Research Article Comparison of Volumetric and Diameter ...
5
Central Journal of Cardiology & Clinical Research Cite this article: Serhal A, Aouad P, Blaisdell J, Carr J (2020) Comparison of Volumetric and Diameter Dimensions in Surveillance of Thoracic Aortic Aneurysm by Computed Tomography Angiography. J Cardiol Clin Res 8(3): 1161. *Corresponding author Ali Serhal, Department of Radiology, Northwestern University, Chicago, IL 60611, USA, Tel: 312-695-5753; Email: [email protected] Submitted: 18 October 2020 Accepted: 05 November 2020 Published: 07 November 2020 Copyright © 2020 Ali Serhal, et al. OPEN ACCESS Keywords • Thoracic aortic aneurysm • CT angiography • Aortic volume • Aortic diameter • Interval growth Research Article Comparison of Volumetric and Diameter Dimensions in Surveillance of Thoracic Aortic Aneurysm by Computed Tomography Angiography Ali Serhal*, Pascale Aouad, Julie Blaisdell, and James Carr Department of Radiology, Northwestern University, USA Abstract Background: Thoracic aortic aneurysm (TAA), is a common condition that requires imaging follow-up to evaluate for complications and intervention timing. In asymptomatic patients, TAA evaluation is done with routine follow up of the aortic dimensions. Purpose: To compare 3D volumetric measurement and 2D diameter measurement in surveillance of TAA using computed tomography angiography (CTA), in asymptomatic patients. Materials and methods: Forty patients (mean age 66.2 y, 29 males), undergoing surveillance of TAAs was retrospectively identified. Quantitative analysis was performed by measuring the diameters at sinus of Valsalva (SOV), and mid ascending aorta (MAA), using standard technique and measuring the volume of the ascending aorta from the annulus to the proximal arch level by two radiologists on a baseline and follow up scans. Results: The mean interval time between baseline and follow up exams was 2.3 ±1.5 years. There was significant diameter growth at the level of the MAA (p=0.0056), but not at the level of the SOV (p=0.08). There was significant growth of the ascending thoracic aorta volume (p=0.0001). There was excellent intra-rater and inter-rater agreement. The percent growth of the volume measurement was 2.7 times greater than the MAA percentage growth (5.1% vs 1.9%, P < 0.001) and 1.8 times greater than the diameter of maximal growth percentage growth (5.1% vs 2.9%, P < 0.001) over the entire follow-up period. Conclusions: Volumetric measurement of the ascending aorta is a reproducible method that offers greater sensitivity than conventional 2D measurements for detection of the growth rate of the ascending thoracic aorta. INTRODUCTION Thoracic aortic aneurysm (TAA), is a life threatening condition causing short-term and long-term mortality due to increased risk of rupture and dissection. It has an overall prevalence of 450 per 100,000 persons [1], is two to four times more frequent in male patients and is more common in elderly population. The incidence is likely underestimated as many patients are asymptomatic at the time of diagnosis and the condition is often discovered incidentally on imaging [2]. An aneurysm is defined as a permanent dilatation of the aorta exceeding the normal measurements by more than two standard deviations at a given anatomic level. The ascending aorta is considered dilated if the diameter is greater than 4cm and considered aneurysmal if the diameter exceeds 5 cm [3]. Most TAAs are degenerative in etiology and are related to alterations in vascular wall biology that lead to loss of structural integrity and aortic wall strength [4]. The natural history of TAAs is slow expansion with an increasing risk of aortic dissection and rupture. Expansion rates range from 0.1 to 1.0 cm per year, depending upon TAA etiology, diameter, and location within the aorta [5,6]. While apparent rapid expansion of the aorta is commonly attributable to measurement error, its presence should raise concern for aortic dissection or superimposed infection. The expansion rate is higher in patients with a larger aorta, in patients with a bicuspid aortic valve, and in patients with genetic disorders related TAA [7-9]. Imaging plays an important role in the management of these patients and accurate measurements of aortic dimensions is crucial for long-term surveillance. Annual or biannual follow-up is generally performed and is dependent on the size of the TAA, its cause, and the expansion rate [10]. Computed tomography angiography and magnetic resonance angiography of the thoracic aorta are both acceptable techniques for this purpose [11,12]. Echocardiography can also be used for follow-up of aortic root aneurysms and any associated valvular disease. TAAs should
Transcript of Research Article Comparison of Volumetric and Diameter ...

Central Journal of Cardiology & Clinical Research
Cite this article: Serhal A, Aouad P, Blaisdell J, Carr J (2020) Comparison of Volumetric and Diameter Dimensions in Surveillance of Thoracic Aortic Aneurysm by Computed Tomography Angiography. J Cardiol Clin Res 8(3): 1161.
*Corresponding author
Ali Serhal, Department of Radiology, Northwestern University, Chicago, IL 60611, USA, Tel: 312-695-5753; Email: [email protected]
Submitted: 18 October 2020
Accepted: 05 November 2020
Published: 07 November 2020
Copyright© 2020 Ali Serhal, et al.
OPEN ACCESS
Keywords•Thoracic aortic aneurysm•CT angiography•Aortic volume•Aortic diameter•Interval growth
Research Article
Comparison of Volumetric and Diameter Dimensions in Surveillance of Thoracic Aortic Aneurysm by Computed Tomography AngiographyAli Serhal*, Pascale Aouad, Julie Blaisdell, and James CarrDepartment of Radiology, Northwestern University, USA
Abstract
Background: Thoracic aortic aneurysm (TAA), is a common condition that requires imaging follow-up to evaluate for complications and intervention timing. In asymptomatic patients, TAA evaluation is done with routine follow up of the aortic dimensions.
Purpose: To compare 3D volumetric measurement and 2D diameter measurement in surveillance of TAA using computed tomography angiography (CTA), in asymptomatic patients.
Materials and methods: Forty patients (mean age 66.2 y, 29 males), undergoing surveillance of TAAs was retrospectively identified. Quantitative analysis was performed by measuring the diameters at sinus of Valsalva (SOV), and mid ascending aorta (MAA), using standard technique and measuring the volume of the ascending aorta from the annulus to the proximal arch level by two radiologists on a baseline and follow up scans.
Results: The mean interval time between baseline and follow up exams was 2.3 ±1.5 years. There was significant diameter growth at the level of the MAA (p=0.0056), but not at the level of the SOV (p=0.08). There was significant growth of the ascending thoracic aorta volume (p=0.0001). There was excellent intra-rater and inter-rater agreement. The percent growth of the volume measurement was 2.7 times greater than the MAA percentage growth (5.1% vs 1.9%, P < 0.001) and 1.8 times greater than the diameter of maximal growth percentage growth (5.1% vs 2.9%, P < 0.001) over the entire follow-up period.
Conclusions: Volumetric measurement of the ascending aorta is a reproducible method that offers greater sensitivity than conventional 2D measurements for detection of the growth rate of the ascending thoracic aorta.
INTRODUCTIONThoracic aortic aneurysm (TAA), is a life threatening condition
causing short-term and long-term mortality due to increased risk of rupture and dissection. It has an overall prevalence of 450 per 100,000 persons [1], is two to four times more frequent in male patients and is more common in elderly population. The incidence is likely underestimated as many patients are asymptomatic at the time of diagnosis and the condition is often discovered incidentally on imaging [2]. An aneurysm is defined as a permanent dilatation of the aorta exceeding the normal measurements by more than two standard deviations at a given anatomic level. The ascending aorta is considered dilated if the diameter is greater than 4cm and considered aneurysmal if the diameter exceeds 5 cm [3]. Most TAAs are degenerative in etiology and are related to alterations in vascular wall biology that lead to loss of structural integrity and aortic wall strength [4]. The natural history of TAAs is slow expansion with an increasing
risk of aortic dissection and rupture. Expansion rates range from 0.1 to 1.0 cm per year, depending upon TAA etiology, diameter, and location within the aorta [5,6]. While apparent rapid expansion of the aorta is commonly attributable to measurement error, its presence should raise concern for aortic dissection or superimposed infection. The expansion rate is higher in patients with a larger aorta, in patients with a bicuspid aortic valve, and in patients with genetic disorders related TAA [7-9].
Imaging plays an important role in the management of these patients and accurate measurements of aortic dimensions is crucial for long-term surveillance. Annual or biannual follow-up is generally performed and is dependent on the size of the TAA, its cause, and the expansion rate [10]. Computed tomography angiography and magnetic resonance angiography of the thoracic aorta are both acceptable techniques for this purpose [11,12]. Echocardiography can also be used for follow-up of aortic root aneurysms and any associated valvular disease. TAAs should

Central
Ali Serhal, et al. (2020)
2/5J Cardiol Clin Res 8(3): 1161 (2020)
ideally be surveilled using the same imaging technique and in the same institution [13]. Measurements are typically made in accordance with AHA guidelines, wherein aortic diameters are measured at six locations. The annual growth rate of most TAAs is low in order of millimeters, making the detection of growth difficult. Furthermore, recent literature has shown that maximal diameter measurements of the aorta may be insensitive to focal aneurysmal changes [14], and 3D volume reconstructions have been used as alternative to study the abdominal aortic growth [14], and more recently to evaluate TAA growth in patients with bicuspid aortic valves [15]. We therefore thought to compare the sensitivity of 2D diameter measurements and 3D volumetric measurements of the ascending thoracic aorta in patients with TAAs undergoing surveillance with CTA.
MATERIAL AND METHODS
Study population
This retrospective study was conducted on 40 adult patients (29 males, 11 females), with known TAA who underwent a baseline and follow-up computed tomography angiography (CTA), exams between September 1, 2009 and March 5, 2014. Patients with a history of aortic dissection or surgery to the heart or thoracic aorta prior to the baseline exam or in the interval between the two scans were excluded from the study. Our institutional review board approved this study and an informed consent was waived.
Imaging technique
All CTA studies of the thoracic aorta were performed on a 64-slice scanner (SOMATOM Definition, Siemens Healthineers, Forchheim, Germany) with ECG gating using the standard protocol in our institution. In all patients, between the initial and the follow up scan, there was no difference in the patient heart rate of more than 5 to ensure image acquisition in same R-R interval. ECG trigger range was 30% if the heart rate is more than 75 and 50% if the heart rate is less than 75. Typical slice thickness was on the order of 0.6-mm to 1-mm. Images were acquired using either iterative reconstruction or filtered back projection. kVp was selected according to the pre-determined BMI-based institutional protocol and ranged between 80 and 140 kVp. 75 ml of iodinated contrast Iohexol (350 mg Iodine /mL) was injected at a rate of 5cc/s. The timing of acquisition was determined using bolus triggering method.
Image processing and aortic measurements
Images were reconstructed on dedicated software Vitrea (Vital Images Inc., Minnesota, USA) allowing for multiplanar reconstruction and volumetric reconstruction and segmentation. Two radiologists with cardiovascular imaging fellowship training performed independently diameter and volumetric measurements. Measurements from baseline and follow-up scans were obtained on different days with both observers being blinded to the measurements obtained from different studies of the same subjects. The primary observer obtained the measurements of all the 40 studied subjects and repeated measurements for 10 randomly chosen subjects to evaluate intraobserver agreement. The second observer obtained measurements of 10 randomly chosen subjects to analyze interobserver agreement.
Diameter measurements
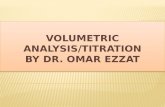
After multiplanar reconstruction, double oblique diameter measurements of the thoracic aorta were obtained at the levels of sinuses of Valsalva (SOV), and of the mid ascending aorta (MAA), using a plane that is orthogonal to the course of the aorta while including the aortic wall in the measurement (Figure 1). At the level of the SOV, three measurements were obtained, from each sinus to the adjacent sinus. At the level of the MAA, two orthogonal measurements were obtained. The higher value of these measurements was recorded as the maximal SOV diameter and maximal MAA diameter respectively. Diameter growth rate was derived from changes in the maximal SOV and maximal MAA diameters between baseline and follow-up scans. As surgical intervention for TAA is recommended based on the fastest growing diameter at either the SOV or MAA [12], the diameter of maximal growth (DMG), defined as the fastest growth rate at either SOV or MAA, was also recorded. The diameter growth at SOV, MAA and DMG were reported as units (mm) and percentages (%). The growth rates were reported as units per time (mm/year) and percentages per time (%/year). Diameter percentage was calculated from the difference of diameter measurements between baseline and follow-up scans divided by the baseline measurement.
Volume measurements
The ascending thoracic aorta was segmented semi-automatically and separated from the surrounding structures. The radiologist selected the start and end levels of the segmented volume and manually edited the contours to ensure adequate
Figure 1 2D Measurements of the aorta at the level of the Sinus-Of-Valsalva (a) and mid ascending aorta (b). 3D reconstruction of the aorta (c) and volumetric measurements (d) of the aortic segment from the annulus to the proximal arch.

Central
Ali Serhal, et al. (2020)
3/5J Cardiol Clin Res 8(3): 1161 (2020)
inclusion of all the aortic lumen and wall and exclusion of the surrounding tissues. The measured volume of ascending thoracic aorta extended proximally from the aortic annulus and distally to the aorta just proximal to the origin of the brachiocephalic artery. Volumetric growth rate was derived from the difference between the baseline and follow-up ascending aortic volumes. The volumetric growth was recorded as both units (milliliter), and percentages (%). Growth rates were reported as units per time (mL/year), and percentage per time (%/year). Volumetric percentage was calculated from the difference in volume between baseline and follow-up scans divided by the baseline volume.
Statistical analysis
Statistical analysis was performed using Stata 14 (StataCorp, College Station, TX).
The measurements obtained from baseline and follow-up scans were compared using a two-tailed paired student t test. Statistical significance was defined by p value of less than 0.05. Intra-rater and inter-rater agreement was analyzed using the intraclass correlation coefficient (ICC) and Bland-Altman analysis.
RESULTSThe mean interval time between baseline and follow up exams
was 2.3 ±1.5 years. The mean age of all the subjects was 66.2 ± 8.4 y at their baseline scan. Table 1 shows the baseline and follow-up measurements of the ascending thoracic aorta at SOV and MAA and of the aortic volume. There was significant growth at the level of the MAA (p=0.0056) however no significant growth was observed at the level of the SOV (p=0.08). There was significant growth of the ascending thoracic aorta volume (p=0.0001).
There was excellent intra-rater and inter-rater agreement on SOV diameter, MAA diameter and ascending aorta volume measurements obtained from randomly chosen 10 subjects (Table 2).
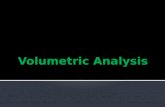
Bland-Altman analyses for interobserver and intraobserver agreement on diameter and volume measurements are displayed in Figure 2 and showed no systematic difference.
Table 3 lists the absolute and percentage values of growth rate per year and over the entire follow-up period for the SOV, MAA, DMG and aortic volume. The percent growth of the volume measurement was 2.7 times greater than the MAA percentage growth (5.1% vs 1.9%, P < 0.001) and 1.8 times greater than the DMG percentage growth (5.1% vs 2.9%, P < 0.001) over the entire follow-up period.
DISCUSSIONThe size of the TAA is a major predictor of predictor of aortic
dissection, rupture and mortality [16]. The annual risk of rupture or dissection of the aorta is less than 2% for TAAs between 4.0 and 4.9 cm but increases to 7% for aortic size greater than 6.0 cm [16]. All symptomatic TAAs should undergo repair. For asymptomatic patients with ascending TAA, indications for intervention include (10): 1) End-diastolic aortic diameter of 5 to 6 cm or aortic size index (aortic diameter [cm] divided by body surface area [m2]) ≥2.75 cm/m2, 2) End diastolic diameter greater than 4.5-5 cm for patients with genetically-related TAA, 3) End diastolic diameter
Table 1: Ascending thoracic aorta measurements in 40 subjects with thoracic aorta aneurysm.
Baseline Follow-Up P value
Age, y 66.2 ± 8.4 68.9 ± 8.8 -Sinus of Valsalva, mm 42.2 ± 5.4 42.7 ± 5.8 0.08
Mid ascending aorta, mm 42.3 ± 5.3 43.1 ± 5.9 0.0056
Ascending aorta, mL 139.7 ± 44.6 145.4 ± 43.9 0.0001
Date is presented as mean ± SD.
Table 2: Intra-rater and inter-rater intraclass correlation coefficient (ICC) for diameter and volumetric measurements on 10 subjects.
Intra-rater ICC (95% CI)
Inter-rater ICC (95% CI)
Sinus of Valsalva diameter 0.99 (0.95-1.00) 0.93 (0.81-0.97)
Mid ascending aorta diameter 0.99 (0.98-1.00) 0.98 (0.92-0.99)
Ascending aorta volume 1.00 (0.99-1.00) 0.99 (0.99-1.00)
Table 3: Diameter and volumetric growth rate and total growth.
Growth rate (unit/
year)
Percentage of growth rate
(%/year)
Total Growth
Percent-age of total
growth (%)
Sinus of Valsalva diameter (mm)
0.1 ± 0.5 0.05 ± 1.8 0.5 ± 1.7 0.6 ± 4.5
Mid ascending aorta diameter (mm)
0.2 ± 0.6 0.4 ±1.4 0.8 ± 1.8 1.9 ± 4.0
Diameter of maximal growth (mm)
0.4 ± 0.6 0.9 ± 1.3 1.3 ± 2.1 2.9 ± 4.0
Ascending aorta volume (mL) 2.7 ± 4.7 2.1 ± 3.2 5.6 ± 8.3 5.1 ± 9.3
Data is presented as mean ± SD
greater than 4.5 cm for non-Turner patients undergoing aortic valve surgery, 4) Rapid expansion greater than or equal to 10 mm per year in the general population or more than 5 mm per year for patients with bicuspid aortic valve or with genetically-related TAA. For patients not meeting these criteria, serial follow up exams to determine the timing for intervention is recommended. Therefore, imaging of the thoracic aorta has a crucial role in surveillance of these subjects and accurate measurements are fundamental. While surveillance imaging can be done with either CTA or MRA of the thoracic aorta, CTA is the most widely used technique due to its widespread availability, optimal spatial resolution, potential for multiplanar and 3D reconstructions, and its fast acquisition which makes it less sensitive to motion artifacts.
There is no standardized method for measuring aortic diameter, but the general consensus is to measure the largest diameter perpendicular to the vessel lumen using multiplanar reconstruction at reproducible anatomical landmarks on

Central
Ali Serhal, et al. (2020)
4/5J Cardiol Clin Res 8(3): 1161 (2020)
Figure 2 Intraobserver and interobserver Bland-Altman analysis of diameter measurements and volume measurements. Limits of agreement and bias are reported on the horizontal bars as a function of the percent of the ensemble mean.
electrocardiogram-gated images. However, opinions differ on whether the aortic wall should be included in the vessel diameter, what phase of the cardiac cycle should be used, and whether SOV measurements should be taken at the cusps or the commissure [17].
Additionally, variability in the plane angulation and of the aortic level at which the diameter measurement is obtained can impact reproducibility of these measurements. These issues render detection of small changes in aortic diameter challenging.
Geisbusch et al., have studied the growth rate of TAAs using volumetric measurements for patients with small-to-moderate aneurysms and reported a growth rate of 0.95 ± 4.5 ml/ year and 0.73 ± 3.7%/year for the ascending aorta. The authors concluded that volumetric measurements provide an objective method for ascertaining aortic size and monitoring expansion [18]. Trinh et al., studied the reliability of contrast-enhanced MRA 3D volumetry compared with 2D diameter measurements to identify thoracic aortic aneurysm growth in patients with bicuspid aortic valve and concluded that the volumetric measurements demonstrate larger effect on the percentage growth than diameter measurements [15]. Other studies have also shown the utility of volumetric measurements of the abdominal aorta and demonstrated better sensitivity to growth change when compared to conventional maximal diameter measurements [19-21]. Based on these studies, we extrapolated that 3D volume measurements of TAA on CTA should similarly produce reliable
and more robust analysis than diameter measurements. The hypothesis is that maximal diameter does not always change with aortic dilatation, furthermore the exponential relationship between diameter and volume makes volume more sensitive for growth detection as suggested by Trinh et al [15].
Our study showed an absolute and percentage growth rate of the DMG of 0.4 ± 0.6 mm/year and 0.9 ± 1.3 %/year and of the aortic volume of 2.7 ± 4.7 ml/year and 2.1 ± 3.2 %/year, respectively. We reported the percentage values of the growth rate and of the overall growth to allow for comparison of different units (mm for diameters and mL for volumes). The observed percentage of growth rate and percentage of total growth were 2.3 fold and 1.8 fold greater with volume measurements by comparison to the diameter measurements of DMG. This larger percentage change observed with volumetric measurements reflects the potential greater sensitivity of the volumetric measurements for detection of size change of the ascending thoracic aorta. These results were in concordance with the reported literature [15,19-21]. As aortic growth does not always occur at the traditionally measured levels of the thoracic aorta, the use of the greatest aortic diameter may fail to detect interval change in aortic dimensions. Volumetric measurements are obtained by including the whole ascending thoracic aorta which offers higher sensitivity for detection of growth at any aortic level.
There are some limitations of our study. First, the sample size is relatively small. Second, the clinical outcome was not evaluated

Central
Ali Serhal, et al. (2020)
5/5J Cardiol Clin Res 8(3): 1161 (2020)
and therefore the clinical impact of the increased sensitivity for detection of aortic size change with volumetric measurements cannot be assessed. Third, 3D reconstructions, segmentation and contouring of the ascending aorta is time consuming with the currently available softwares and requires careful selection of the proximal and distal boundaries. However, our study showed excellent intraobserver and interobserver agreement on measurements, suggesting that a volumetric measurement is reproducible and reliable. Furthermore, we included only part of the thoracic aorta in our study, a segment from the root to the proximal arch. Including the whole aorta is technically feasible with our current method, careful segmentation of the arch and the descending aorta should be done as these segments show more calcification. Fourth, selection bias of CTAs that are interpretable with no significant artifacts. The presence of artifacts may preclude image reconstruction thereby making volumetric measurements inaccurate.
The current guidelines for surgical intervention for TAA are based on the aortic greatest diameter and there is no current consensus on management based on volumetric measurements. The encouraging results of several studies along with the relative simplicity and reliability of volumetric measurement warrants further investigation to better understand how aortic volume correlates with the risk of TAA complications and potentially the inclusion of aortic volumes in the guidelines for monitoring and risk stratification of patients with TAA.
In conclusion, volumetric measurement of the ascending aorta is a highly reproducible method that offers greater sensitivity than conventional 2D measurements for detection of the growth rate of the ascending thoracic aorta and can be reported in addition to the diameter measurements. Further studies should be done to determine the influence of volume change on patient clinical outcome and to establish a threshold growth volume for appropriate timing of intervention.
REFERENCES1. Bickerstaff LK, Pairolero PC, Hollier LH, Melton LJ, Peenen HJV,
Cherry KJ, et al. Thoracic aortic aneurysms: A population-based study. Surgery 1982; 92: 1103-1108.
2. Clouse WD, John W. Hallett J, Schaff HW, Gayari MM, Listrup DM, Melton DJ. Improved Prognosis of Thoracic Aortic Aneurysms: A Population-Based Study JAMA. 1998; 280: 1926-1929.
3. Litmanovich D, Bankier AA, Cantin L, Rautopoulos V, Boiselle PM. CT and MRI in diseases of the aorta. AJR Am J Roentgenol 2009; 193: 928-940.
4. Isselbacher EM. Thoracic and abdominal aortic aneurysms. Circulation. 2005; 111: 816-828.
5. Elefteriades JA, Farkas EA. Thoracic aortic aneurysm: clinically pertinent controversies and uncertainties. J Am Coll Cardiol. 2010; 55: 841-857.
6. Kuzmik GA, Sang AX, Elefteriades JA. Natural history of thoracic aortic aneurysms. J Vasc Surg. 2012; 56: 565-571.
7. Coady MA, Davies RR, Roberts M, Goldstein LJ, Rogalski MJ, Rizzo JA, et al. Familial Patterns of Thoracic Aortic Aneurysms. Arch Surg. 1999; 134: 361-367.
8. Canna G, Ficarra E, Tsagalau E, Nardi M, Morandini A, Chieffo A, et al. Progression Rate of Ascending Aortic Dilation in Patients With Normally Functioning Bicuspid and Tricuspid Aortic Valves. Am J Cardiol. 2006; 98: 249-253.
9. Albornoz G, Coady MA, Roberts M, Davies RR, Tranquilli M, Rizzo JA, et al. Familial Thoracic Aortic Aneurysms and Dissections-Incidence, Modes of Inheritance, and Phenotypic Patterns. Ann Thorac Surg. 2006; 82: 1400-1405.
10. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter Cardiovasc Interv. 2010; 76: E43-E86.
11. Green DB, Palumbo MC, Lau C. Imaging of thoracoabdominal aortic aneurysms. J Thorac Imaging. 2018; 33: 358-365.
12. Blinded for anonymity
13. Mani K, Wanhainen A. Accurate and Reproducible Diameter Measurement is Essential in Surveillance and Treatment of Thoracic Aortic Aneurysms. Eur J Vasc Endovasc Surg. 2014; 47: 27.
14. Renapurkar RD, Setser RM, O’Donnell TP, Egger J, Lieber ML, Desai MY, et al. Aortic volume as an indicator of disease progression in patients with untreated infrarenal abdominal aneurysm. Eur J Radiol. 2012; 81: e87-e93.
15. Blinded for anonymity.
16. Davies RR, Goldstein LJ, Coady MA, Tittle SL, Rizzo JA, Kopf GS, et al. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg. 2002; 73: 17-28.
17. Freeman LA, Young PM, Foley TA, Williamson EE, Bruce CJ, Greason KL, et al. CT and MRI assessment of the aortic root and ascending aorta. Am J Roentgenol. 2013; 200: W581-W592.
18. Geisbüsch S, Stefanovic A, Schray D, Oyfe I, Lin HM, Luozzo GL, et al. A prospective study of growth and rupture risk of small-to-moderate size ascending aortic aneurysms. J Thorac Cardiovasc Surg. 2014; 147: 68-74.
19. Kontopodis N, Lioudaki S, Pantidis D. Advances in determining abdominal aortic aneurysm size and growth. World J Radiol. 2016; 8: 148.
20. van Keulen JW, van Prehn J, Prokop M, Moll FL, Herwaarden JAV. Potential value of aneurysm sac volume measurements in addition to diameter measurements after endovascular aneurysm repair. J Endovasc Ther. 2009; 16: 506-513.
21. Kauffmann C, Tang A, Therasse É, Giroux MF, Elkouri S, Melanson P, et al. Measurements and detection of abdominal aortic aneurysm growth: Accuracy and reproducibility of a segmentation software. Eur J Radiol. 2012; 81: 1688-1694.
Serhal A, Aouad P, Blaisdell J, Carr J (2020) Comparison of Volumetric and Diameter Dimensions in Surveillance of Thoracic Aortic Aneurysm by Computed To-mography Angiography. J Cardiol Clin Res 8(3): 1161.
Cite this article