
Request for proposal and draft agreement healthchoices€¦ · Request for Proposal . and Draft...
12
Request for Proposal and Draft Agreement Summary of the RFP and Changes to Program Requirements Under Governor Tom Wolf’s leadership, the Pennsylvania Departments of Human Services (DHS) and Aging (PDA) are developing a new program for older Pennsylvanians and adults with physical disabilities called Community HealthChoices (CHC). The program will roll out in three phases over three years, beginning in January 2017. Summary of CHC The commonwealth plans to coordinate physical health care and long-term services and supports (LTSS) through CHC managed care organizations (CHC-MCOs). Participants will have a choice of two to five CHC-MCOs in each zone. The CHC rate model will include value-based incentives to increase the use of home and community-based services (HCBS) and meet other program goals. CHC will use standardized outcome measures at both the program- and participant-level to assess overall program performance and improve the CHC program over time. CHC will serve an estimated 450,000 individuals, including 130,000 older Pennsylvanians and adults with physical disabilities who are currently receiving LTSS in the community and in nursing facilities. CHC-MCOs will be accountable for most Medicaid-covered services, including preventive services, primary and acute care, LTSS (HCBS and nursing facilities), prescription drugs, and dental services. Participants who have Medicaid and Medicare coverage (dual eligible participants) will have the option to have their Medicaid and Medicare services coordinated by the same MCO.
Transcript of Request for proposal and draft agreement healthchoices€¦ · Request for Proposal . and Draft...

Request for Proposal and Draft AgreementSummary of the RFP and Changes to Program Requirements
Under Governor Tom Wolf’s leadership, the Pennsylvania Departments of Human Services (DHS) and Aging (PDA) are developing a new program for older Pennsylvanians and adults with physical disabilities called Community HealthChoices (CHC). The program will roll out in three phases over three years, beginning in January 2017.
Summary of CHC
The commonwealth plans to coordinate physical health care and long-term services and supports (LTSS) through CHC managed care organizations (CHC-MCOs). Participants will have a choice of two to five CHC-MCOs in each zone. The CHC rate model will include value-based incentives to increase the use of home and community-based services (HCBS) and meet other program goals. CHC will use standardized outcome measures at both the program- and participant-level to assess overall program performance and improve the CHC program over time.
CHC will serve an estimated 450,000 individuals, including 130,000 older Pennsylvanians and adults with physical disabilities who are currently receiving LTSS in the community and in nursing facilities. CHC-MCOs will be accountable for most Medicaid-covered services, including preventive services, primary and acute care, LTSS (HCBS and nursing facilities), prescription drugs, and dental services. Participants who have Medicaid and Medicare coverage (dual eligible participants) will have the option to have their Medicaid and Medicare services coordinated by the same MCO.
2
COMMUNITY HEALTHCHOICES REQUEST FOR PROPOSAL AND DRAFT AGREEMENT
Comments Requested on Draft RFP and Program RequirementsThe commonwealth is preparing to publish a Request for Proposal (RFP) in January 2016 to procure MCO services to support CHC. Since this program represents a major change to the way Medicaid LTSS are delivered, the commonwealth wants to ensure the RFP reflects a structure that will support the needs and preferences of program participants. For that reason, the draft RFP and Program Requirements will be released for public comment on November 16, 2015. Comments will be accepted until December 11, 2015.
It is important to note that these documents are subject to change before the RFP is officially posted for responses. In addition, several other documents associated with commonwealth RFP’s, including Terms and Conditions and Cost Submittal Templates are not included with this publication as we solicit comments on the draft RFP.
This draft RFP is issued for informational and planning purposes only and does not constitute any type of procurement solicitation or an obligation on the part of the commonwealth to acquire any products or services. Information provided in the draft RFP and the Program Requirements document is not intended to convey any predisposition to a particular solution, method, or service delivery methodology and is likely to change.
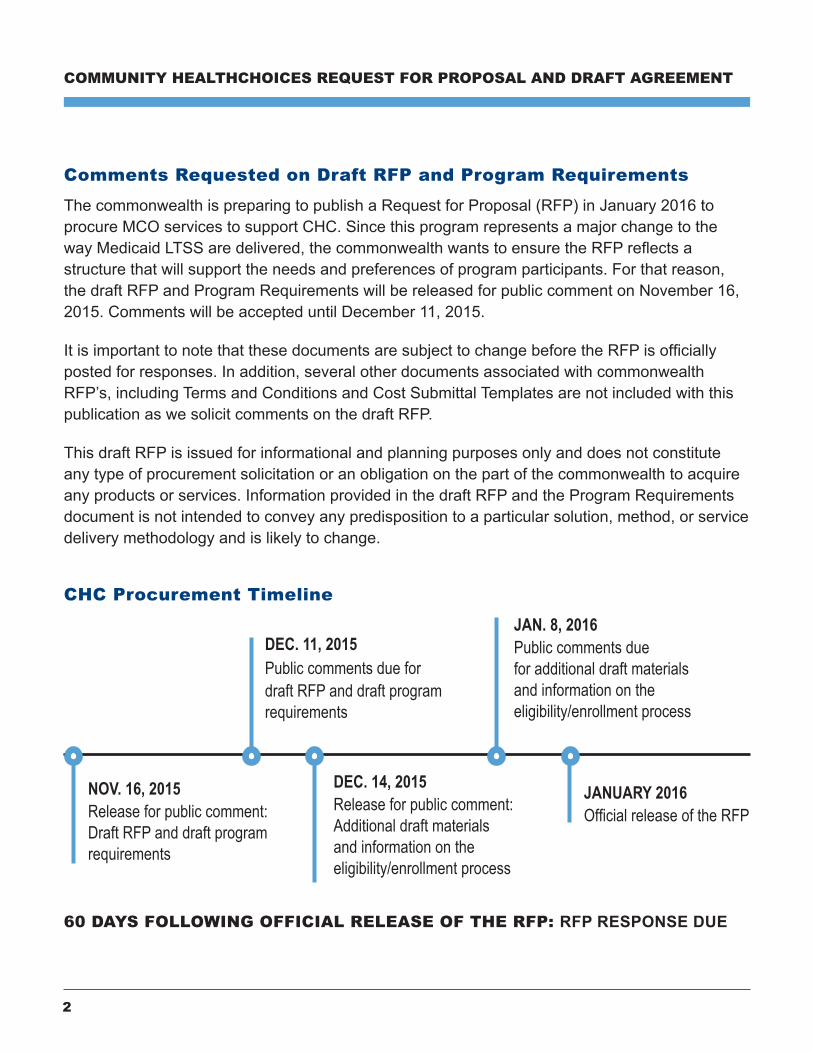
CHC Procurement Timeline
NOV. 16, 2015Release for public comment: Draft RFP and draft program requirements
DEC. 11, 2015Public comments due for draft RFP and draft program requirements
DEC. 14, 2015Release for public comment: Additional draft materials and information on the eligibility/enrollment process
JAN. 8, 2016Public comments due for additional draft materials and information on the eligibility/enrollment process
JANUARY 2016Official release of the RFP
60 DAYS FOLLOWING OFFICIAL RELEASE OF THE RFP: RFP RESPONSE DUE

3
NOVEMBER 2015
The commonwealth does not intend to make this publication any sort of “pre-proposal,” nor does it expect or want entities to provide information that is proprietary or competitively sensitive at this time. While the commonwealth expects that the information gathered through the public comment process will help shape the ultimate project scope and requirements, it is not our goal to define such things at this stage.
Vendors submitting a response should be aware that the responses to this publication will be public information and that no claims of confidentiality will be honored. The information gathered through this process may be used in the development of future procurement documents that will promote vendor competition and provide cost savings opportunities for the commonwealth. Respondents shall not provide recommendations as to specific courses of action. The commonwealth will evaluate the information presented and determine its subsequent course of action.
Specific responses to the publication will not be returned and respondents will not be notified of the results of the review nor will they be provided copies of the review. The Commonwealth of Pennsylvania is not liable for any costs incurred by vendors in developing responses for this publication. When the CHC RFP is published no vendor(s) will be selected, pre-qualified, or exempted based on their participation in this publication.
CHC Procurement and Summary Background
DHS and PDA received thousands of comments from consumers, caregivers, legislators, and stakeholders about the January 2017 transition to CHC and its upcoming procurement. Throughout the course of those conversations there was a recurring theme of the desire for more time for stakeholder review. In order to ensure the commonwealth’s commitment to openness and transparency, the departments adjusted the process to allow for additional public input before officially releasing the CHC RFP.
DHS and PDA will continue to engage program participants along with members of several Medical Assistance Advisory Sub-committees during the RFP review process. These individuals will also review and provide input to the internal RFP technical evaluation committee.
The CHC draft RFP and draft agreement build upon the HealthChoices (HC) RFP and draft agreement. This summary document highlights the customization of the HC documents to support the CHC program and to identify specific changes.
4
COMMUNITY HEALTHCHOICES REQUEST FOR PROPOSAL AND DRAFT AGREEMENT
CHC RFP
The CHC RFP (Appendix 1) includes extensive revisions in support of the new program. The following areas include changes:
Problem Statement
Discusses the goals and objectives specific to CHC as opposed to HC.
Discusses the phased rollout of CHC.
Specifies the population including the dual eligible and the LTSS recipients.
Work Statement Questionnaire
Includes questions specific to the CHC program including service integration between Medicare and Medicaid, coordination of care, participant-directed services, and LTSS.
Includes questions specific to the CHC goals such as emphasizing HCBS services, nursing facility transition, and person-centered service planning.
CHC Draft Agreement Section II: Definitions
This section includes additional definitions for the CHC program related to older adults, adults with physical disabilities, the dual eligible population, Medicare special needs plans, and LTSS.
CHC Draft Agreement Section V: Program RequirementsThis section includes substantial changes and additions to the HC agreement’s program requirements.
Covered Services
Clarifies that physical health services must meet medical necessity requirements for approval whereas LTSS must meet the requirements of the 1915(c) Waiver. (Section V.A.)
Specifies that Exhibit DDD includes the addition of a detailed list of covered services, including definitions. (Section V.A.1)
Specifies that CHC-MCOs are encouraged to provide LTSS at their own expense to those at risk of nursing home level of care. (Section V.A.4)

5
NOVEMBER 2015
Allows the person-centered service plan (service plan) to capture and reflect referrals and states that service coordinators will provide help in obtaining necessary referrals. (Section V.A.6)
Specifies that behavioral health (BH) services will be available through the Behavioral Health Managed Care Organization (BH-MCO), but that CHC-MCO service coordinators must coordi-nate access to BH services. (Section V.A.7)
Clarifies that access to outpatient drugs will be limited for Medicare Part D participants. (Section V.A.8)
Revises the HC requirement that CHC-MCOs pay for examinations to determine abuse or neglect of children to reflect that they must pay for these for adults and older adults under the adult and older adult protective services requirements. (Section V.A.12)
Notes that Medicare may also cover hospice for dual eligibles. (Section V.A.13)
Adds the requirement for CHC-MCOs to cover non-medical transportation and for service coordinators to coordinate access to all medical and non-medical transportation for participants. (Section V.A.15)
Clarifies that nursing facility (NF) care is covered beyond the first 30 days of admission (the HC limit). Explains the indefinite continuity of care protection for NF residents who reside in a nursing facility on the first effective date of the program in the zone. (Section V.A.17)
Requires the CHC-MCOs to ensure that all NF-related processes are completed and monitored. This includes but is not limited to: preadmission screening resident review (PASRR) process, specialized service delivery, participant’s rights, patient pay liability, personal care accounts or other identified processes. (Section V.A.17)
Requires the CHC-MCOs to offer participant-directed personal assistance and respite services, as are currently available in HCBS waivers. (Section V.A.18)
Requires the CHC-MCOs to offer broad health and wellness education and outreach for participants and caregivers on topics including, but not limited to, heart attack and stroke prevention, asthma, living with chronic conditions, back care, stress management, healthy eating and weight management, oral hygiene, and osteoporosis. This service shall also include annual preventive care reminders and caregiver resources and efforts to actively promote healthy lifestyles as well as disease prevention and health promotion. (Section V.A.19)

6
COMMUNITY HEALTHCHOICES REQUEST FOR PROPOSAL AND DRAFT AGREEMENT
Requires CHC-MCOs to provide services in the least restrictive, most integrated setting and that all settings must comply with the HCBS Settings Final Rule. (Section V.A.20)
Requires the CHC-MCOs to promote innovation in service delivery in target areas such as housing innovation, employment innovation, workforce innovation, and technology innovation. (Section V.A.21)
Outlines that approved service plans serve as prior authorization for the provision of services outlined therein, including health services if a health care provider participated in the service plan development process and authorized the physical health services as authorized within his/her scope of practice. If a health care provider is not involved in the development of the service plan and for all physical health services required by the participant between service plans, physical health services will be prior authorized in accordance with the CHC-MCO’s approved prior authorization plan. For any additional LTSS required between service plans, the service coordinator will authorize the LTSS in accordance with the CHC-MCO’s policies approved by DHS. In accordance with Section V.F., trigger events will prompt a comprehensive reassessment and, if needed, a service plan revision. (Section V.B.1)
Prohibits CHC-MCOs from requiring prior authorization of Medicare services for participants with Medicare and encourages CHC-MCOs to conditionally approve cross-over covered services that are pending Medicare decisions so as to expedite Medicaid access in the event that Medicare denies. (Section V.B.1)
Outlines the indefinite continuity of care (COC) period for NF residents, the 180 day COC for LTSS participants, and the 60 day COC for all physical health services, which apply at the outset of the program. Outlines the 60 day COC period for all LTSS and physical health services during plan-to-plan transitions and upon termination of a provider from a network. (Section V.C)
Specifies that choice of provider includes choice of service coordinator. Prohibits CHC-MCO interference with participant choice of provider. (Section V.D)
Requires the CHC-MCOs to conduct a needs screening to identify any unmet needs, health care needs requiring chronic condition or disease management, service gaps, or need for service coordination within 30 days of admission and that any screenings that reflect unmet needs mean the CHC-MCO must conduct a comprehensive needs assessment. Needs screening may be conducted by phone, electronically, by mail, or in person. DHS must preapprove the CHC-MCOs’ needs screening tool. (Section V.E)
Needs Identification, Service Planning, and Service Coordination

7
NOVEMBER 2015
Requires that the CHC-MCOs conduct a comprehensive needs assessment on (1) participants who are receiving LTSS at the time of enrollment, (2) participants whose needs screening reflected a need for further assessment, and (3) participants who request service coordination.(Section V.F)
Outlines that comprehensive needs assessments must be completed within set timeframes using a DHS-designated assessment tool to capture required topic areas. Reassessments must be conducted annually or in the event of one of several outlined triggers. (Section V.F)
Requires each CHC-MCO to develop a person-centered planning approach to service plan development and implementation and that this person-centered planning team (PCPT) approach must be person-centered. Requires the CHC-MCO’s PCPT approach to be approved annually.(Section V.G)
Requires the CHC-MCOs to develop service plans for all participants who have had comprehensive needs assessments. Outlines minimum requirements for service plan content –one list to address physical and behavioral needs and conditions with an additional list for partici-pants with LTSS needs and conditions. Requires service plans to be developed within 30 days of any comprehensive needs assessment or reassessment. (Section V.H)
Specifies the right of DHS to review and revise any service plan. Requires the CHC-MCOsto submit weekly reports on service plan changes. (Section V.I)
Outlines the role of service coordinators. Requires CHC-MCOs to submit for approval their staffing, contact plan, caseloads, and in-person contact minimum requirements as well as how real-time information will be communicated to and from service coordinators. (Section V.J)
Delineates service coordinator, supervisor qualifications, and training requirements. All employed or contracted service coordinators must be an RN or have a bachelor’s degree in social work, psychology or other related fields and at least three years of experience in the coordination of services. All service coordinator supervisors must be employed by the CHC-MCO or a service coordination entity under contract with the CHC-MCO and mustbe: a licensed social worker with at least five years of relevant experience or a registered nurse with at least five years of relevant experience. (Section V.K)
Requires the CHC-MCOs to offer nursing home transition services which may be coordinated by service coordinators. (Section V.L)
8
COMMUNITY HEALTHCHOICES REQUEST FOR PROPOSAL AND DRAFT AGREEMENT
Specifies that services coordinators must coordinate services across all delivery systems including but not limited to BH-MCOs and the Medical Assistance Transportation Program (MATP). (Section V.M)
Enrollment and Education
The CHC-MCO agrees to cooperate with the functions of the independent enrollment entity (IEE), as specified in guidance from DHS. (Section V.EE)
Outlines disenrollment rules. (Section V.O.18)
Requires the CHC-MCOs to send participants translated materials, based on language preferences identified by the CHC-MCO and IEE. (Section V.O.4)
Specifies that newborns will initially be covered by Medical Assistance Fee-for-Service and not be covered by the CHC-MCOs. (Section V.O.7)
Requires CHC-MCO and service coordinator cooperation when a participant transitions between one CHC-MCO and another or between CHC and LIFE, CHC and HC, etc. (Section V.O.8 and V.O.9)
Adds requirements to include information about LTSS, service coordination, and aligned D-SNP coverage in all outreach, marketing, and participant education documents (handbooks, etc.). (Section V.O)
Requires CHC-MCOs to have a 24/7 nurse hotline to answer health questions, in addition to the CHC-MCO’s toll-free call center that can connect to service coordinators. (Section V.P.2)
Plan Organization and Administration
Requires CHC-MCOs to have a Participant Advisory Committee (PAC) that meets quarterly, is representative of the population, and provides input to the CHC-MCO. Meeting minutes are required to be made public and CHC-MCO must report on how they incorporate the PAC recommendations into CHC-MCO operations. (Section V.O.18)
Adds additional required key personnel – a director of quality, a director of LTSS, a director of service coordination, a participant service manager, and a provider claims educator. (Section V.V and V.W)
9
NOVEMBER 2015
Requires the CHC-MCO staff to represent the racial, ethnic and cultural diversity of the program and also be composed of older Pennsylvanians and adult Pennsylvanians with disabilities. (Section V.W)
Removes the obligation to have a special needs unit because 1) all participants have special needs and 2) services will be coordinated by service coordinators.
Networks and Provider Requirement Provisions Differing from HealthChoices Agreement
Expands primary care provider (PCP) selection and assignment concepts to address service coordinator selection and assignment. (Section V.Z and V.AA)
Requires CHC-MCOs to contract with all willing and qualified LTSS providers for the first six months of the roll-out in each zone and to meet enhanced network requirements outlined in Exhibit AAA. (Section V.DD)
Requires CHC-MCOs to hold providers to all minimum qualifications set by DHS. (Section V.DD.1)
Requires CHC-MCO to ensure that the network meets cultural, linguistic, and disability competency requirements. (Section V.DD.3)
Permits all participants to select a specialist as a PCP, since all participants have special needs. Specialist must agree to and comply with all PCP requirements. (Section V.DD.5)
In addition to the HC requirement that related parties of an MCO negotiate with other CHC-MCOs, requires that CHC-MCOs negotiate with providers that are not related parties. (Section V.DD.6)
Quality
Requires CHC-MCOs to provide a Quality Assessment and Performance Improvement program (QAPI), to have a Quality Management/ Quality Improvement (QM/QI) program that addresses physical health and LTSS, and to conduct Performance Improvement Projects (PIPs). (Section V.EE.1)
Requires CHC-MCOs to report on an array of quality measures outlined in Exhibit GGG. (Exhibit GGG)

10
COMMUNITY HEALTHCHOICES REQUEST FOR PROPOSAL AND DRAFT AGREEMENT
Requires CHC-MCOs to cooperate with any research and evaluation activities conducted by or on behalf of DHS. (Section V.EE.12)
Requires the UM process to comply with NCQA requirements. (Section V.EE.3)
Indicates that pay for performance may be employed. (Section V.EE.6)
CHC Draft Agreement ExhibitsThese CHC exhibits include changes and additions from the HC draft agreement.
Exhibit C – Provider Termination Requires providers who leave the CHC-MCO to continue to serve participants until a transition to an in-network provider can be accomplished and requires the CHC-MCO to continue to pay the provider during this transitional period.
Exhibit CC – Data Support for CHC-MCOs Revised to reflect elements specific to CHC.
Exhibit FF – Provider Directories:
Revised to add in requirements around listing languages spoken, communication competencies, and special services.
Revised to add in requirements around LTSS providers.
Exhibit GG – Complaint, Grievance, and DHS Fair Hearing Processes States DHS will form stakeholder focus groups on the grievance and appeals process and will update procedures based on public input.
Exhibit PP – Provider Manuals Revised to require manuals to include information about LTSS and the assessment, service planning, and service coordination processes.

11
NOVEMBER 2015
Exhibit AAA – Provider Network Composition/Service Access
Revised to add requirements around access to LTSS providers.
Revised to change travel and distance requirements for specialists.
Revised to require compliance with Medicare network access rules, to the extent they are stringent.
Articulates Out-of-Network provider access rules where network cannot support the required access.
Revised EPSDT language.
Exhibit DDD: Covered Services New exhibit lists out all covered services and provides definitions for LTSS services.
The draft agreement includes the following CHC exhibits, but includes no major changes from the HC exhibits:
Exhibit E(1): Other Federal Requirements
Exhibit F: Family Planning Services Procedures
Exhibit J: EPSDT Guidance
Exhibit K: Emergency Services
Exhibit L: Medical Assistance Transportation Program
Exhibit U: Behavioral Health Services
Exhibit X: Community HealthChoices CHC-MCO and Service Providers
Exhibit DD: CHC-MCO Participant Handbook
Exhibit II: Required Contract Terms for Administrative Subcontractors
Exhibit KK: Reporting Suspected Fraud and Abuse to the Department
Exhibit LL: Guidelines for Sanctions Regarding Fraud and Abuse
Exhibit WW: Community HealthChoices Audit Clause
Exhibit XX: Encounter Data Submission Requirements and Penalty Applications
Exhibit BBB: Prescription Services
Exhibit CCC: CHC-MCO Provider Agreements
CHC Draft Agreement Section V: Program Requirements
Stakeholders may submit comment for this document in the following way:
FEEDBACK IS DUE BY DECEMBER 11, 2015. Please submit your written feedback by MAIL or EMAIL.
BY MAILApril Leonhard Office of Long-Term Living Bureau of Policy and Regulatory Management P.O. Box 8025 Harrisburg, PA 17105-8025
BY EMAILPlease send your comments to [email protected] and include “Community HealthChoices” in the subject line.


















