
RESI ONLY - CCG Medication Policy Template - Aug 11 · Web viewWhen administering crushed tablets...
114
MEDICATION POLICY TEMPLATE For use in Bromley care homes August 2011
-
Upload
nguyenthuan -
Category
Documents
-
view
214 -
download
1
Transcript of RESI ONLY - CCG Medication Policy Template - Aug 11 · Web viewWhen administering crushed tablets...

MEDICATION POLICY TEMPLATE
For use in Bromley care homes
August 2011
AuthorSue Kieselack
Medication Review PharmacistNHS Bromley
email: [email protected]

Contents
The medication policy template is presented in the form of individual policies with aims, key relevant legislation and guidance and advice. Further reference material and resources are provided under the section References and guidance and in the Appendix.
PageBackground 4
Purpose 4
Scope 4
Responsibilities 5
Legislation 5
Outcome 9: Management of medicines 6
1 Obtaining supplies of medicines 7
2 Receipt of medicines 10
3 Storage of medicines 12
4 Refrigerated medicines 14
5 Shelf-lives of medicines 16
6 Choice and consent 18
7 Administration of oral medicines 20
8 Administration of creams and ointments 24
9 Monitored dosage systems (MDS) 26
10 Medicine administration records (MAR) charts 28
11 When required (prn) medicines 31
Medication Policy Template 2

12 Verbal orders and dose changes 33
13 Self administration of medicines 35
14 Swallowing difficulties and covert administration 37
15 Disposal of medicines 39
16 Controlled drugs 41
17 Medicines errors and adverse drug reactions 48
18 Minor ailments and homely remedies 50
19 Administration of warfarin 52
20 New admissions and returning from hospital stays 56
21 Transfer of medicines to another care setting 58
22 Leave medicines and secondary dispensing 60
23 Training staff to administer medicines 62
Glossary 66
Acknowledgments 68
References and further guidance 69
Appendix 72
Medication Policy Template 3

Background
Following the publication of the Care Home Use of Medicines Study (CHUMS) which revealed a high prevalence of medication errors in care homes for older people, the Department of Health issued an alert in January 2010 requiring Primary Care Trusts (PCTs) to work with primary medical care contractors, providers of pharmaceutical services and social care partners:
to review the safety of local prescribing, dispensing, administration, and monitoring arrangements in the provision of medication to older people in care homes
establish a plan for effective joint working in the future, including auditing on-going progress.
A group was therefore set up in Bromley to action the alert with representatives from the PCT, community pharmacy, GPs, care homes, the local authority and patients. The group ordered a review of the use of medicines in care homes in Bromley in May 2010, which largely substantiated the finding of CHUMS. As a result, an action plan was agreed including the provision of a medication policy template for adaptation by Bromley care homes.
Purpose
The purpose of the medication policy template is to provide pharmaceutical guidance to assist care homes to write their own medication policy based on current legislation and guidance, to optimise the safe management of medication and to ensure that all care homes in Bromley comply with Care Quality Commission (CQC) Essential standards of quality and safety Outcome 9: Management of Medicines.
Scope
The medication policy template is intended for use by all registered care homes in Bromley.
Medication Policy Template 4

Responsibilities
The template applies to all staff working in Bromley care homes who have a responsibility for the safer management of medicines. This includes managers, nursing staff and designated suitably trained care workers.
Registration 13 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 states that:
‘The registered person must protect service users against the risks associated with the unsafe use and management of medicines, by means of the making of appropriate arrangements for the obtaining, recording, handling, using, safe keeping, dispensing, safe administration and disposal of medicines used for the purpose of the regulated activity’.
Legislation
The following legislation underpins medication policy and guidance:
The Medicines Act 1968The Health and Social Care Act 2008The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Mental Capacity Act 2005 and Code of PracticeThe Disability Discrimination Act (DDA) 1995 The Hazardous Waste (England and Wales) Regulations 2005The Misuse of Drugs (Safe Custody) Regulations 1973The Misuse of Drugs Act Regulations 2001The Controlled Drugs (Supervision of Management and Use) Regulations 2006The Misuse of Drugs and Misuse of Drugs (Safe Custody) (Amendment) Regulations 2007
Details of legislation are available at:http://www.legislation.gov.uk
Medication Policy Template 5

Outcome 9: Management of medicines
Care homes registered with the Care Quality Commission (CQC) must comply with Essential standards of quality and safety Outcome 9: Management of medicines which states:
People who use services:
Will have their medicines at the times they need them and in a safe way Wherever possible will have information about the medicine being prescribed made
available to them or others acting on their behalf.
This is because providers who comply with the regulations will:
Handle medicines safely, securely and appropriately Ensure that medicines are prescribed and given by people safely Follow published guidance about how to use medicines safely
CQC use the following prompts to judge whether a provider is complying with Outcome 9:
Are there effective processes for the safe and secure handling ofmedicines and are these in line with the relevant guidance andlegislation?
Are there clear processes in place for the handling of controlled drugs? Are there clear processes to take account of new guidance and alerts
relating to the safe handling and use of medicines? Are there clear processes in place to ensure a person’s medicines
prescription is up to date and reviewed as their needs or conditions change in relation to their medicines
Medication Policy Template 6
1. Obtaining supplies of medicines
Aim: To ensure that patients always have a supply of medicines and that there are good auditable procedures in place to monitor systems so that only the medicines required are ordered.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Obtaining supplies of medicines
Advice For care home use
Who is responsible for ordering medication?
Designated nurse or designated senior care worker
Which community pharmacy dispenses the repeat medicines?What are their contact details and opening hours?
Repeat medicines are usually obtained from a single community pharmacy to ensure continuity of supply.
Which GP practices are the residents registered with?What are their contact details and opening hours?
Ideally residents are registered with one GP practice, which is contracted to provide Visiting Medical Officer (VMO) services. However, some residents may prefer to be registered with another GP
Medication Policy Template 7

When do repeat medicines have to be ordered?
Repeat medicines are normally ordered on a 4 week cycle where a monitored dosage system (MDS) is used. Liaise with GP practice and community pharmacy to allow sufficient time for prescriptions to be issued, checked, dispensed and received for the start of the next cycle. Marking dates on a calendar assists this process.
How are repeat medicines ordered?
Check medicines required by using the medicine administration record (MAR) charts and confirming amounts held within the home. Do not order medicines if there is sufficient for the next cycle.
Order required medicines by the agreed date from GP(s) using right hand side of prescription forms and/or MAR charts (as agreed with the GP practice)
Complete a written record to show what has been ordered.
Check prescriptions issued by the GP to ensure correct medicines have been prescribed. Reorder if necessary and record in the written order records.
Photocopy the prescription as a record of the GP’s authority to administer.
Sign the declaration on the reverse of the prescription if the patient is under 60 years of age.
Send prescriptions to the community pharmacy by the agreed date.
Is the dispensing pharmacy aware of new residents, residents that have been discharged from hospital and any changes in medicines?
The pharmacy needs to have full details of residents’ medicines. Copies of MAR charts can be sent to the pharmacy with prescriptions. This is also important where ‘when required’ medication is not requested every month but is still being used.
What are the arrangements for sending prescription requests to the GP practice(s), collecting prescriptions and sending prescriptions to the community pharmacy?
You may have to post repeat prescriptions requests to the GP practice. Community pharmacies may collect prescriptions from the GP practice and the care home.
What are the arrangements for
New treatment should be started as soon as possible, within 24 hours at the latest.
Medication Policy Template 8

obtaining ‘acute’ supplies of medicines e.g. antibiotics, painkillers?
You may not be able to obtain medicines quickly from the pharmacy that normally dispenses your repeat medicines.
Consider opening hours of other community pharmacies near the home and that they may not supply a MAR chart or have a record of residents’ repeat medicines to check for drug interactions.
Prescriptions may need to be faxed to the pharmacy by either the GP practice or the care home. Confirm with the pharmacy that the fax has been received and when the medicine will be delivered.
Make sure you have a copy of the prescription as a record of the GPs authority to administer
What are the arrangements for obtaining emergency supplies of medicines e.g. if the home has run out of medicines before the next supply is due to be delivered due to poor ordering or spillage?
Identify why the medicines have run out Obtain an additional prescription to align
with the ordering cycle.If the GP surgery is closed, the community pharmacy may make an emergency supply. They can charge for this service.The GP out of hours service EMdoc contact details and opening hours should be noted but they should not be relied on for this service.Tel no: 020 8676 3291Monday to Thursday 6.30pm to 8.00amFriday to Monday 6.30pm to 8.00amBank holidays
Medication Policy Template 9
2. Receipt of medicines
Aim: To ensure that service users always have a record of the medicines received and that there are good auditable procedures in place to monitor systems so that there is an accurate record of all medicines that come into the home.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Receipt of medicines
Advice For care home use
Who is responsible for receiving medicines in the care home?
Designated nurse or designated senior care worker. Medicines will have to be signed for on receipt
What is the procedure for receiving medicines from the pharmacy in the care home?
Check that medicines received are correct by comparing them to a copy of the prescription.
Check that medication has not been stopped or a dose changed since the pharmacy dispensed the medicines.
Should the medicines not match the copy of the prescription, do not administer and contact the supplying pharmacy immediately to rectify the mistake.
Record on the MAR chart the quantity received, date of receipt and the initials of the person receiving the medicine.
Check printed MAR charts for accuracy as the accuracy of the MAR chart is the responsibility of the home.
Check that the MAR chart contains all the patient’s current medicines as well as any “when required” medicines and not just the medicines supplied that month. If a printed MAR chart is not received with the medicines then make a hand- written entry on
Medication Policy Template 10

the resident’s MAR chart. Hand-written entries must be checked and signed by a second authorised person. See Medicine administration records (MAR)charts.
What is the procedure where family members or friends of the resident bring medicines or homely remedies into the home?
The home needs to be informed of all medicines that the resident is taking. Check with the GP and/or pharmacist that the medicines do not interact with prescribed medicines. Written authority from the GP to administer is advisable. Administration of residents’ own medication should be recorded on the resident’s MAR chart in the normal way.
Medication Policy Template 11

3. Storage of medicines
Aim: To ensure that medicines are always fit for purpose, are securely stored to prevent accidental use or theft and good auditable procedures are in place to monitor systems such as temperature of storage rooms and security of keys.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Storage of medicines
Advice For care home use
Are medicines stored in a suitable environment?
Medicines should not be stored in places where they may be damaged by heat or dampness or in unhygienic areas e.g. kitchens, bathrooms, toilets, sluices, windowsills, areas next to heaters
Filing cupboards are unsuitable Only medicines should be stored in medicines
cupboards, not food or valuables. Medicines should be stored discreetly and not
‘advertised’ to anyone who should not have them.
Temperature of medicine storage area should be monitored day and should be not more than 25°C at any time. If the area is too hot, extra ventilation or an air-conditioning unit may be required
The medicine areas, trolley and cupboards must be large enough to safely store all the medicines.
There should be a dedicated space for nutritional supplements, prescribed dressings and ostomy products. These should not be stored on the floor or by a sink and should be on shelves in a locked cupboard.
Are medicines stored securely?
Only designated staff should be key holders and have access to medicines.
Medication Policy Template 12

Medicine room/cupboards/trolleys should be lockable. Medicine trollies should be secured to a solid wall when not in use
Keys for medicine room/cupboards/trolley should not be part of the master system
Keys should be kept securely. They should not be kept on a hook outside the medicine room.
The keys to the medicine room/cupboards/trolley should be carried on the person authorised to administer the medicines at that time.
There should be a recording system for who has the keys at any one time e.g. a signature sheet on shift handover
If a set of keys are lost, locks will have to be changed immediately
Medicines stored in residents’ rooms for self-medication should be in a lockable drawer or cupboard
There should be secure lockable storage for medicines delivered by the pharmacy to the home for the next cycle.
Is oxygen stored securely?
All rooms containing an oxygen cylinder should be clearly signposted and cylinders should be chained to the wall or held in an oxygen trolley
Medication Policy Template 13

4. Refrigerated medicines
Aim: To ensure that refrigerated medicines are stored safely and correctly, that residents always receive medicines of good quality and that there are good auditable procedures in place to monitor systems and storage.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Refrigerated medicines
Advice For care home use
Do staff responsible for handling & administering medicines know which medicines should be kept in the fridge?
Refer to labelling on medicine containers or patient information leaflets.
Is there a separate, lockable fridge for the storage of medicines that require cold storage?
Small homes that do not have regular refrigerated medicines may use a lockable cash box within the domestic fridge in the home.
Is the temperature of the fridge monitored daily when it is in use and recorded?
The temperature of the fridge should be in the range of 2 to 8°C
The temperature of the fridge must be monitored once a day using a minimum/maximum thermometer and following manufacturer’s instructions
Records should be kept of the minimum, maximum and current temperatures of the fridge.
The thermometer should be reset after these temperatures are recorded.
What is the procedure if the fridge temperature exceeds the
Move medicines to another fridge. Contact the pharmacy for advice on whether the
medicines are fit to be used Check that the fridge is functioning correctly. If the
Medication Policy Template 14

acceptable range? fridge has broken down, identify the fault quickly to prevent wastage of medication. Consider whether the door of the fridge was left open inadvertently
Is the fridge cleaned and defrosted regularly?
Some fridges have automatic defrost facility. Otherwise, clean and defrost fridge regularly and make records in the temperature record. Medicines should be moved to another fridge temporarily during the cleaning process.
5. Shelf-lives of medicines
Aim: To ensure that medicines are not used after their expiry date as this could cause harm to service users or they may not work, and to provide guidance on how long medicines will last after they have been opened.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Storage, stability and in-use shelf life guidelines for non-sterile medicines London, Eastern and South East Specialist Pharmacy Services March 2001Date written: August 2011Review date: August 2012Shelf lives of medicines
Advice For care home use
Is medication packed in Monitored Dosage Systems (MDS) i.e. blister packs or cassette-type systems?
Medicines dispensed in MDS should be discarded after 8 weeks if they have not been used. Medicines that are light or moisture sensitive should not be packed in MDS. It is the responsibility of the pharmacy to supply medicines in suitable packaging. Contact the pharmacy if there is any change in appearance of medication.
Apart from MDS, are all medicine containers dated when opened?
The expiry date of products can change once opened. Calculate the expiry date from the information on the medicine label or container see tables below
Do all staff handling medicines understand expiry dates?
See tables below
Are all medicines stored correctly either in a cool, dry place (below 25°C) or
See under Storage of medicines and Refrigerated medicines.
Medication Policy Template 15

refrigerated if required (2 to 8°C)?Are expiry dates of medicines checked on receipt from the pharmacy and every 4 weeks?
Highlight short expiry dates as a reminder to all staff. Rotate stock so that the earliest expiry is at the front and so used first.
Are expired medicines disposed of regularly according to medicines policy?
See under Disposal of medicines.
Suggested Guide to Expiry Dates for Medicines after Opening
ALWAYS check the pharmacy label and refer to the manufacturer’s expiry date and storage instructions in the first instance
Formulation and packaging of medicine
Suggested expiry dates after opening
MDS blister-packed or cassette-type systems
8 weeks
Tablets and capsules dispensed in boxes
Manufacturers expiry date printed on box or foil strip
Tablets and capsules in bottles or pots
Normally 12 months from date of supply.
Oral liquids 6 months ‘Special’ oral liquids, ointments, creams (unlicensed medicines made specially for resident)
Normally 4 weeks from date of manufacture. Some liquid ‘specials’ are produced in batches and last 4 weeks after opening
Tubes or pump packs of creams/ointments
3 months
Tubs of creams/ointments 1 monthEye, Ear, Nose drops/ointments 28 days Inhalers/aerosols Manufacturer’s expiry date
Common Exceptions
Dipyridamole MR caps (Persantin Retard, Asasantin Retard) (6 weeks) Risperidone (Risperdal) liquid (6 weeks)Oramorph 10mg/5ml liquid. (90 days)Antibiotic liquids (7 to 14 days)
Medication Policy Template 16

Examples of different wording of expiry dates.
Wording on packaging MeaningBest before January 2011 Discard on 31st December
2010Use by January 2011 Discard on 31st December
2010Use before end of January 2011
Discard on 31st January 2011
Discard after January 2011 Discard on 31st January 2011
Expires January 2011 Discard on 31st January 2011
6. Choice and Consent
Aim: To ensure that service users have the right to look after all or part of their medicines, that care home staff obtain consent to administer medicines and that the rights of service users to refuse medication is recognised and recorded.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Choice and Consent Advice For care home
useHas the resident given consent for the home to administer medicines?
When a resident first enters the home, check whether they are happy for the home to administer medicines or whether they would like to be responsible for all or part of their medicines. Obtain written confirmation of this choice. See also Self administration policy.
Is the resident asked each time they are given their medicines if they are happy to take them?
Medication Policy Template 17

Are the cultural requirements of the resident considered?
Consider the following: Vegetarians and people from some religious
groups do not want gelatin capsules (made from animal products)
Some people may prefer to have medicines given to them by people of the same gender
Some religious festivals include fasting and some people prefer not to have medicines given at certain times
Muslims may be concerned about medicines containing ‘unclean’ substances. www.islamset.com/bioethics/8thfiqh.html#2 has more advice.
What is the procedure if a resident refuses medication?
If a resident initially refuses a medicine, try again if it is safe to do so (be aware if the medicine is given more than once a day).If the medicine is still refused the medicine should be put into a suitable envelope or container, for later disposal, recording the name of the resident, medicine and date and time of refusal. Record on the MAR chart and in the care plan when medicines are refused, the reasons why if known and any action taken. If a resident refuses their medicines for 24 hours or appears unwell contact their GP for advice (or EMdoc). Action and record the advice given in the care plan.
What is the policy if the resident wishes to take non-prescribed medicines?
See Minor ailments and homely remedies.
Medication Policy Template 18

7. Administration of oral medicines
Aim: To encourage good practice in the administration of medicines to ensure that patients always have the correct medicines at the correct times and there are good auditable procedures in place to monitor systemsLegislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010CQC Professional Advice: The administration of medicines in care homes June 2008CQC Professional Advice: Training care workers to safely administer medicines in care homes November 2008British National Formulary (BNF) 61 March 2011Date written: August 2011Review date: August 2012Administration of oral medicines
Advice For care home use
Are care home staff trained to administer medicines?
Care workers should only give medicines they have been trained to give. See Training staff to administer medicines.
Registered nurses should comply with Nursing and Midwifery Council (NMC) guidance
Do care home staff know what the medicines are intended to do?
Refer to patient information leaflets, BNF or other reliable textbooks,
Ensure basic knowledge of medicines is covered in medication training course.
Are staff aware of any special precautions eg in relation to food or precise timings?
Check labels on dispensed medicines and MAR charts
Medication for Parkinsons Disease or epilepsy may have to be taken at set times during the day
Alendronic acid needs to be taken at least 30 minutes before breakfast and other medicines. See BNF.
See Administration of Warfarin. Is there a process for identifying staff members who handle and administer medication?
A signature list of staff members who handle and administer medication should be kept
Tabards may be worn by staff administering medication to highlight that they should not be disturbed during the medicine round.
Medication Policy Template 19
Have residents consented for the home to administer their medication?
See Choice and Consent.
Are medicines being given to the right person?
Make sure care home staff really know the residents by name.
Confirm the name with resident if possible. Check the photo in the MAR chart. Photos should
be recent. Name and room number may be cross referenced
on MAR chart. What is the process for administering oral medicines?
Refer to MAR chart to select correct medicines for this time of day for that resident, including medicines from the fridge and those not packed in MDS e.g. inhalers, when required medicines. Remember that medication may have changed since last time staff member was on duty.
Check that the resident’s name is on the label and that the medicine is in date.
Ask the resident if they want to take all their medicines before they are taken out of the pack. When required (prn) medicines e.g. for pain, indigestion, constipation may only need to be taken occasionally. Staff may need to assess their need before administration.
Dignity and privacy of resident should be preserved where possible e.g. when asking about bowel movements. Certain medicines may be requested to be administered in the privacy of the resident’s room.
Make sure there is a tumbler of water to wash tablets or capsules down. A hot cup of tea instead of water is not a good idea because many medicines are badly affected by heat.
Medicines must be given from the container they are supplied in and not put in medicines pots or other containers in advance. This is called secondary dispensing and can lead to serious errors.
As each medicine is removed from its package put a dot in the signature box on the MAR chart to confirm that you have each medicine.
Put tablets or capsules into a clean, dry medicine pot without touching them. Several pots may be required where tablets may need to be dispersed in water, dissolved in the mouth or if some are liquid medicines.
Medication Policy Template 20

Some medicines may be harmful to the person administering medicines if they have direct contact with them. It may be advisable to wear plastic gloves if you know there is a health and safety risk.
Use 5ml medicine spoons, oral syringes or graduated medicines cups to correctly measure out liquid medicines. Do not mix liquid medicines together in one cup or syringe. Use a separate measure for each medicine.
Encourage the resident to sit upright or to stand. It is very difficult to swallow tablets or capsules when lying down. Tablets or capsules could get stuck in the throat or gullet where it could cause difficulty with swallowing or could damage the lining of the gullet.
Hand the medicines to the resident and ask them to take the medicines.
When the resident has taken the medicines (and you know they have) sign the MAR chart for each medicine given. Specify how much is given when the directions state for example ‘one or two’.
It is not good practice to hand the medicines to another member of staff to give unless they have personally checked each medicine is correct, and then both should sign the record as both have been involved in its administration.
Where the resident does not want to take the medicines at that time and where the medicines are important, wait a while and ask them again later. See Choice and Consent.
Where a medicine is not given for any reason e.g. patient in hospital, refused write the correct code on the MAR chart in the signature box. A list of codes and their explanations should be printed on the MAR chart. Make records on the reverse of the MAR chart to explain exactly what happened e.g. dose dropped, medicines spat out by resident and sign this record.
Do not begin to administer the medicines to the next resident until the MAR chart has been completed.
Administer and record homely remedies according to Homely Remedy policy. See Minor ailments and homely remedies.
At the end of the medicine round, check that the medicines that should have been given have been
Medication Policy Template 21

given and that the MAR charts have been completed correctly.
Medication Policy Template 22

8. Administration of creams and ointments
Aim: To encourage good practice in the management of external medicines such as creams and ointments to ensure correct administration to patients, correct storage and recording of applications, that medicines are in date and that there are good auditable procedures in place to monitor systems. Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC) Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010CQC Professional Advice: The administration of medicines in care homes June 2008CQC Professional Advice: Training care workers to safely administer medicines in care homes November 2008Date written: August 2011Review date: August 2012Administration of creams and ointments
Advice For care home use
Are all external preparations e.g. creams, ointments, shampoos, bath preparations stored securely in locked cupboards separately form internal medicines?
External preparations can be stored in residents’ rooms with their permission. Safe and secure storage must be available and the temperature of the room should not exceed 25°C
External applications such as Daktacort cream or Timodine cream which need to be stored in the fridge, should be stored in a lockable medicine fridge or in the case of smaller homes a lockable box like a cash tin which is kept in the domestic fridge.
Who can apply external preparations?
Registered nurses can delegate the application of soap substitutes such as aqueous cream, moisturising creams and barrier creams, shampoos or bath preparations to suitably trained care staff. The nurse is responsible for ensuring that these preparations are used correctly.
Medication Policy Template 23

How should creams and ointments be applied?
External applications should be labelled with clear directions for use.
When applying any external preparation, wash your hands and wear protective gloves
Check that the preparation is in date. The date of opening should be written on the label. Any cream or ointment in a tube or pump pack, shampoos, bath and shower preparations and lotions will usually last 3 months after opening (see Shelf-lives of medicines). Any tub in which fingers have to be used to remove the cream (even with gloves on) has a 1 month expiry after opening and any unused cream should not be returned to the tub as this will contaminate it.
Always apply creams and ointments to clean skin. Steroid creams e.g. hydrocortisone,
betamethasone should be applied sparingly to the affected area. One fingertip unit from a tube (the length from the top joint of the index finger to its tip) will cover an area approximately the size of the palm of your hand.
Moisturising creams and ointments can be applied liberally
When using creams and ointments, apply by smoothing them gently into the skin along the line of hair growth and do not rub in.
How should external applications be recorded?
The person administering the external application must sign the MAR chart. If a nurse has delegated the task of administering external applications to care staff, the care staff must sign the MAR chart. Separate MAR charts for this purpose can be supplied by the pharmacy and kept in the resident’s room.
Some people are prescribed creams such as aqueous cream to use as a soap substitute. The care plan should list these products and what they are for. A record could be made in the daily care notes to record that the cream had been used to wash the person to demonstrate that staff are using the cream appropriately.
Medication Policy Template 24

9. Monitored dosage systems (MDS)
Aim: To ensure the safe management and administration of medication packed in monitored dosage systems and that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Monitored dosage systems (MDS)
Advice For care home use
Which MDS system does the home use?
MDS is usually in the form of blister packs or cassettes. Consult with the pharmacy as to the most suitable MDS for the home. Medicines should not be re-packaged by care staff into compliance aids for their own convenience. This is known as secondary dispensing and can lead to mistakes
Are all staff involved in medication administration trained and competent to use MDS?
The community pharmacy will normally provide training on the particular MDS used.
Which medicines are not suitable to be packed in MDS?
Liquids, light or moisture sensitive medicines e.g. effervescent tablets, medicines that may be harmful if handled e.g. cytotoxic medicines, when required medicines that are only given occasionally as this would lead to waste, medicines where the dose is dependent on blood test results e.g. warfarin, The pharmacy will advise which medicines are not suitable for packing in MDS.
How long do medicines last when packed in MDS?
MDS packs should not be used 8 weeks after preparation.
Medication Policy Template 25

What is the procedure for checking MDS packs received by the home?
Check the medication against the medicines that the patient may have had the previous month
Check that the MDS packs have been accurately dispensed by the supplying pharmacy i.e. contain the correct amounts of medicines in each blister
Check that the MDS packs are labelled properly with clear dosage instructions and any special warnings.
If there are more than one type of tablet or capsule in each MDS pack then check that a description of each medicine is included on the pack so that identification can be made of each medicine.
Contact the supplying pharmacy if the MDS packs do not match the current medication regime for the patient, if anything is missing or if the medicine is different to what you expect (i.e. the medicine looks different and no information has been supplied by the pharmacy that the type of medicine supplied is different from before).
Do not administer any medicines if you are not sure whether they are correct or intended until checked with the pharmacy or in the case of a dose change, the resident’s GP.
Check the printed MAR charts for accuracy as the accuracy of the MAR chart is the responsibility of the home
Should a dose change, the care home must consider carefully how the old MDS packs are to be dealt with. This may mean obtaining new prescriptions or removing the discontinued medicine from the MDS if using blister packs. Do not remove, add or move medication in MDS cassette systems.
Medication Policy Template 26

10. Medicine administration records (MAR) charts
Aim: To ensure that MAR charts are complete, up-to-date and accurate records of medication prescribed, received, administered and disposed off including when medicines should be given, the dose and any special information such as giving the medicines with food, to prevent errors in administration and to ensure that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain November 2007Care Quality Commission (CQC): Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010CQC Professional advice: Medicine administration records (MAR) in care homes and domiciliary care June 2008Principles of safe and appropriate production of medicine administration charts Royal Pharmaceutical Society of Great Britain February 2009Date written: August 2011Review date: August 2012MAR charts Advice For care home
useWho is responsible for providing MAR charts?
The care provider, not the supplying pharmacy.
Is the MAR chart a legal document?
Yes, it is a legal requirement that care homes keep records of medicines kept for each resident and the date on which they were administered to the resident. Records must be indelible, contain no obliterations and be kept for 3 years from the last date of entry.
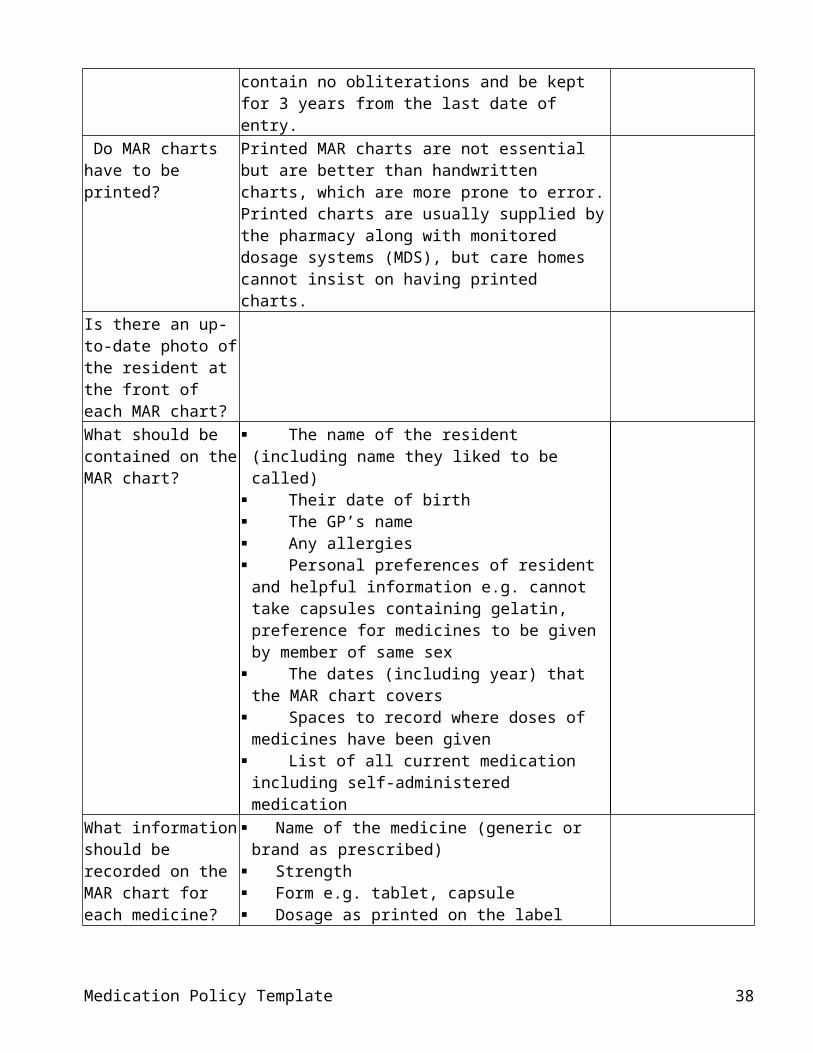
Do MAR charts have to be printed?
Printed MAR charts are not essential but are better than handwritten charts, which are more prone to error. Printed charts are usually supplied by the pharmacy along with monitored dosage systems (MDS), but care homes cannot insist on having printed charts.
Is there an up-to-date photo of the resident at the front of each MAR chart?
Medication Policy Template 27

What should be contained on the MAR chart?
The name of the resident (including name they liked to be called)
Their date of birth The GP’s name Any allergies Personal preferences of resident and helpful
information e.g. cannot take capsules containing gelatin, preference for medicines to be given by member of same sex
The dates (including year) that the MAR chart covers
Spaces to record where doses of medicines have been given
List of all current medication including self-administered medication
What information should be recorded on the MAR chart for each medicine?
Name of the medicine (generic or brand as prescribed)
Strength Form e.g. tablet, capsule Dosage as printed on the label The times of day that the medicine should be
given (these should be agreed with pharmacy so that they are spread out evenly throughout the day)
Any special information e.g. giving the medicine before or after food, where the cream should be applied
When the medicine was first prescribed When a medicine was received, how much and
when it was received Route of administration e.g. oral, topical, PEG Medicines returned for disposal or destroyed
(care homes with nursing only)What is the procedure for hand-writing entries on the MAR chart?
Entries should be written clearly and legibly with the information listed above. The entry should have 2 signatures: the person who made the entry and that of a second person who has checked that the entry is correct.
What is the procedure for recording self-administration on the MAR chart?
If a resident is self-administering their own medicines then record on the MAR chart the date and the amount of the medicine that they have been given (you could ask them to sign the MAR chart to confirm they have received them). See Self-administration of medicines
Is the MAR chart signed after each medicine has been
The MAR chart must be signed immediately after a medicine has been given.
Medication Policy Template 28

given by the person who has given the medicine and not at the end of the medicine round?Is there a list of codes on the MAR chart to show why a medicine has not been given?
These should be printed on the MAR chart with an explanation of what each code means. It is important to keep a record when a prescribed medicine has not been given and why.
Does the MAR chart show how much has been given if the dose on the MAR chart is variable e.g. 1-2 or 5 - 10ml?
The exact dose given should be recorded on the MAR chart or on a separate prn chart. See When required (prn) medicines.
Is the back of the MAR chart used to record any further information concerning medicine administration?
The back of the MAR chart may be used to record where for example a resident was sick soon after administration or when required medicines.
Is the MAR chart used to record medicines that are not ordered each month?
The MAR chart can be used to keep track of medicines that are not ordered every month but only taken occasionally e.g. it can be used to record tablets carried over onto a new chart. Make sure that the pharmacy knows all the medicines that are ongoing and need to be printed on the MAR chart.
What are the arrangements for amending the MAR chart when a service user’s medication is altered?
Care staff are responsible for amending the MAR chart: Cancel the original direction Write the new directions legibly and in ink on a new line of the MAR chart. Write the name of the doctor or other prescriber who gave the new instructions Date the entry and sign (including a witness when this is possible)
How is the application of external preparations e.g. creams, ointments recorded?
Application of external applications may be recorded on a separate MAR chart in the resident’s room.
Medication Policy Template 29

11. When required (prn) medicines
Aim: To encourage good practice in the management of when required medicines that are not given or applied routinely and that there are good auditable procedures in place to monitor systems so that the medicines are only ordered when needed, are in suitable packaging to minimise wastage and their administration is recorded accurately.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012When required medicines
Advice For care home use
What are when required (prn) medicines?
When required medicines are medicines that are not given or applied routinely eg painkillers, laxatives, indigestion mixtures, salbutamol inhalers, glyceryl trinitrate (GTN) sprays. They are usually prescribed to treat short term or intermittent medical conditions. To ensure that medication is given correctly a specific plan for administration must be recorded in the care plan. This should include information on why the medication has been prescribed, how to give it including the maximum dose that can be given in 24 hours. A prn chart can be made up and kept with the MAR charts.
When should prn medicines be offered to residents?
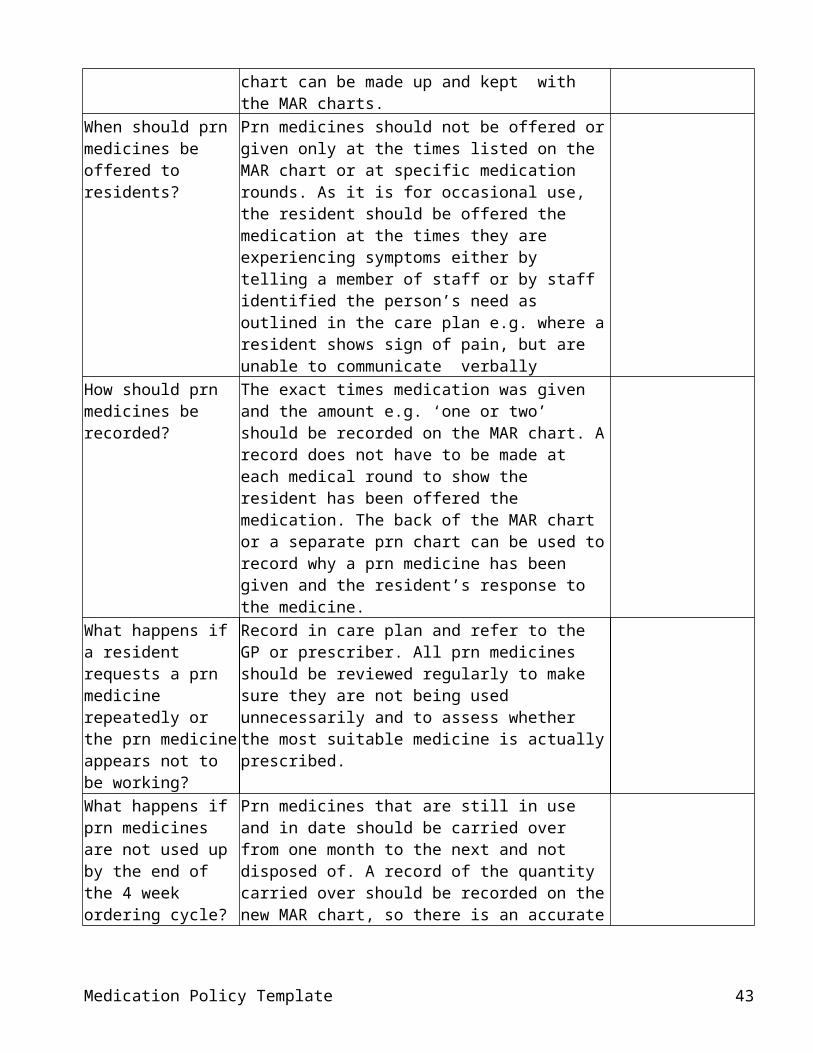
Prn medicines should not be offered or given only at the times listed on the MAR chart or at specific medication rounds. As it is for occasional use, the resident should be offered the medication at the times they are experiencing symptoms either by telling a member of staff or by staff identified the person’s need as outlined in the care plan e.g. where a resident shows sign of pain, but are unable to communicate verbally
How should prn medicines be recorded?
The exact times medication was given and the amount e.g. ‘one or two’ should be recorded on the MAR chart. A record does not have to be made at
Medication Policy Template 30

each medical round to show the resident has been offered the medication. The back of the MAR chart or a separate prn chart can be used to record why a prn medicine has been given and the resident’s response to the medicine.
What happens if a resident requests a prn medicine repeatedly or the prn medicine appears not to be working?
Record in care plan and refer to the GP or prescriber. All prn medicines should be reviewed regularly to make sure they are not being used unnecessarily and to assess whether the most suitable medicine is actually prescribed.
What happens if prn medicines are not used up by the end of the 4 week ordering cycle?
Prn medicines that are still in use and in date should be carried over from one month to the next and not disposed of. A record of the quantity carried over should be recorded on the new MAR chart, so there is an accurate record of the quantity in stock and to help when performing audits. Make sure to inform the pharmacy of prn medication to continue on the MAR chart, even though it may not have been ordered for the next cycle. Quantities of medication should be reviewed regularly to ensure they are used before they go out of date and excess quantities are not stored in the home.
How should prn medicines be supplied?
Prn medication is best supplied in an original box rather than a monitored dosage system (MDS). This allows for a check on the expiry date and reduces waste. Any medication left over in a MDS at the end of the cycle will have to be disposed of, where MDS have a maximum 8 week shelf-life.
Medication Policy Template 31
12. Verbal orders and dose changes
Aim: To ensure that there are good auditable procedures in place to monitor systems to record any change to medication and that residents always receive the correct dose of their medicines.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations March 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010CQC Professional advice: Medicine administration records (MAR) in care homes and domiciliary care June 2008Date written: August 2011Review date: August 2012Verbal orders and dose changes
Advice For care home use
What is the procedure for dealing with verbal orders?
A new prescription is not always necessary for a dose change. The care home should have a procedure to communicate changes clearly and who is responsible for taking the order. Records of telephone calls should include: Who took the telephone call The time of the call The name of the person who called The changes madeIt is good practice to: Read back the information that has been
written down to reduce the chance of misunderstandings
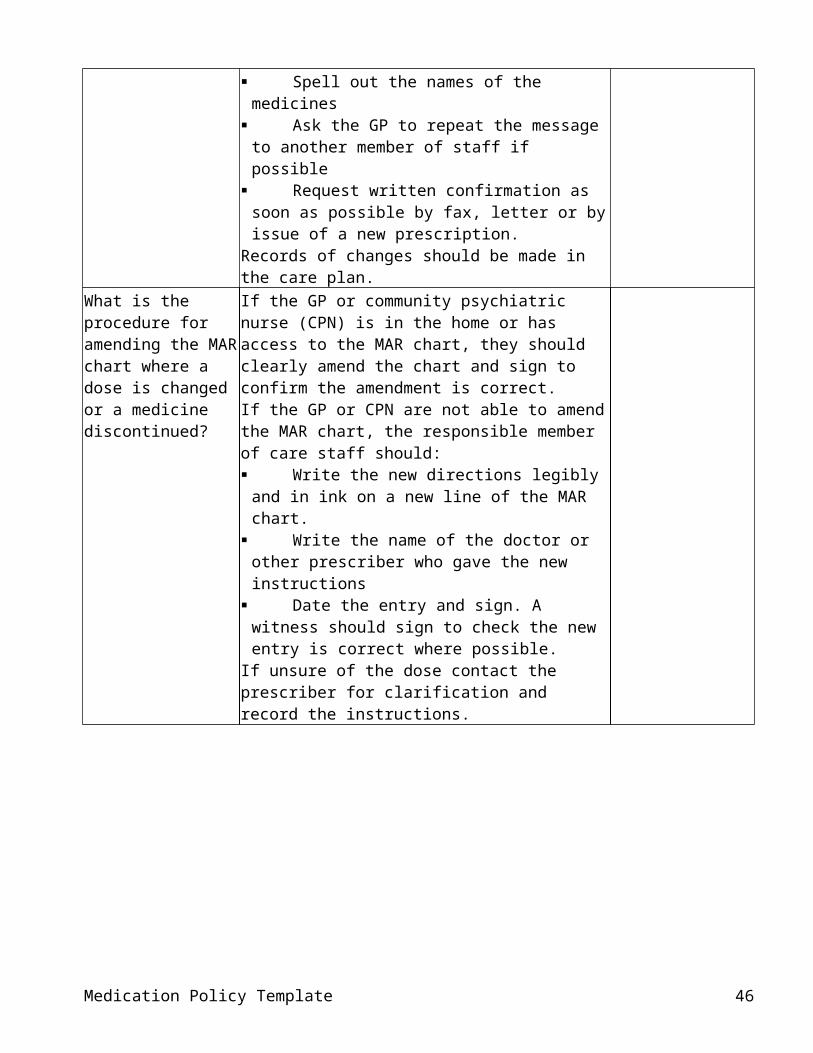
Spell out the names of the medicines Ask the GP to repeat the message to
another member of staff if possible Request written confirmation as soon as
possible by fax, letter or by issue of a new prescription.
Records of changes should be made in the care plan.
What is the procedure for
If the GP or community psychiatric nurse (CPN) is in the home or has access to the MAR chart, they
Medication Policy Template 32

amending the MAR chart where a dose is changed or a medicine discontinued?
should clearly amend the chart and sign to confirm the amendment is correct.If the GP or CPN are not able to amend the MAR chart, the responsible member of care staff should: Write the new directions legibly and in ink on
a new line of the MAR chart. Write the name of the doctor or other
prescriber who gave the new instructions Date the entry and sign. A witness should
sign to check the new entry is correct where possible.
If unsure of the dose contact the prescriber for clarification and record the instructions.
Medication Policy Template 33

13. Self administration of medicines
Aim: To ensure that residents in care homes have the opportunity to self-administer their medicines where possible, that robust systems for risk assessment are in place including regular review and that there are good auditable procedures to monitor self-administration.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007The Mental Capacity Act 2005 and Code of PracticeThe Disability Discrimination Act (DDA) 1995Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010CQC Professional Advice: The administration of medicines in care homes June 2008Date written: August 2011Review date: August 2012Self administration of medicines
Advice For care home use
Is the level of support in the administration of medicines the resident would like discussed on admission to the home?
Residents should be given the choice to take responsibility for their medicines where possible. This promotes independence and dignity and applies to residents in care homes with nursing as well as care homes offering personal care only. It is particularly important for patients in short-term respite care or intermediate care to be encouraged to manage their medicines, as they may need to do so when they return home. Residents may wish to look after some of their medicines e.g. inhalers, creams, but not tablets and liquid medicines. However, many residents, particularly older people prefer care staff to take responsibility for all their medicines.The resident’s choice should be clearly documented in the care plan.
Is there a robust risk assessment process for self-administration of medicines?
Care workers should identify whether residents who are confused or lack cognitive awareness can safely keep and take their own medicines. The risk to the resident who looks after his/her medicines and the potential risk to other people in the care home should be assessed.
Medication Policy Template 34

The assessment should include whether the resident:- Wants to take responsibility for looking after and
taking their medicines and if so which ones to include.
Requires any support to do this. Community pharmacists can adjust labelling or packaging to promote self-administration e.g. monitored dosage systems, large print labels, containers with ordinary caps instead of child-resistant closures
That the person knows the medicines they take, what they are for, and when to take them and what is likely to happen if they omit taking them.
Understands the importance of not leaving medicines lying around where someone else may unintentionally take them.
The resident’s ability to self-medicate should be monitored and reviewed regularly.
What records should be made for self-administration?
Records should be made in the resident’s care plan, listing each medicine that is to be self administered and how to monitor whether the service user is still able to self administer medicines without constantly invading their privacy
The resident should sign this record and agree to let the staff know if they are having any problems, to allow regular reviews as part of their care and that if carers are responsible for obtaining their medicines that they are informed in advance that a new supply is needed.
A record must be kept of all the resident’s medicines in case of hospital admission and this should be updated if any medicines are added or discontinued.
If the staff in the home are responsible for obtaining the medicines, a list of what and when the medicines are given to the resident should be kept. This can also be helpful to review and monitor the resident’s progress
Where a resident self-administers, this should be indicated on the MAR chart. The carer does not need to fill in the administration section.
Do residents have suitable storage facilities for their medicines for self-administration?
A lockable drawer or cupboard should be provided in the resident’s room.
Medication Policy Template 35

14. Swallowing Difficulties and Covert Administration
Aim: To ensure best practice in the selection of suitable formulations for residents with swallowing difficulties, and to ensure that covert administration of medicines only takes place within the context of existing legal and best practice frameworks to protect the resident receiving the medicines and the care workers involved in giving the medicines..Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Mental Capacity Act 2005 and Code of PracticeThe Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC): Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010 CQC Professional Advice: The administration of medicines in care homesNursing and Midwifery Council (NMC) Medication Standards April 2010Choosing medicines for patients unable to take solid oral dosage forms UKMi North West January 2010 (see Appendix)Date written: August 2011Review date: August 2012
Swallowing Difficulties and
Covert Administration
Advice For care home use
What is the procedure for residents who have difficulties with swallowing medication?
The resident should have a medication review to check that the medicines are still needed and are working properly.
Alternative licensed formulations e.g. liquids, soluble tablets, powders for suspension or a similar medicine should be explored first.
If an alternative formulation or medicine is not available, a licensed medicine can sometimes be used in an unlicensed manner e.g. by crushing/dispersing tablets in water or by opening capsules. This must not be done without consulting the GP and pharmacist to ensure thatthe resident will come to no harm and that the tablet is suitable to be crushed. The pharmacist will also advise whether crushed tablets or capsule contents can be safely mixed with food or drinks.A written direction must be recorded in the resident’s care plan.
Medication Policy Template 36

Where no licensed medicine is available, a special-order liquid medicine may be considered. These are unlicensed medicines.
What is covert administration?
Covert administration occurs when medicines are administered in a disguised form, without the knowledge or consent of the person receiving them, for example in food or drink.Medicines should never be given covertly to people who are capable of deciding about their medical treatment. Giving medication by deception is potentially an assault.If a person agrees to having a medicine crushed or mixed with food to make it more palatable or easier to swallow, this is not covert administration.
When can covert administration take place?
Covert administration is sometimes necessary and justified where a medical practitioner states that the person lacks ‘capacity to consent to treatment’ and the medicine is essential to their health and well being.It should only take place in the context of legal and best practice frameworks. This protects both the person receiving the medicines and the care workers involved in giving them.The decision to covertly administer must not be made by the care home. It should be made by careful assessment of the resident’s needs and an open discussion and agreement within a multidisciplinary team including carers, relatives and advocates. Written agreement of all involved must be obtained and documented in the resident’s care plan and be reviewed at regular intervals.The method of administration of the medicines should be agreed with the pharmacist (see above).
Medication Policy Template 37
15. Disposal of Medicines
isposal Aim: To ensure the safe disposal of surplus, unwanted or expired medicines and that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010The National Health Service (Pharmaceutical Services) Regulations 2005Date written: August 2011Review date: August 2012
Disposal of Medicines
Advice For care home use
What are the arrangements for care homes (personal care) for disposing of surplus, unwanted or expired medicines?
Unwanted medicines should be returning to the supplying pharmacy. The pharmacy can then ensure that these medicines are disposed of in accordance with current waste regulations.
What are the arrangements for care homes with nursing for disposing of surplus, unwanted or expired medicines?
Pharmacies are not obliged to collect unwanted medicines from care homes with nursing as part of the NHS community pharmacy contract essential services. Care homes with nursing should make their own arrangements for disposal of medicines and use a licensed waste management company. Records of transactions with the waste management company should be kept.
How are medicines for disposal stored in the home?
All medicines that are unwanted or expired should be stored separately from the medicines in use and securely locked away. This includes any medication disposal bins provided by the waste management company.
What happens when a service user dies?
When a person dies, all the medicines must be kept for 7 days before disposal, in case the Coroner’s Office wants them. The medicines should be stored separately as above.
What records should be made for the disposal of medicines?
The following should be recorded: Date of disposal/return to pharmacy Name and strength of medicines Quantity removed Person for whom medication was prescribed or
purchased Signature of the member who arranges disposal of
Medication Policy Template 38

the medicines In care homes with nursing, the signatures of the
person who disposes of the medicines and a responsible witness.
How is the disposal of controlled drugs managed?
See Controlled drugs.
Medication Policy Template 39

16. Controlled drugs
Aim: To ensure the safe storage, administration, recording and disposal of controlled drugs in line with legal requirements and that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010 The Misuse of Drugs Act Regulations 2001The Misuse of Drugs (Safe Custody) Regulations 1973The Misuse of Drugs and Misuse of Drugs (Safe Custody) (Amendment) Regulations 2007A guide to good practice in the management of controlled drugs in primary care (England) Third edition National Prescribing Centre December 2009Safer Management of Controlled Drugs Regulations 2006Medicines, Ethics and Practice The professional guide for pharmacists Edition 35 July 2011CQC Professional Advice: The safe management of controlled drugs in care homes November 2008
Date written: August 2011Review date: August 2012Controlled drugs (CDs)
Advice For care home use
How should CDs be stored?
Controlled drugs should be stored in a designated CD cupboard conforming to The Misuse of Drugs (Safe Custody) Regulations 1973. The 2007 Amendment to Regulations made this mandatory for all care homes. The cupboard should be: a metal cupboard of specified gauge have a specified double locking mechanism be fixed to a solid wall or a wall that has a
steel plate mounted behind it be fixed with either Rawl or Rag bolts.Suppliers of CD cupboards can confirm that a cupboard meets the legal requirements and care homes should request formal confirmation when purchasing a CD cupboard.The CD cupboard should only store controlled drugs and not items of value such as jewellery or
Medication Policy Template 40

money.Who should hold the keys to the CD cupboard?
Access to the CD cupboard must be restricted to designated key holder. The keys to the CD cupboard are normally held with the keys for the other medicine cupboards on the person in charge.
Which CDs should be stored in the CD cupboard?
All Schedule 2 and some Schedule 3 controlled drugs see table below. The original manufacturer’s pack states CD POM on the packaging of Schedule 2 drugs.
How are CDs obtained?
CDs are prescribed and dispensed for individually named people in the same way as other medicines. However, there are special legal requirements for CD prescriptions and a prescription that does not comply with these requirements may have to be returned to the prescriber for altering before it can be dispensed. Care staff collecting CDs from a pharmacy on behalf of someone else may be asked to provide identification. ‘Stock’ CDs can only be ordered if the organisation has obtained a Home Office Licence.
What records need to be kept for CDs?
The receipt, administration and disposal of CDs must be recorded in the CD register (see also table below). The CD register should be a bound book with numbered pages and not loose sheets. There should be a separate page for each CD for each person. The balance for each product should be included and checked against the amount in the pack or bottle after each administration and also on a regular basis e.g. monthly. All transactions in the CD register should match those recorded on the MAR chart. It is good practice to keep CD registers for longer than the mandatory 2 years, where cases may come to court at a much later date.
How are CDs received into the home?
On receipt of the CD from the supplying pharmacy, the date, quantity and name of supplier should be entered into the CD register and initialled by the receiving nurse or authorised member of staff, with a second person as witness. The correct balance should be verified each time. CDs should be recorded in the CD register as soon as they arrive in the home and locked in the CD cupboard.
How are CDs administered?
Registered nurses should administer CDs in care homes with nursing. In care homes providing personal care, CDs should be administered by appropriately trained care staff and this should be witnessed by another appropriate member of staff.
Medication Policy Template 41

The resident’s name plus time and dose given should be recorded in the CD register after checking the MAR chart. Once the registered nurse/trained carer has witnessed the resident taking the medication, the MAR chart can be initialled by the nurse/trained carer.Before administering the medicine, the nurse/trained carer should measure and check the dose with a competent witness. Oral syringes should be used to measure liquid CDs.The nurse/trained carer and the witness should then initial the CD register, after verifying that the remaining balance is correct.
How should discrepancies be dealt with?
Discrepancies should be reported to the home manager and be investigated promptly. If a discrepancy cannot be resolved, the advice of the pharmacist should be sought and CQC informed. CQC will inform the local Accountable Officer if necessary.If the discrepancy is found to be an error of subtraction or addition in the calculation of the stock balance, do not change the balance column of use correction fluid. Under the last entry, details of the following should be recorded: the date the error in subtraction/addition (indicated
with an asterisk) the correct balance the signature of the nurse/member of staff
and the witnessing nurse/member of staffIn care homes with nursing where a dose is given, but the administering nurse fails to complete the CD register at the time of administration, under the last entry, details of the following should be recorded: the current day’s date ‘dose administered but not recorded at the
time’ followed by the resident details the signature of the administering nurse and
that of a witness the correct balanceIf neither of the above discrepancies can be identified, contact the pharmacist to establish whether there was any unrecorded returns of CDs. If confirmed by the pharmacist, full details of such returns should be entered into the CD register, together with the signature of the person who
Medication Policy Template 42
returned the drugs and the pharmacist who received them. The correct date and the words ‘entered in retrospect’ should be added.If the reason for the discrepancy cannot be found and the CDs appear to have gone missing, then all relevant people, including the police should be notified.
How should the disposal of controlled drugs in care homes (personal care) be managed?
Controlled drugs should be returned to the supplying pharmacy. Records of the return should be made in the controlled drugs register. It is good practice to obtain a signature of receipt from the pharmacist.
How should the disposal of controlled drugs in care homes with Nursing be managed?
The Home Office has advised that all CDs in Schedules 2, 3 and 4 (part 1 CD BenzPOM) (see table below) should be denatured and therefore rendered irretrievable before being placed into waste containers. A denaturing kit specially designed for this purpose should be used and the waste disposed off through the contracteda licensed waste management company in line with their requirements. . The company should have authorisation to transfer and dispose of controlled drugs. A nurse and an appropriate witness should oversee the destruction and sign the record of disposal in the controlled drugs register. The Royal Pharmaceutical Society gives guidance for pharmacists on how specifies how CDs should be destroyed according to their formulation (see table below), but CQC does not expect care homes to conform to this guidance, but to risk assess their processes for disposal of CDs.. Where syringes contain CDs, local guidance advises that the contents of the syringe is must be tipped into the CD denaturing kit directly onto the resin crystals. If the syringe is rinsed with water the first rinsing should be added to the denaturing kit.CDs supplied as stock to the home can only be destroyed in the presence of an authorised person (contact local Accountable Officer for advice 020 8776 3669).
How are CDs for self-administration managed?
If a service user is self-administering their own CDs, then these can be stored in a locked cupboard or drawer in their room. This also applies to monitored dosage systems (MDS) containing CDs. There is no need to keep a record in the CD register when the person is wholly independent and is responsible for requesting a prescription and collecting the CDs
Medication Policy Template 43

personally from the pharmacy. Where the home arranges the supply and collection of CDs for a service user, clear records in the CD register should be made of receipt from the pharmacy, supply to the service user and any subsequent disposal of unwanted CDs. Each individual dose does not have to be recorded.
For care homes (personal care), what are the arrangements for CDs administered by community nurses?
Any CDs given by injection are the responsibility of community nurses. It is important to make sure the care home retains a record of all CD administration, especially when the community nurse completes a record that is not left in the care home. If the community nurse is not willing to make a duplicate record in the CD register, the witness must complete this record.
Medication Policy Template 44

Common controlled drugs and legal requirements for care homes.
Schedule 2 (CD POM)CD Brand names Legal RequirementsMorphine MST, MXL
Zomorph Oramorph Concentrated oral solution 100mg/5ml *
Store in a CD cupboard Record in the CD register. Must be denatured before
disposal
* Oramorph oral solution is also available in 10mg/5ml which is not a controlled drug. However, CD storage and CD records are a good practice recommendation.
DiamorphineMethadone PhyseptoneMethylphenidate Concerta XL
Equasym XL Medikinet, Ritalin
Fentanyl Durogesic DTrans Actiq Effentora
Oxycodone OxyNorm OxyContin
Schedule 3 (CD No Register POM)CD Brand names Legal RequirementsBuprenorphine Butrans, Transtec
Temgesic Buprenorphine, and
Temazepam must be stored in a CD cupboard. Other listed schedule 3 controlled drugs do not need CD storage.
None of the controlled drugs in this schedule need to be recorded in the CD register but this is a good practice recommendation.
Must be denatured before disposal
** Currently not licensed medicines.
Midazolam Hypnovel, Epistatus** Buccolam**
TemazepamPhenobarbitone
Schedule 4 (CD Benz POM)CD Brand names Legal RequirementsDiazepam, NitrazepamLorazepamZolpidem
Valium No CD storage or recording requirements
Must be denatured before disposal
Medication Policy Template 45
Destruction of Controlled DrugsGuidance for pharmacists Royal Pharmaceutical Society July 2011
DOSAGE FORM METHOD OF DESTRUCTION TABLETS AND CAPSULES Remove from outer packaging and, wearing
gloves, remove from blister packaging and place into a CD denaturing kit (a commercial product designed to render Controlled Drugs irretrievable). Best practice would be to grind* or crush* the solid dosage formulation before adding to the CD denaturing kit to ensure that whole tablets or capsules are irretrievable.
LIQUID DOSE FORMULATIONS
Pour from container into a CD denaturing kit, which should then be placed into a pharmaceutical waste container.
AMPOULES Wearing suitable protective gloves, ampoules containing liquid should be opened and the contents emptied into a CD denaturing kit or disposed of in the same manner as the disposal of liquid dose formulations above. The ampoule can then be disposed of in the sharps bin. Wearing suitable protective gloves, ampoules containing powder can be opened and then have water added to dissolve the powder inside. The resulting mixture can then be poured into the CD denaturing kit. The ampoule can be disposed of in the sharps bin.
FENTANYL OR BUPRENORPHINE PATCHES
The active ingredient in the patches can be rendered irretrievable by removing the backing and folding the patch over on itself and then placing it in a waste disposal bin or, preferably, a CD denaturing kit. Gloves must be worn by the person destroying the patch.
Medication Policy Template 46

17. Medication Errors and Adverse Drug Reactions
Aim: To ensure that there are clear and auditable procedures to deal with medication errors and adverse drug reactions to minimise harm to residents and to include taking the appropriate action, keeping records and informing the appropriate people.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Medicines errors and adverse drug reactions
Advice For care home use
What action should be taken on the discovery of prescribing or dispensing errors?
Medication received by the home should be checked on receipt. Any errors or discrepancies should be referred to the dispensing community pharmacy immediately. Any unexpected changes in prescriptions should be queried with the GP.
What action should be taken where there is a medication administration error e.g. wrong dose is given, medication is not given or medication is given to the wrong person?
Care staff and registered nurses should report any error or incident in the administration of medicines to the manager or person in charge.
Clinical advice should always be sought immediately. If the resident is unwell, call the Emergency Services. If the resident is not unwell, call their GP (or EMdoc if out-of-hours) to inform them and ask what they want you to do. The GP should always be told even if advice is sought from a different source.
Make a written report describing what happened, what has been done and any observations of the resident that have been made since the incident took place.
Report any serious incidents to CQC by filling in Regulation 37 form “Statutory Notification about a person who lives in a care home” and send by post to CQC National CorrespondencePO Box 1258 Newcastle upon Tyne NE99 5AU
Medication Policy Template 47

Inform the resident’s relatives Review how the error occurred to prevent a similar
error happening again e.g. through training or change to existing procedures.
It is important to encourage a culture that allows staff to report incidents without the fear of an unjustifiable level of recrimination.
What is the procedure if a resident suffers an adverse drug reaction?
If a new medicine is given to a resident and they subsequently become unwell, this could be caused by the medicine. Seek advice as above and make appropriate records. Update the resident’s care plan and MAR chart under allergies if the medicine is subsequently proven to have caused the adverse reaction.
How are adverse drug reactions reported for safety and monitoring purposes?
Healthcare professionals and patients can report suspected side effects to any medication including vaccines through the Yellow Card Scheme. Details can be found on the MHRA website www.yellowcard.mhra.gov.uk
Medication Policy Template 48

18. Minor Ailments and Homely Remedies
Aim: To ensure safe administration of non-prescribed medication and homely remedies for minor ailments and that there are good auditable procedures in place to monitor systemsLegislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012Minor Ailments and Homely Remedies
Advice For care home use
What are homely remedies?
Homely remedies are medicines that have not been prescribed and can be purchased through retail outlets and over-the-counter (OTC) in pharmacies. They are treatments people use themselves without consulting their GP i.e. for minor ailments such as toothache or indigestion. People may choose to buy herbal remedies or products from other countries e.g. traditional Chinese remedies. There are risks that prescribed medicines will interact with medicines purchased over the counter and cause harm.
Do care homes have to keep homely remedies?
No, the care home is under no obligation to provide treatment for minor ailments. However, the GP may not be willing to prescribe paracetamol for every resident in a care home just in case they need it for an occasional headache or toothache.
What are the arrangements for the treatment of minor ailments in the care home?
If someone is living in their own home, they can choose to buy and take homely remedies and they should have that choice when they live in a care home. However, if the resident is unable to make the choice, the care home will have to make the decision for them. The care home may decide to keep a range of homely remedies in which case they must have a written protocol for administration (see below). Alternatively, they should seek the advice of the GP,
Medication Policy Template 49

pharmacist or nurse. Where relatives or friends buy homely remedies for residents, including vitamins, minerals and other supplements such as glucosamine, the home should check with the GP or pharmacist that there is no interaction with prescribed medicines.Make sure the residents, their relatives and the GP know the policy of the home.
What should be contained in the homely remedies policy?
Homely remedies must be purchased. Residents’ prescribed medicines should never be used as homely remedies. The following should be detailed in the policy: Which medicines are kept, it is good practice to
agree the list with the GP(s) providing medical cover for the home although the home cannot demand that the GP signs the policy.
The indications for offering the medicines e.g. indigestion, mild pain, cough, constipation, diarrhoea are appropriate for treatment with homely remedies.
The dose to give and how often it may be repeated before referring to the resident’s GP.
Maximum daily dose for each medicine. How to establish that the remedies do not interact
with prescribed medicines How to obtain the resident’s consent to treatment
the doctor has not prescribed Records of purchase, administration and disposal.Homely remedies should only be administered by trained nurses or care workers who have undergone accredited training.Homely remedies should be stored separately from the prescribed medication.
How should homely remedies be recorded?
A clear audit trail of homely remedies should be maintained, usually in a separate book with a running total.The administration of homely remedies must be documented preferably on the MAR chart.
Medication Policy Template 50

19. Administration of warfarin
Aim: To ensure the safe administration of warfarin so that potential harm to residents is reduced, blood clotting times are monitored regularly, residents always receive the correct dose of warfarin at the correct time and there are good auditable processes in place to monitor systemsLegislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Patients Safety Alert 18: Actions that can make anticoagulant therapy safer, National Patient Safety Agency (NPSA) March 2007British National Formulary (BNF) 61 March 2011Information for patients attending the Anticoagulant Services provided by Queen Mary’s and Princess Royal Hospitals South London Healthcare NHS Trust ( see Appendix)Date written: August 2011Review date: August 2012Administration of warfarin
Advice For care home use
How does warfarin work and what is it used for?
Warfarin is an anticoagulant. It is used to prevent and treat the formation of harmful blood clots within the body by thinning the blood or dissolving the clots e.g. in deep vein thrombosis (blood clots in the veins of the legs) pulmonary embolism (blood clots in the lungs), atrial fibrillation (rapid heart beat), stroke, heart attack and in patients with mechanical prosthetic heart valves.
Does the home have a medication policy or written safe practice procedures for the administration of warfarin?
The NPSA recommend that local policies should include a specific section on anticoagulants. Care workers who administer warfarin or support people to take their own must be trained to undertake their duties safely.
What information is supplied to the patient when they commence warfarin therapy?
When warfarin treatment starts, the person must be given verbal and written information and this must be updated when necessary. In Bromley, this is in the form of a yellow A5 pack. It contains a credit card sized ‘Alert card’ which identifies that a patient
Medication Policy Template 51

is on anticoagulant therapy. This must be shown to any healthcare practitioner when the person attends for treatment.If a resident does not have a yellow pack or book, copies of the oral anticoagulation therapy patient information book (yellow book) can be obtained from the NPSA. www.nrls.npsa.nhs.uk/resources/?EntryId45=61777
What monitoring is required during warfarin treatment?
The person’s International Normalised Ratio (INR) should be monitored regularly. The INR measures how ‘thin’ the blood is. The anticoagulant clinic based at the Princess Royal University Hospital (PRUH) issues a letter stating the reason for anticoagulation, the date of the blood test, the INR, the dose of warfarin and the date of the next blood test. GPs and pharmacists should check that the person’s INR is being monitored regularly before they issue or dispense a repeat prescription. The repeat prescription should only be dispensed if the INR is at a safe level. The dispensing pharmacist may ask the home to fax over INR results. The dentist should be informed if a resident is taking warfarin. An extra blood test may be required prior to dental treatment. More frequent drug monitoring may be required if it is not possible to avoid drugs that interact with warfarin.
Which medicines and foods interact with warfarin?
Prescription medicines, over-the-counter (OTC) medicines, herbal medicines, vitamins and supplements, certain foods and alcohol may interact with warfarin. The effect of warfarin may be enhanced, increasing the risk of bleeding or reduced, increasing the risk of blood clots forming and thereby heart attacks and strokes.Medicines that interact with warfarin include antibiotics, non-steroidal anti-inflammatory agents (e.g. aspirin, ibuprofen, diclofenac, naproxen), antidepressants, stomach ulcer/acid-reducing drugs, lipid lowering agents and antifungals.Herbal medicines that interact with warfarin include gingseng and ginkgo biloba. Supplements include glucosamine and cod liver oil.Vitamin K reduces the effect of warfarin. Patients should avoid taking vitamin K supplements or large intakes of foods high in vitamin K e.g. liver,
Medication Policy Template 52

cranberry juice, broccoli, brussel sprouts and green leafy vegetables like cabbage and spinach.Refer to the BNF for a comprehensive list of medicines that interact with warfarin or check with the GP, pharmacist or anticoagulant clinic.
What are the side effects and problems associated with warfarin?
Warfarin has been frequently identified as causing preventable harm and admission to hospital. Contact the GP urgently if a resident experiences severe bruising, bleeding, blood in the urine or faeces, blackened stools, coughing up blood or blood in vomit, long nosebleeds (lasting more than 10 minutes), bleeding gums, unusual headaches or (in women) heavy or increased bleeding
during periods or any other bleeding from the vagina.
Other side-effects include diarrhoea, rash, hair loss and sickness.
What are the different strengths of warfarin and the colours of the tablets?
0.5mg (500mcg) – white1mg – brown3mg – blue5mg – pinkChanges to the dose of warfarin should be recorded in mg, not in the number of tablets.
How should warfarin be dispensed?
Warfarin should be dispensed in original packs. It should not be placed in MDS because they are not flexible to cope with frequent drug changes.
What time of day is warfarin usually taken?
Warfarin is usually taken in the evening at the same time of day. If the dose is missed in the evening, it can be taken on the same day up to midnight. The dose should be given at the normal time the next day and a record of the missed dose made. If an extra dose or the wrong dose is administered, contact the GP or anticoagulant clinic for advice.
How is the administration of warfarin recorded in the care home?
The latest letter from the anticoagulant clinic or a copy of this letter, should be kept with the current MAR chart and the MAR chart clearly marked to indicate the dosage of warfarin to be administered each day. Homes may draw up a separate chart to record the administration of warfarin.
How should dose changes of warfarin be confirmed?
All dose changes for warfarin should be confirmed in writing. Only accept a verbal message to change the dose in an emergency and always ask for written confirmation as soon as possible.
Medication Policy Template 53

What are the contact numbers and opening hours of the anticoagulant clinic at the Princess Royal University Hospital (PRUH)?
Monday to Friday9.00am to 4.00pmO1689 864263
Monday to Friday8.00am to 5.00pm (healthcare professionals only)01689 863833
Emergency only01689 863000 Bleep 310
Medication Policy Template 54

20. New admissions and returning from hospital stays
Aim: To ensure that the home has an accurate record of all medicines when a resident is admitted to the home from their own home, another care setting or hospital and that continuity of medicines supply is maintained and that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations March 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Date written: August 2011Review date: August 2012New admissions and returning from hospital stays
Advice For care home use
What is the procedure for checking the medicines of new admissions to the home?
Check the name, strength and quantity of medication against the MAR chart if received from another care home or care setting. Check that the medicines brought in by the resident are current. If there is any doubt, contact the GP before administration.Handwrite a new MAR chart recording the quantity, strength, form, dose, route of administration and date of receipt. Another authorised member of care staff or registered nurse should confirm the record and sign see Medicine administration records (MAR) charts.Do not administer any medicines that do not have an original pharmacy label e.g. those that have been packed by a family member or carer. Request a new prescription as soon as possible to prevent the resident running out of medication.Where a resident brings in over-the-counter (OTC) medicines or homely remedies, check with the GP and/or pharmacist that the medicines do not interact with prescribed medicines. Written authority from the GP to administer is advisable. Administration of patients’ own medication should be recorded on the patient’s MAR chart in the normal way.
Medication Policy Template 55

What is the procedure for checking medication after hospital discharge?
Check the medication received against the discharge letter and MAR chart supplied by the hospital. If there are any immediate concerns, contact the hospital ward for advice.Check the medication against the medicines that the resident had previously before hospital admission. Separate any medicines no longer required for safe disposal.Handwrite a new MAR chart recording the quantity, strength, form, dose, route of administration and date of receipt. Another authorised member of care staff or registered nurse should confirm the record and sign see.Request a new prescription as soon as possible to prevent the resident running out of medication
Medication Policy Template 56

21. Transfer of medicines to another care setting
Aim: To ensure the safe transfer of medicines when a resident moves to another care home or is admitted to hospital and that there are good auditable procedures in place to monitor systems Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010 Keeping patients safe when they transfer between care providers – getting the medicines right, Royal Pharmaceutical Society July 2011Date written: August 2011Review date: August 2012Transfer of medicines to another care setting
Advice For care home use
What is the recommended core content of records for medicines when patients transfer care providers?
It is recommended that the following details are supplied when a patient transfers care providers: Patient details – last name, first name, date
of birth, NHS number, patient address GP details – GP/Practice name Other relevant contacts e.g. community
pharmacist Allergies or adverse reactions to medicines –
causative medicine, brief description of reaction, probability of occurrence
Medications – medicine (generic and brand name where relevant), reason for medication (where known), form, dose strength, dose frequency/time, route
Medication changes – medication started, stopped or dosage changed and reason for change.
Medication recommendations e.g. requirements for adherence support such as compliance aids, prompts and packaging requirements. Any additional information about specific medicines such as brand name, special formulation
Medication Policy Template 57

Any additional information given to patient or authorised representative.
Person completing the transfer record – name, time, date, job title, contact telephone number for queries and signature (if paper based)
What is the procedure for the transfer of medicines where a resident moves to another care home?
A record with the details listed above should be supplied where known. Photocopy the latest MAR chart to show the list of current medicines for the resident and how often and when they are administered. Be sure to include any details of warfarin and insulin dosage and administration of when required medicines recorded on separate charts. Collect all the medicines that belong to the resident. They are the property of the resident, not the home.Make a list of the name, strength and quantity of all the medicines that are handed over. The member of staff handing over the medicines should sign to confirm what has been handed over and the person receiving the medicines should sign to confirm receipt.
What is the procedure for the transfer of medicines where a resident is admitted to hospital?
As above, but there is no need to send MDS blister packs or cassettes. The hospital will not use these for administration. Include all medicines not packed in MDS systems, topical medicines e.g. creams, ointments, eye drops etc and inhalers and any homely remedies that belong to the resident.
Medication Policy Template 58
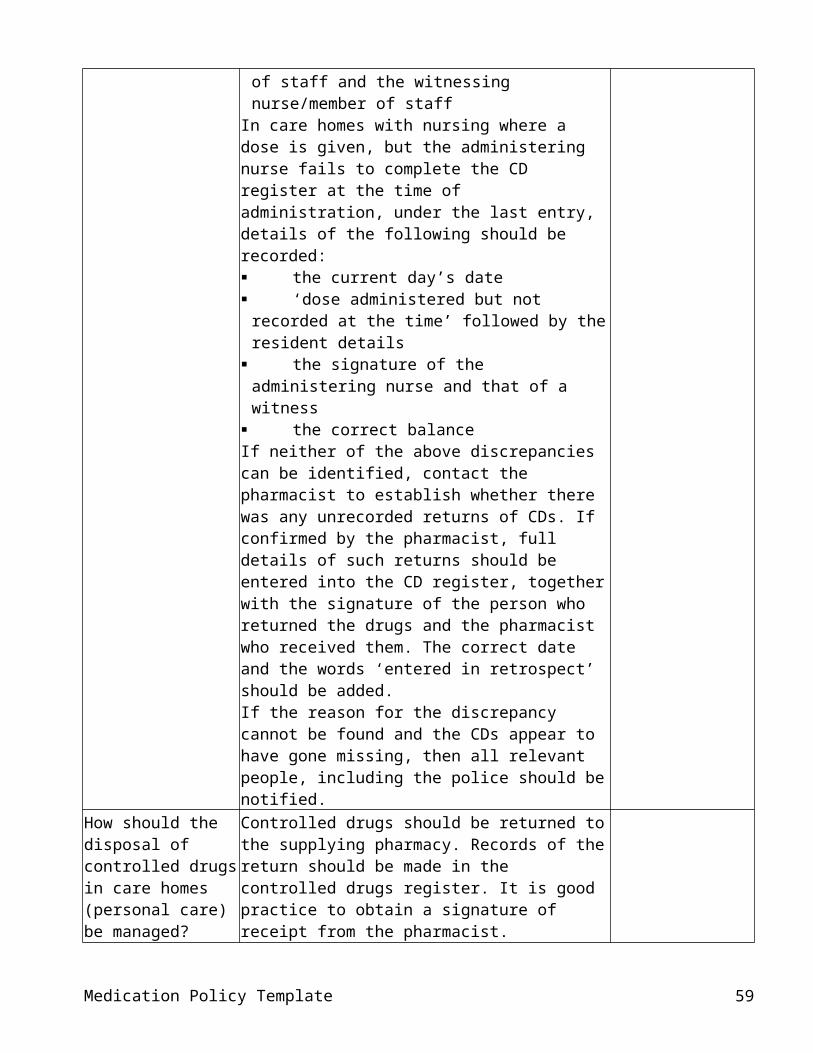
22. Leave medicines and secondary dispensing
Aim: To ensure that residents who leave the care home to attend day centres, visit family or friends or take a short holiday have a supply of the required medicines in suitable containers and that secondary dispensing is avoided and that there are good auditable procedures in place to monitor systems.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission. Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010 CQC Professional Advice: The administration of medicines in care homes June 2008Nursing and Midwifery Council (NMC) Medication Standards April 2010Date written: August 2011Review date: August 2012Leave medicines and secondary dispensing
Advice For care home use
What are the arrangements to ensure that residents always have the required medicines when they leave the care home for short periods e.g. to to go to day centres, visit family or friends or take a short holiday?
Where a resident takes leave from the care home, the home needs to do a risk assessment to ensure that the resident always has the required medicines. The home needs to consider whether the resident can self-medicate (see Self administration of medicines) or whether family, friends or carers can safely handle and administer medicines. Consider all the required medicines that may be needed including ‘when required’ medicines e.g. eye drops, creams.Where the leave is a regular or a planned arrangement e.g. a day centre, holiday or a visit to family or friends, the pharmacy should be asked in advance of preparing the monthly medication to pack up the medicines in separate labelled containers.If a resident regularly goes out for the day e.g. to attend a day centre, it may be possible for the GP to change the formulation of a medicine to a long-acting formulation or to alter the dosage time, so that medicines do not have to be given while the resident is away from the home. If these options are not possible, consider whether it
Medication Policy Template 59

is safe to hand over medicines packaged in MDS cassettes or blister packs and/or labelled medicines in their original packaging. Consider the consequence if a resident takes all their medicines when they leave the home and fails to return them when they come back.The amount of medication taken out of the home and received on return (if any) should be signed for and recorded. The MAR chart should reflect that a medication was not administered because the resident was on leave from the home. Some care homes provide MAR charts for use outside the home.
What is secondary dispensing?
Medicines should only be given from suitably labelled containers with full instructions supplied by the pharmacy. Repackaging medicines into another container with the intention that a different care worker will give the medicines to the resident at a later time is called ‘secondary dispensing’. This is unsafe practice and can lead to drug errors.Registered nurses may consider repackaging medicines into compliance aids under NMC guidance.
Medication Policy Template 60

23. Training staff to administer medicines
Aim: To ensure that care workers and registered nurses are appropriately trained to safely administer medicines and that competences and training requirements are reviewed regularly.Legislation & Guidance: The Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007Care Quality Commission (CQC). Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines March 2010Nursing and Midwifery Council (NMC) Medication Standards April 2010CQC Professional Advice: The administration of medicines in care homes June 2008CQC Professional Advice: Training care workers to safely administer medicines in care homes November 2008Date written: August 2011Review date: August 2012Training staff to administer medicines
Advice For care home use
What are the responsibilities and standards expected of registered nurses employed in care homes with nursing in the safe administration of medicines?
Care homes registered to provide nursing care employ registered nurses who are responsible for administering medicines to residents. They must act according to guidance published by the Nursing and Midwifery Council (NMC). Relevant NMC guidance includes: Guidelines for the administration of medicines Guidelines for professional practice including the
process for delegating nursing tasks to care workers.
What is the process where nurses delegate the administration of medicines to care workers?
Where the nurse delegates the application of external medicines e.g. creams or ointments when the resident is being washed or bathed to a carer, that person must be trained to use the medicines correctly and this should be recorded. The carer administering the medicines must sign the MAR chart, not the responsible nurse.It is not good practice for care workers to take medicines to residents when the nurse has prepared them.
What are the training Medicines should be administered by designated
Medication Policy Template 61

requirements for care staff administering medicines in care homes for personal care only?
and appropriately trained staff. The training must be accredited and include: Basic knowledge of how medicines are used and
how to recognise and deal with problems in use The principles behind all aspects of the home’s
policy on medicines handling and records Establishing from the care home records which
medicines are prescribed for a resident at a specific time in the day
Selecting the correct medicine from a labelled container including MDS systems.
How to give medicines by mouth e.g. tablets, capsules and liquids
Measuring a dose of liquid medicine Applying a cream/ointment; inserting drops to the
eyes, nose or ears; and administering inhaled medicines
Recording that a person has had the medicine or the reason for not administering it.
What to do if a service user refuses medicines What to do if an error occurs Who to inform if the service user becomes unwell
after taking medicines Specialist training on how to administer rectal or
vaginal medicines like suppositories, pessaries or rectal diazepam, insulin by injection, administration through a Percutaneous Endoscopic Gastrostomy (PEG) or oxygen* is not required unless these techniques are to be used. The specialist training must be undertaken with a qualified healthcare professional and the carer assessed as competent by this practitioner. The carer must also sign to say that they agree to accept the delegation however the carer can refuse to assist with any specialised techniques if they do not feel competent. NMC guidance is clear that the healthcare professional will retain responsibility for the delegated duty.
* Training is provided by the oxygen supplier Air Liquide as part of their contract with the PCT.
This training does not allow a carer to administer medicines until a formal assessment of competence to administer medicines has also been completed. A senior care worker should always mentor a care worker until he/she is both confident in giving
Medication Policy Template 62

medicines and competent to do so correctly.What are the arrangements for the administration of controlled drugs?
The administration of controlled drugs should be witnessed by designated and appropriately trained staff in care homes for personal care. This is also advisable in care homes with nursing. Controlled drugs for self-administration do not have to be witnessed. See Controlled Drugs.
Who is responsible for providing the necessary training for the safe administration of medicines in care homes?
The care provider is responsible for providing necessary training. The training outcomes should meet both the needs of the care workers and the needs of the residents, including cultural preferences. The care provider should: Identify what training needs the care worker has Put together a programme of training that will
meet the needs of the residents they care for and care workers
Provide a mentor for the care worker and keeps a record of that progress
Accreditation of training is variable. The care provider is responsible for ensuring that the trainer is knowledgeable in the subject and has relevant, current experience of handling medicines.
Is induction training provided to new employees in the care home?
Induction training should raise awareness of the management of medicines within the care home. It should identify what a care worker can do before they have completed training to administer medication, for example how to respond to a resident who requests paracetamol for a headache.
What resources are available to support medication training?
Skills for Care through their website www.skillsforcare.org.uk include information about induction training, Knowledge and Skills Set for Medication and regional sources to support learning.
What providers are available to deliver medication training?
Distance learning or computer based learning Bromley College of Further & Higher Education
Managing and safe handling of medicines level 2 certificat (ASET) www.bromley.ac.uk
Independent training organisations London Borough of Bromley Care Home Training
Consortium [email protected] Community pharmacists NHS Bromley medication review pharmacist.
[email protected] “In house” where the care home organisation has
a dedicated Training Division.Training from one source alone is unlikely to meet
Medication Policy Template 63

every learning outcome for care workers. Good training is likely to involve both external training organisations and an ’in house’ programme that supports it.
What is the process for assessing competence of care workers and nurses to administer medication?
Care workers on completion of training and nurses should be formally assessed to check competence to administer medicines.The care provider or manager should devise an assessment to include:Can the care worker/nurse confidently and correctly give medicines by:- Checking what the resident takes on both the
MAR chart and the medicine label Checking that it is for the right resident and any
special instructions that they may have as to how they take their medicines
Checking that the medication ‘use by’ date has not expired.
Asking whether the resident wants the medicine Making sure that no-one else has already given
the medicine Preparing the correct dose for the right time of day Selecting the right method/route of administration Gives the medicine to the resident and also offers
a drink of water What to do if a resident refuses to take their
medicine How to administer “as required” medicines like
pain killers and laxatives Signing and completing the MAR chart correctly. Records of all training and competence assessments should be recorded in the care worker’s training file.
How often should assessments for competence be carried out?
Currently, there is no guidance from CQC or The Royal Pharmaceutical Society. Annually seems reasonable or after an error has occurred.
Medication Policy Template 64

Glossary
Accountable Officer Person responsible for monitoring of the safe use and management of controlled drugs in an organisation
Alendronic acid Medicine used to prevent and treat osteoporosis (a bone disease which cause bones to become brittle and fragile and fracture more easily)
Britisn National Formulary (BNF) A reference book with a list of medicines and information about prescribing
Care Quality Commission (CQC) Health and social care regulator for EnglandCommunity pharmacist Pharmacist based in a (high street) community
pharmacyCommunity psychiatric nurse (CPN) Mental health nurse who visits patients in the
communityDesignated worker Someone appointed to do a specific task e.g.
administer medicinesEMdoc Out-of-hours GP service when the GP surgery is
closedEssential services Services offered by all community pharmacy
contractors as part of the NHS Community Pharmacy Contract
Gingko biloba Herbal medicine said to improve memoryGinseng Herbal medicine said to improve energy levelsGlucosamine Supplement for improving joint painGlyceryl trinitrate Medicine to relieve the pain of anginaHomely remedy Medicines for minor ailments that can be
brought over the counter such as paracetamol for headaches or indigestion remedies
Licensed medicine A medicine that has been licensed by the MHRA for specific conditions
Medicine administration record (MAR) A document on which details of all medicines given in a care setting are recorded, designed to show the dose given, the time when given and the identity of the person who gave it
MHRA Medicines and Healthcare products Regulatory Agency
Monitored Dosage System (MDS) Systems for packing medicines to make use easier e.g. by putting medicines for each time of day in separate blisters or compartments
Multidisciplinary Refers to a team of health and social care workers e.g. doctors, pharmacists, nurses, care managers with complimentary experience and
Medication Policy Template 65

skillsNICE National Institute for Healthcare and Clinical
ExcellenceNon-prescribed medicines Medicines such as homely remedies which are
available without a prescription NPSA National Patients Safety AgencyOstomy products Bags, pouches and products to manage
colostomy, ileostomy and urostomyOver-the counter (OTC) medicines Medicines which can be bought in pharmacies
without a prescription under the supervision of a pharmacist.
Parkinsons Disease A disease which affects the way the brain co-ordinates the movement of the muscles in various parts of the body
PEG (Percutaneous endoscopic gastrostomy) tube (PEG)
A flexible tube that goes through the abdominal wall directly into the stomach. Used for giving liquid food.
PRN Latin abbreviation meaning when requiredPrescriber Doctor, dentist or a nurse or pharmacist who has
undertaken additional training to enable him/her to prescribe medicines
Registered person Registered owner or manager of a care settingSalbutamol Medicine to relieve asthma or airways disease‘Special’ medicines Unlicensed medicines that have to be ordered in
specially by the pharmacy for individual patientsSteroid creams Used to reduce inflammation e.g. in eczema.
These steroids are not related to body-building drugs
Topical medicines Medicines applied directly to the part of the body where they are needed e.g. creams, ointments to the skin and ear, eye and nose drops
Unlicensed medicine A medicine that has not been licensed by the MHRA
Visiting Medical Officer (VMO) A GP contracted to look after the medical needs of residents in care homes and provide continuity of care.
Acknowledgements
Medication Policy Template 66
This medication policy template has been adapted from the medicines management policies used in care homes within NHS Nottingham City, with the kind permission of the Medicines Management Team NHS Nottingham City.
The author would like to thank the managers and senior nursing staff at Coloma Court Care Home and Ashcroft nursing homes for their support and feedback in the preparation of the template.
Medication Policy Template 67

References and further guidance
Care homes must have clear processes in place to take account of new guidance and alerts relating to the safe and secure handling of medicines.
British National Formulary (BNF) 61 March 2011http://bnf.org/bnf/index.htm
Care Quality Commissionhttp://www.cqc.org.uk/
CQC Guidance about compliance: essential standards of quality and safety Outcome 9: Management of medicines 2010 March 2010CQC Guidance about compliance Judgement Framework March 2010CQC Professional Advice: The administration of medicines in care homes June 2008CQC Professional Advice: Training care workers to safely administer medicines in care homes November 2008CQC Professional advice: Medicine administration records (MAR) in care homes and domiciliary care June 2008CQC Professional Advice: The safe management of controlled drugs in care homes November 2008
(The Professional Advice guidance is no longer available on the CQC website)
Central Alerting System (CAS)https://www.cas.dh.gov.uk/Home.aspx
Safety alerts are sent by email from the Department of Health’s CAS. They include emergency alerts, drug alerts, Dear Doctor letters and are issued on behalf of the MHRA, the NPSA and the Department of Health.Care homes should register their details with CAS either through the CQC or CAS websites.
Centre for Pharmacy Postgraduate Education (CPPE)
Supporting people in care homes, University of Manchester CPPE September 2011
Department of Health (DH)http://www.dh.gov.uk/en/index.htm
Safer management of controlled drugs: Guidance on strengthened governance arrangements London DH January 2007
Medication Policy Template 68

Safer management of controlled drugs: Guidance on standard operating procedures for controlled drugs London DH February 2007
Medicines and Healthcare products Regulatory Agencyhttp://www.mhra.gov.uk/index.htm
National Patients Safety Agency (NPSA)http://www.npsa.nhs.uk/
Patients Safety Alert 18: Actions that can make anticoagulant therapy safer NPSA March 2007
National Prescribing Centre (NPC)http://www.npc.co.uk/
A guide to good practice in the management of controlled drugs in primary care (England) Third edition NPC December 2009
National Institute for Health and Clinical Excellence (NICE)http://www.nice.org.uk/
NHS London, Eastern and South East Specialist Pharmacy Services
Storage, stability and in-use shelf life guidelines for non-sterile medicines NHS London, Eastern and South East Specialist Pharmacy Services March 2001 http://www.nhsppu.uea.ac.uk/assets/docs/qa/storage_stability_in_use_shelf_lives_of_non_sterile_medicines.pdf
Nursing and Midwifery Council (NMC)http://www.nmc-uk.org/
Nursing and Midwifery Council (NMC) Medication Standards April 2010
The Royal Pharmaceutical Societyhttp://www.rpharms.com/home/home.asp
The Handling of Medicines in Social Care, Royal Pharmaceutical Society of Great Britain Nov 2007http://www.rpharms.com/support-pdfs/handlingmedsocialcare.pdf
Principles of safe and appropriate production of medicine administration charts Royal Pharmaceutical Society of Great Britain February 2009Medicines, Ethics and Practice The professional guide for pharmacists Edition 35 July 2011Keeping patients safe when they transfer between care providers – getting the medicines right, Royal Pharmaceutical Society July 2011The safe and secure handling of medicines: a team approach Royal Pharmaceutical Society of Great Britain March 2007
Medication Policy Template 69

Skills for Care http://www.skillsforcare.org.uk
Social Care Institute for Excellence (SCIE)http://www.scie.org.uk/
Medication Policy Template 70

Appendix
1. Choosing medicines for patients unable to take solid oral dosage forms UKMi North West January 2010
2. Information for patients attending the Anticoagulant Services provided by Queen Mary’s and Princess Royal Hospitals
Medication Policy Template 71

Medication Policy Template 72

Choosing medicines for patients unable to take solid oral dosage formsSelecting suitable formulations for adult patients with swallowing difficulties or feeding tubes.
In most cases a licensed preparation will be
available that meets the patient’s needs.
STEP 1 Use a licensed medicine in a
suitable formulation.For example: Licensed liquid preparation Soluble tablets Powders or granules for suspension
In order to use a licensed medicine, consider switching to a different agent in the same class, or to a different route of administration.
For example, consider: Fluoxetine liquid (licensed preparation) as an
alternative to sertraline tablets. Aspirin dispersible tablets instead of
clopidogrel tablets. HRT patches instead of tablets.
CostSpecial-order medicines are often
considerably more expensive than licensed medicines. They may have short shelf-lives
compared with licensed alternatives and may need fridge storage.
For example, bendroflumethiazide liquid is 75 times more expensive than tablets: 28 doses of 2.5mg tablets costs 80p. 30 doses of 2.5mg/5ml liquid (150ml) costs
£60.
NB: Bendroflumethiazide tablets can be dispersed in water for administration orally or via feeding tubes.
STEP 2Use a licensed medicine in an unlicensed
manner, for example by crushing / dispersing tablets in water or by opening capsules.
For example: Ramipril capsules can be opened and the contents mixed with
water. Bendroflumethiazide tablets can be dispersed in water.Both the above examples are suitable for administration orally or via a feeding tube.
Not all medicines are suitable for administration in this way and it is important to check beforehand. See over for where to get advice.
As before, consider switching to a different agent or route of administration in order to use a licensed product.
STEP 3 In the few situations where there is no licensed option, consider using a ‘special’.
Special-order (‘special’) liquid medicines are unlicensed and expensive. They
should only be used if there is no licensed medicine that meets the
patient’s needs.
Consider the patient’s method of feeding:
Patients on liquid feeds may take oral liquid medicines, dispersible tablets or solid
preparations dispersed in water prior to administration. For patients on thickened fluids, liquid medicines can be mixed with products like
Thick and Easy.
Patients on soft-food diets may be able to swallow crushed tablets or the contents of
capsules given with food.
Patients with enteral feeding tubes may have oral medicines given by this route.
Licensed medicines should be used where possible. Special-order medicines are unlicensed and expensive and should only be used if there it no licensed alternative.
Care staff may only give licensed medicines in an
unlicensed way if there is a written direction in the patient’s
care plan.Practical directions are overleaf.
A stepwise approach is suggested:
Why licensed status mattersTo be granted a licence a medicine must meet quality standards
and be shown to be safe and effective. Licensed medicines usually come with a patient information leaflet and are considered the
safest choice.
Special-order medicines are unlicensed and are not required to meet the same standards as licensed medicines. Prescribers take
greater responsibility when using them.
Is it needed?If the patient is taking medicines that aren’t
needed or aren’t working, stop or change them.

Where can I get advice?For advice on choosing appropriate dosage forms or to check if tablets or capsules can be dispersed, crushed or opened, contact your PCT medicines management team or UKMi medicines information centre.
Medicines Management Dept NHS Bromley 020 8776 3669Contact details for UKMi medicines
information centres are available at www.ukmi.nhs.uk. Click on the map then search for your local or regional centre.
Medicines Q&A This leaflet accompanies a Medicines Q&A document which provides further information and lists options available in several therapeutic areas for adult patients with swallowing difficulties or feeding tubes. Access it online via the National electronic Library for Medicines, www.nelm.nhs.uk (see bottom of the page for the full link). Date of preparation: January 2010
Always check beforehand if a tablet is suitable for dispersing / crushing,
or a capsule suitable for opening.
Crushing / dispersing tabletsMany immediate-release tablets can be dispersed in water without crushing; some medicines need crushing first. Some tablets (e.g. modified release) are not suitable for crushing.
For medicines that are suitable for crushing, crush using a pestle and mortar, a tablet crusher or between two metal spoons.
Only crush medicines one tablet at a time; do not crush all the patient’s medicines together. Crushing or dispersal should only be performed immediately before administration.
Opening capsulesSome hard gelatin capsules can be opened and their contents mixed with water or administered with food. Some capsules are too small to manipulate. Capsules should only be opened immediately before administration.
Only prescribe special-order medicines if there is no suitable licensed medicine available that meets the patient’s needs.It may be appropriate to use a licensed
medicine in an unlicensed way.
Giving medicines in soft foodSome capsule contents or crushed tablets can be given with cold soft food such as a teaspoon of yoghurt or jam. Use a small amount of food to ensure the full dose is taken.
Crushed tablets or capsule contents may taste very bitter to patients taking them orally. Mask the taste by giving with strong flavours such as blackcurrant.
Medicines should only be administered in food with the patient’s knowledge and consent. Hiding medication in food is considered ‘covert administration’ and is only allowed in certain circumstances.
Administering medicines via feeding tubesFeeding tubes should be flushed with water before and after each medicine is administered. If a liquid medicine is thick or syrupy, dilution may be required. Some patients are fluid restricted; this needs to be taken into account.
When administering crushed tablets or opened capsules via a feeding tube, add the powder to 15-30ml water and mix well. Draw into a 50ml oral syringe and administer. If you have used a mortar or tablet crusher, rinse this with water and administer the rinsings also.
Suggested protocol for administering medicines via feeding tubes: 1. Stop the feed (leaving a feeding break if necessary).2. Flush the tube with 30ml water.3. Prepare the first medicine for administration, and give it.4. Flush with 10ml water.5. Repeat stages 3 and 4 with subsequent medicines.6. Flush with 30ml water.7. Re-start the feeding (leaving a feeding break if necessary).
Care staff may only administer medicines in an unlicensed manner on the instruction of the prescriber.
A written direction to crush or disperse tablets or to open capsules must be documented in the patient’s care plan.
References: UKMi. Medicines Q&A 294.1a: Therapeutic options for patients unable to take solid oral dosage forms. December 2009 (partial revision January 2010).
Available online at: www.nelm.nhs.uk/en/NeLM-Area/Evidence/Medicines-Q--A/Therapeutic-options-for-patients-unable-to-take-solid-oral-dosage-forms/ White R and Bradnam V. Handbook of drug administration via enteral feeding tubes. London: RPS Publishing; 2007. Smyth J. The NEWT Guidelines for administration of medication to patients with enteral feeding tubes or swallowing difficulties. Wrexham: North East Wales NHS Trust; 2006.
Choosing medicines for patients unable to take solid oral dosage forms
Practical directions

Information for patients attending the Anticoagulant
Services provided byQueen Mary’s and Princess
Royal Hospitals

Information for patientsAttending the Anticoagulant
Services provided byQueen Mary’s and Princess
Royal Hospitals

Information for patients attending theAnticoagulant service.
Blood tests can be taken at:-
Beckenham Beacon
Orpington Hospital
Princess Royal University Hospital
Queen Mary’s Hospital
Erith Hospital
Blood samples for warfarin testing will be taken during the stated times only.
Monday 08.30am – 11.00amTuesday 08.30am – 11.00amWednesday 08.30am – 11.00amThursday 08.30am – 11.00am
Please note Erith Hospital is 09.30am prompt.
If you attend outside these times you will be asked to return to the next available blood testing session.
Contact details for the clinic
01689-864263
Monday – Friday 9.00am – 4pm
General Information
Your subsequent visits to the anticoagulant clinic will be via your nearest outpatient department. You have the choice of Beckenham, Orpington, Princess Royal, Queen Mary’s or Erith for your routine blood tests. The clinic has a central office at the Princess Royal for all queries.
You need to attend for your test between the hours of 08.30am – 11.00am on the date you have been given taking your dosing sheet with you. Patients attending after 11.00am will be asked to attend the following clinic day. Please note for Erith Hospital patients need to be there at 09.30am prompt.
Your dosing sheet and blood sample are sent to the Princess Royal for testing and for the dosing of warfarin. If we need to make urgent changes to your warfarin dose then we will contact you by 5pm on the day of the test. If you do not receive a phone call then please continue on the same warfarin dose until you hear otherwise. Your dosing sheet

will be posted back to you by first class post with your new results and a new appointment date. Please check you dose when it is returned to you as there may be a small dose change. Please allow up to 4 days for your results to be returned in the post. Please do not telephone the clinic for your results.
Please keep to the appointment date on your dosing sheet. If you cannot make the date that has been given to you then please attend the next available clinic day between the stated times. You do not need to contact the clinic to make this change.
If you require transport then this is booked on a standing order basis and will be automatically booked when your next appointment is issued. Please do not contact the clinic for each transport booking.
Warfarin is available on repeat prescription from your GP. Please ensure you have an adequate supply of all strengths at all times.
Warfarin treatment
How does warfarin work?
Warfarin “thins” your blood and prevents clots from getting any bigger or breaking loose and travelling in your blood stream to another part of your body. It also prevents new clots from forming. Warfarin does not disperse clots that are already clots. This occurs naturally and may take a few months. The treatment is safe as long as you have your blood tested at regular intervals and you take the dose as prescribed by the clinic.
How will my treatment be monitored?
Your treatment is monitored by measuring how “thin” your blood is. The measurement is called an INR which stands for International Normalised Ratio. It is a measurement of how long it takes your blood to clot compared to normal. Normal blood has an INR of 1.0. The higher the INR the thinner the blood and the longer it will take to clot. Each patient has a target INR depending on their condition. The dose of warfarin is adjusted either up or down to achieve that target INR.
How long will my treatment last?
This is determined by the consultant who puts you on warfarin. You will be reviewed by your consultant before your warfarin treatment is stopped. For most clots the average length of treatment is 3-6 months but for heart problems or other conditions the treatment maybe longer. It is quite safe to stay on warfarin long term as long as you follow the advice given to you by the clinic and take the dose as prescribed.
Taking warfarin
How do I make sure I am taking the right dose?

Warfarin tablets come in 4 strengths and colours so you can work out the dose by using colours or numbers. When we advise you of your warfarin dose we will advise you in both colours and numbers so that you can double check that you are taking the right amount.
You will be given a supply of warfarin tablets and they are available on repeat prescription from your GP when you need them. Always keep an adequate supply of tablets at home and always keep some 0.5mg/1mg for small dose changes.
Warfarin comes in tablets as follows:-
Strength Colour0.5mg White1mg Brown3mg Blue5mg Pink
Warfarin should be taken as directed by the clinic after 5pm and at the same time each night.
If you forget to take your warfarin dose then take your usual dose the next day.
DO NOT DOUBLE UP THE DOSE OR TAKE 2 DOSES IN ONE DAY.
Side effects and other medications
Side effects
While on warfarin you may notice that you bruise easily, bleed easily when you cut yourself or have bleeding gums when you brush your teeth. This is normal. If you can account for your bruising or bleeding then there is no need to seek advice.
If you have blood in your stools, urine or vomit, bruising that you cannot account for or a wound that doesn’t stop bleeding then please contact your GP or go to casualty if the problem is severe. Although these problems are rare they have the potential to be serious.
If you have a mild problem like a blood shot eye or bruising then go to your nearest outpatient department on a clinic day to get an INR done. Tell us on your dosing sheet what the problem is. If the problem occurs outside of clinic times but is not severe enough to go to casualty then go to see your GP.
IN THE EVENT OF SERIOUS BLEEDING ATTEND THE CASUALTY DEPARTMENT FOR URGENT TREATMENT.
A less observed side effect of warfarin is a skin rash that develops soon after starting warfarin treatment. If this occurs please contact your clinic.
Other medication
It is important that you continue to take all medications that have been prescribed for you by your GP or consultant. If you are given a new medication then please check with your GP/pharmacist whether it interferes with warfarin. If it does then you will need to attend for a blood test within 5-7 days of starting it. Please leave us a message on the dosing sheet telling us what medication you have started. You may also need to attend for a blood test if you stop a drug that interferes with warfarin, again your GP or pharmacist can advise you.
Avoid all aspirin based drugs including non-steroidal anti-inflammatory drugs like brufen. Paracetamol and codeine can be taken with warfarin for pain and fever. Please check with your pharmacist before purchasing over the counter medicines.
Lifestyle/surgery
Alcohol
Alcohol can be consumed while you are taking warfarin as long as you have no more than 2 units per day. This equals:-
1 pint of normal strength beer/cider 2 small glasses of wine 2 pub measures of spirit
Drinking over the recommended allowance may affect your warfarin and has the potential to be very dangerous.
Diet
There are no diet restrictions with warfarin as long as you eat a normal well balanced diet. Crash diets and binge eating should be avoided.
CRANBERRY JUICE SHOULD BE AVOIDED WHILE ON WARFARIN.
Herbal remedies/Vitamin supplements
Please avoid the use of herbal remedies and vitamin supplements while on warfarin as they can be dangerous. Please contact the clinic for advice if there is something you particularly wish to take.
Dentist/Surgery
You should inform your dentist that you are on warfarin so that extra caution can be taken during treatment. Warfarin does not normally need to be stopped for tooth extractions but an extra blood test may need to be taken so that the dentist has an up to date INR.
If you require surgery then please contact the clinic for advice giving them at least 7-14 days notice to adjust the warfarin if required.
Travel
Please ensure you have valid travel insurance for your holiday/trip and that it covers warfarin treatment. Inform the clinic of your holiday dates using your sheet when you go for a test.
Do not share medication.
Always ensure you have an adequate supply of warfarin.

Seek advice from your clinic, GP or casualty if the tablets are accidentally swallowed.
Dispose of unwanted medications safely.
Always take the dose recommended by your clinic and attend for blood tests at the stated intervals.
Ensure you inform the clinic of any medication changes.
Do not exceed the recommended alcohol limits.
Do not take herbal remedies of vitamin supplements.
Avoid cranberry juice.
Paracetamol and codeine are safe to be taken with warfarin.
Ask you pharmacist before purchasing over the counter medicines to ensure they are safe with warfarin.
Carry your alert card with you at all times.
Advise the clinic of surgery/dental extraction 7-14 days in advance.
THE CLINIC DOES NOT DEAL WITH OTHER MEDICAL PROBLEMS ONLY THOSE DIRECTLY RELATED TO YOUR WARFARIN TREATMENT.







![Untitled-1 [samaygroup.in]samaygroup.in/Userfiles/PdfFiles/636782751384411705.pdf · Rudraksh Resi. Aditya Resi. Poojan Resi. IOC. IOC Circle Hotel o Siddharth Tirupatl laza Tirupati](https://static.fdocuments.us/doc/165x107/5f9ebb498aca803cc45d12fd/untitled-1-rudraksh-resi-aditya-resi-poojan-resi-ioc-ioc-circle-hotel-o.jpg)









