Redox imbalance in the critically ill
27
Redox imbalance in the critically ill John M C Gutteridge* and Jane Mitchell* *Oxygen Chemistry Laboratory, Directorate of Anaesthesia and Critical Care, Royal Brompton and Harefield NHS Trust, London, UK and Wnit of Critical Care Medicine, Imperial College Medical School at Royal Brompton Hospital, London, UK The majority of deaths amongst critically ill patients requiring intensive care are attributable to sepsis and its sequelae: septic shock, the systemic inflammatory response syndrome (SIRS) and the acute respiratory distress syndrome (ARDS). Clinically, sepsis/SIRS and ARDS are characterised by disordered vascular control, manifest as systemic hypotension and peripheral vasodilation refractory to intravascular volume resuscitation and vasopressor therapy; and pulmonary hypertension. Experimental and clinical evidence demonstrates that these patients suffer from severe oxidative stress. Thus, our own and other groups have shown that the vascular pathology of sepsis/SIRS and ARDS is initiated through the uncontrolled production of reactive oxygen (ROS) and reactive nitrogen species (RNS) which modulate inflammatory cell adhesion and cause direct injury to endothelium (Fig. 1). Redox balance between anti-oxidants and pro-oxidants In health, there is a balance between the formation of oxidising chemical species and their effective removal by protective anti-oxidants. Anti- oxidants are a diverse group of molecules with diverse functions. For example, they range from large highly specific proteinaceous molecules with catalytic properties to small lipid- and water-soluble molecules with non-specific scavenging or metal-chelating properties (reviewed by Gutteridge & Halliwell 1 ). Anti-oxidants might, therefore, be defined as substances which, when present at low concentrations compared to those correspondence to: Prof. o f the oxidisable substrate, significantly delay or inhibit oxidation of that John M c Guttendge, substrate 2 . Anti-oxidants, therefore, control the prevailing relationship Oxygen Chemistry . '. . ' i- • • • • i • i Laboratory, Directorate between reducing or oxidising (redox) conditions in biological systems. of Anaesthesia and Such control offers two major advantages: (i) the ability to remove toxic critical care. Royal levels of oxidants before they damage critical biological molecules; and (ii) ^' l ^ e a t»ility to manipulate changes, at the subtoxic level, of molecules that SThist sydne^treet London sw3 6NP, UK can function as signal, trigger or messenger carriers 3 - 4 . British Medical Bulletin 1999;55 (No. 1): 49-75 C The British Council 1999 Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396 by guest on 22 March 2018
Transcript of Redox imbalance in the critically ill

Redox imbalance in the critically ill
John M C Gutteridge* and Jane Mitchell**Oxygen Chemistry Laboratory, Directorate of Anaesthesia and Critical Care, Royal Brompton andHarefield NHS Trust, London, UK and Wnit of Critical Care Medicine, Imperial College MedicalSchool at Royal Brompton Hospital, London, UK
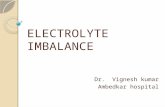
The majority of deaths amongst critically ill patients requiring intensive care areattributable to sepsis and its sequelae: septic shock, the systemic inflammatoryresponse syndrome (SIRS) and the acute respiratory distress syndrome (ARDS).Clinically, sepsis/SIRS and ARDS are characterised by disordered vascular control,manifest as systemic hypotension and peripheral vasodilation refractory tointravascular volume resuscitation and vasopressor therapy; and pulmonaryhypertension. Experimental and clinical evidence demonstrates that thesepatients suffer from severe oxidative stress. Thus, our own and other groupshave shown that the vascular pathology of sepsis/SIRS and ARDS is initiatedthrough the uncontrolled production of reactive oxygen (ROS) and reactivenitrogen species (RNS) which modulate inflammatory cell adhesion and causedirect injury to endothelium (Fig. 1).
Redox balance between anti-oxidants and pro-oxidants
In health, there is a balance between the formation of oxidising chemicalspecies and their effective removal by protective anti-oxidants. Anti-oxidants are a diverse group of molecules with diverse functions. Forexample, they range from large highly specific proteinaceous moleculeswith catalytic properties to small lipid- and water-soluble molecules withnon-specific scavenging or metal-chelating properties (reviewed byGutteridge & Halliwell1). Anti-oxidants might, therefore, be defined assubstances which, when present at low concentrations compared to those
correspondence to: Prof. of the oxidisable substrate, significantly delay or inhibit oxidation of thatJohn M c Guttendge, substrate2. Anti-oxidants, therefore, control the prevailing relationship
Oxygen Chemistry . ' . . ' i- • • • • i • i
Laboratory, Directorate between reducing or oxidising (redox) conditions in biological systems.of Anaesthesia and Such control offers two major advantages: (i) the ability to remove toxiccritical care. Royal levels of oxidants before they damage critical biological molecules; and (ii)
^' l ^ e at»ility to manipulate changes, at the subtoxic level, of molecules thatSThist sydne^treetLondon sw3 6NP, UK can function as signal, trigger or messenger carriers3-4.
British Medical Bulletin 1999;55 (No. 1): 49-75 C The British Council 1999
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
SepsisInflammationTissue damage
Infection
VASCULARFUNCTION &STRUCTURE
Membranephospholipids"
Arachidonicacid release
Isoprostanes
Oxidativestress
Activated leukocytesSubstrate auloxidaliuns
HighPO2
REDOXSIGNALLING
PAF-VASCULAR
FUNCTION &STRUCTURE
Antioxidantregulation
Peroxides, aldehydesRO\ RO-2 (HNE)
oxidation, hydroxylationchlorination, nitration
base damagesuear damage
GCMSdetection
•Proliferation•Apoptosis•Necrosis•Protection (gene regulation)•Heat shock proteins
Antioxidantprotection
Antioxidantrepair
Acute phaseproteins
Fig. 1 The possible role of reactive oxygen species (ROS) in modulating the effects of inflammation on vascularstructure and function. PO2 denotes oxygen tension; COX, cyclo-oxygenase; LO, lipid oxidation; PGs, prostaglandins;TxAy thromboxane A^ LTs, leukotrienes; PAF, platelet activating factor; HjO^ hydrogen peroxide; O2", superoxideanion; NO', nitric oxide; HOCI, hypochlorous acid; FeO2*, ferryl species; "OH, hydroxyl radical; ONOO-, peroxynrtrite;RO", alkoxyl radical; RO2* peroxyl radical; HNE, 4-hydroxy-2-nonenal; DNA, deoxyribonucleic acid; and GC-MS, gaschromatography-mass spectrometry.
Plasma and tissue anti-oxidants operate at primary, secondary andtertiary levels mainly as constitutive molecules. However, it is becomingincreasingly clear that inducible anti-oxidants upregulated by oxidativestress can also play key roles in body protection.
The authors consider 'primary' defences to be those which preventradical formation. The iron-binding properties of transferrin and lacto-ferrin fulfil such roles in extracellular fluids, since iron correctly attachedto their high-affinity binding sites no longer catalyses radical formations5.'Secondary' defences are those which remove, or inactivate, formedreactive oxygen species (ROS). In some cases they may be enzymes such asthe superoxide dismutases (SOD), catalase and glutathione peroxidase, orlow molecular mass molecules such as vitamin E, ascorbate and gluta-
50 British Medical Bulletin 1999;5S (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
thione (GSH). 'Tertiary' defences operate to remove and repair oxidativelydamaged molecules and are particularly important for DNA integrity.
Cellular anti-oxidant defences
Oxygen metabolism occurs within cells, where anti-oxidants have evolvedto deal speedily and specificaUy with reactive oxidants or reductants. Aspreviously mentioned, these are likely to be proteinaceous catalysts, i.e.enzymes.
The superoxide dismutases (SODs) rapidly promote the dismutationof superoxide (O"2~) into hydrogen peroxide (I-^O^ and oxygen at a rateconsiderably faster than it occurs uncatalysed (Eq. I)6.
2O\,- + 2H+ - H2O2 + O2 Eq. 1
Three forms of SOD are present in the body; copper-zinc SOD (CuZn-SOD) in the cytoplasm, manganese SOD (Mn-SOD) in the mitochondria,and extracellular SOD (EC-SOD) the major form in the extracellularmatrix7.
Hydrogen peroxide, a product of the dismutation reaction, can bedestroyed by two different enzymes, namely catalase (Eq. 2) and gluta-thione peroxidase (GSHPx), a selenium-containing enzyme requiringglutathione (GSH) (Eq. 3).
2H2O2 - O2 + 2H2O Eq. 2
H2O2 + 2GSH — GSSG + 2H2O Eq. 3
During normal oxygen metabolism, enzymes such as these function assecondary anti-oxidants to eliminate toxic intermediates of oxygeninside the cell.
Minimizing intracellular radical reactions is an obvious primary anti-oxidant mechanism that must have evolved to restrict oxygen toxicity. Agood example of this is cytochrome oxidase, the terminal oxidase of themitochondrial electron transport chain which, while functioning catalytic-ally, does not release reactive oxygen intermediates from its active centre8.The great advantage to the cell of having constitutive catalysts as anti-oxidants is that, like all catalysts, they are not consumed during theirnormal functioning.
Membrane anti-oxidant defences
Within the hydrophobic lipid interior of membranes, different types oflipophilic radicals are formed to those seen in the intracellular aqueous
British Medial Bulletin 1999;55 (No. 1) 51
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
milieu. Lipophilic radicals require different types of anti-oxidants fortheir removal. Vitamin E (ct-tocopherol), a fat-soluble vitamin, is a pooranti-oxidant outside a membrane bilayer but is extremely effective whenstructurally incorporated into it9. Lipid soluble anti-oxidants are,therefore, extremely important in protecting membrane polyunsaturatedfatty acids (PUFAs) from undergoing autocatalytic free radical chainreactions known as lipid peroxidation. The peroxidation of a PUFAleads to its destruction and the formation of a plethora of oxidationproducts such as lipid peroxides, carbonyls and carboxylic acids. Manyof these are biologically reactive and may be used as signal molecules bythe body10-11.
The way in which a membrane is structured from its lipids appears toplay an important role in decreasing its susceptibility to oxidative damage.Thus, structural integrity requires that the correct ratios of phospholipidand cholesterol are present as well as the correct phospholipids and then-fatty acid side chains9.
Extracellular anti-oxidant defences
Normally, enzymes such as the intracellular SODs, catalase and gluta-thione peroxidase are not present in extracellular fluids. Nevertheless,extracellular fluids are often subjected to fluxes of superoxide (O*2~),nitric oxide (NO), hypochlorous acid (HOC1) and hydrogen peroxide(H2O2) by 'activated' phagocytic cells and some ROS can also arise byauto-oxidation reactions.
Blood is an effective anti-oxidant 'buffering' system with both plasmaand red blood cells offering their own specialised protective systems.Red blood cells (RBCs) have an anion channel through which O'2~ canenter the cell and be destroyed by CuZnSOD. Hydrogen peroxide is anuncharged molecule, which behaves much like water and can bedestroyed by RBC catalase and glutathione peroxidase. Unlike plasma,RBCs contain high levels of GSH. Plasma contains both primary andsecondary anti-oxidants and is usually a powerful inhibitor of freeradical reactions. The question 'what is the most important plasmaantioxidant?' is often asked. To this, there is no simple answer since theexperimental findings change with the pro-oxidant used to bring aboutdetectable oxidation. Thus, vitamin E is reported to be the mostimportant, and one of the least important, plasma anti-oxidants,depending on the different reaction conditions used12*13.
When plasma was first tested for its anti-oxidant activity towards aperoxidising brain homogenate, activity was found to be mainlyproteinaceous14. Detailed fractionation studies later revealed that almostall of this activity resided in two plasma proteins representing no more
52 British Medical Bulletin 1999;5S (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
than 4% of the total13. In normal human plasma, these proteins wereidentified as transferrin and caeruloplasmin13'15. Apotransferrin bindstwo moles of ferric ion per mole of protein with high affinity, producinga coloured complex absorbing at 460 nm. The iron transport proteintransferrin is normally one-third loaded with iron and keeps theconcentration of 'free' iron in plasma at effectively zero. Iron bound totransferrin will not participate in radical reactions, and the availableiron-binding capacity gives it a powerful antioxidant property towardsiron-stimulated radical reactions5. Similar considerations apply tolactoferrin5 which, like transferrin, can bind two moles of iron per moleof protein, but hold onto its iron down to pH values as low as 4.0. Themajor copper-containing protein of human plasma is caeruloplasmin,unique for its intense azure blue colouration. Apart from its knownresponse as an acute-phase reactant its biological functions remain anenigma. Suggestions that it plays a major role in iron metabolism as aferroxidase enzyme (catalysing the oxidation of ferrous ions to the ferricstate for binding to transferrin) have not been widely accepted (reviewedin Gutteridge &c Stocks16). However, the protein's ferroxidase activitymakes a major contribution to the anti-oxidant activities of extracellularfluids113'16. Haptoglobins are glycoproteins found in the a-1-globulinfraction of serum that respond as 'acute-phase' proteins. They bindhaemoglobin (both oxy- and met-) in a 1:1 ratio to form a stablecomplex which has one of the strongest non-covalent protein bondsknown. The normal level of circulating haptoglobin is sufficient to bindsome 3 g of haemoglobin, making sure that no free haemoglobin isnormally present in plasma. Free haemoglobin has the potential tostimulate lipid peroxidation17 as well as to undergo degradation with therelease of reactive forms of iron18. Binding to haptoglobin prevents, ordecreases, both of these pro-oxidant properties of haemoglobin19.Haemopexin is a plasma p-glycoprotein that binds haem tightly in a 1:1ratio to form a pink-coloured complex. When delivering haem to cells,the haemopexin molecule is not degraded and returns to the circulationas a intact protein20 in much the same way as apotransferrin. Haem ironis a reactive form that promotes several radical reactions including lipidperoxidation, a process which is strongly inhibited by haemopexin21.
In addition to these proteins, albumin should also be considered animportant extracellular anti-oxidant. Albumin is a highly water-solubleprotein with important binding, transporting, 'solubilizing', and osmoticproperties. It has one high affinity copper-binding site but, like mostother proteins, readily and non-specifically binds copper ions at manyother sites. Albumin, therefore, effectively inhibits copper-stimulatedradical damage in most systems. Albumin can also scavengehypochlorous acid and peroxyl radicals (RO'2) and decrease damagedone by iron salts (reviewed in Halliwell22). The large amount of
British Medical Bulletin 1999;55 (No. 1) 53
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
albumin present in fluids, its oxidisable thiol group, its high turnover,and the resilience of the molecule to structural damage make it animportant sacrificial, or secondary, anti-oxidant. When consideringiron-binding proteins as primary anti-oxidants, it should be emphasisedthat they evolved for the conservation and transportation of iron in thebody. An essential, but secondary, requirement is that, whilst doing so,they do not allow iron to express its powerful pro-oxidant properties1-2.
Plasma also contains a large number of low molecular mass molecules,many of which are redox active, that have been ascribed secondary anti-oxidant roles as non-specific scavengers of free radicals. These areconsumed during their reactions with radicals examples being, uric acid,vitamin E, ascorbic acid and bilirubin (reviewed by Krinski23). Several ofthese anti-oxidants are important vitamins which has, in the past, led toover-simplistic clinical trials being designed with the aim of investigatingtheix ability to reverse life-threatening diseases.
Signalling by redox control
Redox reactive biological species
The oxidation-reduction (redox) potential of biological ions ormolecules is a measure of their tendency to lose an electron (therebybeing oxidised), and is expressed as EQ in volts. The more stronglyreducing an ion or molecule, the more negative is its EQ. It is becomingincreasingly clear that control of redox balance by anti-oxidants playsan important role in cellular signalling.
Reactive oxygen species (ROS)
The oxygen molecule is used biologically to oxidise (burn) carbon- andhydrogen-rich molecules to obtain the chemical energy and heatessential for life. In the process of this, the oxygen molecule is reducedto water, by a stepwise addition of 4 electrons, giving rise to inter-mediate reactive oxygen species - some of which are free radicals. A freeradical may be defined as any chemical species having one, or more,unpaired electron(s). The unpaired electron of a free radical isrepresented as a bold dot ('). The four-electron reduction of oxygen towater gives rise to the superoxide anion radical (O'2~), hydrogenperoxide, and the hydroxyl radical ('OH). The superoxide radicalrepresented as O*2" is often shown as O2~ since it is less of a radical thanmolecular oxygen (having two unpaired electrons O2", which are notnormally shown in this way). Superoxide is produced in numerousbiological processes, particularly the electron transport chains of
54 British Medical Bulletin 1999;55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
mitochondria and the endoplasmic reticulum (reviewed by Chance etal.s). Production of superoxide by activated phagocytic cells is one of themost studied radical-producing systems24. When opsonized particles arecontacted by neutrophils a 'respiratory burst' occurs, with oxygenuptake and the release of superoxide radicals into the phagocyticvacuole. Neutrophils in the presence of hydrogen peroxide, which isformed by the dismutation of superoxide, can also oxidise chloride ions(Ch) into the powerful oxidant hypochlorous acid (HOC1) (Eq. 5).
H+
H2O2 + Ch • HOCI + H2O Eq. 5
Myeloperoxidase
Hypochlorous acid and hydrogen peroxide are reactive oxygen species(ROS), but they are not free radicals since they do not contain unpairedelectrons. The enzymatic generation of reactive oxygen species byactivated phagocytic cells has evolved as a purposeful contribution tohost defence. The superoxide radical is not a particularly reactive speciesin aqueous solution and is not able to oxidatively damage mostbiological molecules. However, there are a few vulnerable sites withincells at which O"2" can do some direct damage (reviewed by Halliwell &Gutteridge2). Any system producing superoxide would also be expectedto produce hydrogen peroxide, by the dismutation reaction (Eq. 1).
2H+
2OV • 2H2°2 + °2 E c 1 - 1
This reaction (Eq. 1) is greatly accelerated when catalysed by theubiquitous superoxide dismutase enzymes, which remove O*2" fromsolution at the expense of forming hydrogen peroxide. In the absence oftransition metal ions, hydrogen peroxide is relatively stable and candiffuse across membranes in much the same way as water. Superoxidecan react with hypochlorous acid to form hydroxyl radicals ("OH)25, andboth hydrogen peroxide and hypochlorous acid26 can react with reactiveiron species to generate ('OH) radicals. The reaction of iron salts withhydrogen peroxide and hypochlorite to generate a powerful oxidant wasfirst described by Fenton in the 1890s27. We now know that the simplesequence represented in Equation 7, known as the 'Fenton reaction',involves higher oxidation states of iron and is considerably morecomplex than shown.
Fe" + H2O2 - Fe1" + OH" + 'OH Eq. 6
Hydroxyl radicals in free solution can attack most biological moleculesat almost diffusion-controlled rates, but have little or no specificity inFenton chemistry, they have considerable site-specificity because the
British Medical Bulletin 1999;55 (No. 1) 55
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
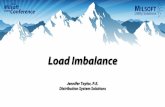
Fig. 2 The derivationof reactive oxygenspecies. NO", nitricoxide; Cu1, copper;
Fe", iron;Hb, haemoglobin;
e~, electron; andDNA, deoxyribo
nudeic acid.
Molecularoxygen
Superoxideanion
Hydrogenperoxide
H 2 O 2 0°
Hydroxylradical Water
NO*
peroxynitrite
H+
Oxidation ofproteins, lipids
&DNA
Transitionmetals,
(e.g. Cu'.Fe11)
HbFe
ferryl haem
Protein-, lipid- and DNA-based radicals,and oxidative changes to lipids, proteins & DNA
hydroxyl radical is formed close to where the iron is located (reviewedby Symons &C Gutteridge28).
Excessive biological production of superoxide can generate all theingredients necessary for the formation of hydroxyl radicals. Superoxidecan form hydrogen peroxide and release and reduce reactive forms ofiron. This sequence is often described as the 'superoxide-driven' Fentonreaction (Fig. 2).
The reactive oxygens and free radicals so far discussed are lowmolecular mass inorganic molecules. However, organic oxygen radicalsof biological polymers are equally important in biological systems withprotein, carbohydrate, lipid and DNA free radicals constantly formed inthe body. When the lipid is a PUFA, free radical attack results in aradical chain reaction known as lipid peroxidation.
Reactive nitrogen species (RNS)
Nitrogen gas accounts for 78 % by volume of the earth's atmosphere andbecause of its inert properties it is a major global anti-oxidant deterringcombustion and other oxidative processes.
56 British Medial Bulletin 1999,55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
Three simple oxides of nitrogen are of current biomedical interest;nitrous oxide (N2O), a colourless gas with anaesthetic properties(laughing gas), nitrogen dioxide (NO"2), a toxic brown colouredparamagnetic gas (free radical) which exists in equilibrium with itsdimer dinitrogen tetroxide (peroxide) N2O4, and nitric oxide (NO').Nitrogen dioxide is an environmental pollutant and may be produced invivo from reactions of NO'. It is an initiator of lipid peroxidation29.Nitric oxide is a colourless gas and a weak reducing agent, firstrecognised by Joseph Priestley in 1772. Biological interest in NO' andother RNS has exploded since the recent observation that the vascularendothelium and other cells in the body produce small amounts of itfrom the amino acid L-arginine (reviewed by Moncada & Higgs30).Nitric oxide is poorly reactive with most molecules in the human body(non-radicals), but as a free radical it can react extremely rapidly withothers such as superoxide, amino acid radicals, and certain transitionmetal ions. The reaction between NO' and superoxide (K̂ 6.7 x 109
M'V1) produces peroxynitrite (ONOO")31, which is, itself, a powerfuloxidant that can decompose to yield further oxidants with the chemicalreactivities of NO'2, 'OH and NO2
+. The exact chemistry of damage byONOO" is a matter of considerable current debate32-33. In addition to theputative 'accidental' generation of ROS/RNS in vivo, some are madedeliberately. For example, NO* has multiple physiological roles30.Activated phagocytes generate O*2", H2O2, NO' and (in the case ofneutrophils HOC1) as one of their many mechanisms for killing foreignorganisms24. NO' and possibly its derivatives (e.g. NO+) are widely usedphysiologically, whereas reactive RNS such as NO2' and ONOO" maybe too indiscriminately damaging. The interactions of RNS and ROS arealso important. H2O2 activates NF-KB34 but NO' inhibits activation35. Invascular endothelium, O"2" antagonises the action of NO" and causesvasoconstriction36 which may represent a physiological mechanism forregulating vascular tone37. Unfortunately, the rapid reaction of NO" withO"2" generates ONOO", a species possibly responsible for several of thecytotoxic effects attributed to excess NO", such as destruction of Fe-Sclusters in certain enzymes38. To add to this complexity, NO' modulatesdamage by ONOO". Peroxynitrite aggravates lipid peroxidation, butNO' reacts fast with the peroxyl radicals (ROO') that propagate thisprocess (Eq. 7)39.
NO' + ROO- — ROONO Eq. 7
If the resulting ROONO (organic peroxynitrite) species can bemetabolised without the release of free radicals, then NO' effectivelyinhibits lipid peroxidation. Clearly, the NO7ROS ratio is all important.Diminished availability of NO* and increased ROS formation may bekey events in the pathology of atherosclerosis39'40.
British Medical Bulletin 1999;55 (No. 1) 57
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
Reactive iron species (RIS)
Within cells, there normally exists a pool of low molecular mass redoxactive iron which is essential for the synthesis of iron-requiring enzymesand proteins, and for the synthesis of DNA. This pool of iron is thetarget of iron chelators and is also a form of iron sensed by ironregulatory proteins. The amount, and nature of the ligands attached tothis iron, remain unknown. However, a recently introduced fluorescenceassay based on calcein may enhance our knowledge of intracellular ironpools41. In contrast to the intracellular environment, extracellularcompartments do not normally require low molecular mass iron. Iron-binding proteins such as transferrin and lactoferrin do not even remotelyapproach saturation in healthy subjects, retaining considerable iron-binding capacity which removes mononuclear forms of iron that entercellular fluids. The differences between intracellular and extracellularcompartments and their requirements for low molecular mass irondeserves special comment since it is iron in this form that is the mostlikely catalyst of biological free radical reactions. Inside the cell, lowmolecular mass iron need not pose a serious threat as a free radicalcatalyst due to the presence of specific defenses to safely and speedilyremove all the O*2~ and H ^ and organic peroxides (such as lipidperoxides) that could react with such iron. This is achieved byintracellular enzymes such as the superoxide dismutases, catalase andglutathione peroxidase and possibly also by thioredoxin-dependentH2O2 removal systems. In the extracellular space, however, a differentpattern of protection is apparent. Here, proteins bind, conserve,transport and recycle iron and, whilst doing so, keep it in non- orpoorly-reactive forms that do not react with H2O2 or organic peroxides.Proteins such as transferrin and lactoferrin bind mononuclear iron,whereas haptoglobins bind haemoglobin19 and haemopexin bindshaem21. In addition, plasma contains a ferrous ion oxidising protein(ferroxidase) called caeruloplasmin16. By keeping iron in a poorlyreactive state, molecules such as O'2~, H2O2, NO', and lipid peroxidescan survive long enough to perform important and useful functions assignal, trigger and intercellular messenger molecules3'4. During situationsof iron-overload, plasma transferrin can become fully loaded with iron(100% iron saturation) and allow low molecular mass iron toaccumulate in the plasma. Such iron, when present in micromolarconcentrations, can bind to various added chelating agents such asEDTA, desferrioxamine and bleomycin that cannot abstract iron fromtransferrin. This non-transferrin bound iron can be associated withseveral ligands including citrate42 and other organic acids, and possiblyalbumin. Low molecular mass ligands for iron inside the cell are also asubject of considerable debate. ATP, ADP, GTP, pyrophosphates, inositolphosphates, amino acids and polypeptides have all been proposed.
58 British Medical Bulletin 1999,55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically i
In 1981, one of the authors introduced the 'bleomycin assay' as a firstattempt to detect and measure chelatable redox active iron that couldparticipate in free radical reactions43. The assay procedure is based onthe ability of the metal-ion binding glycopeptide antitumour antibioticbleomycin to degrade DNA in the presence of an iron salt, oxygen anda suitable iron reducing agent. Data obtained using the bleomycin assayin extracellular fluids for levels of RIS have recently been confirmed byquantitating such iron by its ability to activate the enzyme aconitase44.
Signalling through anti-oxidant control of redox balance
It has been suggested that certain ROS (and perhaps, by extension RISand RNS), might be used as signal, messenger and trigger molecules3-4'34.Increasing evidence of redox regulation of gene expression is ongoing;not only of oxyR (a bacterial reactive oxygen responsive transcriptionfactor) and nuclear factor KB (NFKB) but also the role of thioredoxinand of active protein 1 (AP-1). If redox balance is considered to play apivotal role in signalling cell functions, it becomes highly unlikely thatshort-term changes in anti-oxidants could influence this balance,perhaps explaining the poor record of anti-oxidant therapies to date.
Intracellular iron signalling
Cells normally accumulate iron via the binding of transferrin to highaffinity surface receptors (TfR) followed by endocytosis. There is also atransferrin-independent pathway of cellular iron uptake that is said toinvolve a ferri-reductase and an Fe" transmembrane transport system(reviewed by De Silva et a/.45). The reductase is proposed to provide ironin soluble form to the membrane transporter. When non-transferrinbound iron appears in plasma, due to iron-overload or lack oftransferrin (apotransferrinaemia), it is rapidly cleared by the membrane-bound transport system constitutively present on parenchymal cells;particularly those of liver, heart, pancreas and the adrenals. This systemdoes not require endocytosis of a protein for iron delivery. The rate ofsynthesis of TfR and ferritin is regulated at the post-transcriptional levelby cellular iron and co-ordinated by the iron-dependent binding ofcytosolic proteins called 'the iron responsive element binding proteins'(IRE-BP; now known as iron regulatory proteins, IRP) which bind tospecific sequences on their mRNA46. It appears that low molecular massiron is capable of acting as a signal to regulate ferritin and TfR synthesisin this way. In the absence of iron, ERP-I binds to the iron-responsiveelement (IRE) (the 3'-untranslated region of the TfR message contains aset of stem-loop structures termed IRE) stabilizing the transcript. Wheniron is present, the protein dissociates from the IRE and degradation of
British Medical Bulletin 1999;55 (No. 1) 59
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
the mRNA occurs. Recent work has shown that IRP-I is identical to thecytosolic enzyme aconitase47. The protein functions as an activeaconitase when it has an Fe-S cluster present or as an RNA-bindingprotein when iron is absent. Switching between these two forms dependson cellular iron-status.
Membrane signalling
Within the hydrophobic interior of membranes, lipophilic radicals areformed which are usually different from those seen in the intracellularaqueous space. Lipophilic radicals require hydrophobic anti-oxidants fortheir removal. a-Tocopherol, a fat-soluble vitamin, is a poor anti-oxidantoutside a membrane but is extremely effective when incorporated into themembrane bilayer9. Membrane stability and protection against oxidativeinsult depends very much on the way in which the membrane is assembledfrom its lipid components. Structural organisation requires that the'correct' ratios of phospholipids and their fatty acids are attached(reviewed by Gutteridge & Halliwell1 and Halliwell & Gutteridge2).
When a cell is damaged, or dies, it is highly likely that its membranelipids undergo peroxidation48. Tissue damage releases RIS and activatesenzymes which catalyse peroxidation of polyunsaturated fatty acids,particularly linoleic acid, leading to a build-up of lipid peroxides49.Peroxidation of membrane PUFAs produces a plethora of reactiveprimary peroxides and secondary carbonyls and it was suggested manyyears ago by one of the authors that lipid oxidation products such asthese resulting from cell death could act as triggers for new cell growth10.Through the detailed work of Esterbauer and colleagues50, clearerinsights into the biological reactivity of lipid oxidation products haveemerged. 4-Hydroxy-2-nonenal (HNE), a peroxidation product of (n-6)fatty acids (when RIS are present), is a potent trigger for chemotaxis, caninactive thiol-containing molecules, and activate certain enzymes(reviewed in Esterbauer et al.so). As a general rule, low levels of ROS,and possibly reactive carbonyls, activate cellular processes whilst higherlevels turn them off. The resting cell normally has a redox potential witha reduced state, and is progressively activated as oxidation increases.Too much oxidation deposes all function51 until eventually apoptosis ornecrosis is triggered.
Extracellular signalling
Human body extracellular fluids contain little, or no, catalase activityand extremely low levels of superoxide dismutase. Glutathioneperoxidases in both selenium-containing and non-selenium-containingforms are present in plasma but there is little glutathione substrate (1-2uM). 'Extracellular' superoxide dismutases (EC-SOD) have been
60 British Medical Bulletin 1999;S5 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
identified7 and shown to contain copper, zinc and attached carbohydrategroups. By allowing the limited survival of O"2~, H2O2 lipid peroxides(LOOH) and possibly other ROS/RNS in extracellular fluids the bodycan utilise these molecules, and others such as NO', as useful messenger,signal or trigger molecules3. A key feature of such a proposal is that O'2~,H2O2, LOOH, NO* and HOC1 do not meet with reactive iron or copperand that extracellular anti-oxidant protection has evolved to keep ironand copper in poorly or non-reactive forms3"52.
The major copper-containing protein of human plasma iscaeruloplasmin, unique for its intense blue colouration. The protein'sferroxidase activity makes a major contribution to extracellular anti-oxidant protection by decreasing ferrous salt-driven lipid peroxidationand Fenton chemistry16'53.
Physiological functions of reactive oxygens and nitrogen
Although the excessive generation of ROS at the site of inflammationmay contribute to cell injury, ROS formed in appropriate concentrationshave important signalling roles in the control of a range of physiologicalprocesses. There is increasing evidence that O*2~, H2O2 and ONOO" actas cell signalling molecules in the induction of a number of genes.Moreover, H2O2 is an important co-factor for a number of enzymesincluding guanylyl cyclase and cyclo-oxygenase54. Current interest,however, is strongly directed towards the biological functions of theRNS NO*, now recognised as being a ubiquitous smooth muscle cellrelaxant, with particular importance in the cardiovascular system.Moreover, NO* has potent anti-aggregatory and anti-adhesion effects onplatelets and other blood borne elements55. In most cells, NO* mediatesits regulatory effects by binding to the haem of soluble guanylylcyclase56, which activates the enzyme to cause cGMP production. Inhealthy blood vessels, NO* is predominantly formed by a constitutiveenzyme in endothelial cells (eNOS) which is activated by elevations inintracellular calcium57. In addition, some blood vessels are innervated bynitrergic nerves which also contain a constitutive form of NOS (nNOS).In general, the release of NO* by eNOS and nNOS actively maintainsblood flow without compromising cellular function.
In addition to its role in modulating vascular homeostasis, NO* is animportant endogenous bronchodilator and is implicated in gastricemptying and peristalsis55. Nerves in the central nervous system expresshigh levels of nNOS58, which has been implicated in a number offunctions, including memory.
In addition to the constitutive forms of nNOS and eNOS, an inducibleform exists (iNOS) which is expressed in white blood cells in response
British Medical Bulletin 1999;55 (No. 1) 61
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
to pathogens, endotoxin or some cytokines59. NO* formation by cellsexpressing iNOS tends to be relatively high and continuous. NO*released by immune cells, either directly or via combination with O"2" toform ONOO", is an important anti-microbial agent. However, theinappropriate expression of iNOS systemically or at the site ofinflammation can lead to over-production of NO*. Under similarconditions, there may well be an excess of O"2", leading to the formationof damaging ROS as discussed previously. Since excessive ROSproduction is thought to account for much of the tissue damage seen indiseases of the critically ill, therapeutic interventions designed tointerfere with oxidative balance may prove useful in some patients.
Redox imbalance in the critically ill
In this section, we examine some changes that can occur in the redoxbalance of patients under the care of a critical care unit (ICU) duringtheir illness.
/Acute respiratory distress syndrome (ARDS)
The syndrome of acute respiratory distress in adults (ARDS) ischaracterised by refractory hypoxaemia secondary to non-hydrostaticpulmonary oedema and is associated with a wide variety of precipitatingfactors, often not directly involving the lung (reviewed by Macnaughton& Evans60). Thus, ARDS can result from such diverse clinical conditionsas sepsis, gastric aspiration, polytrauma, pancreatitis, haemorrhagicshock, severe burns, oxygen toxicity, and cardiopulmonary bypass. Inspite of the increasing complexity and scientific basis of medicalsupport, ARDS still carries a mortality rate of around 50%, little haschanged from when it was first described61. The precise mechanisms thatlead to acute lung injury are at present unknown but recent evidencesuggests that patients with ARDS are exposed to a severe oxidativeburden from a variety of sources.
Anti-oxidant changes in ARDS
Primary anti-oxidants. In the preceding discussions, we defined andclassified plasma anti-oxidants by their biological sites of action andtheir specialised functions. Here we discuss some of the anti-oxidantchanges that have been reported to occur in the plasma, andbronchoalveolar lavage fluids, of patients with ARDS. Compared with
62 British Medical Bulletin 1999,55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
normal healthy control subjects, patients with ARDS (without multi-organ failure) show decreased levels of plasma iron-binding anti-oxidantactivity*2. The decreased ability of plasma to protect against ironstimulated oxygen radical formation correlates with the percentage ironsaturation of the transferrin. A small group of patients with ARDS,showing impaired liver function as part of their wider multi-organ failure,have low molecular mass iron present in their plasma63, and a high ironsaturation of their transferrin. In such cases, anti-oxidant protection isgreatly decreased, or even lost63. The primary plasma anti-oxidant,caeruloplasmin, is an acute phase protein, and, as such, concentrationsincrease in the plasma after tissue trauma. In animal experiments, plasmacaeruloplasmin increases after expose to hyperoxia by a mechanismindependent of the acute phase response64. In two recent studies ofpatients with ARDS, plasma caeruloplasmin levels were reported asraised62, and as normal65 compared to healthy controls. The latter findingis surprising in view of the known response of caeruloplasmin to traumaand hyperoxia. The iron oxidising anti-oxidant activity of ARDS plasmain the first study was, however, similar to that of control plasma, in spiteof the measured higher caeruloplasmin protein levels present. The reasonfor this remains unclear, but may suggest that some caeruloplasmin is notfully functional as a ferroxidase62. Caeruloplasmin is particularlysusceptible to proteolytic damage and increased proteolytic activity inplasma or lung tissue66, (where it is also synthesised), from patients withARDS, may contribute to the apparent loss of activity.
Secondary anti-oxidants. Numerous non-specific low molecular massmolecules present in plasma have been ascribed biological anti-oxidantproperties. These include glucose, uric acid, bilirubin, ascorbic acid,vitamin E and thiols (reviewed by Krinsky23). In addition, plasma alsocontains low concentrations of specific high molecular mass scavengers,such as EC-SOD, EC-glutathione peroxidase and catalase. Plasma fromhealthy individuals contains around 500 u.mol/1 of thiols mainlyassociated with the sulphydryl groups of plasma proteins. Plasma thiolvalues are, however, lower in patients with ARDS (around 300 nmol/1)67
and even lower than this when calculated for non-surviving patients67.Interestingly, non-survivors have higher levels of plasma proteinscompared with the survivors. The lung is a primary target for oxidantinjury and damage to lung tissue leads to a loss of sulphydryl groups ofboth protein and non-protein molecules (reviewed by Paterson &Rhoades68). Thiol groups are particularly susceptible to oxidation and canbe destroyed by biological oxidants such as hydrogen peroxide,peroxynitrite, iron salts, peroxyl and hydroxyl radicals. Patients withARDS have depleted levels of plasma, and red blood cell GSH (non-protein thiol)69. The anti-oxidant properties of the drug N-acetylcysteine,
British Medical Bulletin 1999;55 (No. 1) 63
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
together with the observed depletion of thiols in patients with ARDS,have led to clinical trials designed to replace or protect vital thiol groupsusing this drug. However, to date, these have not demonstrated thatthiol supplementation is of great benefit to patients with ARDS70. Lungepithelial lining fluid contains high concentrations of GSH comparedwith plasma from the same individual. Most of the GSH (96%) is in thereduced form, and at levels some 140-fold higher than those of plasma.Normal human plasma GSH values reported in the literature arevariable, probably due to the labile nature of the molecule and the non-specific methods used to measure it. However, it is likely that normalhuman plasma contains around 1-2 umol/1. Using fresh single plasmasamples randomly selected from 8 patients with ARDS, extremely lowlevels of ascorbate were found71, ranging from < 1 to 5 umol/1,compared with 49 ± 1 umol/1 in normal healthy controls. The findingswere interpreted as evidence of increased oxidative stress in vivo andsuggested that the low plasma ascorbate levels reflect increasedneutrophil activity. a-Tocopherol is carried in plasma by lipoproteins,for example, in LDL there are around six molecules of a-tocopherol foreach LDL particle. a-Tocopherol is a fat soluble anti-oxidant that offerslittle protection to the surrounding aqueous milieu9. In three separatestudies, plasma a-tocopherol levels have been reported to be low inpatients with ARDS with values of 7.73 ± 0.54 mg/1 (n = 12)71, 10.4 ±3.5 mg/1 (n = 25)72 and 4.0 mg/1 (n - 6)73, compared with normal healthycontrol values of 11.46 ± 0.55 mg/1 (n = 7), 14.9 ± 2.5 mg/1 (n = 16) and11.2 mg/1 (n = 7), respectively. In a follow-up study, the same group71
concluded that a-tocopherol was not significantly lower in patients withARDS when standardised to the total plasma cholesterol present.Hydrogen peroxide levels are increased in breath condensates of patientswith ARDS undergoing mechanical ventilation74-75, supporting theproposal that neutrophils, by producing ROS, play a major role in theoxidant stress that characterises the syndrome. However, only low orundetectable amounts of H2O2 are found in plasma extracts frompatients with ARDS72. When H2O2 destroying enzymes, such as catalaseand glutathione peroxidases, were measured in the serum of patientswith sepsis complicated by ARDS and appropriate controls, the formergroup had higher catalase activity76 which may explain the undetectablelevels of H2O2 in plasma. Interestingly, there was no evidence to supportred blood cell haemolysis as the origin of the increased serum catalase.Extending these studies to include serum manganese-containingsuperoxide dismutase (Mn-SOD), these researchers assessed enzymelevels and other protein makers and found that of 26 patients withsepsis, six who developed ARDS had higher serum levels of MnSOD andcatalase activity77.
64 British Medical Bulletin 1999;55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
Pro-oxidant changes
Patients with ARDS and multi-organ failure can saturate plasmatransferrin, revealing RIS in their plasma. Unlike plasma from normalhealthy controls, however, BAL fluids from the same controls contain RIS.This may in part explain why the lungs are so sensitive to oxidativedamage from hypoxia, hyperoxia, inhaled oxidants and 'activated'phagocytic cells.
Patients who survive ARDS have more chelatable RIS in their lavagethan controls78, but patients who do not have none78. This latter findingis compatible with increased alveolar capillary permeability leading tothe transfer of plasma proteins to the lung, one of which (transferrin)binds the chelatable iron. Suggestions that the leak of plasma anti-oxidant proteins into the lung is beneficial in ARDS79, may not be truesince survival appears to depend on the severity of lung leak. Poly-unsaturated fatty acids are highly susceptible to free radical mediatedoxidation, and many of the peroxidic and aldehydic products formedhave profound phamacological effects on cells (reviewed by Esterbaueret al.u). In an intensive care stay, patients with ARDS decrease theirplasma concentration (%) of total linoleic acid, but increase theirconcentrations of oleic and palmitoleic acids80. Such changes are highlycharacteristic of essential fatty acid deficiency disease and may becommon to many conditions characterised by oxidative stress wherebyROS act as signal molecules to alter desaturase enzymes81. If suchchanges are an adaptive response, it is difficult to understand why levelsof oleic acid are so increased in ARDS when this mono-unsaturated fattyacid is used pharmacologically in animal models to induce ARDS.
Xanthine dehydrogenase (XDH) is a widely distributed enzyme which,upon oxidation of its thiol groups or following limited proteolysis, isconverted to the oxidase (XOD) form. The oxidase enzyme utilises O2
as a co-factor in the oxidation of hypoxanthine and xanthine formingthe products, O\~, I^C^ and uric acid. Increased levels of XOD or itssubstrates, therefore, increase the formation of ROS. Increased levels ofXOD have been reported in the plasma of patients with ARDS82, andmore recently increased levels of plasma xanthine and hypoxanthine83.Plasma hypoxanthine levels in non-surviving patients (37.48 ± 3.1 uM)were far greater than those in survivors (15.24 ± 2.09 u.M), althoughboth were markedly increased compared to normal healthy controls(1.43 ± 0.38 uM)83.
Redox imbalance in patients with ARDS has two major implications.Firstly, production of toxic levels of ROS, RIS and RNS leads tomolecular damage of key molecules in cells. Secondly, sub-toxicincreases in ROS, RIS and RNS can signal changes in cellular responsessuch as proliferation, apoptosis, and necrosis (Fig. 1).
British Medical Bulletin 1999;55 (No. 1) 65
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
Septic shock
Sepsis is a major cause of mortality in intensive care units. The release ofendotoxin from the cell wall of Gram-negative bacteria is thought toinitiate the major symptoms of septic shock, although Gram-positivebacteria (which do not produce endotoxin) are equally implicated in theattributable mortality. Sepsis is, of course, a major complication of, ormay lead to, ARDS, and much of the literature deals with both conditions.In the following paragraphs we consider sepsis syndrome uncomplicatedlung injury.
Anti-oxidant changes
Studies detailing changes in tissue or plasma anti-oxidants in patientswith sepsis without lung injury are few. Most indicate that anti-oxidantimbalance is present in septic shock84-85. Attempts to correct this by theadministration of anti-oxidants has resulted in reported improvementsin measured haemodynamic variables86, although there is no evidencethat survival rates are favourably influenced by such regimens.
Pro-oxidant changes
Recent reports that plasma RIS are elevated in sepsis86"88 weresubsequently refuted89; the later investigation finding no RIS and evendecreased levels of total non-haem iron, consistent with the body's knowniron-withholding defence to microbial invasion90. Plasma levels of thiolsare lower89, whereas hypoxanthine levels are normal (11.12 ± 0.69 (xM)in patients with sepsis but no lung injury83. Interestingly, levels ofperoxides in the plasma appear to be some 3 times greater than normal91.
Pharmacological implications and interventions
Albumin is often administered to patients with sepsis as fluidresuscitation. Recently, we observed that infused albumin significantlyinfluenced the body's thiol pool, sustaining an increase in plasma thiollevels that may represent a useful repletion of an important anti-oxidant92. A recent discussion of the use of albumin administration incritically ill patients, however, concluded that it was associated withincreased mortality114'115. These data suggest that its continued use incertain critically ill patients requires urgent review.
Cardiopulmonary bypass (CPB)
Patients undergoing cardiopulmonary bypass for a variety of clinicalreasons are routinely transferred at the end of surgery to the critical care
66 British Medical Bulletin 1999;55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically i
unit for periods of up to 48 h. Most bypass patients show signs of asystemic inflammatory response syndrome and have evidence of mildlung injury. However, 1-2% of patients develop ARDS.
Antioxidant changes in CPB
Epidemiological studies suggest that both diet and lifestyle contributesignificantly to premature deaths from heart disease (reviewed byGutteridge93). In particular, micronutrients in fruits and vegetables,several of which are anti-oxidant vitamins, appear to be important long-term protectors against the premature development of atherosclerosis. Itis likely, therefore, that many of the patients receiving CPB surgery enterhospital with disturbed anti-oxidant/pro-oxidant profiles. Here,however, only those changes in primary anti-oxidants that occur duringthe course of surgery are considered.
Haemodilution, inherent in CPB, lowers the levels of all proteinaceousanti-oxidants in plasma. For example, iron-binding anti-oxidant pro-tection (dependent upon transferrin concentration and its percentagesaturation with iron) has been known to fall from 82% protectionbefore surgery to 53% postoperatively. Similarly, iron-oxidising anti-oxidant protection, dependent upon caeruloplasmin, fell from 77% to65% peri-operatively94. Furthermore, at a time when the concentrationof plasma transferrin was decreasing, its saturation with iron increasedfrom 40% to 57%95. In a follow-up study, transferrin saturationincreased from 27% to 62% peri-operatively96. In 90% of thesepatients, there was a significant correlation between the percent increasein iron saturation of transferrin and alveolar capillary permeabilityobserved using a radio isotopic technique96
Pro-oxidant changes during CPB
When blood is circulated extracorporeally through plastic tubing andpumps, it causes severe shear stresses to blood cells and activates severalenzyme cascades. As a result, red cells are lysed and release theircontents and neutrophils are 'activated' to produce O"2~ and H2O r
These ROS can react with free haemoglobin to form ferryl haemoglobinspecies and eventually disintegrate to release chelatable reactive ironspecies (RIS)18'95. In a recent study assessing the risk of iron releaseduring CPB, one of the authors95 showed that all patients increased thepercentage iron saturation of their transferrin, although, some (around13%) went into a plasma iron-overload state95. Extending this study toassess the effect of blood cardioplegia regimens on this observation, theincidence of plasma iron-overload increased to 18% for those receivingcold blood cardioplegia and to 27% for those receiving warm bloodcardioplegia98. The implication that the RIS detected in the plasma of
British Medical Bulletin 1999,55 (No. 1) 67
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

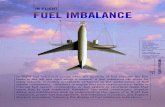
Table 1 Some evidence that patients with ARDS are under severe oxidative stress
Finding Comments Reference
Increased H2O2 in exhaled breath
Inactive a,-antiproteinase in bronchoalveolarlavage fluid (BAL)
Decreased levels of GSM in lung lavage fluid and RBCs
Loss of plasma thiol groups
Increased plasma protein carbonyl groups
Nitrotyrosine formation
Orthotyrosine formation
Chlorotyrosine formation
Presence of catalytic iron in the plasma (RIS)
Presence of catalytic iron in BAL fluid
Increased lipid peroxidatlon products in plasma
Increased plasma xanthine oxidase activity
Increased plasma hypoxanthine
Low levels of plasma ascorbate
Low levels of plasma a-tocopherol
Decreased plasma caeruloplasmin (Cp)'ferroxidase' activity
Low transfemn levels in plasma, with increased% saturation with iron
Breath vapour condensate from normal subjects contains little H2O2 74, 75
Probably damaged by ROS, RNS or reactive chlorine species
107
Increased levels of oxidised GSH (GSSG) found 69, 108
Non-survivors of ARDS often have lower —SH levels 67
Highly suggestive of oxidative damage by ROS 67
Immunostaining of lung tissue from ARDS patients revealed nrtrotyrosinesuggestive of damage by ONOO~ or other RNS 109
HPLC and GC-MS techniques show increased plasma levels of nrtrotyrosine inpatients with ARDS compared to controls 110
HPLC and GC-MS techniques show increased levels of plasma proteinorthotyrosine, suggestive of increased 'OH formation 110
HPLC and GC-MS techniques show increased levels of plasma protein chloro-tyrosine which correlates with myeloperoxidase activity in patients with ARDS 110
Present when ARDS patients are in multi-organ failure 63
Normal healthy BAL fluid contains RIS, as does BAL from ARDS survivors.Non-survivors, however, show no RIS in BAL, but high transferrin levelsdue to leak from the plasma 78
Increased TBA reactivity 111Increased 4-tiydroxynonenal 112Decreased linoleic and arachidonic acids 112
Maybe released from injured tissues after re-oxygenation injury to the lung 82
Indicative of hypoxia, and aberrant ATP catabolism during ischaemia-reperfusion 83
Possibly destroyed by oxidants 71
Appear to be low when not standardised to lipid content of plasma 73, 111, 113
Plasma Cp protein levels often elevated but ferroxidase activity per unit ofprotein is decreased 62
Iron-binding anti-oxidant activity of plasma is low due to loss ofiron-binding capacity 62
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically i
iron-overloaded patients is deleterious comes from the finding that levelsof 4-hydroxy-2-nonenal (a lipid peroxidation product of n-6 PUFAs)greatly increased when iron-overload occurred". Plasma total thiollevels are lower in CPB patients before surgery but rise significantly inthose receiving blood cardioplegia98. A likely source of these thiols is redblood cell lysis; a process which also produces RIS simultaneously.Additional oxidative stress is incurred when the aortic cross clamp isremoved and reoxygenation of tissue follows the ischaemic period.Aberrant ATP catabolism, characteristic of ischaemia/reperfusion injury,follows causing a rise in xanthine and hypoxanthine levels100.Hypoxanthine levels were found to be significantly higher in patientsreceiving warm blood cardioplegia100 and represents another potentialsource of ROS, since it is a substrate for the ROS-producing enzymexanthine oxidase (Table 1).
Therapeutic implications
Acute respiratory distress syndrome
There are two main aspects of ROS and RNS biology that haveimplications for the introduction of treatments for ARDS. Firstly,decreasing the damage incurred by ROS and secondly, introducing NOin inhaled form to redistribute pulmonary blood flow and improveoxygenation. Although, few clinical data exist in man, numerous reportshave shown that ROS scavengers such as N-acetyl-cysteine ordimethylthiourea can reduce cell damage in animal models of ARDS. Asecond strategy examined in animal models has been the administrationof various anti-oxidant enzymes, particularly SOD or catalase. A novelSOD-mimetic that also has catalase activity (EUK-8) has recently beenshown to attenuate LPS-induced ARDS in pigs101. Whether such anapproach would be beneficial in man remains to be determined, butthere is clearly potential for treatment with some form of anti-oxidanttherapy.
Recently, patients with ARDS complicated by pulmonary hypertensionhave been treated with inhaled NO, which improves oxygenation byselectively increasing blood flow to well ventilated areas of lung.Significant benefits in oxygenation index have been shown in patientswith ARDS treated with inhaled NO compared to placebo102. However,since NO can contribute to oxidant stress (i.e. via ONOO") there is thepossibility that when it is inhaled by patients already exposed to highlevels of oxidants, via endogenous pathways, the therapeutic benefits ofimproved blood flow are outweighed by increased cell damage. Indeed,evidence suggests that only around 50% of patients respond positively
British Medical Bulletin 1999;55 (No. 1) 69
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
to inhaled NO103. Whether non-responders represent a patient groupwhere NO contributes significantly to oxidant damage remains to beestablished.
Septic shock
Treatments for septic shock are mainly supportive, typically centringaround reversing the fall in systemic vascular resistance associated withthe condition. After the demonstration that iNOS is expressed in bloodvessels from experimental animal models of sepsis, attention wasfocused on NOS inhibitors which has been shown to lessen orcompletely reverse the associated fall in blood pressure104. However,some reports indicated that NOS inhibition increased mortality inanimal models of sepsis104, possibly due to removal of the NO formedby eNOS and nNOS, which is considered 'protective', along with thatproduced by iNOS. This potential problem would be obviated by the useof specific iNOS inhibitors, which are currently under development.Alternatively, NO formed by iNOS in sepsis may be protective inconstricted vascular beds where eNOS has been lost through endothelialinjury (i.e. the pulmonary circulation). In order to address thispossibility it would be necessary to provide a combined therapeuticapproach, providing a NOS inhibitor together with a carefully titrateddose of a vasodilator (e.g. nitrovasodilator or prostacyclin). Indeed,using animal models of sepsis, the combined administration of a NOSinhibitor together with inhaled NO improves mortality compared toeither treatment alone104.
Other potential therapeutic approaches, related to ROS/RNS imbalancehave concentrated on decreasing oxidative damage. There is nowconsiderable evidence implicating ROS/RNS induced damage in theprogression of organ dysfunction in sepsis. However, in similar fashion toARDS, few data exist to demonstrate the effects of anti-oxidants inhuman sepsis. Nevertheless, studies using rodent hepatic cells in vitro havedemonstrated the potential benefit of SOD-related drugs in sepsis105,although, these benefits are not necessary applicable to the in vivosituation10*.
It seems, therefore, that a considerable amount of basic scientificinvestigation is required before a full understanding of the intricateconsequences of ROS/RNS imbalance in the critically ill can beachieved. Specifically, three main advances are required: first, to be ableto fully characterise the ROS/RNS status of individual patients within adisease cohort; second, to develop new anti-oxidants; and finally, to beable to manipulate constitutive and inducible anti-oxidant productionbefore the onset of, or during the convolution disease states that afflictthe critically ill.
70 British Medical Bulletin 1999,55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically i
Acknowledgements
References
The authors thank the British Lung Foundation and the British OxygenGroup, the Dunhill Medical Trust, and Wellcome Trust for their financialsupport.
1 Gutteridge JMC, HalLwell B. Anti-oxidants in nutrition, health and disease. Oxford: OxfordUniversity Press, 1994
2 Halliwell B, Gutteridge JMC. Free radicals in biology and medicine, 3rd edn. Oxford: OxfordUniversity Press, 1999
3 Halliwell B, Gutteridge JMC. Oxygen free radicals and iron in relation to biology and medicine:some problems and concepts. Arch Biochem Biophys 1986; 246: 501-14
4 Saran M, Bors W. Oxygen radicals acting as chemical messengers: a hypothesis. Free Radic ResCommun 1989; 7: 213-20
5 Gutteridge JMC, Paterson SK, Segal AW, Halliwell B. Inhibition of lipid peroxidation by the iron-binding protein lactoferrin. Biochem] 1981; 199: 259-61
6 McCord JM, Fndovich I. Superoxide dismutase. An enzymatic function or erythrocuprein(hemocuprein). / Biol Chem 1969; 24: 6045-55
7 Marklund SL, Holme E, Hellner L. Superoxide dismutase in extracellular fluids. Clm Chim Ada1982; 126: 41-51
8 Chance B, Sies H, Boveris A. Hydroperoxide metabolism in mammalian organs. Phystol Rev 1979;59: 527-605
9 Gutteridge JMC. The membrane effects of vitamin E, cholesterol and their acetates on peroxidativesusceptibility. Res Commun Chem Path Pharmacol 1978; 22: 563-71
10 Gutteridge JMC, Stocks J. Peroxidation of cell lipids. / Med Lab Sci 1976; 53: 281-511 Esterbauer H, Schaur RJ, Zollner H. Chemistry and biochemistry of 4-hydroxynonenal,
malonaJdehyde and related aldehydes. Free Radic Biol Med 1991; 11: 81-12812 Burton GW, Joyce A, Ingold KU. First proof that vitamin E is major lipid soluble, chain-breaking
anti-oxidant in human blood plasma. Lancet 1982; ii: 32713 Stocks J, Gutteridge JMC, Sharp RJ, Dormandy TL. The inhibition of lipid antioxidarion by
human serum and its relation to serum proteins and a-tocopherol. Clin Sci Mol Med 1974; 47:223-33
14 Barber AA. Inhibition of lipid peroxide formation by vertebrate blood serum. Arch BiochemBiophys 1961; 92: 38-43
15 Gutteridge JMC, Quinlan GJ. Antioxidant protection against organic and inorganic oxygenradicals by normal human plasma: the important primary role for iron-binding and iron-oxidisingproteins. Biochim Biophys Ada 1992; 1159: 248-54
16 Gutteridge JMC, Stocks J. Caeruloplasmin: physiological and pathological perspectives. Crit RevClin Lab Sci 1981; 14: 257-329
17 Wills ED. Mechanisms of lipid peroxide formation in tissues. Role of metals and haematin proteinsin the catalysis of the oxidation of unsaturated fatty acids. Biochim Biophys Ada 1965; 98: 238—51
18 Gutteridge JMC. Iron promoters of the Fenton reaction and lipid peroxidation can be releasedfrom haemoglobin by peroxides. FEBS Lett 1986; 201: 291-5
19 Gutteridge JMC. The ano-oxidant activity of haptoglobins towards haemoglobin stimulated lipidperoxidation. Biochim Biophys Ada 1987; 219: 219-23
20 Smith A, Morgan Wl. Haem transport to the liver by haemopexin: receptor-mediated uptake withrecycling of the protein. Biochem J 1979; 182: 47-54
21 Gutteridge JMC, Smith A. Antioxidant protection by haemopexin of haem-stimulated lipidperoxidation. Biochem} 1988; 256: 261-5
22 Halliwell B. Albumin - an important extracellular anti-oxidant? Biochem Pharmacol 1988; 37:569-71
British Medical Bulletin 1999;55 (No. 1) 7 1
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
23 Krinsky NI. Mechanism of action of biological ann-oxidants. Proc Soc Exp Biol Med 1992;200: 248-54
24 Babior BM. Oxygen-dependent microbial killing by phagocytes. N EnglJ Med 1978; 298: 721-525 Candeias LP, Patel KB, Stratford MRL, Wardman P. Free hydroxyl radicals are formed on reaction
between the neutrophil-derived species superoxide anion and hypochlorous acid. FEBS Lett 1993;333: 151-3
26 Candeias LP, Stratford MRL, Wardman P. Formation of hydroxyl radicals on reaction ofhypochlorous acid with ferrocyanite. A model iron (II) complex. Free Radic Res 1994; 20: 241-9
27 Fenton HJH. Oxidation of tartaric acid in presence of iron. / Chem Soc 1894; 64: 899-90928 Symons MCR, Gutteridge JMC. Free radicals and iron: chemistry, biology and medicine. Oxford:
Oxford University Press, 199829 Thomas HV, Mueller PK, Lyman RL. lipoperoxidation of lung hpids in rats exposed to nitrogen
dioxide. Science 1968; 159: 5 3 2 ^30 Moncada S, Higgs EA. Endogenous nitric oxide: physiology, pathology and clinical relevance. Eur
J Clm Invest 1991; 21: 361-7431 Huie RE, Padmaja S. The reaction of NO" with superoxide. Free Radic Res Common 1993; 18:195-932 Pryor WA, Squadrito GL. The chemistry of peroxynitrite: a product from the reaction of nitric
oxide with superoxide. Am J Physiol 1995; 268: L699-72233 Kaur H, Whiteman M, Halliwell B. Peroxynitrite-dependent aromatic hydroxylation and nitration
of salicylate and phenlyalanine. Is hydroxyl radical involved? Free Radic Res 1997; 26: 71-8234 Schrenk R, Albermann K, Baeuerle PA. Nuclear factor kappa B: an oxidative stress-responsible
transcription factor of eukaryotic cells (review). Free Radic Res Comrnun 1992; 17: 221-3735 Peng HB, libby P. Iiao JK. Induction and stabilization of I kappa B alpha by NO mediates
inhibition of NF-kapa B. / Biol Chem 1995; 270: 14214-936 Laurindo FR, da Luz PL, Vint L, Rocha TF, Jaeger RG, Lopes EA. Evidence for superoxide radical-
dependent coronary vasospasm after angioplasty in intact dogs. Circulation 1991; 83: 1705—1537 Halliwell B. Superoxide, iron, vascular endothelium and reperfusion injury. Free Radic Res
Commun 1989; 5: 315-838 Castro L, Rodriguez M, Radi R. Aconitase is readily inactivated by peroxynitrite, but not by its
precursor nitric oxide. / Biol Chem 1994; 269: 29409-1539 Padmaja S, Huie RE. The reaction of nitric oxide with organic peroxyl radicals. Biochem Biophys
Res Commun 1993; 195: 539-4440 Beckman JS, Ye YZ, Anderson P et al. Extensive nitration of protein tyrosines in human
atherosclerosis detected by immunohistochemistry. Biol Chem Hoppe-Seyler 1994; 375: 81-841 Cabantchik ZI, Glickstein H, Milgram P, Breuer W. A fluorescence assay for assessing chelation
of intracellular iron in a membrane model system and in mammalian cells. Anal Biochem 1996;233:221-7
42 Grootveld M, Bell JD, Halliwell B, Aruoma OI, Bomford A, Sadler PJ. Non-transferrin-boundiron in plasma or serum from patients with idiopathic hemochromatosis. / Biol Cbem 1989;264: 4417-22
43 Gutteridge JMC, Rowley DA, Halliwell B. Superoxide-dependent formation of hydroxyl radicalsin the presence of iron salts. Detection of 'free' iron in biological systems by using bleomycin-dependent degradation of DNA. Biochem / 1981; 199: 263-5
44 Mumby S, Koizumi M, Taniguchi N, Gutteridge JMC. Reactive iron species in biological fluidsactivate the iron-sulphur duster of aconitase. Biochim Biophys Ada 1998; 1380: 102-8
45 De Silva DM, Askwith CC, Kaplan J. Molecular mechanisms of iron uptake in eukaryotes. PhysiolRev 1996; 76: 3 1 4 7
46 Klausner RD, Rouault A, Harford JB. Regulating the fate of mRNA: the control of cellular ironmetabolism. Cell 1993; 72: 19-28
47 Kennedy MN, Mende-Mueller L, Blondin GA, Beinert H. Purification and characterisation ofcytosolic aconitase from beef liver and its relationship to the iron-responsive element bindingprotein (IRE-BP). Proc Natl Acad Sd USA 1992; 89: 11730-4
48 Halliwell B, Gutteridge JMC. Lipid peroxidation, oxygen radicals, cell damage and anti-oxidanttherapy. Lancet 1984; i: 1396-7
49 Herald M, Spiteller G. Enzymic production of hydroperoxides of unsaturated fatty acids by injuryof mammalian cells. Chem Phys LJpids 1996; 79: 113-21
72 British Medical Bulletin 1999,55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
50 Esterbauer H, Schaur RJ, Zollner H. Chemistry and biochemistry of 4-hydroxynoncnal,malonaldehyde and related aldehydes. Free Radio Biol Med 1991; 11: 81-128
51 Burdon RH. Superoxide and H J O J in relation to mammalian cell proliferation. Free Radic BiolMed 1994; 18: 775-94
52 Gutteridge JMC. Signal, messenger and trigger molecules from free radical reactions and theircontrol by anti-oxidants. In: Packer L, Wirtz K (eds). Signalling mechanisms — from transcriptionfactors to oxidative stress. Berlin: Springer, 1995; 157-64
53 Gutteridge JMC, Richmond R, Halliwell B. Oxygen free radicals and lipid peroxidation: inhibitionby the protein caeruloplasmin. FEBS Lett 1980; 112: 269-72
54 Wolin MS. Reactive oxygen species and vascular signal transduction mechanisms. Microctrculation1996; 3: 1-17
55 Moncada S, Higgs EA. Molecular mechanisms and therapeutic strategies related to nitric oxide.FASEBJ 1995; 9: 1319-30
56 Stone JR, Marietta MA. Spectral and kinetic studies on the activation of soluble guanylate cydaseby nitric oxide synthase. Biochemistry 1996; 35: 1093-9
57 Pollock JS, Forsterman U, Mitchell JA et al. Purification and characterisation of EDRF synthase.Froc Natl Acad Sci USA 1991; 89: 10480-5
58 Garthwaite J, Charles SL, Chess-Williams R. Endothelium-derived relaxing factor release onactivation of NMDA receptors suggests role as intercellular messenger in the brain. Nature1988; 336: 385-8.
59 MacMicking M, Xie J, Nathan C. Nitric oxide and macrophage function. Annu Rev Immunol1997; 15: 323-50
60 Macnaughton PD, Evans 1W. Adult respiratory distress syndrome. Lancet 1992; 339: 469-7261 Ashbaugh DG, Biglow DB, Petty TL, Levine B. Active respiratory distress in adults. Lancet 1967;
ii: 319-2362 Gutteridge JMC, Quinlan GJ, Mumby S, Heath A, Evans TW. Primary plasma anti-oxidants in
adult respiratory distress syndrome patients: changes in iron-oxidizing, iron-binding and freeradical-scavenging proteins. / Lab Clm Med 1994; 124: 263-73
63 Gutteridge JMC, Quinlan GJ, Evans TW. Transient iron overload with bleomycin detectable ironin the plasma of patients with adult respiratory distress syndrome. Thorax 1994; 49: 707-10
64 Moak SA, Greenwald RA. Enhancement of rat serum ceruloplasmin levels by exposure tohyperoxia. Froc Soc Exp Biol Med 1984; 177: 97-103
65 Kresek-Staples JA, Kew RR, Webster RO. Ceruloplasmin and transferrin levels are altered in serumand bronchoalveolar lavage fluid of patients wim the adult respiratory distress syndrome. Am RevResptr Dis 1992; 145: 1009-15.
66 Fleming RE, Whitman IP, Gidin JD. Induction of ceruloplasmin gene expression in rat lung duringinflammation and hyperoxia. Am J Pbysiol 1991; 260: L68-74
67 Quinlan GJ, Evans TW, Gutteridge JMC. Oxidative damage to plasma proteins in adult respiratorydistress syndrome. Free Radic Res 1994; 20: 289-98
68 Paterson CE, Rhoades RA. Protective role of sulphydryl reagents in oxidant lung injury. Exp LungRes 1988; 14: 1005-19
69 Bernard GR, Swindell BB, Meredith MJ, Carroll FE, Higgins SB. Glutathione (GSH) repletion byN-acetyl cysteine (NAC) in patients with the adult respiratory distress syndrome (ARDS). Am RevResptr Dis 1989; 139: A221
70 Jepson S, Herlevsen P, Knudesen P, Bud MI, Klausen N-O. Antioxidant treatment with N-acetylcysteine during adult respiratory distress syndrome: a prospective randomized placebo-controlled study. Crit Care Med 1992; 20: 918-23
71 Cross CE, Forte T, Stocker R et al. Oxidative stress and abnormal cholesterol metabolism inpatients with adult respiratory distress syndrome. / Lab Clin Med 1990; 115: 391-404
72 Frei B, Yamamoto Y, Niclas D, Stocker R, Cross CE, Ames B. Analysis of oxidants and anti-oxidants in human plasma of healthy subjects and of patients with adult respiratory distresssyndrome. In: Rice-Evans C, Halliwell B (eds) Free radicals, methodology and concepts. London:Richelieu, 1988; 349-68
73 Bertrand Y, Pincemail J, Hanique G et al. Differences in tocopherol-lipid ratios in ARDS and non-ARDS patients. Intensive One Med 1989; 15: 87-93
British Medical Bulletin 1999;55 (No. 1) 73
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Intensive care medicine
74 Baldwin SR, Grum CM, Boxer LA, Simon RH, Ketai LH, Devall LJ. Oxidant activity in expiredbreath of patients with adult respiratory distress syndrome. Lancet 1986; i: 11-4
75 Sznajder JL Fraiman A, Hall JB et al. Increased hydrogen peroxide in the expired breath of patientswith acute hypoxemic respiratory falure. Chest 1989; 96: 602-12
76 Leff JA, Parson PE, Day CE et al. Increased serum catalase activity in septic patients with the adultrespiratory distress syndrome. Am Rev Resptr Dis 1992; 146: 985-9
77 Leff JA, Parson PE, Day CE et al. Serum anti-oxidants as predictors of adult respiratory distresssyndrome m patients with sepsis. Lancet 1993; 341: 777-80
78 Gutteridge JMC, Mumby S, Quinlan GJ, Chung KF, Evans 1W. Pro-oxidant iron is present inhuman pulmonary epithelial lining fluid: implications for oxidative stress in the lung. BiocbemBiophys Res Commun 1996; 220: 1024-7
79 Pacht ER, Davis B. Role of transferrin and ceruloplasmin in ann-oxidant activity of lung epitheliallining fluid. J Appl Physiol 1988; 64: 2092-9
80 Quinlan GJ, Lamb NJ, Evans TW, Guttendge JMC. Plasma fatty acid changes and increased lipidperoxidation in patients with adult respiratory distress syndrome. Crit Care Med 1996; 24: 241-6
81 Gutteridge JMC, Quinlan GJ, Yamamoto Y. Are fatty acid patterns characteristic of essential fattyacid deficiency indicative of oxidative stress? Free Radic Res 1998; 28: 109-14
82 Grum CM, Ragsdale RA, Ketai LH, Simon RH. Plasma xanthine oxidase activity in patients withadult respiratory distress syndrome. / Crit Care 1987; 2: 22-6
83 Quinlan GJ, Lamb NJ, Tilley R, Evans TW, Gutteridge JMC. Plasma hypoxanthine levels inARDS: Implications for oxidative stress, morbidity and mortality. Am J Res Crit Care Med 1997;155: 479-84
84 Ogilvie AC, Groeneveld AB, Straub JP, Thijs LG. Plasma lipid peroxides and anti-oxidants inhuman septic shock. Intensive Care Med 1991; 17: 40-4
85 Cowley HC, Bacon PJ, Goode HF, Webster NR, Jones JG, Menon DK. Plasma anti-oxidantpotential in severe sepsis: a comparison of survivors and nonsurvivors. Crit Care Med 1996; 24:1179-83
86 Galley HF, Howdle PD, Walker BE, Webster NR. The effects of intravenous anti-oxidants inpatients with septic shock. Free Radic Biol Med 1997; 23: 768-74
87 Galley HF, Webster NR. Elevated serum bleomycin-detectable iron concentrations in patients withsepsis syndrome. Intensive Care Med 1996; 22: 226-9
88 Galley HF, Davies MJ, Webster NR, Ascorbyl radical formation in patients with sepsis: effect ofascorbate loading. Free Radic Biol Med 1996; 20: 139-43
89 Mumby S, Margarson M, Quinlan GJ, Evans TW, Gutteridge JMC. Is bleomycin-detectable ironpresent in the pksma of patients with septic shock? Intensive Care Med 1997; 23: 635-9
90 Weinberg ED. The iron-with-holding defence system. Am Soc Microbiol News 1993; 59: 559-6291 Lands WEM, Pendleton RB. Amplification of tissue peroxides in disease. In: Cerutti PA, Nygaard
OF (eds) Anticarcinogenesis and radiation protection. New York: Plenum, 1987; 81-492 Quinlan GJ, Margarson M, Mumby S, Evans TW, Gutteridge JMC. Administration of albumin to
patients with sepsis syndrome: a possible beneficial role in plasma thiol repletion. Clin Set 1998;95: 459-65
93 Gutteridge JMC. Anti-oxidants, nutritional supplements and life-threatening diseases. BrJ BiomedSet 1994; 51: 288-95
94 Pepper JR, Mumby S, Gutteridge JMC. Sequential oxidative damage, and changes in iron-bindingand iron-oxidising plasma ann-oxidants during cardiopulmonary bypass surgery. Free Radic Res1994; 21: 377-85
95 Pepper JR, Mumby S, Gutteridge JMC. Transient iron-overload with bleomycin-detectable ironpresent during cardiopulmonary bypass surgery. Free Radic Res 1994; 21: 53-8
96 Messent M, Sinclair DG, Quinlan GJ, Mumby S, Gutteridge, Evans TW. Pulmonary vascularpermeability after cardiopulmonary bypass and its relationship to oxidative stress. Crit Care Med1997; 25: 425-9
97 Moat NE, Evans TW, Quinlan GJ, Gutteridge JMC. Chelatable iron and copper can be releasedfrom extracorporeally circulated blood during cardiopulmonary bypass. FEBS Lett 1993; 328:103-6
98 Pepper JR, Mumby S, Gutteridge JMC. Blood cardioplegia increases plasma iron overload andthiol levels during cardiopulmonary bypass. Ann Thorac Surg 1995; 60: 1735-40
74 British Medial Bulletin 1999;55 (No. 1)
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018

Redox imbalance in the critically ill
99 Quinlan GJ, Mumby S, Pepper JR, Gutteridge JMC. Plasma 4-hydroxyl-2-nonenal levels duringcardiopulmonary bypass and their relationship to the iron-loading of transferrin. Biochem MolBiol Int 1994; 34: 1277-82
100 Quinlan GJ, Westerman ST. Mumby S, Pepper JR, Gutteridge JMC. Plasma hypoxanthine levelsduring crystalloid and blood cardioplegias: Warm blood cardioplegia increases hypoxanthine levelswith a greater risk of oxidative stress. / Cardiovasc Surg 1999; 39: In press.
101 Gonzalez PK, Zhuang J, Doctrow SR et al. EUK-8, a synthetic superoxide dismutase and catalasemimetic, ameliorates acute lung injury in endotoxemic swine. / Pharmacol Exp Ther 1995; 275:798-806
102 Dellinger RP, Zimmerman JL, Taylor RW, Straube RC. Placebo and inhaled nitric oxide mortalitythe same in ARDS clinical trial. Crit Care Med 198; 26: 619.
103 Treggiari-Venzi M, Ricou B, Romand JA, Suter PM. The response to repeated nitric oxideinhalation is consistent in patients with acute respiratory distress syndrome. Artestbesiology 1998;88: 634-41
104 Thiemermann C. Nitnc oxide and septic shock. Gen Pharmacol 1997; 29: 159-66105 Rose S, Sayeed MM. Superoxide radical scavenging prevents cellular calcium dysregulation during
intraabdominal sepsis. Shock 1997; 7: 263—8106 de Vos S, Epstein CJ, Carlson E, Cho SK, Koeffler HP. Transgenic mice overexpressing human
copper/zinc-superoxide dismutase (Cu/Zn SOD) are not resistant to endotoxic shock. BiochemBiopbys Res Comrnun 1995; 208: 523-31
107 Cochrane CG, Spragg RG, Revak SD, Cohen AB, McGuiree WW. The presence of neutrophilelastase and evidence of oxidation activity in bronchoalveolar lavage fluid of patients with adultrespiratory syndrome. Am Rev Respir Dis 1983; 127: 25-7
108 Pacht ER, Timerman AP, Lykens MG et al. Deficiency of alveolar fluid glutathione in patients withsepsis and the adult respiratory distress syndrome. Chest 1991; 100: 1397-403
109 Beckman JS, Beckman 1 W, Chen J, Marshall PA, Freeman BA. Apparent hydroxyl radicalproduction by peroxynitrite: implications for endothelial injury from nitric oxide and superoxide.Proc Natl Acad Sa VSA 1990; 87: 1620-4
110 Lamb NJ, Gutteridge JMC, Evans TW, Baker CS, Quinlan GJ. Increased levels of markers ofoxidative damage are present in BAL fluid from patients with ARDS. Am } Respir Crit Care Med1999; In press
111 Richard C, Lemonnier F, Thibault M, Auzepy P. Vitamin E deficiency and lipoperoxidation duringadult respiratory distress syndrome. Crit Care Med 1990; 18: 4—9
112 Quinlan GJ, Evans TW, Gutteridge JMC. 4-hydroxy-2-nonenal levels increase in die plasma ofpatients with adult respiratory distress syndrome as linoleic acid appears to fall. Free Radic Res1994; 21: 95-106
113 Deby C. Difference in tocopherol-lipid ratios in ARDS and non-ARDS patients. Intensive CareMed 1989; 15: 877-93
114 Cochrane Injuries Group Albumin Reviewers. Human albumin administration in critically illpatients: systematic review of randomised controlled trials. BMJ 1998; 317: 235-40
115 Offringa M. Excess mortality after human albumin administration in critically ill patients. BMJ1998; 317: 223-4
British Medial Bulletin 1999;55 (No. 1) 75
Downloaded from https://academic.oup.com/bmb/article-abstract/55/1/49/475396by gueston 22 March 2018