
Research Article Effects of Functional Limb Overloading on ......Research Article Effects of...
46
Research Article Effects of Functional Limb Overloading on Symmetrical Weight Bearing, Walking Speed, Perceived Mobility, and Community Participation among Patients with Chronic Stroke Sami S. Alabdulwahab, 1 Fuzail Ahmad, 2 and Harpreet Singh 3 1 Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh 11952, Saudi Arabia 2 Department of Physical erapy & Health Rehabilitation, College of Applied Medical Sciences, Majmaah University, Al-Majmaah 11451, Saudi Arabia 3 Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, New Delhi 110029, India Correspondence should be addressed to Fuzail Ahmad; [email protected] Received 19 May 2015; Revised 3 September 2015; Accepted 30 September 2015 Academic Editor: Ching-Yi Wu Copyright © 2015 Sami S. Alabdulwahab et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Stroke is a leading cause for long-term disability that oſten compromises the sensorimotor and gait function accompanied by spasticity. Gait abnormalities persist through the chronic stages of the condition and only a small percentage of these persons are able to walk functionally in the community. Material and Method. Patients with chronic stroke were recruited from outpatient rehabilitation unit at Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, having a history of first stroke at least six months before recruitment, with unilateral motor deficits affecting gait. e patients were randomly assigned to either the functional limb overloading (FLO) or Limb Overloading Resistance Training (LORT) group and provided four weeks of training. Result. We found that there was an improvement in gait performance, weight bearing on affected limb, and perceived mobility and community participation. Conclusion. To the best of our knowledge, this is the first study that has evaluated the effects of functional limb overloading training on symmetric weight bearing, walking ability, and perceived mobility and participation in chronic hemiplegic population. e study demonstrated a beneficial effect of training on all the outcomes, suggesting that the functional limb overloading training can be a useful tool in the management of gait problems in chronic stroke patients. 1. Introduction Stroke is becoming a rapidly increasing problem and an important cause of disability and deaths worldwide. Inci- dence and prevalence of strokes in Saudi Arabia are compar- atively lower than western countries, which could be because of the predominance of the younger age groups in this region [1]. e annual stroke incidence ranged from 27.5 to 63 per 100,000 population and prevalence ranged from 42 to 68 per 100,000 population [2]. Stroke is a leading cause for long-term disability due to compromised sensorimotor function. Approximately 85% of stroke survivors learn to walk independently by 6 months aſter stroke, but gait abnormalities persist throughout the chronic stages of the condition. Only a small percentage of stroke survivors are able to walk functionally in the community [3, 4]. e objective of stroke rehabilitation is to enable individ- ual patients to maximize benefits from training in order to attain the highest possible degree of physical and psychologi- cal performance. e ultimate goals for many stroke patients are to achieve a level of functional independence necessary for returning home and to integrate as fully as possible into community life. Ng and Hui-Chan [5] have noted that weakness in hemiplegic stroke patients is sometimes overshadowed over concerns about treatment of spasticity and synergistic move- ments. Studies have revealed positive correlations between Hindawi Publishing Corporation Rehabilitation Research and Practice Volume 2015, Article ID 241519, 6 pages http://dx.doi.org/10.1155/2015/241519
Transcript of Research Article Effects of Functional Limb Overloading on ......Research Article Effects of...

Research ArticleEffects of Functional Limb Overloading on SymmetricalWeight Bearing, Walking Speed, Perceived Mobility, andCommunity Participation among Patients with Chronic Stroke
Sami S. Alabdulwahab,1 Fuzail Ahmad,2 and Harpreet Singh3
1Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh 11952, Saudi Arabia2Department of Physical Therapy & Health Rehabilitation, College of Applied Medical Sciences, Majmaah University,Al-Majmaah 11451, Saudi Arabia3Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, New Delhi 110029, India
Correspondence should be addressed to Fuzail Ahmad; [email protected]
Received 19 May 2015; Revised 3 September 2015; Accepted 30 September 2015
Academic Editor: Ching-Yi Wu
Copyright © 2015 Sami S. Alabdulwahab et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Stroke is a leading cause for long-term disability that often compromises the sensorimotor and gait functionaccompanied by spasticity. Gait abnormalities persist through the chronic stages of the condition and only a small percentageof these persons are able to walk functionally in the community.Material and Method. Patients with chronic stroke were recruitedfrom outpatient rehabilitation unit at Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, having ahistory of first stroke at least sixmonths before recruitment, with unilateral motor deficits affecting gait.The patients were randomlyassigned to either the functional limb overloading (FLO) or Limb Overloading Resistance Training (LORT) group and providedfour weeks of training. Result. We found that there was an improvement in gait performance, weight bearing on affected limb,and perceived mobility and community participation. Conclusion. To the best of our knowledge, this is the first study that hasevaluated the effects of functional limb overloading training on symmetric weight bearing, walking ability, and perceived mobilityand participation in chronic hemiplegic population. The study demonstrated a beneficial effect of training on all the outcomes,suggesting that the functional limb overloading training can be a useful tool in the management of gait problems in chronic strokepatients.
1. Introduction
Stroke is becoming a rapidly increasing problem and animportant cause of disability and deaths worldwide. Inci-dence and prevalence of strokes in Saudi Arabia are compar-atively lower than western countries, which could be becauseof the predominance of the younger age groups in this region[1]. The annual stroke incidence ranged from 27.5 to 63 per100,000 population and prevalence ranged from 42 to 68 per100,000 population [2].
Stroke is a leading cause for long-term disability due tocompromised sensorimotor function. Approximately 85% ofstroke survivors learn to walk independently by 6 monthsafter stroke, but gait abnormalities persist throughout the
chronic stages of the condition. Only a small percentageof stroke survivors are able to walk functionally in thecommunity [3, 4].
The objective of stroke rehabilitation is to enable individ-ual patients to maximize benefits from training in order toattain the highest possible degree of physical and psychologi-cal performance. The ultimate goals for many stroke patientsare to achieve a level of functional independence necessaryfor returning home and to integrate as fully as possible intocommunity life.
Ng and Hui-Chan [5] have noted that weakness inhemiplegic stroke patients is sometimes overshadowed overconcerns about treatment of spasticity and synergistic move-ments. Studies have revealed positive correlations between
Hindawi Publishing CorporationRehabilitation Research and PracticeVolume 2015, Article ID 241519, 6 pageshttp://dx.doi.org/10.1155/2015/241519

2 Rehabilitation Research and Practice
the strength of specific muscle groups and a variety of func-tional attributes [6]. Furthermore, a nonlinear relationshipbetween walking performance and muscle strength in thelower extremities has been suggested [7]. However, as theprotocols were multifaceted, it was not possible to determinethe precise role that the strength-training component mayhave played in improving walking function.
A number of studies have shown that task specificity andintensity of training are the main determinants of functionalimprovement after stroke [6, 8, 9].Moreover, there is growingevidence suggesting that intensive task-oriented practice caninduce greater improvement in walking competency thanusual practice in stroke survivors [10–12].
Yang et al. [13] in their study on stroke patients under-going progressive lower limb strengthening using functionalweight bearing activities foundmoderate increases inwalkingspeed. Sullivan et al. [14] found that task-specific trainingwith body-weight support is more effective in improvingwalking speed but lower limb strength training did notprovide any added benefit to walking outcomes.
A major limitation to the conclusions from these studiesand systematic reviews is the lack of consistency in theintervention and specified protocols [15–17]. Despite thenumber of studies dedicated to task-oriented training, noneof these studies had combined functional task training withprolonged resistance in the form of limb overloading applied90% of the awake time. Therefore, we designed this studyto address the evidence related to our training protocol toenhance symmetric weight bearing andwalking speed and itsimpact on perceived mobility and community participationin patients with chronic stroke.
We hypothesized that intervention programs that com-bine lower limb overload with functional task training wouldbe more effective at improving walking outcomes and com-munity participation than lower limboverload training alone.
Thedesign of our studywas influenced by the literature onlower extremity strength training and task-specific locomotortraining [14, 18, 19]. The use of this design should providevaluable comparisons that reveal the practical benefits offunctional limb overloading training to improve walkingoutcomes after stroke and its effect on perceived communityparticipation.
2. Material and Method
Chronic stroke patients were recruited from outpatient reha-bilitation unit at Department of Neurology & Neurosurgery,All India Institute of Medical Sciences. Patient having; (a)history of first stroke at least six months before recruitment,with unilateral motor deficits affecting gait pattern and/orspeed, (b) independent walking ability with or withoutwalking aid for at least 10m, and (c) ability to perform closed-chain exercise were selected for the study. Exclusion criteriaincluded significant psychiatric or cognitive deficits, majorcardiorespiratory diseases, chronic pain, or lower limb jointscomplication.
Study protocols were explained to patients and writteninformed consent was obtained from them. The patientswere then randomly assigned to either the functional limb
overloading (FLO) group or Limb Overloading ResistanceTraining (LORT) group by drawing one of two sealedenvelopes designating the group membership.
3. Management Protocol
The patients in FLO group underwent task-oriented gaittraining of one-hour duration three times per week forfour weeks. They were requested to wear the weight cuff,equivalent to 5% of the total body weight, for most of theirawake time (approximately 90% of the time). Brown et al.[18] in their study used 15% of the body weight for limboverloading during a cycling task. As our study required thepatients towearweighted cuffmost of their awake time and toperform functional taskswearing these cuffs, therefore, after apilot trial on few patients, we settled for 5%of the bodyweight(3–5Kg), which patients tolerated without much distress.
During the training session, after 5–10 minutes of simplewarm-up exercises, the patients performed various func-tional activities including forward, sideways, and backwardwalking, turning to 90 and 180 degrees during walking, stairclimbing, and so forth. During each session the patientswere also made to walk on treadmill for 15 minutes at speedof 10% above comfortable walking. The progression of thetraining was done by increasing the loading or steps height,or by reducing the speed, or decreasing the patient’s supportand/or doing more individually tailored sets, but as a rule thedifficulty level was adjusted after six sessions.
The patients in the LORT group underwent resistance-training regime consisting of isotonic exercise using weightcuff tied to ankle or foot.The exercise algorithmwas designedby the therapist accounting for strength as well as movementsynergy level, to determine repetition maximum (RM) withthe given load. The training protocol required each partici-pant to isotonically exercise the affected lower extremity (LE)using external resistance of weight cuff, equivalent to 5%of the total body weight. The training session consisted of5–10 minutes of simple warm-up exercises and then threesets of 10–15 repetitions maximum, to moderate fatiguewith limb overloading. The therapist follows an exercisealgorithm that accounted for the participant’s strength aswell as movement synergy level to determine RM for specificmuscle groups, including hip flexors, hip extensors, kneeflexors, knee extensors, ankle dorsiflexors, and ankle plantarflexors, with the given weight.
The outcomemeasures taken for this studywere Cadence,Fast Gait Speed (FGS), Slow Gait Speed (SGS), weightbearing on affected limb (WBAL), and perceived mobilityand participation of stroke patients.
The Walkway gait analysis system (TekScan, USA) wasused to capture plantar pressure data and temporal (time)and spatial (distance) gait parameters. This system consistsof a 5mm thickness of floor mat composed of 2,288 resistivesensors, with a resolution of 1.4 sensors/cm2, a sensor matrixmeasuring 439.5mm by 369.9mm, and a sampling frequencyof 40Hz.
Perceivedmobility and participation were assessed by thestroke impact scale (SIS) which is a self-report questionnaire

Rehabilitation Research and Practice 3
that assesses aspects of the impact of a stroke on an indi-vidual’s self-perceived health [20]. Interrater reliability andconcurrent validity have been found to be good for SIS [21].For our study, we have used only mobility and participationdomain of SIS. For each subject, the mean scores of itemsfrom mobility and participation section were calculatedand converted into percentage. High values represent noor few restrictions in participation and low values indicateparticipation that is more restricted.
An unequal group pretest-posttest design was used andthe group comparisons at baseline and after interventionwereanalysed using a 𝑡-test. An alpha level set at 0.05 determinedsignificance in two-sided hypothesis testing.
All analyses were performed using SPSS version 20.0.
4. Results
Twenty-six patients participated in this study. Three patientsin LORT group dropped out due to motivational reasons.
The mean age of the participants was 45.2 ± 12.5, 78% ofthem were male, and the remaining 22% were female. About44% of the participants had left side hemiplegia and 56% ofthem had right side hemiplegia (Table 1).
All the participants had stroke at least six months priorlywith a mean duration of 16 ± 10 months, unilateral motordeficits affecting gait, independent walking ability with orwithout walking aid, and ability to perform closed-chainexercise.
Table 2 shows the patient characteristics of both groupsat baseline. No statistically significant differences betweenboth groups were found with respect to the selected outcomevariables. No statistically significant differences were found(𝑝 < 0.05) with respect to measurement of Cadence, SGS,FGS, WBAL, and SIS.
Cadence showed an improvement of 33% (𝑡 = 5.03, 𝑝 =0.001∗) and 28% (𝑡 = 2.34, 𝑝 = 0.044∗) in FLO and LOTR
group, respectively, which were statistically significant.The posttest values of SGS suggested an increase of 47%
(𝑡 = 3.62, 𝑝 = 0.004∗) and 32% (𝑡 = 2.6, 𝑝 = 0.029∗),respectively, in FLO and LOTR groups. However the FastGait Speed (FGS) improved by 34% (𝑡 = 4.68, 𝑝 = 0.001∗)and 21% (𝑡 = 2.28, 𝑝 = 0.049∗), respectively, in the FLOand LOTR groups. These improvements were found to bestatistically significant (Tables 3 and 4).
To find the difference between both groups an indepen-dent 𝑡-test was used which showed 19.4% (𝑡 = 2.45, 𝑝 =0.024∗) improvement in Cadence, 55.3% (𝑡 = 2.81, 𝑝 =
0.011∗) improvement in SGS, 45% (𝑡 = 2.47, 𝑝 = 0.023∗)
improvement in FGS, 12.8% (𝑡 = 2.19, 𝑝 = 0.040∗)improvement in WBAL, and 14.3% (𝑡 = 2.27, 𝑝 = 0.046∗)improvement in SIS scores after training (Table 5, Figure 1).
Posttraining weight bearing on affected limb improvedsignificantly by 11% (𝑡 = 2.75, 𝑝 = 0.018∗) in FLO group,while very little improvement in LORT group was detected.
Perceived mobility and community participation signif-icantly improved to 16% in the FLO group (𝑡 = 2.69, 𝑝 =0.020∗). In contrast, they showed insignificant improvement
(6%) in LORT group (𝑡 = 1.71, 𝑝 = 0.121). (Table 5,Figure 1).
Table 1: Descriptive statistics.
%GenderFemale 21.7Male 78.3
Side affectedLeft side 43.5Right side 56.5
Duration since stroke onset6–12 months 30.41-2 years 56.52-3 years 13.0
Table 2: Between-group comparison of the dependent variable atbaseline.
Variables FLO LORT Independent 𝑡-test𝑁 = 13 𝑁 = 10 𝑡 𝑝
Age 45.3 + 12.3 44.7 + 14.1 0.12 0.911Cadence 61.1 + 12.2 53.4 + 15.4 0.98 0.161SGS (m/s) 31.9 + 15.9 22.8 + 11 1.50 0.149FGS (m/s) 59.8 + 26.2 45.5 + 17.7 1.58 0.131WBAL 40.2 + 6.9 38.4 + 8.2 0.31 0.759SIS 55.6 + 7 53.1 + 10.4 0.91 0.376SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
Table 3: Within-group comparison of the dependent variable inFLO group.
VariablesPretest Posttest PairedM ± SD M ± SD 𝑡-test𝑁 = 13 𝑁 = 13 𝑡 𝑝
Cadence 61.1 ± 12.2 81.8 ± 13.8 5.03 5.03SGS (m/s) 31.9 ± 15.9 46.9 ± 15.9 3.62 0.004∗
FGS (m/s) 59.8 ± 26.2 80.50 ± 30 4.68 0.001∗
WBAL 40.2 ± 6.9 44.9 ± 3.4 2.75 0.018∗
SIS 55.6 ± 7 64.6 ± 3.4 2.69 0.020∗
SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
Table 4: Within-group comparison of the dependent variable inLORT group.
VariablesPretest Posttest PairedM ± SD M ± SD 𝑡-test𝑁 = 10 𝑁 = 10 𝑡 𝑝
Cadence 53.4 ± 15.4 68.5 ± 14.5 2.34 2.34SGS (m/s) 22.8 ± 11 30.2 ± 11 2.6 0.029∗
FGS (m/s) 45.5 ± 17.7 55.5 ± 24.1 2.28 0.049∗
WBAL 38.4 ± 8.2 39.8 ± 6.9 0.86 0.412SIS 53.1 ± 10.4 56.5 ± 6.8 1.71 0.121SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.

4 Rehabilitation Research and Practice
Table 5: Posttest between-group comparisons of the dependentvariables.
Variables FLO LORT Independent 𝑡-test𝑁 = 13 𝑁 = 10 𝑡 𝑝
Cadence 81.8 ± 13.8 68.5 ± 14.5 2.45 0.024∗
SGS (m/s) 46.9 ± 15.9 30.2 ± 11 2.81 0.011∗
FGS (m/s) 80.50 ± 30 55.5 ± 24.1 2.47 0.023∗
WBAL 44.9 ± 3.4 39.8 ± 6.9 2.19 0.040∗
SIS 64.6 ± 3.4 56.5 ± 6.8 2.27 0.046∗
SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
0102030405060708090
Cadence SGS FGS WBAL SIS
68.5
30.2
55.5 56.5
81.8
46.9
80.5
64.6
44.939.8
LOTRFLO
Figure 1: Posttest intragroup comparison of outcome variables. SGS:Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
5. Discussion
The aim of the present study was to find the efficacyof functional limb loading training on gait performance,weight bearing on affected limb, and perceived mobility andcommunity participation in chronic community dwellingstroke patients. In our study we found an improvement inall the selected variables. In patient with chronic stroke,the common impairments associated with muscle strength,motor control, and balance appear to have the strongestrelationwithwalking [22]; therefore these improvementsmaybe due to the increased physical activity undertaken duringthe training period as it is well documented that patientswith chronic stroke have relatively sedentary lifestyle withlittle physical activities [23]. In the present study, the fourweeks of training resulted in symmetric weight bearing andimproved gait function, which may be due to the improvedmuscle strength, coordination, and sensory organizationcaused by functional overloading of the affected limb. Thelower limb overloading along with functional activities couldhave increased the weight bearing on the affected leg and theproprioceptive stimuli to the joints of the paretic leg causingincreased stability.
The significant improvement in terms of weight bearingsymmetry on affected leg could be due to the changes inbiomechanical alignment of the body, resulting in equaltransfer of body weight to both lower limbs. These results
can be explained based on previous studies, which suggestthat the hemiplegic patients showing asymmetric lower limbweight bearing generally had associated sensory derange-ments and proprioceptive stimulation can influence posturalcontrol and ambulation in such patients [24]. The complexmechanisms, which contribute to gait, and the varyingenvironments demands during functional mobility requireinterventions that can addresses different elements underly-ing walking. Impaired ability of the paretic limb to maintainsymmetrical loading affects balance and gait. Hendrickson etal. [25] suggested that rehabilitation strategies that increasethe contribution of the paretic limb to standing balancecontrol may increase symmetry of walking after stroke. Theimprovement shown by the subjects in the FLO group maybe due to the continuous loading provided to them, whichamounted to approximately 90% of awake time.
Even though the effects of resistance training on gaitperformance are less clear, various studies have demonstratedstrong correlations between walking speed and lower limbmuscle strength of the paretic side suggesting its positiveeffect on gait speed and endurance [26]. The curvilinearrelationship between muscle strength and functional skillssuggests that further improvements in strength after theachievement of functional level may not lead to any sub-stantive gains. Therefore, the significant improvement in theweight bearing on affected lower limb and gait performancein our study may be because of the fact that limb over-loading is incorporated with functional activities directedat improving the gait function. The results of our studysubstantiate the strong evidence suggesting that task-specifictraining can assist with functional motor recovery, which isdriven by adaptive neural plasticity [27]. In this study, thesubjects in functional limb overloading training showed astatistically significant improvement in perceived mobilityand community participation. The findings are similar tothe study done by Flansbjer et al. [28] assessing the effectof progressive resistance training on perceived participationin stroke patient, which found that improvements in gaitperformance were related to improvements in perceived par-ticipation. Other studies measuring changes in function anddisability found that self-reported limitations in performinglife tasks decreased following resistance training.
6. Conclusion
To the best of our knowledge, this is the first study that hasevaluated the effects of functional limb overloading trainingon weight bearing on affected limb, walking ability, andperceived mobility and community participation in chronichemiplegic population. The study demonstrated a beneficialeffect of training on all the outcomes, suggesting that thefunctional limb overloading training can be a useful tool inthe management of gait problems in chronic stroke patients.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.

Rehabilitation Research and Practice 5
Acknowledgments
This research was funded by Sheikh Abdullah Bin AbdulMohsen Al Tuwaijri Chair for Applied Research in Stroke,Majmaah University, Saudi Arabia.The authors would like toexpress their gratitude towards Sheikh Abdullah Al Tuwaijri,Rector Dr. Khalid Bin Saad Al Muqrin, and Chair SupervisorDr. Raid SAl Baradie for providing the necessary support andassistance for completing this piece of work.
References
[1] A. A. Robert and M. M. Zamzami, “Stroke in Saudi Arabia: areview of the recent literature,” PanAfricanMedical Journal, vol.17, article 14, 2014.
[2] H. T. S. Benamer and D. Grosset, “Stroke in Arab countries: asystematic literature review,” Journal of the Neurological Sci-ences, vol. 284, no. 1-2, pp. 18–23, 2009.
[3] D. T. Wade, V. A. Wood, A. Heller, J. Maggs, and R. LangtonHewer, “Walking after stroke. Measurement and recovery overthe first 3 months,” Scandinavian Journal of RehabilitationMedicine, vol. 19, no. 1, pp. 25–30, 1987.
[4] S. Mulroy, J. Gronley, W. Weiss, C. Newsam, and J. Perry, “Useof cluster analysis for gait pattern classification of patients inthe early and late recovery phases following stroke,” Gait andPosture, vol. 18, no. 1, pp. 114–125, 2003.
[5] S. S. Ng and C. W. Hui-Chan, “Contribution of ankle dorsi-flexor strength to walking endurance, in people with spastichemiplegia after stroke,” Archives of Physical Medicine andRehabilitation, vol. 93, no. 6, pp. 1046–1051, 2012.
[6] G. V. Smith, K. H. C. Silver, A. P. Goldberg, and R. F. Macko,“‘Task-oriented’ exercise improves hamstring strength andspastic reflexes in chronic stroke patients,” Stroke, vol. 30, no.10, pp. 2112–2118, 1999.
[7] C. Carvalho, K. S. Sunnerhagen, and C. Willen, “Walkingperformance and muscle strength in the later stage poststroke:a nonlinear relationship,” Archives of Physical Medicine andRehabilitation, vol. 94, no. 5, pp. 845–850, 2013.
[8] G. Kwakkel, R. Van Peppen, R. C. P. Wagenaar et al., “Effects ofaugmented exercise therapy time after stroke: a meta-analysis,”Stroke, vol. 35, no. 11, pp. 2529–2536, 2004.
[9] C.M.Dean,C. L. Richards, andF.Malouin, “Task-related circuittraining improves performance of locomotor tasks in chronicstroke: a randomized, controlled pilot trial,”Archives of PhysicalMedicine and Rehabilitation, vol. 81, no. 4, pp. 409–417, 2000.
[10] N. M. Salbach, N. E. Mayo, S. Wood-Dauphinee, J. A. Hanley,C. L. Richards, and R. Cote, “A task-orientated interventionenhances walking distance and speed in the first year poststroke: a randomized controlled trial,” Clinical Rehabilitation,vol. 18, no. 5, pp. 509–519, 2004.
[11] C. K. English, S. L. Hillier, K. R. Stiller, and A. Warden-Flood, “Circuit class therapy versus individual physiotherapysessions during inpatient stroke rehabilitation: a controlledtrial,” Archives of Physical Medicine and Rehabilitation, vol. 88,no. 8, pp. 955–963, 2007.
[12] L. Wevers, I. van de Port, M. Vermue, G. Mead, and G.Kwakkel, “Effects of task-oriented circuit class training onwalking competency after stroke. A systematic review,” Stroke,vol. 40, no. 7, pp. 2450–2459, 2009.
[13] Y.-R. Yang, R.-Y. Wang, K.-H. Lin, M.-Y. Chu, and R.-C.Chan, “Task-oriented progressive resistance strength trainingimproves muscle strength and functional performance in indi-viduals with stroke,” Clinical Rehabilitation, vol. 20, no. 10, pp.860–870, 2006.
[14] K. J. Sullivan, D. A. Brown, T. Klassen et al., “Effects of task-specific locomotor and strength training in adults who wereambulatory after stroke: results of the STEPS randomizedclinical trial,” Physical Therapy, vol. 87, no. 12, pp. 1580–1602,2007.
[15] C. Meek, A. Pollock, J. Potter, and P. Langhorne, “A systematicreview of exercise trials post stroke,” Clinical Rehabilitation, vol.17, no. 1, pp. 6–13, 2003.
[16] J. J. Eng and P.-F. Tang, “Gait training strategies to optimizewalking ability in people with stroke: a synthesis of the evi-dence,” Expert Review of Neurotherapeutics, vol. 7, no. 10, pp.1417–1436, 2007.
[17] R. Teasell, N. Foley, K. Salter, J. Jutai, and M. Speechley,Evidence-Based Review of Stroke Rehabilitation Executive Sum-mary, 13th edition, 2010, http://brainstreams.ca/sites/default/files/EBRSR-Executive-summary-Ed13.pdf.
[18] D. A. Brown, S. Nagpal, and S. Chi, “Limb-loaded cyclingprogram for locomotor intervention following stroke,” PhysicalTherapy, vol. 85, no. 2, pp. 159–168, 2005.
[19] R. Fernandez-Gonzalo, C. Nissemark, B. Aslund, P. A. Tesch,and P. Sojka, “Chronic stroke patients show early and robustimprovements in muscle and functional performance inresponse to eccentric-overload flywheel resistance training: apilot study,” Journal of NeuroEngineering and Rehabilitation, vol.11, article 150, 2014.
[20] P. W. Duncan, D. Wallace, S. M. Lai, D. Johnson, S. Embretson,and L. J. Laster, “The stroke impact scale version 2.0. Evaluationof reliability, validity, and sensitivity to change,” Stroke, vol. 30,no. 10, pp. 2131–2140, 1999.
[21] B. Edwards and B. O’Connell, “Internal consistency and validityof the Stroke Impact Scale 2.0 (SIS 2.0) and SIS-16 in anAustralian sample,” Quality of Life Research, vol. 12, no. 8, pp.1127–1135, 2003.
[22] A. Weiss, T. Suzuki, J. Bean, and R. A. Fielding, “High intensitystrength training improves strength and functional perfor-mance after stroke,” American Journal of Physical Medicine andRehabilitation, vol. 79, no. 4, pp. 369–376, 2000.
[23] M. M. Ouellette, N. K. LeBrasseur, J. F. Bean et al., “High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors,”Stroke, vol. 35, no. 6, pp. 1404–1409, 2004.
[24] J. C. Outermans, R. P. Van Peppen, H. Wittink, T. Takken, andG. Kwakkel, “Effects of a high-intensity task-oriented trainingon gait performance early after stroke: a pilot study,” ClinicalRehabilitation, vol. 24, no. 11, pp. 979–987, 2010.
[25] J. Hendrickson, K. K. Patterson, E. L. Inness, W. E. McIlroy,and A. Mansfield, “Relationship between asymmetry of quietstanding balance control and walking post-stroke,” Gait andPosture, vol. 39, no. 1, pp. 177–181, 2014.
[26] L. F. Teixeira-Salmela, S. Nadeau, I. McBride, and S. J. Olney,“Effects of muscle strengthening and physical conditioningtraining on temporal, kinematic and kinetic variables duringgait in chronic stroke survivors,” Journal of RehabilitationMedicine, vol. 33, no. 2, pp. 53–60, 2001.

6 Rehabilitation Research and Practice
[27] L. G. Richards, K. C. Stewart, M. L. Woodbury, C. Senesac,and J. H. Cauraugh, “Movement-dependent stroke recovery:a systematic review and meta-analysis of TMS and fMRIevidence,” Neuropsychologia, vol. 46, no. 1, pp. 3–11, 2008.
[28] U.-B. Flansbjer, D. Downham, and J. Lexell, “Knee musclestrength, gait performance, and perceived participation afterstroke,”Archives of Physical Medicine and Rehabilitation, vol. 87,no. 7, pp. 974–980, 2006.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com

Volume 8 Number 4 October-December 2014
Published, Printed and Owned : Dr. R.K. SharmaDesigned and Printed : M/s Vineeta Graphics, B-188, Subash Colony, Ballabgarh, FaridabadPublished at :
Editor : Dr. R.K. Sharma, Mobile:
4 Floor, Statesman House Building,Barakhamba Road,Connaught Place,New Delhi-110 001
th
91-9971888542, Fax No: +91 11 3044 6500

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 259DOI Number: 10.5958/0973-5674.2014.00344.X
Relative & Cumulative efficacy of Auditory & VisualImagery on Upper Limb Functional Activity among
Chronic Stroke Patients
Fuzail Ahmad1, Sami Al-Abdulwahab2, Nasser Al-Jarallah3, Raidah Al-Baradie4, Mohammad Z Al-Qawi5,Faizan Z Kashoo6, Harpreet S Sachdeva7
1Head, Department of Physical Therapy, College of Applied Medical Sciences, Majmaah University, Kingdom ofSaudi Arabia, 2Professor, Department Rehabilitation Sciences, College of Applied Medical Sciences, King Saud
University, Riyadh, Kingdom of Saudi Arabia, 3Dean, College of Applied Medical Sciences, Majmaah University,Kingdom of Saudi Arabia, 4Consultant Neurologist, Neuroscience Center, King Fahd Specialist Hospital, Departmentof Pediatrics, Dammam University, Dammam, Saudi Arabia, 5Head Stroke Unit, King Faisal Specialist Hospital and
Research Center, Riyadh. Kingdom of Saudi Arabia,6Department of Physical Therapy, College of Applied MedicalSciences, Majmaah University, Kingdom of Saudi Arabia, 7Physical Therapist, Department of Neurology &
Neurosurgery, CN Centre, All India Institute of Medical Sciences, New Delhi, India
ABSTRACT
Introduction: Stroke is a very limiting disease for the patient and a major health problem in mostparts of the world. Activity limitations of the upper extremity are a common finding for individualsliving with the effects of stroke, with its prevalence reported between 33% and 95% of this population.This study aims to explore whether imagery involves the activation of primary sensory cortices andto determine the therapeutic effectiveness and benefits of mental imagery training for arm functionin chronic stroke patients.
Material & Method: The study was conducted as a randomized, pre-post pilot project with fourpatient groups. Patients underwent imagery ability screening using the mental chronometry,autonomic monitoring before group allocation and randomization. We also assessed the patients onMotor Activity Log (MAL) to assess motor impairment in the affected Upper extremity. F-wave, fMRI along with MAL was administered.
Result Recovery between baseline and outcome assessment was evident on all outcome variables.However, no differences between the three groups were found on the primary outcome measure.
Conclusion: The results support the efficacy of programs incorporating mental practice forrehabilitating affected arm function in patients with chronic stroke. Mental imagery is a clinicallyfeasible, cost-effective complement to the therapy that may improve outcomes more than participationin therapy only. This concept in the clinical settings can provide an additional benefit in improvingthe upper limb function in stroke patients.
Keywords: Stroke, Hemiplegia, Mental Imagery, Stroke Rehabilitation
INTRODUCTION
Stroke is a sudden loss of brain function caused bythe interruption of flow of blood to the brain or therupture of blood vessels in the brain1. Stroke is a verylimiting disease for the patient and a major health
problem in most parts of the world. People whoexperience a stroke may undergo sudden and intensechanges in perception, cognition, mood, speech,health-related quality of life, and function2.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM259

260 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Activity limitations of the upper extremity are acommon finding for individuals living with the effectsof stroke, with its prevalence reported between 33%and 95% of this population. These activity limitationsmay occur because of deficits in body structures andfunctions caused by the stroke, such as in motor ability,somatosensation and perceptual ability3.
Traditional stroke rehabilitation therapies addressthis incompatibility by using behavior repetition. Thehope is that repeated physical practice will improvemotor activity, allowing for smooth and controlledmovements to occur, acting as examples for the brainto use in reestablishing the circuitry that mediatesvoluntary movement4-5.
This has led to a variety of interventions thatrehabilitation professionals, may use to maximize theupper extremity function of the individuals, they treat6.
Recently, mental imagery; a technique throughwhich an individual repeatedly mentally rehearses anaction or task without actually physically performingthe action or task have become additional therapyinterventions7.
As the current approaches to stroke rehabilitationis characterized by multiple and unsubstantiatedphilosophies and a tendency to invest efforts in thosewith severe stroke and in goals limited to self-care it isposited that mental practice could be a non-invasive,useful tool in rehabilitating patients with strokes.
This study aims to explore whether imageryinvolves the activation of primary sensory cortices andto determine the therapeutic effectiveness and benefitsof mental imagery training for arm function in chronicstroke patients.
METHODOLOGY
The study was conducted as a randomizedcontrolled trial with four groups; auditory imagerygroup (EA); visual imagery group (EV); cumulativeimagery group (EC) & control group (CG). Subjectsaged having first episode of unilateral stroke within1-6 months with not more than grade 3 spasticity onMotor Assessment Scale (MAS) in the affected upperextremity, without any severe cognitive deficits,aphasia, rheumatologic or musculoskeletal damage inthe affected upper extremity, were selected for thisstudy. The patients were excluded from the study ifthey did not perceive upper extremity motor
weakness. Patients were excluded from the study ifthey were discharged from hospital within 1 week anddid not present with an upper limb motor weakness
All the patients signed an informed consent thenunderwent imagery ability screening using the mentalchronometry before group allocation andrandomization.
Outcome Measures
Action Research Arm Test (ARAT) was used forassessing the functional limitations of the upper limb(UL) on the affected side. It includes 19 items dividedinto four subscales: grasp, grip, pinch, and grossmovement. Reliability (interrater = 0.99, test-retest =0.98), construct validity, and predictive validity of theARAT have been well-established8.
Motor Activity Log (MAL)9, is a focal measure ofself-perceived disability on tasks requiring UL use. Itis used for assessing how much and how well patientsuse their affected arm for activities of daily living(ADL). Thirty specific ADL tasks are evaluated withthe use of a 6-poin amount of use (AOU) scale and a 6-point quality of movement (QOM) scale.
Levels of independence and functional limitationswere evaluated with regards to Activities of DailyLiving using the Barthel Index (BI)10 covering items ofambulation, body care, mobility, alertness andcommunication.
Intervention Protocol
All the four groups received single task trainingduring the physiotherapy sessions in the interventionprogram. The selected task in the study experimentconsisted of four discrete stages; sit upright with handsupported on the lap, reach for and grasp the cup, liftthe cup and drink a sip of water, extend your arm andkeep the cup back to starting point, grasp release, handback to lap. The task was selected since it wasconsidered familiar and not complex for single sessiontraining; moreover, the task involves unilateralextremity activity.
Fig. 1. Discrete stages of the selected task.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM260

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 261
The experimental groups received training withauditory, visual or both auditory and visual imagerytechniques. A blinded examiner performed thescreening assessments and recorded outcomemeasures at baseline (BA), and immediately after thetraining session (TS) on the same day. In total thetreatment time was about 45 – 50 minutes.
RESULTS
Randomization, using a statistical minimizing
procedure, was successful and no group differencesat baseline were found on all the outcome measure oron any of the other demographic or clinicalcharacteristics.
At baseline MAL-QOM score for EA, EV, EAVgroup patients were 3.4+0.5, 3.8+0.5 & 3.3+1, whichhave been changed post training to 3.8+0.6, 4+0.9 and3.7+0.6 respectively. Median MAL-QOM score forcontrol patients before the intervention was 3.4 + 0.6;and the post-intervention score was 3.5 + 0.4.
Table 1: Comparison between baseline and post-training scores of motor activity log.
EA M+SD EV M+SD EC M+SD CG M+SD Kruskal–Wallis test
N=3 N=3 N=3 N=3
X2 P
QOM BA 3.4+0.5 3.8+0.5 3.3+1 3.4+0.6 0.423 0.672
QOM TS 3.8+0. 6 4+0.9 3.7+0.6 3.5+0.4 1.311 0.921
AOU BA 3.8+0.9 3.5+0.8 3.7+0.5 3.9+0.7 0.08 0.934
AOU TS 3.6+0. 6 3.9+0.7 3.2+0.8 3.4+0.5 1.35 0.177
Keys: EA-Auditory Imagery Group EV-Visual Imagery Group EC-Cumulative Imagery Group CG-Control Group, QOM-Quality ofMovement, AOU-Amount of Use
Similarly, at baseline MAL-AOU score for EA, EV,EAV group patients were which have been changed3.8+0.9, 3.5+0.8, 3.7+0.5 post training to 3.6+0.6, 3.9+0.7,3.2+0.8 respectively. Median MAL-AOU score forcontrol patients before the intervention was 3.9+0.7and 3.4+0.5 post-intervention.
There were no differences in motor imagery abilitybetween the treatment groups (Table 2). Control datacollected with age-matched neurologically intacthealthy volunteers on the same measure with the righthand, suggests no difference in motor imagery abilitybetween participants.
No differences between the three groups werefound on the primary outcome measure, the ARAT
(Table 3). Neither were there differences between thegroups on measures of functional impairment.Improvement on the primary outcome measure, theARAT score, correlated with improvement on thesecondary outcome measures of activities of dailyliving level, (r�=� 0.23, P�<� 0.05), QOM-AOU(r�=� -0.60, P�< �0.001), and BI (r�=� -0.25,P�<�0.01), but not with MAL-QOM(r�=�0.12, n.s).Mental status questionnaire score at baseline showeda significant relationship with improvement onactivities of daily living level (r�=�-0.26, P�<�0.01)but not with improvement on any of the other outcomemeasures (P�>�0.12).
Table 2: Between Group mean performance and ANCOVA analysis group differences on primary and secondaryoutcome measures.
Group n Baseline Post-training Between groupassessment assessment difference
Mean (SD) Mean (SD) P-value
Action Reach Arm Test (ARAT)
Mental Imagery Training- Auditory 10 21.22 (14.20) 26.33 (19.24) 0.77 0.35
Mental Imagery Training-Visual 10 25.64 (18.10) 31.51 (20.68)
Mental Imagery Training-Cumulative 10 26.23 (17.92) 32.87 (20.76)
Control-Group 10 23.06 (17.66) 30.38 (20.53)
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM261

262 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Table 2: Between Group mean performance and ANCOVA analysis group differences on primary and secondaryoutcome measures. (Contd.)
Group n Baseline Post-training Between groupassessment assessment difference
Mean (SD) Mean (SD) P-value
Motor Assessment Log (QOM)
Mental Imagery Training- Auditory 10 3.4 (.52) 3.8 (.63) 0.98 0.14
Mental Imagery Training-Visual 10 3.8 (.52) 4 (.93)
Mental Imagery Training-Cumulative 10 3.3 (.97) 3.7 (.59)
Normal Care Control 10 3.4 (.62) 3.5 (.42)
Motor Assessment Log (AOU)
Mental Imagery Training- Auditory 10 3.8 (.87) 3.6 (.63) 0.38 0.19
Mental Imagery Training-Visual 10 3.5 (.81) 3.9 (.73)
Mental Imagery Training-Cumulative 10 3.7 (.53) 3.2 (.79)
Normal Care Control 10 3.9 (.74) 3.4 (.53)
Barthel Index
Mental Imagery Training- Auditory 10 55.20 (11.02) 47.28 (15.16) 0.98 0.54
Mental Imagery Training-Visual 10 58.40 (15.02) 50.28 (18.78)
Mental Imagery Training-Cumulative 10 64.16 (14.04) 55.42 (15.81)
Normal Care Control 10 62.50 (14.26) 53.49 (18.68)
There were no differences in motor imagery abilitybetween the treatment groups [F(2,97)�=�0.65,P�=�0.52). Control data collected with age-matchedneurologically intact healthy volunteers on the samemeasure with the right hand, suggests no differencein motor imagery ability between participants in thetrial and healthy controls [F(1,142)� =� 1.56,P�=�0.21, Graphic�=�0.01]. Motor imagery abilityof the participants in the trial correlated with changebetween baseline and outcome assessments on theprimary outcome measure, the ARAT difference score(r�=�0.28, P�=�0.002). However, within the ‘MotorImagery Training’ group, motor imagery ability wasnot correlated with ARAT change scores (r�=�0.12,P�=�0.23).
Fig. 1. Difference in various outcomes selected for this study.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM262

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 263
DISCUSSION
The aim of this study was to evaluate thetherapeutic benefit of mental practice in sub-acutestroke patients with a moderate motor weakness. Therationale for the efficacy of mental practice in stroke isthat activation of motor brain areas through imagerywill enhance brain plasticity. If the neural principle of‘firing is rewiring’ applies to mental practice in stroke,than we would expect to find a clinical benefit inpatients’ early post-stroke. Processes of functionalredistribution have been demonstrated in earlyrecovery and have been linked to physical practice. Ifthe underlying mechanisms of mental practice can beattributed to brain plasticity rather than motivationalor cognitive factors, then we should see enhancedrecovery in stroke patients participating in mentalpractice independent of physical practice ofmovements11. In the design of this study a number offactors were carefully considered in order to providea more direct evaluation of this plasticity account.Mental practice was not embedded in physical therapy,which was instead offered to all participants as part ofnormal care, in order to provide a more directevaluation of the plasticity account12.
This relates to the issue of combined physical andmental practice. An important part of the rationale ofthe current trial was to exclude the possibility thatmental practice merely provides prolongedopportunity to consolidate particular movementpatterns, and find a more direct indication that mentalpractice works through processes of brain plasticityindependent of the effects of physical movement. Sincewe previously found that combined mental andphysical practice gave improvement on the trainedtask only13, We felt it was necessary to evaluate thebenefit of mental practice when not combined withphysical practice of the movements. The prudence ofevaluating motor imagery training independent ofmotor performance was also pointed out by Sharmaand colleagues14. Previous studies combined mentalpractice with physical practice. In their mental practiceevaluations Page and colleagues15 reported a clinicalbenefit for mental practice in a series of small studiesand one randomized controlled trial. The placebocondition was always audiotape-led relaxation. Thismeans that patients in the treatment group had anopportunity during mental practice to consolidatemovement patterns that they earlier had beenpracticing physically, while the control group did not
have this advantage. The benefit of combined physicaland mental practice can therefore be attributed to anyof the following mechanisms. The mental practiceextended engagement with motor processes, whichmay give rise to enhanced cognitive models ofperformed movements, or may even have amotivational effect. Alternatively, it is possible that anindirect effect of neuroplasticity accounts for thefindings, where mental practice reactivates recentlyused motor representations allowing for an increasedeffect of the physical practice itself. However, all theseexplanations would imply that the benefit of mentalpractice is not independent of physical practice, anddoes not provide a ‘backdoor to the motor systemsafter stroke’ or form an alternative if physical practiceis not possible16.
Furthermore, as patients performed well on theobjective motor imagery ability measure, it is alsounlikely that patients were unable to benefit frommental practice due to impaired motor imagery. It ispossible that spontaneous recovery in these sub-acutepatients masked the subtle benefit of mental practice,but again the reported small effect sizes of thetreatment effects in this study do not suggest this.
As such, the finding of the current carefullycontrolled powered trial, representative of the strokepopulation, is important in the evaluation of thetherapeutic benefit of mental practice. Future researchwill need to investigate the role of both chronic patientstatus and prolonged mental practice in clarifying thetherapeutic benefit of cumulative mental practice instroke.
CONCLUSION
The results support the efficacy of programsincorporating mental practice for rehabilitatingaffected arm function in patients with chronic stroke.Mental imagery is a clinically feasible, cost-effectivecomplement to the therapy that may improveoutcomes more than participation in therapy only. Thisconcept in the clinical settings can provide anadditional benefit in improving the upper limbfunction in stroke patients.
Acknowledgment: I would like to express mygratitude towards Sheikh Abdullah bin Abdul MohsenAl-Tuwaijri, Dr. Raid Al-Baradie and Majmaah Universityfor providing the necessary support for completing thispiece of work.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM263

264 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Source of Funding: This research was funded bySheikh Abdullah bin Abdul Mohsen Al-Tuwaijri Chairfor Applied Research in Stroke at Majmaah University,Al-Majmaah, Saudi Arabia.
Ethical Clearance was taken from the InstitutionalReview Board, Centre for Basic and Applied MedicalSciences at Majmaah University.
Conflict of Interest: Nil
REFERENCES
1. Heart and Stroke Foundation of Canada. Whatis a stroke? http://www.heartandstroke.com/site/c.ikIQLcMWJtE/b.3483935/k.A279/WhatÿisÿStroke.html
2. Mayo N, Wood-Dauphinee S, Ahmed S, GordonC, Higgins J, McEwen S, et al. Disablementfollowing stroke. Disability and Rehabilitation1999; 21(5/6):258–68.
3. Andrews AW, Bohannon RW. Short-termrecovery of limb muscle strength after acutestroke. Archives of Physical Medicine andRehabilitation 2003; 84:125–30.
4. Kosslyn, S.M., Ball, T.M., & Reiser, B.J. Visualimages preserve metric spatial information:Evidence from Studies of image Scanning.Journal of Experimental Psychology: Human,Perception and Performance, 1978:Vol.4, No.1,47-60
5. Jackson PL, Doyon J, Richards CL, Malouin F.Potential role of mental imagery using motorimagery in neurological rehabilitation. Arch PhysMed Rehabil 2001; 82:1133-41.
6. Baddeley, A.D. & Logie, R. Auditory imagery andworking memory. In Auditory Imagery, D.Reisberg, (Ed.), 179-197, Lawrence ErlbaumAssociates, Inc. Publishers, ISBN 0-8058-2292-5,New Jersey, USA
7. Dijkerman HC1, Ietswaart M, Johnston M,MacWalter RS. Does motor imagery trainingimprove hand function in chronic stroke patients?
A pilot study. Clin Rehabil. 2004 Aug; 18(5):538-49.
8. Leeuwen van R, Inglis J. Mental imagery andimagery: a potential role in stroke rehabilitation.Phys Ther Rev 1998; 3:47-52.
9. Taub E, Morris D, Bowman M, Delgado A,Uswatte G. Upper-Extremity Motor Activity Log[Manual].(Available from Edward Taub,Psychology Department, UAB, CH415,Birmingham, Ala); 1996.
10. Mahony FL, Barthel DW. Functional evaluation.The Barthel Index. Maryland State Med J1965;14:61-5.
11. Pylyshyn, Z.W. Mental imagery: In search of atheory. Behavioral & Brain Sciences,2002; Vol25,No.2, 157-238
12. Watson, J., Myers, R., Frackowiak, R., Hajnal, J.,Woods, R., Mazziotta, J., Shipp, S., & Zeki, S. AreaV5 of the human brain: Evidence from acombined study using positron emissiontomography and magnetic resonance imaging.Cerebral Cortex, 1993: Vol.3, No.2, 79–94
13. Sharma N1, Pomeroy VM, Baron JC. Motorimagery: a backdoor to the motor system afterstroke? Stroke. 2006 Jul; 37(7):1941-52.
14. Page SJ, Levine P, Leonard A (2007) Mentalpractice in chronic stroke: results of arandomized, placebo-controlled trial. Stroke38(4):1293–1297.
15. Page SJ, Levine P, Leonard AC (2005) Effects ofmental practice on affected limb use and functionin chronic stroke. Arch Phys Med Rehabil86(3):399–402.
16. Page SJ, Levine P, Sisto S, Johnston MV (2001) Arandomized efficacy and feasibility study ofimagery in acute stroke. Clin Rehabil 15(3):233–240
17. Johnson MR1, Mitchell KJ, Raye CL, D’EspositoM, Johnson MK. A brief thought can modulateactivity in extrastriate visual areas: Top-downeffects of refreshing just-seen visual stimuli.Neuroimage. 2007 Aug 1; 37(1):290-9.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM264

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
687
EFFECT OF LUMBAR STABILIZATION EXERCISES VERSUS PRESSURE FEEDBACK TRAINING IN LOW BACK ACHE PATIENTS
Shadab Uddin Department of Physical therapy, Faculty of Applied Medical Sciences, Jazan University,
Jazan, Kingdom of Saudi Arabia (KSA)
Fuzail Ahmed
Department of Physical therapy, Faculty of Applied Medical Sciences, majmaah University, al majmaah, Kingdom of Saudi Arabia (KSA)
Abstract: Chronic low back pain is the most common complaints in the urban society causing to absent from the work and activity limitation. Its health, social and economic burden is hefty. Despite developments in modern medicine in general and growing knowledge of spinal diseases, problem of nonspecific low back pain remains unsolved. Although the nonspecific types of bach pain affects approximately 85% of patients while 40% of low back pain patients worry that pain affects their work ability and will make them cripple, or that it underlies some serious disese (Waddell 1998). Even though there is ample evidence stating the efficacy of core stability training but not able to find any study which has compared Pressure Biofeedback training with Core Stability Training in the treatment of chronic low back pain. The aim of the present study was to compare the effectiveness of stabilizer pressure biofeedback training and core stability exercises on pain perception as measure by visual analogue scale in chronic low back pain patients.
Key Words: Back pain, core stability training, stabilizer pressure biofeedback Introduction
Chronic low back pain is the most common complaints in the urban society causing to absent from the work and activity limitation. Its health, social and economic burden is hefty. If we look to western societies, it has one of the most human suffering, disabling and enormous economic consequences with the frequent use of medical consultation and visit to rehabilitation unit. It is estimated that 70%-80% of population of United States of America is bear on back pain at one point in their life time.1 It is 2nd most frequent reason for visit to the physician and 5th ranking cause of hospital admission.2-3 In the United Kingdom back pain is the largest single reason of absence from work in 1988-1989 and is responsible for approximately 12.5% of all sick days.4
Despite developments in modern medicine in general and growing knowledge of spinal diseases, the problem of nonspecific low back pain remains unsolved, although the nonspecific type affects approximately 85% of patients reporting any back pain. Approximately 40% of low back pain patients worry that pain affects their work ability, that it will cripple them, or that it underlies some serious disease. Better understanding of multidimensional aspects has widened our concept of low back pain. There are several causes of low back pain. In a mechanical model, research has implicated pain sensitive vertebral structure such as the intervertebral disc and the zygoapophyseal joints as potential sources of low back pain. Irrespective of the actual source of symptoms, it has been shown that muscles are adversely affected secondary to low back pain. This phenomenon is accepted at peripheral joints such as the knee. For example, irrespective of the knee structure which is injured, e.g. meniscus or ligament, it is commonly accepted that quadriceps function will be adversely affected. Possible neurophysiological mechanisms include pain and reflex inhibition. Muscle re-education is therefore a commonly used intervention in the rehabilitation process, and for many years exercise has been advocated in the treatment of low back pain. Many researchers have focussed on issues of muscle strength. The basis for this focus is the premise that strong abdominal and back muscles are able to provide support for the lumbar spine.5

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
688
Despite the common acceptance of this principle, systematic reviews have not on the whole supported general trunk muscle strengthening programs.6 This has led to the development of specific exercise programs designed to protect and support the damaged joints and allow healing of the injured tissues.7,8 Muscles can be broadly divided into two categories, local and global muscles.9 The local muscle system includes deep muscles that are attached to the lumber vertebrae and are capable of directly controlling the stiffness of the lumbar segments.10 In contrast, the global muscle system encompasses larger and more superficial muscles of the trunk. Their role is to move the spine and to control larger external loads, which occur with normal daily function. Biomechanical research has demonstrated that deep, local muscles are important for controlling, protecting and supporting the joints. The muscles of the local synergy, which are important for the lumbo-pelvic region include the segmental lumbar multifidus, the transverses abdominis, the pelvic f loor and the diaphragm. There is evidence that low back pain results in an alteration in function of the local muscles, which lose their protective role.8,10,11
A common clinical finding in low back pain patients is decreased range of motion of the spine with increased paraspinal activity. Disturbances in neuromuscular control have also been frequently connected with chronic low back pain and considered a possible linkage between pain and disability12. These impaired functions recover with treatment or active rehabilitation. Spinal manipulative therapy is commonly recommended for low back pain, although previous systematic reviews and practice guidelines have produced discordant findings as to the effectiveness of this therapy. A recent focus in the management of chronic low back pain patients has been the specific training of the deep abdominal (internal oblique and transversus abdominis) and lumbar multifidus muscles. The primary role of these muscles is considered to be the provision of dynamic stability and segmental control of the spine. For the treatment of chronic low back pain with radiological diagnosis of spondylolysis or spondylolisthesis, one randomized controlled trial of specific stabilizing exercises showed significant and longer-lasting reduction in pain intensity and functional disability levels than did other commonly prescribed conservative treatment programs.
Investigators have reported that individuals with back pain may have motor control deficits or errors that affect their ability to engage the muscles that stabilize the spine. Maintaining segmental control within the trunk contributes to spinal stability and reduces unnecessary movement intersegmentally. This can serve to decrease the risk of back pain by causing a reduction in tissue strain, deformation, compression, and overstretching. Clinicians maintain that the mechanisms involved in spinal stability can be linked to differences in the function of the trunk muscles13. The trunk muscles have been classified into 2 categories, and each one performs distinct functions. The first category is the global muscle system. The muscles in this category are larger and more superficial in comparison to other muscles. The global muscles act to transfer loads and move the spinal column as a whole. Examples include the rectus abdominis and the external oblique14.
The second category is the local muscle system. The local muscles are smaller and deeper than the global muscles. They are intersegmental and produce only small amounts of force. Local muscles aid in proprioception and postural control, which can decrease the risk of injury. The local muscles also contribute to maintaining stiffness along the spinal column. The multifidus and the transverse abdominis are two examples15. A number of investigators have cited evidence that supports the use of stabilization exercises for enhancing spinal stability20. The local muscles are said to be crucial in this mechanism. This may be because of their contribution to maintaining the position of the spine and their ability to improve trunk endurance. Core stability training is frequently used to improve spinal stability. It has been used for many years in physical therapy and has become popular in fitness settings17. It has been speculated that this method of training improves spinal stability and may assist in decreasing the risk of back pain.
Studies that have been done on core stability training demonstrate promise for its effects on the musculature of the trunk18. However, previous investigations have not been designed to explore the involvement of the local muscles, which act to stabilize the spine. In addition, the methods of analysis have typically stressed the global muscles through assessments for strength or surface EMG recordings. These measures may not adequately identify improvements in spinal stability brought on by the local muscles. Core stability training that focuses on exercises with a neutral spine may be

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
689
appropriate for targeting the specific function of the local muscles during the early phases of programming for improving spinal stability19-20. Even though there is ample evidence stating the efficacy of core stability training I was unable find any study which has compared Pressure Biofeedback training with Core Stability Training in the treatment of chronic low back pain. The aim of the present study was to compare the effectiveness of Stabilizer Pressure Biofeedback Training and Core Stability Exercises on pain perception as measure by visual analogue scale in chronic low back pain patients. Methodology
A total of 30 subjects were selected for the study on the basis of inclusion and exclusion criteria. The subjects were randomly assigned to Group 1and Group 2 each comprising 15 subjects. All the patients were recruited from the inpatient outpatient department Government Civil Hospital, Ahmadabad. Only those patients were included who were between 40-60 years of age, presented with chronic nonspecific recurrent low back pain. The duration of the symptoms was diagnosed as sub-acute and chronic according to the IASP classification of pain. Those patients who were having severe or excruciating pain, radiating pain to the legs, history of fracture, surgery, or constitutional symptoms like fever, malaise, etc indicating infection, any inflammatory conditions, radiographic changes showing cervical spinal malformations, osteoporosis, bony abnormalities, scoliotic or kyphotic spine, pregnancy, sensory impairments, vascular causes of radiating pain or neoplasms were excluded. The above stated conditions were ruled out on the discretion of a medical professional. Study Design
The study was designed as a two group pre-test and post-test longitudinal study. Pain and Functional Disability were taken as outcome measure for this study. The experimental design included a pre-test measure of the dependent variables Pain and Disability and after 4 weeks of treatment the dependent variables were measured again. Visual Analouge Scale was used for measuring pain and Oswestry Disability Questionnaire for finding level of functional disability. All the selected subjects were informed in detail about the type and nature of the study and were made to sign the informed consent. After taking down the demographic data the visual analogue scale and Disability scores were noted down. Then the subjects in both the groups were made to do common warm-up exercises initially. These exercises include light aerobic work in the form of exercise on bicycle for 5 minutes at moderate pace or jogging for 10 minutes. Group 1: Core Stability Training
Core stabilization refers to the muscles that act to stabilize the lumbar spine and lumbopelvic and hip complex as well as muscles acting to control position of the head, arms, and trunk segment relative to the body’s base of support.41
All the subjects in the Group 1 had undergone one month core stability training which comprises of exercises aimed at increasing spinal stability. Isolated Lumbar stabilizing muscles training: Development of the perception of the isolated isometric specific contraction of the stabilizing muscles. Group 2: Stabilizer Bio-feedback training
The Stabilizer is a simple device which registers changing pressure in an air filled pressure cell. This allows body movement, especially spinal movement, to be detected during exercise. The unit consists of a combined gauge/inflation bulb connected to a pressure cell. The Stabilizer is used to monitor and provide feedback on body movement during exercise. The three-chamber pressure cell of the Stabilizer was placed between the part of the body and floor. It was inflated till it molds between the body part and the supporting surface. A pressure of 40 mmHg was maintained as the resting pressure of the inflated cell. Changes in body weight on the cell on any of the three compartments will register a pressure change on the gauge.
The Stabilizer biofeedback training was given for 6 days a week for four weeks. This maneuver was repeated for all the muscles responsible for lumbar spinal stability. All the activities were performed in three sets of 10 repetitions each. Each training session comprises of 45 mins.

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
690
Results Thirty subjects, 23 males and 7 females were randomly divided into two groups; group 1 and group 2. Table 1: Demographic Characteristics of Subjects in both the groups
Group
Visual Analogue Scale Score (n=15)
Baseline After 15 Days
After 30 days
Core Stability Exercise
6.7+1 4.6+1.7 2.3+1.7
Pressure Biofeedback
6.2+1.7 3.5+1.8 0.9+1
Group Oswestry Disability Index Score (n=15) Baseline Baseline Baseline
Core Stability Exercise
40.4+12.5
30.6+12.6 19.8+14
Pressure Biofeedback
46.6+21 24.8+18 5.1 + 6
Fifteen subjects were taken in each group, with a mean age and standard deviation of subjects in group 1 and 2 were 23.4±1.95 and 21.66±1.95 respectively. There were 12 males and 3 females in group1 and 11 males and 4 females in group2. Statistical analysis revealed no statistically significant differences between the groups during the baseline readings. The outcome measures were pain, measured on Visual Analogue Scale and functional disability measured by Oswestry Disability Index. All the measurement was taken on the 1st day, 15th day and after completion of the training on 30th day. All the data were compared for both the within group and between group anlysis using repeated measure ANOVA. Effect of Training on Pain and Disability: Assessment of improvement in this experiment included two dependent variables; Visual Analog Scale (VAS) score and Oswestry Disability Index/Questionnaire Score (ODI). One-way MANOVA demonstrated a significant improvement in visual analogue scale and ODI among the three readings taken after 1st, 15th and 30th day respectively. Further analysis was performed to determine the difference in dependent variables between both the groups a post hoc analysis was performed using Bonferroni test. In Group1 it was found that there was a significant difference for visual analogue scale (F = 33.29, P=0.001), and ODI (F= 73.19, P=0.001) among all three readings. In Group 2 also it was found out that there was a significant difference for visual analogue scale (F=20.79, P=0.001) and ODI (F= 32.56, P=0.001) between the three readings. Results are presented in the following sections. (Table 5.2) Effect of Core Stability Exercises on Pain and Disability: The group1 getting Core Stability Training has shown significant improvement in terms of decrease in pain and functional disability. The one month Core Stability Training brought 66% decrease in pain and 25% improvement on Oswestry Disability Index. Even after 15 days of training there was a positive effect of this training which improved further with four weeks of training. Post Hoc analysis has shown that there was a significant improvement in baseline readings of visual analogue scale and ODI when the comparison was made between 1st and 15th day, 1st and 30th day and 15th and 30th. Effect of Stabilizer Bio-Feedback Training on Pain and Disability: In Group2 also a similar improvement was seen as with the Group1. There was a significant decrease among the baseline reading measured on 1st day and the consequent readings taken on 15th and 30th day. Post hoc analysis has shown that there was improvement in pain and disability score with the training which was found statistically significant. Table 2: Repeated Measure ANOVA for visual analogue scale and ODI

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
691
Group1 (n=15)
Group2 (n=15)
Vis
ual A
nalo
gue
Scal
e
Day 1 M ± SD 6.69±0.9 6.2±1.7
Day 15 M ± SD 4.6±1.7 3.46±1.8
Day 30 M ± SD 2.27±1.7 0.94±1
RANOVA F 33.29 73.19 P 0.001 0.001
Post-Hoc Analysis (P=)
1vs15 0 0.001 15vs30 0.002 0.001 1vs30 0.00 0.00
Osw
estry
Dis
abili
ty In
dex
Day 1 M ± SD 40.4±12.5 46.6±21.2
Day 15 M ± SD 30.6±12.6 24±18.2
Day 30 M ± SD 19.8±14.6 5.13±6.1
RANOVA F 20.79 32.56 P 0.001 0.001
Post-Hoc Analysis (P=)
1vs15 0.003 0.003 15vs30 0.003 0.003 1vs30 0.00 0.oo
Between Group Analysis To find out, how both the groups have behaved in terms of improvement and to test the experimental hypothesis, a between group analysis was performed using independent t-test for all the variables. The findings suggested that the group getting Stabilizer Bio-feedback training have shown comparatively more improvement on both Visual Analogue Scale and Oswestry Disability Index. Figure 1: Within Group Comparison of VAS and ODI
The result shows that for initial two weeks treatment both the group behaved similarly and improvement in pain and functional disability was seen in both the groups. Table 3: Between group analysis of visual analogue scale and ODI among all three conditions.
Variables
Group 1 Group2 t-test
(n=15) (n=15) M ± SD M ± SD t p
VAS1 6.7+0.9 6.2+1.7 0.903 0.374** VAS 15 4.6+1.7 3.5+1.8 1.738 0.093**

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
692
VAS 30 2.3+1.7 0.9+1 2.585 0.015*
ODI 1 39.7+12.5
38.8+16.2 0.176 0.861**
ODI 15
30.6+12.6 24.8+14 1.016 0.381**
ODI 30 19.8+14 5.1+6.1 28 0.001*
As evident by the results there was no statistically significant difference between the group
getting Core Stability Training or Stabilizer Pressure Bio-Feedback Training at 1st day (VAS: t =0.903, p=0.374 ODI: t =0.176, p=0.861) or after 15 days of treatment (VAS: t =1.738, p=0.093 ODI: t =1.016, p=0.381). But after four weeks of treatment the result shows a statistically significant difference between both the groups and also it shows that the group getting Stabilizer Bio-Feedback training improved better on both the scales Visual Analogue Scale as well as Oswestry Disability Scale. Figure 2: Between Group Analysis of the VAS and ODI
The results of this study support the initial hypothesis that Stabilizer Pressure Biofeedback
training of the “stability” muscles of the trunk is more effective in reducing pain and functional disability in patients with chronic low back pain. Analysis of the pain and functional disability score data in the experimental group revealed that this treatment approach was more effective than the Core Stability Training. These findings support the Punjabi’s21 hypothesis that the stability of the lumbar spine is dependent not solely on the basic morphology of the spine, but also the correct functioning of the neuromuscular system. Also, Radebold A.22 stated that muscle recruitment and timing pattern play an important role in maintaining lumbar spine stability. Therefore, exercises specifying the isolated contraction of multifidus muscle were incorporated in the Group2, in contrast to the core stability exercises in the group1. Hence, it gets clearer that the significantly better results in the group1 are due to the proper recruitment of the specific back muscles, which was facilitated by the Stabilizer. Hodges and Richardson19 showed that the co-contraction of the transverse abdominis and multifidus muscles occurred prior to any movement of the limbs. They also showed that the timing of coordination of these muscles was very significant, and that back injury patients were unable to recruit their transverse abdominis and multifidus muscles early enough to stabilise the spine prior to movement. It hence makes it utmost important to strengthen these deep and local muscles to uproot the low back aches completely and maintains segmental stability. Therefore, it can be safely stated that in the present study, the group in which this was emphasized showed a significant improvement in terms of pain and functional ability in comparison to the other group, as evident in the result section.
By definition, the deep-trunk muscles act as 'stabilizers' and are not involved in producing movements, but instead use static or isometric contractions. Furthermore, they must act as stabilisers continuously during everyday activities as well as sport, and so require very good endurance of low-level forces. Muscle impairments are not more of strength but rather problems in motor control. This

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
693
is what was kept in mind while planning the exercise regime of the group1, which enhanced the spinal segmental support and control. The subjects were trained to selectively contract the stabilizers by the help of stabilizer biofeedback and later worked on improving the endurance in terms of static control. This form of specific training at low levels of activation supports the recent findings of Cholewicke and McGill24 that only low levels of maximal voluntary contraction of the segmental muscles are required to ensure the stability of the spine in vivo. It is also consistent with assertion that motor learning and control are not simply a process of strength training, but depend on patterning and inhibition of motor neurons, with the acquisition of skills occurring through selective inhibition of unnecessary muscular activity, as well as the activation of additional motor units.
Further, Shaughnessy M25 in a pilot study discovered that program of lumbar stabilization is effective in improving quality of life and functional outcome in patients with chronic low back pain. A similar study conducted by Cholewicke and McGill11 revealed that lumbar stability is maintained in vivo by increasing the activity (stiffness) of the lumbar segmental muscles, and highlighted the importance of motor control to coordinate muscle recruitment between large trunk muscle and small intrinsic muscles during functional activities, to ensure stability is maintained. This concept when merged with that of Bergmark,25 specifying the classification of trunk muscles into local and global muscles, has overemphasized the need to train the deep muscles of the back to provide segmental stability while directly controlling the lumbar segments. The present study on segmental stabilisation has incorporated all these theories and has come out with an exercise regimen working directly at the deep stabiliser muscles. The positive result with a significant difference in terms of pain and functional ability thus supports the hypotheses put forth by eminent researchers as stated above. In addition to this, Tesh K M26 has also suggested that the muscles of the antero-lateral abdominal wall increase the stability of the lumbar region of the vertebral column by tensing the thoracolumbar fascia and by raising intra-abdominal pressure. Of the back extensor muscles, the lumbar muscles is considered to have the greatest potential to provide dynamic control to the motion segment, in its neutral zone. This study was considered important on account of the fact that patients of chronic low back pain would always seek not only a relief from pain but also the ability to perform ADL without discomfort. Hence, the patients need to be trained not only for the static control but also dynamic functional independence. With this view in mind, the exercises focused on the appropriate strengthening of the deep back muscles such that it can lead to alleviation of pain during motor tasks as well, thus aiming at complete recovery.
The most significant finding of the present study was the sustained reduction in symptoms and functional disability levels in the experimental groups at the 15th and 30th day follow up. The findings of this study support the view that a change in the motor program had occurred in both the group after the intervention, such that the automatic pattern of recruitment of the abdominals to stabilize the spine during a motor task incorporated higher levels of deep abdominal muscle activity. This appears to represent an enhanced ability, in those in the experimental group, to stabilize dynamically their spine during functional tasks. Hence it can very well be stated that stabilization exercises do appear to provide additional benefits to patients with sub acute or chronic low back pain who have no clinical signs suggesting the presence of spinal instability. Therefore, such population of chronic low back pain patients must be identified and treated with specific stabilizing exercise intervention based on motor control and motor learning in order to achieve efficient relief of excessive load from the spine, to enhance segmental stabilization and to control pain in a functional manner. Future Research
The significant difference in results observe in this study suggests the effectiveness of both exercise regimes, but also suggests the need for a more comprehensive research for future including patients with gross instability (evident radiologically) and side-to-side differences while administering stabilization exercises. Other factors such as role of age, gender, duration of study etc. may also be included in the future studies. Use of sophisticated devices such as electromyography biofeedback units, or real time ultrasound scanners might have made this study more sensitive in terms of generalization of results. Relevance to Clinical Practice
Since EMG was not used in this study, the results observed in this study suggest the cost effectiveness in assessing pain and disability as would be required in clinical settings (devoid of EMG and other sophisticated equipments to assess level of muscle imbalance). There are studies stating the

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
694
use of exercise regimes only (without electrotherapeutic modalities) in which patients have benefited and thus the exclusion of these does not pose to be unethical. Also, since no other modality was used, it is a cost–effective method of treatment, as would be preferred in clinical settings. Limitations The long term effect of the study could not be established due to lack of follow up on pain and
disability, after the thirty days of treatment. The home care programme taught to the patients could not be done under direct supervision. Apart from the clinical physical therapist palpating the transversus abdominis and multifidus muscle
contraction in the subjects, there was no other means of verifying whether these muscles were recruited appropriately.
Conclusion The findings of this trial support the view that the functional integration of Stabilizer Bio-
feedback training directed at the deep abdominals and the lumbar muscles are effective in reducing pain and functional disability in patients with chronic low back pain. This supports Punjabi’s hypothesis, that spinal stability is dependent on an inter play between the passive, active, and neural control systems. Specific training of the muscles considered to provide dynamics stability to the lumbar spine may act to maintain the neutral zones of the motions segment within more normal limits during functional activity. In addition, the results of this study indicate that a “Stabilizer Bio-Feedback” treatment approach directed at specific muscles activation is more effective than Core Stability Training commonly used in patients with chronic low back pain. References: 1. Anderson GBJ. Epidemiology features of chronic low back pain.Lancet 1999; 354: 581-585 2. Taylor VM, Deyo RA, Cherkin DC, Keuter W. Low back pain hospitalization: recent United
States trends and regional variation. Spine 1994; 19: 1207-1213 3.Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine 1995; 20: 11-19.pko;l./ 3. Frank A. Low back pain. BMJ 1993; 306: 901-909 4. Koes B, Bouter L, Beckerman H Physiotherapy Exercises and Back Pain: a blinded review,
British Medical Journal 1991; 302: 1572-1576. 5. Richardson CA, Jull GA Muscle control – pain control. What exercises would you prescribe?
Manual Therapy 1995; 1: 2-10. 6. Richardson C, Jull G, Hodges P, et al; Therapeutic Exercise for Spinal Segmental Stabilization in
Low Back Pain – Scientific Basis and Clinical Approach. Churchill Livingstone, Edinburgh. 1999.
7. Bergmark A Stability of the lumbar spine. A study in mechanical engineering. Acta Orthopaedica Scandinavica 1989; 230(Suppl): 20-24.
8. Hides JA, Richardson CA, Jull GA Multifidus muscle recovery is not automatic following resolution of acute first episode low pack pain. Spine 1996; 21: 2763-2769.
9. Hodges PW, Richardson CA Inefficient muscular stabilisation of the abdominis. Spine 1996; 21: 2640-2650.
10. Richardson CA, Snijders CJ, Hides JA, et al; The relationship between the transversely oriented abdominal muscles, sacroiliac joint mechanics and low back pain. Spine 2002; 27(4):399-405.
11. Hodges, P. and Moseley, L., Pain and motor control of the lumbopelvic region: effect andpossible mechanisms, J Electromyogr Kinesiol, 13 (2003) 361-70.
12. Hodges, P.W., B.P. Hons, and C. Richardson. Inefficient muscular stabilization of the lumbar spine associated with low back pain: A motor control evaluation of transversus abdominis. Spine 21:2640–2650. 1996.
13. Nichols, J.F., D. Medina, and E. Dean. Effects of strength, balance, and trunk stabilization training on measures of functionalfitness in older adults. Am. J. Med. Sports 3:279–285.2001.
14. Richardson, C.A., and G.A. Jull. Muscle control—pain control: What exercises would you prescribe? Man. Ther. 1:2–10.1995

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
695
15. Richardson, C., G. Jull, P. Hodges, and J. Hides. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach. Edinburgh, Scotland: Churchill Livingstone, 1999.
16. Mc Gills, S.M. Low back exercises: Evidence for improving exercise regimens. Phys. Ther. 78:754–765. 1998.
17. O’sullivan, P.B., G.D.M. Phyty, L.T. Twomey, and G.T. Allison. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine 22:2959–2967. 1997.
18. Stanton, R., P.R. Reaburn, and B. Humphries. The effect of short-term Swiss ball training on core stability and running economy. J. Strength Cond. Res. 18:522–528. 2004.
19. Mcgill, S., A. Childs, and C. Liebenson. Endurance times for low back stabilization exercises: Clinical targets for testing and training from a normal database. Arch. Phys. Med. Rehabil. 80:941–944. 1999.
20. Radebold A,Cholwicki J, PasnjabiMM, et al. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 2000;25;947-54
21. Richardson CA, Jull GA, Hodges P Hides . Therapeutic exercise for spinal segmental stabilization in low back pain scientific basis and clinical approach, Edinburgh, Churchill Livingstine ,1999
22. Cholewicki J, Mc G ill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech 1996; 11: 1-15.
23. Shaughnessy M, Caulfield B. Apilot study to investigate the effect of lumbar stabilization exercise training on functional ability and quality of life in patients with chronic low back pain. Int J Rehab Res. 2004 Dec;7(4):297-301.
24. Bergmark A . Stability of the lumbar spine. Acta Orthop Scand 1989;60:1-54. 25. Tesh KM, Dunn JS, Evans JH.The abdominal muscles and vertebral stability. Spine. 1987
Jun;12(5):501-8.

Research ArticleEffects of Functional Limb Overloading on SymmetricalWeight Bearing, Walking Speed, Perceived Mobility, andCommunity Participation among Patients with Chronic Stroke
Sami S. Alabdulwahab,1 Fuzail Ahmad,2 and Harpreet Singh3
1Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh 11952, Saudi Arabia2Department of Physical Therapy & Health Rehabilitation, College of Applied Medical Sciences, Majmaah University,Al-Majmaah 11451, Saudi Arabia3Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, New Delhi 110029, India
Correspondence should be addressed to Fuzail Ahmad; [email protected]
Received 19 May 2015; Revised 3 September 2015; Accepted 30 September 2015
Academic Editor: Ching-Yi Wu
Copyright © 2015 Sami S. Alabdulwahab et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Stroke is a leading cause for long-term disability that often compromises the sensorimotor and gait functionaccompanied by spasticity. Gait abnormalities persist through the chronic stages of the condition and only a small percentageof these persons are able to walk functionally in the community.Material and Method. Patients with chronic stroke were recruitedfrom outpatient rehabilitation unit at Department of Neurology & Neurosurgery, All India Institute of Medical Sciences, having ahistory of first stroke at least sixmonths before recruitment, with unilateral motor deficits affecting gait.The patients were randomlyassigned to either the functional limb overloading (FLO) or Limb Overloading Resistance Training (LORT) group and providedfour weeks of training. Result. We found that there was an improvement in gait performance, weight bearing on affected limb,and perceived mobility and community participation. Conclusion. To the best of our knowledge, this is the first study that hasevaluated the effects of functional limb overloading training on symmetric weight bearing, walking ability, and perceived mobilityand participation in chronic hemiplegic population. The study demonstrated a beneficial effect of training on all the outcomes,suggesting that the functional limb overloading training can be a useful tool in the management of gait problems in chronic strokepatients.
1. Introduction
Stroke is becoming a rapidly increasing problem and animportant cause of disability and deaths worldwide. Inci-dence and prevalence of strokes in Saudi Arabia are compar-atively lower than western countries, which could be becauseof the predominance of the younger age groups in this region[1]. The annual stroke incidence ranged from 27.5 to 63 per100,000 population and prevalence ranged from 42 to 68 per100,000 population [2].
Stroke is a leading cause for long-term disability due tocompromised sensorimotor function. Approximately 85% ofstroke survivors learn to walk independently by 6 monthsafter stroke, but gait abnormalities persist throughout the
chronic stages of the condition. Only a small percentageof stroke survivors are able to walk functionally in thecommunity [3, 4].
The objective of stroke rehabilitation is to enable individ-ual patients to maximize benefits from training in order toattain the highest possible degree of physical and psychologi-cal performance. The ultimate goals for many stroke patientsare to achieve a level of functional independence necessaryfor returning home and to integrate as fully as possible intocommunity life.
Ng and Hui-Chan [5] have noted that weakness inhemiplegic stroke patients is sometimes overshadowed overconcerns about treatment of spasticity and synergistic move-ments. Studies have revealed positive correlations between
Hindawi Publishing CorporationRehabilitation Research and PracticeVolume 2015, Article ID 241519, 6 pageshttp://dx.doi.org/10.1155/2015/241519

2 Rehabilitation Research and Practice
the strength of specific muscle groups and a variety of func-tional attributes [6]. Furthermore, a nonlinear relationshipbetween walking performance and muscle strength in thelower extremities has been suggested [7]. However, as theprotocols were multifaceted, it was not possible to determinethe precise role that the strength-training component mayhave played in improving walking function.
A number of studies have shown that task specificity andintensity of training are the main determinants of functionalimprovement after stroke [6, 8, 9].Moreover, there is growingevidence suggesting that intensive task-oriented practice caninduce greater improvement in walking competency thanusual practice in stroke survivors [10–12].
Yang et al. [13] in their study on stroke patients under-going progressive lower limb strengthening using functionalweight bearing activities foundmoderate increases inwalkingspeed. Sullivan et al. [14] found that task-specific trainingwith body-weight support is more effective in improvingwalking speed but lower limb strength training did notprovide any added benefit to walking outcomes.
A major limitation to the conclusions from these studiesand systematic reviews is the lack of consistency in theintervention and specified protocols [15–17]. Despite thenumber of studies dedicated to task-oriented training, noneof these studies had combined functional task training withprolonged resistance in the form of limb overloading applied90% of the awake time. Therefore, we designed this studyto address the evidence related to our training protocol toenhance symmetric weight bearing andwalking speed and itsimpact on perceived mobility and community participationin patients with chronic stroke.
We hypothesized that intervention programs that com-bine lower limb overload with functional task training wouldbe more effective at improving walking outcomes and com-munity participation than lower limboverload training alone.
Thedesign of our studywas influenced by the literature onlower extremity strength training and task-specific locomotortraining [14, 18, 19]. The use of this design should providevaluable comparisons that reveal the practical benefits offunctional limb overloading training to improve walkingoutcomes after stroke and its effect on perceived communityparticipation.
2. Material and Method
Chronic stroke patients were recruited from outpatient reha-bilitation unit at Department of Neurology & Neurosurgery,All India Institute of Medical Sciences. Patient having; (a)history of first stroke at least six months before recruitment,with unilateral motor deficits affecting gait pattern and/orspeed, (b) independent walking ability with or withoutwalking aid for at least 10m, and (c) ability to perform closed-chain exercise were selected for the study. Exclusion criteriaincluded significant psychiatric or cognitive deficits, majorcardiorespiratory diseases, chronic pain, or lower limb jointscomplication.
Study protocols were explained to patients and writteninformed consent was obtained from them. The patientswere then randomly assigned to either the functional limb
overloading (FLO) group or Limb Overloading ResistanceTraining (LORT) group by drawing one of two sealedenvelopes designating the group membership.
3. Management Protocol
The patients in FLO group underwent task-oriented gaittraining of one-hour duration three times per week forfour weeks. They were requested to wear the weight cuff,equivalent to 5% of the total body weight, for most of theirawake time (approximately 90% of the time). Brown et al.[18] in their study used 15% of the body weight for limboverloading during a cycling task. As our study required thepatients towearweighted cuffmost of their awake time and toperform functional taskswearing these cuffs, therefore, after apilot trial on few patients, we settled for 5%of the bodyweight(3–5Kg), which patients tolerated without much distress.
During the training session, after 5–10 minutes of simplewarm-up exercises, the patients performed various func-tional activities including forward, sideways, and backwardwalking, turning to 90 and 180 degrees during walking, stairclimbing, and so forth. During each session the patientswere also made to walk on treadmill for 15 minutes at speedof 10% above comfortable walking. The progression of thetraining was done by increasing the loading or steps height,or by reducing the speed, or decreasing the patient’s supportand/or doing more individually tailored sets, but as a rule thedifficulty level was adjusted after six sessions.
The patients in the LORT group underwent resistance-training regime consisting of isotonic exercise using weightcuff tied to ankle or foot.The exercise algorithmwas designedby the therapist accounting for strength as well as movementsynergy level, to determine repetition maximum (RM) withthe given load. The training protocol required each partici-pant to isotonically exercise the affected lower extremity (LE)using external resistance of weight cuff, equivalent to 5%of the total body weight. The training session consisted of5–10 minutes of simple warm-up exercises and then threesets of 10–15 repetitions maximum, to moderate fatiguewith limb overloading. The therapist follows an exercisealgorithm that accounted for the participant’s strength aswell as movement synergy level to determine RM for specificmuscle groups, including hip flexors, hip extensors, kneeflexors, knee extensors, ankle dorsiflexors, and ankle plantarflexors, with the given weight.
The outcomemeasures taken for this studywere Cadence,Fast Gait Speed (FGS), Slow Gait Speed (SGS), weightbearing on affected limb (WBAL), and perceived mobilityand participation of stroke patients.
The Walkway gait analysis system (TekScan, USA) wasused to capture plantar pressure data and temporal (time)and spatial (distance) gait parameters. This system consistsof a 5mm thickness of floor mat composed of 2,288 resistivesensors, with a resolution of 1.4 sensors/cm2, a sensor matrixmeasuring 439.5mm by 369.9mm, and a sampling frequencyof 40Hz.
Perceivedmobility and participation were assessed by thestroke impact scale (SIS) which is a self-report questionnaire

Rehabilitation Research and Practice 3
that assesses aspects of the impact of a stroke on an indi-vidual’s self-perceived health [20]. Interrater reliability andconcurrent validity have been found to be good for SIS [21].For our study, we have used only mobility and participationdomain of SIS. For each subject, the mean scores of itemsfrom mobility and participation section were calculatedand converted into percentage. High values represent noor few restrictions in participation and low values indicateparticipation that is more restricted.
An unequal group pretest-posttest design was used andthe group comparisons at baseline and after interventionwereanalysed using a 𝑡-test. An alpha level set at 0.05 determinedsignificance in two-sided hypothesis testing.
All analyses were performed using SPSS version 20.0.
4. Results
Twenty-six patients participated in this study. Three patientsin LORT group dropped out due to motivational reasons.
The mean age of the participants was 45.2 ± 12.5, 78% ofthem were male, and the remaining 22% were female. About44% of the participants had left side hemiplegia and 56% ofthem had right side hemiplegia (Table 1).
All the participants had stroke at least six months priorlywith a mean duration of 16 ± 10 months, unilateral motordeficits affecting gait, independent walking ability with orwithout walking aid, and ability to perform closed-chainexercise.
Table 2 shows the patient characteristics of both groupsat baseline. No statistically significant differences betweenboth groups were found with respect to the selected outcomevariables. No statistically significant differences were found(𝑝 < 0.05) with respect to measurement of Cadence, SGS,FGS, WBAL, and SIS.
Cadence showed an improvement of 33% (𝑡 = 5.03, 𝑝 =0.001∗) and 28% (𝑡 = 2.34, 𝑝 = 0.044∗) in FLO and LOTR
group, respectively, which were statistically significant.The posttest values of SGS suggested an increase of 47%
(𝑡 = 3.62, 𝑝 = 0.004∗) and 32% (𝑡 = 2.6, 𝑝 = 0.029∗),respectively, in FLO and LOTR groups. However the FastGait Speed (FGS) improved by 34% (𝑡 = 4.68, 𝑝 = 0.001∗)and 21% (𝑡 = 2.28, 𝑝 = 0.049∗), respectively, in the FLOand LOTR groups. These improvements were found to bestatistically significant (Tables 3 and 4).
To find the difference between both groups an indepen-dent 𝑡-test was used which showed 19.4% (𝑡 = 2.45, 𝑝 =0.024∗) improvement in Cadence, 55.3% (𝑡 = 2.81, 𝑝 =
0.011∗) improvement in SGS, 45% (𝑡 = 2.47, 𝑝 = 0.023∗)
improvement in FGS, 12.8% (𝑡 = 2.19, 𝑝 = 0.040∗)improvement in WBAL, and 14.3% (𝑡 = 2.27, 𝑝 = 0.046∗)improvement in SIS scores after training (Table 5, Figure 1).
Posttraining weight bearing on affected limb improvedsignificantly by 11% (𝑡 = 2.75, 𝑝 = 0.018∗) in FLO group,while very little improvement in LORT group was detected.
Perceived mobility and community participation signif-icantly improved to 16% in the FLO group (𝑡 = 2.69, 𝑝 =0.020∗). In contrast, they showed insignificant improvement
(6%) in LORT group (𝑡 = 1.71, 𝑝 = 0.121). (Table 5,Figure 1).
Table 1: Descriptive statistics.
%GenderFemale 21.7Male 78.3
Side affectedLeft side 43.5Right side 56.5
Duration since stroke onset6–12 months 30.41-2 years 56.52-3 years 13.0
Table 2: Between-group comparison of the dependent variable atbaseline.
Variables FLO LORT Independent 𝑡-test𝑁 = 13 𝑁 = 10 𝑡 𝑝
Age 45.3 + 12.3 44.7 + 14.1 0.12 0.911Cadence 61.1 + 12.2 53.4 + 15.4 0.98 0.161SGS (m/s) 31.9 + 15.9 22.8 + 11 1.50 0.149FGS (m/s) 59.8 + 26.2 45.5 + 17.7 1.58 0.131WBAL 40.2 + 6.9 38.4 + 8.2 0.31 0.759SIS 55.6 + 7 53.1 + 10.4 0.91 0.376SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
Table 3: Within-group comparison of the dependent variable inFLO group.
VariablesPretest Posttest PairedM ± SD M ± SD 𝑡-test𝑁 = 13 𝑁 = 13 𝑡 𝑝
Cadence 61.1 ± 12.2 81.8 ± 13.8 5.03 5.03SGS (m/s) 31.9 ± 15.9 46.9 ± 15.9 3.62 0.004∗
FGS (m/s) 59.8 ± 26.2 80.50 ± 30 4.68 0.001∗
WBAL 40.2 ± 6.9 44.9 ± 3.4 2.75 0.018∗
SIS 55.6 ± 7 64.6 ± 3.4 2.69 0.020∗
SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
Table 4: Within-group comparison of the dependent variable inLORT group.
VariablesPretest Posttest PairedM ± SD M ± SD 𝑡-test𝑁 = 10 𝑁 = 10 𝑡 𝑝
Cadence 53.4 ± 15.4 68.5 ± 14.5 2.34 2.34SGS (m/s) 22.8 ± 11 30.2 ± 11 2.6 0.029∗
FGS (m/s) 45.5 ± 17.7 55.5 ± 24.1 2.28 0.049∗
WBAL 38.4 ± 8.2 39.8 ± 6.9 0.86 0.412SIS 53.1 ± 10.4 56.5 ± 6.8 1.71 0.121SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.

4 Rehabilitation Research and Practice
Table 5: Posttest between-group comparisons of the dependentvariables.
Variables FLO LORT Independent 𝑡-test𝑁 = 13 𝑁 = 10 𝑡 𝑝
Cadence 81.8 ± 13.8 68.5 ± 14.5 2.45 0.024∗
SGS (m/s) 46.9 ± 15.9 30.2 ± 11 2.81 0.011∗
FGS (m/s) 80.50 ± 30 55.5 ± 24.1 2.47 0.023∗
WBAL 44.9 ± 3.4 39.8 ± 6.9 2.19 0.040∗
SIS 64.6 ± 3.4 56.5 ± 6.8 2.27 0.046∗
SGS: Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
0102030405060708090
Cadence SGS FGS WBAL SIS
68.5
30.2
55.5 56.5
81.8
46.9
80.5
64.6
44.939.8
LOTRFLO
Figure 1: Posttest intragroup comparison of outcome variables. SGS:Slow Gait Speed, FGS: Fast Gait Speed, WBAL: weight bearing onaffected limb, and SIS: stroke impact scale score.
5. Discussion
The aim of the present study was to find the efficacyof functional limb loading training on gait performance,weight bearing on affected limb, and perceived mobility andcommunity participation in chronic community dwellingstroke patients. In our study we found an improvement inall the selected variables. In patient with chronic stroke,the common impairments associated with muscle strength,motor control, and balance appear to have the strongestrelationwithwalking [22]; therefore these improvementsmaybe due to the increased physical activity undertaken duringthe training period as it is well documented that patientswith chronic stroke have relatively sedentary lifestyle withlittle physical activities [23]. In the present study, the fourweeks of training resulted in symmetric weight bearing andimproved gait function, which may be due to the improvedmuscle strength, coordination, and sensory organizationcaused by functional overloading of the affected limb. Thelower limb overloading along with functional activities couldhave increased the weight bearing on the affected leg and theproprioceptive stimuli to the joints of the paretic leg causingincreased stability.
The significant improvement in terms of weight bearingsymmetry on affected leg could be due to the changes inbiomechanical alignment of the body, resulting in equaltransfer of body weight to both lower limbs. These results
can be explained based on previous studies, which suggestthat the hemiplegic patients showing asymmetric lower limbweight bearing generally had associated sensory derange-ments and proprioceptive stimulation can influence posturalcontrol and ambulation in such patients [24]. The complexmechanisms, which contribute to gait, and the varyingenvironments demands during functional mobility requireinterventions that can addresses different elements underly-ing walking. Impaired ability of the paretic limb to maintainsymmetrical loading affects balance and gait. Hendrickson etal. [25] suggested that rehabilitation strategies that increasethe contribution of the paretic limb to standing balancecontrol may increase symmetry of walking after stroke. Theimprovement shown by the subjects in the FLO group maybe due to the continuous loading provided to them, whichamounted to approximately 90% of awake time.
Even though the effects of resistance training on gaitperformance are less clear, various studies have demonstratedstrong correlations between walking speed and lower limbmuscle strength of the paretic side suggesting its positiveeffect on gait speed and endurance [26]. The curvilinearrelationship between muscle strength and functional skillssuggests that further improvements in strength after theachievement of functional level may not lead to any sub-stantive gains. Therefore, the significant improvement in theweight bearing on affected lower limb and gait performancein our study may be because of the fact that limb over-loading is incorporated with functional activities directedat improving the gait function. The results of our studysubstantiate the strong evidence suggesting that task-specifictraining can assist with functional motor recovery, which isdriven by adaptive neural plasticity [27]. In this study, thesubjects in functional limb overloading training showed astatistically significant improvement in perceived mobilityand community participation. The findings are similar tothe study done by Flansbjer et al. [28] assessing the effectof progressive resistance training on perceived participationin stroke patient, which found that improvements in gaitperformance were related to improvements in perceived par-ticipation. Other studies measuring changes in function anddisability found that self-reported limitations in performinglife tasks decreased following resistance training.
6. Conclusion
To the best of our knowledge, this is the first study that hasevaluated the effects of functional limb overloading trainingon weight bearing on affected limb, walking ability, andperceived mobility and community participation in chronichemiplegic population. The study demonstrated a beneficialeffect of training on all the outcomes, suggesting that thefunctional limb overloading training can be a useful tool inthe management of gait problems in chronic stroke patients.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.

Rehabilitation Research and Practice 5
Acknowledgments
This research was funded by Sheikh Abdullah Bin AbdulMohsen Al Tuwaijri Chair for Applied Research in Stroke,Majmaah University, Saudi Arabia.The authors would like toexpress their gratitude towards Sheikh Abdullah Al Tuwaijri,Rector Dr. Khalid Bin Saad Al Muqrin, and Chair SupervisorDr. Raid SAl Baradie for providing the necessary support andassistance for completing this piece of work.
References
[1] A. A. Robert and M. M. Zamzami, “Stroke in Saudi Arabia: areview of the recent literature,” PanAfricanMedical Journal, vol.17, article 14, 2014.
[2] H. T. S. Benamer and D. Grosset, “Stroke in Arab countries: asystematic literature review,” Journal of the Neurological Sci-ences, vol. 284, no. 1-2, pp. 18–23, 2009.
[3] D. T. Wade, V. A. Wood, A. Heller, J. Maggs, and R. LangtonHewer, “Walking after stroke. Measurement and recovery overthe first 3 months,” Scandinavian Journal of RehabilitationMedicine, vol. 19, no. 1, pp. 25–30, 1987.
[4] S. Mulroy, J. Gronley, W. Weiss, C. Newsam, and J. Perry, “Useof cluster analysis for gait pattern classification of patients inthe early and late recovery phases following stroke,” Gait andPosture, vol. 18, no. 1, pp. 114–125, 2003.
[5] S. S. Ng and C. W. Hui-Chan, “Contribution of ankle dorsi-flexor strength to walking endurance, in people with spastichemiplegia after stroke,” Archives of Physical Medicine andRehabilitation, vol. 93, no. 6, pp. 1046–1051, 2012.
[6] G. V. Smith, K. H. C. Silver, A. P. Goldberg, and R. F. Macko,“‘Task-oriented’ exercise improves hamstring strength andspastic reflexes in chronic stroke patients,” Stroke, vol. 30, no.10, pp. 2112–2118, 1999.
[7] C. Carvalho, K. S. Sunnerhagen, and C. Willen, “Walkingperformance and muscle strength in the later stage poststroke:a nonlinear relationship,” Archives of Physical Medicine andRehabilitation, vol. 94, no. 5, pp. 845–850, 2013.
[8] G. Kwakkel, R. Van Peppen, R. C. P. Wagenaar et al., “Effects ofaugmented exercise therapy time after stroke: a meta-analysis,”Stroke, vol. 35, no. 11, pp. 2529–2536, 2004.
[9] C.M.Dean,C. L. Richards, andF.Malouin, “Task-related circuittraining improves performance of locomotor tasks in chronicstroke: a randomized, controlled pilot trial,”Archives of PhysicalMedicine and Rehabilitation, vol. 81, no. 4, pp. 409–417, 2000.
[10] N. M. Salbach, N. E. Mayo, S. Wood-Dauphinee, J. A. Hanley,C. L. Richards, and R. Cote, “A task-orientated interventionenhances walking distance and speed in the first year poststroke: a randomized controlled trial,” Clinical Rehabilitation,vol. 18, no. 5, pp. 509–519, 2004.
[11] C. K. English, S. L. Hillier, K. R. Stiller, and A. Warden-Flood, “Circuit class therapy versus individual physiotherapysessions during inpatient stroke rehabilitation: a controlledtrial,” Archives of Physical Medicine and Rehabilitation, vol. 88,no. 8, pp. 955–963, 2007.
[12] L. Wevers, I. van de Port, M. Vermue, G. Mead, and G.Kwakkel, “Effects of task-oriented circuit class training onwalking competency after stroke. A systematic review,” Stroke,vol. 40, no. 7, pp. 2450–2459, 2009.
[13] Y.-R. Yang, R.-Y. Wang, K.-H. Lin, M.-Y. Chu, and R.-C.Chan, “Task-oriented progressive resistance strength trainingimproves muscle strength and functional performance in indi-viduals with stroke,” Clinical Rehabilitation, vol. 20, no. 10, pp.860–870, 2006.
[14] K. J. Sullivan, D. A. Brown, T. Klassen et al., “Effects of task-specific locomotor and strength training in adults who wereambulatory after stroke: results of the STEPS randomizedclinical trial,” Physical Therapy, vol. 87, no. 12, pp. 1580–1602,2007.
[15] C. Meek, A. Pollock, J. Potter, and P. Langhorne, “A systematicreview of exercise trials post stroke,” Clinical Rehabilitation, vol.17, no. 1, pp. 6–13, 2003.
[16] J. J. Eng and P.-F. Tang, “Gait training strategies to optimizewalking ability in people with stroke: a synthesis of the evi-dence,” Expert Review of Neurotherapeutics, vol. 7, no. 10, pp.1417–1436, 2007.
[17] R. Teasell, N. Foley, K. Salter, J. Jutai, and M. Speechley,Evidence-Based Review of Stroke Rehabilitation Executive Sum-mary, 13th edition, 2010, http://brainstreams.ca/sites/default/files/EBRSR-Executive-summary-Ed13.pdf.
[18] D. A. Brown, S. Nagpal, and S. Chi, “Limb-loaded cyclingprogram for locomotor intervention following stroke,” PhysicalTherapy, vol. 85, no. 2, pp. 159–168, 2005.
[19] R. Fernandez-Gonzalo, C. Nissemark, B. Aslund, P. A. Tesch,and P. Sojka, “Chronic stroke patients show early and robustimprovements in muscle and functional performance inresponse to eccentric-overload flywheel resistance training: apilot study,” Journal of NeuroEngineering and Rehabilitation, vol.11, article 150, 2014.
[20] P. W. Duncan, D. Wallace, S. M. Lai, D. Johnson, S. Embretson,and L. J. Laster, “The stroke impact scale version 2.0. Evaluationof reliability, validity, and sensitivity to change,” Stroke, vol. 30,no. 10, pp. 2131–2140, 1999.
[21] B. Edwards and B. O’Connell, “Internal consistency and validityof the Stroke Impact Scale 2.0 (SIS 2.0) and SIS-16 in anAustralian sample,” Quality of Life Research, vol. 12, no. 8, pp.1127–1135, 2003.
[22] A. Weiss, T. Suzuki, J. Bean, and R. A. Fielding, “High intensitystrength training improves strength and functional perfor-mance after stroke,” American Journal of Physical Medicine andRehabilitation, vol. 79, no. 4, pp. 369–376, 2000.
[23] M. M. Ouellette, N. K. LeBrasseur, J. F. Bean et al., “High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors,”Stroke, vol. 35, no. 6, pp. 1404–1409, 2004.
[24] J. C. Outermans, R. P. Van Peppen, H. Wittink, T. Takken, andG. Kwakkel, “Effects of a high-intensity task-oriented trainingon gait performance early after stroke: a pilot study,” ClinicalRehabilitation, vol. 24, no. 11, pp. 979–987, 2010.
[25] J. Hendrickson, K. K. Patterson, E. L. Inness, W. E. McIlroy,and A. Mansfield, “Relationship between asymmetry of quietstanding balance control and walking post-stroke,” Gait andPosture, vol. 39, no. 1, pp. 177–181, 2014.
[26] L. F. Teixeira-Salmela, S. Nadeau, I. McBride, and S. J. Olney,“Effects of muscle strengthening and physical conditioningtraining on temporal, kinematic and kinetic variables duringgait in chronic stroke survivors,” Journal of RehabilitationMedicine, vol. 33, no. 2, pp. 53–60, 2001.

6 Rehabilitation Research and Practice
[27] L. G. Richards, K. C. Stewart, M. L. Woodbury, C. Senesac,and J. H. Cauraugh, “Movement-dependent stroke recovery:a systematic review and meta-analysis of TMS and fMRIevidence,” Neuropsychologia, vol. 46, no. 1, pp. 3–11, 2008.
[28] U.-B. Flansbjer, D. Downham, and J. Lexell, “Knee musclestrength, gait performance, and perceived participation afterstroke,”Archives of Physical Medicine and Rehabilitation, vol. 87,no. 7, pp. 974–980, 2006.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com

Volume 8 Number 4 October-December 2014
Published, Printed and Owned : Dr. R.K. SharmaDesigned and Printed : M/s Vineeta Graphics, B-188, Subash Colony, Ballabgarh, FaridabadPublished at :
Editor : Dr. R.K. Sharma, Mobile:
4 Floor, Statesman House Building,Barakhamba Road,Connaught Place,New Delhi-110 001
th
91-9971888542, Fax No: +91 11 3044 6500

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 259DOI Number: 10.5958/0973-5674.2014.00344.X
Relative & Cumulative efficacy of Auditory & VisualImagery on Upper Limb Functional Activity among
Chronic Stroke Patients
Fuzail Ahmad1, Sami Al-Abdulwahab2, Nasser Al-Jarallah3, Raidah Al-Baradie4, Mohammad Z Al-Qawi5,Faizan Z Kashoo6, Harpreet S Sachdeva7
1Head, Department of Physical Therapy, College of Applied Medical Sciences, Majmaah University, Kingdom ofSaudi Arabia, 2Professor, Department Rehabilitation Sciences, College of Applied Medical Sciences, King Saud
University, Riyadh, Kingdom of Saudi Arabia, 3Dean, College of Applied Medical Sciences, Majmaah University,Kingdom of Saudi Arabia, 4Consultant Neurologist, Neuroscience Center, King Fahd Specialist Hospital, Departmentof Pediatrics, Dammam University, Dammam, Saudi Arabia, 5Head Stroke Unit, King Faisal Specialist Hospital and
Research Center, Riyadh. Kingdom of Saudi Arabia,6Department of Physical Therapy, College of Applied MedicalSciences, Majmaah University, Kingdom of Saudi Arabia, 7Physical Therapist, Department of Neurology &
Neurosurgery, CN Centre, All India Institute of Medical Sciences, New Delhi, India
ABSTRACT
Introduction: Stroke is a very limiting disease for the patient and a major health problem in mostparts of the world. Activity limitations of the upper extremity are a common finding for individualsliving with the effects of stroke, with its prevalence reported between 33% and 95% of this population.This study aims to explore whether imagery involves the activation of primary sensory cortices andto determine the therapeutic effectiveness and benefits of mental imagery training for arm functionin chronic stroke patients.
Material & Method: The study was conducted as a randomized, pre-post pilot project with fourpatient groups. Patients underwent imagery ability screening using the mental chronometry,autonomic monitoring before group allocation and randomization. We also assessed the patients onMotor Activity Log (MAL) to assess motor impairment in the affected Upper extremity. F-wave, fMRI along with MAL was administered.
Result Recovery between baseline and outcome assessment was evident on all outcome variables.However, no differences between the three groups were found on the primary outcome measure.
Conclusion: The results support the efficacy of programs incorporating mental practice forrehabilitating affected arm function in patients with chronic stroke. Mental imagery is a clinicallyfeasible, cost-effective complement to the therapy that may improve outcomes more than participationin therapy only. This concept in the clinical settings can provide an additional benefit in improvingthe upper limb function in stroke patients.
Keywords: Stroke, Hemiplegia, Mental Imagery, Stroke Rehabilitation
INTRODUCTION
Stroke is a sudden loss of brain function caused bythe interruption of flow of blood to the brain or therupture of blood vessels in the brain1. Stroke is a verylimiting disease for the patient and a major health
problem in most parts of the world. People whoexperience a stroke may undergo sudden and intensechanges in perception, cognition, mood, speech,health-related quality of life, and function2.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM259

260 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Activity limitations of the upper extremity are acommon finding for individuals living with the effectsof stroke, with its prevalence reported between 33%and 95% of this population. These activity limitationsmay occur because of deficits in body structures andfunctions caused by the stroke, such as in motor ability,somatosensation and perceptual ability3.
Traditional stroke rehabilitation therapies addressthis incompatibility by using behavior repetition. Thehope is that repeated physical practice will improvemotor activity, allowing for smooth and controlledmovements to occur, acting as examples for the brainto use in reestablishing the circuitry that mediatesvoluntary movement4-5.
This has led to a variety of interventions thatrehabilitation professionals, may use to maximize theupper extremity function of the individuals, they treat6.
Recently, mental imagery; a technique throughwhich an individual repeatedly mentally rehearses anaction or task without actually physically performingthe action or task have become additional therapyinterventions7.
As the current approaches to stroke rehabilitationis characterized by multiple and unsubstantiatedphilosophies and a tendency to invest efforts in thosewith severe stroke and in goals limited to self-care it isposited that mental practice could be a non-invasive,useful tool in rehabilitating patients with strokes.
This study aims to explore whether imageryinvolves the activation of primary sensory cortices andto determine the therapeutic effectiveness and benefitsof mental imagery training for arm function in chronicstroke patients.
METHODOLOGY
The study was conducted as a randomizedcontrolled trial with four groups; auditory imagerygroup (EA); visual imagery group (EV); cumulativeimagery group (EC) & control group (CG). Subjectsaged having first episode of unilateral stroke within1-6 months with not more than grade 3 spasticity onMotor Assessment Scale (MAS) in the affected upperextremity, without any severe cognitive deficits,aphasia, rheumatologic or musculoskeletal damage inthe affected upper extremity, were selected for thisstudy. The patients were excluded from the study ifthey did not perceive upper extremity motor
weakness. Patients were excluded from the study ifthey were discharged from hospital within 1 week anddid not present with an upper limb motor weakness
All the patients signed an informed consent thenunderwent imagery ability screening using the mentalchronometry before group allocation andrandomization.
Outcome Measures
Action Research Arm Test (ARAT) was used forassessing the functional limitations of the upper limb(UL) on the affected side. It includes 19 items dividedinto four subscales: grasp, grip, pinch, and grossmovement. Reliability (interrater = 0.99, test-retest =0.98), construct validity, and predictive validity of theARAT have been well-established8.
Motor Activity Log (MAL)9, is a focal measure ofself-perceived disability on tasks requiring UL use. Itis used for assessing how much and how well patientsuse their affected arm for activities of daily living(ADL). Thirty specific ADL tasks are evaluated withthe use of a 6-poin amount of use (AOU) scale and a 6-point quality of movement (QOM) scale.
Levels of independence and functional limitationswere evaluated with regards to Activities of DailyLiving using the Barthel Index (BI)10 covering items ofambulation, body care, mobility, alertness andcommunication.
Intervention Protocol
All the four groups received single task trainingduring the physiotherapy sessions in the interventionprogram. The selected task in the study experimentconsisted of four discrete stages; sit upright with handsupported on the lap, reach for and grasp the cup, liftthe cup and drink a sip of water, extend your arm andkeep the cup back to starting point, grasp release, handback to lap. The task was selected since it wasconsidered familiar and not complex for single sessiontraining; moreover, the task involves unilateralextremity activity.
Fig. 1. Discrete stages of the selected task.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM260

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 261
The experimental groups received training withauditory, visual or both auditory and visual imagerytechniques. A blinded examiner performed thescreening assessments and recorded outcomemeasures at baseline (BA), and immediately after thetraining session (TS) on the same day. In total thetreatment time was about 45 – 50 minutes.
RESULTS
Randomization, using a statistical minimizing
procedure, was successful and no group differencesat baseline were found on all the outcome measure oron any of the other demographic or clinicalcharacteristics.
At baseline MAL-QOM score for EA, EV, EAVgroup patients were 3.4+0.5, 3.8+0.5 & 3.3+1, whichhave been changed post training to 3.8+0.6, 4+0.9 and3.7+0.6 respectively. Median MAL-QOM score forcontrol patients before the intervention was 3.4 + 0.6;and the post-intervention score was 3.5 + 0.4.
Table 1: Comparison between baseline and post-training scores of motor activity log.
EA M+SD EV M+SD EC M+SD CG M+SD Kruskal–Wallis test
N=3 N=3 N=3 N=3
X2 P
QOM BA 3.4+0.5 3.8+0.5 3.3+1 3.4+0.6 0.423 0.672
QOM TS 3.8+0. 6 4+0.9 3.7+0.6 3.5+0.4 1.311 0.921
AOU BA 3.8+0.9 3.5+0.8 3.7+0.5 3.9+0.7 0.08 0.934
AOU TS 3.6+0. 6 3.9+0.7 3.2+0.8 3.4+0.5 1.35 0.177
Keys: EA-Auditory Imagery Group EV-Visual Imagery Group EC-Cumulative Imagery Group CG-Control Group, QOM-Quality ofMovement, AOU-Amount of Use
Similarly, at baseline MAL-AOU score for EA, EV,EAV group patients were which have been changed3.8+0.9, 3.5+0.8, 3.7+0.5 post training to 3.6+0.6, 3.9+0.7,3.2+0.8 respectively. Median MAL-AOU score forcontrol patients before the intervention was 3.9+0.7and 3.4+0.5 post-intervention.
There were no differences in motor imagery abilitybetween the treatment groups (Table 2). Control datacollected with age-matched neurologically intacthealthy volunteers on the same measure with the righthand, suggests no difference in motor imagery abilitybetween participants.
No differences between the three groups werefound on the primary outcome measure, the ARAT
(Table 3). Neither were there differences between thegroups on measures of functional impairment.Improvement on the primary outcome measure, theARAT score, correlated with improvement on thesecondary outcome measures of activities of dailyliving level, (r�=� 0.23, P�<� 0.05), QOM-AOU(r�=� -0.60, P�< �0.001), and BI (r�=� -0.25,P�<�0.01), but not with MAL-QOM(r�=�0.12, n.s).Mental status questionnaire score at baseline showeda significant relationship with improvement onactivities of daily living level (r�=�-0.26, P�<�0.01)but not with improvement on any of the other outcomemeasures (P�>�0.12).
Table 2: Between Group mean performance and ANCOVA analysis group differences on primary and secondaryoutcome measures.
Group n Baseline Post-training Between groupassessment assessment difference
Mean (SD) Mean (SD) P-value
Action Reach Arm Test (ARAT)
Mental Imagery Training- Auditory 10 21.22 (14.20) 26.33 (19.24) 0.77 0.35
Mental Imagery Training-Visual 10 25.64 (18.10) 31.51 (20.68)
Mental Imagery Training-Cumulative 10 26.23 (17.92) 32.87 (20.76)
Control-Group 10 23.06 (17.66) 30.38 (20.53)
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM261

262 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Table 2: Between Group mean performance and ANCOVA analysis group differences on primary and secondaryoutcome measures. (Contd.)
Group n Baseline Post-training Between groupassessment assessment difference
Mean (SD) Mean (SD) P-value
Motor Assessment Log (QOM)
Mental Imagery Training- Auditory 10 3.4 (.52) 3.8 (.63) 0.98 0.14
Mental Imagery Training-Visual 10 3.8 (.52) 4 (.93)
Mental Imagery Training-Cumulative 10 3.3 (.97) 3.7 (.59)
Normal Care Control 10 3.4 (.62) 3.5 (.42)
Motor Assessment Log (AOU)
Mental Imagery Training- Auditory 10 3.8 (.87) 3.6 (.63) 0.38 0.19
Mental Imagery Training-Visual 10 3.5 (.81) 3.9 (.73)
Mental Imagery Training-Cumulative 10 3.7 (.53) 3.2 (.79)
Normal Care Control 10 3.9 (.74) 3.4 (.53)
Barthel Index
Mental Imagery Training- Auditory 10 55.20 (11.02) 47.28 (15.16) 0.98 0.54
Mental Imagery Training-Visual 10 58.40 (15.02) 50.28 (18.78)
Mental Imagery Training-Cumulative 10 64.16 (14.04) 55.42 (15.81)
Normal Care Control 10 62.50 (14.26) 53.49 (18.68)
There were no differences in motor imagery abilitybetween the treatment groups [F(2,97)�=�0.65,P�=�0.52). Control data collected with age-matchedneurologically intact healthy volunteers on the samemeasure with the right hand, suggests no differencein motor imagery ability between participants in thetrial and healthy controls [F(1,142)� =� 1.56,P�=�0.21, Graphic�=�0.01]. Motor imagery abilityof the participants in the trial correlated with changebetween baseline and outcome assessments on theprimary outcome measure, the ARAT difference score(r�=�0.28, P�=�0.002). However, within the ‘MotorImagery Training’ group, motor imagery ability wasnot correlated with ARAT change scores (r�=�0.12,P�=�0.23).
Fig. 1. Difference in various outcomes selected for this study.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM262

Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4 263
DISCUSSION
The aim of this study was to evaluate thetherapeutic benefit of mental practice in sub-acutestroke patients with a moderate motor weakness. Therationale for the efficacy of mental practice in stroke isthat activation of motor brain areas through imagerywill enhance brain plasticity. If the neural principle of‘firing is rewiring’ applies to mental practice in stroke,than we would expect to find a clinical benefit inpatients’ early post-stroke. Processes of functionalredistribution have been demonstrated in earlyrecovery and have been linked to physical practice. Ifthe underlying mechanisms of mental practice can beattributed to brain plasticity rather than motivationalor cognitive factors, then we should see enhancedrecovery in stroke patients participating in mentalpractice independent of physical practice ofmovements11. In the design of this study a number offactors were carefully considered in order to providea more direct evaluation of this plasticity account.Mental practice was not embedded in physical therapy,which was instead offered to all participants as part ofnormal care, in order to provide a more directevaluation of the plasticity account12.
This relates to the issue of combined physical andmental practice. An important part of the rationale ofthe current trial was to exclude the possibility thatmental practice merely provides prolongedopportunity to consolidate particular movementpatterns, and find a more direct indication that mentalpractice works through processes of brain plasticityindependent of the effects of physical movement. Sincewe previously found that combined mental andphysical practice gave improvement on the trainedtask only13, We felt it was necessary to evaluate thebenefit of mental practice when not combined withphysical practice of the movements. The prudence ofevaluating motor imagery training independent ofmotor performance was also pointed out by Sharmaand colleagues14. Previous studies combined mentalpractice with physical practice. In their mental practiceevaluations Page and colleagues15 reported a clinicalbenefit for mental practice in a series of small studiesand one randomized controlled trial. The placebocondition was always audiotape-led relaxation. Thismeans that patients in the treatment group had anopportunity during mental practice to consolidatemovement patterns that they earlier had beenpracticing physically, while the control group did not
have this advantage. The benefit of combined physicaland mental practice can therefore be attributed to anyof the following mechanisms. The mental practiceextended engagement with motor processes, whichmay give rise to enhanced cognitive models ofperformed movements, or may even have amotivational effect. Alternatively, it is possible that anindirect effect of neuroplasticity accounts for thefindings, where mental practice reactivates recentlyused motor representations allowing for an increasedeffect of the physical practice itself. However, all theseexplanations would imply that the benefit of mentalpractice is not independent of physical practice, anddoes not provide a ‘backdoor to the motor systemsafter stroke’ or form an alternative if physical practiceis not possible16.
Furthermore, as patients performed well on theobjective motor imagery ability measure, it is alsounlikely that patients were unable to benefit frommental practice due to impaired motor imagery. It ispossible that spontaneous recovery in these sub-acutepatients masked the subtle benefit of mental practice,but again the reported small effect sizes of thetreatment effects in this study do not suggest this.
As such, the finding of the current carefullycontrolled powered trial, representative of the strokepopulation, is important in the evaluation of thetherapeutic benefit of mental practice. Future researchwill need to investigate the role of both chronic patientstatus and prolonged mental practice in clarifying thetherapeutic benefit of cumulative mental practice instroke.
CONCLUSION
The results support the efficacy of programsincorporating mental practice for rehabilitatingaffected arm function in patients with chronic stroke.Mental imagery is a clinically feasible, cost-effectivecomplement to the therapy that may improveoutcomes more than participation in therapy only. Thisconcept in the clinical settings can provide anadditional benefit in improving the upper limbfunction in stroke patients.
Acknowledgment: I would like to express mygratitude towards Sheikh Abdullah bin Abdul MohsenAl-Tuwaijri, Dr. Raid Al-Baradie and Majmaah Universityfor providing the necessary support for completing thispiece of work.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM263

264 Indian Journal of Physiotherapy & Occupational Therapy. October-December 2014, Vol. 8, No. 4
Source of Funding: This research was funded bySheikh Abdullah bin Abdul Mohsen Al-Tuwaijri Chairfor Applied Research in Stroke at Majmaah University,Al-Majmaah, Saudi Arabia.
Ethical Clearance was taken from the InstitutionalReview Board, Centre for Basic and Applied MedicalSciences at Majmaah University.
Conflict of Interest: Nil
REFERENCES
1. Heart and Stroke Foundation of Canada. Whatis a stroke? http://www.heartandstroke.com/site/c.ikIQLcMWJtE/b.3483935/k.A279/WhatÿisÿStroke.html
2. Mayo N, Wood-Dauphinee S, Ahmed S, GordonC, Higgins J, McEwen S, et al. Disablementfollowing stroke. Disability and Rehabilitation1999; 21(5/6):258–68.
3. Andrews AW, Bohannon RW. Short-termrecovery of limb muscle strength after acutestroke. Archives of Physical Medicine andRehabilitation 2003; 84:125–30.
4. Kosslyn, S.M., Ball, T.M., & Reiser, B.J. Visualimages preserve metric spatial information:Evidence from Studies of image Scanning.Journal of Experimental Psychology: Human,Perception and Performance, 1978:Vol.4, No.1,47-60
5. Jackson PL, Doyon J, Richards CL, Malouin F.Potential role of mental imagery using motorimagery in neurological rehabilitation. Arch PhysMed Rehabil 2001; 82:1133-41.
6. Baddeley, A.D. & Logie, R. Auditory imagery andworking memory. In Auditory Imagery, D.Reisberg, (Ed.), 179-197, Lawrence ErlbaumAssociates, Inc. Publishers, ISBN 0-8058-2292-5,New Jersey, USA
7. Dijkerman HC1, Ietswaart M, Johnston M,MacWalter RS. Does motor imagery trainingimprove hand function in chronic stroke patients?
A pilot study. Clin Rehabil. 2004 Aug; 18(5):538-49.
8. Leeuwen van R, Inglis J. Mental imagery andimagery: a potential role in stroke rehabilitation.Phys Ther Rev 1998; 3:47-52.
9. Taub E, Morris D, Bowman M, Delgado A,Uswatte G. Upper-Extremity Motor Activity Log[Manual].(Available from Edward Taub,Psychology Department, UAB, CH415,Birmingham, Ala); 1996.
10. Mahony FL, Barthel DW. Functional evaluation.The Barthel Index. Maryland State Med J1965;14:61-5.
11. Pylyshyn, Z.W. Mental imagery: In search of atheory. Behavioral & Brain Sciences,2002; Vol25,No.2, 157-238
12. Watson, J., Myers, R., Frackowiak, R., Hajnal, J.,Woods, R., Mazziotta, J., Shipp, S., & Zeki, S. AreaV5 of the human brain: Evidence from acombined study using positron emissiontomography and magnetic resonance imaging.Cerebral Cortex, 1993: Vol.3, No.2, 79–94
13. Sharma N1, Pomeroy VM, Baron JC. Motorimagery: a backdoor to the motor system afterstroke? Stroke. 2006 Jul; 37(7):1941-52.
14. Page SJ, Levine P, Leonard A (2007) Mentalpractice in chronic stroke: results of arandomized, placebo-controlled trial. Stroke38(4):1293–1297.
15. Page SJ, Levine P, Leonard AC (2005) Effects ofmental practice on affected limb use and functionin chronic stroke. Arch Phys Med Rehabil86(3):399–402.
16. Page SJ, Levine P, Sisto S, Johnston MV (2001) Arandomized efficacy and feasibility study ofimagery in acute stroke. Clin Rehabil 15(3):233–240
17. Johnson MR1, Mitchell KJ, Raye CL, D’EspositoM, Johnson MK. A brief thought can modulateactivity in extrastriate visual areas: Top-downeffects of refreshing just-seen visual stimuli.Neuroimage. 2007 Aug 1; 37(1):290-9.
48. Fuzail Ahmad-259--264.pmd 11/6/2014, 11:26 AM264

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
687
EFFECT OF LUMBAR STABILIZATION EXERCISES VERSUS PRESSURE FEEDBACK TRAINING IN LOW BACK ACHE PATIENTS
Shadab Uddin Department of Physical therapy, Faculty of Applied Medical Sciences, Jazan University,
Jazan, Kingdom of Saudi Arabia (KSA)
Fuzail Ahmed
Department of Physical therapy, Faculty of Applied Medical Sciences, majmaah University, al majmaah, Kingdom of Saudi Arabia (KSA)
Abstract: Chronic low back pain is the most common complaints in the urban society causing to absent from the work and activity limitation. Its health, social and economic burden is hefty. Despite developments in modern medicine in general and growing knowledge of spinal diseases, problem of nonspecific low back pain remains unsolved. Although the nonspecific types of bach pain affects approximately 85% of patients while 40% of low back pain patients worry that pain affects their work ability and will make them cripple, or that it underlies some serious disese (Waddell 1998). Even though there is ample evidence stating the efficacy of core stability training but not able to find any study which has compared Pressure Biofeedback training with Core Stability Training in the treatment of chronic low back pain. The aim of the present study was to compare the effectiveness of stabilizer pressure biofeedback training and core stability exercises on pain perception as measure by visual analogue scale in chronic low back pain patients.
Key Words: Back pain, core stability training, stabilizer pressure biofeedback Introduction
Chronic low back pain is the most common complaints in the urban society causing to absent from the work and activity limitation. Its health, social and economic burden is hefty. If we look to western societies, it has one of the most human suffering, disabling and enormous economic consequences with the frequent use of medical consultation and visit to rehabilitation unit. It is estimated that 70%-80% of population of United States of America is bear on back pain at one point in their life time.1 It is 2nd most frequent reason for visit to the physician and 5th ranking cause of hospital admission.2-3 In the United Kingdom back pain is the largest single reason of absence from work in 1988-1989 and is responsible for approximately 12.5% of all sick days.4
Despite developments in modern medicine in general and growing knowledge of spinal diseases, the problem of nonspecific low back pain remains unsolved, although the nonspecific type affects approximately 85% of patients reporting any back pain. Approximately 40% of low back pain patients worry that pain affects their work ability, that it will cripple them, or that it underlies some serious disease. Better understanding of multidimensional aspects has widened our concept of low back pain. There are several causes of low back pain. In a mechanical model, research has implicated pain sensitive vertebral structure such as the intervertebral disc and the zygoapophyseal joints as potential sources of low back pain. Irrespective of the actual source of symptoms, it has been shown that muscles are adversely affected secondary to low back pain. This phenomenon is accepted at peripheral joints such as the knee. For example, irrespective of the knee structure which is injured, e.g. meniscus or ligament, it is commonly accepted that quadriceps function will be adversely affected. Possible neurophysiological mechanisms include pain and reflex inhibition. Muscle re-education is therefore a commonly used intervention in the rehabilitation process, and for many years exercise has been advocated in the treatment of low back pain. Many researchers have focussed on issues of muscle strength. The basis for this focus is the premise that strong abdominal and back muscles are able to provide support for the lumbar spine.5

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
688
Despite the common acceptance of this principle, systematic reviews have not on the whole supported general trunk muscle strengthening programs.6 This has led to the development of specific exercise programs designed to protect and support the damaged joints and allow healing of the injured tissues.7,8 Muscles can be broadly divided into two categories, local and global muscles.9 The local muscle system includes deep muscles that are attached to the lumber vertebrae and are capable of directly controlling the stiffness of the lumbar segments.10 In contrast, the global muscle system encompasses larger and more superficial muscles of the trunk. Their role is to move the spine and to control larger external loads, which occur with normal daily function. Biomechanical research has demonstrated that deep, local muscles are important for controlling, protecting and supporting the joints. The muscles of the local synergy, which are important for the lumbo-pelvic region include the segmental lumbar multifidus, the transverses abdominis, the pelvic f loor and the diaphragm. There is evidence that low back pain results in an alteration in function of the local muscles, which lose their protective role.8,10,11
A common clinical finding in low back pain patients is decreased range of motion of the spine with increased paraspinal activity. Disturbances in neuromuscular control have also been frequently connected with chronic low back pain and considered a possible linkage between pain and disability12. These impaired functions recover with treatment or active rehabilitation. Spinal manipulative therapy is commonly recommended for low back pain, although previous systematic reviews and practice guidelines have produced discordant findings as to the effectiveness of this therapy. A recent focus in the management of chronic low back pain patients has been the specific training of the deep abdominal (internal oblique and transversus abdominis) and lumbar multifidus muscles. The primary role of these muscles is considered to be the provision of dynamic stability and segmental control of the spine. For the treatment of chronic low back pain with radiological diagnosis of spondylolysis or spondylolisthesis, one randomized controlled trial of specific stabilizing exercises showed significant and longer-lasting reduction in pain intensity and functional disability levels than did other commonly prescribed conservative treatment programs.
Investigators have reported that individuals with back pain may have motor control deficits or errors that affect their ability to engage the muscles that stabilize the spine. Maintaining segmental control within the trunk contributes to spinal stability and reduces unnecessary movement intersegmentally. This can serve to decrease the risk of back pain by causing a reduction in tissue strain, deformation, compression, and overstretching. Clinicians maintain that the mechanisms involved in spinal stability can be linked to differences in the function of the trunk muscles13. The trunk muscles have been classified into 2 categories, and each one performs distinct functions. The first category is the global muscle system. The muscles in this category are larger and more superficial in comparison to other muscles. The global muscles act to transfer loads and move the spinal column as a whole. Examples include the rectus abdominis and the external oblique14.
The second category is the local muscle system. The local muscles are smaller and deeper than the global muscles. They are intersegmental and produce only small amounts of force. Local muscles aid in proprioception and postural control, which can decrease the risk of injury. The local muscles also contribute to maintaining stiffness along the spinal column. The multifidus and the transverse abdominis are two examples15. A number of investigators have cited evidence that supports the use of stabilization exercises for enhancing spinal stability20. The local muscles are said to be crucial in this mechanism. This may be because of their contribution to maintaining the position of the spine and their ability to improve trunk endurance. Core stability training is frequently used to improve spinal stability. It has been used for many years in physical therapy and has become popular in fitness settings17. It has been speculated that this method of training improves spinal stability and may assist in decreasing the risk of back pain.
Studies that have been done on core stability training demonstrate promise for its effects on the musculature of the trunk18. However, previous investigations have not been designed to explore the involvement of the local muscles, which act to stabilize the spine. In addition, the methods of analysis have typically stressed the global muscles through assessments for strength or surface EMG recordings. These measures may not adequately identify improvements in spinal stability brought on by the local muscles. Core stability training that focuses on exercises with a neutral spine may be

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
689
appropriate for targeting the specific function of the local muscles during the early phases of programming for improving spinal stability19-20. Even though there is ample evidence stating the efficacy of core stability training I was unable find any study which has compared Pressure Biofeedback training with Core Stability Training in the treatment of chronic low back pain. The aim of the present study was to compare the effectiveness of Stabilizer Pressure Biofeedback Training and Core Stability Exercises on pain perception as measure by visual analogue scale in chronic low back pain patients. Methodology
A total of 30 subjects were selected for the study on the basis of inclusion and exclusion criteria. The subjects were randomly assigned to Group 1and Group 2 each comprising 15 subjects. All the patients were recruited from the inpatient outpatient department Government Civil Hospital, Ahmadabad. Only those patients were included who were between 40-60 years of age, presented with chronic nonspecific recurrent low back pain. The duration of the symptoms was diagnosed as sub-acute and chronic according to the IASP classification of pain. Those patients who were having severe or excruciating pain, radiating pain to the legs, history of fracture, surgery, or constitutional symptoms like fever, malaise, etc indicating infection, any inflammatory conditions, radiographic changes showing cervical spinal malformations, osteoporosis, bony abnormalities, scoliotic or kyphotic spine, pregnancy, sensory impairments, vascular causes of radiating pain or neoplasms were excluded. The above stated conditions were ruled out on the discretion of a medical professional. Study Design
The study was designed as a two group pre-test and post-test longitudinal study. Pain and Functional Disability were taken as outcome measure for this study. The experimental design included a pre-test measure of the dependent variables Pain and Disability and after 4 weeks of treatment the dependent variables were measured again. Visual Analouge Scale was used for measuring pain and Oswestry Disability Questionnaire for finding level of functional disability. All the selected subjects were informed in detail about the type and nature of the study and were made to sign the informed consent. After taking down the demographic data the visual analogue scale and Disability scores were noted down. Then the subjects in both the groups were made to do common warm-up exercises initially. These exercises include light aerobic work in the form of exercise on bicycle for 5 minutes at moderate pace or jogging for 10 minutes. Group 1: Core Stability Training
Core stabilization refers to the muscles that act to stabilize the lumbar spine and lumbopelvic and hip complex as well as muscles acting to control position of the head, arms, and trunk segment relative to the body’s base of support.41
All the subjects in the Group 1 had undergone one month core stability training which comprises of exercises aimed at increasing spinal stability. Isolated Lumbar stabilizing muscles training: Development of the perception of the isolated isometric specific contraction of the stabilizing muscles. Group 2: Stabilizer Bio-feedback training
The Stabilizer is a simple device which registers changing pressure in an air filled pressure cell. This allows body movement, especially spinal movement, to be detected during exercise. The unit consists of a combined gauge/inflation bulb connected to a pressure cell. The Stabilizer is used to monitor and provide feedback on body movement during exercise. The three-chamber pressure cell of the Stabilizer was placed between the part of the body and floor. It was inflated till it molds between the body part and the supporting surface. A pressure of 40 mmHg was maintained as the resting pressure of the inflated cell. Changes in body weight on the cell on any of the three compartments will register a pressure change on the gauge.
The Stabilizer biofeedback training was given for 6 days a week for four weeks. This maneuver was repeated for all the muscles responsible for lumbar spinal stability. All the activities were performed in three sets of 10 repetitions each. Each training session comprises of 45 mins.

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
690
Results Thirty subjects, 23 males and 7 females were randomly divided into two groups; group 1 and group 2. Table 1: Demographic Characteristics of Subjects in both the groups
Group
Visual Analogue Scale Score (n=15)
Baseline After 15 Days
After 30 days
Core Stability Exercise
6.7+1 4.6+1.7 2.3+1.7
Pressure Biofeedback
6.2+1.7 3.5+1.8 0.9+1
Group Oswestry Disability Index Score (n=15) Baseline Baseline Baseline
Core Stability Exercise
40.4+12.5
30.6+12.6 19.8+14
Pressure Biofeedback
46.6+21 24.8+18 5.1 + 6
Fifteen subjects were taken in each group, with a mean age and standard deviation of subjects in group 1 and 2 were 23.4±1.95 and 21.66±1.95 respectively. There were 12 males and 3 females in group1 and 11 males and 4 females in group2. Statistical analysis revealed no statistically significant differences between the groups during the baseline readings. The outcome measures were pain, measured on Visual Analogue Scale and functional disability measured by Oswestry Disability Index. All the measurement was taken on the 1st day, 15th day and after completion of the training on 30th day. All the data were compared for both the within group and between group anlysis using repeated measure ANOVA. Effect of Training on Pain and Disability: Assessment of improvement in this experiment included two dependent variables; Visual Analog Scale (VAS) score and Oswestry Disability Index/Questionnaire Score (ODI). One-way MANOVA demonstrated a significant improvement in visual analogue scale and ODI among the three readings taken after 1st, 15th and 30th day respectively. Further analysis was performed to determine the difference in dependent variables between both the groups a post hoc analysis was performed using Bonferroni test. In Group1 it was found that there was a significant difference for visual analogue scale (F = 33.29, P=0.001), and ODI (F= 73.19, P=0.001) among all three readings. In Group 2 also it was found out that there was a significant difference for visual analogue scale (F=20.79, P=0.001) and ODI (F= 32.56, P=0.001) between the three readings. Results are presented in the following sections. (Table 5.2) Effect of Core Stability Exercises on Pain and Disability: The group1 getting Core Stability Training has shown significant improvement in terms of decrease in pain and functional disability. The one month Core Stability Training brought 66% decrease in pain and 25% improvement on Oswestry Disability Index. Even after 15 days of training there was a positive effect of this training which improved further with four weeks of training. Post Hoc analysis has shown that there was a significant improvement in baseline readings of visual analogue scale and ODI when the comparison was made between 1st and 15th day, 1st and 30th day and 15th and 30th. Effect of Stabilizer Bio-Feedback Training on Pain and Disability: In Group2 also a similar improvement was seen as with the Group1. There was a significant decrease among the baseline reading measured on 1st day and the consequent readings taken on 15th and 30th day. Post hoc analysis has shown that there was improvement in pain and disability score with the training which was found statistically significant. Table 2: Repeated Measure ANOVA for visual analogue scale and ODI

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
691
Group1 (n=15)
Group2 (n=15)
Vis
ual A
nalo
gue
Scal
e
Day 1 M ± SD 6.69±0.9 6.2±1.7
Day 15 M ± SD 4.6±1.7 3.46±1.8
Day 30 M ± SD 2.27±1.7 0.94±1
RANOVA F 33.29 73.19 P 0.001 0.001
Post-Hoc Analysis (P=)
1vs15 0 0.001 15vs30 0.002 0.001 1vs30 0.00 0.00
Osw
estry
Dis
abili
ty In
dex
Day 1 M ± SD 40.4±12.5 46.6±21.2
Day 15 M ± SD 30.6±12.6 24±18.2
Day 30 M ± SD 19.8±14.6 5.13±6.1
RANOVA F 20.79 32.56 P 0.001 0.001
Post-Hoc Analysis (P=)
1vs15 0.003 0.003 15vs30 0.003 0.003 1vs30 0.00 0.oo
Between Group Analysis To find out, how both the groups have behaved in terms of improvement and to test the experimental hypothesis, a between group analysis was performed using independent t-test for all the variables. The findings suggested that the group getting Stabilizer Bio-feedback training have shown comparatively more improvement on both Visual Analogue Scale and Oswestry Disability Index. Figure 1: Within Group Comparison of VAS and ODI
The result shows that for initial two weeks treatment both the group behaved similarly and improvement in pain and functional disability was seen in both the groups. Table 3: Between group analysis of visual analogue scale and ODI among all three conditions.
Variables
Group 1 Group2 t-test
(n=15) (n=15) M ± SD M ± SD t p
VAS1 6.7+0.9 6.2+1.7 0.903 0.374** VAS 15 4.6+1.7 3.5+1.8 1.738 0.093**

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
692
VAS 30 2.3+1.7 0.9+1 2.585 0.015*
ODI 1 39.7+12.5
38.8+16.2 0.176 0.861**
ODI 15
30.6+12.6 24.8+14 1.016 0.381**
ODI 30 19.8+14 5.1+6.1 28 0.001*
As evident by the results there was no statistically significant difference between the group
getting Core Stability Training or Stabilizer Pressure Bio-Feedback Training at 1st day (VAS: t =0.903, p=0.374 ODI: t =0.176, p=0.861) or after 15 days of treatment (VAS: t =1.738, p=0.093 ODI: t =1.016, p=0.381). But after four weeks of treatment the result shows a statistically significant difference between both the groups and also it shows that the group getting Stabilizer Bio-Feedback training improved better on both the scales Visual Analogue Scale as well as Oswestry Disability Scale. Figure 2: Between Group Analysis of the VAS and ODI
The results of this study support the initial hypothesis that Stabilizer Pressure Biofeedback
training of the “stability” muscles of the trunk is more effective in reducing pain and functional disability in patients with chronic low back pain. Analysis of the pain and functional disability score data in the experimental group revealed that this treatment approach was more effective than the Core Stability Training. These findings support the Punjabi’s21 hypothesis that the stability of the lumbar spine is dependent not solely on the basic morphology of the spine, but also the correct functioning of the neuromuscular system. Also, Radebold A.22 stated that muscle recruitment and timing pattern play an important role in maintaining lumbar spine stability. Therefore, exercises specifying the isolated contraction of multifidus muscle were incorporated in the Group2, in contrast to the core stability exercises in the group1. Hence, it gets clearer that the significantly better results in the group1 are due to the proper recruitment of the specific back muscles, which was facilitated by the Stabilizer. Hodges and Richardson19 showed that the co-contraction of the transverse abdominis and multifidus muscles occurred prior to any movement of the limbs. They also showed that the timing of coordination of these muscles was very significant, and that back injury patients were unable to recruit their transverse abdominis and multifidus muscles early enough to stabilise the spine prior to movement. It hence makes it utmost important to strengthen these deep and local muscles to uproot the low back aches completely and maintains segmental stability. Therefore, it can be safely stated that in the present study, the group in which this was emphasized showed a significant improvement in terms of pain and functional ability in comparison to the other group, as evident in the result section.
By definition, the deep-trunk muscles act as 'stabilizers' and are not involved in producing movements, but instead use static or isometric contractions. Furthermore, they must act as stabilisers continuously during everyday activities as well as sport, and so require very good endurance of low-level forces. Muscle impairments are not more of strength but rather problems in motor control. This

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
693
is what was kept in mind while planning the exercise regime of the group1, which enhanced the spinal segmental support and control. The subjects were trained to selectively contract the stabilizers by the help of stabilizer biofeedback and later worked on improving the endurance in terms of static control. This form of specific training at low levels of activation supports the recent findings of Cholewicke and McGill24 that only low levels of maximal voluntary contraction of the segmental muscles are required to ensure the stability of the spine in vivo. It is also consistent with assertion that motor learning and control are not simply a process of strength training, but depend on patterning and inhibition of motor neurons, with the acquisition of skills occurring through selective inhibition of unnecessary muscular activity, as well as the activation of additional motor units.
Further, Shaughnessy M25 in a pilot study discovered that program of lumbar stabilization is effective in improving quality of life and functional outcome in patients with chronic low back pain. A similar study conducted by Cholewicke and McGill11 revealed that lumbar stability is maintained in vivo by increasing the activity (stiffness) of the lumbar segmental muscles, and highlighted the importance of motor control to coordinate muscle recruitment between large trunk muscle and small intrinsic muscles during functional activities, to ensure stability is maintained. This concept when merged with that of Bergmark,25 specifying the classification of trunk muscles into local and global muscles, has overemphasized the need to train the deep muscles of the back to provide segmental stability while directly controlling the lumbar segments. The present study on segmental stabilisation has incorporated all these theories and has come out with an exercise regimen working directly at the deep stabiliser muscles. The positive result with a significant difference in terms of pain and functional ability thus supports the hypotheses put forth by eminent researchers as stated above. In addition to this, Tesh K M26 has also suggested that the muscles of the antero-lateral abdominal wall increase the stability of the lumbar region of the vertebral column by tensing the thoracolumbar fascia and by raising intra-abdominal pressure. Of the back extensor muscles, the lumbar muscles is considered to have the greatest potential to provide dynamic control to the motion segment, in its neutral zone. This study was considered important on account of the fact that patients of chronic low back pain would always seek not only a relief from pain but also the ability to perform ADL without discomfort. Hence, the patients need to be trained not only for the static control but also dynamic functional independence. With this view in mind, the exercises focused on the appropriate strengthening of the deep back muscles such that it can lead to alleviation of pain during motor tasks as well, thus aiming at complete recovery.
The most significant finding of the present study was the sustained reduction in symptoms and functional disability levels in the experimental groups at the 15th and 30th day follow up. The findings of this study support the view that a change in the motor program had occurred in both the group after the intervention, such that the automatic pattern of recruitment of the abdominals to stabilize the spine during a motor task incorporated higher levels of deep abdominal muscle activity. This appears to represent an enhanced ability, in those in the experimental group, to stabilize dynamically their spine during functional tasks. Hence it can very well be stated that stabilization exercises do appear to provide additional benefits to patients with sub acute or chronic low back pain who have no clinical signs suggesting the presence of spinal instability. Therefore, such population of chronic low back pain patients must be identified and treated with specific stabilizing exercise intervention based on motor control and motor learning in order to achieve efficient relief of excessive load from the spine, to enhance segmental stabilization and to control pain in a functional manner. Future Research
The significant difference in results observe in this study suggests the effectiveness of both exercise regimes, but also suggests the need for a more comprehensive research for future including patients with gross instability (evident radiologically) and side-to-side differences while administering stabilization exercises. Other factors such as role of age, gender, duration of study etc. may also be included in the future studies. Use of sophisticated devices such as electromyography biofeedback units, or real time ultrasound scanners might have made this study more sensitive in terms of generalization of results. Relevance to Clinical Practice
Since EMG was not used in this study, the results observed in this study suggest the cost effectiveness in assessing pain and disability as would be required in clinical settings (devoid of EMG and other sophisticated equipments to assess level of muscle imbalance). There are studies stating the

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
694
use of exercise regimes only (without electrotherapeutic modalities) in which patients have benefited and thus the exclusion of these does not pose to be unethical. Also, since no other modality was used, it is a cost–effective method of treatment, as would be preferred in clinical settings. Limitations The long term effect of the study could not be established due to lack of follow up on pain and
disability, after the thirty days of treatment. The home care programme taught to the patients could not be done under direct supervision. Apart from the clinical physical therapist palpating the transversus abdominis and multifidus muscle
contraction in the subjects, there was no other means of verifying whether these muscles were recruited appropriately.
Conclusion The findings of this trial support the view that the functional integration of Stabilizer Bio-
feedback training directed at the deep abdominals and the lumbar muscles are effective in reducing pain and functional disability in patients with chronic low back pain. This supports Punjabi’s hypothesis, that spinal stability is dependent on an inter play between the passive, active, and neural control systems. Specific training of the muscles considered to provide dynamics stability to the lumbar spine may act to maintain the neutral zones of the motions segment within more normal limits during functional activity. In addition, the results of this study indicate that a “Stabilizer Bio-Feedback” treatment approach directed at specific muscles activation is more effective than Core Stability Training commonly used in patients with chronic low back pain. References: 1. Anderson GBJ. Epidemiology features of chronic low back pain.Lancet 1999; 354: 581-585 2. Taylor VM, Deyo RA, Cherkin DC, Keuter W. Low back pain hospitalization: recent United
States trends and regional variation. Spine 1994; 19: 1207-1213 3.Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine 1995; 20: 11-19.pko;l./ 3. Frank A. Low back pain. BMJ 1993; 306: 901-909 4. Koes B, Bouter L, Beckerman H Physiotherapy Exercises and Back Pain: a blinded review,
British Medical Journal 1991; 302: 1572-1576. 5. Richardson CA, Jull GA Muscle control – pain control. What exercises would you prescribe?
Manual Therapy 1995; 1: 2-10. 6. Richardson C, Jull G, Hodges P, et al; Therapeutic Exercise for Spinal Segmental Stabilization in
Low Back Pain – Scientific Basis and Clinical Approach. Churchill Livingstone, Edinburgh. 1999.
7. Bergmark A Stability of the lumbar spine. A study in mechanical engineering. Acta Orthopaedica Scandinavica 1989; 230(Suppl): 20-24.
8. Hides JA, Richardson CA, Jull GA Multifidus muscle recovery is not automatic following resolution of acute first episode low pack pain. Spine 1996; 21: 2763-2769.
9. Hodges PW, Richardson CA Inefficient muscular stabilisation of the abdominis. Spine 1996; 21: 2640-2650.
10. Richardson CA, Snijders CJ, Hides JA, et al; The relationship between the transversely oriented abdominal muscles, sacroiliac joint mechanics and low back pain. Spine 2002; 27(4):399-405.
11. Hodges, P. and Moseley, L., Pain and motor control of the lumbopelvic region: effect andpossible mechanisms, J Electromyogr Kinesiol, 13 (2003) 361-70.
12. Hodges, P.W., B.P. Hons, and C. Richardson. Inefficient muscular stabilization of the lumbar spine associated with low back pain: A motor control evaluation of transversus abdominis. Spine 21:2640–2650. 1996.
13. Nichols, J.F., D. Medina, and E. Dean. Effects of strength, balance, and trunk stabilization training on measures of functionalfitness in older adults. Am. J. Med. Sports 3:279–285.2001.
14. Richardson, C.A., and G.A. Jull. Muscle control—pain control: What exercises would you prescribe? Man. Ther. 1:2–10.1995

1st Annual International Interdisciplinary Conference, AIIC 2013, 24-26 April, Azores, Portugal - Proceedings-
695
15. Richardson, C., G. Jull, P. Hodges, and J. Hides. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach. Edinburgh, Scotland: Churchill Livingstone, 1999.
16. Mc Gills, S.M. Low back exercises: Evidence for improving exercise regimens. Phys. Ther. 78:754–765. 1998.
17. O’sullivan, P.B., G.D.M. Phyty, L.T. Twomey, and G.T. Allison. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine 22:2959–2967. 1997.
18. Stanton, R., P.R. Reaburn, and B. Humphries. The effect of short-term Swiss ball training on core stability and running economy. J. Strength Cond. Res. 18:522–528. 2004.
19. Mcgill, S., A. Childs, and C. Liebenson. Endurance times for low back stabilization exercises: Clinical targets for testing and training from a normal database. Arch. Phys. Med. Rehabil. 80:941–944. 1999.
20. Radebold A,Cholwicki J, PasnjabiMM, et al. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 2000;25;947-54
21. Richardson CA, Jull GA, Hodges P Hides . Therapeutic exercise for spinal segmental stabilization in low back pain scientific basis and clinical approach, Edinburgh, Churchill Livingstine ,1999
22. Cholewicki J, Mc G ill SM. Mechanical stability of the in vivo lumbar spine: implications for injury and chronic low back pain. Clin Biomech 1996; 11: 1-15.
23. Shaughnessy M, Caulfield B. Apilot study to investigate the effect of lumbar stabilization exercise training on functional ability and quality of life in patients with chronic low back pain. Int J Rehab Res. 2004 Dec;7(4):297-301.
24. Bergmark A . Stability of the lumbar spine. Acta Orthop Scand 1989;60:1-54. 25. Tesh KM, Dunn JS, Evans JH.The abdominal muscles and vertebral stability. Spine. 1987
Jun;12(5):501-8.








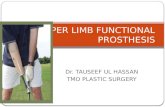

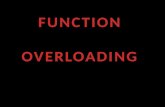
![Upper Limb Treatment Principles in Intensive Functional ...currentneurobiology.org/neurobiology/upper-limb-treatment-principles-in-intensive...CIMT [H-CIMT], bimanual intensive movement](https://static.fdocuments.us/doc/165x107/5ea2417b6d256b24c6549424/upper-limb-treatment-principles-in-intensive-functional-cimt-h-cimt-bimanual.jpg)




