(Relates to Chapter 11, “Palliative Care at End of Life,” in the textbook) Copyright © 2011,...
113
(Relates to Chapter 11, “Palliative Care at End of Life,” in the textbook) Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
-
Upload
collin-pope -
Category
Documents
-
view
219 -
download
0
Transcript of (Relates to Chapter 11, “Palliative Care at End of Life,” in the textbook) Copyright © 2011,...

(Relates to Chapter 11, “Palliative Care at End of Life,”in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

2
•Any form of care or treatment that focuses on reducing the severity of disease symptoms, rather than trying to delay or reverse the progression of the disease itself or provide a cure
• Includes hospice, end-of-life care, and bereavement
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
3
•Overall goals Prevent and relieve suffering Improve quality of life for patients with serious, life-limiting illnesses
•Initiated after a person receives a diagnosis of a life-limiting illness
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

4
•Ideally, involves interdisciplinary team Physicians Social workers Pharmacists Nurses Chaplains Other health care professionals
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

5
• Concept of care that provides compassion, concern, and support for the dying and their families
• Exists to provide support and care for persons in last phases of incurable diseases
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

6
•Approximately 1½ million patients receive hospice services each year.
•Organized under a variety of models Hospital-based, part of existing
home health care agencies, free-standing, or community-based
•Emphasizes palliative rather than curative care
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

7
•Care is provided in a variety of locations.
•Can be part-time, intermittent, on-call, regularly scheduled, or continuous basis
•Services are available 24 hours a day, 7 days a week.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

8
•Medically supervised interdisciplinary team of professionals and volunteers
•Hospice nurse is an integral part. Pivotal role in coordination of hospice team
Educated in pain control and symptom management
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

9
•To begin hospice is a difficult decision. Lack of information about hospice care
Physician may view decline as personal failure.
Patients or family may see it as giving up.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
10
•Admission has two criteria: Patient must desire services.
▪ Must agree that curative care can be used to treat the terminal illness
Physicians must certify that patient has 6 months or less to live.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

11
A patient with advanced cancer is referred for hospice care. The nurse explains to the patient and the family that the goal of hospice care differs from the goal of traditional care in that hospice care1. Provides for more complete pain control.2. Focuses on helping the patient and family prepare for death.3. More readily recognizes advance directives related to “right to die.”4. Is delivered in the home and does not rely on the technology of hospitals.
Audience Response Questions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

12
The hospice nurse identifies an abnormal grief reaction in the wife of a dying patient who says,1. “I don’t think that I can live without my husband to take care of me.”2. “I wonder if expressing my sadness makes my husband feel worse.”3. “We have shared so much that it is hard to realize that I will be alone.”4. “I don’t feel guilty about leaving him to go to lunch with my friends.”
Audience Response Questions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

13
•Occurs when all vital organs and body systems cease to function
•Irreversible cessation of cardiovascular, respiratory, and brain function
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

14
• An irreversible loss of all brain functions, including the brainstem
• A clinical diagnosis that can be made in patients whose hearts continue to beat and who are maintained on mechanical ventilation in the ICU
• Cerebral cortex stops functioning or is irreversibly damaged.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
15
•Controversies have arisen related to an exact definition of death.
•Currently, legal and medical standards require that all brain function must cease for brain death to be pronounced and life support to be disconnected by the physician.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

16
•Generally refers to the final phase of a patient’s illness, when death is imminent
•The time from diagnosis of a terminal illness to death varies considerably, depending on the patient’s diagnosis and extent of disease.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

17
•In some cases, it is obvious to health care providers that the patient is in this phase.
•In other cases, they may be uncertain whether the end is close at hand.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

18
•Term used for issues related to death and dying, as well as for services provided to address these issues
•Focuses on physical and psychosocial needs of the patient and the patient’s family
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

19
•Goals Provide comfort and supportive care during dying process
Improve quality of remaining life
Help ensure a dignified death Provide emotional support to the family
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

20
•Metabolism is decreased. •Body gradually slows down
until all function ends.•Respiration generally ceases
first. Heart stops beating within a few minutes.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

21
• Hearing is usually last sense to disappear.
•Decreased sensation•Decreased perception of pain
and touch
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

22
•Blurring of vision•Blink reflex absent•Patient appears to stare.•Decreased sense of taste and
smell
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
23
•Mottling on hands, feet, arms, and legs
•Cold or clammy skin•Cyanosis on nose, nail beds,
or knees•“Waxlike” skin when very
near death
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

24
•Irregular breathing•Cheyne-Stokes respiration •Inability to cough or clear
secretions Grunting, gurgling, or noisy congested breathing (“death rattle”)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

25
•Gradual decrease in urinary output
•Incontinent of urine•Unable to urinate
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

26
•Slowing of digestive tract and possible cessation of function
•Accumulation of gas•Distention and nausea •Loss of sphincter control•Bowel movement may occur
before imminent death or at the time of death.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

27
•Gradual loss of ability to move
• Loss of facial muscle tone Sagging of jaw Difficulty speaking Swallowing can become more difficult.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

28
•Difficulty maintaining body posture and alignment
•Loss of gag reflex •Jerking seen in patients on
large amounts of opioids
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

29
•Decreased heart rate Later slowing and weakening of
pulse • Irregular rhythm•Decreased blood pressure•Delayed absorption of drugs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

30
•Altered decision making•Anxiety about unfinished
business•Decreased socialization•Fear of loneliness•Fear of meaninglessness•Fear of pain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

31
•Helplessness•Life review•Peacefulness•Restlessness•Saying goodbyes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

32
•Unusual communication•Vision-like experiences•Withdrawal
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
33
•Bereavement is the period of time following the death of a loved one during which grief is experienced and mourning occurs.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

34
•Grief is the normal process of reacting to loss or adapting to change.
•Dynamic process•Includes both psychologic
and physiologic responses following a loss
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
35
•Manifested in a variety of ways Feelings Behaviors Thoughts Physical manifestations
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

36
•Intensity of grief is driven by Individual’s personality Nature of the relationship with the dying person
Concurrent life crises Coping resources Availability of support systems Cultural beliefs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
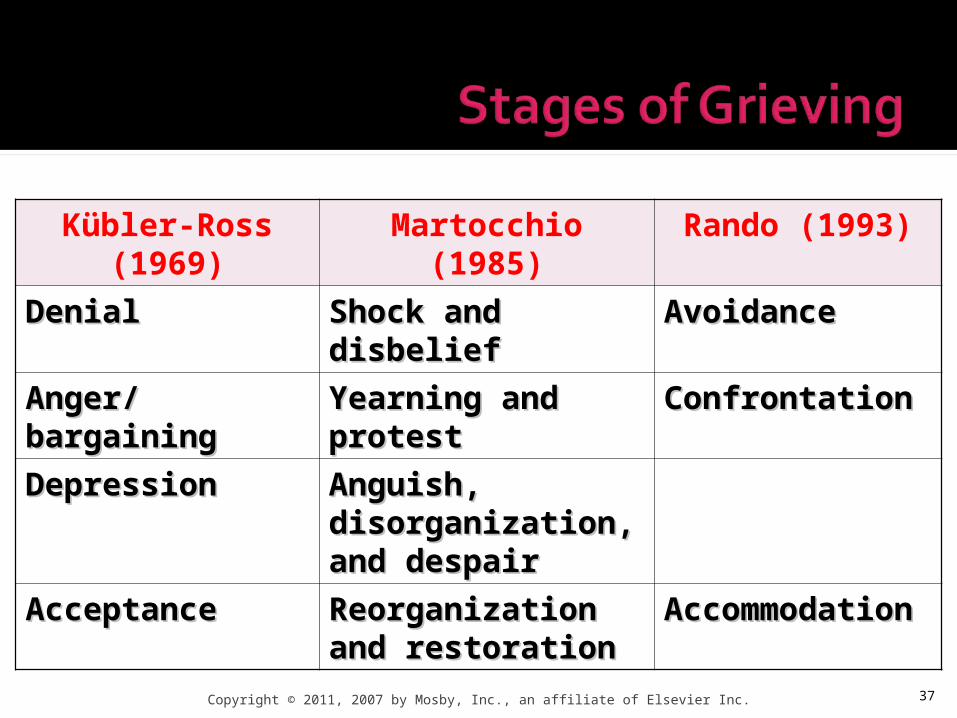
Kübler-Ross (1969) Martocchio (1985) Rando (1993)
DenialDenial Shock and disbelief Shock and disbelief AvoidanceAvoidance
Anger/bargainingAnger/bargaining Yearning and protestYearning and protest ConfrontationConfrontation
DepressionDepression Anguish, Anguish, disorganization, and disorganization, and despairdespair
AcceptanceAcceptance Reorganization and Reorganization and restorationrestoration
Accommodation Accommodation
37Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

38
•Adaptive grief Healthy response Grief that assists the person in accepting the reality of death
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
39
•Prolonged grief disorder Prolonged and intense mourning
Denial of the loss for longer than 6 months
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
40
•Goals for the grief process Resolving emotions Reflecting on the dying person Expressing feelings of loss and sadness
Valuing what has been shared
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

41
•Patient also experiences grief.•Goals for grief resolution include
Patient expression of feelings related to grief
Acknowledgment of the impending loss
Demonstration of behaviors that reflect progress in grief resolution
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

42
•Spiritual needs do not necessarily equate to religion.
•At the end of life, many patients question their beliefs about a higher power, their own journey through life, religion, and an afterlife.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

43
•Deep-seated spiritual beliefs may surface for some patients when they deal with their terminal diagnosis and related issues.
•Spiritual distress may occur.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

44
•Cultural beliefs affect a person’s understanding of and reaction to death or loss.
•In some cultural/ethnic groups, death and dying are private matters shared only with significant others. Often feelings are repressed or internalized.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

45
•Other cultural groups, such as African Americans and Hispanic/Latinos, may express their feelings and emotions easily.
•In such cultures, family members, both immediate and extended, provide support for one another.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

46
•Families with non–English-speaking members are at risk for receiving less information about their family member’s critical illness and prognosis.
•Cultural variations in symptom expression (e.g., pain expression) and use of health care services also exist.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

47
• Nursing assessment of beliefs and preferences should be made on an individual basis.
• Avoids stereotyping individuals with different cultural belief systems
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

48
•Outcomes related to care based on patient’s wishes Organ and tissue donations Advance directives
▪ Medical power of attorney or living wills
Resuscitation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

49
•Advance directives Written statements of medical care wishes
•Directive to physicians Patient’s desire to accept or deny treatment
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

50
•Do not resuscitate (DNR) Order instructing health care providers not to attempt CPR
Variety of CPR decisions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
51
•Withholding or withdrawing treatment must be included in an advance directive.
•What is to be done and what is not to be done must be included in clear terms.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

52
•Euthanasia is the deliberate act of hastening death.
•The ANA statement on active euthanasia states that the nurse should not participate in active euthanasia.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
53
•Holistic Psychosocial and physical needs
•Focuses on Psychosocial manifestations Grieving process Physical changes associated with dying
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

54
•Varies with Patient condition Proximity of approaching death
•Limited to essential data•Document specific change
that brought patient into health care agency
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
55
•If patient is alert Brief review of body systems to detect signs and symptoms
Assess for discomfort, pain, nausea, or dyspnea.
•Assess coping abilities of patient and family.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

56
•Functional assessment of activities of daily living Patient’s abilities Food and fluid intake Patterns of sleep and rest Response to the stress of terminal illness
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

57
•Frequency of assessment depends on stability, but it is done at least every 8 hours. As changes occur, assessment and documentation need to be done more frequently.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

58
•As death approaches, neurologic assessment is important. Level of consciousness Presence of reflexes Pupil responses
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

59
•Evaluate and monitor Circulation changes
▪ Vital signs, skin color, and temperature
Respiratory status▪ Character and pattern of respirations
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

60
•Evaluate and monitor (cont’d) Gastrointestinal/renal functioning▪ Nutritional/fluid intake, urinary output, and bowel function
Skin condition▪ Fragile: Note breakdown
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

61
•Be sensitive.•Assess patient frequently
(but not unnecessarily). Use health history data available in chart.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

62
•Acute confusion•Chronic confusion•Compromised family coping•Death anxiety•Disturbed thought processes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

63
•Fear•Grieving•Hopelessness•Impaired religiosity•Impaired social interaction
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

64
•Impaired verbal communication
•Ineffective coping•Ineffective denial•Interrupted family processes•Insomnia
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
65
•Readiness for enhanced spiritual well-being
•Risk for loneliness•Social isolation•Spiritual distress
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

66
•Acute pain•Bowel incontinence•Chronic pain•Constipation•Decreased cardiac output•Diarrhea
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

67
•Fatigue•Imbalanced nutrition: less
than body requirements•Impaired bed mobility•Impaired comfort•Impaired gas exchange•Impaired oral mucous
membrane
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

68
•Impaired physical mobility•Impaired skin integrity•Impaired swallowing•Impaired tissue integrity•Impaired urinary elimination•Ineffective airway clearance
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

69
•Ineffective breathing pattern•Ineffective thermoregulation•Ineffective tissue perfusion•Nausea•Risk for aspiration•Risk for infection
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

70
• Risk for injury• Self-care deficit• Total urinary incontinence
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

71
•Coordination of care focus Patient’s needs Family and significant other’s needs
Education, counseling, advocacy, and support
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

72
•Nursing goals Center on patient’s abilities to express and share feelings with others
Involve comfort measures and physical maintenance care
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
73
•Education Ongoing information about the disease
Dying process Any care provided How to cope
•Denial and grieving may be barriers to patient’s learning.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
74
•Uneasy feeling caused by a source not easily identified
•Frequently related to fear•Management
Pharmacologic or nonpharmacologic interventions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

75
•Causes Uncontrolled pain, psychosocial
factors from disease process or impending death, altered physiologic states, drugs used in increasing doses
•Management Encouragement, support, and
education
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

76
•The surviving family members may be angry with the dying loved one who is leaving them.
•Nurses are sometimes the target of the anger and must understand what is happening and not react on a personal level.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

77
•Common emotions at the end of life
•You need to encourage realistic hope within the limits of the situation.
•Decision making about care can foster a sense of power and control for the patient.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

78
•Four specific fears Pain Shortness of breath Loneliness and abandonment Meaninglessness
•Management Coping strategies
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

79
•Tendency to associate death with pain
•Physiologically: No indication that death is always painful
•Psychologically: Pain may occur based on anxieties or separations related to dying
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
80
•Terminally ill patients experiencing pain should have pain-relieving drugs available.
•Most patients want their pain relieved without the side effects of grogginess or sleepiness. Do not want to be deprived of
ability to interact with others
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

81
•The sensation of air hunger results in anxiety for the patient and family members.
•Current therapies involve the use of opioids, bronchodilators, and oxygen, depending on the cause of the dyspnea.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

82
•Do not want to be alone•Worry loved ones cannot
cope and will abandon them•Want someone they know
and trust to stay Loved one or caregiver provides comfort and support.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

83
•High-quality nursing responses Holding hands, touching, and listening
•Simply providing companionship allows a sense of security.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

84
•Leads most to review their lives Intentions during life and examining actions
Expressing regret Helps recognize life’s value
•Worth needs to be expressed
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

85
•Nurse can assist patients and their families in identifying positive qualities of patient’s life.
•Respect and accept practices or rituals associated with patient’s life review without being judgmental.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

86
•Therapeutic communication is important nursing intervention.
•Use empathy and active listening.
•Allow patients and families time to express their feelings and thoughts.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

87
•Silence is OK.•Listening to the silence
sends a message of acceptance and comfort.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

88
•Unusual communication by patient may take place at end of life. Confused, disoriented, or garbled
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

89
•Patients may speak To or about family members or others who have died before them
To give instructions to those who survive them
To speak of projects yet to be completed
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

90
•Active, careful listening allows identification of specific patterns in patient’s communication. Increased risk for inappropriate labeling of behaviors
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

91
•Symptom management•Priority is to meet
physiologic and safety needs.
•Deserve same care as people who are expected to recover
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

92
•Needs Oxygen Nutrition Pain relief Mobility Elimination Skin care
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

93
•After patient is pronounced dead, the nurse prepares or delegates preparation of the body for immediate viewing by the family.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

94
•Considerations when preparing body Cultural customs In accordance with state law Agency policies and procedures
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

95
•Considerations when preparing body Close the patient’s eyes. Replace dentures. Wash the body as needed.
▪ Place pads under perineum. Remove tubes and dressings. Straighten body.
▪ Leave pillow to support head.Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

96
•Family should be allowed privacy and as much as time as they need with the deceased person.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

97
•Unexpected or unanticipated death Preparation of the body for viewing or release to a funeral home depends on state law and agency policies and procedures.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

98
•Role of caregiver includes Working and communicating with the patient
Supporting concerns Helping resolve any unfinished business
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

99
•Role of caregiver includes (cont’d) Working with family members and friends
Dealing with own needs and feelings
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

100
•Recognizing signs and behaviors among family members who may be at risk for dysfunctional grief reactions is an important nursing intervention.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

101
•Risk for dysfunctional grief Dependency Negative feelings about the dying person
Inability to express feelings Concurrent life crises History of depression
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

102
•Risk for dysfunctional grief (cont’d) Difficult reactions to previous losses
Perceived lack of social or family support
Low self-esteem Multiple previous bereavements Alcoholism Substance abuse
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

103
•Encouragement to continue their usual activities
•Discuss their activities and maintain some control over their lives
•Discuss what can and cannot change
•Encouragement to take care of themselves
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

104
•Many nurses who care for dying patients are passionate about providing quality EOL care.
•Caring for dying patients is intense and emotionally charged.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

105
•Common for nurse to feel helpless and powerless when dealing with death. Feelings of sorrow, guilt, and frustration need to be expressed.
Should be aware of how these feelings affect them
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

106
•Recognize and acknowledge what can and cannot be controlled.
•Recognize personal feelings to allow openness.
•Okay to cry with the patient or family during the grieving process
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 107

108
•78-year-old man has stage IV lung cancer with metastasis to liver, pancreas, and stomach.
•No treatments were successful.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

•Patient has completed a directive to physicians: Stated not to initiate life-prolonging measures
109Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
•Patient admitted to ICU through ED for respiratory distress Placed on ventilator and sedated
•Spouse is fearful and requests all measures to prolong life.
110Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

111
•Multidisciplinary team scheduled to meet with spouse to discuss plan of care
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

1.How might you assess the spouse’s understanding of the situation?
2.What complications from the disease process might he encounter? How can you minimize these?
112Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

113
3. What psychosocial issues should be addressed?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.