DSS), Upazila Women Affairs Officers, and Upazila Nirbahi Officer (UNO)
have undertaken field visits to the CFS and adolescent clubs.
EVALUATION PENDING
NO EVALUATION PLANNED

18
4 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 5 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: UNICEF 5. CERF grant
period: 05/01/2017 - 04/07/2017
2. CERF project
code: 16-RR-CEF-130
6. Status of CERF
grant:
Ongoing
3.
Cluster/Sector: Nutrition Concluded
4. Project title: Nutrition interventions for children under 5 and pregnant and lactating women (PLW) in Cox‟s Bazar
7.F
un
din
g
a. Total funding
requirements4: US$ 1,300,000 d. CERF funds forwarded to implementing partners:
b. Total funding
received5: US$ 511,148
NGO partners and Red
Cross/Crescent: US$ 220,492
c. Amount received
from CERF:
US$ 282,667 Government Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF
funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 5,477 4,716 10,193 5,492 4,701 10,193
Adults (≥ 18) 3,045 0 3,045 3,806 0 3806
Total 8,522 4,716 13,238 9,298 4701 13,999
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 13,238 13,999
IDPs

19
CERF Result Framework
9. Project objective
To reduce mortality and morbidity among 13,238 UNMs by improving the nutrition status of 6,072
children under 5 and 3806 pregnant and lactating women and 3280 adolescents in a six-month time
frame.
10. Outcome statement Children under 5 and pregnant and lactating women have access to essential nutrition services.
11. Outputs
Output 1 Improved access to nutritional services among 6072 children under 5, 3806 pregnant and lactating
women and 3280 adolescents in host communities and makeshift settlements.
Output 1 Indicators Description Target Reached
Indicator 1.1 Number of children under 5 screened for malnutrition 6,072 6,122
Indicator 1.2 Number of children under 5 referred and treated for
SAM 600 750
Indicator 1.3
Number of Pregnant and Lactating Women (PLW)
reached with counselling on Infant Young Child
Feeding in emergency (IYCF-E) practices
3,806 3,806
Indicator 1.4 Number of 6-23 month children reached with
Micronutrient Powder (MNP) supplementation 1,426 2,632
Indicator 1.5 Number of U5 children and adolescent reached with
deworming 9,352 9,352
Output 1 Activities Description Implemented by
(Planned)
Implemented by
(Actual)
Activity 1.1
Screening of children under 5 for detection of
nutritional status by Mid Upper Arm Circumference
(MUAC). MUAC is available through the Government
storage as well as through implementing partners.
MNP will be provided by partners.
UNICEF/ACF/SHED UNICEF/ACF/SHED
Activity 1.2
Referral and treatment of Severed Acute Malnutrition
(SAM) children at health facilities. National supply
replenishment of F-75 and F-100 was carried out
UNICEF/ACF/SHED UNICEF/ACF/SHED
Host population
Other affected people
Total (same as in 8a) 13,238 13,999
In case of significant discrepancy
between planned and reached
beneficiaries, either the total
numbers or the age, sex or category
distribution, please describe reasons:
Not applicable

20
during September/October 2016 with UNICEF
logistical support.
Activity 1.3 Establish Infant and Young Child Feeding (IYCF)
counselling and support for PLW UNICEF/ACF/SHED UNICEF/ACF/SHED
Activity 1.4 Provide Micronutrient Powder (MNP) supplementation
to for 6-23 months children UNICEF/ACF/SHED UNICEF/ACF/SHED
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy
between planned and actual outcomes, outputs and activities, please describe reasons:
To address prevailing undernutrition situation of the Rohingya new arrivals, additional 1,206 children aged 6-23 months were
supplemented with MNPs mostly in the Balukhali settlement (the most concentrated settlement for newly arrived Rohingya) and
additional 150 SAM children were referred and received life-saving therapeutic treatment at Out-Patient Treatment (OPT)
centres. Under this project a total of 94 community nutrition workers and volunteers and 114 government health service provides
in Ukhiya and Teknaf were trained on infant and young child feeding (IYCF) counselling and promotion in emergency.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design,
implementation and monitoring:
Implementing partners (ACF and SHED), beneficiaries, cluster/Sectoral partners, UN agencies were consulted during project
design, implementation and sharing of the monitoring observations. The project has maintained good coordination and
complementarity with other agencies on the ground particularly WFP and IOM. Implementing Partners (SHED and ACF)
participated in routine coordination mechanisms already existing at district & Upazila levels such as the district nutrition cluster
meetings lead by government and newly established TWG (Technical Working Group) meeting led by UNICEF. Rohingya
emergency nutrition response was regularly updated by UNICEF in ISCG meeting and IACM meeting at Cox‟s Bazar level.
UNICEF organised joint program monitoring visits in makeshifts and in the host communities with the implementing partner and
senior health officials from Ministry of Health & Family Welfare to observe implementation progress, issues/bottlenecks to access
to service delivery for Rohingya from mainstreamed health facilities and cross-checked uptake of services with the beneficiaries.
Reporting was done on a monthly basis by the implementing partners and shared with ISCG and were reflected in monthly ISCG
SITREPs. Additionally, two quarterly meetings were organised with implementing partners, health and family planning
departments at district and Upazila level, cluster/sector partners to review program implementation. In addition, an experience
sharing workshop was organized in Cox‟s Bazar in partnership with the Civil Surgeon Office to document and to share
achievements, best practices, lesson learned of the project implementation with all concerned partners.
At implementation level, initially UNICEF Chittagong field office and then after establishment of UNICEF Cox‟s Bazar field office
was responsible for overall coordination and oversight of the planned activities in consultation with UNICEF Bangladesh Country
Office. Other than the Nutrition Officer based at Chittagong, two additional technical experts were deployed to support in
planning, monitoring and accelerate the implementation.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
A significant number of routine monitoring visits by nutrition officer, several visits by district
nutrition support officer (DNSO) were conducted jointly with the implementing partner,
MoHFW officials and UNICEF to monitor the implementation status. In addition, two review
meetings were organized with the partner, MoHFW and UNICEF. Implementation status
and progress were also discussed in district nutrition cluster meetings held at district level.
EVALUATION PENDING
NO EVALUATION PLANNED

21
6 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 7 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: UNFPA 5. CERF grant period:
29/12/2016 - 28/06/2017
2. CERF project code:
16-RR-FPA-054 6. Status of CERF grant:
Ongoing
3. Cluster/Sector:
Sexual and/or Gender-Based Violence
Concluded
4. Project title: Saving lives and dignity of Undocumented Myanmar Nationals (UMN) women and girls through multi-sectoral prevention and response to gender-based violence
7.F
un
din
g
a. Total funding requirements6:
US$ 510,000 d. CERF funds forwarded to implementing partners:
b. Total funding received7:
US$ 203,895 NGO partners and
Red Cross/Crescent:
c. Amount received from CERF:
US$ 203,895 Government Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 6,400 6,400 6,315 101 6,416
Adults (≥ 18) 4,800 4,800 4,815 89 4,904
Total 11,200 11,200 11,130 190 11,320
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 11,200 11,320
IDPs
Host population
Other affected people
Total (same as in 8a) 11,200 11,320
In case of significant discrepancy between planned and reached beneficiaries, either the total numbers or the age, sex or category distribution, please describe reasons:
Not applicable

22
CERF Result Framework
9. Project objective Saving lives and dignity of Undocumented Rohingya women and girls refugee through multi-sectoral GBV response.
10. Outcome statement Increased access of Rohingya new-arrivals to information and services to prevent and respond to GBV.
11. Outputs
Output 1 11,200 women‟s and girls‟ GBV-related psychological needs supported by psycho-social counsellors
Output 1 Indicators Description Target Reached
Indicator 1.1 No. of psycho-social counsellors hired and deployed to cover the GBV-related needs of women and girls among Rohingya new-arrivals
8 8
Output 1 Activities Description Implemented by (Planned)
Implemented by (Actual)
Activity 1.1 Hire and deploy eight (8) psycho-social counsellors UNFPA, NGO UNFPA, MUKTI
Activity 1.2 Conduct psycho-social counselling sessions in makeshift settlements
NGO MUKTI
Activity 1.3 Monitoring and Evaluation UNFPA, NGO UNFPA, MUKTI
Output 2 Three (3) Women Friendly Spaces established to provide safe space for women and girls, psycho-social counselling service and functioning referral for GBV survivors
Output 2 Indicators Description Target Reached
Indicator 2.1 No. of Women Friendly Space established 3 3
Output 2 Activities Description Implemented by (Planned)
Implemented by (Actual)
Activity 2.1 Identify locations near makeshift settlements for establishing Women Friendly Spaces
UNFPA, NGO UNFPA, MUKTI
Activity 2.2 Set up functional Women Friendly Spaces UNFPA, NGO UNFPA, MUKTI
Activity 2.3 Provide psycho-social counselling and transportation for referral of GBV survivors
UNFPA, NGO UNFPA, MUKTI
Activity 2.4 Monitoring and Evaluation
Output 3 7,200 women and girls of reproductive age provided with Dignity Kits and blankets to restore their sense of dignity
Output 3 Indicators Description Target Reached
Indicator 3.1 No. of women and girls receiving Dignity Kits and blankets
7,200 7,200
Output 3 Activities Description Implemented by (Planned)
Implemented by (Actual)
Activity 3.1 Procure Dignity Kits and blankets UNFPA UNFPA
Activity 3.2 Identify a partner NGO(s) UNFPA UNFPA
Activity 3.3 Distribute Dignity Kits and blankets through NGO, UN and other partner(s)
UNFPA, NGO UNFPA, MUKTI
Activity 3.4 Monitoring and Evaluation UNFPA UNFPA

23
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy between planned and actual outcomes, outputs and activities, please describe reasons:
CERF enabled UNFPA to broaden its community engagement approach to also include men and boys, which was not originally included in the project scope. UNFPA targeted those males who assume the role of gatekeepers for women and girls, for instance, community leaders, male heads of house and adolescent boys, through community education and awareness. Learning themes focused on gender-equity, available support services for women and girls, community safety, and violence prevention. A total of 190 men and boys were reached, with CERF‟s support.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design, implementation and monitoring:
UNFPA-supported safe spaces for women and girls, or Women Friendly Spaces (WFS), were led by women and girls among the affected populations. More specifically, an initial assessment was conducted in the affected communities to gather information about the needs, preferences, and constraints of women and girls to ensure access and participation in WFS programming. Regular exchanges with women and girls informed the selection of WFS locations, opening hours, and the types of activities to be undertaken. Activities and approaches in the WFS were tailored to the needs, interests, age, and culture of women and girls based on their continued feedback. Social acceptance and continuation of the WFS activities were secured through the inputs and support of many stakeholders, including husbands, parents, and community leaders that influence the ability of women and girls to participate in programs. Men and boys, in particular, were engaged to understand the purpose, location, and benefits of the spaces to broaden the participation of women and girls. Participation of women and girls in the WFS activities was monitored using participatory methods that engage women and girls and invite views of community members. The Dignity Kits were also designed in partnership with the affected populations, to ensure that the most appropriate items were included, such as culturally-appropriate covering garments and menstrual hygiene products.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
The project was monitored very closely by UNFPA‟s technical officers. Dignity kits distribution was monitored closely by UNFPA‟s logisticians. Periodic reviews were held with implementing partners including joint monitoring missions with concerned officials of the Government of Bangladesh.
EVALUATION PENDING
NO EVALUATION PLANNED

24
8 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 9 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: UNFPA IOM
5. CERF grant period: 29/12/2016 - 28/06/2017 (UNFPA) 30/12/2016 - 29/06/2017 (IOM)
2. CERF project code:
16-RR-FPA-055 16-RR-IOM-043 6. Status of CERF
grant:
Ongoing
3. Cluster/Sector:
Health Concluded
4. Project title: Provision of critical primary health care including the Minimum Initial Service Package (MISP) for reproductive health in crisis to recently arrived Undocumented Myanmar Nationals (UMNs) in Cox's Bazar.
7.F
un
din
g
a. Total funding requirements8:
US$ 1,000000 d. CERF funds forwarded to implementing partners:
b. Total funding received9:
US$ 687,092 NGO partners and Red
Cross/Crescent: US$ 163,101
c. Amount received from CERF:
US$ 587,092 Government Partners: US$ 0
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 6,475 5,627 12,102 9,852 7,376 17,228
Adults (≥ 18) 5,296 4,602 9,898 17,960 6,649 24,609
Total 11,771 10,229 22,000 27,812 14,025 41,837
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 22,000 41,837
IDPs
Host population
Other affected people
Total (same as in 8a) 22,000 41,837
In case of significant discrepancy between planned and reached beneficiaries, either the total numbers or the age, sex or category distribution, please describe reasons:
More beneficiaries were reached than originally planned, as all efforts were made to maximize the reach of the intervention, particularly through community outreach activities for supporting vaccination campaigns, emergency first aid, reproductive health support, and support for pregnant women and children under 5 years. Moreover, additional female staff including doctors and midwives were deployed to encourage more adult women to access health services. This also contributed to reaching more beneficiaries than planned. Overall, the project contributed to increase access to critical life-saving primary health care services including MISP to the affected Undocumented Myanmar Nationals living in the Makeshift Settlements of Kutupalong, Leda, and Shamlapur and within the host communities of Teknaf and Ukhiya Upazilas.

25
CERF Result Framework
9. Project objective Improving the health outcomes of 22,000 Undocumented Myanmar Nationals (UMNs) living in three makeshift settlements and in host communities through accessible primary health care
10. Outcome statement Undocumented Myanmar Nationals living in makeshift settlements and Host Community experience reduced morbidity and mortality and improved access to treatment for injury and illness and other health issues.
11. Outputs
Output 1 22,000 Undocumented Myanmar Nationals have access to outreach primary health care from 8 IOM supported health facilities
Output 1 Indicators Description Target Reached
Indicator 1.1 Coverage of affected population with access to primary health care increased
50% 50%
Indicator 1.2 Number of newly arrived UMN patients received First Aid
8,000 8,127
Indicator 1.3 Number of newly arrived UMN patients managed through IOM supported 8 health facilities
3,000 3,225
Output 1 Activities Description Implemented by (Planned)
Implemented by (Actual)
Activity 1.1 Procurement of medicines for first aid kits and distribution to 124 community based health promoters to conduct primary health care outreach for 4 months
IOM IOM
Activity 1.2 Deployment of 54 Health Promoters to provide community based First Aid services to the newly arrived affected population according to SPHERE standards
IOM and local NGO Mukti and Bangla
German Sempreeti (BGS)
IOM and local NGO Mukti and Bangla
German Sampreeti (BGS)
Activity 1.3 Deployment of 1 midwife to enable primary health care services at two understaffed health facilities in Ukhiya and Teknaf
IOM IOM
Activity 1.4 Procurement and supply of medicines to 8 IOM supported health facilities
IOM IOM
Activity 1.5 Establishment of 8 Vaccination centres in Leda makeshift settlement
IOM IOM
Activity 1.6 Printing of IEC materials IOM IOM
Output 2 22,000 Undocumented Myanmar Nationals have access to life saving minimum initial service package for reproductive health service in crisis situations
Output 2 Indicators Description Target Reached
Indicator 2.1 Number of deliveries conducted in all targeted facilities together per month.
400 422
Indicator 2.2 Number of obstetric emergencies managed in Ukhiya Upazila health complex
50 84
Indicator 2.3 Number of pregnant women provided with Safe Delivery Kits
1,000 1,000
Indicator 2.4 % health facilities with Rape Treatment Kits available in Teknaf and Ukhiya facilities that provide treatment for rape survivors
100 100

26
Indicator 2.5 Number of condoms distributed at health facilities 5,000 5,000
Indicator 2.6 Number of patients provided travel vouchers for higher level of care
3000 3006
Output 2 Activities Description Implemented by (Planned)
Implemented by (Actual)
Activity 2.1
Recruit a Reproductive Health (RH) Officer to support coordination and ensure international standards in reproductive health provision during crisis situations is met through coordination with all actors.
UNFPA UNFPA
Activity 2.2 Recruit and deploy Midwives to the district hospital UNFPA / RTMI UNFPA/RTMI
Activity 2.3 Recruit and deploy a OB-GYN doctor to Ukhiya Health Complex
UNFPA / RTMI UNFPA/RTMI
Activity 2.4 Procure and distribute interagency RH kits and equipment for MISP
UNFPA / RTMI UNFPA/RTMI
Activity 2.5 Develop referral pathway and provide transportation for victims of sexual violence
UNFPA / IOM / RTMI
UNFPA/IOM/RTMI
Activity 2.6 Provide travel vouchers to patients who require higher level of care by midwives and refer clinicians in the 11 supported health facilities
UNFPA / RTMI UNFPA/Mukti
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy between planned and actual outcomes, outputs and activities, please describe reasons:
Overall the planned targets were all achieved, with some cases even exceeded, during the project period. In most areas reach was much greater than planned, as the deployment and additional midwives and extra supplies and equipment enabled many women to access SRHR care at facilities. Increasing the staffing capacity was the central aspect of the CERF project for UNFPA, and the facilities were indeed able to absorb these increased SRHR care providers. It was particularly rewarding to see that the number of women seeking care for emergencies was higher than expected, which was made possible by UNFPA‟s intentional implementation of the CERF intervention for emergency care at a facility much closer to the refugees that had previously not provided emergency care. This high number of women presenting with emergencies indicates that the community became more aware of the SRHR services, and that the services provided were acceptable to them. CERF indeed functioned as a catalyst - UNFPA was eventually able to distribute even a larger number of both Clean Delivery Kits and condoms than reported herewith in this report, as the performance of the CERF-funded assistance enabled UNFPA to mobilize additional funding with which UNFPA procured and distributed more items.
The project ended up reaching a lower number for boys under 18. This could be a result of adolescents who seek SRHR services having inflated their age, which is a common practice within health facilities in many parts of this country, given the social norms against young adolescents‟ access to SRHR info and services and due to the prevalence of child marriage. Healthcare facilities were provided with necessary medical equipment, adequate human resources – a key need, given more than doubling of the caseload – medicines, and other medical supplies to cater clinical services to the target population. Health service providers including doctors, midwives, nurses, and pharmacists were oriented and/or trained in sexual and reproductive health (SRH), basic emergency obstetric and neonatal care (BEmONC), sexual and gender-based violence (SGBV), and basic monitoring and evaluation to improve the quality of services. A total of 8,127 patients were provided first aid and 3,225 patients were provided with clinical consultation and treatment at the healthcare facilities. Referral services and travel vouchers were provided to 3,000 patients to access services at higher level facilities, and 1,000 women were provided with safe delivery kits. Maternal care services to women included ante-natal care, normal delivery and post-natal care.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design,

27
implementation and monitoring:
UNFPA has a strong internal control framework which includes a policy and procedural manual that guides the operations of all the projects to ensure the accountability to the beneficiaries. The guidelines were used for the implementation of this CERF project as well. For instance, a “spot check” was performed against UNFPA‟s Implementing Partners in the past year, including RTMI involved in the implementation of this CERF project. This Spot Check included both financial and programmatic observations, and in RTMI‟s case, no problems were identified. Both the Implementing Partner(s) and UNFPA staff monitored all aspects of the programming and operations regarding the CERF and other sources of funds. UNFPA staff had regular contacts with the international MISP Coordinator and the national OB-GYN doctor who were hired through CERF. The MISP Coordinator visited all the CERF-supported health facilities regularly and monitored activities, with a particular emphasis on monitoring emergency care, midwives‟ activities, and response to sexual violence. Beneficiaries were involved in UNFPA‟s project implementation. For instance, regarding the voucher distribution, the selection criteria for the target beneficiaries was determined with the stakeholders involved. Local health authorities and relevant partners provided UNFPA with a list of community members who met the criteria, and community leaders were present for all distributions. A community feedback mechanism was in place since the beginning of the project to ensure accountability to the affected populations. This mechanism included initiatives to build trust within the community and establishing an inter-sectoral model that supported feedback to all sectors across the target area. A dedicated Community Response Map (CRM) was in place, ensuring that beneficiaries can provide feedback about implementation throughout the project cycle. This included a Helpline number, integration of feedback into CRM, and necessary follow-up to the feedback, ensuring accountability to affected populations.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
Regular monitoring was carried out throughout the life of the project in accordance with IOM and UNFPA procedural requirements. Under the coordination outcome of the wider intervention, the project had (still does) a data management information system to collect, compile and document data/output throughout the duration of the project. Furthermore, the project ensured effective process documentation to guarantee that the standard project implementation procedures are well documented. This also helped identify best practices as well as processes that required future adjustments. Project activities were also monitored through field monitoring reports (monthly basis) and regular field visits by the project management, UNFPA, and other IOM (e.g. M&E) staff. Regularly briefings on project implementation through National and District level coordination committees have been established to guide and coordinate programme implementation activities with the involvement of the GoB, IOM, implementing partners, and other stakeholders, such as donor agencies. In addition, IOM carried out an evaluation of its overall humanitarian response in Cox‟s Bazar. The finalized evaluation will be shared widely with stakeholders.
EVALUATION PENDING
NO EVALUATION PLANNED

28
10 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 11 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: IOM 5. CERF grant
period: 05/01/2017 - 04/07/2017
2. CERF project
code: 16-RR-IOM-042
6. Status of CERF
grant:
Ongoing
3.
Cluster/Sector: Water, Sanitation and Hygiene Concluded
4. Project title: Provision of safe water and access to improved sanitation for vulnerable newly arrived UMNs in Teknaf and
Ukhiya Upazilas of Cox‟s Bazar district
7.F
un
din
g
a. Total funding
requirements10: US$ 787,163 d. CERF funds forwarded to implementing partners:
b. Total funding
received11: US$ 787,163
NGO partners
and Red
Cross/Crescent:
c. Amount received
from CERF:
US$ 236,149 Government
Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF
funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 6,475 5,627 12,102 6,768 6,270 13,037
Adults (≥ 18) 5,296 4,602 9,898 5,267 4,572 9,840
Total 11,771 10,229 22,000 12,035 10,842 22,877
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 22,000 22,877
IDPs
Host population

29
CERF Result Framework
9. Project objective
Improving the health, hygiene, and wellbeing of newly arrived UMNs and their hosts through access to
safe water, hygienic sanitation facilities and practices in Ukhiya and Teknaf Upazilas of Cox‟s Bazar
district.
10. Outcome
statement UMNs and host communities access essential WASH services.
11. Outputs
Output 1 Provision of adequate safe drinking water to targeted newly arrived UMNs and their hosts
Output 1 Indicators Description Target Reached
Indicator 1.1 # of people with access to sufficient (15 litres/person/day)
safe water 22,000 22,877
Indicator 1.2
# of people that are able to access water within a total
collection time of 30 minutes or less for a round trip
including queuing
22,000 22,877
Output 1 Activities Description Implemented by
(Planned)
Implemented by
(Actual)
Activity 1.1 Selection of type of water sources in a particular area
according the geophysical conditions
IOM/Partner NGO
(PNGO) IOM
Activity 1.2 Selection of sites for new water installations IOM/PNGO IOM
Activity 1.3 Processing of procurements for water installations IOM/PNGO IOM
Activity 1.4 Installation of new water sources IOM/PNGO IOM
Activity 1.5 Mapping of exiting dysfunctional water sources IOM/PNGO IOM
Activity 1.6 Rehabilitation of dysfunctional water sources IOM/PNGO IOM
Activity 1.7 Regular monitoring and reporting IOM IOM
Output 2 Provision of adequate and improved sanitation and hygiene in makeshifts and HCs
Output 2 Indicators Description Target Reached
Indicator 2.1 # of people with adequate access to improved latrine
facilities 22,000 22,877
Indicator 2.2 # of people with adequate access to improved bathing
facilities 22,000 22,877
Other affected people
Total (same as in 8a) 22,000 22,877
In case of significant discrepancy
between planned and reached
beneficiaries, either the total
numbers or the age, sex or category
distribution, please describe reasons:
Not applicable

30
Indicator 2.3 # of people reached with hygiene promotion messages 22,000 22,877
Output 2 Activities Description Implemented by
(Planned)
Implemented by
(Actual)
Activity 2.1 Processing of procurements for construction of latrines and
hand washing devices IOM/PNGO IOM
Activity 2.2 Processing of procurements for construction of bathing
cubicles IOM/PNGO IOM
Activity 2.3 Construction of latrines IOM/PNGO IOM
Activity 2.4 Construction of bathing cubicles IOM/PNGO IOM
Activity 2.5 Conducting hygiene sessions IOM/PNGO IOM
Activity 2.6 Conducting specific menstrual hygiene session with
adolescent girls and women IOM/PNGO IOM
Activity 2.7 Procurement and distribution of hygiene kits IOM/PNGO IOM
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy
between planned and actual outcomes, outputs and activities, please describe reasons:
The project targets were all achieved, with some cases even exceeded, during the project period. The arrival of 74,000 UMNs
between October 2016 and June 2017 meant that the UMN population in project areas – makeshift settlements and selected
host villages – increased considerably. To respond to the situation, IOM pumped, treated, and supplied 240,000 litres of drinking
water a day in Leda makeshift Settlement (LMS) of Teknaf upazila, Cox‟s Bazar. IOM accessed raw (non-curated) water from up-
stream reservoir from where water was diverted during dry season to a reservoir. 3 ring wells were connected by gutters and one
rainwater pond connected to roof catchment by gutters and PVC pipes. Due to roof damage by Cyclone Mora in May 2017,
gutter fitting was not possible to another 9 ring wells. An existing rain water pond was also maintained throughout the project and
connected to the roof catchments to harvest rainwater. 20 Deep tube-wells were installed; and 5 community latrines were
constructed. 60 household latrines built; 30 bathing cubicles constructed; formed 6 groups of adolescent girls with 134
participants and conducted menstrual hygiene sessions; all 5 community latrines had hand washing devices installed.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design,
implementation and monitoring:
A community feedback mechanism was in place since the beginning of the project to ensure accountability to the affected
populations. This mechanism included initiatives to build trust within the community and establishing an inter-sectoral model that
supported feedback to all sectors across the target area. A dedicated Community Response Map (CRM) was in place, ensuring
that beneficiaries can provide feedback about implementation throughout the project cycle. This included a Helpline number,
integration of feedback into CRM, and necessary follow-up to the feedback, ensuring accountability to affected populations.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
Regular monitoring was carried out throughout the period of the project in accordance with
IOM procedural requirements. Under the coordination outcome of the wider intervention,
the project had (still does) a data management information system to collect, compile and
document data/output throughout the duration of the project.
EVALUATION PENDING
NO EVALUATION PLANNED
31
Furthermore, the project ensured effective process documentation to guarantee that the
standard project implementation procedures are well documented. This also helped
identify best practices as well as processes that required future adjustments.
Project activities were also monitored through field monitoring reports (monthly basis) and
regular field visits by the project management and other IOM (e.g. M&E) staff.
Regular briefings on project implementation through National and District level coordination
committees have been established to guide and coordinate programme implementation
activities with the involvement of the GoB, IOM, implementing partners, and other
stakeholders, such as donor agencies.
In addition, IOM carried out an evaluation of its overall humanitarian response in Cox‟s
Bazar. The finalized evaluation will be shared with stakeholders.

32
12 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 13 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: IOM 5. CERF grant
period: 05/01/2017 - 04/07/2017
2. CERF project
code: 16-RR-IOM-044
6. Status of CERF
grant:
Ongoing
3.
Cluster/Sector: Shelter Concluded
4. Project title: Provision of temporary shelter and other essential basic supplies for vulnerable newly arrived UMNs in
Teknaf and Ukhiya Upazilas of Cox‟s Bazar district
7.F
un
din
g
a. Total funding
requirements12: US$ 3,268,636 d. CERF funds forwarded to implementing partners:
b. Total funding
received13: US$ 3,268,636
NGO partners
and Red
Cross/Crescent:
c. Amount received
from CERF:
US$ 980,591 Government
Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF
funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 6,475 5,627 12,102 6,768 6,270 13,037
Adults (≥ 18) 5,296 4,602 9,898 5,267 4,572 9,840
Total 11,771 10,229 22,000 12,035 10,842 22,877
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 22,000 22,877
IDPs
Host population

33
CERF Result Framework
9. Project objective Improving the wellbeing of newly arrived UMNs and their hosts through access to shelter and other
essential basic supplies in Ukhiya and Teknaf Upazilas of Cox‟s Bazar district
10. Outcome statement Vulnerable UMNs access temporary shelter and other essential basic supplies
11. Outputs
Output 1 Provision of emergency NFIs including shelter and basic household items
Output 1 Indicators Description Target Reached
Indicator 1.1 # of households with shelter materials 4,000 4,620
Indicator 1.2 # of targeted households with essential basic
supplies in their possession 4,000 4,620
Output 1 Activities Description Implemented by
(Planned)
Implemented by
(Actual)
Activity 1.1 Procurement and distribution of general NFI kits
including winter clothing IOM/PNGO IOM
Activity 1.2 Procurement, distribution, and provision of
temporary shelter IOM/PNGO IOM
Activity 1.3 Regular monitoring and reporting IOM IOM
Other affected people
Total (same as in 8a) 22,000 22,877
In case of significant discrepancy
between planned and reached
beneficiaries, either the total
numbers or the age, sex or category
distribution, please describe reasons:

34
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy
between planned and actual outcomes, outputs and activities, please describe reasons:
A total of 4,620 of the most vulnerable newly arrived UMNs were provided with shelter materials and essential basic supplies
(general NFI kits) that included items such as mosquito net, utensils, basic clothing articles, and a bag to carry the items.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design,
implementation and monitoring:
A community feedback mechanism was in place since the beginning of the project to ensure accountability to the affected
populations. This mechanism included initiatives to build trust within the community and establishing an inter-sectoral model that
supported feedback to all sectors across the target area. A dedicated Community Response Map (CRM) was in place, ensuring
that beneficiaries can provide feedback about implementation throughout the project cycle. This included a Helpline number,
integration of feedback into CRM, and necessary follow-up to the feedback, ensuring accountability to affected populations.
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
Regular monitoring was carried out throughout the life of the project in accordance with
IOM procedural requirements. Under the coordination outcome of the wider intervention,
the project had (still does) a data management information system to collect, compile and
document data/output throughout the duration of the project. Furthermore, the project
ensured effective process documentation to guarantee that the standard project
implementation procedures are well documented. This also helped identify best practices
as well as processes that required future adjustments.
Project activities were also monitored through field monitoring reports (monthly basis) and
regular field visits by the project management and other IOM (e.g. M&E) staff.
Regular briefings on project implementation through National and District level coordination
committees have been established to guide and coordinate programme implementation
activities with the involvement of the GoB, IOM, implementing partners, and other
stakeholders, such as donor agencies.
In addition, IOM carried out an evaluation of its overall humanitarian response in Cox‟s
Bazar. The finalized evaluation will be shared with the stakeholders.
EVALUATION PENDING
NO EVALUATION PLANNED

35
14 This refers to the funding requirements of the requesting agency (agencies in case of joint projects) in the prioritized sector for this specific emergency. 15 This should include both funding received from CERF and from other donors.
TABLE 8: PROJECT RESULTS
CERF project information
1. Agency: WFP 5. CERF grant period: 20/12/2016 - 19/06/2017
2. CERF project code:
16-RR-WFP-072 6. Status of CERF grant:
Ongoing
3. Cluster/Sector:
Food Aid Concluded
4. Project title: Emergency Food and Nutrition Assistance for Rohingya Refugees
7.F
un
din
g
a. Total funding requirements14:
US$ 1,731,824 d. CERF funds forwarded to implementing partners:
b. Total funding received15:
US$ 1,720,000 NGO partners and
Red Cross/Crescent:
US$ 77,593
c. Amount received from CERF:
US$ 692,002 Government
Partners:
Beneficiaries
8a. Total number (planned and actually reached) of individuals (girls, boys, women and men) directly through CERF funding (provide a breakdown by sex and age).
Direct Beneficiaries Planned Reached
Female Male Total Female Male Total
Children (< 18) 6,475 5,627 12,102 10,726 9,581 20,307
Adults (≥ 18) 5,296 4,602 9,898 7,836 5,883 13,719
Total 11,771 10,229 22,000 18,562 15,464 34,026
8b. Beneficiary Profile
Category Number of people (Planned) Number of people (Reached)
Refugees 22,000 30,426
IDPs
Host population
Other affected people
Total (same as in 8a) 22,000 34,026
In case of significant discrepancy between planned and reached beneficiaries, either the total numbers or the age, sex or category distribution, please describe reasons:
The CERF funding reached a higher beneficiary number as compared to planned totals due to commodity price decrease. During the program period, the price of rice was much lower resulting in a higher tonnage being procured. The price of vegetable oil and WSB+ and WSB ++ was also lower resulting in higher tonnage being procured translating to more beneficiary being reached from 22,000 to 34,026. WFP was also able to negotiate
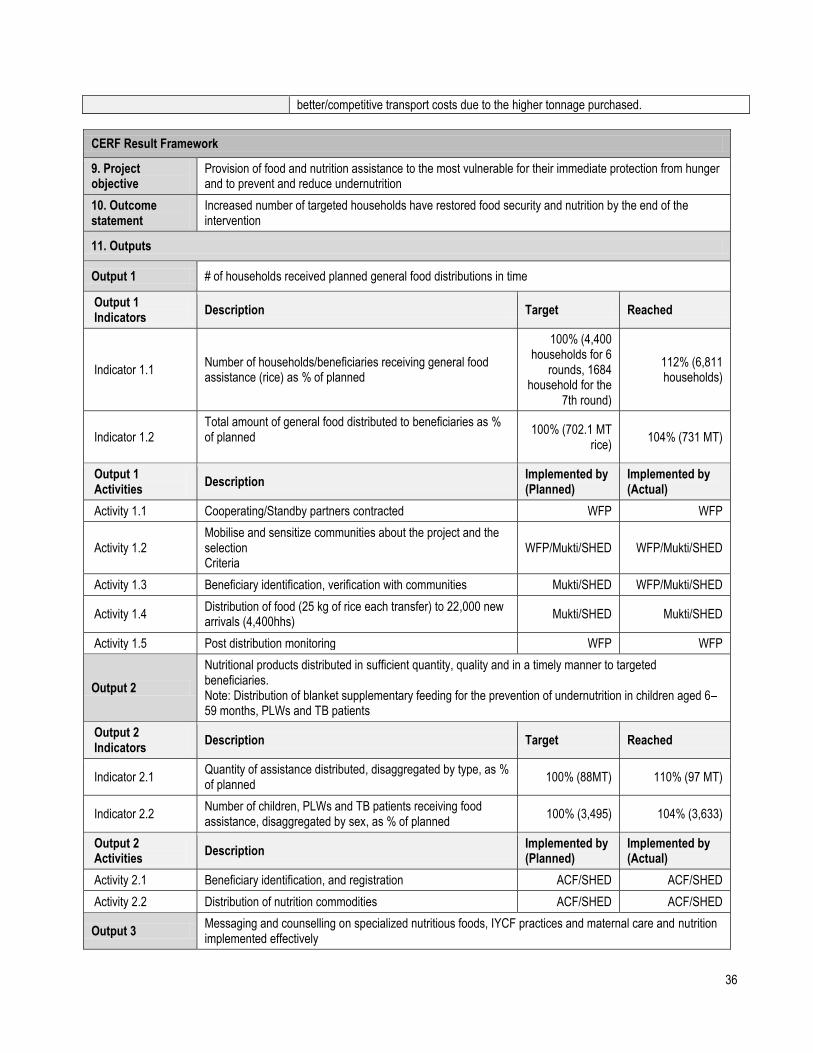
36
CERF Result Framework
9. Project objective
Provision of food and nutrition assistance to the most vulnerable for their immediate protection from hunger and to prevent and reduce undernutrition
10. Outcome statement
Increased number of targeted households have restored food security and nutrition by the end of the intervention
11. Outputs
Output 1 # of households received planned general food distributions in time
Output 1 Indicators
Description Target Reached
Indicator 1.1 Number of households/beneficiaries receiving general food assistance (rice) as % of planned
100% (4,400 households for 6
rounds, 1684 household for the
7th round)
112% (6,811 households)
Indicator 1.2 Total amount of general food distributed to beneficiaries as % of planned
100% (702.1 MT rice)
104% (731 MT)
Output 1 Activities
Description Implemented by (Planned)
Implemented by (Actual)
Activity 1.1 Cooperating/Standby partners contracted WFP WFP
Activity 1.2 Mobilise and sensitize communities about the project and the selection Criteria
WFP/Mukti/SHED WFP/Mukti/SHED
Activity 1.3 Beneficiary identification, verification with communities Mukti/SHED WFP/Mukti/SHED
Activity 1.4 Distribution of food (25 kg of rice each transfer) to 22,000 new arrivals (4,400hhs)
Mukti/SHED Mukti/SHED
Activity 1.5 Post distribution monitoring WFP WFP
Output 2
Nutritional products distributed in sufficient quantity, quality and in a timely manner to targeted beneficiaries. Note: Distribution of blanket supplementary feeding for the prevention of undernutrition in children aged 6–59 months, PLWs and TB patients
Output 2 Indicators
Description Target Reached
Indicator 2.1 Quantity of assistance distributed, disaggregated by type, as % of planned
100% (88MT) 110% (97 MT)
Indicator 2.2 Number of children, PLWs and TB patients receiving food assistance, disaggregated by sex, as % of planned
100% (3,495) 104% (3,633)
Output 2 Activities
Description Implemented by (Planned)
Implemented by (Actual)
Activity 2.1 Beneficiary identification, and registration ACF/SHED ACF/SHED
Activity 2.2 Distribution of nutrition commodities ACF/SHED ACF/SHED
Output 3 Messaging and counselling on specialized nutritious foods, IYCF practices and maternal care and nutrition implemented effectively
better/competitive transport costs due to the higher tonnage purchased.

37
Note: Nutrition awareness provided to PLW, caregivers of children, community men and women through centre based courtyard sessions, home visits and cooking demonstrations.
Output 3 Indicators
Description Target Reached
Indicator 3.1 Number of women/men exposed to nutrition messaging supported by WFP, against number planned
100% (3,495) 104% (3,633)
Indicator 3.2
Number of targeted caregivers (male and female) receiving 3 key messages delivered through WFP-supported messaging and counselling Note: Targeted caregivers are individuals identified as beneficiary children‟s primary caregivers, who are responsible for collecting rations and who know the most about what beneficiary children are fed
100% (3,495) 104% (3,633
Indicator 3.3
Number of women/men receiving nutrition counselling supported by WFP, against number planned Nutrition counselling sessions Note: Nutrition counselling sessions can include individual or group sessions
100% (3,495) 104% (3,633)
Output 3 Activities
Description Implemented by (Planned)
Implemented by (Actual)
Activity 3.1 Organizing BCC sessions, community mobilization and community sensitization before the food distribution
SHED/ACF SHED/ACF
Activity 3.2 Demonstration to caretakers and PLW on how to use the BSFP ration: daily quantity, feeding frequency, desired consistency of the porridge and the preservation methods
SHED/ACF SHED/ACF
Activity 3.3 Post distribution monitoring of the utilisation of the supplementary food and BCC and counselling sessions
SHED/ACF SHED/ACF
12. Please provide here additional information on project’s outcomes and in case of any significant discrepancy between planned and actual outcomes, outputs and activities, please describe reasons:
The CERF funding reached a higher beneficiary number as compared to planned totals due to commodity price decrease. During the program period, the price of rice was much lower resulting in a higher tonnage being procured. The price of vegetable oil and WSB+ and WSB ++ was also lower, resulting in higher tonnage being procured translating to more beneficiary being reached from 22,000 to a total of 34,026 beneficiaries. The higher beneficiary number was also in part due to the modality of sensitization at block levels. WFP was able with the extra tonnage procured to incorporate and assist new arrivals that were not initially targeted in the proposal.
13. Please describe how accountability to affected populations (AAP) has been ensured during project design, implementation and monitoring:
The programme ensures strict monitoring and recording. This is achieved in part through weekly measurements and household visits to ensure children and PLWs receive and are consuming their food rations in the eventuality sharing is ongoing that may have an impact on malnutrition levels. The household visits also ensured that WFP received beneficiary feedback on programme implementation. A community feedback mechanism was in place to ensure accountability to the beneficiaries. WFP cross-monitored the project sites to gain feedback from the beneficiaries and address complaints and issues. A hotline number was in place (and still is) and displayed at various public places, including the project and distribution sites, where people can report any complaints or irregularities. During the project period, regular calls were received on targeting & registration, seeking information and reporting service delivery issues regarding this project. All calls received have been verified and feedback provided with corresponding priority. The verification has been done by CP‟s and WFP staff based on the complaint type and priority.

38
14. Evaluation: Has this project been evaluated or is an evaluation pending? EVALUATION CARRIED OUT
The project planned to monitor the activities through post distribution monitoring, where the major findings of the General Food Distribution are:
The post distribution monitoring confirmed 100% respondents were informed and received their full entitlement whereby 73% rated the quality of rice as good, 14% rated fair and 13% rated bad. Those who rated fair or bad quality, reportedly received „broken rice‟ (Grain that is short or is fragmented having been broken in the field, during drying, transportation or milling)
Among the beneficiaries, 59% consumed all of the rice and 41% were reported to consume 60-70% of the assistance with the remainder bartered with other commodities or sold to purchase other food items.
The beneficiary selection process was reportedly „clean‟ or corruption free. Beneficiaries did not need to pay anyone to be included in the distribution list.
Travel routes to and from the distribution point were reported as safe. Beneficiaries did not need to pay anyone to receive their entitlement.
EVALUATION PENDING
NO EVALUATION PLANNED
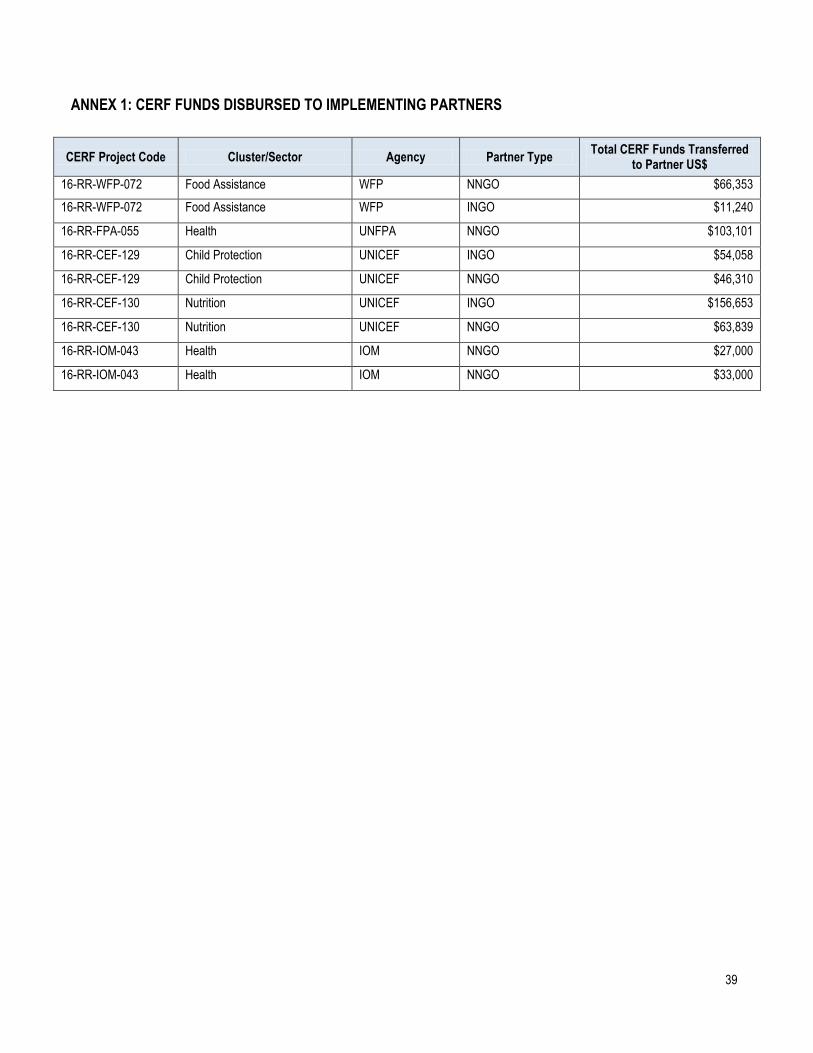
39
ANNEX 1: CERF FUNDS DISBURSED TO IMPLEMENTING PARTNERS
CERF Project Code Cluster/Sector Agency Partner Type Total CERF Funds Transferred
to Partner US$
16-RR-WFP-072 Food Assistance WFP NNGO $66,353
16-RR-WFP-072 Food Assistance WFP INGO $11,240
16-RR-FPA-055 Health UNFPA NNGO $103,101
16-RR-CEF-129 Child Protection UNICEF INGO $54,058
16-RR-CEF-129 Child Protection UNICEF NNGO $46,310
16-RR-CEF-130 Nutrition UNICEF INGO $156,653
16-RR-CEF-130 Nutrition UNICEF NNGO $63,839
16-RR-IOM-043 Health IOM NNGO $27,000
16-RR-IOM-043 Health IOM NNGO $33,000

40
ANNEX 2: ACRONYMS AND ABBREVIATIONS (Alphabetical)
ACF Action Contre la Faim
BCC Behavioural Change Communication
BDRC Bangladesh Red Crescent
BGS Bangla German Sampreeti
BRAC Building Resources Across Communities
BSFP Blanket Supplementary Feeding Program
CBCPC Community Based Child Protection Committees
CFS Child Friendly Spaces
CP Cooperating Partner
CRM Community Response Map
DNSO District Nutrition Support Officer
DSS Department of Social Services
GBV Gender Based Violence
GoB Government of Bangladesh
HCTT Humanitarian Coordination Task Team
HRP Humanitarian Response Plan (HRP)
IEC Information, Education and Communication
IMS Information Management System
IOM International Organization for Migration
IPT Interactive Popular Theatre
ISCG Inter-Sector Coordination Group
IYCF Infant & Young Child Feeding
LMS Leda makeshift Settlement
LSBE Life Skills-Based Education
M&E Monitoring & Evaluation
MAM Moderate Acute Malnutrition
MIRA Multi-sector Initial Rapid Assessment
MISP Minimum Initial Service Package
MNP Micronutrient Powder
MoDMR Ministry of Disaster Management and Relief
MoFA Ministry of Foreign Affairs
MoHFW Ministry of Health and Family Welfare
MT Metric Ton
MUAC Mid Upper Arm Circumference
NFI Non-Food Item
OB-GYN Obstetrician-Gynecologist
OPT Out-Patient Treatment
PLW Pregnant and Lactating Women
RC Resident Coordinator
RCO Resident Coordinator‟s Office
RH Reproductive Health
ROAP Regional Office for Asian and the Pacific
RTMI Research, Training and Management International
SAM Severed Acute Malnutrition
SGBV Sexual and Gender Based Violence
SHED Society for Health Extension and Development

41
SO Strategic Objective
SRHR Sexual and Reproductive Health and Rights
SW Social Worker
TB Tuberculosis
TWG Technical Working Group
UMN Undocumented Myanmar National
UNFPA United Nations Population Fund
UNHCR United Nations High Commissionner for Refugees
UNICEF United Nations Children‟s Fund
UNO Upazilla Nirbahi Officer
USSO Upazilla Social Services Officer
WFP World Food Programme
WFS Women Friendly Space


















