Regulatory Toxicology and Pharmacology
6
Prescribing patterns of the four most commonly used sedatives in endoscopic examination in Korea: Propofol, midazolam, diazepam, and lorazepam Ju-Young Shin a , Shin Haeng Lee a , Sun Mi Shin a , Mi Hee Kim a , Sung Geon Park b , Byung-Joo Park a,c,⇑ a Korea Institute of Drug Safety and Risk Management (KIDS), 136 Changgyeonggung-ro, Jongno-gu, Seoul 110-750, Republic of Korea b Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 108 Pyeong-dong, Jongno-gu, Seoul 110-746, Republic of Korea c Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 110-799, Republic of Korea article info Article history: Received 24 November 2014 Available online 7 February 2015 Keywords: Propofol Midazolam Diazepam Lorazepam Sedatives Abuse Endoscopic examination abstract As the sedative use increases due to the effectiveness and relatively safe profile, the abuse potential is also increasing. This study was conducted to examine the usage of four sedative agents in endoscopic examination and to compare the propofol use with the other three sedatives. Using National Health Insurance claims data from 2008 to 2012, we identified the number of cases of conscious sedation during endoscopy using one or more of the following agents: propofol, midazolam, diazepam, and lorazepam. The general characteristics of patients and medical service providers were analyzed, and the regional and annual distributions of frequency of use were compared. We also identified patient cases with exces- sive number of endoscopic examinations. Among the total of 3,156,231 sedatives users, midazolam was the most commonly used agent (n = 2,845,250, 90.1%). However, the largest increase in patient number, which increased from 11,410 in 2008 to 28,170 in 2012, was observed with propofol. While the majority of patients received an annual endoscopy, we identified several suspected abuse cases of patients receiv- ing endoscopies repetitively as many as 114 times in five years. The rise of sedative use in endoscopic examinations and several patient cases of repeated sedative administration suggest a potential risk for abuse. Medical service providers should be cautious when using sedatives and carefully review each patient’s medical history prior to the procedure. Ó 2015 Elsevier Inc. All rights reserved. 1. Introduction Recently, conscious sedation has been widely utilized to reduce patients’ anxiety and pain during endoscopic examination. It is well known that both patients and physicians generally prefer sedated over unsedated endoscopy (Brandt, 2001). According to a survey conducted in the United States, the interest in propofol use for endoscopy is growing rapidly (Faulx et al., 2005). Liu showed that the proportion of sedated endoscopic procedures has more than doubled, from approximately 14% in 2003 to 30% in 2009 (Liu et al., 2012). In another study, the percentage of sedat- ed endoscopy was expected to increase by 53% in 2015 (Inadomi et al., 2010). Generally, periodic surveillance endoscopy is recommended for various conditions and risk factors, varying from every three months to every 2–3 years (Hirota et al., 2006). For example, in Korea, the National Cancer Screening Program provides biannual gastrointestinal (GI) endoscopy for cancer screening (National Cancer Information Center). Propofol (2,6-diisopropylphenol) is an intravenously administered sedative that was first introduced to clinical practice in 1989. Recently, many clinical trials demon- strated intravenous sedation with propofol to be more effective than sedation with other sedative agents (Koshy et al., 2000; Carlsson and Grattidge, 1995; Seifert et al., 2000). With its rapid onset of action and recovery time and good quality of recovery after sedation (Vargo, 2004; Riphaus et al., 2006), propofol is wide- ly used for induction and maintenance of sedation in endoscopy. However, since the first report of propofol abuse in 1992 (Follette and Farley, 1992), several other reports have been pub- lished that expand on propofol’s potential for abuse using molecu- lar and clinical evidence (Pain et al., 2002; Weerts et al., 1999; Zacny et al., 1993). Recently, abuse and misuse of propofol has been a social problem in Korea, particularly when used in endoscopy. Roh et al. described a patient who visited a number http://dx.doi.org/10.1016/j.yrtph.2015.01.007 0273-2300/Ó 2015 Elsevier Inc. All rights reserved. ⇑ Corresponding author at: Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 110-799, Republic of Korea. Fax: +82 2 747 4830. E-mail address: [email protected] (B.-J. Park). Regulatory Toxicology and Pharmacology 71 (2015) 565–570 Contents lists available at ScienceDirect Regulatory Toxicology and Pharmacology journal homepage: www.elsevier.com/locate/yrtph
-
Upload
piter-pen -
Category
Health & Medicine
-
view
33 -
download
1
Transcript of Regulatory Toxicology and Pharmacology

Regulatory Toxicology and Pharmacology 71 (2015) 565–570
Contents lists available at ScienceDirect
Regulatory Toxicology and Pharmacology
journal homepage: www.elsevier .com/locate /yr tph
Prescribing patterns of the four most commonly used sedatives inendoscopic examination in Korea: Propofol, midazolam, diazepam, andlorazepam
http://dx.doi.org/10.1016/j.yrtph.2015.01.0070273-2300/� 2015 Elsevier Inc. All rights reserved.
⇑ Corresponding author at: Department of Preventive Medicine, Seoul NationalUniversity College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 110-799, Republicof Korea. Fax: +82 2 747 4830.
E-mail address: [email protected] (B.-J. Park).
Ju-Young Shin a, Shin Haeng Lee a, Sun Mi Shin a, Mi Hee Kim a, Sung Geon Park b, Byung-Joo Park a,c,⇑a Korea Institute of Drug Safety and Risk Management (KIDS), 136 Changgyeonggung-ro, Jongno-gu, Seoul 110-750, Republic of Koreab Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 108 Pyeong-dong, Jongno-gu, Seoul 110-746, Republic of Koreac Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 110-799, Republic of Korea
a r t i c l e i n f o
Article history:Received 24 November 2014Available online 7 February 2015
Keywords:PropofolMidazolamDiazepamLorazepamSedativesAbuseEndoscopic examination
a b s t r a c t
As the sedative use increases due to the effectiveness and relatively safe profile, the abuse potential isalso increasing. This study was conducted to examine the usage of four sedative agents in endoscopicexamination and to compare the propofol use with the other three sedatives. Using National HealthInsurance claims data from 2008 to 2012, we identified the number of cases of conscious sedation duringendoscopy using one or more of the following agents: propofol, midazolam, diazepam, and lorazepam.The general characteristics of patients and medical service providers were analyzed, and the regionaland annual distributions of frequency of use were compared. We also identified patient cases with exces-sive number of endoscopic examinations. Among the total of 3,156,231 sedatives users, midazolam wasthe most commonly used agent (n = 2,845,250, 90.1%). However, the largest increase in patient number,which increased from 11,410 in 2008 to 28,170 in 2012, was observed with propofol. While the majorityof patients received an annual endoscopy, we identified several suspected abuse cases of patients receiv-ing endoscopies repetitively as many as 114 times in five years. The rise of sedative use in endoscopicexaminations and several patient cases of repeated sedative administration suggest a potential risk forabuse. Medical service providers should be cautious when using sedatives and carefully review eachpatient’s medical history prior to the procedure.
� 2015 Elsevier Inc. All rights reserved.
1. Introduction
Recently, conscious sedation has been widely utilized to reducepatients’ anxiety and pain during endoscopic examination. It iswell known that both patients and physicians generally prefersedated over unsedated endoscopy (Brandt, 2001). According to asurvey conducted in the United States, the interest in propofoluse for endoscopy is growing rapidly (Faulx et al., 2005). Liushowed that the proportion of sedated endoscopic procedureshas more than doubled, from approximately 14% in 2003 to 30%in 2009 (Liu et al., 2012). In another study, the percentage of sedat-ed endoscopy was expected to increase by 53% in 2015 (Inadomiet al., 2010).
Generally, periodic surveillance endoscopy is recommended forvarious conditions and risk factors, varying from every
three months to every 2–3 years (Hirota et al., 2006). For example,in Korea, the National Cancer Screening Program provides biannualgastrointestinal (GI) endoscopy for cancer screening (NationalCancer Information Center). Propofol (2,6-diisopropylphenol) isan intravenously administered sedative that was first introducedto clinical practice in 1989. Recently, many clinical trials demon-strated intravenous sedation with propofol to be more effectivethan sedation with other sedative agents (Koshy et al., 2000;Carlsson and Grattidge, 1995; Seifert et al., 2000). With its rapidonset of action and recovery time and good quality of recoveryafter sedation (Vargo, 2004; Riphaus et al., 2006), propofol is wide-ly used for induction and maintenance of sedation in endoscopy.
However, since the first report of propofol abuse in 1992(Follette and Farley, 1992), several other reports have been pub-lished that expand on propofol’s potential for abuse using molecu-lar and clinical evidence (Pain et al., 2002; Weerts et al., 1999;Zacny et al., 1993). Recently, abuse and misuse of propofol hasbeen a social problem in Korea, particularly when used inendoscopy. Roh et al. described a patient who visited a number

566 J.-Y. Shin et al. / Regulatory Toxicology and Pharmacology 71 (2015) 565–570
of endoscopists with the sole aim of receiving propofol until he wasadmitted to a closed psychiatric facility for treatment of his propo-fol addiction (Roh et al., 2011). Kim et al. examined the degree ofabuse liability among those of the general population who had gas-tric endoscopic examination and used propofol as a sedative (Kimet al., 2013). Not only is there the potential for dependence on thedrug and serious accompanying social problems, but its overusecan easily lead to death caused by respiratory suppression.
In this study, we investigated the usage of four commonly usedsedatives in endoscopic examination, including propofol, midazo-lam, diazepam, and lorazepam, using the Korean National HealthInsurance claims database. By comparing the prescribing patternsof the four drugs, we examined if the extent of propofol use chan-ged over the study period more than the other three sedatives.
2. Methods
2.1. Data source
We analyzed National Health Insurance claims data retrievedfrom the Health Insurance Review and Assessment Service(HIRA). In Korea, the National Health Insurance system providescoverage to the entire Korean population. All medical services pro-vided to a beneficiary must be reported to HIRA by the medical ser-vice provider, which are then reviewed for reimbursement of theexpenses. Therefore, the HIRA database contains all informationon claims submitted, including medical services and prescribedmedications. The database contains anonymized patient identi-fiers, demographics, including age and gender, medical diagnoses(according to the International Classification of Disease, TenthRevision (ICD-10)), dispensed medications (drug code, date dis-pensed and number of doses supplied), medical procedures per-formed, and details of medical service providers (identifier, typeand region). The database was retrieved from HIRA with de-identi-fied codes that enabled sorting and linking only for researchpurposes.
2.2. Study subjects
We included subjects who received sedated endoscopy withone of the following intravenous sedatives from 2008 to 2012:propofol, midazolam, diazepam, or lorazepam. Patients who wereaged 12 years and younger, cases of sedation during surgery, andsedation for inpatients were excluded. Sedation performed forinpatients in the operating room involves a more complicatedrationale for use that requires a clinical review, which was notappropriate for our analysis. Endoscopy was defined by procedurecodes, which were confirmed by a practitioner. An endoscopypatient was defined as a patient who received sedation at leastonce for a non-operative outpatient endoscopy with propofol,midazolam, diazepam, or lorazepam. In cases of a patient receivingtwo or more sedatives per procedure or having more than one pro-cedure performed during the study period, each sedative receivedby the patient was counted.
2.3. Gender, age and type of medical service provider
Descriptive statistics, including frequencies, proportions, andmeans (±SD), were used to characterize study subjects by genderand age. We categorized age into groups of ten years (i.e., 13–19,20–29, 30–39, 40–49, 50–59, 60–69, 70–79, and P80). The typeof medical service provider was analyzed by frequency and propor-tion and was categorized into three groups according to the level ofmedical care: tertiary hospitals, secondary hospitals, and primarycare clinics. The escalating levels of care indicate the degree of size
and specialty. Primary care clinics generally provide basic healthservices, which are the most accessible to the patients. Based onthe condition, the patient who initially visited a primary care clinicmay be referred to a specialist in secondary hospitals for a higherlevel of care. Tertiary hospitals provide the most advanced carefor patients who were referred from a primary or secondaryhealthcare professional. In general, the bed capacities in primary,secondary, and tertiary hospitals are a minimum of 30, 100, and500 respectively.
2.4. Trends of sedative use over time and regional distribution
We presented the total number of patients from 2008 to 2012receiving each sedative to show the changes in yearly usage. Wealso indicated the frequencies and proportions by visit year. Theregions were categorized into three groups, metropolitan area,major city, and rural area, according to the number of population.The metropolitan area included Seoul, the capital city of Korea,Gyeonggi, and Incheon. The major cities included Busan, Daegu,Gwangju, Daejeon, and Ulsan. The rural area was the rest ofregions, which included Gangwon, Chungcheong, Jeolla,Gyongsang, and Jeju. The proportion of sedative use for each regionwas calculated for propofol and midazolam, which was shown inmaps.
2.5. Distributions of visit frequency of endoscopy and cases ofsuspected abuse patients
For each sedative, the frequency of sedated endoscopy perpatient was calculated. The number of patients for different visitfrequencies are calculated and presented by year from 2008 to2012. And we identified suspected abuse patients who receivedsedation endoscopies with sedatives repeatedly during study peri-od. Then we showed the safety profile of several cases about thegeneral characteristics of patients and medical service providersin sequence of date of visit.
2.6. Statistical analysis
Categorical variables, including gender and categorized age, arepresented as numbers and percentages. Means and standard devia-tions (SD) of age were also calculated. The regional distribution andfrequency of receiving endoscopies were visualized by QuantumGeographic Information Systems (QGIS) (OSGeo, Beaverton, OR,USA). This geographic software effectively presents the nationwidedrug use pattern. P-values were calculated by the chi-squared testfor discrete variables, and P-values of less than 0.05 were consid-ered to be statistically significant for all analyses. All statisticalanalyses were performed using SAS version 9.3 (SAS InstituteInc., Cary, NC, USA).
2.7. Ethics statement
The study protocol was approved by the Institutional ReviewBoard of the Korea Institute of Drug Safety and RiskManagement. The requirement for informed consent from thestudy population was waived by the board.
3. Results
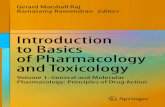
The total number of upper gastrointestinal endoscopic proce-dures in each year during the study period is shown in Fig. 1.This number increased from 3,723,460 in 2008 to 4,234,539 in2010, and decreased to 3,940,443 in 2012. Despite the decreasein the number of endoscopies from 2010 to 2012, there was a sharp

Fig. 1. Percentage of patients receiving propofol, midazolam, diazepam, andlorazepam between 2008 and 2012.
J.-Y. Shin et al. / Regulatory Toxicology and Pharmacology 71 (2015) 565–570 567
increase in the number of propofol users, which doubled from10,343 in 2011 to 28,650 in 2012, while the number of other seda-tive users decreased. The number of midazolam users slightlyincreased from 2008 to 2011 and decreased from 2011 to 2012.A continuous decrease in the number of diazepam and lorazepamusers was observed during the five-year study period.
During the study period, the number of patients who receivednon-operative outpatient endoscopy was 73,739 under sedationwith propofol, 2,845,250 with midazolam, 235,633 with diazepam,and 1,609 with lorazepam. The number of patients according togender, age, and the type of medical service providers are shown
Table 1Gender, age and type of medical service provider for propofol, midazolam, diazepam, and
Characteristics Propofol (n = 73,739) Midazolam (n = 2,845,25
GenderMale 32,834 (44.5%) 1,217,228 (42.8%)Female 40,905 (55.5%) 1,628,022 (57.2%)
Age (years)c: Mean ± SD 46.1 ± 15.2 48.4 ± 15.213–19 1,458 (2.0%) 55,946 (2.0%)20–29 9,480 (12.9%) 350,711 (12.3%)30–39 18,879 (25.6%) 724,208 (25.5%)40–49 15,291 (20.7%) 683,223 (24.0%)50–59 14,669 (19.9%) 779,109 (27.4%)60–69 10,190 (13.8%) 555,213 (19.5%)70–79 4,877 (6.6%) 294,147 (10.3%)80+ 830 (1.1%) 38,809 (1.4%)
Type of medical service providerc
Tertiary hospital 18,792 (25.5%) 1,184,290 (41.6%)Secondary hospital 19,656 (26.7%) 365,517 (12.8%)Primary care clinic 35,376 (48.0%) 1,401,690 (49.3%)
a An endoscopy patient was defined as a patient who received at least one endoscopy wand midazolam for one sedation, or received two different sedations with propofol and mmidazolam patient.
b P-value was calculated by the Chi square test with bonferroni correction.c Patients may have more than one value in the study period.
in Table 1. There were significant differences between the foursedatives in terms of patients’ gender, age and type of medical ser-vice provider (P < 0.01). For all sedatives, there were slightly higherpercentages of female than male patients. The mean age of patientswho used propofol (46.1 ± 15.2) was the lowest and it was fol-lowed by lorazepam (48.2 ± 15.4) and midazolam (48.4 ± 15.2).There were significant differences in the use of the four sedativesin terms of the type of medical service providers. Diazepam wasmostly used in endoscopy in primary care clinics (n = 203,826,86.5%). For propofol, 48.0% (n = 35,376) of the users were in prima-ry care clinics, 26.7% (n = 19,656) in secondary hospitals, and 25.5%(n = 18,792) in tertiary hospitals. Unlike propofol, midazolam, anddiazepam, which were mainly used in primary care clinics, loraze-pam was used the most in tertiary hospitals (n = 805, 50.0%).
Regional distribution of the users of propofol and midazolam isshown in Fig. 2. Geographically, all four sedatives were used most-ly in metropolitan regions. The use of midazolam and lorazepamwas mostly located in Seoul (22.8% and 18.0% of all patients,respectively) and the use of propofol and diazepam was mainlylocated in Gyeonggi (22.4% and 25.2%, respectively).
Table 2 demonstrates the frequency of endoscopic examinationwith propofol and midazolam. The majority of the patients under-went endoscopy with sedation only once during five years: 96.4%with propofol and 80.9% with midazolam. The proportion ofpatients receiving more than one sedated endoscopy with propofolincreased slightly from 0.95% (n = 98) in 2011 to 1.68% (n = 480) in2012, while the proportion of patients receiving more than onesedated endoscopy with one or more of the other three sedativesremained unchanged or slightly decreased. Patients undergoingthe highest numbers of sedated endoscopies received either mida-zolam (114 sedated endoscopies in one patient) or propofol (12sedated endoscopies). Notably, the patient who received a totalof 114 endoscopies under midazolam sedation underwent morethan 20 endoscopic examinations every year, from the same med-ical service provider. Table 3 shows the frequency of sedativeadministration in five suspected patient cases of abuse; twopatient cases with propofol and three patient cases with midazo-lam are shown. The frequency of endoscopy ranged from one tofive times per month for the 71-year-old male patient whoreceived a total of 114 endoscopies. Detailed treatment histories,including the date of visits, patient age, medical service provider
lorazepam between 2008 and 2012.a
0) Diazepam (n = 235,633) Lorazepam (n = 1,609) P-value b
99,925 (42.4%) 636 (39.5%) <.001135,708 (57.6%) 973 (60.5%)
52.6 ± 16.0 48.2 ± 15.43,926 (1.7%) 24 (1.5%) <.00123,912 (10.1%) 170 (10.6%) <.00141,548 (17.6%) 347 (21.6%) <.00146,557 (19.8%) 366 (22.7%) <.00163,941 (27.1%) 327 (20.3%) <.00159,086 (25.1%) 232 (14.4%) <.00140,192 (17.1%) 163 (10.1%) <.0016,450 (2.7%) 17 (1.1%) <.001
8,780 (3.7%) 805 (50.0%) <.00123,485 (10.0%) 571 (35.5%) <.001203,826 (86.5%) 235 (14.6%) <.001
ith propofol, midazolam, diazepam, or lorazepam. If a patient received both propofolidazolam during an endoscopy, the patient was classified as both a propofol and a

Fig. 2. Regional distributiona of patients using propofol and midazolamb. aThe region is classified by the location of the medical service provider. bRegional distributionshowed a significant difference by each sedative (P-value < 0.05).
Table 2Frequency of receiving propofol and midazolam during endoscopy.
Frequency 2008 2009 2010 2011 2012 Total
Propofol 1 11,242 (98.5%) 12,353 (98.6%) 12,604 (98.9%) 10,245 (99.1%) 28,170 (98.3%) 71,061 (96.4%)2 163 (1.4%) 169 (1.3%) 131 (1.0%) 97 (0.9%) 457 (1.6%) 2,398 (3.3%)3+ 5 (0.0%) 10 (0.1%) 3 (0.0%) 1 (0.0%) 23 (0.1%) 280 (0.4%)Total 11,410 12,532 12,738 10,343 28,650 73,739
Midazolam 1 584,640 (95.5%) 646,542 (95.5%) 693,294 (95.5%) 718,724 (95.7%) 683,486 (95.6%) 2,303,012 (80.9%)2 25,322 (4.1%) 27,623 (4.1%) 30,021 (4.1%) 29,670 (3.9%) 28,765 (4.0%) 380,795 (13.4%)3 1,949 (0.3%) 2,172 (0.3%) 2,501 (0.3%) 2,470 (0.3%) 2,411 (0.3%) 101,220 (3.6%)4 269 (0.0%) 278 (0.0%) 314 (0.0%) 302 (0.0%) 304 (0.0%) 35,457 (1.2%)5+ 51 (0.0%) 46 (0.0%) 55 (0.0%) 66 (0.0%) 59 (0.0%) 24,767 (0.9%)Total 612,231 676,661 726,185 751,232 715,025 2,845,250
Table 3Frequency of administration of propofol and midazolam in suspected patient cases of abuse.
Sedative PatientNo.
Gender AgeaTotalVisits
Propofol 1 Female 42 12 1 * 1 1 1 1 1 1 2 1 1
Propofol 2 Male 77 8 1 1 1 1 1 1
Midazolam 3 Male 71 114 2 2 2 1 1 1 1 2 2 2 2 3 1 3 2 2 3 2 1 3 2 2 3 3 2 4 1 3 2 3 2 3 5 2 3 2 4 3 3 1 1 1
Midazolam 4 Male 40 72 1 1 1 7 7 6 2 3 1 2 2 2 4 10 2 2 3 1 1
Midazolam 5 Female 37 37 1 1 1 2 8 3 1 1 2 3 2 2 3 1 2
Jan-11 Jul-11 Jan-12 Jul-12Jan-08 Jul-08 Jan-09 Jul-09 Jan-10 Jul-10
1
1
1
2 2 2 2
1
2 1
2 7 4
1
3 3 2 5
⁄Number of visits
568 J.-Y. Shin et al. / Regulatory Toxicology and Pharmacology 71 (2015) 565–570
number and type, and region of the five suspected abuse cases arepresented in Appendix 1.
4. Discussion
Our study quantitatively describes the trends of sedative useamong patients receiving non-operative outpatient endoscopies,using a National Health Insurance claims database. We identified
the number of users of four commonly used sedatives, includingpropofol, midazolam, diazepam, and lorazepam, from 2008 to2012. The most frequently used agent was midazolam, whichwas used in 2,845,250 patients, and the second most used agentwas diazepam, with 235,633 patients. This observation agrees withthe guidelines of the American Society for GastrointestinalEndoscopy, which recommend using an intravenous benzodi-azepine, either alone or in combination with an opiate, in mostpatients undergoing a routine endoscopy (Vargo et al., 2002). In

J.-Y. Shin et al. / Regulatory Toxicology and Pharmacology 71 (2015) 565–570 569
2012, the number of patients who received propofol sedations forendoscopy increased by more than doubled, whereas the numberof patients who received the other three sedatives remainedrelatively unchanged. This increase reflects the recent trendtowards a preference to use propofol in many endoscopic examina-tions due to its benefits such as rapid onset and offset, improvedpatient comfort, and prompt recovery and hallucination effects(Koshy et al., 2000; Ljubicic et al., 2003; Bendiksen and Larsen,1998; ML et al., 2000; Thomson and Knight, 1988).
The number of outpatients who received propofol three or moretimes in a year was remarkably increased from 1 in 2011 to 23 in2012, respectively accounting for 0.01% and 0.08% of the totalnumber of patients receiving propofol. Although low when com-pared with the frequency of use of other drugs, the incidence ofrepetitive propofol use showed a significant increase. This meansthat not only the total number of propofol users increased, but alsothat the number of patients repetitively exposed to propofol sig-nificantly increased. Because our study involved cases of propofoluse during an endoscopy for a medical check-up, we cannotdefinitely say that the cases of repetitive propofol use were abu-sive. However, several studies have reported that propofol depen-dency initiated by repeated application of the drug withinanesthetic use and have demonstrated that the one of the maincontributing factors to dependence might be repeated exposureto the drug over several years. Therefore, vigilance is needed, espe-cially in patients who experience repeated exposure to propofolapplication, in order to minimize the possibility of drug abuse.
Our data indicates that endoscopies with sedation were mostlyperformed in primary care clinics rather than in secondary or ter-tiary hospitals. This corresponds with the fact that endoscopicexaminations are often done in local primary care clinics for rou-tine check-ups. Regional distribution of the users of propofol andmidazolam corresponds with the differences in the type of medicalservice providers. For midazolam, there were large proportions ofusers in Seoul, Gyeonggi, and Busan, where most large tertiary hos-pitals are located. Compared to midazolam, the use of propofol wasmostly in Gyeonggi, where there are a number of primary care clin-ics, rather than large tertiary hospitals.
The distributions of endoscopy frequencies for each patientwere analyzed, and one patient case of 114 endoscopic examina-tions under sedation with midazolam is shown in detail. Thisextreme case is an example of a substantial misuse and suspectedabuse of a sedative in patients receiving endoscopy. Several othercases that demonstrated abuse potential of sedatives were alsoidentified in our study. A case of a young woman who visited sev-eral different hospitals in Korea for more than 100 endoscopicexaminations for the sole purpose of receiving propofol injectionshas been previously reported (Kim, 2012). A study by Ahn (2010)reported that 20 autopsy referrals for mysterious deaths thatoccurred outside of hospitals found the deaths to be related topropofol abuse in 2000–2009. Similarly, Iwersen-Bergmann et al.(2001) reported a case of a 26-year-old male nurse in Germanywho died from chronic propofol abuse.
The healthcare professionals and system may have a large rolein sedative abuse. Although all medical procedures and medica-tions that a patient receives are documented, the records are notnecessarily shared real-time among different healthcare profes-sionals. Therefore, if a patient intentionally doctor-shops for a pur-pose of receiving a certain medical procedure or a prescription, it isdifficult for the doctor to know all medical history of the patient.Due to the lack of an interactive record sharing system, retrospec-tive drug review can be a meaningful resource for identifying theusage patterns. Currently, Korean government and medical institu-tions are collaborating to create a system where different health-care providers can share the medical records wherever patientsreceive medical care.
This study has several strengths. It is the first study conducted ata national level to quantify the trends of sedative use in non-operative outpatient endoscopy. We analyzed the proportion ofthe entire Korean patient population who met the inclusion criteria,instead of using extracted sample data or presenting individual casereports. Also, to accurately evaluate the trends of sedative abuse, weonly included sedative use in non-operative endoscopies performedon an outpatient basis. Sedation for surgery or sedation given duringhospitalization is considered more clinically serious and is less likelyto lead to abuse; these were excluded from analysis.
The present study also has some limitations. Even though theKorean National Health Insurance system covers the entire popula-tion, and all medical information is transmitted to HIRA, some med-ical services and dispensed medications that are not covered byinsurance or are paid by the patients per request are not included.Because of this, many patients who are addicted to sedatives suchas propofol prefer to pay out of pocket for its use, and these occa-sions may not be recorded. It is possible that many sedative abusecases were left out due to a lack of data and therefore this studymight have underestimated the number of patients receiving endo-scopy with sedation. Also, we were not able to examine the specificindication of each case; however, we excluded the sedative use insurgery and hospitalization from study subjects. Therefore, the pos-sibility of including critical cases requiring a clinical review wasminimal. Further study is needed to evaluate drug abuse in this set-ting, covering cases that may not have been recorded in the claimsdatabase. Finally, more in-depth analysis is needed to investigatethe indications for each case, the risk of drug dependence afterrepeated exposure, and the characteristics of such at-risk patients.
5. Conclusion
Although midazolam was the most used sedative during thestudy period, the use of propofol increased sharply between 2008and 2012 in Korea. With such a continuous increase, the potentialfor misuse and abuse of propofol also rises. Suspected cases ofabuse were identified mainly with propofol and midazolam whilediazepam and lorazepam were not used as repetitively as the othertwo sedatives. It is important that medical service providers usecaution when using sedatives for endoscopy, by carefully review-ing patients’ medical history in order to select an appropriate agentfor the procedure. In addition, patients should be provided withinformation on the abuse potential of sedatives.
Acknowledgements
This study was supported by the Korean Ministry of Food andDrug Safety (MFDS) (No. 14172-174). The authors would like tothank the Korean Health Insurance Review and AssessmentService for providing the insurance claims data. Special thanksare due to Hannah Shin and Sohyun Choi for their help with draw-ing the figures and tables.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.yrtph.2015.01.007.
References
Bendiksen, A., Larsen, L., 1998. Convulsions, ataxia and hallucinations followingpropofol. Acta Anaesthesiol. Scand. 42, 739–741.
Brandt, L.J., 2001. Patients’ attitudes and apprehensions about endoscopy: how tocalm troubled waters. Am. J. Gastroenterol. 96, 280–284.
Carlsson, U., Grattidge, P., 1995. Sedation for upper gastrointestinal endoscopy: acomparative study of propofol and midazolam. Endoscopy 27, 240–243.

570 J.-Y. Shin et al. / Regulatory Toxicology and Pharmacology 71 (2015) 565–570
Faulx, A.L. et al., 2005. The changing landscape of practice patterns regardingunsedated endoscopy and propofol use: a national Web survey. Gastrointest.Endosc. 62, 9–15.
Follette, J.W., Farley, W.J., 1992. Anesthesiologist addicted to propofol.Anesthesiology 77, 817–818.
Hirota, W.K. et al., 2006. ASGE guideline: the role of endoscopy in the surveillance ofpremalignant conditions of the upper GI tract. Gastrointest. Endosc. 63, 570–580.
Inadomi, J.M. et al., 2010. Projected increased growth rate of anesthesiaprofessional–delivered sedation for colonoscopy and EGD in the UnitedStates: 2009 to 2015. Gastrointest. Endosc. 72, 580–586.
Iwersen-Bergmann, S. et al., 2001. Death after excessive propofol abuse. Int. J. LegalMed. 114, 248–251.
Kim, D.-K., 2012. Propofol use for sedation or sedation for propofol use? J.Anesthesia 26, 289–291.
Kim, J.H. et al., 2013. Abuse potential of propofol used for sedation in gastricendoscopy and its correlation with subject characteristics. Korean J.Anesthesiol. 65, 403–409.
Koshy, G. et al., 2000. Propofol versus midazolam and meperidine for conscioussedation in GI endoscopy. Am. J. Gastroenterol. 95, 1476–1479.
Liu, H. et al., 2012. Utilization of anesthesia services during outpatient endoscopiesand colonoscopies and associated spending in 2003–2009. JAMA 307, 1178–1184.
Ljubicic, N. et al., 2003. Efficacy and safety of propofol sedation during urgent uppergastrointestinal endoscopy – a prospective study. Collegium Antropologicum27, 189–195.
Ml, M.V. et al., 2000. Erotic hallucinations associated with the use of propofol.Revista española de anestesiología y reanimación 47, 90–92.
National Cancer Information Center, National Cancer Screening Program.Pain, L. et al., 2002. In vivo dopamine measurements in the nucleus accumbens after
nonanesthetic and anesthetic doses of propofol in rats. Anesth. Analg. 95, 915–919.
Riphaus, A. et al., 2006. Quality of psychomotor recovery after propofol sedation forroutine endoscopy: a randomized, controlled study. Gastrointest. Endosc. 63,AB189.
Roh, S. et al., 2011. A case of propofol dependence after repeated use for endoscopy.Endoscopy 43, E362–E362.
Seifert, H. et al., 2000. Sedation with propofol plus midazolam versus propofol alonefor interventional endoscopic procedures: a prospective, randomized study.Aliment. Pharmacol. Ther. 14, 1207–1214.
Thomson, K., Knight, A., 1988. Hallucinations after propofol. Anaesthesia 43, 170–171.
Vargo, J.J., 2004. Propofol: a gastroenterologist’s perspective. Gastrointest. Endosc.Clin. N. Am. 14, 313–323.
Vargo, J.J. et al., 2002. Guidelines for the use of deep sedation and anesthesia for GIendoscopy. Gastrointest. Endosc. 56, 613–617.
Weerts, E.M. et al., 1999. Comparison of the intravenous reinforcing effects ofpropofol and methohexital in baboons. Drug Alcohol Depend. 57, 51–60.
WS, A., Study of the regulatory affairs and the abuse investigation on the propofol.Research report of National Institute of Food and Drug Safety Evaluation 2010.<http://img.kisti.re.kr/originalView/originalView.jsp?url=/tr_img/2010206/trko201000015755.pdf>.
Zacny, J.P. et al., 1993. Propofol at a subanesthetic dose may have abuse potential inhealthy volunteers. Anesth. Analg. 77, 544–552.


















