Reporters: JI Tabajonda, Jennifer M. JI Vio, Rachel Louise S.
102
Reporters: JI Tabajonda, Jennifer M. JI Vio, Rachel Louise S.
-
Upload
jeffrey-norton -
Category
Documents
-
view
223 -
download
0
Transcript of Reporters: JI Tabajonda, Jennifer M. JI Vio, Rachel Louise S.

Reporters:JI Tabajonda, Jennifer M.JI Vio, Rachel Louise S.
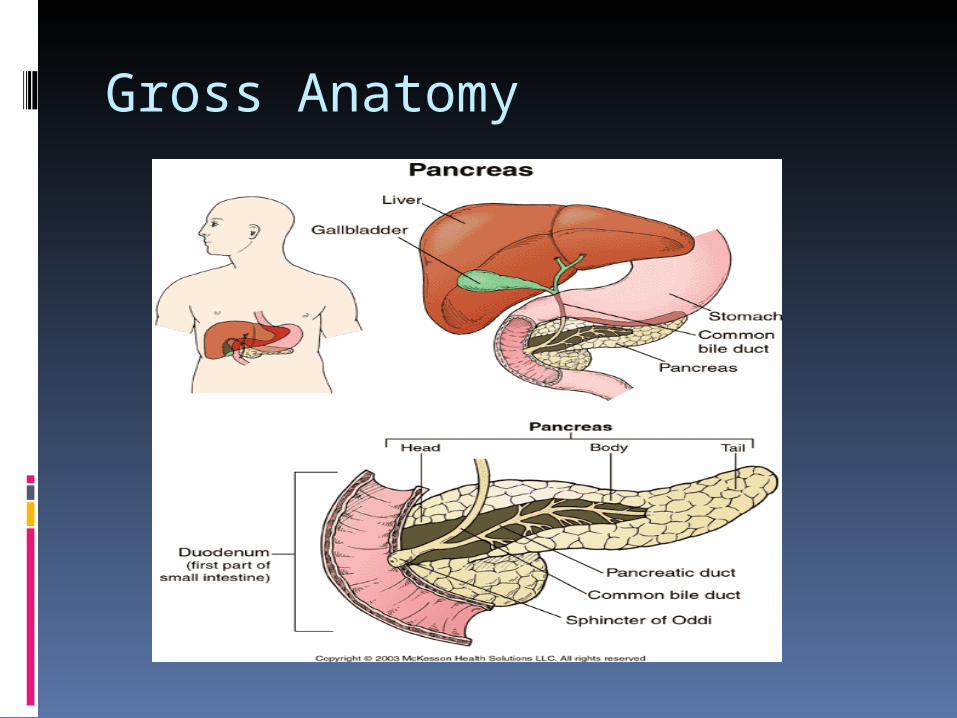
Gross Anatomy

Microscopic Anatomy
Physiology
Glucagon single-chain polypeptide that contains
29 amino acid residues and has a molecular weight of 3483
increases blood glucose and relaxes smooth muscle of the gastrointestinal tract.
potent stimulator of hepatic glycogenolysis, gluconeogenesis, and ketogenesis
Insulin
Preproinsulin (86 aa)
proteolytic processing
Proinsulin
site specific peptide cleavage
C-peptide Insulin
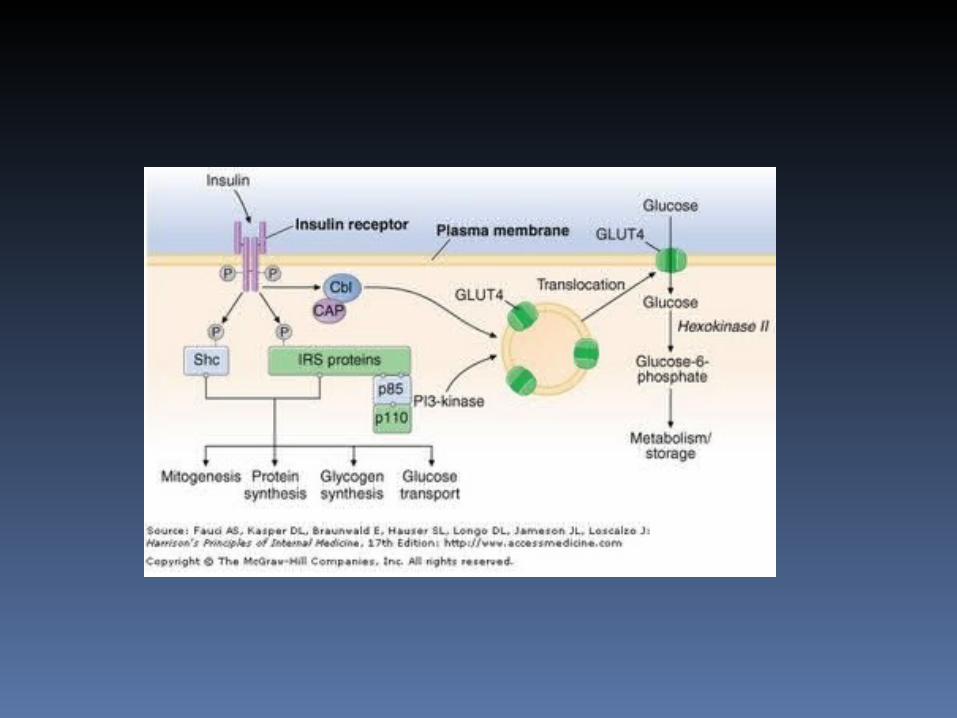

Effects of Insulin
Liver Adipose Muscle
Increased by insulin
FA synthesisGlycogen synthesisCHON synthesis
Glucose uptakeFA synthesis
FA synthesisGlycogen synthesisCHON synthesis
Decreased by insulin
KetogenesisGluconeogenesis
Lipolysis
Increased by glucagon
GlycogenolysisGluconeogenesisKetogenesis
Lipolysis
Diabetes Mellitus
Refers to a group of metabolic disorders that share the phenotype of hyperglycemia
With several distinct types Interaction of genetics and
environment Reduced Insulin secretion Decreased glucose utilization Increased glucose production

Classic Symptoms of Diabetes Polyuria Polydipsia Unexplained weight loss

Levels of Glycemia
Normal Pre- Diabetes
(IFG and IGT)
Diabetes Mellitus
FPG <100 mg/dl
(5.5 mmol/L)
100-125 mg/dL
(5.5-6.9 mmol/L)
> 126 mg/dL
(7.0 mmol/L)
2 hour PG < 140 mg/dL
(7.8 mmol/L)
140- 199 mg/dL
(7.8-11.0 mmol/L)
> 200 mg/dL
(11.1 mmol/L)

Criteria for the Dx of DM Fasting Plasma Glucose (FPG) ≥126 mg/dl (7.0 mmol/L) - Must be repeated on a separate day to
confirm diagnosis OR Postprandial Plasma Glucose (2h PG) ≥200 mg/dl (11.1 mmol/L) -Measured with Oral Glucose Tolerance
Test (OGTT) -Must be repeated on a separate days to
confirm diagnosis OR

Classic Symptoms + Casual Plasma Glucose (CPG) > 200 mg/dl (> 11.1 mmol/L).
-Considered diagnostic of diabetes but should be confirmed on a separate day with FPG or 2hPG.
- Casual plasma glucose ( plasma glucose taken without regard to the last meal)
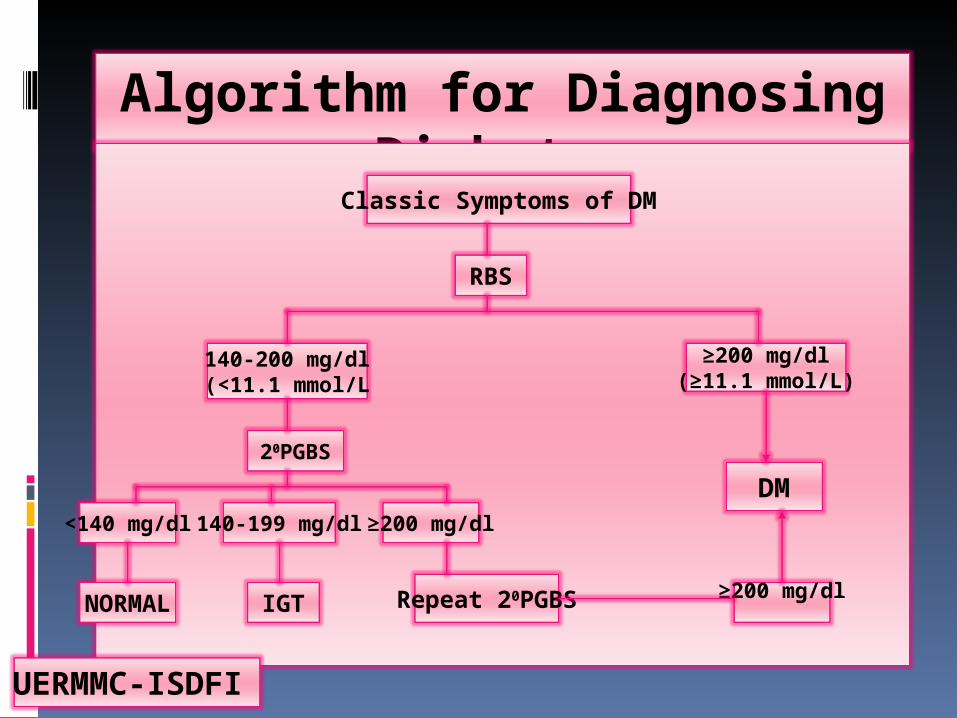
Algorithm for Diagnosing Diabetes
Classic Symptoms of DM
RBS
140-200 mg/dl(<11.1 mmol/L
≥200 mg/dl(≥11.1 mmol/L)
20PGBS
<140 mg/dl140-199 mg/dl≥200 mg/dl
NORMAL IGT Repeat 20PGBS ≥200 mg/dl
DM
UERMMC-ISDFI
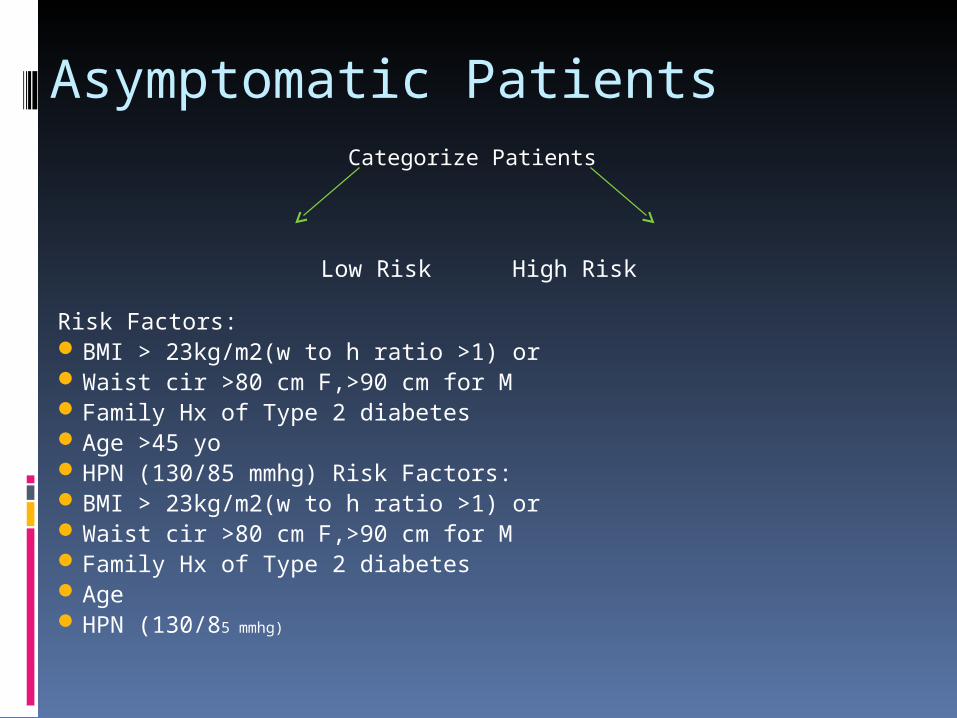
Asymptomatic PatientsCategorize Patients
Low Risk High Risk
Risk Factors:BMI > 23kg/m2(w to h ratio >1) orWaist cir >80 cm F,>90 cm for MFamily Hx of Type 2 diabetesAge >45 yoHPN (130/85 mmhg) Risk Factors:BMI > 23kg/m2(w to h ratio >1) orWaist cir >80 cm F,>90 cm for MFamily Hx of Type 2 diabetesAgeHPN (130/85 mmhg)
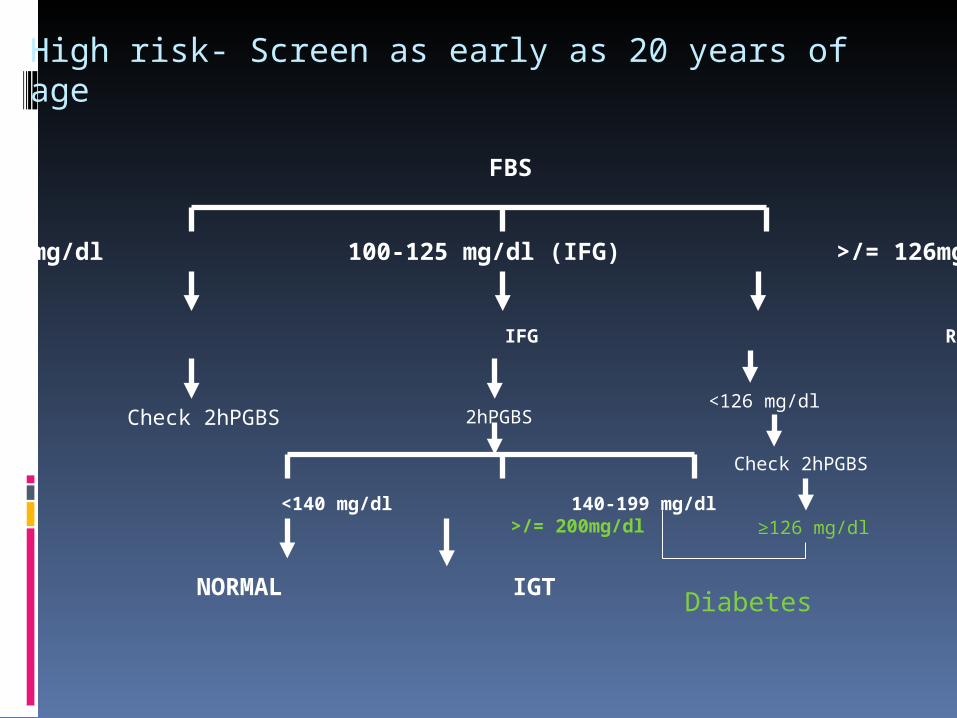
High risk- Screen as early as 20 years of age
FBS
<100 mg/dl 100-125 mg/dl (IFG) >/= 126mg/dl
NORMAL IFG Rpt FBS
<140 mg/dl 140-199 mg/dl >/= 200mg/dl
NORMAL IGT
Check 2hPGBS 2hPGBS<126 mg/dl
Check 2hPGBS
≥126 mg/dl
Diabetes

Classification
Type 1 Complete or near total insulin deficiency
Type 2 Insulin resistance impaired insulin secretion Increased glucose production Preceded by IFG and IGT
DM Type 3 and 4
DM type 3 Other specific types of Diabetes
DM type 4 Gestational Diabetes Mellitus
Pathophysiology
DM Type I Complete or near total insulin deficiency
circulating insulin is very low or absent plasma glucagon and the pancreatic beta cells fail to
respond to all insulin-secretory stimuli.
Pathophysiology of DM Type I
Autoimmune islet cell antibodies anti-insulin antibodies genetic susceptibility
HLA markers Infectious and/or environmental agents ?
viruses (eg, mumps, rubella, Coxsackie B4), toxic chemicals, exposure to cow's milk in infancy, and cytotoxins

Dm Type 2
Predominantly insulin resistance with relative insulin deficiency to predominantly insulin deficiency with insulin resistance
Excessive hepatic glucose production Abnormal fat metabolism
*Insulin resistance, is the decreased ability of insulin to act effectively on target tissues (especially muscle, liver, and fat)

GDM
Any degree of glucose intolerance with the onset or first recognition during pregnancy
Does not exclude the possibility that undiagnosed glucose intolerance may have occurred prior to pregnancy
Usually 24-48 weeks

Pathophysiology
Placental hormones causing insulin resistance Estrogen, progesterone, cortisol, HPL
Decreased insulin secretion Borderline pancreatic function, cannot
produce insulin levels to meet metabolic needs
Pre-Diabetes
Impaired Fasting glucose FBS of 100-125 mg/dL
IGT 2HPGBS 140-199 mg/dL
Associated with the metabolic syndrome, which includes obesity (especially abdominal or visceral obesity), dyslipidemia of the high-triglyceride and/or low-HDL type, and hypertension.
Complications of Diabetes Mellitus
ACUTEDiabetic Ketoacidosis (DKA)Hyperglycemic Hyperosmolar State (HHS)
CHRONIC:Macrovascular (CAD,CVD,PVD)Microvascular (retinopathy, nephropathy,
neuropathy)Others (e.g. GI, GU, Dermatologic, Infectious)

Acute Complications of DMDKA and HHS are medical
emergencies
associated with potentially serious complications if not promptly diagnosed and treated.
associated with absolute or relative insulin deficiency, volume depletion, and acid-base abnormalities.
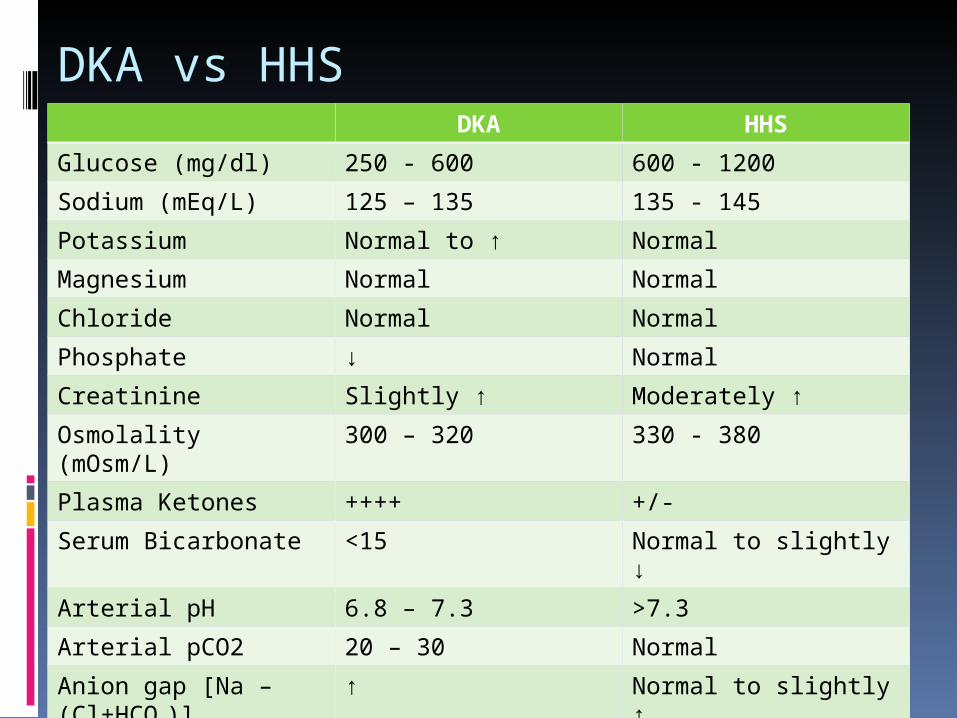
DKA vs HHSDKA HHS
Glucose (mg/dl) 250 - 600 600 - 1200
Sodium (mEq/L) 125 – 135 135 - 145
Potassium Normal to ↑ Normal
Magnesium Normal Normal
Chloride Normal Normal
Phosphate ↓ Normal
Creatinine Slightly ↑ Moderately ↑
Osmolality (mOsm/L) 300 – 320 330 - 380
Plasma Ketones ++++ +/-
Serum Bicarbonate <15 Normal to slightly ↓
Arterial pH 6.8 – 7.3 >7.3
Arterial pCO2 20 – 30 Normal
Anion gap [Na – (Cl+HCO3)]
↑ Normal to slightly ↑
DKA
Can occur in both type 1 and type 2 DM Signs & symptoms develop over 24hrs results from relative or absolute insulin
deficiency combined with counterregulatory hormone excess

DKA
Diagnostic Criteria:
Glucose >250mg/dl pH <7.3 High anion gap Positive ketones

Clinical Features of DKA
Precipitating events: Inadequate insulin administration Infection Infarction Drugs Pregnancy
Clinical Features of DKA
Symptoms: Nausea / vomiting Thirst / polyuria Abdominal pain Shortness of breath
Clinical Features of DKA
Physical Findings: Tachycardia Dehydration / Hypotension Tachypnea / Kussmaul respirations/
respiratory distress Abdominal tenderness (may
resemble acute pancreatitis or surgical abdomen)
Lethargy / obtundation / cerebral edema/ possibly coma
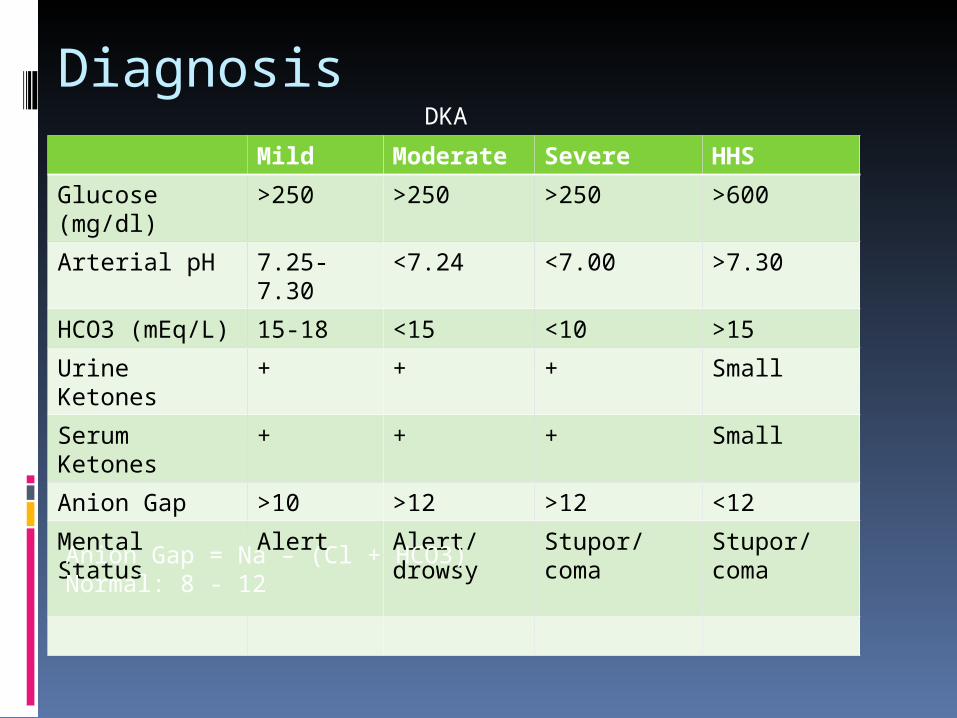
Diagnosis
Mild Moderate Severe HHS
Glucose (mg/dl)
>250 >250 >250 >600
Arterial pH 7.25-7.30 <7.24 <7.00 >7.30
HCO3 (mEq/L) 15-18 <15 <10 >15
Urine Ketones + + + Small
Serum Ketones
+ + + Small
Anion Gap >10 >12 >12 <12
Mental Status Alert Alert/drowsy
Stupor/coma
Stupor/coma
DKA
Anion Gap = Na – (Cl + HCO3) Normal: 8 - 12

Management of DKA
Hydration Insulin administration Glucose monitoring Electrolyte correction
HHS
Prototype case is an elderly type 2 DM patient with several week history of polyuria, weight loss, ↓oral intake that culminates in mental confusion, lethargy or coma.
Clinical features of HHS
Precipitating events: serious, concurrent illness (e.g. MI,
CVA) Sepsis, pneumonia, and other
serious infections debilitating condition (prior stroke or
dementia) or social situation that compromises water intake
Clinical features of HHS
Physical findings: Profound dehydration Hypotension Tachycardia Altered mental status

Clinical features of HHS
Symptoms: Notable absence of nausea,
vomiting, and abdominal pain and the Kussmaul respirations
HHS
Diagnostic criteria:
Glucose >600mg/dl Total serum osmolality
>300mOsm/kg Absence of severe ketoacidosis

Management of HHS
Hydration Insulin administration Glucose monitoring Electrolyte correction
Chronic Complications of DM Macrovascular (CAD, CVD, PVD) Microvascular (retinopathy,
nephropathy,neuropathy)
Others (e.g. GI, GU, dermatologic, infectious)

Macrovascular Complications Largest cause of morbidity and
mortality Risk of CVD increased 2 to 4 fold Reduced survival post-MI. post-
CABG, and particularly PTCA Risk of stroke and PVD substantially
increased

Clinical Manifestations
Heart Angina pectoris Acute MI Silent MI Arrhythmias

Clinical Manifestations
Brain TIA (Transient ischemic attack) RIND (Reversible Ischemic
Neurological Deficits) Stroke in evolution Completed stroke
(infarction,embolism, hge) Lacunar infarcts
Clinical Manifestations
Limbs Peripheral vascular disease
(claudication; pain relieved by rest; pain does not go away with continued walk; primarily affects calves)
Poor wound healing, foot ulcers, gangrene
Neuropathy
Nephropathy
Retinopathy
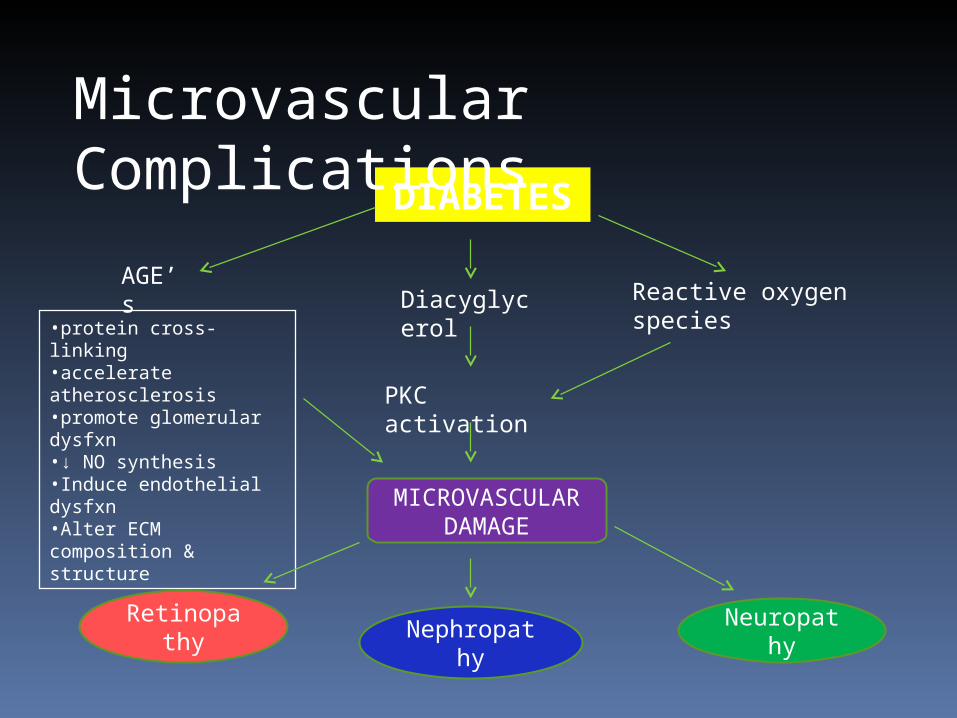
MICROVASCULAR DAMAGE
DIABETES
AGE’s Diacyglyce
rol
Reactive oxygen species
PKC activation
•protein cross-linking•accelerate atherosclerosis•promote glomerular dysfxn•↓ NO synthesis•Induce endothelial dysfxn•Alter ECM composition & structure
Microvascular Complications

DM Retinopathy
DM is the leading cause of blindness in ages 20-74 in the US
Blindness is primarily the result of progressive diabetic retinopathy and clinically significant macular edema.
Incidence: Found in almost all individuals with DM for
> 20yrs and 25% incidence with 5 years, and 80% incidence with 15 years of type 1 DM

Pathophysiology of DM Retinopathy
loss of retinal pericytes
↑ retinal vascular permeability
altered retinal blood flow
abnormal retinal microvasculature
Retinal Ischemia
Neovascularization
•Vitreous hemorrhage•Fibrosis
Retinal Detachmen
t
Classifications of DM RetinopathyStage I – Non-proliferative Thickening of capillary endothelial
BM Reduction of pericytes Microaneurysms Multiple hemorrhages Macular edema Microvascular occlusion and
ischemia

Classifications of DM RetinopathyStage II – Proliferative Hallmark – Neovascularization in
response to retinal hypoxia newly formed vessels appear near
the optic nerve and/or macula and rupture easily
vitreous hemorrhage, fibrosis retinal detachment

Stages of DM Retinopathy
Normal -fine yellow line, red bld column
Gr I - broadened yellow line, rbc Gr II - broad yellow line, copper wire,
bld column not visible Gr III - Broad white line, silver
wire, bld column not visible Gr IV - Fibrous cord, blood column
not visible
DM Nephropathy
Occurs in 20-40% of patients with diabetes is the leading cause of End stage renal disease
Basement membranes of the glomerular capillaries are thickened
microalbuminuria and macroalbuminuria
in individuals with DM are associated with increased risk of cardiovascular disease

Stage Chronology Main Lesion
GFR Albumin excretion
Baseline
BP Reversible by Strict Insulin
1.Acute renal hypertrophy,hyperfx
(+) at dx of DM (reversible with good control
Inc kidney size, inc glomerular size
Inc by 20-50%
Maybe inc but reversible
Inc but reversible
Usually normal
yes
2. Normoalbuminuria (UAE <20ug/min
Almost all px normoalbuminuric in 1st 5 years
On renal biopsy, inc BM thickness
Inc by 20-40%
N by defn.(15-20 ug/min) maybe abN
Maybe abN after a few years
normal.
Inc by about 1mmhg/yr
Hyperfiltration reduced
Classification of Renal Changes and Lesions in DM
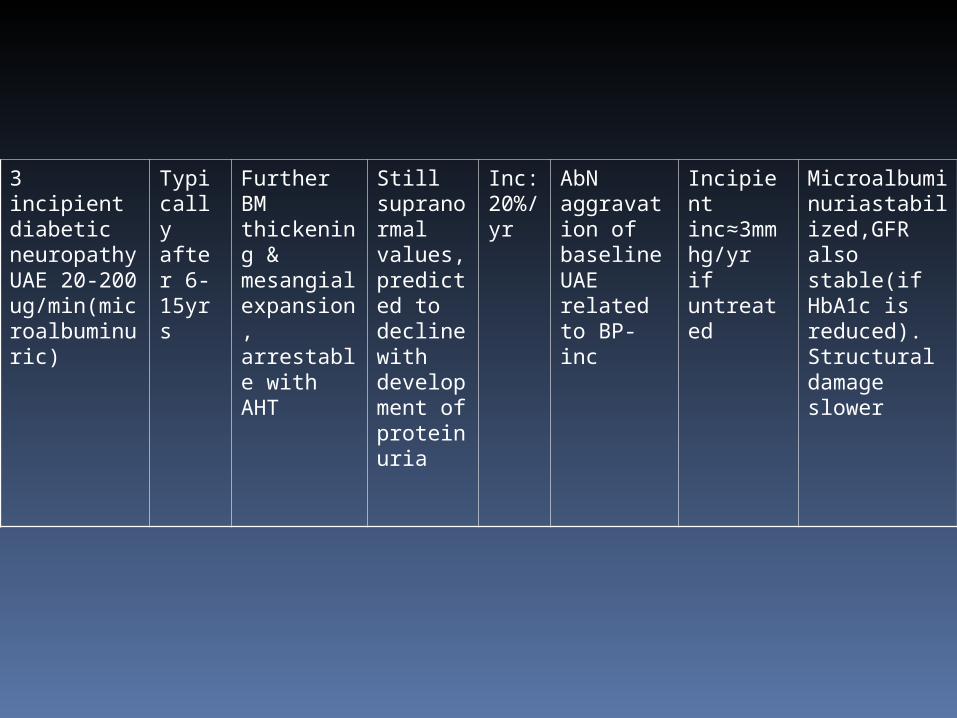
3 incipient diabetic neuropathy UAE 20-200 ug/min(microalbuminuric)
Typically after 6-15yrs
Further BM thickening & mesangial expansion, arrestable with AHT
Still supranormal values, predicted to decline with development of proteinuria
Inc: 20%/yr
AbN aggravation of baseline UAE related to BP-inc
Incipient inc≈3mmhg/yr if untreated
Microalbuminuriastabilized,GFR also stable(if HbA1c is reduced). Structural damage slower

4.Proteinuria, clinical overt diabetic nephropathy
Afetr 15-25 yrs (in ≈35% of px)
Clear and pronounced abN
Decline ≈ 10ml/min/year with clear CHONuria
Progressive clinical CHONuria of glomerular origin
Pronounced inc in BP during exercise
High BP, inc by ≈5 mmhg/yr(if untreated)
Higher fall if GFR with poor control
5 End Stage renal failure
Final outcome after 25-30yrs or more
Glomerular closure and advanced glomerulopathy
<10 ml/min
Often some decline due to nephron closure
Not studied
High if untreated
No. previous glycemic important in prevention

Diabetic Neuropathy
occurs in ~50% of individuals with long-standing type 1 and type 2 DM
may manifest as polyneuropathy, mononeuropathy, and/or autonomic neuropathy
Slow progression
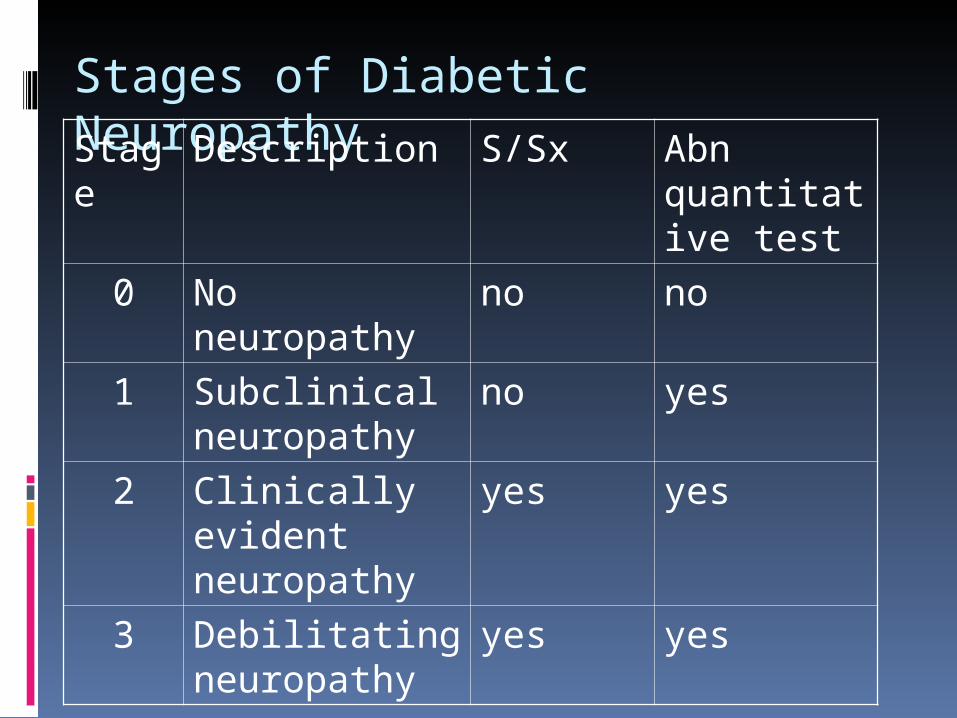
Stages of Diabetic NeuropathyStage Description S/Sx Abn
quantitative test
0 No neuropathy no no
1 Subclinical neuropathy
no yes
2 Clinically evident neuropathy
yes yes
3 Debilitating neuropathy
yes yes

Screening and Detection of Neuropathy Symptoms profile Neurologic examination Quantitative sensory testing (QST) Nerve conduction studies Quantitative autonomic function test
(QAFT)

Neurologic Examination
Cranial nerve deficits Sensory deficits Muscle changes Motor deficits Diminished or absent reflexes Autonomic disturbances
Treatment Goals
Halt progressive nerve fiber loss Early intervention Good glycemic control Decrease symptoms, especially pain Prevent ulcers and amputations
Other Complications
Gastrointestinal Delayed gastric emptying
(gastroparesis) Altered small or large bowel motility
(constipation or diarrhea)

Other Complications
Genitourinary Cystopathy Erectile dysfunction Female sexual dysfunction

Other Complications
Infections Pneumonia, UTI, and skin and soft
tissue infections are all more common in the diabetic population
Other Complications
Dermatologic Manifestations Protracted wound healing Skin ulcerations Diabetic dermopathy (e.g.
pigmented pretibial papules or “diabetic skin spots”; bullous diabeticorum; necrobiosis lipoidica; vitiligo; acanthosis nigricans; Lipoatrophy and lipohypertrophy )

Goals of treatment in type 2 DM Glucose control Decrease morbidity/mortality Preserve Beta cell function Maintenance of weight to as near
normal as possible BP control Eliminate symptoms Lipid control Decrease microvascular complications Decrease macrovascular complications
Pharmacologic Agents for Glycemic Control
Insulin Secretagogues (SU, Meglitinides)- ↑ insulin secretion
Insulin Sensitizers (Metformin, Thiazolidinediones)- ↑ peripheral glucose uptake- ↓ hepatic glucose production
Αlpha glucosidase inhibitors (Acarbose, Voglibose)- ↓ carbohydrate absorption
Factors to consider in use of OHAPatient
Age 60-70, AGI, glitazones, SU and meglitinidesMetformin may be used with caution, may lead to
lactic acidosisWeight
UW, insulin resistance, use insulin sensitizersOW, insulin deficiency use insulin secretagogues
Severity of hyperglycemiaRenal/ liver dse
Liver disease/ anti Koch meds, think of insulinDrugs
Efficacy and safetySite of actionTiming of BG lowering effect

Timing of BG lowering
Blood sugar lowering greater during fasting than post prandialMetforminSUInsulin
Blood sugar lowering greater during post prandial than fastingAGIInsulin sensitizersMeglitinidesinsulin

Mild
Upper limit or
overweight
Lean/Underweig
ht
Any of the ff:•TZD•Met
•A-gluc inhibitors
Any of the ff:•A-gluc inhibitors
•TZD•Met
•Small doses of mild SU•Repaglinide•Nateglinide
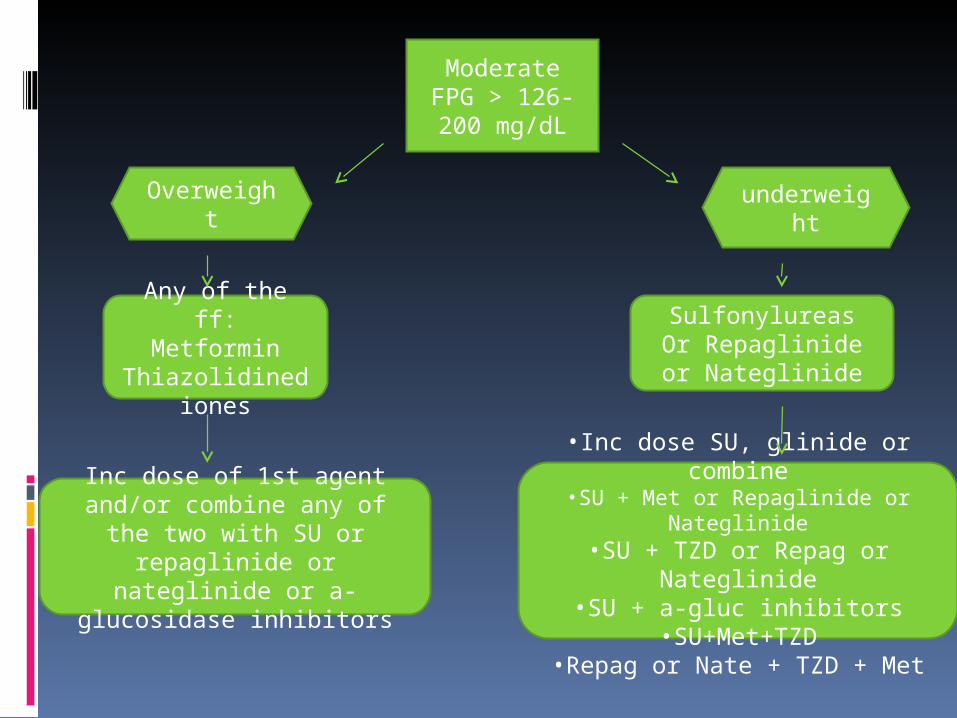
ModerateFPG > 126-200 mg/dL
Overweight
Any of the ff:Metformin
Thiazolidinediones
underweight
SulfonylureasOr Repaglinide or
Nateglinide
Inc dose of 1st agent and/or combine any of the two with
SU or repaglinide or nateglinide or a-glucosidase
inhibitors
•Inc dose SU, glinide or combine•SU + Met or Repaglinide or
Nateglinide•SU + TZD or Repag or
Nateglinide•SU + a-gluc inhibitors
•SU+Met+TZD•Repag or Nate + TZD + Met
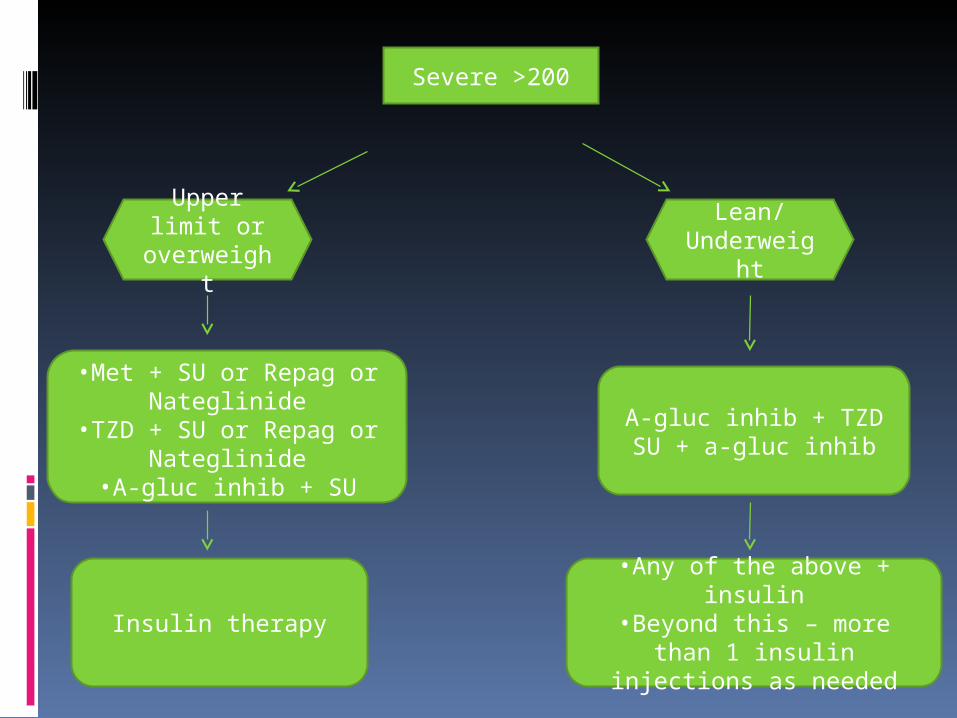
Severe >200
Upper limit or
overweight
Lean/Underweig
ht
•Met + SU or Repag or Nateglinide
•TZD + SU or Repag or Nateglinide
•A-gluc inhib + SU
A-gluc inhib + TZDSU + a-gluc inhib
Insulin therapy•Any of the above + insulin•Beyond this – more than 1 insulin injections as needed
Very severe >250-300, PPBS not restored to basal
Refer to Diabetes center or Diabetologist for insulin Therapy

Timing of BG lowering
Blood sugar lowering greater during fasting than post prandialMetforminSUInsulin
Blood sugar lowering greater during post prandial than fastingAGIInsulin sensitizersMeglitinidesinsulin
Dosing adjustment
Insulin secretagogues Titrate at 1-2 wks interval
Metformin Maximum lowering at 1-2 weeks Can be increased every 2-4 weeks
AGI Inc. dose every 2-4 weeks to minimize SE
TZD Max. lowering occurs at 16 weeks
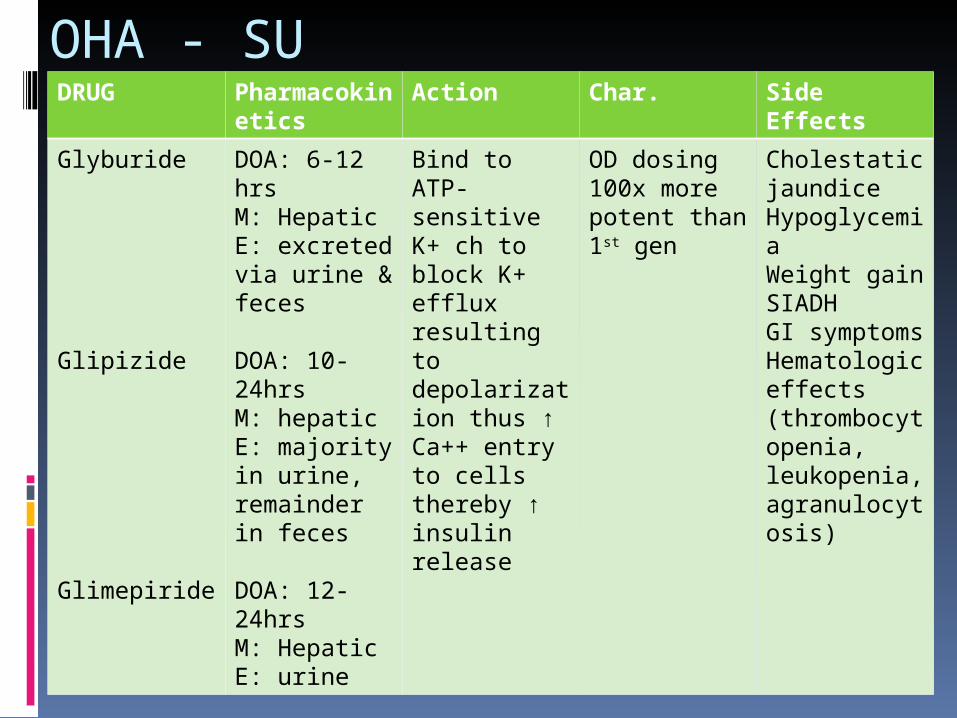
OHA - SUDRUG Pharmacok
ineticsAction Char. Side
Effects
Glyburide
Glipizide
Glimepiride
DOA: 6-12 hrsM: HepaticE: excreted via urine & feces
DOA: 10-24hrsM: hepaticE: majority in urine, remainder in feces DOA: 12-24hrsM: HepaticE: urine
Bind to ATP-sensitive K+ ch to block K+ efflux resulting to depolarization thus ↑ Ca++ entry to cells thereby ↑ insulin release
OD dosing100x more potent than 1st gen
Cholestatic jaundiceHypoglycemiaWeight gainSIADHGI symptomsHematologic effects (thrombocytopenia, leukopenia, agranulocytosis)

OHA - Meglitinide
DRUG Pharmacokinetics
Action Char. Side Effects
Repaglinide
•DOA: 1-3hrs•M: hepatic p450 enzymes•E: majority in urine
•Closes an ATP-dependent K+ ch to block K+ efflux resulting to depolarizn thus ↑ Ca++ entry to cells thereby ↑ insulin release
Similar effect to bld glucose as SUUseful for px w/ allergy to sulfur
Arthralgia, diarrhea, headache, hypoglycemia, neausea, paresthesia
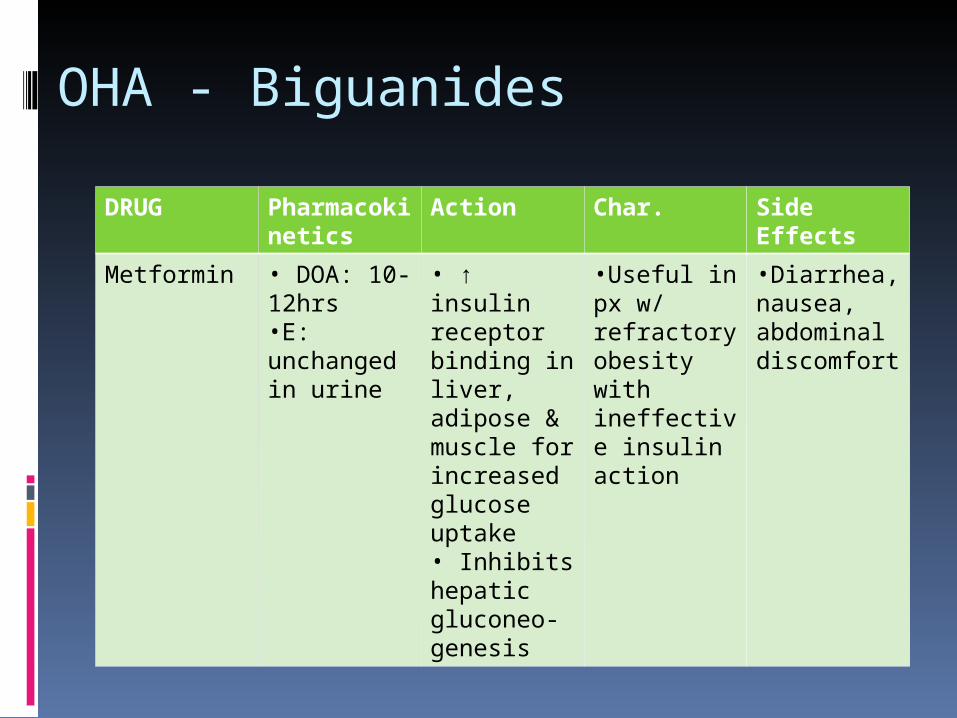
OHA - Biguanides
DRUG Pharmacokinetics
Action Char. Side Effects
Metformin • DOA: 10-12hrs•E: unchanged in urine
• ↑ insulin receptor binding in liver, adipose & muscle for increased glucose uptake• Inhibits hepatic gluconeo-genesis
•Useful in px w/ refractory obesity with ineffective insulin action
•Diarrhea, nausea, abdominal discomfort
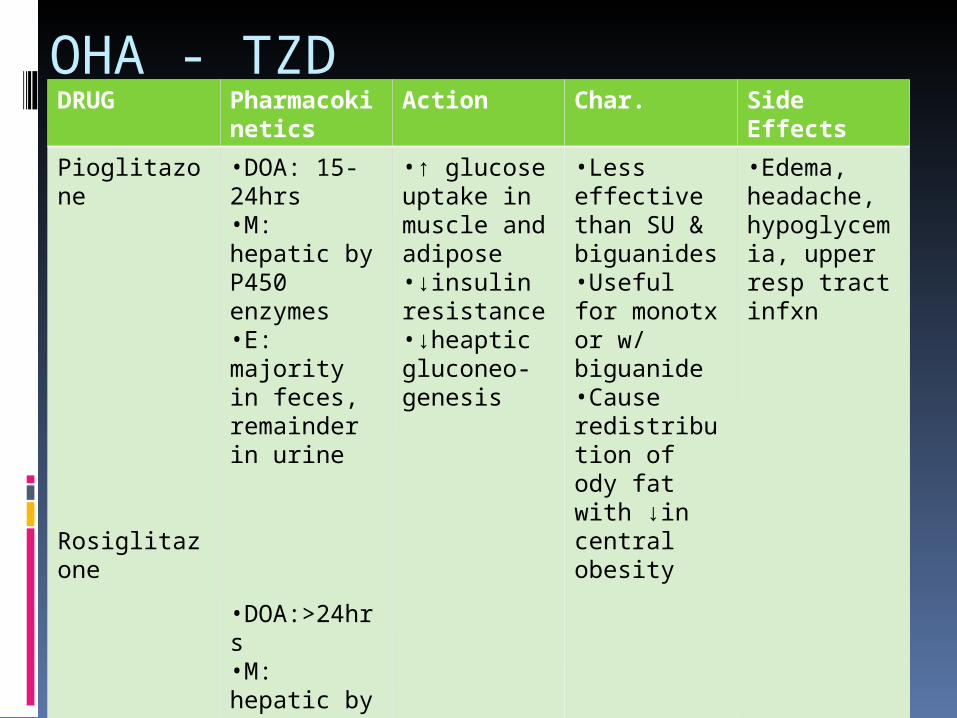
OHA - TZDDRUG Pharmacok
ineticsAction Char. Side
Effects
Pioglitazone
Rosiglitazone
•DOA: 15-24hrs•M: hepatic by P450 enzymes•E: majority in feces, remainder in urine
•DOA:>24hrs•M: hepatic by P450 enzymes•E: urine & feces
•↑ glucose uptake in muscle and adipose•↓insulin resistance•↓heaptic gluconeo-genesis
•Less effective than SU & biguanides•Useful for monotx or w/ biguanide•Cause redistribution of ody fat with ↓in central obesity
•Edema, headache, hypoglycemia, upper resp tract infxn

OHA – α-glucosidase inhibitorDRUG Pharmacokin
eticsAction Char. Side Effects
Acarbose •DOA: 3-4hrs•M: intestinal flora•E: absorbed portion-urine; unabsorbed portion - feces
•Slows CHO digestion & absorption time to prevent exaggerated postprandial rise in blood glucose
•↓ post- prandial hyper-glycemia by 30-50%•No hypo-glycemia•↓insulin release due to ↓ blood glucose•↓non-enzymatic glycation of proteins•improves overall glucose control & insulin sensitivity
•Abdominal pain, diarrhea, flatulence, jaundice

Guideline for use of Insulin Secretagouges
Action Generic Trade Name Preparation Daily dose
Short Tolbutamide Rastinon 500mg/tab ½ - 6tabs
Intermediate Glibenclamide
Gliclazide
Glipizide
Glimepiride
Euglucon
Daonil
Orabetie
Diamicron MR
Diamicron
Dianorm
Clizid
Minidiab
Solosa
2.5/5.0mg/tab
5.0mg
30mg/tab
80mg/tab
5 mg/tab
1,2,3 mg/tab
½-3 tabs
1-4 tab/day pre breakfast
½ - 4 tab
½ - 6 tabs
1-4 mg
Long acting Chlorpropamide Diabenese 250mg/tab ½ - 2 tabs
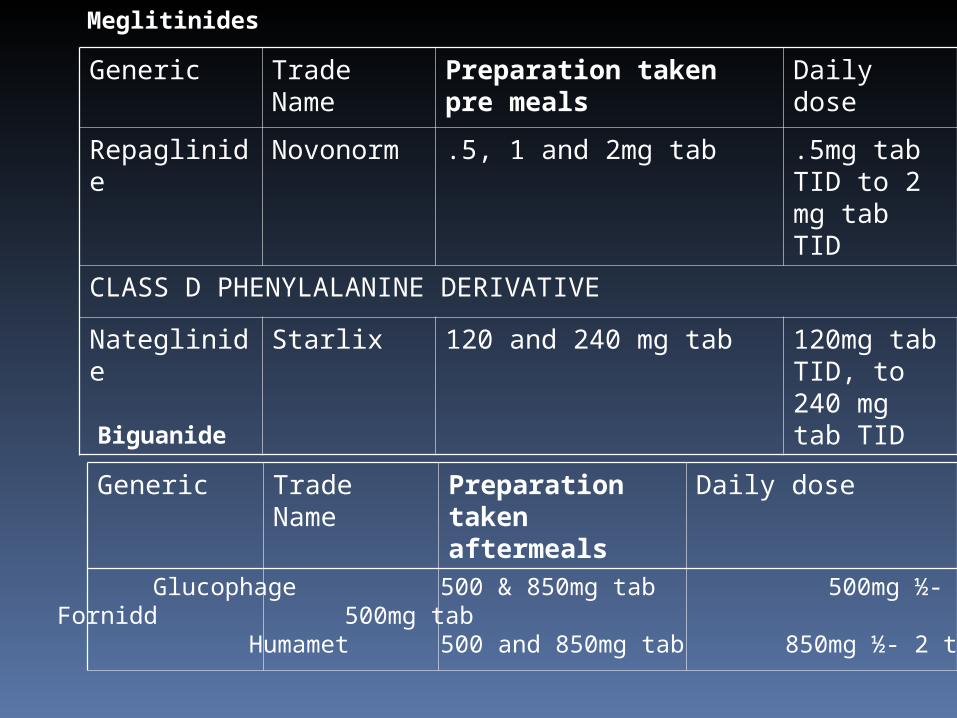
Generic Trade Name Preparation taken pre meals
Daily dose
Repaglinide Novonorm .5, 1 and 2mg tab .5mg tab TID to 2 mg tab TID
CLASS D PHENYLALANINE DERIVATIVE
Nateglinide Starlix 120 and 240 mg tab 120mg tab TID, to 240 mg tab TID
Generic Trade Name Preparation taken aftermeals
Daily dose
Meglitinides
Biguanide
Metformin Glucophage 500 & 850mg tab 500mg ½- 4 tabsFornidd 500mg tab
Humamet 500 and 850mg tab 850mg ½- 2 tabs
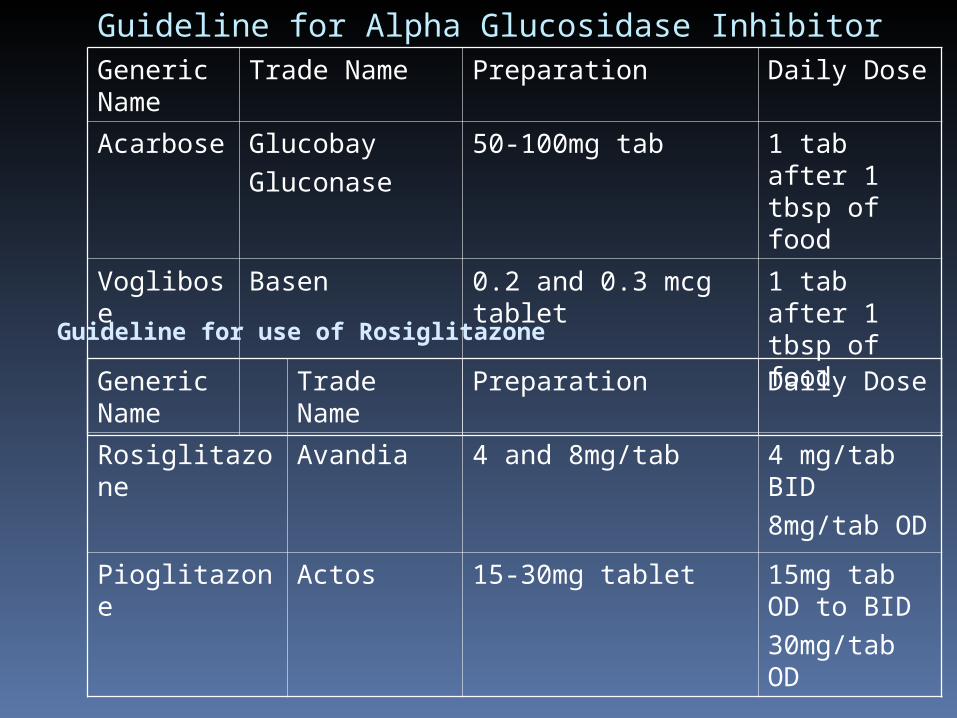
Guideline for Alpha Glucosidase InhibitorGeneric Name
Trade Name Preparation Daily Dose
Acarbose Glucobay
Gluconase
50-100mg tab 1 tab after 1 tbsp of food
Voglibose Basen 0.2 and 0.3 mcg tablet 1 tab after 1 tbsp of food
Generic Name Trade Name Preparation Daily Dose
Rosiglitazone Avandia 4 and 8mg/tab 4 mg/tab BID
8mg/tab OD
Pioglitazone Actos 15-30mg tablet 15mg tab OD to BID
30mg/tab OD
Guideline for use of Rosiglitazone
Newer Drugs
DPP4 inhibitorsMOA :small molecules that enhance the
effects of GLP-1 and GIP, increasing glucose-mediated insulin secretion and suppressing glucagon secretion
Inhibits degradation of GLP-1 and glucose-dependent insulinotropic peptide (GIP), the main insulinotropic peptides of intestinal origin (incretins ) by Dipeptidyl peptidase IV
Sitagliptin 100 mg (Januvia) once daily with or without food
Sitagliptin 100mg + metformin (Janumet)Vidagliptin
New drugs
Incretins Exenetide
derived from a compound found in the saliva of the Gila monster
functional analog of Glucagon-Like Peptide-1 (GLP-1), a naturally occuring peptide which enhances insulin secretion in response to elevated plasma glucose levels.
specifically indicated as adjunctive therapy to improve glycemic control in patients with Type 2 diabetes mellitus who are taking metformin, a sulfonylurea, or a combination of both, but have not achieved adequate glycemic control.
initiated at 5 mcg per dose 60 mins AC BID SubQ

When to start Insulin?
May be started Marked FPG >280mg/dL HBA1c of >9% Rapid uncontrolled weight loss GDM not controlled by dietary
modificaation Must be started
Acute stress, injury, surgery, steroid tx Renal/hepatic/allergies to OHA Patient’s choice

SHORT and RAPID ACTING
Contents Onset Peak Duration
RAPID
Insulin lispro
15-30 min 1-2 hrs 3-5 hours
Short Acting
Regular
0.5-0.7 hr 1.5-4 hr 5-8 hours

Intermediate Acting
Contents Onset Peak Duration
Insultard 1-4 hrs 8-10 hrs 12-20 hrs
Lente 2-4 hrs 8-12 hr 12-20 hr
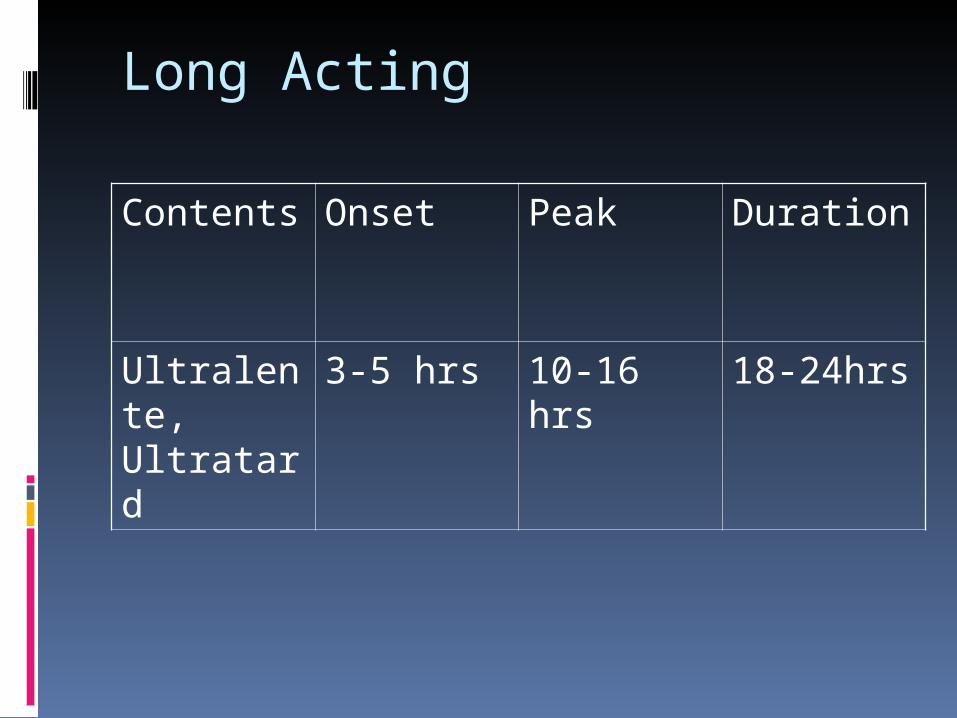
Long Acting
Contents Onset Peak Duration
Ultralente, Ultratard
3-5 hrs 10-16 hrs 18-24hrs
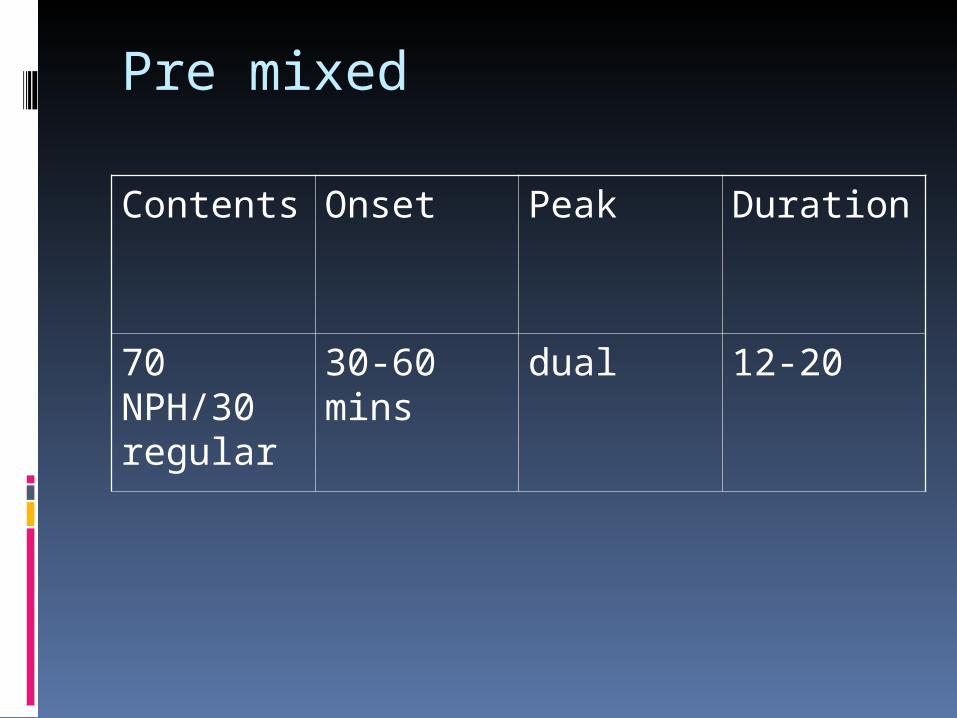
Pre mixed
Contents Onset Peak Duration
70 NPH/30 regular
30-60 mins dual 12-20
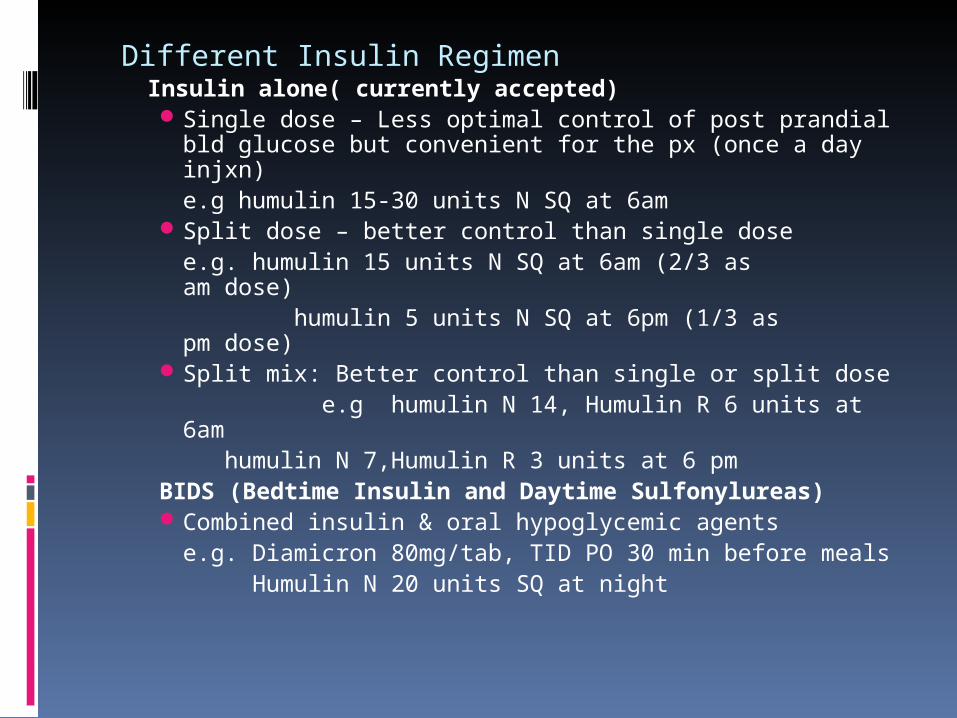
Different Insulin RegimenInsulin alone( currently accepted)Single dose – Less optimal control of post prandial bld
glucose but convenient for the px (once a day injxn)e.g humulin 15-30 units N SQ at 6am
Split dose – better control than single dosee.g. humulin 15 units N SQ at 6am (2/3 as am dose) humulin 5 units N SQ at 6pm (1/3 as pm dose)
Split mix: Better control than single or split dose e.g humulin N 14, Humulin R 6 units at
6am humulin N 7,Humulin R 3 units at 6 pmBIDS (Bedtime Insulin and Daytime Sulfonylureas)Combined insulin & oral hypoglycemic agents
e.g. Diamicron 80mg/tab, TID PO 30 min before meals Humulin N 20 units SQ at night

Different Insulin Regimen
Insulin + Oral Hypoglycemic Agents
Add insulin treatment on top of oral hypoglycemic agents. Choose any of the 3 regimens in (usually single dose or split dose
e.g. Humulin N 20 units SQ at 6am single dose
+ Diamicron 80mg 1 tab TID 30 min premeals

Medical Nutrition Therapy Calculate Desirable Body weight Determine the TEA Distribute to energy allowance CHO,
CHON, fats
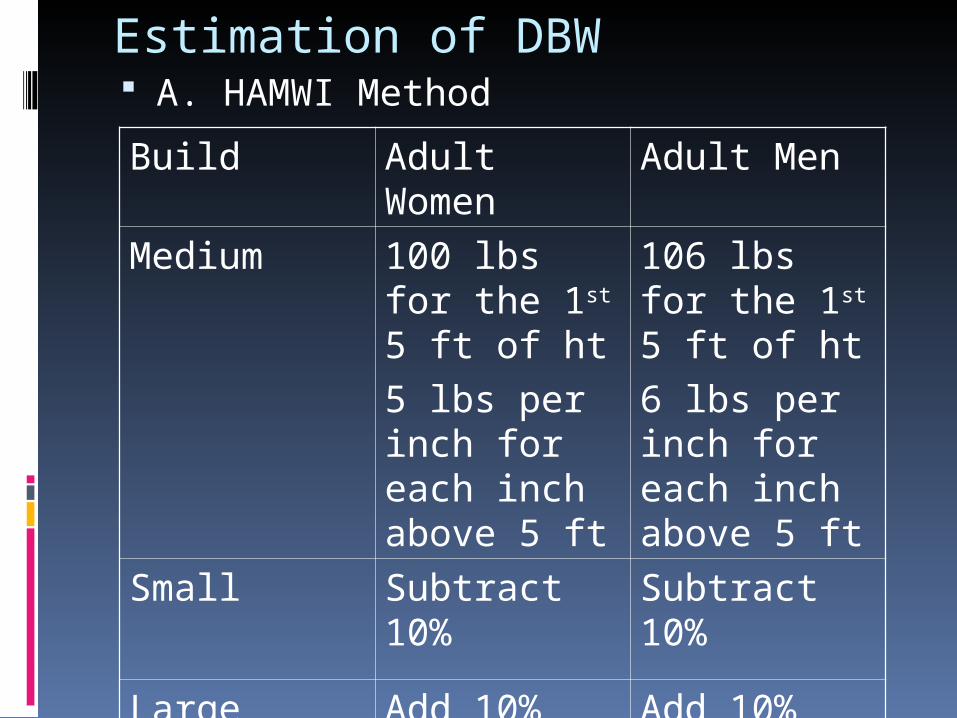
Estimation of DBW A. HAMWI Method
Build Adult Women Adult Men
Medium 100 lbs for the 1st 5 ft of ht
5 lbs per inch for each inch above 5 ft
106 lbs for the 1st 5 ft of ht
6 lbs per inch for each inch above 5 ft
Small Subtract 10% Subtract 10%
Large Add 10% Add 10%
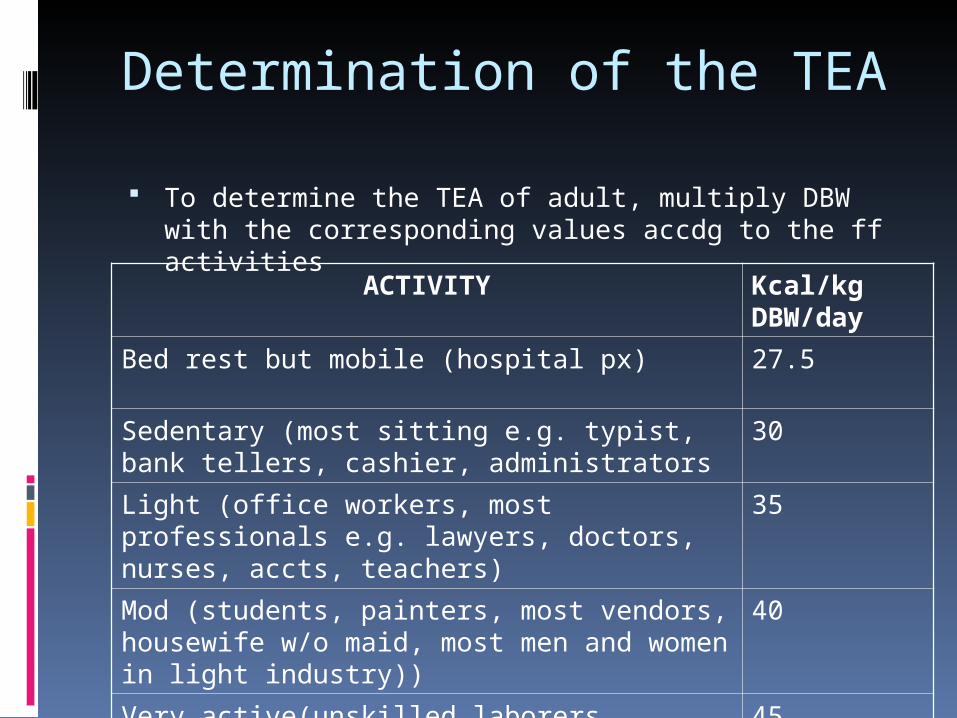
Determination of the TEA
To determine the TEA of adult, multiply DBW with the corresponding values accdg to the ff activities
ACTIVITY Kcal/kg DBW/day
Bed rest but mobile (hospital px) 27.5
Sedentary (most sitting e.g. typist, bank tellers, cashier, administrators
30
Light (office workers, most professionals e.g. lawyers, doctors, nurses, accts, teachers)
35
Mod (students, painters, most vendors, housewife w/o maid, most men and women in light industry))
40
Very active(unskilled laborers, athletes, dancers, fishermen, steel workers, soldiers on active service)
45
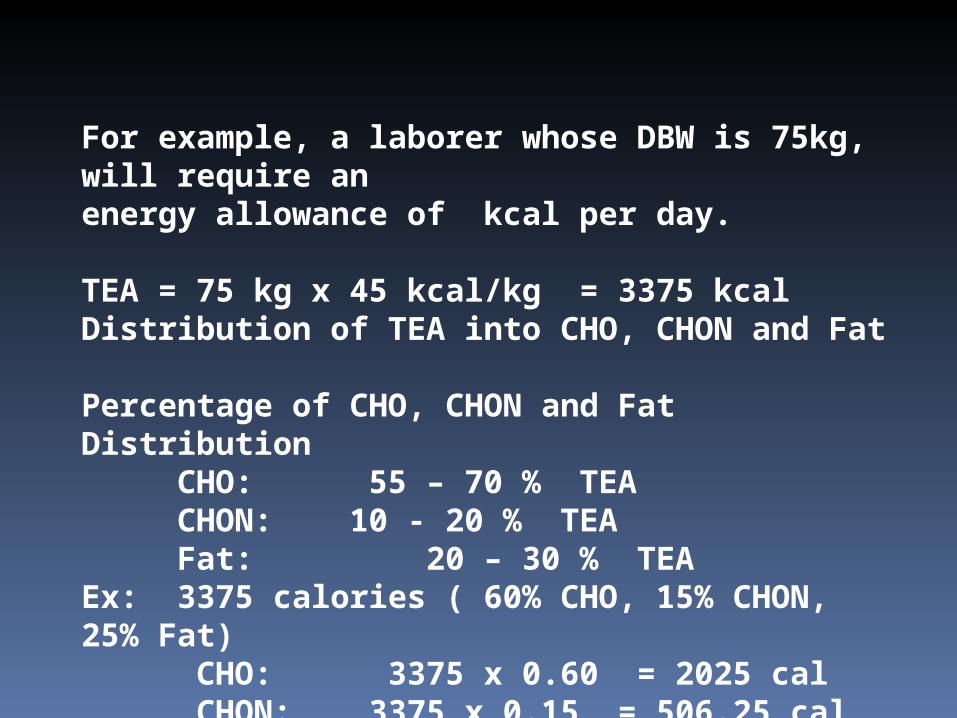
For example, a laborer whose DBW is 75kg, will require an energy allowance of kcal per day. TEA = 75 kg x 45 kcal/kg = 3375 kcal Distribution of TEA into CHO, CHON and Fat Percentage of CHO, CHON and Fat Distribution
CHO: 55 – 70 % TEACHON: 10 - 20 % TEA
Fat: 20 – 30 % TEAEx: 3375 calories ( 60% CHO, 15% CHON, 25% Fat) CHO: 3375 x 0.60 = 2025 cal CHON: 3375 x 0.15 = 506.25 cal Fat: 3375 x 0.25 = 843.75 cal
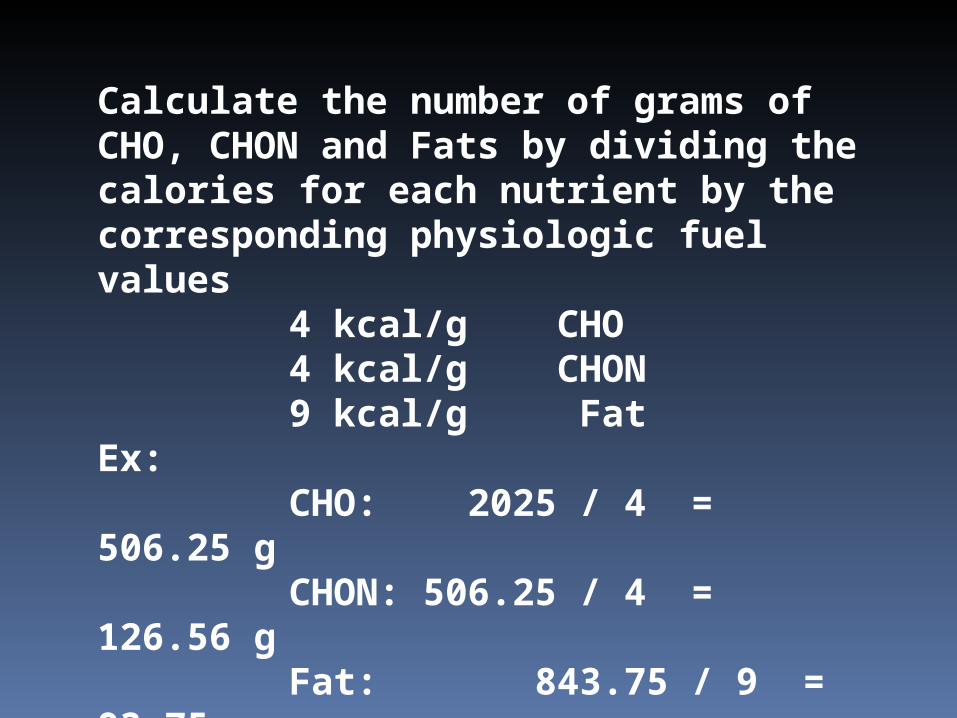
Calculate the number of grams of CHO, CHON and Fats by dividing the calories for each nutrient by the corresponding physiologic fuel values
4 kcal/g CHO4 kcal/g CHON9 kcal/g Fat
Ex: CHO: 2025 / 4 = 506.25
gCHON: 506.25 / 4 = 126.56
g Fat: 843.75 / 9 = 93.75
g Diet Rx: 3375 kcal ; CHO: 506.3 g; CHON: 126.6 g; Fat: 94 g

Medical Nutritional Therapy (MNT)
term used by the ADA to describe the optimal coordination of caloric intake with other aspects of diabetes therapy (insulin, exercise, weight loss
three types of MNT
10 prevention measures - directed at preventing or delaying the onset of type 2 DM in high-risk individuals (obese or with pre-diabetes)
2o prevention measures of MNT - preventing or delaying diabetes-related complications in diabetic individuals by improving glycemic control

3o prevention measures of MNT - managing diabetes-related complications (cardiovascular disease, nephropathy) in diabetic individuals

Exercise
cardiovascular risk reduction, reduced blood pressure, maintenance of muscle mass, reduction in body fat, and weight loss
lowering plasma glucose increasing insulin sensitivity ADA recommends 150 min/week
(distributed over at least 3 days) physical activity

Guidelines for Ongoing Medical Care for Patients with Diabetes
Self-monitoring of blood glucose (individualized frequency) A1C testing (2–4 times/year) Patient education in diabetes management (annual) Medical nutrition therapy and education (annual) Eye examination (annual) Foot examination (1–2 times/year by physician; daily by
patient) Screening for diabetic nephropathy (annual; see Fig. 338-11) Blood pressure measurement (quarterly) Lipid profile and serum creatinine (estimate GFR) (annual) Influenza/pneumococcal immunizations Consider antiplatelet therapy
Thank You!