
REGIONAL COLLEGE LECTURE Acute Medicine Is it time for a ...
75
Dr Mark Holland Consultant Physician in Acute Medicine, Salford Royal Hospital Visiting Professor University of Bolton REGIONAL COLLEGE LECTURE Acute Medicine – Is it time for a rethink?
Transcript of REGIONAL COLLEGE LECTURE Acute Medicine Is it time for a ...

Dr Mark Holland Consultant Physician in Acute Medicine, Salford Royal Hospital
Visiting Professor University of Bolton
REGIONAL COLLEGE LECTURE Acute Medicine – Is it time for a rethink?

Salford EAU AEC

Emergency Village AEC
ED EAU

Take Home Message 1
• There is more that unites us than that which divides us oThere is enough work to go round oPeople relationships are key

What is Acute Medicine?

Dr Kevin Jones Royal Bolton Hospital
“When I was a junior doctor, the hospital take at weekends was completely run by the juniors – the least qualified doctors.
The consultants didn’t come in until Tuesday, when their job was to interview the survivors”

https://shop.rcplondon.ac.uk/products/acute-medical-care-the-right-person-in-the-right-setting-first-time http://www.rcpmedicalcare.org.uk/


Acute Medicine
• Processes • Ideology
oSenior people getting hands dirty oMDT oTraining oGeography of a unit oQuality improvement o (Research)
Patients Timely Intervention

In reality is it just about ‘flow’?
Source: A Dr Goddard Presentation

Take Home Message 2
• Acute medicine is a force for good oThe ideology is remains correct oBut what about the process?

Acute Medicine in ED – 2017 at SRFT
• Cortical Homunculus oThink of how our brain thinks of our body oHow is acute medicine really represented in ED?
https://en.wikipedia.org/wiki/Cortical_homunculus





Question: How much ‘surgery’ does medicine do?

Take Home Message 3
• The footprint of Acute Medicine in ED is more than the admission rate oBut should we even be in ED? o I think we should

SAMBA

Society for Acute Medicine Benchmarking Audit
• 2012 – 2018 • 2018
o24-hour audit 00.00-23.59 oThursday 28th June o6114 patients o127 registered units
123 hospitals o104 acute trusts
http://www.acutemedicine.org.uk/wp-content/uploads/2017/12/Society-for-Acute-Medicine-Benchmarking-Audit-2017-National-Report.pdf
http://www.acutemedicine.org.uk/wp-content/uploads/2018/09/SAMBA18-Interim-Report-for-SAMBournemouth.pdf

SAMBA 18 – The Patients
361 340 418 549 743 965 1072 456 484 471 547 736 883 1246 1307 434 0
200
400
600
800
1000
1200
1400
16-29 30-39 40-49 50-59 60-69 70-79 80-89 90+
Nu
mb
er
of
Pat
ien
ts
Age Range
SAMBA17 Number
SAMBA18 Number
We all need to be geriatricians

51% of patients were double clerked

Really!!
• We have a workforce shortage oBut we are remarkably inefficient oTime for a change?

SRFT data
• 1078 patients over 28 days
o 63% are double clerked!!
• Source: Jennifer Tainsh

SRFT data ED versus Acute Medicine Clerking

Current assessment pathway ED Clerking
(currently 76% first clerkings at SRFT)
Acute Medicine non-consultant clerking
Acute Medicine Consultant Review
Patient Admission

New assessment pathway?
ED Clerking
Acute Medicine Consultant Review
(currently 10.4% at SRFT)

New assessment pathway? ED Clerking
Acute Medicine Consultant Review
Acute Medicine first Clerkings in ED Increase
Acute Medicine Consultant Review
At SRFT a consultant acute physician (bleep holder) monitors the ED tracking board and ‘pulls’ patients before they are referred

New assessment pathway? Time to First Clerking by Specialty

From SAMBA17

From SAMBA17

Take Home Message 4
• Emergency Medicine and Acute Medicine must plan care together
oThis type of change is possible
oThe barriers will be people
Culture inhibiting progress?
Threat or oppurtunity

SAMBA

From SAMBA17
31% of patients are
frail

From SAMBA17

From SAMBA17

From SAMBA17

From SAMBA17

From SAMBA17
Issues raised 1. Frailty or co-morbidity 2. Training

From SAMBA17

Take Home Message 5
• Acute Medicine is a shared problem oDo we just have ‘specialists’? oMaking internal medicine training fit for purpose is a priority
Managing frailty and older people must be a universal skill

Standards • How can we audit standards when the model of care has changed?
• So many standards oWest Midlnads / SAM
oKeogh
o London
oNICE
• The challenge now
oReduce variability

SAMBA18 • Site level data- organisation and delivery of acute medical care
o Numbers of staff/beds/critical care beds
o Elderly care ‘take’, frailty units, surgical units
o Access to point of care (POC) diagnostics
• Patient level data o Clinical quality indicators (CQI)
EWS on admission
Time to first assessment
Time to see a consultant physician
Readmission rate
Mortality at 7-days

0
10
20
30
40
50
60
70
80
90
100
1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 69 73 77 81 85 89 93 97 101105109113117121125
Variation in % of patients >80 years old%age of Patients > 80 years old

0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
50.00
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87 89 91 93 95 97 99 101
103
105
107
109
111
113
115
117
119
121
123
125
127
Unit variation in % of patients who are being readmitted within 30 days%age of Patients readmitted within 30 days

0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
1 4 7
10
13
16
19
22
25
28
31
34
37
40
43
46
49
52
55
58
61
64
67
70
73
76
79
82
85
88
91
94
97
100
103
106
109
112
115
118
121
124
127
Variation in % of patients with NEWS < 3%age of Patients with NEWS < 3
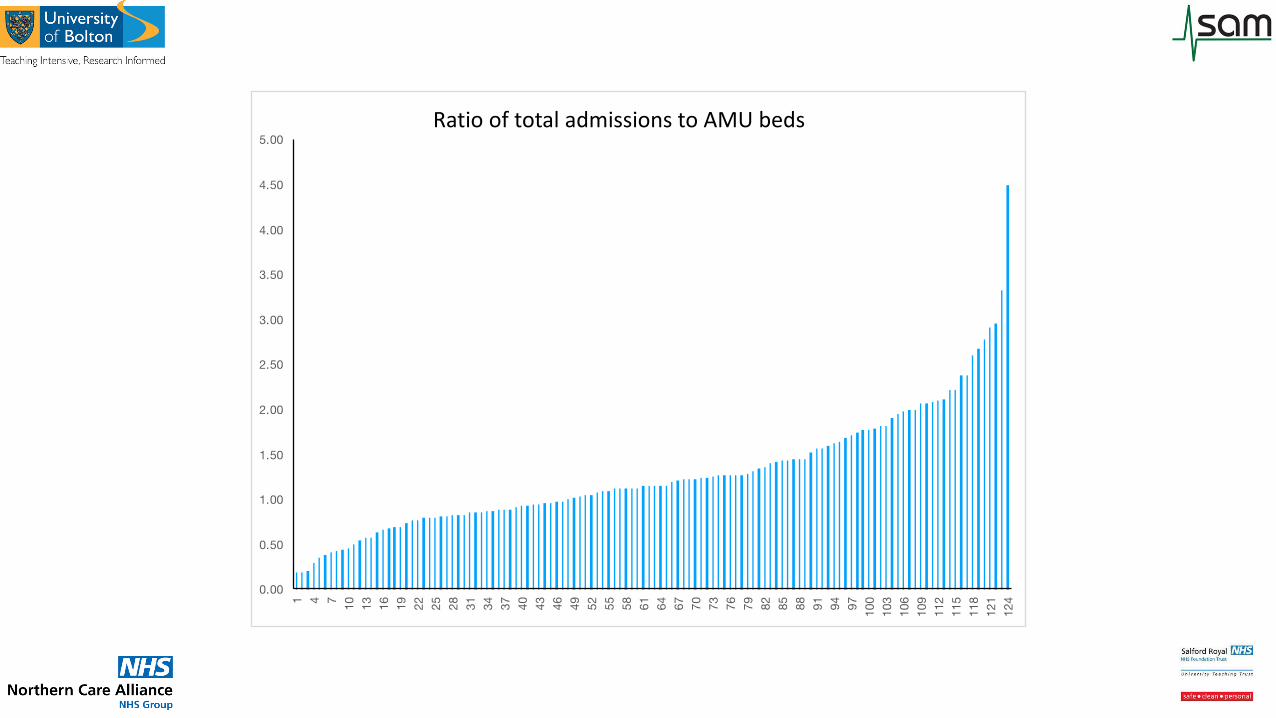
Ratio of total admissions to AMU beds

Take Home Message 6
• We do not know which model and processes work best

Quality

CQI 1 – EWS within 30 minutes of arrival
Variation in scoring systems
NEWS 75.3%
MEWS 10.8%
Hospital own 8.3%
NEWS2 2.5%
VIEWS 1.7%
SEWS 0.8%
84.1% of patients had EWS < 30 minutes of arrival
• AEC 82.2%
• ED 85.4%
• AMU 84.9%

0
10
20
30
40
50
60
70
80
90
100
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100 103 106 109 112 115 118 121 124 127
Variation in % EWS < 30 minutes
CQI 1 – EWS within 30 minutes of arrival

CQI 2 – Review by a competent clinical decision maker < 4 hours
• Tier 1 competent decision makers – capable of making an initial assessment of a patient with acute illness
• Includes oFY1 and above oAdvanced Care Practitioners oPhysician Associates
91.6% of patients reviewed < 4 hours
• AEC 95.0%
• AMU 88.9%
• ED 91.4%

0
10
20
30
40
50
60
70
80
90
100
1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 69 73 77 81 85 89 93 97 101105109113117121125
variation in % competent clinican review < 4 hoursCQI 2 – Review by a competent clinical decision maker < 4 hours

CQI 3 – Consultant review time
• Many patients spend a significant amount of their initial acute care journey in ED /waiting for a bed
• Capturing robust times for embedded process difficult to capture and validate (time referred to medicine, time seen by medicine, decision to admit)
• Time of arrival in hospital usually very well captured oMakes sense from the perspective of the patient

When should the clock start?
Presents to ED
Seen by ED
Seen in ED by medicine
Decision to admit
Arrives on AMU (or other ward)
Here?
Here?

CQI 3 – Consultant review time • SAM
o8 hours from admission if 08:00 – 20:00 o14 hours if admitted 20:00 – 08:00
• NICE Quality Standards o6 hours from admission if 08:00 – 20:00
• NHS England (ECIST) o3 hours daytime o12 hours overnight
• NHS England (7 day clinical services standards) o6 hours daytime o If predicted mortality 10% - consultant ‘involvement’ in 1 hour

CQI 3 – Consultant review time
• 62.8 % of patients requiring consultant review were seen within 12 hours of arrival in hospital
• AEC 73.8% (most well patients are being seen soonest) • AMU 65.3% • ED 59.0% (slower when patients double clerked)

0
10
20
30
40
50
60
70
80
90
100
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100 103 106 109 112 115 118 121 124 127
Variation in % of patients reviewed by consultant < 12 hours
CQI 3 – Consultant review time

CQI 4 - Hospital mortality rates for all patients admitted via AMU
• 7 day outcomes in SAMBA18
Outcome % of all SAMBA
patients
Died in hospital 2.01
In patient 23.18
Medically discharged 72.20
Self-discharged 1.31
Transferred 1.30

0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100103106109112115118121124
Variation in % of patients in hospital at 7 days %
of
pat
ien
ts%age patients discharged at 7 days

Ambulatory Emergency Care (AEC)
NHS Improvement
“We expect that hospitals introducing AEC could convert 30% of acute medical admissions to ambulatory care episodes”
https://improvement.nhs.uk/documents/2715/AEC_publications_index_intro.pdf

AEC
• 20.1% of patients had their first medical assessment in AEC o17% in 2017 for units with AEC
• 22% of units met the NHS Improvement expectation of 30% of first assessments being undertaken in AEC o8% in 2017
• Of patients seen in AEC o79.5% were sent home the same day

0.00
10.00
20.00
30.00
40.00
50.00
60.00
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100 103 106 109 112 115 118 121 124 127
Variation in % of initial medical assessments undertaken in AEC%age medical assessments in AEC

Take Home Message 7
• There is massive variation in processes and outcomes oHow representative is a one day audit? oCan data like this help us improve care?

Plug for Acute Medicine
• The notion of Acute Medicine based solely in AMU is dead
• Acute Medicine is bigger than AMU
oWe do need a new model
oMore not less
oWe need all the talents
• Rightly or wrongly
oAcute Medicine will always be part of the patient journey And in so doing we must design this care
oBoth RCP and RCEM must join forces

Plug for Acute Medicine
• This talk oNot full of answers
oFull of questions
=Curioisty
• = Research
o= The basis of a specialty which is truly coming of age

Plug for Acute Medicine
• My 7-day mortality rate is approximately 0.7%
oAcute Medicine is more than life and death
• Preclinical exams at St George’s Hospital Medical School 1983/84 YEAR 1 YEAR 2
oAnataomy Emryology and Ageing
oBiochemistry Neurosciences
oPhysiology Pathology
oMedical Statistics Clinical Pharmacology
Psychology / sociology
• Those subjects in red are what we did not value at the time
• Now they are at least, if not more important, in our day-to-day work

Plug for Acute Medicine
• Acute physician's are psychopaths

Emergency and acute medical care in over 16s: service delivery and organisation NICE guideline [NG94] Published date: March 2018
• In section 1.3.1 they say healthcare providers should: omonitor total acute hospital bed occupancy….. ohave capacity planning to minimise risks when occupancy rates exceed 90%

0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69
% bed occupancy during June 2018 of acute trusts submitting data to SAMBA18% bed occupancy in SAMBA18

0
5
10
15
20
25
AEC ED
Next ward after AEC and ED (% of admissions)
Direct to medical ward Direct to outly ing ward
Bypassing the AMU – % next ward after ED or AEC

SAMBA 18
• Increase in AEC activity
o91.6% at home at 7 days
o4.7% in hospital
o0.2% died

The SAMBA18 team • Cat Atkin • Tim Cooksley • Tom Cozens • Adnan Gebril • Mark Holland • Dan Lasserson • Ivan Le Jeune • LLiwen Jones • Madhu Kannan • Adrian Kennedy • Thomas Knight • Adam Seccombe • Christian Subbe

1. There is more that unites us than that which divides us
2. Acute medicine is a force for good
3. The footprint of Acute Medicine in ED is more than the admission rate
4. Emergency Medicine and Acute Medicine must plan together
5. Acute Medicine is a shared problem
6. We do not know which model and processes work best
7. There is massive variation in processes and outcomes
8. There is opportunity
9. Proper clinical medicine must be preserved

Thank you
I really do remember when this City had a decent football team!!


















