Reproductive Sciences-2016-Rao-1933719116658705
14
Review Involvement of Luteinizing Hormone in Alzheimer Disease Development in Elderly Women C. V. Rao, PhD 1,2,3 Abstract Alzheimer disease (AD) is a slow progressive neurodegenerative disease that affects more elderly women than elderly men. It impairs memory, typically progresses into multidomain cognitive decline that destroys the quality of life, and ultimately leads to death. About 5.3 million older Americans are now living with this disease, and this number is projected to rise to 14 million by 2050. Annual health-care costs in the United States alone are projected to increase to about US$1.1 trillion by 2050. The initial theory that decreasing estrogen levels leads to AD development in postmenopausal women has been proven inconclusive. For example, Women’s Health Research Initiative Memory Study and the population-based nested case–control study have failed to demonstrate that estrogen/progesterone (hormone replacement therapy [HRT]) or estrogen replacement therapy could prevent the cognitive decline or reduce the risk of AD. This led to the realization that AD development could be due to a progressive increase in luteinizing hormone (LH) levels in postmenopausal women. Accordingly, a large number of studies have demonstrated that an increase in LH levels is positively correlated with neuropathological, behavioral, and cognitive changes in AD. In addition, LH has been shown to promote amyloidogenic pathway of precursor protein metabolism and deposition of amyloid b plaques in the hippocampus, a region involved in AD. Cognate receptors that mediate LH effects are abundantly expressed in the hippo- campus. Reducing the LH levels by treatment with gonadotropin-releasing hormone agonists could provide therapeutic benefits. Despite these advances, many questions remain and require further research. Keywords Alzheimer disease, luteinizing hormone, estrogens, androgens, LH/hCG receptors, Ab plaques, neurofibrillary tangles Introduction Alzheimer disease (AD) is a neurodegenerative disease that primarily affects elderly women. 1-3 The disease progression is exceedingly slow and can take decades before the symptoms appear and a clinical diagnosis can be made. 1-3 Dementia, which is a decline in cognitive ability and memory loss, is the hallmark feature of AD. 1-3 It accounts for more dementias than from any other illnesses, including vascular etiologies. The distinction between them often made by an expert neurolo- gist. 1-3 Since some of the AD symptoms overlap with those due to other neurodegenerative diseases and even from taking certain medications, careful clinical history and neurological examination are important for AD diagnosis. 1,3 The risk factors, which can influence each person differ- ently, include family history, genetics, heart disease, stroke, high blood pressure, dyslipidemia, low levels of vitamin folate, and so on. 1-3,4 Obesity and type 2 diabetes increase the risk 3.0- and 1.5-fold, respectively. 1-3,5,6 Only 1% of all cases with AD are inherited. 1-3 There are risk (apolipoprotein E4) and deter- ministic (amyloid precursor protein [APP], presenilin 1 and 2) AD genes. 7,8 The mutations in deterministic genes cause a rare form of the disease. 7,8 Healthy weight maintenance, prevention of type 2 diabetes, exercise, and drinking coffee and red wine in moderation appear to reduce the risks of AD. 1-3 Being physically and men- tally active and engaging in social activities can delay the onset and slow the progression of AD. 1-3 There are no simple diag- nostic tests. 1-3 Position emission tomography (PET), spinal taps to determine brain amyloid b (Ab) levels, and brain 1 Department of Cellular Biology and Pharmacology, Reproduction and Development Program, Herbert Wertheim College of Medicine, Florida International University, Miami, FL, USA 2 Department of Molecular and Human Genetics, Reproduction and Development Program, Herbert Wertheim College of Medicine, Florida International University, Miami, FL, USA 3 Department of Obstetrics and Gynecology, Reproduction and Development Program, Herbert Wertheim College of Medicine, Florida International University, Miami, FL, USA Corresponding Author: C. V. Rao, Departments of Cellular Biology and Pharmacology, Molecular and Human Genetics, and Obstetrics and Gynecology, Reproduction and Development Program, Herbert Wertheim College of Medicine, Florida International University, Miami, FL 33199, USA. Email: [email protected] Reproductive Sciences 1-14 ª The Author(s) 2016 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/1933719116658705 rs.sagepub.com by guest on July 20, 2016 rsx.sagepub.com Downloaded from
Transcript of Reproductive Sciences-2016-Rao-1933719116658705

Review
Involvement of Luteinizing Hormonein Alzheimer Disease Developmentin Elderly Women
C. V. Rao, PhD1,2,3
AbstractAlzheimer disease (AD) is a slow progressive neurodegenerative disease that affects more elderly women than elderly men. Itimpairs memory, typically progresses into multidomain cognitive decline that destroys the quality of life, and ultimately leads todeath. About 5.3 million older Americans are now living with this disease, and this number is projected to rise to 14 million by2050. Annual health-care costs in the United States alone are projected to increase to about US$1.1 trillion by 2050. The initialtheory that decreasing estrogen levels leads to AD development in postmenopausal women has been proven inconclusive. Forexample, Women’s Health Research Initiative Memory Study and the population-based nested case–control study have failed todemonstrate that estrogen/progesterone (hormone replacement therapy [HRT]) or estrogen replacement therapy could preventthe cognitive decline or reduce the risk of AD. This led to the realization that AD development could be due to a progressiveincrease in luteinizing hormone (LH) levels in postmenopausal women. Accordingly, a large number of studies have demonstratedthat an increase in LH levels is positively correlated with neuropathological, behavioral, and cognitive changes in AD. In addition,LH has been shown to promote amyloidogenic pathway of precursor protein metabolism and deposition of amyloid b plaques inthe hippocampus, a region involved in AD. Cognate receptors that mediate LH effects are abundantly expressed in the hippo-campus. Reducing the LH levels by treatment with gonadotropin-releasing hormone agonists could provide therapeutic benefits.Despite these advances, many questions remain and require further research.
KeywordsAlzheimer disease, luteinizing hormone, estrogens, androgens, LH/hCG receptors, Ab plaques, neurofibrillary tangles
Introduction
Alzheimer disease (AD) is a neurodegenerative disease that
primarily affects elderly women.1-3 The disease progression
is exceedingly slow and can take decades before the symptoms
appear and a clinical diagnosis can be made.1-3 Dementia,
which is a decline in cognitive ability and memory loss, is the
hallmark feature of AD.1-3 It accounts for more dementias than
from any other illnesses, including vascular etiologies. The
distinction between them often made by an expert neurolo-
gist.1-3 Since some of the AD symptoms overlap with those
due to other neurodegenerative diseases and even from taking
certain medications, careful clinical history and neurological
examination are important for AD diagnosis.1,3
The risk factors, which can influence each person differ-
ently, include family history, genetics, heart disease, stroke,
high blood pressure, dyslipidemia, low levels of vitamin folate,
and so on.1-3,4 Obesity and type 2 diabetes increase the risk 3.0-
and 1.5-fold, respectively.1-3,5,6 Only 1% of all cases with AD
are inherited.1-3 There are risk (apolipoprotein E4) and deter-
ministic (amyloid precursor protein [APP], presenilin 1 and 2)
AD genes.7,8 The mutations in deterministic genes cause a rare
form of the disease.7,8
Healthy weight maintenance, prevention of type 2 diabetes,
exercise, and drinking coffee and red wine in moderation
appear to reduce the risks of AD.1-3 Being physically and men-
tally active and engaging in social activities can delay the onset
and slow the progression of AD.1-3 There are no simple diag-
nostic tests.1-3 Position emission tomography (PET), spinal
taps to determine brain amyloid b (Ab) levels, and brain
1 Department of Cellular Biology and Pharmacology, Reproduction and
Development Program, Herbert Wertheim College of Medicine, Florida
International University, Miami, FL, USA2 Department of Molecular and Human Genetics, Reproduction and
Development Program, Herbert Wertheim College of Medicine, Florida
International University, Miami, FL, USA3 Department of Obstetrics and Gynecology, Reproduction and Development
Program, Herbert Wertheim College of Medicine, Florida International
University, Miami, FL, USA
Corresponding Author:
C. V. Rao, Departments of Cellular Biology and Pharmacology, Molecular
and Human Genetics, and Obstetrics and Gynecology, Reproduction and
Development Program, Herbert Wertheim College of Medicine, Florida
International University, Miami, FL 33199, USA.
Email: [email protected]
Reproductive Sciences1-14ª The Author(s) 2016Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1933719116658705rs.sagepub.com
by guest on July 20, 2016rsx.sagepub.comDownloaded from

imaging can be helpful in the diagnosis of AD.1-3 These tests
are expensive and not widely available. Therefore, blood
biomarker-based tests, which detect Ab, are being developed.
However, unequivocal diagnosis can only be made at
autopsy.1-3,9
The incidence of AD is higher among older African and
Hispanic than Caucasian Americans.10 The total number of
cases with AD is increasing each year in the United States, due
to an increase in life expectancy from better health care and the
number of people surviving into their 80s, 90s, and beyond.
There are mild, moderate, and severe forms of the disease.1-3
Although individuals with mild AD can live up to 25 years, the
ones with severe AD typically live for only 5 years.1-3 In severe
form of AD, most of the cortex is severely damaged and brain
dramatically shrinks due to widespread cell death.1-3 Alzhei-
mer disease is one of the top 10 leading causes of death in the
United States, sixth leading cause of death among adults, and
fifth leading cause of death among 65- to 85-year-old people.1-3
Alzheimer disease is a very expensive disease. For exam-
ple, US$226 billion is estimated to cost for AD care in the
United States in 2015.11 These costs do not include unpaid
care given by family members and friends, which is roughly
estimated to be 18 billion hours or about US$218 billion.3
Living with AD is extremely difficult because of pain, suffer-
ing, loss of individuals’ dignity, financial setbacks, disruption
of families, among others.1-3
Amyloid Plaques and Neurofibrillary Tangles
The deposition of Ab protein plaques and formation of neuro-
fibrillary tangles of hyperphosphorylated tau proteins in the
hippocampus and frontal cortex are hallmark features of
AD.12-15 The plaques are formed due to an imbalance between
the production and the clearance of Ab from the brain.12,13 The
plaques are rather inert and its Ab aggregates promote synaptic
dysfunction, disrupt mitochondrial activity, induce cascades of
generation of free radicals, cause oxidative damage, increase
tau phosphorylation, impair receptor signaling, Ca2þ homeos-
tasis, induce membrane depolarization, proinflammatory
changes, and so on.12,13 The neurofibrillary tangles consist of
intraneuronal paired helical filaments of hyperphosphorylated
tau protein. These tau proteins contain more phosphorylation
sites and have a higher molecular weight than the normal tau
protein.14,16 The tangles interfere with protein and nutrient
traffic in neurons.1-3,16,17 Plaques and tangles can also cause
an immune response and work synergistically to promote neu-
rodegeneration in the brain.12-16
Amyloid bs are formed from APP, a single-pass transmem-
brane protein, with a large extracellular domain and a small
cytoplasmic tail.17 Amyloid bs are formed by the sequential
cleavage at the N-terminal domain by b-secretase, resulting in
shedding of APP ectodomain.18 Then, g secretase cleaves
membrane-associated APP C-terminus domain, releasing Abmolecules.18 There are 2 forms of Ab molecules, Ab1-40 and
Ab1-42.18 They are sticky, but Ab1-42 is more neurotoxic
because it aggregates much more rapidly, which facilitate
further deposition of Ab molecules.18 The Ab plaques can be
cleared from the brain by efflux, phagocytosis, and enzyme
degradation by neprilysin and insulin-degrading enzyme (pre-
ferential toward insulin).12,13 Neurofibrillary tangles, on the
other hand, can disappear due to dissolution.16
Neuroprotective agents, such as estrogens and androgens,
promote nonamyloidgenic pathway of APP metabolism in
which a-secretase cleaves within Ab domain of APP, prevent-
ing the formation of Ab molecules and releasing neuroprotec-
tive a-APP fragments.18-20 The neurotoxic agents, such as
luteinizing hormone (LH)/human chorionic gonadotropin
(hCG), promote amyloidogenic pathway of APP metabolism
in which Abs are formed.21,22 The mutations in deterministic
genes result in the overproduction and deposition of Abmolecules.7,8
Paradigm Shift on the Actions of LH/hCG
Luteinizing hormone and hCG are structural and functional
homologs that are secreted by anterior pituitary gland and
human placenta, respectively.23 They belong to glycoprotein
and cystine-knot growth factor families.23,24 The latter super-
family includes nerve growth factor (NGF).24 Luteinizing hor-
mone and hCG bind to the same cell surface G-protein-coupled
receptors, which are different from the NGF receptors.25,26
According to the old paradigm, LH/hCG receptors are only
present in gonads and LH/hCG can only regulate gonadal
functions. The paradigm shift has changed this dogma.27 It
has revealed that functional LH/hCG receptors are also pres-
ent in central and peripheral (spinal cord and adrenal pheo-
chromocytoma cells, which have an embryological origin
with neural crest) nervous systems among the other nongona-
dal tissues.28-30
The LH/hCG receptors have been demonstrated in fetal rat
brain and in adult rat, mouse, bovine, and human brains.28,31,32
In fetal rat brains, receptors have been found in diencephalon,
mesencephalon, rhombencephalon, and telencephalon.31 The
receptors are present in neurons as well as in the glial cells.33,34
The neuronal receptors are involved in neurite outgrowth and
their survival.33 The glial cell receptors are involved in the
regulation of prostaglandins (PGs) synthesis, which influence
cell proliferation.34 The sum of all the LH actions can contrib-
ute to growth, development, and differentiation of fetal brains.
Adult brain receptors have been well characterized. The
receptors were found in hippocampus; dentate gyrus; cerebel-
lum; cerebral cortex; hypothalamus; preoptic area; anterior
pituitary; choroid plexus; ependymal cells of third, fourth, and
lateral ventricles; pineal gland; and brain stem, with the highest
levels in rat hippocampus.28,30,32,35 Unlike adults, fetal hippo-
campus does not contain higher receptor levels than the other
brain areas.31
The receptors were also detected in primary as well as in
immortalized cells, such as hypothalamic GT1-7 neurons, a-T3
anterior pituitary gonadotropins, HN33p hippocampal neurons,
and so on.36-40 The receptor promoter usage appears to be the
same among these cells.41 However, the transacting protein
2 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

levels are different, which may explain the receptor level dif-
ferences among the cells.41
The functional relevance of adult brain LH/hCG receptors
has been investigated by primary GnRH and hippocampal neu-
rons as well as by GT1-7, a-T3, and human M17 neuroblas-
toma cells. In primary and in GT1-7 cells, hCG inhibited the
release of gonadotropin-releasing hormone (GnRH).36,38 This
inhibition was due to a decrease in the transcription of GnRH
gene in GT1-7 neurons.36 The mechanisms involved downre-
gulation of GnRH receptor gene by decreasing the stability of
the transcripts and induction of a 95-kDa transacting protein,
which binds to AT-rich sequence (�91 to �81 base pair) in the
50-flanking region of GnRH gene promoter.36,39,42 The induc-
tion preceded by an activation of cyclic AMP (cyclic AMP
[cAMP])/protein kinase A (PKA) signaling and increase in
protein synthesis, phosphor-CREB, c-Fos, and c-Jun lev-
els.38,43 Dimer conformation of the hormone and the receptor
presence are required for the LH/hCG actions.36 These findings
support the presence of short-loop negative feedback mechan-
ism in which some of the LH released from anterior pituitary
gets back into portal circulation to reach hypothalamus to inhi-
bit GnRH release.44-47
The LH/hCG treatment of a-T3 cells resulted in a dose- and
time-dependent and hormone-specific increase in gonadotropin
a-subunit levels.37,48 As expected, GnRH treatment also
increased the gonadotropin-a subunit levels.48 Both LH and
GnRH are synergistic, however, they differed in their mechan-
ism of action. Thus, while LH acted to increase the stability of
gonadotropin-a subunit transcripts, GnRH increased not only
the stability of transcripts but also the transcription of the
gene.48 The LH actions in a-T3 cells suggest that LH promotes
its own synthesis by an ultra-short-loop positive feedback
mechanism, and several previous studies have shown its exis-
tence.44-47 A similar mechanism has been found for hCG synth-
esis in human placenta.49
The neuronal receptors are colocalized with cytochrome
P450 side-chain cleavage enzyme (P450scc).32 The LH/hCG
receptor activation results in a 2-fold increase in pregneno-
lone secretion and an increase in steroidogenic acute regula-
tory protein expression in rat primary hippocampal neurons
and in human M17 neuroblastoma cells.50,51 These findings
suggest that LH and hCG are capable of increasing mitochon-
drial cholesterol transport and its subsequent cleavage by
P450 scc. Thus, LH/hCG can induce steroid production just
as in the gonads.
As peripheral macrophages,52-54 central nervous system
(CNS) macrophages, that is, glial cells, also contain LH/hCG
receptors.34,55 Their activation results in an increase in induci-
ble nitric oxide synthesis, mediated by tumor necrosis factor
a.55 Glial cells can also synthesize PGs and neurosteroids.34,50
Luteinizing hormone/hCG can stimulate glial cell synthesis of
PGs, and whether they can also regulate the synthesis of neu-
rosteroids is unknown.34
The hippocampal receptors are involved in behavioral reg-
ulation.56-61 Thus, central and peripheral injection of hCG
resulted in several behavioral changes, which include:
a. decrease in taste neophobia,61
b. increase in non-rapid eye movement sleep (NREM),
with no effect on rem (REM) sleep,61
c. decrease in exploratory and increase in resting beha-
viors,60,61 and
d. decrease in active awake phase, walking, sniffing, and
chewing.60
The behavioral changes are similar regardless of the route of
injection.61 About 1% of peripherally injected hCG can cross
blood barrier and reach cerebrospinal fluid and hippocampus in
an intact form.61 Some of the above behavioral changes were
considered typical of human pregnancy. Thus, pregnancy-
specific behaviors are likely mediated by the increasing hCG
levels during the first half of pregnancy.
The behavioral hCG effects are blocked by coadministration of
indomethacin.60 Moreover, hCG treatment increased prostaglandin
D2 (PGD2) and decreased prostaglandin E2 (PGE2) synthesis.60
Treatment of hippocampal HN33p cells resulted in a modest dose-
and time-dependent and hormone-specific increase in 5-
lipoxygenase levels.40 These findings support that the products of
arachidonic acid metabolism mediate the behavioral effects of hCG.
Neural retina, which is an extension of CNS, also contains
LH/hCG receptors.62,63 The receptor transcript levels are sim-
ilar between retina and cerebral cortex.62 Photoreceptor cells
contained the highest receptor levels, followed by a gradual
decline through inner retinal layers.62 The findings support the
previously suspected LH/hCG role in visual processing and in
pathological eye conditions.64,65
Different cells in gray and white matter of spinal cord con-
tain LH/hCG receptors.29 The receptors seem to mediate the
neurotropic effects of hCG.66 Thus, hCG-treated rats showed a
possible functional recovery and physiological communication
across the spinal cord injured site.67
It is possible that not only the hippocampal LH/hCG recep-
tors but also those in the other brain areas could somehow be
involved in the complex pathogenesis of AD. Further research
is required to verify and extend this possibility.
Evidence Implicating LH in AD Developmentin Elderly Women
Estrogens are neuroprotective.68-70 This protection comes from a
host of different mechanisms such as reducing the neuronal loss
and cerebral ischemia, stimulating axonal sprouting, dendrite spine
formation, and promoting nonamyloidgenic pathway of APP meta-
bolism.19,68-73 In addition, estrogens levels are positively corre-
lated with cognitive performance. Their replacement in women
with cognitive impairment results in an improvement.74-100 Spatial
memory decreases in ovariectomized rats, but estrogen treatment
reverses it.101,102 These findings suggest that HRT and ERT should
prevent cognitive decline in women who had an ovarian failure or a
natural age-dependent decline in ovarian activity. However,
the results of clinical testing were inconclusive.74-100 This could
be due to a number of different reasons, and one of them could
be the recipient’s age when the treatment began.
Rao 3
by guest on July 20, 2016rsx.sagepub.comDownloaded from

The Women’s Health Research Initiative Memory Study
(WHIMS) is ancillary to Women’s Health Initiative (WHI)
on hormone therapy trials. From 39 of 40 WHI clinical centers,
the WHIMS recruited 4894 eligible women (aged 65 years or
older) free of dementia.103,104 They were either placed on HRT
(n¼ 2229) or on placebo (n¼ 2303). Global cognitive function
was measured annually.103,104 The results revealed that HRT
did not improve cognitive function when compared with pla-
cebo group.103,104 Moreover, a subset of women showed a
small increased risk of cognitive decline.103 Another study,
population-based nested control, revealed that ERT did not
reduce AD risk in 112 481 women as compared with a similar
number of cohorts who did not use the therapy.105 The studies
of this size can be expected to have some uncontrolled vari-
ables, which could possibly undermine their conclusions. Nev-
ertheless, the bottom line of the studies is that neither HRT nor
ERT could prevent cognitive decline or AD development in
older women.103-105 The results led to a critical period hypoth-
esis as well as initiated a search for other hormonal causes for
AD development.
According to the critical period hypothesis, while HRT
started immediately after menopause could have worked, it
becomes detrimental with time delay.106,107 In fact, HRT was
administered more than 5 years after the menopause onset in
about 36% of women.103,104 The time delay effect can perhaps
be explained by neurological damage, which increases with an
advancing age of patients with AD.
Concerning the other hormonal basis for AD develop-
ment, it is well known that ovarian function declines with
age, which results in a decrease in estrogen levels and an
increase in LH levels, due to a loss of negative feedback
mechanism by estrogens.108,109 Therefore, the consequence
of estrogens decrease is an increase in LH and/or follicle-
stimulating hormone (FSH) levels. However, this possibil-
ity received almost no attention until the discovery of hip-
pocampal LH/hCG receptors, greater elevation in LH
levels in women with AD, and direct LH effects on cogni-
tion and biochemical changes typical of AD. The role of
FSH is unknown even though its synthesis and receptors
have been demonstrated in rat hippocampus.110 Further
studies are now required to test the possibility of FSH invol-
vement in AD.
There were a now many reports demonstrating the role of
LH in AD development. These are:
– Epidemiological studies have shown that higher LH lev-
els parallel an increase in AD risk.4,111
– Circulating LH levels are more than doubled in postme-
nopausal women who have developed AD than the
cohorts who did not develop the disease or in non-AD
patients with cognitive deficits.112,113
– Ovariectomy causes an elevation in Ab levels in cere-
brospinal fluid and hippocampus.114
– The reduction in LH levels improves cognition,
decreases Ab levels in mouse brain, and prevents mem-
ory loss in neurotoxin-induced AD model.21,115-118
– Similar reduction in LH levels in AD models results in a
decrease in cognitive deficits.114-116,119
– Blocking LH synthesis improves cognition in an intact
AD Tg 2516 mice.116
– Overexpression of LH impairs memory in a mouse AD
model.120
– Elevated LH levels correlate with an increased AD risk
and progression, cognitive decline, and increased Ablevels.112,113,120-124
– Alzheimer disease brains have a strong immunoreactive
LH than the control brains. Moreover, LH accumulates
in pyramidal neurons of AD brains compared with the
age-matched normal brains.121
– Direct exposure of guinea pig brain to LH results in
altered Ab levels.125
– Luteinizing hormone promotes amyloidogenic pathway
of APP metabolism, Ab secretion, and its deposition in
the aging brain.21
– Human chorionic gonadotropin increases b-secretase
activity in a dose-dependent manner.22 The hCG admin-
istration leads to an increase in Ab40 accumulation and
cognitive deficits in a mouse model of AD.22,126,127
– The same hCG treatment applied even to ovariecto-
mized rats results in the disruption of spatial mem-
ory and increase in soluble Ab1-40 and Ab1-42
levels.126
– Treatment of AD transgenic mice with gonadotropin
releasing hormone analog (GnRHA) decreases Abdeposition and improves working memory.120
– The GnRH analogs (GnRHa) treatment results in a 3.5-
fold reduction in Ab1-42 and 1.5-fold reduction in Ab1-
40 levels and improved cognition in the absence of any
changes in estrogen receptors (ERs) a and b, cyto-
chrome P450 119, and StAR levels.21,115
– The GnRHa treatment, but not HRT, improved hippo-
campal spatial memory in 3xTg AD female mice in an
advanced stages of the disease.119,120
– The GnRHa treatment upregulates the pathways associ-
ated with a cognition improvement such as Ca2+/calmo-
dulin-dependent protein kinase 1 (CAMK 1), glutamate
receptor 1 serine residue831 (GluR1Ser831). Estrogens,
on the other hand, had no effect.115,119
– Ablation of LH actions through inactivation of LH/hCG
receptor gene resulted in a reduced Ab accumulation,
plaque formation, and improvement in neuropathologic
features in mouse model of APPSWþ/LHr�.128
– Infants from Down syndrome pregnancies, who had an
in utero exposure to high hCG levels, have an increased
prevalence and an early onset of AD.129-131
Luteinizing Hormone Actions in the Peripheral OrgansThat Can Potentially Contribute to the AD Development
Ovaries, adrenal glands, adipose tissue, and pancreas also
contain functional LH/hCG receptors.132-136 The LH
4 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

actions in them could potentially contribute to AD devel-
opment in postmenopausal women through further eleva-
tion in LH levels. The LH elevation comes from the
estrogen formation from the androgen precursors, which
then positively feedback on hypothalamic–pituitary axis to
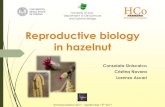
release even more LH (Figure 1).
The involvement of ovaries is related to the LH stimulation
of stromal cell luteinization and their secretion of andro-
gens.137,138 The adrenal involvement is related to the LH sti-
mulation of zona fasciculate to secrete androgens.139-141
Adipose tissue involvement is related to an aromatization of
ovarian and adrenal-derived androgens.142-144
As obesity is one of the risk factors for the AD devel-
opment, it is possible that LH-induced risk involves its fat
deposition property.134 For example, LH can stimulate cell
proliferation, differentiation, and leptin secretion from pre-
adipocytes.134 These actions are mediated by cAMP-/PKA-
independent mitogen-activated protein kinase (MAPK)/
c-Fos signaling.134 Obesity decreases sex steroid–binding
globulin, which results in an increase in circulating free
estradiol levels.145 The free estradiol is a powerful stimu-
lus for bioactive LH release from the anterior pituitary.146
The involvement of the pancreas is related to the LH stimu-
lation of pancreatic b-cells to release more insulin.135 The
increased insulin levels can stimulate proliferation and luteini-
zation of ovarian stromal cells, their secretion of androgens,
and aromatization in adipose tissue.145,147 The impact of per-
ipheral insulin on CNS actions is not known.
The sum of all the LH actions in peripheral organs can result
in further elevation in LH levels in postmenopausal women
who develop AD as compared with cohorts who do not develop
the disease. It is not just the elevation in LH levels alone that
can cause AD development, as not all postmenopausal women
will develop the disease. The subset of women who develop
AD must have other predisposing genetic, epigenetic, environ-
mental, lifestyle risk factors, and so on. This reasoning should
not be surprising as AD, like most other diseases, has multi-
factorial etiology.
Can the Other Conditions of Elevated LH/hCG Leadto AD Development in Women?
Short-term LH elevations, such as preovulatory surges, are not
likely to lead to AD development, not only because of its
Brain
Ovaries AdrenalsPancreas
Adipose�ssue
LHLH
Androgens AndrogensInilusn
Estrogens
LH
Figure 1. The proposed model of luteinizing hormone (LH) involvement in the development of Alzheimer disease (AD) in elderly women. Inthis model, LH released from anterior pituitary gland gets back to hippocampus to promote amyloidogenic pathway of amyloid precursorprotein (APP) metabolism (line thickness denotes the primary action). Secondarily, LH can also act on peripheral tissues either to increaseandrogens secretion or insulin release. The androgens are then aromatized into estrogens in adipose tissue, which positively feedback to releasemore LH. Endogenously produced brain LH may also have a role in the disease process, but this remains to be further investigated.
Rao 5
by guest on July 20, 2016rsx.sagepub.comDownloaded from

shorter duration of elevation but also due to concomitant
increase in estrogen levels, which are neuroprotective.19,68-70
Similarly, pregnancy may also not lead to the AD development,
even though hCG levels are elevated for a longer duration,
because estrogen levels are also elevated to a greater degree
at the same time. These predictions should be further ver-
ified by epidemiological studies on AD incidence in women
who have incessantly ovulated, like nuns, as compared with
those who had interrupted cycles due to pregnancy. Similar
information can come from comparing women who had
multiple pregnancies with those who had fewer pregnancies
during their lifetime.
The AD incidence in other elevated LH/hCG states, such as
polycystic ovarian syndrome (PCOS) and pituitary and placental
(gestational trophoblastic neoplasms) tumors that secrete exces-
sive amounts of LH and hCG, respectively, in the absence of
concomitant increase in estrogen levels, is unknown. However,
there are leads for women with PCOS. There are reports on
women with PCOS having long-term health consequences
including cognitive decline and altered brain microstruc-
ture.148-150 Further affirmation can come from retrospective chart
reviews of the patients. The possibility of AD incidence in rare
cases, such as inactivating and activating LH/hCG receptor muta-
tions, can also be obtained by the reviews of patient charts.
Infants born from Down syndrome pregnancies seem to
develop AD at younger ages.129-131 This is presumably due
to intrauterine exposure to high maternal hCG levels. However,
whether the same high hCG levels can influence AD develop-
ment in the mother is not known. But it is not likely because of
a concomitant elevation in estrogen levels in the mother.
Potential Mechanisms of LH Actions in AD
The following scenarios can be envisioned from what is already
known about the LH/hCG actions in neurons, glial cells, and in
the other somatic cells.27,30,33,34,36-40,42,48,50,51,55
The LH actions can be nongenomic and genomic. In both
cases, initial cell surface receptor binding is required. The
binding results in an activation of second messenger signaling
systems such as cAMP/PKA, protein kinase C (PKC), MAPK,
and so on.
The second messengers can then mediate the nongenomic
actions such as alterations in protein phosphorylation and ion
flux changes. The phosphorylation may include secretases,
other enzymes, proteins associated with APP metabolism
toward the amyloidogenic pathway, hyperphosphorylation of
abnormal tau proteins, and so on.
The chronic actions may require genomic changes, where
activated kinases, directly and indirectly, affect the transacting
factors, which could either increase or decrease the transcrip-
tion of genes. However, the identity of these genes is unknown
for the most part.
The LH actions may also include influencing the stability of
preexisting transcripts, their translation efficiency, and post-
translational modifications of proteins. These changes could
involve both nongenomic and/or genomic mechanisms.
In the above scenarios, the molecular details are not known.
Obviously, a great deal of further research is required to fill the
knowledge gaps to better understand how LH/hCG acts, which
could reveal new therapeutic targets.
Further Research to Answer SomeImportant Questions on AD in ElderlyWomen
The AD development in elderly women is due to physiological
hormonal changes that are associated with aging. Since not all
women going through these changes will develop AD, others
such as genetic, epigenetic, environmental, lifestyle factors,
and so on, must also be required. The identity of them remains
elusive, and only further research can reveal them. Even though
AD is a terrible disease and deaths from it are increasing rela-
tive to cancer and heart disease, AD research funding (US$660
millions) pales by comparison with cancer (US$5.4 billion) and
heart disease (US$1.2 billion).151 This disparity must somehow
be reconciled in order to make the necessary scientific
advances to conquer AD.
Part of the further research should focus on answering the
following fundamental questions.
a. Does age alter brain’s response to estrogens and LH?
b. What role, if any, FSH plays in AD development?
c. The brain can also make estrogens and LH.152-160 The
question then are:
1. What role do the brain-derived hormones play in
AD development in contrast to those that come
from periphery?
2. Is there a relationship between peripheral and brain
levels of estrogens and LH?
3. Do high estrogens suppress brain LH signaling dur-
ing premenopausal period and that this suppression
somehow is lost in an age-dependent manner dur-
ing postmenopausal years? If so, why and how the
suppression mechanisms are lost during aging.
d. What molecular mechanisms are involved in the neuro-
protective role of estrogens?
e. Luteinizing hormone/hCG do not seem to be neurotoxic
when estrogen levels are high. How does the falling
estrogen levels trigger/enhance the development of neu-
rotoxicity of LH?
f. What are the critical genetic and nongenetic factors that
work in concert with LH in AD development?
g. Does LH regulate brain’s insulin synthesis as it does in
the pancreas?
Role of Testosterone (T) and LH in ADDevelopment in Elderly Men
Elderly men account for about one-third of total cases with
AD.1,2 This gender difference could partly be due to a higher
mortality from atherosclerosis, cardiovascular disease, and so
6 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

on, among them, as compared with elderly women. The other
reason could be hormonal changes. For example, age-
dependent hormonal changes are different in elderly men as
compared with elderly women. Thus, elderly men have gradual
increase and lower peak LH levels as compared with elderly
women.161-167 Moreover, the decrease in serum T levels is
gradual as compared with faster and greater decrease in estro-
gens in elderly women.161,163,164,166-168 It is also possible that
the brain sensitivity to androgens is maintained in elderly men,
whereas the estrogen sensitivity dramatically decreases in
elderly women. Elderly men also have an increased androgen
resistance and what role this might play is unknown.18 Inter-
estingly, the gender difference is even seen in APP transgenic
mice. Thus, male mice have a lower brain Ab deposition than
female mice.169
It is possible that both decreasing T levels and increasing
LH levels are involved in AD development in elderly men.18
However, it is not clear whether T is secondary to LH and vice
versa or both work in concert in reciprocal manner.18,170-178 In
support of the LH involvement, increase in its levels results in
neuropathological and cognitive changes characteristic of AD,
reducing its levels in male gonadectomized mice, causing cog-
nitive benefits, and LH/hCG receptor variant reduces AD risk
in men.18,171,175-179 The risk of death in men with AD decreases
when they are placed on GnRHa therapy for prostate cancer.180
The GnRHa treatment works in elderly men, with variable
results just as in elderly women with AD.18
Multiple lines of evidence suggest that T is neuroprotective
and decrease in its levels leads to neuropathological and beha-
vioral changes that are the hallmark of AD.20,181-183 The evi-
dence includes:
– Testosterone levels are positively associated with cogni-
tion in elderly men.184
– The AD development increases as the T levels decline
during aging.170
– The men with AD have a lower T levels, low T levels are
an independent risk factor for AD, and T deprivation
increases the future AD risk.99,112,184
– Testosterone levels are negatively associated and LH
levels are positively associated with the brain Abdeposition during early stages (mild cognitive impair-
ment) and presymptomatic phase of AD (subjective
memory complemers).177
– The T therapy works in hypogonadal men with AD.185
– Men who have undergone chemical castration have
increased Ab levels.171,186,187
– Men with AD have reduced brain T levels.188
– Declining T levels is a risk factor for AD.183,188,189
– Testosterone levels are inversely correlated with Ablevels.171,176,187
– Testosterone has distinct effects on plasma and cere-
brospinal fluid levels of Ab protein.189,190
– Testosterone decreases neuronal Ab secretion.20,174
– Testosterone decreases Ab toxicity in cultured hippo-
campal cells.18,191
– Testosterone improves neuronal viability, synaptic
plasticity, cognition, and reduce AD pathology
treatment.173,184,192,193
– Gonadectomy increases Ab levels, and reducing LH
levels improves cognition.176,178
– Androgen depletion in transgenic mice increases brain
Ab deposition and impairs hippocampal-dependent
behavioral performance.175
– Testosterone regulates the development of AD neuro-
pathology in mice model of AD.194,195
– T lowers Ab levels in a 3x Tg-D male mice.18
The studies on whether T conversion to E is necessary in AD
are inconclusive.18,196 Regardless, the findings suggest that T
replacement should work for the treatment of elderly men with
AD. However, the results are contradictory, which is eerily
similar to the results of HRT or ERT in women with AD.18 If
both T decline and LH rise are independently involved in AD
development, perhaps a better approach will be to combine T
replacement with GnRHa in the treatment of elderly men. This
possibility requires clinical verification. Since T replacement
therapy may increase prostate cancer and cardiovascular
risks, it can be replaced with selective androgen receptor
modulators.18,197
Currently Approved Treatments for AD
There are 6 Food and Drug Administration (FDA)-approved
prescription drugs for the treatment of AD symptoms.198 Four
are acetylcholinesterase inhibitors and they are sold under
brand names of Aricept, Razadyne, Exelon, and Cognex.198
The first 3 are commonly prescribed, and Cognex is rarely
prescribed because of the side effects, including liver dam-
age.198 They all work by increasing acetylcholine, a neuro-
transmitter required for memory, judgment, and thought
processes.198 The fifth is Namenda (brand name), which blocks
N-methyl-D-aspartate (NMDA) receptors, thus protect neurons
from an excess glutamate.198 The sixth one Namzaric, a com-
bination of Aricept and Namenda (brand name Namzaric), is
indicated for patients with moderate to severe disease.198 Acet-
ylcholinesterase inhibitors are indicated either for all stages
(Aricept) or only for those with mild to moderate disease
(Razadyne and Exelon). All the drugs are rather well tolerated.
They cannot, however, reverse the disease or stop further
destruction of the nerve cells. Thus, their effectiveness
decreases as the nerve cell damage increases.198
Finally, there is an antiepileptic drug, Levetiracetam, which
has been tested in patients with dementia at 12 times the lower
dose than that used in epileptics.199 It works by decreasing the
hippocampal neuronal overactivity.199,200 The FDA has
recently approved it for phase III clinical trials.199
There are several new drugs in pipeline that decrease the Abproduction, inhibit its aggregation, or increase its clearance.201
They are MK-8931, which block the b-secretase activity,198
and Solanezumab, a monoclonal antibody, which binds Ab,
Rao 7
by guest on July 20, 2016rsx.sagepub.comDownloaded from

prevent the formation of new plaques and carry excess Abaway from the brain.198
Abnormal form of tau protein can collapse and twist into
tangles, which destroy microtubules and ultimately neu-
rons.14,16 AADvac1 is a vaccine that stimulates the body’s
immune system to attack an abnormal tau protein.198 Microglia
act as a first line of immune defense in the brain and it helps
clear Ab from the brain. CSP-1103, a microglial modulator, is
being evaluated for AD therapy.
Insulin is required for brain health.6,202,203 Part of the brain
insulin is locally synthesized, and the rest comes from periph-
eral circulation.203-206 Insulin activates its brain receptors to
regulate hippocampal metabolism, memory formation, and so
on.203,207 In type 2 diabetes, hippocampal Ab accumulation
increases, and this increase prevents insulin binding to its
receptors, resulting in insulin resistance and exacerbation of
neurodegeneration.202,203,205 Therefore, nasal insulin adminis-
tration is being evaluated to increase brain insulin signaling.198
Future Therapeutic Possibilities
The involvement of LH in AD development in postmenopausal
women offers an obvious therapeutic approach of reducing its
levels by treatment with GnRHa. There are several studies
demonstrating the therapeutic benefit of GnRHa treatment.208
However, a recent phase 2 48-week, double-blind, and placebo-
controlled clinical study on 109 women aged 65 years or older,
with mild to moderate AD, with low- or high-dose GnRHa
(Lupron), showed no benefit especially with a low dose.209 The
high dose, on the other hand, showed statistically nonsignifi-
cant trend of benefit.209 The individuals in the high-dose group,
who are already taking acetylcholinesterase inhibitor, showed a
statistically significant improvement.209 This is likely to be due
to the differences in their mechanism of action. More such
combination therapies and with varying doses need to be tested
to determine whether therapeutic efficiency can be further
improved.
The failure of Lupron treatment alone is not the last verdict,
because most of the other previous clinical trials of AD drugs
on people with dementia diagnosis have failed, presumably due
to prior irreversible brain damage, small sample size, and host
of other factors such as dose, route, duration of treatment, and
so on. Since the treatment failures are common, one should
consider starting the therapies on individuals who have a strong
family history and/or at high risk, as determined by PET, spinal
taps, or brain scans, or even at the onset of early warning signs
such as memory loss, confusion, frequent falling, disorienta-
tion, inability to comprehend, and complete the simple tasks.
The other therapeutic possibilities include developing even
more potent GnRHa, LH/hCG receptor inhibitors, and LH/hCG
receptor gene silencers that can be selectively directed to hip-
pocampus and frontal cortex. Multipronged therapeutic
approaches that prevent further destruction of nerve cells and
also reverse pathological biochemical changes will be optimal
to combat AD. It is estimated that any therapy that can delay
AD progression even by 5 years could reduce the disease
prevalence by 40% and saves over US$300 billion for the
US economy.199
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, author-
ship, and/or publication of this article.
References
1. Alzheimer’s Society. What is Alzheimer’s disease? 2014. Web
site. www.alzheimers.org.uk/site/scripts/documents_info.php?
documentID¼100. Accessed October 3, 2015.
2. Center for Disease Control and Prevention. Alzheimer’s disease.
2015. Web site. http://www.cdc.gov/aging/aginginfo/alzheimers
.htm. Updated March 5, 2015. Accessed October 3, 2015.
3. Alzheimer’s Organization. 2015 Alzheimer’s Disease Facts and
Figures. 2016. Web site. www.alz.org/facts/downloads/facts_
figures_2015.pdf. Updated January 2016. Accessed March 7,
2016.
4. Gao S, Hendrie HC, Hall KS, Hui S. The relationships between
age, sex, and the incidence of dementia and Alzheimer disease: a
meta-analysis. Arch Gen Psychiatry. 1998;55(9):809-815.
5. Wang YC, Pamplin J, Long MW, Ward ZJ, Gortmaker SL,
Andreyeva T. Severe obesity in adults cost state medicaid pro-
grams nearly $8 billion in 2013. Health Aff. 2015;34(11):
1923-1931.
6. Biessels GJ, Reijmer YD. Brain changes underlying cognitive
dysfunction in diabetes: what can we learn from MRI? Diabetes.
2014;63(7):2244-2252.
7. Suzuki N, Cheung TT, Cai XD, et al. An increased percentage of
long amyloid beta protein secreted by familial amyloid beta pro-
tein precursor (beta APP717) mutants. Science. 1994;264(5463):
1336-1340.
8. Scheuner D, Eckman C, Jensen M, et al. Secreted amyloid beta-
protein similar to that in the senile plaques of Alzheimer’s disease
is increased in vivo by the presenilin 1 and 2 and APP mutations
linked to familial Alzheimer’s disease. Nat Med. 1996;2(8):
864-870.
9. Burnham SC, Faux NG, Wilson W, et al. A blood-based predictor
for neocortical Ab burden in Alzheimer’s disease: results from the
AIBL study. Mol Psych. 2014;19(4):519-526.
10. Herbert LE, Scherr PA, Bienias HL, Bennett DA, Evans DA.
Alzheimers disease in the US population: prevalence estimates
using the 2000 census. Arch Neurol. 2003;60(8):1119-1122.
11. Stefanacci RG. The costs of Alzheimer’s disease and the value of
effective therapies. Am J Manage Care. 2011;17(suppl 13):
S356-S362.
12. Bates KA, Verdile G, Li QX, et al. Clearance mechanisms of
Alzheimer’s amyloid-beta peptide: implications for therapeutic
design and diagnostic tests. Mol Psychiatry. 2009;14(5):469-486.
13. Walsh DM, Teplow DB. Alzheimer’s disease and the amyloid
beta-protein. Prog Mol Biol Transl Sci. 2012;107:101-124.
8 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

14. Goedert M, Jakes R, Crowther RA, et al. The abnormal phosphor-
ylation of tau protein at Ser-202 in Alzheimer disease recapitu-
lates phosphorylation during development. Proc Natl Acad Sci U
S A. 1993;90(11):5066-5070.
15. Ittner A, Yazi DK, van Eersel J, Gladbach A, Gotz J, Ittner LM.
Brief update on different roles of tau in neurodegeneration.
IUBMB Life. 2011;63(7):495-502.
16. Hyman B. Untangling tau. Translational Sci. 2016;1:20-21.
17. Goldgaber D, Lerman MI, McBride WO, Saffiotti Y, Gajdusek
DC. Isolation, characterization, and chromosomal localization of
human brain cDNA clones coding for the precursor of the amyloid
of brain in Alzheimer’s disease, Down’s syndrome and aging.
J Neural Transm Suppl. 1987;24:23-28.
18. Verdile G, Asih PR, Barron AM, Wahjoepramono EJ, Ittner LM,
Martins RN. The impact of luteinizing hormone and testosterone
on beta amyloid (Ab) accumulation: animal and human clinical
studies. Horm Behav. 2015;76:81-90.
19. Xu H, Gouras GK, Greenfield JP, et al. Estrogen reduces neuronal
generation of Alzheimer beta-amyloid peptides. Nat Med. 1998;
4(4):447-451.
20. Gouras GK, Xu H, Gross RS, et al. Testosterone reduces neuronal
secretion of Alzheimer’s beta-amyloid peptides. Proc Natl Acad
Sci U S A. 2000;97(3):1202-1205.
21. Bowen RL, Verdile G, Liu T, et al. Luteinizing hormone, a repro-
ductive regulator that modulates the processing of amyloid-b pre-
cursor protein and amyloid-b deposition. J Biol Chem. 2004;
279(19):20539-20545.
22. Saberi S, Du YP, Christie M, Goldsburry C. Human chorionic
gonadotropin increases b-cleavage of amyloid precursor protein
in SH-SY5Y cells. Cell Mol Neurobiol. 2013;33(6):747-751.
23. Pierce JG, Parsons TF. Glycoprotein hormones: structure and
function. Ann Rev Biochem. 1981;50:465-495.
24. Lapthorn AJ, Harris DC, Littlejohn A, et al. Crystal structure of
human chorionic gonadotropin. Nature. 1994;369(6480):
455-461.
25. Loosfelt H, Misrahi M, Atger M, et al. Cloning and sequencing of
porcine LH-hCG receptor cDNA: variants lacking transmem-
brane domain. Science. 1989;245(4917):525-528.
26. McFarland KC, Sprengel R, Phillips HS, et al. Lutropin-
choriogonadotropin receptor: an unusual member of the G
protein-coupled receptor family. Science. 1989;245(4917):
494-499.
27. Rao CV. There is no turning back on the paradigm shift on the
actions of human chorionic gonadotropin and luteinizing hor-
mone. J Reprod Health and Med. 2016;2:4-10.
28. Lei ZM, Rao ChV, Kornyei JL, Licht P, Hiatt ES. Novel expres-
sion of human chorionic gonadotropin/luteinizing hormone recep-
tor gene in brain. Endocrinology. 1993;132(5):2262-2270.
29. Rao SC, Li X, Rao ChV, Magnuson DSK. Human chorionic
gonadotropin/luteinizing hormone receptor expression in the
adult rat spinal cord. Neuroscience Lett. 2003;336(3):
135-138.
30. Meng X-L, Rennert OM, Chan W-Y. Human chorionic gonado-
tropin induces neuronal differentiation of PC12 cells through acti-
vation of stably expressed lutropin/choriogonadotropin receptor.
Endocrinology. 2007;148(12):5865-5873.
31. AL-Hader AA, Tao YX, Lei ZM, Rao ChV. Fetal rat brains con-
tain luteinizing hormone/human chorionic gonadotropin recep-
tors. Early pregnancy. Biol Med. 1997;3(4):323-329.
32. Apaja PM, Harju KT, Aatsinki JT, Petaja-Repo UE, Rajaniemi
HJ. Identification and structural characterization of the neuronal
luteinizing hormone receptor associated with sensory systems. J
Biol Chem. 2004;279(3):1899-1906.
33. AL-Hader AA, Lei ZM, Rao ChV. Neurons from fetal brains
contain functional luteinizing hormone/chorionic gonadotropin
receptors. Biol Reprod. 1997;56(5):1071-1076.
34. Al-Hader AA, Lei ZM, Rao ChV. Novel expression of functional
luteinizing hormone/chorionic gonadotropin receptors in cultured
glial cells from neonatal rat brains. Biol Reprod. 1997;56(2):
501-507.
35. Bhatnagar KP, Li X, Lei ZM, Rao CV. Human pineal luteinizing
hormone receptors. Biotech Histochem. 2002;77(4):223-228.
36. Lei ZM, Rao ChV. Novel presence of luteinizing hormone/human
chorionic gonadotropin (hCG) receptors and the down-regulating
action of hCG on gonadotropin-releasing hormone gene expres-
sion in immortalized hypothalamic GT1-7 neurons. Mol Endocri-
nol. 1994;8(8):1111-1121.
37. Huang ZH, Lei ZM, Rao ChV. Immortalized anterior pituitary
aT3 gonadotropes contain functional luteinizing hormone/human
chorionic gonadotropin receptors. Mol Cell Endocrinol. 1995;
114(1-2):217-222.
38. Mores N, Krsmanovic LZ, Catt KJ. Activation of LH receptors
expressed in GnRH neurons stimulates cyclic AMP production
and inhibits pulsatile neuropeptide release. Endocrinology. 1996;
137(12):5731-5734.
39. Li X, Lei ZM, Rao ChV. Human chorionic gonadotropin down-
regulates the expression of gonadotropin-releasing hormone
receptor gene in GT1-7 neurons. Endocrinology. 1996;137(12):
899-904.
40. Zhang W, Lei ZM, Rao ChV. Immortalized hippocampal cells
contain functional luteinizing hormone/human chorionic gonado-
tropin receptors. Life Sci. 1999;65(20):2083-2098.
41. Hu YL, Lei ZM, Rao ChV. Analysis of the promoter of the lutei-
nizing hormone/human chorionic gonadotropin receptor gene in
neuroendocrine cells. Life Sci. 1998;63(24):2157-2165.
42. Lei ZM, Rao ChV. Cis-Acting elements and trans-acting proteins
in the transcriptional inhibition of gonadotropin-releasing hor-
mone gene by human chorionic gonadotropin in immortalized
hypothalamic GT1-7 neurons. J Biol Chem. 1997;272(22):
14365-14371.
43. Lei ZM, Rao ChV. Signaling and transacting factors in the tran-
scriptional inhibition of gonadotropin releasing hormone gene by
human chorionic gonadotropin in immortalized hypothalamic
GT1-7 neurons. Mol Cell Endocrinol. 1995;109(2):151-157.
44. David MA, Fraschini F, Martini L. Control of LH secretion: role of
a ‘‘short’’ feedback mechanisms. Endocrinology. 1966;78(1):55-60.
45. Molitch M, Edmonds M, Jones EE, Odell WD. Short-loop feed-
back control of luteinizing hormone in the rabbit. Am J Physiol.
1976;230(4):907-910.
46. Patritti-Laborde N, Wolfsen AR, Heber D, Odell WD. Site of
short-loop feedback for luteinizing hormone. J Clin Invest.
1979;64(4):1066-1069.
Rao 9
by guest on July 20, 2016rsx.sagepub.comDownloaded from

47. Melrose PA. In vitro evidence for short-loop gonadotropin feed-
back on gonadotropin-releasing hormone neurons harvested from
adult male rats. Endocrinology. 1987;121(1):200-204.
48. Huang ZH, Lei ZM, Rao ChV. Novel independent and synergistic
regulation of gonadotropin-a subunit gene by luteinizing hor-
mone/human choriogonadotropin and gonadotropin releasing hor-
mone in the aT3-1 gonadotrope cells. Mol Cell Endocrinol. 1997;
130(1-2):23-31.
49. Licht P, Cao H, Lei ZM, Rao CV, Merz WE. Novel self-
regulation of human chorionic gonadotropin biosynthesis in
term pregnancy human placenta. Endocrinol. 1993;133(6):
3014-3025.
50. Webber KM, Stocco DM, Casadesus G, et al. Steroidogenic acute
regulatory protein (StAR): evidence of gonadotropin-induced
steroidogenesis in Alzheimer disease. Mol Neurodegener. 2006;
1:14.
51. Liu T, Wimalasena J, Bowen RL, Atwood CS. Luteinizing hor-
mone receptor mediates neuronal pregnenolone production via
up-regulation of steroidogenic acute regulatory protein expres-
sion. J Neurochem. 2007;100(5):1329-1339.
52. Kim HM, Moon YH. Human chorionic gonadotropin induces
nitric oxide synthase mRNA in mouse peritoneal macrophages.
Biochem Biophys Res Commun. 1996;229(2):548-552.
53. Zhang YM, Rao CV, Lei ZM. Functional importance of human
monocyte luteinizing hormone and chorionic gonadotropin recep-
tors. J Soc Gynecol Investig. 1999;6. Abstract #6.
54. Zhang YM, Rao CV, Lei ZM. Macrophages in human reproduc-
tive tissues contain luteinizing hormone/chorionic gonadotropin
receptors. Am J Reprod Immunol. 2003;49(2):93-100.
55. Kim HM, Rim HK, Shin T, et al. Human chorionic gonadotropin
induces nitric oxide synthesis by murine microglia. Int J Immu-
nopharmacol. 2000;22(6):453-461.
56. Kawakami M, Sawyer CH. Induction of behavioral and electro-
encephalographic changes in the rabbit by hormone administra-
tion or brain stimulation. Endocrinology. 1959;65:631-643.
57. Telegdy G, Rozsahegyi. Effect of gonadotropins on extinction of
an avoidance conditioned reflex and exploratory behaviors in the
rat. Acta Physiol Acad Sci Hung. 1971;40(2):209-214.
58. Telegdy G, RozsahegyiLissak K. Further data on the effect of
human chorionic gonadotrophin on avoidance and exploratory
behavior in the rat. Acta Physiol Acad Sci Hung. 1971;40(2):
215-220.
59. Emanuele NV, Tentler J, Metcalfe L, et al. Intracerebroventricu-
lar luteinizing hormone (LH) depresses feeding in male rats. Neu-
roendocrinol Lett. 1991;13(6):413-418.
60. Toth P, Lukacs H, Hiatt ES, Reid KH, Iyer V, Rao ChV. Admin-
istration of human chorionic gonadotropin affects sleep-wake
phases and other associated behaviors in cycling female rats.
Brain Res. 1994;654(2):181-190.
61. Lukacs H, Hiatt ES, Lei ZM, Rao ChV. Peripheral and intracer-
ebroventricular administration of human chorionic gonadotropin
alters several hippocampus-associated behaviors in cycling
female rats. Horm Behav. 1995;29(1):42-58.
62. Thompson DA, Othman MI, lei ZM, et al. Localization of recep-
tors for luteinizing hormone/chorionic gonadotropin in neural
retina. Life Sci. 1998;63(12):1057-1064.
63. Dukic-Stefanovic S, Walther J, Wosch S, et al. Chorionic gona-
dotropin and its receptor are both expressed in human retina,
possible implications in normal and pathological conditions. PloS
One. 2012;7(12):e52567-e52567.
64. Elman J, Capriolo J, Sears M, Mead A, Rubin P. Chorionic
gonadotropin decreases intraocular pressure and aqueous humor
flow in rabbit eyes. Invest Ophthalmol Vis Sci. 1987;28(1):
197-200.
65. Carmichael DN, Morgan NG, Scarpello JHB. Human chorionic-
gonadotropin stimulates the growth of retinal vascular cells. Dia-
betologia. 1994;38:A275.
66. Patil A, Fillmore K, Valentine J, Hill D. The study of the effect of
human chorionic gonadotrophic (hCG) hormone on the survival
of adrenal medulla transplant in brain. Preliminary study. Acta
Neurochir. 1987;87(1-2):76-78.
67. Patil AA, Nagaraj MP. The effect of human chorionic gonadotro-
pin (hCG) on functional recovery of spinal cord sectioned rats.
Acta Neurochir. 1983;69(3-4):205-218.
68. Garcia-Segura LM, Azcoitia L, DonCarlos LL. Neuroprotection
by estradiol. Prog Neurobiol. 2001;63(1):29-60.
69. Norbury R, Cutter WJ, Compton J, et al. The neuroprotective
effects of estrogen on the aging brain. Exp Gerontol. 2003;
38(1-2):109-117.
70. Pike CJ, Carroll JC, Rosario ER, Barron AM. Protective actions
of sex steroid hormones in Alzheimer’s disease. Front Neuroen-
docrinol. 2009;30(2):239-258.
71. Jaffe AB, Toran-Allerand CD, Greengard P, Gandy SE. Estrogen
regulates metabolism of Alzheimer amyloid beta precursor pro-
tein. J Biol Chem. 1994;269(18):13065-13068.
72. Chang D, Kwan J, Timiras PS. Estrogens influence growth,
maturation, and amyloid beta-peptide production in neuroblas-
toma cells and in beta-APP transfected kidney 293 cell line. Adv
Exp Med Biol. 1997;429:261-271.
73. Zhang Y, Champagne N, Beitel LJ, Goodyer CG, Trifiro M,
LeBlanc A. Estrogen and androgen protection of human neurons
against intracellular amyloid beta1-42 toxicity through heat shock
protein 70. J Neurosci. 2004;24(23):5315-5321.
74. Paganini-Hill A, Henderson VW. Estrogen deficiency and risk of
Alzheimer disease in women. Am J Epidemiol. 1994;140(3):
256-261.
75. Fillit H. Estrogens in the pathogenesis and treatment of Alzhei-
mer’s disease in postmenopausal women. Ann N Y Acad Sci.
1994;743:233-239.
76. Tang MX, Jacobs D, Stern Y, et al. Effects of oestrogen during
menopause on risk and age at onset of Alzheimer’s disease. Lan-
cet. 1996;348(9025):429-432.
77. Birge SJ. The role of estrogen in the treatment and prevention of
dementia: introduction. Am J Med. 1997;103(3A):1S-2S.
78. Kawas C, Resnick S, Morrison A, et al. A prospective study of
estrogen replacement therapy and the risk of developing Alzhei-
mer’s disease: the Baltimore longitudinal study of aging. Neurol-
ogy. 1997;48(6):1517-1521.
79. Polo-Kantola P, Portin R, Polo O, Helenius H, Irjala K, Erkkola R.
The effect of short-term estrogen replacement therapy on cogni-
tion: a randomized, double blind, cross-over trial in postmeno-
pausal women. Obstet Gynecol. 1998;91(3):449-466.
10 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

80. Jacobs DM, Tang MX, Stern Y, et al. Cognitive function in non-
demented older women who took estrogen after menopause. Neu-
rology. 1998;50(2):368-373.
81. Rissanen A, Puolivali J, van Groen T, Riekkinen P. In mice tonic
estrogen replacement therapy improves non-spatial and spatial
memory in a water maze task. Neuroreport. 1999;10(6):
1369-1372.
82. Bimonte HA, Denenberg VH. Estradiol facilitates performance as
working memory load increases. Psychoneuroendocrinology.
1999;24(2):161-173.
83. Petanceska SS, Nagy V, Frail D, Gandy S. Ovariectomy and
17beta-estradiol modulate the levels of Alzheimer’s amyloid beta
peptides in brain. Exp Gerontol. 2000;35(9-10):1317-1325.
84. Monk D, Brodaty H. Use of estrogens for the prevention and
treatment of Alzheimer’s disease. Dement Geriatr Cogn Disord.
2000;11(1):1-10.
85. Green PS, Simpkins JW. Estrogens and estrogen-like non-
feminizing compounds. Their role in the prevention and treatment
of Alzheimer’s disease. Ann N Y Acad Sci. 2000;924:93-98.
86. Manly JJ, Merchant CA, Jacobs DM, et al. Endogenous estrogen
levels and Alzheimer’s disease among postmenopausal women.
Neurology. 2000;54(4):833-837.
87. Henderson VW, Paganini-Hill A, Miller BL, et al. Estrogen for
Alzheimer’s disease in women: randomized, double-blind,
placebo-controlled trial. Neurology. 2000;54(2):295-301.
88. Mulnard RA. Estrogen as a treatment for Alzheimer disease. J Am
Med Assoc. 2000;284(20):307-308.
89. Mulnard RA, Cotman CW, Kawas C, et al. Estrogen replacement
therapy for treatment of mild to moderate Alzheimer disease: a
randomized controlled trial. Alzheimer’s Disease Cooperative
Study. JAMA. 2000;283(8):1007-1015.
90. Birge SK, McEwen BS, Wise PM. Effects of estrogen deficiency
on brain function. Implications for the treatment of postmenopau-
sal women. Postgrad Med Spec. 2001;(spec no):11-16.
91. Zandi PP, Carlson MC, Plassman BL, et al. Hormone replacement
therapy and incidence of Alzheimer disease in older women.
JAMA. 2002;288(17):2123-2129.
92. Sherwin BB. Estrogen and cognitive functioning in women.
Endocr Rev. 2003;24(2):133-151.
93. Henderson VW, Guthrie JR, Dudley EC, Burger HG, Dennerstein
L. Estrogen exposures and memory at midlife: a population-based
study of women. Neurology. 2003;60(8):1369-1371.
94. Sherwin BB. Surgical menopause, estrogen and cognitive func-
tion in women: what do the findings tell us? Ann N Y Acad Sci.
2005;1052:133-151.
95. Yue X, Lu M, Lancaster T, et al. Brain estrogen deficiency accel-
erates Abeta plaque formation in an Alzheimer’s disease animal
model. Proc Natl Acad Sci U S A. 2005;102(52):19198-19203.
96. Simpkins JW, Yang SH, Wen Y, Singh M. Estrogens, progestins,
menopause and neurodegeneration: basic and clinical studies.
Cell Mol Life Sci. 2005;62(3):271-280.
97. Almeida OP, Lautenschlager NT, Vasikaran S, Leedman P, Gela-
vis A, Flicker L. A 20-week randomized controlled trial of estra-
diol replacement therapy for women aged 70 years and older:
effect on mood, cognition and quality of life. Neurobiol Aging.
2006;27(1):141-149.
98. Henderson VW.Cognitive changes after menopause: influence
of estrogen. Clin Obstet Gynecol. 2008;51(3):618-626.
99. Hogervorst E. Effects of gonadal hormones on cognitive beha-
vior in elderly men and women. J Neuroendocrinol. 2013;
25(11):1182-1195.
100. Casadesus G, Garrett MR, Webber KM, et al. The estrogen myth:
potential use of gonadotropin-releasing hormone agonists for the
treatment of Alzheimer’s disease. Drugs R D. 2006;7(3):187-193.
101. Simpkins JW, Green BS, Gridley KE, Singh M, de Fiebre NC,
Rajakumar G. Role of estrogen replacement therapy in memory
enhancement and the prevention of neuronal loss associated with
Alzheimer disease. Am J Med. 1997;103(3A):19s-25s.
102. Sansdstrom NJ, Williams CL. Memory retention is modulated
by acute estradiol and progesterone replacement. Behav Neu-
rosci. 2001;115(2):384-393.
103. Rapp SR, Espeland MA, Shumaker SA, et al. Effect of estrogen
plus progestin on global cognitive function in postmenopausal
women. JAMA. 2003;289(20):2663-2672.
104. Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus proges-
tin and the incidence of dementia and mild cognitive impairment
in postmenopausal women: the Women’s Health Initiative
Memory Study: a randomized controlled trial. JAMA. 2003;
289(20):2651-2662.
105. Seshadri S, Zornberg GL, Derby LE, Myers MW, Jick H, Drach-
man DA. Postmenopausal estrogen replacement therapy and the
risk of Alzheimer disease. Arch Neurol. 2001;58(3):435-440.
106. Daniel JM, Hulst JL, Berbling JL. Estradiol replacement
enhances working memory in middle-aged rats when initiated
immediately after ovariectomy but not after a long-term period
of ovarian hormone deprivation. Endocrinology. 2006;147(1):
607-614.
107. Bohacek J, Daniel JM. The beneficial effects of estradiol on
attentional processes are dependent on timing of treatment initia-
tion following ovariectomy in middle-aged rats. Psychoneuroen-
docrinology. 2010;35(5):694-705.
108. Chakravarti S, Collins WP, Forecast JD, Newton JR, Oram DH,
Studd JW. Hormonal profiles after the menopause. Br Med J.
1976;2(6039):784-787.
109. Rossmanith WG, Reichelt C, Scherbaum WA. Neuroendocrinol-
ogy of aging in humans: attenuated sensitivity to sex steroid
feedback in elderly postmenopausal women. Neuroendocrinol-
ogy. 1994;59(4):355-362.
110. Chu C, Gao G, Huang W. A study on co-localization of FSH and
its receptor in rat hippocampus. J Mol Hist. 2008;39(1):49-55.
111. Payami H, Montee K, Grimslid H, Shattuc S, Kaye J. Increased
risk of familial late-onset Alzheimer’s disease in women. Neu-
rology. 1996;46(1):126-129.
112. Bowen RL, Isley JP, Atkinson RL. An association of elevated
serum gonadotropin concentrations and Alzheimer disease?
J Neuroendocrinol. 2000;12(4):351-354.
113. Short RA, O’Brien PC, Graff-Radford NR, Bowen RL. Elevated
gonadotropin levels in patients with Alzheimer disease. Mayo
Clin Proc. 2001;76(9):906-909.
114. Barron AM, Cake M, Verdile RN. Ovariectomy and 17beta-
estradiol replacement do not alter beta-amyloid levels in sheep
brain. Endocrinology. 2009;150(7):3228-3236.
Rao 11
by guest on July 20, 2016rsx.sagepub.comDownloaded from

115. Bryan KJ, Mudd JC, Richardson SL, et al. Down-regulation of
serum gonadotropins is as effective as estrogen replacement at
improving menopause-associated cognitive deficits. J Neuro-
chem. 2010;112(4):870-881.
116. Casadesus G, Webber KM, Atwood CS, et al. Luteinizing hor-
mone modulates cognition and amyloid-b deposition in Alzhei-
mer APP transgenic mice. Biochem Biophys Acta. 2006;1762(4):
447-452.
117. Ziegler SG, Thornton JW. Low luteinizing hormone enhances
spatial memory and has protective effects on memory loss in
rats. Horm Behav. 2010;58(5):705-713.
118. Blair JA, Bjatta S, McGee H, Casadesus G. Luteinizing hor-
mone: evidence for direct action in the CNS. Horm Behav.
2015;76:57-62.
119. Palm R, Chang J, Blair J, et al. Down-regulation of serum gona-
dotropins but not estrogen replacement improves cognition in
aged-ovariectomized 3xTg AD female mice. J Neurochem.
2014;130(1):115-125.
120. Casadesus G, Milliken EL, Webber KM, et al. Increases in lutei-
nizing hormone are associated with declines in cognitive perfor-
mance. Mol Cell Endocrinol. 2007;269(1-2):107-111.
121. Bowen RL, Smith MA, Harris PLR, et al. Elevated luteinizing
hormone expression colocalizes with neurons vulnerable to Alz-
heimer’s disease pathology. J Neurosci Res. 2002;70(3):
514-518.
122. Barron A, Verdile G, Martins RN. The role of gonadotropins in
Alzheimer’s disease: potential neurodegenerative mechanisms.
Endocrine. 2006;29(2):257-270.
123. Rodrigues MA, Verdile G, Foster JK, et al. Gonadotropins and
cognition in older women. J Alzheimers Dis. 2008;13(3):
267-274.
124. Burnham VL, Thornton JE. Luteinizing hormone as a key player
in the cognitive decline of Alzheimer’s disease. Horm Behav.
2015;76:48-56.
125. Wahjoepramono EJ, Wijaya LK, Taddei K, et al. Direct expo-
sure of guinea pig CNS to human luteinizing hormone increases
cerebrospinal fluid and cerebral beta amyloid levels. Neuroen-
docrinol. 2011;94(4):313-322.
126. Berry A, Tomidokoro Y, Ghiso J, Thornton J. Human chorionic
gonadotropin (a luteinizing hormone homologue) decreases spa-
tial memory and increases brain amyloid-b levels in male rats.
Horm Behav. 2008;54(1):143-152.
127. Barron AM, Verdile G, Taddei K, Bates KA, Martins RN. Effect
of chronic hCG administration on Alzheimer’s-related cognition
and Ab accumulation in PS1KI mice. Endocrinology. 2010;
151(11):5380-5388.
128. Lin J, Li X, Yuan F, et al. Genetic ablation of luteinizing hor-
mone receptor improves the amyloid pathology in a mouse
model of Alzheimer disease. J Neuropathol Exp Neurol. 2010;
69(3):253-261.
129. Masters CL, Simms G, Weinman NA, Multhaup G, McDonald
BL, Beyreuther K. Amyloid plaque core protein in Alzheimer
disease and Down syndrome. Proc Natl Acad Sci U S A. 1985;
82(12):4245-4249.
130. Takashima S, Kuruta H, Mito T, Nishizawa M, Kunishita T,
Tabira T. Developmental and aging changes in the expression
patterns of beta-amyloid in the brains of normal and Down syn-
drome cases. Brain. 1990;12(4):367-371.
131. Schupf N, Kapell D, Nightingale B, Rodriguez A, Tycko B,
Mayeux R. Earlier onset of Alzheimer’s disease in men with
Down syndrome. Neurology. 1998;50(4):991-995.
132. Nakano R, Shina K, Yarnoto M, Kobayashi M, Nishimori K,
Hiraoka JI. Binding sites for gonadotropins in human postme-
nopausal ovaries. Obstet Gynecol. 1989;73:196-200.
133. Pabon J, Li X, Lei Z, Sanfilippo J, Yussman M, Rao CV. Novel
presence of luteinizing hormone/chorionic gonadotropin recep-
tors in human adrenal glands. J Clin Endocrinol Metab. 1996;
81(2):2397-2400.
134. Dos Santo E, Dieudonne M-N, Leneveu M-C, Pacquery R, Ser-
azin V, Giudicelli Y. In vitro effects of chorionic gonadotropin
hormone on human adipose development. J Endocrinol. 2007;
194(2):313-325.
135. Parkash J, Lei ZM, Rao CV. The presence of human chorionic
gonadotropin/luteinizing hormone receptors in pacreatic beta-
cells. Reprod Sci. 2015;22(8):1000-1007.
136. Lasley BL, Conley AJ, Morrison JH, Gee NA, Rao CV. Identi-
fication of immunoreactive luteinizing hormone receptors in the
adrenal cortex of the female rhesus macaque. Reprod Sci. 2016;
23(4):524-530.
137. Poliak A, Jones GES, Goldberg B, Soloman D, Woodruff ID.
Effect of human chorionic gonadotropin on postmenopausal
women. Am J Obstet Gynecol. 1968;101:731-739.
138. Dennefors BL, Janson PO, Knutson F, Hamberger L. Steroid
production and responsiveness to gonadotropin in isolated stro-
mal tissue of human postmenopausal ovaries. Am J Obstet Gyne-
col. 1980;136(4):997-1002.
139. Rao CV, Zhou XL, Lei ZM. Functional luteinizing hormone/
chorionic gonadotropin receptors in human adrenal cortical
H295R cells. Biol Reprod. 2004;71(2):579-587.
140. Moran F, Chen J, Lohstroh PN, Gee NA, Lasley BL.
Dehydroepiandrosterone sulfate (DHEAS) levels reflect
endogenous LH production and response to human chor-
ionic gonadotropin (hCG) challenge in the older female
macaque (Macaca fascicularis). Menopause. 2013;20(3):
329-335.
141. Saxena AR, Seely. Luteinizing hormone correlates with adrenal
function in postmenopausal women. Menopause. 2012;19(11):
1280-1283.
142. Cuatrecasas P. Insulin-receptor interactions in adipose tissue
cells: direct measurement and properties. Proc Natl Acad Sci
U S A. 1971;68(6):1264-1268.
143. Schindler AE, Ebert A, Friedrich E. Conversion of androstene-
dione to estrone by human fat tissue. J Clin Endocr Metab. 1972;
35(4):627-630.
144. Ackerman GE, Smoth ME, Mendelson CR, MacDonald PC,
Simpson ER. Aromatization of androstenedione by human adi-
pose tissue stromal cells in monolayer culture. J Clin Endocrinol
Metab. 1981;53(2):412-417.
145. Nagamani M, Hannigan EV, Dinh VT, Stuart CA. Hyperinsuli-
nemia and stromal luteinizing of the ovaries in postmenopausal
women with endometrial cancer. J Clin Endocrinol Metab.
1988;67(1):144-148.
12 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from

146. Urban RJ, Veldhuis JD, Dufau LM. Estrogen regulates the
gonadotropin-releasing hormone-stimulated secretion of biolo-
gically active luteinizing hormone. J Clin Endocrinol Metab.
1991;72(3):660-668.
147. McTernan PG, Anderson LA, Anwar AJ, et al. Glucocorticoid
regulation of P450 aromatase activity in human adipose tissue:
gender and site differences. J Clin Endocrinol Metab. 2002;
87(3):1327-1336.
148. Barnard L, Balen AH, Ferriday D, Tiplady B, Dye L. Cognitive
functioning in polycystic ovary syndrome. Psychoneuroendocri-
nology. 2007;32(8-10):906-914.
149. Hart R, Doherty DA. The potential implications of a PCOS
diagnosis on a woman’s long-term health using data linkage. J
Clin Endocrinol Metab. 2015;100(3):911-919.
150. Rees DA, Udiawar M, Berlot R, Jones DK, O’Sullivan MJ.
White matter microstructure and cognitive function in young
women with polycystic ovary syndrome. J Clin Endocrinol
Metab. 2016;101(1):314-323.
151. The Translational Scientist. Navigating the complexities of Alz-
heimer’s. 2016. https://thetranslationalscientist.com/issues/
0116/navigating-alzheimers/. Accessed March 2016.
152. Croxatto H, Arrau J, Croxatto H. Luteinizing hormone-like
activity in human median eminence extracts. Nature. 1964;
204:584-585.
153. Antunes JL, Carmel PW, Zimmerman EA, Ferin M. The pars
tuberalis of the rhesus monkey secretes luteinizing hormone.
Brain Res. 1979;166(1):49-55.
154. Gross DS, Page RB. Luteinizing hormone and follicle-
stimulating hormone production in the pars tuberalis of hypo-
physectomized rats. Am J Anat. 1979;156(2):285-291.
155. Hostetter G, Gallo RV, Brownfield MS. Presence of immunor-
eactive luteinizing hormone in the rat forebrain. Neuroendocri-
nology. 1981;33(4):241-245.
156. Emanuele N, Connick E, Howell T, et al. Hypothalamic luteiniz-
ing hormone (LH): characteristics and response to hypophysect-
omy. Biol Reprod. 1981;25(2):321-326.
157. Emanuele N, Oslapas R, Connick E, Kirsteins L, Lawrence AM.
Hypothalamic LH may play a role in control of pituitary LH
release. Neuroendocrinology. 1981;33(1):12-17.
158. Emanuele N, Anderson J, Andersen E, et al. Extrahypothalamic
brain luteinizing hormone: characterization by radioimmunoas-
say, chromatography, radioligand assay and bioassay. Neuroen-
docrinology. 1983;36(4):254-260.
159. Weill-Engerer S, David JP, Sazdovitch V, et al. Neurosteroid
quantification in human brain regions: comparison between Alz-
heimer’s and nondemented patients. J Clin Endocrinol Metab.
2002;87(11):5138-5143.
160. Murakami G, Tanabe N, Ishii HT, et al. Role of cytochrome
p450 in synaptocrinology: endogenous estrogen synthesis in the
brain hippocampus. Drug Metab Rev. 2006;38(3):353-369.
161. Neaves WB, Johnson L, Porter JC, Parker CR, Petty CS. Leydig
cell numbers, daily sperm production, and serum gonadotropin
levels in aging men. J Clin Endocrinol Metab. 1984;59(4):756-763.
162. Butchart J, birch B, basil R, Wolfe L, Holmes C. Male sex
hormones and systematic inflammation in Alzheimer disease.
Alzheimer Dis Assoc Disord. 2013;27(2):153-156.
163. Tenover JS, Matsumoto AM, Plymate SR, Bremmer WJ. The
effects of aging in normal men on bioavailable testosterone and
luteinizing hormone secretion: response to clomiphene citrate.
J Clin Endocrinol Metab. 1987;65(6):1118-1126.
164. Morley JE, Kaiser FE, Perry HM, et al. Longitudinal changes in
testosterone, luteinizing hormone, and follicle-stimulating hor-
mone in healthy older men. Metab Clin Exp. 1997;46(4):
410-413.
165. Morley JE. Androgens and aging. Maturitas. 2001;38(1):61-71;
discussion 71-73.
166. Kaufman JM, Vermeulen A. The decline of androgen levels in
elderly men and its clinical and therapeutic implications. Endocr
Rev. 2005;26(6):833-876.
167. Yeap BB, Almeida OP, Hyde Z, et al. In men older than 70 years,
total testosterone remains stable while free testosterone declines
with age. The Health in Men Study. Eur J Endocrinol. 2007;
156(5):585-594.
168. Veldhuis JD, Keenan DM, Liu PY, Iranmanesh A, Takahashi
PY, Nehra AX. The aging male hypothalamic-pituitary-gonadal
axis: pulsatility and feedback. Mol Cell Endocrinol. 2009;
299(1):14-22.
169. Wang J, Tanila H, Puolivali J, Kadish I, van Groen T. Gender
differences in the amount and deposition of amyloid beta in
APPswe and PS1 double transgenic mice. Neurobiol Dis.
2003;14(3):318-327.
170. Barrett-Connor E, Goodman-Gruen D, Patay B. Endogenous sex
hormones and cognitive function in older men. J Clin Endocri-
nol Metab. 1999;84(10):3681-3685.
171. Gillet MJ, Martins RN, Clarnette RM, Chubb SA, Bruce DG,
Yeap BB. Relationship between testosterone, sex hormone bind-
ing globulin and plasma amyloid beta peptide 40 in older men
with subjective memory loss or dementia. J Alzheimers Dis.
2003;5(4):267-269.
172. Hogervorst E, Combrinck M, Smith AD. Testosterone and gona-
dotropin levels in men with dementia. Neuro Endocrinol Lett.
2003;24(3-4):203-208.
173. Janowsky JS. The role of androgens in cognition and brain aging
in men. Neuroscience. 2006;138(3):1015-1020.
174. Rosario ER, Pike CJ. Androgen regulation of beta-amyloid pro-
tein and the risk of Alzheimer’s disease. Brain Res. 2008;57(2);
444-453.
175. McConnell SEA, Alla J, Wheat E, Romeo RD, McEwen B,
Thornton JE. The role of testicular hormones and luteinizing
hormone in spatial memory in adult male rats. Horm Behav.
2012;61(4):479-486.
176. Rosario ER, Carrol JC, Pike CJ. Evaluation of the effects of
testosterone and luteinizing hormone on regulation of b-amyloid
in male 3xTg-AD mice. Brain Res. 2012;1466:137-145.
177. Verdile G, Laws SM, Henley D, et al. Associations between
gonadotropins, testosterone and b amyloid in men at risk of
Alzheimer’s Disease. Mol Psych. 2014;19(1):69-75.
178. Verdile G, Yeap BB, Clamette RM, et al. Luteinizing hormone
levels are positively correlated with plasma amyloid-b protein
levels in elderly men. J Alzheimers Dis. 2008;14(2):201-208.
179. Haasl RJ, Ahmadi MR, Meethal SV, et al. A luteinizing hormone
receptor intronic variant is significantly associated with
Rao 13
by guest on July 20, 2016rsx.sagepub.comDownloaded from

decreased risk of Alzheimer’s disease in males carrying on apo-
lipoprotein E epsilon 4 allele. BMC Med Genet. 2008;9:37.
180. D’Amico AV, Braccioforte MH, Moran BJ, Chen MH.
Luteinizing-hormone releasing hormone therapy and the risk
of death from Alzheimer disease. Alzheimer Dis Assoc Disord.
2010;24(1):85-89.
181. Leranth C, Petnehazy O, MaclUsky NJ. Gonadal hormones
affect spine synaptic density in the CA1 hippocampal subfield
of male rats. J Neurosci. 2003;23(5):1588-1592.
182. Hogervorst E, Williams J, Budge M, Barnetson L, Combrinck
M, Smith AD. Serum total testosterone is lower in men with
Alzheimer’s disease. Neuro Endocrinol Lett. 2001;22(3):
163-168.
183. Hogervorst E, Bandelow S, Combrinck M, Smith AD. Low free
testosterone is an independent risk factor for Alzheimers disease.
Exp Gerontol. 2004;39(11-12):1633-1639.
184. Rosario ER, Chang L, Stanczyk FZ, Pike CJ. Age related tes-
tosterone depletion and the development of Alzheimer disease.
J Am Med Assoc. 2004;292(12):1431-1432.
185. Tan RS, Pu SJ. A pilot study on the effects of testosterone in
hypogonadal aging male patients with Alzheimer’s disease.
Aging Male. 2003;6(1):13-17.
186. Gandy S, Almeida OP, Fonte J, et al. Chemical andropause and
amyloid-beta peptide. JAMA. 2001;285(17):2195-2196.
187. Almeida OP, Waterreus A, Spry N, Flicker L, Martins RN. One
year follow-up study of the association between chemical cas-
tration, sex hormones, beta-amyloid, memory and depression in
men. Psychoneuroendocrinology. 2003;29(8):1071-1081.
188. Nead KT, Gaskin G, Chester C, Swisher-McClure S, Leeper NJ,
Shah NH. Androgen deprivation therapy and future Alzheimer’s
disease risk. J Clin Oncol. 2016;34(6):533-571.
189. Ahlbom E, Prins GS, Ceccatelli S. Testosterone protects cere-
bellar granule cells from oxidative stress-induced cell death
through a receptor mediated mechanism. Brain Res. 2001;
892(2):255-262.
190. Wahjoepramono EJ, Wijaya LK, Taddei K, et al. Distinct effects
of testosterone on plasma and cerebrospinal fluid amyloid-beta
levels. J Alzheimers Dis. 2008;15(1):129-137.
191. Moffat SD, Zonderman AB, Metter EJ, et al. Free testosterone
and risk of Alzheimer disease in older men. Neurology. 2004;
62(2):188-193.
192. Pike CJ. Testosterone attenuates beta-amyloid toxicity in cul-
tured hippocampal neurons. Brain Res. 2001;919(1):160-165.
193. Hammond J, Le Q, Goodyer C, Gelfand M, Trifiro M, LeBlanc
A. Testosterone-mediated neuroprotection through the androgen
receptor in human primary neurons. J Neurochem. 2001;77(5):
1319-1326.
194. Rosario ER, Carroll JC, Oddo S, LaFerla FM, Pike CJ. Andro-
gens regulate the development of neuropathology in a triple
transgenic mouse model of Alzheimer’s disease. J Neurosci.
2006;26(51):13384-13389.
195. Rosario ER, Carroll J, Pike CJ. Testosterone regulation of
Alzheimer-like neuropathology in male 3xTg-AS mice involves
both estrogen and androgen pathways. Brain Res. 2010;1359:
281-290.
196. McAllilster C, Long J, Bowers A, et al. Genetic targeting aro-
matase in male amyloid precursor protein transgenic mice down-
regulates beta-secretase (BACE1) and prevents Alzheimer-like
pathology and cognitive impairment. J Neurosci. 2010;30(21):
7326-7334.
197. Walsch JP, Kitchens AC. Testosterone therapy and cardiovascu-
lar risk. Trends Cardiovasc Med. 2015;25(3):250-257.
198. Alzheimer’s Association. FDA-approved treatments for Alz-
heimer’s. Web site. http://www.alz.org/dementia/downloads/
topicsheet_treatments.pdf. Accessed March 2016. Updated
February 2016.
199. Gallagher M. The overactive brain. Translational Sci. 2016;1:
23.
200. Bakker A, Krauss GL, Albert MS, et al. Reduction of hippocam-
pal hyperactivity improves cognition in amnestic mild cognitive
impairment. Neuron. 2016;74(3):467-474.
201. Defelice FG, Ferreira ST. Physiopathological modulators of
amyloid aggregation and novel pharmacological approaches in
Alzheimer’s disease. Anais da Academia Brasileira de Ciencias.
2002;74(2):265-284.
202. Verdile G, Fuller SJ, Martins RN. The role of type 2 diabetes in
neurodegeneration. Neurobiol Dis. 2015;84:22-38.
203. McNay E. Food for thought. Translational Sci. 2016;1:24-25.
204. Havrankova J, Roth J, Brownstein MJ. Concentrations of insulin
and insulin receptors in the brain are independent of peripheral
insulin levels. Studies of obese and streptozotocin-treated
rodents. J Clin Invest. 1979;64(2):636-642.
205. Blazquez E, Velazquez E, Hurtado-Carneiro V, Ruiz-Albusac
JM. Insulin in the brain: its pathophysiological implications for
states related with central insulin resistance, type 2 diabetes and
Alzheimer’s disease. Front Endocrinol. 2014;5:161.
206. Havrankova J, Schmechel D, Roth J, Brownstein M. Identifica-
tion of insulin in rat brain. Proc Natl Acad Sci U S A. 1978;
75(11):5737-5741.
207. Havrankova J, Roth J, Brownstein M. Insulin receptors are
widely distributed in the central nervous system of the rat.
Nature. 1978;272(5656):827-829.
208. Antigonadotropin-Leuprolide in Alzheimer’s Disease Drug
Investigation (ALADDIN) VP 104 Study. Web site. http://
www.clinicaltrials.gov/ct/show/NTC00076440. Accessed
February 22, 2016.
209. Bowen RL, Perry G, Xiong C, Smith MA, Atwood CS. A
clinical study of Lupron depot in the treatment of women with
Alzheimer’s disease: preservation of cognitive function in
patients taking an acetylcholinesterase inhibitor and treated
with high dose Lupron over 48 weeks. J Alzheimers Dis.
2015;44(2):549-560. Updated December 2009.
14 Reproductive Sciences
by guest on July 20, 2016rsx.sagepub.comDownloaded from