Relation between regional distribution of thallium-201 and myocardial blood flow in normal, acutely...
4
Relation Between Regional Distribution of Thallium-20 1 and Myocardial Blood Flow in Normal, Acutely Ischemic, and Infarcted Myocardium ALAN CHU, MD, ROBERT H. MURDOCK, Jr., MA, and FREDERICK R. COBB, MD Myocardlal localization of thallium-201 was com- pared wlth direct measurements of myocardlal perfusion in normal, acutely lschemic, and recently infarcted myocardlum. Studies were performed in 6 chronically Instrumented dogs that were subjected to myocardlal infarction by occlusion of the proximal left circumflex coronary artery. Four days after myocardial lnfarctlon, thallium-201 and 9 f 1 pm niobium-95labelled mlcrospheres were injected simultaneously after acute left anterior descending coronary arterial occlusion; the animals were killed 5 minutes later and the entire left ventricle was sectioned into 1 to 2 g samples. Regresston analyses between thallium-201 actlvlty and regional myo- cardlal blood flow using all myocardlal samples demonstrated a very close linear relation In each dog; r values were 0.96 or greater, Indicating that the Initial localization of thallium-201 in acutely ischemic and recently infarcted myocardlum as a function of regional blood flow was essentially identical. Consequently, in each dog the regional distribution of thallium-201 closely approximated myocardlal perfusion over a wide range of blood flow and potentially different local metabolic conditions that may be encountered in the clinical use of the isotope. Thallium-201, a biologically active ion, is the most commonly used tracer isotope for evaluating regional myocardial perfusion. Thallium-201 scintigraphy is used to assess transient myocardial ischemia induced by exercise stress1-3; evaluation is commonly required in the presence as well as absence of prior myocardial infarction. Thallium-201 scintigrams have been re- corded serially after acute myocardial infarction as measurements of initial and subsequent dimensions of the ischemic zone (that is, a thallium-201 deficit that decreases on repeat scintigraphy has been interpreted as a decrease in the zone of initial ischemia and conse- quently salvage of ischemic myocardium).495 Optimal assessment of baseline or serial changes, or both, in myocardial perfusion in these different pathologic sit- uations requires that the myocardial localization of an imaging agent be principally determined by regional myocardial perfusion and not by perturbations in cel- lular metabolism which may vary with different con- ditions of reduced blood flow. From the Departments of Cardiology and Radiology, Duke University Medical Center and the Veterans Administration Medical Center, Dur- ham, North Carolina. This work was supported in part by Research Grant HL 18537 from the National Heart, Lung, and Blood Institute, Bethesda, Maryland, and the Medical Research Service of the Veterans Admin- istration Medical Center, Durham, North Carolina. Manuscript received November 23, 1981; revised manuscript received April 12. 1982. ac- cepted April 18, 1982. Address for reprints: Frederick R. Cobb, MD, Division of Cardiology, Veterans Administration Medical Center, 508 Fulton Street, Durham, North Carolina 27705. The objective of the present study was to compare the myocardial localization of thallium-201 with direct measurements of myocardial perfusion by inert non- diffusable microspheres in normal, acutely ischemic, and recently infarcted myocardium. These interven- tions were selected to simulate the different conditions of reduced blood flow and potentially different local myocardial metabolic influences that may be encoun- tered in the clinical use of this isotope. Methods Experimental preparation: Six mongrel dogs weighing 15 to 25 kg were anesthetized intravenously with thiamylal sodium, 30 to 40 mg/kg body weight, and ventilated with a respirator. A left thoractomy was performed in the fourth intercostal space. The circumflex coronary artery was dis- sected free just proximal to the first marginal branch, and the left anterior descending coronary artery was dissected free just distal to the first diagonal branch. An adjustable occluder was loosely positioned around each vessel and stabilized to the fibrous tissue adjacent to the vessel bed. Polyvinyl chloride catheters (outer diameter, 3 mm) were filled with heparin and inserted into the left atrium through the left atria1 appendage and in the ascending aorta through the left internal thoracic artery. The occluders and catheters were tunneled to separate subcutaneous pouches at the base of the neck. The dogs were then allowed to recover from the surgical procedure. Seven to 10 days after recovery from the surgical proce- dure, each dog was sedated with 0.3 to 0.4 mg/kg of morphine sulfate intramuscularly and the circumflex occluder was ex- teriorized from the subcutaneous pouch after lidocaine infil- tration anesthesia. The circumflex coronary artery was per- November 1982 The American Journal of CARDIOLOGY Volume 50 1141
Transcript of Relation between regional distribution of thallium-201 and myocardial blood flow in normal, acutely...

Relation Between Regional Distribution of Thallium-20 1 and Myocardial Blood Flow in Normal, Acutely Ischemic, and Infarcted Myocardium
ALAN CHU, MD, ROBERT H. MURDOCK, Jr., MA, and FREDERICK R. COBB, MD
Myocardlal localization of thallium-201 was com- pared wlth direct measurements of myocardlal perfusion in normal, acutely lschemic, and recently infarcted myocardlum. Studies were performed in 6 chronically Instrumented dogs that were subjected to myocardlal infarction by occlusion of the proximal left circumflex coronary artery. Four days after myocardial lnfarctlon, thallium-201 and 9 f 1 pm niobium-95labelled mlcrospheres were injected simultaneously after acute left anterior descending coronary arterial occlusion; the animals were killed 5 minutes later and the entire left ventricle was sectioned into 1 to 2 g samples. Regresston analyses
between thallium-201 actlvlty and regional myo- cardlal blood flow using all myocardlal samples demonstrated a very close linear relation In each dog; r values were 0.96 or greater, Indicating that the Initial localization of thallium-201 in acutely ischemic and recently infarcted myocardlum as a function of regional blood flow was essentially identical. Consequently, in each dog the regional distribution of thallium-201 closely approximated myocardlal perfusion over a wide range of blood flow and potentially different local metabolic conditions that may be encountered in the clinical use of the isotope.
Thallium-201, a biologically active ion, is the most commonly used tracer isotope for evaluating regional myocardial perfusion. Thallium-201 scintigraphy is used to assess transient myocardial ischemia induced by exercise stress1-3; evaluation is commonly required in the presence as well as absence of prior myocardial infarction. Thallium-201 scintigrams have been re- corded serially after acute myocardial infarction as measurements of initial and subsequent dimensions of the ischemic zone (that is, a thallium-201 deficit that decreases on repeat scintigraphy has been interpreted as a decrease in the zone of initial ischemia and conse- quently salvage of ischemic myocardium).495 Optimal assessment of baseline or serial changes, or both, in myocardial perfusion in these different pathologic sit- uations requires that the myocardial localization of an imaging agent be principally determined by regional myocardial perfusion and not by perturbations in cel- lular metabolism which may vary with different con- ditions of reduced blood flow.
From the Departments of Cardiology and Radiology, Duke University Medical Center and the Veterans Administration Medical Center, Dur- ham, North Carolina. This work was supported in part by Research Grant HL 18537 from the National Heart, Lung, and Blood Institute, Bethesda, Maryland, and the Medical Research Service of the Veterans Admin- istration Medical Center, Durham, North Carolina. Manuscript received November 23, 1981; revised manuscript received April 12. 1982. ac- cepted April 18, 1982.
Address for reprints: Frederick R. Cobb, MD, Division of Cardiology, Veterans Administration Medical Center, 508 Fulton Street, Durham, North Carolina 27705.
The objective of the present study was to compare the myocardial localization of thallium-201 with direct measurements of myocardial perfusion by inert non- diffusable microspheres in normal, acutely ischemic, and recently infarcted myocardium. These interven- tions were selected to simulate the different conditions of reduced blood flow and potentially different local myocardial metabolic influences that may be encoun- tered in the clinical use of this isotope.
Methods
Experimental preparation: Six mongrel dogs weighing 15 to 25 kg were anesthetized intravenously with thiamylal sodium, 30 to 40 mg/kg body weight, and ventilated with a respirator. A left thoractomy was performed in the fourth intercostal space. The circumflex coronary artery was dis- sected free just proximal to the first marginal branch, and the left anterior descending coronary artery was dissected free just distal to the first diagonal branch. An adjustable occluder was loosely positioned around each vessel and stabilized to the fibrous tissue adjacent to the vessel bed. Polyvinyl chloride catheters (outer diameter, 3 mm) were filled with heparin and inserted into the left atrium through the left atria1 appendage and in the ascending aorta through the left internal thoracic artery. The occluders and catheters were tunneled to separate subcutaneous pouches at the base of the neck. The dogs were then allowed to recover from the surgical procedure.
Seven to 10 days after recovery from the surgical proce- dure, each dog was sedated with 0.3 to 0.4 mg/kg of morphine sulfate intramuscularly and the circumflex occluder was ex- teriorized from the subcutaneous pouch after lidocaine infil- tration anesthesia. The circumflex coronary artery was per-
November 1982 The American Journal of CARDIOLOGY Volume 50 1141

THALLIUM-201 AND MYOCARDIAL BLOOD FLOW-CHU ET AL.
manently occluded. Lidocaine, 2 mg/kg, and morphine sulfate, 0.08 to 0.08 mg/kg, were administered intravenously to reduce arrhythmias and to minimize discomfort. The electrocardio- gram was monitored before and after occlusion; proper func- tion of the occluder was verified by elevation of S-T segments and an increase in heart rate after occlusion, and the presence of ventricular arrhythmias 24 hours after occlusion. The dogs were then allowed to recover from the occlusion.
Thallium-201 and microsphere injection: Three to 4 days after infarction, each dog was again sedated with 0.3 to 0.4 mg/kg of morphine sulfate intramuscularly. The pouches were infiltrated with lidocaine and the catheters and the left anterior descending occluder were exteriorized. Each dog was given lidocaine and morphine sulfate intravenously. Blood flow was measured using 9 f 1 pm scandium4’j-labelled mi- crospheres before occlusion to ensure that premature closure of the snare had not occurred and that acute &hernia was subsequently initiated. The left anterior descending coronary artery was then completely occluded. One minute after com- plete occlusion, thallium-201,0.5 mCi, was injected into the left atrium; niobiumg5-labelled microspheres were injected into the left atrium immediately after the thallium-201 in- jection. Serial blood samples were withdrawn from the aortic catheter as previously described 6’ for calculation of regional blood flow. The occlusion was maintained and 5 minutes after injection of thallium-201 each animal was anesthetized rapidly with 40 mg/kg of thiamylal sodium; the heart was fibrillated with potassium chloride solution and immediately extracted and cooled to approximately 5 to 10°C.
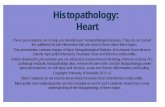
Tissue samples for comparing blood flow and thallium distribution: The heart was immediately prepared for sec- tioning. The right ventricle, atria, aorta, and pericardial fat were removed. The left ventricle was sectioned into 4 transverse layers of approximately equal thickness (Fig. 1); the apical ring was sectioned into 1 anterior and 1 or 2 poste- rior regions; the other rings were sectioned into anterior, an- terior papillary, lateral, posterior papillary, posterior, and septal regions. Each apical region was further sectioned into 3 transmural layers of approximately equal thickness, whereas each of the other regions was sectioned into 4 transmural layers. This procedure generated approximately 80 tissue samples, weighing 0.7 to 2.0 g, for comparison of blood flow and thallium distribution. The samples were placed in scin- tillation vials containing formalin for subsequent histologic processing.
Thallium-201 activity in the tissue sample in each vial was counted with a gamma spectrometer with a 54-100 keV win- dow. The tissue samples and reference blood samples were then recounted for niobium95 and scandium46 activity at op- timal window settings. Background activity and spillover activity were corrected by an appropriate computer program. Flow to each myocardial region was calculated using the fol- lowing standard formula: Qm = Qr X C&/C,, where Qm = myocardial blood flow (ml/min), Qr = reference blood flow (ml/min), C, = count activity in the myocardium, and C, = count activity in the reference blood samples. Myocardial blood flow for each sample was expressed as ml/min per g. Thallium-201 activity was expressed as counta/min per g. The relation of regional myocardial blood flow and thallium-201 distribution was analyzed by linear regression analyses.
Histology: After measurement of tissue radioactivity, the samples were prepared for histologic sectioning as described previously.7 Each tissue sample was sectioned serially with a microtome and 4 histologic sections were taken from dif- ferent depths through each small sample and stained with hematoxylin and eosin. Myocardial infarction was defined as inflammatory cell infiltrate, loss of normal cell architecture, and cellular dissolution. The extent of infarcted myocardium
1
FIGURE 1. Diagram illustrating the technique for sectioning the left ventricle. The atrial tissue and right ventricle were removed as indicated by the stippled and llned areas. The left ventricle was sectioned into 4 transverse rings. Each ring was sectioned into circumferential regions: anterior (A), septai (S), posterior (P), posterior papillary (PP). lateral (L), and anterior papillary (AP). Each circumferential region in rings 1, 2, and 3 was divided into 4 equal epicardial and endocardiai layers.
in each sample was determined with planimetry of histologic infarction in each section using a projection microscope and ultrasonic graph pen.7
Results
Figure 2 illustrates the relation between the regional distribution of thallium-201 and myocardial blood flow as measured by 9 f 1 pm microspheres. Data from all samples are plotted in each dog. In each dog there were myocardial regions in which blood flow was reduced less than 0.10 ml/min per g as a result of acute ischemia as well as of the infarction, initiated 3 days earlier. These data demonstrate a very close linear relation between thallium-201 localization and regional myocardial blood flow; r values were 0.98 or more in each dog. Thus the initial net localization of thallium-201 in acutely ischemic and recently infarcted myocardium as a function of regional blood flow was essentially identical. The y intercepts of each regression equation were slightly above zero. The slight scatter in data points was no greater at low as compared with normal flow ranges. The close linear relation and intercepts that approach zero indicate that net initial localization of thallium-201 closely approximates regional myocardial perfusion over a wide range of blood flow in acutely ischemic and re- cently infarcted myocardium. The differences in slopes resulted from differences in animal weights.
Proximal circumflex arterial occlusion resulted in an average infarct of 28.8% of the left ventricle (range 24 to 35%). The infarction extended to a variable degree of the epicardial surface. In the larger infarcts, infarc- tion in the central ischemic regions extended to the epicardial surface.
1142 November 1982 The American Journal of CARDIOLOGY Volume 50

THALLIUM-201 AND MYOCARDIAL BLOOD FLOW-CHU ET AL.
FIGURE 2. Relation between thal- lium-201 activity and myocardial blood flow in 6 dogs. Closed squares represent samples with greater than 5 % histologic infarc- tion.
0.40 080 1 20 I 60 200 040 080 120 1.60 2.00
MYOCARDIAL BLOOD FLOW, ml/min/g
Discussion
Possible limitation of thallium-201 for assessing myocardial perfusion during acute ischemia: Op- timal scintigraphic assessment of myocardial perfusion in the clinical situations associated with coronary heart disease requires that myocardial localization of the imaging agent be a direct function of tissue perfusion over a wide range of reduced and increased blood flow, and variable local metabolic condition. Studies have suggested that the biologically active tracer ions such as potassium, rubidium, and thallium, which are ex- tracted by the myocardial cell, have certain limitations as agents for accurately assessing myocardial perfusion during the variable metabolic conditions that may ac- company acute or prolonged ischemia or evolving myocardial infarction, or both. Weich et aL8 observed
that the extraction fraction of thallium-201 remained constant when myocardial blood flow was altered by changing myocardial metabolic demands, but decreased when blood flow was increased in excess of metabolic demands or during systemic hypoxia or acidosis. Becker et a1.g found a disproportionately high rubidium-86 content at very low flow rates as compared with mea- surements with nondiffusable inert microspheres. Di- Cola et al.1° reported a close linear correlation between the distribution of thallium-201 and blood flow mea- sured with microspheres in transmural myocardial sections 24 hours after coronary arterial occlusion. However, when the transmural samples were divided into epicardial and endocardial halves, there was a poor correlation between thallium-201 and microsphere distribution in the latter samples. The poor correlation in endocardial samples results from disproportionately
November 1992 The American Journal of CARDIOLOGY Volume 50 1143

THALLIUM-201 AND MYOCARDIAL BLOOD FLOW-CHU ET AL.
high thallium activity when blood flow was reduced less than 30% of normal.
Strauss et al.ll reported a close linear correlation between regional blood flow determined with micro- spheres and thallium-201 distribution after acute cor- onary occlusion; thallium-201 underestimated blood flow when measurements were made during the reactive hyperemic phase after transient ischemia. In studies from our laboratory,12 the regional distribution of thallium-201 and myocardial blood flow by micro- spheres was determined in dogs subjected to treadmill exercise and acute ischemia. We observed a very close linear correlation between thallium-201 localization and regional blood flow over a wide range of blood flow; in each dog blood flow was reduced to less than 0.1 ml/g per min in the ischemic region and increased 3.3 to 7.2 times resting blood flow in the nonischemic region; linear correlation coefficients were 0.98 or more in each dog.
Thallium-201 distribution in normal, ischemic, and infarcted myocardium: The purpose of the present study was to compare the initial myocardial localization of thallium-201 with simultaneous direct measurements of myocardial perfusion in normal, acutely ischemic, and recently infarcted myocardium. These conditions were chosen to simulate the poten- tially different pathologic conditions of reduced flow that may be encountered in the clinical use of thal- lium-201. Three to 4 days after initiation of infarction in the circumflex region, acute ischemia was produced in regions of the left anterior descending coronary ar- tery. The 3 to 4 day period after acute myocardial in- farction was selected to allow completion of the acute infarction process; at this interval the region subjected to prolonged ischemia was sharply delineated into in- farcted and noninfarcted myocardium. The nonin- farcted tissue was indistinguishable by routine histo- logic stains from tissue that had not been subjected to ischemia. Because substantial increases in collateral flow occur in the early days after acute coronary occlu- sion13 the myocardium, which has been subjected to prolonged ischemia but which has not developed in- farction, may no longer be subjected to ischemia. Thus, in samples with a mixture of normal and infarcted tissue it was not possible in the present study to determine whether blood flow to the normal tissue was normal or reduced. Although local metabolic conditions were not measured in the present study, it is possible that met- abolic conditions of myocardial cells that have been subjected to no ischemia, acute ischemia, or prolonged ischemia but no infarction are different.
The results of our study demonstrate essentially identical localization of thallium-201 in these different regions when compared with direct measurements of blood flow by nondiffusable inert microspheres. These data indicate that regional myocardial perfusion is the principal determinant of initial localization of thal- lium-201 in each of the zones studied. Because the linear correlation coefficients approximated 1.0 and the in- tercepts of the regression equation were only slightly above zero in each dog, the data indicate that localiza- tion of thallium-201 very closely approximated regional
perfusion over the entire range of myocardial blood flow. These data suggest that, compared with regional blood flow, the local metabolic conditions that may differ in normal and acutely ischemic myocardium and in regions containing recently infarcted myocardial tissue have inconsequential effects on initial thallium localiza- tion.
In the present study the animals were killed 5 minutes after thallium-201 and microsphere injection. Schwartz et a1.l4 reported that the myocardial extraction of thallium-201 may become negative approximately 10 minutes after injection, suggesting early loss of the ion from the normal myocardium. Schwartz,14 Pohost,15 and their co-workers described early redistribution of thallium-201 to the ischemic region early after relief of ischemia. Thus, although the initial localization of thallium-201 may be closely related to regional perfu- sion over a wide range of blood flow and differing met- abolic conditions, distribution at later intervals may not accurately reflect perfusion in either normal or ischemic myocardium or regions containing infarcted myocar- dium. These studies emphasize the need for early thallium scintigraphy after intravenous injection for optimal assessment of regional myocardial perfusion.
Acknowledgment
We acknowledge the technical assistance of Marjorie Grubb, the surgical assistance of Eric Fields and Kirby Coo- per, the illustrative assistance of Medical Media Production Service of the Veterans Administration Medical Center, and the secretarial assistance of Cathie Collins.
References
1.
2.
3.
4.
5.
6.
7.
6.
9.
10.
11.
12.
13.
14.
15.
Bailey IK, Grlfflth LSC, Rouleau J, Strauss HW, Pitt B. Thallium-201 myocardial perfusion imaging at rest and during exercise: comparative sensitivity to electrocardiography in coronary artery disease. Circulation 1978;55:79-07. Mof_au@ffn PR, Marlin RO, Doherty P, et al. Reproducibility of thallium201 myocardial imaging. Circulation 1977;55:497-503. Rltchls JL, Trobaugh GB, Hamllton GW, et al. Myocardial imaging with thallium-201 at rest and during exercise: comparison with coronary arte- riography and resting and stress electrocardiography. Circulation 1977;’ 56166-71. Wackers FJTh, Busemann SE, Samson 0, et al. Valve and limitations of thallium-201 scinti raphy in the awake phase of myocardial infarction. N Engl J Med 8 1976;2 5:1-5. Becker LC, Bulkley BH, Pitt B, et al. Enhanced reduction of thallium-201 in acute myocardial infarction by nitroglycerin treatment: initial results of a prospective trial (abstr). Clin Res 1978:26:219A. Cobb FR, Bathe RJ, Greenlleld JC Jr. Regional myocardial blood flow in awake dogs. J Clin Invest 1974;53:1618-1625, Cobb FR, Bathe RJ, Rlvas F, Greenfield JC Jr. Local effects of acute cellular iniurv on reaional mvocardlal blood flow. J Clin Invest 1976;57: 1359-1368: - . Welch HF, Strauss HW, Pitt B. The extraction of thallium-201 by the myocardium. Circulation 1977;56:186-191. Becker L, Ferrelra R, Thomas M. Comparison of %b and microsphere x~!s$~s of left ventricular blood flow distribution. J Nucl Med 1974:15: “I”-“. _.
DlCola VC, Dow&g SE, Donabedlan RK, Zaret BL. Pathophysiologlcal correlates of thallium-201 myocardial uptake in experimental infarction. CardiovascRes 1977;11:141-146. Strauss HW. Ha&on K. Lanaan JK. Lebowitz E. Pitt HB. Thallium-201 for myocardiil imaging: r&at&hip oi thallium20i to regional myocardial perfusion. Circulation 1975;51:641-645. Nfataen AP, Morris KG, Yurdock R, BNM FP, Cobb FR. Linear relationship betwaen the distribution of thallium-201 and blood flow in ischemic and nonischemic myocardium during exercise. Circulation 1980:61:797- 601. Rlvas F, Cobb FR, Bathe RJ, Grwnftald JC Jr. Relationship between bleed flow to ischemic regions and extent of myocardial infarction: serial mea- surements of blood flow to ischemic regions. Circ Res 1976;38:439- 447. Schwartz JS, Pento R, Carlyle P, Forstrom L, Cohn JN. Early redistribution of thallium-201 after temporary ischemia. Circulation 1978;57:332-335. Pohost GM, Zlr LM, Moore RH, McKuslck KA, Gulney TE, Belier GA. Dif- ferentiation of transiently ischemic from infarcted myocardium by serial imaging after a single dose of thallium-201. Circulation 1977;55:294- 302.
1144 November 1992 The American Journal of CARDIOLOGY Volume 50