
Research Article Lynx: Automatic Elderly Behavior...
19
Research Article Lynx: Automatic Elderly Behavior Prediction in Home Telecare Jose Manuel Lopez-Guede, 1,2 Aitor Moreno-Fernandez-de-Leceta, 3 Alexeiw Martinez-Garcia, 3 and Manuel Graña 2,4,5 1 Department of Systems Engineering and Automatic Control, University College of Engineering of Vitoria, Basque Country University (UPV/EHU), Nieves Cano 12, 01006 Vitoria, Spain 2 Computational Intelligence Group, Faculty of Informatics, Basque Country University (UPV/EHU), Paseo Manuel de Lardizabal 1, 20018 San Sebastian, Spain 3 Instituto Iberm´ atica de Innovaci´ on, Sistemas Inteligentes de Control y Gesti´ on Parque Tecnol´ ogico de ´ Alava Leonardo Da Vinci, 9–2 ∘ Edificio E5, Mi˜ nano, 01510 ´ Alava, Spain 4 Department of Computer Science and Artificial Intelligence, Faculty of Informatics, Basque Country University (UPV/EHU), Paseo Manuel de Lardizabal 1, 20018 San Sebastian, Spain 5 ENGINE Centre, Wrocław University of Technology, Wybrze˙ ze Wyspia´ nskiego 27, 50-370 Wrocław, Poland Correspondence should be addressed to Jose Manuel Lopez-Guede; [email protected] Received 2 August 2015; Revised 21 October 2015; Accepted 22 October 2015 Academic Editor: Peter Krustrup Copyright © 2015 Jose Manuel Lopez-Guede et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. is paper introduces Lynx, an intelligent system for personal safety at home environments, oriented to elderly people living independently, which encompasses a decision support machine for automatic home risk prevention, tested in real-life environments to respond to real time situations. e automatic system described in this paper prevents such risks by an advanced analytic methods supported by an expert knowledge system. It is minimally intrusive, using plug-and-play sensors and machine learning algorithms to learn the elder’s daily activity taking into account even his health records. If the system detects that something unusual happens (in a wide sense) or if something is wrong relative to the user’s health habits or medical recommendations, it sends at real-time alarm to the family, care center, or medical agents, without human intervention. e system feeds on information from sensors deployed in the home and knowledge of subject physical activities, which can be collected by mobile applications and enriched by personalized health information from clinical reports encoded in the system. e system usability and reliability have been tested in real-life conditions, with an accuracy larger than 81%. 1. Introduction Ambient Assisted Living (AAL) [1] is defined as the use of information and communication technology to shape intelligent living environments reacting to the needs of the inhabitants, providing relevant assistance, and helping them to live a fully independent life. End users are the stakeholders in the AAL ecosystem: citizens, formal and informal care givers, service providers, technology providers, and policy makers. e beneficiaries will be those people who wish to be able to avoid dependency on nursing homes, preferring to continue to live independently in their own homes. Assistance might be needed in any aspect of daily life, from health safety and security to social integration and mobility support. e steering board of the European Innovation Partnership on Active and Healthy Ageing (EIP-AHA) asserts [2]: “ICT solutions can prolong independent living of older people and extend the time they remain active and safe in their preferred environment. ey also have a huge potential to enhance social inclusion and participation of older people, reduce depression rates, enhance quality of work for carers and make overall care provision economically sustainable (e.g., by avoiding and reducing hospital stays).” Health knowledge about the elder’s state is the starting point to identify behavior patterns and to assess his/her status like taking medication, activity recommendations, social interactions, early memory loss, disorientation, falls at home, and symptoms of weakness, tiredness, or fatigue. Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 201939, 18 pages http://dx.doi.org/10.1155/2015/201939
Transcript of Research Article Lynx: Automatic Elderly Behavior...

Research ArticleLynx: Automatic Elderly Behavior Prediction in Home Telecare
Jose Manuel Lopez-Guede,1,2 Aitor Moreno-Fernandez-de-Leceta,3
Alexeiw Martinez-Garcia,3 and Manuel Graña2,4,5
1Department of Systems Engineering and Automatic Control, University College of Engineering of Vitoria,Basque Country University (UPV/EHU), Nieves Cano 12, 01006 Vitoria, Spain2Computational Intelligence Group, Faculty of Informatics, Basque Country University (UPV/EHU),Paseo Manuel de Lardizabal 1, 20018 San Sebastian, Spain3Instituto Ibermatica de Innovacion, Sistemas Inteligentes de Control y Gestion Parque Tecnologico de Alava Leonardo Da Vinci,9 – 2∘ Edificio E5, Minano, 01510 Alava, Spain4Department of Computer Science and Artificial Intelligence, Faculty of Informatics, Basque Country University (UPV/EHU),Paseo Manuel de Lardizabal 1, 20018 San Sebastian, Spain5ENGINE Centre, Wrocław University of Technology, Wybrzeze Wyspianskiego 27, 50-370 Wrocław, Poland
Correspondence should be addressed to Jose Manuel Lopez-Guede; [email protected]
Received 2 August 2015; Revised 21 October 2015; Accepted 22 October 2015
Academic Editor: Peter Krustrup
Copyright © 2015 Jose Manuel Lopez-Guede et al. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
This paper introduces Lynx, an intelligent system for personal safety at home environments, oriented to elderly people livingindependently, which encompasses a decision supportmachine for automatic home risk prevention, tested in real-life environmentsto respond to real time situations.The automatic systemdescribed in this paper prevents such risks by an advanced analyticmethodssupported by an expert knowledge system. It is minimally intrusive, using plug-and-play sensors and machine learning algorithmsto learn the elder’s daily activity taking into account even his health records. If the system detects that something unusual happens(in a wide sense) or if something is wrong relative to the user’s health habits or medical recommendations, it sends at real-timealarm to the family, care center, or medical agents, without human intervention. The system feeds on information from sensorsdeployed in the home and knowledge of subject physical activities, which can be collected by mobile applications and enriched bypersonalized health information from clinical reports encoded in the system. The system usability and reliability have been testedin real-life conditions, with an accuracy larger than 81%.
1. Introduction
Ambient Assisted Living (AAL) [1] is defined as the useof information and communication technology to shapeintelligent living environments reacting to the needs of theinhabitants, providing relevant assistance, and helping themto live a fully independent life. End users are the stakeholdersin the AAL ecosystem: citizens, formal and informal caregivers, service providers, technology providers, and policymakers. The beneficiaries will be those people who wish tobe able to avoid dependency on nursing homes, preferringto continue to live independently in their own homes.Assistance might be needed in any aspect of daily life, fromhealth safety and security to social integration and mobility
support. The steering board of the European InnovationPartnership onActive andHealthyAgeing (EIP-AHA) asserts[2]: “ICT solutions can prolong independent living of olderpeople and extend the time they remain active and safe intheir preferred environment. They also have a huge potentialto enhance social inclusion and participation of older people,reduce depression rates, enhance quality of work for carersand make overall care provision economically sustainable(e.g., by avoiding and reducing hospital stays).”
Health knowledge about the elder’s state is the startingpoint to identify behavior patterns and to assess his/herstatus like taking medication, activity recommendations,social interactions, early memory loss, disorientation, fallsat home, and symptoms of weakness, tiredness, or fatigue.
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015, Article ID 201939, 18 pageshttp://dx.doi.org/10.1155/2015/201939

2 BioMed Research International
It can be stated that we are looking for an Intention Detec-tion System. Various experiments on AAL environmentshave demonstrated the possibilities and the complexities ofintention detection [3]. User action measurement and real-time monitoring of user experience enable a new rangeof innovative systems and key enhancements to existingproducts [4].
The main objectives of Lynx, the system described in thispaper, are as follows:
(i) Develop a knowledge management system able tostore and understand the user clinical status, activity,context, and situation aware, allowing to integratethis semantic information in the intelligent system, inorder to detect health abnormal events.
(ii) Create intelligent monitoring services of an elder andhis medical issues, so that the system adapts to him,creating automatically rules that determine the usualvalues for each individual and evolve with the subjectunder monitoring, so that they are always up to date.These rules allow launching fully customized alertswithout human intervention.
(iii) Create a telecare third-party system based on anexpert system and an inference engine that canautomatically detect dangerous situations decreasingfalse positives, firing events only at abnormal circum-stances.
The critical task of the system is the automatic profiling ofuser behaviors. Several systems were introduced in recentyears to address elder-care issues, principally fall detectionsystems [5–9]. However, most of these systems either aretoo expensive for mass use or are of low quality. Mostcommercial solutions are capable only of fall detection [10].Previous efforts have been done addressing this problem byour research group [11] based on ontologies [12], but the auto-matic data capture from electronic health records (writtenby medical personnel in natural language) and automaticmedical summaries creation has not been considered untilthe present work.
The remainder of the paper is organized as follows.Section 2 introduces the system architecture. Sections 3 and4 give details about the system data-source types. Section 5describes the automatic data capture from health record innatural language for creation of medical summaries, whileSections 6, 7, and 8 explain the intelligence system. Up to thispoint, each section has explained each one of the differentmodules of the system. Section 9 discusses the results of thereal implantation of the system. Finally, Section 10 presentsour conclusions and future work.
2. System Architecture
Context Awareness (CA) [13, 14] definitions focus on thesituation of an entity, that is, the user’s context, or the contextof the devices carried by the user. Context includes location,identity, activity, and time. Recently the viewpoint has shiftedtowards a notion of the user being part of a process or ecology,as exemplified by Ambient Intelligence (AmI) [15]. In AmI
vision devices interact to support people in carrying out theireveryday life activities and tasks in a natural way on the basisof information and intelligence that is hidden in this networkof interconnected devices. Research in smart environmentsis often related to AAL attempts to extract information aboutpeople well-being (sleeping, being awake, daily rhythm, falls,or level of general activity) from the various sensors, oftenincluding cameras [16].
The Lynx system is designed to fulfill two main require-ments. First, the extraction, transformation, and load ofsensor information are to be carried out in a simply way:the sensor is plugged on the network, and its raw datais automatically integrated in the platform. Second, theplatformmust be able to measure the elderly’s habits in orderto track his behavior to find deviations from their daily tasks(wake-up times, sleep habits, diary strolls, etc.) or regardingtheir health situation and provide a detailed summary to thecaregivers and the family about their evolution.
Figure 1 shows how the system is organized in five mainmodules, which are discussed in the following sections:
(i) Data Capture from Heterogeneous Sensors.(ii) Relevant Electronic Health Record Evidences.(iii) Central Ontology and Expert Rules System.(iv) Intention Detection System.(v) Anomaly Detection System.
The overall operation of the system represented in Figure 1can be explained as follows: sensors collect and send infor-mation through the “SensorListenerSystem” when they areactivated (by, e.g., presence, smoke, or opened doors) to theCentral Ontology and Expert Rules System, which checkswhether this information generates a status change over pre-vious values. If this new information generates a status changeover previous values, the event is recorded in the centraldatabase system. The collected information, depending onthe type of the sensor, is checked with end user configuredthresholds in a rule editor. If the taken measures do notmeet those thresholds, a technical error event is generatedby the system. Usually, since the sensors are very simple (theactivation information is binary), this check is not usuallynecessary, only in physiological sensors. Finally, the correctdata are transformed from raw data to context data (e.g.,being at kitchen in the morning after a shower, it is translateto “taking breakfast”) by the Central Ontology System andits rules. This context stage is, finally, compared with theelderly usual behavior (based on the Intention DetectionSystem and the Anomaly Detection System). If they do notmatch, the systemwill generate alert events, and, according totheir pathologies (medical history), the Expert Rules Systemmodule provides concrete recommendations for action (noti-fication to family, dialing to an ambulance, recommendationsfor improvement directly health habits, etc.)
3. Data Capture from Heterogeneous Sensors
The main component of this platform at the gateway level isthe so-called Home Box Service (HSB), a structured software

BioMed Research International 3
Elderly people care at home
Risk events
Intention DetectionSystem
Expert knowledgeRelevant electronic health record
evidences
Elder people
Data capture fromheterogeneous sensors
Medical summariescreation
Emergencyservices
Central Ontology andExpert Rules System
Anomaly DetectionSystem
Physiologicalsensors
Home sensors
SensorListenerSystem
Decision engine monitor
Hou
ses
Elderly personin charge
Figure 1: Lynx artificial intelligence platform over real housing with care systems.
system, flexible and hardware platform independent, whichis the system kernel processing the remote data received.Regarding the technologies involved, we use the UPnP [17]protocol which does not only cover internet protocols suchas TCP/IP, HTTP, SOAP, UDP, or XML, but also integrateZigbee, USB, IEEE802.11, BT, BLE Wi-Fi, and security con-siderations using security techniques like X.509 certificates.Moreover, this protocol is open and it can be extended (e.g., todefine a specific type of message adding extra attributes).TheLynx system contains three types of sensors: environmental,physiological, and embedded service and audiovisual sensors,connected to one or more hubs.
Lynx has been admitted in universAAL [18], the Europeanplatform of reference in telecare systems.There is muchmoresupplementary information about technical specifications ofdata capturing in previously published papers [19, 20].
4. Relevant Electronic HealthRecord Evidences
Caring for elderly requires a multidisciplinary approach andmay include monitoring of the health status of elderly andthe management of chronic conditions and the inclusion ofone or more medications prescribed for regular use. Thiscomplex context must be taken into account in a telecaresystem [21]. Personal medical knowledge of elderly people ina teleassistance system allows improving the quality of theirlife habits, predicting dangerous situations derived from their
pathologies. This knowledge, enriched with actual sensorinformation, is both manual and automatically stored in aspecialized medical-telecare context-aware ontology repre-senting information in a hierarchical way, with a dynamicand variable structure, which can be automatically updated“online” with new clinical information, new kinds of sensors,or new units ofmeasurement. Also, this ontology implementsthe rules inferring new knowledge based on the raw data,health status, medical or behavior recommendations, andfinally the expert system alerts rules.
Semantic networks implemented in ontologies allow forconcept disambiguation [22], but even using huge medicalresources collection of relations is not enough to createsemantic networks. These relations are based on cooccur-rences and do not contain any systematic description ofthe ontological concepts. Ontology itself may be used as acomplex set of concepts joined in a parent-child structure,where each concept has been linked with some possiblesynonym, being most useful to resolve semantic conflicts ofambiguity in a concrete context. To be able to prioritize, weare using a rule-based system that has facility for explaininginferences as a framework for supporting clinicians at thepoint of care [23]. Given the large amount of informationto be managed, we need to use storage techniques able tomanage efficiently large volumes of data (data warehouse)and provide easy access and efficient management of theinformation (big data paradigm) [24]. So, in this project, weare using a no-SQL database, storing the information in atriple mode over the Virtuoso system [25, 26].

4 BioMed Research International
5. Automatic Data Capture from EHR NaturalLanguage: Medical Summaries Creation
Nowadays, electronic health records (EHR) store most ofthe patient evolution information in natural language reports(80% of relevant information), written by the medical per-sonnel, so that the percentage of structured informationcontaining quantitative data is minimal. EHR systems can becombined with Diagnostic Support Systems (DSS) to alloworder entry and provide alerts on errors of drug dosage,allergies, and contraindications, guided selection of diagnos-tic tests, reminders for procedures, tests, visits, computer-assisted diagnosis, and trend analysis. The extraction of theinformation is not an easy task and requires the developmentof correlation, noise reduction, and inference algorithms.Thestandardization of EHR is not a trivial problem.The coding ofdata within EHR and clinical databases is essential for sharingand exchanging across heterogeneous systems. Challenges toadoption of terminology standards [27] include the use oflocal coding vocabularies and idioms and efforts tomap fromdisparate systems to a given standard, as well as identifyingthe appropriate standards for medications, laboratory, andother diagnostic tests and problems. In general, it involvesthe use of a combination of approaches (automated, semi-automated, and manual) and terminology systems (MasterDrug Data Base (MDDB), RxNorm, Systematized Nomen-clature of Medicine-Clinical Terms (SNOMED CT), and theUnified Medical Language System (UMLS) Metathesaurus)for identifying SNOMEDCT concepts and hierarchies as wellas UMLS Concept Unique Identifiers (CUI) for medications[28].
It is not easy to identify the principal diagnosis or diseasein natural language over EHR fields. There are descriptionsabout the family history, secondary diagnosis, and a constel-lation of comorbid diseases.We have developed a preclassifierto detect the main disease and diagnosis, the principalmedical procedures, treatments, and medications impactingdirectly in the user’s life, embedding it into the teleassistanceplatform as a new indicator. Normal age-related changes maybe accompanied by chronic health problems such as diabetesor heart disease. Managing many such chronic conditionsmay include one or more medications prescribed for regularor daily use. Combined, these factors increase the complexityof telecare systems [29]. Usually, this information is in severalclinical records stored in a not structured way but is veryrelevant in order to supply an optimal service. As seen inFigure 2, Lynx system is able to translate literal medical textsinto a semantic structure system (the Central Ontology), inorder to find the correlations between the clinical diseases,treatments, and drugs with the lifeday personal requirementsof each elder.
There are mathematical techniques that are used tocapture the semantic structure of documents based on cor-relations among textual elements within them [30]; however,inside Lynx system we propose a new method for creat-ing medical summaries, supported by a statistical/semantichybrid system.The annotation algorithmswork over differentsources, languages, and data types, based on vast text infor-mation sources (over the different natural medical language
written clinical histories and medical reports comprising thebroad set of medical disciplines and the different medicalfields and tests). The achievement of this goal involves thefollowing actions:
(i) To extract information fromnatural languagemedicalreports in EHR that comprise a broad number ofmedical context and a great variability among thedifferent medical fields, countries, and even hospitals.
(ii) To define a new model that is able to comprise,normalize, and structure the information containedin the different clinical reports generating a uniquestructured descriptor in a standard format.
(iii) To enrich the information from other sources, bothexternal and internal, of heterogeneous data.
(iv) To compress the generated models and descriptors tosupport compactness and real time response and toimprove inference strength in semantic summaries.
(v) To develop a semantic ontology model that is ableto structure, normalize, enrich, and compact thewritten clinical histories, test reports, and clinicalrecords regardless of the medical discipline, country,language, hospital, and practitioner. This task willfocus on the modeling of relevant information forclinical practice applications, for instance, the inte-gration with other clinical collected data, and use thisinformation for search new medical researches. Ourkey involvement focuses on linking to clinical IT andto the knowledge collected in clinical practice.
The system takes into account the correlation of all the con-cepts in the clinical records about the primary diagnosis of thepatient, by calculating the different concepts vectors with the“tf/idf” frequency algorithm. Later, we run a “map” processwhich will analyze the direct correlation of secondaries vari-ables with the principal concepts, extracting their relation-ships and recoding themunder theUnifiedMedical LanguageSystem (UMLS) Metathesaurus.The UMLSMetathesaurus isa large, multipurpose, and multilingual vocabulary databasethat is organized by concepts. The current release com-prises more than 1.5 million biomedical terms from over100 sources. Synonymous terms are clustered together toform a unique concept or cluster. Concepts are linked toother concepts by means of various types of relationships,resulting in a rich graph. The Semantic Network providesa consistent categorization of all concepts represented inthe UMLS Metathesaurus as well as information about theset of basic semantic types, or categories, which may beassigned to those concepts. Lynx Semantic Network contains133 semantic types and 54 relationships.
Sharing common understanding of the structure ofinformation among people or software agents is one of themost common objectives developing ontologies [31]. Forexample, if there is a set of different specialized medi-cal databases (containing medical information), specializedgenomic databases (providing genomic information), andother statistic databases sharing demographic and econom-ical information regarding the population in a certain situa-tion, there could be services able to share and publish all this

BioMed Research International 5
Figure 2: Data capture from clinical records.
information under the same ontology and vocabulary. So, atthe end, computer agents could extract, join, aggregate, andinfer new information from these different sites. The agentscould use this aggregated information to answer user com-plex and cross-domain queries or as input data to other appli-cations. Enabling reuse of domain knowledge was one of thedriving forces behind recent surge in ontology research [12].
First, we built a large general medical ontology (illus-trated in Figure 3) merging ontologies from oncological, aheart failure, and a general medicine contexts, all basedon OpenEHR archetypes, used as the main basis to buildthe semantic classes, subclasses, and properties. OpenEHRarchetypes are reusable definitions for fragments of clin-ical information. Translating them to ontology languagesenables the use of inference and mapping to existing formalontologies in the biomedical and clinical domains. Oncethese clinical archetypes are translated into Ontology WebLanguage (OWL) objects, we combine them to set up ourSummariesOntologywhich becomes the starting point of theinference process. It is shown that the OWL technology (asemantic storage format) achieves high efficiency, accuracy,scalability, and effectivity [32]. Also it is necessary to store thepatients evolution (clinical actuations) named “observations”in OpenEHR. To join these concepts into our ontology, weenrich our base ontology with a specific and a universal“observation” ontology, including identifying informationmodel elements, vocabulary concepts, and data types fromkey standards such as HL7/RIM, Detailed Clinical Models(DCM), Clinical Document Architecture (CDA), and theStudy Data Tabulation Model [33].
Figure 3: Medical observations in the summaries ontology.
Figure 3 shows that the ontology is able to store infor-mation in a semantic format, episode by episode, aboutwhat the most important concepts extracted from eachepisode are. Examples of such extracted concepts are whetherthere has been a secondary diagnosis, the episode speaksabout a previous general diagnosis, there has been anykind of treatment, medical, or surgery procedure, he hasrecommended a drug in particular, the treatment has beenmodified, any specific pathology has been detected, or simplythe patient has been informed of something. Also, each

6 BioMed Research International
Table 1: (a) Diagnostics. (b) Treatment and diagnostics.
(a)
D 4755 4270 C0007124 1 dcis neop Noninfiltrating intraductal carcinomaD 4755 4279 C0337354 1 Quadrantectomy topp Quadrantectomy of breastD 4755 4280 C0222600 1 Right breast bpoc Right breastD 4756 4298 C1176475 1 Ductal carcinoma neop Ductal carcinomaD 4756 4299 C1318216 1 4 qnco 4D 4756 4300 C0237753 1 4 mm GATE length 4.0mm
(b)
D 4757 4303 C0007097 1 Carcinoma neop CarcinomaD 4757 4308 C0450367 1 4.5 qnco 04-mayD 4757 4309 C0237753 1 4.5 cm GATE length 4.5 cmT 4757 4311 C0543467 1 Surgical diap, topp Operative surgical procedures
episode has a type of “Clinical Action,” as “diagnostic act,”“therapeutic act,” and so forth, extracted from the OpenEHRstandard ontology.The Lynx ontology supports the CEN/ISOEN13606 norm, that is, a European norm from the EuropeanCommittee for Standardization (CEN) designed to achievesemantic interoperability in the electronic health recordcommunication.
The general algorithm to create summaries has the fol-lowing steps:
(1) Perform the text preprocessing steps: stemming, stop-list, and spell-checking, either correcting or removingstrings that are not recognized.
(2) Use MetaMap [34] with very restrictive settings toavoid highly ambiguous results whenmapping text toUMLS ontology and try to expand some acronyms.
(3) Use UMLS relations to create first-order classes,adding only those types of relations that lead toimprovement of classification results.
(4) Annotate the concepts on the summaries ontologywith a set of rules joining automatically pair conceptswith their relationships or properties.
Table 1 shows through an example the result of the describedalgorithm. It can be seen that the electronic health recordwritten in natural language which is the original source ofinformation, and the diagnostic and the treatment derivedfrom it expressed in UMLS.
The use of a No-SQL database to store Resource Descrip-tion Framework (RDF) andWeb Ontology Language (OWL)descriptions makes it possible to query, manipulate, andreason about the data with standard tools, such as OWLreasoners and languages (e.g., the SPARQL Query Languagefor RDF).
5.1. Text Preprocessing Steps, MetMap Annotations, and Con-cepts Weights. The EHR typically contain description ofdifferent episodes written in natural language by the medicalstaff; often they are multilingual (English, Spanish, etc.) withtheir diagnostic impressions, treatments, procedures, and soforth [35]. The first step is to determine the break points
in each episode regarding a principal disease, a principaltreatment, or the medical recommendations and the trans-formation of the concepts found in every group over UMLScodes in an indexed process according to the following steps:
(i) For indexing, there are public tables with “stop-words” (not relevant words) and some dictionaries tohelp in the automatic translation between concepts(one or more words regarding a medical disease, pro-cedure, treatment, drug or observation) and codes,scripts errors, abbreviations, or names of very localconcepts (e.g., Rt is radiotherapy). However, thesecodes are plain; that is, their importance is basedon the frequency, assigned to a group, and basically,it is proportional to the way of occurrence of theterms in each document or group and inverselyproportional to the appearance of such terms wherethey have the whole information set. Figure 4 showsan example of the absolute frequency of apparitionof different terms in a set of clinical records. Toincorporate semantics [36] that can “understand”what really means the medical staff, two externalsources are used: hierarchies of UMLS coding and amedical dictionary of synonyms and acronyms. Notall episodes of a medical record have the same weightwithin a patient history, and also within each episode,not all sentences are relevant: there may be referencesto background, notmedically significant observationsor not sufficiently relevant to appear in a medicalsummary, although subsequent to an analytical pro-cess. Therefore, the system records all the conceptsin the ontology, but later, in the presentation of thefinal summary, only the information of those that arethe most relevant episodes is shown, that is, thosethat have objective correlation with main diagnosisof each patient. The whole text in the clinical recordis split into sentences using the tokenizer, whichcarries out such transformation following the gram-mar of the natural language. The tokenizer is part ofspeech tagger and sentence splitter modules of theGeneral Architecture for Text Engineering (GATE)

BioMed Research International 7
PREF
ERRE
D_N
AM
E
0 5 10 15
YearVaginal swab (specimen)
UnusualThick
Surgical marginsSize
Segmental mastectomyRight
RegularQuadrantectomy of breast
PreviousPlant bulbPalpation
Noninfiltrating intraductal carcinomaMonday
Mammographic microcalcification found on diagnostic imaging of breastLeukorrhea
InternalHysteroscopy
GynecologyGenital system
FirmErythematous
EasyDesignatedCribriform
ComprehensionChecking (action)
CarryingBiopsy
Atrophic endometriumAnthropological culture
ACETIC50
4/52008-09-30
16.5mm06/02/2009
Figure 4: Absolute frequency of terms found in clinical records.
0 days16.5mm 9.8 cm
Maximum Tamoxifen Aspect-kind of quantity
Fixation-actionYear
SmallRight breast
Normal sizeSegmental mastectomy
12.0mmQuadrantectomy of breast Volume
Nipplesmonth ECHO protocol
6.0 months Lumpectomy of breast Rh positive (finding) 34.0GyTherapeutic procedure Ultrafiltration (procedure)
4.0mm
4.0 cm Breast 20.0m Surgical marginsMilligram/dayQuadrantectomy
2+ scoreDosage distance
Operative surgicalprocedures
Hormone therapy
200.0CgY cGy
Noninfiltrating intraductalcarcinomaCarcinomaMalignant neoplasmsUterine polyp
CONCDDESCCONCTDESC
1.7
1.2 1.4 1.6 1.8 2 2.2 2.4 2.6 2.8 3
Figure 5: Grouping by principal diseases.
architecture for text engineering and transforminginto the UMLS codification.
(ii) Each UMLS concept belongs to a hierarchical class,that is, the key of the Lynx system.There is a statisticalmodel that calculates the weight of the episodesanalyzing the “td/idf” frequency of each concept intoan episode, taking into account the weight of the classto which each concept belongs. A diagnosis does nothave the same weight compared to a treatment, a partof the body, a drug or compared to different combina-tions of different concepts. With our weighting algo-rithm the Lynx system selects all entries and choosesthemost relevant episodes, and,within them, it selectsthemain and secondary diseases for each episode (seeFigure 5). In addition, the relevant knowledge is notin the amount of concepts in a basic list with theirweights but how these concepts are related betweenthem. Each pair of concepts is transformed into a
relationship join (a graph), and a graph correspondsto a different category of information (e.g., diseases,symptoms and signs, or medicaments). In order tocreate this graph, we need to score in the ontologyconcepts in “triplets” according to a set of high levelrules defined in the inference system. In this way,the system is able to transform the plain databaseconcepts in a hierarchical semantic structure, frommedical annotation engine developed in the Lynxsystem.
So, the annotation process is as follows:
(i) Extract relevant tokens from sentences along differentepisodes in the whole health record (stop-words,dictionaries, translates, UMLS codes, etc.).
(ii) Assign the UMLS concepts to their principal classes.This research requires a proper mechanism to selectthem in order to support further tasks like adding

8 BioMed Research International
semantic rules by means of Semantic Web RuleLanguage (SWRL) and launching inference, settingbindings to terminologies, validating archetypes, andso forth. Thus, it should be noted that describingconstraints as human-readable comments should beavoided as far as possible given that they cannot beused by semantic reasoners.
(iii) Calculate the weight of each episode of the healthrecords and the weight of each concept into theepisode.
(iv) Calculate, from each set of sentences, when the textis talking about the same diagnosis, treatment, orprocedure and grouping sentences by principal orsecondary diseases.
With this plain information, we are able to transform theconcepts into a hierarchical (semantic) format, in order to
(i) annotate only the relevant information,(ii) present to the medical staff only the relevant relation-
ships between concepts,(iii) analyze unknown relationships between diseases,
procedures, treatments, and personal patient data asfamiliar issues, gender, age, demographic or econom-ical situations, personal context, drugs, and so forth,
(iv) detect unknown relationships between differentepisodes along the time; the statistical models,mainly on clinic records, lose knowledge if they donot take into account the evolution over time. Timeevolution is a variable which has not been deeplystudied within repetitive sets of data in the medicaldomain. the Lynx system uses machine learning withsliding windows to solve this issue [37].
5.2. UMLS Relations and Filling the Ontology. Once theconcepts are grouped by primary and secondary diseases,treatments, or procedures and extracted from a relationaldatabase, some semantic rules are executed to convert intriplets (sets of subject-predicate-object) the relationshipsfound in the different principal groups. In addition, eachtriplet is assigned to a principal disease, if it exits in the group,or to a secondary disease, depending on its content. Eachconcept in the clinical record belongs to a UMLS class (seeexamples of hierarchies in the table of Figure 6). Previously,statistical learning processes the entire corpus of EHR hasbeen carried out.With a weighting and association algorithmwe selected those classes or pairs of semantic types or relatedhierarchies with a minimal relevant gain to be taken intoaccount in the general summaries, as shown in Figure 6.
Each unique class or pair of semantic types is manuallyassigned to an annotation rule. Figure 7 shows this assig-nation. For example, the first line means that when in thesame sentence there is a type of concept named “acty” (whichmeans “activity”) and close to it there is another concept oftype “topp” (which in turns means “therapeutic procedure”),then the real instance in the ontology is that “patient” “hastreatment” “topp” (where “topp” is instanced bymeans of thetherapeutic procedure found in the text).
So the system is able to recognize the semantic types andto infer new semantic instances that are the real annotationsin the ontology. The system uses a reasoner engine (Pellet),so once all the semantic instances relating to the samegroup of diagnosis, treatment, or procedures are recordedin a temporal memory, the system runs several rules todetermine if the triplet within that group belongs to an earlierprincipal disease, that is, a newmain diagnosis or a secondarydiagnosis. Finally, all the triples processed are stored in theno-SQL structure and can be used directly for consultationsor queries by medical practitioners, almost in a naturallanguage format in the style of queries that can be similar andlinked to other platforms like “LinkedLifeData” [38], based onsemantic “endpoints” to access the information. There is alsoa web platform where doctors can analyze and summarizemedical history based on the dates of diagnoses and maintreatments, so that medical staff can see the evolution ofall patients in a graphic format and, secondly, see at aglance the diagnostic, procedures, treatments and relevantabnormalities of a patient in a digital format.
Reasons for sharing and reusing semantic (SWRL) rulesinclude the ones listed below:
(i) Interoperable decision support: the ability of systemsto reliably communicate with each other regardingclinical decision support, to encourage the devel-opment of interoperable mechanisms for triggeringcritical aids to decision making like alerts, remindersand monitoring tasks that improve effectiveness andreduce clinical risks.
(ii) Inheritable compatibility: given the archetypes’ capa-bility of being defined as specialization of moregeneral archetypes, a SWRL rule originally designedaccording to the OWL version of a parent archetypeis also applicable to derived archetypes.
(iii) Fostering semantics for clinical guidelines: the intro-duction of SWRL rules and inferential mechanismstogether with the archetypes expands the boundariesof the declarative knowledge that can be migratedfrom clinical guidelines to healthcare informationsystems. In this way, a means for standardized repre-sentation, reuse, and execution of the essential frag-ments of declarative knowledge contained in clinicalguidelines is provided.
(iv) Specialists’ empowerment: to enable domain rulesand guidelines to be modeled in a formal way bydomain experts. By defining the declarative knowl-edge they work with, they can gain direct control overtheir information systems.
(v) Consistency checking: rules integration can offer con-sistency checks to help guaranteeing data correctnessin EHR fragments.
(vi) Archetype validation: to support archetype validationand inconsistent restrictions detection.
(vii) Full semantic interoperability: for all abovemen-tioned reasons, integrating rules with clinical arche-types and EHR is an essential step towards extractingrelevant information into summaries.

BioMed Research International 9
Antecedent
Palpation0.055Support Item 1 Item 2
Free of attributemonthmenpmeddinpo
Shapes
Shapes
Shapes
Mammographyspcospcospcospcospcospcospcospcospcospco
bpocqnco
qnco
qncoqncoqnco
diap
diap
diap
topp
topp
topp
fndg
fndg
neopdsyn
Uterus
UterusVagina
Right breast
tmco
bpocbpocbpocbpocbpocbpocbpocbpoc
0.0480.0480.0480.0480.0480.048
0.0480.0480.0480.0480.048
0.048
0.1170.1100.090
0.0900.055
0.0550.055
0.055
0.055
0.062
0.062
0.0620.069
0.069
0.076
Free of attributeBodily secretions
GynecologyInspection-action
Right breast
Intravenous:Finding:Pointin time:Breast:Narrative:Radnuc
Area
Ganglia
Printing
Ambulatory care facilitiesPalpation
Vagina normalNormal size
Uterus
EmotionsVagina
Month
6.0 months
Control function
Uterus
Touch sensation
Colposcopy
Injury
Vagina normal
ShapesPrinting
Consequent
Views∧W radionuclide
GATE_length
Cervix Uteri
Figure 6: Minimal relevant gain between principal UMLS classes.
Figure 7: Annotation rule system.
The advantage of the system is that the rules for conceptweight calculation and for creation of relationships betweenconcepts, joined to the rules that determine whether adisease, treatment, or procedure is the principal or not in thecontext of the patient, are fully configurable by the medicalstaff, without computer, statistical, or semantic knowledge,therefore, in a very dynamic, elastic way, allowing a variation
of different medical contexts. Figure 8 shows the semantictool view of a clinical record in a semantic store, instantiatingthe ontology of Figure 3 with annotated values of a concretepatient. More specifically, Figure 8 shows how is instantiateda case of medical diagnostic (“diagnostic act”) through an“Atypical ductal hyperplasia” diagnostic in an adult witha “Quadritectomy of breast” treatment, and this medical

10 BioMed Research International
Figure 8: Clinical record in a semantic store (semantic tool view).
diagnostic corresponds to a “clinical-act” in the generalontology of Figure 3.
5.3. Joining the Summaries and Teleassistance Central Ontol-ogy. The ultimate goal of automatic summaries is to feed thetelecare platformwith themost relevant clinical data obtainedby an unassisted way from medical summaries and move thetherapeutics procedures, treatments, or medical recommen-dations from medical summaries to universAAL ontology.So, the anomaly engine and the predicting intentions engineare capable of learning about personal living habits of thepatients, highly correlated with their clinical conditions andprescriptions. To build this integration, thanks to semanticannotation process, we need only to join the most relevantconcepts (principal diseases, diagnosis, treatment, and proce-dures) in the control platform (see Figure 9) with a “same as”link between ontologies, by the paradigm of Linked Datarecommendations [39].
6. Central Ontology and Expert Rules System
Expert systems represent formal knowledge to solve humanproblems. This type of systems is applicable to any domainand is present today in nearly any application that requireshigh computational cost to automatize processes with somereasoning. Expert systems are suited to specific tasks whichrequire a lot of knowledge derived from a particular domainexperience as diagnostics, instructions, predictions, or adviceto real situations that arise and can also serve as training tools,mimicking the human behavior.
By their nature, the Semantic (Knowledge-Based) Man-agement Decision Support Systems (MDSS) work overstructured data representation (schema). The knowledge ispersistent in data-storages, and the expert knowledge (system
rules) is heuristic evidence based rules, with reasoningcapacity using an inference engine. This means that the rulesare well-known and always are true (an uncertainty factorin the MDSS systems by their definition is not possible,in principle). The use of the Resource Description Frame-work (RDF) standard (and thus its associated representationmachinery such as RDF schema and OWL) offers the pos-sibility of making inferences when retrieving and queryinginformation, in away very similar to humannatural language,being the advantage in query-answer systems. AlthoughOWL automated reasoning does not scale up for use inlarge knowledge bases, researchers and practitioners have justbegun to explore the problems and technical solutions whichmust be addressed in order to build a distributed system. Onthe other hand, there are nonknowledge-basedMDSS, whichlearn from raw data (semi/unstructured) and are based onprobabilistic techniques: patterns are taken as examples orcases in the past and the system has learning and probabilisticprediction capability.The direction of the last researches [40]is merging both engine capacities in a hybridmotor platform.
“Semantic smoothing for language modeling” emergedrecently as an important technique to improve probabilityestimations using document collections or ontologies, andthis was the way followed to design this system. This isthe technical way in this project. In Figure 10 we show thedeveloped two joined ontologies, that is, the “Home Care”ontology (right part) and the “Health Habits Recommenda-tion” ontology (left part). The sensor and the clinical recordssystem fill them automatically on real time processes, basedon a set of semantic rules.Therefore, the Expert Rules Systemhas two main goals:
(1) Fill the ontology with the sensor and clinical recordsraw data bymeans of “process rules.” Since these rules

BioMed Research International 11
Figure 9: Joining summaries and central ontologies.
are easy to adapt, alter, and maintain, this featuremakes them an attractive solution for nonexpertcaregivers. The caregiver is able to directly defineand modify the rules that specify the behavior of asystem in a given situation. For example, context-aware behaviors could be specified by a rich setof rules. In addition, the use of rules on top ofontologies can enable adaptive functionality that isboth transparent and controllable for users [41]. Someexamples of rules which are used to fill the “HealthHabits Recommendation” ontology are the following:
(a) Transformation of raw data into complex con-cepts, for example, “at noon in the kitchen overhalf an hour, the patient is eating.”
(b) Avoid data processing outside certain limits orthresholds set by the caregiver.
(c) Simple warning rules: more than 2 hours in thebathroom throws an alert.
(d) Medical inferences: “if cholesterol is more thana threshold, the patient is suffering from hyper-cholesterolemia.”
(2) Execute expert rules (see Figure 10, right bottompart)in order to suggest health recommendations to theelders or send alerts about abnormal situations aboutthe elder’s behaviors, by means of a set of “homecare rules.” Context-aware applications should con-tinuously monitor the elder’s environment in orderto detect changes and react to them. So, rule-basedarchitectures offer flexibility to tackle the variability ofthe environment and support the reconfiguration ofsystems according to changing needs without requir-ing reprogramming nor human intervention. Rule-based approaches are suitable for highly dynamiccontext-aware services [42].
Both set of rules are running over the ontologies witha semantic reasoner (Pellet), and the main advantage of thesystem is that it is open to future development: the functionsare out of the kernel code, and the program flow or thealarms system can be modified changing the rules; that is,it is not necessary to change the code of the system kernel.So, this can be done by an expert who does not necessarilyhave to be a programmer. Defining personalized and adaptiveelder interaction/behavior models is a key challenge whenconsidering the issue of analyzing or predicting elder inten-tions.The intention aware elderly care application can predictthe activities of the elder based on historic usual activity,profiting automatically the elder usual activity information.So, the system has a hybrid “inference engine” that joinsheuristics rules (first conditions to check without elder data)mainly with a supervised system, in order to discover newrules, adapting the heuristic rules to the personal behaviorchanging, with an unsupervised system, with two objectives:
(i) Detect unknown alerts (not registered in heuristicsnor supervised system).
(ii) Join similar users’ behaviors in homogeneous groups(segment usual activity, customizing automaticallythe user usual activity, state, or profile), in orderto send new extracted knowledge to the medicaland care agents about the general behavior of theirpatients.
In general, after the home installation, the inference machineruns the following tasks:
(i) Step 1: identification of the observable behaviors ofthe user.
(ii) Step 2: matching the heuristics rules to detect abnor-mal facts.

12 BioMed Research International
Figure 10: Ontologies and rules in the expert system.
(iii) Step 2: start the learning process during the learningperiod.
(iv) Step 3: put the learnt behavior model into practiceby applying the described process, modifying theheuristic general rules by heuristic personal rules.
(v) Finally, back to Step 1.Human actions are influenced by context, knowledge, orexperience of dependencies between actions and by expec-tations of how the situation is going to develop [43]. Forexample, if it is raining, even though it is summer, the elderprobably does not go outdoor unless he likes walking in therain. These subjective observations should be treated and theinference systemmust be able to learn these behaviors. In fact,the inference engine is an “Activity Tracker” system, and it isintended to track daily activities of the elderly via automaticor manual inputs. The real system uses some cases runningover the “Activity Tracker” for example:
(i) The system infers whether the elderly is eating at aspecific time of day. The indoor localization system isaware of the time of day and the amount of time thatthe elderly stays in the kitchen. Electrical applianceusage is also taken into account to infer if the elderlyhas been preparing his/her meal. Contact doors onkitchen furniture is also used to track this situation.
(ii) During the day, the system infers whether the elderlyis doing the housework. The indoor localizationsystem is aware of the time of day and the amount oftime that the elderly spends tracking his/her position.Vacuum cleaning can also be detected.
(iii) Physical exercise like hiking or strolling can bedetected through the GPS-enabled smart-phone ofthe elderly. The position, velocity, and path will beanalyzed tomeasure the amount of kilometers of eachday.

BioMed Research International 13
The “Activity Tracker” system provides three services for theelderly activities intention aware API:
(i) Current activity: it is the activity that the elderly isperforming at the present time.
(ii) Last 24 hour activities: they are the activities per-formed during the last 24 hours split into 15-minutetime slots.
(iii) Next 15-minute forecast activity: the next activitythat will perform the elderly based on the historicdata of the elderly intention is inferred. This horizonwas determined in a heuristic way, since 15 minutesis much more than enough for the purpose of thesystem, and the higher the horizon, the lower theaccuracy (in this and in all prediction systems).
This service provides the likelihood of the tracked activities tohappen and takes the activity whose probability of happeningis higher than the other ones.
7. Intention Detection System
The main task of the Intention Detection System is thedevelopment of decision trees that are running on centralserver and, based on information collected by differentsensors deployed in the home, make decisions about thestatus of the patients, depending on their health situation(extracted from clinical records), treatment procedures, levelof stress, behaviors, risk of exposure to harsh circumstances,and so forth. To do this, as exposed in Section 6, we havedeveloped an expert system which reflects the knowledge,about which is the best guideline of action as would beadvised by a specialist in the area.
As each home user could adapt differently to his envi-ronment and could have a recent history of actions thatinvolve a danger due to accumulation of negative elementsthat can affect him, it is important that the general rulesgenerated by experts adapt automatically to each user insidethe platform with implicit knowledge, so the system willpersonalize the information to each patient, their currentparameters, and their last actions, allowing elimination ofthe false positives. These supervised models exploit thereasoning power of expert system to derive new knowledgeand facts. The Intention Detection System reasons over thebase knowledge to infer new facts, resolves context conflicts,and maintains the consistence. The situation of a user isderived from his personal context, but the context is derivedfrom the aggregation of all the user’s situations plus theenvironment situation, too.
Through these techniques of intelligent information pro-cessing, we are given special emphasis on the detection andprediction of anomalies (trend analysis, deviations in thedata, etc.), such as lifestyle changes and poorly executedexercises.
One easy way to detect changes and behavior anomaliesis to compare the actual situation or state of the elderly withone prediction of his state. In this paper, is proposed a 24-hour sliding window that is analyzed with a decision tree (asupervised machine learning algorithm), in order to predict
the next user action over the time. For each time window, thedecision tree takes into account a multivariate set of valuesgenerating a predictive model (decision tree) and extracts thenext status of the user, with confidence and probability levels.
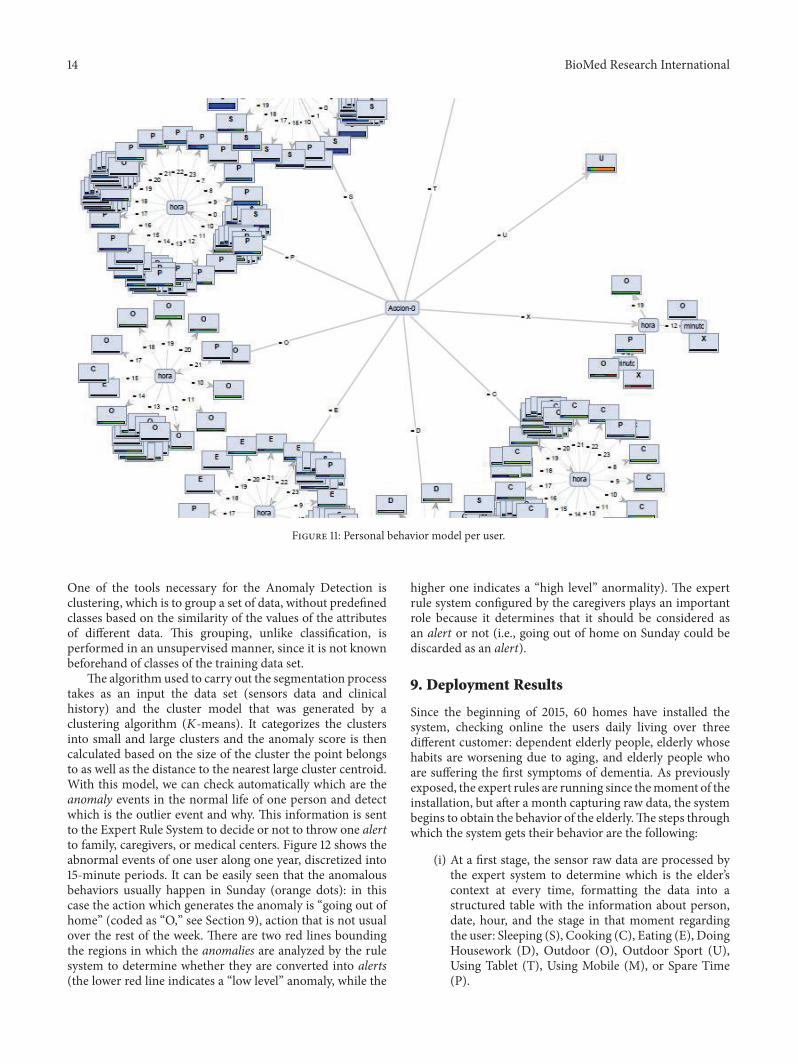
Compared to the current technology for evaluatingcontext-aware systems, we focus in particular on the quan-titative evaluation of each one of the rules of our rule-based system with a temporal data set. The challenge of thisproposal is a novel and distinctive base technology repositorythat has been developed in the treatment of time seriesand another algorithm repository for rule generation basedon probabilistic rules directly from RDF semantic systems,without human knowledge, and automatic insertion of theserules in the central ontology again, assigning weights to thesemantic confidence (triple-stores), in order to customizethe personal behaviors of each user. The described systemis proposed as a new development and addressing modeof the current telecare systems taking into account thecharacteristics and preferences of each person in such away that a personal behavior is built. For example, Figure 11shows the personal behavior model of a concrete elder. It is adecision tree, in which the main branch is the current action(Accion-0) carried out by the elder, being in themost of casesthe hour (hora), the second condition to check in order todetermine the future action (codified by a letter as explainedin Section 9).
8. Anomaly Detection System
Usually, interest driven analysis tends to overlook unexpectedpatterns in data. To avoid this inconvenience the systemcontains unsupervised algorithms (clustering and associ-ation models). Data Mining deals with applications suchas Anomaly Detection to prevent excessive consumption,pollution, escapes, and, in general, abnormal patterns of whatan expected profile for each segment is.
To detect anomalies, we use the Local Outlier Factor(LOF) algorithm [44]. The algorithm compares the densityof data instances around a given instance A with the densityaround A’s neighbors. If the former is low compared to thelatter, it means that A is relatively isolated; that is, it is anoutlier. Such outliers are considered anomalous. With theaim of identifying and grouping those outliers, they can beclassified by means of techniques based on statistical modelsor region density distances [45]:
(i) Statistical models: they are based on the field of statis-tics, given the premise of knowing the distribution ofdata. Based primarily on measurements of distancesbetween objects, the greater distance of the objectrelative to others is considered an anomaly.
(ii) Region density distances: based on the estimation ofdensity of objects, the objects located in regions oflowdensity and relatively distant from their neighborsare considered anomalous. The main feature is thatgenerally it is considered unsupervised learning anda score is assigned to each instance that reflects thedegree to which the instance is anomalous.
14 BioMed Research International
Figure 11: Personal behavior model per user.
One of the tools necessary for the Anomaly Detection isclustering, which is to group a set of data, without predefinedclasses based on the similarity of the values of the attributesof different data. This grouping, unlike classification, isperformed in an unsupervised manner, since it is not knownbeforehand of classes of the training data set.
The algorithm used to carry out the segmentation processtakes as an input the data set (sensors data and clinicalhistory) and the cluster model that was generated by aclustering algorithm (𝐾-means). It categorizes the clustersinto small and large clusters and the anomaly score is thencalculated based on the size of the cluster the point belongsto as well as the distance to the nearest large cluster centroid.With this model, we can check automatically which are theanomaly events in the normal life of one person and detectwhich is the outlier event and why. This information is sentto the Expert Rule System to decide or not to throw one alertto family, caregivers, or medical centers. Figure 12 shows theabnormal events of one user along one year, discretized into15-minute periods. It can be easily seen that the anomalousbehaviors usually happen in Sunday (orange dots): in thiscase the action which generates the anomaly is “going out ofhome” (coded as “O,” see Section 9), action that is not usualover the rest of the week. There are two red lines boundingthe regions in which the anomalies are analyzed by the rulesystem to determine whether they are converted into alerts(the lower red line indicates a “low level” anomaly, while the
higher one indicates a “high level” anormality). The expertrule system configured by the caregivers plays an importantrole because it determines that it should be considered asan alert or not (i.e., going out of home on Sunday could bediscarded as an alert).
9. Deployment Results
Since the beginning of 2015, 60 homes have installed thesystem, checking online the users daily living over threedifferent customer: dependent elderly people, elderly whosehabits are worsening due to aging, and elderly people whoare suffering the first symptoms of dementia. As previouslyexposed, the expert rules are running since themoment of theinstallation, but after a month capturing raw data, the systembegins to obtain the behavior of the elderly.The steps throughwhich the system gets their behavior are the following:
(i) At a first stage, the sensor raw data are processed bythe expert system to determine which is the elder’scontext at every time, formatting the data into astructured table with the information about person,date, hour, and the stage in that moment regardingthe user: Sleeping (S), Cooking (C), Eating (E), DoingHousework (D), Outdoor (O), Outdoor Sport (U),Using Tablet (T), Using Mobile (M), or Spare Time(P).

BioMed Research International 15
Diasem3
4
5
6
7
1
2
0.30
0.35
0.40
0.45
0.50
0.55
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
1.05
1.10
1.15A
nom
aly
2,500 32,50030,00010,000 12,500 15,000 25,00020,000 35,0000 27,50017,5007,5005,000 22,500idv
Figure 12: Anomaly Detection System.
(ii) At the same time, the system checks the physiologicalstatus of the users, as temperature, heart pulse, bloodpressure, and so forth. In this way the data willbe managed more compactly and only the relevantinformation to the alerts is managed (e.g., “the elderlyhas a fever unusual at 08:02 more than 15 minutes”).Initially the thresholds that are in the table are definedmanually by the doctors (e.g., a temperature of36,5∘C), leaving the detection of statistical thresholdsfor later, where the average temperature threshold ismodified by historical and statistical processes andunsupervised algorithms.These thresholds are able tomodify the medical rules directly regarding the userpersonal historical set.
(iii) The system also checks environmental sensors, suchas smoke, temperature, and humidity, throwing alertswhen activated.
(iv) At every moment, the system is taking external datato integrate them into users data, with a number ofvalues: Haze (C), Fog (N), Low Fog (N), Fog (I),Precipitation (P), Drizzle (L), Rain (U), Torn Rain(V), Tornado Sight (R), Rain Shower (H), Rain (E),Snow (E), Shower Hail (T), and Freezing Rain (T).
The first conclusion, as expected, is that the outdoor weatherconditions are themost relevant in order to predict whichwillbe the user behavior, in second correlation place (by a ChiSquared statistical test), after the hour of the stage, but beforeother indicators such as the day week, or even the month ofaction. With the temporal sliding windowmethod, including
the last action in order to predict the new stage of the user, theaccuracy trust by the system using cross-validation is about81,80%, as shown in Table 2.
Thus, it is shown that external data on local weather anddata from past actions are representative to make predictionsabout the future status of the elderly immediately. Thus, ifthe prediction state does not match with the actual state andthis situation has a significant score, the system sends analert to remote care services to immediately launch protocols.On the other hand, the anomaly clustering method used is acomplement to the supervised system, in order to detect notso usual behaviors.
10. Conclusions and Future Work
In this paper, we have introduced a behavior predictionsystem to be used in anhome telecare platform. Suchplatformis an assisted living system for monitoring elderly peopleat their homes, with the final aim of providing a robust,easily deployable, and cost-contained solution to ensurethe safety of the elderly. It obtains both physiological andenvironmental data through a multisensor infrastructure,connecting the homewith both the carer and the family, beingaware of the state of the elderly.
Our next steps in the closed future are two: on one hand,to transform this validated system into a reference product inthemarket of home telecare platforms and, on the other hand,reinforce the intelligent systems for analysis of anomaliesand behaviors taking advantage of the health informationto detect how the clinical records, medical diagnoses, and

16 BioMed Research International
Table 2: Confusion matrix with previous stages.
Accuracy: 81.80%True S True P True E True T True O True C True D True U True X Class precision
Pred. S 7404 270 9 2 74 23 0 0 3 95.11%Pred. P 313 2318 136 51 66 207 23 2 0 74.39%Pred. E 16 175 851 84 6 68 124 0 0 64.27%Pred. T 0 73 17 994 126 27 6 38 1 77.54%Pred. O 0 87 44 6 843 119 1 72 14 71.08%Pred. C 36 197 244 42 3 1321 56 0 0 69.56%Pred. D 2 25 0 83 8 75 345 0 0 64.13%Pred. U 0 28 2 0 59 33 2 242 5 65.23%Pred. X 0 0 0 0 1 0 0 3 2 33.33%Class recall 95.28% 73.05% 65.31% 78.76% 71.08% 70.53% 61.94% 67.79% 8.00%
treatments are affecting the usual behavior of different patientprofiles in their daily lives, specially, at home, and if thesetreatments are appropriate or not.
Finally, as a medium term step, we are researching on thechallenge of creating a new method for automatic big dataanalysis over the medical summaries (obtained from clinicalrecords, usually written in plain text natural language), inorder to discover new relationships betweendiseases,medicalprocedures, treatments, and their correlation with homepersonalized medicine.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgments
The research was supported by the REAAL Project (CIPICT PSP – 2012 - 325189), the ASK-MED Project (Aggre-gated Semantic Knowledge Medical), a Gaitek Program byThe Basque Country Government. Thanks are due to theOnkologikoa (http://www.onkologikoa.com/) medical stafffor their support regarding the medical summaries valida-tions.Without their valuable assistance the work described inthis paper would not have been possible. The ComputationalIntelligence Group is funded by the BasqueGovernment withGrant IT874-13. Manuel Grana was supported by EC underFP7, Coordination and Support Action, Grant Agreementno. 316097, ENGINE European Research Centre of NetworkIntelligence for Innovation Enhancement.
References
[1] M. Darwish, E. Senn, C. Lohr, and Y. Kermarrec, “A comparisonbetween ambient assisted living systems,” in Smart Homes andHealth Telematics, C. Bodine, S. Helal, T. Gu, and M. Mokhtari,Eds., vol. 8456 of LectureNotes in Computer Science, pp. 231–237,Springer, 2015.
[2] EIP-AHA, “EIP-AHA operational plan: final text adopted bythe steering group on 7/11/11,” 2011, http://ec.europa.eu/active-healthy-ageing.
[3] S. Giroux, J. Bauchet, H. Pigot, D. Lussier- Desrochers, andY. Lachappelle, “Pervasive behavior tracking for cognitiveassistance,” in Proceedings of the 1st International Conferenceon Pervasive Technologies Related to Assistive Environments(PETRA ’08), ACM, Corfu Island, Greece, June-July 2008.
[4] H. Medjahed, D. Istrate, J. Boudy, and B. Dorizzi, “A fuzzylogic system for home elderly people monitoring (EMUTEM),”in Proceedings of the 10th WSEAS International Conferenceon Fuzzy Systems (FS ’09), pp. 69–75, World Scientific andEngineering Academy and Society (WSEAS), Prague, CzechRepublic, March 2009.
[5] C.-N. Huang and C.-T. Chan, “A zigbee-based location-awarefall detection system for improving elderly telecare,” Interna-tional Journal of Environmental Research and Public Health, vol.11, no. 4, pp. 4233–4248, 2014.
[6] R. Igual, C. Medrano, and I. Plaza, “Challenges, issues andtrends in fall detection systems,”BioMedical EngineeringOnline,vol. 12, no. 1, article 66, 2013.
[7] N. Pannurat, S. Thiemjarus, and E. Nantajeewarawat, “Auto-matic fallmonitoring: a review,” Sensors, vol. 14, no. 7, pp. 12900–12936, 2014.
[8] G. Pravettoni, R. Folgieri, and C. Lucchiari, “Cognitive sciencein telemedicine: from psychology to artificial intelligence,” inTele-oncology, G. Gatti, G. Pravettoni, and F. Capello, Eds.,TELe-Health, pp. 5–22, Springer International, 2015.
[9] K. Wang, Y. Shao, L. Shu, G. Han, and C. Zhu, “LDPA: alocal data processing architecture in ambient assisted livingcommunications,” IEEE Communications Magazine, vol. 53, no.1, pp. 56–63, 2015.
[10] M. Lustrek, B. Kaluza, B. Cvetkovic et al., “An agent-basedapproach to care in independent living,” inAmbient Intelligence,B. de Ruyter, R. Wichert, D. Keyson et al., Eds., vol. 6439 ofLecture Notes in Computer Science, pp. 177–186, Springer, Berlin,Germany, 2010.
[11] J. M. Lopez-Guedea, A. Moreno-Fernandezde Leceta, and M.Grana, Behavior Prediction in Home Telecare Systems, 2015.
[12] N. F. Noy and D. L. McGuinness, Ontology Development 101:A Guide to Creating Your First Ontology, Stanford University,Stanford, Calif, USA, 2001.
[13] T. Gross and M. Specht, “Awareness in context-aware informa-tion systems,” in Mensch & Computer 2001, H. Oberquelle, R.Oppermann, and J. Krause, Eds., vol. 55 of Berichte des German

BioMed Research International 17
Chapter of the ACM, pp. 55–173, Vieweg+Teubner, Wiesbaden,Germany, 2001.
[14] M. Lustrektrek, B. Kaluza, E. Dovgan, B. Pogorelc, and M.Gams, “Behavior analysis based on coordinates of body tags,” inAmbient Intelligence, M. Tscheligi, B. de Ruyter, P. Markopouluset al., Eds., vol. 5859 of Lecture Notes in Computer Science, pp.14–23, Springer, Berlin, Germany, 2009.
[15] A. Lugmayr, T. Risse, B. Stockleben, K. Laurila, and J. Kaario,“Semantic ambient media—an introduction,”Multimedia Toolsand Applications, vol. 44, no. 3, pp. 337–359, 2009.
[16] M. J. Arif, I. M. M. El Emary, and D.-D. Koutsouris, “A reviewon the technologies and services used in the self-management ofhealth and independent living of elderly,”Technology andHealthCare, vol. 22, no. 5, pp. 677–687, 2014.
[17] UPnP, “Upnp open development tools,” http://pupnp.source-forge.net/.
[18] UniversAAL, http://universaal.org/.[19] A. Moreno-Fernandez-de-Leceta, P. la Pena, D. Barrios, B.
Granciaenteparaluceta, J. Lopez-Guede, and M. Grana, “Anautomatic telemonitoring system for elderly people at home,”International Journal of Sensors Wireless Communications andControl, vol. 4, no. 2, pp. 57–66, 2015.
[20] A. Moreno-Fernandez-de-Leceta, U. A. Gomez, J. M. Lopez-Guede, and M. Grana, “Real implantation of an expert systemfor elderly home care,” in Hybrid Artificial Intelligent Systems,E. Onieva, I. Santos, E. Osaba, H. Quintian, and E. Corchado,Eds., vol. 9121 of Lecture Notes in Computer Science, pp. 668–678, Springer, 2015.
[21] G. Acampora, D. J. Cook, P. Rashidi, and A. V. Vasilakos, “Asurvey on ambient intelligence in health care,” Proceedings of theIEEE, vol. 101, no. 12, pp. 2470–2494, 2013.
[22] J. F. Sowa, Principles of Semantic Networks: Explorations in theRepresentation of Knowledge, Morgan Kaufmann Publishers,San Mateo, Calif, USA, 1991.
[23] T. Garcia-Valverde, A. Munoz, F. Arcas, A. Bueno-Crespo, andA. Caballero, “Heart health risk assessment system: a nonin-trusive proposal using ontologies and expert rules,” BioMedResearch International, vol. 2014, Article ID 959645, 12 pages,2014.
[24] I. Merelli, H. Perez-Sanchez, S. Gesing, and D. D’Agostino,“Managing, analysing, and integrating big data in medi-cal bioinformatics: open problems and future perspectives,”BioMed Research International, vol. 2014, Article ID 134023, 13pages, 2014.
[25] K.U. Idehen, “Virtuoso, the prometheus of RDF—sematics 2014conference keynote,” in Proceedings of the 10th InternationalConference on Semantic Systems, Leipzig, Germany, September2014, http://www.slideshare.net/kidehen/ogl-semantic-leipzigse-mantics2014.
[26] HCLSIG, Hclsig semantic web for health care and life sciencesinterest group, http://www.w3.org/wiki/HCLSIG.
[27] N. S. Abdul Karim,M.Ahmad, andN.Mohamed, “A frameworkfor electronic health record (EHR) implementation impacton system service quality and individual performance amonghealthcare practitioners,” in Proceedings of the 10th WSEASInternational Conference on E-Activities (E-ACTIVITIES ’11),pp. 197–201, World Scientific and Engineering Academy andSociety (WSEAS), Jakarta, Indonesia, December 2011.
[28] L. L. Matıas, Combining ontologies and rules with clinicalarchetypes [Ph.D. dissertation], University of Alcala, Alcala deHenares, Spain, 2011.
[29] N. Evans, Older Adults and Their Care, 2008, http://www.nurs-ingceu.com/courses/251/.
[30] K. Krishnamurthi, V. R. P. Griet, and V. V. B. Jntuh, “Capturingthe semantic structure of documents using summaries insupplemented latent semantic analysis,” WSEAS Transactionson Computers, vol. 14, article 32, pp. 314–323, 2015.
[31] H. Eriksson, A. R. Puerta, and M. A. Musen, “Generation ofknowledge-acquisition tools from domain ontologies,” Interna-tional Journal of Human-Computer Studies, vol. 41, no. 3, pp.425–453, 1994.
[32] H. Chen, X. Chen, P. Gu, Z. Wu, and T. Yu, “OWL reasoningframework over big biological knowledge network,” BioMedResearch International, vol. 2014, Article ID 272915, 16 pages,2014.
[33] D. Russler,M.Moores, H. Chen et al.,RDF/OWLRepresentationof HL7/RIM V3.0, 2008.
[34] MetaMap, http://mmtx.nlm.nih.gov/.
[35] K. C. Lin, Y. C. Long, and H. C. Tsai, “Developing knowledge-based emr services using semantic web technology,” Journal ofInternet Technology, vol. 16, no. 3, pp. 403–414, 2015.
[36] M. Kreuzthaler, P. Daumke, and S. Schulz, “Semanticretrieval and navigation in clinical document collections,”in eHealth2015—Health Informatics Meets eHealth, vol. 212 ofStudies in Health Technology and Informatics, pp. 9–14, IOSPress, Amsterdam, The Netherlands, 2015.
[37] C. Ahlin, D. Stupica, F. Strle, L. Lusa, and Y. Xue, “medplot: aweb application for dynamic summary and analysis of longitu-dinal medical data based on R,” PLoS ONE, vol. 10, no. 4, ArticleID e0121760, 2015.
[38] M. R. Kamdar, D. Zeginis, A. Hasnain, S. Decker, and H.F. Deus, “ReVeaLD: a user-driven domain-specific interactivesearch platform for biomedical research,” Journal of BiomedicalInformatics, vol. 47, pp. 112–130, 2014.
[39] D. Damljanovic, M. Stankovic, and P. Laublet, “Linked data-based concept recommendation: comparison of different meth-ods in open innovation scenario,” inTheSemanticWeb: Researchand Applications: 9th Extended Semantic Web Conference,ESWC 2012, Heraklion, Crete, Greece, May 27–31, 2012. Proceed-ings, vol. 7295 of Lecture Notes in Computer Science, pp. 24–38,Springer, Berlin, Germany, 2012.
[40] X. Zhou, X. Zhang, and X. Hu, “Semantic smoothing of doc-ument models for agglomerative clustering,” in Proceedings ofthe 20th International Joint Conference on Artificial Intelligence(IJCAI ’07), pp. 2922–2927, Hyderabad, India, January 2007.
[41] L. Aldin and S. de Cesare, “A literature review on businessprocess modelling: new frontiers of reusability,” EnterpriseInformation Systems, vol. 5, no. 3, pp. 359–383, 2011.
[42] L. Daniele, P. Dockhorn Costa, and L. Ferreira Pires, “Towardsa rule-based approach for context-aware applications,” inDependable and Adaptable Networks and Services, A. Pras andM. van Sinderen, Eds., vol. 4606 of Lecture Notes in ComputerScience, pp. 33–43, Springer, Berlin, Germany, 2007.
[43] J. Noyes, “Human reliability analysis: context and control byHollnagel, E,” Ergonomics, vol. 38, no. 12, pp. 2614–2615, 1995.

18 BioMed Research International
[44] M. M. Breunig, H. P. Kriegel, R. T. Ng, and J. Sander, “Lof:identifying densitybased local outliers,” in Proceedings of theACM SIGMOD International Conference on Management ofData (SIGMOD ’00), pp. 93–104, Dallas, Tex, USA, May 2000.
[45] A. Singh and J. Nocerino, “Robust procedures for the identifi-cation of multiple outliers,” in Chemometrics in EnvironmentalChemistry—Statistical Methods, J. Einax, Ed., vol. 2/2G of TheHandbook of Environmental Chemistry, pp. 229–277, SpringerBerlin Heidelberg, 1995.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com


















