
Report on DTC pharmaceutical promotion for PHARMAC
46
Report on DTC pharmaceutical promotion for PHARMAC From Peter Mansfield, MaLAM Contents Contents.............................................................1 Acknowledgments......................................................2 Introduction.........................................................2 Background............................................................ 2 It is extremely difficult to evaluate drugs and information about drugs even with specialist postgraduate medical training........................2 Pharmaceutical promotion is a major influencing on prescribing, drug taking and health care......................................................3 Pharmaceutical promotion often includes potentially misleading claims.3 Doctors do not have all the skills required to avoid being adversely influenced by promotion and many consumers have less skills..........4 Misleading promotion can lead to adverse health outcomes.............5 It is unreasonable to expect drug companies to be able to produce reliable information about drugs..............................................6 Adverse economic effects..............................................6 Regulation of promotion is not anti-competitive......................6 DTC drug promotion increases costs for drug companies, consumers and taxpayers............................................................7 DTC drug promotion can cause market distortions that divert resources towards less cost effective therapy and/or less serious conditions and thus away from cost effective therapy for serious conditions that deserve priority on the basis on health care needs...........................9 DTC drug promotion can cause wasteful expenditure on drugs for conditions where there is little or no benefit.................................11 Adverse effects on Health............................................11 There is no evidence of benefit from DTC pharmaceutical promotion. The limited evidence available suggests that DTC pharmaceutical promotion is harmful to health...................................................11 DTC promotion is not a helpful source of information for the public. 12 DTC drug promotion may cause severe adverse outcomes because many patients believe they can make decisions with their doctor’s advice..........13 DTC promotion increases patient demands which can lead to inappropriate drug use.................................................................14 DTC drug promotion leads to increased use of new drugs which are less well tested because they are new and consequently may be more dangerous.. 14 DTC promotion may involve loss of patient confidentiality...........15 The argument that “the battle against DTC drug promotion is lost already because of the Internet” is false...................................15 Key interest groups do not support DTCA..............................15 Many drug companies are not keen on DTC drug promotion..............15 Disease foundations and patients groups oppose DTC promotion because it can overwhelm their agenda..............................................15
Transcript of Report on DTC pharmaceutical promotion for PHARMAC

Report on DTC pharmaceutical promotion for PHARMACFrom Peter Mansfield, MaLAM
Contents
Contents........................................................................................................................................................1Acknowledgments........................................................................................................................................2Introduction..................................................................................................................................................2
Background.......................................................................................................................................................2It is extremely difficult to evaluate drugs and information about drugs even with specialist postgraduate medical training..........................................................................................................................................................2Pharmaceutical promotion is a major influencing on prescribing, drug taking and health care..................3Pharmaceutical promotion often includes potentially misleading claims....................................................3Doctors do not have all the skills required to avoid being adversely influenced by promotion and many consumers have less skills..............................................................................................................................................4Misleading promotion can lead to adverse health outcomes........................................................................5It is unreasonable to expect drug companies to be able to produce reliable information about drugs.........6
Adverse economic effects.................................................................................................................................6Regulation of promotion is not anti-competitive..........................................................................................6DTC drug promotion increases costs for drug companies, consumers and taxpayers.................................7DTC drug promotion can cause market distortions that divert resources towards less cost effective therapy and/or less serious conditions and thus away from cost effective therapy for serious conditions that deserve priority on the basis on health care needs.......................................................................................................................9DTC drug promotion can cause wasteful expenditure on drugs for conditions where there is little or no benefit.....................................................................................................................................................................11
Adverse effects on Health...............................................................................................................................11There is no evidence of benefit from DTC pharmaceutical promotion. The limited evidence available suggests that DTC pharmaceutical promotion is harmful to health..........................................................................11DTC promotion is not a helpful source of information for the public.......................................................12DTC drug promotion may cause severe adverse outcomes because many patients believe they can make decisions with their doctor’s advice...........................................................................................................................13DTC promotion increases patient demands which can lead to inappropriate drug use..............................14DTC drug promotion leads to increased use of new drugs which are less well tested because they are new and consequently may be more dangerous........................................................................................................14DTC promotion may involve loss of patient confidentiality......................................................................15The argument that “the battle against DTC drug promotion is lost already because of the Internet” is false.....................................................................................................................................................................15
Key interest groups do not support DTCA.....................................................................................................15Many drug companies are not keen on DTC drug promotion....................................................................15Disease foundations and patients groups oppose DTC promotion because it can overwhelm their agenda15Pharmacists oppose DTC drug promotion because they do not provide useful information.....................16Consumer advocates oppose DTC drug promotion because it decreases consumers’ abilities to make good choices........................................................................................................................................................17Medical educators oppose DTC drug promotion because it is does not provide the information that is needed for optimal health care outcomes.....................................................................................................................25Doctors oppose DTC drug promotion because it damages the doctor patient relationship and harms patients.....................................................................................................................................................................25
Advances in Technology................................................................................................................27How Direct-to-Consumer Advertising Strains the Physician-Patient Relationship.......................28
The last word..............................................................................................................................................34

AcknowledgmentsI thank:Alistair Lloyd (Melbourne), Barbara Mintzes (Vancover), Charles Medawar (London), Clare Mansfield (Adelaide), Joel Lexchin (Toronto), Lynn Telfer (Adelaide) and Nicola Young, Ruth Casavalone and Sarah Thomson (Wellington) for invaluable assistance just at the right time.
I hope that together we have contributed towards preventing unnecessary suffering for large numbers of people in New Zealand.
IntroductionThe best evidence available strongly suggests that Direct To Consumer Advertising (DTCA) does much more harm to public health than good. Unless well-designed, independent studies can overturn that the government should consider stricter rather than more permissive regulations and restrictions.1
Expenditure on expensive drugs “exerts pressure for cuts to funding for hospitals and for GPs. DTC promotion exacerbates that problem by increasing demand for more expensive drugs and reduces the funds available for independent information. As long as drug companies are paid according to sales, regardless of the impact on health outcomes, DTC promotion is harmful to taxpayers, health professionals and most importantly our patients. … DTC promotion… should be prohibited urgently.”2
Background
It is extremely difficult to evaluate drugs and information about drugs even with specialist postgraduate medical training.
There is one type of goods that can be accurately evaluated by consumers prior to purchase so that the consumers can make good decisions about whether or not the good is worth the price. For goods of this type consumers are in a strong position to evaluate promotional claims.
There is another more common type of good that can only be accurately evaluated by consumers after purchase and use. . For goods of this type consumers are vulnerable to misleading promotion prior to the first purchase. However after first use of goods of this type consumers can make good decisions about whether or not the good was worth the price and/or whether or not the promotion was reliable. If the evaluation is negative then the consumer can choose not to purchase again and may warn others against that product. The costs of this market correcting mechanism for the consumer depend on how big and/or important and/or frequent the purchase is.
Pharmaceuticals do not belong to either of those groups. They belong to a group of goods that cannot be accurately evaluated by the individual consumer before or even after use. For most drugs even the probabilities of benefits and adverse effects on average are incompletely known even by experts.
Many people incorrectly believe that they can determine the effect of a drug by observing any changes that occur after taking the drug. This common form of reasoning is well known by logicians as the fallacy of “post hoc ergo propter hoc” (after that therefore because of that). Improvements are observed after taking a drug may be due to the drug or another therapy or an improvement in the disease that would have happened any way or wishful thinking or the placebo effect or regression to the mean (a property of the statistics of random fluctuations) or any combination of those factors. Please note that for many drugs the placebo effect is more powerful than the active ingredient effect. Adverse events observed following taking a drug may be due to the drug or the disease or another disease or another therapy or any combination of those factors. Evaluation is made even more difficult by the fact that the real benefits and/or adverse effects of a drug may not occur for many years after starting the drug. For example blood pressure therapy commenced by a 40 year old woman to prevent a heart attack at the age of 60 will take 20 years of costs before the real benefit occurs. An additional difficulty which can be illustrated by the previous example is the fact that we can not predict when the heart attack would have occurred with out therapy. Further more we can not
1 Hollon MF. Direct to consumer marketing of prescription drugs: creating consumer demand. JAMA 1999;281:4:382-42 Mansfield P. No. Aust Doc Weekly 1999; 8 October:64

predict which women with high blood pressure will die from an unrelated condition and thus never receive any benefit.
Pharmaceutical promotion is a major influencing on prescribing, drug taking and health care.
An international survey has revealed that typical Trade name drug companies estimate that they spend around 35% of sales on promotion.3 (The Pharmac subsidy for 1997-98 was $ 769 million. If the 35% estimate is accurate for New Zealand then $ 269 million of taxpayers’ money was spent on promotion that year.) Companies would not spend such massive amounts on promotion if it was not effective at influencing prescribing and thus drug sales.
Many studies have shown that promotion is a major influence on health care.4,5,6,7,8
Pharmaceutical promotion often includes potentially misleading claims.
Studies of promotion show that misleading claims and misleading appeals are frequently used.
A 1992 study of 109 drug advertisements in US medical journals found that 57% of these advertisements had little or no educational value and found that 44% would lead to improper prescribing if relied upon.9 That study was conducted in the US where advertisements are generally more reliable than in other countries because there is active government regulation of drug promotion in the US unlike in most other countries..
Wade et al. asked pharmaceutical companies to supply their best evidence in support of marketing claims. Of 67 references cited, only 31 contained relevant original date and only 13 were controlled trials. These investigators concluded, “Standards of evidence used to justify advertising claims are inadequate”.10
In a study of advertising in the leading medical journals in 18 countries, Herxheimer et al reported that important warnings and precautions were missing in half of the 6,700 advertisements surveyed.11
Stryer and Bero concluded that advertisements contained a higher proportion of promotional material than educational material, and little of this material contained information about important therapeutic breakthroughs.12
Consumer Reports, evaluated the accuracy of information in prescription drug advertisements directed at patients in the USA and found similar results to the studies of marketing directed at physicians. The study concluded that information from marketing has little educational benefit and, in general, its quality is poor. Less that half of DTC advertisements reviewed were candid about efficacy. Consumer Reports concluded, “the rules governing
3 Devlin J, Hemsley P. Management views on industry issues, pressures and consultants. Scrip Magazine. 1997; June: 16-184 Caudill TS, Johnson MS, Rich EC, McKinney P. Physicians, pharmaceutical sales representatives and the cost of prescribing. Arch Fam Med 1996; 5:201-65 Orlowski JP, Wateska L. The effects of pharmaceutical firm enticements on physician prescribing patterns: There’s no such thing as a free lunch. Chest 1992; 102: 270-736 Waud DR. Pharmaceutical promotions. New Engl J Med 1992; 327: 23: 16887 Chren M-M, Landefeld CS. Physicians' behaviour and their interactions with drug companies: A controlled study of physicians who requested additions to a hospital drug formulary. JAMA 1994; 271: 9: 684-98Vitry A. Pharmaceutical promotion: Drug advertising affects your prescribing. Australian Prescriber 1996; 19: 4: 1039 Wilkes MS, Doblin BH, Shapiro MF. Pharmaceutical advertisements in leading medical journals: Experts’ assessments. Ann Int Med 1992; 116: 912-91910 Wade VA, Mansfield PR, McDonald PJ. Drug companies’ evidence to justify advertising. Lancet 1989;2 :1261-4. 11 Herxheimer A, Lundborg CS, Westerholm B. Advertisements for medicines in leading medical journals in 18 countries: a 12-month survey of information content and standards. Int J Health Serv 1993;23:161-72.12 Stryer D, Bero LA. Characteristics of material distributed by drug companies: an evaluation of appropriateness. J Gen Intern Med 1996;11:575-83.

prescription drug advertising should not be loosened.” and that “advertisements are not public service messages – they’re meant to move goods.”13
A study of drug representatives in Melbourne found that the product information was contradicted in 11 of 16 visits.14 This was despite the fact that contradicting the product information is not just harmful to patients but it is also illegal and the representative knew that they were being taped. That study was performed in Australia. Similar results have been found in the US15 and France.16
Television and magazine advertisements for children’s medications were monitored from March 15, 1988 to May 3, 1988 and were analysed for their content to see how well they complied with South Korean regulations governing advertisement of medications. This report presents numerous examples of advertisements that violate the regulations. For television ads the conclusion was that drug companies continue to overtly violate the regulations and the appropriate government authorities have failed to take any measures to end these violations despite the fact that they are aired on public stations. 66 out of 74 ads in magazines contained phrases that violated the regulations.
An analysis of texts of advertisements for non-registered pharmaceutical products published in a popular magazine in the Netherlands found a gap between legislation and practice involving 65% of the analysed advertisements.17
Unless much money is spent on government regulation then we can expect similar results in New Zealand.
Doctors do not have all the skills required to avoid being adversely influenced by promotion and many consumers have less skills.
Mansfield (1999) has explained to doctors that not have all the skills required to avoid being adversely influenced by promotion as follows:
“Can you sort the wheat from the chaff?Some people believe that doctors are not adversely influenced by promotion because we are intelligent enough to sort the wheat from the chaff. It is just as helpful to say that we are all smart enough to pilot a space shuttle. In both cases what we need first is adequate training. Our ability to evaluate promotion depends on our understanding of General Practice, Pharmacology, Epidemiology, Public Health, Evidence Based Medicine, Drug Evaluation, Pharmacovigilance, Statistics, Psychology, Economics, Sociology, Anthropology, Management, History, Politics, Media Studies, Logic, Rhetoric, Epistemology, Linguistics, Evaluation of Literature and Art, and various sub disciplines of Marketing including Product Management, Advertising Account Planning and Public Relations. This article will now introduce of just one of those areas: Logic.
Fallacies of logic.Pharmaceutical promotion may lead to unjustified conclusions via over 100 fallacies. It is difficult to find promotion that does not contain at least one fallacy. Fallacies are used in deliberate deception but often occur more innocently with self-deception. Some fallacies are relatively easy to detect if you know about them. Others are very difficult. Some can only be detected after time consuming double-checking and we rarely have the time required.
13 Drug advertising: is this good medicine? Consumer Reports 1996;June:61:6:62-314 Roughead EE. The pharmaceutical representative and medical practitioner encounter: implications for quality use of medicines. Masters Thesis. School of Health Systems Sciences. La Trobe University. Aug 199515 Ziegler, M.G., Lew P. and Singer, B.C. The Accuracy of Drug Information from Pharmaceutical Sales Representatives. 1995 JAMA 273. pp.1296-129816 Bardelay D, Bécel B. Visits from medical representatives: fine principles, poor practice. Presr Intern 1995: 4: 18: 120-122 Vo-Kyung, Song and Ok Kim, Jai. Investigation of the violations of pharmaceutical regulations in advertisements of children’s medicines. ARDA review, evaluation and planning meeting; Manila, Philippines. 198817 Wieringa, N. F.; de Meijer, A. H. R.; Schutjens, M. D. B., and Vos, R. The gap between legal rules and practice in advertising non-registered pharmaceutical products: a new method of analysis. Social Science and Medicine. 1992; 35:1497-1504

Most of the fallacies used in promotion belong to one or more of the following categories:
Unjustified claims. For example, drug reps often contradict the approved product information. Beware promotion that accurately conveys investigators’ conclusions when those conclusions are not justified by the rest of the study.
Exaggeration of benefits or Minimization of risks. This may be done in the headlines or pictures. These influence even those who try not to read advertisements.
Omission. “Bad news” may be omitted completely or effectively omitted by use of fine print that few doctors find time to read.
Wrong reasons. Promotion often uses appeals to biased experts, peer pressure, gifts (reciprocal obligations), friendship, attractiveness and other methods because they work regardless of how good the drug is. Beware surrogate endpoints. Focus on clinically important endpoints.
Oversimplification. “If it is simple its false.” Beware any attempt to reduce the effect of a drug to one or two numbers eg relative risk reductions. Request a Kaplan Meier survival analysis because a graph is worth a thousand numbers. Beware single averages that may cover more than one category because it is just as helpful to say that the average adult has one breast and one testicle.
Unclear information. This includes vague statements that take advantage of optimistic interpretation, numerous fallacies of ambiguity and “blinding with science”.
Conclusion:Unless you have many skills not taught in medical schools and the time required to double-check everything and if you are human then you are probably adversely influenced by drug promotion.”18
“The aim of promotion is not to educate but to persuade. Promotion uses conscious and subconscious appeals to the head and to the heart which have been developed over thousands of years since they were discussed by the ancient Greeks. Promotion is a sophisticated applied science. Advertisers were using controlled trials involving as many as 25,000 subjects back in the 1920s. Promotion is better resourced and more sophisticated than modern medicine. DTC promotion uses sophisticated methods to get patients to jump to a decision to demand a specific drug with out hearing the other side of the story.”19
Consumers who have university training in one or more of the areas listed above may be better able to avoid being mislead than doctors but are vulnerable because of lack of medical knowledge. Promotion does not fool all of the people all of the time. It fools the more vulnerable. Those in society who have less skill are more likely to suffer illness and also less likely to be able to avoid being mislead.
Misleading promotion can lead to adverse health outcomes.
Reliance on promotional information correlates with more expensive and less appropriate prescribing ,20 and may lead to serious adverse effects including deaths.21 22
18 Mansfield P. Are you adversely influenced by drug promotion? National prescribing Service News [Submitted for publication 1999]19 Mansfield P. No. Aust Doc Weekly 1999; 8 October:64 Haayer F. Rational prescribing and sources of information. Soc Sci Med 1982;16:2017-23. 20 Caudill TS, Johnson MS, Rich EC, McKinney P. Physicians, pharmaceutical sales representatives and the cost of prescribing. Arch Fam Med 1996; 5:201-621 Gijsbers AJ, Clarke BG. Ketorolac. Med J Aust 1993; 158: 72022 Aders HP. Legal liability and drug prescribing. Cur Therap 1991; 32 6: 17-21
Examples provided by Hollon (1999) include: “Consider also benoxaprofen, a prescription non-steroidal anti-inflammatory agent, launched in 1980 in the United Kingdom and subsequently the United States. The product gained “a major foothold merely on the strength of a well-orchestrated marketing strategy, which included full-page advertisements in the popular press. “Sixty-one drug-related deaths occurred during the 2 years in which the drug remained on the market.
For example, a recent survey of trends in antipypertensive drug use in the United States revealed that despite the recommendations of the Fifth Joint National Committee on the Detection, Evaluation, and Treatment of High Blood Pressure, the use of calcium antagonists and angiotensin-converting enzyme inhibitors has increased. The investigators cite the effectiveness of pharmaceutical promotion practices as one of the possible reasons for this. They note, “the cost implications of these practice patterns are enormous.”23
It is unreasonable to expect drug companies to be able to produce reliable information about drugs.
It is extremely difficult for anyone to provide reliable information about health care. A study of therapy guidelines produced in Australia by medical experts found that the majority failed to meet the lenient NHMRC guidelines for producing guidelines.24 A study of pamphlets for consumers about breast cancer screening found that they were all misleading.25 The difficulty is not only because drugs are difficult to evaluate but also because complex and uncertain information is difficult to communicate. As the French writer Paul Valery pointed out: “If it’s simple it’s false but if not then it’s useless.”
It is even more difficult for drug companies to provide reliable drug information because of deliberate and/or subconscious bias. The current system rewards drug companies for increasing sales regardless of impact on health care outcomes. Companies that are less effective are taken over by those that are more effective. Consequently company staff have little choice but to increase sales regardless on impact on health care outcomes or leave their very well paid jobs. One way of coping with this is for companies to develop a “group think” where staff reinforce each others belief that their drugs really are superior and underused and that it is only enemy companies which use misleading promotion.26
Adverse economic effects
Regulation of promotion is not anti-competitive.
If the Review is assuming that regulation of advertising is anti-competitive then that assumption must be questioned. Regulation of misleading promotion enables companies to compete fairly on the merits of their products (cost/benefit ratios) by protecting companies with superior products from unfair competition based on dishonesty and/or self-deception. An industry consultant has predicted that with increasing DTCA: “The winners in the prescription drug category are not going to be the ones with the best patents or products, but those that are the best marketers.”27
Direct to Consumer Advertising of prescription drugs (DTCA-Rx) reduces competition by making it more difficult for new companies to enter the market and by making it more difficult for Generic companies (who by definition compete by using less promotion and therefore lower prices) to compete with Trade name companies (who by definition compete by using more promotion and therefore higher prices). Smeeding (1990) states that the first of “five major motivations for the [Trade name] pharmaceutical industry’s entrance into DTCA-Rx [appears to
23 Hollon MF. Direct to consumer marketing of prescription drugs: creating consumer demand. JAMA 1999;281:4:382-424
25
26 Mansfield P. Are Pharmaceutical customers prey or partners? Scrip magazine 1995: June: 14-527 Freeman L. Aggressive strategy helps propel Claritin to top slot. Advertising age 1998; 16 March:69:11:S6-7

be that] a rise in generic substitution has lead to increasing competition and the need to develop brand loyalty” to reduce competition from Generic companies who provide the same drug at a lower price.28 The most recent report on DTCA-Rx in the USA from IMS (the leading market research company) confirms Smeeding’s analysis. IMS gives two main reasons for DTC advertising. “Companies are using DTC advertising as a short-term marketing strategy to bring patients into physicians’ offices and generate new prescriptions [ie expanding the market rather than competing within it] and also for longer term reasons, to generate brand loyalty and therefore to counteract the downturn from patent expiry [which enables generic competition] and OTC product switches.”29
Dr Philip Brown is the editor of Scrip Magazine which is the leading journal for pharmaceutical company executives. He states that “What brought home to me the significance of direct –to-consumer promotion was a comment last week from a senior industry executive who believes that it could become a major factor in shaping the future of the industry. He argued that the success or failure of a new R&D- based prescription product in the US now depends on the size of the direct-to-consumer advertising budget. What chance, he asked, does company A have with, for example, a US$50 million budget for direct-to-consumer advertising for its new prescription medicine, if the far bigger competitor, company B, decides to spend US$600 million? The short answer is very little. So are we facing a whole new scenario where the market will become dominated by the big direct-to-consumer advertisers – and that means the big companies - and where customer choice, stimulated by advertising, will determine a prescription product’s success? Providing the prescribing doctor acquiesces to the demands of the patient, the answer must be yes. All the evidence suggests that in a free market, what the patient asks for, the doctor will prescribe. As a Consumer Association survey published a few weeks ago shows, even in the impoverished UK National Health Service, patient demand holds sway when it comes to prescribing. According to the Association hundreds of millions of pounds worth of pharmaceutical are being prescribed because patients demand them. Of particular concern is the fact that in many cases the prescription was inappropriate, notably where antibiotics were prescribed in viral conditions. But even in these cases, although prescribing was irrational, the doctors still gave in to patient demand.”30
DTC drug promotion increases costs for drug companies, consumers and taxpayers.
DTC promotion increases costs.31
An international survey has revealed that typical brand-based drug companies estimate that they spend around 35% of sales on promotion.32 According to a report in New Zealand Doctor an AC Nielsen audit of the media (using rate card estimates for the prices of advertising) has produced estimates for spending on DTC drug advertising in New Zealand of 57.2 million dollars in 1997 and 50.7 million dollars in 1998.33 This may not include all the payments to advertising agencies. Those estimates would not include the companies’ internal costs for developing the advertising or the costs of public relations activities. To the extent that some of the drugs were subsidised by the taxpayer contributes to costs for taxpayers. To the extent that patients had to pay for the drugs that advertising c contributes to costs for patients.
If company A increases market share by spending on DTC drug promotion then their competitor - company B is under pressure to also spend on DTC promotion. This then puts pressure on company A to spend more on DTC promotion to regain the earlier advantage. This puts further pressure on company B leading to a vicious cycle of increasing costs that can only be recovered by passing them on to the consumer. This is an example of inefficiency from competition that is well known to economists and is sometimes called the “the soap box effect”.
28 Smeeding. JE. Direct-to consumer advertising of prescription pharmaceuticals: Strategic issues for the pharmaceutical industry. Top Hosp Pharm Manage 1990;10:1:40-6429 US DTC advertising producing investment returns. Scrip 1999;12 June:2446:1730 Brown P. Will DTC advertising shape the future of the industry? Scrip Magazine 1998; September: 3-4 31 O’Brien, M. Advertising prescription drugs to the public. New England Journal of Medicine. 1986; 314:52332 Devlin J, Hemsley P. Management views on industry issues, pressures and consultants. Scrip Magazine. 1997 June 16-1833 MacKinven M. Pill purveyors go direct. New Zealand Doctor 1999;17 March

On the basis of a survey performed by Prevention magazine in the USA in May 1998 it has been estimated that direct-to-consumer advertising prompted an estimated 21.2 million Americans to talk to their doctors about a medical condition or illness they had never discussed with a physician before.34 For many of those people the reason for not mentioning it was that it was not severe enough or they were coping with their symptoms perhaps by not focusing on them. Focusing on physical sensations increases the perception and thus the severity. The result is increased costs for the individual or the taxpayer.
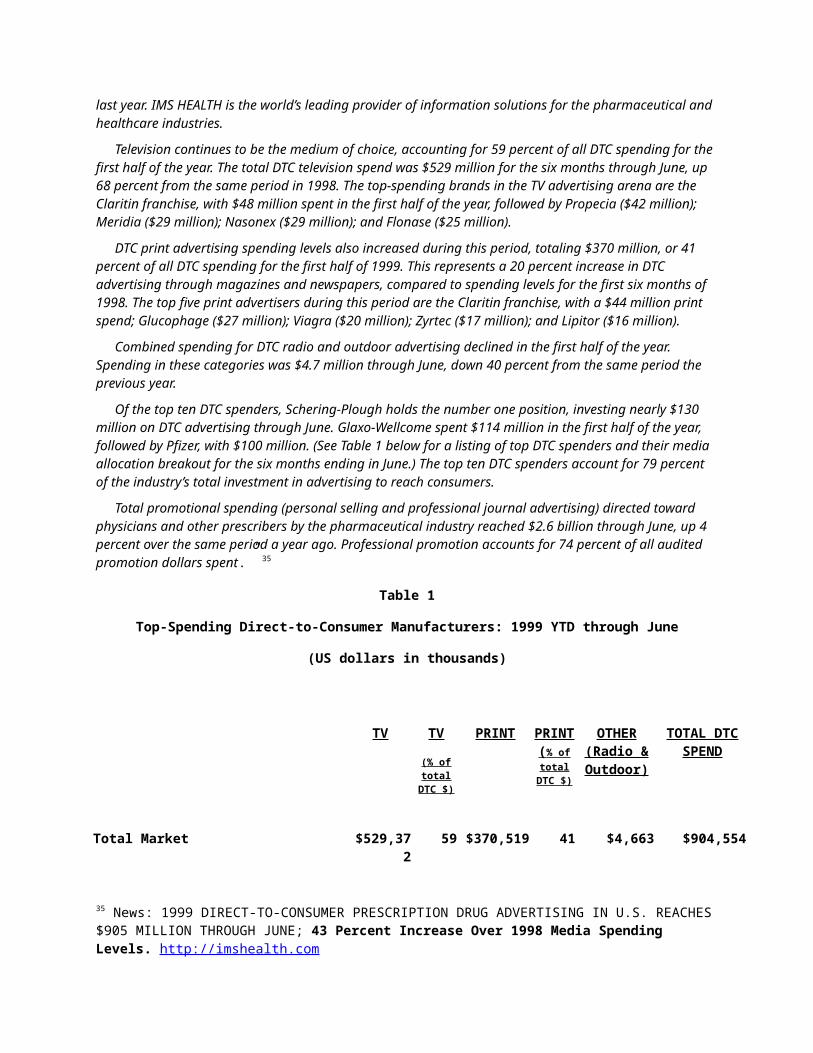
DTCA in the US is now costing the economy about US$ 2 billion per annum. “LONDON, October 12, 1999 – IMS HEALTH (NYSE:RX) reported today that direct-to-consumer (DTC) prescription drug advertising in the U.S. continues its strong, double-digit growth, reaching $905 million for the first half of 1999. This represents a 43 percent increase over spending levels for the same period last year. IMS HEALTH is the world’s leading provider of information solutions for the pharmaceutical and healthcare industries.
Television continues to be the medium of choice, accounting for 59 percent of all DTC spending for the first half of the year. The total DTC television spend was $529 million for the six months through June, up 68 percent from the same period in 1998. The top-spending brands in the TV advertising arena are the Claritin franchise, with $48 million spent in the first half of the year, followed by Propecia ($42 million); Meridia ($29 million); Nasonex ($29 million); and Flonase ($25 million).
DTC print advertising spending levels also increased during this period, totaling $370 million, or 41 percent of all DTC spending for the first half of 1999. This represents a 20 percent increase in DTC advertising through magazines and newspapers, compared to spending levels for the first six months of 1998. The top five print advertisers during this period are the Claritin franchise, with a $44 million print spend; Glucophage ($27 million); Viagra ($20 million); Zyrtec ($17 million); and Lipitor ($16 million).
Combined spending for DTC radio and outdoor advertising declined in the first half of the year. Spending in these categories was $4.7 million through June, down 40 percent from the same period the previous year.
Of the top ten DTC spenders, Schering-Plough holds the number one position, investing nearly $130 million on DTC advertising through June. Glaxo-Wellcome spent $114 million in the first half of the year, followed by Pfizer, with $100 million. (See Table 1 below for a listing of top DTC spenders and their media allocation breakout for the six months ending in June.) The top ten DTC spenders account for 79 percent of the industry’s total investment in advertising to reach consumers.
Total promotional spending (personal selling and professional journal advertising) directed toward physicians and other prescribers by the pharmaceutical industry reached $2.6 billion through June, up 4 percent over the same period a year ago. Professional promotion accounts for 74 percent of all audited promotion dollars spent.” 35
Table 1
Top-Spending Direct-to-Consumer Manufacturers: 1999 YTD through June
(US dollars in thousands)
TV TV
(% of total
DTC $)
PRINT PRINT ( % of total
DTC $)
OTHER (Radio & Outdoor)
TOTAL DTC SPEND
34 http://www.phrma.org/facts/bkgrndr/advert.html35 News: 1999 DIRECT-TO-CONSUMER PRESCRIPTION DRUG ADVERTISING IN U.S. REACHES $905 MILLION THROUGH JUNE; 43 Percent Increase Over 1998 Media Spending Levels. http://imshealth.com

Total Market $529,372 59 $370,519 41 $4,663 $904,554
SCHERING-PLOUGH CORP $76,930 59 $50,465 39 $2,315 $129,710
GLAXO WELLCOME PLC $89,253 78 $25,048 22 $146 $114,447
PFIZER INC $45,621 45 $54,201 54 $498 $100,319
ASTRAZENECA PLC $62,493 72 $24,036 28 $0 $86,528
MERCK & CO INC $45,898 71 $18,891 29 $29 $64,818
JOHNSON & JOHNSON $41,419 66 $21,163 33 $620 $63,203
WARNER-LAMBERT CO $20,099 46 $23,716 54 $18 $43,833
PHARMACIA & UPJOHN INC $20,306 55 $16,849 45 $0 $37,155
KNOLL PHARMACEUTICAL CO $29,599 81 $7,098 19 $0 $36,697
AMERICAN HOME PDTS CORP $8,292 23 $28,212 77 $0 $36,504
Source: IMS HEALTH and Competitive Media Reporting (CMR)
Those huge cost increases are either an increased cost for the industry or they are expanding the market in proportion to the 43% increase in spending since last year. If DTCA is allowed to continue in New Zealand then it will cause severe damage to Health Care Funding and may place a significant strain on the entire New Zealand economy.
DTC drug promotion can cause market distortions that divert resources towards less cost effective therapy and/or less serious conditions and thus away from cost effective therapy for serious conditions that deserve priority on the basis on health care needs.
DTC promotion diverts attention and resources away from many important conditions that are not sources of big profits for drug companies including conditions that are only common amongst poorer people or best treated with non-drug therapy or less expensive drugs. Often this distortion is away from serious life threatening conditions such as malaria towards less serious conditions such as baldness where drugs provide less benefit for money.
An industry consultant has predicted that with increasing DTCA: “The winners in the prescription drug category are not going to be the ones with the best patents or products, but those that are the best marketers.”36
A study of the content of direct-to-consumer prescription drug advertising in eight popular consumer magazines in the US from 1992 to 1995 found dramatic increases in the frequency of such ads and greater numbers of ads for drugs that treat chronic ailments rather than life-threatening medical conditions.37
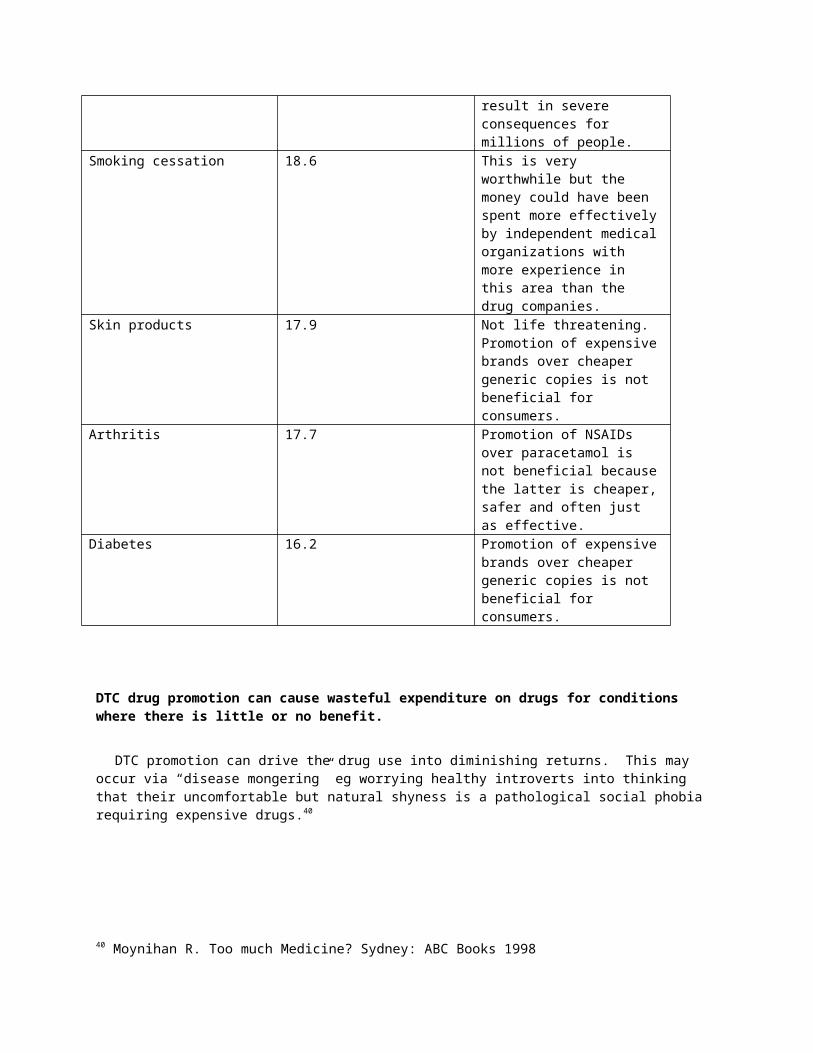
The 14 disease categories with the highest spending on DTC promotion in the US during 1997 according to Time Inc38 are presented in table 2 to indicate with comments about how well those advertisements meet real health care priorities.
Table 2.
Category Ad spend in 1997 US $ millions Comments
36 Freeman L. Aggressive strategy helps propel Claritin to top slot. Advertising age 1998; 16 March:69:11:S6-737 Parker, Betty J. and Delene, Linda M. Direct-to-consumer prescription drug advertising: content analyis and public policy implications. Journal of Pharmaceutical Marketing & Management. 1998; 12(4):27-4238 US DTC TV ads work, Web “useless”. Scrip 1998;16 September:2370:16-7

Allergy 139.5 Hay fever is not life threatening. Promotion leads to increased use of new expensive drugs when small doses of older drugs have much lower costs and similar benefits.
Antihypertensives 65.5 Most of the promotion was for expensive new calcium channel blockers which according to the limited evidence available are less effective than older cheaper drugs such as thiazides.39
Anticholesterol 65 Statins may be beneficial. However much better results might be obtained by spending the same amount of money on better diets and physical activity.
Antifungal 46 Not life threatening. Promotion of expensive brands over cheaper alternatives may not be beneficial for consumers.
Ulcer/reflux 42.6 Newer drugs are more effective but much more expensive when for many people the older therapies where adequate. Use of more expensive new drugs for reflux rather than cheaper ones has been a major component of the soaring increases in the cost of the PBS to the Australian taxpayer.
Asthma 41 Newer drugs are much more expensive with little or no advantage.
Migraine 33.3 Newer drugs are much more expensive with little or no advantage.
Contraceptives 27.4 Newer drugs are more expensive and less safe than the old drugs.
Antidepressants 26.5 Newer drugs are much more expensive. They do have less minor adverse effects but similar levels of severe adverse effects. The newer drugs are safer in overdose but the suicide rate is the same perhaps because the severely depressed just use a non-drug method to kill themselves.
Antibiotics 21.1 Overuse of antibiotics is leading to resistance which will result in severe consequences for millions of people.
39 Mansfield P. Delaying the complications of hypertension: Part 2 Calcium channel blockers. Healthy Scepticism NZ 1999 January: 2:1:1-4

Smoking cessation 18.6 This is very worthwhile but the money could have been spent more effectively by independent medical organizations with more experience in this area than the drug companies.
Skin products 17.9 Not life threatening. Promotion of expensive brands over cheaper generic copies is not beneficial for consumers.
Arthritis 17.7 Promotion of NSAIDs over paracetamol is not beneficial because the latter is cheaper, safer and often just as effective.
Diabetes 16.2 Promotion of expensive brands over cheaper generic copies is not beneficial for consumers.
DTC drug promotion can cause wasteful expenditure on drugs for conditions where there is little or no benefit.
DTC promotion can drive the drug use into diminishing returns. This may occur via “disease mongering” eg worrying healthy introverts into thinking that their uncomfortable but natural shyness is a pathological social phobia requiring expensive drugs.40
Adverse effects on Health
There is no evidence of benefit from DTC pharmaceutical promotion. The limited evidence available suggests that DTC pharmaceutical promotion is harmful to health.
Advertising agencies have much to gain from DTC pharmaceutical promotion. Consequently it would be in their interests to publish evidence of benefits if there are any benefits. To date it has not been possible to locate any such evidence.
“The rationale for allowing direct-to-consumer advertising of prescription drugs is that it would lead to better health outcomes for consumers. There is no data available to evaluate this outcome. Therefore, the consequences of DTCA for prescription drugs needs to be assessed against the quality of DTCA for nonprescription medicines and the quality of promotion to physicians. In both cases there are significant problems. Moreover, it is likely that DTCA will negatively affect physician prescribing. Consumers want and need more information but there is a fundamental distinction between advertising and information.”41
“Spending on DTCA in the United States is increasing rapidly from $150 million in 1992 to an expected $1.3 billion in 1998. Despite this level of expenditure, there is no literature on how DTCA affects patients’ level of knowledge about medications, physicians’ prescribing behaviour or health outcomes. It seems certain that DTCA will affect patients’ expectations of care in disease management, but without answers to the questions outlined above, the direction of that effect is unclear. This paper will approach this topic by analyzing existing quantitative literature. Two reviews have documented that many DTC ads do not give an accurate picture of the products they
40 Moynihan R. Too much Medicine? Sydney: ABC Books 199841 Lexchin J. Consequences of direct-to-consumer advertising of prescription drugs. Canadian Family Physician. 1997; 43:594-596
are promoting. Although there are arguments in favour of leaving out risk information they are far from proven. Surveys have looked at how DTCA effects consumers’ attitudes towards medication and care seeking behaviour. Consumers feel that DTCA will enhance the doctor-patient relationship but physicians believe the opposite. Many consumers respond to DTCA by calling or visiting a health professional to discuss either medications or health problems. A sizeable minority ask for drugs by brand name. These products tend to be newer, more expensive ones where safety information may be incomplete because they are early in their life cycles. Not only are consumers asking for such medications but in a substantial number of cases they are receiving them. If they do not, then up to one third of patients say they would switch doctors. Responding to these requests does not necessarily lead to greater patient satisfaction and may result in inappropriate prescribing. On the whole it is likely that DTCA will have negative consequences for patients’ expectations of disease management. Patients may ask for and receive more expensive and newer products that have less well defined safety characteristics than older drugs. They may switch doctors if they do not receive the medications that they request and transfer negative feelings about denial of therapy to the disease management setting. Good communication necessary for disease management may suffer. Finally the clash between patients’ and doctors’ expectations about how DTCA will affect the doctor-patient relationship may erode patients’ confidence in their physicians and the system they are working in.”42
In October 1999, the New Zealand Advertising Standards Board found that TV advertisements for AstraZenica’s Turbuhaler were confusing to the point of being misleading. This was in response to a complaint that the advertisement contained an exaggerated claim that could lead a previously well-controlled asthmatic switching to an inadequate dose of a different medication and ending up in hospital. “AstraZeneca said its claims were appropriately qualified and the advertisement recommended people seek advice from their doctor. The Turbuhaler was a prescription-only device.”43 AstraZeneca’s defensiveness and lack of remorse may stem from lack of understanding that their advertising was misleading even after the Complaints Board process. If so, then that company does not have the understanding of the issues involved that is required to be capable of producing reliable information. An examination of DTC advertising in New Zealand might find that all are misleading.
DTC promotion is not a helpful source of information for the public.
As noted above in October 1999, the New Zealand Advertising Standards Board found that TV advertisements for AstraZenica’s Turbuhaler were confusing to the point of being misleading.
In a statement dated September 21, 1999 the Pharmaceutical Research and Manufacturers of America (PhRMA) claim that “Direct-to-consumer advertising enhances consumer knowledge about diseases and treatments.”44 The only evidence that they provide to support this claim is from surveys of consumers and doctors opinions. They do not provide any evidence of improved knowledge. Given that DTC promotion has been occurring in the USA for many years the inability of industry to produce any evidence of benefit is telling.
Consumer Reports evaluated the accuracy of information in prescription drug advertisements directed at patients in the USA and found similar results to the studies of marketing directed at physicians. The study concluded that information from marketing has little educational benefit and, in general, its quality is poor. Less that half of DTC advertisements reviewed were candid about efficacy. Consumer Reports concluded, “the rules governing prescription drug advertising should not be loosened.” and that “advertisements are not public service messages – they’re meant to move goods.”45
An article in the November 1999 edition of Scrip Magazine (the journal for drug company executives) reports on the evidence about DTC promotion in the USA as follows:
“But is this burgeoning expenditure achieving a commensurate increase in public understanding of the benefits and risks, of individual medications? The answer according to a survey carried out in April of this year by the US publication, Prevention Magazine, is that it is at best doubtful…
42 Lexchin J. Direct-to-consumer advertising: impact on patient expectations regarding disease management. Disease Management & Health Outcomes. 1999; 5:273-28343 Diaz D. Watchdog rules against inhaler ad. NZ Herald 1999;13 October44 www.phrma.org/facts/bkgrndr/advert.html45 Drug advertising: is this good medicine? Consumer Reports 1996;June:61:6:62-3

The survey showed that most consumers do not know which medical conditions advertised medicines are intended to treat.” 46
The first priority of promotion is to link the name of the product with the indication. The evidence above suggests that DTC promotion is rarely effective at that first priority. Consequently it is not likely that DTC promotion has achieved more complex and lower priority objectives such as giving the public a balanced understanding of the cost, benefits and risks of all the alternative therapies.
More evidence on this topic is presented below in the sections about the opposition of pharmacists, consumer advocates and doctors to DTC promotion.
DTC drug promotion may cause severe adverse outcomes because many patients believe they can make decisions with their doctor’s advice.
There are many ways in which DTC drug promotion may cause severe adverse outcomes. “A telephone survey of 1,500 consumers, conducted for Time Inc by Ziment Associates in March/April 1998, [in the US], found that 11% of respondents agreed completely and 21% agreed somewhat, with the statement “I believe I can choose medication without my doctors advice.” Nearly the same percentages (11% and 17%) said they would switch doctors to get the medication they desired. One physician at the meeting said he was “appalled” by these numbers.”47 Consider for example if a man who was taking Isodil decided in response to DTC promotion to try Viagra by borrowing some from a friend. He would die despite reading the warning against combining Viagra with nitrates because he did not know that Isodil is a nitrate drug.
There is little hard evidence yet that directly links DTC drug promotion in NewZealand with severe adverse outcomes because there is currently no mechanism for collection such evidence. However there has been at least one unpublished report of a death in Australia due to a patient deciding to go against his doctor’s advice because of misleading drug information. The report was presented to grand rounds at the teaching hospital in Hobart in February 1999. The man died after ceasing warfarin against his doctor’s advice after the patient obtained on the Internet true but misleading that about warfarin being a rat poison.
DTC promotion increases patient demands which can lead to inappropriate drug use.
On the basis of a survey performed by Prevention magazine in the USA in May 1998 it has been estimated that direct-to-consumer advertising prompted an estimated 21.2 million Americans to talk to their doctors about a medical condition or illness they had never discussed with a physician before.48 For many of those people the reason for not mentioning it was that it was not severe enough or they were coping with their symptoms perhaps by not focusing on them. Focusing on physical sensations increases the perception and thus the severity.
Market Research commissioned by Roche as part of the promotion of Xenical in New Zealand in 1998 found that 35% of a random sample of GPs had been faced with patients demanding the drug. Of those 30% had reported difficulty with coping with those demanding patients. Separate from that study one Northland GP was so angry about the DTC promotion of Xenical that he called for all doctors to boycott the manufacturer.49
It is part of the psychological make up of many doctors to feel under pressure to “do something” for every patient that consults them. Many doctors report that pressure from patients is an important and sometimes adverse influence on their prescribing. There is evidence that patients deny putting pressure on their doctors to over-prescribe drugs. However it is likely and understandable that most people when ill have strong desires for simple solutions. These desires may be felt and expressed to doctors subconsciously so doctors may be influenced by pressure coming from the patient without the patient being aware that they are put their doctor under that pressure.
46 Charlish P. DTC advertising encourages consumers to talk about drugs. Scrip Magazine 1999;November:9-1047 US DTC TV ads work, Web “useless”. Scrip 1998;16 September:2370:16-748 http://www.phrma.org/facts/bkgrndr/advert.html49 GP boycotts Roche drugs. New Zealand Doctor 1998;8 July

Consequently it is not surprising that when patients are asked they may deny the desire for drug therapy or deny that they put their doctor under pressure.
Increased participation in prescribing decisions by well informed patients who express their preferences is likely to improve outcomes. One of the biggest threats to this is Direct to the Consumer promotion because it can distort patient preferences.
Hollon summarised the available evidence as follows: “Schwatz et al identified physicians who prescribed 3 drugs “at a rate far greater that that warranted by scientific evidence of their effectiveness.” In this study, patient demand was the most commonly cited motivation for prescribing the target drugs. In a study of antibiotic use for upper respiratory tract infections, Hamm et al documented that the patient’s expectation for an antibiotic is an important factor in the decision to prescribe the drug. Moreover, 2 recent studies concur with previous finding s that patients who expect a prescription are “many times more likely to receive one.”50
As noted above: “All the evidence suggests that in a free market, what the patient asks for, the doctor will prescribe. As a Consumer Association survey published a few weeks ago shows, even in the impoverished UK National Health Service, patient demand holds sway when it comes to prescribing. According to the Association hundreds of millions of pounds worth of pharmaceutical are being prescribed because patients demand them. Of particular concern is the fact that in many cases the prescription was inappropriate, notably where antibiotics were prescribed in viral conditions. But even in these cases, although prescribing was irrational, the doctors still gave in to patient demand.”51
DTC drug promotion leads to increased use of new drugs which are less well tested because they are new and consequently may be more dangerous.
DTC promotion is only used for expensive new drugs under patent protection. Such drugs are less well tested and may turn out to be more dangerous because what ever adverse effects they have are not know and thus to allowed for. An important recent example in Australia is Posicor which lasted on the Australian market for only one week before being withdrawn worldwide because of safety problems. Switching patients onto and then off Posicor was associated with some deaths.
DTC promotion may involve loss of patient confidentiality.
DTC promotion may involve data collection by big brothers who are less accountable than government.
In the US: “To support their marketing programs, drug companies are soliciting patient lists from physicians and pharmacists. They also compile huge mailing lists through package inserts, mailings, and magazine and television ads that offer information about medications to people who call or write. At least one major mailing-list broker is gathering the names of the ill and Metromail has a 15 million-name list of patients that it markets to the pharmaceutical industry.”52
The argument that “the battle against DTC drug promotion is lost already because of the Internet” is false.
Some argue that because it is difficult to regulate the Internet there is no additional harm done by deregulation of DTC drug promotion via other media. This argument is demolished by the evidence regarding the ratio of exposure to the Web vs TV or print. For example of a series of surveys of allergy sufferers in the US found that 45-60% became aware of the drug Allegra (fexofenadine) from advertisements. Of those 80-90% saw an advertisement on
50 Hollon MF. Direct to consumer marketing of prescription drugs: creating consumer demand. JAMA 1999;281:4:382-451 Brown P. Will DTC advertising shape the future of the industry? Scrip Magazine 1998; September: 3-4 52 What drug companies know. Consumer Reports October 1994: 631

TV and 10-20% saw an advertisement in a magazine. Only 0.2% of allergy sufferers visited the Allegra Web site despite the fact that the site was promoted in the TV and magazine advertisements.53
The number of people in New Zealand who are currently exposed to DTC drug promotion on the Internet is tiny compared to the number who would be exposed if DTC drug promotion were allowed on other media. Also frequent Internet users are mostly better-educated and more wealthy than frequent TV viewers so the former are less vulnerable than the latter.
Key interest groups do not support DTCA
Many drug companies are not keen on DTC drug promotion.
In March 1999 senior medical journalist Melissa Sweet reported that regarding DTC prescription drug promotion in Australia: “For once, there’s little disagreement among the health sector’s diverse interest groups. The APMA [Australian Pharmaceutical Manufacturers Association] isn’t keen (but would like greater opportunity for “highlighting specific disease states” to the public), and nor are consumers or medical groups.”54
Given that Australia and New Zealand are similar in many ways and that the operations in New Zealand of many drug companies are controlled from Australia it is reasonable to conclude that many drug companies are not keen on DTC drug promotion.
Bayer (New Zealand) general manager, Anthony Nagle has been reported as saying that he has no plans to go direct to the consumer in the short to medium term. and doesn’t think Kiwis will see a flood of it. “companies could lose because of putting the doctor in a compromising position and if they confuse the patient” Mr Nagle reportedly said.55
Disease foundations and patients groups oppose DTC promotion because it can overwhelm their agenda
Media work for World Asthma Day in New Zealand in December 1998 by The Asthma and Respiratory Foundation of New Zealand was overwhelmed by promotion of Singulair by press release at the same time.56
Pharmacists oppose DTC drug promotion because they do not provide useful information
“Proponents and opponents of direct-to-consumer (DTC) advertising enjoyed an opportunity to vent and persuade during a debate at the Academy of Managed Care Pharmacy (AMCP) annual meeting this past spring in Minneapolis. Speaking first and in opposition to DTC advertising was Kjel Johnson, vice president of pharmacy services, University of Pittsburgh Medical Center Health Plan (Pittsburgh). Praising, or at least apologizing for, DTC was Steve Barrett, vice president of Klemtner Advertising, New York City.
Johnson commenced his jeremiad with an argumentum ad hominem -- ie, a video clip of Bob Dole's Viagra commercial. "What are we supposed to be learning here?" Johnson asked, perhaps not rhetorically. "That there's an inverse correlation between erectile dysfunction and political success?" In spite of contentions to the contrary, Johnson asserted that DTC advertising is utterly devoid of science and utterly useless as a patient learning tool. "Proponents of DTC argue that disease-specific patient information does not work and therefore information needs to be product-specific," he said. "The first part of that statement is true. But guess what? Product-specific information doesn't work either... at least as a learning tool."
Johnson cited a recent study of 300 patients divided into three groups: one group saw no ads, one group saw disease-specific ads, and the last saw product-specific ads. Disease-specific questions were then asked of each of the groups. "Results showed no difference in knowledge," Johnson said. "The group that saw no ads knew just as much,
53 US DTC TV ads work, Web “useless”. Scrip 1998;16 September:2370:16-754 Sweet M. Getting to the consumer direct. Aust Doc Weekly 1999; 5 March:2955 MacKinven M. Pill purveyors go direct. New Zealand Doctor 1999;17 March56 Thomson S. Personal communication. 1999; 8 Novemeber
or as little, as the groups seeing the two types of ads. And as for the group seeing the product-specific ads, well, they recalled the ads, but they neither retained, nor did they seem to glean, any useful information."
DTC advertising, while of questionable utility as patient education, is also neither liked nor trusted by significant numbers of consumers, Johnson contended. "Here's a study by AgeWaves," he said. "A survey of 1,000 consumers read ads for the 18 top-selling DTC-advertised drugs. The finding was consumers were twice as likely to dislike an ad for medicines as to like it. The consumers were then asked why, in their opinion, drug makers were advertising: to help educate patients or to increase profits? Overwhelmingly, patients said DTC was about driving profits. "What's the Problem? If many consumers don't like the ads and distrust their motivation, what's all the fuss about whether or not they should exist? The problem, Johnson explained, is that consumers in sufficient numbers are being beguiled enough by the ads to go to their physicians and ask for the drug. That same AgeWaves survey found that 35% of consumers who saw a DTC ad told their docs they wanted the drug featured. And 33% of that 35% got it.
"Here's one DTC factoid that's empirically verifiable: drug makers are spending hundreds of millions of dollars on DTC ads and are reaping billions of dollars in sales," said Johnson. "But," he added, "there's no evidence the ads are making patients smarter or healthier."
Speaking for the defence, advertising executive Steve Barrett pleaded with managed care to "stop attacking the intelligence of the American consumer; P. T. Barnum was wrong. Consumers are not the unwitting dupes of pharma industry ad campaigns."
In fact, Barrett opined, the real concern among manufacturers and their ad agencies is whether DTC is working at all. "A huge study by market researchers Market Measures found that after seeing an ad, only 13% of the target audience asked for the drug, and only 4% got it," Barrett asserted. "DTC working like gangbusters? We're wondering if it's working at all."
But while they wonder, drug manufacturers will, without a doubt, continue to advertise. Wyeth-Ayerst will spend $5 million on a big Enbrel campaign (aimed at women with rheumatoid arthritis). Look for ads in Time, Women's Day, Parade, and other consumer slicks. Xenical, Roche's new anti-obesity drug, is also destined to have a huge consumer presence. Barrett summed up his defense of DTC ads by posing the following paradox to the AMCP audience. "You expect patients with serious conditions like asthma and hypertension to manage themselves post-Rx," Barrett observed. "But you would deny those patients any decision-making authority or information pre-Rx. And what about managed care's own marketing and advertising? Isn't that direct-to-consumer? Doesn't that also appeal to emotions? Perhaps your ads are also bad for the consumer."”57
Consumer advocates oppose DTC drug promotion because it decreases consumers’ abilities to make good choices.
In 1996 Public Citizen the US consumer advocate organisation founded by Ralph Nader responded to a request for comments on direct-to-consumer (DTC) prescription drug promotion as follows:
“August 12, 1996
Dockets Management Branch (HFA-305)Food and Drug Administration12420 Parklawn Dr., Rm.. 1-23Rockville, MD 20857
RE: Direct-To-Consumer Promotion (Docket No. 95N-0227)Public Citizen's Health Research Group, representing consumers nationwide, submits the following statement in response to the Food and Drug Administration's (FDA) request for comments on direct-to-consumer (DTC) prescription drug promotion dated May 14, 1996. The FDA has the legal responsibility for regulating the labeling and advertising of prescription drugs and the obligation to ensure that consumers are adequately safeguarded from false or misleading drug promotion. Under the Federal Food, Drug, and Cosmetic Act an advertisement for a prescription drug must contain, in addition to the
57 McCarthy R. DTC Advertising: The Big Face-Off. Drug Benefit Trends 1999;11:7:26

product's established name and quantitative composition, "such other information in brief summary relating to side effects, contraindications, and effectiveness . . .".(1) Drug advertising provisions in the Federal Food, Drug and Cosmetic Act do not differentiate between advertising intended for trained medical professionals and the general public, containing no specific language that is directed at DTC promotion. As a consequence there may be differences between prescribers and prescription drug consumers in perceptions, comprehension and interpretation of promotional claims. Any misunderstanding and misinterpretation of claims made about powerful drugs is potentially dangerous. If the purpose of DTC prescription drug advertising is to educate and inform the public about drugs, it would not be unreasonable to assume that complete and accurate information would best accomplish this goal. Then a key question is whether current DTC advertising of prescription drugs can be expected to result in consumers receiving more appropriate treatment of their health problems, or conversely, leads to choices of less appropriate, perhaps more dangerous, or needlessly more expensive therapy. If the latter situation is found to be true, the FDA must act immediately to halt DTC advertising of prescription drugs until regulations specific to this form of promotion are finalized that will ensure the public safety. To address these issues our initial comments will focus on the following: - The use of DTC advertising - The purpose of DTC advertising - Accuracy of prescription drug advertising to consumers and doctors - The effect of prescription drug advertising on consumers and doctor - Nabumetone (Relafen) as an example of DTC advertising - Evidence that DTC promotion leads to better health outcomes Our final comments will directly address the following questions asked by the FDA in their May 14, 1996 request for comments: - Are there differences in the information needs of professionals and consumers? - What information should be included in DTC prescription drug advertising? - Should the FDA permit different disclosures for different media? The Use of DTC Prescription Drug Promotion by Pharmaceutical Manufacturers Evidence from surveys of total advertising expenditure and the number of products advertised shows that DTC prescription drug advertising is increasing. In 1988, $25 million was spent on DTC advertising. By 1994, this figure had increased 10 fold to between $225 and $250 million. DTC expenditures increased by 65 percent in 1994 alone.(2) In 1992, 17 prescription drug products were advertised in consumer media, in 1995 the number increased to 50. More than 60 percent of the ads appear in magazines, including the news magazines, women's magazines, People and Reader's Digest most notably. Another 15 percent are in newspaper Sunday magazines and about 15 percent on television.(3) The Purpose of DTC Prescription Drug Advertising One of the primary purposes of consumer product advertising is to generate brand-name awareness in the minds of the public. The clear goal of advertising is to generate product demand and increase sales. One action that consumers can take as a result of effective advertising is purchasing the product which is the most desirable to marketers. However, prescription drugs are not like consumer products and consumers have had a relative lack of authority in the decision process. Drugs that are only available by prescription are selected by physicians, managed care organizations and hospital formulary committees and are purchased only through a pharmacist in a licensed pharmacy.(4) If prescription drug consumers have a relative lack of authority in choosing a drug product why then should drug companies invest in DTC drug advertising? One of the most compelling explanations is the increasing ability of consumers to influence physicians prescribing decisions. In a 1995 survey, 99 percent of 4,000 physicians said they would consider prescribing, or would prescribe a drug suggested by a consumer, compared to 84 percent in 1989.2 (see exhibit 1) DTC advertising as a marketing strategy may in part be due to an attempt to challenge the efforts of managed care corporations to hold costs by limiting the drugs doctors can choose. An advertising agency executive has been quoted as saying; "Pharmaceutical companies are realizing that the patient is a major force in determining which prescriptions get written."(5) The singular purpose of DTC drug advertising is summed up in a quote from a recent issue of Medical Marketing & Media, a medical advertising industry trade publication:

In the old marketing model, pharmaceutical companies created patient demand by influencing doctors to write prescriptions. In DTC promotion, companies listen to the patient, respond to their needs, and hope to increase sales by driving consumers to a doctor's office and requesting their product.2 The Accuracy of Prescription Drug Advertising To Consumers The chief legal councel for the Washington Legal Foundation, an organization frequently supporting the view of drug companies, has been quoted as saying: "...the FDA has chosen to erect needless barriers to advertising that hinder health care...." and implies that consumer advertising plays an important role in health care by making medical information readily available. An executive of a major pharmaceutical manufacturer has stated: "A properly educated, properly motivated patient-partner is the best bet the physician has for getting a good outcome for the patient overall...."3 Proponents of DTC promotion imply it serves a vital public health role by improving health outcomes through education of the public about drugs. If the primary purpose of DTC is improving health outcomes through consumer education then there is the reasonable assumption that more complete and accurate information in DTC ads would lead to even better health outcomes. Consumer Reports reviewed the accuracy of 28 DTC prescription drug ads that appeared recently in U.S. magazines. The accuracy of the ads was assessed by a panel of 32 medical specialists who evaluated ads in their own areas of medical specialty.5 The findings of the study are as follows: - Two-thirds of the ads were judged to be factually accurate and backed by scientific evidence. But many left out important information or it was only in the fine print. - Only half were judged to convey important information on adverse effects in the main promotional text. - Approximately 40 percent were judged honest about efficacy and fairly described the benefits and risks in the main promotional text. According to one reviewer participating in this study 39 percent of the ads were "more harmful than helpful". Effect of DTC Advertising on Consumers The goal of DTC advertising to build awareness and market share appears to be working. The chief executive officer of Scott-Levin Associates, a pharmaceutical market research and consulting firm has been quoted as saying: "Our 1995 survey of DTC ads show that they are having the impact sponsors [drug companies] hoped for. Patients are asking doctors about advertised drugs more often, and they are more likely to get the product they ask for."2
NPD Group, a market research company, surveyed 175,000 consumer households and found that 25 percent of consumers said they changed the way they took care of their medical problems after being exposed to DTC promotion. Twenty percent of consumers claimed they called or visited or were more likely to call or visit their doctors.2 The Accuracy of Prescription Drug Advertising To Doctors The pharmaceutical industry also has a dismal record of accurate advertising to physicians. A major study published in 1992 assessed both the accuracy of scientific data presented in 109 full page prescription drug advertisements appearing in 10 leading U.S. medical journals and the compliance of these advertisements with FDA standards.(6) The major findings of this study are as follows: - 38 percent of the ads potentially violated five or more FDA regulations. - 40 percent did not present a fair balance between effectiveness and adverse effects. - 47 percent of the 49 ads where such information was relevant did not highlight potential problems with the drug in special patient populations such as the elderly. In 44 percent of ads, reviewers felt that the advertisement would lead to improper prescribing if a physician had no other information about the drug other than that contained in the advertisement. Effect of Prescription Drug Advertising on Doctors Research has shown that scientifically unsupported information used in drug advertising had greater influence on physician's prescribing decisions than the scientific literature.(7) Physicians were surveyed as to what sources of information they used to make drug therapy decisions, academic or commercial. Academic sources were defined as the scientific medical literature such as journal articles. Commercial sources were defined as visits from drug company representatives and journal advertising. The source of prescribing information used by the physicians was determined indirectly by asking their beliefs about a drug where information about the drug given in commercial sources from drug companies was opposite to information found in academic sources. For example, a physician may respond that she or he bases prescribing on

the scientific literature alone and never reads drug company advertisements or pays attention to representatives. However, answers in another part of the survey may reveal that the physician believes cerebral vasodilators are effective in the treatment of senile dementia. Such information is highly unlikely to have come from the scientific literature since it does not demonstrate efficacy of cerebral vasodilators in the treatment of senile dementia. An important observation made by the authors of this study, in addition to their conclusion, was that initial advertising of a new drug is accompanied by extensive promotion of its virtues either real or manufactured. However, if with continued experience the benefits are found to be lower and the risks higher for a given drug, this information is reported in the academic literature or in the small print in the prescribing information sections of the advertisements, neither of which places for such information apparently strongly influence physicians' knowledge about drugs. Nabumetone (Relafen) the Remarkable Success of an Unremarkable Drug Nabumetone (Relafen), a nonsteroidal anti-inflammatory drug (NSAID), was approved by the FDA for the treatment of rheumatoid arthritis and osteoarthritis in 1992. The manufacturer claimed that nabumetone is as effective as other NSAIDs (ibuprofen or Motrin and naproxen or Naprosyn are two examples) and causes a relatively low incidence of ulcers.(8) The following two statements come directly from the CLINICAL TRIALS section of the FDA approved labeling (package insert) for nabumetone(9) : Osteoarthritis: The use of Relafen in relieving the signs and symptoms of osteoarthritis was assessed in double-blind controlled trials in which 1,047 patients were treated for 6 weeks to 6 months. In these trials, Relafen in a dose of 1,000 mg/day administered at night was comparable to naproxen [Naprosyn] 500 mg/day and to aspirin 3,600 mg/day. Rheumatoid Arthritis: The use of Relafen in relieving the signs and symptoms of rheumatoid arthritis was assessed in double-blind, randomized, controlled trials in which 770 patients were treated for 3 weeks to 6 months. Relafen, in a dose of 1,000 mg/day administered at night was comparable to naproxen 500 mg/day and to aspirin 3,600 mg/day. The most serious adverse effects associated with the use of NSAIDs are hemorrhage or perforation of the gastrointestinal tract. By 1994 clear evidence was emerging of differences in the risk of gastrointestinal toxicity with different NSAIDs. Ibuprofen (Motrin and many generics) clearly was showing the least risk and naproxen, the drug mentioned in the nabumetone package insert, was showing an intermediate risk of severe gastrointestinal toxicity.(10)
The risk of gastrointestinal hemorrhage or perforation with nabumetone in relation to these other two NSAIDs remains unknown. The difference in average wholesale costs for nabumetone and naproxen in 1995, in doses shown to be equally effective, was over seven fold. Using the 1995 Drug Topics Red Book, a standard price guide, the wholesale cost to the pharmacist for enough nabumetone to last 30 days at a dose of 1,000 milligrams per day, its minimum recommended dose, was $58.68. By comparison the cost to the pharmacist for enough generic naproxen to last a month at its minimum recommended dose of 500 milligrams per day was $8.08. The wholesale cost of a month's supply of generic ibuprofen at a usual starting dose of 1,200 milligrams per day was $8.64. SmithKline Beecham sales of nabumetone during the second quarter of 1994 were boosted by a DTC advertising campaign and were increased by 52 percent.(11) Nabumetone moved from the 48th most frequently prescribed drug in the U.S. in 1994 to number 44 with more than 7 million prescriptions dispensed in 1995.(12) SmithKline Beecham spent $11 million on DTC advertising for nabumetone in 1995.3 It is difficult to imagine a set of circumstances in which a prescription drug consumer given accurate complete comparative information would accept the unknown risk of toxicity and the higher cost of nabumetone as a treatment over ibuprofen or naproxen. Evidence that DTC Promotion Leads to Better Health Outcomes We are aware of no valid scientific evidence that suggests DTC prescription drug advertising leads to better health outcomes for the public. On the contrary, based on the prevailing evidence presented above unregulated DTC advertising as currently allowed may induce needless economic hardship and perhaps physical harm to consumers.
* * * Our remaining remarks directly address the questions asked by the FDA in their May 14, 1996 request for comments.
ANSWERS TO SPECIFIC FDA QUESTIONS Are There Differences in the Information Needs of Professionals and Consumers?

Consumers have become an integral part of their own prescription drug selection process, as they should be, and have the same need for objective accurate and complete drug information as health professionals. However, by virtue of their training skillful health professionals know how to find and interpret the complex medical literature to make rational comparative decisions between drugs and non-drug treatments. Comparative information is absolutely essential for consumers to make informed decisions about drugs, however barriers to finding and interpreting comparative drug information are almost insurmountable to the average consumer. In order that DTC advertisements are not misinterpreted and lead to drug treatment choices that are needlessly expensive or potentially harmful, it is paramount that consumers be presented with comparative information in all DTC advertising. What Information Should Be Included in DTC Prescription Drug Advertising? Given that consumers and health professionals have the same need for objective drug information, the existing Federal Food, Drug and Cosmetic Act must be redesigned to apply to DTC advertising and be enforced. In addition, DTC ads, depending on the therapeutic class of drug being advertised, should contain comparative information for all drugs with the same approved indication(s) and information about non-drug treatments. Should the FDA Permit Different Disclosures for Different Media? Any but the most stringent regulation of DTC prescription drug advertising risks misleading the public and it would be illogical and dangerous to permit different levels of disclosure for different media. Conclusions Evidence shows that physicians are influenced by advertising; that consumers are persuaded by DTC ads to sway physicians' prescribing decisions; and that drug advertising both to health professionals and directly to consumers is frequently misleading. This is a formula for potential harm, both physical and economic, to consumers. Advertising of prescription drugs whether directly to health professionals or to consumers serves no purpose other than to sell products. Promotion of prescription drugs directly to the public, as is done with consumer goods, requires that every DTC ad gives full and complete disclosure of a drug's risks regardless of the advertising media in which the ad appears. In the absence of valid evidence showing that present DTC prescription drug ads promote the appropriate selection or the safe and effective use of prescription drugs or improves health outcomes, we are opposed to any but the most stringent regulations and their enforcement to ensure the public's safety. Because of obvious differences in training and background between consumers and health professionals, consumers are much more vulnerable to the influences of misleading drug advertising. Given the evidence presented in these comments, it is critical that DTC prescription drug advertising be stopped until consumer protective regulations can be proposed and finalized. The only reliable way to ensure that consumers will not be misled is to require that all DTC advertising be approved by the FDA prior to its distribution. Drug manufacturers who are truly committed to educating consumers about drugs will not object to full and complete comparative disclosure of adverse effects, contraindications and effectiveness of their products with respect to those of their competitors or to prior approval of their advertising by the FDA. Sincerely, Larry D. Sasich, Pharm.D., FASHP Research Analyst Public Citizen's Health Research Group Sidney M. Wolfe, M.D. Director Public Citizen's Health Research Group References 1. Code of Federal Regulation. Title 21: Food and Drugs. Part 202, Prescription Drug Advertising. Washington, DC: US Government Printing Office; 1996. 2. Hodnett J. Targeting consumers. Medical Marketing & Media November 1995:91-95. 3. Conlan MF. In-your-face pharmacy. Drug Topics July 8, 1996:92-98. 4. Basara LR. Practical considerations when evaluating direct-to-consumer advertising as a marketing strategy for prescription medications. Drug Information Journal 1994; 28:461-470. 5. Drug advertising--Is this good medicine? Consumer Reports June 1996:62-63. 6. Wilkes MS, Doblin BH, Shapiro MF. Pharmaceutical advertisements in leading medical journals: experts' assessments. Annals of Internal Medicine 1992; 116:912-919.

7. Avorn J, Chen M, Hartley R. Scientific versus commercial sources of influence on the prescribing behavior of physicians. American Journal of Medicine 1982; 73:4-8. 8. Nabumetone--a new NSAID. The Medical Letter on Drugs and Therapeutics 1992; 34: 37-40. 9. Nabumetone (Relafen) Product Information. Physicians' Desk Reference Montvale, NJ: Medical Economics, 1996. 10. Bateman DN. NSAIDs: time to re-evaluate gut toxicity. Lancet 1994; 343:1051-1052. 11. SCRIP August 16, 1994; 1949:12. 12. The top 200 drugs 1995. American Druggist February 1996:18-26.”58
Mansfield (1999)of MaLAM wrote that “DTC promotion uses sophisticated methods to get patients to jump to a decision to demand a specific drug with out hearing the other side of the story…Consumers’ organisations are very keen on increased access to information. However they oppose DTC promotion. They understand that it harms their constituents because it is so difficult to distinguish the “needle” of reliable information that they need from the “haystack” of unreliable promotion. Consumers do not need the “haystack” to be made any larger.”59
A report published in 1992 by the US Consumers Association found that: “Drug companies want consumers’ attention and they are stepping up their efforts to get it, focusing on a new audience: the drug buying public. They know that while the doctor writes the prescription, the patient often guides the pen. Nearly one third of prescriptions for new products are now written at the request of the patient. Beyond creating public demand, mass media is also a direct route to physicians as doctors often get their medical news from newspapers first. Sometimes journalists are willing accomplishes of the drug industry, but more often they’re skillfully misled by doctors who are paid company employees being passed off as independent experts and by press conferences and press releases. Companies hire celebrities to sell their drugs without telling the public that the celebrities are being paid. Public relations firms are hired to put positive spins on stories in the medical literature. Many reporters cover medical stories part-time and can be misled by drug company propaganda. Companies will try and hide their involvement in promotion by working through seemingly independent third parties such as patient organizations. If an appropriate third party isn’t available for partnership, sometimes drug companies invent one.”60
A study by Consumers International of advertising in 11 industrialized countries provides additional evidence that stronger measures are needed to deal with advertising of over-the-counter products.61
Medawar (1999)of Social Audit raises many questions about the ill effects of DTCA: “Once DTC advertising gets a real hold, the danger is that it will become increasingly difficult ever to feel well again. What will happen when such ads become part of the normal diet? How will people come to feel about each other and themselves when the air becomes thick with warnings about possible hidden illness, and easy promises of restoration of health? Always there is the nagging suggestion that people are less and less able to cope themselves - that they can and should turn to drugs and medicine for help. Won't our children and grandchildren find it sickening to be mobbed by thoughts of hidden illness and smothered with images of the ostentatiously well?
To this extent, the ill-effects of DTC advertising are not really to do with the wording of individual examples of ads: increased dependence on medicine(s) would follow, even if advertisers complied scrupulously with strong codes. However, as DTC advertising develops, inevitably brand names will become more prominent, and initial high standard will fall…
This is indeed a complex subject because what happens now raises huge questions about public and personal health - and yet the battle already feels lost and very nearly over. In theory, DTC advertising could be kept at bay through resistance from the medical establishment and patient organisations. In practice, there are too many strong vested interests and just too much industry money and covert influence sloshing around. No stopping it when there is no strong and independent leadership, no political mileage in censorship, no political sense in trying to deprive the
58 www.citizen.org/hrg/PUBLICATIONS/1400.htm59 Mansfield P. No. Aust Doc Weekly 1999; 8 October:6460 Miracle drugs or media drugs? Consumer Reports 1992 Mar: 142-14661 Chetley, Andrew. OTC advertising: in whose interest? A consumer’s viewpoint. WHO Drug Information. 1995; 9(1):10-11.

media of vast advertising revenues, and no realistic prospect of tight enforcement. The existence of the Internet (overwhelmingly US output) means in effect that DTC adverting already exists, that enforcement would not get far.
Still, if you can't stop it, you can at least recognise it for what it is and what it means. And if you don't like the idea, you can then oppose and try to stall it and think about ways of minimising its harmful effects. This seems a worthwhile exercise, for there has been precious little hard and impartial analysis of the deeper impact of DTC advertising - though this is surely a defining moment, a watershed in the development of medicine, community and health?
What does it all mean? The only certain answer is that we've almost left it too late, but have barely begun to understand the consequences. These are some of the questions that belong in the debate there needs to be:
1. To what extent does ill-health result from fear of ill-health, loss of confidence and personal autonomy - and to what extent is it created by suggestion and contagion? Lewis Thomas wrote wisely about the dangers of this long before DTC advertising had begun to make it mark:
"If people are educated to believe they are fundamentally fragile, always on the verge of mortal disease, perpetually in need of health-care professionals at every side, always dependent on an imagined discipline of ‘preventive’ medicine, there can be no limit to the numbers of doctors’ offices, clinics, and hospitals required to meet the demand ... We are, in real life, a reasonably healthy people. Far from being ineptly put together, we are amazingly tough, durable organisms, full of health, ready for most contingencies. The new danger to our well-being, if we continue to listen to all the talk, is in becoming a nation of healthy hypochondriacs, living gingerly, worrying ourselves half to death" (L. Thomas, "The Health Care System" in The Medusa and the Snail, New York, Bantam Books, 1980, 39-40)
2. To what extent does a powerfully market-driven system create unsustainable demand and promote division and inequality of access to health? The nub of the fallacy is that "health for me" is barely attainable without "health for all"? My health is intimately to do the health of my community: real madness is to be the only kid on the block not on Prozac or Ritalin. When the flood of marketing translates into whole communities crying more "health for me", there will always be less for you and me - and no healthcare system could possibly meet the demand. It's a paradoxical effect, not unrelated to the notion of a mass market packed with unique beings and rugged individuals.
3. Why should this model of medicine, deemed suitable in the USA, be a good thing for the rest of the world? The question arises because of the high cost of US medicine - with stark lack of evidence of commensurate health gains - and because of the wholesale exclusion from adequate healthcare of a large proportion of the population. To what extent is it appropriate that America's values and priorities dictate trends for the rest of the world?
4. By nature, partial, superficial, repetitive and impersonal - is advertising really a useful source of information, compared with other methods of learning? How much useful and misleading information has it given doctors? Does it not tend to debase and overwhelm good science and promote partial understanding on fundamental issues - e.g. on the relationship between benefit and risk?
5. To what extent will DTC advertising act as a substantial barrier to entry to products of comparable therapeutic value, and lead to higher prices and reduced access to essential drugs? Philip Brown (publisher of the industry newsletter, SCRIP) has a strong handle on this:
"What brought home to me the significance of direct-to-consumer promotion was a comment last week from a senior industry executive who believes that it could become a major factor in shaping the future of the industry. He argued that the success or failure of a new R&D-based prescription product in the US now depends on the size of the direct-to-consumer advertising budget.
"What chance, he asked, does Company A have with, for example, a US$50 million budget for direct-to-consumer advertising for its new prescription medicine, if the far bigger competitor, Company B, decides to spend US$600 million? The short answer is very little …" (P. Brown, Will DTC advertising shape the future of the industry? SCRIP Magazine, September 1998, 3)
6. To what extent will DTC advertising corrupt or improve the relationship between doctors and patients, and the quality of treatment and prescribing practice? Philip Brown, again:
"So are we facing a whole new scenario where the market will become dominated by the big direct-to-consumer advertisers - and that means the big companies - and where customer choice, stimulated by advertising, will

determine a prescription product's success? Providing the prescribing doctor acquiesces to the demands of the patient, the answer must be yes.
All the evidence suggests that in a free market, what the patient asks for, the doctor will prescribe" … Of particular concern is … that in many cases the prescription (is) inappropriate, notably where antibiotics were prescribed in viral conditions. But even in these cases, although the prescribing was irrational, the doctors still gave in to patient demand." (Ibid.)
7. What is the dominance of the pharmaceutical industry doing to the leadership of medicine, and to the critical faculties of the press and media? What is happening to the progress and direction of health?
Virtually all of my instincts lead me to think of DTC advertising as a profoundly unhealthy development. I fear its overall effect will be paradoxical: it will promote the very opposite of what health is, and was surely meant to be.”62
Mintzes (1998) of Health Action International produced a major report on DTC promotion and related issues. Key sections of that report include:
“A prerequisite for any improvement in treatment and health outcomes is accurate information. In order to predict potential accuracy -- since DTC ads are not allowed in Canada -- he looked first at non-prescription drug advertising to consumers, then at prescription drug advertising to doctors. A 1993 survey of 15 Canadian magazines found that 24% of advertisements for OTC drugs contained "minor errors" such as stating that there were no side effects or exaggerating a product's merits; 39% had major violations such as unapproved claims or misrepresentations. Advertising aimed at doctors was no more accurate, a 1991 survey of 111 ads in 14 Canadian journals found that risks were mentioned only 53% of the time, and that this was almost always in the context of a statement about lack of side effects. In contrast, benefits were discussed in 91% of the ads.
In other words, the information on risks and benefits was skewed towards a misleadingly positive representation of the product and a lack of attention to warning both health professionals and consumers about potential risks. A similar bias was found in a 1995 US Consumer Reports evaluation of 28 DTC advertisements for prescription drugs. The advertisements were submitted to a panel of 32 medical specialists who evaluated ads for products related to their specialty. The reviewers found that one-third contained factual inaccuracies or assertions that were not scientifically supported; only half conveyed important information on side effects in the main promotional text; fewer than half presented the drug's effectiveness, potential benefits and risks fairly; and 11 ads -- nearly 40%-- were considered more harmful than helpful by at least one reviewer.
The Consumer Reports review also highlighted several themes in the advertisements which contribute little to rational use:
implied 100% effectiveness (four anti-allergy products);
failure to mention age groups in which the product is more or less effective (minoxidil, Rogaine)
an appeal to maternal guilt (DDAVP nasal spray for bedwetting);
romantic scenes used to sell the drug (an anti-psoriasis drug and menopausal hormones).
Studies in Belgium, The Netherands, the UK and the US over more than 20 years have shown that doctors who rely heavily on commercial sources of information are less likely to prescribe appropriately, as judged by whether they use medicines in the correct dose and for the appropriate duration, their restricted use of drugs with serious side effects, use of non-drug treatments when they are most appropriate, better knowledge of drug therapy, and using the least costly of equivalent alternatives.
If reliance on promotion is associated with negative effects on prescribing, what of consumer demand?
Does DTC promotion create a demand from consumers which results in pressure on doctors to prescribe? After all, consumers need to convince their doctors to prescribe a drug they see advertised. A US marketing firm, Scott-Levin Associates compared results of surveys in 1987 and 1992, a period of rapid growth of DTC promotion in the US. They found that 18% of patients asked their doctors about specific drugs in 1987, as compared to 54% in 1992. According to a 1989 survey of 3,6oo US doctors, over half of patients mention advertised drugs. Eighty-four percent
62 Medawar C. DIRECT TO CONSUMER ADVERTISING. 1999 October

of the doctors said they would consider prescribing a drug if a patient requested it and 16%said they were very likely to prescribe the drug…
Should DTC promotion be allowed?
Consumers need better access to independent information in order to make informed choices about both drug and non-drug treatments. Funding for this is scarce and in many countries consumers have little access to the information they need to truly participate in treatment decisions. Industry groups are arguing that DTC promotion provides much needed information to consumers. These arguments obscure the fundamental difference between promotion, which aims to sell a product, and the type of information needed to choose how best to treat a health problem. Given the industry's track record on drug promotion to health professionals, and its DTC track record in the US, there is no reason to believe that DTC drug promotion will lead to any improvement in prescribing or use of medicines. On the contrary, existing evidence points to a likely rational prescribing and use.
RECOMMENDATIONS
Direct-to-consumer promotion of prescription drugs
1. Direct-to-consumer advertisements of prescription-only drugs should not be allowed, given the lack of evidence of health benefits and the serious potential for harm.
2. Legislation controlling promotion should apply equally to promotional activities disguised as education about drugs or diseases, including prohibition of direct-to-consumer prescription drug promotion where this applies. This will require clear definitions of promotional versus non-promotional information based on criteria. such as:
* whether a manufacturer is the direct or indirect source of the information,
* whether information on a disease is linked to recommendations for drug treatment,
* whether disease risks are presented in a manner which could be construed as inciting the public to seek drug treatment,
* whether use of specific drugs is recommended,
* whether diagnostic testing is recommended which may lead to drug treatment,
* and whether all available drug and non-drug treatment options are discussed in a fair and balanced manner.
3. Regulatory authorities may wish to consider a tax on pharmaceutical sales which could be used to set up a blind trust to fund independent drug information for both health professionals and consumers, as well as patient groups and other non-profit and charitable health organisations. Gilbert and Chetley recently recommended a similar model for the UK as a means to ensure the quality of information reaching consumers. Such a trust should be administered by an independent board with full provisions for transparency, public representation and accountability.63
Medical educators oppose DTC drug promotion because it is does not provide the information that is needed for optimal health care outcomes.
Ellen t’Hoen, Coordinator of the International Society of Independent Drug Bulletins examined the new Food and Drug Administration guidelines for television and radio direct-to-consumer advertising for prescription drugs. She questioned whether the FDA has the resources to adequately monitor DTCA. Although drug information needs to be independent, reliable, comparative and of good quality, drug advertising is none of these things. DTCA also encourages the use of new drugs that can pose safety problems since they have only been tested on a limited number of people and therefore their safety profile is less well known.64
63 Mintzes B. Blurring the boundaries: new trends in drug promotion. HAI 199864’t Hoen, Ellen. Direct-to-consumer advertising: for better profits or for better health? American Journal of Health-Systems Pharmacy. 1998; 55:594-597

Doctors oppose DTC drug promotion because it damages the doctor patient relationship and harms patients.
A IMS/New Zealand Doctor fax poll of 400 GPs with 121 respondents and a margin of error of ± 8.7% published in June 1998 found:
44% wanted DTCA to stop altogether
31% wanted a it decreased
16 wanted the levels to remain the same
7 % wanted it increased.
The poll also found that :
61% of GPs believed that DTCA creates disharmony in the doctor/patient relationship.
62% of GPs believed that there was no benefit for patients from DTCA.65
The evidence available supports the beliefs expressed by the majority of NZ doctors. A study has found that: “After viewing television advertisements patients may doubt the worth of their current medications and of their physician’s advice.”66
One Northland GP was so angry about the DTC promotion of Xenical that he called for all doctors to boycott the manufacturer.67
New Zealand GP council chair Dr Philip Rushmer is reported as telling New Zealand Doctor magazine that he believed the promotion of Singulair via the media was an inappropriate way to introduce a new drug because it put pressure on doctors. Also the “free” for a month promotion put an unnecessary strain on patients faced later with paying the full price. He was “staggered” at the report from MSD that 600 GPs (20%) prescribed Singulair within the first 2 weeks it come on the market.68 It should be noted that:
little information was available about Singulair at the time,
Singulair is less effective than adequate doses of corticosteriods
the place of Singulair in therapy has not yet been defined but is probably small.
the use of free introductory offers is a very effective promotional technique which in this case is likely to take advantage of the usual unpredictable fluctuations in the severity of asthma and the placebo effect plus the common fallacies of wishful thinking and post hoc ergo propter hoc to lead patients to believe that Singulair is much more effective than it really is.
Mansfield (1999) reported that “In New Zealand and the USA DTC promotion is allowed with little restriction. Surveys of doctors in both countries have found that the majority are opposed to DTC promotion. In February, I spoke with many GPs in New Zealand whilst on tour to launch “Healthy Scepticism” a new newsletter for GPs about misleading drug promotion. Many New Zealand GPs expressed distress about interference with the doctor patient relationship from DTC promotion. Patients who demand inappropriate drugs can be very difficult to cope with let alone help. Time is wasted which should be used making the right diagnosis before selecting the most appropriate therapy.”69
Dr. Reardon, President-Elect of the American Medical Association, presented a keynote address at the International Business Communications' Direct-to-Consumer Marketing Congress, at the Plaza Hotel, in New York City, on February 24, 1999. Dr. Reardon discussed the positive and negative aspects of direct-to-consumer advertising and offered his perspective on how this increasingly popular trend is affecting patient-physician
65 Floyd K. GPs have little faith in direct to consumer ads. New Zealand Doctor 1998;22 July:366 Kerr, Harry D. and Brobny, Elaine C. Advertising prescription drugs to the public. New England Journal of Medicine. 1986; 314:523-52467 GP boycotts Roche drugs. New Zealand Doctor 1998;8 July68 MacKinven M. Singulair popularity comes in for criticism. New Zealand Doctor 1999;20 January:369 Mansfield P. No. Aust Doc Weekly 1999; 8 October:64

relationships, ethical matters, cost accountability, and patient privacy. The full transcript of his address is reproduced below:
“On behalf of the 300,000 member physicians and medical students of the American Medical Association (AMA), it is a pleasure to be here. I am delighted to have this chance to talk with you about an issue that so deeply affects all our professions--direct-to-consumer (DTC) advertising.The Journal of the American Medical Association (JAMA) recently published a set of articles about the positives and the negatives of DTC prescription drug advertising. On the "pro" side, the JAMA article stated that such advertising builds bridges between patients and physicians. On the "con" side, researchers state that DTC marketing of prescription drugs can create consumer demand of a kind that is not entirely healthy. In fact, the article's authors are seeking stricter, not more permissive, FDA regulation over this form of pharmaceutical advertising.I would like to focus on these points of view, and also add my own perspective. I believe one of the critical aspects of DTC advertising is the effect it has on the patient-physician relationship, the cost of care, and patient privacy and confidentiality. I would also like to discuss the benefits, and the drawbacks, of DTC advertising as consumer education, as well as the moral and ethical responsibility and accountability for the costs associated with such advertising.The High Cost of Health CareLet's begin with costs. The cost of our health care system has become an increasing concern that we all face. In 1965, U.S. health care spending represented 6% of our gross national product (GNP). By 1995, health care spending had grown to 14% of the GNP. What factors are driving this rise in costs?One factor is America's aging population. Baby boomers are now reaching the age where they require more medical care. This will accelerate after the year 2010, when the first wave of boomers becomes eligible for Medicare. Our population is also expanding. At the same time, because of the threat of liability, more physicians are practicing "defensive medicine" than they did in 1965. Meanwhile, patients are better educated, and their use of the health care system is growing.A far greater problem in driving up costs than these demographics is related to developing technology. These innovations do not come without a high price tag, yet American innovation applied to health care has had enormous successes. The arrival of insulin in the 1920s, followed by childhood immunizations and antibiotics in the 1930s and 1940s, gave physicians greater ability than they ever have had.In fact, many acute and life-threatening illnesses, such as diabetes, asthma, and congestive heart failure, have now been transformed into chronic conditions that can be controlled. Cholesterol levels, blood pressure, diet, and nutrition can be controlled as well. The risk factors that drive disease are now recognizable. All this results in greater longevity, and a better quality of life, for more people.Cures will become even more common as biotechnology advances, giving us even more powerful biological and pharmaceutical tools to use. However, as we approach the new millennium, cures are not necessarily our final destination. Nor is controlling chronic diseases, because today we are on the verge of another technological revolution--the prediction and prevention of disease. That revolution will grow out of the use of genetic information, or genetic mapping, and will lead to the next great advancement in patient care. This revolution will bring us new specialists, more rigorous physician training, new techniques for measurement, and, of course, escalating costs, as these newest technologies will need to be paid for as well.New challenges will be created, such as how to pay for this new care, as well as the "Big Brother" challenge of maintaining privacy and confidentiality when we can unfold the entire blueprint of a human being and have access to the innermost workings of a single human cell.Advances in TechnologyThe marvelous advances in health care of the past century form a backdrop to our discussion of the issues involved in the advertising of pharmaceuticals directly to consumers. Physicians must keep something in mind--that communications have had a century of exponential growth in content, as well as in methods of reaching the individual. This perpetual nonstop growth of our knowledge base and our tools for communicating creates expectations from society and from patients. We live in a society where one can buy Levi's jeans from Hong Kong directly on the Internet cheaper than in local department stores. Consumers can bid for airline tickets at prices much lower than the airlines could advertise to the public at large. Amazon (www.amazon.com) stocks more books in its virtual warehouse than any bookstore could possibly hold. An Internet communications giant like America On-Line can provide coupons to save money when buying groceries.Computers have given consumers and marketers instant access to information and, increasingly, to services. Individual consumers are no longer lumped together as part of a mass audience. Instead, they can develop their own

tastes and find new power in their personal choices. Marketers make the most of their databases to find and store information about these individuals and their preferences. Since our founding more than 150 years ago, the AMA has been supportive of giving information to patients that is reliable, accurate, and meaningful; that will help patients to make good decisions in treatment choices; and that will help to make them better partners in their health care.Today, thanks to the Internet (where medical information is proliferating), and to DTC advertising, patients are better equipped than ever to take part in their care. A clear benefit of DTC advertising is that it encourages millions of Americans to consult their physicians. This can certainly help to improve the public health.In fact, a recent national survey conducted by Prevention Magazine found that DTC advertising encouraged more than 21 million consumers to discuss medical conditions or illnesses with their doctors--conditions they had never mentioned to physicians before seeing an advertisement. The survey also reported that more than 12 million consumers received a prescribed drug as a direct result of seeing a DTC pharmaceutical advertisement.The Challenges of Direct-to-Consumer AdvertisingThe power of direct advertising is so strong that when the first DTC television advertisement for a nicotine patch aired during the Super Bowl in 1992, within a few weeks, the public's demand for the patches exceeded the supply. The nicotine patches actually had been available for several months before the ad aired, but those who may have wanted to quit smoking were simply not aware of them.Rather than easing the physician's job, the increased patient knowledge base that results from DTC advertising is instead creating new challenges. First, there is the challenge of supplying accurate information. With so much health data available, it is especially important that resources be reliable. Nevertheless, Consumer Reports recently evaluated the accuracy of information in prescription drug advertisements directed at patients. It concluded that information from such marketing has little educational benefit, and in general, is of poor quality. Like the researchers of the JAMA article, the Consumer Reports researchers did not advocate the loosening of FDA regulation over DTC advertising. Instead, the report reminded consumers that "advertisements are not public service messages; they are meant to move goods."In addition to the challenges of truth in advertising, DTC advertising also creates the challenge of escalating costs. This includes not only the marketing costs of developing and placing the ads or the research and development costs of creating new medications, but the costs to the system as a whole.As physicians, we are concerned about advertising that ignores the overall cost of medical care by promoting a switch to the newest, and usually more expensive, pharmaceuticals when older, less expensive medications are just as effective. If a new medicine is as effective as an old one, and does not produce unwanted side effects, then obviously that is desirable. At the same time, newer is not always better--just more expensive. The ratio of cost versus benefits must be balanced, because we are facing a crisis in the cost of care. Anything that does not add to the solution is part of the problem of rising costs.Consider, for an example, the Medicare Commission's proposition to offer pharmaceutical benefits to Medicare beneficiaries. It is a great idea, but it certainly raises a question: Which benefits do we cut in order to add these pharmacy benefits to the Medicare entitlement? If Medicare covered pharmaceutical expenditures, that would add significantly to the growing segment of patients who are insulated by insurance from the real costs of the medications they take.It is important to remember that in DTC advertising for pharmaceuticals, the target audience is often not paying for the product. This has a profound effect on behavior. Without third-party insurance coverage, medications would be more like clothes and cars and other consumer products, where consumers feel the financial implications of their decision making. However, this is not the case today.I have experienced the results of this problem in my own practice. In fact, in 30 years of practice, I can honestly say that the only times my clinical judgement was challenged has been by patients who did not have insurance coverage. They say things like, "Doctor, I don't have insurance. Is this prescription or test or procedure necessary?"I have also heard stories of other physicians who, when they apologize to their patients for writing a very expensive prescription, are surprised to hear this response: "That's okay, doctor. Give me anything you want. I only pay $5 or $10 for my prescriptions."This experience raises a question in my mind. In this climate of cost containment and price pressure within the health care system, don't pharmaceutical companies have the same moral and ethical responsibility to be accountable for containing costs as physicians and hospitals? Perhaps that is not a question that we can answer right now, but it certainly gives us something to think about.How Direct-to-Consumer Advertising Strains the Physician-Patient RelationshipI am also concerned about how the relationship between patient and physician can be stressed and strained by advertising pharmaceuticals directly to consumers. These ads have the potential to create adverse effects on

patients' relationship with and trust in their physicians. When patients come to doctors after seeing a new product advertised, often they demand that product on the spot. Remember, they are covered by insurance, so they do not care about the cost. Yet, in my opinion as their physician, the medication is not necessary, because their present treatment is appropriate and the new medication is only more costly.That is why consumers cannot purchase prescription medications without a doctor's signature. We are trained in prescribing these drugs, because the use as well as the misuse of prescription drugs can have very some serious consequences. The improper use of antibiotics is one of the major factors accelerating antimicrobial resistance. Consider, too, the recent uproar over the use of the combination of fenfluramine and phentermine, commonly known as fen-phen, which was found to be associated with valvular heart disease.It is not just rhetoric to say that prescribing decisions are often a matter of life or death. So when patients come to us with demands for a specific drug, sometimes we have to refuse. In these cases patients may respond with anger and frustration because, although they have limited knowledge, they have full coverage and cannot understand why they cannot "have it all." Swayed by the advertising, they believe needed care is being denied. In fact, patients have been known to switch physicians just because of an ad.Another one of my concerns about DTC pharmaceutical advertising is the practice of obtaining prescription information from pharmacies. Pharmaceutical companies use this information to market new products to patients and physicians. Too often, however, these new medications are more expensive and not always of greater therapeutic benefit. Further, this is a potential invasion of privacy that affects the confidentiality of patient information, because from prescribing information, one can often extrapolate disease conditions or illnesses.Any records of physician encounters with patients, including the medications prescribed, should be solely used for the clinical diagnosis and treatment of patients. Information in medical and prescription records, which results from a privileged relationship, should be protected. Patients understandably fear the misuse of confidential information by insurers and employers. When the information is stored outside the medical record, this is a distinct possibility. The issues of the privacy and confidentiality of patient records are currently under debate by legislators and physicians, but my mind is already made up. Patient records, including pharmacy records, must be used to heal, not to reveal.Our AMA policy is to ensure that any DTC advertising of prescription drugs will contain "accurate and reasonable information on warnings, precautions, and adverse reactions." It must also be presented in terms that patients can understand, and it must be good information that will help our patients make good decisions.Whether we are patients, physicians, pharmaceutical companies, or communicators, we must keep uppermost in our minds that our nation is facing a cost crisis in health care. That means we must all be responsible and accountable in what we do. We must remember that DTC pharmaceutical advertising to patients who are not financially responsible for these decisions does not always result in prudent choices. Nor does it always strengthen the patient-physician relationship.In addition, the use of prescribing information from pharmacies is an invasion of a patient's privacy and the confidentiality of the patient record, which can potentially be harmful to the patient if the information is misused by insurers or employers.ConclusionIn closing, I encourage you to engage in dialogue about the DTC trend, with both its positive and negative sides. Do not make this the end of our discussion. Keep the dialogue open. We have much to learn from one another, and our open dialogue can only help to promote even better care for the patients of America. Our future promises to be more exciting than the past century of health care innovation and growth, filled with technological advances that will give us the tools to cure diseases and illnesses as never before, to control the risk factors involved in diseases, and even to predict and prevent those diseases.We have heard laments about the passing of "the good old days." I believe that the good old days of health care are yet to come. We will be able to determine how tomorrow's innovations will be used, as we engage patients as consumers of their own health care, bringing to bear the same ethics and high standards that have made American medicine the very best in the world. That will keep the state of medical care in America strong, as we enter the threshold of health care's next century of progress--for patients, for physicians, and for society as a whole.”
Dr Matthew F. Hollon, of the Department of Medicine, University of Washington, Seattle has expressed concern about DTC promotion in the Journal of the American Medical Association70 as follows:
70 http://jama.ama-assn.org/issues/v281n4/full/jcv80002.html#aainfo

“Direct-to-Consumer Marketing of Prescription Drugs: Creating Consumer Demand In the early 1980s, the pharmaceutical industry began marketing prescription drugs directly to patients. The Food and Drug Administration (FDA) imposed a moratorium on this marketing strategy in 1983, then lifted it in 1985.1 Since then, the industry has devoted increasing resources to this strategy. In a 1988 editorial on direct-to-consumer (DTC) marketing, Eric P. Cohen, MD, wrote, "Issues of regulation of advertising, cost, competition, public health, and individual well being need to be carefully examined."2 Examination of these issues in rigorous, independent studies has not occurred. Despite the lack of studies, the FDA has relaxed regulations governing DTC marketing of prescription drugs.3
Proponents hypothesize that DTC marketing, by providing educational information, is valuable, notifying consumers of new therapies and motivating them to seek care. However, the pharmaceutical industry, driven in part by financial motives, is providing information of suspect quality and thus minimal benefit. Reckoning the costs, economic and otherwise, the public health value of DTC marketing is negligible. Moreover, the effects of DTC marketing are undesirable. Most important, by creating consumer demand, DTC marketing undermines the protection that is a result of requiring a physician to certify a patient's need for a prescription drug. For the benefit of patients, physicians, and the public's health, the FDA should consider stricter—not more permissive—regulations.While providing educational information may be one of the industry's motives, the bottom-line desire for profit is undoubtedly another. In this respect, industry efforts have been successful. Advertising nicotine patches directly to consumers turned patches into "an $800 million dollar category."4 Aggressive marketing of Claritin (Schering-Plough, Madison, NJ) captured 56% of the $1.8 billion nonsedating antihistamine market.5 In the wake of successes, spending on DTC advertising rocketed from $13.1 million in 1989 to more than $900 million in 1997, double the $438 million spent on advertisements in medical journals.6, 7
The pharmaceutical industry's interest in the bottom line is legitimate. The industry, which has made important medical contributions, exists because it is profitable. However, as the profit motive can affect the content of information in advertisements, the public health value of DTC marketing should be examined by comparing the benefits the public gains with the costs the public incurs.The industry is not marketing to consumers in a health information vacuum. A vast amount of health information is accessible to and inundates the public every day.8, 9 Since "almost every drug product has some advantage for some patient," it is anecdotally true that any information the industry provides about a product has some benefit for someone.10 However, when dumped into the ocean of available information, the sum of these anecdotes does not necessarily equal public health benefit, especially when the quality of the information provided is suspect. If studies of advertising directed at physicians offer a clue, this information, in fact, has minimal educational benefit.In one study, Wade et al11 asked pharmaceutical companies to supply their best evidence in support of marketing claims. Of 67 references cited, only 31 contained relevant original data and only 13 were controlled trials. These investigators concluded, "Standards of evidence used to justify advertising claims are inadequate." In a study of advertising in the leading medical journals in 18 countries, Herxheimer et al12 reported that important warnings and precautions were missing in half of the 6700 advertisements surveyed. In yet another study, Stryer and Bero13 concluded that advertisements contained a higher proportion of promotional material than educational material, and little of this material contained information about important therapeutic breakthroughs. In 1992, Wilkes et al14 evaluated 109 pharmaceutical advertisements and found that 57% of these advertisements had little or no educational value.Recently, Consumer Reports, evaluating the accuracy of information in prescription drug advertisements directed at patients, substantiated the conclusions drawn from studies of marketing directed at physicians.15 Information from marketing has little educational benefit and, in general, its quality is poor. Less than half of DTC advertisements reviewed were candid about efficacy. Consumer Reports concluded, "the rules governing prescription drug advertising should not be loosened," and that "[advertisements] are not public service messages—they're meant to move goods."David A. Kessler, MD, while commissioner of the FDA, wrote in response to the study by Wilkes et al, "[it] serves an important purpose. It heightens awareness of the degree to which misleading information may pervade the 'informational marketplace.' "16 In his editorial, Kessler documented the subtle techniques used by the pharmaceutical industry to distort information including "data dredging" and making claims of "no difference" from studies with limited statistical power. Providing poor quality information in today's marketplace of health information results in little or no benefit for the public. Considering the costs, providing this information is unlikely to have public health value.

Costs can include an increase in expenditures, improper use of drugs, and harm from adverse events. Unlike many products, the use of prescription drugs can have serious consequences. The improper use of antibiotics in humans is one of the major factors accelerating antimicrobial resistance.17, 18 Prescription drugs can and do cause harm. Consider the recent concern that the use of the combination of anorectic agents, fenfluramine and phentermine, may be associated with valvular heart disease.19 Consider also benoxaprofen, a prescription nonsteroidal anti-inflammatory agent, launched in 1980 in the United Kingdom and subsequently the United States.20 The product gained "a major foothold merely on the strength of a well-orchestrated marketing strategy, which included full-page advertisements in the popular press." Sixty-one drug-related deaths occurred during the 2 years in which the drug remained on the market.Expenditures are also an important consideration. Drugs reduce expenditures by preventing complications from diseases.21 However, this statement is not axiomatic. Expenditures may increase when marketing of prescription drugs creates need, when disease complications are rare or nonexistent, or when choices of drug therapy for a disease are available. For example, a recent survey of trends in antihypertensive drug use in the United States revealed that despite the recommendations of the Fifth Joint National Committee on the Detection, Evaluation, and Treatment of High Blood Pressure, the use of calcium antagonists and angiotensin-converting enzyme inhibitors has increased.22 The investigators cite the effectiveness of pharmaceutical promotion practices as one of the possible reasons for this. They note, "the cost implications of these practice patterns are enormous."If DTC marketing affects physicians' prescribing practices, then DTC marketing has no public health value because the public ostensibly incurs costs that exceed the minimal benefits. Some argue that physicians serve as the system's safety net, preventing the inappropriate use of prescription drugs. This argument, however, rests on a number of questionable assumptions. It assumes that physicians are always rational in prescribing. It assumes that such things as patients' demands do not influence physicians' prescribing practices. It assumes that, at a population level, physicians are nearly infallible. Available evidence casts doubt on these assumptions.Variability not explained solely by the pharmacological needs of patients exists in physicians' prescribing practices.23, 24 Examining this variability, Schwartz et al25 identified physicians who prescribed 3 drugs "at a rate far greater than that warranted by scientific evidence of their effectiveness." In this study, patient demand was the most commonly cited motivation for prescribing the target drugs. In a study of antibiotic use for upper respiratory tract infections, Hamm et al26 documented that the patient's expectation for an antibiotic is an important factor in the decision to prescribe the drug. Moreover, 2 recent studies concur with previous findings that patients who expect a prescription are "many times more likely to receive one."27 At the population level, Willcox et al28 found that 23.5% of Americans aged 65 years or older living in the community receive at least 1 of 20 inappropriate drugs. These authors call for broader educational and regulatory initiatives. Finally, preliminary evidence from a study by Hueston et al29 suggests managed care organizations have not reduced inappropriate prescribing.The act of issuing a prescription is the culmination of a complex set of decisions; certainly, physicians' decisions can improve. What effect does DTC marketing have on these decisions? Consumer advocates of DTC marketing argue that this strategy, highlighting the evolving relationship between physicians and patients, shifts control over prescription decisions from physicians to patients, giving patients greater command over their health care.30 In reality, the principal effect of DTC marketing is to create consumer demand, changing the physician-patient relationship to a physician-consumer relationship. The consequences of this change are open for debate, but the impact is noticeable.In 1992, physicians reported that 88% of patients asked for a drug by brand name, up from 45% in 1989.6 At the same time, a survey revealed that 63% of consumers do not believe they can tell if they are being misled by advertisements for prescription drugs.31 An advertising industry executive concludes, "Creating consumer demand [among patients] for prescription pharmaceuticals is now an attainable marketing objective."32 Physicians' prescribing decisions can improve, but creating consumer demand does not help. Rather, by influencing these decisions, consumer demand undermines the protection that is a result of requiring a physician to consider seriously a patient's need for a drug, then certify that need.Neither physicians nor patients are immune to the effects of marketing. However, while physicians are not immune, their education and knowledge presumably make them more competent than consumers in interpreting promotional material for prescription drugs. Additionally, unlike consumers who hear of just 1 drug, physicians are capable of offering sound advice to patients about a range of therapeutic options. If the value of DTC marketing is negligible and the primary effect of this strategy is to create consumer demand, then, unlike the truly valuable contributions of the pharmaceutical industry, DTC marketing is not good for patients, physicians, or the public's health.

An industry consultant predicts, "The winners in the prescription drug category are not going to be the ones with the best patents or products, but those that are the best marketers."5 Currently the industry is pursuing the next steps in DTC marketing, including using broadcast media and the Internet. The industry is moving beyond mass media vehicles to more focused efforts such as direct marketing through databases to targeted consumers.32 Until well-designed, independent studies based on available observational data prove the information from DTC marketing has public health value and desirable effects, the FDA should consider stricter—not more permissive—regulations.1.Food and Drug Administration. Direct-to-consumer advertising of prescription drugs: withdrawal of moratorium. Federal Register. September 9, 1985;50:36677-36678.2. Cohen EP. Direct-to-the-public advertisement of prescription drugs. N Engl J Med. 1988;318:373-376.3.US Department of Health and Human Services, Public Health Service, Food and Drug Administration.FDA to review standards for all direct-to-consumer Rx drug promotion.Available at: http://www.fda.gov/bbs/topics/NEWS/NEW00582.html. Accessed August 25,1997.4.Weber J, Carey J. Drug ads: a prescription for controversy. Business Week. January 18, 1993:58-59.5.Freeman L. Aggressive strategy helps propel Claritin to top slot. Advertising Age. March 16, 1998;69(11):S6-S7.6.Liebman H. Consumer, heal thyself: ads for prescription drugs are popping up more frequently in consumer media. Mediaweek. July 5, 1993;3(27):12.7. Wilke M. Prescription for profit. Advertising Age. March 16, 1998;69(11):S1, S26.8. Why do Americans resist a healthy lifestyle. USA Today Magazine.October 1994;123(2593):1-2.9. Harper J. Information overload may be making some Americans sick. Insight on the News. September 15, 1997;13(34):40-41.10. Peck CC, Rheinstein PH. FDA regulation of prescription drug advertising. JAMA. 1990;264:2424-2425.11. Wade VA, Mansfield PR, McDonald PJ. Drug companies' evidence to justify advertising. Lancet. 1989;2:1261-1264. 12. Herxheimer A, Lundborg CS, Westerholm B. Advertisements for medicines in leading medical journals in 18 countries: a 12-month survey of information content and standards. Int J Health Serv. 1993;23:161-172. 13. Stryer D, Bero LA. Characteristics of materials distributed by drug companies. J Gen Intern Med. 1996;11:575-583. 14. Wilkes MS, Doblin BH, Shapiro MF. Pharmaceutical advertisements in leading medical journals: experts' assessments.Ann Intern Med. 1992;116:912-919.15. Drug advertising: is this good medicine. Consumer Reports. June 1996;61(6):62-63.16. Kessler DA. Addressing the problem of misleading advertising. Ann Intern Med 1992;116:950-951. 17. Williams RJ, Heymann DL. Containment of antibiotic resistance. Science. 1998;279:1153-1154. 18. Low DE, Scheld WM. Strategies for stemming the tide of antimicrobial resistance. JAMA. 1998;279:394-395. 19. Connolly HM, Crary JL, McGoon MD, et al. Valvular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588. 20.Gerber P. Mass product-liability litigation. Med J Aust. 1988;148:485-488. 21.US Department of Health and Human Services, Public Health Service, Food and Drug Administration.FDA public hearing: direct-to-consumer promotion.Available at: http://www2.evolvingtech.com/etc/industry/hearings/95N227contents.html. Accessed June 21, 1997.22.Siegel D, Lopez J. Trends in antihypertensive drug use in the United States: do the JNC V recommendations affect prescribing? JAMA. 1997;278:1745-1748. 23. Hemminki E. Review of literature on the factors affecting drug prescribing. Soc Sci Med. 1975;9:111-115. 24.Weiss MC, Fitzpatrick R, Scott DK, Goldacre MJ. Pressures on the general practitioner and decisions to prescribe. Fam Pract. 1996;13:432-438. 25.Schwartz RK, Soumerai SB, Avorn J. Physician motivations for nonscientific drug prescribing. Soc Sci Med. 1989;28:577-582. 26. Hamm RM, Hicks RJ, Bemben DA. Antibiotics and respiratory infections: are patients more satisfied when expectations are met? J Fam Pract. 1996;43:56-62 27.Greenhalgh T, Gill P.Pressure to prescribe. BMJ. 1997;315:1482-1483.

28. Willcox SM, Himmelstein DU, Woolhandler S. Inappropriate drug prescribing for the community-dwelling elderly. JAMA. 1994;272:292-296. 29. Hueston WJ, Mainous III AG, Brauer N, Mercuri J. Evaluation and treatment of respiratory infections: does managed care make a difference? J Fam Pract. 1997;44:572-577. 30.Golodner LF, National Consumers League. Consumer group responds to FDA's draft guidance on direct-to-consumer advertising on television. Available at: http://www.natlconsumersleague.org/dtcp.htm. Accessed August 26, 1997.31.Whyte J. Direct consumer advertising of prescription drugs. JAMA. 1993;269:146, 150. 32.Wilke M, Teinowitz I, Kelly KJ. Ad fever sweeps healthcare industry. Advertising Age. January 13, 1997;68(2):1, 18-19.
That article was published with an article that supported DTC promotion.71 Two letters in response were published72 which follow:
Direct-to-Consumer Advertising: Education or Anathema? To the Editor: Mr Holmer1 makes a case in support of direct-to-consumer (DTC) advertising that puts critics on the defensive. After all, who can be against free speech and educating and empowering patients?Holmer plays down the inflationary effect of DTC advertising, with which the costliest drugs are pitched with all the skill that the advertising budgets of pharmaceutical companies can buy. There is no corresponding lobby for less expensive drugs with lower profit potential. Instead, spin doctors take over from medical doctors and profitability supersedes the presentation of balanced information.Holmer neglects the role of managed care. Because benefit managers are able to negotiate for lower drug prices, pharmaceutical manufacturers seek to offset managed care "losses." What could be simpler than doing an end run around the cost-containment efforts of health managers and physicians by going directly to patients to create demand that will be difficult to refuse?Nor does Holmer discuss the effect on physicians who become involuntary appendages of manufacturers' public relations departments as they field questions inspired by print and television drug ads. He argues that physicians are not unduly influenced by the DTC ad campaigns because only 51% of patients who inquire actually get a prescription (according to 1 unpublished manufacturer's survey Holmer cites), but this statistic may also be interpreted as a costly waste of physician time in the other half of the cases.This kind of cost-shifting is eroding the close and collaborative relationship that physicians once had with the pharmaceutical industry. Our relationship is becoming competitive and, at times, hostile. Thus far, industry may be considered the winner. Some health insurers, including Medicaid, are now spending more on pharmaceuticals than on physicians' fees.2, 3
Holmer hints that physicians should not complain because they share the wealth created by DTC advertising. But such collusion would ultimately erode the barriers to cost-effective prescribing. This is hardly preferable, even if the only other choice is for physicians to be ill-treated.Higher costs, friction between professional ethics and business, and the inevitable abuses of unbridled competition may, in the long run, cause the pharmaceutical industry to look back to the gentler pre-DTC times with nostalgia.
Philip R. Alper, MDUniversity of California at San Francisco
1. Holmer AF. Direct-to-consumer prescription drug advertising builds bridges between patients and physicians. JAMA. 1999;281:380-382. 2. Tanoiwye E. Drug dependency—US has developed an expensive habit: now, how to pay for it? Wall Street Journal. November 16, 1998;1. 3. Iglehart JK. The American health care system—Medicaid. N Engl J Med. 1999;340:403-408.
71 Holmer AF. Direct-to-consumer prescription drug advertising builds bridges between patients and physicians. JAMA. 1999;281:380-38272 http://jama.ama-assn.org/issues/v282n13/full/jlt1006-4.html

To the Editor: As members of the Committee on Bioethical Issues of the Medical Society of the State of New York, we agree with Dr Hollon1 that DTC advertising creates consumer demand, but disagree with Mr Holmer's2 claim that such advertising builds bridges between patients and physicians.Direct drug advertising provides no real benefit to patients, is potentially harmful, and is costly. We therefore urge the US Food and Drug Administration (FDA) to review and strengthen its policies concerning this practice. We believe that direct promotion to consumers should be limited to over-the-counter drugs. We urge the FDA to request and designate additional resources for the policing of its regulations by preclearing submissions from advertisers, monitoring advertisements, and investigating complaints from consumers and health care professionals. False, misleading, or deceptive drug promotions and advertisements that cannot be supported by clinically valid and statistically reliable data or that contain confusing or misleading words and phrases or give an overall inaccurate impression3 should be forcefully dealt with and, if necessary, penalties imposed and those responsible prosecuted.We urge the FDA to establish a commission to oversee the marketing activities of the pharmaceutical industry and to monitor its adherence to the FDA rules and regulations. Such a commission in Sweden functions as a "watchdog" in monitoring written information such as advertisements.4 The FDA should empower such a commission to monitor drug promotions on radio, television, and the World Wide Web. We believe that Congress should strengthen the FDA by providing adequate funds to permit the FDA to fulfill its oversight responsibilities of prescription drug advertising and to establish an oversight commission.
Fred Rosner, MDPieter Kark, MDSamuel Packer, MDAllen Bennett, MDJeffrey Berger, MDMedical Society of the State of New YorkLake Success
1. Hollon MF. Direct-to-consumer marketing of prescription drugs: creating consumer demand. JAMA. 1999;281:382-384 2. Holmer AF. Direct-to-consumer prescription drug advertising builds bridges between patients and physicians. JAMA. 1999;281:380-382. 3. Lexchin J. Consequences of direct-to-consumer advertising of prescription drugs. Can Fam Physician. 1997;43:594-596. 4. Perman E. Voluntary control of drug promotion in Sweden. N Engl J Med. 1990;323:616-617.
The last wordThe following is a report by one of the staff reporters of the British Medical Journal on a debate about DTC
promotion in the UK held in October 1999.
Selling drugs to consumers “Time was when fat people were counselled to eat less and shy people were advised to get out more. Now, if they are living in the United States, such people are exhorted to take pills. Hoffman-La Roche is spending $75m (£47m) persuading Americans to take its slimming pill Xenical (orlistat), and SmithKline Beecham is spending $30m promoting its anti-shyness pill, Paxil (paroxetine). In Britain, however, consumers are protected from, or deprived of (depending on your point of view), such blandishments. Both products are prescription only medicines, and the pharmaceutical industry is not allowed to promote them direct to the general public. But how long will this last? The British drugs industry sees changing the law as its most pressing task. It is promoting discussion of the issue throughout the media. You can hardly open a newspaper today without seeing another article on the subject. And last week, the King's Fund, an independent think tank, held a debate on the issue entitled: "Drug companies should be able to advertise their prescription products to the public."
Margot James, chief executive of Shire Hall Group, a public relations company whose clients include several large drug companies, outlined the arguments in favour of the motion. She claimed that many poor people with chronic conditions were unaware of the fact that effective treatments existed. She cited the example of incontinence. Until recently, many women suffered in silence, not knowing that treatment was available. A television public awareness campaign shown, among other times, during breaks in Granada Television's Coronation Street had changed all that and had transformed peoples' lives, she said. "Most communication to the public about health comes from the editorial columns in newspapers and magazines," Ms James said. "This increases the inequality in our society because people from lower socioeconomic groups get their information from television and the tabloids. It is in the quality press that you see the best information. People who read the tabloids are more likely to be at the end of a sensational health scare than receive useful information." Other speakers suggested that there was a conspiracy of silence, whereby neither the medical profession nor the government told patients about new drugs because doctors wanted to keep their individual prescribing budgets down and the government wanted to keep a lid on the country's drugs bill. Dr Paul Hooper, UK general manager of the drug company Eisai, pointed out that, with the advent of the National Institute for Clinical Excellence (NICE), it was likely that certain new drugs would not be available on the NHS. The industry had some powerful allies in the shape of Claire Rayner, president of the Patients Association, Dr Ian Banks, chairman of the Men's Health Forum, and several chairmen of NHS trusts. Ms James also pointed out that when the US Food and Drugs Administration recently asked for data showing that direct to consumer advertising had harmed public health no one provided any. But how well do these arguments stand up? Joe Collier, professor of medicines policy, at St George's Hospital Medical School, and editor of the Drug and Therapeutics Bulletin, does not think that they stand up at all. More information for patients is good, but biased information is not the same as unbiased information, he says. In many ways, biased information is worse than no information at all because it thoroughly confuses people. "A company is there to look after its shareholders and keep its profits up. There is no point in advertising unless you are going to increase the use of your products. Advertising is about increasing sales." He said that most of his time at the Drugs and Therapeutics Bulletin was spent trying to unravel the distortions put about by doctors, who had been "bought" by the drugs industry, and by patients groups, which had also been "bought" by the industry. "Very rarely, if ever, do you get advertising that is not distorted. If you abolished advertising to doctors, it would improve prescribing," he claimed. Claire Rayner accused Professor Collier of "hating" the drugs industry. He denied it. "The industry has done some wonderful things. What I don't like is when it distorts the truth," he explained. "If you allow drug companies to advertise to patients, they are going to distort the truth. They will promote their own product as if it is the only product. It might well be a new product, it may well be more expensive than existing products, it may not work as well as older products," he said. The drug companies would enlist members of the public as "foot soldiers" in their campaigns to increase sales by persuading them to go and ask their doctors for their drugs. "They are cheaper than sales representatives," he added. He also pointed out that he was not alone in opposing direct to consumer advertising: "Most of the organisations which have campaigned for better information for patients over the years are also opposed to it." He cited, as examples, the Consumers' Association, Social Audit, the International Society of Drug Bulletins, Health Action International, and the Public Citizen in the United States. Although the King's Fund debate lasted only an hour and a half, the national debate is going to last much longer and is not likely to end until the drugs industry gets its way. Spending on direct to consumer advertising in the United States has now reached $1bn, and where the United States leads, Britain usually follows. A change in the law could result in millions being spent. The humorist Stephen Leacock defined advertising as "the science of arresting the human intelligence long enough to get money from it." In the case of prescription medicines, of course, the money
will not come from the consumer but from the public purse.”


















