Report on Formative Research Findings - Fight … on Formative Research Findings This report has...
135
Transcript of Report on Formative Research Findings - Fight … on Formative Research Findings This report has...
Report on Formative Research Findings
This report has been developed under the project entitled “Improving household decision-making for the management of Pediatric pneumonia in Uttar Pradesh and Bihar” funded by Bill and Melinda Gates Foundation (Global Health Grant No: OPP1093327).
We are extremely grateful to the Bill and Melinda Gates Foundation who provided us with an opportunity to carry on this research. We would like to acknowledge with gratitude the functionaries and academicians of King George`s Medical University who facilitated the smooth conduction of this project since inception. We are also thankful to the health functionaries of the Department of Health and Family Welfare, GoUP, NRHM, Uttar Pradesh and State Health Society, Bihar without whose cooperation this project would not have accomplished its objective. We are extremely thankful to all the Chief Medical Officers, Chief Superintendents and Medical Officers-in charge of the project blocks who cooperated with the project team in every possible aspect. We also wish to extend our gratitude to all respondents from the community-mother, father and grandmother-who shared with us their opinions, perceptions, thoughts and beliefs related to pneumonia. It helped us to understand the dynamics of health seeking behavior and to identify the delays in health care seeking which need to be addressed in future public policies/programs on childhood pneumonia. This research also benefitted from the technical guidance provided by the members of Childhood Pneumonia Behavior Change Communication Committee Group (CPBCCCG) group during the group meetings. We wish to thank all the members of the consultative group for endorsing and providing handholding support to this project.
Members of Childhood Pneumonia Behavior Change Communication Committee (CPBCCCG):
Dr. Gaurav Kumar-National Health Society (Bihar), Dr. Aruna Narain- NRHM (U.P.), Dr. Hari Om Dixit-NRHM (U.P.), Dr. Anil Verma-NRHM, (U.P.), Prof. Sanjata R. Chaudhary-Deptt. of Pediatrics, Patna Medical College & Hospital, Dr. Neeraj Agrawal-Deptt. of Community Medicine, AIIMS (Patna), Prof. J.V. Singh, Director-U.P. Rural Institute of Medical Sciences & Research, (Saifai), Dr. Chitranjan Roy-Deptt. of Community Medicine, Darbhanga Medical College (Laheriasarai Bihar), Dr. Shraddha Dwivedi-Deptt. of Community Medicine, Motilal Nehru Medical College, (Allahabad), Prof. Uday Mohan-Deptt. of Community Medicine, KGMU, (Lucknow), representative from Bill & Melinda Gates Foundation, representative from Rajiv Gandhi Mahila Vikas Pariyojna, representative from UNICEF, Lucknow, representative from Clinton Access Foundation, representative from FHI 360, representative from IIPH- Delhi,
representative from ICDS, Lucknow and team from project subgrantee-Point Blank Advertising Pvt. Ltd., Mumbai.
Acknowledgement
Report on Formative Research Findings
Project Investigators
Principal Investigator: Prof. Shally Awasthi, Department of Pediatrics, KGMU, Lucknow.
Co-Investigator: Dr. Monika Agarwal, Department of Community Medicine, KGMU, Lucknow.
Consultants
Prof. Mark Nichter: Public Health and Family Medicine, University of Arizona, USA
Dr. Neeraj Mohan Srivastava : Knowledge Consultant, UNICEF, Uttar Pradesh.
Data Collection and Analysis:
Dr. Anant Prakash Mishra Project Coordinator
Ms. Tuhina Verma Social Scientist
Mr. Gulshan Sami Social Scientist
Mr. Ram Dhani Sharma Community Interviewer
Mr. Ranjan Khare Community Interviewer
Mr. Vijay Verma Community Interviewer
Mr. Manish Pandey Community Interviewer
Mr. Vineet Shukla Field Assistant
Mr. Sushil Kumar Field Assistant
Mr. Atul Chandra Secretarial Assistance
Mr. Hasib-ur- Rehman Data Manager
Ms. Shobha Pandey Translator
Report Writing: Prof. Shally Awasthi , Ms. Tuhina Verma and Mr. Gulshan Sami
Design and layout: Mr. Hasib-ur- Rehman and Mr. Atul Chandra
Note: Pictures used in this report have been exclusively taken for this project. The respondents have given written informed consent for use of these photographs in this report.
Project Team
Report on Formative Research Findings
S. No. Contents Page No.
1. Executive Summary 1 2. Introduction
2.1 Socio-Demographic and Health Profile of Project Area 2.2. Project Background & Goal Study Rationale Project Goal and Objectives Geographic Focus Ethical Compliance 2.3 Preparation for Data Collection
Video clippings on Childhood Respiratory Illness Vignettes Development & Pilot Testing of formative tools Themes for Data Collection in Formative Research Tools Team formation and Training
5 10 11 12 12 13 13 15 18
3. Methodology 3.1 Data Collection
Selection of districts Selection of blocks and sub-centers
3.2 Study Respondents and Eligibility Criteria Respondents for Key informant interviews Respondents for Semi structured interviews Respondents for Focus group discussion interviews
3.3 Data Management & Analysis Data Management Data Analysis
21 23 24 26 27 31 31
4. Results 4.1 Background characteristics of the respondents 4.2 Recognition of Common Childhood Illnesses 4.3 Local Terms for Pneumonia & Symptoms of Pneumonia 4.4 Home Remedies and Self Medication 4.5 Decision Making Process 4.6 Health Care Seeking Behavior 4.7 Community Health Worker 4.8 Rural Medical Practitioner
33 44 55 58 66 71 96 109
5 Emerging Themes and Conclusion 5.1 Message Domain 1: Symptoms recognition 5.2 Message Domain 2: Where and when to seek health care 5.3 Message Domain 3: How approach a Health Care Provider and negotiate for quality of care 5.4 Message Domain 4: Risk vulnerability perception
6. Recommendations and further research priorities
116 117 118 119 120
7 References 121 8 Maps
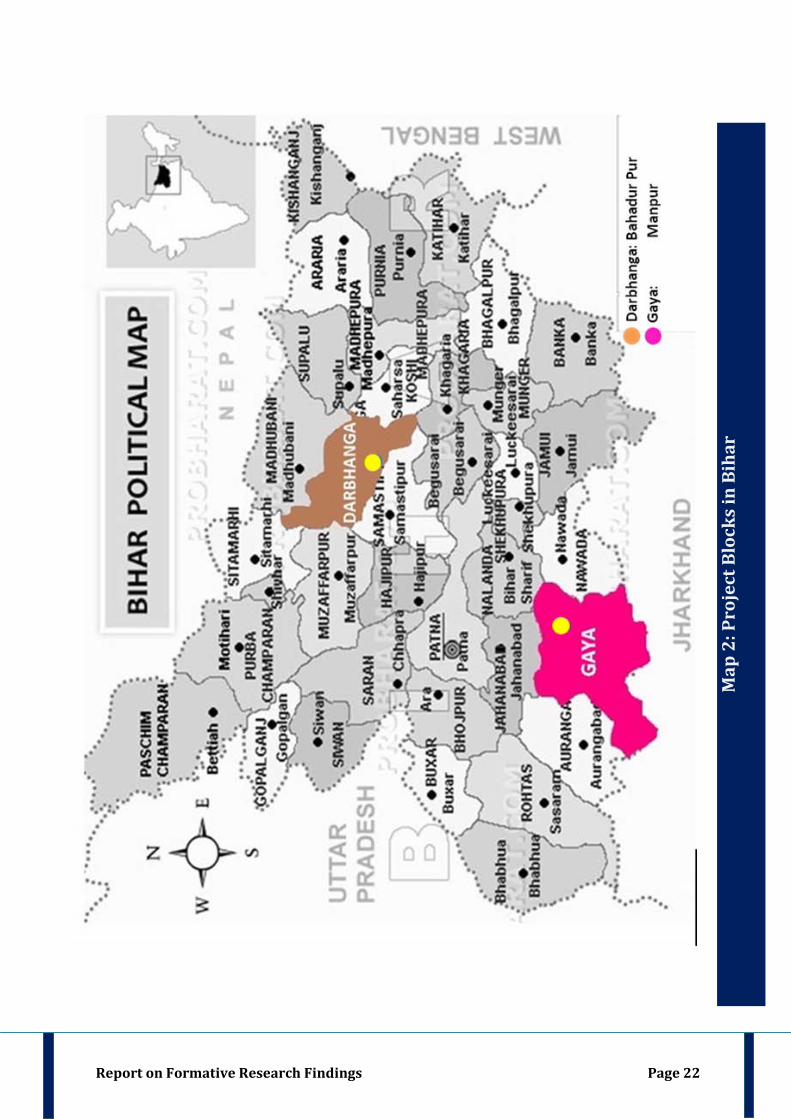
Map 1: Project Blocks in Uttar Pradesh Map 2: Project Blocks in Bihar
21 22
Table of Contents
Report on Formative Research Findings
9. LIST OF TABLES Table 1: Demographic & Health Profile Uttar Pradesh & Bihar Table 2: Rural Health Care Facilities and manpower in Uttar Pradesh and Bihar Table 3: Infrastructure available at the Rural Health Care Facilities in U.P. & Bihar Table 4: Population and Literacy rate in Project Districts Table 5: Infant Mortality Rates and Birth Indicators in Project Districts Table 6: Availability of Public Health Facilities and ASHAs in the Project Districts Table 7: Project Geographic Area and dialects spoken in that area Table 8: Training Sessions and Trainers Table 9: Eligibility Criteria for Caregivers of Key Informant Interview Table 10: Eligibility Criteria for Care providers of Key Informant Interview Table 11: Eligibility Criteria for Caregivers of Semi Structured Interview Table 12: Group and participant characteristic of Caregiver and Care provider Table 13: Frequency of responses obtained against each code and the standard term used
in this report Table 14: Field Schedule of the Data Collection Team Table 15: Number of Interviews/Discussions Conducted In Each State Table 16: Number of respondents in each interview/discussion Table 17: Median age of the Caregivers Table 18: Religion and Caste of the caregivers Table 19: Family Size and Family Type of the caregivers Table 20: Education and Occupation of the Caregivers Table 21: Sources of Information available with the Caregivers Table 22: Signs or Symptoms of Pneumonia Table 23: Caregivers Reporting of Signs of Severe Pneumonia & IMNCI Danger Signs Table 24: Terms for Pneumonia in Local Dialect Table 25: Terms/Phrases on signs / symptoms of Pneumonia in local dialect Table 26: Popular Home remedies used in project districts that are applied topically Table 27: Popular Home remedies used in project districts that are given orally Table 28: Popular Home remedies used in project districts that are applied topically and
given orally Table 29: Unique Home Remedies used in project Districts Table 30: Caregiver`s comparative of Village Based Doctor vs. Block Based Private
Doctor Table 31: Baseline Characteristics of Community Health Workers –Key Informant Table 32: Religion and Caste of Community Health Worker Table 33: Family Structure and Family Size of CHW Table 34: Educational status of CHW Table 35: Breathing Type Reported In Common Respiratory Illness. Table 36: Baseline Characteristics of RMP Table 37: Prescription pattern of RMP LIST OF FIGURES Fig. 1: Formative Research Techniques used in this project Fig. 2: Eligibility Criteria for Key Informant Interviews Fig. 3: Eligibility Criteria for Semi Structured Interviews Fig. 4: Eligibility Criteria for Focus Group Discussion Fig. 5: Relationship of Caregivers with the child Fig 6: Religion of the caregivers Fig 7: Caste of the caregivers Fig. 8: Family Type of the Caregivers Fig. 9: Family Size of the caregivers Fig. 10: Education of the Caregivers Fig. 11: Occupation of the respondents Fig. 12: Sources of information in Caregivers Family Fig. 13: Common Childhood Illnesses as reported by caregivers in Key Informant
interviews Fig. 14: Common Childhood Illnesses as reported by caregivers in Semi Structured
interviews
5 6 7 8 9 9 12 19 24 25 26 27 32 33 34 34 36 36 38 40 43 48 50 55 57 59 60 62 62 87 97 99 100 101 103 109 113 14 25 27 28 35 37 37 38 39 41 42 43 44 45
Report on Formative Research Findings
Fig. 15: Common Respiratory Illnesses as reported by caregivers in Key Informant interviews
Fig. 16: Common Respiratory Illnesses as reported by caregivers in Semi Structured interviews
Fig. 17: Breathing Pattern in Pneumonia as reported by caregivers in Key Informant interviews
Fig. 18: Breathing Pattern in Pneumonia as reported by caregivers in Semi Structured interviews
Fig. 19: Reported Danger Signs of Respiratory Illnesses in Key Informant Interviews Fig. 20: Reported Danger Signs of Respiratory Illnesses in Semi Structured Interviews Fig. 21: Signs and Symptoms of Pneumonia in Vignette I Fig. 22: Signs and Symptoms of pneumonia in Vignette II Fig. 23: Signs and Symptoms of pneumonia in Vignette III Fig. 24: Local Names of Pneumonia Fig. 25: Unique Home Remedies of Uttar Pradesh & Bihar Fig. 26: Primary Decision Maker as Reported by Younger Caregivers of Key Informant
Interviews Fig. 27: Primary Decision Maker as Reported by Older Caregivers of Key Informant
Interviews Fig. 28: Primary Decision Maker in Semi Structured Interviews Fig. 29: Health Care Seeking Pattern Reported by Respondents of Key Informant
Interviews in Scenario I Fig. 30: Health Care Seeking Pattern Reported by Respondents of Semi structured
Interviews in Scenario I Fig. 31: Health Care Seeking Pattern Reported by Respondents of Key Informant
Interviews in Scenario II Fig. 32: Health Care Seeking Pattern Reported by Respondents of Semi structured
Interviews in Scenario II Fig. 33: Health Care Seeking Pattern Reported by Respondents of FGD in Scenario II Fig. 34: Health Care Seeking Pattern Reported by Respondents of Key Informant
Interviews in Scenario III Fig. 35: Health Care Seeking Pattern Reported by Respondents of Semi structured
Interviews in Scenario III Fig. 36: Health Care Seeking Pattern Reported by Respondents of Focus Group
Discussions in Scenario III Fig 37: Duration of illness of cases till the date of interview Fig. 38: Choice of Health Care Providers based on 30 Cases from Uttar Pradesh and Bihar Fig. 39: Religion of the CHW Fig. 40: Caste of the CHW`s Fig. 41: Family Structure of CHW Fig. 42: Level of Education of the CHW`S Fig. 43: Common Childhood Illnesses as reported by CHW`s Fig. 44: Common Respiratory Illnesses as reported by CHW`s Fig. 45: Breathing Type in Pneumonia reported by CHW`s Fig. 46: Breathing Type in Cold/Flu/Congestion reported by CHW`s Fig. 47: Symptoms considered as danger signs Fig. 48: Common Childhood Illness as reported by RMP`s Fig. 49: Common Respiratory Illness as reported by RMP`s Fig. 50: Breathing Type - in Common Cold/Flu/Congestion as reported by RMP`s Fig. 51: Breathing Type - in Pneumonia as reported by RMP`s Fig. 52: Symptoms Considered As Danger Signs as reported by RMPs
45 46 47 47 49 50 51 52 53 56 64 66 67 67 72 73 75 76 77 79 80 81 83 85 99 99 100 101 102 103 104 104 105 110 111 111 111 112
Report on Formative Research Findings
1. Accredited Social Health Activists ASHAs
2. Acute Lower Respiratory Infection ALRI
3. Bachelor of Ayurvedic Medicine and Surgery B.A.M.S.
4. Block Based Private Doctor BBD
5. Chief Medical Officer CMO
6. Chief Medical Superintendent CMS
7. Community Health Centre CHC
8. Community Health Worker CHW
9. Health Education Officer H.E.O
10. Health worker (Male) HW(Male)
11. Integrated Management of Neonatal and Childhood Illness IMNCI
12. King George’s Medical University KGMU
13. National Family Health Survey NFHS
14. Other Backward Class OBC
15. Scheduled Caste SC
16. Scheduled Tribe ST
17. Village Based Rural Medical Practitioner RMP
Acronyms
Report on Formative Research Findings
Report on Formative Research Findings Page 1
Background:
In 2005, 2.3 million deaths were reported in children less than 5 years of age, and between ages of 1
month to 5 years, half of them were due to pneumonia or diarrhea, attributable to delayed
recognition of illness by families, delayed and poor access to qualified health care in a setting which
has untested home and traditional remedies for such illnesses and faith in incompetent and
unqualified rural medical practitioners in a background of high prevalence of under nutrition,
overcrowding, exposure to ambient air pollutants as a result of use of biomass fuel for cooking and
second hand smoke and low rates of immunization etc.
Hypothesis: Community empowerment for prompt recognition of childhood pneumonia,
understanding its severity and vulnerability of their child to adverse outcome due to delayed
qualified care seeking is possible by development of appropriate messages by in-depth formative
analysis of community constraints in real life and possibly diverse settings.
Goal: To create communications materials to improve household decision making when confronted
by lower respiratory illness in children in northern India.
Objective: One of the objectives of this project was to conduct formative research to assess
community perceptions about symptoms of pneumonia, care seeking behaviour and risk
vulnerability due to it. This report presents the findings of formative research of this Objective.
Settings: Since there are multiple dialects in Uttar Pradesh and Bihar, this formative research work
was done in dialect specific rural village settings as well as in the corresponding Primary Health
Centre (PHC) and Community Health Centre (CHC) of 7 districts of Uttar Pradesh and Bihar. The
project districts and the dialects spoken in each district were Lucknow (Awadhi), Gorakhpur
(Bhojpuri), Mahoba (Bundelkhandi), Agra (Braj) and Meerut (Khari Boli) in Uttar Pradesh and
Gaya (Maghai) and Darbhanga (Maithali) in Bihar.
Methods: Key Informant interviews, semi-structured interviews and focus group discussions were
used to collect information. Interview/discussion guides were prepared in English and Hindi. Case
studies that were collected as a part of another objective of this project were used to create vignettes.
These vignettes were used in interviews and focus group discussions probing decision making and
health care seeing behavior. Real life video clippings on a range of mild to severe ARI in children
under 5 years were shot. Three of these video clippings were used in focus group discussions
(n=42) with stakeholders across 7 districts to ascertain what signs were recognized and how serious
they were considered. All data collection guides were designed to collect information on taxonomy
of terms used for childhood pneumonia and pneumonia like presentations, perceptions of disease
Report on Formative Research Findings Page 2
severity, factors influencing health care seeking and choice of health care provider. Attempt was
made to elicit responses to various case scenarios and collect information on home remedies and
self-medication. Data was transcribed and translated into English. Codebook was developed for
coding and data interpretation. Themes were analyzed under each of the following four domains (a)
symptom recognition (b) where and when to seek treatment (c) how to approach a care provider and
negotiate for quality of care (d) risk vulnerability perception. These emerging themes gave insight
to the concepts for message development.
Findings: 43 Key informant interviews, 42 Semi-structured interviews and 42 Focus group
discussions were conducted in seven districts of Uttar Pradesh and Bihar. We recruited 303
caregivers and 75 care providers between October 2013 - January 2014. Among these 215/303 (70.9
%) caregivers and 58/75 (77.3%) care providers were from Uttar Pradesh and the rest were from
Bihar. The caregivers comprised of younger and older caregivers and fathers. The care providers
comprised of Community Health Worker (CHW) and Village Based Rural Medical Practitioner
(RMP). Baseline characteristics of the caregivers showed that 91.7% caregivers followed Hindu
religion while 7.9% followed Muslim religion. About 35.97 % caregivers identified themselves as
belonging to Other Backward Class (OBC) and almost a similar percentage (35.31%) identified
themselves as belonging to Scheduled Caste (SC). 23.10% belonged to General Category while the
rest belonged to Scheduled Tribe (ST). 53.80% belonged to single/nuclear family while 46.20%
belonged to joint family. 56.11 % respondents had family size of 6-10 members. Almost one-third
(31.35 %) caregivers were illiterate and 72.61 % caregivers were housewives. Information was
collected from the study participants on the availability of means of communication in their
household like mobile, newspaper, television without satellite network, television with satellite
network, radio. Mobile was the most popular source of information among the caregivers followed
by information obtained from other persons like neighbors/relatives in community. Radio was least
popular.
Sixty-seven CHWs participated in this study. Among these 77.61% (52/67) were from U.P. while
22.38% (15/67) were from Bihar. Sixty CHW`s participated in FGD`s while seven were a part of
key informant interviews. Out of the 60 CHWs who participated in focus group discussion, 95%
(57/60) were Hindus and 48.94 % (23/47) belonged to general category. 53.33% (32/60) CHW`s
belonged to nuclear family and 51.67% (31/60) had a family size of 0-5 members. Almost half 45%
(27/60) of the CHWs who participated in discussion were educated up to intermediate level. Eight
RMP`s were included for the interview. The youngest RMP was 33 years while the oldest one was
65 years. RMP practicing in Gaya was most experienced with 35 years of practice. The qualification
Report on Formative Research Findings Page 3
of only 3 RMPs were known while the qualifications of rest of them were unknown. Qualified
RMPs identified themselves as Bachelor of Ayurvedic Medicine and Surgery (B.A.M.S.).
Domain 1: Symptom Recognition: It was found that caregivers universally knew the term
‘pneumonia’ but did not know what the term “pneumonia” stands for & the risks associated with it.
Fast breathing as a symptom of pneumonia was not recognized universally. The caregivers
recognized chest in-drawing and fast breathing only when it was accompanied by chest in-drawing.
They were unable to appreciate signs of severe pneumonia like altered sensorium or audible sounds
like grunting and groaning when it appeared in our video clippings. The caregivers had no concept
of viewing the chest to observe respiratory rate. Interestingly, fever in isolation was not considered
as a symptom of respiratory illness. The caregivers missed the early stage of pneumonia when only
fast breathing was present. It led to delayed disease recognition.
Theme for Message Development (Domain 1)
Caregivers should be made aware that Fast Breathing is an early symptom and Chest in drawing is a
relatively late symptom of pneumonia. Chest exposure for thorough inspection should be done at
home in children with cough/cold.
Domain 2: Where and When to Seek Health Care: Caregivers/providers choose health care
facilities according to perceived severity of illness. There is an informal triage at community level.
The caregivers chose either to `wait & watch` or visit traditional healer or visit a RMP for a child
perceived as “less sick”. When the child was perceived to be “more sick” caregivers preferred to
visit a Block Based Private Doctor (BBD) more than RMP. The BBD or a Private Hospital at the
main block was preferred more for the child perceived to be “very sick child”. The Govt. Hospital
was least preferred for a child in similar condition because of the distrust of the community in the
public health system.
Theme for Message Development (Domain 2)
Early care seeking should be promoted. Faith of the community in Government Health System needs
to be strengthened. Caregivers must be made aware that care seeking from RMP for pneumonia
leads to delay which in turn can lead to prolonged illness and increased cost of treatment. They must
also be taught to closely look for fast breathing and chest in drawing and danger signs in their sick
child so that care seeking can be sought as early as possible.

Report on Formative Research Findings Page 4
Domain 3: How to Approach a Care Provider & Recognize for Quality of Care: Caregivers
were not concerned about the qualifications of a doctor as long as s/he had a good reputation in the
community. There was no concept of correct quality of care and perhaps the community was not
empowered/educated to recognize quality of care. They chose the RMP who was not usually
qualified. BBD was mostly qualified but such qualified doctors charge five times more fees than
RMP. BBD`s did not dispense medicines like the RMP but prescribed medicines and investigations.
RMP was available 24/7 and mothers would feel free to visit them even unaccompanied without
much decision making. There was no concept of “course of treatment” among caregivers. They were
told about feeding and diet changes during sickness. Community felt satisfied when the provider
reinforced the belief that pneumonia is caused by “cold”. Caregivers were not advised to monitor the
course of pneumonia. Doctors did not tell them about: (a) how to look for improvement or
deterioration (b) how long to wait while taking prescribed treatment & (c) where to go when
condition worsens
Theme for Message Development in (Domain 3)
Caregivers must be taught to ask the doctor about visible symptoms of improvement and for how
long to wait and where to go when the disease worsens.
Domain 4: Risk Vulnerability Perception: Caregivers were not able to report all WHO-IMNCI
Danger Signs. Only few respondents self-reported ‘refusal to feed’ and excessive crying, lethargy
and unconsciousness/seizures. Additional symptoms like fever, cold, coughing were reported as
Danger Signs much more than WHO-IMNCI Danger Signs. Caregivers did not knew that fever
alone is not an indicative of disease progression or improvement. They also were unaware that
maternal cough/cold can be self-limiting however a child with similar symptoms can progress to
fatal pneumonia. In addition, caregivers were unaware that children with cough/cold can have
different outcomes in same child or in different children.
Theme for Message Development (Domain 4)
Some children with ‘cough/common cold’ can progress to life-threatening pneumonia. Most of them
have self-limiting disease. Therefore, it was important to watch for early signs of pneumonia.

Report on Formative Research Findings Page 5
Report on Formative Research Findings Page 5
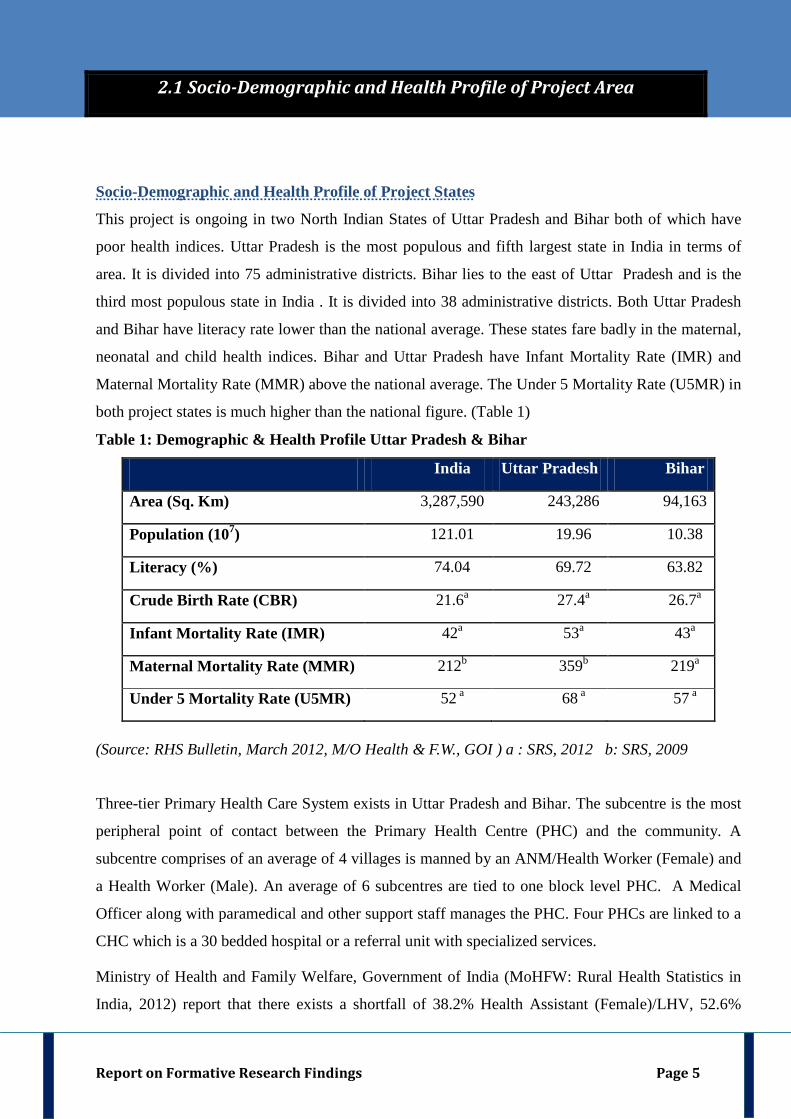
Socio-Demographic and Health Profile of Project States
This project is ongoing in two North Indian States of Uttar Pradesh and Bihar both of which have
poor health indices. Uttar Pradesh is the most populous and fifth largest state in India in terms of
area. It is divided into 75 administrative districts. Bihar lies to the east of Uttar Pradesh and is the
third most populous state in India . It is divided into 38 administrative districts. Both Uttar Pradesh
and Bihar have literacy rate lower than the national average. These states fare badly in the maternal,
neonatal and child health indices. Bihar and Uttar Pradesh have Infant Mortality Rate (IMR) and
Maternal Mortality Rate (MMR) above the national average. The Under 5 Mortality Rate (U5MR) in
both project states is much higher than the national figure. (Table 1)
Table 1: Demographic & Health Profile Uttar Pradesh & Bihar
India Uttar Pradesh Bihar
Area (Sq. Km) 3,287,590 243,286 94,163
Population (107 121.01 ) 19.96 10.38
Literacy (%) 74.04 69.72 63.82
Crude Birth Rate (CBR) 21.6 27.4a 26.7a a
Infant Mortality Rate (IMR) 42 53a 43a a
Maternal Mortality Rate (MMR) 212 359b 219b a
Under 5 Mortality Rate (U5MR) 52 68 a 57 a a
(Source: RHS Bulletin, March 2012, M/O Health & F.W., GOI ) a : SRS, 2012 b: SRS, 2009
Three-tier Primary Health Care System exists in Uttar Pradesh and Bihar. The subcentre is the most
peripheral point of contact between the Primary Health Centre (PHC) and the community. A
subcentre comprises of an average of 4 villages is manned by an ANM/Health Worker (Female) and
a Health Worker (Male). An average of 6 subcentres are tied to one block level PHC. A Medical
Officer along with paramedical and other support staff manages the PHC. Four PHCs are linked to a
CHC which is a 30 bedded hospital or a referral unit with specialized services.
Ministry of Health and Family Welfare, Government of India (MoHFW: Rural Health Statistics in
India, 2012) report that there exists a shortfall of 38.2% Health Assistant (Female)/LHV, 52.6%
2.1 Socio-Demographic and Health Profile of Project Area
Report on Formative Research Findings Page 6
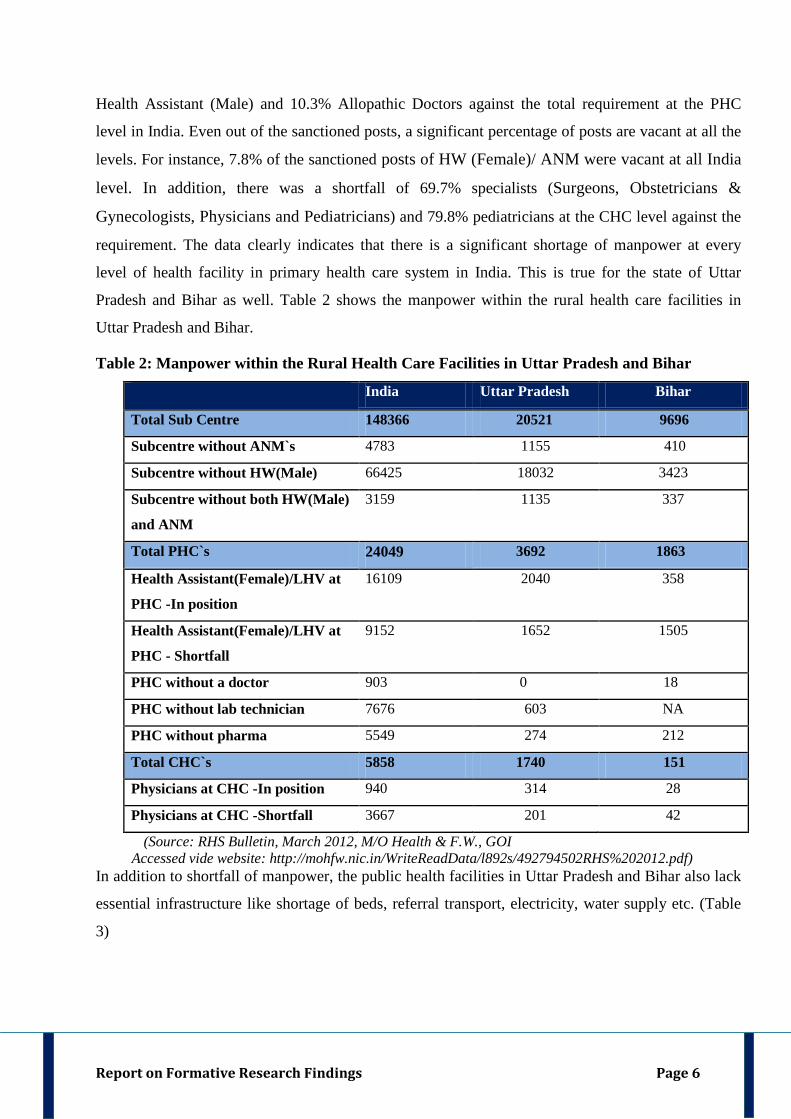
Health Assistant (Male) and 10.3% Allopathic Doctors against the total requirement at the PHC
level in India. Even out of the sanctioned posts, a significant percentage of posts are vacant at all the
levels. For instance, 7.8% of the sanctioned posts of HW (Female)/ ANM were vacant at all India
level. In addition, there was a shortfall of 69.7% specialists (Surgeons, Obstetricians &
Gynecologists, Physicians and Pediatricians) and 79.8% pediatricians at the CHC level against the
requirement. The data clearly indicates that there is a significant shortage of manpower at every
level of health facility in primary health care system in India. This is true for the state of Uttar
Pradesh and Bihar as well. Table 2 shows the manpower within the rural health care facilities in
Uttar Pradesh and Bihar.
Table 2: Manpower within the Rural Health Care Facilities in Uttar Pradesh and Bihar
India Uttar Pradesh Bihar
Total Sub Centre 148366 20521 9696
Subcentre without ANM`s 4783 1155 410
Subcentre without HW(Male) 66425 18032 3423
Subcentre without both HW(Male)
and ANM
3159 1135 337
Total PHC`s 24049 3692 1863
Health Assistant(Female)/LHV at
PHC -In position
16109 2040 358
Health Assistant(Female)/LHV at
PHC - Shortfall
9152 1652 1505
PHC without a doctor 903 0 18
PHC without lab technician 7676 603 NA
PHC without pharma 5549 274 212
Total CHC`s 5858 1740 151 70
Physicians at CHC -In position 940 314 28
Physicians at CHC -Shortfall 3667 201 42
(Source: RHS Bulletin, March 2012, M/O Health & F.W., GOI Accessed vide website: http://mohfw.nic.in/WriteReadData/l892s/492794502RHS%202012.pdf)
In addition to shortfall of manpower, the public health facilities in Uttar Pradesh and Bihar also lack
essential infrastructure like shortage of beds, referral transport, electricity, water supply etc. (Table
3)
Report on Formative Research Findings Page 7
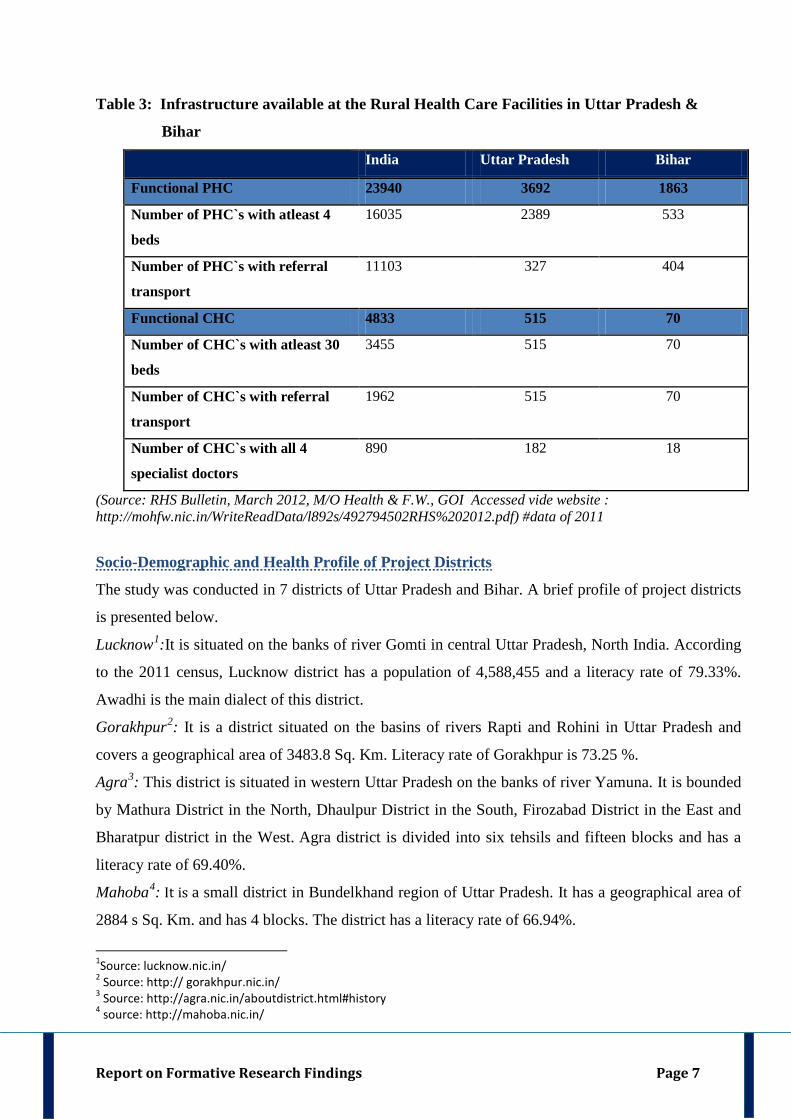
Table 3: Infrastructure available at the Rural Health Care Facilities in Uttar Pradesh &
Bihar
India Uttar Pradesh Bihar
Functional PHC 23940 3692 1863
Number of PHC`s with atleast 4
beds
16035 2389 533
Number of PHC`s with referral
transport
11103 327 404
Functional CHC 4833 515 70
Number of CHC`s with atleast 30
beds
3455 515 70
Number of CHC`s with referral
transport
1962 515 70
Number of CHC`s with all 4
specialist doctors
890 182 18
(Source: RHS Bulletin, March 2012, M/O Health & F.W., GOI Accessed vide website : http://mohfw.nic.in/WriteReadData/l892s/492794502RHS%202012.pdf) #data of 2011
Socio-Demographic and Health Profile of Project Districts
The study was conducted in 7 districts of Uttar Pradesh and Bihar. A brief profile of project districts
is presented below.
Lucknow1
Gorakhpur
:It is situated on the banks of river Gomti in central Uttar Pradesh, North India. According
to the 2011 census, Lucknow district has a population of 4,588,455 and a literacy rate of 79.33%.
Awadhi is the main dialect of this district. 2
Agra
: It is a district situated on the basins of rivers Rapti and Rohini in Uttar Pradesh and
covers a geographical area of 3483.8 Sq. Km. Literacy rate of Gorakhpur is 73.25 %. 3
Mahoba
: This district is situated in western Uttar Pradesh on the banks of river Yamuna. It is bounded
by Mathura District in the North, Dhaulpur District in the South, Firozabad District in the East and
Bharatpur district in the West. Agra district is divided into six tehsils and fifteen blocks and has a
literacy rate of 69.40%. 4
1Source: lucknow.nic.in/ 2 Source: http:// gorakhpur.nic.in/ 3 Source: http://agra.nic.in/aboutdistrict.html#history 4 source: http://mahoba.nic.in/
: It is a small district in Bundelkhand region of Uttar Pradesh. It has a geographical area of
2884 s Sq. Km. and has 4 blocks. The district has a literacy rate of 66.94%.
Report on Formative Research Findings Page 8
Meerut5: Meerut district is a part of Meerut division in Uttar Pradesh. According to the 2011 census,
Meerut district has a population of 3,447,405 and a literacy rate of 74.80%, higher than the state
average of 69.72%. The child sex ratio of Meerut is 850, lower than the state average of 899.
(
Gaya
"Census of India 2011 – Provisional Population Totals – Uttar Pradesh – Data Sheet" ) 6
Darbhanga
: Gaya District lies in the Magadh Division in Bihar. The district has a common boundary
with the state of Jharkhand to the south. In 2006, the Ministry of Panchayati Raj named Gaya one of
the country's 250 most backward districts. 7: Darbhanga district of Bihar has a geographic area of 2279 sq. km. It is bounded on the
north by Madhubani district, on the south by Samastipur district, on the east by Saharsa district and
on the west by Sitamarhi and Muzaffarpur districts. Maithili is one of the main languages spoken in
this district.
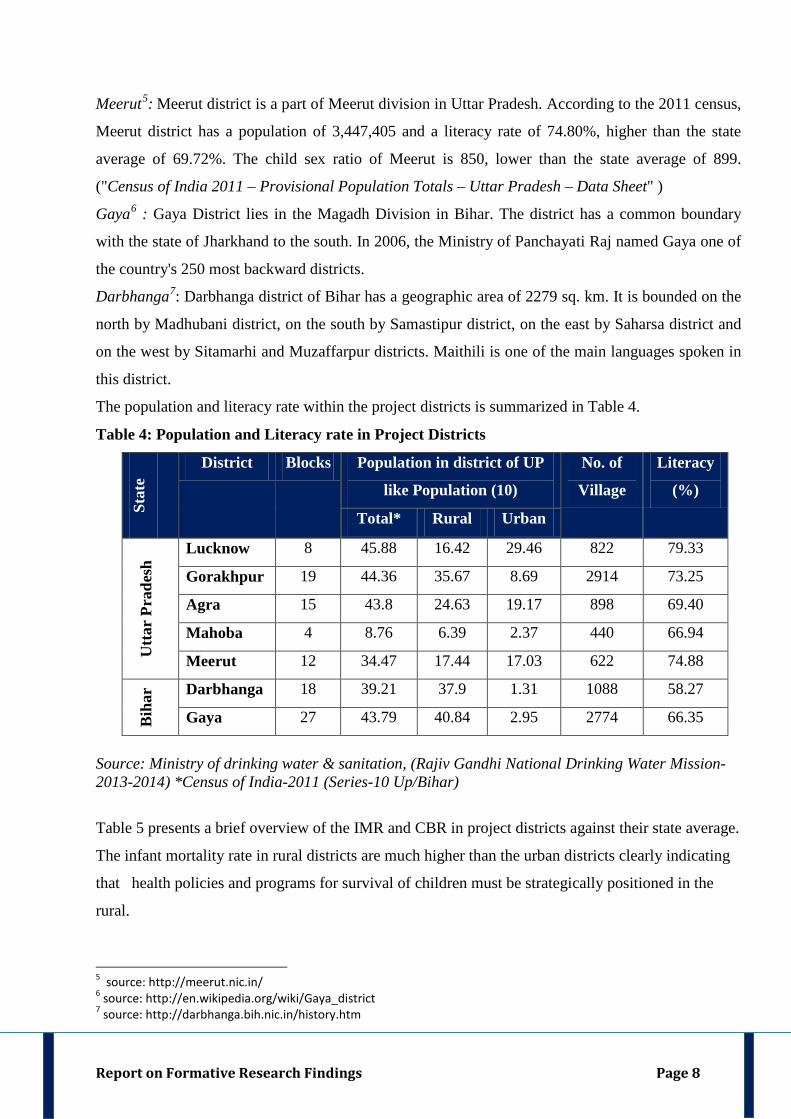
The population and literacy rate within the project districts is summarized in Table 4.
Table 4: Population and Literacy rate in Project Districts
Stat
e
District Blocks Population in district of UP
like Population (10)
No. of
Village
Literacy
(%)
Total* Rural Urban
Utta
r Pr
ades
h Lucknow 8 45.88 16.42 29.46 822 79.33
Gorakhpur 19 44.36 35.67 8.69 2914 73.25
Agra 15 43.8 24.63 19.17 898 69.40
Mahoba 4 8.76 6.39 2.37 440 66.94
Meerut 12 34.47 17.44 17.03 622 74.88
Bih
ar Darbhanga 18 39.21 37.9 1.31 1088 58.27
Gaya 27 43.79 40.84 2.95 2774 66.35
Source: Ministry of drinking water & sanitation, (Rajiv Gandhi National Drinking Water Mission-2013-2014) *Census of India-2011 (Series-10 Up/Bihar)
Table 5 presents a brief overview of the IMR and CBR in project districts against their state average.
The infant mortality rate in rural districts are much higher than the urban districts clearly indicating
that health policies and programs for survival of children must be strategically positioned in the
rural.
5 source: http://meerut.nic.in/ 6 source: http://en.wikipedia.org/wiki/Gaya_district 7 source: http://darbhanga.bih.nic.in/history.htm
Report on Formative Research Findings Page 9
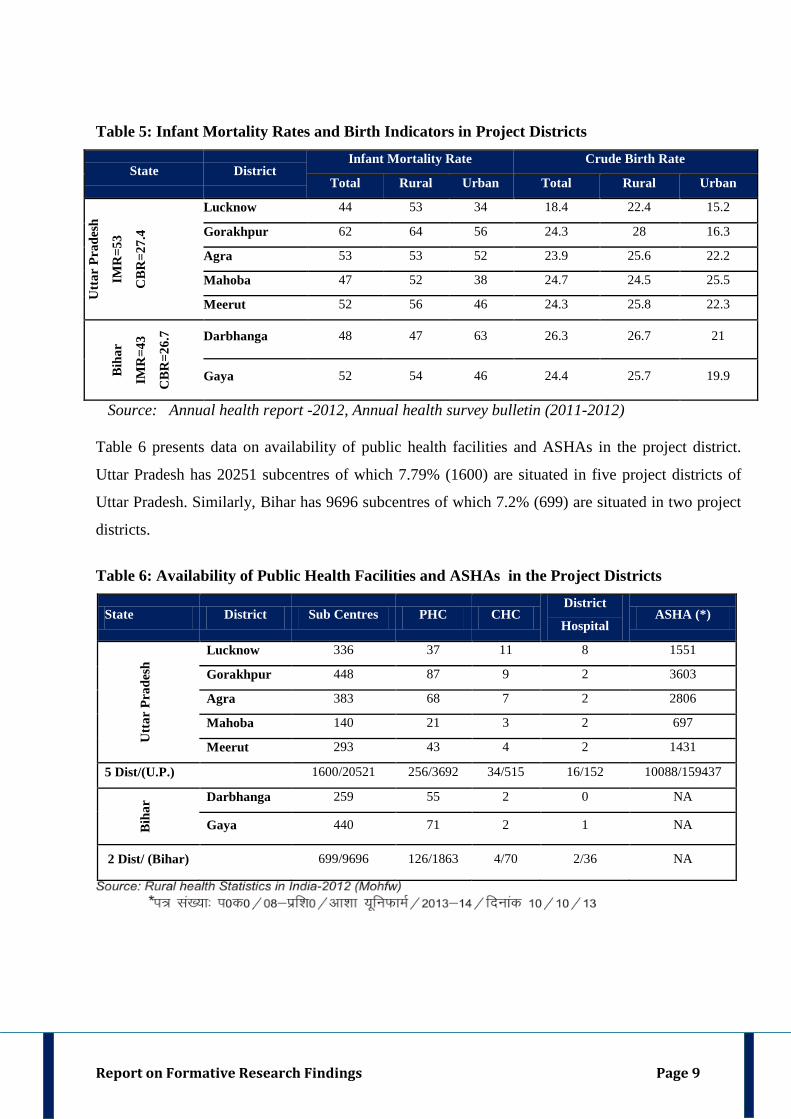
Table 5: Infant Mortality Rates and Birth Indicators in Project Districts
State District Infant Mortality Rate Crude Birth Rate
Total Rural Urban Total Rural Urban
Utt
ar P
rade
sh
IMR
=53
CB
R=2
7.4
Lucknow 44 53 34 18.4 22.4 15.2
Gorakhpur 62 64 56 24.3 28 16.3
Agra 53 53 52 23.9 25.6 22.2
Mahoba 47 52 38 24.7 24.5 25.5
Meerut 52 56 46 24.3 25.8 22.3
Bih
ar
IMR
=43
CB
R=2
6.7 Darbhanga 48 47 63 26.3 26.7 21
Gaya 52 54 46 24.4 25.7 19.9
Source: Annual health report -2012, Annual health survey bulletin (2011-2012)
Table 6 presents data on availability of public health facilities and ASHAs in the project district.
Uttar Pradesh has 20251 subcentres of which 7.79% (1600) are situated in five project districts of
Uttar Pradesh. Similarly, Bihar has 9696 subcentres of which 7.2% (699) are situated in two project
districts.
Table 6: Availability of Public Health Facilities and ASHAs in the Project Districts
State District Sub Centres PHC CHC District
Hospital ASHA (*)
Utt
ar P
rade
sh Lucknow 336 37 11 8 1551
Gorakhpur 448 87 9 2 3603
Agra 383 68 7 2 2806
Mahoba 140 21 3 2 697
Meerut 293 43 4 2 1431
5 Dist/(U.P.) 1600/20521 256/3692 34/515 16/152 10088/159437
Bih
ar Darbhanga 259 55 2 0 NA
Gaya 440 71 2 1 NA
2 Dist/ (Bihar) 699/9696 126/1863 4/70 2/36 NA
Report on Formative Research Findings Page 10
Study Rationale Pneumonia is one the leading causes of childhood deaths in developing countries. The incidence of
clinical pneumonia is 0.29 episodes per child-year in developing countries. This equates to 151.8
million new cases every year, of which 13.1 million or 8.7% are severe enough and require
hospitalization. The estimated incidence of pneumonia in India is 0.37 episodes per child-year,
which translates into 43 million new cases annually. (Igor Rudan, 2008). The third annual
International Vaccine Access Center's (IVAC) Pneumonia Progress Report 2012 says that almost
1,088 children under 5 years of age die every day in India, an increase of 6.7 per cent from 2008
IVAC data which reported 3.71 lakh annual deaths. These deaths due to pneumonia can be attributed
to low rates of exclusive breast-feeding (26.2%) (Srivastava & Awasthi, 2013), poor access to health
care and lack of finances (Pandey, 2012), exposure to ambient air pollutants, low immunization rates
(Corsi et al, 2009; Nath B et al, 2007).
According to National Family Health Survey-3 (NFHS), India has a high Neonatal Mortality Rate
(NMR) of 42.5, high Infant Mortality Rate (IMR) of 62.1 and Under Five Mortality Rate (U5MR)
An equally important reason for poor access to health care is lack of physical access to qualified
health care providers. In a recent survey by Chronic Care Foundation it was found that only 57.7 %
of the urban respondents found diagnostic centers available within accessible distance whereas only
34.3 % of the rural respondents state that there are diagnostic facilities available within accessible
distance (Ratna Devi, 2012). Hence, most rural persons seek first level of curative healthcare close
to home, and pay for a composite convenient service of consulting-cum-dispensing of medicines.
(Gautam et al, 2011)
of
81.9 [India Fact Sheet]. States of Uttar Pradesh and Bihar have a higher IMR of 67 and 91
respectively when compared to rest of India. In 2005, 2.3 million deaths were reported in children
between ages of 1 month to 5 years and half of them were due to pneumonia or diarrhea (Million
Death Study Collaborators, 2010]. Majority of deaths in India occur in rural areas (Kalter et al,
2011). One important reason for larger proportion of deaths in rural area is poor access to qualified
health care providers due to their shortage (Kalter et al, 2011).
Children between 12–23 months of age, 43.5% had received primary immunization in India whereas
only 23% had done so in U.P. (India Fact Sheet, NFHS-3 data, 2012) and 66.7% in Bihar (State
Health Society of Bihar). In urban Lucknow, it was found that care seeking for a neonatal sickness
2.2 PROJECT BACKGROUND & GOAL
Report on Formative Research Findings Page 11
from at least one qualified provider was only 50.8% (Awasthi et al, 2009), which is likely to be
much lower in rural areas. As per NFHS-3, in UP, only about half of children with diarrhea or ARI
or fever in the last two weeks were taken to a health facility (India Fact Sheet).
In order to reduce infant mortality, deaths due to childhood pneumonia have to be reduced, Thus,
there is a need to change community behavior in three distinct aspects: timely recognition of disease
and its severity, avail treatment from qualified health care provider and understanding the
consequences of inadequate and delayed care. There has to be a synergy between diarrhea as well as
pneumonia mortality reduction in India as lessons learned from former can be applied to the latter
(Nichter, 1993 & Gove and Pelto, 1994).
In order to leverage this gap , the study entitled “Improving household decision-making for the
management of Pediatric pneumonia in Uttar Pradesh and Bihar” has been sponsored by Bill
and Melinda Gates Foundation to create communications materials to improve household decision
making that will result in early care seeking for suspect pediatric pneumonia and hence improve
child survival.
Project Goal and Objectives Goal: To create communications materials to improve household decision making when confronted
by lower respiratory illness in children in Northern India.
Objective 1: To constitute a Childhood Pneumonia Behavior Change Communication Consultative
Group (CPBCCCG) of various stakeholders who can be potential change agents from the
government and non-government sector, civil society, potential implementation partners, content
experts and other community gatekeepers, like politicians.
Objective 2: To conduct formative research to assess community perceptions about symptoms of
pneumonia, care seeking behavior and risk vulnerability due to it.
Objective 3: To compile a set of pneumonia case studies where there was bad outcome, like
prolongation of hospital stay or development of complications or death.
Objective 4: To develop potential messages for improving recognition of symptoms of pneumonia
early, care seeking from a qualified provider and understanding the risks as a result of delay in
recognition and quality care.
Objective 5:( i) To test the potential messages in the community to identify the ones which are most
informative and validate their understandability on another set of community (ii) To customize the
selected messages for various different audience, if required prior to roll out.
Objective 6: To disseminate the research findings and messages among various stakeholders as
identified by the CPBCCCG.
Report on Formative Research Findings Page 12
In pursuance of objective 2, we conducted formative research in 7 pre-identified districts of Uttar
Pradesh and Bihar. Its findings are presented in this report.
Geographic Focus
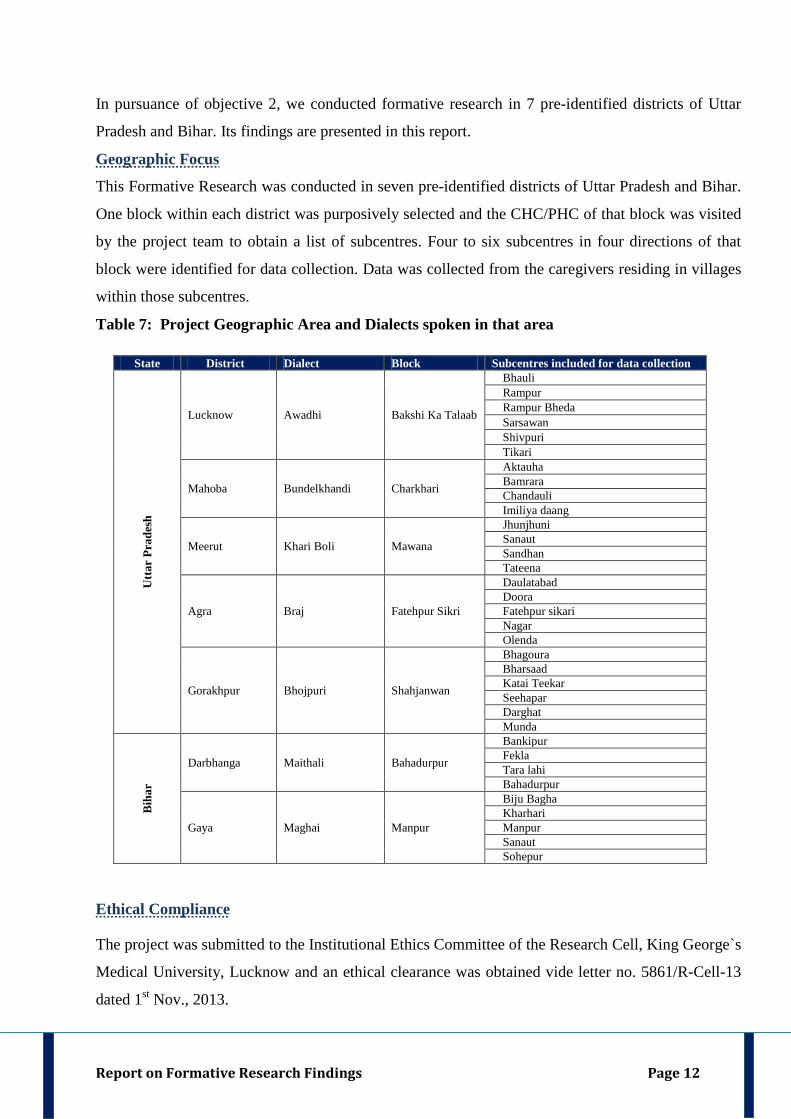
This Formative Research was conducted in seven pre-identified districts of Uttar Pradesh and Bihar.
One block within each district was purposively selected and the CHC/PHC of that block was visited
by the project team to obtain a list of subcentres. Four to six subcentres in four directions of that
block were identified for data collection. Data was collected from the caregivers residing in villages
within those subcentres.
Table 7: Project Geographic Area and Dialects spoken in that area
State District Dialect Block Subcentres included for data collection
Utt
ar P
rade
sh
Lucknow Awadhi Bakshi Ka Talaab
Bhauli Rampur Rampur Bheda Sarsawan Shivpuri Tikari
Mahoba Bundelkhandi Charkhari
Aktauha Bamrara Chandauli Imiliya daang
Meerut Khari Boli Mawana
Jhunjhuni Sanaut Sandhan Tateena
Agra Braj Fatehpur Sikri
Daulatabad Doora Fatehpur sikari Nagar Olenda
Gorakhpur Bhojpuri Shahjanwan
Bhagoura Bharsaad Katai Teekar Seehapar Darghat Munda
Bih
ar
Darbhanga Maithali Bahadurpur
Bankipur Fekla Tara lahi Bahadurpur
Gaya Maghai Manpur
Biju Bagha Kharhari Manpur Sanaut Sohepur
Ethical Compliance
The project was submitted to the Institutional Ethics Committee of the Research Cell, King George`s
Medical University, Lucknow and an ethical clearance was obtained vide letter no. 5861/R-Cell-13
dated 1st Nov., 2013.
Report on Formative Research Findings Page 13
Video Clippings on Childhood Respiratory Illness Vignettes
Fifteen Video Clippings of Childhood Respiratory Illness Scenarios or Vignettes were made.
Children less than 5 years admitted in the in-patient ward of the Department of Pediatrics of King
George`s Medical University (KGMU) or attending the outpatient facility of KGMU else from the
Trauma Centre of KGMU were captured in video clippings. Childhood respiratory illness video
clippings were made for WHO-defined conditions like (a) non-severe pneumonia (b) severe
pneumonia (c) very severe disease with one or more danger signs (d) upper respiratory tract
infection, like common cold (e) noisy breathings as depicted by patient of croup and audible wheeze.
Written and informed consent was taken from the parents/legal guardians of the children prior to
making of the clippings. The identity of the subjects was kept anonymous. These vignettes were
shown to the CPBCCCG members during the first Childhood Pneumonia Behavior Change
Communication Consultative Group (CPBCCCG) prior to use in the field.
From among the 15 video clippings, three-which clearly demonstrated specific signs of pneumonia-
were selected. These were later used during the Focus Group Discussions in the field. The following
were the salient features of selected vignettes:
Respiratory Illness Vignette 1: It showed a child less than 5 years suffering from pneumonia.
The child had only fast breathing, which is an early sign of pneumonia.
Respiratory Illness Vignette 2: It showed a child less than 5 years suffering from severe
pneumonia. The child had chest in drawing along with fast breathing and difficult breathing.
Respiratory Illness Vignette 3: It showed a child less than 5 years suffering from very severe
pneumonia and danger signs. The child had chest in drawing along with fast breathing and
difficult breathing. In addition, it had signs of severe pneumonia like grunting/groaning and
altered sensorium.
Development and Pilot Testing of Formative Tools
Key informant interviews, semi structured interviews and focus group discussions were the
formative research techniques used in this project.
2.3 Preparation For Data Collection
Report on Formative Research Findings Page 14
Fig. 1: Formative Research Techniques used in this project
Data was collected using the following data collection tools from different category of stakeholders:
i. Key Informant Interview schedule - Caregivers
ii. Key Informant Interview schedule- Community Health Workers & Rural Medical
Practitioner
iii. Semi Structured Interview schedule - Caregivers
iv. Focus Group Discussion schedule - Caregivers & Community Health Workers
Case studies collected as part of Objective 3 in this project also helped in development of data
collection schedules.
Each interview schedule was developed in English and then translated into Hindi. Pilot Testing of
study instruments was done in hospital setting in Lucknow and in the rural areas adjoining Lucknow.
Mothers of children less than 5 years who were either admitted for Acute Lower Respiratory
Infection (ALRI) or who attended the outpatient department of Pediatrics in King George’s Medical
University (KGMU), Lucknow were approached for initial pilot testing. After this, instruments were
modified and another pilot testing was conducted in the rural area of Bakshi Ka Talaab (BKT) block
within Lucknow district. Here caregivers of healthy children less than 5 years were interviewed.
Based on the findings of pilot testing and experiential learning, the instrument was again modified
for understandability and content validity. The modified tool was again used for pilot testing on a
different set of mothers accompanying children admitted for ALRI in KGMU, Lucknow and on the
Report on Formative Research Findings Page 15
rural population in BKT. The instruments finalized after three stages of pilot testing were henceforth
used for data collection.
Themes for Data Collection in Formative Research Tools
Data was collected on the following thematic areas using the following questions to elicit responses:
Section I: Awareness about Respiratory Illnesses, Symptoms and Management
1. Can you tell us about the common illnesses experienced by children (<5 years) in this place?
2. Please tell us about ALL types of respiratory illnesses that children (<5 years) commonly get
here?
3. You have told us about some respiratory illnesses in children less than 5 years just now.
Which among these respiratory illnesses are the ones in which the child suffers from difficult
breathing OR slow breathing OR rapid breathing?
4. Describe each of these respiratory illnesses and help us learn the terms you use for the
symptoms associated with each illness? [Note each respiratory illness and its description.
Also probe for differences between different respiratory diseases –what are distinguishing
symptoms or features, seasons when they occur etc.]
5. You have told us about symptoms that are common in respiratory illnesses in children less
than 5 years. Now tell us, which among these symptoms are very serious and would lead you
to seek immediate medical care?
6. Can you tell us about common remedies that are readily available at home that you or your
neighbours use when your children less than 5 years suffers from respiratory illnesses?
7. Can you tell us about common medicines that are readily available at the nearest
pharmacy/drugstore or that is commonly prescribed by any healthcare provider that you or
your neighbours use when your children less than 5 years suffers from respiratory illnesses?
8. How long and for what should one wait and self treat before taking the child less than 5 years
suffering from respiratory illness to a clinic/practitioner?
9. Can you tell us about any diet changes that should be followed for a child less than 5 years
suffering from respiratory illness? [Probe: changes in quantity of diet, changes in
composition of diet, food perceived to be `cold` by the community, food perceived to be
`hot` by the community, changes in breastfeeding, changes in the amount of water to be
given to the child etc.]
Report on Formative Research Findings Page 16
10. Can you tell us about the things that we should do & not do when our children suffer from
respiratory illnesses? [Probe the practices related to respiratory illnesses: bundling the baby,
stop bathing, prayers, giving steam etc.]
Section II: Decision making within the family and Health Care Seeking
11. Which health care providers and health care facilities are there in your village and in the
adjoining village and within 20 km of this place who are commonly consulted by the local
people to treat children`s illnesses? Name them. [Probe about the availability of (a)
Traditional healers (`ojha`, `tantrik `, `baba` etc.) (b) Rural probably non-qualified
practitioners (`vaids` or doctors who give allopathic/ayurvedic medicine/homeopathic
medicine medicine and/or syrup after removing its commercial packaging and injections ) (c)
Government Health Facilities (d) Community Health workers (ASHA, ANM etc.) (e) Rural
Qualified Medical Practitioners.]
12. Who is the primary decision maker in your family once the child less than 5 years is
recognized as being very ill?
13. What happens if the primary decision maker(s) named above is/are not at home? In that case,
who can make a decision?
14. Under what circumstances can you, being a mother/grandmother/ female relative of the child,
leave home, if person who often accompanied you to the doctor is not there? Suppose if there
is an emergency then which person may be approached to accompany you to clinic or doctor-
-neighbour, health worker etc.?
15. Are the neighbors or relatives ever involved in decision-making?
Section III: Case Scenarios / Video Clippings of Childhood Respiratory Illness Vignettes
In this section Case Scenarios or Respiratory Illness Vignettes were given to the respondents.
It should be noted that Case Scenarios were a part of Key Informant Interviews and Semi
Structured Interviews and were narrated to the respondents. Video clips on Respiratory Illness
Vignettes were shown during the Focus Group Discussions.
Case Scenarios
Case Scenario 1: Let us consider a situation in which your child less than 5 years is having
cough, runny nose and is warm to touch. He/she is otherwise healthy and is also feeding
/breastfeeding normally? Where will you go first to seek care if your child is having such a
condition? [Probe if local practitioner (`vaid`, `ojha`, ` tantrik ` or any other traditional
Report on Formative Research Findings Page 17
healer), RMP or private doctor visited first over government health facility or community
health worker then for what reasons- for convenience , proximity, cost, trust, reputation of
that facility/practitioner, availability of doctor or medicines, quality of care etc?]
Case Scenario 2: Let us consider a situation in which your child less than 5 years was having
cough, runny nose, fever PLUS fast breathing and chest in drawing AND was drinking /
breastfeeding less than his/her daily intake? Where will you go first to seek care if your child
is having such a condition? [Probe if local practitioner (`vaid`, `ojha`, ` tantrik ` or any other
traditional healer), RMP or private doctor visited first over government health facility or
community health worker then for what reasons- for convenience , proximity, cost, trust,
reputation of that facility/practitioner, availability of doctor or medicines, quality of care
etc.]
Case Scenario 3: Let us consider a situation in which your child was having cough, fever
PLUS difficult breathing, chest in drawing PLUS was unable
Video Clippings of Childhood Respiratory Illness Vignettes
to drink/breastfeed normally.
S/he is ALSO drowsy AND is having bluish discolouration of the lips? Where will you go
first to seek care if your child is having such a condition? [Probe if local practitioner (`vaid`,
`ojha`, ` tantrik ` or any other traditional healer), RMP or private doctor visited first over
government health facility or community health worker then for what reasons- for
convenience , proximity, cost, trust, reputation of that facility/practitioner, availability of
doctor or medicines, quality of care etc.]
Video Clippings were shown during the Focus Group Discussions to ascertain what signs
were recognized and how serious they were considered. They also helped elicit the local
language of illness. Three video clips of 17 to 30 seconds duration were shown to group
participants using a hand held PICO projector. Vignettes depicting the following video
presentations were shown to the group:
Respiratory Illness Vignette 1:
It showed a child less than 5 years suffering from pneumonia.
The child had only fast breathing, which is an early sign of pneumonia.
Respiratory Illness Vignette 2:
It showed a child less than 5 years suffering from severe
pneumonia. The child had chest in drawing along with fast breathing and difficult breathing.
Respiratory Illness Vignette 3: It showed a child less than 5 years suffering from very severe
pneumonia and danger signs. The child had chest in drawing along with fast breathing and
Report on Formative Research Findings Page 18
difficult breathing. In addition, it had signs of severe pneumonia like grunting/groaning and
altered sensorium.
Section IV: Quality of Care
When you visited a health care provider for treatment of your child suffering from respiratory
illness and less than 5 years
16. Did you know whether he was a qualified or an unqualified health care provider? How did
you ascertain it?
17. Did the health care provider explain you about the illness and why it has occurred?
18. Was the child`s chest exposed for examination or was the child examined bundled
up/covered with clothes?
19. Did he measure body temperature with thermometer or did he not use the thermometer but
touched the child to know about temperature?
20. Did he have tools for examination: Stethoscope, thermometer etc.?
21. Did the practitioner tell you about the medicines and how much and in what method they
should be given to the child?
22. Did the practitioner tell you what to look for to know whether the child`s condition is
improving or not?
23. Were you asked to follow up after a certain period or did he visit your house to know the
condition of the child?
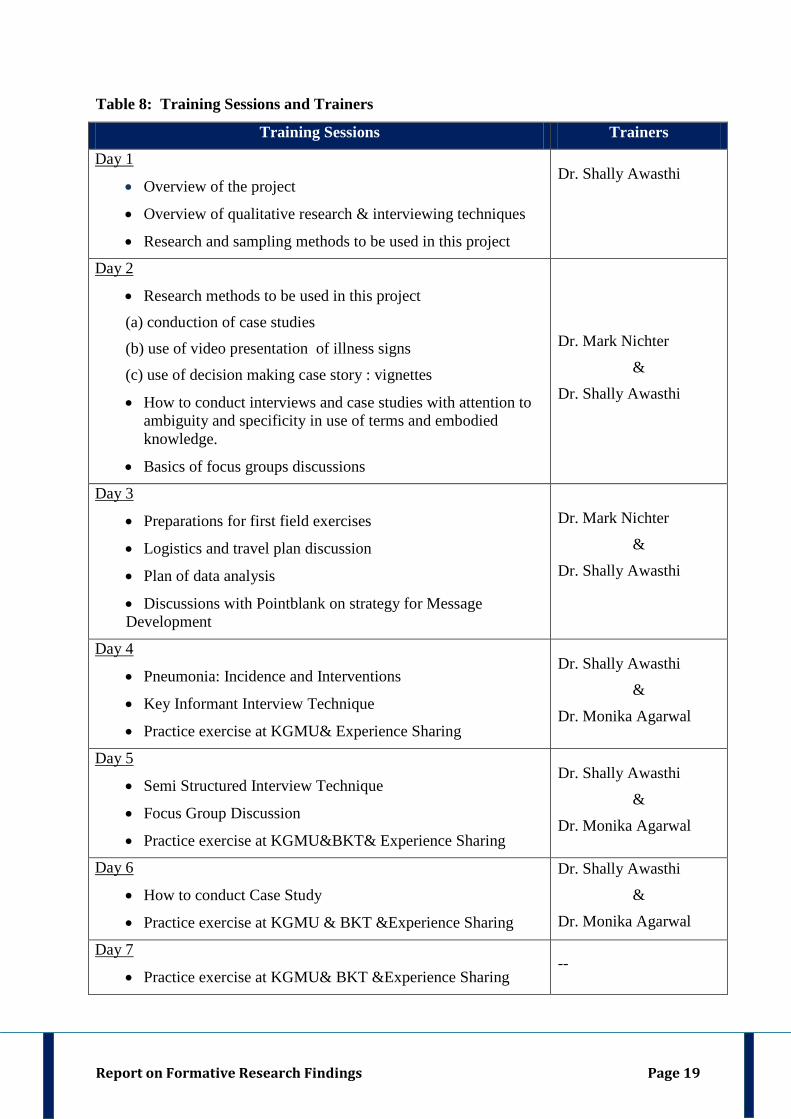
Team Formation & Training:
Researchers were hired and trained for work in the field settings. The team comprised of a Project
Coordinator, Social Scientists, Community Interviewers and Field Assistants. It was ensured that the
team members were fluent in local dialect of project districts. The project staff was provided seven
day training from 16th - 23rd
Sep., 2013. Trainers were Dr. Mark Nichter – Project Consultant, Dr.
Shally Awasthi- Principal Investigator and Dr. Monika Agarwal- Co-Principal Investigator.
Ms. Bindu Menon from our subgrantee PointBlank also participated in the meeting as observer.
Training was imparted using both class room teaching and field practice techniques. The sessions of
the training were as follows:
Report on Formative Research Findings Page 19
Table 8: Training Sessions and Trainers
Training Sessions Trainers
• Overview of the project
Day 1
• Overview of qualitative research & interviewing techniques
• Research and sampling methods to be used in this project
Dr. Shally Awasthi
• Research methods to be used in this project
Day 2
(a) conduction of case studies
(b) use of video presentation of illness signs
(c) use of decision making case story : vignettes
• How to conduct interviews and case studies with attention to ambiguity and specificity in use of terms and embodied knowledge.
• Basics of focus groups discussions
Dr. Mark Nichter
&
Dr. Shally Awasthi
• Preparations for first field exercises
Day 3
• Logistics and travel plan discussion
• Plan of data analysis
• Discussions with Pointblank on strategy for Message Development
Dr. Mark Nichter
&
Dr. Shally Awasthi
• Pneumonia: Incidence and Interventions
Day 4
• Key Informant Interview Technique
• Practice exercise at KGMU& Experience Sharing
Dr. Shally Awasthi
&
Dr. Monika Agarwal
• Semi Structured Interview Technique
Day 5
• Focus Group Discussion
• Practice exercise at KGMU&BKT& Experience Sharing
Dr. Shally Awasthi
&
Dr. Monika Agarwal
• How to conduct Case Study
Day 6
• Practice exercise at KGMU & BKT &Experience Sharing
Dr. Shally Awasthi
&
Dr. Monika Agarwal
• Practice exercise at KGMU& BKT &Experience Sharing
Day 7 --
Report on Formative Research Findings Page 20
The trainees conducted 12 in-depth interviews, 12 case studies and 2 focus group discussions to gain
firsthand experience in conducting formative research.
In discussion (L-R): Ms. Bindu Menon (Subgrantee), Prof. Shally Awasthi (PI) and Dr. Mark
Nichter (Consultant)
In addition to the above-mentioned training, the social scientist of this project was imparted training
for improved data management and analysis. The social scientist attended a five day workshop on
'Qualitative Research Methods and Data Analysis' organized by the Public Health Foundation of
India (PHFI) at New Delhi between Dec 2 - 6, 2013. Topics that were covered during the workshop
were: epistemology of qualitative research, choosing appropriate study designs in qualitative
research, recording qualitative data and data management using best practices, focus group
discussions and in-depth interviews, approaches to analysis of qualitative data and writing up
qualitative research for publication.
After training, the data collection team was divided into 2 independent teams each supervised by a
Project Coordinator and a Social Scientist respectively. Each Team comprised of two community
interviewers and a field assistant. Field schedule of the team was prepared.
Report on Formative Research Findings Page 21
Report on Formative Research Findings Page 21
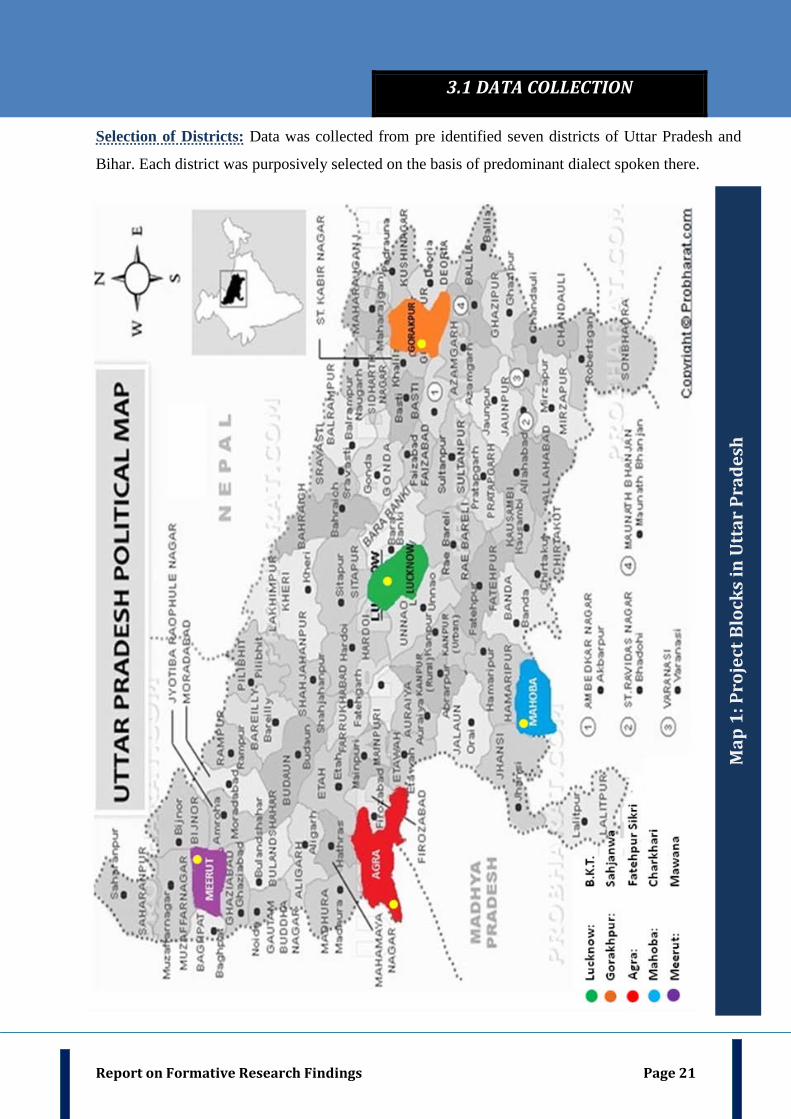
Selection of Districts: Data was collected from pre identified seven districts of Uttar Pradesh and
Bihar. Each district was purposively selected on the basis of predominant dialect spoken there.
3.1 DATA COLLECTION
Map
1: P
roje
ct B
lock
s in
Utt
ar P
rade
sh
Report on Formative Research Findings Page 22
Map
2: P
roje
ct B
lock
s in
Bih
ar

Report on Formative Research Findings Page 23
Selection of Block and Sub Center`s:. List of all the blocks within a district was obtained. Out of
all the blocks, one block per district was purposively selected. The blocks selected in project district
were: Manpur block in Gaya district, Bahadurpur block in Darbhanga district, Bakshi Ka Talab
block in Lucknow district, Sahjanwan block in Gorakhpur district, Fatehpur Sikri block in Agra
district, Charkhari block in Mahoba district, Mawana block in Meerut district. Selected block was at
a distance of 20-25 km from the district capital and the Chief Medical Officer (CMO)/Chief Medical
Superintendent (CMS) of that block consented to cooperate in the study.
After this, the CHC/ PHC within that block were visited by the team. The team visited the CHC in
Uttar Pradesh. However, since there are no CHC`s in Bihar and only a Main PHC along with its
additional PHC`s at the block level, the team visited the main PHC in Bihar District. The team met
the CMO/ CMS and sensitized him about the project. After this, a list of all subcentres functional
within the selected CHC/PHC was obtained. From the list of subcentres, four to six sub-centers in
four corners of the CHC were identified and selected for data collection. Then, 1-2 villages
randomly selected within each sub center were selected and visited by the team for data collection.
Report on Formative Research Findings Page 24
Respondents for Key Informant Interviews
Six Key Informants per district were interviewed. They were: two younger caregivers, two older
caregivers, one Community Health Worker and one Rural Medical Practitioner in each block of
chosen district.
Table 9: Eligibility Criteria for Caregivers of Key Informant Interview
Younger Caregivers Older Caregivers
• Married woman aged 30 – 45 years • Mother of at least ONE child aged 1 month
to 5 years
• Married woman aged 45 – 60 years • Grandmother or
any other female relative of a family in which there is a child between 1 month to 5 years
• All children < 5 years of age in family of respondent reported healthy on day of interview • At least ONE child in the family of the respondent < 5 years of age suffered from respiratory
illness and took medical treatment in last 6 months. • Be local residents • Have time of about 1 hour for interview • Have given written, informed consent for participation
Interview with a younger mother in Meerut, Uttar Pradesh
3.2 STUDY RESPONDENTS & ELIGIBILITY CRITERIA
Report on Formative Research Findings Page 25
Identification and Selection of Caregivers for Key Informant Interviews: For the identification
and selection of caregivers, the team visited the village of the selected subcentre. The ASHA of that
village was approached and sensitized about the project. Project team identified the respondents with
assistance of ASHA. At places where the ASHA was unavailable, the Pradhan or any other
influential person from the community was approached for identifying respondents. Those
respondents were included who fulfilled the eligibility criteria and could provide rich contextual
information (Table 9).
After the caregivers were identified, they were approached and briefed about the project and purpose
of conducting this interview. The respondents were also informed that their identity will be kept
confidential and that their participation is purely voluntary. Only those respondents were included
who agreed to give written, informed consent for participation and those who had time for about 50
minutes for interview. Each interview lasted for approx. 40-50 minutes. Interviews were recorded
using a digital voice recorder. The care providers were chosen as per the eligibility criteria
described in Table 10.
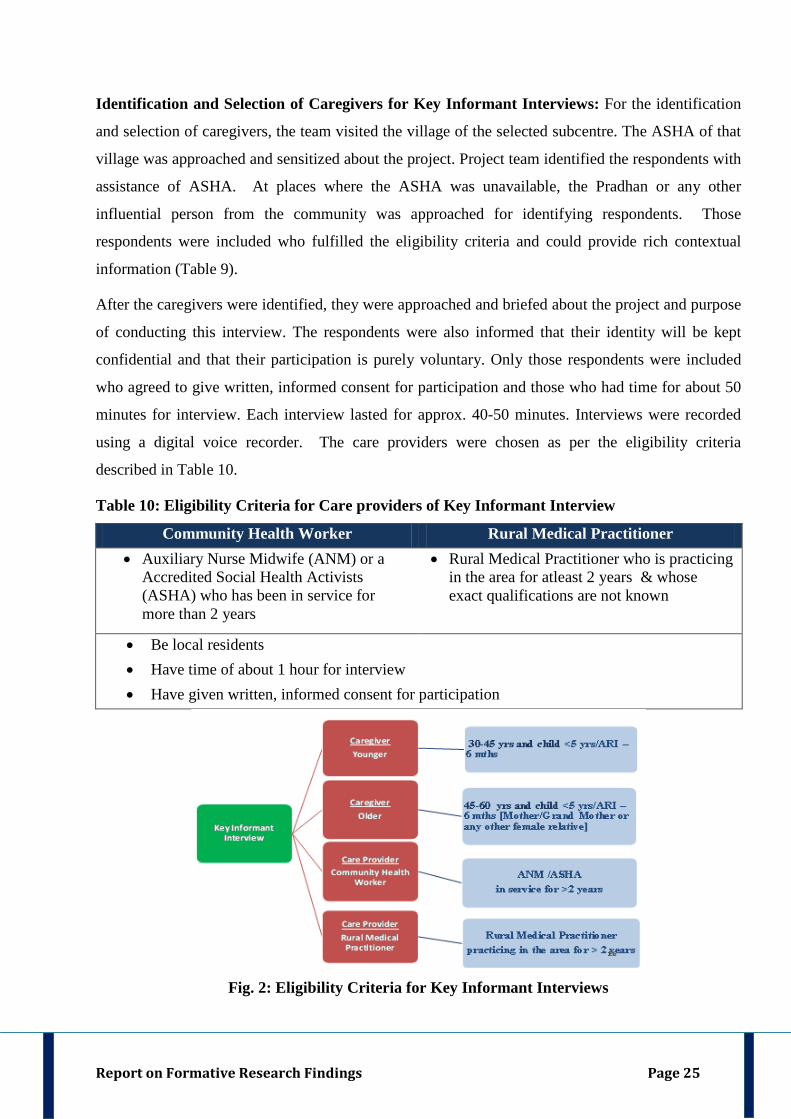
Table 10: Eligibility Criteria for Care providers of Key Informant Interview
Community Health Worker Rural Medical Practitioner • Auxiliary Nurse Midwife (ANM) or a
Accredited Social Health Activists (ASHA) who has been in service for more than 2 years
• Rural Medical Practitioner who is practicing in the area for atleast 2 years & whose exact qualifications are not known
• Be local residents • Have time of about 1 hour for interview • Have given written, informed consent for participation
Fig. 2: Eligibility Criteria for Key Informant Interviews
Report on Formative Research Findings Page 26
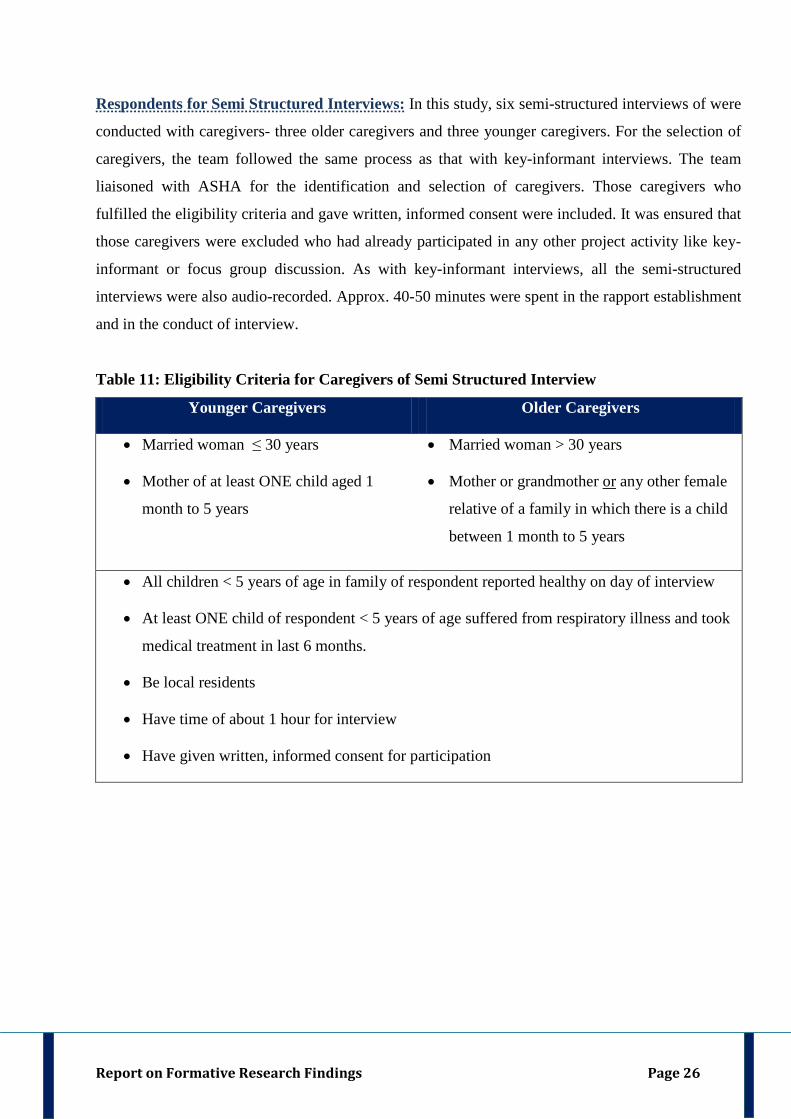
Respondents for Semi Structured Interviews: In this study, six semi-structured interviews of were
conducted with caregivers- three older caregivers and three younger caregivers. For the selection of
caregivers, the team followed the same process as that with key-informant interviews. The team
liaisoned with ASHA for the identification and selection of caregivers. Those caregivers who
fulfilled the eligibility criteria and gave written, informed consent were included. It was ensured that
those caregivers were excluded who had already participated in any other project activity like key-
informant or focus group discussion. As with key-informant interviews, all the semi-structured
interviews were also audio-recorded. Approx. 40-50 minutes were spent in the rapport establishment
and in the conduct of interview.
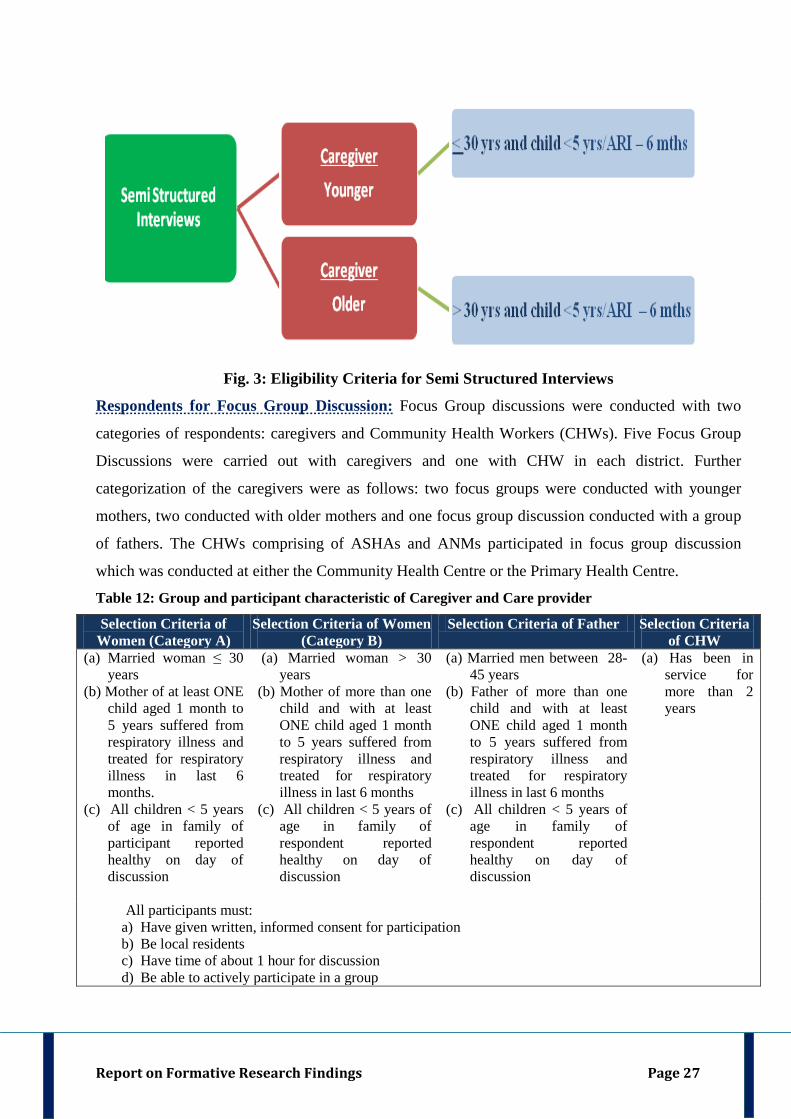
Table 11: Eligibility Criteria for Caregivers of Semi Structured Interview
Younger Caregivers Older Caregivers
• Married woman ≤ 30 years
• Mother of at least ONE child aged 1
month to 5 years
• Married woman > 30 years
• Mother or grandmother or any other female
relative of a family in which there is a child
between 1 month to 5 years
• All children < 5 years of age in family of respondent reported healthy on day of interview
• At least ONE child of respondent < 5 years of age suffered from respiratory illness and took
medical treatment in last 6 months.
• Be local residents
• Have time of about 1 hour for interview
• Have given written, informed consent for participation
Report on Formative Research Findings Page 27
Fig. 3: Eligibility Criteria for Semi Structured Interviews
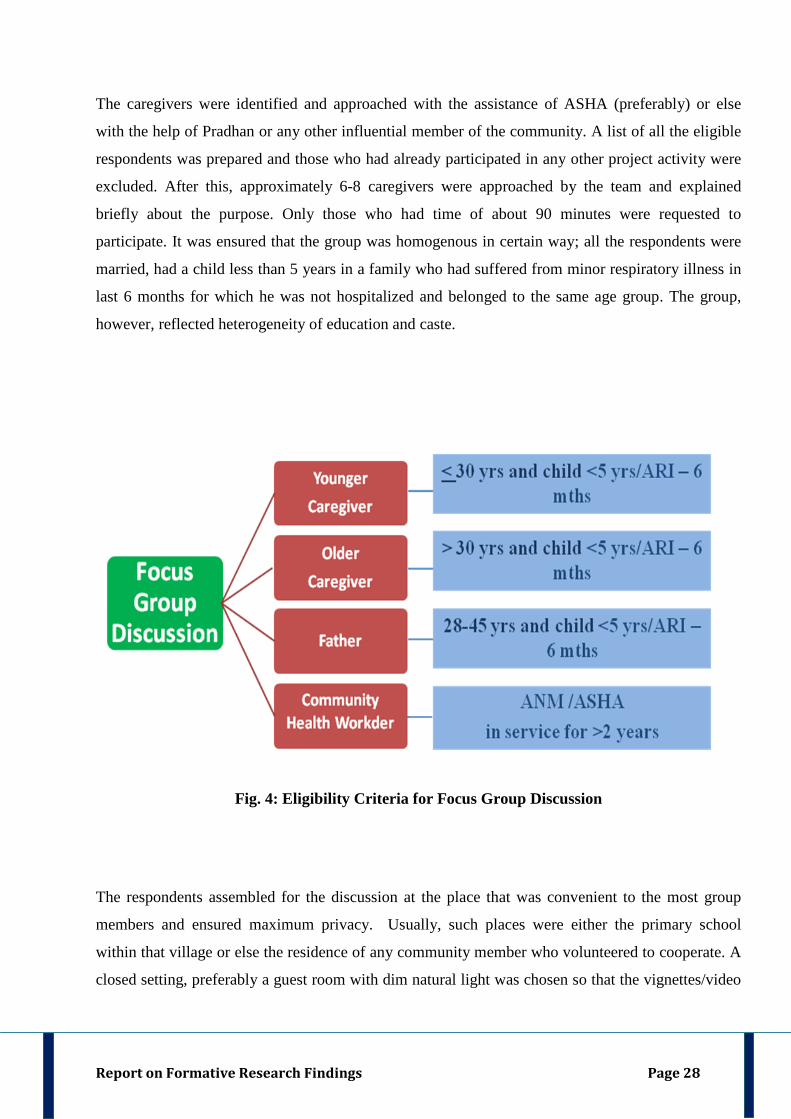
Respondents for Focus Group Discussion: Focus Group discussions were conducted with two
categories of respondents: caregivers and Community Health Workers (CHWs). Five Focus Group
Discussions were carried out with caregivers and one with CHW in each district. Further
categorization of the caregivers were as follows: two focus groups were conducted with younger
mothers, two conducted with older mothers and one focus group discussion conducted with a group
of fathers. The CHWs comprising of ASHAs and ANMs participated in focus group discussion
which was conducted at either the Community Health Centre or the Primary Health Centre.
Table 12: Group and participant characteristic of Caregiver and Care provider
Selection Criteria of Women (Category A)
Selection Criteria of Women (Category B)
Selection Criteria of Father Selection Criteria of CHW
(a) Married woman ≤ 30 years
(b) Mother of at least ONE child aged 1 month to 5 years suffered from respiratory illness and treated for respiratory illness in last 6 months.
(c) All children < 5 years of age in family of participant reported healthy on day of discussion
(a) Married woman > 30 years
(b) Mother of more than one child and with at least ONE child aged 1 month to 5 years suffered from respiratory illness and treated for respiratory illness in last 6 months
(c) All children < 5 years of age in family of respondent reported healthy on day of discussion
(a) Married men between 28-45 years
(b) Father of more than one child and with at least ONE child aged 1 month to 5 years suffered from respiratory illness and treated for respiratory illness in last 6 months
(c) All children < 5 years of age in family of respondent reported healthy on day of discussion
(a) Has been in service for more than 2 years
All participants must: a) Have given written, informed consent for participation b) Be local residents c) Have time of about 1 hour for discussion d) Be able to actively participate in a group
Report on Formative Research Findings Page 28
The caregivers were identified and approached with the assistance of ASHA (preferably) or else
with the help of Pradhan or any other influential member of the community. A list of all the eligible
respondents was prepared and those who had already participated in any other project activity were
excluded. After this, approximately 6-8 caregivers were approached by the team and explained
briefly about the purpose. Only those who had time of about 90 minutes were requested to
participate. It was ensured that the group was homogenous in certain way; all the respondents were
married, had a child less than 5 years in a family who had suffered from minor respiratory illness in
last 6 months for which he was not hospitalized and belonged to the same age group. The group,
however, reflected heterogeneity of education and caste.
Fig. 4: Eligibility Criteria for Focus Group Discussion
The respondents assembled for the discussion at the place that was convenient to the most group
members and ensured maximum privacy. Usually, such places were either the primary school
within that village or else the residence of any community member who volunteered to cooperate. A
closed setting, preferably a guest room with dim natural light was chosen so that the vignettes/video
Report on Formative Research Findings Page 29
clips can be shown to the respondents during the discussion. Although the ASHA helped in the
identification or selection of caregivers but was not present during the time of discussion.
The prospective respondents were seated in a semi-circular manner. They were sensitized about the
project and the purpose of conducting this interview. Only those respondents who gave written,
informed consent to participate were included. It was clarified to the respondents that their
participation was purely voluntary and they can leave the discussion any time, if they feel so.
Baseline information of the respondents was collected on relationship of the respondent to the child
and on the respondent’s age, education, occupation, caste, religion, family type, number of family
members. In addition, information was also collected on the resources available with them which
they used to obtain information. It was specifically asked if the respondents had a mobile, a
television with/without satellite facility, radio, read newspaper or obtained information from any
other sources.
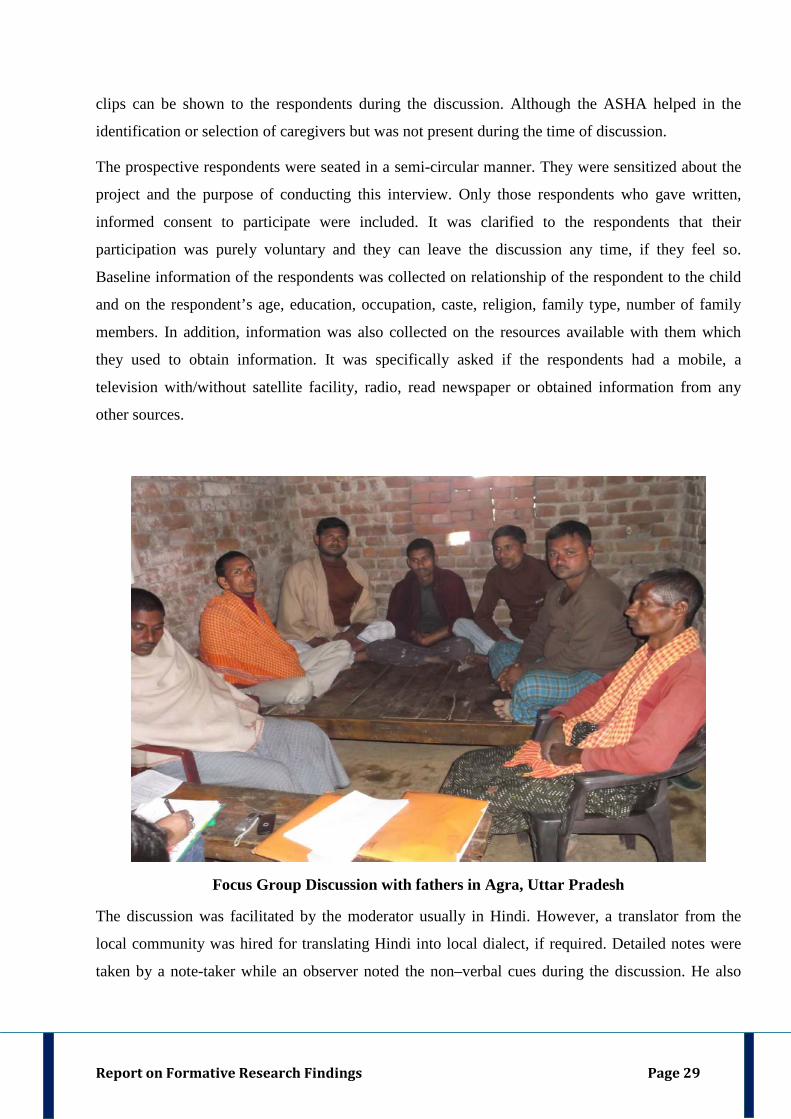
Focus Group Discussion with fathers in Agra, Uttar Pradesh
The discussion was facilitated by the moderator usually in Hindi. However, a translator from the
local community was hired for translating Hindi into local dialect, if required. Detailed notes were
taken by a note-taker while an observer noted the non–verbal cues during the discussion. He also
Report on Formative Research Findings Page 30
drew the organogram. Most of the discussions lasted for about an hour. All the discussions were
audio-recorded using a digital voice recorder.
During the discussion, three illness video clippings were shown depicting different grades of
pneumonia and responses on key themes elicited around these three vignettes. Hand held projectors
(PICOs) were used to project video clippings of childhood respiratory diseases. After the video
clippings, two conceptualized stories/vignettes were narrated to the respondents.
The first story focused on `Absence of Decision Maker`. The facilitator narrated the story of a nine
month old gild child who was perceived “sickly” by her parents. Once when she falls ill, the parents
resort to home treatment, which causes delay health care seeking. Health care seeking is further
delayed in the absence of primary decision maker, the father. The story explores in detail about the
decision making process and the constraints perceived by the respondents in decision-making. The
second story focused on `Absence of Enabling Factors`. The story revolved around a 3 year old boy
who belonged to a financially weak family. Once when he falls sick, he is taken to multiple health
care facilities for health care facilities and delay is caused due to time spent during unqualified care
seeking. Both stories invoked responses from the caregivers on decision-making process, pattern of
health care utilization, choice of health care providers in each situation and concept of quality of
care in the community.
Report on Formative Research Findings Page 31
Data Management
Transcripts of Key Informant interviews, Semi Structured Interviews and FGDs were written by the
facilitator in Hindi. It was ensured that each transcript was prepared only after referring the field
notes and audio recordings. After this, the transcript was translated into English by a hired translator.
Transcripts and their translations were reviewed by Social Scientists as well as the Project Co-
coordinator. 10% transcripts were reviewed by the Principal Investigator and Co-Investigators.
Transcripts and audio recordings were also shared with the sub grantee Point Blank.
Data Analysis
Codebook
A codebook was developed for coding and data interpretation. Codebook was divided into five
heads: (i) Code Level I (ii) Short code -Level I (iii) Code Level II (iv) Short code - Level II (v)
Definitions of Code level I & II. Code Level I was the main code and the Code Level II was the Sub
Code that was a part of the broader domain of main code. Code definitions along with levels of code
were discussed and standardized as analysis progressed. Code Definition also included `When To
Use` and `When Not To Use` instructions. `When To Use` section gave specific instances, usually
based on the data, in which that particular code should be applied. Similarly `When Not To Use `
section gave instances in which the code might be considered but should not be applied (often
because another code would be more appropriate).
Coding, Analysis & Interpretation At the time of conception of the study, it was proposed that data analysis will be done using AnSWR
software, an unpaid software provided by Centre for Communicable Diseases (CDC). It was later
found that this software has been withdrawn by CDC for technical reasons and therefore unavailable
for use. The PI communicated with the website management team of CDC and the team confirmed
that AnSWR was unavailable for use at present. The team from CDC suggested another unpaid
software for qualitative analysis called EZ-Text (Version 4.0) [Assessed through: http://www.cdc-
eztext.com/]. The research team, however, faced some technical issues in importing its files to
different software. Therefore, the team decided not to use it for data analysis. Yet another qualitative
research software called ATLAS Ti was tested by the project team and used in Objective 3
[Compilation of Case Studies] of this project. Its trial version however had a limitation of only 50
codes and 100 quotations. It was for this reason it was decided not to use it for formative research
which will involve large volumes of data. After trying out multiple options for computer assisted
3.3. DATA MANAGEMENT & ANALYSIS
Report on Formative Research Findings Page 32
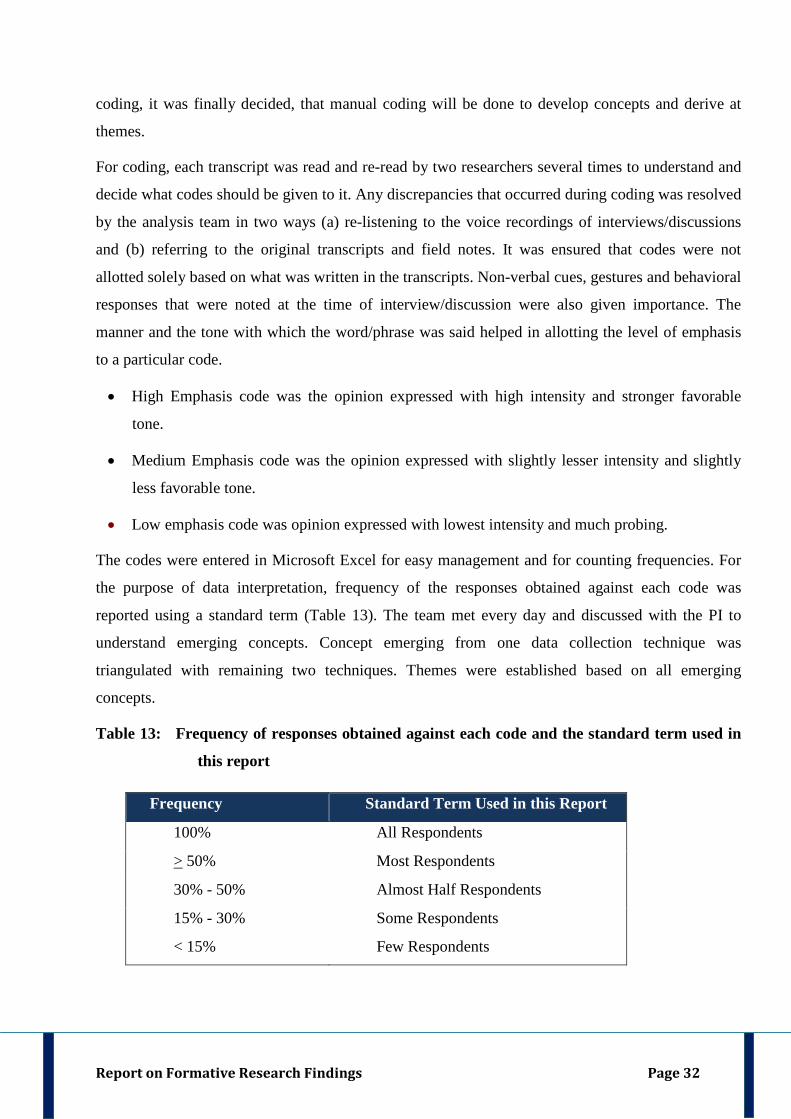
coding, it was finally decided, that manual coding will be done to develop concepts and derive at
themes.
For coding, each transcript was read and re-read by two researchers several times to understand and
decide what codes should be given to it. Any discrepancies that occurred during coding was resolved
by the analysis team in two ways (a) re-listening to the voice recordings of interviews/discussions
and (b) referring to the original transcripts and field notes. It was ensured that codes were not
allotted solely based on what was written in the transcripts. Non-verbal cues, gestures and behavioral
responses that were noted at the time of interview/discussion were also given importance. The
manner and the tone with which the word/phrase was said helped in allotting the level of emphasis
to a particular code.
• High Emphasis code was the opinion expressed with high intensity and stronger favorable
tone.
• Medium Emphasis code was the opinion expressed with slightly lesser intensity and slightly
less favorable tone.
• Low emphasis code was opinion expressed with lowest intensity and much probing.
The codes were entered in Microsoft Excel for easy management and for counting frequencies. For
the purpose of data interpretation, frequency of the responses obtained against each code was
reported using a standard term (Table 13). The team met every day and discussed with the PI to
understand emerging concepts. Concept emerging from one data collection technique was
triangulated with remaining two techniques. Themes were established based on all emerging
concepts.
Table 13: Frequency of responses obtained against each code and the standard term used in
this report
Frequency Standard Term Used in this Report
100% All Respondents
> 50% Most Respondents
30% - 50% Almost Half Respondents
15% - 30% Some Respondents
< 15% Few Respondents
Report on Formative Research Findings
Report on Formative Research Findings 33
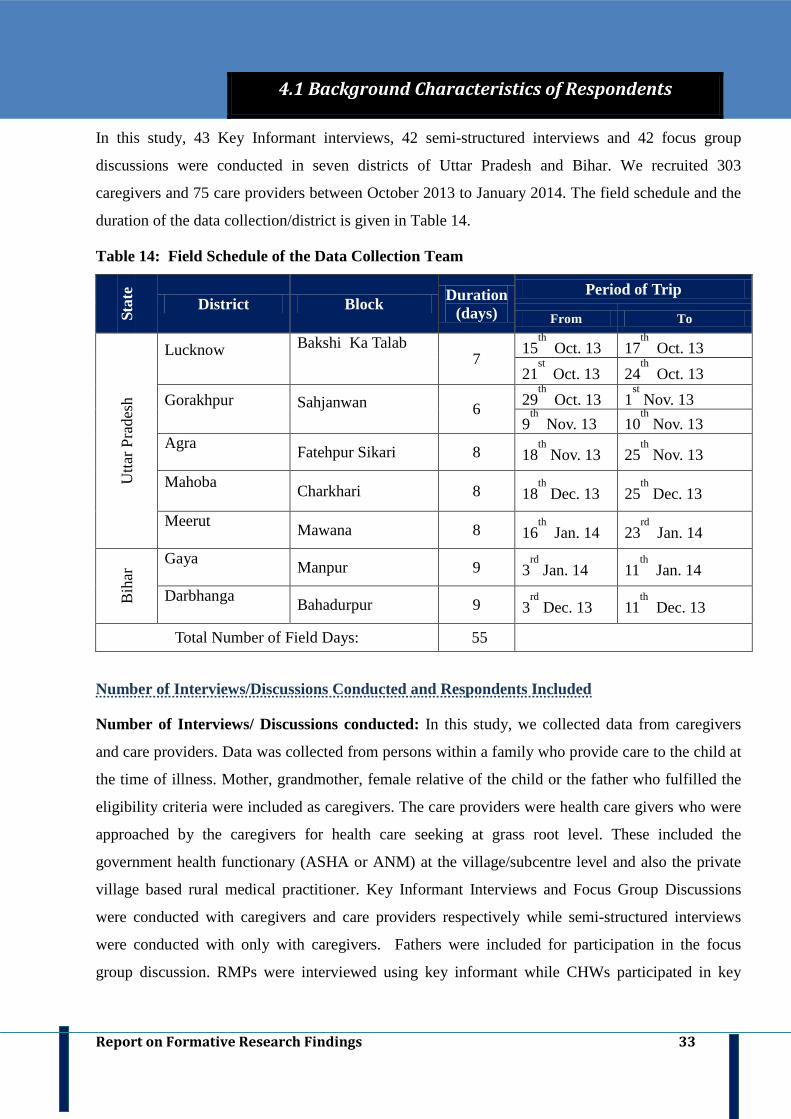
In this study, 43 Key Informant interviews, 42 semi-structured interviews and 42 focus group
discussions were conducted in seven districts of Uttar Pradesh and Bihar. We recruited 303
caregivers and 75 care providers between October 2013 to January 2014. The field schedule and the
duration of the data collection/district is given in Table 14.
Table 14: Field Schedule of the Data Collection Team
Stat
e
District Block Duration (days)
Period of Trip
From To
Utta
r Pra
desh
Lucknow
Bakshi Ka Talab 7
15th
17 Oct. 13 th
Oct. 13 21
st24 Oct. 13
th Oct. 13
Gorakhpur
Sahjanwan 6 29th
1 Oct. 13 st Nov. 13
9th
10 Nov. 13 th
Nov. 13 Agra Fatehpur Sikari 8 18
th25 Nov. 13
th Nov. 13
Mahoba Charkhari 8 18
th25 Dec. 13
th Dec. 13
Meerut Mawana 8 16
th23 Jan. 14
rd Jan. 14
Bih
ar Gaya
Manpur 9 3rd
11 Jan. 14 th
Jan. 14 Darbhanga Bahadurpur 9 3
rd11 Dec. 13
th Dec. 13
Total Number of Field Days: 55
Number of Interviews/Discussions Conducted and Respondents Included
Number of Interviews/ Discussions conducted: In this study, we collected data from caregivers
and care providers. Data was collected from persons within a family who provide care to the child at
the time of illness. Mother, grandmother, female relative of the child or the father who fulfilled the
eligibility criteria were included as caregivers. The care providers were health care givers who were
approached by the caregivers for health care seeking at grass root level. These included the
government health functionary (ASHA or ANM) at the village/subcentre level and also the private
village based rural medical practitioner. Key Informant Interviews and Focus Group Discussions
were conducted with caregivers and care providers respectively while semi-structured interviews
were conducted with only with caregivers. Fathers were included for participation in the focus
group discussion. RMPs were interviewed using key informant while CHWs participated in key
4.1 Background Characteristics of Respondents
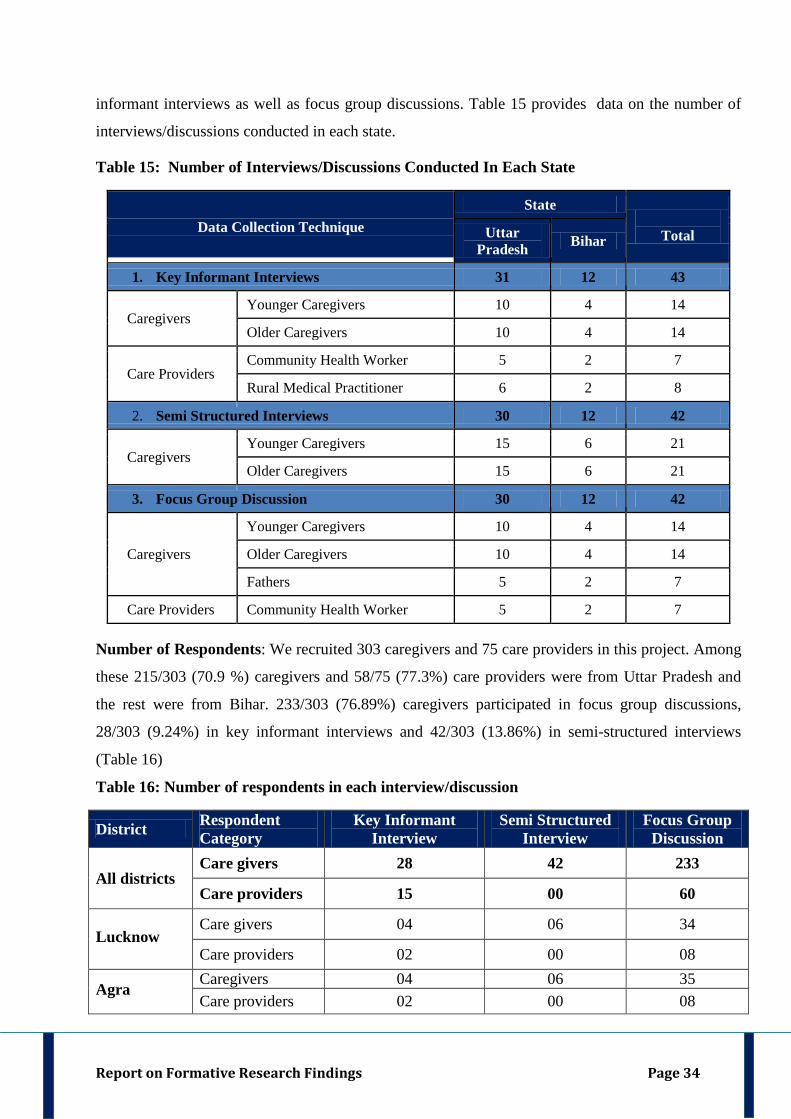
Report on Formative Research Findings Page 34
informant interviews as well as focus group discussions. Table 15 provides data on the number of
interviews/discussions conducted in each state.
Table 15: Number of Interviews/Discussions Conducted In Each State
Data Collection Technique State
Total Uttar
Pradesh Bihar
1. Key Informant Interviews 31 12 43
Caregivers Younger Caregivers 10 4 14
Older Caregivers 10 4 14
Care Providers Community Health Worker 5 2 7
Rural Medical Practitioner 6 2 8
2. Semi Structured Interviews 30 12 42
Caregivers Younger Caregivers 15 6 21
Older Caregivers 15 6 21
3. Focus Group Discussion 30 12 42
Caregivers
Younger Caregivers 10 4 14
Older Caregivers 10 4 14
Fathers 5 2 7
Care Providers Community Health Worker 5 2 7 Number of Respondents: We recruited 303 caregivers and 75 care providers in this project. Among
these 215/303 (70.9 %) caregivers and 58/75 (77.3%) care providers were from Uttar Pradesh and
the rest were from Bihar. 233/303 (76.89%) caregivers participated in focus group discussions,
28/303 (9.24%) in key informant interviews and 42/303 (13.86%) in semi-structured interviews
(Table 16)
Table 16: Number of respondents in each interview/discussion
District Respondent Category
Key Informant Interview
Semi Structured Interview
Focus Group Discussion
All districts Care givers 28 42 233
Care providers 15 00 60
Lucknow Care givers 04 06 34
Care providers 02 00 08
Agra Caregivers 04 06 35 Care providers 02 00 08
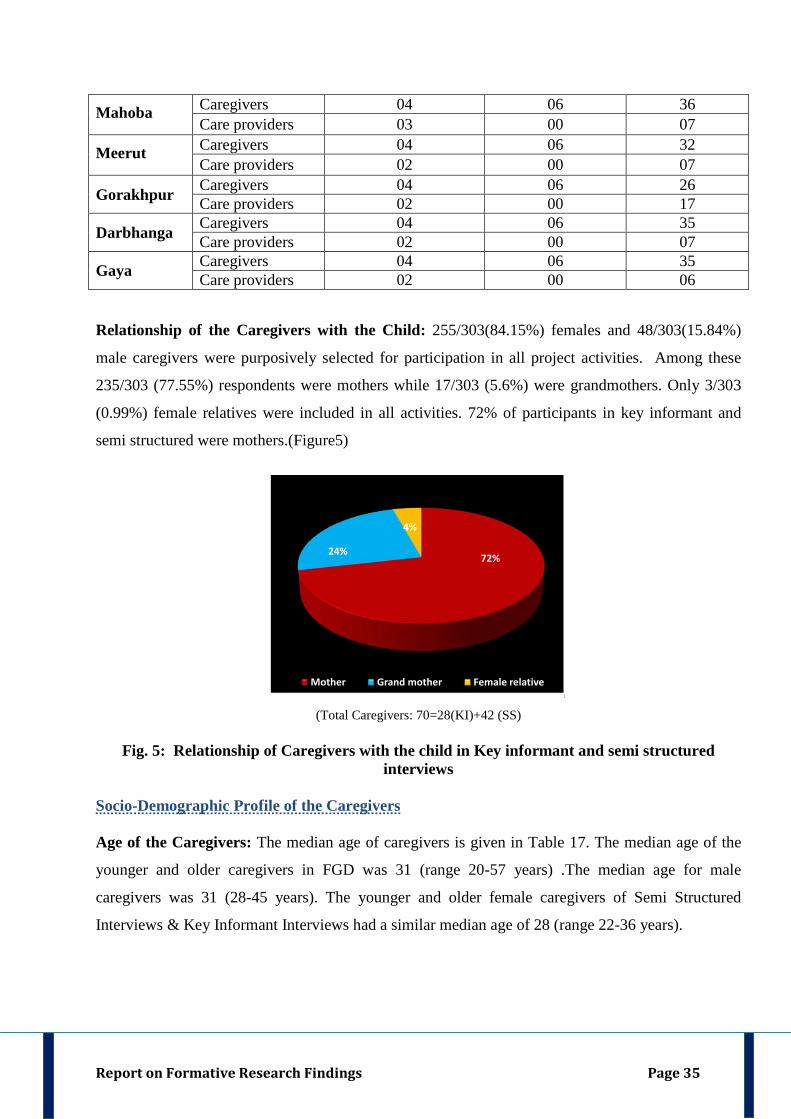
Report on Formative Research Findings Page 35
Mahoba Caregivers 04 06 36 Care providers 03 00 07
Meerut Caregivers 04 06 32 Care providers 02 00 07
Gorakhpur Caregivers 04 06 26 Care providers 02 00 17
Darbhanga Caregivers 04 06 35 Care providers 02 00 07
Gaya Caregivers 04 06 35 Care providers 02 00 06
Relationship of the Caregivers with the Child: 255/303(84.15%) females and 48/303(15.84%)
male caregivers were purposively selected for participation in all project activities. Among these
235/303 (77.55%) respondents were mothers while 17/303 (5.6%) were grandmothers. Only 3/303
(0.99%) female relatives were included in all activities. 72% of participants in key informant and
semi structured were mothers.(Figure5)
72%24%
4%
Mother Grand mother Female relative1
(Total Caregivers: 70=28(KI)+42 (SS)
Fig. 5: Relationship of Caregivers with the child in Key informant and semi structured interviews
Socio-Demographic Profile of the Caregivers Age of the Caregivers: The median age of caregivers is given in Table 17. The median age of the
younger and older caregivers in FGD was 31 (range 20-57 years) .The median age for male
caregivers was 31 (28-45 years). The younger and older female caregivers of Semi Structured
Interviews & Key Informant Interviews had a similar median age of 28 (range 22-36 years).
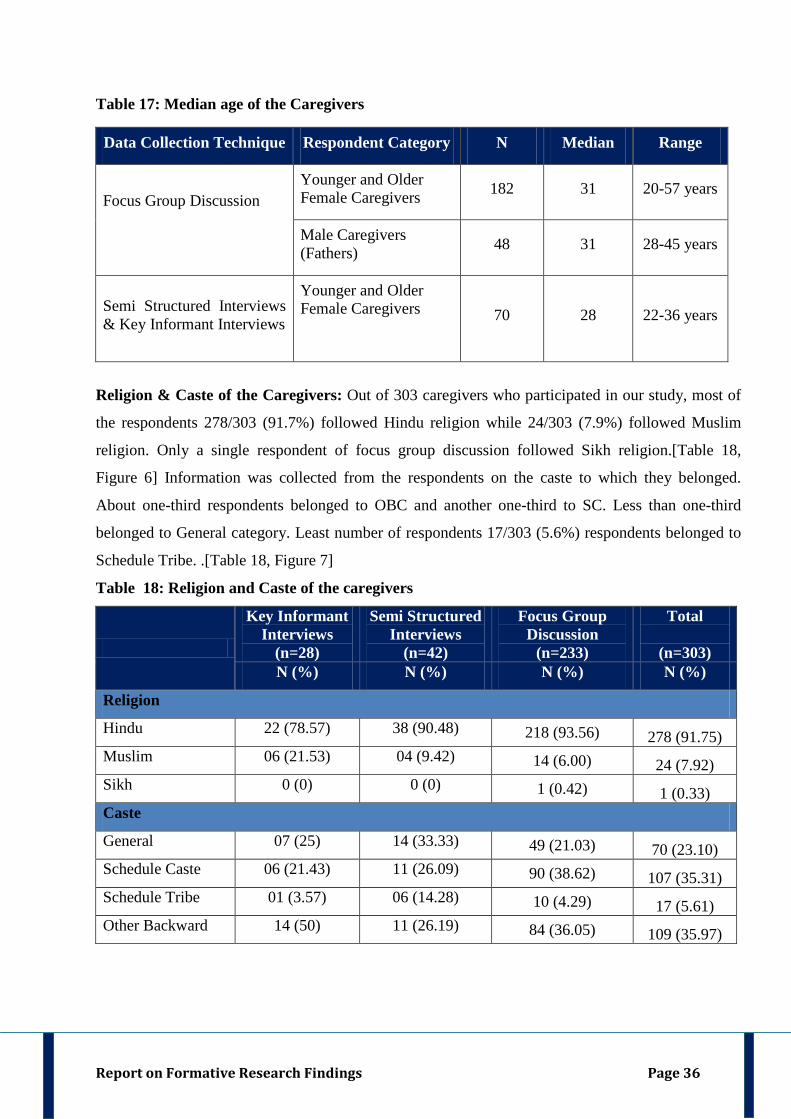
Report on Formative Research Findings Page 36
Table 17: Median age of the Caregivers
Data Collection Technique Respondent Category N Median Range
Focus Group Discussion
Younger and Older Female Caregivers 182 31 20-57 years
Male Caregivers (Fathers) 48 31 28-45 years
Semi Structured Interviews & Key Informant Interviews
Younger and Older Female Caregivers
70 28 22-36 years
Religion & Caste of the Caregivers: Out of 303 caregivers who participated in our study, most of
the respondents 278/303 (91.7%) followed Hindu religion while 24/303 (7.9%) followed Muslim
religion. Only a single respondent of focus group discussion followed Sikh religion.[Table 18,
Figure 6] Information was collected from the respondents on the caste to which they belonged.
About one-third respondents belonged to OBC and another one-third to SC. Less than one-third
belonged to General category. Least number of respondents 17/303 (5.6%) respondents belonged to
Schedule Tribe. .[Table 18, Figure 7]
Table 18: Religion and Caste of the caregivers
Key Informant Interviews
(n=28)
Semi Structured Interviews
(n=42)
Focus Group Discussion
(n=233)
Total
(n=303) N (%) N (%) N (%) N (%)
Religion
Hindu 22 (78.57) 38 (90.48) 218 (93.56) 278 (91.75) Muslim 06 (21.53) 04 (9.42) 14 (6.00) 24 (7.92) Sikh 0 (0) 0 (0) 1 (0.42) 1 (0.33) Caste
General 07 (25) 14 (33.33) 49 (21.03) 70 (23.10) Schedule Caste 06 (21.43) 11 (26.09) 90 (38.62) 107 (35.31) Schedule Tribe 01 (3.57) 06 (14.28) 10 (4.29) 17 (5.61) Other Backward 14 (50) 11 (26.19) 84 (36.05) 109 (35.97)
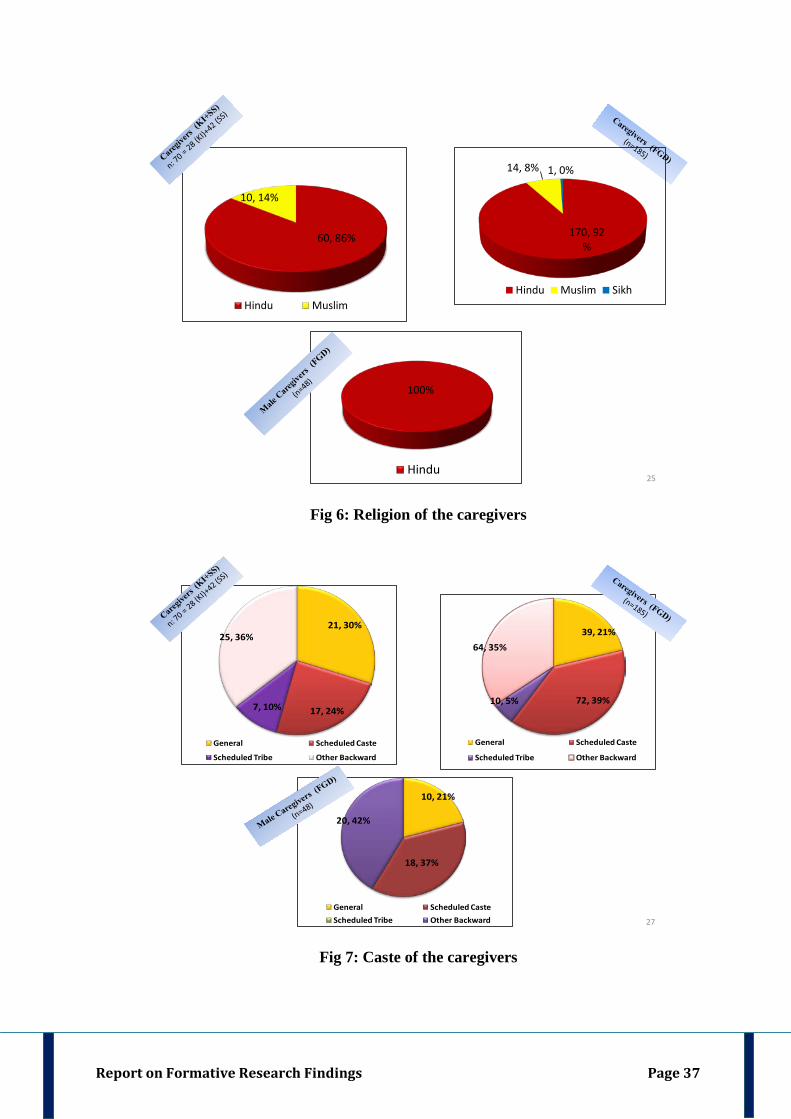
Report on Formative Research Findings Page 37
60, 86%
10, 14%
Hindu Muslim
100%
Hindu25
170, 92%
14, 8% 1, 0%
Hindu Muslim Sikh
Fig 6: Religion of the caregivers
21, 30%
17, 24%7, 10%
25, 36%
General Scheduled Caste
Scheduled Tribe Other Backward
39, 21%
72, 39%10, 5%
64, 35%
General Scheduled Caste
Scheduled Tribe Other Backward
10, 21%
18, 37%
20, 42%
General Scheduled CasteScheduled Tribe Other Backward 27
Fig 7: Caste of the caregivers
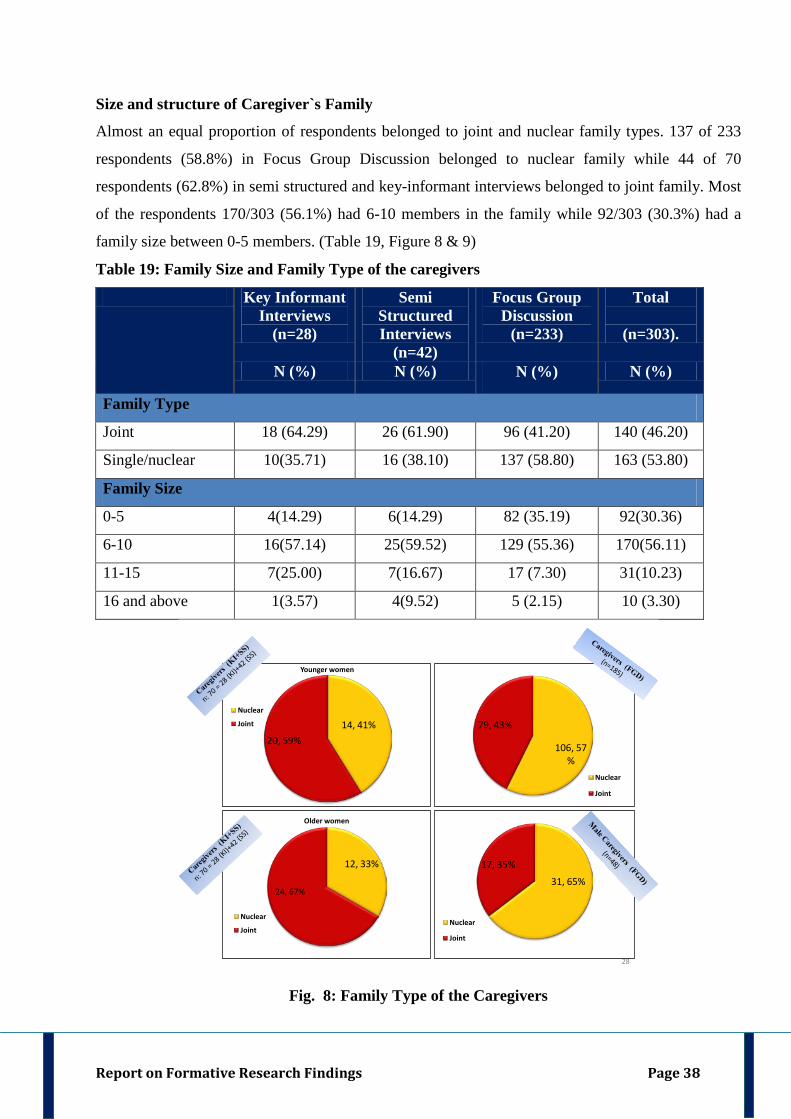
Report on Formative Research Findings Page 38
Size and structure of Caregiver`s Family
Almost an equal proportion of respondents belonged to joint and nuclear family types. 137 of 233
respondents (58.8%) in Focus Group Discussion belonged to nuclear family while 44 of 70
respondents (62.8%) in semi structured and key-informant interviews belonged to joint family. Most
of the respondents 170/303 (56.1%) had 6-10 members in the family while 92/303 (30.3%) had a
family size between 0-5 members. (Table 19, Figure 8 & 9)
Table 19: Family Size and Family Type of the caregivers
Key Informant Interviews
(n=28)
Semi Structured Interviews
(n=42)
Focus Group Discussion
(n=233)
Total
(n=303).
N (%) N (%) N (%) N (%)
Family Type
Joint 18 (64.29) 26 (61.90) 96 (41.20) 140 (46.20)
Single/nuclear 10(35.71) 16 (38.10) 137 (58.80) 163 (53.80)
Family Size
0-5 4(14.29) 6(14.29) 82 (35.19) 92(30.36)
6-10 16(57.14) 25(59.52) 129 (55.36) 170(56.11)
11-15 7(25.00) 7(16.67) 17 (7.30) 31(10.23)
16 and above 1(3.57) 4(9.52) 5 (2.15) 10 (3.30)
106, 57%
79, 43%
Nuclear
Joint
14, 41%20, 59%
Younger women
Nuclear
Joint
12, 33%
24, 67%
Older women
Nuclear
Joint
31, 65%
17, 35%
Nuclear
Joint
28
Fig. 8: Family Type of the Caregivers
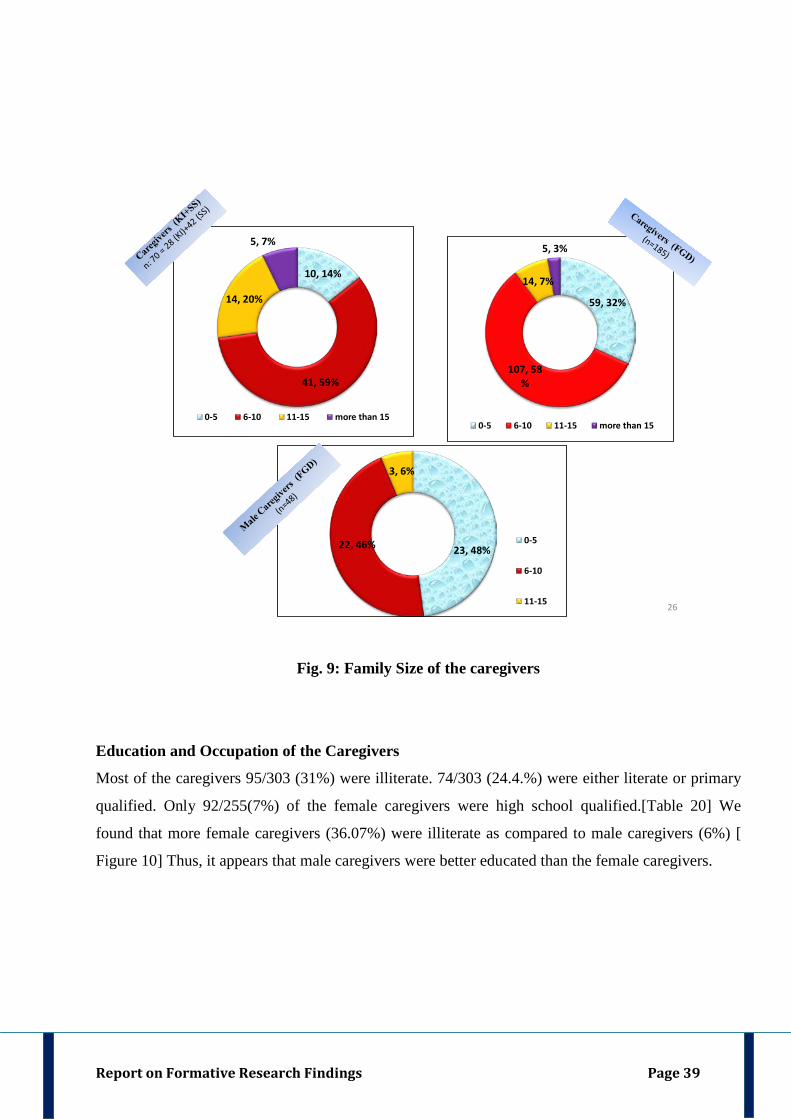
Report on Formative Research Findings Page 39
10, 14%
41, 59%
14, 20%
5, 7%
0-5 6-10 11-15 more than 15
59, 32%
107, 58%
14, 7%
5, 3%
0-5 6-10 11-15 more than 15
23, 48%22, 46%
3, 6%
0-5
6-10
11-15 26
Fig. 9: Family Size of the caregivers
Education and Occupation of the Caregivers
Most of the caregivers 95/303 (31%) were illiterate. 74/303 (24.4.%) were either literate or primary
qualified. Only 92/255(7%) of the female caregivers were high school qualified.[Table 20] We
found that more female caregivers (36.07%) were illiterate as compared to male caregivers (6%) [
Figure 10] Thus, it appears that male caregivers were better educated than the female caregivers.
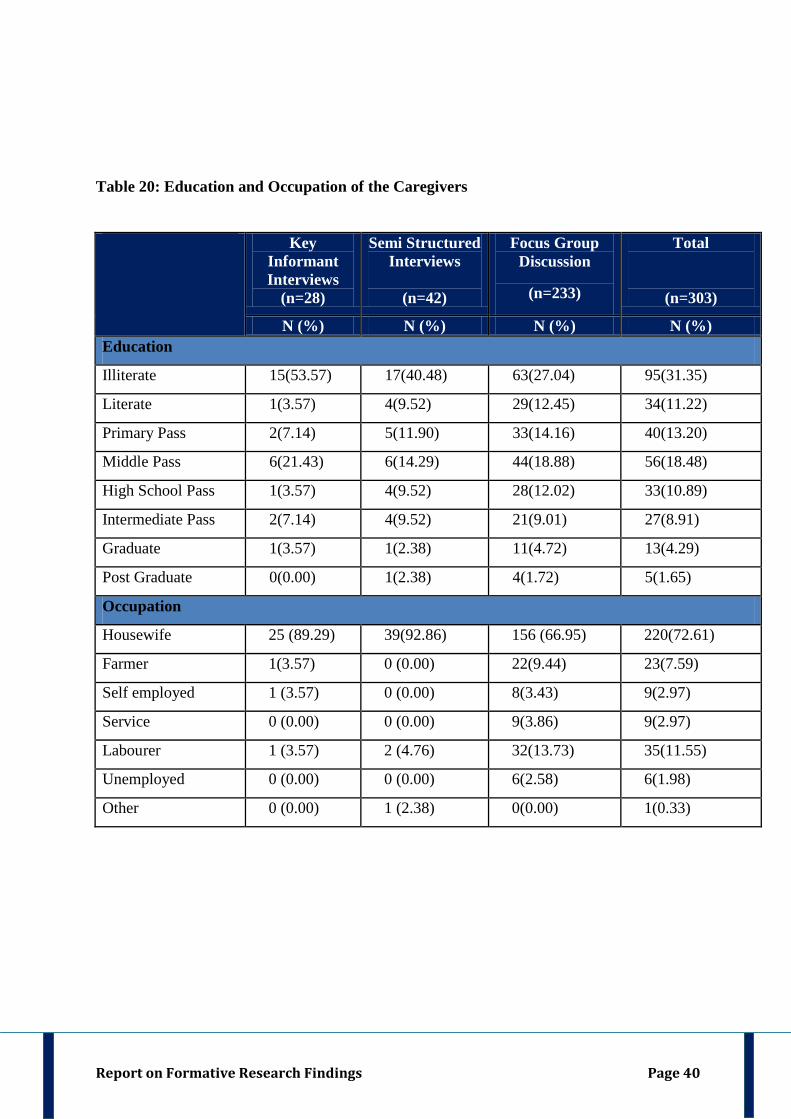
Report on Formative Research Findings Page 40
Table 20: Education and Occupation of the Caregivers
Key Informant Interviews
(n=28)
Semi Structured Interviews
(n=42)
Focus Group Discussion
(n=233)
Total
(n=303)
N (%) N (%) N (%) N (%) Education
Illiterate 15(53.57) 17(40.48) 63(27.04) 95(31.35)
Literate 1(3.57) 4(9.52) 29(12.45) 34(11.22)
Primary Pass 2(7.14) 5(11.90) 33(14.16) 40(13.20)
Middle Pass 6(21.43) 6(14.29) 44(18.88) 56(18.48)
High School Pass 1(3.57) 4(9.52) 28(12.02) 33(10.89)
Intermediate Pass 2(7.14) 4(9.52) 21(9.01) 27(8.91)
Graduate 1(3.57) 1(2.38) 11(4.72) 13(4.29)
Post Graduate 0(0.00) 1(2.38) 4(1.72) 5(1.65)
Occupation
Housewife 25 (89.29) 39(92.86) 156 (66.95) 220(72.61)
Farmer 1(3.57) 0 (0.00) 22(9.44) 23(7.59)
Self employed 1 (3.57) 0 (0.00) 8(3.43) 9(2.97)
Service 0 (0.00) 0 (0.00) 9(3.86) 9(2.97)
Labourer 1 (3.57) 2 (4.76) 32(13.73) 35(11.55)
Unemployed 0 (0.00) 0 (0.00) 6(2.58) 6(1.98)
Other 0 (0.00) 1 (2.38) 0(0.00) 1(0.33)
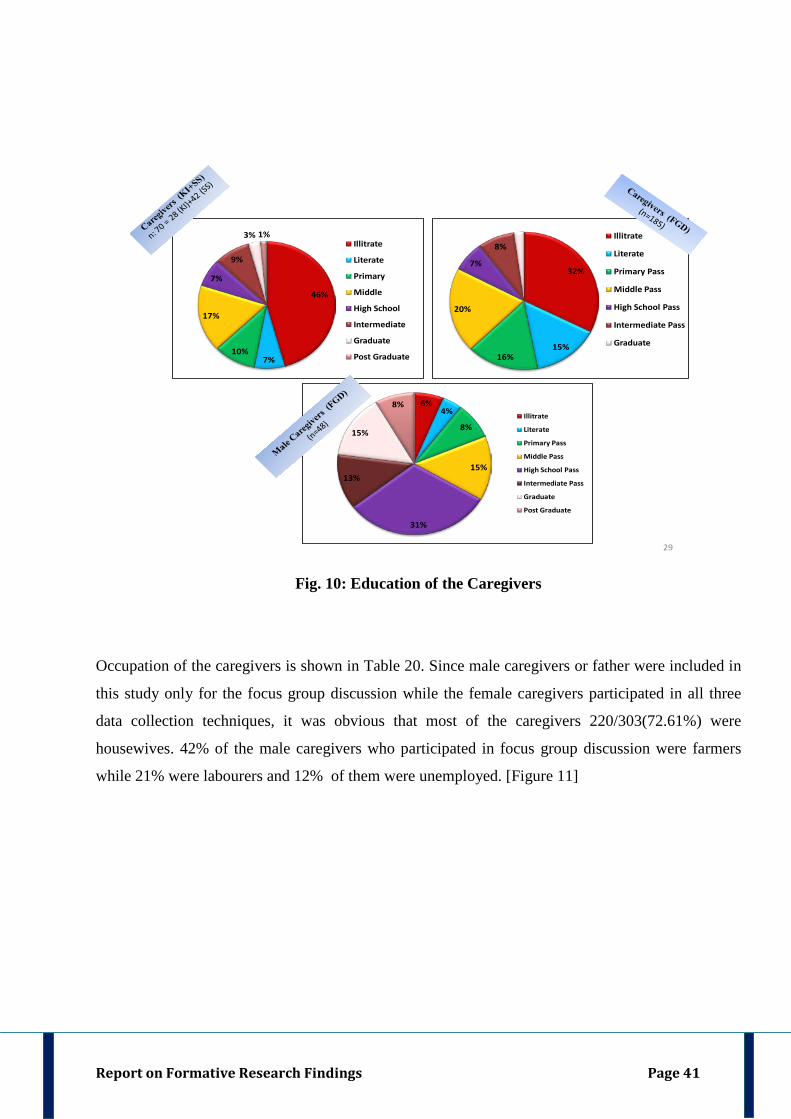
Report on Formative Research Findings Page 41
46%
7%10%
17%
7%
9%
3% 1%Illitrate
Literate
Primary
Middle
High School
Intermediate
Graduate
Post Graduate
32%
15%16%
20%
7%
8%
2%Illitrate
Literate
Primary Pass
Middle Pass
High School Pass
Intermediate Pass
Graduate
6%4%
8%
15%
31%
13%
15%
8%Illitrate
Literate
Primary Pass
Middle Pass
High School Pass
Intermediate Pass
Graduate
Post Graduate
29
Fig. 10: Education of the Caregivers
Occupation of the caregivers is shown in Table 20. Since male caregivers or father were included in
this study only for the focus group discussion while the female caregivers participated in all three
data collection techniques, it was obvious that most of the caregivers 220/303(72.61%) were
housewives. 42% of the male caregivers who participated in focus group discussion were farmers
while 21% were labourers and 12% of them were unemployed. [Figure 11]
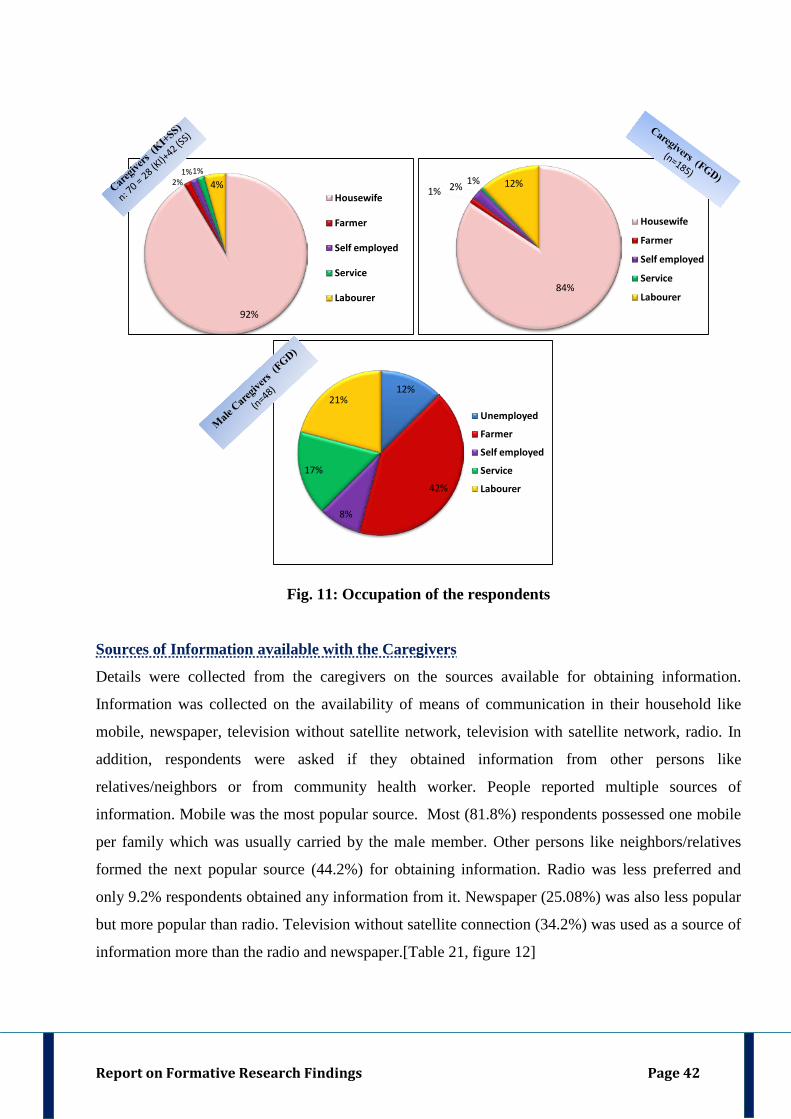
Report on Formative Research Findings Page 42
84%
1% 2% 1% 12%
Housewife
Farmer
Self employed
Service
Labourer
12%
42%
8%
17%
21%Unemployed
Farmer
Self employed
Service
Labourer
92%
2%1%1%
4%Housewife
Farmer
Self employed
Service
Labourer
Fig. 11: Occupation of the respondents
Sources of Information available with the Caregivers
Details were collected from the caregivers on the sources available for obtaining information.
Information was collected on the availability of means of communication in their household like
mobile, newspaper, television without satellite network, television with satellite network, radio. In
addition, respondents were asked if they obtained information from other persons like
relatives/neighbors or from community health worker. People reported multiple sources of
information. Mobile was the most popular source. Most (81.8%) respondents possessed one mobile
per family which was usually carried by the male member. Other persons like neighbors/relatives
formed the next popular source (44.2%) for obtaining information. Radio was less preferred and
only 9.2% respondents obtained any information from it. Newspaper (25.08%) was also less popular
but more popular than radio. Television without satellite connection (34.2%) was used as a source of
information more than the radio and newspaper.[Table 21, figure 12]
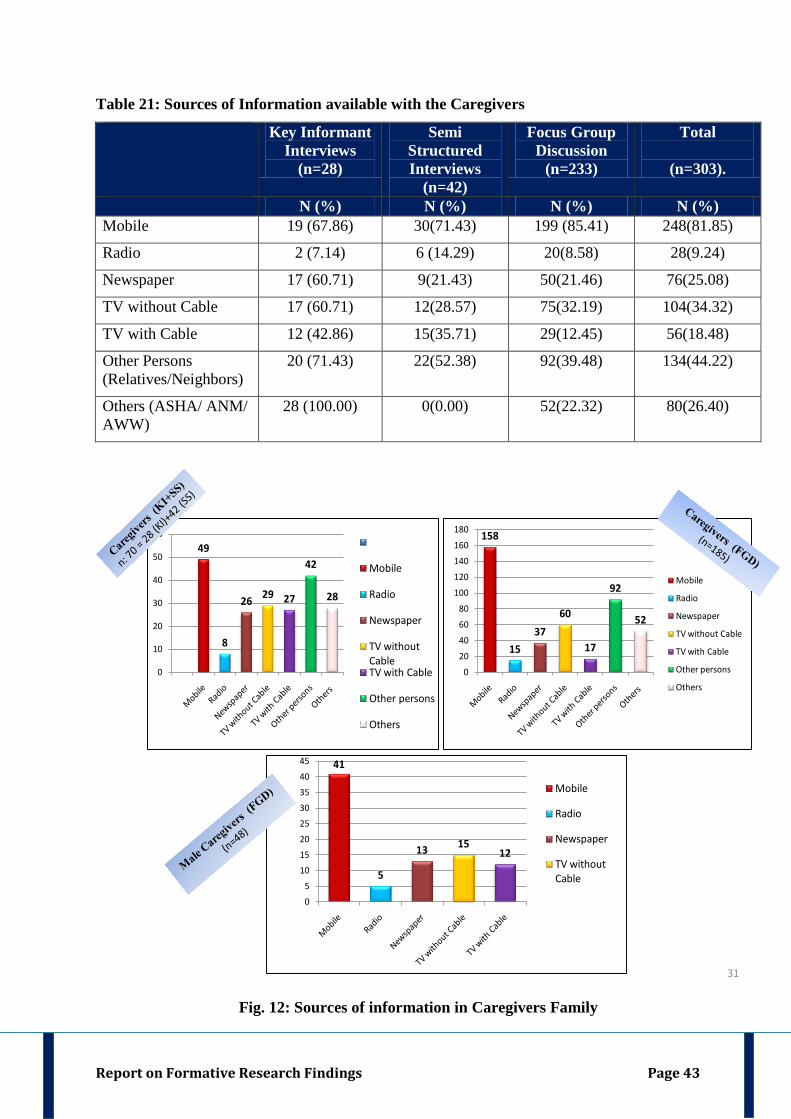
Report on Formative Research Findings Page 43
Table 21: Sources of Information available with the Caregivers
Key Informant Interviews
(n=28)
Semi Structured Interviews
(n=42)
Focus Group Discussion
(n=233)
Total
(n=303).
N (%) N (%) N (%) N (%) Mobile 19 (67.86) 30(71.43) 199 (85.41) 248(81.85)
Radio 2 (7.14) 6 (14.29) 20(8.58) 28(9.24)
Newspaper 17 (60.71) 9(21.43) 50(21.46) 76(25.08)
TV without Cable 17 (60.71) 12(28.57) 75(32.19) 104(34.32)
TV with Cable 12 (42.86) 15(35.71) 29(12.45) 56(18.48)
Other Persons (Relatives/Neighbors)
20 (71.43) 22(52.38) 92(39.48) 134(44.22)
Others (ASHA/ ANM/ AWW)
28 (100.00) 0(0.00) 52(22.32) 80(26.40)
49
8
26 29 27
42
28
0
10
20
30
40
50
60
Mobile
Radio
Newspaper
TV without CableTV with Cable
Other persons
Others
158
1537
60
17
92
52
0
20
40
60
80
100
120
140
160
180
Mobile
Radio
Newspaper
TV without Cable
TV with Cable
Other persons
Others
41
5
13 1512
0
5
10
15
20
25
30
35
40
45
Mobile
Radio
Newspaper
TV without Cable
31
Fig. 12: Sources of information in Caregivers Family
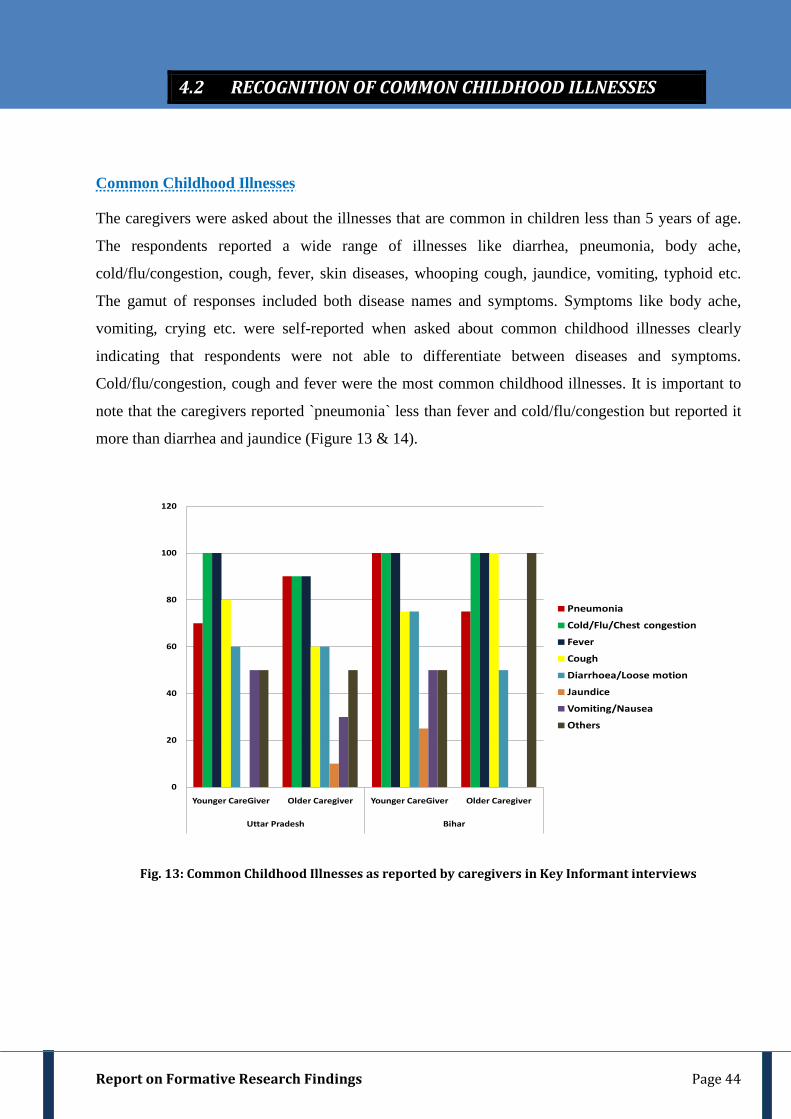
Report on Formative Research Findings Page 44
Common Childhood Illnesses
The caregivers were asked about the illnesses that are common in children less than 5 years of age.
The respondents reported a wide range of illnesses like diarrhea, pneumonia, body ache,
cold/flu/congestion, cough, fever, skin diseases, whooping cough, jaundice, vomiting, typhoid etc.
The gamut of responses included both disease names and symptoms. Symptoms like body ache,
vomiting, crying etc. were self-reported when asked about common childhood illnesses clearly
indicating that respondents were not able to differentiate between diseases and symptoms.
Cold/flu/congestion, cough and fever were the most common childhood illnesses. It is important to
note that the caregivers reported `pneumonia` less than fever and cold/flu/congestion but reported it
more than diarrhea and jaundice (Figure 13 & 14).
0
20
40
60
80
100
120
Younger CareGiver Older Caregiver Younger CareGiver Older Caregiver
Uttar Pradesh Bihar
Pneumonia
Cold/Flu/Chest congestion
Fever
Cough
Diarrhoea/Loose motion
Jaundice
Vomiting/Nausea
Others
Fig. 13: Common Childhood Illnesses as reported by caregivers in Key Informant interviews
4.2 RECOGNITION OF COMMON CHILDHOOD ILLNESSES
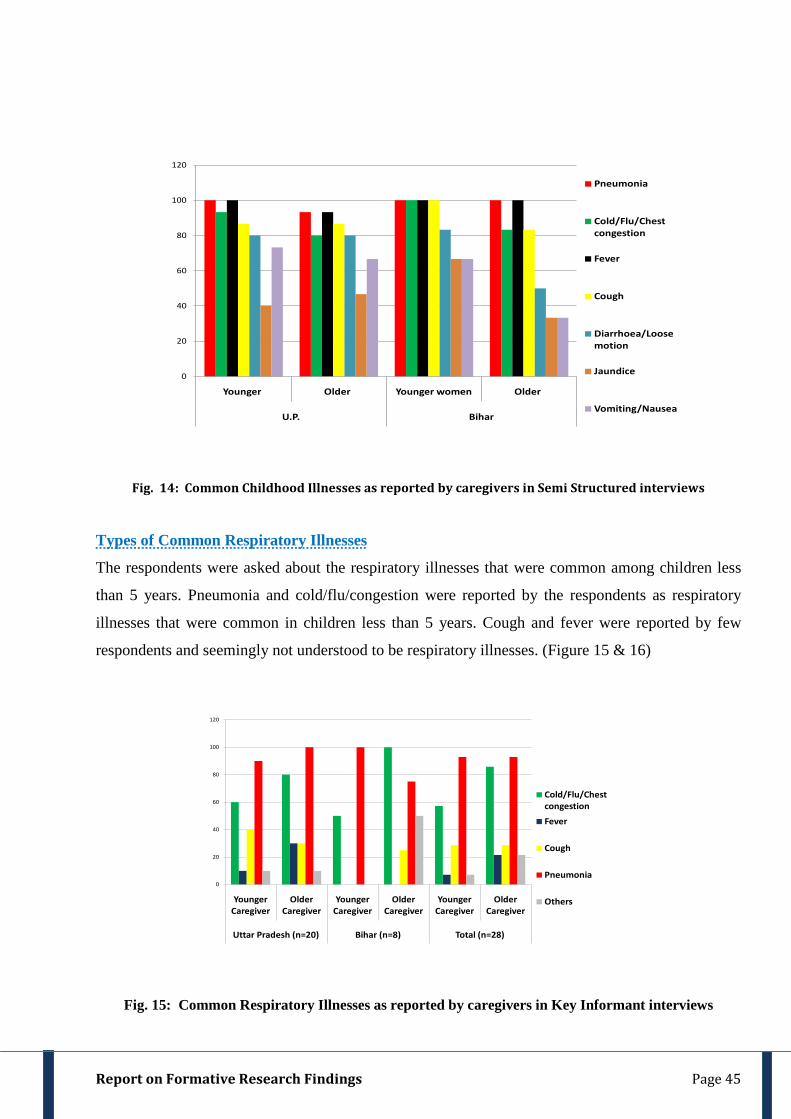
Report on Formative Research Findings Page 45
0
20
40
60
80
100
120
Younger Older Younger women Older
U.P. Bihar
Pneumonia
Cold/Flu/Chest congestion
Fever
Cough
Diarrhoea/Loose motion
Jaundice
Vomiting/Nausea
Fig. 14: Common Childhood Illnesses as reported by caregivers in Semi Structured interviews
Types of Common Respiratory Illnesses
The respondents were asked about the respiratory illnesses that were common among children less
than 5 years. Pneumonia and cold/flu/congestion were reported by the respondents as respiratory
illnesses that were common in children less than 5 years. Cough and fever were reported by few
respondents and seemingly not understood to be respiratory illnesses. (Figure 15 & 16)
0
20
40
60
80
100
120
Younger Caregiver
Older Caregiver
Younger Caregiver
Older Caregiver
Younger Caregiver
Older Caregiver
Uttar Pradesh (n=20) Bihar (n=8) Total (n=28)
Cold/Flu/Chest congestion
Fever
Cough
Pneumonia
Others
Fig. 15: Common Respiratory Illnesses as reported by caregivers in Key Informant interviews
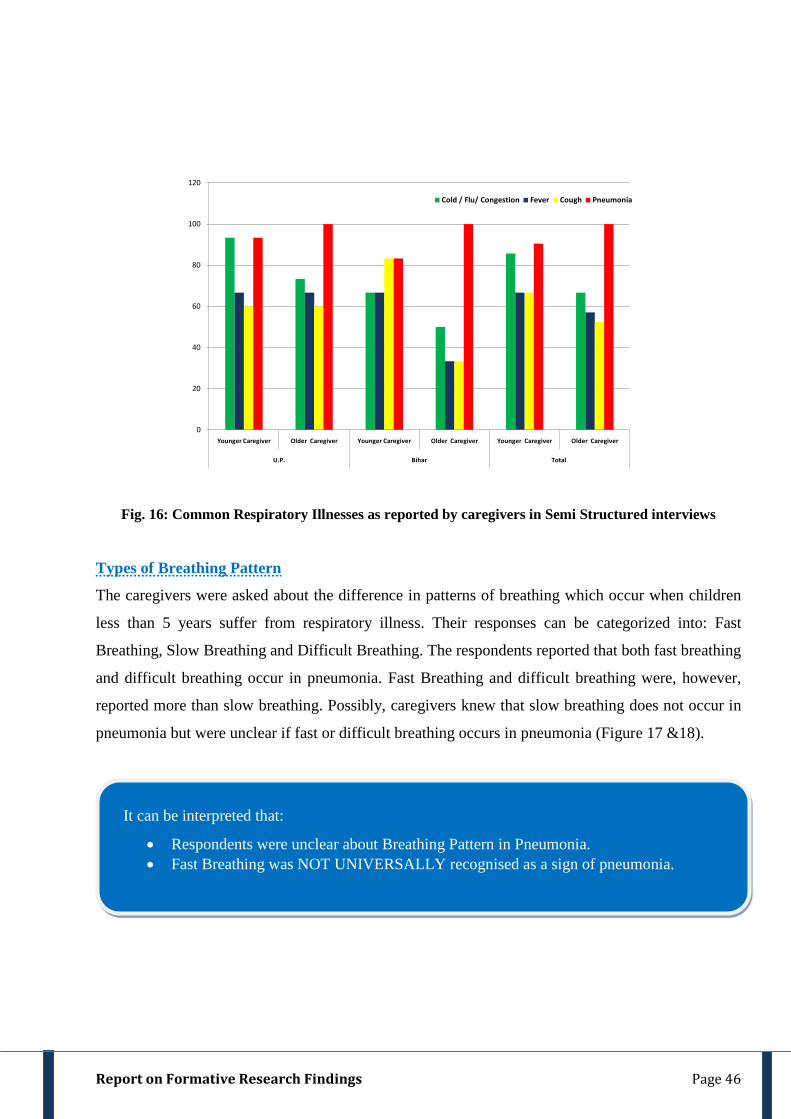
Report on Formative Research Findings Page 46
0
20
40
60
80
100
120
Younger Caregiver Older Caregiver Younger Caregiver Older Caregiver Younger Caregiver Older Caregiver
U.P. Bihar Total
Cold / Flu/ Congestion Fever Cough Pneumonia
Fig. 16: Common Respiratory Illnesses as reported by caregivers in Semi Structured interviews
Types of Breathing Pattern
The caregivers were asked about the difference in patterns of breathing which occur when children
less than 5 years suffer from respiratory illness. Their responses can be categorized into: Fast
Breathing, Slow Breathing and Difficult Breathing. The respondents reported that both fast breathing
and difficult breathing occur in pneumonia. Fast Breathing and difficult breathing were, however,
reported more than slow breathing. Possibly, caregivers knew that slow breathing does not occur in
pneumonia but were unclear if fast or difficult breathing occurs in pneumonia (Figure 17 &18).
It can be interpreted that:
• Respondents were unclear about Breathing Pattern in Pneumonia. • Fast Breathing was NOT UNIVERSALLY recognised as a sign of pneumonia.
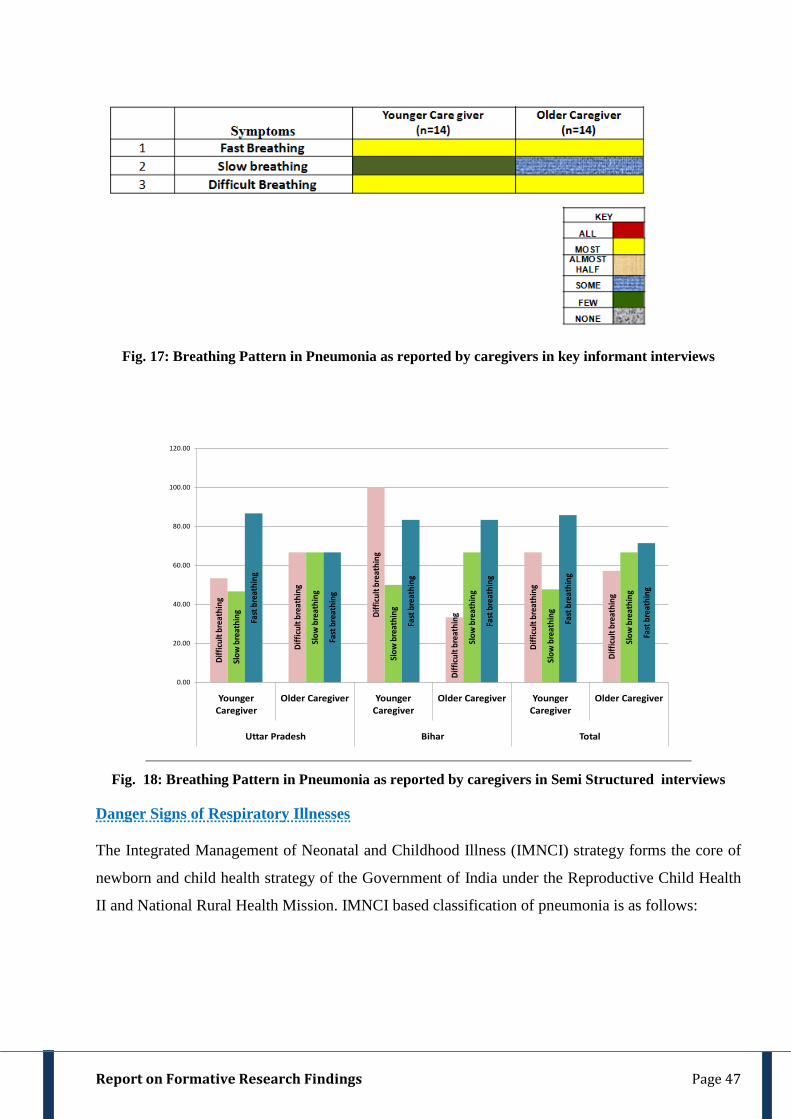
Report on Formative Research Findings Page 47
Fig. 17: Breathing Pattern in Pneumonia as reported by caregivers in key informant interviews
Diffi
cult
brea
thin
g
Diffi
cult
brea
thin
g
Diffi
cult
brea
thin
g
Diffi
cult
brea
thin
g
Diffi
cult
brea
thin
g
Diffi
cult
brea
thin
g
Slow
bre
athi
ng
Slow
bre
athi
ng
Slow
bre
athi
ng
Slow
bre
athi
ng
Slow
bre
athi
ng
Slow
bre
athi
ng
Fast
bre
athi
ng
Fast
bre
athi
ng
Fast
bre
athi
ng
Fast
bre
athi
ng
Fast
bre
athi
ng
Fast
bre
athi
ng
0.00
20.00
40.00
60.00
80.00
100.00
120.00
Younger Caregiver
Older Caregiver Younger Caregiver
Older Caregiver Younger Caregiver
Older Caregiver
Uttar Pradesh Bihar Total
Fig. 18: Breathing Pattern in Pneumonia as reported by caregivers in Semi Structured interviews
Danger Signs of Respiratory Illnesses The Integrated Management of Neonatal and Childhood Illness (IMNCI) strategy forms the core of
newborn and child health strategy of the Government of India under the Reproductive Child Health
II and National Rural Health Mission. IMNCI based classification of pneumonia is as follows:
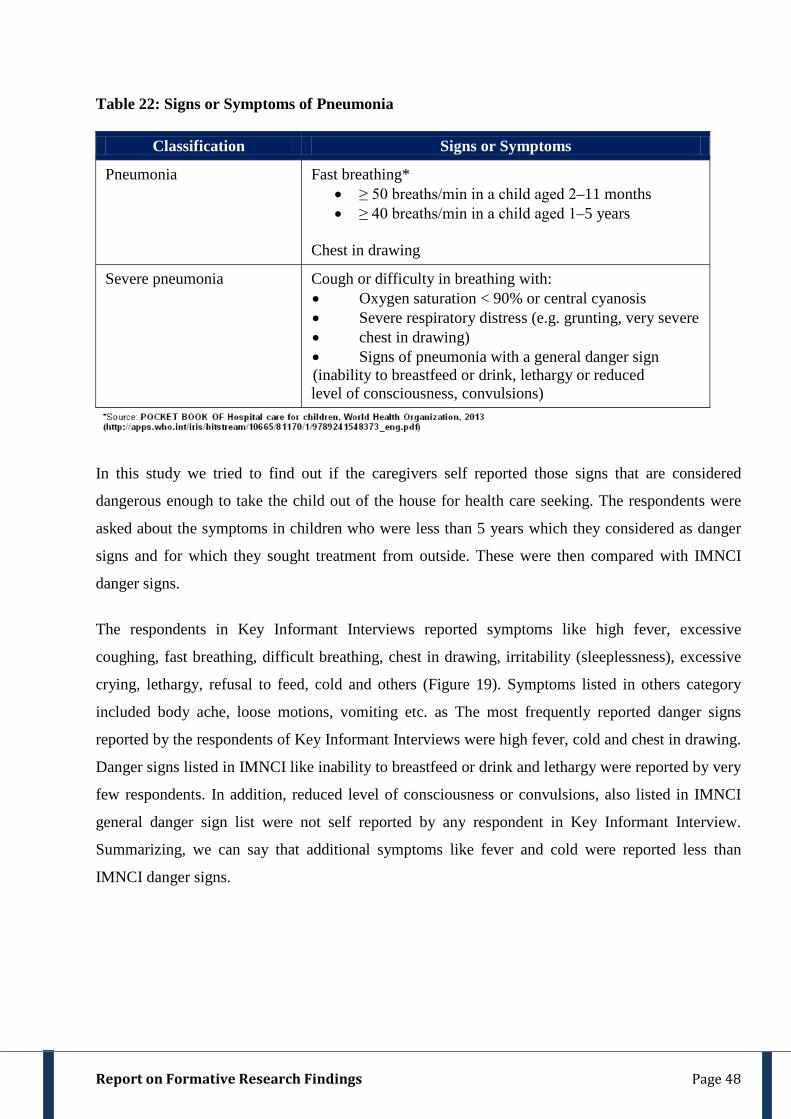
Report on Formative Research Findings Page 48
Table 22: Signs or Symptoms of Pneumonia
Classification Signs or Symptoms
Pneumonia Fast breathing* • ≥ 50 breaths/min in a child aged 2–11 months • ≥ 40 breaths/min in a child aged 1–5 years
Chest in drawing
Severe pneumonia Cough or difficulty in breathing with: • Oxygen saturation < 90% or central cyanosis • Severe respiratory distress (e.g. grunting, very severe • chest in drawing) • Signs of pneumonia with a general danger sign (inability to breastfeed or drink, lethargy or reduced level of consciousness, convulsions)
In this study we tried to find out if the caregivers self reported those signs that are considered
dangerous enough to take the child out of the house for health care seeking. The respondents were
asked about the symptoms in children who were less than 5 years which they considered as danger
signs and for which they sought treatment from outside. These were then compared with IMNCI
danger signs.
The respondents in Key Informant Interviews reported symptoms like high fever, excessive
coughing, fast breathing, difficult breathing, chest in drawing, irritability (sleeplessness), excessive
crying, lethargy, refusal to feed, cold and others (Figure 19). Symptoms listed in others category
included body ache, loose motions, vomiting etc. as The most frequently reported danger signs
reported by the respondents of Key Informant Interviews were high fever, cold and chest in drawing.
Danger signs listed in IMNCI like inability to breastfeed or drink and lethargy were reported by very
few respondents. In addition, reduced level of consciousness or convulsions, also listed in IMNCI
general danger sign list were not self reported by any respondent in Key Informant Interview.
Summarizing, we can say that additional symptoms like fever and cold were reported less than
IMNCI danger signs.
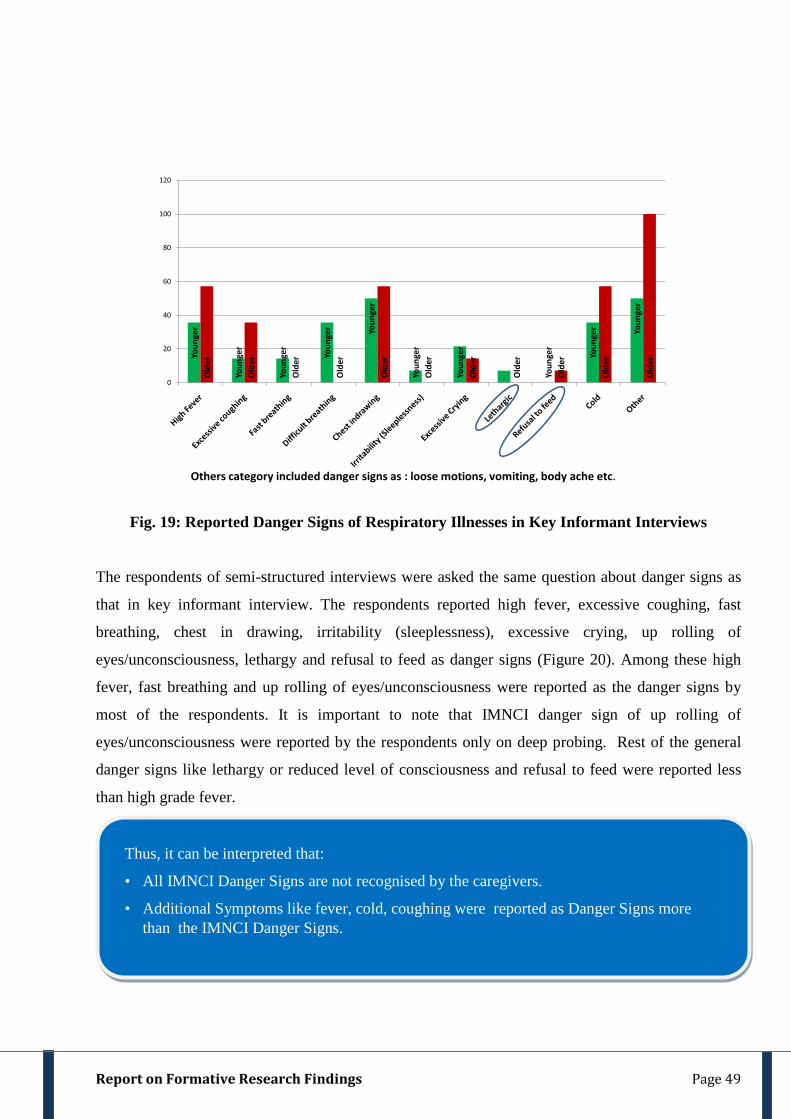
Report on Formative Research Findings Page 49
Youn
ger
Youn
ger
Youn
ger
Youn
ger Yo
unge
r
Youn
ger
Youn
ger
Youn
ger
Youn
ger Yo
unge
r
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
Old
er
0
20
40
60
80
100
120
Others category included danger signs as : loose motions, vomiting, body ache etc.
Fig. 19: Reported Danger Signs of Respiratory Illnesses in Key Informant Interviews
The respondents of semi-structured interviews were asked the same question about danger signs as
that in key informant interview. The respondents reported high fever, excessive coughing, fast
breathing, chest in drawing, irritability (sleeplessness), excessive crying, up rolling of
eyes/unconsciousness, lethargy and refusal to feed as danger signs (Figure 20). Among these high
fever, fast breathing and up rolling of eyes/unconsciousness were reported as the danger signs by
most of the respondents. It is important to note that IMNCI danger sign of up rolling of
eyes/unconsciousness were reported by the respondents only on deep probing. Rest of the general
danger signs like lethargy or reduced level of consciousness and refusal to feed were reported less
than high grade fever.
Thus, it can be interpreted that:
• All IMNCI Danger Signs are not recognised by the caregivers.
• Additional Symptoms like fever, cold, coughing were reported as Danger Signs more than the IMNCI Danger Signs.
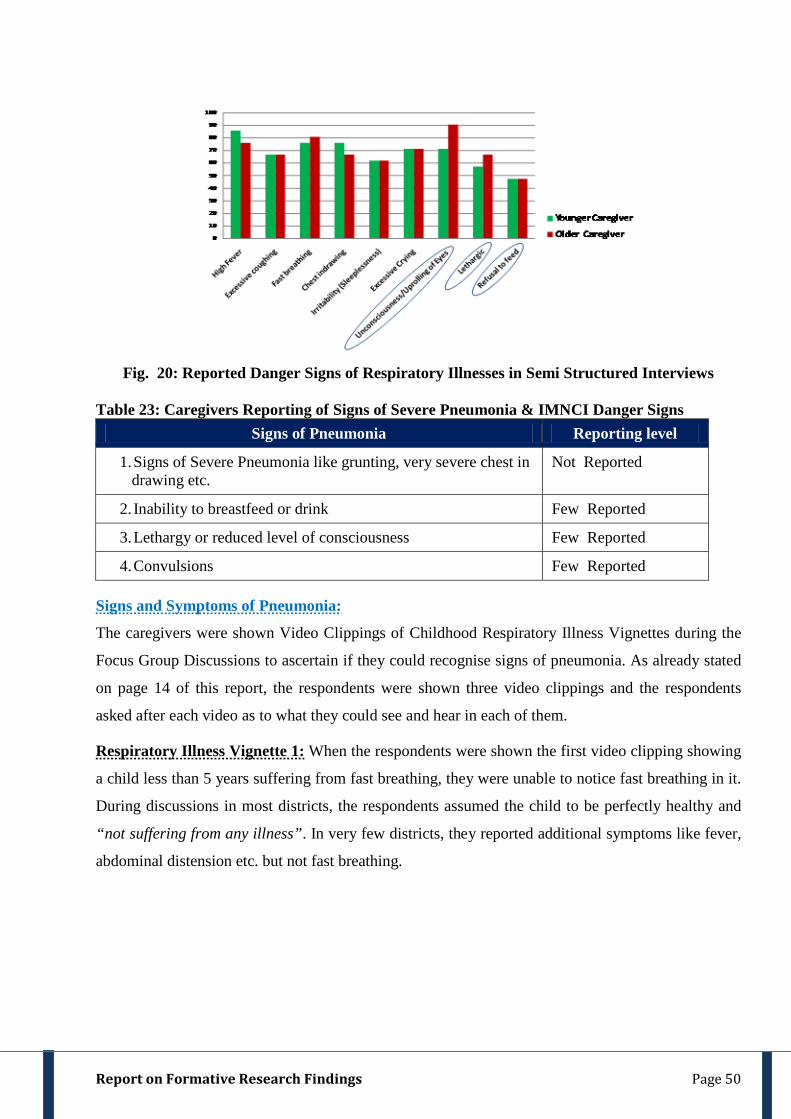
Report on Formative Research Findings Page 50
Fig. 20: Reported Danger Signs of Respiratory Illnesses in Semi Structured Interviews
Table 23: Caregivers Reporting of Signs of Severe Pneumonia & IMNCI Danger Signs
Signs of Pneumonia Reporting level
1. Signs of Severe Pneumonia like grunting, very severe chest in drawing etc.
Not Reported
2. Inability to breastfeed or drink Few Reported
3. Lethargy or reduced level of consciousness Few Reported
4. Convulsions Few Reported Signs and Symptoms of Pneumonia:
The caregivers were shown Video Clippings of Childhood Respiratory Illness Vignettes during the
Focus Group Discussions to ascertain if they could recognise signs of pneumonia. As already stated
on page 14 of this report, the respondents were shown three video clippings and the respondents
asked after each video as to what they could see and hear in each of them.
Respiratory Illness Vignette 1: When the respondents were shown the first video clipping showing
a child less than 5 years suffering from fast breathing, they were unable to notice fast breathing in it.
During discussions in most districts, the respondents assumed the child to be perfectly healthy and
“not suffering from any illness”. In very few districts, they reported additional symptoms like fever,
abdominal distension etc. but not fast breathing.
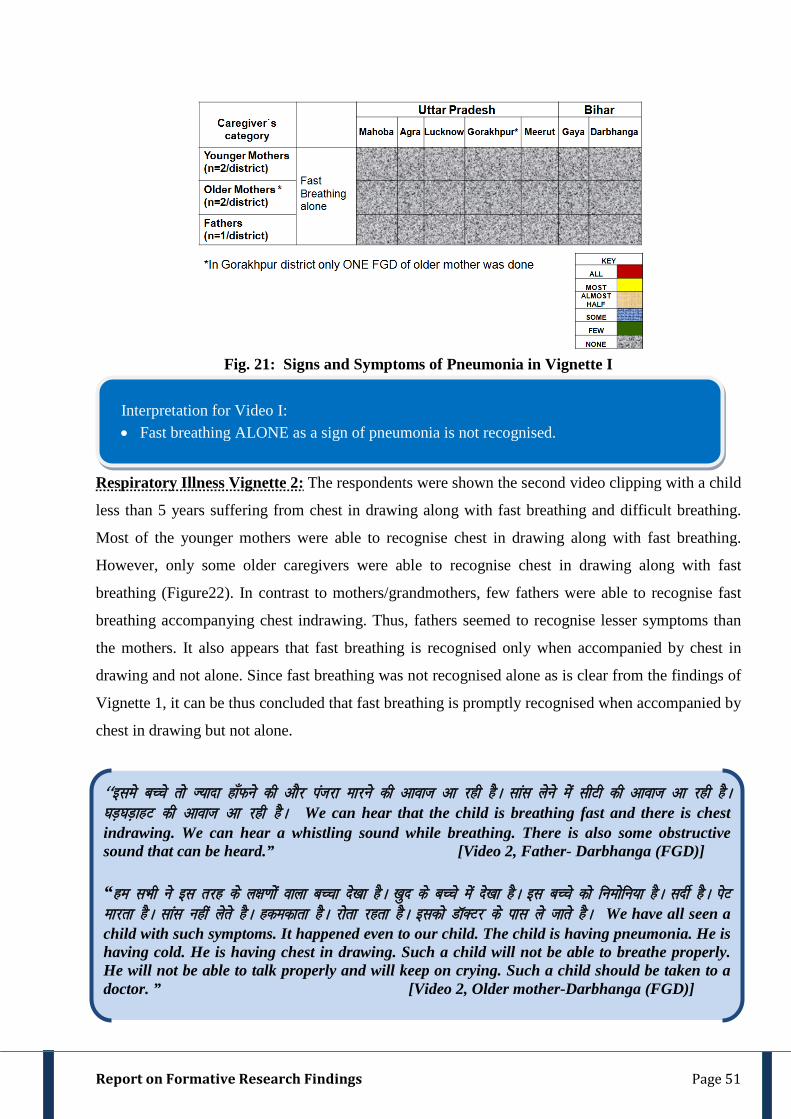
Report on Formative Research Findings Page 51
Fig. 21: Signs and Symptoms of Pneumonia in Vignette I
Respiratory Illness Vignette 2: The respondents were shown the second video clipping with a child
less than 5 years suffering from chest in drawing along with fast breathing and difficult breathing.
Most of the younger mothers were able to recognise chest in drawing along with fast breathing.
However, only some older caregivers were able to recognise chest in drawing along with fast
breathing (Figure22). In contrast to mothers/grandmothers, few fathers were able to recognise fast
breathing accompanying chest indrawing. Thus, fathers seemed to recognise lesser symptoms than
the mothers. It also appears that fast breathing is recognised only when accompanied by chest in
drawing and not alone. Since fast breathing was not recognised alone as is clear from the findings of
Vignette 1, it can be thus concluded that fast breathing is promptly recognised when accompanied by
chest in drawing but not alone.
Interpretation for Video I: • Fast breathing ALONE as a sign of pneumonia is not recognised.
^^bles cPps rks T;knk gk¡Qus dh vkSj iatjk ekjus dh vkokt vk jgh gSA lkal ysus esa lhVh dh vkokt vk jgh gSA ?kM+?kM+kgV dh vkokt vk jgh gSA We can hear that the child is breathing fast and there is chest indrawing. We can hear a whistling sound while breathing. There is also some obstructive sound that can be heard.” [Video 2, Father- Darbhanga (FGD)] “ge lHkh us bl rjg ds y{k.kksa okyk cPpk ns[kk gSA [kqn ds cPps esa ns[kk gSA bl cPps dks fueksfu;k gSA lnhZ gSA isV ekjrk gSA lkal ugha ysrs gSA gdedkrk gSA jksrk jgrk gSA bldks MkWDVj ds ikl ys tkrs gSA We have all seen a child with such symptoms. It happened even to our child. The child is having pneumonia. He is having cold. He is having chest in drawing. Such a child will not be able to breathe properly. He will not be able to talk properly and will keep on crying. Such a child should be taken to a doctor. ” [Video 2, Older mother-Darbhanga (FGD)]
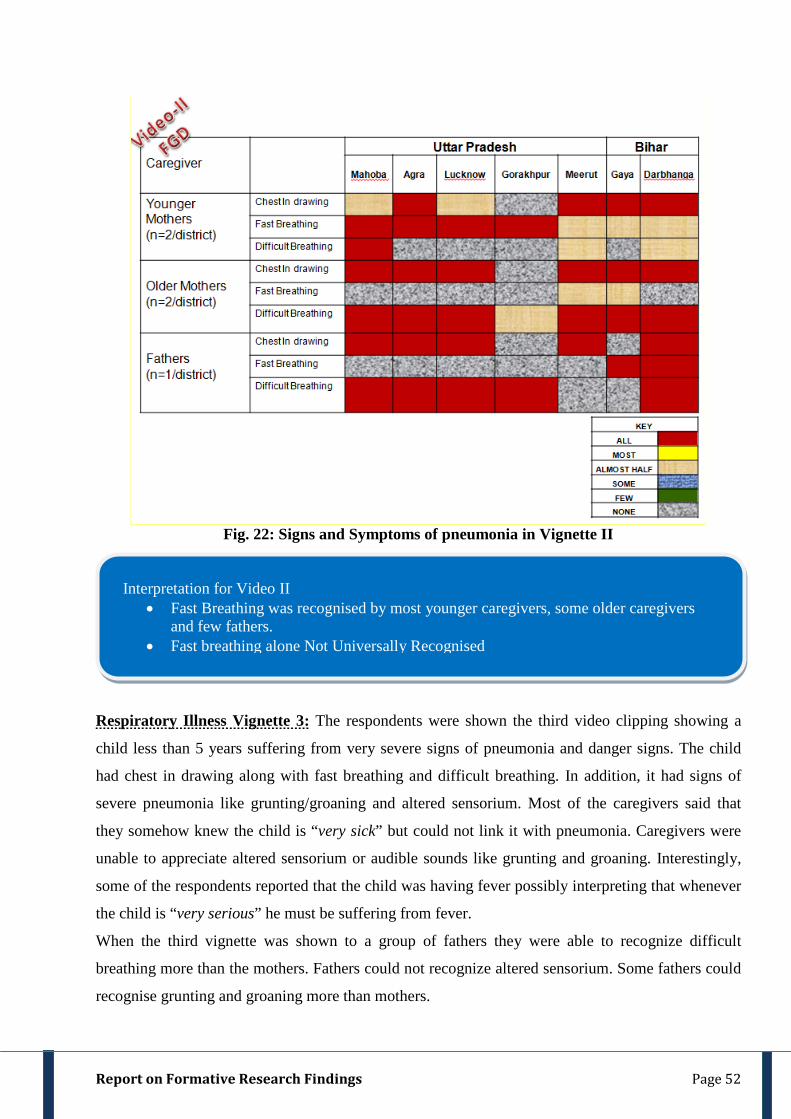
Report on Formative Research Findings Page 52
Fig. 22: Signs and Symptoms of pneumonia in Vignette II
Respiratory Illness Vignette 3: The respondents were shown the third video clipping showing a
child less than 5 years suffering from very severe signs of pneumonia and danger signs. The child
had chest in drawing along with fast breathing and difficult breathing. In addition, it had signs of
severe pneumonia like grunting/groaning and altered sensorium. Most of the caregivers said that
they somehow knew the child is “very sick” but could not link it with pneumonia. Caregivers were
unable to appreciate altered sensorium or audible sounds like grunting and groaning. Interestingly,
some of the respondents reported that the child was having fever possibly interpreting that whenever
the child is “very serious” he must be suffering from fever.
When the third vignette was shown to a group of fathers they were able to recognize difficult
breathing more than the mothers. Fathers could not recognize altered sensorium. Some fathers could
recognise grunting and groaning more than mothers.
Interpretation for Video II • Fast Breathing was recognised by most younger caregivers, some older caregivers
and few fathers. • Fast breathing alone Not Universally Recognised
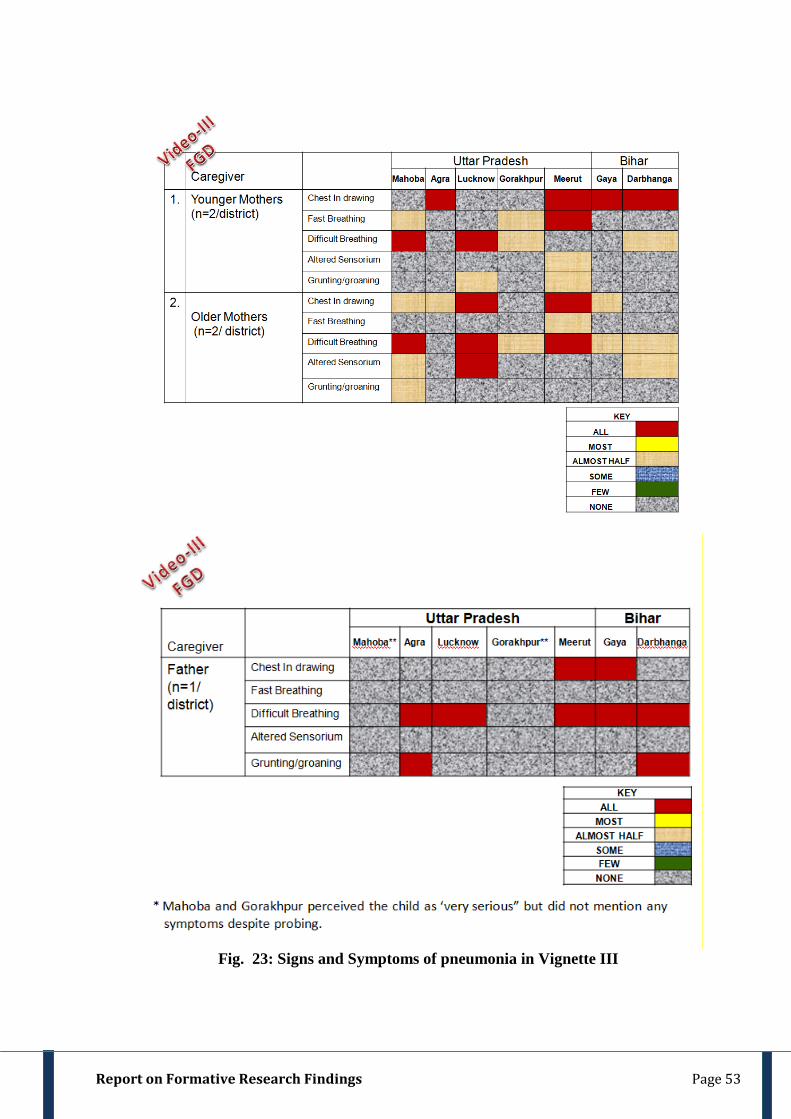
Report on Formative Research Findings Page 53
Fig. 23: Signs and Symptoms of pneumonia in Vignette III

Report on Formative Research Findings Page 54
Interpretation for Video III • Caregiver knew the child is “very sick” but could not link it with pneumonia.
*Interestingly some respondents also perceived child in video was having fever.
• Caregiver could not appreciate altered sensorium or audible sounds like grunting and groaning.
• Fathers were able to recognise difficult breathing more than the mothers
• Some fathers could recognise grunting and groaning more than mothers.
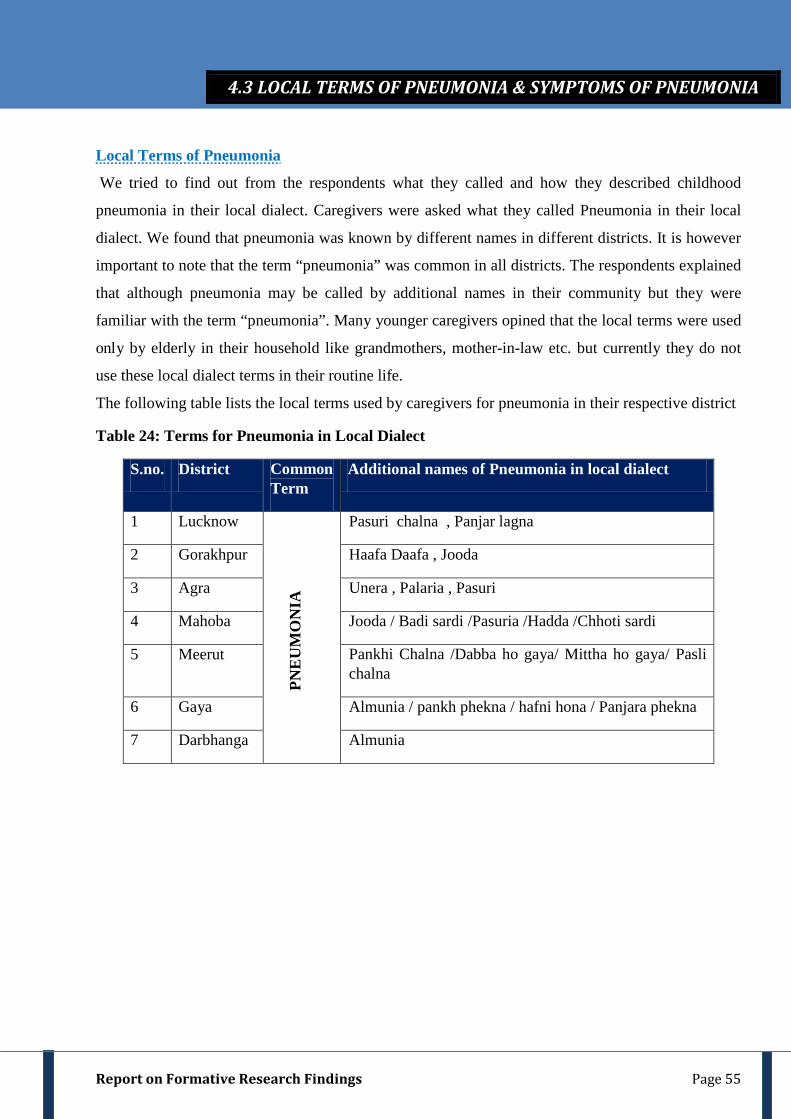
Report on Formative Research Findings Page 55
Local Terms of Pneumonia
We tried to find out from the respondents what they called and how they described childhood
pneumonia in their local dialect. Caregivers were asked what they called Pneumonia in their local
dialect. We found that pneumonia was known by different names in different districts. It is however
important to note that the term “pneumonia” was common in all districts. The respondents explained
that although pneumonia may be called by additional names in their community but they were
familiar with the term “pneumonia”. Many younger caregivers opined that the local terms were used
only by elderly in their household like grandmothers, mother-in-law etc. but currently they do not
use these local dialect terms in their routine life.
The following table lists the local terms used by caregivers for pneumonia in their respective district
Table 24: Terms for Pneumonia in Local Dialect
S.no. District Common Term
Additional names of Pneumonia in local dialect
1 Lucknow
PNE
UM
ON
IA
Pasuri chalna , Panjar lagna
2 Gorakhpur Haafa Daafa , Jooda
3 Agra Unera , Palaria , Pasuri
4 Mahoba Jooda / Badi sardi /Pasuria /Hadda /Chhoti sardi
5 Meerut Pankhi Chalna /Dabba ho gaya/ Mittha ho gaya/ Pasli chalna
6 Gaya Almunia / pankh phekna / hafni hona / Panjara phekna
7 Darbhanga Almunia
4.3 LOCAL TERMS OF PNEUMONIA & SYMPTOMS OF PNEUMONIA
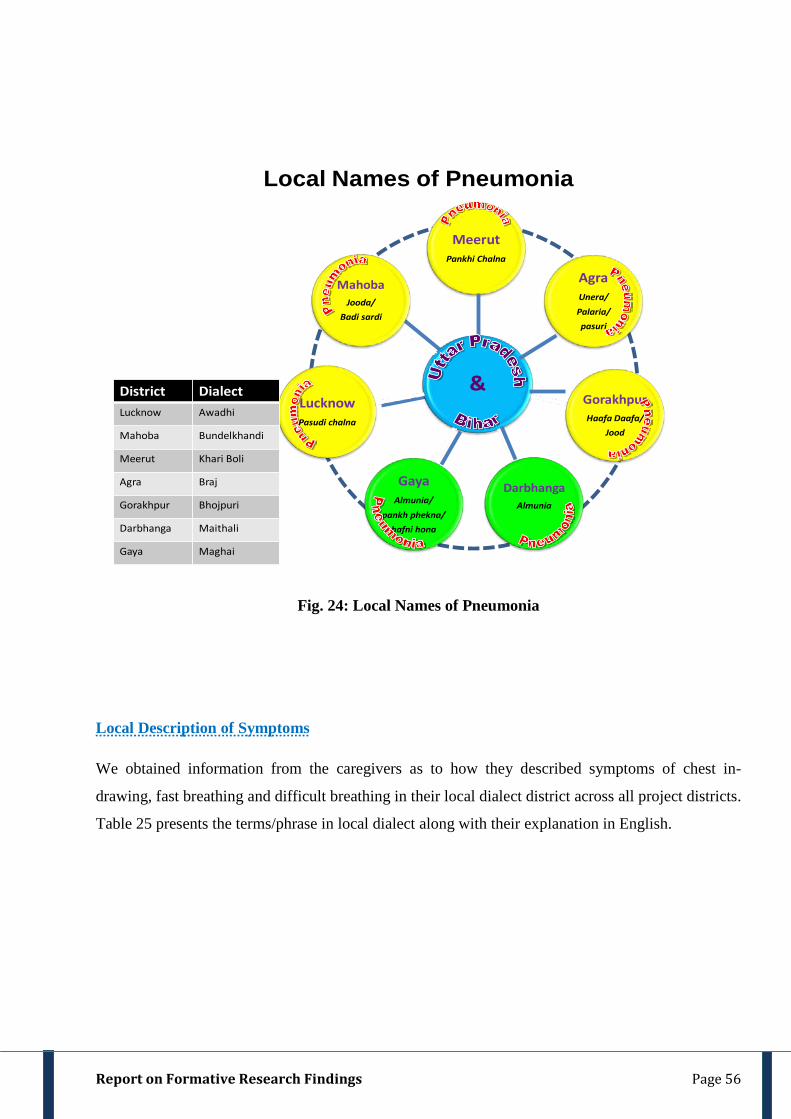
Report on Formative Research Findings Page 56
Local Names of Pneumonia
&
MeerutPankhi Chalna
AgraUnera/Palaria/pasuri
GorakhpurHaafa Daafa/
Jood
DarbhangaAlmunia
GayaAlmunia/
pankh phekna/hafni hona
LucknowPasudi chalna
MahobaJooda/
Badi sardi
District DialectLucknow Awadhi
Mahoba Bundelkhandi
Meerut Khari Boli
Agra Braj
Gorakhpur Bhojpuri
Darbhanga Maithali
Gaya Maghai
Fig. 24: Local Names of Pneumonia
Local Description of Symptoms
We obtained information from the caregivers as to how they described symptoms of chest in-
drawing, fast breathing and difficult breathing in their local dialect district across all project districts.
Table 25 presents the terms/phrase in local dialect along with their explanation in English.
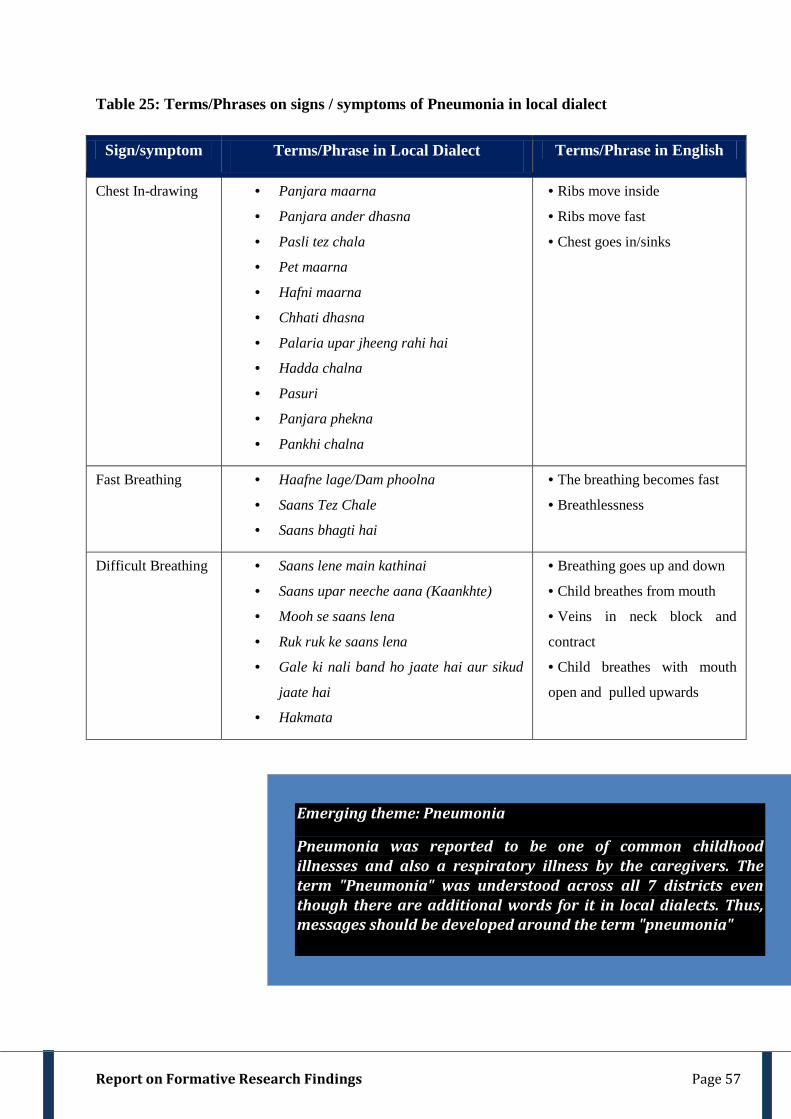
Report on Formative Research Findings Page 57
Table 25: Terms/Phrases on signs / symptoms of Pneumonia in local dialect
Sign/symptom Terms/Phrase in Local Dialect Terms/Phrase in English
Chest In-drawing • Panjara maarna
• Panjara ander dhasna
• Pasli tez chala
• Pet maarna
• Hafni maarna
• Chhati dhasna
• Palaria upar jheeng rahi hai
• Hadda chalna
• Pasuri
• Panjara phekna
• Pankhi chalna
• Ribs move inside
• Ribs move fast
• Chest goes in/sinks
Fast Breathing • Haafne lage/Dam phoolna
• Saans Tez Chale
• Saans bhagti hai
• The breathing becomes fast
• Breathlessness
Difficult Breathing • Saans lene main kathinai
• Saans upar neeche aana (Kaankhte)
• Mooh se saans lena
• Ruk ruk ke saans lena
• Gale ki nali band ho jaate hai aur sikud
jaate hai
• Hakmata
• Breathing goes up and down
• Child breathes from mouth
• Veins in neck block and
contract
• Child breathes with mouth
open and pulled upwards
Emerging theme: Pneumonia
Pneumonia was reported to be one of common childhood illnesses and also a respiratory illness by the caregivers. The term "Pneumonia" was understood across all 7 districts even though there are additional words for it in local dialects. Thus, messages should be developed around the term "pneumonia"
Report on Formative Research Findings Page 58
Information was elicited about the home remedies given to children less than 5 years who suffered
from respiratory illness. They were also asked to explain as to how the home remedy was prepared,
for how long was it administered to the child and how was it administered to a sick child .
We prepared a list of all the remedies that were prepared at home by the caregivers. From this list,
we segregated remedies based on the method of administration of home remedies into:
o Home Remedies that were used for Topical Application
o Home Remedies that were used for Oral administration
o Home Remedies that were used for both Topical and Oral Administration.
These remedies included under each category were common across all project districts. The
respondents reported that the information about these home remedies has percolated from the elders
in their family very often from grandmother/grandfather of the child. Sometimes they obtained
information from other persons in locality. Most of these remedies were used for 1-2 days or until
the illness did not subside. The period till the remedies were used depended on the perception of the
caregivers about the severity of disease. The caregivers administered home remedies till they
perceived illness to be manageable at home and “not severe”. As soon as they felt that it cannot be
managed at home, they sought medical advice outside their home.
Home Remedies Commonly Used for Topical Application
Home remedies were applied on the chest, forehead and palms of hand and on the toes of the child.
They were prepared using different ingredients in different types of oil or by extracting juices of
locally available wild herbs/plants. Egg was another ingredient commonly used in many topically
applied home remedies. Vicks Vaporub (Topical Ointment with medicated vapors) was also
commonly used for topical application. List of commonly applied home remedies is presented in
Table 26
4.4. HOME REMEDIES & SELF MEDICATION
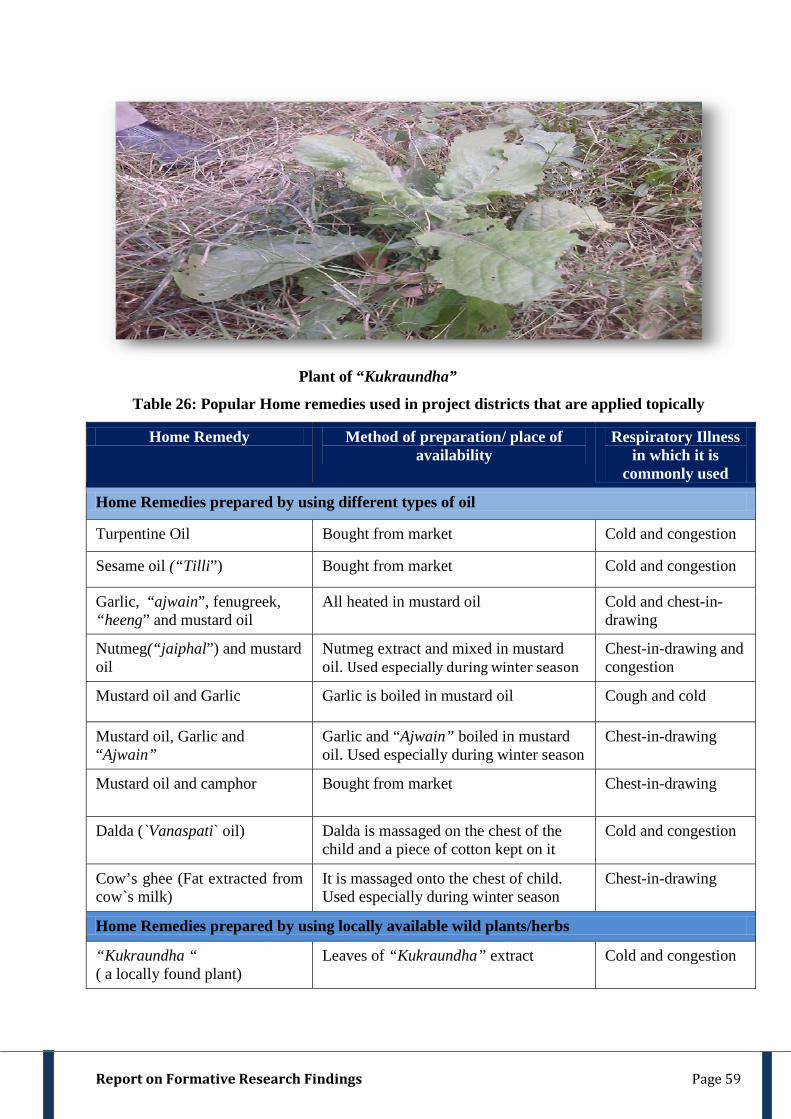
Report on Formative Research Findings Page 59
Plant of “Kukraundha”
Table 26: Popular Home remedies used in project districts that are applied topically
Home Remedy Method of preparation/ place of availability
Respiratory Illness in which it is
commonly used
Home Remedies prepared by using different types of oil
Turpentine Oil Bought from market Cold and congestion
Sesame oil (“Tilli”) Bought from market Cold and congestion
Garlic, “ajwain”, fenugreek, “heeng” and mustard oil
All heated in mustard oil Cold and chest-in-drawing
Nutmeg(“jaiphal”) and mustard oil
Nutmeg extract and mixed in mustard oil. Used especially during winter season
Chest-in-drawing and congestion
Mustard oil and Garlic Garlic is boiled in mustard oil Cough and cold
Mustard oil, Garlic and “Ajwain”
Garlic and “Ajwain” boiled in mustard oil. Used especially during winter season
Chest-in-drawing
Mustard oil and camphor Bought from market Chest-in-drawing
Dalda (`Vanaspati` oil) Dalda is massaged on the chest of the child and a piece of cotton kept on it
Cold and congestion
Cow’s ghee (Fat extracted from cow`s milk)
It is massaged onto the chest of child. Used especially during winter season
Chest-in-drawing
Home Remedies prepared by using locally available wild plants/herbs
“Kukraundha “ ( a locally found plant)
Leaves of “Kukraundha” extract Cold and congestion
Report on Formative Research Findings Page 60
“Gendla” (a locally found plant)
Leaves of “Gendla” extract Cold
Home Remedies prepared by using eggs
Crude egg Massage with yolk of crude egg Cold and congestion
Egg Yolk of egg poured on a plain paper and pasted on the chest of sick child
Chest-in-drawing
Additional remedies used at home
Vicks Bought from market Cold
Fomentation by cotton cloth Cloth is fomented on fire. Cold and congestion
Home Remedies Commonly Used for Oral Administration
Information was obtained from the caregivers on home remedies that were administered orally to the
child who suffered from respiratory illness. Some home remedies were prepared using ingredients
easily available at home like turmeric, nutmeg, fats, ginger, honey, garlic etc. Sometimes juice of
extracts of herbs/locally available plants like “seej”, basil (“tulsi”) etc. were given to treat respiratory
illness. Occasionally, locally available commercially packaged non–allopathic tablets like
“Sanjeevani” and Musk (“kasturi”) tablets were given to the sick child. They were easily available at
the village grocery store or chemist shop at an affordable price. (Table 27).
Table 27: Popular Home remedies used in project districts that are given orally
Home Remedy Method of preparation/place of availability
Illness in which it is commonly used
Home Remedies prepared by using different ingredients easily available at home
Turmeric and Nutmeg Turmeric and Nutmeg extracted and mixed in mother’s milk
Cold
Turmeric and “ghee” (clarified butter)
Both mixed together Congestion
Garlic Garlic crushed and burnt in earthen lamp then given with mother’s milk
Cold
Asafetida (“Heeng”) It is mixed with mother’s milk and given to the child
Cold and stomach related ailment.
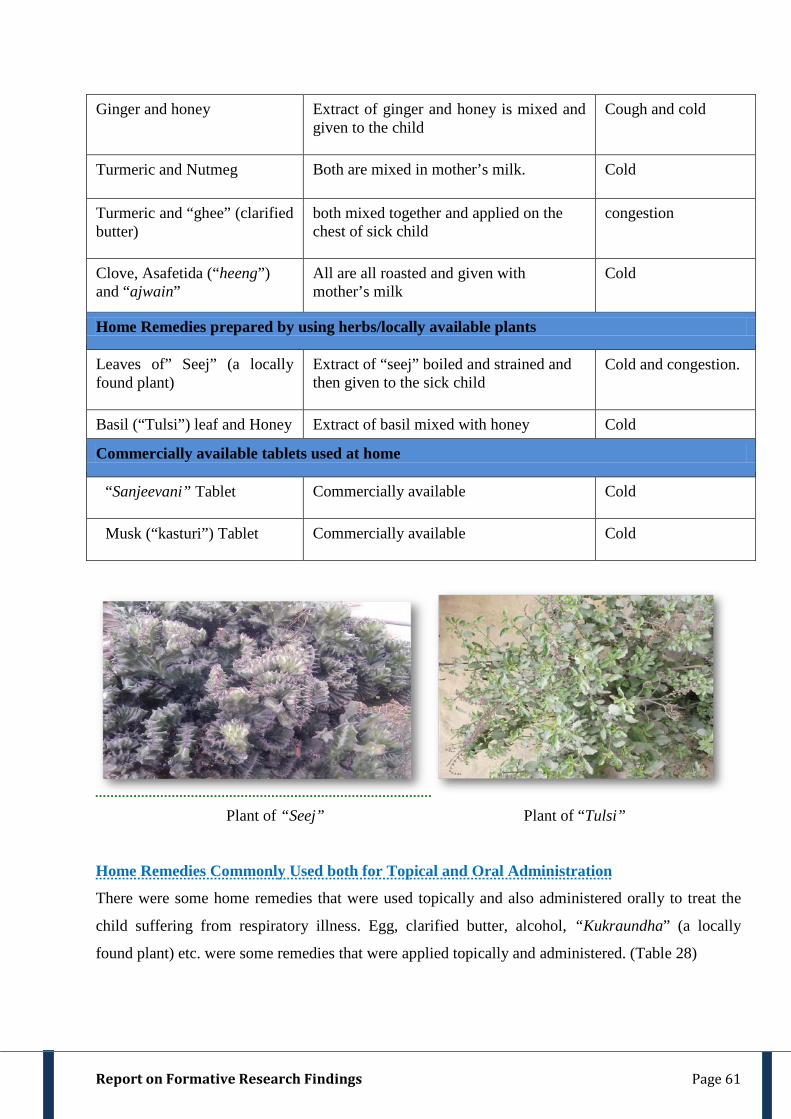
Report on Formative Research Findings Page 61
Ginger and honey Extract of ginger and honey is mixed and given to the child
Cough and cold
Turmeric and Nutmeg Both are mixed in mother’s milk. Cold
Turmeric and “ghee” (clarified butter)
both mixed together and applied on the chest of sick child
congestion
Clove, Asafetida (“heeng”) and “ajwain”
All are all roasted and given with mother’s milk
Cold
Home Remedies prepared by using herbs/locally available plants
Leaves of” Seej” (a locally found plant)
Extract of “seej” boiled and strained and then given to the sick child
Cold and congestion.
Basil (“Tulsi”) leaf and Honey Extract of basil mixed with honey Cold
Commercially available tablets used at home
“Sanjeevani” Tablet Commercially available Cold
Musk (“kasturi”) Tablet Commercially available Cold
Plant of “Seej” Plant of “Tulsi”
Home Remedies Commonly Used both for Topical and Oral Administration
There were some home remedies that were used topically and also administered orally to treat the
child suffering from respiratory illness. Egg, clarified butter, alcohol, “Kukraundha” (a locally
found plant) etc. were some remedies that were applied topically and administered. (Table 28)
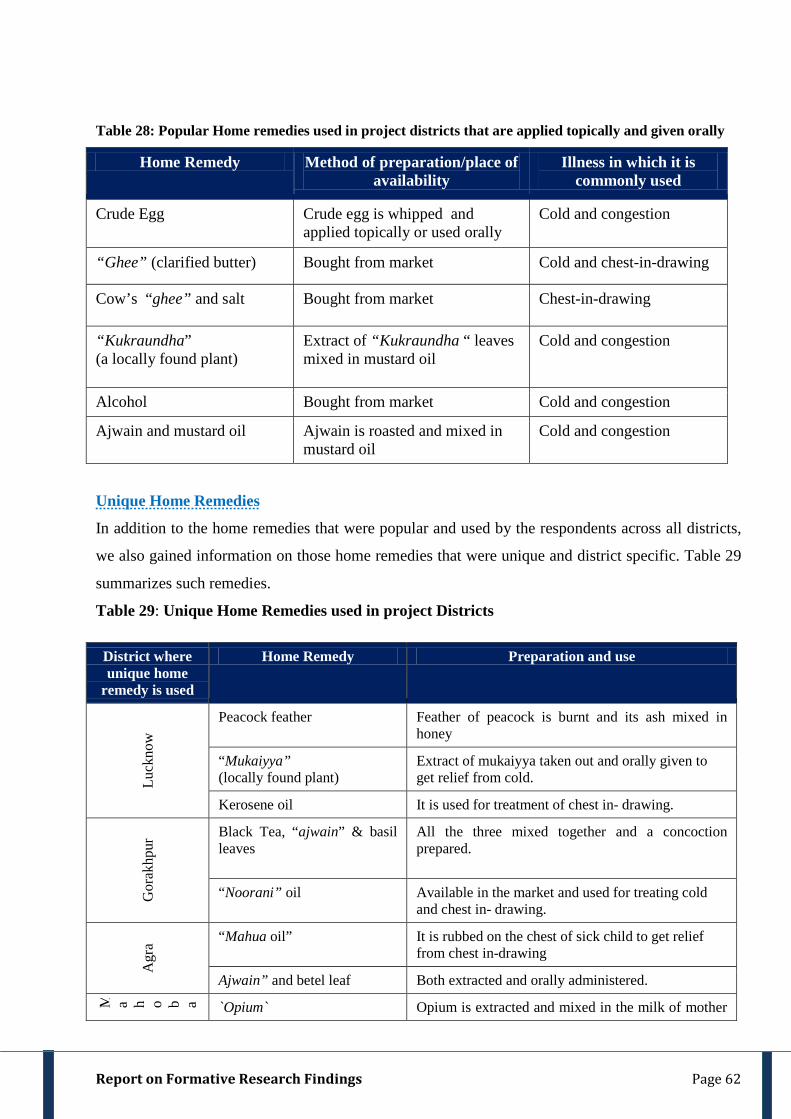
Report on Formative Research Findings Page 62
Table 28: Popular Home remedies used in project districts that are applied topically and given orally
Home Remedy Method of preparation/place of availability
Illness in which it is commonly used
Crude Egg Crude egg is whipped and applied topically or used orally
Cold and congestion
“Ghee” (clarified butter) Bought from market Cold and chest-in-drawing
Cow’s “ghee” and salt Bought from market Chest-in-drawing
“Kukraundha” (a locally found plant)
Extract of “Kukraundha “ leaves mixed in mustard oil
Cold and congestion
Alcohol Bought from market Cold and congestion
Ajwain and mustard oil Ajwain is roasted and mixed in mustard oil
Cold and congestion
Unique Home Remedies
In addition to the home remedies that were popular and used by the respondents across all districts,
we also gained information on those home remedies that were unique and district specific. Table 29
summarizes such remedies.
Table 29: Unique Home Remedies used in project Districts
District where unique home
remedy is used
Home Remedy Preparation and use
Luck
now
Peacock feather Feather of peacock is burnt and its ash mixed in honey
“Mukaiyya” (locally found plant)
Extract of mukaiyya taken out and orally given to get relief from cold.
Kerosene oil It is used for treatment of chest in- drawing.
Gor
akhp
ur Black Tea, “ajwain” & basil
leaves All the three mixed together and a concoction prepared.
“Noorani” oil Available in the market and used for treating cold and chest in- drawing.
Agr
a “Mahua oil”
It is rubbed on the chest of sick child to get relief from chest in-drawing
Ajwain” and betel leaf Both extracted and orally administered.
M a h o b a `Opium` Opium is extracted and mixed in the milk of mother
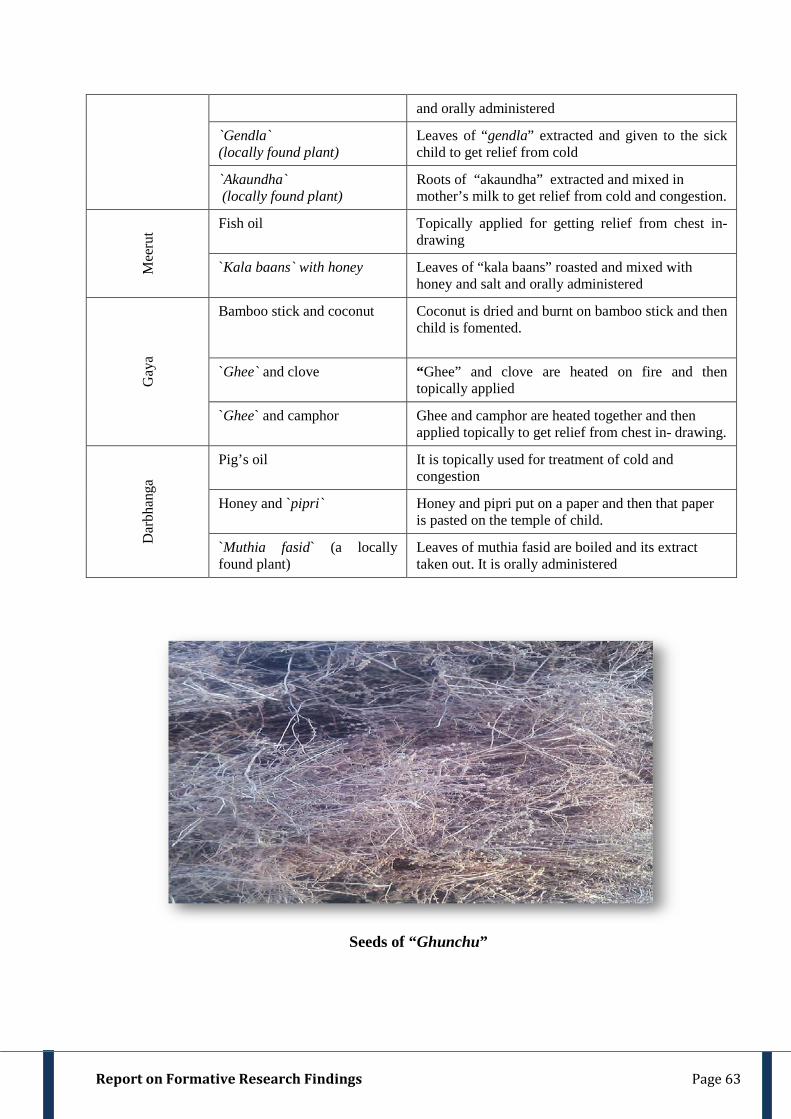
Report on Formative Research Findings Page 63
and orally administered
`Gendla` (locally found plant)
Leaves of “gendla” extracted and given to the sick child to get relief from cold
`Akaundha` (locally found plant)
Roots of “akaundha” extracted and mixed in mother’s milk to get relief from cold and congestion.
Mee
rut Fish oil Topically applied for getting relief from chest in-
drawing
`Kala baans` with honey Leaves of “kala baans” roasted and mixed with honey and salt and orally administered
Gay
a
Bamboo stick and coconut Coconut is dried and burnt on bamboo stick and then child is fomented.
`Ghee` and clove “Ghee” and clove are heated on fire and then topically applied
`Ghee` and camphor Ghee and camphor are heated together and then applied topically to get relief from chest in- drawing.
Dar
bhan
ga
Pig’s oil It is topically used for treatment of cold and congestion
Honey and `pipri`
Honey and pipri put on a paper and then that paper is pasted on the temple of child.
`Muthia fasid` (a locally found plant)
Leaves of muthia fasid are boiled and its extract taken out. It is orally administered
Seeds of “Ghunchu”

Report on Formative Research Findings Page 64
Fig. 25: Unique Home Remedies of Uttar Pradesh & Bihar
Self Medication
We discussed from the caregivers if they self medicated when their child suffered from respiratory
illnesses. Only few caregivers reported self-prescription. Caregivers named oral antibiotic medicines
like Amoxicillin and Septran and injectible antibiotics like Gentamycin, Monoceff, antipyretics like
Paracetamol, Crocin, Calpol and Combiflam, anti tussives like Imbrodil and Corex syrup. Cortico-
steroids like Betnisol, Broncho–dilator like Deriphylin, injection/tablet and anti-diarrheal,
antispasmodics and also topical medicines. The caregivers who shared the names of medicines
clarified that self-prescription was done only until they perceived illness to be manageable at home.
Caregiver generally named more than one medicine. Some caregivers also reported use of Over the
Counter(OTC) Drugs like “Sanjeevani” tablets, Musk deer “Kasturi” tablets, “Vicks” (vaporizer
ointment) “Pudinhara”(a digestive syrup made from herbs), “Anand kar”, “Ajoobi”(a balm for
headache) and “Raahat rooh oil”. The formulations of some OTC drugs are unknown.
Caregivers mostly purchased the drugs from the local grocery store and sometimes from local
chemist. They also said that they stored the medicines at home and sometimes used stored
blisters/bottles of medicines earlier prescribed by RMPs without consulting any practitioner.

Report on Formative Research Findings Page 65
After the self-prescription or home remedies failed to show any improvement the caregivers decided
to seek care from outside. The decision making process has been dealt in detail in the subsequent
chapter.
^^ ,d ckj MkDVj dks fn[kykrs gSa nok j[kh jgrh gSA ;fn cPpk ml nok ls Bhd gks x;k rks fQj t:jr iM+us ij mls fiykrs gSaA Medicine is kept at home. In case the child had got well on using that particular medicine, it is used again when required” [Caregiver, BKT, (FGD)]
MkDVj tks nok nsrs gSa mldk uke 'kh'ks ij fy[k nsrs gSaA tc cPpk nksckjk chekj iM+rk gS ogh ns nsrs gSaA We write names of medicines on bottles. When the child gets ill we use the same bottles of medicine.” [Caregiver, BKT (FGD)]
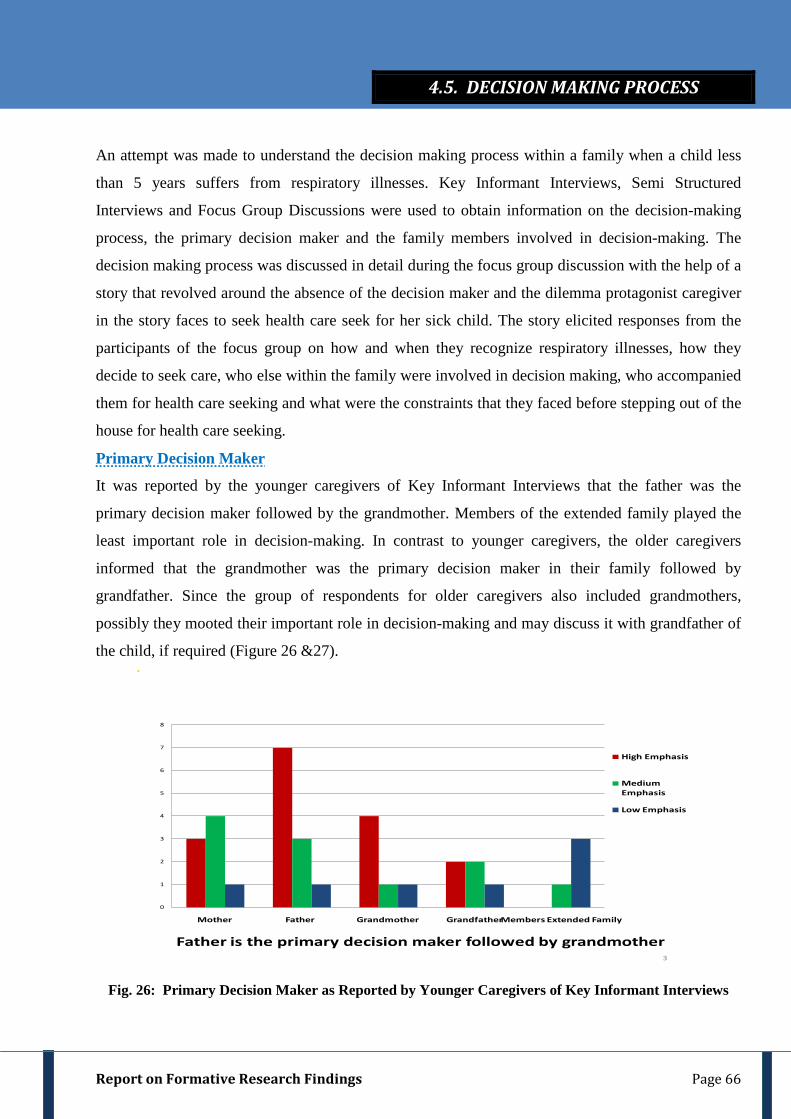
Report on Formative Research Findings Page 66
An attempt was made to understand the decision making process within a family when a child less
than 5 years suffers from respiratory illnesses. Key Informant Interviews, Semi Structured
Interviews and Focus Group Discussions were used to obtain information on the decision-making
process, the primary decision maker and the family members involved in decision-making. The
decision making process was discussed in detail during the focus group discussion with the help of a
story that revolved around the absence of the decision maker and the dilemma protagonist caregiver
in the story faces to seek health care seek for her sick child. The story elicited responses from the
participants of the focus group on how and when they recognize respiratory illnesses, how they
decide to seek care, who else within the family were involved in decision making, who accompanied
them for health care seeking and what were the constraints that they faced before stepping out of the
house for health care seeking.
Primary Decision Maker
It was reported by the younger caregivers of Key Informant Interviews that the father was the
primary decision maker followed by the grandmother. Members of the extended family played the
least important role in decision-making. In contrast to younger caregivers, the older caregivers
informed that the grandmother was the primary decision maker in their family followed by
grandfather. Since the group of respondents for older caregivers also included grandmothers,
possibly they mooted their important role in decision-making and may discuss it with grandfather of
the child, if required (Figure 26 &27).
Father is the primary decision maker followed by grandmother
0
1
2
3
4
5
6
7
8
Mother Father Grandmother GrandfatherMembers Extended Family
High Emphasis
Medium Emphasis
Low Emphasis
3
Fig. 26: Primary Decision Maker as Reported by Younger Caregivers of Key Informant Interviews
4.5. DECISION MAKING PROCESS
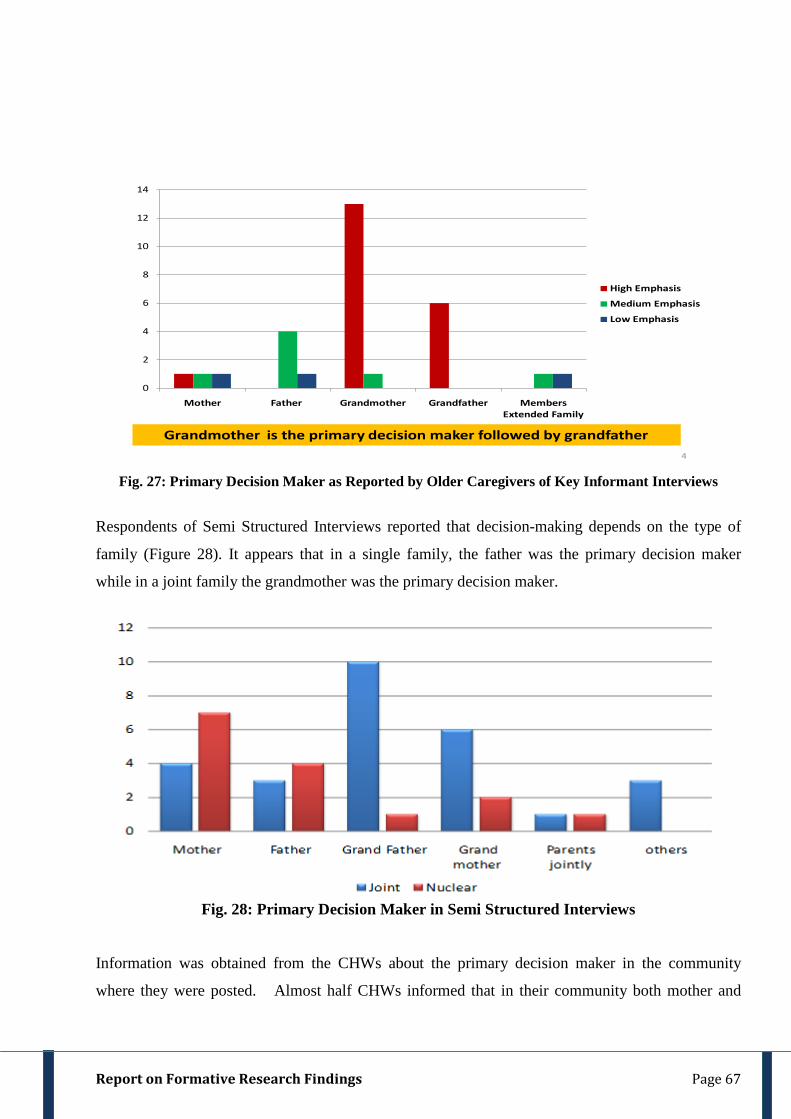
Report on Formative Research Findings Page 67
Grandmother is the primary decision maker followed by grandfather 4
0
2
4
6
8
10
12
14
Mother Father Grandmother Grandfather Members Extended Family
High Emphasis
Medium Emphasis
Low Emphasis
Fig. 27: Primary Decision Maker as Reported by Older Caregivers of Key Informant Interviews
Respondents of Semi Structured Interviews reported that decision-making depends on the type of
family (Figure 28). It appears that in a single family, the father was the primary decision maker
while in a joint family the grandmother was the primary decision maker.
Fig. 28: Primary Decision Maker in Semi Structured Interviews
Information was obtained from the CHWs about the primary decision maker in the community
where they were posted. Almost half CHWs informed that in their community both mother and

Report on Formative Research Findings Page 68
father were the primary decision makers. However, some CHWs named both grandfather and
grandmother as the primary decision makers.
Decision Making Process The mothers were not the primary decision makers. Discussions during focus groups clearly
indicated that the mother is the first to recognize illness as she spends more time with the child than
any other family member. Even the father who participated in focus group discussion clearly opined
that mothers are “responsible for the child” and thus “she is the first to notice that the child is
unwell”. They added that even before alarming the family to seek health care from outside, she
usually tries out home remedy. They added that it is only when the mother found the home remedies
ineffective thereafter she approached the primary decision maker for further advice. The father of
the child is involved at this stage of decision making if it is single family. Within the joint family,
the father along with grandmother/grandfather may be involved the decision- making. In case the
Thus for Primary Decision Making, it can be interpreted that
• Mother is NOT the Primary Decision maker
o First to recognise illness BUT not the sole decision maker. She INFORMS
“primary decision makers”
• Other People within the family were primary Decision makers
o Father (Single family).
o Grandmother/grandfather (Joint family).
• Thus the trio finally involved in decision making are:
o Mother+ Father+ Grandmother/Grandfather
^^Ekk¡&cki ¼ekrk&firk½ gh fu.kZ; ysrs gSaA Only mother-father are the primary decision makers" [CHW-Agra (Key Informant)]
^^llqj dk QSlyk eq[; gksrk gSaA Father-in-law (grandfather) is the main decision maker"
[CHW-Darbhanga (Key Informant)]
^^?kj ds cM+s] nknk&nknh ;k ukuk ukuhA Elders of the family. Grandfather-grandmother or maternal grandfather grandmother".
[CHW –Gaya (Key Informant)]
Report on Formative Research Findings Page 69
primary decision maker is absent then the mother may use the mobile to seek advice from him for
further plan of action.
Person accompanying sick child for seeking health care
Most of the respondents reported that they sought help from other family members for health care
seeking. Most of them sought help from the father of the child or the grandfather or grandmother.
However, some of them opined that they may go alone to the village based rural medical practitioner
if they perceived the sickness to be unmanageable and there was an urgency.
The respondents added that if they had to visit a health facility or a practitioner outside the village
then they seek the help of their family members. They opined that they may take the help of
neighbours or relatives if the primary decision maker within their family was not present.
The CHW`s were also asked about the members of a family who according to them accompanied the
sick child for health care seeking in their community. Almost half CHWs perceived that both mother
and father accompany the sick child for health care seeking. Some CHWs also informed that
grandfather might accompany the sick child for health care seeking. Few CHWs reported either
father or grandfather might accompany the sick child for health care seeking.
We collected information from the RMP as to which family members usually accompanied the sick
child to their clinic. Most RMPs said that often mother alone would carry the sick child to their
clinic. Almost half reported father as the family member who often accompanies the sick child.
Some RMPs said grandfather/grandmother may come with the child.
^^cPps ds ekrk&firk vkrs gSaA Both mother and father come with the child" [CHW, Agra (Key Informant)]
^^cPps ds ekrk&firk] nknk&nknh vkrs gSaA T;knkrj cPps dh ek¡&nknk vkrs gSaA xk¡o dk ;gh :y gS] fd cPps dh ek¡ vk;sxh vkSj mldk nknk cPps ds lkFk vk;sxkA firk dHkh dHkkj vkrs gSaA Child’s mother-father, grandfather-grandmother come. Mostly, mother and grandfather come with the child. Rule of the village is that mother will always be accompanied by grandfather. Father comes rarely". [ CHW , Mahoba (Key Informant)]
^^ igys ek¡ gh ijs’kku gksrh gSA ifr dks crkrh gSA igys viuk mipkj djrh gSA It is the mother who first gets upset (when she notices that the child is sick). She then tells her husband. First she does treatment at home". [Father, Gorakhpur (FGD)]
Report on Formative Research Findings Page 70
Thus after triangulating information from the key informant interview, semi structured
interview and focus group discussion it can be interpreted that:
• The mother was reported to be the first person to recognise and report “if the child is
sick or needs to be taken out”
• After this she consults either her husband or in-laws for health care-seeking. This
may be in two ways:
o Face-to-face discussion
o Discussion over mobile
• The mother is accompanied by either the husband or the members of extended
family to accompany her for health care seeking.
Emerging Theme: Decision Making for Health Care Seeking Mother is responsible for the recognition of illness. Decision making for health care seeking is done by the father along with the grandmother / grandfather especially in a joint family.

Report on Formative Research Findings Page 71
Caregivers were asked about the health care seeking behavior when their child less than 5 years
suffers from respiratory illness. We tried to elicit information from the respondents on the range of
health care providers available within their community and the factors that influence community`s
health seeking behavior and choice of health care providers. The health seeking behavior was
understood from both the caregivers perspective and care providers perspective. The respondents of
key informant interviews and semi structured interviews were narrated some sickness scenarios
while the respondents of focus group discussions were shown video clippings on clinical illness
vignettes and response obtained from them on who and why would they visit for health care seeking,
thinking prospectively.
Sickness Scenario I
Caregivers Perspective on Sickness Scenario I
The respondents of Key Informant Interviews were narrated Sickness Scenario I and were asked
about the type of facility/practitioner they would choose for the treatment of child in similar
scenario. Some of the caregivers in U.P. opined that they would choose services of a village based
RMP or a BBD in such scenario. In Bihar, all the younger mothers and most of the older mothers
preferred village based RMP over BBD as none mothers chose a BBD in such scenario. Few of the
caregivers in U.P. also expressed the need of visiting a government facility in such scenario.
Traditional Healer was chosen by only a few care givers. Few younger and older mothers in U.P.
opined that they would prefer to visit a traditional healer in such scenario. In contrast in Bihar none
opined visiting a traditional healer in such condition (Figure 29).
Illness Vignette on Sickness Scenario I(Video Clip)
Child less than 5 years having only fast breathing as a symptom of pneumonia
Sickness Scenario I (Narrated)
Child less than 5 yrs. is having cough, runny nose and is warm to touch. He/she is otherwise healthy and is also feeding/ breastfeeding normally
4.6. HEALTH CARE SEEKING BEHAVIOR OF CAREGIVERS
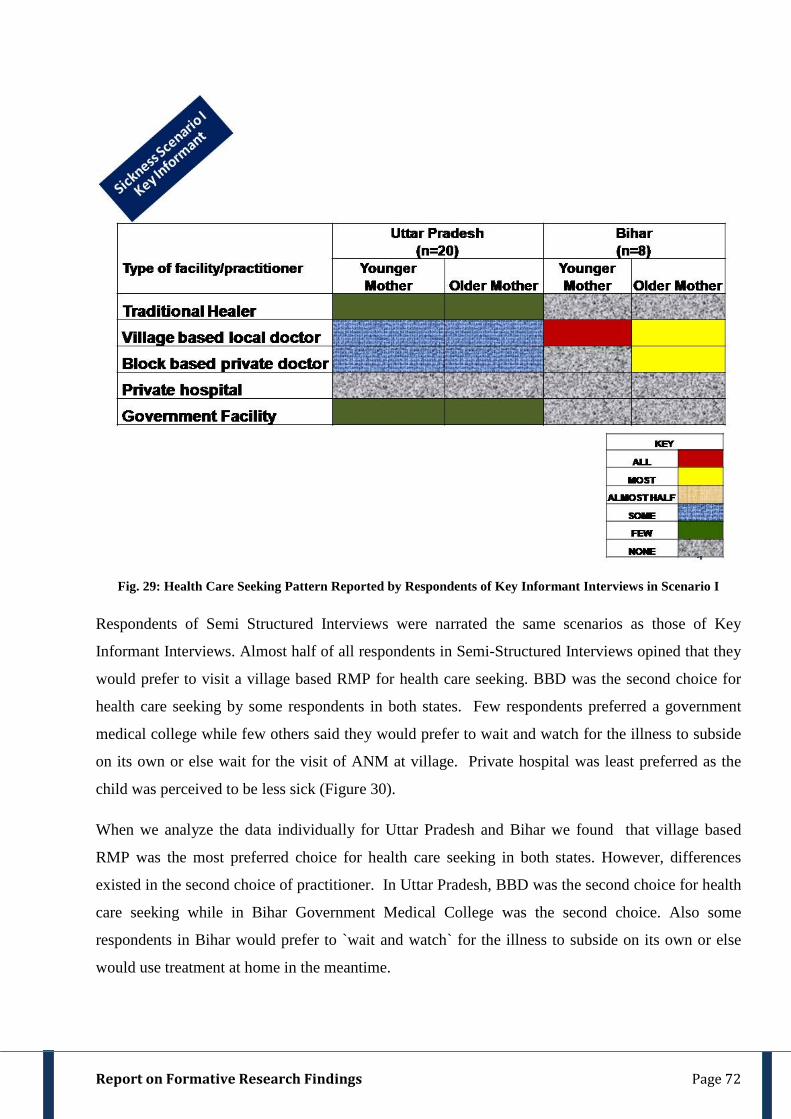
Report on Formative Research Findings Page 72
Fig. 29: Health Care Seeking Pattern Reported by Respondents of Key Informant Interviews in Scenario I
Respondents of Semi Structured Interviews were narrated the same scenarios as those of Key
Informant Interviews. Almost half of all respondents in Semi-Structured Interviews opined that they
would prefer to visit a village based RMP for health care seeking. BBD was the second choice for
health care seeking by some respondents in both states. Few respondents preferred a government
medical college while few others said they would prefer to wait and watch for the illness to subside
on its own or else wait for the visit of ANM at village. Private hospital was least preferred as the
child was perceived to be less sick (Figure 30).
When we analyze the data individually for Uttar Pradesh and Bihar we found that village based
RMP was the most preferred choice for health care seeking in both states. However, differences
existed in the second choice of practitioner. In Uttar Pradesh, BBD was the second choice for health
care seeking while in Bihar Government Medical College was the second choice. Also some
respondents in Bihar would prefer to `wait and watch` for the illness to subside on its own or else
would use treatment at home in the meantime.
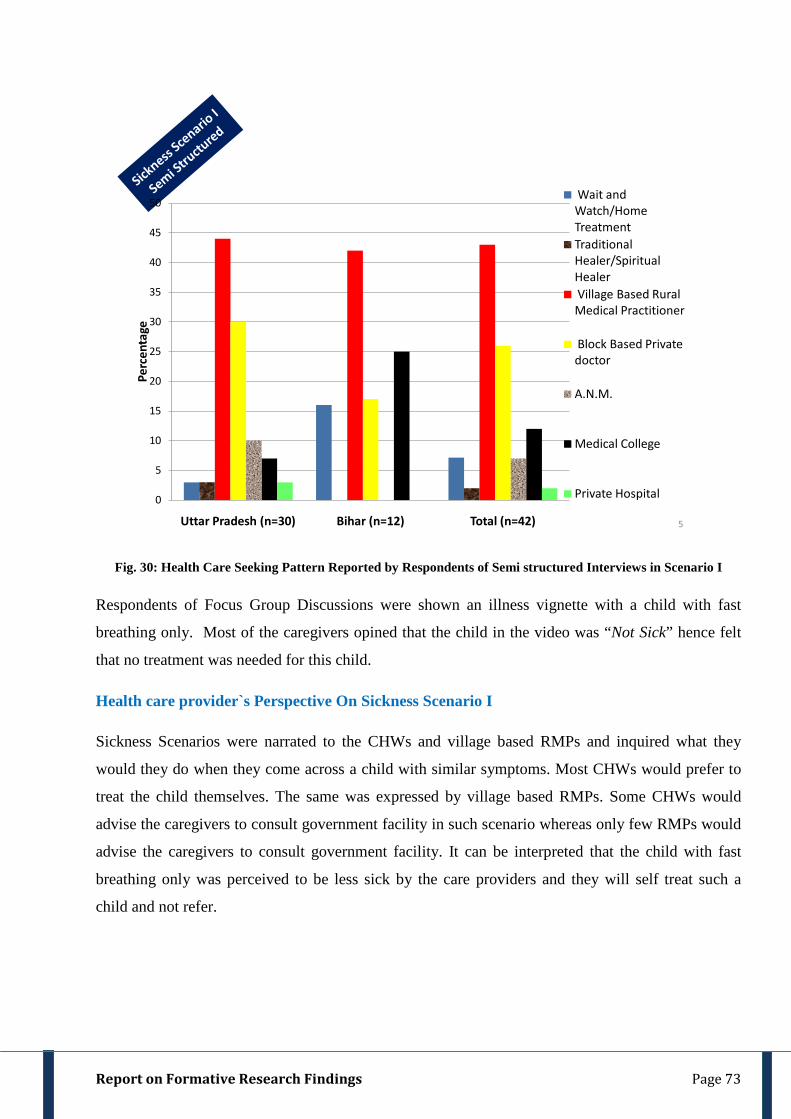
Report on Formative Research Findings Page 73
5
0
5
10
15
20
25
30
35
40
45
50
Uttar Pradesh (n=30) Bihar (n=12) Total (n=42)
Perc
enta
ge
Wait and Watch/Home TreatmentTraditional Healer/Spiritual HealerVillage Based Rural Medical Practitioner
Block Based Private doctor
A.N.M.
Medical College
Private Hospital
Fig. 30: Health Care Seeking Pattern Reported by Respondents of Semi structured Interviews in Scenario I
Respondents of Focus Group Discussions were shown an illness vignette with a child with fast
breathing only. Most of the caregivers opined that the child in the video was “Not Sick” hence felt
that no treatment was needed for this child.
Health care provider`s Perspective On Sickness Scenario I
Sickness Scenarios were narrated to the CHWs and village based RMPs and inquired what they
would they do when they come across a child with similar symptoms. Most CHWs would prefer to
treat the child themselves. The same was expressed by village based RMPs. Some CHWs would
advise the caregivers to consult government facility in such scenario whereas only few RMPs would
advise the caregivers to consult government facility. It can be interpreted that the child with fast
breathing only was perceived to be less sick by the care providers and they will self treat such a
child and not refer.

Report on Formative Research Findings Page 74
Sickness Scenario II:
Caregivers of Key Informant Interviews were narrated Sickness Scenario II and were asked in detail
about the type of facility/practitioner they would choose for their sick child suffering with similar
situation. In U.P. few of the younger and older caregivers said that they would prefer to go to village
based RMP for treatment .In contrast, in Bihar, most younger and all older caregivers would choose
to go to village based RMP. Most caregivers in U.P and younger mothers in Bihar would prefer to
visit a BBD for a child in similar sitaution. None of the caregivers preferred to avail the facilities of
either private hospital or government facility in such a situation (Figure 31).
Illness Vignette on Sickness Scenario II (Video Clip)
Child less than 5 years having fast breathing , difficult breathing and chest in- drawing.
Sickness Scenario II (Narrated)
Child less than 5 yrs. is having cough, runny nose fever, fast breathing and chest in-drawing. He/she is also feeding/ breastfeeding less than usual.
Emerging Theme: Sickness scenario I
Emerging theme in scenario I is that since caregivers perceived the child “Not Sick” hence no treatment was required to this child. If the child is “Mild” sick then they would consult traditional healer and village based rural medical practitioner. Likewise, in the case of care providers emerging theme is that all of them would treat themselves and would not refer the child in scenario I.
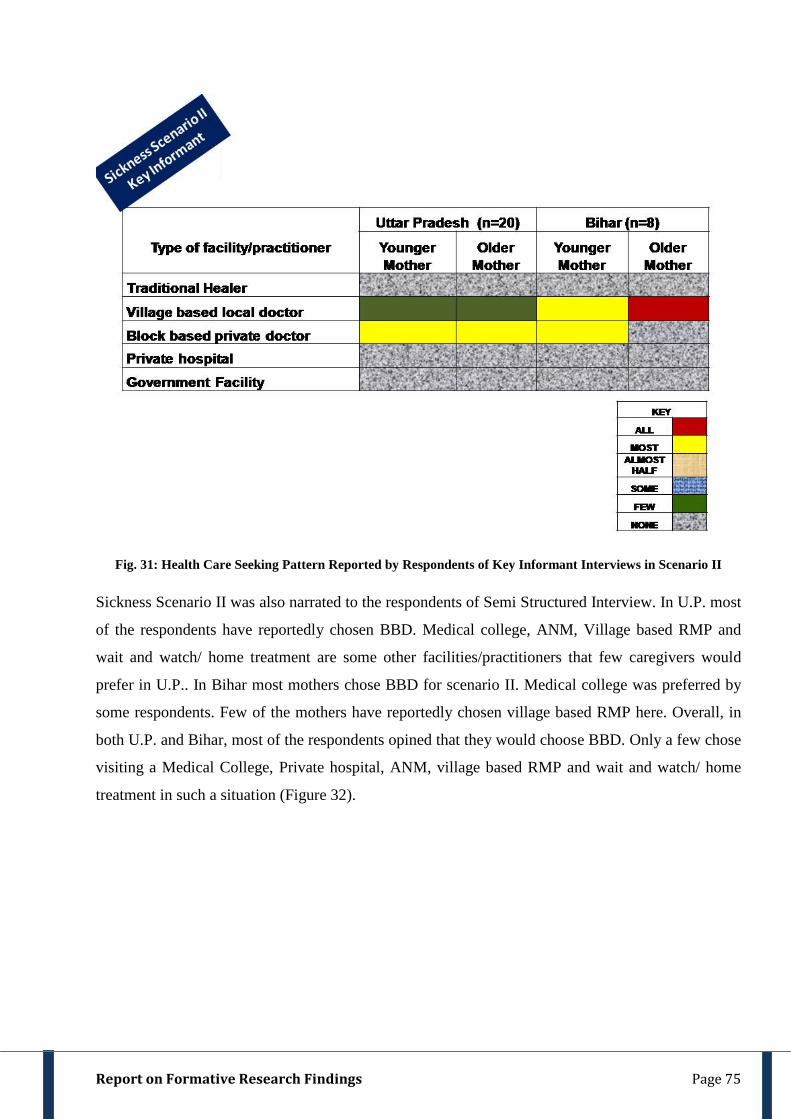
Report on Formative Research Findings Page 75
Fig. 31: Health Care Seeking Pattern Reported by Respondents of Key Informant Interviews in Scenario II
Sickness Scenario II was also narrated to the respondents of Semi Structured Interview. In U.P. most
of the respondents have reportedly chosen BBD. Medical college, ANM, Village based RMP and
wait and watch/ home treatment are some other facilities/practitioners that few caregivers would
prefer in U.P.. In Bihar most mothers chose BBD for scenario II. Medical college was preferred by
some respondents. Few of the mothers have reportedly chosen village based RMP here. Overall, in
both U.P. and Bihar, most of the respondents opined that they would choose BBD. Only a few chose
visiting a Medical College, Private hospital, ANM, village based RMP and wait and watch/ home
treatment in such a situation (Figure 32).

Report on Formative Research Findings Page 76
11
0
10
20
30
40
50
60
70
80
Uttar Pradesh (n=30)
Bihar (n=12) Total (n=42)
Wait and Watch/Home Treatment
Village Based Local Doctor
Block Based Private doctor
A.N.M.
Medical College
Fig. 32: Health Care Seeking Pattern Reported by Respondents of Semi structured Interviews in Scenario II
Video II: Focus Group discussion
Respondents of focus group discussion were shown an illness vignette and health care seeking
discussed in detail in response to sick child.
Video Clip during the Focus Group Discussion with CHW in Gorakhpur
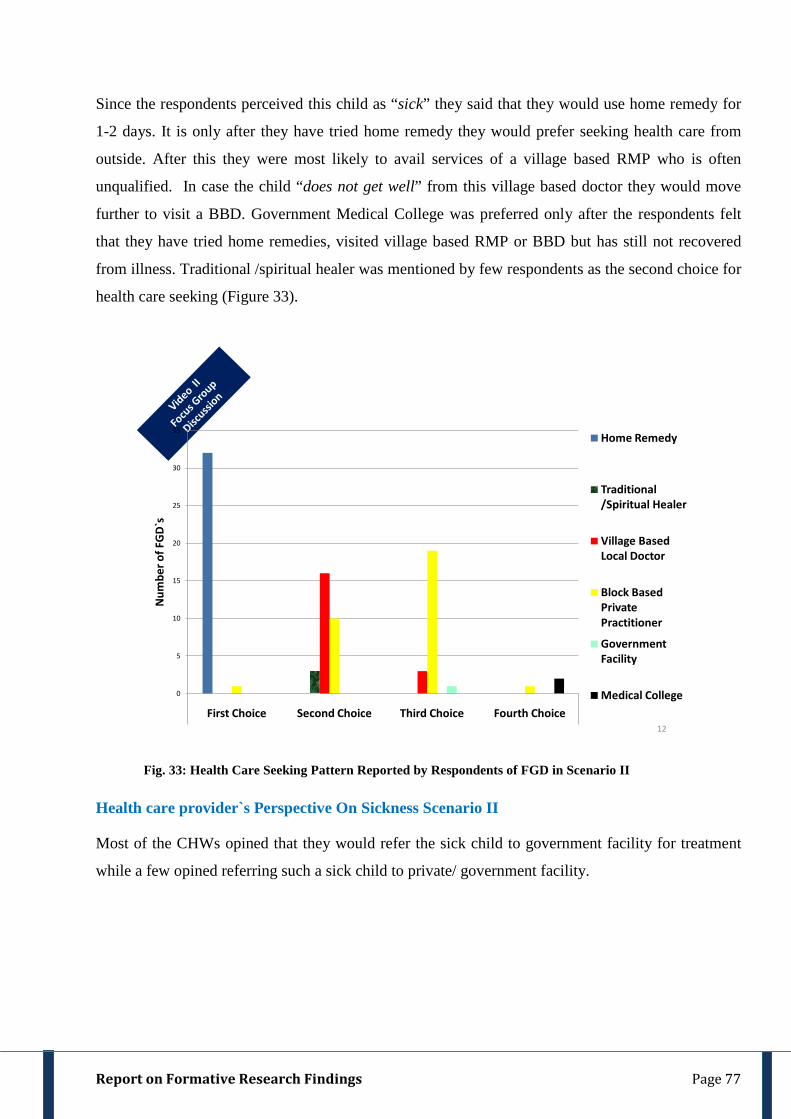
Report on Formative Research Findings Page 77
Since the respondents perceived this child as “sick” they said that they would use home remedy for
1-2 days. It is only after they have tried home remedy they would prefer seeking health care from
outside. After this they were most likely to avail services of a village based RMP who is often
unqualified. In case the child “does not get well” from this village based doctor they would move
further to visit a BBD. Government Medical College was preferred only after the respondents felt
that they have tried home remedies, visited village based RMP or BBD but has still not recovered
from illness. Traditional /spiritual healer was mentioned by few respondents as the second choice for
health care seeking (Figure 33).
0
5
10
15
20
25
30
35
First Choice Second Choice Third Choice Fourth Choice
Num
ber o
f FG
D`s
Home Remedy
Traditional /Spiritual Healer
Village Based Local Doctor
Block Based Private Practitioner
Government Facility
Medical College
12
Fig. 33: Health Care Seeking Pattern Reported by Respondents of FGD in Scenario II
Health care provider`s Perspective On Sickness Scenario II
Most of the CHWs opined that they would refer the sick child to government facility for treatment
while a few opined referring such a sick child to private/ government facility.

Report on Formative Research Findings Page 78
Almost half village based RMP opined that they would prefer themselves to provide treatment to a
sick child with similar condition as in Scenario II. Another half village based RMP said that they
would monitor the condition of the child themselves and if the child with similar condition does not
improve even after 1-2 days treatment, then they would advise the caregivers to take such a child to
a government hospital.
Sickness Scenario III
Caregivers of Key Informant were narrated Sickness Scenario III also and were asked about the type
of facility/practitioner they would choose to avail treatment for a sick child in this scenario. In U.P.
Illness Vignette on Sickness Scenario III (Video Clip)
Child less than 5 years having fast breathing, difficult breathing, chest in- drawing as well as grunting/ groaning and altered sensorium.
Sickness Scenario III (Narrated)
Child less than 5 yrs. is having cough, runny nose fever, difficulty in breathing and chest in- drawing. He/she is unable to drink/ breastfeed normally. He/ she is also unconscious and is having bluish
^^bl rjg ds cPps dks rqjar lkeqnkf;d LokLF; dsUnz esa pkbYM Lis'kfyLV ds ikl Hkstuk pkfg,A This child should be immediately sent to child specialist at CHC''
[CHW-Gorakhpur] ^^bl rjg ds cPps dks pkbYM Lis'kfyLV ds ikl fjQj dj nsaaxsaA ge muds vfHkHkkodksa ls vPNs MkDVj ds ikl tkus dks dgrs gSa& pkgsa og izkbZosV gks ;k ljdkjhA Refer this child to a child specialist. I ask them to consult a good doctor either private or government''
[CHW- Meerut]
Emerging Theme: Sickness scenario II
Care Givers: Caregivers prefer use of home remedy while they wait and watch at home. If there is no improvement in the condition of the child then they first go to village based doctor and then to block based private doctor.
Care Providers: Rural medical practitioner would treat the sick child themselves in scenario II while Community health workers would advise the caregiver to avail treatment at government hospital for a sick child.
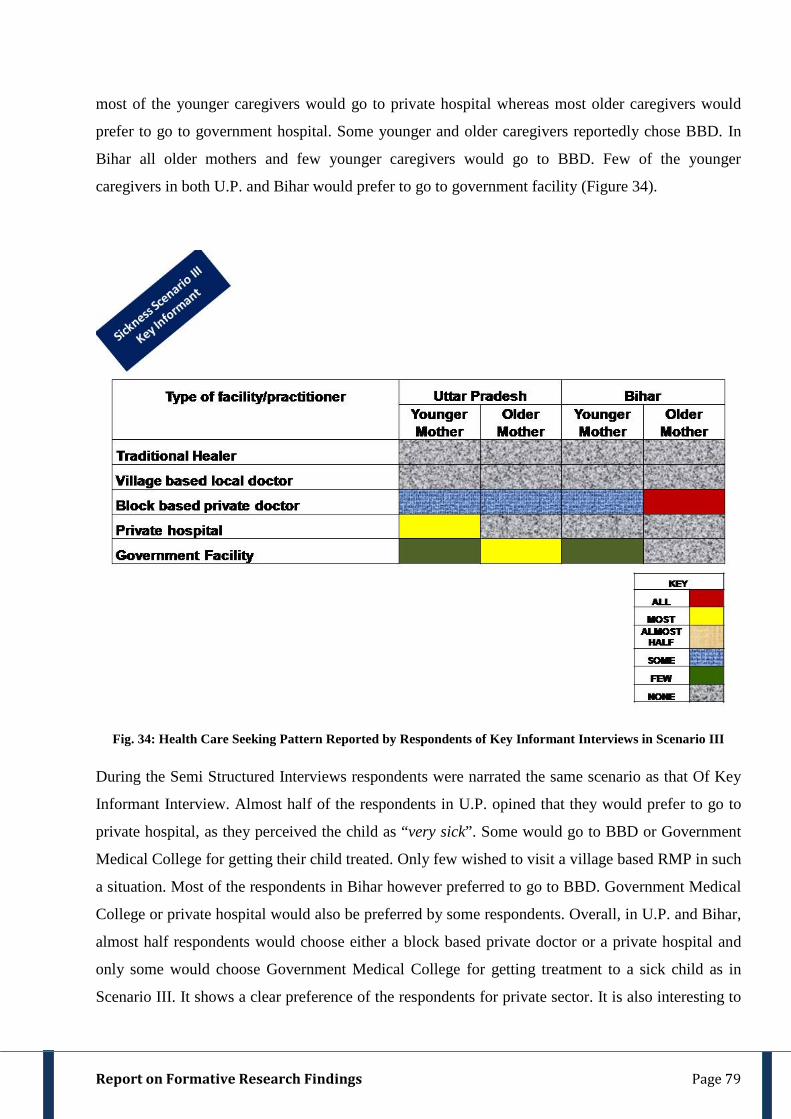
Report on Formative Research Findings Page 79
most of the younger caregivers would go to private hospital whereas most older caregivers would
prefer to go to government hospital. Some younger and older caregivers reportedly chose BBD. In
Bihar all older mothers and few younger caregivers would go to BBD. Few of the younger
caregivers in both U.P. and Bihar would prefer to go to government facility (Figure 34).
Fig. 34: Health Care Seeking Pattern Reported by Respondents of Key Informant Interviews in Scenario III
During the Semi Structured Interviews respondents were narrated the same scenario as that Of Key
Informant Interview. Almost half of the respondents in U.P. opined that they would prefer to go to
private hospital, as they perceived the child as “very sick”. Some would go to BBD or Government
Medical College for getting their child treated. Only few wished to visit a village based RMP in such
a situation. Most of the respondents in Bihar however preferred to go to BBD. Government Medical
College or private hospital would also be preferred by some respondents. Overall, in U.P. and Bihar,
almost half respondents would choose either a block based private doctor or a private hospital and
only some would choose Government Medical College for getting treatment to a sick child as in
Scenario III. It shows a clear preference of the respondents for private sector. It is also interesting to
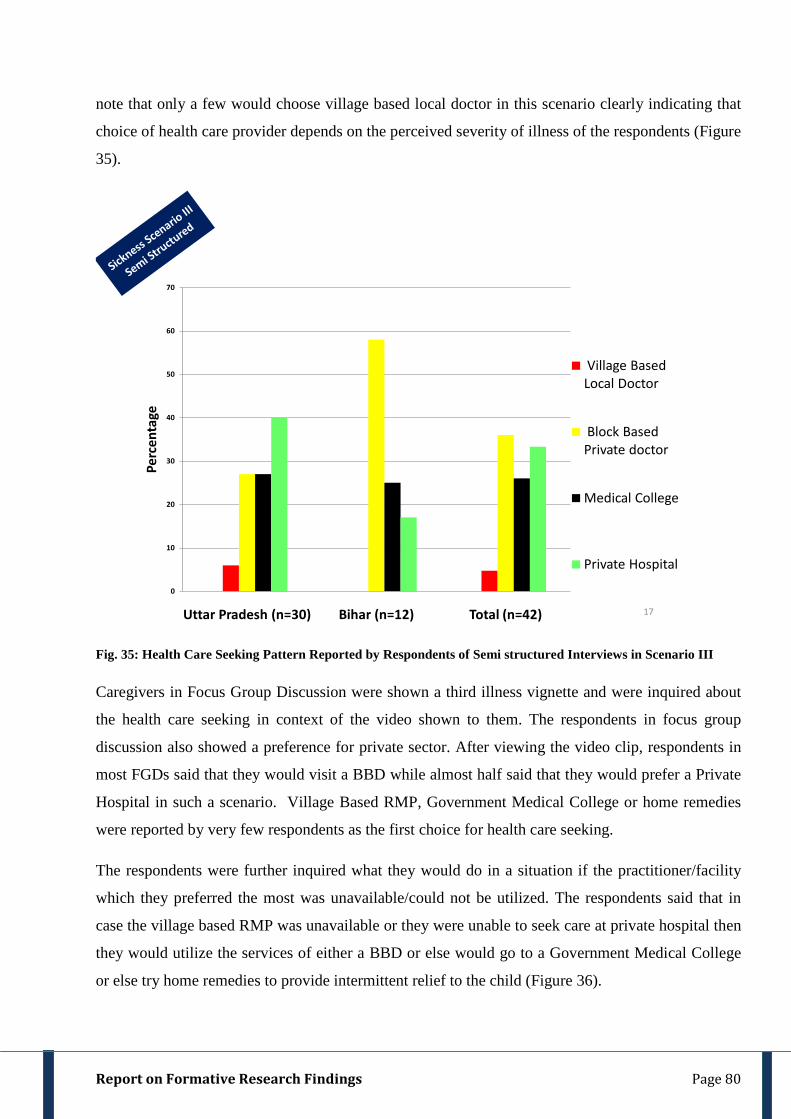
Report on Formative Research Findings Page 80
note that only a few would choose village based local doctor in this scenario clearly indicating that
choice of health care provider depends on the perceived severity of illness of the respondents (Figure
35).
17
0
10
20
30
40
50
60
70
Uttar Pradesh (n=30) Bihar (n=12) Total (n=42)
Perc
enta
ge
Village Based Local Doctor
Block Based Private doctor
Medical College
Private Hospital
Fig. 35: Health Care Seeking Pattern Reported by Respondents of Semi structured Interviews in Scenario III
Caregivers in Focus Group Discussion were shown a third illness vignette and were inquired about
the health care seeking in context of the video shown to them. The respondents in focus group
discussion also showed a preference for private sector. After viewing the video clip, respondents in
most FGDs said that they would visit a BBD while almost half said that they would prefer a Private
Hospital in such a scenario. Village Based RMP, Government Medical College or home remedies
were reported by very few respondents as the first choice for health care seeking.
The respondents were further inquired what they would do in a situation if the practitioner/facility
which they preferred the most was unavailable/could not be utilized. The respondents said that in
case the village based RMP was unavailable or they were unable to seek care at private hospital then
they would utilize the services of either a BBD or else would go to a Government Medical College
or else try home remedies to provide intermittent relief to the child (Figure 36).
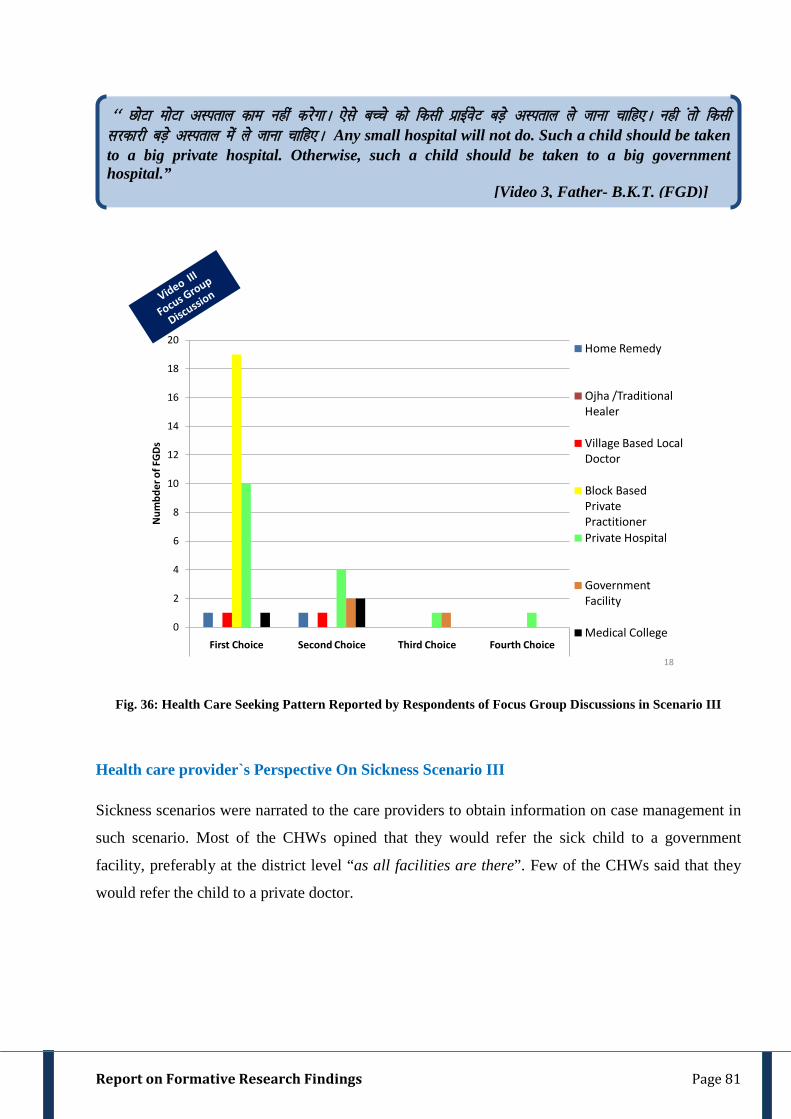
Report on Formative Research Findings Page 81
0
2
4
6
8
10
12
14
16
18
20
First Choice Second Choice Third Choice Fourth Choice
Num
bder
of F
GDs
Home Remedy
Ojha /Traditional Healer
Village Based Local Doctor
Block Based Private PractitionerPrivate Hospital
Government Facility
Medical College
18
Fig. 36: Health Care Seeking Pattern Reported by Respondents of Focus Group Discussions in Scenario III
Health care provider`s Perspective On Sickness Scenario III
Sickness scenarios were narrated to the care providers to obtain information on case management in
such scenario. Most of the CHWs opined that they would refer the sick child to a government
facility, preferably at the district level “as all facilities are there”. Few of the CHWs said that they
would refer the child to a private doctor.
^^ NksVk eksVk vLirky dke ugha djsxkA ,sls cPps dks fdlh izkbZosV cM+s vLirky ys tkuk pkfg,A ugh arks fdlh ljdkjh cM+s vLirky esa ys tkuk pkfg,A Any small hospital will not do. Such a child should be taken to a big private hospital. Otherwise, such a child should be taken to a big government hospital.” [Video 3, Father- B.K.T. (FGD)]
Report on Formative Research Findings Page 82
As with the CHW`s, some village based RMP would refer the sick child to district level
government health facility. Some village based RMP said they would advice treatment of such a
child at the hospital level –this hospital may be a government hospital or a private hospital. They
believed that the child requires treatment at the hospital level, as he was perceived “serious”.
^^,sls cPps dk dksbZ bykt ugha djsxsaA muls ¼vfHkHkkod ls½ dgssaxsa fd bl cPps dks rqjar ftyk vLirky ys tkvks vkSj Bhd ls bykt djokvksA Will not give any treatment to this child. Take this child to a district hospital as soon as possible and treat there properly''. [RMP – Mahoba (Key Informant)]
^^,sls cPps dks rqjar fjQj dj nsaxsaA mls ftyk vLirky ds cPpksa okys okMZ ys tk,aA Will refer the child immediately. Take him/her to children’s ward at district hospital'' [RMP - KI -Darbhanga.] ;g cPpk cgqr xEHkhj gS] ,sls cPps dks ,d vPNs izkbZosV MkDVj ds ikl fjQj dj nsaxsa D;ksafd ogka ij lHkh lqfo/kk,a gksrh gSaA This child is very serious. Will refer him/her to a good doctor in private as there are all the facilities available. Here, there is no facility available. Here, time goes waste".
[RMP –Agra (Key Informant)
Emerging Theme: Sickness scenario III
Caregivers: In the context of scenario III caregivers first prefer to go to block based private doctor then to private hospital and in the end when there is no relief then they go to government hospital.
Care Providers:
Community Health Workers: Community health workers would send the sick child having symptoms mentioned in the above scenario directly to government health facility.
Village Based Local Doctor: Village based local doctor would advise the parents of sick child having symptoms mentioned in the above scenario to go to child specialist and government health facility.
Report on Formative Research Findings Page 83
Health Care Seeking Behaviour from Case Studies (Information obtained from another
Objective of this project)
We recruited 30 cases between September 2013 - January 2014 of which 25 were from Uttar
Pradesh and 5 were from Bihar. Children between 1 month to 5 years of age were recruited from the
following government hospitals:
(a) King George's Medical University in Lucknow, Uttar Pradesh
(b) Darbhanga Medical College and Hospital in Darbhanga, Bihar
(c) Anugrah Narayan Magadh Medical College & Hospital (ANMMCH) in Gaya, Bihar
(d) Lala Lajpat Rai Meerut Medical College in Meerut, Uttar Pradesh.
In addition to hospitals, we also recruited a case from Mahoba District Hospital and another from the
field.
Anugrah Narayan Magadh Medical College & Hospital (ANMMCH) in Gaya, Bihar
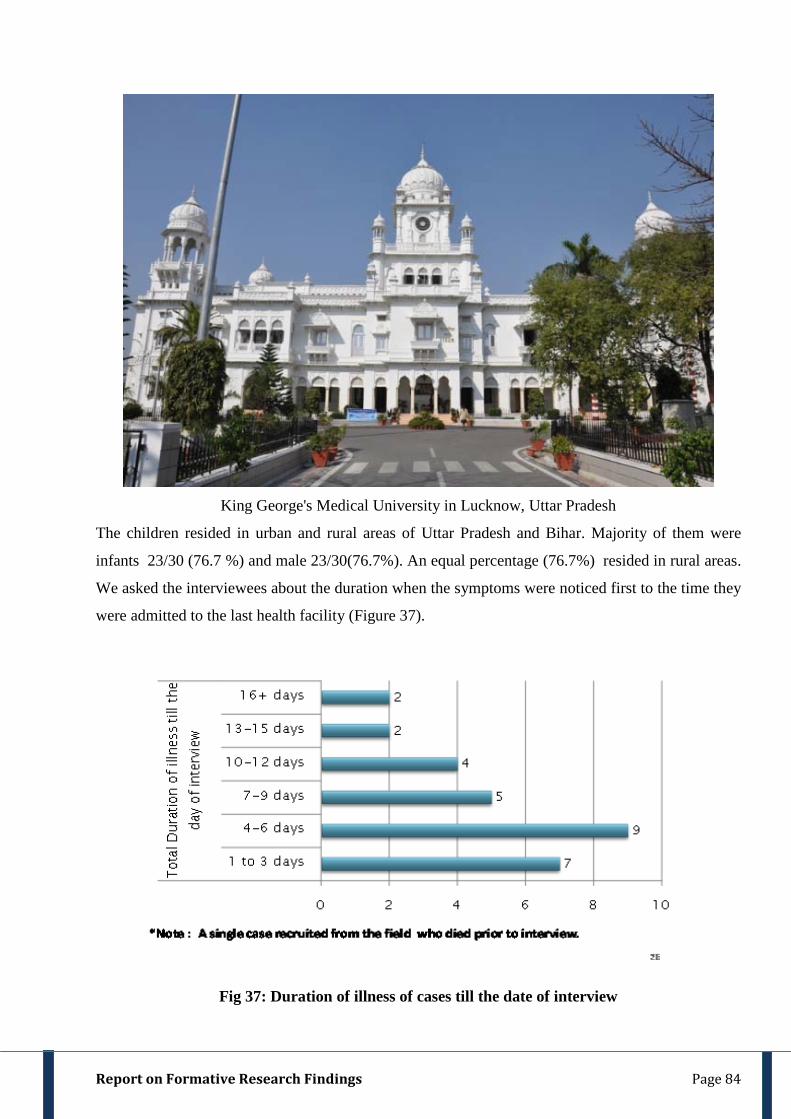
Report on Formative Research Findings Page 84
King George's Medical University in Lucknow, Uttar Pradesh
The children resided in urban and rural areas of Uttar Pradesh and Bihar. Majority of them were
infants 23/30 (76.7 %) and male 23/30(76.7%). An equal percentage (76.7%) resided in rural areas.
We asked the interviewees about the duration when the symptoms were noticed first to the time they
were admitted to the last health facility (Figure 37).
Fig 37: Duration of illness of cases till the date of interview

Report on Formative Research Findings Page 85
We interviewed the parents or the close relative of the child to understand the entire episode of
illness. With the exception of a single case where the respondent was grandfather and in another
case where the interviewee was a grandmother in all other cases interviewees was either the mother
or the father. All the interviewees had been with child since the onset of illness. 53.3% interviewees
lived to a joint family and 46.7% lived in a single family.
Fig. 38: Choice of Health Care Providers Based on 30 Cases from Uttar Pradesh and Bihar
Caregivers were asked about the pathways which they adopted when they sought health care for
their sick child. Almost half the respondents visited Village Based RMP soon after the onset of
illness while some caregivers visited BBD. Even a few had visited a traditional healer immediately
after the onset of illness. Unqualified health care seeking may have caused delay. Only few
caregivers had visited the Government Medical Hospital or a government facility and those that had
visited had been shifted to another practitioner/facility due to different reasons. The caregivers had
visited the private hospital or the government facility only when they were advised/self-decided to
move to a second facility as their child was not showing improvement.
Emerging Theme Case studies
Village based local doctor and Traditional healer was preferred over Private block based doctor as the first choice for health care seeking. Unqualified health care seeking was found to be the cause of delay in almost all of the cases. Before coming to the Medical College/Hospital caregivers visited at least 2 health practitioners / facilities.
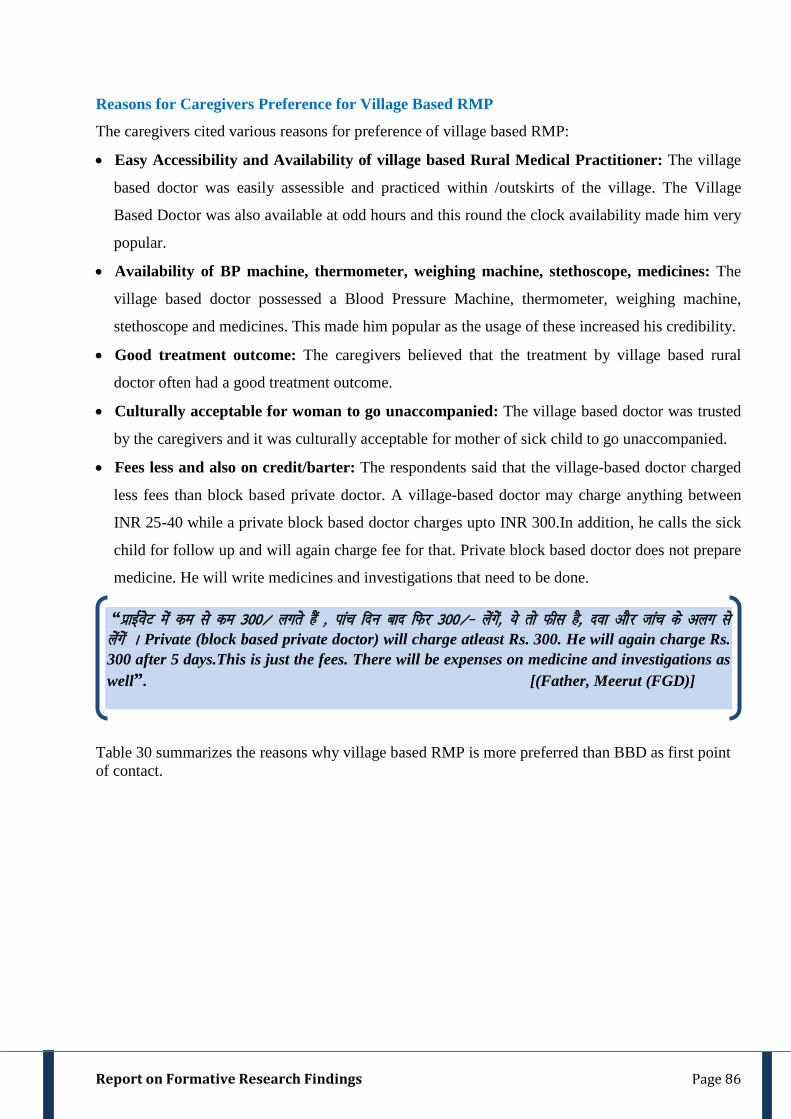
Report on Formative Research Findings Page 86
Reasons for Caregivers Preference for Village Based RMP
The caregivers cited various reasons for preference of village based RMP:
• Easy Accessibility and Availability of village based Rural Medical Practitioner: The village
based doctor was easily assessible and practiced within /outskirts of the village. The Village
Based Doctor was also available at odd hours and this round the clock availability made him very
popular.
• Availability of BP machine, thermometer, weighing machine, stethoscope, medicines: The
village based doctor possessed a Blood Pressure Machine, thermometer, weighing machine,
stethoscope and medicines. This made him popular as the usage of these increased his credibility.
• Good treatment outcome: The caregivers believed that the treatment by village based rural
doctor often had a good treatment outcome.
• Culturally acceptable for woman to go unaccompanied: The village based doctor was trusted
by the caregivers and it was culturally acceptable for mother of sick child to go unaccompanied.
• Fees less and also on credit/barter: The respondents said that the village-based doctor charged
less fees than block based private doctor. A village-based doctor may charge anything between
INR 25-40 while a private block based doctor charges upto INR 300.In addition, he calls the sick
child for follow up and will again charge fee for that. Private block based doctor does not prepare
medicine. He will write medicines and investigations that need to be done.
Table 30 summarizes the reasons why village based RMP is more preferred than BBD as first point of contact.
“izkbZZosV esa de ls de 300@ yxrs gSa ] ikap fnu ckn fQj 300@& ysaxsa] ;s rks Qhl gS] nok vkSj tkap ds vyx ls ysaxsa A Private (block based private doctor) will charge atleast Rs. 300. He will again charge Rs. 300 after 5 days.This is just the fees. There will be expenses on medicine and investigations as well”. [(Father, Meerut (FGD)]
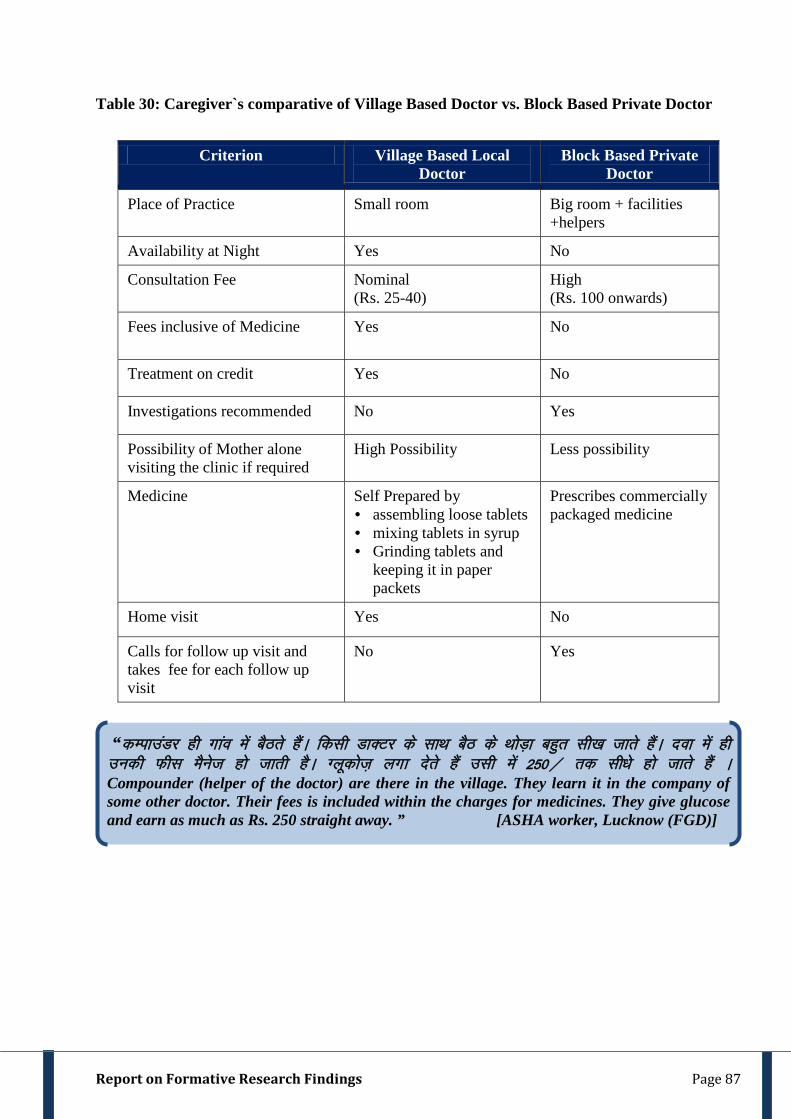
Report on Formative Research Findings Page 87
Table 30: Caregiver`s comparative of Village Based Doctor vs. Block Based Private Doctor
Criterion Village Based Local Doctor
Block Based Private Doctor
Place of Practice Small room Big room + facilities +helpers
Availability at Night Yes No
Consultation Fee Nominal (Rs. 25-40)
High (Rs. 100 onwards)
Fees inclusive of Medicine Yes No
Treatment on credit Yes No
Investigations recommended No Yes
Possibility of Mother alone visiting the clinic if required
High Possibility Less possibility
Medicine
Self Prepared by • assembling loose tablets • mixing tablets in syrup • Grinding tablets and
keeping it in paper packets
Prescribes commercially packaged medicine
Home visit Yes No
Calls for follow up visit and takes fee for each follow up visit
No Yes
“dEikmaMj gh xkao esa cSBrs gSaA fdlh MkDVj ds lkFk cSB ds FkksM+k cgqr lh[k tkrs gSaA nok esa gh mudh Qhl eSust gks tkrh gSA Xywdkst+ yxk nsrs gSa mlh esa 250@ rd lh/ks gks tkrs gSa A Compounder (helper of the doctor) are there in the village. They learn it in the company of some other doctor. Their fees is included within the charges for medicines. They give glucose and earn as much as Rs. 250 straight away. ” [ASHA worker, Lucknow (FGD)]
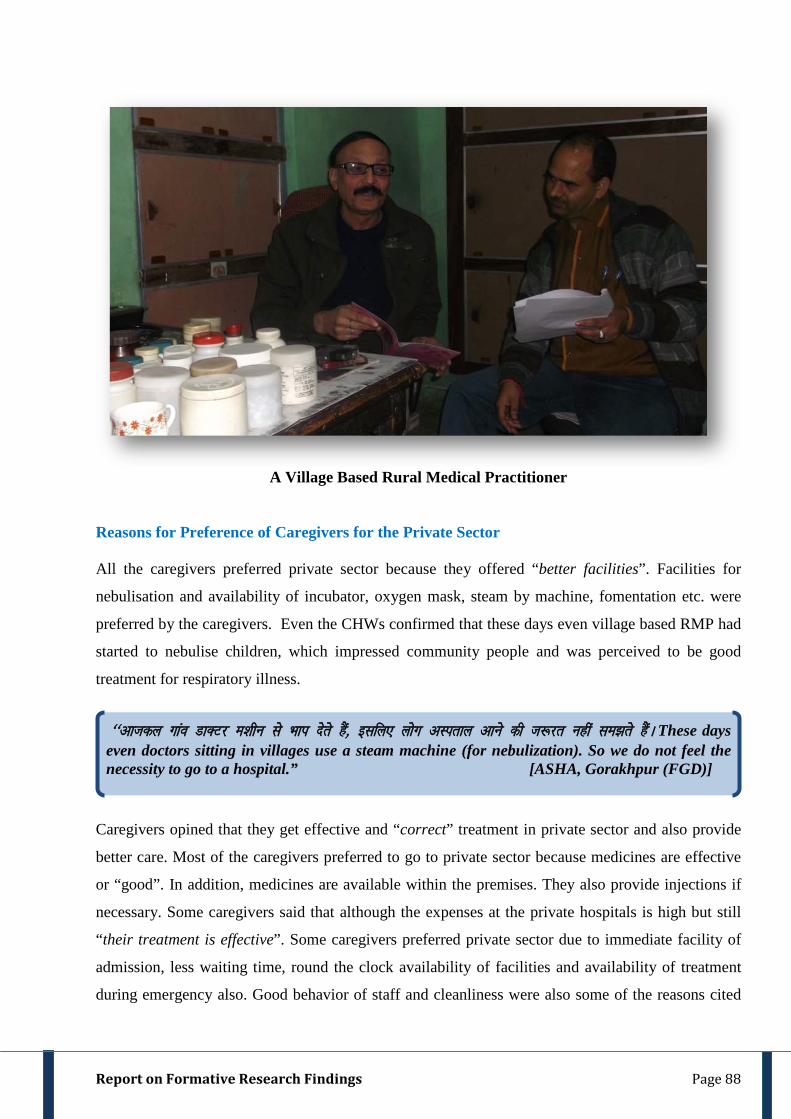
Report on Formative Research Findings Page 88
A Village Based Rural Medical Practitioner
Reasons for Preference of Caregivers for the Private Sector
All the caregivers preferred private sector because they offered “better facilities”. Facilities for
nebulisation and availability of incubator, oxygen mask, steam by machine, fomentation etc. were
preferred by the caregivers. Even the CHWs confirmed that these days even village based RMP had
started to nebulise children, which impressed community people and was perceived to be good
treatment for respiratory illness.
Caregivers opined that they get effective and “correct” treatment in private sector and also provide
better care. Most of the caregivers preferred to go to private sector because medicines are effective
or “good”. In addition, medicines are available within the premises. They also provide injections if
necessary. Some caregivers said that although the expenses at the private hospitals is high but still
“their treatment is effective”. Some caregivers preferred private sector due to immediate facility of
admission, less waiting time, round the clock availability of facilities and availability of treatment
during emergency also. Good behavior of staff and cleanliness were also some of the reasons cited
^^vktdy xkao MkDVj e'khu ls Hkki nsrs gSa] blfy, yksx vLirky vkus dh t:jr ugha le>rs gSaA These days even doctors sitting in villages use a steam machine (for nebulization). So we do not feel the necessity to go to a hospital.” [ASHA, Gorakhpur (FGD)]

Report on Formative Research Findings Page 89
by the caregivers for preference. Some said that they prefer private because it is secure with less
crowding. Less consultation time was also the reason told by few caregivers.
In addition to the above reasons, a certain social status was attached with the private sector.
Caregivers opined that well-to-do families sought private care while lesser offs went to government
hospitals.
Reasons for Non Preference of Caregivers for the Government Sector
Most of the community did not prefer to go to government facility as they lacked trust on its
treatment because of perceived poor outcome. They felt that the government doctors prescribe
medicines which is unavailable in the government facility but has to be purchased from the market.
In addition the government facilities were overcrowded. Some of the community members did not
prefer government facility because they believed that government facilities do not admit patient even
if he/she is critical. Instead they refer the patient to some other place. Their perception was that sick
child will not be benefitted even if they go to government facility and medicine is also not available
there. Thus lack of trust, unavailability or limited availability of medicines/facilities/services and
overcrowding were some of the factors cited by the caregivers for not opting a government facility
as first preference.
^^iSls okys izkbZosV esa tkrs gSa] de iSls okys ljdkjh esa fn[kkrs gSA Only people who are well to do go to private” [ASHA, Gorakhpur (FGD)]
“ljdkjh esa MkWDVj Bhd ls bykt ugha djrs gSaA nokbZ Hkh ugha nsrs gSaA vxj dHkh nsrs Hkh gSa] rks ljdkjh nok;sa gekjs cPpksa dks lwV ugha djrh gSA The government doctor does not treat us well. They do not give medicines. Even if they give us, and that is rare, government medicines do not suit our children”
[Younger Mother, Darbhanga, Bihar (FGD)]

Report on Formative Research Findings Page 90
Community Health Centre at Sahjanwa Block in Gorakhpur District (U.P.)
In Patient ward of the Department of Pediatrics, Mahoba District Hospital
Report on Formative Research Findings Page 91
Caregivers Perception of Quality Of Care
Ways by which a community ascertains the qualification of a doctor Most of the respondents did not ascertain the qualifications of a doctor by viewing the signboard.
Only some said they believed that the doctor was qualified by reading at the signboard of a doctor.
Rest of the respondents described different ways to ensure that the doctor whom they intend to visit
was qualified. Some of these methods were:
1. Ask from other villagers/neighbours/relative to know if the doctor`s treatment is effective and
had a good outcome. If the information obtained was in favour of a particular doctor, he was
believed to be good. Some of them also reported a good outcome within their family after
treatment, which had increased trust.
2. Respondents said that they did not prefer to ask the doctor face-to-face about his qualifications.
They would rather collect information about the doctor from the villagers/neighbours/relative.
3. If the doctor used a stethoscope to examine the child or else if the clinic of the doctor was
always crowded with patients (hence showing popularity) he was believed to be a good doctor.
4. One interesting fact that emerged from the findings was that a doctor was presumed qualified if
he had better 'suvidha' (facilities). A doctor having a better infrastructure and facilities in clinic
like having a glass partition in the clinic, helper etc. was considered better qualified than a non
qualified (`jhola chaap`) doctor.
^^fMxzh okyk MkDVj 'kh'ks ds dejs esa cSBrs gSaA muds ikl gsYij gksrs gSaA >ksyk>ki vdsys cSBrs gSaA A doctor with a degree sits in a room with glass partitions. He has helpers. A jhola chaap sits alone at his room (clinic).” [Older Caregiver, Meerut (Key Informant)]
“>ksyk >ki MkDVj dh NksVh Dyhfud gksrh gS] izf'kf{kr MkDVj dh cM+h Dyhfud gksrh gS vkSj lHkh lqfo/kk,a gksrh gSaA fMxzh okys MkDVj ds ;gka cksMZ yxk gksrk gSA Jholachhap has a small clinic. Qualified has a big clinic, there are all facilities. A degree holder has a signboard” [Older caregiver, Meerut (Semi Structured)]
^^MkDVj vPNs gSa] i<+s fy[ks gSaA MkDVjh Hkh i<+h gSA vkyk yxkdj ns[krs gSaA ukM+h idM+dj ns[krs gSaA lhad Mkydj ns[krs gSaA He is a good doctor. He has studied medicine. He uses a stethoscope and also counts the pulse. He uses a long rod (thermometer) for examination”.
[Younger caregiver, Lucknow (Key Informant)]
oks ,slk ekurs gSa fd tgka cPps dks ges'kk ns[krs gSa] ogha fn[kkus ij cPpk Bhd gks tk,xk] dga vkSj tkus ij ugha** Community always believes that the doctor whom they have always been visiting routinely will make the child well. They will not go elsewhere.” [CHW, Gorakhpur (FGD)]

Report on Formative Research Findings Page 92
5. The respondents believed that a qualified doctor did not visit the homes of the sick patients. An
unqualified doctor visited their homes and asked their well-being.
Similar to the respondents in Semi structured interviews and focus groups, most of the respondents
from key informant interviews also felt that popularity of the doctor was the most important attribute
that they looked for before seeking health care. More older than younger women in all districts
believed popularity to be an important parameter. The younger caregivers reported that good
outcome and better infrastructure were some important things that they ascertained before selecting
a village-based doctor.
Method of Examination and Consultation The respondents were also asked about the method of consultation, examination and prescription of
medicine of the village based doctor, whom they most frequently visited.
Conversation between the doctor and caregiver prior to examination: The caregivers were asked
if the doctor they visited (i) informed them about illness (what has happened to the child) and (ii)
explained the reason as to why this particular illness has occurred. Most of the caregivers said that
the doctor informed them about the name of illness. Almost half the respondents reported that the
doctor which they frequently visited never told them about the cause of illness. In contrast, another
half said that the doctor told them about the cause of illness. The causes that commonly led to
sickness in the child as told by the doctor to these caregivers were: change in season, lower
immunity of the child, unhygienic living conditions etc.
Similar to the respondents in Semi Structured Interviews and Focus Groups, most of the respondents
from Key Informant Interviews in all districts also reported that the doctor informed them about the
name of illness. Except in Meerut district, less than half respondents in remaining 6 districts reported
that the doctor informed them about the cause of illness.
Examination:
^^izf'kf{kr MkDVj csgrj iksft'ku esa gksrk gS] >ksykNki MkDVj >ksyk Mkydj iwjs xkao esa ?kwerk gSA vPNk MkDVj ,d txg gh dqlhZ ij cSBrk gSA A qualified doctor has a better position. A non-qualified doctor roams around with a bag on his shoulders. A qualified one sits on chairs.”
[Older caregiver, Charkhari, Bihar (Key Informant)]
^^ >ksykNki MkDVj gekjs ?kj Hkh vk tkrk gS] i<+k fy[kk MkDVj dHkh ugha vk,xkA i<+kfy[kk MkDVj >ksyk ugha Mkyrk gSA The Jhola Chaap visited our houses himself where as an educated will never come. A person who is educated do not hang bag.” [Older caregiver, Mahoba (FGD)]
Report on Formative Research Findings Page 93
Unbundling the child for examination: Most of the respondents reported that the doctor whom
they very often visited removed the clothes
Use of stethoscope: All the respondents used a stethoscope for examining the child.
Use of thermometer: Most of the respondents said that their doctor used a thermometer to measure
temperature. Few of them said that their doctor counted pulse rate instead of thermometer. Almost
an equal number said that the doctor used both the thermometer and counted pulse rate.
Similar to the respondents in Semi Structured Interviews and Focus Groups, most of the respondents
from Key Informant Interviews reported that the doctor uncovered the child just to put a stethoscope.
All the respondents reported that the doctor, which they visited, used a stethoscope and a
thermometer. None of the respondents self reported that the doctor asked them if the child was
feeding or not. In all districts, younger caregivers reported about the use of thermometer as well as
counting pulse.
Availability of facilities and medical equipments with doctor: The respondents were asked about
the facilities or medical equipments available with the village based doctor that they most frequently
visited. Among the medical equipments commonly reported by most of the respondents were
thermometer and stethoscope. In addition to these items, few respondents also mentioned availability
of blood pressure monitors, X-ray machines, stretcher, `bhaap dene wala yantra` ( instrument used
to give steam / nebulizer machine) , fomentation machine, weighing machine etc.
Frequency and method of administration of medicine: The respondents were asked as to whether
the doctor explained them about the dose and method of administration of the medicine to the sick
child. Most of the respondents said that the doctor informed them as to how frequently the medicine
has to be given to the sick child. They further informed that the doctor told them whether the
medicine has to be given in morning, evening, or every X hours. For this, few respondents reported
that the doctors whom they consulted wrote on the medicine sachets and educated members.
The respondents were also asked if the doctor explained them as to how a medicine has to be given
to the child. Most of the respondents could not self-report about the method of administration of the
medicine. Only some (26%) respondents were able to explain the method of administration. They
informed that the doctor sometimes told them orally or otherwise wrote the instructions for giving
^^iqfM+;k ij uEcj Mky nsrs gSa&1]2] 3A rhu VkbZe f[kykuk gSa] lqcg] nksigj] 'kke A tks i<+k gS og rks i<+ ds tku ysrk gSA lhji ij Hkh uEcj Mky nsrs gSaA He (doctor) writes numbers like 1, 2, 3 on the sachet. It should be given three times-morning, afternoon, evening. Those who are educated know it by reading. Numbers are given on syrup bottle also". [ Younger Mother, Mahoba ( FGD) ]
Report on Formative Research Findings Page 94
medicines on a slip or a paper sachet in which he dispensed loose medicines. Some common
methods of administration self-reported by the respondents were:
Giving medicine along with luke warm water
Mixing dry powdered medicine in hot water and then giving it to child
Pill to be given with milk or water
Time spent on Consultation: The village based doctors spent 1-2 minutes with the patient and
another 2-3 minute for medicine.
All the respondents in key informant interviews said that the doctor told them about dose and
method of administration. Few respondents also self reported that doctor told them as to what diet
should be given to the child and also informed that the doctor prepared medicines himself.
Monitoring the condition of sick child: The respondents were asked if the doctor explained them
how to monitor the condition of the child at home. Most of the respondents reported that the doctor
did not inform them as to how to monitor the condition of the sick child at home. The respondents
said that the doctor examined the child himself in the follow up visit and then informed the parents
that the child`s condition is improving, deteriorating or stable. They were not able to clearly tell on
their own on what symptoms he looked for to ascertain if the child was improving. On probing, they
informed that progression of fever or cough were the signs they looked for to ascertain if the child
was improving.
They never educated the parents to monitor the condition of the child. Only few (14 %) respondents
reported that the doctor informed them
1) To monitor if the child starts playing
as to how to ascertain if the child is improving at the time of
first visit. The doctor usually told them one of the following
2) To monitor if the breathing in the sick child becomes normal
3) To monitor if difficult breathing reduces.
One caregiver narrated how their doctor tells them to monitor in the following verbatim
“;fn eka cki i<+s fy[ks gSa rks crkrs gSa fd FkekZehVj yxkdj cq[kkj ns[k ysukA ;fn lq/kkj ugha gqvk rks fQj vkukA If the parents are educated the doctor tells them to use a thermometer and keep on checking the progress of fever. If there is no improvement, then come again.”
[Older caregiver, Meerut, KI]
Report on Formative Research Findings Page 95
Most of the respondents reported that the doctor himself told them about the condition of the child
when they visited his clinic for follow up. None of them mentioned that the doctor taught them as to
how to monitor a sick child at home.
Follow up: The respondents were asked if the doctor which they consulted called them for follow up
at his clinic and after how long. In addition, the respondents were asked if the doctor ever visited
their homes for follow up. All respondents reported that the doctor called them for follow up at the
clinic. Some (23%) of the respondents reported that the doctor advised them for follow up in 1-2
days. Almost a similar number of respondents reported that the doctor called them for follow up
within 3-4 days. Rest visited them visited doctor after more than 4 days None of the respondents
reported that the doctor visited their home for follow up. Also it was not clear from the verbatim of
the respondents if they complied with the advice of the doctor for follow up or not.
All the respondents reported that they were called for follow up but did not clear if they complied
with follow up advice given by the doctor.
Report on Formative Research Findings Page 96
The Community Health Workers (CHWs) namely the ANM and the ASHA participated in this
study. Key Informant Interviews and Focus Group Discussions were conducted with the Community
Health Workers to obtain information on their recognition of symptoms of pneumonia and how they
manage cases of pneumonia at the community level. Information was also obtained from them on
their perception of risk vulnerability. In addition, we collected information from the CHWs on the
health care seeking behavior of the community in which they lived.
Identification and Selection of Community Health Workers
For the identification and selection of Community Health Worker, the project team visited the office
of the Chief Medical Officer (C.M.O.) at the Community Health Centre (CHC) in Uttar Pradesh or
Medical Officer In Charge (MO i/c) at the Primary Health Centre (PHC) in Bihar and sensitized him
about the project. After seeking his cooperation, the team obtained a list of all functional subcentres
within selected block from the Health Education Officer (H.E.O) in Uttar Pradesh /Health Manager
(in Bihar). The list of subcentre also included names of ANM`s posted in a particular sub centre and
AHSA` posted at the villages in the ambit of a particular subcentre. Health Education Officer
(H.E.O)/Health Manager also helped the team to establish liaison with the CHWs and informed the
day where the CHW could be met at the CHC/PHC during routine meeting / reporting. The team
decided to conduct interview/discussion on that particular day at the CHC/PHC.
Key Informant Interview: One CHW who could provide rich information was interviewed at each
project district. The team identified and purposively selected a CHW with the help of Health
Education Officer (H.E.O) /Health Manager who fulfilled the eligibility criteria. Before the initiation
of the interview, the respondent was explained about the purpose of project and the interview.
Thereafter, written informed consent was obtained and baseline characteristics of the respondents
were noted. Each interview was audio recorded. In six of seven project districts, ANMs were key
informants while in Lucknow district ASHA was the key-informant.
Focus Group Discussion: One discussion per district was conducted at the CHC/ PHC of the
selected block. A heterogeneous group of 6-8 ASHA and ANM was formed for each discussion. It
was ensured that the ASHA and ANM belonged to different subcentres. ASHAs who were already
included for Key Informant interviews were not included in FGD. Informed consent was taken from
the CHWs before the start of every discussion. Baseline characteristics of the respondents were
noted. Each discussion was audio recorded.
4.7 Community Health Worker
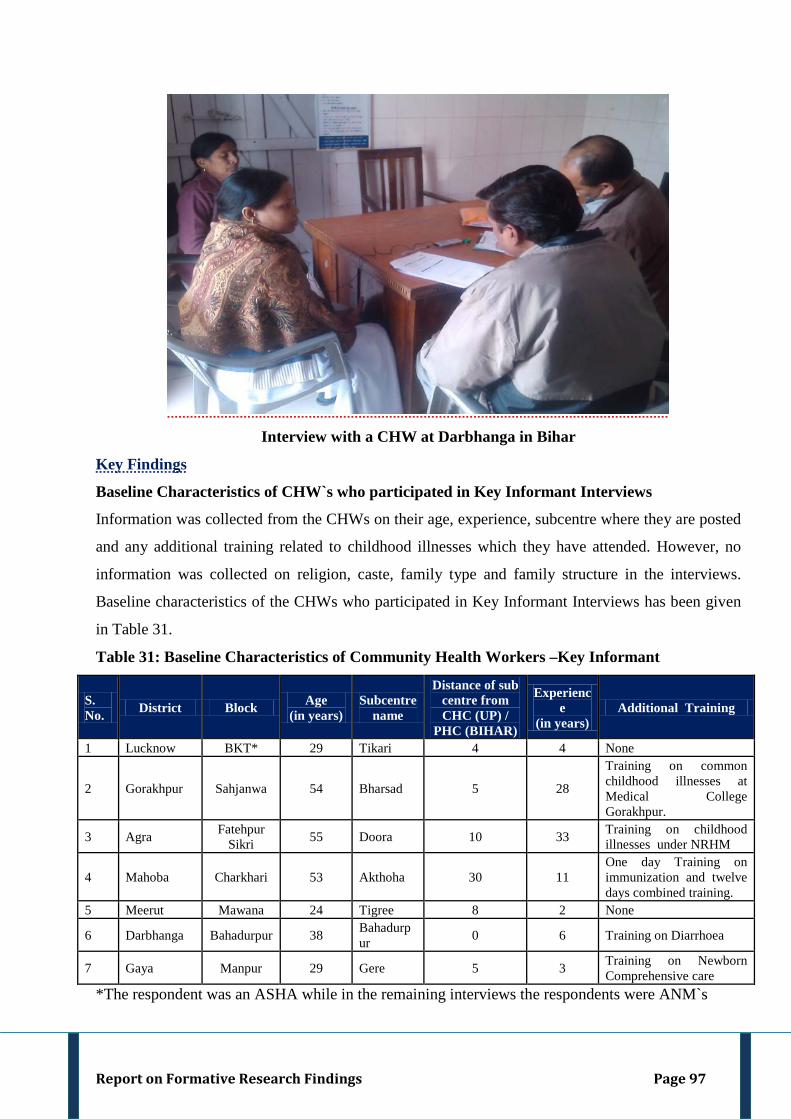
Report on Formative Research Findings Page 97
Interview with a CHW at Darbhanga in Bihar
Key Findings
Baseline Characteristics of CHW`s who participated in Key Informant Interviews
Information was collected from the CHWs on their age, experience, subcentre where they are posted
and any additional training related to childhood illnesses which they have attended. However, no
information was collected on religion, caste, family type and family structure in the interviews.
Baseline characteristics of the CHWs who participated in Key Informant Interviews has been given
in Table 31.
Table 31: Baseline Characteristics of Community Health Workers –Key Informant
S. No. District Block Age
(in years) Subcentre
name
Distance of sub centre from CHC (UP) /
PHC (BIHAR)
Experience
(in years) Additional Training
1 Lucknow BKT* 29 Tikari 4 4 None
2 Gorakhpur Sahjanwa 54 Bharsad 5 28
Training on common childhood illnesses at Medical College Gorakhpur.
3 Agra Fatehpur Sikri 55 Doora 10 33 Training on childhood
illnesses under NRHM
4 Mahoba Charkhari 53 Akthoha 30 11 One day Training on immunization and twelve days combined training.
5 Meerut Mawana 24 Tigree 8 2 None
6 Darbhanga Bahadurpur 38 Bahadurpur 0 6 Training on Diarrhoea
7 Gaya Manpur 29 Gere 5 3 Training on Newborn Comprehensive care
*The respondent was an ASHA while in the remaining interviews the respondents were ANM`s
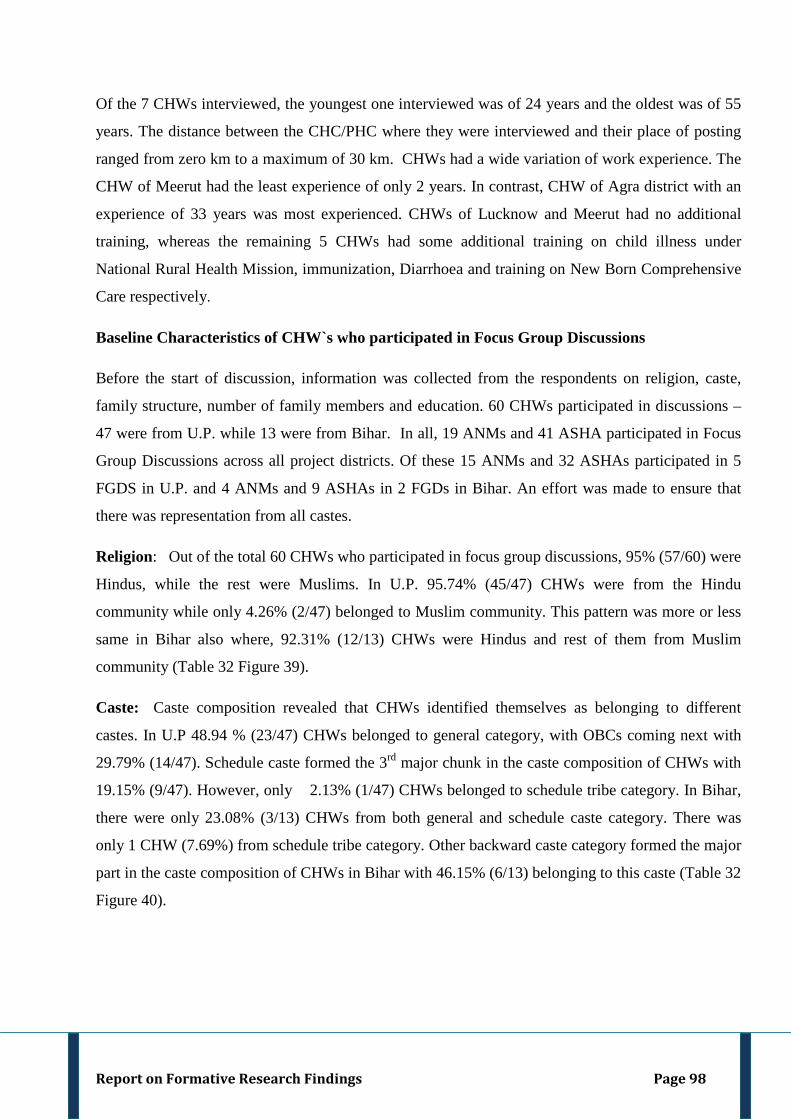
Report on Formative Research Findings Page 98
Of the 7 CHWs interviewed, the youngest one interviewed was of 24 years and the oldest was of 55
years. The distance between the CHC/PHC where they were interviewed and their place of posting
ranged from zero km to a maximum of 30 km. CHWs had a wide variation of work experience. The
CHW of Meerut had the least experience of only 2 years. In contrast, CHW of Agra district with an
experience of 33 years was most experienced. CHWs of Lucknow and Meerut had no additional
training, whereas the remaining 5 CHWs had some additional training on child illness under
National Rural Health Mission, immunization, Diarrhoea and training on New Born Comprehensive
Care respectively.
Baseline Characteristics of CHW`s who participated in Focus Group Discussions
Before the start of discussion, information was collected from the respondents on religion, caste,
family structure, number of family members and education. 60 CHWs participated in discussions –
47 were from U.P. while 13 were from Bihar. In all, 19 ANMs and 41 ASHA participated in Focus
Group Discussions across all project districts. Of these 15 ANMs and 32 ASHAs participated in 5
FGDS in U.P. and 4 ANMs and 9 ASHAs in 2 FGDs in Bihar. An effort was made to ensure that
there was representation from all castes.
Religion: Out of the total 60 CHWs who participated in focus group discussions, 95% (57/60) were
Hindus, while the rest were Muslims. In U.P. 95.74% (45/47) CHWs were from the Hindu
community while only 4.26% (2/47) belonged to Muslim community. This pattern was more or less
same in Bihar also where, 92.31% (12/13) CHWs were Hindus and rest of them from Muslim
community (Table 32 Figure 39).
Caste: Caste composition revealed that CHWs identified themselves as belonging to different
castes. In U.P 48.94 % (23/47) CHWs belonged to general category, with OBCs coming next with
29.79% (14/47). Schedule caste formed the 3rd major chunk in the caste composition of CHWs with
19.15% (9/47). However, only 2.13% (1/47) CHWs belonged to schedule tribe category. In Bihar,
there were only 23.08% (3/13) CHWs from both general and schedule caste category. There was
only 1 CHW (7.69%) from schedule tribe category. Other backward caste category formed the major
part in the caste composition of CHWs in Bihar with 46.15% (6/13) belonging to this caste (Table 32
Figure 40).
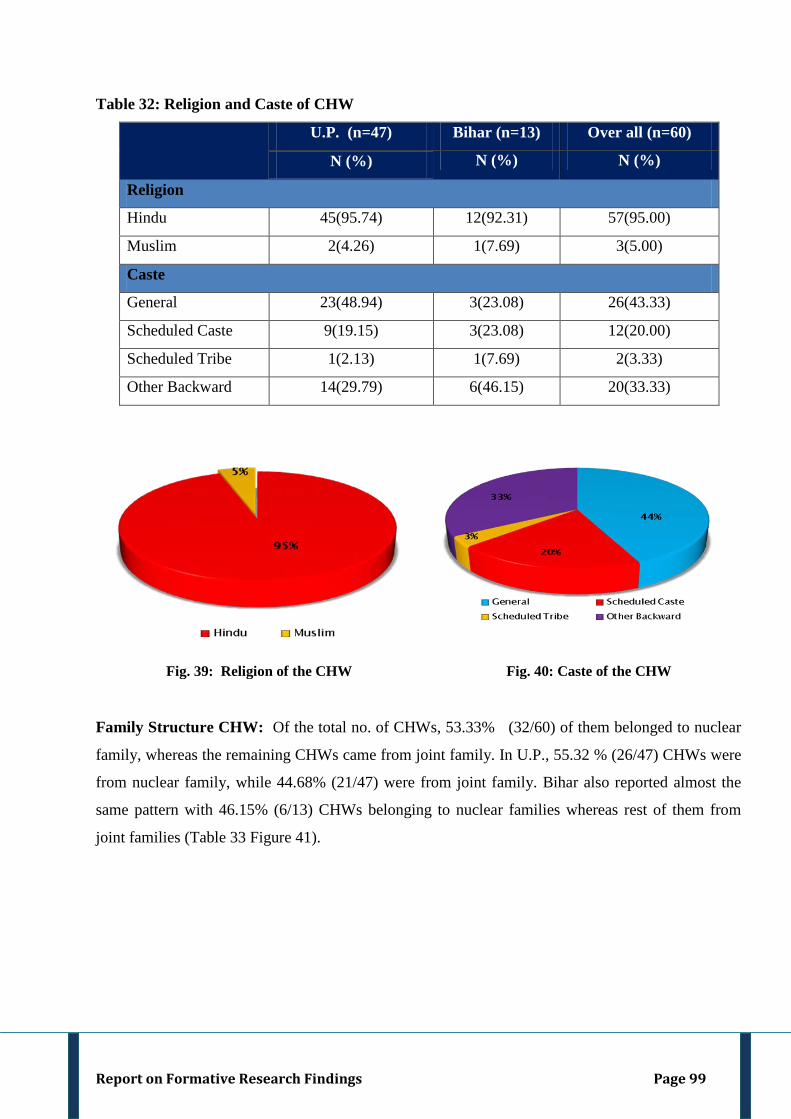
Report on Formative Research Findings Page 99
Table 32: Religion and Caste of CHW
U.P. (n=47) Bihar (n=13) Over all (n=60)
N (%) N (%) N (%)
Religion
Hindu 45(95.74) 12(92.31) 57(95.00)
Muslim 2(4.26) 1(7.69) 3(5.00)
Caste
General 23(48.94) 3(23.08) 26(43.33)
Scheduled Caste 9(19.15) 3(23.08) 12(20.00)
Scheduled Tribe 1(2.13) 1(7.69) 2(3.33)
Other Backward 14(29.79) 6(46.15) 20(33.33)
Fig. 39: Religion of the CHW Fig. 40: Caste of the CHW
Family Structure CHW: Of the total no. of CHWs, 53.33% (32/60) of them belonged to nuclear
family, whereas the remaining CHWs came from joint family. In U.P., 55.32 % (26/47) CHWs were
from nuclear family, while 44.68% (21/47) were from joint family. Bihar also reported almost the
same pattern with 46.15% (6/13) CHWs belonging to nuclear families whereas rest of them from
joint families (Table 33 Figure 41).
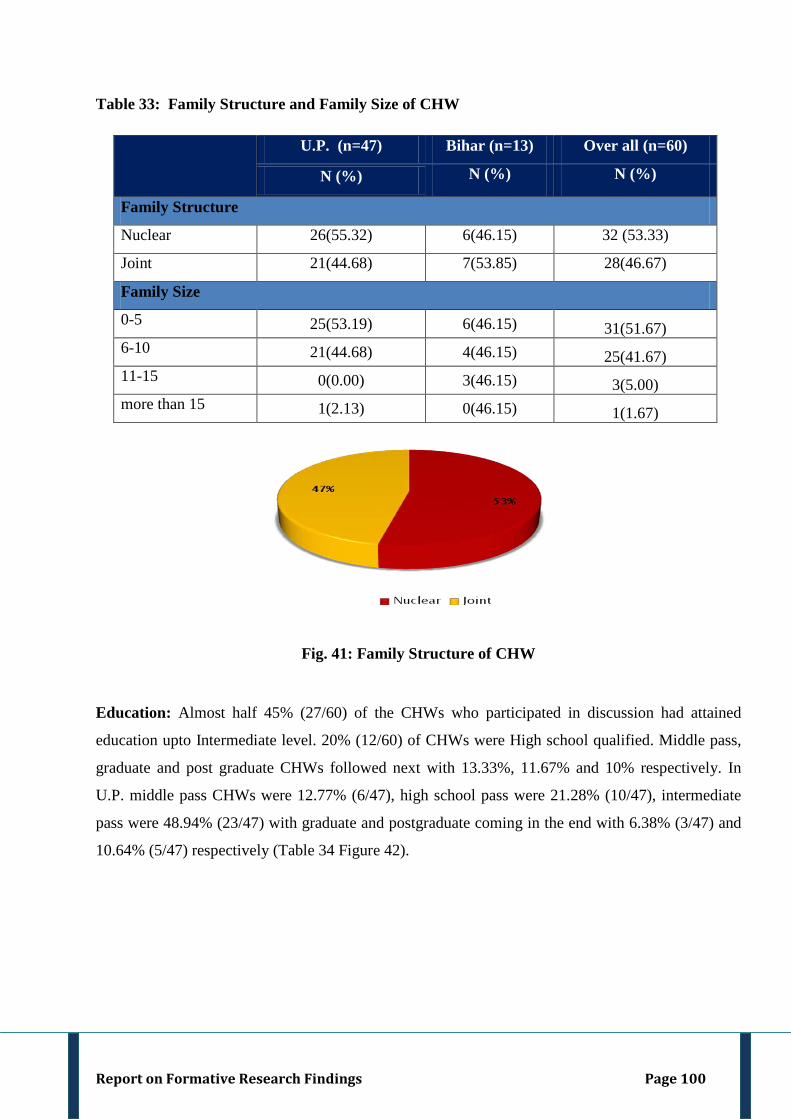
Report on Formative Research Findings Page 100
Table 33: Family Structure and Family Size of CHW
U.P. (n=47) Bihar (n=13) Over all (n=60)
N (%) N (%) N (%)
Family Structure
Nuclear 26(55.32) 6(46.15) 32 (53.33)
Joint 21(44.68) 7(53.85) 28(46.67)
Family Size
0-5 25(53.19) 6(46.15) 31(51.67) 6-10 21(44.68) 4(46.15) 25(41.67) 11-15 0(0.00) 3(46.15) 3(5.00) more than 15 1(2.13) 0(46.15) 1(1.67)
Fig. 41: Family Structure of CHW
Education: Almost half 45% (27/60) of the CHWs who participated in discussion had attained
education upto Intermediate level. 20% (12/60) of CHWs were High school qualified. Middle pass,
graduate and post graduate CHWs followed next with 13.33%, 11.67% and 10% respectively. In
U.P. middle pass CHWs were 12.77% (6/47), high school pass were 21.28% (10/47), intermediate
pass were 48.94% (23/47) with graduate and postgraduate coming in the end with 6.38% (3/47) and
10.64% (5/47) respectively (Table 34 Figure 42).
Report on Formative Research Findings Page 101
Table 34: Educational status of CHW
Education U.P. (n=47) Bihar (n=13) Over all (n=60)
N (%) N (%) N (%) N (%) N (%) N (%)
Middle Pass 6 (12.77) 2(15.38) 8(13.33)
High School Pass 10 (21.28) 2(15.38) 12(20.00)
Intermediate Pass 23(48.94) 4(30.77) 27(45.00)
Graduate 3(6.38) 4(30.77) 7(11.67)
Post Graduate 5(10.64) 1(7.69) 6(10.00)
Fig. 42: Level of Education of the CHW`S
Common childhood illness: The community health workers were asked about the common
illnesses that are likely to occur in children less than 5 years of age in the key informant interview
and focus group discussion. All the CHWs named Pneumonia, Diarrhoea and Fever as common
childhood illness. Most of the CHWs reported cough, cold and congestion as common childhood
illness. Jaundice, Polio, Malaria, Cholera, Measles and Chicken pox, Diphtheria, Tuberculosis,
Night blindness, Typhoid, whooping cough etc. were some other common childhood illnesses
reported by CHW. All the CHWs named Pneumonia, Fever, Diarrhoea, Jaundice as common
childhood illness. Cholera, Measles, Polio, Whooping cough, Tuberculosis, Tetanus, Asthma was
reported by some CHWs in the FGD (Figure 43).
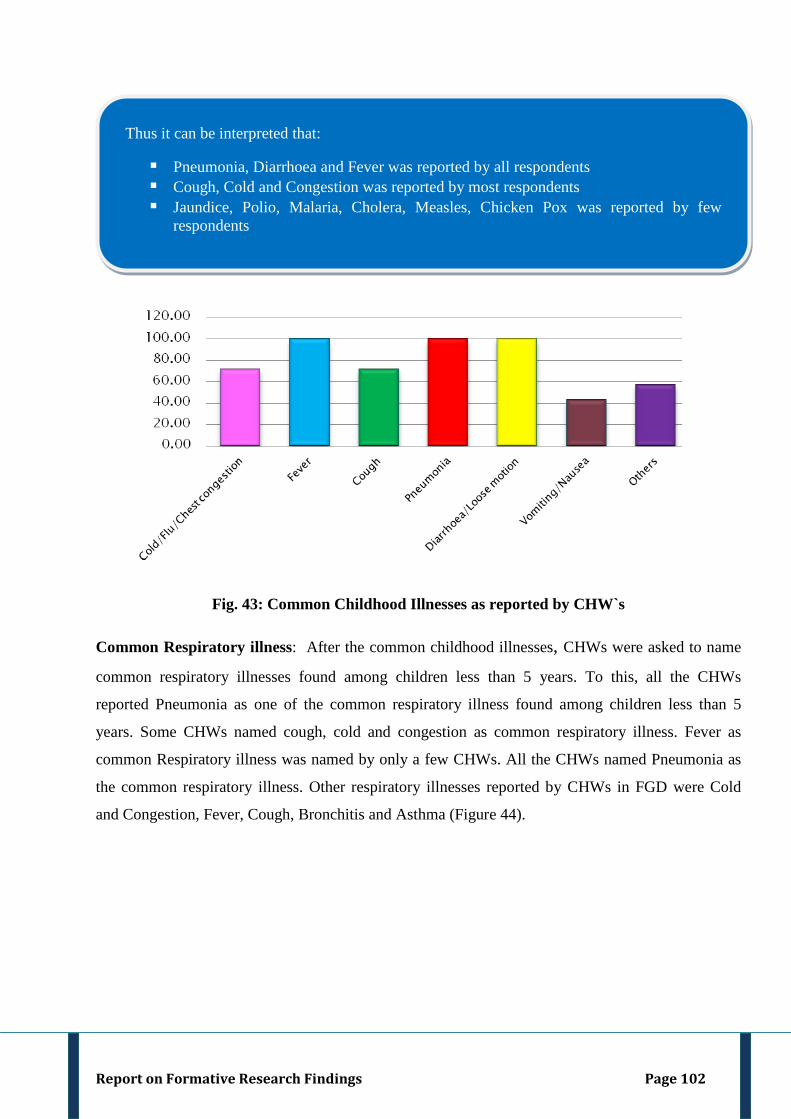
Report on Formative Research Findings Page 102
Fig. 43: Common Childhood Illnesses as reported by CHW`s
Common Respiratory illness: After the common childhood illnesses, CHWs were asked to name
common respiratory illnesses found among children less than 5 years. To this, all the CHWs
reported Pneumonia as one of the common respiratory illness found among children less than 5
years. Some CHWs named cough, cold and congestion as common respiratory illness. Fever as
common Respiratory illness was named by only a few CHWs. All the CHWs named Pneumonia as
the common respiratory illness. Other respiratory illnesses reported by CHWs in FGD were Cold
and Congestion, Fever, Cough, Bronchitis and Asthma (Figure 44).
Thus it can be interpreted that:
Pneumonia, Diarrhoea and Fever was reported by all respondents Cough, Cold and Congestion was reported by most respondents Jaundice, Polio, Malaria, Cholera, Measles, Chicken Pox was reported by few
respondents
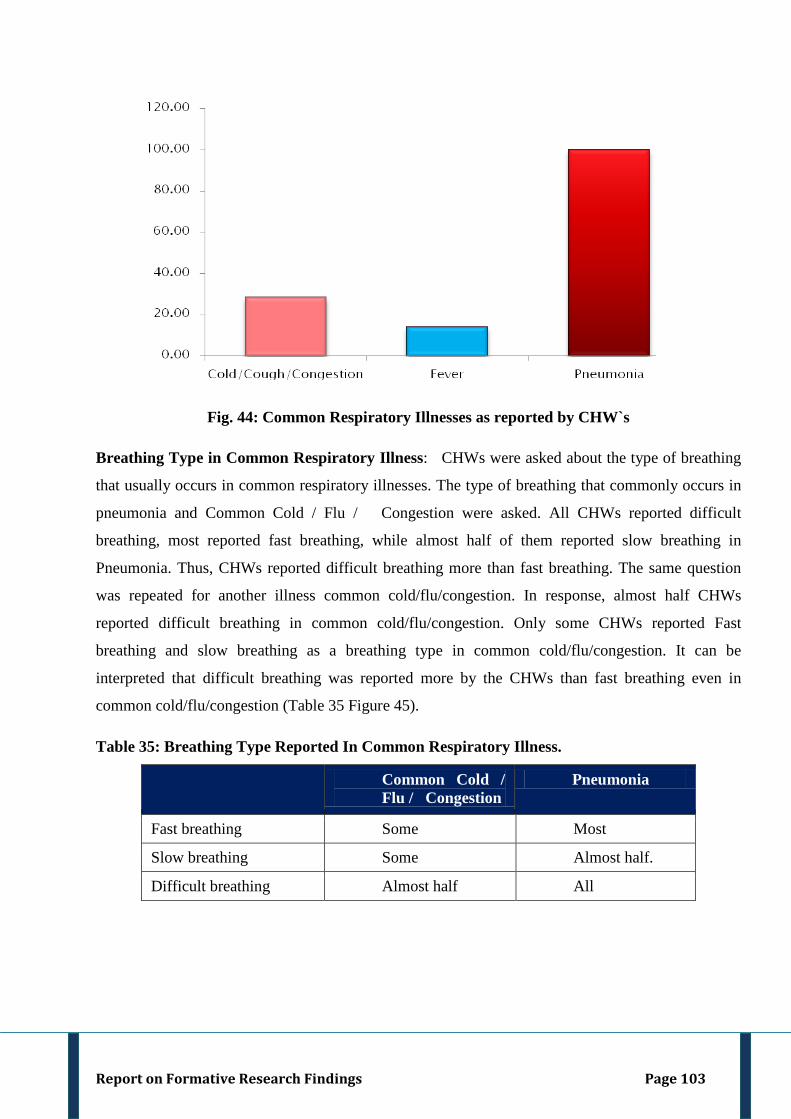
Report on Formative Research Findings Page 103
Fig. 44: Common Respiratory Illnesses as reported by CHW`s
Breathing Type in Common Respiratory Illness: CHWs were asked about the type of breathing
that usually occurs in common respiratory illnesses. The type of breathing that commonly occurs in
pneumonia and Common Cold / Flu / Congestion were asked. All CHWs reported difficult
breathing, most reported fast breathing, while almost half of them reported slow breathing in
Pneumonia. Thus, CHWs reported difficult breathing more than fast breathing. The same question
was repeated for another illness common cold/flu/congestion. In response, almost half CHWs
reported difficult breathing in common cold/flu/congestion. Only some CHWs reported Fast
breathing and slow breathing as a breathing type in common cold/flu/congestion. It can be
interpreted that difficult breathing was reported more by the CHWs than fast breathing even in
common cold/flu/congestion (Table 35 Figure 45).
Table 35: Breathing Type Reported In Common Respiratory Illness.
Common Cold / Flu / Congestion
Pneumonia
Fast breathing Some Most
Slow breathing Some Almost half.
Difficult breathing Almost half All
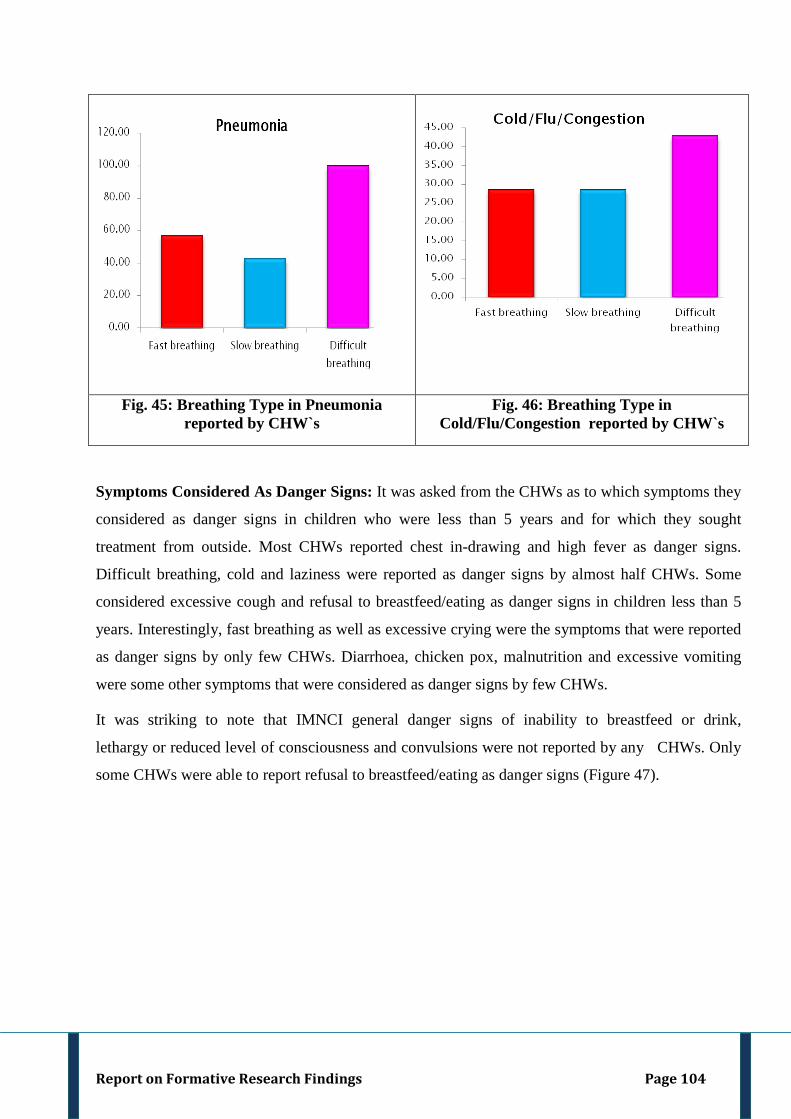
Report on Formative Research Findings Page 104
Fig. 45: Breathing Type in Pneumonia reported by CHW`s
Fig. 46: Breathing Type in Cold/Flu/Congestion reported by CHW`s
Symptoms Considered As Danger Signs: It was asked from the CHWs as to which symptoms they
considered as danger signs in children who were less than 5 years and for which they sought
treatment from outside. Most CHWs reported chest in-drawing and high fever as danger signs.
Difficult breathing, cold and laziness were reported as danger signs by almost half CHWs. Some
considered excessive cough and refusal to breastfeed/eating as danger signs in children less than 5
years. Interestingly, fast breathing as well as excessive crying were the symptoms that were reported
as danger signs by only few CHWs. Diarrhoea, chicken pox, malnutrition and excessive vomiting
were some other symptoms that were considered as danger signs by few CHWs.
It was striking to note that IMNCI general danger signs of inability to breastfeed or drink,
lethargy or reduced level of consciousness and convulsions were not reported by any CHWs. Only
some CHWs were able to report refusal to breastfeed/eating as danger signs (Figure 47).
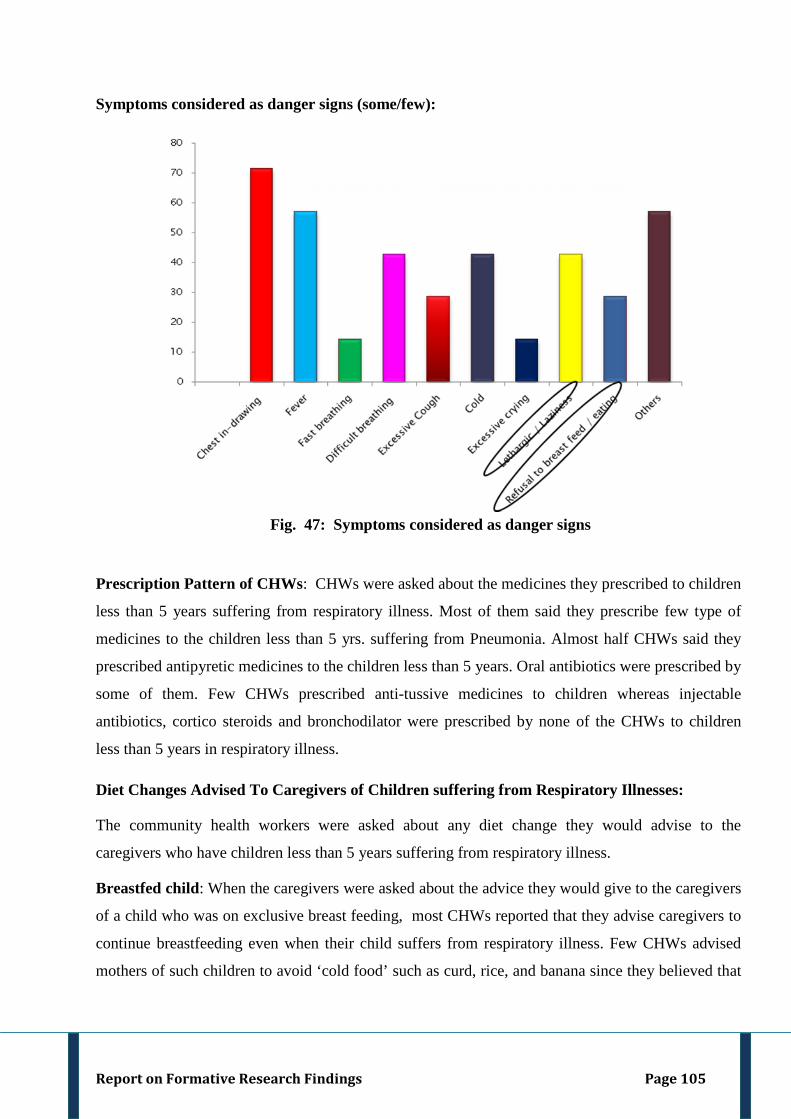
Report on Formative Research Findings Page 105
Symptoms considered as danger signs (some/few):
Fig. 47: Symptoms considered as danger signs
Prescription Pattern of CHWs: CHWs were asked about the medicines they prescribed to children
less than 5 years suffering from respiratory illness. Most of them said they prescribe few type of
medicines to the children less than 5 yrs. suffering from Pneumonia. Almost half CHWs said they
prescribed antipyretic medicines to the children less than 5 years. Oral antibiotics were prescribed by
some of them. Few CHWs prescribed anti-tussive medicines to children whereas injectable
antibiotics, cortico steroids and bronchodilator were prescribed by none of the CHWs to children
less than 5 years in respiratory illness.
Diet Changes Advised To Caregivers of Children suffering from Respiratory Illnesses:
The community health workers were asked about any diet change they would advise to the
caregivers who have children less than 5 years suffering from respiratory illness.
Breastfed child: When the caregivers were asked about the advice they would give to the caregivers
of a child who was on exclusive breast feeding, most CHWs reported that they advise caregivers to
continue breastfeeding even when their child suffers from respiratory illness. Few CHWs advised
mothers of such children to avoid ‘cold food’ such as curd, rice, and banana since they believed that
Report on Formative Research Findings Page 106
if the mother continues to have `cold food` the cold may pass on to the mother and further on to the
breastfed child. Only few CHWs promoted use of warm water/fluids.
Older child: All CHWs advised the caregivers of older children to avoid ‘cold food’ like banana,
curd, rice, oranges etc. when their child suffers from respiratory illness. Most CHWs promote ‘hot
food’ items like almond, groundnut, eggs, masoor lentil, jaggery etc. They also advised use of warm
water/fluids to a child suffering from respiratory illnesses.
General advice to Caregivers of Children suffering from Respiratory Illnesses: It was asked
from the community health workers whether they give any advice to caregivers when their children
less than 5 years suffer from respiratory illness. All CHW's said they inform caregivers on what they
should do and what they should not do to help early recovery of their sick child. They advise that
child should be protected from catching cold, not to bath the child with cold water, make the child
wear warm / extra clothes and not to let them play outside the house when it is too cold.
^^cksyrs gS cPps dks BaM ls cpk;saA xeZ j[ksA [kkus&ihus esa BaMh thts ugha nsus dks dgsxsa] tSls twl] Qy] pkoy uk nsA xje pht esa lwi] nky dk ikuh] nfy;k] ek<+ ¼pkoy dk ikuh½ nsaaA ikuh xje djds fiyk;saA Advise them to keep the children away from cold. Keep them warm. Avoid giving ‘cold food’ like juice, fruits, rice. Give ‘hot food’ like soup, porridge, water strained from pulses and rice. Warm/boiled water should be given" [CHW-Gaya(Key Informant)] ^^cPpks dks BaMh pht euk djrs gSaA ngh] eB~Bk] ve:n vkfnA Advise the children to avoid eating curd, buttermilk, guava etc". [CHW-Agra(Key Informant)] ^^BaMk lkeku ugha nsuk] xje lkeku nsuk gSaA pkoy ugha nsuk] Qy&Qwy ugha nsuk] twl ugha nsuk] xje pht jksVh] nky] lCth nsaA ikuh xje djds nsaA Avoid giving ‘cold’ food; promote hot food .Rice, fruits, juice should not be given. Hot food stuff like chapatti, pulses, and vegetables should be given. Water should be given boiled". [CHW- Darbhanga (Key Informant)]
^^vxj cPps dks [kk¡lh vk jgh gS rks cPps dks pkoy ugha nsxsa] ngh ugha nsxsaA Lruiku djkrs jgrs gSA xje ikuh mcky dj nsrs gSaA If the child is having cough, avoid giving rice and curd as sputum is formed. Continue breastfeeding; give boiled water to the child as suggested by doctor".
[CHW-Gorakhpur (Key Informant)] ^^BaM ds ekSle esa BaMh pht u f[kyk;sa] tSls j[kk [kkuk u nsa] dqN lfCt;k¡] f?k;k] rksjh u nsa] pkoy] dsyk] phdw] iihrk] larjk ugha nsrs gSaA xquxquk ikuh gh nsaA ek¡ dk nw/k ,sls gh fiykrs gSaA Avoid giving ‘cold’ food during winters like rice, banana, papaya,`cheeku’, orange; some vegetables like bottle gourd, torai and stale food. Give fresh food, almond, groundnut. Give lukewarm water. Continue breastfeeding." [CHW-Meerut (Key Informant)]
Report on Formative Research Findings Page 107
Method of Examination of a child with respiratory illness: It was discussed with the respondents
as to how they examined the child with respiratory illness. Most CHWs said they touched the pulse
to know the temperature. Surprisingly only a few of them used a thermometer.
Information about dose of medicine and method of administration: Information was gathered
from the CHW about the dose of medicine and method of administering these medicines which they
advice to caregivers of children less than 5 years suffering from respiratory illness. Most CHWs said
that they informed caregivers about the dose of medicine and how the medicine has to be
administered to a child with respiratory illness. Almost half CHWs give antipyretics like
paracetamol while some of them give oral antibiotics like cotrimoxazole.
^^gekjs ikl tk¡p djus dk lk/ku ugha gSaA gkFk ls Nw¡ dj gh tk¡p dj ysrs gSaA We don’t have tools of examination. We only touch to know the temperature of the child.” CHW-Mahoba (Key Informant) ^^cq[kkj Nwdj ns[krs gSaA uk[kwu esa ihykiu ns[krs gSaA thHk dk rkyw ns[ksaA vk¡[k dk ihykiu ns[ksaA Mk;fj;k esa pqVdh djds ns[krs gSaA We touch to know the temperature of the child. Observe yellowishness in the eyes, nails and palate of tongue of the child. Pinch the child in case of diarrhea". [CHW-Darbhanga(Key Informant)]
^^ cPpks dks BaM ls cpk dj j[ksa] xje diM+s iguk;saA BaMh pht [kkus dks uk nsA Protect the child from cold; make him/her wear warm clothes. Avoid giving ‘cold food’" [CHW-Lucknow (Key Informant)]
^^foDl dh ekfy'k djus dh lykg nsrs gSaA BaM ls cpk dj j[kksa] dSi oxSjk iguk dj j[kksaA I advise them to massage the child with Vicks. Protect them from cold, make them wear woolen cap etc."
[CHW-Meerut (Key Informant)] ^^cPps dks ges'kk BaM ls cpk;sa] ckgj [ksyus uk ns] xje diM+s iguk;sa] BaMh pht [kkus dks u nsA ikuh mcky dj ds nsaA cPps dk iSj <dk gksuk pkfg;sA Always protect the child from cold, do not let them play outside. Make them wear warm clothing, avoid giving’ cold ‘food, water should be given boiled, legs and head of the child should be covered properly".
[CHW- Gaya (Key Informant)]
Report on Formative Research Findings Page 108
Signs of Improvement told by CHWs to Caregivers: CHWs were asked about the signs of
improvement that they explain to the caregivers to help them ascertain if their child’s condition is
improving or stable. All the CHWs informed that they explain the parents to assess themselves if
their child’s condition is improving or not. They told the parents that if the child’s condition
improves, then the child will become playful, his/her temperature will come down, he/she will
breathe normally and ribs will not retract. They also told the parents that the child will feed normally
and will stop crying.
^^cPps esa vxj lq/kkj gks jgk gSa] rks cq[kkj de gks tk;sxkA ilfy;k¡ ugha /klsaxh] lkal ukeZy ysxkA If the child’s condition is improving then his/her temperature will come down, ribs will stop retracting and child will breathe normally." [CHW-Meerut(Key Informant)]
^^vxj cPpk lkal Bhd ls ys jgk gSa] nw/k ih jgk gSa] cq[kkj de gks rks lq/kkj gks jgk gSaA If the child is breathing normally, is feeding and temperature is also down, then it means there is some improvement in the condition of pneumonia.” [CHW-Darbhanga (Key Informant)]
^^ukeZyh 2 fnu dh nok nsrs gSaA 2 lky rd ds cPps ds fy, VSCysV ds pkj VqdM+s djds 2 lky ds ls Åij dk gS] rks vk/kh xksyh lqcg nksigj 'kke dks nsrs gSaA Normally give medicines for 2 days. For children up to 2 yrs.1/4 of tablet and for children above 2 yrs. ½ tablet thrice a day."
[ CHW-Meerut (Key Informant)] ^^rhu fnu rd nok nsrs gSA T;knk ugha nsrs gSaA nks lky ls Åij okyksa dks vk/kh&vk/kh xksyh lqcg&'kke nsrs gSaA nks lky ls de mez okyks dks ge nok ugha nsrsA I prescribe medicines only for three days, not more than that. 1/2 tablet twice a day for children above 2 years. I do not give medicines to children less than 2 years". [CHW- Agra(Key Informant)] ^^cq[kk+j jgus ij ,d lky ls de mez ds cPps dks 2-5 ,e-,y rFkk ,d o"kZ ls Åij okys cPps dks 5 ,e-,y- ,d ls nks fnu rd nsus ds fy, dgrs gSaA ,d ls nks fnu ls T;knk ughaA In case of fever we give 2.5 ml. syrup for a child less than 1 year. For child above 1 year we advice 5 ml. syrup for 1-2 days. We do not ask to give medicine themselves for more than 2 days" [CHW-Gaya(Key Informant)]
Emerging Theme: Community Health Worker
The Community Health Worker is not able to recognize fast breathing as an early sign of pneumonia. They were also not able to report IMNCI danger signs. The CHW have
limited information on how to manage pneumonia cases at the community level.
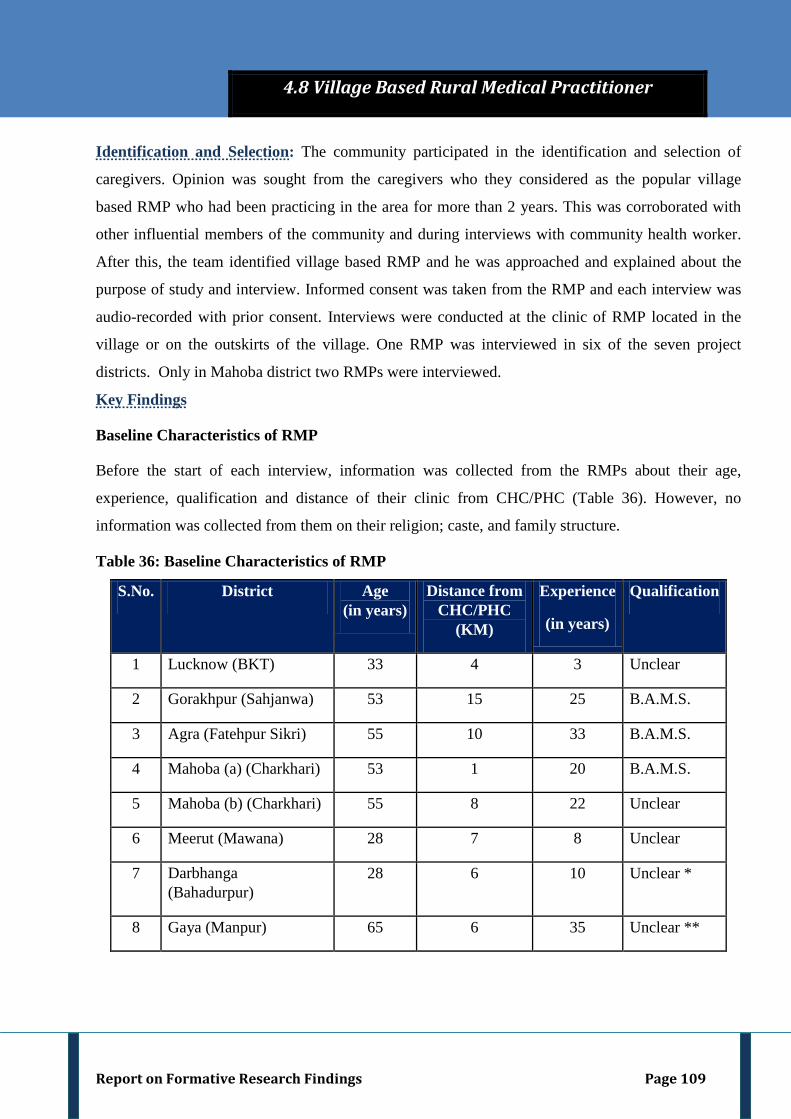
Report on Formative Research Findings Page 109
Identification and Selection: The community participated in the identification and selection of
caregivers. Opinion was sought from the caregivers who they considered as the popular village
based RMP who had been practicing in the area for more than 2 years. This was corroborated with
other influential members of the community and during interviews with community health worker.
After this, the team identified village based RMP and he was approached and explained about the
purpose of study and interview. Informed consent was taken from the RMP and each interview was
audio-recorded with prior consent. Interviews were conducted at the clinic of RMP located in the
village or on the outskirts of the village. One RMP was interviewed in six of the seven project
districts. Only in Mahoba district two RMPs were interviewed.
Key Findings
Baseline Characteristics of RMP
Before the start of each interview, information was collected from the RMPs about their age,
experience, qualification and distance of their clinic from CHC/PHC (Table 36). However, no
information was collected from them on their religion; caste, and family structure.
Table 36: Baseline Characteristics of RMP
S.No. District Age (in years)
Distance from CHC/PHC
(KM)
Experience
(in years)
Qualification
1 Lucknow (BKT) 33 4 3 Unclear
2 Gorakhpur (Sahjanwa) 53 15 25 B.A.M.S.
3 Agra (Fatehpur Sikri) 55 10 33 B.A.M.S.
4 Mahoba (a) (Charkhari) 53 1 20 B.A.M.S.
5 Mahoba (b) (Charkhari) 55 8 22 Unclear
6 Meerut (Mawana) 28 7 8 Unclear
7 Darbhanga (Bahadurpur)
28 6 10 Unclear *
8 Gaya (Manpur) 65 6 35 Unclear **
4.8 Village Based Rural Medical Practitioner
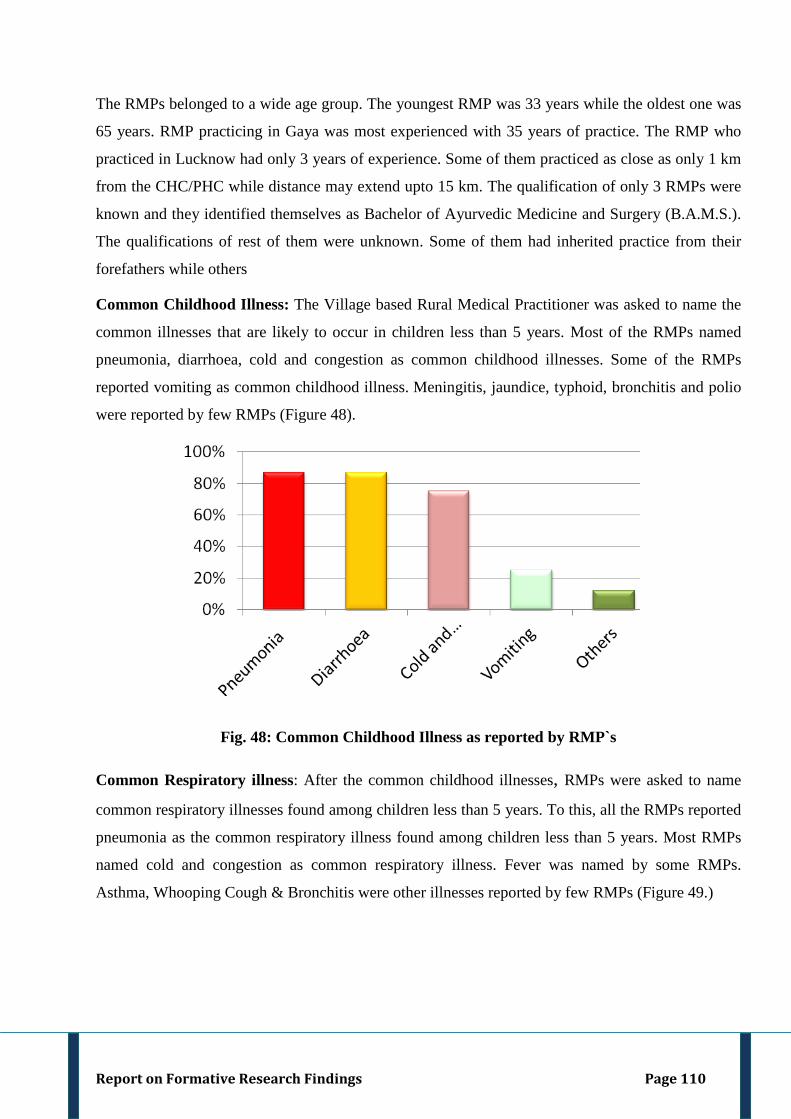
Report on Formative Research Findings Page 110
The RMPs belonged to a wide age group. The youngest RMP was 33 years while the oldest one was
65 years. RMP practicing in Gaya was most experienced with 35 years of practice. The RMP who
practiced in Lucknow had only 3 years of experience. Some of them practiced as close as only 1 km
from the CHC/PHC while distance may extend upto 15 km. The qualification of only 3 RMPs were
known and they identified themselves as Bachelor of Ayurvedic Medicine and Surgery (B.A.M.S.).
The qualifications of rest of them were unknown. Some of them had inherited practice from their
forefathers while others
Common Childhood Illness: The Village based Rural Medical Practitioner was asked to name the
common illnesses that are likely to occur in children less than 5 years. Most of the RMPs named
pneumonia, diarrhoea, cold and congestion as common childhood illnesses. Some of the RMPs
reported vomiting as common childhood illness. Meningitis, jaundice, typhoid, bronchitis and polio
were reported by few RMPs (Figure 48).
Fig. 48: Common Childhood Illness as reported by RMP`s
Common Respiratory illness: After the common childhood illnesses, RMPs were asked to name
common respiratory illnesses found among children less than 5 years. To this, all the RMPs reported
pneumonia as the common respiratory illness found among children less than 5 years. Most RMPs
named cold and congestion as common respiratory illness. Fever was named by some RMPs.
Asthma, Whooping Cough & Bronchitis were other illnesses reported by few RMPs (Figure 49.)
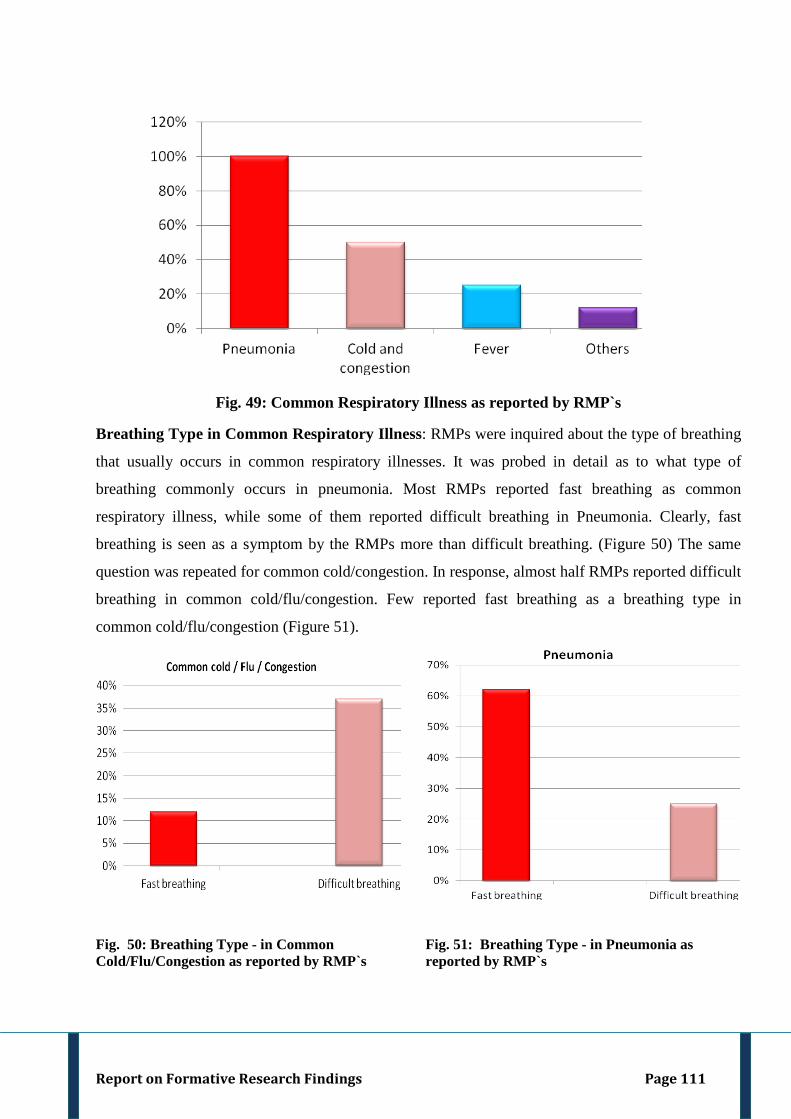
Report on Formative Research Findings Page 111
Fig. 49: Common Respiratory Illness as reported by RMP`s
Breathing Type in Common Respiratory Illness: RMPs were inquired about the type of breathing
that usually occurs in common respiratory illnesses. It was probed in detail as to what type of
breathing commonly occurs in pneumonia. Most RMPs reported fast breathing as common
respiratory illness, while some of them reported difficult breathing in Pneumonia. Clearly, fast
breathing is seen as a symptom by the RMPs more than difficult breathing. (Figure 50) The same
question was repeated for common cold/congestion. In response, almost half RMPs reported difficult
breathing in common cold/flu/congestion. Few reported fast breathing as a breathing type in
common cold/flu/congestion (Figure 51).
Fig. 50: Breathing Type - in Common Cold/Flu/Congestion as reported by RMP`s
Fig. 51: Breathing Type - in Pneumonia as reported by RMP`s
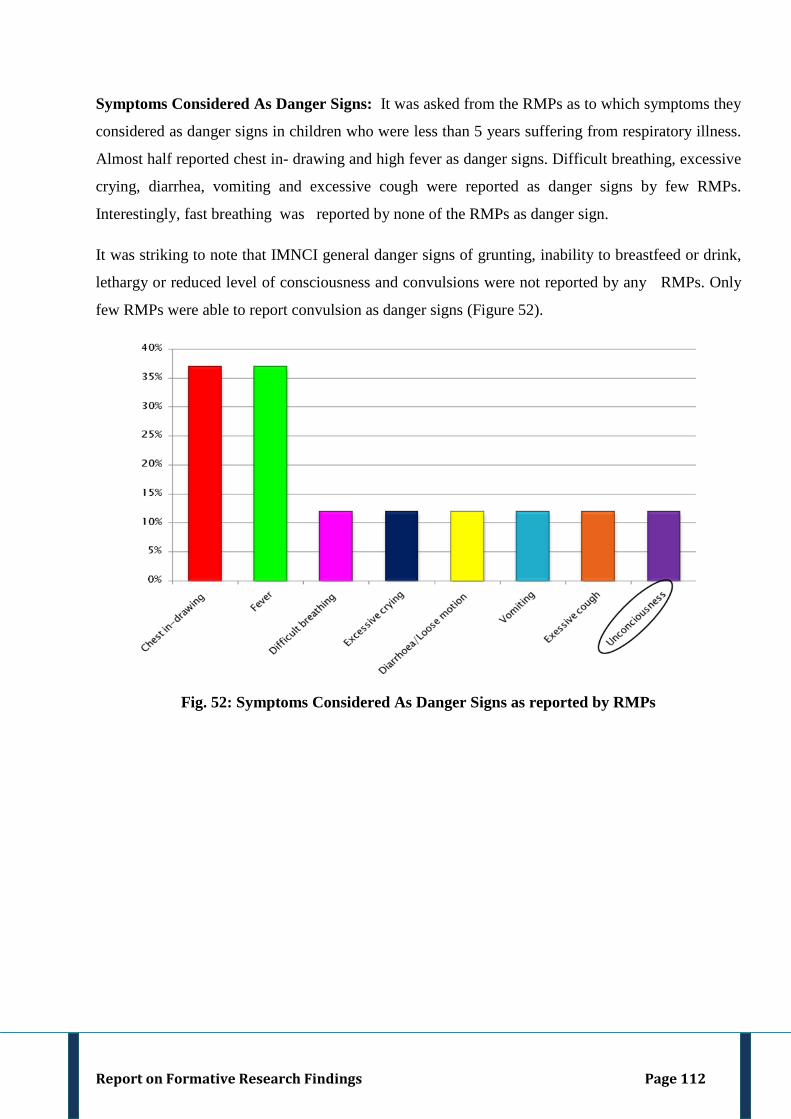
Report on Formative Research Findings Page 112
Symptoms Considered As Danger Signs: It was asked from the RMPs as to which symptoms they
considered as danger signs in children who were less than 5 years suffering from respiratory illness.
Almost half reported chest in- drawing and high fever as danger signs. Difficult breathing, excessive
crying, diarrhea, vomiting and excessive cough were reported as danger signs by few RMPs.
Interestingly, fast breathing was reported by none of the RMPs as danger sign.
It was striking to note that IMNCI general danger signs of grunting, inability to breastfeed or drink,
lethargy or reduced level of consciousness and convulsions were not reported by any RMPs. Only
few RMPs were able to report convulsion as danger signs (Figure 52).
Fig. 52: Symptoms Considered As Danger Signs as reported by RMPs
Report on Formative Research Findings Page 113
Prescription Pattern of RMP
Table 37: Prescription pattern of RMP Prescription Pattern RMP
(Self Reported) (N=8)
Oral antibiotics* Almost half
Injectible antibiotics Some**
Antipyretics Some
Anti tussives Some
Cortico steroids Some
Broncho-dilator Some
Indigenous No information
Mixed (anti-diarrheals, antispasmodics, topical) Few
* Syrup and tablets both ** However, most said injections are important
RMPs were asked about the type of medicines they prescribed to children less than 5 years suffering
from respiratory illness. Almost half of them said they prescribed oral antibiotic medicines like
Amoxicillin, Sporidex, and Sefodoxim syrup. Some of them said they prescribed Injectible
antibiotics like Monoceff, Taxim and Salbectum, antipyretic medicines like Cenarest, Paracetamol
and Aceclopara, anti tussives like Trimonic and Tixylyx syrup, Cortico steroids like Dexona
injections and Broncho dilator like Deriphylin injection/tablet to the children less than 5 years. Few
of them said they prescribed anti-diarrheal like Lomophen, antispasmodics like Baralgon and topical
medicines also (Table 37).
Importance of Injections: RMPs were asked about the importance of injections to which most of
them said injections are important. They recounted that injections helps to manage “situation” and
keep “situation under control” when the child is very critical. They also opined that injection
provides “fast relief” from illness. Many RMPs also reported that injections are demanded from the
caregivers to provide easy relief.
^^batsD’ku nsuk t:jh gS] batsD’ku 'kjhj esa rqjUr dke djrk gSA 5 feuV ;k 20&30 feuV esa daVªksy dj ysrk gSA Giving injections is important; its starts working immediately in the body. It controls the disease in 5 minutes or 20-30 minutes." [RMP-Darbhanga (Key Informant)] ^^eS batsD’ku de yxkrk gw¡] ij cgqr ls ek¡&cki gh batsD’ku yxkus dks dgrs gSaA I give injections rarely. Many parents insist on giving injections to their child."
[RMP-Lucknow (Key Informant)]
Report on Formative Research Findings Page 114
General Advise to Caregivers at the Clinic: RMPs were inquired about the advice they give to
caregivers at the clinic. All the RMPs said they advise the caregivers to protect the child from
catching cold, not to bath the child with cold water and also avoid giving cold food items and make
the child wear extra clothes/covered.
Diet Changes Advised for Children Suffering From Respiratory Illness:
The village based Rural Medical Practitioners were asked if they advised any changes in diet for a
child who suffered from respiratory illnesses. The RMPs recounted that they advised diet changes
during respiratory illnesses.
Breastfed child: When the RMPs were asked about the advice they would give to a child who was
breast feeding they informed that for a child who was breastfeeding the mother has modify her diet.
Most RMPs advised mothers of breastfed child to avoid ‘cold food’ items such as curd, rice, banana,
orange etc. Some RMPs advise caregivers to continue breastfeeding even during respiratory illness.
Further, RMPs advised that intake of warm water/fluids should be increased to provide relief .
Older child: All RMPs advised older children to avoid ‘cold food’ like banana, curd etc. when the
older child suffered from respiratory illness. Most RMPs advocated intake of ‘hot food’ items like
jiggery, groundnuts etc. They also advised increased intake of warm water/fluids in childhood
respiratory illnesses.
^^ ek¡ BaMh phtsa u [kk,] tks cPpk eka dk nw/k ihrk gS] eka dk vlj cPps esa tkrk gS nw/k ds }kjkA Mother’s who breastfeed their child should not eat cold food items. Through milk that cold transfers to the sick child." [RMP—Meerut (Key Informant)]
^^Ekk¡ dks BaMh pht ugha [kkuh pkfg, & ngh] eV~Bk] lVj iVj pht ugha [kkuh pkfg,A Mother should not eat cold food items-like curd buttermilk and all such things."
[RMP-Gaya (Key Informant)]
^^ek¡ dk nw/k cPps dks fiykus ds fy, dgrs gSaA ;fn ugha ihrk gS rks xk; dk nw/k fiykus ds fy, dgrs gSaA I advise to give mother’s milk to the child. If he/she is not able to drink, then ask to give cow’s milk" [RMP-Agra (Key Informant)]
^^[kkus esa pkoy uk ns] larjk] ekSleh uk ns cPps dksA Child should not be given rice, orange, sweet lime" [RMP-Meerut (Key Informant)]
^^cPpk cM+k gS rks Hkkr ugha [kkuk pkfg,] ikyd] dn~nw ugha [kkuk pkfg,] BaMk ikuh ugha ihuk pkfg,A It the Child is older, then he/she should not eat rice, spinach, pumpkin. Should not drink cold water". [RMP-Darbhanga (Key Informant)]
^^cPps dks lnhZ okyk [kkuk ugha feyuk pkfg,] mM+n dh nky] elwj dh nky] lnhZ okys Qy& xUUkk] ve:n ugha [kkuk pkfg,A Child should not get cold food items like urad dal, masoor dal, fruits cold in nature like sugar care, guava should not be eaten" [RMP -Mahoba(Key Informant]
Report on Formative Research Findings Page 115
Methods of Examination and Consultation: : It was also inquired from the RMPs about the
method used by them for examining the children less than 5 years suffering from respiratory illness.
All RMPs took the history of the sick child who comes to their clinic. Most of them use stethoscope
and thermometer for examining the sick child. Some examined the sick child by exposing the chest,
while some RMPs touched the pulse to know temperature. Normally, RMPs take 1-2 minutes for
examining the sick child but if they are dispensing drugs also then they may take 2-3 minutes.
Signs of improvement assessed by RMP: RMPs were inquired about the signs of improvement
they have to look for, to ascertain whether sick child’s condition is improving or not. They were not
able to specify the signs of improvement they have to look for, when probed further, they said they
monitor improvement in the sick child through reduction in fever, cough and breathing rate.
Follow-up: RMPs were inquired about the follow-up of sick child less than 5 years suffering from
respiratory illness. Most RMPs said they do not visit the house of sick child instead they call the
patients at their clinic, while some of them said they visit the house of patients whenever they get a
call from the parents of sick child.
^^lnhZ dk osx ¼lkal½ T;knk gS rks dksbZ lq/kkj ughaA gk¡duk de gS] rks lq/kkj gks jgk gSaA If there is rapid breathing, then there is no improvement in the condition of child, however if the rate of breathing is less, it means there is some improvement" [RMP-Mahoba (Key Informant)]
Emerging Theme: Village Based Rural Medical Practitioner
The RMP is not able to recognize fast breathing as an early sign of pneumonia. They were also not able to report IMNCI danger signs. The RMP has limited information on how to manage pneumonia cases at the community level although they were very popular and often the first contact of health care seeking at the community level.
Report on Formative Research Findings
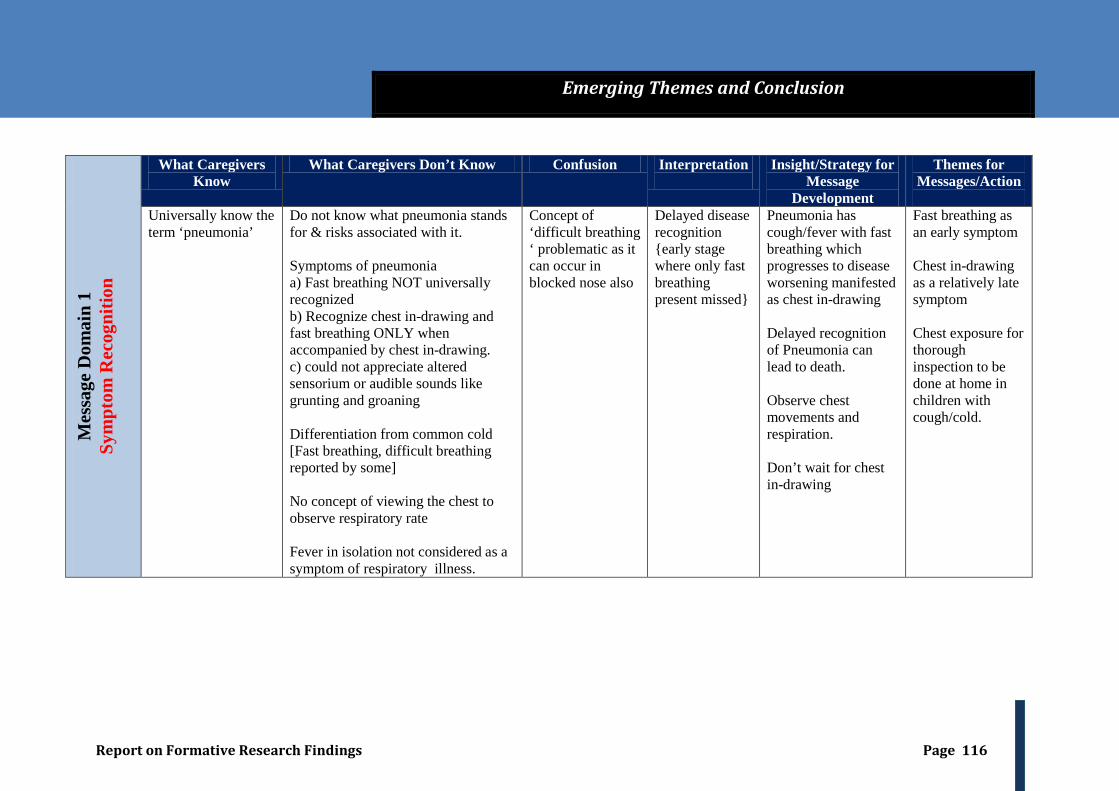
Report on Formative Research Findings Page 116
Mes
sage
Dom
ain
1 Sy
mpt
om R
ecog
nitio
n
What Caregivers Know
What Caregivers Don’t Know Confusion Interpretation
Insight/Strategy for Message
Development
Themes for Messages/Action
Universally know the term ‘pneumonia’
Do not know what pneumonia stands for & risks associated with it. Symptoms of pneumonia a) Fast breathing NOT universally recognized b) Recognize chest in-drawing and fast breathing ONLY when accompanied by chest in-drawing. c) could not appreciate altered sensorium or audible sounds like grunting and groaning Differentiation from common cold [Fast breathing, difficult breathing reported by some] No concept of viewing the chest to observe respiratory rate Fever in isolation not considered as a symptom of respiratory illness.
Concept of ‘difficult breathing ‘ problematic as it can occur in blocked nose also
Delayed disease recognition {early stage where only fast breathing present missed}
Pneumonia has cough/fever with fast breathing which progresses to disease worsening manifested as chest in-drawing Delayed recognition of Pneumonia can lead to death. Observe chest movements and respiration. Don’t wait for chest in-drawing
Fast breathing as an early symptom Chest in-drawing as a relatively late symptom Chest exposure for thorough inspection to be done at home in children with cough/cold.
Emerging Themes and Conclusion
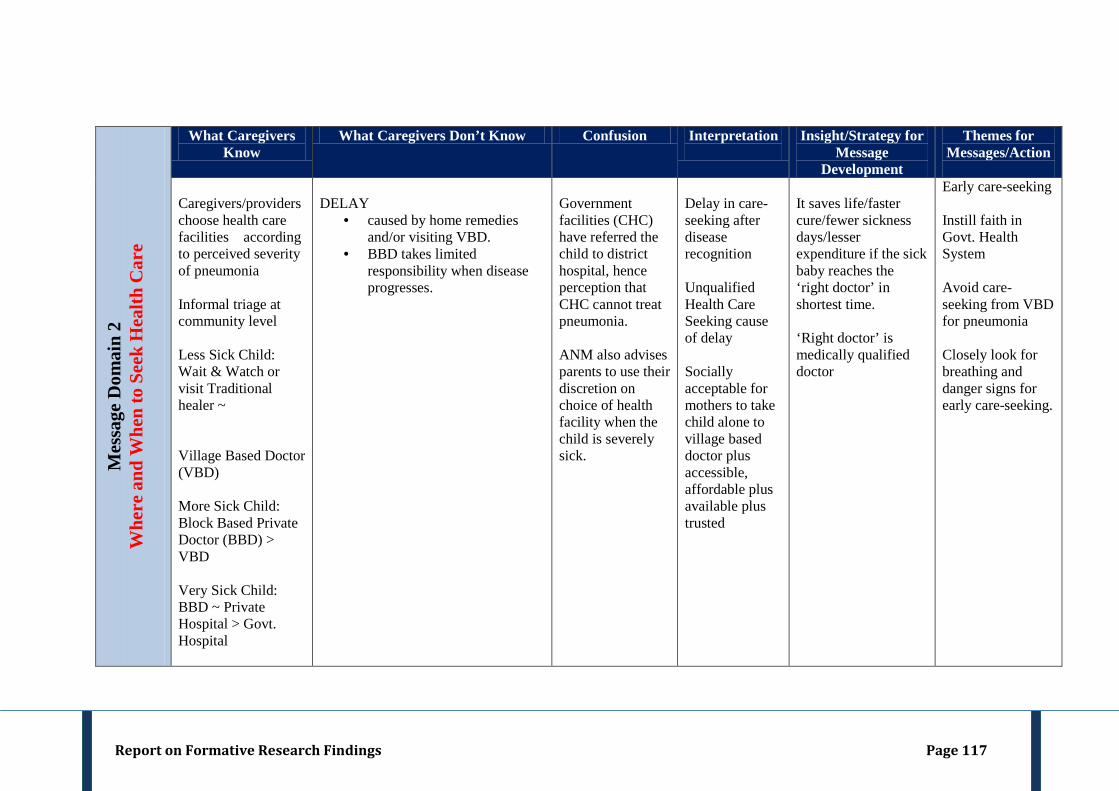
Report on Formative Research Findings Page 117
M
essa
ge D
omai
n 2
Whe
re a
nd W
hen
to S
eek
Hea
lth C
are
What Caregivers Know
What Caregivers Don’t Know Confusion Interpretation
Insight/Strategy for Message
Development
Themes for Messages/Action
Caregivers/providers choose health care facilities according to perceived severity of pneumonia Informal triage at community level Less Sick Child: Wait & Watch or visit Traditional healer ~ Village Based Doctor (VBD) More Sick Child: Block Based Private Doctor (BBD) > VBD Very Sick Child: BBD ~ Private Hospital > Govt. Hospital
DELAY
• caused by home remedies and/or visiting VBD.
• BBD takes limited responsibility when disease progresses.
Government facilities (CHC) have referred the child to district hospital, hence perception that CHC cannot treat pneumonia. ANM also advises parents to use their discretion on choice of health facility when the child is severely sick.
Delay in care-seeking after disease recognition Unqualified Health Care Seeking cause of delay Socially acceptable for mothers to take child alone to village based doctor plus accessible, affordable plus available plus trusted
It saves life/faster cure/fewer sickness days/lesser expenditure if the sick baby reaches the ‘right doctor’ in shortest time. ‘Right doctor’ is medically qualified doctor
Early care-seeking Instill faith in Govt. Health System Avoid care-seeking from VBD for pneumonia Closely look for breathing and danger signs for early care-seeking.
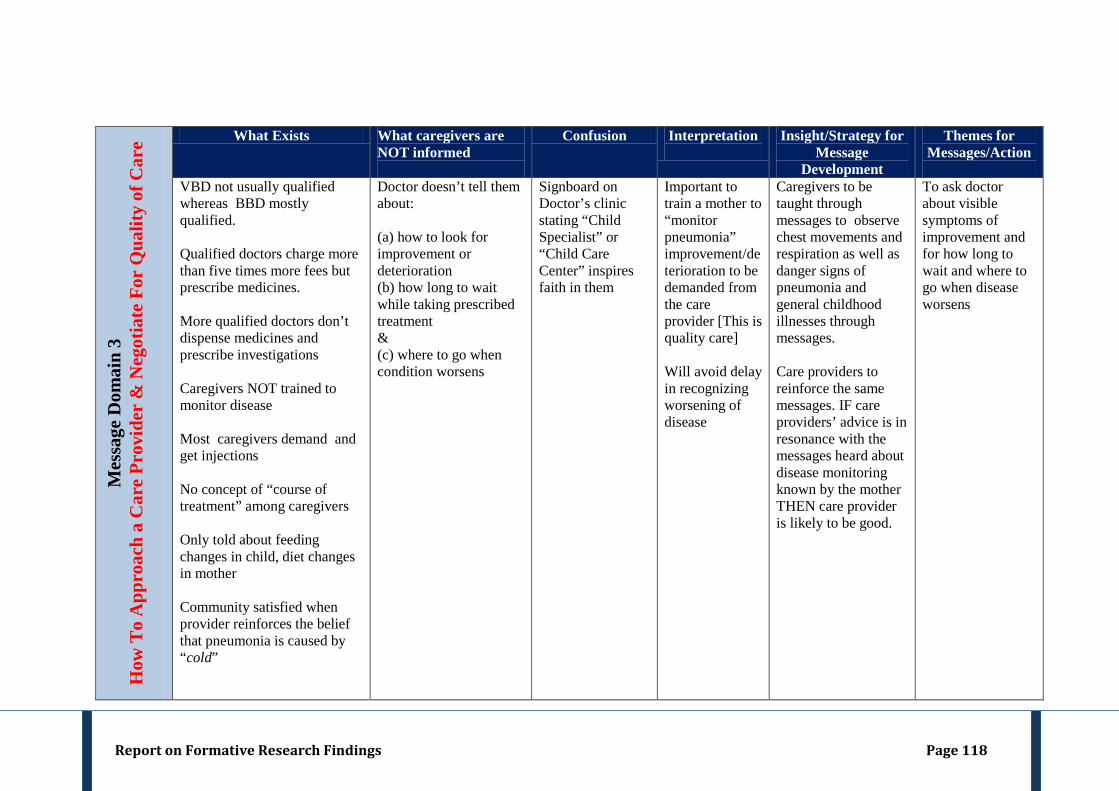
Report on Formative Research Findings Page 118
M
essa
ge D
omai
n 3
How
To
App
roac
h a
Car
e Pr
ovid
er &
Neg
otia
te F
or Q
ualit
y of
Car
e
What Exists What caregivers are NOT informed
Confusion Interpretation
Insight/Strategy for Message
Development
Themes for Messages/Action
VBD not usually qualified whereas BBD mostly qualified. Qualified doctors charge more than five times more fees but prescribe medicines. More qualified doctors don’t dispense medicines and prescribe investigations Caregivers NOT trained to monitor disease Most caregivers demand and get injections No concept of “course of treatment” among caregivers Only told about feeding changes in child, diet changes in mother Community satisfied when provider reinforces the belief that pneumonia is caused by “cold”
Doctor doesn’t tell them about: (a) how to look for improvement or deterioration (b) how long to wait while taking prescribed treatment & (c) where to go when condition worsens
Signboard on Doctor’s clinic stating “Child Specialist” or “Child Care Center” inspires faith in them
Important to train a mother to “monitor pneumonia” improvement/deterioration to be demanded from the care provider [This is quality care] Will avoid delay in recognizing worsening of disease
Caregivers to be taught through messages to observe chest movements and respiration as well as danger signs of pneumonia and general childhood illnesses through messages. Care providers to reinforce the same messages. IF care providers’ advice is in resonance with the messages heard about disease monitoring known by the mother THEN care provider is likely to be good.
To ask doctor about visible symptoms of improvement and for how long to wait and where to go when disease worsens
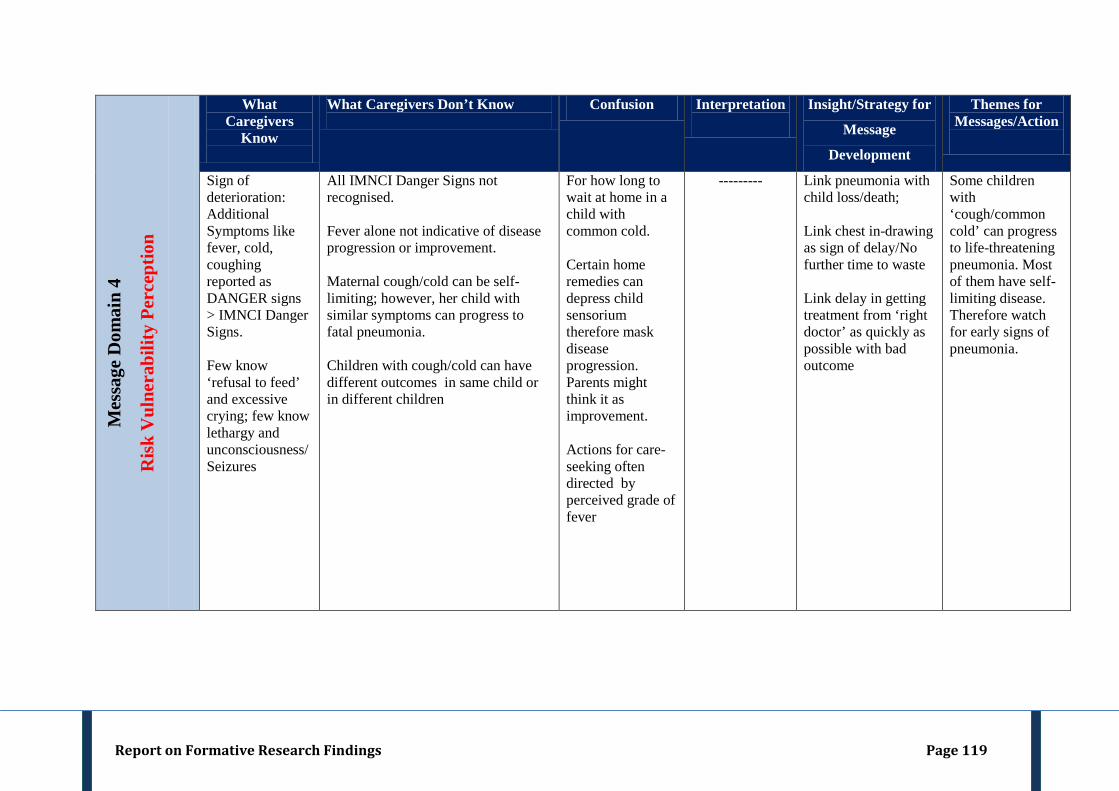
Report on Formative Research Findings Page 119
Mes
sage
Dom
ain
4
Ris
k V
ulne
rabi
lity
Perc
eptio
n
What Caregivers
Know
What Caregivers Don’t Know
Confusion Interpretation
Insight/Strategy for
Message
Development
Themes for Messages/Action
Sign of deterioration: Additional Symptoms like fever, cold, coughing reported as DANGER signs > IMNCI Danger Signs. Few know ‘refusal to feed’ and excessive crying; few know lethargy and unconsciousness/Seizures
All IMNCI Danger Signs not recognised. Fever alone not indicative of disease progression or improvement. Maternal cough/cold can be self-limiting; however, her child with similar symptoms can progress to fatal pneumonia. Children with cough/cold can have different outcomes in same child or in different children
For how long to wait at home in a child with common cold. Certain home remedies can depress child sensorium therefore mask disease progression. Parents might think it as improvement. Actions for care-seeking often directed by perceived grade of fever
---------
Link pneumonia with child loss/death; Link chest in-drawing as sign of delay/No further time to waste Link delay in getting treatment from ‘right doctor’ as quickly as possible with bad outcome
Some children with ‘cough/common cold’ can progress to life-threatening pneumonia. Most of them have self-limiting disease. Therefore watch for early signs of pneumonia.
Report on Formative Research Findings Page 120
Recommendations and Areas of Future Research
1. Community Awareness of pneumonia: Our study found that the community is familiar with the word pneumonia but was unable to recognize its signs and symptoms. They also were unaware of the consequence of late recognition of pneumonia. The communication tools developed in this project target these findings. Thus, there is a need of wide dissemination of messages developed through this project. Messages must percolate from caregivers to grass-root level health care providers to district hospital. All private health care providers including the village based local doctor need to be given the same messages. IEC material may be displayed in the community through Village Health Nutrition and Sanitation Committee (VHNSC). It needs to be explored further as to how NGOs can be involved to impart health education to the community. A Pneumonia information book may be developed and distributed widely across all stakeholders.
2. Strengthening the Government Public Health Services: We have learnt from our study that there exists distrust in the community of public health services. Therefore, the community resorts to seek care from unqualified health care provider, which causes further delay. Hence, there is a need to build trust of the community in the public health system through system strengthening and quality improvement. Few of the reasons for the lack of community`s trust are unavailability of the medicines as well as health care functionaries at public health facilities. Research on managing ARIs should focus on newer, innovative mechanism to strengthen services and facilities at the public health facilities and make them more responsive to the needs of the community. We found in our research that the community aspires to seek information from the ASHAs on childhood illnesses but in contrast, the ASHA workers have limited knowledge on childhood pneumonia management. They have not been trained on ARI management. The presence of ASHAs in each village must be leveraged for management of childhood pneumonia cases. Initiatives must be taken to orient the ASHAs about the barriers to health care seeking that exist in the community and ways of mitigating these. Further research can be undertaken to explore if ASHAs can play a role to provide outreach education on pneumonia to caregivers in villages.
3. Involving the RMPs in community wide pneumonia program: We found in our research that RMPs were not only the first point of contact for health care seeking but also the most trusted. We also found that these RMPs were able to judge when to treat and when to refer cases of childhood pneumonia based on “perceived severity of illness” but were unable to recognize IMNCI danger signs. Therefore, strategies to define the role of RMPs in a community wide pneumonia program needs to be explored further. Future research has to look into ways as to how the services of the RMPs can be acknowledged.
Report on Formative Research Findings Page 121
1. MoHFW: Rural Health Statistics In India. New Delhi: Ministry of Health & Family Welfare; 2012.
2. Srivastava NM, Awasthi S. Breastfeeding practices for newborns among urban poor in Lucknow, northern India: A prospective follow-up study. Clinical Epidemiology and Global Health. 2013. 10.1016/j.cegh.2013.03.003
3. Pandey N. Perceived Barriers
4. Corsi DJ, Bassani DG, Kumar R, Awasthi S, Jotkar R, Kaur N &Jha P. Gender inequity and age-appropriate immunization coverage in India from 1992 to 2006.BMC International Health & Human Rights 2009; 9 (Suppl 1): S3
to Utilization of Maternal Health and Child Health Services: Qualitative Insights from Rural Uttar Pradesh, India. http://paa2011.princeton.edu/papers/ 111751
5.
doi:10.1186/1472-698X-9-S1-S3
Kalter HD, MohanP,MishraA,GaonkarN,Biswas AB, Balakrishnan S, AryaG,Babille M.
6. Igor Rudan, Epidemiology and etiology of childhood pneumonia, Bull World Health Organ. 2008
Maternal death inquiry and response in India - the impact of contextual factors on defining an optimal model to help meet critical maternal health policy objectives.Health Res Policy Syst.2011;9: 41.
7. Ratna Devi. Barriers of access to health care in India. http://www.indiahealthprogress.in /barriers-access-healthcare-india accessed on 28th
8. Awasthi S, Srivastava NM, Agarwal GG, Pant S &Ahluwalia TP. Effect of behavior change communication on qualified medical care-seeking for sick neonates among urban poor in Lucknow, northern India: a before and after-intervention study.Tropical Medicine & International Health 2009; 14(10): 1199-1209
May 2012.
9. Nichter M. Social Science lessons from diarrhea research and their application to ARI. Human Organization 1993; 52(1): 53-67.
10. Gattam M. ‘First We Go To The Small Doctor’: First Contact For Curative Health Care Sought By Rural Communities In Andhra Pradesh & Orissa, India . Indian J Med Res. Nov 2011; 134(5): 627–638.
References
Project Team Members