
RESEARCH & SCIENCE - Armourbite · Compendium: A Supplement of ... Exercise and Sports Science, The...
34
RESEARCH & SCIENCE TABLE OF CONTENTS 1. The effects of mouthpiece use on gas exchange parameters during steady-state exercise in college-aged men and women The Journal of the American Dental Association 2. The effects of mouthpiece use on salivary cortisol levels during exercise The official Journal of the American College of Sports Medicine 3. The effects of mouthpiece use during endurance exercise on lactate and cortisol levels The official Journal of the American College of Sports Medicine 4. The effect of mouthpiece use on muscular endurance Southeast Chapter of the American College of Sports Medicine 5. MP use increases VO2, VCO2 and VO2/kg during steady state running Southeast Chapter of the American College of Sports Medicine 6. Effects of mouthpiece use on airways Openings Lactate Levels in Healthy College Males Compendium: A Supplement of Continuing Education in Dentistry 7. Effects of Mouth Piece Use on Auditory and Visual Reaction Time in College Males and Females Compendium: A Supplement of Continuing Education in Dentistry 8. The Role of Intraoral Protective Appliances in the Reduction of Mild Traumatic Brain Injury Compendium: A Supplement of Continuing Education in Dentistry 9. A Study on the Effectiveness of a Self-fit Mandibular Repositioning Appliance on Increasing Human Strength and Endurance Capabilities Knoxville, University of Tennessee 10. The Effects of ArmourBite® Mouthpiece Use on Baseball Pitching Velocity. Rod Dedeaux Research & Baseball Institute Other Research Accepted for Publication Accepted for publication in renowned medical journals (pending print) 1) The effects of mouthpiece use on cortisol levels during an intensive resistive bout of exercise
Transcript of RESEARCH & SCIENCE - Armourbite · Compendium: A Supplement of ... Exercise and Sports Science, The...
RESEARCH & SCIENCETABLE OF CONTENTS
1. The effects of mouthpiece use on gas exchange parameters during
steady-state exercise in college-aged men and women
The Journal of the American Dental Association
2. The effects of mouthpiece use on salivary cortisol levels during exercise
The official Journal of the American College of Sports Medicine
3. The effects of mouthpiece use during endurance exercise on lactate and cortisol levels
The official Journal of the American College of Sports Medicine
4. The effect of mouthpiece use on muscular endurance
Southeast Chapter of the American College of Sports Medicine
5. MP use increases VO2, VCO2 and VO2/kg during steady state running
Southeast Chapter of the American College of Sports Medicine
6. Effects of mouthpiece use on airways Openings Lactate Levels in Healthy College Males
Compendium: A Supplement of Continuing Education in Dentistry
7. Effects of Mouth Piece Use on Auditory and Visual Reaction Time in College Males and Females
Compendium: A Supplement of Continuing Education in Dentistry
8. The Role of Intraoral Protective Appliances in the Reduction of Mild Traumatic Brain Injury
Compendium: A Supplement of Continuing Education in Dentistry
9. A Study on the Effectiveness of a Self-fit Mandibular Repositioning Appliance on Increasing Human Strength and Endurance Capabilities
Knoxville, University of Tennessee
10. The Effects of ArmourBite® Mouthpiece Use on Baseball Pitching Velocity.
Rod Dedeaux Research & Baseball Institute
Other Research Accepted for PublicationAccepted for publication in renowned medical journals (pending print)
1) The effects of mouthpiece use on cortisol levels during an intensive resistive bout of exercise

2011;142;1041-1047J Am Dent Assoc Scheett and Erica J. McDivittDena P. Garner, Wesley D. Dudgeon, Timothy P.college-aged men and womenparameters during steady-state exercise in The effects of mouthpiece use on gas exchange
jada.ada.org ( this information is current as of September 1, 2011):The following resources related to this article are available online at
http://jada.ada.org/content/142/9/1041in the online version of this article at:
including high-resolution figures, can be foundUpdated information and services
http://jada.ada.org/content/142/9/1041/#BIBL, 11 of which can be accessed free:23 articlesThis article cites
http://www.ada.org/990.aspxthis article in whole or in part can be found at: of this article or about permission to reproducereprintsInformation about obtaining
© 2011 American Dental Association. The sponsor and its products are not endorsed by the ADA.
on September 1, 2011
jada.ada.orgD
ownloaded from

Research in the late 1970sand early 1980s indicatedthat mouthguards mayenhance performance during
strength and endurance exercise.1-3
However, the research findings weredifficult to interpret because of thesubjective methodology used.Garabee1 reported that enduranceathletes felt they recovered morequickly after endurance trainingand could run at a higher intensitywhen wearing a mouthpiece thanwhen not wearing a mouthpiece;however, he provided no physiolog-ical measures from the study.
Smith2,3 reported the results oftwo studies in which football playersincreased their muscular strengthwhen wearing a mouthguardadjusted kinesiologically versuswhen they wore an unadjustedmouthguard. The investigator meas-ured the participants’ strength byusing a stress gauge kinesiometer,which measures the amount of pres-sure resistance in kilograms of forceper unit of time.
The question remains whetherSmith informed the athletes beforethe study that their performancemight be affected positively bymouthpiece use during testing. IfDr. Garner is an associate professor, Department of Health, Exercise and Sports Science, The Citadel, 171 Moultrie St., Charleston, S.C. 29409, e-mail “[email protected]”. Address reprint requests to Dr. Garner.Dr. Dudgeon is an assistant professor, Department of Health, Exercise and Sports Science, The Citadel, Charleston, S.C.Dr. Scheett is an assistant professor, Department of Health and Human Performance, College of Charleston, Charleston, S.C.Ms. McDivitt is a research assistant, Department of Health, Exercise and Sports Science, The Citadel, Charleston, S.C.
The effects of mouthpiece use on gasexchange parameters during steady-stateexercise in college-aged men and womenDena P. Garner, PhD; Wesley D. Dudgeon, PhD; Timothy P. Scheett, PhD; Erica J. McDivitt, MS
AB ST RACTBackground. The authors conducted a study to assess theeffects of custom-fitted mouthpieces on gas exchange parameters,including voluntary oxygen consumption (VO2), voluntary oxygenconsumption per kilogram of body weight (VO2/kg) and voluntarycarbon dioxide production (VCO2).Methods. Sixteen physically fit college students aged 18 through21 years performed two 10-minute treadmill runs (6.5 miles perhour, 0 percent grade) for each of three treatment conditions(mouthpiece, no mouthpiece and nose breathing). The authorsassigned the conditions randomly for each participant and for eachsession. They assessed gas exchange parameters by using a meta-bolic measurement system.Results. The authors used analysis of variance to compare allvariables. They set the significance level at ! = .05 and used aTukey post hoc analysis of treatment means to identify differencesbetween groups. The results showed significant improvements (P < .05) in VO2, VO2/kg and VCO2 in the mouthpiece condition.Conclusions. The study findings show that use of a custom-fitted mouthpiece resulted in improved specific gas exchangeparameters. The authors are pursuing further studies to explainthe mechanisms involved in the improved endurance performanceexhibited with mouthpiece use.Clinical Implications. Dental care professionals have an obli-gation to understand the increasing research evidence in support ofmouthpiece use during exercise and athletic activity and to educatetheir patients. Key Words. Mouthpiece; mouthguard; gas exchange; exercise;voluntary oxygen consumption; carbon dioxide.JADA 2011;142(9):1041-1047.
JADA 142(9) http://jada.ada.org September 2011 1041
R E S E A R C H
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

1042 JADA 142(9) http://jada.ada.org September 2011
players assumed that their performance wouldimprove, the psychosomatic effect may havecaused the reported improvements in muscularstrength.
In an effort to measure breathing outcomeswith a mouthguard, Francis and Brasher4 con-ducted a study composed of 10 participants toassess the physiological effects of mouthguarduse during five minutes of low-intensity andhigh-intensity exercise on a cycle ergometer.They found that during the higher-intensityexercise, those wearing a mouthguard exhibitedimprovement in expiratory volume, with signifi-cant decreases in ventilation (Ve).
Expanding on the work of Francis andBrasher,4 Garner and McDivitt5 conducted astudy to determine the effects of mouthpiece useduring endurance exercise. In their study, 24participants ran at 75 to 85 percent of maximalheart rate (HR) for 30 minutes on two occasions.The investigators assigned mouthpiece use ran-domly to enable them to determine the effects ofmouthpiece use on lactate levels before, duringand immediately after the protocol. Outcomesfrom this study demonstrated that mouthpieceuse had a positive effect on blood lactate levels,which were significantly lower (22.7 percent) at30 minutes (4.01 millimoles per liter withmouthpiece use versus 4.92 mmol/L with nomouthpiece use).5
This finding was confirmed in another studyby Garner and McDivitt,6 the results of whichshowed that lactate levels were 18.1 percentlower after a 30-minute run in the mouthpiececondition versus that in the no-mouthpiece con-dition (4.41 mmol/L versus 5.21 mmol/L, respec-tively). The study results also showed thatmouthpiece use had a significant effect onairway area in 10 participants, as measured bycomputed axial tomography. Specifically, bothwidth and diameter measurements were 9 per-cent greater in participants who wore a mouth-piece, with the difference in width measurementbeing statistically significant.6
Because we discovered both anatomical andphysiological changes associated with mouth-piece use during exercise, our goal was to eluci-date specific mechanisms involved with this phe-nomenon. Consequently, we conducted aninvestigation to examine possible gas exchangedifferences associated with wearing a mouth-piece during steady-state exercise. If partici-pants experienced an improvement in enduranceoutcomes (that is, lowered lactate levels), as pre-vious research findings indicate, then there mayhave been some association with improvedoxygen/carbon dioxide exchange during steady-
state exercise. The novel aspect of our researchwas the use of a custom-fitted, unobtrusivemouthpiece rather than the bulky mouthguardused in the study by Francis and Brasher.4
Therefore, the purpose of this study was toassess the effects of a custom-fitted mandibularmouthpiece on gas exchange parameters inhealthy, college-aged participants.
PARTICIPANTS AND METHODSWe recruited 16 participants (13 men and threewomen) aged 18 through 21 years (mean ±standard deviation [SD] age, 21.2 ± 0.75 years)for this study. Participants’ mean (± SD) heightand body mass were 176.37 ± 7.3 centimetersand 75.20 ± 12.96 kilograms, respectively. Themen were physically active and had participatedin university-mandated physical exercise, whichconsisted of a minimum of two cardiovascularand two resistance exercise sessions per week.The three women were college athletes, of whomtwo were on the track and field team and onewas on the soccer team. All participantsreported that they had refrained from physicalexercise the day of testing and were free ofinjury or illness.
The institutional review board of The Citadel,Charleston, S.C., approved the study. All partici-pants provided oral and written consent beforeparticipating in the study; we asked themwhether they understood all of the study’smethods and procedures; and we informed themof their right to drop out of the study at any time.
Dental impressions. Before testing, a den-tist made impression molds of each participant’slower teeth. We then sent the molds to the BiteTech laboratory (Danica Beach, Fla.) for fabrica-tion of custom-fitted mandibular mouthpieces(Under Armour Performance Mouthpiece,Under Armour, Baltimore, in cooperation withBite Tech, Minneapolis) (Figure 1).
Treadmill runs. Participants performed two10-minute treadmill runs for each of the threetreatment conditions assessed in this study:mouthpiece, no mouthpiece and nose breathing.We assigned the conditions randomly for eachparticipant and for each session. We tested eachcondition on a separate day; thus, participantswere required to come to the human perform-ance laboratory on three occasions. For both ofthe 10-minute runs on each day of testing, we
R E S E A R C H
ABBREVIATION KEY. HR: Heart rate. RR: Respira-tory rate. VCO2: Voluntary carbon dioxide produc-tion. Ve: Ventilation. VO2: Voluntary oxygen con-sumption. VO2/kg: Voluntary oxygen consumptionper kilogram of body weight. Vt: Tidal volume.
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

JADA 142(9) http://jada.ada.org September 2011 1043
asked participants to run at 6.5 miles per hourwith 0 percent grade so that we could analyzerespiratory gas levels during steady-state exer-cise. Before the first run on each test day, par-ticipants warmed up by running on the tread-mill for five minutes at 5.0 mph and 0 percentgrade. They then immediately began a 10-minute run at 6.5 mph and 0 percent grade.Afterward, the participants cooled down withthree minutes of walking at 3.0 mph and sevenminutes of seated rest.
The second trial of each day was the same asthe first trial, minus the five-minute warm-up.We scheduled conditions two to three days apartduring which participants were allowed to par-ticipate in their normal physical fitness routine,but we did not allow them to exercise on the dayof testing.
One of us (E.J.M.) attached a face mask to eachparticipant for each condition and adjusted ituntil she detected no air leaks. We used a meta-bolic cart (ParvoMedics, Sandy, Utah) to measurevoluntary oxygen consumption (VO2), voluntaryoxygen consumption per kilogram of body mass(VO2/kg) and voluntary carbon dioxide production(VCO2). VO2 is defined as the amount of oxygen inliters that the body uses per minute during aer-obic exercise.7 VO2/kg is the amount of oxygen inmilliliters that a person consumes per minute rel-ative to body mass. VCO2 is the expired byproductof metabolism that occurs during aerobic exerciseand is measured in liters per minute. In additionto VO2, VO2/kg and VCO2, we measured partici-pants’ respiratory rate (RR) (number of breathsper minute), tidal volume (Vt) (amount of airinspired and expired per breath), Ve (total volumeof inspired and expired air per minute) and HRby using the metabolic cart.
We measured these parameters every five sec-onds and averaged the measurements for eachminute of the 10-minute run for all three condi-tions. On all test days, we calibrated the meta-bolic cart according to the manufacturer’s speci-fications. For the mouthpiece condition (group1), we asked participants to bite down on thecustom-fitted mouthpiece and breathe throughtheir mouths while their noses were clampedwith a metal clamp attached to the face mask.For the no-mouthpiece condition (group 2), weasked participants to breathe through their openmouths while their noses were clamped. For thenose-breathing condition (group 3), we tapedparticipants’ mouths shut, which forced them tobreathe through their noses.
Statistical analysis. One of us (T.P.S.)entered all data into a spreadsheet (Excel,Microsoft, Redmond, Wash.) for data manage-
ment and exported the data (SigmaStat 3.5,Systat, Point Richmond, Calif.) for statisticalanalysis. For each of the three conditions, wegrouped and averaged measurements for bothtrials for each participant to yield mean values,which we used for the statistical analysis. Weused analysis of variance (ANOVA) to comparevariables (HR, RR, Vt, Ve, VCO2, VO2 andVO2/kg). We set the significance level at ! = .05and used a Tukey post hoc analysis of treatmentmeans to identify differences between groups.For nonparametric data, we performed aKruskal-Wallis ANOVA on ranks and used theDunn method for post hoc analysis. All valuesare expressed as mean ± SD. We did not performany ancillary analyses.
RESULTSData from two of the 16 participants wereincomplete; thus, results for this study arebased on data from 14 participants. As shown inFigures 2 through 4, VO2, VO2/kg and VCO2
were statistically significantly (P < .05) higherin participants in group 1 than in participantsin groups 2 and 3 during the 10-minute trial,and they were higher in participants in group 2than in participants in group 3. The resultswere similar for minutes 1 through 5 (Table 1,page 1045). During minutes 6 through 10, VCO2, VO2 and VO2/kg were significantly (P < .05) higher in participants in group 1 thanin participants in groups 2 and 3 (Table 2, page1045). The results showed no differences (P > .05) in Ve, RR or Vt between groups 1 and 2; however, as expected, the results for groups 1 and 2 were statistically significantly different (P < .05) from those for group 3 during the entire
R E S E A R C H
Figure 1. Custom-fitted mandibular mouthpiece (Under ArmourPerformance Mouthpiece, Under Armour, Baltimore, in coopera-tion with Bite Tech, Minneapolis) worn by college-aged partici-pants in the study. Image reproduced with permission of UnderArmour.
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

1044 JADA 142(9) http://jada.ada.org September 2011
10-minute test (Table 3, page 1046), during min-utes 1 through 5 (Table 1) and during minutes 6through 10 (Table 2). Finally, we found no differ-ences in HR at any time points between allthree conditions (Tables 1 through 3).
DISCUSSION Athletes and others have worn mouthpiecesduring sports as protective devices against dentalinjuries and concussions. The American DentalAssociation’s Council on Access, Prevention andInterprofessional Relations and Council on Scien-tific Affairs8 concluded that mouthguards providea protective effect against hard-tissue or soft-tissue damage in the mouth (such as tooth frac-tures, lip lacerations and mandibular damage).However, increased use of mouthpieces for per-formance enhancement is a recent trend in sportand exercise. In a study of mouthpiece useduring endurance exercise, Garner and McDi-vitt5,6 reported lower lactate levels in participantswho wore a mouthpiece compared with levels inthose who did not wear a mouthpiece. Thus, thepurpose of this study was to explain the lowerlactate levels observed with mouthpiece useduring exercise by elucidating the oxygen/carbondioxide differences with mouthpiece use.Increases in VCO2 would suggest an improvedability to buffer the hydrogen ion associated withlactate, thereby lowering hydrogen in the bloodand subsequent lactate levels.
Respiratory gas exchange. To elucidatethe potential mechanisms involved with mouth-piece use during exercise, we assessed the pat-terns of respiratory gas exchange in a mouth-piece condition, a no-mouthpiece condition and anose-breathing condition. Previous researchersin the area of airway dynamics have reporteddifferences between nasal and mouth breathingduring various intensities of exercise.9-12 Specifi-cally, these authors found better gas exchangewith mouth breathing than with nasalbreathing. Consequently, we expected to findlower Vt, VO2, VO2/kg, VCO2 and RR with nasalbreathing because these results have beenreported in previous research.9-12
However, we observed a novel finding whencomparing mouth breathing with no mouthpieceuse to mouth breathing with mouthpiece use.We had hypothesized that mouth breathing inthe no-mouthpiece condition would elicit out-comes similar to those in the mouth-breathing-with-mouthpiece condition; however, this wasnot the case. Specifically, the results showed sig-nificant improvements in VCO2 and oxygenparameters and no significant differences in Vewhen participants wore the mouthpiece versus
R E S E A R C H
Figure 4. Voluntary carbon dioxide production during steady-state exercise. Asterisk indicates statistically significant difference(P < .05) from group 3. Dagger indicates statistically significantdifference (P < .05) from group 1.
Figure 2. Voluntary oxygen consumption during steady-stateexercise. Asterisk indicates statistically significant difference (P <.05) from group 3. Dagger indicates statistically significant differ-ence (P < .05) from group 1.
*
*†
†
2.6
2.4
2.2
2.0
1.8
1.6
1.4
1.2
1.01 (Mouthpiece)
GROUP
VO
LU
NTA
RY
OX
YG
EN
CO
NSU
MP
TIO
N(L
ITER
S/M
INU
TE)
2 (No Mouthpiece) 3 (Nose Breathing)
Figure 3. Voluntary oxygen consumption per kilogram of bodyweight during steady-state exercise. Asterisk indicates statisticallysignificant difference (P < .05) from group 3. Dagger indicates sta-tistically significant difference (P < .05) from group 1.
*
†
†
35
30
25
20
15
10
5
01 (Mouthpiece) 2 (No Mouthpiece) 3 (Nose Breathing)
GROUP
VO
LU
NTA
RY
OX
YG
EN
CO
NSU
MP
TIO
N(M
ILLIL
ITER
S/K
ILO
GR
AM
/MIN
UT
E)
*
*†
†
2.4
2.2
2.0
1.8
1.6
1.4
1.2
1.01 (Mouthpiece)
GROUP
VO
LU
NTA
RY
CA
RB
ON
DIO
XID
E P
RO
DU
CT
ION
(LIT
ER
S/M
INU
TE)
2 (No Mouthpiece) 3 (Nose Breathing)
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from
JADA 142(9) http://jada.ada.org September 2011 1045
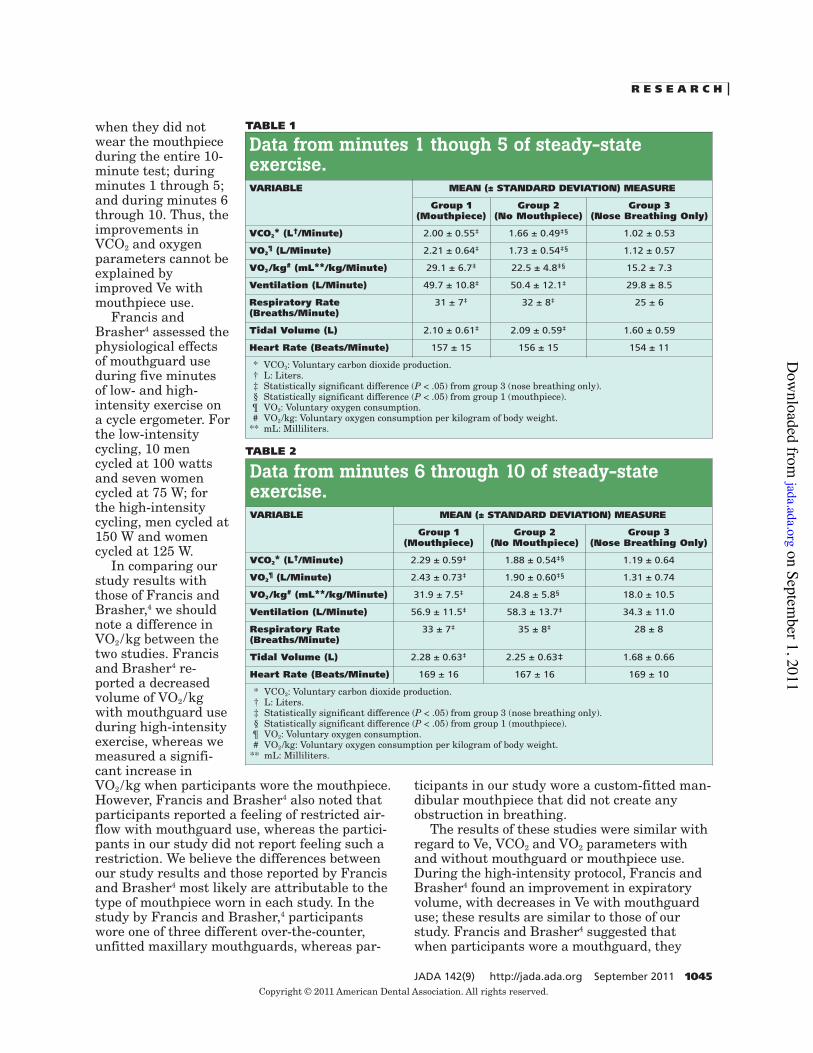
when they did notwear the mouthpieceduring the entire 10-minute test; duringminutes 1 through 5;and during minutes 6through 10. Thus, theimprovements inVCO2 and oxygenparameters cannot beexplained byimproved Ve withmouthpiece use.
Francis andBrasher4 assessed thephysiological effectsof mouthguard useduring five minutesof low- and high-intensity exercise ona cycle ergometer. Forthe low-intensitycycling, 10 mencycled at 100 wattsand seven womencycled at 75 W; forthe high-intensitycycling, men cycled at150 W and womencycled at 125 W.
In comparing ourstudy results withthose of Francis andBrasher,4 we shouldnote a difference inVO2/kg between thetwo studies. Francisand Brasher4 re -ported a decreasedvolume of VO2/kgwith mouthguard useduring high-intensityexercise, whereas wemeasured a signifi-cant increase inVO2/kg when participants wore the mouthpiece.However, Francis and Brasher4 also noted thatparticipants reported a feeling of restricted air-flow with mouthguard use, whereas the partici-pants in our study did not report feeling such arestriction. We believe the differences betweenour study results and those reported by Francisand Brasher4 most likely are attributable to thetype of mouthpiece worn in each study. In thestudy by Francis and Brasher,4 participantswore one of three different over-the-counter,unfitted maxillary mouthguards, whereas par-
ticipants in our study wore a custom-fitted man-dibular mouthpiece that did not create anyobstruction in breathing.
The results of these studies were similar withregard to Ve, VCO2 and VO2 parameters withand without mouthguard or mouthpiece use.During the high-intensity protocol, Francis andBrasher4 found an improvement in expiratoryvolume, with decreases in Ve with mouthguarduse; these results are similar to those of ourstudy. Francis and Brasher4 suggested thatwhen participants wore a mouthguard, they
R E S E A R C H
Data from minutes 1 though 5 of steady-stateexercise.VARIABLE MEAN (± STANDARD DEVIATION) MEASURE
Group 1(Mouthpiece)
Group 2(No Mouthpiece)
Group 3(Nose Breathing Only)
VCO2* (L†/Minute) 2.00 ± 0.55‡ 1.66 ± 0.49‡§ 1.02 ± 0.53
VO2¶ (L/Minute) 2.21 ± 0.64‡ 1.73 ± 0.54‡§ 1.12 ± 0.57
VO2/kg# (mL**/kg/Minute) 29.1 ± 6.7‡ 22.5 ± 4.8‡§ 15.2 ± 7.3
Ventilation (L/Minute) 49.7 ± 10.8‡ 50.4 ± 12.1‡ 29.8 ± 8.5
Respiratory Rate(Breaths/Minute)
31 ± 7‡ 32 ± 8‡ 25 ± 6
Tidal Volume (L) 2.10 ± 0.61‡ 2.09 ± 0.59‡ 1.60 ± 0.59
Heart Rate (Beats/Minute) 157 ± 15 156 ± 15 154 ± 11
* VCO2: Voluntary carbon dioxide production.† L: Liters.‡ Statistically significant difference (P < .05) from group 3 (nose breathing only).§ Statistically significant difference (P < .05) from group 1 (mouthpiece).¶ VO2: Voluntary oxygen consumption.# VO2/kg: Voluntary oxygen consumption per kilogram of body weight.
** mL: Milliliters.
TABLE 1
TABLE 2
Data from minutes 6 through 10 of steady-stateexercise.VARIABLE MEAN (± STANDARD DEVIATION) MEASURE
Group 1(Mouthpiece)
Group 2(No Mouthpiece)
Group 3(Nose Breathing Only)
VCO2* (L†/Minute) 2.29 ± 0.59‡ 1.88 ± 0.54‡§ 1.19 ± 0.64
VO2¶ (L/Minute) 2.43 ± 0.73‡ 1.90 ± 0.60‡§ 1.31 ± 0.74
VO2/kg# (mL**/kg/Minute) 31.9 ± 7.5‡ 24.8 ± 5.8§ 18.0 ± 10.5
Ventilation (L/Minute) 56.9 ± 11.5‡ 58.3 ± 13.7‡ 34.3 ± 11.0
Respiratory Rate(Breaths/Minute)
33 ± 7‡ 35 ± 8‡ 28 ± 8
Tidal Volume (L) 2.28 ± 0.63‡ 2.25 ± 0.63‡ 1.68 ± 0.66
Heart Rate (Beats/Minute) 169 ± 16 167 ± 16 169 ± 10
* VCO2: Voluntary carbon dioxide production.† L: Liters.‡ Statistically significant difference (P < .05) from group 3 (nose breathing only).§ Statistically significant difference (P < .05) from group 1 (mouthpiece).¶ VO2: Voluntary oxygen consumption.# VO2/kg: Voluntary oxygen consumption per kilogram of body weight.
** mL: Milliliters.
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

1046 JADA 142(9) http://jada.ada.org September 2011
might have been using a type of breathing called“pursed lip breathing,” which they defined aspursing one’s lips and breathing out deeply. Thistype of breathing has been linked to improvedrespiratory measures such as reduced breathingrates and increased Vt in people with respiratorydisorders, but it has not been studied exten-sively in a healthy population.13-15
We propose that a similar, but more plau-sible, mechanism may have occurred when par-ticipants wore the custom-fitted mandibularmouthpiece. We asked participants to bite downon the mouthpiece, which has two wedges (oneon either side of the mouthpiece) that create anopening between the maxillary and mandibularteeth (Figure 1). In addition, according to theproduct description,16 this mouthpiece shifts themandible down and into a more forward posi-tion, which Garner and McDivitt6 reportedresulted in increased airway openings.
Genioglossus muscle. We also propose acontribution from a neuromuscular responsethat occurs when participants bite down on themouthpiece and breathe through the mouth.What might have occurred, and which some par-ticipants reported anecdotally, is that when aparticipant bit down on the mouthpiece andbreathed during steady-state exercise, thetongue moved forward, resulting in a contrac-tion of the genioglossus muscle. The results ofextensive research regarding the genioglossusmuscle show that contraction of this muscleleads to relaxation of the pharyngeal airway,thereby improving airway dynamics.17-22
Remmers23 reported that the genioglossusmay be associated with a reflex that leads to thedilation of the pharyngeal area, thereby aidingin respiration in both humans and animals. Pre-liminary research in our laboratory has showndifferences in electromyographic activity of thegenioglossus when one wears a mouthpiece and
breathes through themouth versus whenone does not wear amouthpiece andbreathes through themouth. Thus, theimproved airwaydynamics we found inour study may beexplained in part byanatomical and neu-romuscular changesthat occur duringexercise with custom-fitted mouthpiece useas the mouthpiece
affects the genioglossus.Cortisol and epinephrine. We also reported
that the use of a custom-fitted mandibularmouthpiece is associated with a decrease in thestress hormone cortisol after high-intensity exer-cise.24 This finding is consistent with the findingsof Hori and colleagues,25 who reported a decreasein corticotrophin-releasing factor levels (stress-induced response of the hypothalamic-pituitary-adrenal axis and a precursor to corticosteronerelease, the rat equivalent to cortisol in humans)in rats that were allowed to bite down on awooden stick while experiencing a stressor. Ifbiting down on the mouthpiece results in adecrease in cortisol levels, it stands to reasonthat it also would affect other stress-related hor-mones, namely epinephrine. Epinephrine isreleased quickly in response to a stressor, andone of its many functions is to stimulate the gly-colytic process (that is, breaking down of glucoseto provide energy) to increase the rate of energyproduction. Two of the key byproducts of glycol-ysis are lactate and CO2. We have shown that useof the custom-fitted mouthpiece decreases lactateproduction and increases VCO2 production. Wenow believe that a decrease in epinephrinerelease may be the reason for these observedchanges; however, more research is needed.
Thus, if an anatomical and neuromuscularimprovement in airway dynamics occurs alongwith a diminished stress response (that is, lowercortisol and epinephrine levels) with mouthpieceuse during steady-state exercise, this couldexplain the improved oxygen and carbon dioxidekinetics, as well as the improvements in lactateproduction, that the results of our study show.
CONCLUSIONThe results of this study show improved airwaydynamics in participants who wore a custom-fitted mandibular mouthpiece during steady-
R E S E A R C H
TABLE 3
Data from minutes 1 through 10 of steady-stateexercise.VARIABLE MEAN (± STANDARD DEVIATION) MEASURE
Group 1(Mouthpiece)
Group 2(No Mouthpiece)
Group 3(Nose Breathing Only)
Ventilation (L*/Minute) 53.4 ± 11.0† 54.6 ± 12.8† 32.3 ± 9.9
Respiratory Rate(Breaths/Minute)
32 ± 7† 34 ± 8†‡ 26 ± 7
Tidal Volume (L) 2.16 ± 0.62† 2.14 ± 0.61† Not applicable
Heart Rate (Beats/Minute) 163 ± 15 162 ± 16 161 ± 11
* L: Liters.† Statistically significant difference (P < .05) from group 3 (nose breathing only).‡ Statistically significant difference (P < .05) from group 1 (mouthpiece).
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

JADA 142(9) http://jada.ada.org September 2011 1047
state exercise. The improvements in gasexchange and Ve observed with mouthpiece usemay explain the physiological outcomes ofimproved lactate levels during endurance run-ning, as reported previously.5,6 Specifically,improved VCO2 exhalation, as observed withmouthpiece use throughout the 10-minutetreadmill protocol, leads to improved bufferingof hydrogen ion levels, which, in turn, decreaseslactate levels during endurance exercise. Thisexplanation is consistent with the differences inVCO2 observed in this study (21.0 percenthigher with mouthpiece use than withoutmouthpiece use), as well as with differences inlactate levels observed in a previous study (22.7percent lower with mouthpiece use than thatwithout mouthpiece use).5
In addition, the improvement in oxygenkinetics during the beginning of the exercise pro-tocol (that is, minutes 1 through 5), as demon-strated by the significantly higher VO2 andVO2/kg levels in participants in group 1 (themouthpiece condition), also may affect initialoxygen deficit (defined as the amount of oxygenneeded for exercise and actual oxygen consump-tion26). At the beginning of exercise, there is a lagof approximately one to two minutes duringwhich oxygen is transported to the skeletal mus-cles. Therefore, one theory of how the mouth-piece may affect lactate levels is by decreasingthe time for oxygen to reach the muscle beingexercised, thereby decreasing fatigue duringendurance exercise.27 Further research is neededto fully elucidate the physiological mechanismsinvolved in improved performance when onewears a custom-fitted mouthpiece. !
Disclosure. Dr. Garner and Ms. McDivitt received honoraria fromBite Tech, Minneapolis.
The authors thank Michael Engel, DDS (Charleston, S.C.), formaking the models of the mouthpiece and Bite Tech Laboratories(Dania Beach, Fla.) for supplying the custom-fitted mouthpieces toeach participant.
1. Garabee WF Jr. Craniomandibular orthopedics and athletic per-formance in the long distance runner: a three year study. Basal Facts1981;4(3):77-81.
2. Smith SD. Muscular strength correlated to jaw posture and thetemporomandibular joint. N Y State Dent J 1978;44(7):278-285.
3. Smith SD. Adjusting mouthguards kinesiologically in profes-sional football players. N Y State Dent J 1982;48(5):298-301.
4. Francis KT, Brasher J. Physiological effects of wearing mouth-
guards. Br J Sports Med 1991;25(4):227-231.5. Garner DP, McDivitt EJ. The effects of mouthpiece use during
endurance exercise on lactate and cortisol levels. Med Sci SportsExerc 2009;41(5):S448
6. Garner DP, McDivitt E. Effects of mouthpiece use on airwayopenings and lactate levels in healthy college males. CompendContin Educ Dent 2009;30(special no. 2):9-13.
7. Beam WC, Adams GM. Exercise Physiology Laboratory Manual.6th ed. New York City: McGraw Hill; 2011.
8. ADA Council on Access, Prevention and Interprofessional Rela-tions; ADA Council on Scientific Affairs. Using mouthguards toreduce the incidence and severity of sports-related oral injuries.JADA 2006;137(12):1712-1720.
9. Camner P, Bakke B. Nose or mouth breathing? Environ Res1980;21(2):394-398.
10. Chinevere TD, Faria EW, Faria IE. Nasal splinting effects onbreathing patterns and cardiorespiratory responses. J Sports Sci1999;17(6):443-447.
11. Fregosi RF, Lansing RW. Neural drive to neural dilator mus-cles: influence of exercise intensity and oronasal flow partitioning. J Appl Physiol 1995;79(4):1330-1337.
12. Saibene F, Mognoni P, Lafortuna CL, Mostardi R. Oronasalbreathing during exercise. Pflugers Arch 1978;378(1):65-69.
13. Dechman G, Wilson CR. Evidence of underlying breathingretraining in people with sta ble chronic obstructive pulmonary dis-ease. Phys Ther 2004;84(12):1189-1197.
14. Faager G, Stâhle A, Larsen FF. Influence of spontaneouspursed lips breathing on walking endurance and oxygen saturationin patients with moderate to severe chronic obstructive pulmonarydisease. Clin Rehabil 2008;22(8):675-683.
15. Tiep BL. Pursed lips breathing: easing does it. J CardiopulmRehabil Prev 2007;27(4):245-246.
16. Under Armour. Armourbite technology. “www.underarmour.com/shop/us/en/accessories”. Accessed Aug. 8, 2011.
17. Bailey EF, Huang YH, Fregosi RF. Anatomic consequences ofintrinsic tongue muscle activation. J Appl Physiol 2006;101(5):1377-1385.
18. Cheng S, Butler JE, Gandevia SC, Bilston LE. Movement of thetongue during normal breathing in awake healthy humans. J Physiol2008;586(part 17):4283-4294.
19. Fogel RB, Trinder J, Malhotra A, et al. Within-breath control ofgenioglossal muscle activation in humans: effect of sleep-wake state.J Physiol 2003;550(part 3):899-910.
20. Mann EA, Burnett T, Cornell S, Ludlow CL. The effect of neu-romuscular stimulation of the genioglossus on the hypopharyngealairway. Laryngoscope 2002;112(2):351-356.
21. Sokoloff AJ. Activity of tongue muscles during respiration: ittakes a village? J Appl Physiol 2004;96(2):438-439.
22. Blumen MB, Perez de La Sota A, Quera-Salva MA, Frachet B,Chabolle F, Lofaso F. Genioglossal electromyogram during main-tained contraction in normal humans. Eur J Appl Physiol 2002;88(1-2):170-177.
23. Remmers JE. Wagging the tongue and guarding the airway:reflex control of the genioglossus. Am J Respir Crit Care Med 2001;164(11):2013-2014.
24. Garner DP, Dudgeon WD, McDivitt E. The effects of mouth-piece use on cortisol levels during an intense bout of resistance exer-cise. J Strength Cond Res. In press.
25. Hori N, Yuyama N, Tamura K. Biting suppresses stress-induced expression of corticotropin-releasing factor (CRF) in the rathypothalamus. J Dent Res 2004;83(2):124-128.
26. Wilmore JK, Costill DL, Kenney WL. Physiology of Sport andExercise. 4th ed. Champaign, Ill.: Human Kinetics; 2007.
27. Kilding AE, Winter EM, Fysh M. Moderate-domain pulmonaryoxygen uptake kinetics and endurance running performance. J Sports Sci 2006;24(9):1013-1022.
R E S E A R C H
Copyright © 2011 American Dental Association. All rights reserved.
on September 1, 2011
jada.ada.orgD
ownloaded from

!

!"#$%#&'()*)'"$+',-(./.00&'1)''234456)''78%'%99%-0:';9'<;=08>.%-%'=:%';$':"?./"#@'-;#0.:;?'?%/%?:'+=#.$A'%B%#-.:%)''!"#$%$&"'(&#')%$"&%"'$&')*+,-.'(&#'/0",%$."1'232C6D'EFG5''H.<.0%+'+"0"':=AA%:0:'<;=08>.%-%:'<"@'%$8"$-%'>%#9;#<"$-%)''!"#"I%%'2JK5J6'-.0%+'08"0'#=$$%#:'L8;'L;#%'"'<;=08>.%-%'#%>;#0%+'08"0'08%@'L%#%':0#;$A%#&'?%::'>#;$%'0;'.$M=#@'"$+'-;=?+'#%-;/%#'N=.-O?@'"90%#'"'#=$$.$A':%::.;$)''P#"$-.:'"$+'Q":8%#'2JKKJ6'9;=$+'08"0'=:%';9'"'<;=08>.%-%'L8.?%'%B%#-.:.$A'-;=?+'.$-#%":%'/%$0.?"0.;$&'"$+'08%#%I@'.<>#;/%'>%#9;#<"$-%)''*#%/.;=:'#%:%"#-8'.$';=#'?"I;#"0;#@'8":':=AA%:0%+'08"0'"'<;=08>.%-%'+"<>%$:'%B-%::./%'-;#0.:;?'+=#.$A'%B%#-.:%)''78.:'9.$+.$A'.:':.<.?"#'0;'L8"0'R;#.&'S=@"<"'"$+'7"<=#"'2344F6'9;=$+'.$'-;#0.;-;0#;>8.$T#%?%":.$A'8;#<;$%'L8%$'#%:0#".$%+'#"0:'L%#%'"??;L%+'0;'I.0%';$'"':0.-O)'''!"#$"%&'('7;'.$/%:0.A"0%'08%'>;::.I?%'-;##%?"0.;$'I%0L%%$'-;#0.:;?'?%/%?:'L8%$'L%"#.$A'"$+'$;0'L%"#.$A'"'<;=08>.%-%&'08%'L1+A%'2Q.0%T7%-8'U;#>6&'+=#.$A'0L;':%>"#"0%'%B%#-.:%'>#;0;-;?:)'''!)'*+%,&(''E=IM%-0:&'"A%'J5T3F'@%"#:';?+&'L%#%'":O%+'0;'-;<>?%0%'08%':"<%'%B%#-.:%'>#;0;-;?';$'0L;':%>"#"0%';--":.;$:&'JT3'+"@:'">"#0&'L.08'0%:0.$A'0"O.$A'>?"-%'"0'">>#;B.<"0%?@'08%':"<%'0.<%'%"-8'+"@)''E=IM%-0:'L;#%'"'<;=08>.%-%'+=#.$A'J'0%:0.$A'>#;-%+=#%'"$+'#%>%"0%+'08%':"<%'0%:0.$A'>#;-%+=#%';$'"$;08%#'+"@'L.08;=0'08%'=:%';9'08%'<;=08>.%-%)''E=IM%-0:'>#;/.+%+'"'>"::./%'+#;;?':"<>?%'I%9;#%'"$+'"90%#'%"-8'%B%#-.:%'I;=0'.$';#+%#'0;'0%:0':"?./"#@'-;#0.:;?'?%/%?:)''7L%$0@';$%'2$V3J6':=IM%-0:'L%#%'":O%+'0;'-;<>?%0%'"$'%B%#-.:%'>#;0;-;?';$'"':0"0.;$"#@'I.O%'%#A;<%0%#'9;#'J4'<.$=0%:'"0'5CWTK4W'8%"#0'#"0%'<"B.<=<)'X'C'<.$=0%'L"#<'=>'L":'=:%+'0;'#%"-8'K4W'8%"#0'#"0%'<"B.<=<)''78%'O.?;>;$+'?%/%?'=:%+'0;'"-8.%/%'08.:'L":'#%-;#+%+'"$+'=:%+'9;#'08%':%-;$+'0#."?)'''!$'&#-*&(''78%'=:%';9'08%'<;=08>.%-%'%?.-.0%+'?;L%#'-;#0.:;?'?%/%?:'9;#'JJ';9'08%'3J':=IM%-0:'L.08'08%'#%<".$.$A':=IM%-0:':%%.$A'$;'+.99%#%$-%'.$'-;#0.:;?'?%/%?:'L.08'=:%';9'08%'<;=08>.%-%)'''Y$'#%A"#+:'0;';/%#"??'<%"$'-;#0.:;?'?%/%?:'08%#%'L":'$;':.A$.9.-"$0'+.99%#%$-%'>;:0'%B%#-.:%'I%0L%%$'L%"#.$A'"$+'$;0'L%"#.$A'08%'<;=08>.%-%)'''!.%/.-#&0%/(''*;::.I?@'+=%'0;':<"??'$=<I%#:'.$'08.:':0=+@&'L%':"L'$;';/%#"??':.A$.9.-"$0'+.99%#%$-%:'.$'-;#0.:;?'?%/%?:'L.08'=:%';9'08%'<;=08>.%-%)''R;L%/%#&'08%'9"-0'08"0';/%#'8"?9';9'08%':=IM%-0:':"L'"'?;L%#.$A'%99%-0';9'-;#0.:;?'L.08'=:%';9'08%'<;=08>.%-%'L"##"$0:'<;#%'#%:%"#-8'0;'+%0%#<.$%'.9'"'<;=08>.%-%'8":'"$@'>8@:.;?;A.-"?'%99%-0:';$'-;#0.:;?'?%/%?:'+=#.$A'%B%#-.:%)'''

!

The Effects Of Mouthpiece Use During Endurance Exercise On Lactate And Cortisol Levels: 2416: Board #61 May 29 9:00 AM - 10:30 AM
Garne, Dena P.; McDivitt, Erica
Medicine & Science in Sports & Exercise . 41(5) Supplement 1:339, May 2009.
doi: 10.1249/01.MSS.0000355581.74244.c0
Author Information
The Citadel, Charleston, SC.
(No relationships reported)
Protective mouthpieces have been used in a variety of sports to decrease the risk of orofacial injury. However, there is limited research on the physiological effects of mouthpiece use during exercise.
PURPOSE: To investigate the possible effect on lactate and cortisol levels when wearing and not wearing a mouthpiece, the wEdge (Bite-Tech Corp).
METHODS: Subjects (n=24), age 18-24, ran at 75 -85% of their maximal heart rate for 30 minutes on 2 separate trials, being randomly assigned the use of the mouthpiece on 1 of the 2 trials. Lactate levels were assessed before, 15 and 30 minutes during, and post 10 minutes exercise. Subjects provided a passive drool sample before and after each exercise bout to assess salivary cortisol levels.
RESULTS: Lactate data indicated a significant difference between wearing and not wearing the mouthpiece at 30 minutes exercise (p-value = 0.024). Mean lactate levels at 30 minutes with the mouthpiece was 4.01 mmol/L versus 4.92 mmol/L without the mouthpiece. Mean cortisol levels showed no significant difference between wearing and not wearing the mouthpiece (p-value= 0.111). However, there was a trend towards lower mean cortisol levels with use of the mouthpiece (0.1484 ug/dL) versus no mouthpiece (0.2201 ug/dL).
CONCLUSION: This study suggests that use of a mouthpiece may reduce lactate and cortisol increases and thereby improve exercise performance.
©2009The American College of Sports Medicine!


!"#$%&&#'($)&$*)+(",-#'#$./#$)0$*+/'+123$%04+320'#$
5)6#07$897$:2&&#;7$<97$=230#((7$:97$=3##0#7$=97$*'>2#7$:97$*)3-07$!97$?)1207$597$<"#21;7$!9$204$=230#37$@9$$$
@#,(9$)&$A#21("7$%B#3'-/#$204$<,)3($<'-#0'#7$!"#$:-(24#17$:"231#/()07$<:$CDEFD$
$
!"#3#$"2G#$H##0$I20;$/(+4-#/$)0$")6$()$-I,3)G#$I+/'+123$/(3#0J("$4+3-0J$#B#3'-/#9$$<)I#$3#/#23'"$/+JJ#/(/$("2($("#$+/#$)&$2$I)+(",-#'#$6-11$-0'3#2/#$I+/'+123$/(3#0J("$204$#04+320'#$K81#B204#37$LDDD$204$<I-("7$LDMCN9$$$
!"#$%&'O$!)$(#/($-&$("#$-0&1+#0'#$)&$6#23-0J$2$I)+(",-#'#$'20$-I,3)G#$I+/'+123$#04+320'#9$$$$$$$$$$$$
(')*%+&,$P23(-'-,20(/$())Q$,23($-0$2$C$42;$#B,#3-I#0(9$$R0$("#$&-3/($42;7$,23(-'-,20(/$,#3&)3I#4$("#-3$I2B-I+I$2I)+0($)&$3#,#(-(-)0/$2($STU$)&$("#-3$L$3#,#(-(-)0$I2B-I+I$)&$("#$,3#2'"#3$'+31$#B#3'-/#$204$H#0'"$,3#//$6-(")+($2$I)+(",-#'#9$$R0$42;$C7$,23(-'-,20(/$,#3&)3I#4$("#$/2I#$#B#3'-/#$6-("$2$I)+(",-#'#$K!"#$%4J#7$5-(#$!#'"$:)3,9N9$$!"-/$I)+(",-#'#$62/$/,#'-&-'211;$&-((#4$()$#2'"$/+HV#'($6-("$2$H)-1$204$H-(#$(#'"0-W+#9$$$
-'&".)&,$!"#$+/#$)&$("#$5-(#X!#'"$I)+(",-#'#$/-J0-&-'20(1;$-0'3#2/#4$I+/'+123$#04+320'#$-0$H)("$I21#/$204$&#I21#/9$!"#$3#/+1(/$6#3#$3+0$+/-0J$2$4#,#04#0($(X(#/($+/-0J$<P<<9$R+3$4#,#04#0($(X(#/($3#/+1(/$"24$2$,XG21+#$)&$9FY$&)3$H#0'"$,3#//$KLFU$-I,3)G#I#0(N$204$2$,XG21+#$)&$9FFE$&)3$,3#2'"#3$'+31$KLSU$-I,3)G#I#0(N9$$
/%01."&2%0,3!"#$3#/+1(/$)&$("-/$/(+4;$/")6$("2($("#$+/#$)&$2$I)+(",-#'#$-I,3)G#/$)0#Z/$I+/'+123$#04+320'#7$/,#'-&-'211;$-0$("#$H#0'"$,3#//$204$("#$,3#2'"#3$'+31$#B#3'-/#/9$$$$$
$
5)6#07$897$:2&&#;7$:97$=230#((7$:97$=3##0#7$=97$*'>2#7$:97$*)3-07$!97$?)1207$597$<"#21;7$!97$204$=230#37$@9P9$$K[#H3+23;7$CFFDN9$$!"#$#&&#'($)&$I)+(",-#'#$+/#$)0$I+/'+123$#04+320'#9$$P3#/#0(#4$2($("#$CFFD$<)+("#2/($>#J-)021$:"2,(#3$)&$8I#3-'20$:)11#J#$)&$<,)3(/$*#4-'-0#$K5-3I-0J"2I7$8\N9$$$
$
$


!"#$%&'()(*#+(*',)-(.+(+*',*/"01*/)"0*.,2*/"0345*2#-',5*+$(.26*+$.$(*-#,,',5***!"#"$%&'()'*+$,"#"$-./))001+$2"!"$!345)6(*+$7"8"$9.!:;:00*+$&(4$9"<"$=64':53)>*"$$?*@!)A0$6B$C)&D0/+$
7E)'.:F)+$&(4$-A6'0$-.:)(.)+$,/)$G:0&4)D+$?1@$!)A0"$6B$C)&D0/$&(4$C3H&($#)'B6'H&(.)+$G/&'D)F06(+$-G$$
1IJKI*$
7H)'5:(5$')F)&'./$F355)F0F$0/&0$A)'B6'H&(.)$H630/A:).)F$H&L$M)()B:0$&0/D)0:.$A)'B6'H&(.)+$0/635/$0/)$
H)./&(:FH?F@$6B$&.0:6($&')$L)0$3(N(6O("$$$
$
&789:;<=*,/)$F034L$D66N)4$&0$0/)$)BB).0$6B$&$.3F06H$B:0$H630/A:).)$?9#@$6($5&F$)E./&(5)$43':(5$F0)&4L$F0&0)$
)E)'.:F)$:($*P$F3MQ).0F$O/6$.6HAD)0)4$0O6$*K$H:(30)$0':&DF$6($1$F)A&'&0)$4&LF"$$
$
!<>?:@;=*,/)$0')&4H:DD$FA))4$O&F$F)0$&0$R"K$HA/$O:0/$KS$)D);&0:6($&(4$5&F$)E./&(5)$A&'&H)0)'F$O)')$&(&DL>)4$
?#&';69)4:.F@$43':(5$)&./$0':&D"$$7&./$F3MQ).0$O&F$:(F0'3.0)4$06$M')&0/)$0/'635/$0/):'$H630/F$43':(5$)&./$
.6(4:0:6($?O:0/$&(4$O:0/630$0/)$9#@+$O:0/$0/)$9#$5'63A$M:0:(5$46O($&(4$M')&0/:(5$O/:D)$0/)$(6$9#$5'63A$
M')&0/)4$0/'635/$&($6A)($H630/"$$%&F$)E./&(5)$A&'&H)0)'F$O)')$H)&F3')4$O:0/$&$H&FN$0/&0$B:0$F(35DL$
6;)'$0/)$F3MQ).0TF$H630/$&(4$(&F&D$&')&+$O:0/$0/)$(6F)$M):(5$.D&HA)4$43':(5$&DD$0':&DF"$$
$
-<;7A>;=*,/)')$O&F$&$F:5(:B:.&(0$4:BB)')(.)$:($;6D3(0&'L$6EL5)($.6(F3HA0:6($A)'$N:D65'&H$6B$M64L$O):5/0$?UV1WN5@+$
.&'M6($4:6E:4)$?UGV1@+$&(4$6EL5)($?UV1@$:($&DD$.6(4:0:6(F$O:0/$0/)$9#$.6(4:0:6($)D:.:0:(5$/:5/)'$UV1WN5+$
UGV1$&(4$UV1$;)'F3F$(6$9#"$UV1WN5$O:0/$&$9#$O&F$P*"PX$HDWN5WH:($O/:D)$(6$9#$.6(4:0:6($O&F$1P"IY$
HDWN5WH:("$$UGV1$O:0/$0/)$9#$O&F$1"1P$DWH:($O/:D)$0/)$(6$9#$.6(4:0:6($O&F$*"ZX$DWH:("$$[:(&DDL+$UV1$O&F$
1"PZ$DWH:($O:0/$9#$&(4$*"ZJ$DWH:($O:0/$(6$9#"$$$
$
):BCA7;D:B=**,/)F)$')F3D0F$F/6O)4$:HA'6;)H)(0F$:($5&F$)E./&(5)$O:0/$0/)$9#$;)'F3F$(6$9#$&(4$F355)F0F$0/&0$9#$3F)$
43':(5$)(43'&(.)$)E)'.:F)$H&L$:HA'6;)$A)'B6'H&(.)$ML$:HA'6;)4$GV1$')H6;&D"$$$
$
-3AA6'0)4$ML$&$5'&(0$B'6H$\:0)$,)./$G6'A6'&0:6($
$
of Continuing Education in Dentistry ®
A Supplement to
July/August 2009 — Vol. 30 (Special Issue 2)
Published by AEGIS Publications, LLC © 2009

Compendium—Volume 30 (Special Issue 2) 9
Mouthpieces have been used for a variety of con-tact sports to prevent oral-facial injury.1 In areview of dental trauma literature, Glendor2
noted that participation in sports is the greatest cause ofdental injuries. To minimize injury associated with contactsport participation, the American Dental Association (ADA)recommends the use of mouthguards to protect againstdental trauma during contact sports.3 In addition to therecommendation of the ADA, such sport-governing bodiesas the National Alliance of Football Rules Committee havemandated mouthguards for use in high school football inthe United States.4 The 2008-2009 National Athletic As-sociation (NCAA) Sports Medicine Handbook mandatesmouthguards for athletes involved with football, field hock-ey, lacrosse, and ice hockey in order to minimize dentaltrauma during these sports.5
While there is compelling research to support the use ofmouthguards to protect against oral-facial injuries duringcontact sports, there is also research to suggest that mouth-pieces may enhance performance. Smith6,7 noted that pro-fessional football players exhibited greater arm strength withproperly fitted mouthguards that resulted in changes in bitepatterns. Smith also noted that those players with the mostextreme overbite corrected with a mouthguard experiencedthe greatest increase in strength. Specifically, he observedthat with a properly adjusted mouthguard, 66% of the play-ers exhibited significant strength improvements on the iso-metric deltoid press.7 He stated that the increase in strengthwith a properly fitted mouthguard was because of decreasedpressure in the temporomandibular joint (TMJ).
Not only has improvement in strength been noted, butGarabee8 described improvement in 7 runners’ endurance
1Assistant Professor, Department of Health, Exercise and Sport Science, The Citadel, Charleston, South Carolina2Research Assistant, Department of Health, Exercise and Sport Science, The Citadel, Charleston, South Carolina
Effects of Mouthpiece Use on Airway Openings and Lactate Levels
in Healthy College MalesDena P. Garner, PhD;1 and Erica McDivitt, MS2
Abstract: Research has described the use of mouthpieces not only in preventing oral-facial injuries, but linking use to
improvements in muscular strength and endurance. However, the mechanisms by which these improvements occur have
not been elucidated. The purpose of this study was to understand possible physiological explanations for improvements
in exercise performance with the use of a mouthpiece. Specifically, this study focused on differences in lactate levels after
30 minutes of endurance exercise with and without a mouthpiece. In addition, computed tomography (CT) scans were
taken of the cross-sectional area of the oropharynx in each participant (N = 10) with and without a mouthpiece. CT scans
showed a significant difference in mean width (28.27 mm with the mouthpiece vs 25.93 mm without the mouthpiece,
P = .029) and an increase in mean diameter with a mouthpiece (12.17 mm vs 11.21 mm, P = .096). Lactate levels were
lowered with the mouthpiece at 1.86 mmol/L vs 2.72 mmol/L without mouthpiece. This research suggests that there is
an improvement in endurance performance that may be linked to improved airway openings resulting from the use of a
mouthpiece. Future studies should continue to clarify the possible mechanisms for these exercise outcomes as well as to
understand the optimal mandibular advancement to elicit these exercise improvements.
RESEARCH UPDATE

10 Compendium—Volume 30 (Special Issue 2)
Research Update—Lactate Levels
and recovery with use of a mouthpiece to promote proper oc-clusion. He observed that when runners wore a wax bitemouthpiece, there was an increase in mileage: 64 to 100 milesper week in one runner, and 50 to 80-100 miles per week inanother. He also noted quicker recovery times and decreasedperceived exertion with use of the mouthpiece vs without themouthpiece. Garabee hypothesized that this improvementwas because of decreased stress with mouthpiece use thatreduced clenching and grinding of teeth during exercise.
As the research evolved, thepossible reasons for improvementsin performance were elucidatedby Francis and Brasher.9 In astudy of 10 men and 7 women,they found that wearing a mouth-piece during 20 minutes of highintensity cycling resulted in im-provements in ventilation (averageof 43.13 l/min with mouthpiecevs 50.98 l/min without mouth-piece). They noted that this im-provement may be from pursedlips breathing which results ingreater oxygen saturation. Ugaldeand colleagues10 confirmed thatpursed lips breathing resulted inincreased oxygen saturation inmyotonic muscular dystrophy patients, while Tiep11 statedthat such breathing results in increased tidal volume, car-bon dioxide removal, and oxygen saturation.
Drawing from the research by Frances and Brasher,9 thepossible reasons for improvements in endurance perform-ance while wearing a mouthpiece provide insight into thephysiological mechanisms that may be occurring. In orderto first understand if there were improvements in perform-ance, the authors’ laboratory conducted a series of pilotstudies primarily to determine if lactate levels were affect-ed by the use of a mouthpiece. If, as Frances and Brasher9
suggested, there was improvement in ventilation (ie, in-creased oxygen saturation and removal of carbon diox-ide), then there could consequently be an improvementin lactate levels. The authors found that with 24 partici-pants, there was improvement in lactate levels after 30 min-utes of running on a treadmill at 85% of maximal heart rate(4.01 mmol/L with mouthpiece vs 4.92 mmol/L withoutmouthpiece).12
With this data suggesting a physiological improvementwhen a mouthpiece is used, the next step was to clarify fur-ther the possible reasons for this improvement. Trenouthand Timms13 found a positive association between theorpharyngeal airway opening and mandibular length, witha narrower opening associated with a shorter mandibularlength. They cited previous research that suggested repo-sitioning the mandible in an anterior position, therebyopening airways and promoting respiratory gas exchange
to and from the lungs. In the litera-ture associated with sleep apnea(where airway openings are dimin-ished during sleep) and mouth-pieces, it can be noted that thereis significant improvement in air-way openings for patients wear-ing a mouthpiece (a device thatfits like a retainer and forces thelower teeth to relax in a forwardposition). Kyung and colleagues14
advanced the mandible forwardwith an oral appliance in 12sleep apnea patients and found areduction of the apnea-hypop-nea index from 44.9 (withoutappliance) to 10.9 (with appli-ance). Gale and colleagues15 also
found a significant improvement in mean airway openingwith an anterior mandibular device while patients weresupine in a conscious state. Specifically, Gale et al15 foundthat in 32 participants, the mean minimal pharyngeal cross-sectional area was increased 28 mm2 with the mouthpiecevs without the mouthpiece. Gao and collegues16 statedthat for their participants, the mandibular advancement was7.5% with a mouthpiece. They specifically found a signifi-cant opening of the oropharynx (P = .0258) and velo-pharynx areas (P = .006). Zhao et al17 also found that thevelopharynx opening increased significantly with an ad-justable mandibular custom mouthpiece, from 3.27 mm2
at 0 mm, to 8.45 mm2 at 2 mm, 17.73 mm2 at 4 mm,24.45 mm2 at 6 mm, and 35.82 mm2 at 8 mm. This re-search suggests that the positioning of the mouthpiece willimpact the degree of airway opening, with greater movementof mandible in a forward position resulting in a greater open-ing of the velopharynx. With the findings of previous stud-ies as well as those in the authors’ laboratory, the hypothesis
THIS PRESENT STUDY SUGGESTS
MECHANISMS BY WHICH
LACTATE PRODUCTION MAY
BE IMPROVED WITH INCREASED
AIRWAY OPENINGS, THEREBY
IMPROVING OXYGEN KINETICS
SUCH AS LOWERED OXYGEN
DEFICIT AND/OR IMPROVED
BREATHING WORK RATES.
Compendium—Volume 30 (Special Issue 2) 11
Garner and McDivitt
of this study is that there will be increased airway openingand a decrease in lactate levels with the use of a mouthpiece.
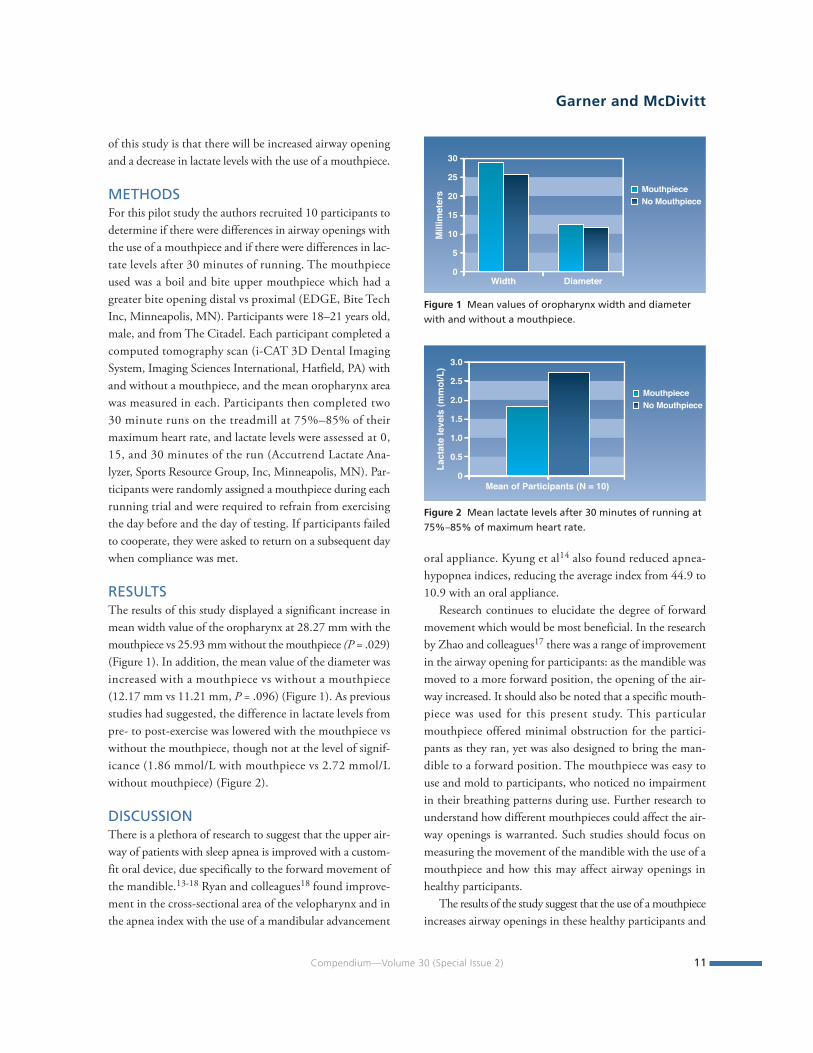
METHODSFor this pilot study the authors recruited 10 participants todetermine if there were differences in airway openings withthe use of a mouthpiece and if there were differences in lac-tate levels after 30 minutes of running. The mouthpieceused was a boil and bite upper mouthpiece which had agreater bite opening distal vs proximal (EDGE, Bite TechInc, Minneapolis, MN). Participants were 18–21 years old,male, and from The Citadel. Each participant completed acomputed tomography scan (i-CAT 3D Dental ImagingSystem, Imaging Sciences International, Hatfield, PA) withand without a mouthpiece, and the mean oropharynx areawas measured in each. Participants then completed two30 minute runs on the treadmill at 75%–85% of theirmaximum heart rate, and lactate levels were assessed at 0,15, and 30 minutes of the run (Accutrend Lactate Ana-lyzer, Sports Resource Group, Inc, Minneapolis, MN). Par-ticipants were randomly assigned a mouthpiece during eachrunning trial and were required to refrain from exercisingthe day before and the day of testing. If participants failedto cooperate, they were asked to return on a subsequent daywhen compliance was met.
RESULTSThe results of this study displayed a significant increase inmean width value of the oropharynx at 28.27 mm with themouthpiece vs 25.93 mm without the mouthpiece (P = .029)(Figure 1). In addition, the mean value of the diameter wasincreased with a mouthpiece vs without a mouthpiece(12.17 mm vs 11.21 mm, P = .096) (Figure 1). As previousstudies had suggested, the difference in lactate levels frompre- to post-exercise was lowered with the mouthpiece vswithout the mouthpiece, though not at the level of signif-icance (1.86 mmol/L with mouthpiece vs 2.72 mmol/Lwithout mouthpiece) (Figure 2).
DISCUSSIONThere is a plethora of research to suggest that the upper air-way of patients with sleep apnea is improved with a custom-fit oral device, due specifically to the forward movement ofthe mandible.13-18 Ryan and colleagues18 found improve-ment in the cross-sectional area of the velopharynx and inthe apnea index with the use of a mandibular advancement
oral appliance. Kyung et al14 also found reduced apnea-hypopnea indices, reducing the average index from 44.9 to10.9 with an oral appliance.
Research continues to elucidate the degree of forwardmovement which would be most beneficial. In the researchby Zhao and colleagues17 there was a range of improvementin the airway opening for participants: as the mandible wasmoved to a more forward position, the opening of the air-way increased. It should also be noted that a specific mouth-piece was used for this present study. This particularmouthpiece offered minimal obstruction for the partici-pants as they ran, yet was also designed to bring the man-dible to a forward position. The mouthpiece was easy touse and mold to participants, who noticed no impairmentin their breathing patterns during use. Further research tounderstand how different mouthpieces could affect the air-way openings is warranted. Such studies should focus onmeasuring the movement of the mandible with the use of amouthpiece and how this may affect airway openings inhealthy participants.
The results of the study suggest that the use of a mouthpieceincreases airway openings in these healthy participants and
Figure 2 Mean lactate levels after 30 minutes of running at75%–85% of maximum heart rate.
0
0.5
1.0
1.5
2.0
2.5
3.0
Lact
ate l
evels
(mm
ol/L
)
MouthpieceNo Mouthpiece
Mean of Participants (N = 10)
Figure 1 Mean values of oropharynx width and diameterwith and without a mouthpiece.
0
5
10
15
20
25
30
Millim
eter
s MouthpieceNo Mouthpiece
DiameterWidth

12 Compendium—Volume 30 (Special Issue 2)
Research Update—Lactate Levels
that the use of a mouthpiece while exercising may improvelactate levels. While previous studies with sleep apnea popu-lations indicated improvements in airway openings withthe use of a mouthpiece, there were limited data on ayounger, healthy population (age 21 +/- 1.1 years). Thisstudy, however, is similar in a study by Gao and col-leagues16 which took magnetic images of 14 healthy Japa-nese men (age 27.7 +/- 1.9 years). Gao et al16 saw improve-ments in airway opening with a custom-fit oral device thatwas specifically designed to move the mandible in a moreforward position. Their study found significant improve-ments in the velopharynx (P = .0006) and the oropharynx(P = .0258), while the current study noted a significant im-provement in the oropharynx width (P = .029).
Because of the financial costs of obtaining 2 CT scansfor each participant, this study was limited in the numberof participants. In addition, this was designed as a pilotstudy to determine: 1) if there were changes in airwayopenings with a mouthpiece in healthy participants; and2) if this could translate into lowered lactate levels. Theresults suggest there may be a link, which could be one pos-sible physiological explanation for performance improve-ment with a mouthpiece.
It may be surmised that the lack of significant differ-ences in lactate levels in this study may be because of thelow number of subjects, even though the trend was lowerlactate levels with the mouthpiece vs no mouthpiece. Asthe authors’ previous study suggested (N = 24), lactate lev-els were significantly lower with a mouthpiece vs without amouthpiece after 30 minutes of running on a treadmill(4.01 mmol/L mouthpiece vs 4.92 mmol/L no mouth-piece) (Figure 3).
Research has consistently noted the correlation betweenexercise fatigue and higher lactate levels. As one increases
exercise intensity, the glycolytic pathway is highly utilized tomeet energy needs. The end product of this pathway is theproduction of lactic acid. Lactic acid is broken down intolactate and hydrogen ions, and it is this increase of hydro-gen ions that is negatively associated with metabolic proc-esses, leading to fatigue.19-20 Thus, any mechanism whichelicits lowered hydrogen levels resulting from lactic acidshould increase an athlete’s time to fatigue. For example, ifthe pathways used during exercise rely more on oxygen,then lactate levels will be lowered. Yet understanding thislink between lowered lactate levels and increased airwayopenings is a complex issue needing further investigation.12
Previous studies have noted that an improvement inbreathing work rates leads to improved exercise time be-cause of reduced oxygen uptake and ventilation.21-22 Spe-cifically, if breathing mechanics are improved, then there isa decreased need for oxygen and blood flow by the respira-tory muscles which typically require approximately 10% ofthe oxygen needs during strenuous exercise. Less bloodflow to the respiratory muscles suggests an increase ofblood flow to the exercising skeletal muscles, which wouldprolong time to fatigue. Specifically, Harms and colleaguesfound that when respiratory muscle work was decreased(via a proportional-assist ventilator), time to exercise ex-haustion was increased in 76% of the trials by an averageof 1.3 minutes (+/-0.4 minutes).22
Improvement in respiratory muscle function may notbe the only mechanism that occurs during mouthpieceuse. An interesting study by Kilding and colleagues23 exam-ined response time of oxygen kinetics in endurance runners(N = 36) to understand its possible effect on a 5 kilometertime trial. An important finding from their study was thata faster phase II oxygen uptake kinetic response at the on-set of moderate intensity exercise resulted in faster 5 kilo-meter performance. Thus, they concluded that those runnerswho had a shorter oxygen deficit at the onset of exercise (asindicated by shortened phase II response) could increasetime to exhaustion, as indicated by the better 5 kilometerperformance. Kilding cited previous work by Casaburi andcolleagues24 stating a decrease in oxygen deficit at the onsetof exercise could result in decreased lactate production,which could potentially improve endurance performance.This present study suggests mechanisms by which lactateproduction may be improved with increased airway open-ings, thereby improving oxygen kinetics such as loweredoxygen deficit and/or improved breathing work rates.
Figure 3 Mean lactate levels after 30 minutes of running at85% of maximum heart rate.
0
1
2
3
4
5
6
Lact
ate l
evels
(mm
ol/L
)
MouthpieceNo Mouthpiece
Mean of Participants (N = 24)

CONCLUSIONThis study found that the use of a mouthpiece significant-ly improves airway openings in participants as comparedwith these same participants who do not wear the mouth-piece. In addition, lactate levels are improved when partici-pants wear the mouthpiece vs when they do not wear themouthpiece. One explanation for the decrease in lactatelevels may be an improvement in oxygen kinetics at theonset of exercise or improvement in breathing work rateswhich may be prompted by enhanced airway openings withthe use of a mouthpiece. Previous research in the field ofmouthpiece use and its effect on human performance sug-gests that mouthpieces improve performance. However,these studies have been unable to elucidate the possible phys-iological mechanisms for this improvement. This researchis novel in the area of human movement because it suggestsa possible physiological explanation for the improvement inperformance as noted by athletes. Further studies should focuson the reasons for these improvements, noting differences injaw morphology and airway dynamics for individuals whomay benefit from a mouthpiece during exercise and sport.
DISCLOSUREDr. Garner has received an honorarium from Bite Tech Inc.
REFERENCES1. Hughston JC. Prevention of dental injuries in sports. Am J Sports
Med. 1980;8(2):61-62. 2. Glendor U. Aetiology and risk factors related to traumatic den-
tal injuries—a review of the literature. Dent Traumatol. 2009;25(1):19-31.
3. ADA Council on Access, Prevention and Interprofessional Re-lations; and ADA Council on Scientific Affairs. Using mouth-guards to reduce the incidence and severity of sports-related oralinjuries. J Am Dent Assoc. 2006;137(12):1712-1720.
4. Bureau of Dental Education, American Dental Association. Eval-uation of mouth protectors used by high school football players.J Am Dent Assoc. 1964;68:430-442.
5. Klossner D, ed. 2008-2009 NCAA Sports Medicine Handbook.19th ed. Indianapolis, IN: NCAA; 2008:94-95.
6. Smith S. Muscular strength correlated to jaw posture and the tem-poromandibular joint. N Y State Dent J. 1978;44(7):278-285.
7. Smith SD. Adjusting mouthguards kinesiologically in profes-sional football players. N Y State Dent J. 1982;48(5):298-301.
8. Garabee WF. Craniomandibular orthopedics and athletic per-formance in the long distance runner: a three year study. BasalFacts. 1981;4(3):77-81.
9. Francis KT, Brasher J. Physiological effects of wearing mouth-guards. Br J Sports Med. 1991;25(4):227-231.
10.Ugalde V, Breslin EH, Walsh SA, et al. Pursed lips breathingimproves ventilation in myotonic muscular dystrophy. ArchPhys Med Rehabil. 2000;81(4):472-478.
11.Tiep BL. Pursed lips breathing—easing does it. J CardiopulmRehabil Prev. 2007;27(4):245-246.
12.Garner DP, McDivitt E. The effects of mouthpiece use on sa-livary cortisol and lactate levels during exercise. MSSE Suppl.In press.
13.Trenouth MJ, Timms DJ. Relationship of the functional oro-pharynx to craniofacial morphology. Angle Orthod. 1999;69(5):419-423.
14.Kyung SH, Park YC, Pae EK. Obstructive sleep apnea patientswith the oral appliance experience pharyngeal size and shapechanges in three dimensions. Angle Orthod. 2005;75(1):15-22.
15.Gale DJ, Sawyer RH, Woodcock A, et al. Do oral appliancesenlarge the airway in patients with obstructive sleep apnea? Aprospective computerized tomographic study. Eur J Orthod.2000;22(2):159-168.
16.Gao X, Otsuka R, Ono T, et al. Effect of titrated mandibularadvancement and jaw opening on the upper airway in nonap-neic men: a magnetic resonance imaging and cephalometricstudy. Am J Orthod Dentofacial Orthop. 2004;125(2):191-199.
17.Zhao X, Liu Y, Gao Y. Three-dimensional upper-airway changesassociated with various amounts of mandibular advancementin awake apnea patients. Am J Orthod Dentofacial Orthop. 2008;133(5):661-668.
18.Ryan CF, Love LL, Peat D, et al. Mandibular advancement oralappliance therapy for obstructive sleep apnoea: effect on awakecaliber of the velopharynx. Thorax. 1999;54(11):972-977.
19.Green HJ. Neuromuscular aspects of fatigue. Can J Sport Sci.1987;12(3):7S-19S.
20.Westerblad, H, Lee JA, Lännergren J, Allen DG. Cellular mech-anisms of fatigue in skeletal muscle. Am J Physiol. 1991;261(2 pt 1): C195-C209.
21.Harms CA, Wetter T, McClaran SR, et al. Effect of respiratorymuscle work on cardiac output and its distribution during max-imal exercise. J Appl Physiol. 1998;85(2):09-618.
22.Harms CA, Wetter TJ, St Croiz CM, et al. Effect of respiratorymuscle work on exercise performance. J Appl Physiol. 2000;89(1):131-138.
23.Kilding AE, Winter EM, Fysh M. Moderate-domain pulmo-nary oxygen uptake kinetics and endurance running perform-ance. J Sports Sci. 2006;24(9):1013-1022.
24.Casaburi R, Storer TW, Ben-Dov I, Wasserman K. Effect of en-durance training on possible determinants of VO2 during heavyexercise. J Appl Physiol. 1987;62(1):199-207.
Compendium—Volume 30 (Special Issue 2) 13
Garner and McDivitt

14 Compendium—Volume 30 (Special Issue 2)
Reaction time is the period that occurs between astimulus and the initiation of muscle response1
and can be assessed as simple reaction time,choice reaction time, and discriminate reaction time.1 Sig-nals to any sensory system in a variety of populations canbe ascertained in any of the above situations. For exam-ple, Borysiuk2 evaluated reaction and movement time withtactile, acoustic, and visual stimuli in advanced and novicefencers. He found that the advanced fencers had a signif-icantly improved reaction time with the visual (P < .057)and the tactile (P < .029) stimuli, with no significant differ-ences in the acoustic stimuli between novice and advancedfencers. However, the mean reaction and movement timeswith all three stimuli were lower in experienced fencers vs thebeginners. Borysiuk found fencing training improved reaction
times in people with advanced fencing skills, thereby explain-ing improved performance.2
Many studies in exercise science have suggested that the useof a mouthpiece can improve performance, which may be relat-ed to an enhancement in temporomandibular joint position-ing. Without proper temporomandibular joint positioning,nerves and arteries within the joint may become occluded,resulting in strain in nearby tissues, thereby reducing bloodflow.3-7 By neutralizing the temporomandibular joint with amouthpiece, patients have reported to their dentists reducedpain in the jaw, head, and neck areas, along with increased phys-ical strength. This improvement in strength may be linked toimproved blood flow and oxygen kinetics associated with re-duced stress in the temporomandibular joint, thereby produc-ing improved blood flow to the exercising skeletal muscles.8-10
1Assistant Professor, Department of Health, Exercise and Sport Science, The Citadel, Charleston, South Carolina2ACSM Health and Fitness Specialist, Boeing Activity Center, The Boeing Company, Everett, Washington
Abstract: Studies in exercise science have suggested that the use of a mouthpiece can improve performance, and these
improvements may be linked to an enhancement in temporomandibular joint (TMJ) positioning. Studies have suggested
that by improving TMJ positioning, there is improved blood flow in the area of the TMJ. Changes in TMJ positioning may
be improved with an oral device. The purpose of this study was to determine if there were improvements in auditory
and visual reaction time with the use of a boil and bite mouthpiece. Using a BIOPAC system, study participants (N = 34)
were asked to respond to an auditory signal during 40 trials. In the visual reaction time test, participants (N = 13) were
assessed on how quickly they responded to a computer cue for a total of 30 trials. Auditory results showed a significant
improvement with the use of a mouthpiece (241.44 ms) vs without a mouthpiece (249.94 ms). Visual results showed that
participants performed slightly better with the mouthpiece (285.55 ms) vs without the mouthpiece (287.55 ms). These
findings suggest that the use of mouthpiece positively affects visual and auditory reaction time, which is a vital aspect
to optimal sport and exercise performance. Future studies should continue to shed light on possible reasons for the
improvements in auditory and visual reaction time with the use of a mouthpeice. In addition, future studies should further
illuminate what, if any, connection these improvements have with enhanced TMJ positioning.
RESEARCH UPDATE
Effects of Mouthpiece Use on Auditory and Visual Reaction Time
in College Males and FemalesDena P. Garner, PhD;1 and Jenni Miskimin, MS2

Several studies have shown thatmouthpieces result in improvedstrength and endurance.11-14 Spe-cifically, Fuchs7 found the iso-metric strength of the upper andlower body in 40 females wasimproved when participants worea wax bite between the upper andlower teeth, resulting in a 3-mmvertical dimension. The great-est improvement with the waxbite was in isometric strength,with an increase of 8% in the leftarm, 4.5% in the right arm, 6.3%in the left foot, and 11% in theleft foot. Alexander15 confirmedthis finding when she tested theEDGE mouthpiece (Bite TechInc, Minneapolis, MN) in 61 male and female participantsand found 74% had improved grip strength when usingthe mouthpiece.
The authors found that muscular endurance improvedsignificantly with the use of the mouthpiece vs not using one.Specifically, they determined mean bench press repetitionsincreased 11% while preacher curl repetitions increased 17%when participants used the mouthpiece compared with non-use (P = .03 bench press; P = .004 preacher curl). Thus, basedon the indicative data that a mouthpiece improves exerciseoutcomes, this study’s goal was to further elucidate the possi-ble benefits of wearing a mouthpiece in regard to athletic per-formance, specifically improved reaction time.
METHODSThe research involved assessments of visual and auditory re-action times. There were 34 participants for the auditory armand 13 for the visual. Ages ranged from 18 years to 21 years,with participants recruited from The Citadel’s student body.The study was approved by the school’s internal reviewboard, and all participants signed consent forms.
BIOPAC Systems (BIOPAC Systems Inc, Goleta, CA)equipment was used to gauge auditory reaction time. TheBSL-SS10L push button hand switch (BIOPAC SystemsInc), BSL-OUT1 headphones (BIOPAC Systems Inc),and Windows 95/98/NT 4.0/2000 (Microsoft® Corp,Redmond, WA) were employed. Each participant sat in arelaxed position with closed eyes and held the hand switch
with the dominant hand, withthe thumb in position to pressthe button. They were in-structed to press this button whenthe headphones emitted a sound.Everyone underwent four seg-ments, with 10 trials each. Seg-ments one and two included astimulus at pseudo-random inter-vals (1 to 10 seconds) while seg-ments three and four used astimulus at fixed intervals (every4 seconds).
The visual test used a MS-DOS-based Motor LearningActivity Software System devel-oped at Texas A&M University.This system uses Hick’s Law,
which states that reaction time increases as a function of abinary logarithm (log2 n), in which “n” is the number ofequally likely possibilities. Specifically, the participantwas asked to place his or her fingers on letters on a com-puter keyboard that corresponded to the same letters thatwere displayed on the computer screen. Above each letteron the computer screen were four large circles. The pro-gram proceeded through three sets of 10 trials. During thefirst trial, a line would appear over one circle with the let-ter beneath it. After a pseudo-random amount of time(1-10 seconds), the circle became white, at which pointparticipants were to respond as quickly as possible by strik-ing the corresponding letter on the keyboard. During thesecond set of 10 trials, the line would appear over two circles,
Compendium—Volume 30 (Special Issue 2) 15
Figure 1 Mean values of auditory reaction time with andwithout mouthpiece.
235
240
245
250
255
Millis
econ
ds MouthpieceNo Mouthpiece
Mean of ParticIpants (N = 34)
BY NEUTRALIZING THE
TEMPOROMANDIBULAR
JOINT WITH A MOUTHPIECE,
PATIENTS HAVE REPORTED
TO THEIR DENTISTS
REDUCED PAIN IN THE JAW,
HEAD, AND NECK AREAS,
ALONG WITH INCREASED
PHYSICAL STRENGTH.
Garner and Miskimin
but only one circle became white, and participants were tostrike as quickly as possible the corresponding letter onthe keyboard. For the final set of 10 trials, a line appearedover all four circles, one circle turned white after a pseudo-random amount of time, and participants were to respondas quickly as possible by striking the corresponding key onthe keyboard. Participants completed two sets of the out-lined Hick’s Law test for a total of 60 trials.
For both arms of the study, participants completed thetrials with and without a mouthpiece (the EDGE boil andbite). This mouthpiece was designed specifically to create agreater bite opening distal vs proximal in the mouth. As-signment of the mouthpiece was random, and participantswere not told if any effect, either positive or negative, wouldresult from its use.
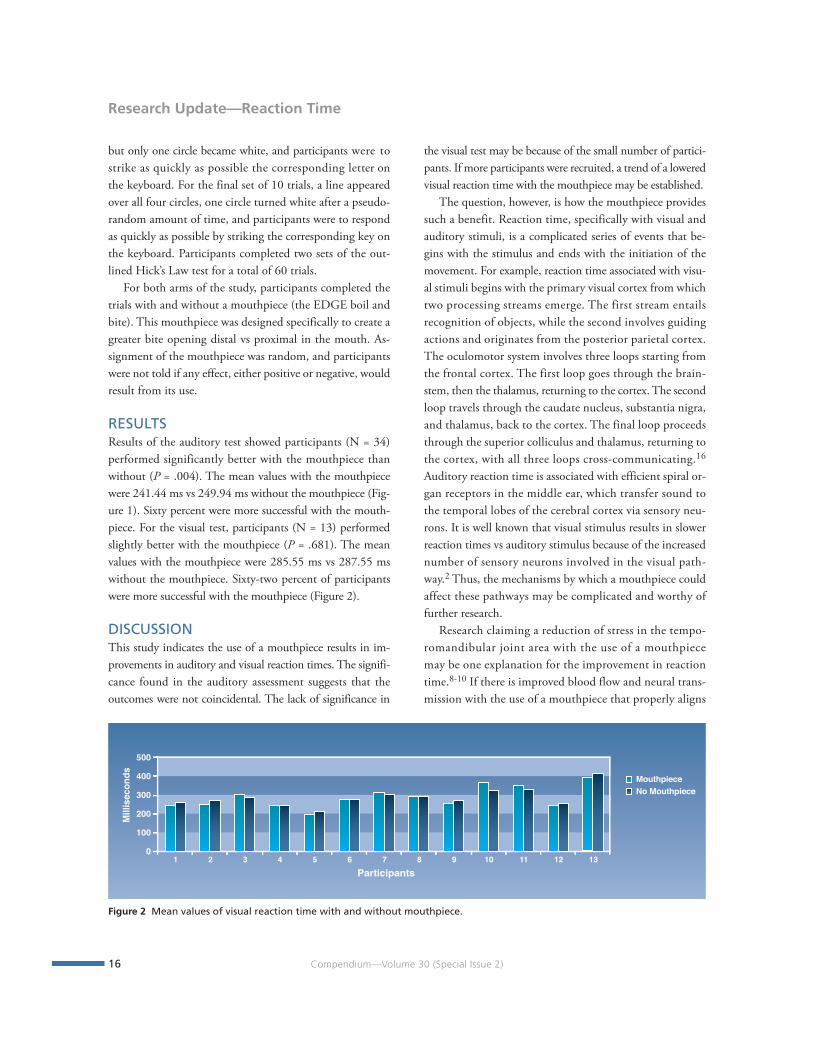
RESULTSResults of the auditory test showed participants (N = 34)performed significantly better with the mouthpiece thanwithout (P = .004). The mean values with the mouthpiecewere 241.44 ms vs 249.94 ms without the mouthpiece (Fig-ure 1). Sixty percent were more successful with the mouth-piece. For the visual test, participants (N = 13) performedslightly better with the mouthpiece (P = .681). The meanvalues with the mouthpiece were 285.55 ms vs 287.55 mswithout the mouthpiece. Sixty-two percent of participantswere more successful with the mouthpiece (Figure 2).
DISCUSSIONThis study indicates the use of a mouthpiece results in im-provements in auditory and visual reaction times. The signifi-cance found in the auditory assessment suggests that theoutcomes were not coincidental. The lack of significance in
the visual test may be because of the small number of partici-pants. If more participants were recruited, a trend of a loweredvisual reaction time with the mouthpiece may be established.
The question, however, is how the mouthpiece providessuch a benefit. Reaction time, specifically with visual andauditory stimuli, is a complicated series of events that be-gins with the stimulus and ends with the initiation of themovement. For example, reaction time associated with visu-al stimuli begins with the primary visual cortex from whichtwo processing streams emerge. The first stream entailsrecognition of objects, while the second involves guidingactions and originates from the posterior parietal cortex.The oculomotor system involves three loops starting fromthe frontal cortex. The first loop goes through the brain-stem, then the thalamus, returning to the cortex. The secondloop travels through the caudate nucleus, substantia nigra,and thalamus, back to the cortex. The final loop proceedsthrough the superior colliculus and thalamus, returning tothe cortex, with all three loops cross-communicating.16
Auditory reaction time is associated with efficient spiral or-gan receptors in the middle ear, which transfer sound tothe temporal lobes of the cerebral cortex via sensory neu-rons. It is well known that visual stimulus results in slowerreaction times vs auditory stimulus because of the increasednumber of sensory neurons involved in the visual path-way.2 Thus, the mechanisms by which a mouthpiece couldaffect these pathways may be complicated and worthy offurther research.
Research claiming a reduction of stress in the tempo-romandibular joint area with the use of a mouthpiecemay be one explanation for the improvement in reactiontime.8-10 If there is improved blood flow and neural trans-mission with the use of a mouthpiece that properly aligns
16 Compendium—Volume 30 (Special Issue 2)
Research Update—Reaction Time
Figure 2 Mean values of visual reaction time with and without mouthpiece.
0
100
200
300
400
500
Millis
econ
ds MouthpieceNo Mouthpiece
1 2 3 4 5 6 7 8 9 10 11 12 13Participants

Compendium—Volume 30 (Special Issue 2) 17
Garner and Miskimin
the temporomandibular joint, then blood flow with increasedoxygen unloading could be enhanced in other areas of thehead and neck, leading to improvements in such events asreaction time. Reaction time with both the auditory andvisual cues is a complicated series of events that may in someway be modulated with improved blood flow. Further studiesshould ascertain whether the physiologic mechanism withineach of these systems is affected by proper temporomandibu-lar alignment that occurs with the use of a mouthpiece.
CONCLUSIONThis study explored auditory and visual reaction times withand without the use of a mouthpiece. Many sports engagethe use of auditory and visual cues and depend on im-proved reaction times to obtain positive performance out-comes. If these findings are correct, it can be hypothesizedthat a number of athletes may be able to enhance perform-ance when using a mouthpiece. Further studies are neededfor a greater understanding of how mouthpieces affect per-formance physiologically.
DISCLOSUREDr. Garner has received an honorarium from Bite Tech Inc.
REFERENCES1. Magill RA. The measurement of motor performance is critical
to understanding motor learning. In: Magill, RA, ed. MotorLearning Concepts and Applications. 5th ed. Boston, MA:McGraw-Hill; 1998:17-20.
2. Borysiuk Z. The significance of sensorimotor response com-ponents and EMG signals depending on stimuli type fencing.Acta Uni Palacki Olomuc Gymn. 2008;38(1):43-51.
3. Fonder AC, Alter JL, Allemand LE, et al. Malocclusion as itrelates to general health. Ill Dent J. 1965;34:292-302.
4. Fonder AC, Allemand LE. Malocclusion, dental distress andeducability. Basal Facts. 1977;2(2):74-87.
5. Fonder AC. The Dental Physician. Blacksburg, VA: UniversityPublications; 1977:25-162.
6. Salaam A. The orthopedic approach to muscular dysfunction.Basal Facts. 1980;4(2):57-60.
7. Fuchs CZ. The Effect of the Temporomandibular Joint Positionon Isometric Muscle Strength and Power in Adult Females [disser-tation]. Boston, MA: Boston University; 1981.
8. Gelb H. Patient evaluation. Clinical Management of Head,Neck, and TMJ Pain and Dysfunction: A MultidisciplinaryApproach to Diagnosis and Treatment. Philadelphia, PA: WBSaunders Co; 1977:73-116.
9. Shore NA. Temporomandibular Joint Dysfunction and OcclusalEquilibrium. 2nd ed. Philadelphia, PA: JB Lippincott Co.; 1976.
10.Fonder AC. Stress and the dental distress syndrome. Basal Facts.1976;1(3):119-132.
11.Stenger JM. Physiologic dentistry with Notre Dame athletes.Basal Facts. 1977;2(1):8-18.
12.Smith SD. Muscular strength correlated to jaw posture andthe temporomandibular joint. N Y State Dent J. 1978;44(7):278-285.
13.Smith SD. Adjusting mouthguards kinesiologically in profes-sional football players. N Y State Dent J. 1982;48(5):298-301.
14.Garabee WF. Craniomandibular orthopedics and athletic per-formance in the long distance runner: a three year study. BasalFacts. 1981;4(3):77-81.
15.Alexander CF. A Study of the Effectiveness of a Self-Fit Man-dibular Repositioning Appliance on Increasing Human Strengthand Endurance Capabilities [master’s thesis]. Knoxville, TN:University of Tennessee; 1999.
16.Stuphorn V, Schall JD. Neuronal control and monitoring ofinitiation of movements. Muscle Nerve. 2002;26(3):326-339.
THUS, THE MECHANISMS
BY WHICH A MOUTHPIECE
COULD AFFECT THESE
PATHWAYS MAY BE
COMPLICATED AND WORTHY
OF FURTHER RESEARCH.
RESEARCH CLAIMING
A REDUCTION OF STRESS
IN THE TEMPOROMANDIBULAR
JOINT AREA WITH THE
USE OF A MOUTHPIECE
MAY BE ONE EXPLANATION
FOR THE IMPROVEMENT IN
REACTION TIME.

Abstract: Intraoral appliances (mouthguards) have long
been used and mandated for several sports, with good
results on the reduction of dentition injury. Recently claims
have arisen that mouthguards prevent brain injury. This
article reviews the data on such claims, the basic science
that has been conducted, and how an intraoral appliance
may in the future become part of an engineered system
to reduce transfer of energy from impacts to specific loca-
tions on the head, in an effort to mitigate some types of
mild traumatic brain injury.
Intraoral appliances, or mouthguards, designed to pro-tect the dentition have been in use for many years andmandated in most collision sports for some time.1
These devices have demonstrated some degree of effective-ness in limiting certain types of dental injuries.2 Recently,research has attempted to demonstrate that mouthguardsprevent mild traumatic brain injury (MTBI). This intereststems from growing emphasis on the causes, incidents, andidentification of MTBI, as well as potential preventive inter-ventions associated with MTBI. Some of this science is basedon acceleration measurements of the empty skull, while someis ascertained from field data.3 While skull measurementresearch is of interest, the magnitude of the impact and thusthe impulse is necessarily low. Although the data show someattenuation of energy, it is insufficient to make any claims.The field data also fall short of providing proof of any mean-ingful reduction in MTBI. A more recent controlled study ofneurologic impairment and recovery showed no change inoutcome with the use of mouthguards.4
This lack of data is not unexpected: to understand theseissues, the mechanics of MTBI and the use of the term“mouthguard” should be examined. The term “mouthguard”seems to refer to anything from a “buy them by the hun-dreds” boil and bite device that has little to no functional ef-fect on occlusion, to professionally made custom appliances,which may offer functional occlusion limits with a wide vari-ety of possible mandible positions and which can be madefrom different materials. While many of these custom appli-ances have a good track record of dental injury reduction,there is no standard for determining the function of theseappliances in MTBI, and they are functionally useless inMTBI prevention.5 The construction and fit of these customappliances is as variable as the practitioners and laboratoriesthat create them. In addition, other “in between” devices,which make various safety claims and offer insurance plans,can be purchased at retail and sporting goods stores and aresold by the millions. These devices sometimes use the word“brain” in the product name or include illustrated claims ofMTBI reduction or even prevention.6,7 Scientific data showthese claims to be misleading at best, and fraudulent at worst.
The previously mentioned studies often lack a descriptionof the actual devices employed at the time of data collection;this is particularly true of retrospective cohort studies inwhich athletes are polled after the fact to see if they werewearing an appliance. The data is of little value, except that itoffers no evidence of mitigation in the MTBI event. Otherrecent data suggest that some appliances may even increasethe transferred energy of an impact.5 In this author’s opinion,medically trained individuals should not believe that a device
18 Compendium—Volume 30 (Special Issue 2)
*Director, Sports Biomechanics Impact Research Lab, University of Tennessee, Knoxville, Tennessee; Principal Investigator/Scientist,
Engineering Institute for Injury and Trauma Prevention, University of Tennessee, Knoxville, Tennessee
The Role of Intraoral ProtectiveAppliances in the Reduction of MildTraumatic Brain InjuryP. D. Halstead*
LITERATURE REVIEW

placed between the mandible and the maxilla will somehowmitigate the energy from blows to any location on the headthat result in MTBI. At best, placing a simple “boil and bite”appliance in the space between the mandible and maxillamay effectively prevent interdigitation, but it could also pro-vide a slippery surface for the dentition of the mandible.
Consider typical athletes in contact sports: they are givena helmet, a face protector, a chin cup, and a “boil and bite”mouthguard. They are told repeatedly to “keep their headup” or “hit with the face.” What happens when athletes followthese rules? The energy from an impact is transferred fromthe face protector to the chin cup, then to the mandible, thedentition of which is on that slippery surface. The mandibleis then allowed to transfer to the rear with considerable force.The mechanics of this event, while not likely to cause MTBIor dentition injuries, will probably cause mandibular injury.This type of event can also endanger the delicate areas of theintercondylar space, perhaps leading to basilar skull fracturesor penetration of the glenoid fossa. As this is not a typicalconsideration for which the athlete is examined, and theproblem may not present clinically for years, the claim for thesuccessful prevention of dentition injury persists. From anengineering or biomechanics point of view, one of the basicsof any intervention is to understand how it will impact thesurrounding tissues and structures. In this case, the simplemechanics of the above impact scenario makes the potentialfor injury obvious.
MECHANICS OF THE MTBITo understand MTBI, and any role a mouthguard mayplay in the prevention of such injury, the mechanics of theMTBI should be examined. While the pathophysiology isonly now being understood, the mechanism of tissue dis-tortion that triggers these cascades is better comprehend-ed.8 The basic mechanical properties of the brain, while avery complex issue, are outlined here for the purposes ofthis discussion. The brain—within the confines of the cra-nial vault and protected by the dura mater, pia mater andarachnoid sheath, bathed in cerebral spinal fluid—is divid-ed into approximate halves separated by the falx, a verytough layer that limits the motion of the brain as a unit.Interspersed with the functional grey and white matter isthe blood supply. If one could hold the blood supply of thebrain intact in one hand, and the grey and white matterwith the falx in the other, one would appear to be holdingtwo brains. This intimate and complex system of tissues is
at times very different in the way it reacts to impacts andimpulses that demand a response from this viscous system.
As the system is combined of materials with differentmechanical properties, the issue of tissue distortion becomesapparent. Imagine shaking this complex, and visualize theneuronal axons of the grey and white matter distortingaround the more rigid materials of the falx and blood supply.One can see how tissue distortion can be highly variablebased on several factors, not the least of which is the magni-tude and direction of the impact or force vector. It alsobecomes clear that rotational or angular forces are the mostlikely to invoke problems at low levels. These kinds of insultsdo not require an actual impact to the head itself but can bethe result of rapid non-impact motion.9 More likely, there isan impact component at either the beginning or the end ofthe event.9 Therefore, both linear and rotational forces are atwork in almost all events that result in MTBI. For this rea-son, helmets demonstrate mixed and limited usefulness inthe prevention of MTBI and diffuse axonal injury (DAI).
While somewhat over-simplified, the following two sce-narios are examples of the complexity of these injuries. In thefirst, a head relatively not in motion is struck with an object.The impact results in a linear acceleration followed by a rota-tion, as the head is tethered to the torso and can translate onlya short distance. In this case, without a helmet, the person islikely, depending on the impact magnitude, to have a pointload, perhaps a skull fracture and significant linear injuryprior to the onset of any rotational acceleration. In this kind ofevent a helmet is indispensible, as it will spread the load area,which reduces the point load, thereby reducing the translationand rotational impulse as well. For this reason helmets have astellar record of injury reduction and prevention of eventssuch as skull fracture, subdural hematoma, and sudden death.
In the second scenario, the head is in motion: for examplewhen a person falls from a bike, and the head hits the pave-ment after the shoulder lands. In this case, there is a very highrotational impulse prior to head strike because the linear por-tion of this event is after the rotational event. Even if a helmetis worn, serious brain damage occurs, limited to the diffuseaxonal damage, which is the result of the rotation. The hel-met prevents the linear impact from causing immediatedeath by preventing skull fracture and tissue-destroying lin-ear impact. Although the helmet proved life-saving, the per-son is seriously injured. The helmet could not protect thebrain; the energy that injured the brain is the result of thebrain’s motion, while the helmet is on the skull.9
Halstead
Compendium—Volume 30 (Special Issue 2) 19

These events are only two possible examples: there aremany other incidents with varying degrees of magnitude.For example, if the helmet is too stiff, the impulse at the endof the rotation may exacerbate the rotational acceleration. Asofter helmet may limit the rotational rebound inside thehead but may have allowed the point load to take place, stillresulting in serious injury, but now more from the linearrather than rotational impact. In the first scenario, a too-softhelmet can result in death.
As a final step in this introduction to MTBI, imagine thesescenarios, and others, occurring at much lower impulses, sothat the damage is limited to a smaller number of axons (typ-ically farther from the center of rotation). In the case of lowermagnitude insult, MTBI can occur. There are standards forthe thresholds of more serious brain injuries, but not yet forMTBI.10,11 As some MTBIs can occur without head impact,no helmet, and thus no mouthguard, can prevent them.
PREVENTING INJURYHowever, there are measures that can be taken to preventMTBI. There is a point where the right mouthguard canlimit some of the forces that might cause MTBI. Based onthe above explanation, it is clear that the possibility is limitedto blows that occur to or are transferred to the mandible—and only the mandible. A device that 1) interdigitates theupper and lower dentition so the mandible is fixed, 2) sepa-rates the upper and lower dentition by providing a physicalbarrier of deformable material with the appropriate mechan-ical properties, and 3) wears comfortably, will limit the accel-eration of the head in impacts where the mandible is a primarypoint of load to the head. This device will protect the denti-tion and the mandible, and will limit the acceleration trans-lated to the head, thus reducing both linear and rotationalforces that result from the impact impulse.
While this is all good, it is neither a panacea or a simpleprocess. The mechanical properties of such a device mustallow it to work, via deformation, at the right time, for themaximum amount of displacement, while still maintaininginterdigitation and remaining comfortable. This is not asmall task. A standard must be developed to test various com-pounds and approaches to determine if this device could per-form as needed and further to determine the range of func-tion given the limits of materials and space. However, thisauthor believes, based on ongoing testing, that there is a bal-ance of mechanical properties that will result in a device that,when impacted with reasonable forces, either directly or via a
chin cup, will limit head acceleration to a degree that makesthis of value.5 This device will work best when coupled withother devices that limit the impulse, such as deformableface protector systems and chin anchor systems with care-fully designed properties, resulting in a system that works inharmony to limit the widest range of impulses while trans-ferring the least amount of acceleration to the head.
CONCLUSIONShould such devices exist, they will be important in the toolbox used to limit MTBI; however they will not be the criticalcomponent. Broad claims that such devices prevent concus-sion remain unsupported, and any claim that the device hassome function even when the mandible is not the point ofload should be discounted by the knowledgeable practitioner.
DISCLOSUREBite Tech Inc. has provided graduate student support in the past.
REFERENCES1. National Collegiate Athletic Association. 2008 NCAA® Football
Rules and Interpretations. Indianapolis, IN: NCAA; 2008:32.2. Knapik JJ, Marshall SW, Lee RB, et al. Mouthguards in sport
activities: history, physical properties and injury preventioneffectiveness. Sports Med. 2007;37(2):117-144.
3. Takeda T, Ishigami K, Hoshina S, et al. Can mouthguards pre-vent mandibular bone fractures and concussions? A laboratorystudy with an artificial skull model. Dent Traumatol. 2005;21(3):134-140.
4. Mihalik JP, McCaffrey MA, Rivera EM, et al. Effectiveness ofmouthguards in reducing neurocognitive deficits following sports-related cerebral concussion. DentTraumatol. 2007;23(1):14-20.
5. Padgett K. Evaluation of Human Performance Characteristics andPeak Head Acceleration Through the Use of Protective Mouthguards[master’s thesis]. Knoxville, Tennessee: The University of Ten-nessee; 2005.
6. Brain-Pad Inc. Brain-Pad Protective Solutions Technology.http://www.brainpads.com/index.php?option=com_content&view=article&id=112&Itemid=123. Accessed April 17, 2009.
7. Pro-Tekt Mouthguards. Mouthguard Facts. http://www.protektmouthguards.com/mouthguardfacts.htm. Accessed April 17, 2009.
8. Giza CC, Hovda DA. The neurometabolic cascade of concus-sion. J Athl Train. 2001;36(3):228-235.
9. Roy R. Evaluation of Head Linear and Rotational AccelerationResponse to Various Linear-Induced Impact Scenarios [master’s the-sis]. Knoxville, Tennessee: The University of Tennessee; 2007.
10.Pellman EJ, Viano DC, Withnall C, et al. Concussion in profes-sional football: helmet testing to assess impact performance—part 11. Neurosurgery. 2006;58(1):78-96.
11.Torg JS. Athletic Injuries to the Head, Neck, and Face. Philadel-phia, PA: Lea & Febiger; 1982.
Literature Review
20 Compendium—Volume 30 (Special Issue 2)
!"#$%&'#()*+,*-%""%''%%.*/"+0$#11%-&23%4*-%""%''%%*5%'%2&36*2"7*8&%2(#$%90362":%
!"#$%&#'()%#%# *&"+,"$%'-.)//0
123444
!"#$%&'"()"$*+",--+.$/0+)+11"(-"2"#+3-45/$62)&/7%328"9+:(1/$/()/);"!::3/2).+"()"<).8+21/);=%>2)"#$8+);$*"2)&",)&%82).+"?2:27/3/$/+1?*+8/+"52'+"!3+@2)&+8!"#$%&'#()*+,*-%""%''%%*.*/"+0$#11%
()5#'()%#5#'5#'6&/,7)$'$/'8/,'9/&'9&%%'":+'/;%:'"..%##'68'$)%'*&"+,"$%'-.)//0'"$'(&".%<'(%::%##%%'=%#%"&.)'":+'>&%"$5?%'@A.)":7%B'C$')"#'6%%:
"..%;$%+'9/&'5:.0,#5/:'5:'!"#$%&#'()%#%#'68'":'",$)/&5D%+'"+E5:5#$&"$/&'/9'(&".%<'(%::%##%%'=%#%"&.)'":+'>&%"$5?%'@A.)":7%B'F/&'E/&%'5:9/&E"$5/:G
;0%"#%'./:$".$ $&".%H,$IB%+,B
=%./EE%:+%+'>5$"$5/:J0%A":+%&G'>)%&5%'F"8%G'KJ'-$,+8'/:'$)%'@99%.$5?%:%##'/9'"'-%092F5$'!":+56,0"&'=%;/#5$5/:5:7'J;;05":.%'/:'C:.&%"#5:7'L,E":-$&%:7$)'":+'@:+,&":.%'>";"6505$5%#B'K'!"#$%&M#'()%#5#G'N:5?%$8'/9'(%::%##%%G'3444B)$$;<OO$&".%B$%::%##%%B%+,O,$IP7&"+$)%#O14Q

"A Study on the Effectiveness of a Self-Fit Mandibular Repositioning Ap" by Cherie Faye Alexander 4/29/11 8:50 AM
Trace: Tennessee Research and Creative Exchange MASTERS THESES 1 Title A Study on the Effectiveness of a Self-Fit Mandibular Repositioning Appliance on Increasing Human Strength and Endurance Capabilities 2 Author Cherie Faye Alexander, University of Tennessee - Knoxville 3 Date of Award 5-1999 Degree Type Thesis Degree Name Master of Science Major Engineering Science Major Professor Jack Wasserman Committee Members John Hungerford, Tyler Kress http://trace.tennessee.edu/utk_gradthes/594/ "A Study on the Effectiveness of a Self-Fit Mandibular Repositioning Ap" by Cherie Faye Alexander 4/29/11 8:50 AM
Abstract Years of study and constant anecdotal infonnation dating back to the ancient Romans exists regarding the relationship of mandibular position, occlusion surface changes, and human performance. Such old sayings and practices like "bite the bullet" and the actual act of clenching one's teeth on a stick prior to exertion or in anticipation of pain are but two examples of how this relationship has been intuitively understood by man for some time. Previous scientific works in this area have generally suffered at least one serious shortcoming in data collection, data analysis, test device flaws or lack of control measures. There seem to be emotionally charged efforts to either prove or disprove the apparent relationship between jaw positioning and human performance. It is unclear why there has been so much controversy but the fact that this emotional side taking exists leads to concerns about preconceptions on the part of the previous research teams. In an effort to reach some realistic levels of confidence, this effort has been accomplished in a double blind, placebo controlled, unbiased manner utilizing the tenets of the scientific method throughout. The data indicate that a self-fit, intra-oral device is beneficial in improving grip strength values for both men and women at a confidence level of at least 95 percent. In addition, there is a 96 percent confidence level that a mandibular repositioning appliance is of greater assistance in grip strength tests than a placebo device. Therefore, the results of this research initiative demonstrate that statistically relevant human performance increases are possible by employing a self-fit, intra-oral device in active men and women of all ages. Recommended Citation Alexander, Cherie Faye, "A Study on the Effectiveness of a Self-Fit Mandibular Repositioning Appliance on Increasing Human Strength and Endurance Capabilities. " Master's Thesis, University of Tennessee, 1999. http://trace.tennessee.edu/utk_gradthes/594 Links 1. http://trace.tennessee.edu/utk_gradthes 2. http://trace.tennessee.edu/cgi/viewcontent.cgi?article=1747&context=utk_gradthes 3. http://trace.tennessee.edu/cgi/query.cgi? field_1=lname&value_1=Alexander&field_2=fname&value_2=Cherie&advanced=1 http://trace.tennessee.edu/utk_gradthes/594/!
THE EFFECTS OF ARMOURBITE® MOUTHPIECE USE ON BASEBALL PITCHING VELOCITY
STUDY PERFORMED AT Rod Dedeaux Research & Baseball Institute

The Effects of ArmourBite® Mouthpiece Use on Baseball Pitching Velocity House, Tom; Wishmyer, Randy Rod Dedeaux Research & Baseball Institute. March, 2011. Performance Mouthpieces, particularly ArmourBite® (Bite-Tech Corp), are becoming more and more prevalent among rotational sports such as baseball. There is limited research to date examining these mouthpieces and any direct effect on pitching velocity (mph). PURPOSE: To investigate the possible effect on pitching velocity (mph) when wearing and not wearing a mouthpiece, ArmourBite® (Bite-Tech Corp), during several offseason training periods. METHODS: Subjects, amateur and professional baseball pitchers, were asked to take part in Personal Adaptive Joint Threshold Training, 1 day a week, over a 6 week training period at the Rod Dedeaux Research & Baseball Institute. Subjects would train with 6 differently weighted training baseballs, 2lb., 1lb., 6oz., 5oz. (regulation baseball), 4oz., 2oz., during a training session (6 total). Subjects would alternate throwing with and without ArmourBite® mouthpiece, in 2 pitch increments, while velocity was actively recorded by a standard radar speed gun. Ten (n=10) subjects were asked to complete the training protocol while alternating with and without ArmourBite®. Pitching velocity (mph) of all subjects were recorded for each of the 6 differently weighted training baseballs per session with and without the use of ArmourBite®, and the averages were recorded. RESULTS: The use of the mouthpiece elicited an average of 2 mph increase in pitching velocity among all subjects for all 6 variously weighted training baseballs, including a 5 oz. weighted baseball (regulation weight). CONCLUSION: This study suggests that the use of a mouthpiece (ArmourBite®) may be used to directly increase pitching velocity amongst amateur and professional baseball pitchers. ! !!!!! !"#$%&$'#(!!)*!*+#!Rod Dedeaux Research & Baseball Institute! !!!!!!!!!


















