Reinaldo Rosario, MD-presentation
59
CHRONIC KIDNEY DISEASE CHRONIC KIDNEY DISEASE Reinaldo Rosario MD, FASN Reinaldo Rosario MD, FASN Renal Electrolyte & Renal Electrolyte & Hypertension Consultants Hypertension Consultants (REHC) (REHC)
Transcript of Reinaldo Rosario, MD-presentation

CHRONIC KIDNEY CHRONIC KIDNEY DISEASEDISEASE
Reinaldo Rosario MD, FASNReinaldo Rosario MD, FASN
Renal Electrolyte & Hypertension Renal Electrolyte & Hypertension Consultants (REHC)Consultants (REHC)

NATURAL HISTORY OF RENAL NATURAL HISTORY OF RENAL DISEASEDISEASE
Initial injury to the kidney Initial injury to the kidney Adaptive hyperfiltrationAdaptive hyperfiltrationLong-term damage to the remaining nephrons – Long-term damage to the remaining nephrons – proteinuria and progressive renal insufficiencyproteinuria and progressive renal insufficiencyAdvanced renal disease dysfunction – volume Advanced renal disease dysfunction – volume overload, hyperkalemia, metabolic acidosis, overload, hyperkalemia, metabolic acidosis, HTN, anemia and bone diseaseHTN, anemia and bone diseaseEnd Stage Renal Disease (ESRD)End Stage Renal Disease (ESRD)

CKD - DEFINITIONCKD - DEFINITION
Evidence Evidence of structural or functional kidney of structural or functional kidney abnormalities that persists for at least ≥3 abnormalities that persists for at least ≥3 months, with or without a decreased GFR.months, with or without a decreased GFR.GFR GFR <60 mL/min/1.73m² for ≥3 months, <60 mL/min/1.73m² for ≥3 months, with or without kidney damagewith or without kidney damagePrevalence 4.7% or 8.3 millionPrevalence 4.7% or 8.3 million
NKF. Am J Kidney Dis. 2002;39(supp1):S1NKF. Am J Kidney Dis. 2002;39(supp1):S1

STAGES OF CHRONIC KIDNEY STAGES OF CHRONIC KIDNEY DISEASEDISEASE
Stage Description GFR (mL/min/1.73m²)
I Kidney Damage with normal or increased GFR
>90
II Kidney Damage with mildly decrease GFR
60-89
III Moderately decreased GFR
30-59
IV Severely decreased GFR
15-29
V Kidney Failure <15

PREVALENCE OF CKDPREVALENCE OF CKD
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
7,000,000
8,000,000
>90 60-89 30-59 15-29 <15
GFR (ml/min/1.73m2)
NKF. Am J Kidney Dis. 2002;39(supp 1):S1NKF. Am J Kidney Dis. 2002;39(supp 1):S1

ESRDESRD
As of Dec. 31 2006 506,256 dialysis ptsAs of Dec. 31 2006 506,256 dialysis ptsIn 2006 alone, 110,854 pts entered the In 2006 alone, 110,854 pts entered the ESRD programESRD programMedicare expenditure - $22.7 billion in 2006Medicare expenditure - $22.7 billion in 2006Projected number of ESRD pts by 2010 – Projected number of ESRD pts by 2010 – 651,330 and Medicare cost in excess of $28 651,330 and Medicare cost in excess of $28 billion dollarsbillion dollars
U.S. Renal Data System: USRDS 2006U.S. Renal Data System: USRDS 2006

ESRDESRD
Annual mortality rate for all ESRD pts on treatment is Annual mortality rate for all ESRD pts on treatment is 20-fold higher than the general population20-fold higher than the general populationAt age 45 life expectancy: At age 45 life expectancy: - - General population: General population:
34.7 years 34.7 years - ESRD: - ESRD: 6.2 years on dialysis / 19.5 years 6.2 years on dialysis / 19.5 years
with a functioning kidney graftwith a functioning kidney graft
U.S. Renal Data System: USRDS 2002U.S. Renal Data System: USRDS 2002

CAUSES OF DEATH IN ESRDCAUSES OF DEATH IN ESRD
39%
5%26%
11%
15%4%
Cardiac
Cerebrovascular
Other known
Unknown
Infection
Malignancy
U.S. Renal Data System: USRDS 2002U.S. Renal Data System: USRDS 2002

MULTIPLE RISK FACTORS FOR CKDMULTIPLE RISK FACTORS FOR CKD
DiabetesDiabetes
HypertensionHypertension
Autoimmune diseaseAutoimmune disease
Systemic infectionsSystemic infections
Exposure to drugs Exposure to drugs associated with acute associated with acute decline in kidney functiondecline in kidney function
Recovery from acute Recovery from acute kidney failurekidney failure
NKF. Am J Kidney Dis. 2002;39:S46NKF. Am J Kidney Dis. 2002;39:S46
Pinto-Sietsma. Ann Intern Med. 2000;133:585Pinto-Sietsma. Ann Intern Med. 2000;133:585
Older ageOlder age
Family history of kidney Family history of kidney diseasedisease
Reduced kidney massReduced kidney mass
Racial/ethnic backgroundRacial/ethnic background
SmokingSmoking

EVALUATING PATIENTS AT RISK EVALUATING PATIENTS AT RISK FOR CKDFOR CKD
Evaluating risk factors and identifying GFR Evaluating risk factors and identifying GFR declines are essential to the prompt and declines are essential to the prompt and appropriate management of CKDappropriate management of CKD
GFR or age/weight-sensitive eGFRGFR or age/weight-sensitive eGFR
Blood pressureBlood pressure
GlucoseGlucose
UrinalysisUrinalysis
Microalbuminuria/proteinuriaMicroalbuminuria/proteinuria

COMORBIDITIES AND COMORBIDITIES AND COMPLICATIONS OF CKDCOMPLICATIONS OF CKD
AnemiaAnemia
HypertensionHypertension
Cardiovascular Cardiovascular diseasedisease
DiabetesDiabetes
Osteodystrophy Osteodystrophy
Malnutrition Malnutrition
Metabolic acidosisMetabolic acidosis
DyslipidemiaDyslipidemia
Deficits in functioning Deficits in functioning and well-beingand well-being
Zabetakis. Am J Kidney Dis. 2000;36(suppl 3):S31Zabetakis. Am J Kidney Dis. 2000;36(suppl 3):S31
NKF. Am J Kidney Dis. 2002;39:S17NKF. Am J Kidney Dis. 2002;39:S17

DELAYED DIAGNOSIS OF CKD LEADS TO DELAYED DIAGNOSIS OF CKD LEADS TO
UNDERUSE OF INTERVENTIONSUNDERUSE OF INTERVENTIONS
Lack of interventions to treat HTN, CVD, Lack of interventions to treat HTN, CVD, DM, anemia, and malnutritionDM, anemia, and malnutrition
Under use and delayed consultations with Under use and delayed consultations with nephrologists, cardiovascular specialists, nephrologists, cardiovascular specialists, or dietitiansor dietitians
Lack of patient educationLack of patient education
Lack of a permanent vascular access at Lack of a permanent vascular access at initiation of hemodialysisinitiation of hemodialysis

OPTIMAL CKD PATIENT CAREOPTIMAL CKD PATIENT CARE
Early detection of CKDEarly detection of CKD
Delay Delay Prevent Prevent Treat Treat Prepare Prepare progression complicationsprogression complications comorbidities comorbidities or RRTor RRT
ACE inhibitorsACE inhibitors Anemia Cardiac disease Anemia Cardiac disease Educate patient Educate patient
BP control MalnutritionBP control Malnutrition Vascular disease Vascular disease Select RRT Select RRT modality modality
Blood sugar OsteodystrophyBlood sugar Osteodystrophy Diabetes Create access Diabetes Create access controlcontrol and initiate and initiate
AcidosisAcidosis dialysis in a dialysis in a ProteinProtein timely fashion timely fashion restriction? restriction?
Pereira. Kidney International. 2000;57:351Pereira. Kidney International. 2000;57:351

MANAGEMENT OF PATIENTS WITH MANAGEMENT OF PATIENTS WITH CKDCKD
Blood pressure controlBlood pressure controlDiabetes controlDiabetes controlCardiovascular disease managementCardiovascular disease managementAnemia managementAnemia managementIron managementIron managementVitamin D and vital bone protectionVitamin D and vital bone protectionEating well and exerciseEating well and exerciseAccess planningAccess planning

CARDIOVASCULAR RISK AND GFRCARDIOVASCULAR RISK AND GFR
0
5
10
15
20
25
30
35
Ag
e-s
tan
dari
zed
rate
of
CV
even
ts (
per
100
pers
on
s/y
ear)
>60 45-59 30-44 15-29 <15
GFR (ml/min/1.73m2)
Go AS. N Engl J Med 2004;351:1300Go AS. N Engl J Med 2004;351:1300

CARDIOVASCULAR MORTALITY CARDIOVASCULAR MORTALITY AND HYPERTENSIONAND HYPERTENSION
0
1
2
3
4
5
6
7C
ard
iovascu
lar
Mo
rtali
ty R
isk
115/75 135/85 155/95 175/105
Systolic/Diastolic Blood Pressure (mm Hg)
Lewington S . Lancet 2002; 360: 1903-13.Lewington S . Lancet 2002; 360: 1903-13.

PREVALENCE OF HYPERTENSION PREVALENCE OF HYPERTENSION IN CKDIN CKD
Normotensive
17%
Hypertensive
83%
1795 patients with kidney 1795 patients with kidney diseases were screeneddiseases were screened
GFR range 13-55 GFR range 13-55 mL/min/1.73mmL/min/1.73m²²
↑ ↑ BP in 83% of patients BP in 83% of patients (n=1494)(n=1494)
Buckalew. Am J Kidney Dis 1996;28:811.Buckalew. Am J Kidney Dis 1996;28:811.

BLOOD PRESSURE IS POORLY BLOOD PRESSURE IS POORLY CONTROLLED IN CKDCONTROLLED IN CKD
62%
27%
11%
>140/90
<140/90
<135/90
Coresh. Arch Intern Med. 2001;161:1207Coresh. Arch Intern Med. 2001;161:1207

Aggressive Blood Pressure Goals:Aggressive Blood Pressure Goals:
Consensus Across TreatmentConsensus Across Treatment GuidelinesGuidelines
Organization Patient Type BP Goals (mm Hg)
ADA(American Diabetes Association)
Diabetes <130/80
ISHIB(Isolated Systolic Hypertension in Blacks)
ISHIB(Isolated Systolic Hypertension in Blacks)
<140/90<130/80
JNC 7(Joint National Committee)
Uncomplicated HTN With DM, CKD
<140/90<130/80
NKF(National Kidney Foundation)
Albuminuria (>300 mg/d or >200 mg/g creatinine), with or without diabetes
<130/80“Consider even lower than <130/80”
WHO-ISHWorld Health Organization – Isolated Systolic Hypertension)
Low risk for CVDPresence of Diabetes Mellitus, target organ damage
SBP<140 <130/80

BLOOD PRESSURE CONTROL IN BLOOD PRESSURE CONTROL IN CKD: GOALSCKD: GOALS
NKF. Am J Kidney Dis. 2002;3a(suppl 1):S1NKF. Am J Kidney Dis. 2002;3a(suppl 1):S1
Target populationTarget population SBPSBP DBPDBP
CKD stages 1-4 with CKD stages 1-4 with proteinuria(>1g/day)or proteinuria(>1g/day)or diabetic kidney diseasediabetic kidney disease
<125<125 <75<75
CKD stages 1-4 without CKD stages 1-4 without proteinuriaproteinuria
<135<135 <85<85
CKD stage 5CKD stage 5 <140<140 <90<90

↓↓GFR = ↑BP MEDSGFR = ↑BP MEDS
00.5
11.5
22.5
33.5
4
90-99 80-89 70-79 60-69 50-59 40-49
GFR
Nu
mb
er
of
Blo
od
Pre
ssu
re M
ed
icati
on
s
Diabetic Studies Non-Diabetic Studies
Nephsap. American Society of Nephrology 2005; 4:101Nephsap. American Society of Nephrology 2005; 4:101

BP CONTROL: INTERVENTIONSBP CONTROL: INTERVENTIONS
ACE inhibitorsACE inhibitors
Angiotensin-receptor blockers (ARBs)Angiotensin-receptor blockers (ARBs)
Calcium channel blockers (CCBs)Calcium channel blockers (CCBs)
DiureticsDiuretics
Low-sodium dietLow-sodium diet
Combination therapyCombination therapy




DIABETES MELLITUS: PREDICTIONSDIABETES MELLITUS: PREDICTIONS
In the next 10 years there will be a 50% In the next 10 years there will be a 50% increase in the number of diabetics.increase in the number of diabetics.
25 to 40% of these individuals will develop 25 to 40% of these individuals will develop kidney disease.kidney disease.
Obesity, poor dietary habits, lack of Obesity, poor dietary habits, lack of physical activity, family history are risks.physical activity, family history are risks.

THE EPIDEMIC OF DIABETESTHE EPIDEMIC OF DIABETES
Prevalence increased by 40% 1990-99.Prevalence increased by 40% 1990-99.Estimated increase by 165% 2000-2050.Estimated increase by 165% 2000-2050.Individuals born in 2000: risk developing Individuals born in 2000: risk developing
diabetes 32.8% males, 38.5% females. diabetes 32.8% males, 38.5% females. Hispanic lifetime risk 45.4% males, 52.5% Hispanic lifetime risk 45.4% males, 52.5% females.females.

Adults With Diagnosed Adults With Diagnosed Diabetes*Diabetes*
*Includes women with a history of gestational diabetes.
1990
No dataavailable
Less than 4% 4%–6% Above 6%
Mokdad AH et al. Diabetes Care. 2000;23(9):1278-1283.

Adults With Diagnosed Adults With Diagnosed Diabetes*Diabetes*
2000
4%–6% Above 6%
*Includes women with a history of gestational diabetes.
Mokdad AH et al. JAMA. 2001;286(10):1195-1200.

DIABETIC KIDNEY DISEASE DIABETIC KIDNEY DISEASE SIGNIFICANCESIGNIFICANCE
Accounts for 40-50% total kidney failure in Accounts for 40-50% total kidney failure in the United Statesthe United States
40-50% of TYPE 1 Patients and 40% of 40-50% of TYPE 1 Patients and 40% of TYPE 2 Patients will develop clinical TYPE 2 Patients will develop clinical diabetic kidney disease.diabetic kidney disease.
Diabetes affects certain ethnic groups Diabetes affects certain ethnic groups more frequently than caucasians: native more frequently than caucasians: native americans 7x, hispanics and latinos 4-5x, americans 7x, hispanics and latinos 4-5x, african americans 4x.african americans 4x.

ANEMIA IN PATIENTS WITH CKDANEMIA IN PATIENTS WITH CKD
39%
52%
9%
Hb 10-12
Hb >12
Hb <10
N= 5222N= 5222
CKDCKD
SCr 1.5-6.0 mg/d(women)SCr 1.5-6.0 mg/d(women)
SCr 2.0-6.0 mg/dL (men)SCr 2.0-6.0 mg/dL (men)
McClellan, NKF. 2002McClellan, NKF. 2002

Severe Anemia is Common at the Severe Anemia is Common at the Start of DialysisStart of Dialysis
Obrador. Kidney Int. 2001; 60:1875Obrador. Kidney Int. 2001; 60:1875
43%
57%
HCT >28%
HCT <28%

ANEMIA SIGNIFICANTLY IMPACTS ANEMIA SIGNIFICANTLY IMPACTS CKD PATIENTSCKD PATIENTS
Cardiovascular system-related Cardiovascular system-related morbidity/mortalitymorbidity/mortality
Increased cardiac outputIncreased cardiac output
Left ventricular hypertrophy Left ventricular hypertrophy (LVH)(LVH)
Symptomatic angina pectorisSymptomatic angina pectoris
Lower physical work capacityLower physical work capacity Decreased pulmonary diffusionDecreased pulmonary diffusion
Decreased oxygen utilizationDecreased oxygen utilization
Lower aerobic exercise Lower aerobic exercise capacitycapacity
Negative impact on daily livingNegative impact on daily living Decreased energy levelDecreased energy level
Impaired functional abilityImpaired functional ability
Reduced cognitive functionReduced cognitive function
Macdougall. Semin Oncol. 1998;25(suppl 7):40Macdougall. Semin Oncol. 1998;25(suppl 7):40

EVALUATION OF ANEMIAEVALUATION OF ANEMIA
Hemoglobin and/or hematocritHemoglobin and/or hematocrit
Red-blood-cell indicesRed-blood-cell indices
Reticulocyte countReticulocyte count
Iron parametersIron parameters
Test for occult-blood in stoolTest for occult-blood in stool
NKF. Am J Kidney Dis. 2001;37:S192NKF. Am J Kidney Dis. 2001;37:S192

TREATMENT OF ANEMIATREATMENT OF ANEMIA
Iron supplementation (IV/PO)Iron supplementation (IV/PO)
Erythropoiesis stimulating agentsErythropoiesis stimulating agents

IRON DEFICIENCY IN CKDIRON DEFICIENCY IN CKD
Preexisting Iron Preexisting Iron DeficiencyDeficiency
Poor nutritionPoor nutrition
Blood lossBlood loss
Iron deficiency with Iron deficiency with erythropoiesis-erythropoiesis-stimulating agentsstimulating agents
Increased iron needsIncreased iron needs

ASSESSMENT OF IRON STATUSASSESSMENT OF IRON STATUS
Frequently used testsFrequently used tests
Serum ferritinSerum ferritin
Transferrin saturationTransferrin saturation
TargetTarget
100 ng/mL100 ng/mL
>20%>20%
Additional measurementsAdditional measurements
Reticulocyte Hb contentReticulocyte Hb content
% Hypochromic RBCs% Hypochromic RBCs
Erythrocyte ferritinErythrocyte ferritin
NKF. Am J Kidney Dis. 2001;37(suppl 1);S182NKF. Am J Kidney Dis. 2001;37(suppl 1);S182
Macdougall. Curr Opin Hematol. 1999;6:121Macdougall. Curr Opin Hematol. 1999;6:121
Goodnough. Blood. 2000;96:823Goodnough. Blood. 2000;96:823

POSSIBLE INADEQUACY OF ORAL POSSIBLE INADEQUACY OF ORAL IRONIRON
Low intestinal absorption of oral iron, even in Low intestinal absorption of oral iron, even in healthy personshealthy personsPoor patient adherencePoor patient adherenceIntravenous iron has improved anemia in CKD and Intravenous iron has improved anemia in CKD and ESRD when oral iron has failedESRD when oral iron has failed
NKF. Am J Kidney Dis. 2001;37 (suppl 1):S182NKF. Am J Kidney Dis. 2001;37 (suppl 1):S182Silverberg. Kidney Int. 1999;55(suppl 69):S79Silverberg. Kidney Int. 1999;55(suppl 69):S79

Anemia and LVHAnemia and LVH
CrClCrCl
Levin. Nephrol Dial Transplant, 2001;16 Suppl 2) : 7.Levin. Nephrol Dial Transplant, 2001;16 Suppl 2) : 7.
0
10
20
30
40
50
>50 35 - 49 25 - 34 <25
Mean Hb (g/dL) 14.1 13.2 12.5 11.4Mean Hb (g/dL) 14.1 13.2 12.5 11.4
Prevalence of LVH Prevalence of LVH
(% Patients)(% Patients)

LVH and CKDLVH and CKD
LVH is an independent risk predictor of cardiac LVH is an independent risk predictor of cardiac deathdeathHTN, anemia and diabetes are modifiable HTN, anemia and diabetes are modifiable predictors of LVHpredictors of LVH
Blood pressure increase is associated with Blood pressure increase is associated with 3% increase in LVH risk3% increase in LVH riskHb decrease of 1 g/dL is associated with Hb decrease of 1 g/dL is associated with
6% 6% increase in LVH riskincrease in LVH risk
Greaves. Am J Kid Dis. 1994; 24;768Greaves. Am J Kid Dis. 1994; 24;768Levin. Am J Kid Dis. 1996; 27:347.Levin. Am J Kid Dis. 1996; 27:347.

Normal Hematocrit TrialNormal Hematocrit Trial
Study Objective: Whether normal Hct value should be Study Objective: Whether normal Hct value should be the target level in dialysis patients the target level in dialysis patients
Study Design : 1233 HD patients with cardiac disease. Study Design : 1233 HD patients with cardiac disease. Baseline Hct. 27- 33%. Mean age 65 years.Baseline Hct. 27- 33%. Mean age 65 years.
Primary Endpoint: time to death or first nonfatal Primary Endpoint: time to death or first nonfatal myocardial infarctionmyocardial infarction
Methods: Patients randomly assigned to achieve and Methods: Patients randomly assigned to achieve and maintain a Hct of 42 or 32% WITH EPO txmaintain a Hct of 42 or 32% WITH EPO tx
Results: Study terminated early (29 months) due to Results: Study terminated early (29 months) due to increase mortality in the group targeted for normal increase mortality in the group targeted for normal Hct level.Hct level.
N Eng J Med 1998; 339:584N Eng J Med 1998; 339:584

CHOIR Study CHOIR Study (Correction of Hemoglobin and Outcomes in Renal Insufficiency)(Correction of Hemoglobin and Outcomes in Renal Insufficiency)
Study Objective: Whether a normal or near-normal Study Objective: Whether a normal or near-normal Hb value should be the target level in pre-dialysis Hb value should be the target level in pre-dialysis pts with CKDpts with CKD
Study Design: 1432 CKD patients (eGFR 15-50 Study Design: 1432 CKD patients (eGFR 15-50 mL/min) with Hb < 11g/dLmL/min) with Hb < 11g/dL
Primary Endpoint: Composite of death, myocardial Primary Endpoint: Composite of death, myocardial infarction, stroke, and hospitalization for heart infarction, stroke, and hospitalization for heart failurefailure
Methods: Randomization to achieve target Hb of Methods: Randomization to achieve target Hb of either 13.5 or 11.3g/dLeither 13.5 or 11.3g/dL
Results: Study terminated early(16 months) due to Results: Study terminated early(16 months) due to higher number of events in the high Hb group.higher number of events in the high Hb group.
Drueke, TB et al. N Engl J Med 2006;355:2071Drueke, TB et al. N Engl J Med 2006;355:2071

CREATE StudyCREATE Study(Cardiovascular Risk Reduction by Early Anemia Treatment with (Cardiovascular Risk Reduction by Early Anemia Treatment with
Epoietin Beta)Epoietin Beta)
Study Objective: Whether a normal or near-normal Study Objective: Whether a normal or near-normal Hb value should be the target level in pre-dialysis Hb value should be the target level in pre-dialysis pts with CKD.pts with CKD.
Study Design: 603 pts with GFRs between 15-35 Study Design: 603 pts with GFRs between 15-35 mL/minmL/min
Primary Endpoint: Composite of eight CV eventsPrimary Endpoint: Composite of eight CV eventsMethods: Randomization to normal Hb (13-15 g/dL) Methods: Randomization to normal Hb (13-15 g/dL)
or subnormal (10.5 – 11.5 g/dL)or subnormal (10.5 – 11.5 g/dL)Results: At 3 years similar risk of experiencing the Results: At 3 years similar risk of experiencing the
primary endpoint in bot groups ( HR of 0.78, 95% primary endpoint in bot groups ( HR of 0.78, 95% CI 0.53-1.14)CI 0.53-1.14)
Singh, AK et al. N Engl J Med 2006; 355:2085Singh, AK et al. N Engl J Med 2006; 355:2085

Ongoing and Future Studies Ongoing and Future Studies
TREAT study – Randomized, placebo-controlled trial in TREAT study – Randomized, placebo-controlled trial in Predialysis pts with DM type 2 to Hb 13 or greater than9 Predialysis pts with DM type 2 to Hb 13 or greater than9 g/dL.g/dL.Primary endpoint is overall mortality and nonfatal CV Primary endpoint is overall mortality and nonfatal CV events.events.NEPHRODIAB2 trial – Prospective randomized open-NEPHRODIAB2 trial – Prospective randomized open-label trial in CKD stage 3 and 4 with DM type 2. label trial in CKD stage 3 and 4 with DM type 2. Randomization to Hb 13-14.9 g/dL or 11-12 g/dL.Randomization to Hb 13-14.9 g/dL or 11-12 g/dL.Primary endpoint is decline in kidney function.Primary endpoint is decline in kidney function.Secondary outcomes include mortalitySecondary outcomes include mortality

Anemia – current recommendationsAnemia – current recommendations
Close monitoring of predialysis Hb levels Close monitoring of predialysis Hb levels
Erythropoietic agents rather than blood Erythropoietic agents rather than blood transfusions transfusions
Target Hb should generally be in the range Target Hb should generally be in the range of 11 – 12 g/dL and should not exceed 13 of 11 – 12 g/dL and should not exceed 13 g/dL.g/dL.
Supplemental ironSupplemental iron

SECONDARY SECONDARY HYPERPARATHYROIDISMHYPERPARATHYROIDISM
Most common form of renal Most common form of renal osteodystrophyosteodystrophy
PrevalencePrevalence
47% of 176 patients with ESRD had 47% of 176 patients with ESRD had a a PTH level more than three times the PTH level more than three times the
normal amountnormal amount
Mizumoto. Nephrol Dial Transplant. 1994:9:1751Mizumoto. Nephrol Dial Transplant. 1994:9:1751
Billa. Perit Dial Int. 2000;20:315Billa. Perit Dial Int. 2000;20:315

VITAMIN D DEFICIENCY AND VITAMIN D DEFICIENCY AND PHOSPHATE RETENTIONPHOSPHATE RETENTION
CKDCKD
Vitamin D DeficiencyVitamin D Deficiency Phosphate Retention Phosphate Retention
Hypocalcemia Hypocalcemia
HyperparathyroidismHyperparathyroidism
OsteodystrophyOsteodystrophy
Liach. In: Brenner. The Kidney. 1996:2187Liach. In: Brenner. The Kidney. 1996:2187
Schomig.Nephrol Dial Transplant. 2000;15(suppl 5):18Schomig.Nephrol Dial Transplant. 2000;15(suppl 5):18

HyperphosphatemiaHyperphosphatemia
Begins early in renal diseaseBegins early in renal diseaseIntimately related to secondary Intimately related to secondary hyperparathyroidism which contributes to hyperparathyroidism which contributes to release of calcium and phosphorus from release of calcium and phosphorus from boneboneElevated Ca x PO4 promotes precipitation of Elevated Ca x PO4 promotes precipitation of such in arteries, joints, soft tissues and the such in arteries, joints, soft tissues and the viceraviceraCa x PO4 >55 associated with increased Ca x PO4 >55 associated with increased mortality, similar to that observed with mortality, similar to that observed with elevated PO4 level aloneelevated PO4 level alone
Menon, V. Am J Kidney Dis 2005; 46:455.Menon, V. Am J Kidney Dis 2005; 46:455.

MANAGEMENT OF VITAMIN D MANAGEMENT OF VITAMIN D DEFICIENCY AND PHOSPHATE DEFICIENCY AND PHOSPHATE
RETENTIONRETENTION
Vitamin D analogsVitamin D analogsLow phosphate diet (800 mg/day)Low phosphate diet (800 mg/day)Phosphate binders (calcium and Phosphate binders (calcium and non-calcium based)non-calcium based)CalciumCalcium
Coburn. J Am Soc Nephrol. 1998;9:S71Coburn. J Am Soc Nephrol. 1998;9:S71Schroeder. Nephrol Dial Transplant. 2000;15:460Schroeder. Nephrol Dial Transplant. 2000;15:460Chertow. Clin Nephrol. 1999;51:18Chertow. Clin Nephrol. 1999;51:18

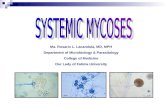
Phosphate BindersPhosphate BindersPO4 Binder Blood Ca Blood PO4 Blood level LDL Adverse Effects
Calcium acetate ↑ ↓ Promotes coronary artery calcification
Calcium Carbonate
↑ ↓ Promotes coronary artery calcification
Renagel/ Renvela
↓ ↓ Metabolic acidosis; not seen with Renvela
Lanthanum ↓ ↑ Not yet reported
Aluminum ↓ ↑ Anemia, dementia, CNS abn, osteomalacia

ACID/BASE BALANCEACID/BASE BALANCE
Renal NH4+Renal NH4+
ExcretionExcretion
40 mEq/day40 mEq/day
EndogenousEndogenous Renal Net Acid Renal Net Acid
H+ ProductionH+ Production Renal Renal Excretion Excretion
70 mEq/day70 mEq/day Excretion Excretion 70 mEq/day 70 mEq/day
30 mEq/day30 mEq/day
Normal Acid/Base BalanceNormal Acid/Base Balance
[HCO3] = 24 mEq/L[HCO3] = 24 mEq/L
Alpem. Am J Kidney Dis. 1997;29:291Alpem. Am J Kidney Dis. 1997;29:291

CONSEQUENCES OF METABOLICCONSEQUENCES OF METABOLIC ACIDOSISACIDOSIS
Abnormal renal handling of ionsAbnormal renal handling of ions
↓ ↓ tubular-phosphate reabsorptiontubular-phosphate reabsorption
↑ ↑ filtered load of calcium and phosphatefiltered load of calcium and phosphate
↓ ↓ tubular-calcium reabsorptiontubular-calcium reabsorption
Increased resorption of boneIncreased resorption of bone
Increased muscle catabolismIncreased muscle catabolism
Franch. J Am Soc Nephrol. 1998;9:S78Franch. J Am Soc Nephrol. 1998;9:S78

TREATMENT OF METABOLIC TREATMENT OF METABOLIC ACIDOSIS IN CKDACIDOSIS IN CKD
Goal Goal Serum HCO3- > 20 mEq/LSerum HCO3- > 20 mEq/LpH > 7.35pH > 7.35AgentsAgentsSodium bicarbonate tabletsSodium bicarbonate tablets
(650 mg = (650 mg = ~ 8 mEq HCO3-)~ 8 mEq HCO3-)Sodium citrate (Shohl’s solution)Sodium citrate (Shohl’s solution)Dose of HCO3-Dose of HCO3-1.0 – 1.5 mEq/kg/day1.0 – 1.5 mEq/kg/dayDependent upon initial serum HCO3- and degree of Dependent upon initial serum HCO3- and degree of renal insufficiencyrenal insufficiency
Dubose TD. Harrison’s Principles of Internal Medicine. 1998:277Dubose TD. Harrison’s Principles of Internal Medicine. 1998:277

Recommendations in Metabolic Recommendations in Metabolic Acidosis TreatmentAcidosis Treatment
Alkali therapy to maintain plasma Alkali therapy to maintain plasma bicarbonate concentration above 22 meq/L bicarbonate concentration above 22 meq/L (K/DOQI guideline recommendation)(K/DOQI guideline recommendation)
Sodium bicarbonate – Agent of choice; Sodium bicarbonate – Agent of choice; may cause bloating.may cause bloating.
Sodium Citrate – Avoid when also taking Sodium Citrate – Avoid when also taking aluminum-containing anti-acids since it aluminum-containing anti-acids since it markedly enhances aluminum absoption markedly enhances aluminum absoption

EATING WELL AND EXERCISEEATING WELL AND EXERCISE
Protein malnutrition is common in CKDProtein malnutrition is common in CKDConsider dietary protein restrictionConsider dietary protein restrictionProperly monitored by experienced Properly monitored by experienced dietitian and nephrologistdietitian and nephrologistMay improve long-term survival of patientsMay improve long-term survival of patientsExerciseExerciseImproves physical functioningImproves physical functioningImproves cardiovascular healthImproves cardiovascular health
Bailey. Therapy in Nephrology and Hypertension. 1998:474Bailey. Therapy in Nephrology and Hypertension. 1998:474

EXERCISEEXERCISE
↑ ↑ Physical functioningPhysical functioning
↑ ↑ Blood pressure controlBlood pressure control
↑ ↑ Muscle, bone strengthMuscle, bone strength
↓ ↓ Level of cholesterol and Level of cholesterol and triglyceridestriglycerides
Better sleepBetter sleep
↑ ↑ Control of body weightControl of body weight
NKF. Staying fit with Kidney DiseaseNKF. Staying fit with Kidney Disease

VASCULAR ACCESS FOR VASCULAR ACCESS FOR HEMODIALYSISHEMODIALYSIS
Establish communication between Establish communication between nephrologist and PCPnephrologist and PCPPreserve an arm: no intravenous Preserve an arm: no intravenous injections or blood drawsinjections or blood drawsRefer to surgeon for fistula when SCr Refer to surgeon for fistula when SCr >4mg/dL, CrCl <25 mL/min, or dialysis >4mg/dL, CrCl <25 mL/min, or dialysis anticipated within 1 yearanticipated within 1 yearFistula may take 3 to 4 months to matureFistula may take 3 to 4 months to mature
NKF. Am J Kidney Dis. 2001;37(suppl 1):S147NKF. Am J Kidney Dis. 2001;37(suppl 1):S147

TEAM APPROACH: ROLE OF TEAM APPROACH: ROLE OF PRIMARY PHYSICIAN AND PRIMARY PHYSICIAN AND NEPHROLOGIST IN CKDNEPHROLOGIST IN CKD
Primary PhysicianPrimary Physician
Screen and identify Screen and identify risk factors of CKDrisk factors of CKD
Provide ongoing Provide ongoing management of management of patients with CKDpatients with CKD
Provide role-specific Provide role-specific patient educationpatient education
NephrologistsNephrologists
Assist in development Assist in development of care strategy of care strategy
Aid recommendation Aid recommendation and implementation of and implementation of patient carepatient care
Provide role-specific Provide role-specific patient educationpatient education

BENEFITS OF EARLY BENEFITS OF EARLY INTERVENTION IN THE INTERVENTION IN THE MANAGEMENT OF CKDMANAGEMENT OF CKD
Delayed progression of CKDDelayed progression of CKD
Improved teamwork between physiciansImproved teamwork between physicians
Decreased risk of cardiovascular Decreased risk of cardiovascular complicationscomplications
Improved dialysis outcomesImproved dialysis outcomes
Better educated and prepared patientsBetter educated and prepared patients
Pereira. Kidney Int. 2000;57:351.Pereira. Kidney Int. 2000;57:351.