Renal Tubular Acidosis. Normal Renal Function Proximal Tubule Reabsorption: HCO 3 - (90%) –...
74
Renal Tubular Acidosis
-
Upload
margery-newton -
Category
Documents
-
view
227 -
download
3
Transcript of Renal Tubular Acidosis. Normal Renal Function Proximal Tubule Reabsorption: HCO 3 - (90%) –...

Renal Tubular Acidosis

Normal Renal FunctionProximal Tubule
Reabsorption:
• HCO3- (90%) – carbonic
anhydrase
• calcium
• glucose
• Amino acids
• NaCl, water
Distal Tubule
• Na+ reabsorbed
• H+ (NH4+ or
phosphate salts) excreted
• molar competition between H+ and K+
• Aldosterone

OUTLINE Renal tubular acidosis (RTA) is applied to a group of
transport defects in the reabsorption of bicarbonate (HCO3
-), the excretion of hydrogen ion (H+), or both.
The RTA syndromes are characterized by a relatively normal GFR and a metabolic acidosis accompanied by hyperchloremia and a normal plasma anion gap.

OBJECTIVES Physiology of Renal acidification. Types of RTA and characteristics Lab diagnosis of RTA Approach to a patient with RTA Treatment

Physiology of Renal Acidification Kidneys excrete 50-100 meq/day of acid generated daily. This is achieved by H+ secretion at different levels in the
nephron. The daily acid load cannot be excreted as free H+ ions. Secreted H+ ions are excreted by binding to either buffers,
such as HPO42- and creatinine, or to NH3 to form NH4+.
The extracellular pH is the primary physiologic regulator of net acid excretion.

Renal acid-base homeostasis may be broadly divided into 2 processes
1. Proximal tubular absorption of HCO3- (Proximal
acidification)2. Distal Urinary acidification. Reabsorption of remaining HCO3
- that escapes proximally.
Excretion of fixed acids through buffering & Ammonia recycling and excretion of NH4
+.
Proximal tubule physiology Proximal tubule contributes to renal acidification by
H+ secretion into the tubular lumen through NHE3 transporter and by HCO3
- reabsorption. Approx. 85% of filtered HCO3
- is absorbed by the proximal tubule.
The remaining 15 % of the filtered HCO3- is
reabsorbed in the thick ascending limb and in the outer medullary collecting tubule.

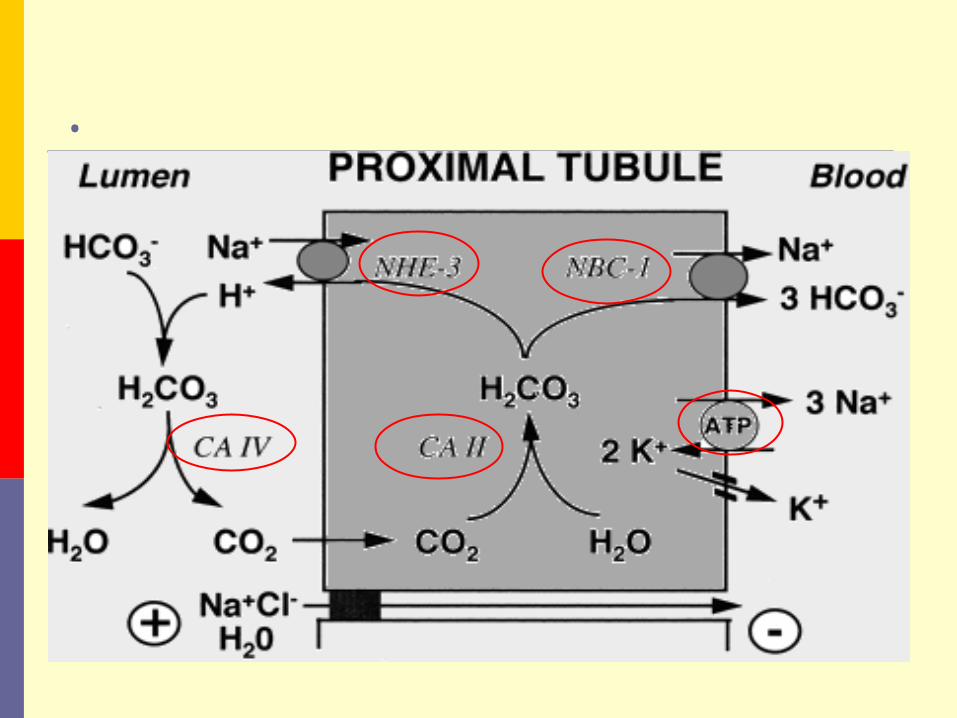
Proximal tubule physiology
Multiple factors are of primary importance in normal bicarbonate reabsorption
The sodium-hydrogen exchanger in the luminal membrane(NHE3).
The Na-K-ATPase pump The enzyme carbonic anhydrase II & IV The electrogenic sodium-bicarbonate
cotransporter(NBC-1).
.

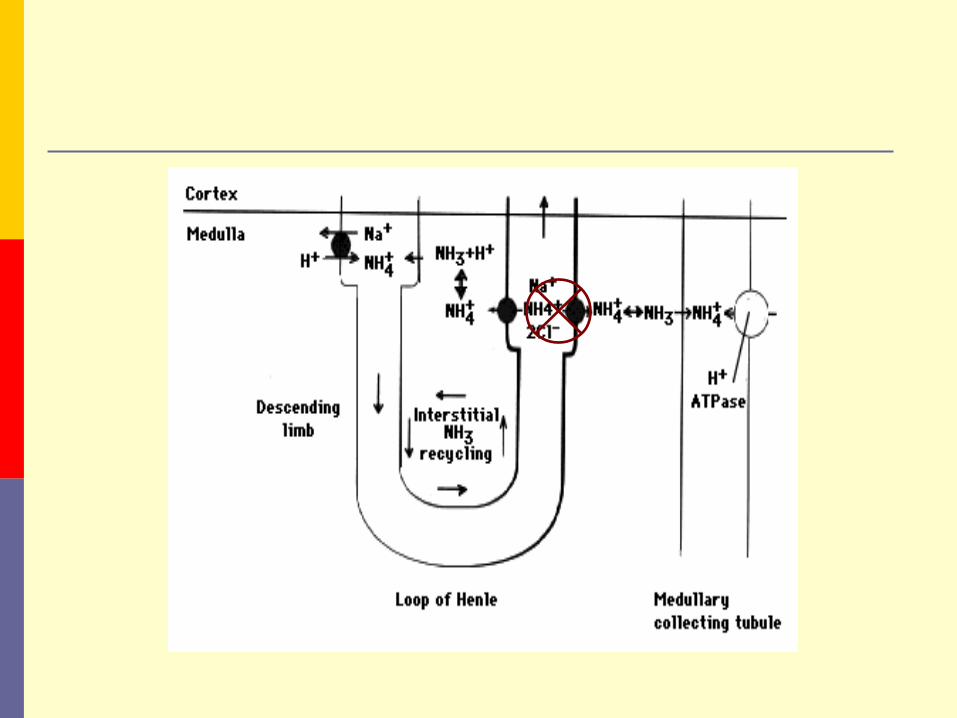
Ammonia recycling Ammonium synthesis and excretion is one of the
most important ways kidneys eliminate nonvolatile acids.
Ammonium is produced via catabolism of glutamine in the proximal tubule cells.
Luminal NH4+ is partially reabsorbed in the thick
ascending limb and the NH3 then recycled within the renal medulla

Ammonia Recycling
The medullary interstitial NH3 reaches high concentrations that allow NH3 to diffuse into the tubular lumen in the medullary collecting tubule, where it is trapped as NH4
+ by secreted H+.

Distal Urinary Acidification The thick ascending limb of Henle’s loop reabsorbs
about 15% of the filtered HCO3- load by a mechanism
similar to that present in the proximal tubule, i.e., through Na+-H+ apical exchange(NHE3).

H+ secretion The collecting tubule (CT) is the major site of H+
secretion and is made up of the medullary collecting duct (MCT) and the cortical collecting duct (CCT).
Alpha and Beta-intercalated cells make up 40% of the lining while Principal cells and collecting tubule cells make up the remainder.
Alpha-Intercalated Cells are thought to be the main cells involved with H+ secretion in the CT.
This is accomplished by an apically placed H+-K+-ATPase and H+-ATPase with a basolateral Cl-/HCO3
- exchanger and the usual basolateral Na+ - K+ ATPase.


Beta-Intercalated Cells in contrast to the above have a luminal Cl-/HCO3
- exchanger and a basolateral H+-ATPase.
They play a role in bicarbonate secretion into the lumen that is later reabsorbed by the CA IV rich luminal membrane of medullary collecting duct.

CCT H+ secretion is individually coupled to Na+ transport. Active Na+ reabsorption generates a negative lumen potential favoring secretion of H+ and K+ ions.
In contrast the MCT secretes H+ ions independently of Na+.
Medullary portion of the Collecting duct is the most important site of urinary acidification
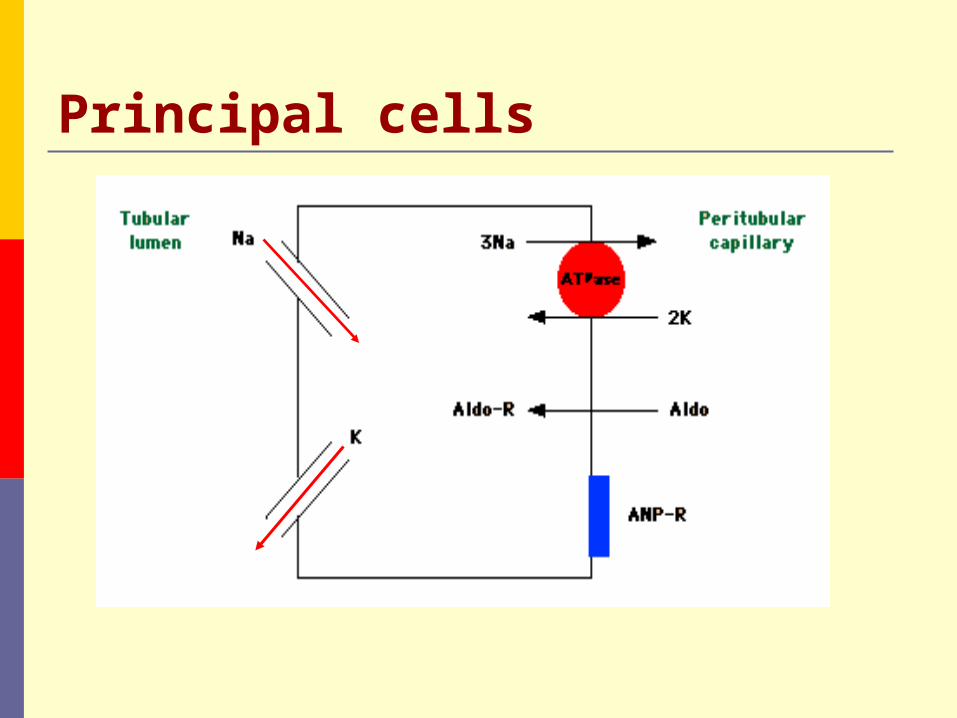
Principal cells

Aldosterone and Renal acidification Favors H+ and K+ secretion through enhanced sodium
transport. Recruits more amiloride sensitive sodium channels in
the luminal membrane of the collecting tubule. Enhances H+-ATPase activity in cortical and
medullary collecting tubules. Aldosterone also has an effect on NH4+ excretion by
increasing NH3 synthesis
Summary of renal physiology H+ secretion, bicarbonate reabsorption and NH4
+ production occur at the proximal tubule. Luminal CA IV is present in the luminal membrane at this site and in MCT.
NH4+ reabsorption occurs at TAL of loop of Henle and helps in ammonia recycling that facilitates NH4+ excretion at MCT.
H+ secretion occurs in the CCT either dependent or independent of Na availability and in the MCT as an independent process..

OBJECTIVES Physiology of Renal Acidification. Types of RTA and characteristics Lab diagnosis of RTA Approach to a patient with RTA Treatment

Renal Tubular Acidosis

TYPES OF RTA Proximal RTA (type 2) Isolated bicarbonate defect Fanconi syndrome
Distal RTA (type 1) Classic type Hyperkalemic distal RTA
Hyperkalemic RTA (Type 4)

Renal Tubular AcidosisType 2 RTA Type 1 RTA
Type 4 RTA

PROXIMAL RTA Proximal RTA (pRTA) is a disorder leading to
HCMA secondary to impaired proximal reabsorption of filtered bicarbonate.
Since the proximal tubule is responsible for the reabsorption of 85-90% of filtered HCO3
- a defect at this site leads to delivery of large amounts of bicarbonate to the distal tubule.

This leads to bicarbonaturia, kaliuresis and sodium losses.
Thus patients will generally present with hypokalemia and a HCMA (hyperchloremic metabolic acidosis).

.

Isolated defects in PCT function are rarely found. Most patients with a pRTA will have multiple defects in PCT function with subsequent Fanconi Syndrome.
The most common causes of Fanconi syndrome in adults are multiple myeloma and use of acetazolamide.
In children, cystinosis is the most common.

pRTA is a self limiting disorder and fall of serum HCO3
- below 12 meq/l is unusual, as the distal acidification mechanisms are intact..
Urine ph become remains acidic(<5.5) mostly but becomes alkaline when bicarbonate losses are corrected.
FEHCO3 increases(>15%)with administration of alkali for correction of acidosis
(FEHCO3 = fractional excretion of HCO3)
Cause of hypokalemia in Type 2 RTA Metabolic acidosis in and of itself decreases pRT Na+
reabsorption leading to increased distal tubule delivery of Na+ which promotes K+ secretion.
The pRTA defect almost inevitably leads to salt wasting, volume depletion and secondary hyperaldosteronism.
The rate of kaliuresis is proportional to distal bicarbonate delivery. Because of this alkali therapy tends to exaggerate the hypokalemia.

Patients with pRTA rarely develop nehrosclerosis or nephrolithiasis. This is thought to be secondary to high citrate excretion.
In children, the hypocalcemia as well as the HCMA will lead to growth retardation, rickets, osteomalacia and an abnormal vitamin D metabolism. In adults osteopenia is generally seen.

To summarise Type 2 RTA Proximal defect Decreased reabsorption of HCO3
-
HCO3- wasting, net H+ excess
Urine pH < 5.5, although high initially K+: low to normal

Type 2 RTACauses: Primary
Idiopathic, sporadic Familial: Cystinosis,
Tyrosinemia, Hereditary Fructose intolerance, Galactosemia, Glycogen storage disease (type 1), Wilson’s disease, Lowe’s syndrome
Fanconi’s Syndrome Generalized proximal
tubule dysfunction Proximal loss of phos, uric
acid, glucose, AA
Acquired Multiple Myeloma Carbonic anhydrase inhibitors
(Acetazolamide) Other drugs (Ampho B, 6-
mercaptopurine) Heavy Metal Poisonings (Lead,
Copper, Mercury, Calcium) Amyloidosis Disorders of protein, Carb, AA
metabolism
Hypophosphatemia, hypouricosuria, renal glycosuria with normal serum glucose

DISTAL RTA Distal RTA (dRTA) is a disorder leading to HCMA
secondary to impaired distal H+ secretion. It is characterized by inability to lower urine ph
maximally(<5.5) under the stimulus of systemic acidemia. The serum HCO3
- levels are very low <12 meq/l.
It is often associated with hypercalciuria, hypocitraturia, nephrocalcinosis, and osteomalacia.

The term incomplete distal RTA has been proposed to describe patients with nephrolithiasis but without metabolic acidosis.
Hypocitraturia is the usual underlying cause.

The most common causes in adults are autoimmune disorders, such as Sjögren's syndrome, and other conditions associated with chronic hyperglobulinemia.
In children, type 1 RTA is most often a primary, hereditary condition.

Secretory defects causing Distal RTA

Non secretory defects causing Distal RTA
Gradient defect: backleak of secretd H+ ions. Ex. Amphotericin B
Voltage dependent defect: impaired distal sodium transport ex. Obstructive uropathy, sickle cell disease, Congenital Adrenal Hyperplasia, Lithium and amiloride etc.
This form of distal RTA is associated with hyperkalemia(Hyperkalemic distal RTA)
A high urinary pH (5.5) is found in the majority of patients with a secretory dRTA.
Excretion of ammonium is low as a result of less NH4
+trapping. This leads to a positive urine anion gap.
Urine PCO2 does not increase normally after a bicarbonate load reflecting decreased distal hydrogen ion secretion.
Serum potassium is reduced in 50% of patients. This is thought to be from increased kaliuresis to offset decreased H+ and H-K-ATPase activity.

What Charles Dicken’s character is theorized to have suffered from RTA?
Tiny Tim
Growth retardation Bone disease Intermittent muscle
weakness (hypokalemia) Kidney stones Progressive renal failure Death
Lewis DW, Am J Dis Child. 1992 Dec; 146(12): 1403-7.
To summarise Type 1 RTA First described, classical form Distal defect decreased H+ secretion H+ builds up in blood (acidotic) K+ secreted instead of H+ (hypokalemia) Urine pH > 5.5 Hypercalciuria Renal stones

Type 1 RTACauses: Primary
Idiopathic, sporadic Familial – AD, AR
Secondary – Autoimmune (SLE, Sjogren’s, RA) Hereditary hypercalciuria, hyperparathyroidism, Vit D
intoxication Hypergammaglobulinemia Drugs (Amphotericin B, Ifosfamide, Lithium) Chronic hepatitis Obstructive uropathy Sickle cell anemia Renal transplantation


Serrano A and Batlle D. N Engl J Med 2008;359:e1
A 37-year-old man was referred for evaluation of distal renal tubular acidosis

Type 4 RTA (Hyperkalemic RTA) This disorder is characterized by modest HCMA with
normal AG and association with hyperkalemia. This condition occurs primarily due to decreased
urinary ammonium excretion. Hypoaldosteronism is considered to be the most
common etiology. Other causes include NSAIDS, ACE inhibitors, adrenal insufficiency etc.

Mechanism of action

In contrast to hyperakalemic distal RTA, the ability to lower urine ph in response to systemic acidosis is maintained.
Nephrocalcinosis is absent in this disorder.

To summarise Type 4 RTA Aldosterone deficiency or distal tubule
resistance to Aldosterone Impaired function of Na+/K+-H+ (cation)
exhange mechanism Decreased H+ and K+ secretion plasma
buildup of H+ and K+ (hyperkalemia) Urine pH < 5.5

Renal Tubular AcidosisType 2 RTA Type 1 RTA
LOW serum K+
Type 4 RTA
HIGH serum K+

Type 4 RTAAcquired Causes Renin:
Diabetic nephropathy NSAIDS Interstitial Nephritis
Normal renin, Aldo: ACEs, ARBs Heparin Primary adrenal
response
response to Aldo: Medications: K+ sparing
drugs (Sprinolactone), TMP-SMX, pentamidine, tacrolimus
Tubulointerstitial ds: sickle cell, SLE, amyloid, diabetes

What happened to Type 3 RTA? Very rare Used to designate mixed dRTA and pRTA
of uncertain etiology Now describes genetic defect in Type 2
carbonic anhydrase (CA2), found in both proximal, distal tubular cells and bone

OBJECTIVES Physiology of Renal Acidification. Types of RTA and characteristics Lab diagnosis of RTA Approach to a patient with RTA Treatment
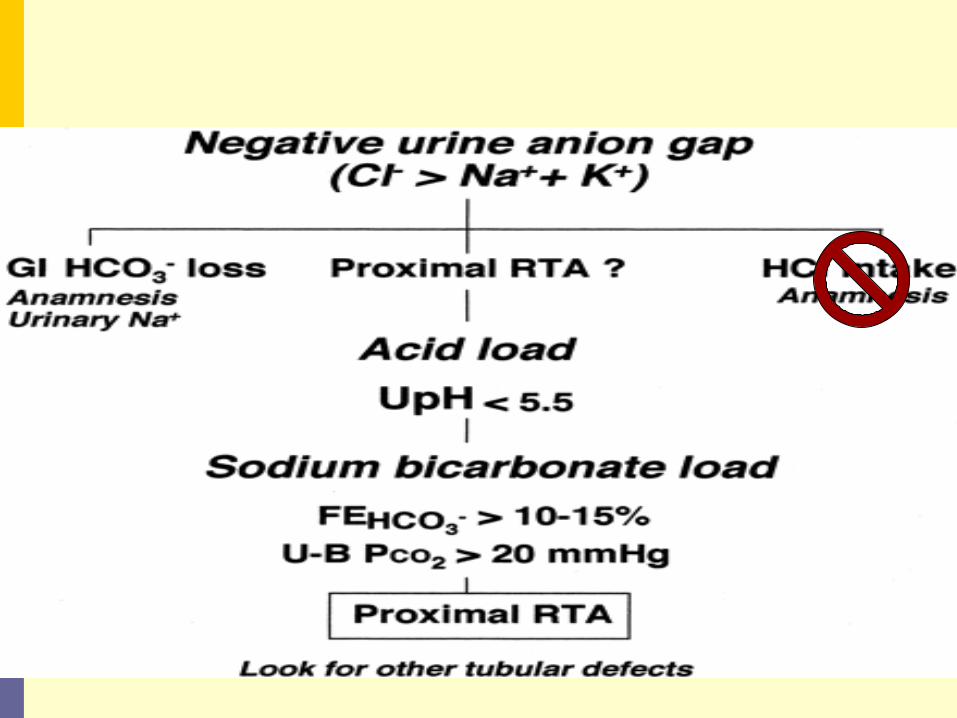
Lab diagnosis of RTA RTA should be suspected when metabolic acidosis is
accompanied by hyperchloremia and a normal plasma anion gap (Na+ - [Cl- + HCO3
-] = 8 to 16 mmol/L) in a patient without evidence of gastrointestinal HCO3
- losses and who is not taking acetazolamide or ingesting exogenous acid.

Functional evaluation of proximal bicarbonate absorption
Fractional excretion of bicarbonate Urine ph monitoring during IV administration of
sodium bicarbonate. FEHCO3 is increased in proximal RTA >15% and is
low in other forms of RTA
(FEHCO3 = fractional excretion of HCO3)

Functional Evaluation of Distal Urinary Acidification and Potassium Secretion
Urine pH Urine anion gap Urine osmolal gap Urine pCO2
TTKG (transtubular potassium gradient) Urinary citrate

Urine ph In humans, the minimum urine pH that can be
achieved is 4.5 to 5.0. Ideally urine ph should be measured in a fresh
morning urine sample. A low urine ph does not ensure normal distal
acidification and vice versa. The urine pH must always be evaluated in
conjunction with the urinary NH4+ content to assess
the distal acidification process adequately . Urine sodium should be known and urine should not
be infected.

Urine Anion Gap
Urine AG = Urine (Na + K - Cl). The urine AG has a negative value in most patients
with a normal AG metabolic acidosis. Patients with renal failure, type 1 (distal) renal
tubular acidosis (RTA), or hypoaldosteronism (type 4 RTA) are unable to excrete ammonium normally. As a result, the urine AG will have a positive value.

There are, however, two settings in which the urine AG cannot be used.
When the patient is volume depleted with a urine sodium concentration below 25 meq/L.
When there is increased excretion of unmeasured anions

Urine osmolal gap
When the urine AG is positive and it is unclear whether increased excretion of unmeasured anions is responsible, the urine ammonium concentration can be estimated from calculation of the urine osmolal gap.
UOG=Uosm - 2 x ([Na + K]) + [urea nitrogen]/2.8 + [glucose]/18.
UOG of >100 represents intact NH4 secretion.
Urine pCO2
Measure of distal acid secretion. In pRTA, unabsorbed HCO3 reacts with secreted H+
ions to form H2CO3 that dissociate slowly to form CO2 in MCT.
Urine-to-blood pCO2 is <20 in pRTA.
Urine-to-blood pCO2 is >20 in distal RTA reflecting impaired ammonium secretion.
TTKG
TTKG is a concentration gradient between the tubular fluid at the end of the cortical collecting tubule and the plasma.
TTKG = [Urine K ÷ (Urine osmolality / Plasma osmolality)] ÷ Plasma K.
Normal value is 8 and above. Value <7 in a hyperkalemic patient indicates
hypoaldosteronism. This formula is relatively accurate as long as the
urine osmolality exceeds that of the plasma urine sodium concentration is above 25 meq/L

Urine citrate The proximal tubule reabsorbs most (70-90%) of the
filtered citrate. Acid-base status plays the most significant role in
citrate excretion. Alkalosis enhances citrate excretion, while acidosis
decreases it. Citrate excretion is impaired by acidosis,
hypokalemia,high–animal protein diet and UTI.

Table - Renal Tubular Acidosis
Primary defect Serum K+
Urine pH
Other Causes
Type 1distal
H+ secretion decreased
Low-nl > 5.5 Renal stones
Autoimmune (SLE, Sjogrens)HypercalciuriaDrugs (Ampho B, Ifosfamide, lithium)Hypergammaglobulinemia
Type 2proximal
HCO3- reab decreased
Low-nl < 5.5, although high initially
Multiple MyelomaAcetazolamideHeavy Metal Poisonings (Lead, Copper, Mercury, Calcium)AmyloidosisDisorders of protein, Carb, AA metabolism
Type 4 Aldosterone deficiency, cation exchange decreased
High < 5.5 Aldosterone deficiencyDiabetic nephropathy SpirinolactoneInterstitial nephritisObstructive uropathyRenal transplant
OBJECTIVES Physiology of Renal acidification. Types of RTA and characteristics Lab diagnosis of RTA Approach to a patient with RTA Treatment

OBJECTIVES Physiology of Renal acidification. Types of RTA and characteristics Lab diagnosis of RTA Approach to a patient with RTA Treatment

Treatment Proximal RTA A mixture of Na+ and K+ salts, preferably citrate, is
preferable. 10 to 15 meq of alkali/kg may be required per day to
stay ahead of urinary losses. Thiazide diuretic may be beneficial if large doses of
alkali are ineffective or not well tolerated. Vit D

Distal RTA Bicarbonate wasting is negligible in adults who can generally
be treated with 1 to 2 meq/kg of sodium citrate or bicarbonate. Sodium citrate tolerated better than sodium bicarb
Potassium citrate, alone or with sodium citrate, is indicated for persistent hypokalemia or for calcium stone disease.
For patients with hyperkalemic distal RTA, high-sodium, low-potassium diet plus a thiazide or loop diuretic if necessary.
Hyperkalemic RTA Treatment and prognosis depends on the underlying
cause. Potassium-retaining drugs should always be
withdrawn.. Fludrocortisone therapy may also be useful in
hyporeninemic hypoaldosteronism, preferably in combination with a loop diuretic such as furosemide to reduce the risk of extracellular fluid volume expansion
Dietary restriction of sodium

Take Home Points Distinguish RTA Types 1, 2 and 4
See Table(slide no. 65) + Some clues: Type 1: renal stones, hypercalciuria, high urine
pH despite metabolic acidosis Type 2: think acetazolamide and bicarbonate
wasting; Fanconi syndrome Type 4: aldosterone deficiency and
hyperkalemia Mainstay of treatment of RTA
Bicarbonate therapy

THANK YOU !