Report on the Universal Data Collection Program...Report on the Universal Data Collection Program A...
27
Report on the Universal Data Collection Program A special report on children under two years of age in UDC Includes data collected from April 2003 through September 2005 UDC UDC UDC UDC UDC The Universal Data Collection Program The Universal Data Collection Program The Universal Data Collection Program The Universal Data Collection Program The Universal Data Collection Program July 2006/Vol.8/No.1
Transcript of Report on the Universal Data Collection Program...Report on the Universal Data Collection Program A...

Report on the Universal DataCollection Program
A special report on children under two yearsof age in UDC
Includes data collected from April 2003 through September 2005
UDCUDCUDCUDCUDCThe Universal Data Collection ProgramThe Universal Data Collection ProgramThe Universal Data Collection ProgramThe Universal Data Collection ProgramThe Universal Data Collection Program
July 2006/Vol.8/No.1

UDC Report Vol. 8, No 1Vol2
The Report on the Universal Data Collection Program is published by the Division of Hereditary Blood Disorders, National Center on Birth Defects and DevelopmentalDisabilities, Centers for Disease Control and Prevention (CDC), Atlanta, Georgia 30333. All data are provisional.
Centers for Disease Control and Prevention................................Julie L.Gerberding, MD., MPHDirector
National Center on Birth Defectsand Developmental Disabilities..............................................................José Cordero, MD, MPH
DirectorDivision of Hereditary Blood Disordrers........................................................Roshni Kulkarni,M.D.
Director
J. Michael Soucie, PhDEpidemiologist, Hemophilia Surveillance
Sally OwensDirector, Hemophilia Treatment Center Program
Meredith Oakley, DVM, MPHProject Coordinator
Nina Larsen, MSPHAssociate Project Coordinator
The Report on the Universal Data Collection Program is accessible via internet at http://www.cdc.gov/ncbddd/hbd/surveillance.htm Confidential information, referrals, and educationalmaterial on hemophilia and other bleeding disorders are also available by calling the NationalHemophilia Foundatation’s information line, HANDI, at 800-42-HANDI.
Suggested Citation: Centers for Disease Control and Prevention. Report on theUniversal Data Collection Program. 2006;8(No.1):[inclusive page numbers].

3UDC Report Vol. 8, No 1Vol
Contents
Commentary .......................................................................................................................................4
TablesTable 1. New Enrollment in UDC, April 2003 -September 2005 ........................................................8Table 2. Enrollment in UDC by region, April 2003 - September 2005 ...............................................8Table 3. Demographic characteristics of children with hemophilia < 2 years of age
enrolled in UDC ................................................................................................................10Table 4. Sources of health care reimbursement listed by children with hemophilia <2 years of age enrolled in UDC ................................................................................................................ 11Table 5. Birth Information of children with hemophilia < 2 years of age enrolled in UDC ..............12Table 6. Diagnostic testing on children with hemophilia < 2 years of age enrolled in UDC............13Table 7. Site of blood draw for factor activity level in children with hemophilia < 2 years of age
enrolled in UDC ................................................................................................................14Table 8. Treatment type for children with hemophilia < 2 years of age enrolled in UDC ................15Table 9. Blood and factor products used by children with hemophilia <2 years of age enrolled in UDC ................................................................................................................15Table 10. Home infusion in children with hemophilia < 2 years of age enrolled in UDC ...................15Table 11. Bleed data in children with hemophilia <2 years of age enrolled in UDC...........................16Table 12. Head injuries and intracranial hemorrhages (ICH) in children with hemophilia <2 years of age enrolled in UDC .........................................................................................................17Table 13. Hepatitis B vaccination in children with hemophilia <2 years of age enrolled in UDC .......18Table 14. Central venous access devices (CVADs) in children with hemophilia < 2 years of age enrolled in UDC Table ......................................................................................................18Table 15. Prevalence of current inhibitors by titer among children with hemophilia < 2 years of age enrolled in UDC ..............................................................................................................19
FiguresFigure 1. UDC visits by year, April 2003-September 2005 ..........................................................9Figure 2. Disease severity of children with hemophilia < 2 years of age enrolled in UDC ......14
Technical Notes .................................................................................................................................20Acknowledgements ...........................................................................................................................22Hemophilia Treatment Center Regional Map .....................................................................................27

UDC Report Vol. 8, No 1Vol4
CommentaryThe two most common congenital bleed-
ing disorders are von Willebrand disease(VWD) and hemophilia. VWD is caused bythe defective synthesis or function of a pro-tein, von Willebrand factor that is necessaryfor normal blood clotting. VWD occurs withequal frequency in males and females. Al-though the prevalence of this disease is notprecisely known, it is estimated that betweenone and two percent of the population areaffected. There are different types and sever-ity of VWD. Symptoms include heavy orprolonged menstrual bleeding, easy bruising,frequent or prolonged nosebleeds, and pro-longed bleeding following surgery, dentalwork, childbirth, or injury.
Hemophilia is caused by a defect in thegene located on the X chromosome thatcontains the genetic code for one of theclotting factor proteins necessary for normalblood clotting. A deficiency of factor VIII isreferred to as hemophilia A or “classic” hemophilia. In contrast, a deficiency of factorIX characterizes hemophilia B, also known asChristmas disease. The defect usually occurson one of the two female X chromosomes andresults in a carrier state. When males havethe defect on their only X chromosome, theyhave the disease. Thus, almost all of theapproximately 17,000 people with hemophiliain the United States are male.
People with severe hemophilia can experience serious bleeding into tissues,muscles, joints, and internal organs, oftenwithout any obvious trauma. Repeatedbleeding into joints without adequatetreatment results in crippling chronic jointdisease, one of the severe complications ofbleeding disorders. In the mid-1970s, treat-ment for hemophilia was improved throughthe use of clotting factor concentrates,
products made from the plasma of donatedblood. However, because blood donationsfrom thousands of donors are pooled togetherto make these products, many people withbleeding disorders were infected withhepatitis B and C viruses and with humanimmunodeficiency virus (HIV), the virus thatcauses AIDS, before the risk of diseasetransmission in blood products wasrecognized and prevention measures taken.
In 1975, Congress initiated federal fundingto specialized hemophilia treatment centers(HTCs) to provide comprehensive care topeople with bleeding disorders. Since 1986,the Centers for Disease Control andPrevention (CDC) has been involved with thehemophilia community through the HTCsystem, primarily through risk-reduction effortsaimed at preventing secondary infection offamily members with HIV.
In 1991, CDC received a request from theNational Hemophilia Foundation to expandtheir collaborative activities within thebleeding disorders community. Meetings withpatients and hemophilia care providers wereheld during 1992 to determine the areas ofhighest priority. Based on recommendationsfrom these constituents, a congressionalmandate was issued to CDC, with the goal ofreducing the human suffering and financialburden of bleeding disorders by focusingnational emphasis on prevention and earlyintervention. The issues of greatest concernidentified by the bleeding disorderscommunity were: (1) the safety of the bloodsupply from infectious diseases and (2) theprevention of joint disease.
In response, CDC developed the UniversalData Collection Program (UDC). Thepurpose of UDC is two-fold: (1) to establish asensitive blood safety monitoring system

5UDC Report Vol. 8, No 1Vol
among people with bleeding disorders and(2) to collect a uniform set of clinicaloutcomes information that can be used tomonitor the occurrence of and potential riskfactors for infectious diseases and jointcomplications.
People with bleeding disorders are enrolledin UDC by care providers in each of thenation’s 134 federally funded HTCs. As partof the project, a uniform set of clinical dataand plasma specimens is collected by HTCstaff each year during each participant’sannual comprehensive clinic visit. A portionof the plasma specimen is used to performfree screening tests for hepatitis A, B, and Cviruses and for HIV. The remainder of thespecimen is stored for use as needed infuture blood safety investigations.
Enrollment in UDC began in May 1998.Information about eligibility requirements,enrollment procedures, and data collectioncan be found in the Technical Notes of thisreport. Participating HTCs are listed byregion in the Acknowledgements. A regionalmap is included at the end of this report.
The purpose of this surveillance report is todisseminate the information being collectedby UDC to public health workers, healtheducators and planners, other care providers,and patients in the bleeding disorderscommunity. The report contains informationabout the demographic characteristics of theparticipants, their blood and factor productuse, and the occurrence and treatment of jointand infectious diseases.
We hope that this information will proveuseful to those involved in efforts to reduce orprevent the complications of these conditions.
The proper interpretation and appropriateuse of surveillance data require anunderstanding of how the data are collected,reported, and analyzed. Therefore, readersof this report are encouraged to review theTechnical Notes, beginning on page 18.
Highlights
This issue of the UDC Surveillance Report isa special report that focuses on data col-lected from children under two years of age(babies) who have been enrolled throughSeptember 2005. Data collection on thisgroup began its pilot phase in April 2003.The data collected on these initial 38 babiesis included in this report. The pilot phase ranthrough April 2004. Official enrollment ofbabies into UDC began in May 2004 andcontinues. In this report, data on enrollmentand visits (Tables 1 and 2, Figure 1) includeall babies seen through September 2005.However, all subsequent tables and graphsdescribe the hemophilia population only.
Since April, 2003, 220 babies with bleedingdisorders have been enrolled and there havebeen 229 UDC visits.
Tables 1 and 2 show new enrollment in UDC.211 and 7 babies with hemophilia and VWDrespectively have been enrolled. In addition2 with Factor VII deficiency were also enrolled(data not shown). Enrollment has approxi-mately doubled in each year, with 30 babiesin 2003, 55 in 2004, and 133 throughSeptember 2005. (Table 1). Table 2 showsthat regional enrollment has ranged from 1in Region VII to as many as 40 babies inRegion VIII.

UDC Report Vol. 8, No 1Vol6
Figure 1 shows the number of babies with aUDC visit in each year through September2005 according to visit type. The number ofbabies with a first time UDC visit is muchgreater than those with a follow-up visitbecause enrollment and data collection hasonly recently begun and enough time has notpassed to adequately capture return visits. Inthe UDC population aged 2 years and over,follow-ups visits outnumber first-time visits ata ratio of approximately 3.5 to 1 over time.
The distribution of demographic characteris-tics is shown in Table 3. Just over half are 1year or less and all are males. The populationdistribution by race and ethnicity is similar tothat of the general population
Table 4 lists the sources of healthcare reim-bursement. About 50% of participants havesome form of commercial insurance, about40-45% have government sponsored cover-age, and the remainder have other types ofinsurance. Only about 3-4% of the partici-pants are uninsured.
Table 5 shows information on birth. Almosttwo-thirds of the babies were deliveredvaginally. Instrumentation during delivery wasperformed on 7 babies (3.3%). There were20 pre-term births (defined as less than 37weeks at birth) and the mean age of thesewas 34.7 weeks. Vitamin K was administeredalmost two-thirds of the time. Less than 10%received clotting factor concentrate at birthand then it was given either for prophylaxis ortreatment of a bleed. An HTC was contactedbefore delivery in only 32.5% of the cases.
Diagnostic testing is described in Table 6.62% of babies enrolled, had hemophiliadiagnostic testing performed because themother was a known carrier or there was apositive family history. In 34% of the babies , ableeding symptom prompted the diagnostic
testing. The mean age of diagnosis was 18days and almost 70% of the babies werediagnosed before one month of age. Sevenbabies had prenatal testing performed, and13.7% of participants had geneticanalysis for the hemophilia genetic mutation.
Figure 2 shows the distribution of diseaseseverity. Over half of the babies had severedisease, 27.5% had moderate disease and16.1% had mild disease.
Table 7 show site of blood draw for factoractivity level that determines disease severity.Over 70% had venipuncture as their site ofblood draw.
Table 8 shows that the most common type oftreatment used for all severity levels ofhemophilia was episodic care. As expected,babies with severe disease were the mostlikely to be on continuous prophylaxis.
The proportion of overall factor product use isshown in Table 9. The majority of babies withhemophilia who require factor infusion areadministered recombinant products. About25% of babies received no product during theyear prior to their UDC visit. Also of note isthat 8 babies received cryoprecipitate orfresh frozen plasma, products which are notas effective as clotting factor in treatingbleeds.
Table 10 illustrates that among the 158babies receiving factor product, 22.8% arehome infused. Of these, two-thirds receivetheir infusion from a family member.
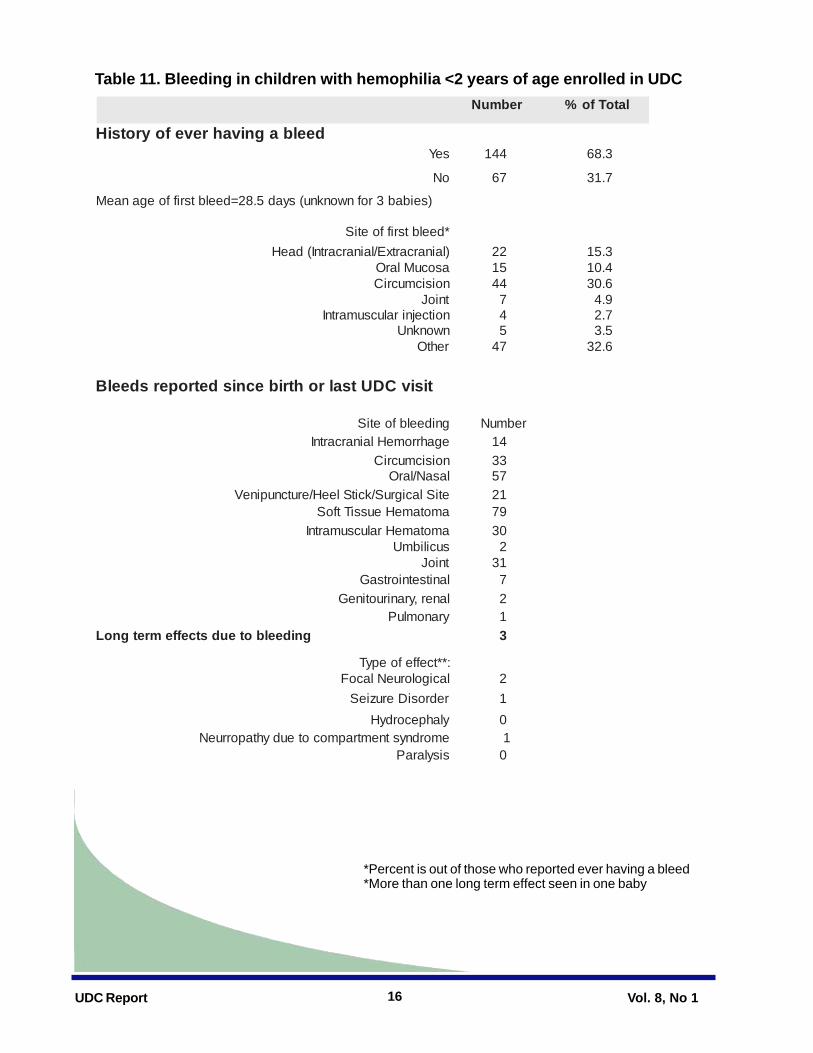
Data on bleeding are shown in Tables 11. Atenrollment, 68.3% of babies had experienceda bleed and the mean age of the first bleedwas 28.5 days. In nearly one-third of cases,the first bleed occurred at the site ofcircumcision. However, the sites with the

7UDC Report Vol. 8, No 1Vol
Suggested Reading
Centers for Disease Control and Prevention.Prevention of hepatitis A through active orpassive immunization. Recommendations ofthe Advisory Committee on ImmunizationPractices (ACIP). MMWR 1996;45(No. RR-15):1-30.
Centers for Disease Control and Prevention.Blood safety monitoring among persons withbleeding disorders — United States, May1998—June 2002. MMWR 2003;51(51);1152-1154
most frequent bleeding episodes were thesoft tissues (79 participants), followed by oral/nasal sites (57 participants). Three babieshad long-term effects due to bleeding includ-ing focal neurological deficits, seizure disor-der and neuropathy due to compartmentsyndrome.
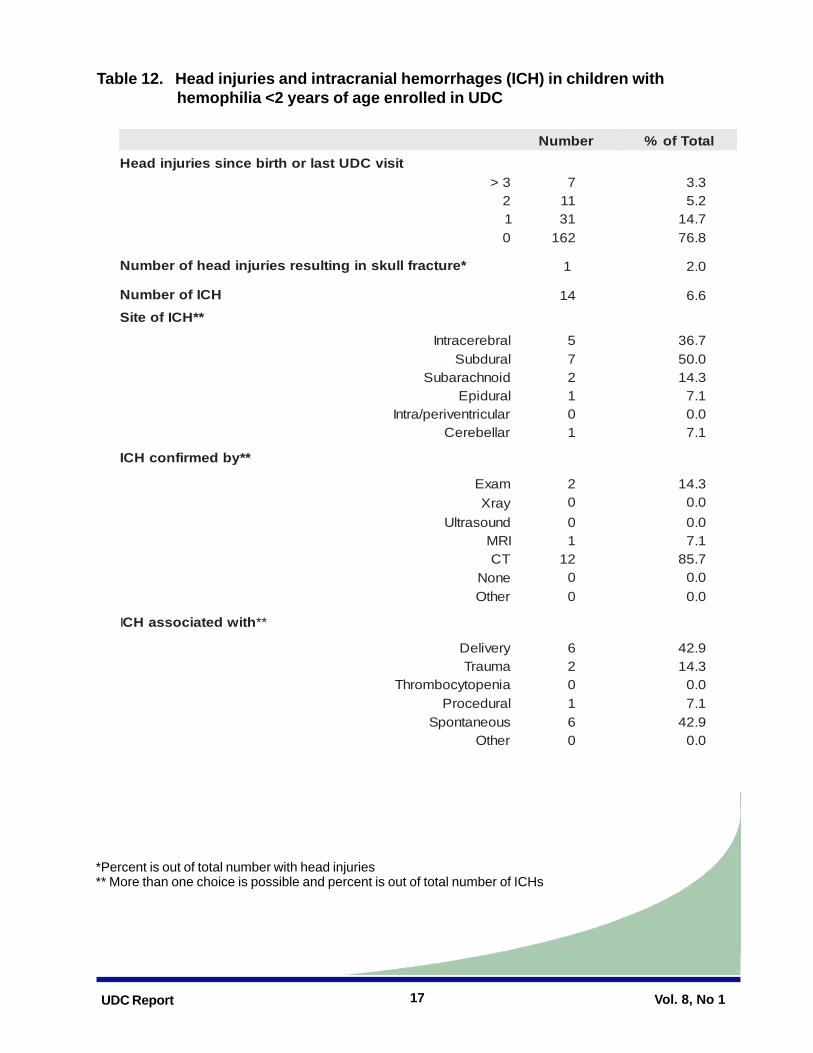
Table 12 lists information on head injuries andintracranial hemorrhages. A majority ofbabies, 162/211 (76.8%) did notexperience a head injury since birth or lastUDC visit. Of the 49 babies who had a headinjury, 31 had one head injury, 11 had two,and 7 had 3 or more. One of the head injuriesresulted in a skull fracture. Finally, 14 babieshad an intracranial hemorrhage (ICH). Themost common site of ICH was subdural(50%), followed by intracerebral (36.7%) andsubarachnoid (14.3%). In most cases, ICHwas confirmed by computerized tomographyand ICH was found to be associated withdelivery at birth orspontaneous occurrence in equal proportions.
Table 13 describes Hepatitis B vaccinationstatus and route of administration. More thanhalf of the babies had completed the basicHepatitis B vaccination series at UDC enroll-ment and almost a third (29.9%) were cur-rently receiving the series. Route ofadministration was intramuscular in 23.7% ofbabies, subcutaneous in 18.5%, and unknownfor 52.6%. The high proportion of unknownadministration route data reflects the fact thatmost of the babies do not receive the vaccinein the treatment center and the parents usuallydo not know this information.
Table 14 describes the use of central venousaccess devices for clotting factor infusion. Atthe latest visit, 11.4% of babies had had atleast one CVAD placed since birth or the lastUDC visit and, of these, 79.1% were ports. Of
those with a CVAD, 10 babies had at leastone CVAD complication. The most commonCVAD complication was infection, whichoccurred in 8 of the 10 babies with a compli-cation.
Table 15 shows the prevalence of inhibitorsamong persons with hemophilia under age 2enrolled in UDC. The majority of inhibitorsoccurred in babies with hemophilia A andsevere disease and most of these inhibitors

UDC Report Vol. 8, No 1Vol8
Table 1. New Enrollment in UDC, April 2003 -September 2005
*See map (page 27) for regional designations.
noigeR ailihpomeH DWVI 8 0
II 8 0
III 11 1
N-VI 71 1S-VI 62 0E-V 73 2W-V 61 1IV 91 1IIV 1 0IIIV 04 1
XI 12 0X 7 0
latoT 112 7
Table 2. Enrollment in UDC by region*, April 2003 - September 2005
htnoM ailihpomeH DWV3002ceD-lirpA 92 1
4002ceD-naJ 45 15002yraunaJ 11 05002yraurbeF 61 0
5002hcraM 51 0
5002lirpA 71 15002yaM 11 2
5002enuJ 71 15002yluJ 02 0
5002tsuguA 21 0
5002rebmetpeS 9 1latoT 112 7

9UDC Report Vol. 8, No 1Vol
0
20
40
60
80
100
120
140
2003 2004 2005
Num
ber o
f Pat
ient
s
First-time visit Follow-up visit
n=34 n=62 n=133
Figure 1. UDC visits by year, April 2003-September 2005

UDC Report Vol. 8, No 1Vol10
Table 3. Demographic characteristics of children with hemophilia* < 2 years ofage enrolled in UDC
ailihpomeH
)851=n(A )35=n(B
citsiretcarahC rebmuN tnecreP rebmuN tnecreP
shtnom(puorGegA )
3-0 22 9.31 7 2.31
6-4 02 7.21 7 2.31
9-7 71 8.01 3 7.5
21-01 32 6.41 8 1.51
51-31 32 6.41 9 0.71
81-61 81 4.11 5 4.9
42-91 53 2.22 41 4.62
yticinhtE/ecaR
etihW 59 1.06 73 8.96
naciremAnacirfA 91 0.21 2 8.3
cinapsiH 13, 6.91 8 1.51
rednalsIcificaP/naisA 4 5.2 1 9.1
naciremAevitaN 2 3.1 0 0.0
rehtO 7 4.4 5 4.9
xeS
elaM 851 001 35 001
elameF 0 -- 0 --
*One person was reported to have both hemophilia and VWD (this person is included in analyses as ahemophilia patient only and not as a VWD patient). A total of 2 persons had Factor VII deficiency.

11UDC Report Vol. 8, No 1Vol
ecruoStnemesrubnieR )112=n(rebmuN latoTfotnecreP
ecnarusnIlaicremmoC 92 7.31OMHecnarusnIlaicremmoC 53 6.61OPPecnarusnIlaicremmoC 14 4.91
eracideM 2 0.1OMHeracideM 0 --
diacideM 15 2.42OMHdiacideM 12 0.01
SUPMAHC 8 8.3
nalpksirhgihetatS 7 3.3
rehtO 52 9.11
derusninU 7 3.3
Table 4. Sources* of health care reimbursement listed by children with hemophilia <2 years of age enrolled in UDC
*Some people may have listed more than one source of reimbursement. HMO = Health maintenance organization; PPO = Preferred provider organization

UDC Report Vol. 8, No 1Vol12
Table 5. Birth Information of children with hemophilia < 2 years of age enrolled in UDC
*More than one delivery method may be selected**Percent is out of total number with clotting factor given
rebmuN latoTfo%
*dohteMyrevileD
lanigaV 831 4.56noitceS-CevitcelE 04 0.91
noitceS-Cevitcele-noN 82 3.31nwonknU 3 4.1
rehtO 1 5.0
yreviledgnirudnoitatnemurtsnI
specroF 1 5.0muucaV 6 8.2
htribmret-erP )skeew73<()7.43=stnafnimret-erpfoeganaeM(
02 5.9
htribtaderetsinimdaKnimatiVseY 331 3.36
oN 91 1.9nwonknU 95 6.72
htribtanevigetartnecnocrotcaFgnittolC
seY 61 6.7oN 291 4.19
nwonknU 3 0.1sixalyhporP:**nosaer,seyfI 01 5.26deelbfoxR 6 5.73
yrevilederofebdetcatnocCTH
seY 86 5.23oN 831 0.66
nwonknU 3 4.1

13UDC Report Vol. 8, No 1Vol
Table 6. Diagnostic testing on children with hemophilia < 2 years of age enrolled in UDC
rebmuN latoTfo%
gnitsetcitsongaidrofnosaeRreirracnwonkrehtoM 68 0.14yrotsihylimafrehtO 54 4.12
motpmysgnideelB 27 3.43
nwonknU 2 4.0rehtO 6 9.2
desongaidtsrifredrosidgnideelbegA)syad81=sisongaidtaeganaeM(
latan-erP 6 8.2htnom1< 741 7.96
shtnom6-1 33 6.51
shtnom21-7 51 1.7
shtnom42-21 01 7.4
gnitsetlatanerP
sisetnecoinmA 6 8.2
rehtO 1 5.0
nwonknU 2 9.0
tisivtsalrohtribecnissisylanaciteneG
seY 92 7.31
oN 471 5.28
gnissiM 8 8.3

UDC Report Vol. 8, No 1Vol14
Figure 2. Disease severity of children with hemophilia < 2 years of age enrolled in UDC
Table 7. Site of blood draw for factor activity level in children with hemophilia < 2 years of age enrolled in UDC
rebmuN latoTfo%
warddoolbfoetIS
doolbdroC 64 3.22erutcnupineV 741 4.17
nwonknU 81 3.6
56.4%
16.1%
27.5%
Mild (Factor Activity >5%)
Moderate (Factor Activity 1-5 %)
Severe (Factor Activity <1%)

15UDC Report Vol. 8, No 1Vol
Table 8. Treatment type for children with hemophilia < 2 years of age enrolled in UDC
*Prophylaxis is considered continuous when clotting factor is administered on a regular basis to prevent allbleeding and is expected to continue indefinitely.
dliM etaredoM ereveS
tnemtaerT rebmuN tnecreP rebmuN tnecreP rebmuN tnecreP
eraccidosipE 43 001 25 7.98 69 7.08suounitnoCsixalyhporP 0 -- 5 6.8 81 1.51
latoT 43 85 911
Table 9. Blood and factor products used* by children with hemophilia <2 years of age enrolled in UDC
*Any use of the product(s) during the 12-month period preceding the UDC visit.NOTE: Individuals may have used more than one type of treatment product.
AailihpomeH BailihpomeH
tcudorptnemtaerT rebmuN tnecreP rebmuN tnecreProtcaftnanibmoceR 801 4.86 63 9.76
IIIVrotcaflanolcnoM 0 -- 0 --IIIVrotcafnamuhrehtO 4 5.2 0 --
IIIVrotcafenicroP 0 -- 0 --XIrotcafnamuH 0 -- 1 9.1
xelpmocnibmorhtorP 0 -- 0 --xelpmocnibmorhtorpdetavitcA 4 5.2 0 --
PFFfoetatipicerpoyrC 6 8.3 2 8.3nisserpmoseD 1 6.0 0 --
racimA 91 3.21 9 0.71desuenoN 93 7.42 41 4.62
Table 10. Home factor infusion in children with hemophilia < 2 years of age enrolled in UDC
*Percent is out of total number of those receiving home infusion. Indivdiuals may have more than onemethod of home infusion.
rebmuN tnecreP)851=n(noisufniemoH 63 8.22
:ybnevignoisufnI rebmemylimaF 42 7.66redivorperaC 51 7.14
UDC Report Vol. 8, No 1Vol16
Table 11. Bleeding in children with hemophilia <2 years of age enrolled in UDC
*Percent is out of those who reported ever having a bleed*More than one long term effect seen in one baby
rebmuN latoTfo%
deelbagnivahrevefoyrotsiHseY 441 3.86
oN 76 7.13
)seibab3rofnwonknu(syad5.82=deelbtsriffoeganaeM
*deelbtsriffoetiS)lainarcartxE/lainarcartnI(daeH 22 3.51asocuMlarO 51 4.01noisicmucriC 44 6.03tnioJ 7 9.4noitcejniralucsumartnI 4 7.2nwonknU 5 5.3rehtO 74 6.23
tisivCDUtsalrohtribecnisdetropersdeelB
gnideelbfoetiS rebmuNegahrromeHlainarcartnI 41noisicmucriC 33lasaN/larO 75
etiSlacigruS/kcitSleeH/erutcnupineV 12amotameHeussiTtfoS 97amotameHralucsumartnI 03sucilibmU 2tnioJ 13lanitsetniortsaG 7laner,yraniruotineG 2
yranomluP 1gnideelboteudstceffemretgnoL 3
**tceffefoepyT :lacigolorueNlacoF 2redrosiDeruzieS 1ylahpecordyH 0emordnystnemtrapmocoteudyhtaporrueN 1sisylaraP 0
17UDC Report Vol. 8, No 1Vol
Table 12. Head injuries and intracranial hemorrhages (ICH) in children with hemophilia <2 years of age enrolled in UDC
*Percent is out of total number with head injuries** More than one choice is possible and percent is out of total number of ICHs
rebmuN latoTfo%tisivCDUtsalrohtribecnisseirujnidaeH
> 3 7 3.32 11 2.51 13 7.410 261 8.67
*erutcarflluksnignitluserseirujnidaehforebmuN 1 0.2
HCIforebmuN 41 6.6**HCIfoetiS
larberecartnI 5 7.63larudbuS 7 0.05
dionhcarabuS 2 3.41larudipE 1 1.7ralucirtnevirep/artnI 0 0.0rallebereC 1 1.7
**ybdemrifnocHCI
maxE 2 3.41yarX 0 0.0dnuosartlU 0 0.0IRM 1 1.7
TC 21 7.58enoN 0 0.0rehtO 0 0.0
I htiwdetaicossaHC **
yrevileD 6 9.24amuarT 2 3.41ainepotycobmorhT 0 0.0larudecorP 1 1.7
suoenatnopS 6 9.24rehtO 0 0.0

UDC Report Vol. 8, No 1Vol18
Table 13. Hepatitis B vaccination in children with hemophilia <2 years of age enrolled in UDC
Table 14. Central venous access devices (CVADs) in children with hemophilia < 2 years of age enrolled in UDC
*Percent is out of total number of babies with CVADs placed** Percent is out of total number of babies with complications
rebmuN latoTfo%
noitaniccavBsititapeHfosutatSseiresnoitaniccavcisabdetelpmoC 901 7.15
seiresnoitaniccavcisabgnivieceR 36 9.92sesodynadeviecerreveN 51 1.7
nwonknU 42 4.11
noitartsinimdafoetuoRralucsumartnI 05 7.32suoenatucbuS 93 5.81QSdnaMIhtoB 11 2.5
nwonknU 111 6.25
rebmuN latoTfo%
decalpDAVCenotsaeltahtiwseibaB 42 4.11**DAVCfoepyT troP 91 1.97
retehtaC 6 0.52CCIP 2 3.8
noitacilpmocDAVCenotsaeltahtiwseibaB**noitacilpmocfoepyT noitcefnI 8 0.08
submorhT 0 --
lacniahceM 3 0.03gnideelB 3 0.03
rehtO 0 --

19UDC Report Vol. 8, No 1Vol
Table 15. Prevalence of current inhibitors by titer* among children with hemophilia < 2 years of age enrolled in UDC
* Inhibitor titer is determined by the highest reported inhibitor titer for any visit. Low titer is defined as an inhibitor level of 0.5 - 5 Bethesda units (BU). High titer is defined as an inhibitor level of >5 BU.
AailihpomeH BailhpomeH
ytireveS rebmuN retitwoL retithgiH rebmuN retitwoL retiThgiH
dliM 92 0 000.00 0 00.00 5 0 00.00 0 00.00
etaredoM 43 )%8.8(3 0 00.00 42 )%2.4(1 0 .00
ereveS 59 )%5.9(9 )%3.6(6 42 )%2.4(1 )%2.4(1

UDC Report Vol. 8, No 1Vol20
Technical NotesEligibility RequirementsTo participate in UDC, patients must receivecare in a federally funded HTC and meet atleast one of the following criteria: (1) have ableeding disorder due to congenitaldeficiency or acquired inhibitors in which anyof the coagulation proteins is missing, re-duced, or defective and has a functional levelof less than 50 %; or (2) have a diagnosis bya physician of von Willebrand disease.Individuals specifically excluded fromparticipation in UDC include persons withany of the following: (1) an exclusivediagnosis of a platelet disorder,(2) thrombophilia, or (3) coagulation proteindeficiencies due to liver failure.
Data CollectionUDC data are collected during a participant's"annual visit", which ideally should occur onceeach calendar year (January-December),with the interval between visits as close aspossible to 12 months. However, partici-pants under 2 years of age are encouragedto be evaualated every 6 months until the ageof 2, and data are collected during thesevisits according to guidelines and definitionsdetailed in surveillance manuals provided toHTC staff by CDC. Demographic informationand reasons for refusal are obtained using apatient refusal form for all eligible people whodecline to participate. To protect patientconfidentiality, all data sent to CDC do notcontain personal identifying information, butrather use a unique 12-digit code that isgenerated by a computer software programsupplied to HTCs by CDC.
Eligible participants are registered into UDCthrough a registration form completed byHTC staff; information collected on this formincludes patient demographic, diagnostic,and historical information. Month and year of
birth are used to calculate age on the last dayof the current year. Information on race andethnicity is obtained from clinic records andmight be based either on self-report or onobservations made by care providers. Duringthe annual visit, clinical information is recorded on a standardized data collectionform (annual visit form or baby visit form). Forchildren under the age of two, informationabout their birth; diagnostic testing; site ofblood draw; the type of treatment (episodic vs.prophylactic); the presence and treatment ofinhibitors; the number of intracranial bleedingepisodes experienced; the type and brandname of all factor concentrates or other treat-ment products used; and whether or notclotting factor is infused at home is collected.Data are also recorded about the status ofvaccination against hepatitis B; and amongpatients with an intravenous access device,the occurrence of a device-associatedinfection.
All data collection forms are sent to CDCwhere they are then key entered into a data-base using double-entry software to minimizedata entry errors. Data are then screened foromissions, inconsistencies, and unusualvalues that possibly represent abstraction ordata-entry errors. Error reports are generatedand faxed to the HTC, where a designatedUDC contact uses available information toresolve discrepancies and complete missingdata items.
Laboratory TestingBlood specimens are not obtained fromparticipants under the age two, thus no labo-ratory testing is preformed.
Mortality ReportingDeaths occurring among all HTC patients

21UDC Report Vol. 8, No 1Vol
(regardless of whether they have beenenrolled in UDC) are reported to CDC using amortality form. Data collected include age atdeath, sex, race or ethnicity, type and severityof disease, and whether or not blood productshad been used during the year prior to death.Additionally, information about the death,including the date, cause (primary and con-tributing), and whether or not an autopsy wasperformed, is also collected.
Tabulation and Presentation of DataData in this report are provisional. The datarepresent the most current data available froman on-going surveillance project. Futurereports will include expanded data tables tocover subsequent surveillance periods andwill provide the results of more detailedanalyses of available data and findings fromspecial studies.

UDC Report Vol. 8, No 1Vol22
Acknowledgements
Region IAnn Forsberg M. A., M.P.H.New England Hemophilia Center Worcester, MAYale University School of Medicine New Haven, CTMaine Medical Center Scarborough, MEDartmouth Hitchcock Hemophilia Center Lebanon, NHRhode Island Hospital Providence, RIUCONN Hemophilia Treatment Center Farmington, CTVermont Regional Hemophilia Center Burlington, VTBoston Children's Hospital Boston, MA
Region IIMariam Voutsis, R.N., M.P.A.Weill Medical College of Cornell University New York, NYPuerto Rico Hemophilia Treatment Center San Juan, PRUMDNJ Robert Wood Johnson University Hospital, New Brunswick, NJSt. Michael's Comprehensive Hemophilia Care Center, Newark, NJThe Mary M. Gooley Hemophilia Center, Inc. Rochester, NYSUNY Health Science Center Adult Syracuse, NYSUNY Health Science Center Pediatric Syracuse, NYHemophilia Center of Western New York -Adult Buffalo, NY
We thank the Regional Coordinators (listed below in italics) of the federal HTC regions for theirassistance in the implementation and technical support of UDC. Data for this report werecollected by care providers in HTCs at the following institutions:
Hemophilia Center of Western New York -Pediatric Buffalo, NYThe Regional Comprehensive Hemophiliaand von Willebrand Treatment Center Albany, NYUHSH Blood Disorders Center Johnson City, NYLong Island Jewish Medical Center New Hyde Park, NYMount Sinai Medical Center New York, NYNewark Beth Israel Medical Center Newark, NJ
Region III Sue Cutter, M.S.W., M.P.A.Children's Hospital of Philadelphia Philadelphia, PAChildren's National Medical Center Washington, DCGeorgetown University Medical Center Washington, DCSt. Agnes Hospital Baltimore, MDUniversity of Virginia Hospital Charlottesville, VAVirginia Commonwealth University Richmond, VAChildren's Hospital of the King's Daughters Norfolk, VACardeza Foundation Hemophilia Center Philadelphia, PAChristiana Care Health Services Newark, DEHemophilia Center of Central Pennsylvania Hershey, PALehigh Valley Hospital Allentown, PA

23UDC Report Vol. 8, No 1Vol
Hemophilia Center of Western Pennsylvania Pittsburgh, PAWest Virginia University Medical Center Morgantown, WVCharleston Area Medical Center Charleston, WVJohns Hopkins University Medical Center Baltimore, MDChildren's Hospital of Philadelphia Specialty Center, Voorhees, NJPenn Comprehensive Hemophilia Program Philadelphia, PA
Region IV-NSteve Humes, M.P.H.Wake Forest University School of Medicine Winston Salem, NCNorton Kosair Children's Medical Center Louisville, KYBrown Cancer Center Louisville, KYMarkey Cancer Center Lexington, KYEast Carolina University Greenville, NCChildren's Hospital of Palmetto-RichlandMemorial Columbia, SCUniversity of Tennessee - Memphis Memphis, TNEast Tennessee Comprehensive HemophiliaCenter Knoxville, TNVanderbilt University Medical Center Nashville, TNUniversity of North Carolina at Chapel Hill Chapel Hill, NC
Region IV-SKaren Droze, M.S.Nemours Children's Clinic Jacksonville, FL
University of South Florida - Adult Tampa, FLMiami Comprehensive Hemophilia Center -Pediatrics Miami, FLUniversity of Florida Gainesville, FLChildren's Healthcare of Atlanta at ScottishRite Atlanta, GAMedical College of Georgia Adult Augusta, GAUniversity of Mississippi Medical Center Jackson, MSUniversity of Alabama Birmingham MedicalCenter Birmingham, ALMiami Comprehensive Hemophilia CenterAdult Miami, FLChildren's Rehabilitation Services Mobile, ALChildren's Rehabilitation Services Birmingham, ALEmory University Hemophilia Program Office Atlanta, GAChildren's Rehabilitation Services Opelika, ALChildren's Rehabilitation Services Huntsville, ALMedical College of Georgia Pediatrics Augusta, GA
Region V-E Tamara Wood-Lively, M.H.A., J.D.Children's Hospital of Michigan Detroit, MIMunson Medical Center Traverse City, MIHemophilia Clinic of West Michigan CancerCenter Kalamazoo, MI

UDC Report Vol. 8, No 1Vol24
Eastern Michigan Hemophilia TreatmentCenter Flint, MIDeVos Children's Hospital at Butterworth Grand Rapids, MIOhio State University Medical Center Columbus, OHCincinnati Children's Hospital Medical Center Cincinnati, OHUniversity of Cincinnati Medical Center Cincinnati, OHColumbus Children's Hospital Columbus, OHNorthwest Ohio Hemophilia Treatment Center Toledo, OHDayton Children's Medical Center Dayton, OHIndiana Hemophilia and Thrombosis Center Indianapolis, INMichigan State University ComprehensiveCenter for Bleeding Disorders East Lansing, MIAkron Children's Hospital Medical Center Akron, OHUniversity of Michigan Hemophilia TreatmentCenter Ann Arbor, MI
Region V-W Mary Anne Schall, R.N., M.S.Northwestern University Chicago, ILCook County Hospital Adult Chicago, ILChildren's Memorial Hospital Chicago, ILComprehensive Bleeding Disorders Center Peoria, ILFairview University Medical Center Minneapolis, MNMayo Clinic Rochester, MN
MeritCare Hospital DBA Roger Maris Cancer Center, Fargo, NDHemophilia Outreach Centre Green Bay, WIGunderson Clinic LaCrosse, WIAmerican Red Cross Badger Chapter Madison, WIRush Children's Hospital Chicago, ILMichael Reese Hospital - Adult Chicago, ILSouth Dakota Children's Specialty Clinics Sioux Falls, SDComprehensive Center for Bleeding Disor-ders Milwaukee, WICook County Children's Hospital Chicago, IL
Region VI John Drake, R.N., M.S.N.Gulf States Hemophilia and ThrombosisCenter Houston, TXLouisiana Comprehensive Hemophilia Center New Orleans, LAHemophilia Center of Arkansas Little Rock, AROklahoma Comprehensive Hemophilia Treatment Center, Oklahoma City, OKFort Worth Comprehensive HemophiliaCenter Ft. Worth, TXNorth Texas Comprehensive HemophiliaCenter - Adult Program Dallas, TXSouth Texas Comprehensive HemophiliaCenter San Antonio, TXNorth Texas Comprehensive HemophiliaCenter - Pediatric Program Dallas, TX

25UDC Report Vol. 8, No 1Vol
Region VIIBecky Dudley, L.C.S.W.University of Iowa Hospitals and Clinics Iowa City, IAKansas City Regional Hemophilia Center Kansas City, MONebraska Regional Hemophilia TreatmentCenter Omaha, NEMissouri/Illinois Regional Hemophilia Center St. Louis, MOCenter for Bleeding and Thrombotic Disor-ders St. Louis, MOHemophilia Treatment Center Columbia, MO
Region VIIIBrenda Riske, M.S., M.B.A., M.P.A.Mountain States Regional Hemophilia andThrombosis Center Denver, COTed R. Montoya Hemophilia Center Albuquerque, NMMountain States Regional Hemophilia Center Tucson, AZPhoenix Children's Hospital Phoenix, AZMountain States Regional Hemophilia Center- Utah Salt Lake City, UT
Region IXJudith Baker, M.H.S.A.Children's Hospital of Los Angeles Los Angeles, CAUniversity of California San Diego, CALucile Salter Packard Children's Hospital atStanford Palo Alto, CAAlta Bates Medical Center Berkeley, CA
Hemophilia and Thrombosis Center of Hawaii Honolulu, HIUniversity of California at Davis Sacramento, CAUniversity of California, San Francisco San Francisco, CAOrthopaedic Hospital of Los Angeles Los Angeles, CAChildren's Hospital, San Diego San Diego, CAChildren's Hospital of Orange County Orange, CAChildren's Hospital Oakland Oakland, CACity of Hope National Medical Center Duarte, CAGuam Comprehensive Hemophilia Care Program, Agana, GUValley Children's Hospital Madera, CAHemophilia and Thrombosis Center of LasVegas Las Vegas, NV
Region X Robina Ingram-Rich, R.N., M.S., M.P.H.Puget Sound Blood Center and Program Seattle, WAOregon Hemophilia Treatment Center Portland, ORAlaska Hemophilia Association Anchorage, AKIdaho Regional Hemophilia Center Boise, ID

UDC Report Vol. 8, No 1Vol26
Tom Abshire. M.D. Atlanta, GARandall Curtis, M.B.A Berkeley, CAJohn Drake, R.N., M.S.N. Houston, TXNancy Duffy, R.N. Dayton, OHAngela Forsyth, M.S., P.T. Philadelphia, PA
We would also like to acknowledge the assistance of the membersof the UDC Working Group
Nigel Key, M.D., F.R.C.P Chapel Hill, NCEdward Kuebler, M.D. Houston, TXBarbara Konkle, M.D. Philadelphia, PARoshni Kulkarni, M.D. Atlanta, GABrenda Nielson, R.N., M.S.N. Chapel Hill, NCClaire Phillipp, M.D. New Brunswick, NJ

27UDC Report Vol. 8, No 1Vol
Region X Region VIII Region V- WestRegion V- East
Region I
Region II
Region III
Region IV- North
Region IV- South
Region VI
Region IX
Region VII
Hemophilia Treatment Center Regions
**
**
***
*
*
*
*
*
Hawaii & Guam Region IX
Puerto Rico & Virgin Is. Region II
Department of Health and Human ServicesDepartment of Health and Human ServicesDepartment of Health and Human ServicesDepartment of Health and Human ServicesDepartment of Health and Human ServicesCenters for Disease Control and PreventionCenters for Disease Control and PreventionCenters for Disease Control and PreventionCenters for Disease Control and PreventionCenters for Disease Control and Prevention
*Location of regional core center.