Redox Homeostasis and Epigenetics in Non-Alcoholic Fatty Liver Disease (NALFD)
10
Send Orders of Reprints at [email protected] Current Pharmaceutical Design, 2013 , 19, 000-000 1 1381-6128/1 3 $58.00+.00 © 2013 Bentham Science Publishers Redox Homeostasis and Epigenetics in N on-alcoho lic Fatty Liver Disease (NAFLD) Christine Podrini 1 , Michela Borghesan 1 , Azzura Greco 1 , Valerio Pazienza 2 , Gianluigi Mazzoccoli 3 and Manlio Vinciguerra 1,4, * 1 The Institute of Hepatology, The Foundation for Liver Research, London, United Kingdom; 2 Division and Laboratory of Gastroen- terology, IRCCS “Casa Sollievo della Sofferenza” Hospital, San Giovanni Rotondo, Italy; 3 Department of Internal Medicine Unit IRCCS “Casa So llievo della Sofferenza” Hospita l, San Giovanni Rotondo, Italy 4 EuroMediterranean Institute o f Scienc e and Tech- nology (IEMEST), Palermo, Italy Abstract: Non-alcoholic fatty live r disease (NAFLD), an accumulation of intra-hepatic triglycerides that is often c onsidered the hepatic manifestation of insulin resistance, is the most common cause of chronic liver disease in the Western countries with up to one third of the population affected. NAFLD is a spectrum of disturbances that encompasses various degrees of liver damage ranging from simple steato- sis to non-alcoholic steatohepatitis (NASH). NASH is characterized by hepatocellular injury/inflammation with or without fibrosis. The individuals with NAFLD develop NASH in 10% of the cases, and are also at risk of developing hepatocellular carcinoma (HCC). Epige- netic mechanisms of nuclear chromatin remodeling, such as DNA methylation, post-translational modifications of histones, and incorpo- ration of histone variants into the chromatin are increasingly recognized as crucial factors in the pathophysiology of NAFLD. NAFLD is often accompanied by oxidative stress: reactive oxygen species (ROS) are implicated in altered reduction/oxidation (redox) reactions that attack cellular macromolecules and are detected in the liver of patients and animal models of NAFLD. In this review, we summarize re- cent knowledge advancements in the hepatic epigenetic and redox mechanisms, and their possible links, involved in the pathogenesis and treatment of NAFLD. Keywords: Non-alcoholic fatty liver disea se (NAFLD), epigenetics, ox idative stress. 1.1. INTRODUCTION The liver is a central organ for regulation of biochemical func- tions necessary for whole-body metabolic homeostasis. The main function of the liver is to regulate blood glucose, lipids levels and synthesis of the majority of plasma proteins [1]. In addition, the liver is also responsible for the removal of toxins and waste prod- ucts from the blood. The predominant liver cell type is the hepato- cyte, a large polyhedral epithelial cell responsible for numerous metabolic functions [2]. Hepatocytes accumulate lipids, (mainly triglycerides (TGs) and cholesterol); an increased accumulation of TGs in the hepatocytes give the liver its ‘fatty’ yellowish appear- ance, typical of non-alcoholic fatty liver disease (NAFLD). TGs accumulation can also be due to other causes such as alcohol intake and hepatitis infections, which will not be discussed here. NAFLD is a pathological condition and generally begins as simple hepatic accumulation of lipids (steatosis). The term NAFLD is used to describe fat accumulation in the liver exceeding 5% - 10% of the liver weight, as determined from the percentage of fat- laden hepatocytes by light microscopy [3]. NAFLD is considered by many as the hepatic m anifestation of in sulin resistanc e (IR) and is strongly associated with features of the metabolic syndrome [4]. Associated with the rapid increase in obesity during the last decade, is an increased prevalence of NAFLD. With 30% of the population affected, NAFLD is the most common cause of chronic liver dis- ease in the Western countries [5]. Liver injury caused by NAFLD can go undiagnosed until non-invasive surrogate markers, such as liver transaminases (alanine transaminase (ALT)), are measured incidentally. Elevated transaminase levels indicate a high hepato- cyte cell death and an increased membrane permeability, allowing these enzymes to leak out into the blood stream. However, the accu- racy and the diagnostic value of transaminases levels is controver- stial for NAFLD with histological evaluation the gold standard for *Address correspondence to this author at the The Institute of Hepatology, The Foundation for Liver Research, 69-75 Chenies Mews, London, WC1E 6HX, United Kingdom; Tel: +44 (0) 20 7255 9848; Fax: +44 (0) 20 7380 0405; E-mail: [email protected] precisely estimating the degree of liver damage in simple steatosis and non-alcoholic steatohepatitis (NASH) [6]. Nowadays, non- invasive techniques, such as ultrasounds for steatosis or transient elastography (FibroScan), are widely used for the clinical diagnosis of NAFDL/NASH. Individuals with NAFDL develop NASH in 10% of the cases, with 8-26% progressing to cirrhosis putting these patients at risk of developing hepatocellular carcinoma (HCC) [7]. The mechanisms behind steatosis and its progression to NASH are not completely understood; particularly the factors that lead to increasing hepato- cellular damage after triglycerides accumulation. The classical “two-hit” hypothesis for the pathogenesis of NAFLD has been sug- gested for the progression to NASH - described as the consequence of hepatic fat accumulation followed by an increase in sensitivity to oxidative stress and inflammation [8] (discussed in more detail in “Molecular pathogenesis of NAFLD” section). Several genetic and dietary models have been used to study the progression from steato- sis to NASH. Animal models may be divided into two large catego- ries: either induced by genetic mutations or produced by dietary or pharmacological maneuvers. Several distinct mouse models exhibit histological evidence of hepatic steatosis or steatohepatitis, al- though few replicate the full spectrum of the human diseases. The most widely reported models in the literature are the leptin-deficient (ob/ob) or leptin-resistant (db/db) mouse, and the methionine/ cho- line dietary deficient model [9]. A recent study by Bieghs et al. reported that the low-density-lipoprotein (LDL) receptor knock-out mice developed hepatic inflammation and liver damage upon high- fat feeding due to an increased uptake of oxidized LDL [10]. This reported model is a very promising new tool to study the onset of NASH in the context of steatosis, with specific immunizatio n strategies against oxidized LDL aiding the reduction in steatohepa- titis [11]. Epigenetic level of transcriptional control, such as DNA methy- lation and modification of the histones amino-terminal tails, is gain- ing acceptance in the pathophysiology of NAFLD. Indeed, mount- ing evidence suggests that cellular epigenetic modifications may be a predetermining factor to individual susceptibilities to the condi-
-
Upload
sanjeev-saxena -
Category
Documents
-
view
4 -
download
0
description
8
Transcript of Redox Homeostasis and Epigenetics in Non-Alcoholic Fatty Liver Disease (NALFD)
-
Send Orders of Reprints at [email protected]
Current Pharmaceutical Design, 2013, 19, 000-000 1
1381-6128/13 $58.00+.00 2013 Bentham Science Publishers
Redox Homeostasis and Epigenetics in Non-alcoholic Fatty Liver Disease (NAFLD)
Christine Podrini1, Michela Borghesan
1, Azzura Greco
1, Valerio Pazienza
2, Gianluigi Mazzoccoli
3 and
Manlio Vinciguerra1,4,
*
1The Institute of Hepatology, The Foundation for Liver Research, London, United Kingdom;
2 Division and Laboratory of Gastroen-
terology, IRCCS Casa Sollievo della Sofferenza Hospital, San Giovanni Rotondo, Italy; 3 Department of Internal Medicine Unit
IRCCS Casa Sollievo della Sofferenza Hospital, San Giovanni Rotondo, Italy 4
EuroMediterranean Institute of Science and Tech-
nology (IEMEST), Palermo, Italy
Abstract: Non-alcoholic fatty liver disease (NAFLD), an accumulation of intra-hepatic triglycerides that is often considered the hepatic
manifestation of insulin resistance, is the most common cause of chronic liver disease in the Western countries with up to one third of the population affected. NAFLD is a spectrum of disturbances that encompasses various degrees of liver damage ranging from simple steato-
sis to non-alcoholic steatohepatitis (NASH). NASH is characterized by hepatocellular injury/inflammation with or without fibrosis. The individuals with NAFLD develop NASH in 10% of the cases, and are also at risk of developing hepatocellular carcinoma (HCC). Epige-
netic mechanisms of nuclear chromatin remodeling, such as DNA methylation, post-translational modifications of histones, and incorpo-ration of histone variants into the chromatin are increasingly recognized as crucial factors in the pathophysiology of NAFLD. NAFLD is
often accompanied by oxidative stress: reactive oxygen species (ROS) are implicated in altered reduction/oxidation (redox) reactions that attack cellular macromolecules and are detected in the liver of patients and animal models of NAFLD. In this review, we summarize re-
cent knowledge advancements in the hepatic epigenetic and redox mechanisms, and their possible links, involved in the pathogenesis and treatment of NAFLD.
Keywords: Non-alcoholic fatty liver disease (NAFLD), epigenetics, oxidative stress.
1.1. INTRODUCTION
The liver is a central organ for regulation of biochemical func-tions necessary for whole-body metabolic homeostasis. The main function of the liver is to regulate blood glucose, lipids levels and synthesis of the majority of plasma proteins [1]. In addition, the liver is also responsible for the removal of toxins and waste prod-ucts from the blood. The predominant liver cell type is the hepato-cyte, a large polyhedral epithelial cell responsible for numerous metabolic functions [2]. Hepatocytes accumulate lipids, (mainly triglycerides (TGs) and cholesterol); an increased accumulation of TGs in the hepatocytes give the liver its fatty yellowish appear-ance, typical of non-alcoholic fatty liver disease (NAFLD). TGs accumulation can also be due to other causes such as alcohol intake and hepatitis infections, which will not be discussed here.
NAFLD is a pathological condition and generally begins as simple hepatic accumulation of lipids (steatosis). The term NAFLD is used to describe fat accumulation in the liver exceeding 5% - 10% of the liver weight, as determined from the percentage of fat-laden hepatocytes by light microscopy [3]. NAFLD is considered by many as the hepatic manifestation of insulin resistance (IR) and is strongly associated with features of the metabolic syndrome [4]. Associated with the rapid increase in obesity during the last decade, is an increased prevalence of NAFLD. With 30% of the population affected, NAFLD is the most common cause of chronic liver dis-ease in the Western countries [5]. Liver injury caused by NAFLD can go undiagnosed until non-invasive surrogate markers, such as liver transaminases (alanine transaminase (ALT)), are measured incidentally. Elevated transaminase levels indicate a high hepato-cyte cell death and an increased membrane permeability, allowing these enzymes to leak out into the blood stream. However, the accu-racy and the diagnostic value of transaminases levels is controver-stial for NAFLD with histological evaluation the gold standard for
*Address correspondence to this author at the The Institute of Hepatology,
The Foundation for Liver Research, 69-75 Chenies Mews, London, WC1E
6HX, United Kingdom; Tel: +44 (0) 20 7255 9848; Fax: +44 (0) 20 7380 0405; E-mail: [email protected]
precisely estimating the degree of liver damage in simple steatosis and non-alcoholic steatohepatitis (NASH) [6]. Nowadays, non-invasive techniques, such as ultrasounds for steatosis or transient elastography (FibroScan), are widely used for the clinical diagnosis of NAFDL/NASH.
Individuals with NAFDL develop NASH in 10% of the cases, with 8-26% progressing to cirrhosis putting these patients at risk of developing hepatocellular carcinoma (HCC) [7]. The mechanisms behind steatosis and its progression to NASH are not completely understood; particularly the factors that lead to increasing hepato-cellular damage after triglycerides accumulation. The classical two-hit hypothesis for the pathogenesis of NAFLD has been sug-gested for the progression to NASH - described as the consequence of hepatic fat accumulation followed by an increase in sensitivity to oxidative stress and inflammation [8] (discussed in more detail in Molecular pathogenesis of NAFLD section). Several genetic and dietary models have been used to study the progression from steato-sis to NASH. Animal models may be divided into two large catego-ries: either induced by genetic mutations or produced by dietary or pharmacological maneuvers. Several distinct mouse models exhibit histological evidence of hepatic steatosis or steatohepatitis, al-though few replicate the full spectrum of the human diseases. The most widely reported models in the literature are the leptin-deficient (ob/ob) or leptin-resistant (db/db) mouse, and the methionine/ cho-line dietary deficient model [9]. A recent study by Bieghs et al. reported that the low-density-lipoprotein (LDL) receptor knock-out mice developed hepatic inflammation and liver damage upon high-fat feeding due to an increased uptake of oxidized LDL [10]. This reported model is a very promising new tool to study the onset of NASH in the context of steatosis, with specific immunization strategies against oxidized LDL aiding the reduction in steatohepa-titis [11].
Epigenetic level of transcriptional control, such as DNA methy-lation and modification of the histones amino-terminal tails, is gain-ing acceptance in the pathophysiology of NAFLD. Indeed, mount-ing evidence suggests that cellular epigenetic modifications may be a predetermining factor to individual susceptibilities to the condi-
-
2 Current Pharmaceutical Design, 2013, Vol. 19, No. 00 Podrini et al.
tion [12]. Epigenetic modifications are herited and provide a flexi-ble interface between the organism and its environment [13]. Al-though most common metabolic, degenerative diseases and multi-ple cancers present with heritable traits, they do not follow classical Mendelian inherited. The complex outcome of these diseases has been attributed to epigenetic changes in response to the environ-ment [13, 14]. Moreover, there is evidence for trans-generational epigenetic effects including metabolic and liver disturbances [15]. Although in most cases the molecular mechanism of inheritance is not understood, recent evidence suggest that diffusible factors, in particular RNA molecules, seem to be an attractive candidate that promotes epigenetic changes [16]. The potential role of epigenetics beyond gene regulation in the inter-generational heritability is only recently beginning to emerge.
Another key factor accompanying NAFLD is oxidative stress. Oxidative stress results from an imbalance between pro-oxidant and antioxidant chemical species that leads to oxidative damage of cel-lular macromolecules [17]. Pro-oxidant chemicals in fatty livers include singlet oxygen molecules, superoxide anions, hydrogen peroxide, and hydroxyl radicals; molecules collectively referred to as reactive oxygen species (ROS) and are implicated in reduc-tion/oxidation (redox) reactions. Consequences of an increased ROS imbalance include the depletion of ATP and nicotinamide adenine dinucleotide (NAD
+), DNA damage, protein degradation,
damage of membranes via peroxidation of constituent lipids, and the release of inflammatory cytokines [17, 18]. An increased pro-duction of ROS/lipid peroxidation induce by an accrued intake of dietary fatty acids has been confirmed in animal models of NAFLD [19]. Human livers with NASH have increased by-product levels of lipid peroxidation, providing further evidence of an increased oxi-dative stress [20].
In this review, we will focus our discussion on selected litera-ture on the hepatic epigenetic and redox mechanisms involved in the pathogenesis of NAFLD, touching also on the crosstalk between liver and other systems (i.e. gut, cardiovascular) during the occur-rence of this disease. We will also describe the current drug treat-ments for NAFLD.
1.2. MOLECULAR PATHOGENESIS OF NAFLD
The liver plays a major role in lipid metabolism, importing free fatty acids (FFAs) and manufacturing, storing, and exporting lipids; derangements in any of these processes can lead to NAFLD [21]. The ectopic accumulation of fat in the liver has been strongly asso-ciated with insulin resistance (IR) [4, 22]. IR in peripheral adipose tissue enhances lipolysis (lipid synthesis) and increases delivery of adipose-derived FFAs to the liver. Under physiological conditions, TGs synthesis is stimulated to dispose the excess FFAs. TGs can then be stored as lipid droplets within hepatocytes or secreted into the blood as very-low-density lipoprotein (VLDL) [23]. Rodent studies have shown that the mechanisms leading to the excessive accumulation of hepatic TGs are associated with an increased sup-ply of FFA from peripheral adipose tissue to the liver and an en-hanced de novo lipid synthesis via the lipogenic pathway. Con-versely, liver disposal via the -oxidation and VLDL export are moderately affected [24]. In a simplified model, NAFLD is the result of an imbalance between lipid availability (in which fatty acid uptake and de novo lipogenesis exceeds secretion) and lipid disposal via free fatty acid oxidation resulting in hepatic steatosis [25, 26]. At the cellular level, defects in the insulin signaling path-ways contribute to the increase of FFAs flux in the liver which, in turn activate a series of signaling cascades and leads to the phos-phorylation of several substrates. In the case of IR, there is a de-creased insulin receptor kinase activity resulting in lower AKT activity [23]. Insulin is the main driver of the global response to nutrient ingestion, and acts in hepatic fat metabolism through the phosphatidylinositol kinase signalling pathway through the accu-mulation of the intracellular lipid small messenger phosphatidyli-
nositol [3,4,5]-trisphosphate. This situation is reproduced by phos-phatase and tensin homologue (PTEN) loss, which similarly ac-companies fatty liver development [27-33]. When PTEN knock out mice were crossed with AKT knock out mice, hepatic steatosis was significantly ameliorated, due to AKT-dependent lipogenic gene expression [34]. In addition, this effect was partially restored by expression of transcription regulatory factor forkhead box protein O (FOXO1), downstream of AKT [35]. FOXO1 is involved in con-trolling the activity of the rate-controlling enzymes both of glu-coneogenesis and lipogenesis. Reduced AKT activity results in decreased phosphorylation, ubiquination and proteasomal degrada-tion of FOXO1, and thereby increases the production of phosphoe-nolpyruvate carboxykinase (PEPCK). PEPCK in turn catalyzes the rate-limiting steps of gluconeogenesis - the reaction of oxaloacetic acid to phosphenol pyruvate. Hepatic loss of FOXO1 results in increased VLDL secretion, increased levels of sterol regulatory element-binding proteins (SREBPs) and increased lipogenesis [36, 37]. In mice overexpressing SREBP-1c in liver, there was a dra-matic build-up of hepatic TGs and elevated expression of lipogenic genes [38]. Hence, under a high fat diet, IR inhibits AKT/FOX01 pathway, promoting de novo fatty acid and glucose synthesis, with a parallel increased fatty acid oxidation [39]. De novo fatty acid synthesis is chiefly regulated by other transcription factors includ-ing - the carbohydrate response element-binding protein (ChREBP), peroxisome proliferator-activated receptor- (PPAR-), liver X receptors (LXRs), the aryl hydrocarbon receptor (AHR), the nuclear receptor TAK1/TR4/NR2C2 and asparaginyl hydroxylase (factor inhibiting HIF-1alpha, FIH). ChREBP co-ordinately regulates the genes required for the conversion of glucose to fatty acids in the liver and causes a reduced mRNA level of all lipogenic genes in the liver [40]. Down regulation of PPAR- favors lipogenesis over fatty acid (FA) oxidation, leading to the development of steatosis c [41]. Liver X receptors (LXRs) are the master regulators of hepatic lipid metabolism and directly target key genes involved in lipogenic pathways [42]. Transgenic mice lacking LXRs show a decreased expression of genes involved in lipogenesis (Fasn, Scd1) [43]. Im-portantly, synthetic LXRs agonists also induce lipogenesis, leading to hepatic steatosis. However, the treatment with LXR agonist may attenuate the development of atherosclerosis in the mouse model, suggesting that they may be promising anti-atherosclerotic agents despite causing hepatic steatosis [44]. A current challenge relies in the identification of novel therapeutic molecules that would act as selective LXRs modulators in order to obtain the desired cardio-protection and other benefits, without causing liver damage [45].
AHR has been reported to increase steatosis through a combina-tion of processes including upregulation of FA uptake and trans-port, suppression of fatty acid oxidation and the inhibition of he-patic triglyceride export [46]. As for the nuclear receptor TAK1/ TR4/NR2C2, its genetic ablation in mice induced lower hepatic triglyceride levels and increased energy expenditure. The livers of these mice also displayed a decreased expression of genes involved in lipid uptake and triglyceride synthesis and storage [47]. Finally, mice lacking FIH are resistant to high-fat-diet-induced hepatic stea-tosis [48]. Thus, ChREBP, PPAR-, LXRs, AHR, TAK1/TR4/ NR2C2 and FIH may promote steatosis and NAFLD. Recently, the understanding of the effects of microRNAs (miR) on the expression of hepatic lipid metabolism genes is representing a new research and therapeutic frontier (see for review [26, 49]). In this respect, we have recently shown that up regulation of miR-21 in the liver de-creases the expression of its target PTEN, thereby increasing triglyceride accumulation in the liver [31].
As already mentioned, the two-hit theory proposed is one of the leading models to explain the pathogenesis of the NAFLD spec-trum [8]. According to this conceptual framework, the first hit is an imbalance in hepatic lipid accumulation, the likely cause being IR which leads to an increased traffic of FFAs in the hepatocytes. The second hit is represented by inflammatory cytokines/adi-
-
Redox Homeostasis and Epigenetics Current Pharmaceutical Design, 2013, Vol. 19, No. 00 3
pokines, mitochondrial dysfunction and oxidative stress, promoting apoptosis through several pathways leading to inflammatory infil-trates in the liver that may progress to fibrosis [50]. This old model is now revitalized and implemented by recent studies analyz-ing the role of liver cell types other than hepatocytes and the gut microbiota. Hepatic stellate cells are devoted to producing extracel-lular matrix and are believed to mediate the fibrotic mechanisms driving the transition from steatosis to NASH in presence of in-flammation [51]. Hepatic Kupffer cells, specialized macrophages lining the walls of the liver sinusoids, also critically contribute to NAFLD progression by augmenting inflammation. Toll-like recep-tors (such as TLR4) are major transducers of inflammatory stimuli linked to Kupffer cell activation, a process which may be perturbed at multiple steps in NAFLD. Steatosis may interfere with hepatic clearance of microbial and host-derived inflammatory cues, along with TLR4 receptor complex assembly triggering the activation of Kupffer cells in a positive feedback loop [52]. The nucleotide-binding domain and leucine-rich-repeat-containing (NLR) family of pattern-recognition molecules (NLRP6 and NLRP3) form cytosolic protein complexes termed inflammasomes, which in turn have vari-ous roles in immune defenses [53]. Henao-Mejia et al. showed that the NLRP6 and NLRP3 inflammasomes and the downstream cyto-kine IL-18 negatively regulate NAFLD/NASH progression by tun-ing the gut microbiota. Altered interactions between the gut micro-biota and the host produced by defective NLRP3 and NLRP6 in-flammasome sensing, may govern the progression of NAFLD spec-trum [54]. Further evidence that fatty liver disease may result from the disruption of the gut-liver axis, comes from the study of an acti-vated mutant of morphogenic signal Notch [intracellular domain E, (ICD-E)] in a knock-in inducible mouse model [55]. Liver overex-pression of ICD-E has no phenotype, but simultaneous induction of ICD-E in both the liver and small intestine results in NAFLD and IR within four days [55]. Finally, the impact of simple dietary ele-ments such as choline in the development and progression of NAFLD is also important and now analyzed closely, as low levels of choline in humans may be sufficient to trigger NAFLD devel-opment. However, this may vary depending on an individual's genotype and hormonal status [56].
1.3. EPIGENETICS CAUSES OF NAFLD
The understanding that epigenetic mechanisms contribute to the development of human diseases has been a major breakthrough in the last decades [57]. Most of the heritable changes are established during differentiation and are maintained through multiple cycles of cells division, enabling cells to have different entities while con-taining the same genetic information [58]. The heritability of the gene expression pattern is mediated by epigenetic modifications that include DNA methylation, post-translational modifications of histones proteins and RNA-mediated gene silencing [59]. DNA methylation is a potent regulator of gene expression and has been well studied in the context of carcinogenesis [60]. Histone modifi-cations are maintained through cell division and distinct histone modifications, on one or more tails, act sequentially or in combina-tion to form a histone code. This code is read by other proteins bringing about distinct downstream events dictating disease out-comes [61, 62]. Interestingly, some epigenetic mechanisms of gene expression are regulated by non-coding RNA (ncRNA), which rep-resent key regulators of chromatin remodeling and modulate in turn DNA methylation and histone modifications [62, 63]. During the occurrence of NAFLD several epigenetic alterations may concur. In inbred C57BL/6J and DBA/2J strains of mice, hepatic steatosis was accompanied by loss of genomic cytosine methylation, through aberrant histone modifications, and alterations in expression of the DNA methyltransferase 1 (DNMT1) and DNMT3A proteins in the liver [12]. The DBA/2J strain of mice is characterized by a lower degree of DNA methylation under a normal diet (compared to C57BL/6J mice) and developed more aggressive NASH-specific pathology under a lipogenic methyl deficient diet [12]. Therefore,
the hepatic epigenetic phenotype may predetermine individual sus-ceptibility to hepatic steatosis. In this respect, there is no doubt that an adverse early life environment may increase the susceptibility to later-life metabolic disorders such as NAFLD. Livers of rat off-spring, born of high fat fed mothers (MHF), display a fatty pheno-type reflecting NAFLD [64]. Furthermore, the offspring born to MHF mothers, display an increased expression of the hepatic cell cycle inhibitor Cdkn1a, which in turn was hypomethylated at spe-cific DNA sites, at post natal day 2. Since Cdkn1a upregulation has been associated with hepatocyte growth in liver disease, this may be suggestive of early hepatic dysfunction in neonates born to high fat fed mothers, which are then predisposed to long-term liver diseases such as NAFLD [64]. Intriguingly, rodent studies seem to suggest that the offspring from high fat fed fathers are also prone to develop obesity and related disorders [65], suggesting that intergenerational transmission of metabolic traits such as NAFLD may persist through epigenetic changes in determined genome regions of male gametes [66].
The most prominent epigenetic modification is the acetylation of histones on lysine residues, which are also altered in genetic murine models of steatosis [67, 68]. Loss of acetylation is mediated by the activity of epigenetic enzymes histone deacetylases (HDAC): among those there are the sirtuins. There are 7 mammal-ian sirtuins (SIRT 1-7), NAD
+-dependent protein deacetylases in-
volved in multiple cellular events including chromatin remodelling, energy metabolism and stress resistance [69-72]. The most studied member of the family is SIRT1. SIRT1 is believed to mediate the beneficial effects of caloric restricted dietary regimen in species ranging from yeast to mammals and it is believed that these protec-tive actions may result, at least in part, from the regulation of en-ergy homeostasis, circadian rhythms and anti-oxidant responses in each cell type studied [69-75]. Consistently, SIRT1 is an important regulator of metabolic processes such as lipolysis, fatty acid oxida-tion, mitochondrial activity and gluconeogenesis, which occur in response to an intracellular increase in the NAD+/NADH ratio [76]. In the liver, SIRT1 activates gluconeogenesis through the deacety-lation of peroxisome proliferation activating receptor (PPAR-), co-activator-1- (PGC-1), forkhead O1 (FOXO1) and signal transducer and activator of transcription 3 (STAT3) [77]. SIRT1 also regulates hepatic cholesterol and bile acid homeostasis through direct modulation of LXR and farnesoid X receptor (FXR) [78]. Li et al. showed that SIRT1 can directly deacetylate LXRs, resulting in increased LXR turnover and target gene expression [79]. Whilst a systemic deletion of SIRT1 in mice results in decreased high den-sity lipoprotein (HDL) levels, Kemper et al. showed that bile sensor FXR is a target of hepatic SIRT1 in metabolic regulation [80]. Ace-tylation of FXR inhibits its activity and down-regulation of hepatic SIRT1 increase FXR acetylation causing NAFLD and decreased bile output [81]. Using liver-specific KO mice (SIRT1 LKO), Pu-rushotham et al. showed that the deletion of SIRT1 in liver im-paired PPAR signalling and decreased fatty acid -oxidation, whereas over-expression of SIRT1 induces expression of PPAR- target genes [68]. As a result, SIRT1 LKO mice are susceptible to high-fat diet induced dyslipidemia and hepatic steatosis. Recent evidence suggests that SIRT1 activity is regulated by c-Jun N-terminal kinase 1 (JNK1): persistent JNK1 activation leads to inhi-bition of SIRT1 activity through extensive protein degradation, which may contribute to hepatic steatosis [82]. As discussed above, Notch signaling activation may induce hepatic steatosis [55]. We and others have shown that SIRT1 counteracts Notch signaling in a variety of non hepatic cell types [83, 84]. The interaction between SIRT1 and Notch signaling might be part of a well-defined molecu-lar circuitry also in NAFLD, which is unexplored to date. Further-more, activation of SIRT1 by resveratrol and several synthetic pharmacologic activators have been shown to protect against high-fat induced obesity and metabolic derangements [85]. Resveratrol is a natural polyphenol present in the skin of grapes, nuts and is most concentrated in wine. Recent studies have implicated resveratrol in
-
4 Current Pharmaceutical Design, 2013, Vol. 19, No. 00 Podrini et al.
antagonizing cellular lipid accumulation, and in modulating cellular proliferation and cellular differentiation [86, 87]. Resveratrol also plays an important role in the prevention and therapy of liver dis-eases [88]. In this context, resveratrol is emerging as the lead prom-ising molecule as a natural antioxidant and possibly anti-inflammatory molecule. The activation of SIRT1 by resveratrol in hepatocytes might be intertwined with the activation of AMP-activated protein kinase (AMPK), an energy- sensing enzyme [89]. Mechanistic studies indicate that resveratrol could increase AMPK phosphorylation, with the beneficial effects of resveratrol and other phytoestrogens may be depend upon AMPK activation [90, 91]. It was thought that AMPK signaling was the main upstream event [92]. However, Park et al. recently provided evidence that resvera-trol directly inhibits several phosphodiesterase (PDE) enzymes that indirectly activate SIRT1. This signaling cascade involves the ex-change protein directly activated by cyclic AMP (Epac1), and in turn AMPK [93]. Research in to the cell signaling interactions be-tween resveratrol and resveratrol-like molecules and the sirtuins in the control of the pathogenesis of metabolic diseases such as NAFLD is controversial, rapidly evolving and of pharmaceutical interest.
One of the molecular targets of SIRT1 is macroH2A1, a variant of canonical histone H2A, which has been associated with X-chromosome inactivation [94]. MacroH2A1 can modulate transcrip-tion in a negative or in a positive manner in cancer cells [95]. Mac-roH2A1 homozygosity in mice induces a metabolic phenotype, with hepatic steatosis and glucose intolerance, depending on the genetic background [96, 97]. Interestingly, the gene encoding macroH2A1 can give rise to two alternatively spliced variants: macroH2A1.1 and macroH2A1.2 [98]. MacroH2A1.1 is strongly expressed in post-mitotic tissues, whereas macroH2A1.2 is expressed in prolifer-ating and cancer cells [99]. The two isoforms differ functionally in that macroH2A1.1 binds with very tight affinity the small metabo-lite O-acetyl ADP-ribose (OAADPR) (produced by the enzymatic reaction catalyzed by SIRT1), whereas macroH2A1.2 does not [98]. The expression levels of macroH2A1 isoforms have been shown to predict lung and breast cancer recurrence and to be implicated in the development of skin cancer [99, 100]. Changolkar et al. pro-duced a genome-wide map of the distribution of macroH2A1 nu-cleosomes in mouse liver and found that the macroH2A bounds genes which functionally cluster in the area of lipid metabolism suggesting that this histone variant has a role in regulating genes involved in fatty acid/lipid metabolism [101]. The role of mac-roH2A1 in the pathogenesis of metabolic syndrome-associated NAFLD and hepatocyte malignancy has never been addressed and it is of interest to clarify the molecular mechanism by which histone variants are able to influence the expression of genes related to NAFLD and liver cancer.
1.4. NAFLD AND CARDIOVASCULAR DISEASES: EPIGE-
NETIC ASPECTS
NAFLD is strongly associated with the metabolic syndrome, which is characterized by IR, obesity, dyslipidemia and hyperten-sion [102]. Subjects with features of the metabolic syndrome are at risk in developing cardiovascular disease (CHD) and recent evi-dence suggest that also NAFLD patients have a similar risk [102]. Patients with type 2 diabetes, IR and NAFLD had early features of left ventricular (LV) diastolic dysfunction, even if the LV morphol-ogy and systolic function were preserved, suggesting that there may be early features of LV diastolic dysfunction [103]. The mecha-nisms by which IR may influence LV dysfunction are not com-pletely understood, although they could be related to the ability of insulin to regulate glucose and/or fatty acids metabolism, in turn affecting energy production in cardiomyocytes [104]. These mechanisms may potentially occur with minor changes in LV mass, which seems to grow predominantly because of increased cardiac afterload. Interestingly, heart and liver share common mechanisms of lipotoxicity, which may contribute substantially to the patho-
physiology of IR, type 2 diabetes, steatotic liver and heart failure [105]. Interestingly, Fotbolcu et al. found that NAFLD patients had impaired LV systolic and diastolic function even in the absence of morbid obesity, hypertension or diabetes [106]. Further, Hamaguchi et al. showed that NAFLD might serve as a strong predictor of car-diovascular disease in apparently healthy people, suggesting that the association between NAFLD and cardiovascular disease (CVD) events is independent of conventional cardiovascular risk factors (e.g. dyslipidaemia, diabetes, smoking) [107]. In turn NAFLD, especially in its inflammatory form NASH, may promote pro-inflammatory and pro-atherogenic factors that are likely to play a major role in CVD pathogenesis [108]. Oxidative stress is also a strong atherogenic stimulus, associated with the secretion of in-flammation biomarkers and endothelial dysfunction such as inter-leukin-6 (IL-6) and tumour-necrosis factor- (TNF-), which can be ameliorated by low fat, low caloric dietary adjustments [109]. During the chronic inflammation present in NASH, a systemic re-lease of pro-inflammatory mediators from the liver including C-reactive protein (CRP), fibrinogen and plasminogen activator in-hibitor-1 (PAI-1) and other acute-phase proteins occurs [108]. CRP levels and the degree of carotid atherosclerosis were found to be higher in NAFLD patients than in the control subjects and was also associated with increasing ALT levels, suggesting a link between hepatic injury, inflammation and development and progression of CVD [110].
Epigenetic regulation of gene expression, such as histone modi-fication and DNA methylation, contribute to the atherogenic stim-uli. Methylation levels of the H3 histone tail of lysine 4 and 9 have recently been correlated with gene expression conferred by hyper-glycemia during vascular injury [111]. Environmental factors, such as high fat diet and smoking, may contribute to the pathogenesis of vascular lesions and CVD by modulating DNA methylation in the arterial wall [112]. Additionally, DNA methylation is emerging as a primary regulator of inflammation and has been linked to several cardiovascular related biomarkers, including CRP and homocys-teine levels [113]. DNA methylation is a crucial process in control-ling leukocyte functions related to cardiovascular risk including the expression of soluble mediators and surface molecules that direct margination (pavementing), adhesion and migration of blood leu-kocytes in vessels. Studies in ApoE knock-out mice, which display fatty liver and high cholesterol levels, have shown that changes in DNA methylation pattern in the aorta occurred as early of age and prior to the appearance of vascular lesions, supporting a pathogenic role for abnormal DNA methylation in atherosclerosis [114]. Moreover, DNA methylation changes occur during atherogenesis may contribute to lesion development and accelerated atherosclero-sis. It is clear from these epigenetic studies that the endothelium is the ultimate effector of the metabolic syndrome and should be con-sidered as the main target of studies focusing on the underlying complex network between NAFLD, IR, hypertension and CVD. Understanding the epigenetic and systemic mechanisms of NAFLD-associated cardiac stress is of clinical relevance; as the treatment strategies for NAFLD and cardiovascular disease are similar, aimed at reducing IR and modifying cardiovascular risk factor such as weight reduction, increased physical activity and treatment of individual components of the metabolic syndrome [115]. Research in this direction would be beneficial in discovering new therapeutic guidelines to prevent the development of CVD and to further understand the signaling and epigenetic mechanisms be-hind liver and heart crosstalk during NAFLD-dependent cardiovas-cular disease.
1.5. OXIDATIVE STRESS AND NAFLD
Oxidative stress is often defined as an imbalance of pro-oxidants and antioxidants chemical species (in favor of the former), which leads to oxidative damage of cellular macromolecules [17]. The predominant pro-oxidant chemicals in fatty liver, as in other systems, are singlet oxygen molecules, superoxide anions, hydro-
-
Redox Homeostasis and Epigenetics Current Pharmaceutical Design, 2013, Vol. 19, No. 00 5
gen peroxide, and hydroxyl radicals; collectively referred to as reactive oxygen species (ROS). ROS are highly reactive and unsta-ble due to the fact that they contain an unpaired electron in their outer shell. This conformation promotes their ability to rapidly interact with cellular macromolecules, such as proteins, lipids and nucleic acid [116]. ROS are key secondary messengers in numerous cellular processes including transcriptional regulation, differentia-tion, proliferation to oncogenic transformation and activation of programmed cell death [117]. In the healthy liver, there is an elabo-rate antioxidant defense system consisting of enzymatic antioxi-dants such as catalase, superoxide dismutase, glutathione peroxi-dase and non-enzymatic including glutathione and dietary vitamin A, C, E, which efficiently remove excess ROS to maintain the nor-mal cell homeostasis. In contrast, during chronic liver diseases such as HCC and viral infections, there is an increased ROS production as well as decreased activity of antioxidant systems resulting in oxidative stress [118]. Mitochondria are responsible for oxidative phosphorylation and fatty acid -oxidation and are the major sources of ROS; in turn, they have also a high exposure and suscep-tibility to oxidative damage. Excessive generation of ROS itself may be considered a direct effector of mitochondrial dysfunction in diabetes ROS has been shown to interfere with mitochondrial DNA stability [119]. Mitochondrial dysfunction and inflammatory cells are believed to act in concert in the perpetuation of ROS pro-duction occurring during the progression from simple steatosis to NASH [120]. Abnormal mitochondrial morphology and injury as manifested by mega-mitochondria (giant mitochondria) with crys-talline inclusions have been shown in the liver in NASH patients [121], although the exact function of these structures remains to be defined. Interestingly, mitochondrial dysfunction resulting from a deficiency of long chain acyl-CoA dehydrogenase causes fatty liver and hepatic IR in mice as a result of fatty acid oxidation impairment [122]. Mitochondrial -oxidation of fatty acids can be increased as in IR associated NAFLD, or decreased as in drug-induced NAFLD [123]. In either situation, generation of ROS is augmented, which in a lipid-rich environment leads to lipid peroxidation and subsequent cascade of inflammation and necrosis. In mice fed a high fat diet, genes responsible for ROS production were upregulated in both liver and adipose tissue before the onset of IR, suggesting that ROS may trigger high fat diet-induced IR [124]. An important source of ROS is also the NOX family of NADPH oxidases. Several NOX isoforms are expressed in hepatocytes, hepatic stellate cells and Kupffer cells in the liver, and there is now evidence that inappro-priate activation of NOX enzymes may damage the liver (reviewed in [125, 126]). In the context of NAFLD, as observed in obese rats fed a high fat diet, NADPH oxidase is a key source of ROS produc-tion independently of the mitochondrial respiratory chain [127]. ROS may mediate liver injury by 3 main mechanisms: lipid peroxi-dation, cytokine induction and Fas ligand induction. The increased production of ROS causes lipid peroxidation of plasma or mito-chondrial membranes causing necrosis or inducing apoptosis [128]. Lipid peroxidation can also cause immunological dysfunction, which may link to hepatic fibrosis. In fact, among the results of lipid peroxidation, there is the release of by products such as malondialdehyde (MDA) and 4-hydroxynonenal (HNE), which can bind to hepatocyte proteins and initiate harmful immune response or activate hepatic stellate cells promoting collagen synthesis and stimulate neutrophil chemotaxis [129]. Recent clinical trials suggest that lipid replacement therapy administered as a nutritional supple-ment with antioxidants can prevent excess oxidative membrane damage and restore mitochondrial functions [130].
ROS also increases expression of Fas-ligand on hepatocytes that interacts with normally expressed membrane receptor. Fas on the adjacent hepatocytes can activate apoptotic cell death through caspase activation [131]. Fas activation has also been involved with the activation of stress responsive intracellular signaling pathways, including the mitogen-activated protein kinase (MAPK) pathway and the transcription factor NFB signal cascade. Finally, ROS may
mediate release of TNF-, increasing the expression of several cy-tokines, including transforming growth factor- (TGF-), IL-6 and IL-8. These chemoattractants may account, in part, for the neutro-phil infiltrate observed in NAFLD/NASH [132]. Lipid peroxidation and ROS-induced release of chemo-attractant cytokines concur-rently contribute to NASH [123].
The expression and activity of hepatic microsomal fatty acid oxidizing enzyme cytochrome P450 2E1 (CYP2E1), a putative source for excessive ROS, has been found augmented in both hu-man and animal models of NASH [133]. Interestingly, transgenic over-expression of CYP2E1 resulted in down-regulation of insulin signaling pathways, which may also contribute to IR and NAFLD [134]. As discussed, a causal link between IR and NAFLD is strongly supported by experimental evidence. Hoehn et al. demon-strated that IR may be part of an antioxidant defense mechanism to protect cells from further oxidative damage [135]. There is also suggestive evidence of a strong interrelationship between oxidative stress and NAFLD even in the absence of IR. Subjects with and without type 2 diabetes, with NAFLD, exhibited an increased state of oxidative stress, which could occur in absence of IR and of the metabolic syndrome [136]. Cotrim et al. have consistently shown that the development of fatty liver is not associated with IR and other mechanisms might be involved, such as exposure to environ-mental chemicals, potential sources of oxidant stress [137]. A nice paradigm supporting the proposed function of ROS in NAFLD progression is the role of transcription factor Nrf1, previously de-scribed to be essential for embryonic development. Nrf1 has been implicated in mediating the activation of oxidative stress response genes through the antioxidant response element (ARE) [138]. Se-lective hepatic deletion of the Nrf-1 gene showed that the mouse livers progressively developed all the characteristic features found in the progression of human NAFLD, including steatosis, apoptosis, necrosis, hepatitis, fibrosis and even liver cancer [138].
The pathogenesis of NAFLD is yet not fully understood, but accumulating data suggest that oxidative stress and altered redox balance play a crucial role in its pathogenesis, even in absence of other components of the metabolic syndrome.
1.6. A LINK BETWEEN OXIDATIVE STRESS AND EPIGE-
NETIC MODIFICATIONS IN NAFLD PATHOGENESIS?
Both genetic control of inflammatory responses and epigenetic causes of oxidative stress/inflammation contribute to NAFLD [139]. In this regard, several sirtuins isoforms, chromatin remodel-ing enzymes, are found to be activated during redox stress and may modulate crucial responses, including adaptation to hypoxia and amelioration of ROS-induced pathologies [140], providing a link between epigenetic modifications and redox state. SIRT1 protein deacetylase activity and function is modulated by numerous post-translational modifications in response to altered redox state, which in turn alter its deacetylase activity on target genes. Yang et al. showed that oxidative stress promotes desumoylation and subse-quent inactivation of SIRT1, resulting in increased susceptibility to apoptosis [141]. In the liver, inactivation of SIRT1 decreases PPAR signaling, inducing hepatic steatosis [142]. Moreover, oxi-dative stress classically activates hepatic JNK1, which in turn trig-gers SIRT1 degradation, triggering hepatic steatosis [143].
An additional link between oxidative stress, epigenetics and NAFLD is provided by mitochondria, the major factory of cellu-lar ROS. Decreased liver mitochondrial DNA (mtDNA) content is associated with hepatic steatosis and peripheral IR in patients [139]. Most pathogenic mtDNA mutations induce defects in mitochondrial oxidative phosphorylation, which can occur to different extents in a tissue-type specific manner, suggesting that oxidative phosphoryla-tion cannot be the exclusive pathogenic cause, and epigenetic mechanisms may contribute to diseases. Studies have identified a possible effect on the epigenetic landscape of the nuclear genome, such as methylation pattern of a number of genes, as a consequence
-
6 Current Pharmaceutical Design, 2013, Vol. 19, No. 00 Podrini et al.
of mitochondrial dysfunction in cancer. Recently, it has been pro-posed that persistent pathogenic mutations in mtDNA may lead to epigenetic changes, causing genomic instability in the nuclear ge-nome of cancer cells [144]. If changes in mtDNA could affect lipo-genic gene expression and thereby contribute to the pathogenesis of NAFLD remains to be determined.
Interestingly, the SIRT3 member of the sirtuin family, localizes mainly in the mitochondria and it is required for maintenance of mitochondrial integrity and metabolism upon oxidative stress [145]. SIRT3 has however been localized also in the cell nucleus, where it can deacetylate histones, and it relocalizes to mitochondria upon cellular stress [146]. In the liver, SIRT3 regulates global protein lysine acetylation, fatty acid oxidation and intermediary metabolism by governing mitochondrial 3-hydroxy-3-methylglutaryl CoA syn-thase 2 (HMGCS2) activity and ketone body production depending on the nutritional status [147, 148]. Disruption of SIRT3 activity in mice, either by genetic ablation or during high-fat feeding, is asso-ciated with accelerated development of metabolic abnormalities similar to the metabolic syndrome in humans: SIRT3 knockout mice have been reported to display NASH [149]. SIRT1 and SIRT3 enzymes differ in the subcellular localization and target distinct substrates. Nevertheless, they are evolutionary related in the fact that they both possess histone/protein deacetylase activity and they target homologous substrates in the cytoplasmic and mitochondrial compartment [Acetyl-CoA Synthase 1 (AceCS1)/Acetyl-CoA Syn-thase 2 (AceCS2); 3-hydroxy-3-methylglutaryl CoA synthase 1 (HMGCS1)/3-hydroxy-3-methylglutaryl CoA synthase 2 (HMGCS2)], respectively [150]. Altogether, the published data point to SIRT1 and SIRT3 as crucial gatekeepers of redox status, epigenetic landscape and lipid homeostasis in the hepatocytes. Sev-eral other characterized epigenetic marks, including histone methy-lation, ADP-ribosylation and DNA methylation, may have direct linkages to central metabolism through critical redox intermediates such as NAD
+, which in turn boosts SIRT1 and SIRT3 mediated
enzymatic reactions. These signaling cascades are intertwined in NAFLD pathogenesis.
1.7. COMPOUNDS TO CURE NAFLD
With the increased prevalence of NAFLD worldwide, novel and safe treatments to prevent these diseases are urgently needed. Since NAFLD are often a consequence of obesity and IR/type 2 diabetes, lifestyle modification and weight reduction remain the cornerstones of treatment because they can ameliorate or even reverse the dis-ease. Nonetheless, many compounds have been developed that have a significant beneficial impact on NAFLD. An exhaustive coverage of the topic is out of the scope of this review. However, we will discuss some compounds whose anti-oxidant properties have been explored. Drugs highly effective against NAFLD are the insulin sensitizers, metformin, pioglitazone and rosiglitazone, which all reduce oxidative stress. Studies on overweight or obese patients with ultrasonographic diagnosis of hepatic steatosis, metformin was found to be more effective than dietary treatment alone in amelio-rating metabolic derangements and NAFLD [151]. The metabolic effects of metformin are mainly mediated through the activation of AMPK, and most recently a role of SIRT1 for metformin mecha-nism of action was demonstrated in hepatocytes [152]. Thiazolidin-ediones class of molecules, such as pioglitazione and rosiglitazone, activate peroxisome proliferator-activated receptor-gamma PPAR, which regulates triglyceride homeostasis, contributing to hepatic steatosis [153]. Pioglitazone and rosiglitazone are highly effective in improving NAFLD outcome in patients [154]. Like metformin, thiazolidinediones may exert their effect partly by impinging on the SIRT1/AMPK signaling axis [155]. Unfortunately, the use of thia-zolidinediones in the clinic against NAFLD has been hampered by side effects. Rosiglitazone was put under restrictions in the US and withdrawn from the market in Europe due to an increased risk of cardiovascular events [156], while pioglitazone was suspended because it could raise the risk of bladder cancer [157]. Pioglitazone
also causes fluid retention at the kidney level, which may lead to congestive heart failure [158].
Studies on NASH patients as well as on murine models have suggested some beneficial roles of natural antioxidant molecules [159], which are in most cases over-the-counter nutritional supple-ment sold in many countries. Supplementation of lipoic acid, bene-ficial on mitochondrial function and oxidative stress, reduced he-patic steatosis in Wistar rats by increasing the enzymatic activities of epigenetic enzymes SIRT1 and SIRT3 [160]. Vitamin D or vita-min E anti-oxidant therapies hold a potential therapeutic role for NAFLD. Vitamin D deficiency exacerbated NAFLD and inflamma-tion in a Western diet rat model, causing IR and upregulation of hepatic inflammatory and oxidative stress genes, suggesting that its supplementation might be beneficial for NAFLD [161]. Vitamin E treatment, compared with placebo, was associated with a signifi-cantly higher rate of improvement in NAFLD patients and did not cause the weight gain observed with pioglitazone and rosiglitazone [154]. Despite these interesting findings, the impact of vitamin D supplementation in human NAFLD awaits validation, and treatment with high dose vitamin E should be carefully considered due to its association with higher risk for stroke and mortality [162]. Fur-thermore, the intake of bioactive phytochemicals that are present in fruit, vegetables, herbs and medicinal plants have been shown to activate the expression of several antioxidants that might be benefi-cial for the metabolic syndrome and NAFLD [163]. Resveratrol, a polyphenol contained in red grapes well known to activate SIRT1, seems effective in reducing hepatic lipid accumulation in several rodent models of obesity and metabolic syndrome [164-166]. How-ever, it is difficult to recommend specific dietary products in pa-tients as it is yet unknown whether high amount of specific antioxi-dants will decrease the risk of NAFLD progression to chronic liver disease. It can be expected that further exploring the potential of natural compounds could potentially lead to a new generation of drugs for fat-induced liver disease.
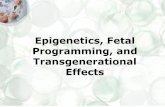
Fig. (1). Schematic representation of the interplay of epigenetics, oxidative
stress and inflammation in the pathogenesis of NAFLD. Abbreviations:
E.S., extracellular space; M, mitochondria; N, nucleus; TG, triglycerydes;
FFA, free fatty acids; NASH, non alcoholic steatohepatitis. See text for
details.
1.8. CONCLUSION
NAFLD is among the most common liver diseases in the West-ern World, and is expected to rise even further due to increase in major risk factors including diabetes and obesity. NAFLD starts with lipid accumulation and often progresses to NASH, and in some cases to HCC. The prevention of liver failure is to halt the loss of
-
Redox Homeostasis and Epigenetics Current Pharmaceutical Design, 2013, Vol. 19, No. 00 7
hepatocytes and to develop novel therapeutic or dietary interven-tions. However, understanding the molecular defects in the intracel-lular signaling and epigenetic events involved in the onset of meta-bolic and oxidative stress-associated NAFLD is of crucial impor-tance (Fig. 1). For instance, the role of the chromatin remodeling enzymes and histone variants on the complex interplay of enzymes and signaling cascades regulating hepatocytes intracellular lipid turnover is unexplored. Understanding the epigenetic molecular details behind NAFLD holds important prospects for medical treatments, because epigenetic therapy could offer the potential of targeting several genes with one drug. The near future is likely to bring important insights into epigenetic gene regulation in both normal and sick liver as new technologies to explore chromatin transcriptional plasticity are developing fast.
COMPETING INTERESTS
The authors declare no competing financial interests.
ACKNOWLEDGEMENTS
M.V. is supported by the Foundation for Liver Research (Lon-don, UK). We are grateful to Giuseppe Costanza for preparing the illustration.
REFERENCES
[1] Fabbrini E, Sullivan S, Klein S. Obesity and nonalcoholic fatty liver disease: biochemical, metabolic, and clinical implications.
Hepatology. ; 51(2): 679-89. [2] Malhi H, Guicciardi ME, Gores GJ. Hepatocyte death: a clear and
present danger. Physiol Rev 2010; 90(3): 1165-94. [3] Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steatohepati-
tis: summary of an AASLD Single Topic Conference. Hepatology 2003; 37(5): 1202-19.
[4] Petta S, Muratore C, Craxi A. Non-alcoholic fatty liver disease pathogenesis: the present and the future. Dig Liver Dis 2009; 41(9):
615-25. [5] Myers RP. Noninvasive diagnosis of nonalcoholic fatty liver dis-
ease. Ann Hepatol 2009; 8 Suppl 1: S25-33. [6] Sass DA, Chang P, Chopra KB. Nonalcoholic fatty liver disease: a
clinical review. Dig Dis Sci 2005; 50(1): 171-80. [7] Kantartzis K, Schick F, Haring HU, Stefan N. Environmental and
genetic determinants of fatty liver in humans. Dig Dis 2010; 28(1): 169-78.
[8] Day CP, James OF. Steatohepatitis: a tale of two "hits"? Gastroen-terology 1998; 114(4): 842-5.
[9] Anstee QM, Goldin RD. Mouse models in non-alcoholic fatty liver disease and steatohepatitis research. Int J Exp Pathol 2006; 87(1):
1-16. [10] Bieghs V, Van Gorp PJ, Wouters K, Hendrikx T, Gijbels MJ, van
Bilsen M, et al. LDL receptor knock-out mice are a physiological model particularly vulnerable to study the onset of inflammation in
non-alcoholic fatty liver disease. PLoS ONE 2012; 7(1): e30668. [11] Bieghs V, van Gorp PJ, Walenbergh S, Gijbels MJ, Verheyen F,
Buurman WA, et al. Specific immunization strategies a gainst oxi-dized LDL: A novel way to reduce non-alcoholic steatohepa titis in
mice. Hepatology 2012 Feb 15. [12] Pogribny IP, Tryndyak VP, Bagnyukova TV, Melnyk S, Montgom-
ery B, Ross SA, et al. Hepatic epigenetic phenotype predetermines individual susceptibility to hepatic steatosis in mice fed a lipogenic
methyl-deficient diet. J Hepatol 2009; 51(1): 176-86. [13] Feinberg AP. Phenotypic plasticity and the epigenetics of human
disease. Nature 2007 May 24; 447(7143): 433-40. [14] Feinberg AP. Epigenetics at the epicenter of modern medicine.
JAMA 2008 Mar 19; 299(11): 1345-50. [15] Youngson NA, Whitelaw E. Transgenerational epigenetic effects.
Annu Rev Genomics Hum Genet 2008; 9: 233-57. [16] Daxinger L, Whitelaw E. Understanding transgenerational epige-
netic inheritance via the gametes in mammals. Nat Rev Genet 2012; 13(3): 153-62.
[17] Robertson G, Leclercq I, Farrell GC. Nonalcoholic steatosis and steatohepatitis. II. Cytochrome P-450 enzymes and oxidative stress.
Am J Physiol Gastrointest Liver Physiol 2001; 281(5): G1135-9.
[18] Bergamini CM, Gambetti S, Dondi A, Cervellati C. Oxygen, reac-
tive oxygen species and tissue damage. Curr Pharm Des 2004; 10(14): 1611-26.
[19] Browning JD, Horton JD. Molecular mediators of hepatic steatosis and liver injury. J Clin Invest 2004; 114(2): 147-52.
[20] Seki S, Kitada T, Yamada T, Sakaguchi H, Nakatani K, Wakasa K. In situ detection of lipid peroxidation and oxidative DNA damage
in non-alcoholic fatty liver diseases. J Hepatol 2002; 37(1): 56-62. [21] Musso G, Gambino R, Cassader M. Recent insights into hepatic
lipid metabolism in non-alcoholic fatty liver disease (NAFLD). Prog Lipid Res 2009; 48(1): 1-26.
[22] Utzschneider KM, Kahn SE. Review: The role of insulin resistance in nonalcoholic fatty liver disease. J Clin Endocrinol Metab 2006;
91(12): 4753-61. [23] Postic C, Girard J. Contribution of de novo fatty acid synthesis to
hepatic steatosis and insulin resistance: lessons from genetically engineered mice. J Clin Invest 2008; 118(3): 829-38.
[24] Lewis GF, Carpentier A, Adeli K, Giacca A. Disordered fat storage and mobilization in the pathogenesis of insulin resistance and type
2 diabetes. Endocr Rev 2002; 23(2): 201-29. [25] De Gottardi A, Vinciguerra M, Sgroi A, Moukil M, Ravier-
Dall'Antonia F, Pazienza V, et al. Microarray analyses and molecu-lar profiling of steatosis induction in immortalized human hepato-
cytes. Lab Invest 2007; 87(8): 792-806. [26] Lou-Bonafonte JM, Arnal C, Osada J. New genes involved in he-
patic steatosis. Curr Opin Lipidol 2011; 22(3): 159-64. [27] Horie Y, Suzuki A, Kataoka E, Sasaki T, Hamada K, Sasaki J, et
al. Hepatocyte-specific Pten deficiency results in steatohepatitis and hepatocellular carcinomas. J Clin Invest 2004; 113(12): 1774-
83. [28] Vinciguerra M, Carrozzino F, Peyrou M, Carlone S, Montesano R,
Benelli R, et al. Unsaturated fatty acids promote hepatoma prolif-eration and progression through downregulation of the tumor sup-
pressor PTEN. J Hepatol 2009; 50(6): 1132-41. [29] Vinciguerra M, Foti M. PTEN and SHIP2 phosphoinositide phos-
phatases as negative regulators of insulin signalling. Arch Physiol Biochem 2006; 112(2): 89-104.
[30] Vinciguerra M, Foti M. PTEN at the crossroad of metabolic dis-eases and cancer in the liver. Ann Hepatol 2008 Jul-Sep; 7(3): 192-
9. [31] Vinciguerra M, Sgroi A, Veyrat-Durebex C, Rubbia-Brandt L,
Buhler LH, Foti M. Unsaturated fatty acids inhibit the expression of tumor suppressor phosphatase and tensin homolog (PTEN) via
microRNA-21 up-regulation in hepatocytes. Hepatology 2009; 49(4): 1176-84.
[32] Vinciguerra M, Veyrat-Durebex C, Moukil MA, Rubbia-Brandt L, Rohner-Jeanrenaud F, Foti M. PTEN down-regulation by unsatu-
rated fatty acids triggers hepatic steatosis via an NF-kappaBp65/mTOR-dependent mechanism. Gastroenterology 2008;
134(1): 268-80. [33] Clement S, Peyrou M, Sanchez-Pareja A, Bourgoin L, Ramadori P,
Suter D, et al. Down-regulation of phosphatase and tensin homolog by hepatitis C virus core 3a in hepatocytes triggers the formation of
large lipid droplets. Hepatology 2011; 54(1): 38-49. [34] Leavens KF, Easton RM, Shulman GI, Previs SF, Birnbaum MJ.
Akt2 is required for hepatic lipid accumulation in models of insulin resistance. Cell Metab 2009; 10(5): 405-18.
[35] He L, Hou X, Kanel G, Zeng N, Galicia V, Wang Y, et al. The critical role of AKT2 in hepatic steatosis induced by PTEN loss.
Am J Pathol 2010; 176(5): 2302-8. [36] Horton JD. Sterol regulatory element-binding proteins: transcrip-
tional activators of lipid synthesis. Biochem Soc Trans 2002; 30(Pt 6): 1091-5.
[37] Haeusler RA, Han S, Accili D. Hepatic FoxO1 ablation exacerbates lipid abnormalities during hyperglycemia. J Biol Chem 2010 Aug
27; 285(35): 26861-8. [38] Kersten S. Mechanisms of nutritional and hormonal regulation of
lipogenesis. EMBO Rep 2001; 2(4): 282-6. [39] Schwarz JM, Linfoot P, Dare D, Aghajanian K. Hepatic de novo
lipogenesis in normoinsulinemic and hyperinsulinemic subjects consuming high-fat, low-carbohydrate and low-fat, high-
carbohydrate isoenergetic diets. Am J Clin Nutr 2003; 77(1): 43-50.
[40] Iizuka K, Bruick RK, Liang G, Horton JD, Uyeda K. Deficiency of carbohydrate response element-binding protein (ChREBP) reduces
-
8 Current Pharmaceutical Design, 2013, Vol. 19, No. 00 Podrini et al.
lipogenesis as well as glycolysis. Proc Natl Acad Sci U S A 2004
May 11; 101(19): 7281-6. [41] Pettinelli P, Del Pozo T, Araya J, Rodrigo R, Araya AV, Smok G,
et al. Enhancement in liver SREBP-1c/PPAR-alpha ratio and stea-tosis in obese patients: correlations with insulin resistance and n-3
long-chain polyunsaturated fatty acid depletion. Biochim Biophys Acta 2009; 1792(11): 1080-6.
[42] Ducheix S, Lobaccaro JM, Martin PG, Guillou H. Liver X Recep-tor: an oxysterol sensor and a major player in the control of lipo-
genesis. Chem Phys Lipids 2011; 164(6): 500-14. [43] Peet DJ, Turley SD, Ma W, Janowski BA, Lobaccaro JM, Hammer
RE, et al. Cholesterol and bile acid metabolism are impaired in mice lacking the nuclear oxysterol receptor LXR alpha. Cell 1998
May 29; 93(5): 693-704. [44] Im SS, Osborne TF. Liver x receptors in atherosclerosis and in-
flammation. Circ Res 2011 Apr 15; 108(8): 996-1001. [45] Fievet C, Staels B. Combination therapy of statins and fibrates in
the management of cardiovascular risk. Curr Opin Lipidol 2009; 20(6): 505-11.
[46] Lee JH, Wada T, Febbraio M, He J, Matsubara T, Lee MJ, et al. A novel role for the dioxin receptor in fatty acid metabolism and he-
patic steatosis. Gastroenterology 2010; 139(2): 653-63. [47] Kang HS, Okamoto K, Kim YS, Takeda Y, Bortner CD, Dang H, et
al. Nuclear orphan receptor TAK1/TR4-deficient mice are pro-tected against obesity-linked inflammation, hepatic steatosis, and
insulin resistance. Diabetes 2011; 60(1): 177-88. [48] Zhang N, Fu Z, Linke S, Chicher J, Gorman JJ, Visk D, et al. The
asparaginyl hydroxylase factor inhibiting HIF-1alpha is an essential regulator of metabolism. Cell Metab 2010 May 5; 11(5): 364-78.
[49] Cermelli S, Ruggieri A, Marrero JA, Ioannou GN, Beretta L. Cir-culating microRNAs in patients with chronic hepatitis C and non-
alcoholic fatty liver disease. PLoS ONE 2011; 6(8): e23937. [50] Dowman JK, Tomlinson JW, Newsome PN. Systematic review: the
diagnosis and staging of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2010; 33(5):
525-40. [51] Fujii H, Kawada N. Inflammation and fibrogenesis in steatohepati-
tis. J Gastroenterol 2012; 47(3): 215-25. [52] Baffy G. Kupffer cells in non-alcoholic fatty liver disease: the
emerging view. J Hepatol 2009; 51(1): 212-23. [53] Tschopp J, Schroder K. NLRP3 inflammasome activation: The
convergence of multiple signalling pathways on ROS production? Nat Rev Immunol 2010; 10(3): 210-5.
[54] Henao-Mejia J, Elinav E, Jin C, et al. Inflammasome-mediated dysbiosis regulates progression of NAFLD and obesity. Nature. ;
482(7384): 179-85. [55] Fowler JC, Zecchini VR, Jones PH. Intestinal activation of Notch
signaling induces rapid onset hepatic steatosis and insulin resis-tance. PLoS ONE 2011; 6(6): e20767.
[56] Corbin KD, Zeisel SH. Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Curr Opin
Gastroenterol 2012; 28(2): 159-65. [57] Portela A, Esteller M. Epigenetic modifications and human disease.
Nat Biotechnol 2010; 28(10): 1057-68. [58] Sharma S, Kelly TK, Jones PA. Epigenetics in cancer. Carcino-
genesis 2010; 31(1): 27-36. [59] Sawan C, Vaissiere T, Murr R, Herceg Z. Epigenetic drivers and
genetic passengers on the road to cancer. Mutat Res 2008; 642(1-2): 1-13.
[60] Gertych A, Farkas DL, Tajbakhsh J. Measuring topology of low-intensity DNA methylation sites for high-throughput assessment of
epigenetic drug-induced effects in cancer cells. Exp Cell Res 2010; 316(19): 3150-60.
[61] Strahl BD, Allis CD. The language of covalent histone modifica-tions. Nature 2000; 403(6765): 41-5.
[62] Lennartsson A, Ekwall K. Histone modification patterns and epige-netic codes. Biochim Biophys Acta 2009; 1790(9): 863-8.
[63] Gibbs JR, van der Brug MP, Hernandez DG, et al. Abundant quan-titative trait loci exist for DNA methylation and gene expression in
human brain. PLoS Genet 2011; 6(5): e1000952. [64] Dudley KJ, Sloboda DM, Connor KL, Beltrand J, Vickers MH.
Offspring of mothers fed a high fat diet display hepatic cell cycle inhibition and associated changes in gene expression and DNA
methylation. PLoS ONE 2011; 6(7): e21662.
[65] Ng SF, Lin RC, Laybutt DR, Barres R, Owens JA, Morris MJ.
Chronic high-fat diet in fathers programs beta-cell dysfunction in female rat offspring. Nature 2010; 467(7318): 963-6.
[66] Curley JP, Mashoodh R, Champagne FA. Epigenetics and the ori-gins of paternal effects. Horm Behav 2011; 59(3): 306-14.
[67] Feng D, Liu T, Sun Z, et al. A circadian rhythm orchestrated by histone deacetylase 3 controls hepatic lipid metabolism. Science
2011 Mar 11; 331(6022): 1315-9. [68] Purushotham A, Schug, TT, Xu, Q, Surapureddi, S, Guo, X, Li, X.
Hepatocyte-specific deletion of SIRT1 alters fatty acid metabolism and results in hepatic steatosis and inflammation. . Cell Metab
2009; 9(4): 327-38. [69] Guarente L. Franklin H. Epstein Lecture: Sirtuins, aging, and
medicine. N Engl J Med 2011 Jun 9; 364(23): 2235-44. [70] Vinciguerra M, Santini MP, Martinez C, et al. mIGF-1/JNK1/SirT1
signaling confers protection against oxidative stress in the heart. Aging Cell 2012; 11(1): 139-49.
[71] Vinciguerra M, Fulco M, Ladurner A, Sartorelli V, Rosenthal N. SirT1 in muscle physiology and disease: lessons from mouse mod-
els. Dis Model Mech 2010; 3(5-6): 298-303. [72] Vinciguerra M, Santini MP, Claycomb WC, Ladurner AG, Rosen-
thal N. Local IGF-1 isoform protects cardiomyocytes from hyper-trophic and oxidative stresses via SirT1 activity. Aging (Albany
NY) 2009; 2(1): 43-62. [73] Mazzoccoli G, Pazienza V, Vinciguerra M. Clock genes and clock-
controlled genes in the regulation of metabolic rhythms. Chrono-biol Int 2012; 29(3): 227-51.
[74] Tonkin J, Villarroya F, Puri PL, Vinciguerra M. SIRT1 signaling as potential modulator of skeletal muscle diseases. Curr Opin Phar-
macol 2012 Mar 6. [75] Pazienza V, Piepoli A, Panza A, Valvano MR, Benegiamo G, Vin-
ciguerra M, et al. SIRT1 and the clock gene machinery in colorec-tal cancer. Cancer Invest 2012; 30(2): 98-105.
[76] Feige J, Auwerx, J. Transcriptional targets of sirtuins in the coordi-nation of mammalian physiology. Curr Opin Cell Biol 2008; 20(3):
303-9. [77] Horio Y. Diabetes: Insulin signal meets SIRT1 at AKT. Nat Rev
Endocrinol 2011; 8(3): 131-2. [78] Lee J, Padhye A, Sharma A, et al. A pathway involving farnesoid
X receptor and small heterodimer partner positively regulates he-patic sirtuin 1 levels via microRNA-34a inhibition. J Biol Chem
2010; 285(17): 12604-11. [79] Li X, Zhang S, Blander G, Tse JG, Krieger M, Guarente L. SIRT1
deacetylates and positively regulates the nuclear receptor LXR. Mol Cell 2007; 28(1): 91-106.
[80] Kemper JK, Xiao Z, Ponugoti B, et al. FXR acetylation is normally dynamically regulated by p300 and SIRT1 but constitutively ele-
vated in metabolic disease states. Cell Metab 2009; 10(5): 392-404. [81] Li X, Kazgan N. Mammalian sirtuins and energy metabolism. Int J
Biol Sci 2011; 7(5): 575-87. [82] Gao Z, Zhang J, Kheterpal I, Kennedy N, Davis RJ, Ye J. Sirtuin 1
(SIRT1) protein degradation in response to persistent c-Jun N-terminal kinase 1 (JNK1) activation contributes to hepatic steatosis
in obesity. J Biol Chem 2011; 286(25): 22227-34. [83] Guarani V, Deflorian G, Franco CA, et al. Acetylation-dependent
regulation of endothelial Notch signalling by the SIRT1 deacety-lase. Nature 2011; 473(7346): 234-8.
[84] Sciacca S, Pilato M, Mazzoccoli G, Pazienza V, Vinciguerra M. Anti-correlation between longevity gene SirT1 and Notch signaling
in ascending aorta biopsies from patients with bicuspid aortic valve disease. Heart Vessels 2012 Feb 28; [Epub ahead of print].
[85] Pfluger P, Herranz D, Velasco-Miguel S, Serrano M, Tschp MH. Sirt1 protects against high-fat diet-induced metabolic damage. Proc
Natl Acad Sci U S A 2008; 105(28): 9793-8. [86] Singh UP, Singh NP, Singh B, et al. Resveratrol (trans-3,5,4'-
trihydroxystilbene) induces silent mating type information regula-tion-1 and down-regulates nuclear transcription factor-kappaB acti-
vation to abrogate dextran sulfate sodium-induced colitis. J Phar-macol Exp Ther 2011; 332(3): 829-39.
[87] Warnke I, Goralczyk R, Fuhrer E, Schwager J. Dietary constituents reduce lipid accumulation in murine C3H10 T1/2 adipocytes: A
novel fluorescent method to quantify fat droplets. Nutr Metab (Lond) 2011; 8(1): 30.
[88] Bishayee A, Dhir N. Resveratrol-mediated chemoprevention of diethylnitrosamine-initiated hepatocarcinogenesis: inhibition of cell
-
Redox Homeostasis and Epigenetics Current Pharmaceutical Design, 2013, Vol. 19, No. 00 9
proliferation and induction of apoptosis. Chem Biol Interact 2009;
179(2-3): 131-44. [89] Hou X, Xu S, Maitland-Toolan KA, et al. SIRT1 regulates hepato-
cyte lipid metabolism through activating AMP-activated protein kinase. J Biol Chem 2008; 283(29): 20015-26.
[90] Um JH, Park SJ, Kang H, et al. AMP-activated protein kinase-deficient mice are resistant to the metabolic effects of resveratrol.
Diabetes 2010; 59(3): 554-63. [91] Cederroth CR, Vinciguerra M, Gjinovci A, et al. Dietary phytoes-
trogens activate AMP-activated protein kinase with improvement in lipid and glucose metabolism. Diabetes 2008; 57(5): 1176-85.
[92] Canto C, Gerhart-Hines Z, Feige JN, et al. AMPK regulates energy expenditure by modulating NAD+ metabolism and SIRT1 activity.
Nature 2009; 458(7241): 1056-60. [93] Park SJ, Ahmad F, Philp A, et al. Resveratrol ameliorates aging-
related metabolic phenotypes by inhibiting cAMP phosphodi-esterases. Cell 2012; 148(3): 421-33.
[94] Gamble MJ, Kraus WL. Multiple facets of the unique histone vari-ant macroH2A: From genomics to cell biology. Cell Cycle 2010;
9(13). [95] Gamble M, Frizzell KM, Yang C, Krishnakumar R, Kraus WL.
The histone variant macroH2A1 marks repressed autosomal chro-matin, but protects a subset of its target genes from silencing.
Genes Dev 2010; 24(1): 21-32. [96] Boulard M, Storck S, Cong R, Pinto R, Delage H, Bouvet P. His-
tone variant macroH2A1 deletion in mice causes female-specific steatosis. Epigenetics Chromatin 2010; 3(1): 8. [Epub ahead of
print]. [97] Changolkar L, Costanzi C, Leu NA, Chen D, McLaughlin KJ,
Pehrson JR. Developmental changes in histone macroH2A1-mediated gene regulation. Mol Cell Biol 2007; 27(7): 2758-64.
[98] Kustatscher G, Hothorn M, Pugieux C, Scheffzek K, Ladurner AG. Splicing regulates NAD metabolite binding to histone macroH2A.
Nat Struct Mol Biol 2005; 12(7): 624-5. [99] Sporn J, Kustatscher G, Hothorn T, et al. Histone macroH2A iso-
forms predict the risk of lung cancer recurrence. Oncogene 2009; Aug 3. [Epub ahead of print].
[100] Kapoor A, Goldberg MS, Cumberland LK, et al. The histone vari-ant macroH2A suppresses melanoma progression through regula-
tion of CDK8. Nature 2010; 468(7327): 1105-9. [101] Changolkar LN, Singh G, Cui K, et al. Genome-Wide Distribution
of MacroH2A1 Histone Variants in Mouse Liver Chromatin. Mol Cell Biol 2010 Oct 11.
[102] Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med 2010;
363(14): 1341-50. [103] Bonapace S, Perseghin G, Molon G, et al. Nonalcoholic fatty liver
disease is associated with left ventricular diastolic dysfunction in patients with type 2 diabetes. Diabetes Care 2012; 35(2): 389-95.
[104] Ouwens DM, Boer C, Fodor M, et al. Cardiac dysfunction induced by high-fat diet is associated with altered myocardial insulin signal-
ling in rats. Diabetologia 2005; 48(6): 1229-37. [105] Martinez de Morentin PB, Varela L, Ferno J, Nogueiras R, Dieguez
C, Lopez M. Hypothalamic lipotoxicity and the metabolic syn-drome. Biochim Biophys Acta 2010; 1801(3): 350-61.
[106] Fotbolcu H, Yakar T, Duman D, et al. Impairment of the left ven-tricular systolic and diastolic function in patients with non-
alcoholic fatty liver disease. Cardiol J 2010; 17(5): 457-63. [107] Hamaguchi M, Kojima T, Takeda N, et al. Nonalcoholic fatty liver
disease is a novel predictor of cardiovascular disease. World J Gas-troenterol 2007; 13(10): 1579-84.
[108] Targher G, Bertolini L, Rodella S, et al. NASH predicts plasma inflammatory biomarkers independently of visceral fat in men.
Obesity (Silver Spring) 2008; 16(6): 1394-9. [109] Fontana L, Vinciguerra M, Longo VD. Growth factors, nutrient
signaling, and cardiovascular aging. Circ Res 2012 Apr 13; 110(8): 1139-50.
[110] Brea A, Mosquera D, Martin E, Arizti A, Cordero JL, Ros E. Non-alcoholic fatty liver disease is associated with carotid atherosclero-
sis: a case-control study. Arterioscler Thromb Vasc Biol 2005; 25(5): 1045-50.
[111] Cooper ME, El-Osta A. Epigenetics: mechanisms and implications for diabetic complications. Circ Res 2010; 107(12): 1403-13.
[112] Ordovas JM, Smith CE. Epigenetics and cardiovascular disease. Nat Rev Cardiol 2010; 7(9): 510-9.
[113] Baccarelli A, Tarantini L, Wright RO, et al. Repetitive element
DNA methylation and circulating endothelial and inflammation markers in the VA normative aging study. Epigenetics 2010; 5(3).
[114] Lund G, Andersson L, Lauria M, et al. DNA methylation polymor-phisms precede any histological sign of atherosclerosis in mice
lacking apolipoprotein E. J Biol Chem 2004; 279(28): 29147-54. [115] Erlinger S. Do patients with nonalcoholic fatty liver disease die
from their heart? Clin Res Hepatol Gastroenterol 2011; 35(3): 163-5.
[116] Valko M, Rhodes CJ, Moncol J, Izakovic M, Mazur M. Free radi-cals, metals and antioxidants in oxidative stress-induced cancer.
Chem Biol Interact 2006; 160(1): 1-40. [117] Circu ML, Aw TY. Reactive oxygen species, cellular redox sys-
tems, and apoptosis. Free Radic Biol Med 2010; 48(6): 749-62. [118] Ha HL, Yu DY. HBx-induced reactive oxygen species activates
hepatocellular carcinogenesis via dysregulation of PTEN/Akt pathway. World J Gastroenterol 2010; 16(39): 4932-7.
[119] Savu O, Sunkari VG, Botusan IR, Grunler J, Nikoshkov A, Catrina SB. Stability of mitochondrial DNA against reactive oxygen spe-
cies (ROS) generated in diabetes. Diabetes Metab Res Rev 2011; 27(5): 470-9.
[120] Begriche K, Igoudjil A, Pessayre D, Fromenty B. Mitochondrial dysfunction in NASH: causes, consequences and possible means to
prevent it. Mitochondrion 2006; 6(1): 1-28. [121] Le TH, Caldwell SH, Redick JA, et al. The zonal distribution of
megamitochondria with crystalline inclusions in nonalcoholic stea-tohepatitis. Hepatology 2004; 39(5): 1423-9.
[122] Zhang D, Liu ZX, Choi CS, et al. Mitochondrial dysfunction due to long-chain Acyl-CoA dehydrogenase deficiency causes hepatic
steatosis and hepatic insulin resistance. Proc Natl Acad Sci U S A 2007; 104(43): 17075-80.
[123] Fromenty B, Robin MA, Igoudjil A, Mansouri A, Pessayre D. The ins and outs of mitochondrial dysfunction in NASH. Diabetes Me-
tab 2004; 30(2): 121-38. [124] Matsuzawa-Nagata N, Takamura T, Ando H, et al. Increased oxi-
dative stress precedes the onset of high-fat diet-induced insulin re-sistance and obesity. Metabolism 2008; 57(8): 1071-7.
[125] Guichard C, Moreau R, Pessayre D, Epperson TK, Krause KH. NOX family NADPH oxidases in liver and in pancreatic islets: a
role in the metabolic syndrome and diabetes? Biochem Soc Trans 2008; 36(Pt 5): 920-9.
[126] Bedard K, Krause KH. The NOX family of ROS-generating NADPH oxidases: physiology and pathophysiology. Physiol Rev
2007; 87(1): 245-313. [127] Carmiel-Haggai M, Cederbaum AI, Nieto N. A high-fat diet leads
to the progression of non-alcoholic fatty liver disease in obese rats. Faseb J 2005; 19(1): 136-8.
[128] Das K, Kar P. Non-alcoholic steatohepatitis. J Assoc Physicians India 2005; 53: 195-9.
[129] Duvnjak M, Lerotic I, Barsic N, Tomasic V, Virovic Jukic L, Ve-lagic V. Pathogenesis and management issues for non-alcoholic
fatty liver disease. World J Gastroenterol 2007; 13(34): 4539-50. [130] Nicolson GL. Metabolic syndrome and mitochondrial function:
molecular replacement and antioxidant supplements to prevent membrane peroxidation and restore mitochondrial function. J Cell
Biochem 2007; 100(6): 1352-69. [131] Malhi H, Gores GJ, Lemasters JJ. Apoptosis and necrosis in the
liver: a tale of two deaths? Hepatology 2006; 43(2 Suppl 1): S31-44.
[132] Carter-Kent C, Zein NN, Feldstein AE. Cytokines in the patho-genesis of fatty liver and disease progression to steatohepatitis: im-
plications for treatment. Am J Gastroenterol 2008; 103(4): 1036-42.
[133] Aubert J, Begriche K, Knockaert L, Robin MA, Fromenty B. In-creased expression of cytochrome P450 2E1 in nonalcoholic fatty
liver disease: mechanisms and pathophysiological role. Clin Res Hepatol Gastroenterol 2011; 35(10): 630-7.
[134] Schattenberg JM, Wang Y, Singh R, Rigoli RM, Czaja MJ. Hepa-tocyte CYP2E1 overexpression and steatohepatitis lead to impaired
hepatic insulin signaling. J Biol Chem 2005 Mar 18; 280(11): 9887-94.
[135] Hoehn KL, Salmon AB, Hohnen-Behrens C, et al. Insulin resis-tance is a cellular antioxidant defense mechanism. Proc Natl Acad
Sci U S A 2009; 106(42): 17787-92. [136] Narasimhan S, Gokulakrishnan K, Sampathkumar R, Farooq S,
Ravikumar R, Mohan V, et al. Oxidative stress is independently as-
-
10 Current Pharmaceutical Design, 2013, Vol. 19, No. 00 Podrini et al.
sociated with non-alcoholic fatty liver disease (NAFLD) in subjects
with and without type 2 diabetes. Clin Biochem 2010; 43(10-11): 815-21.
[137] Cotrim HP, Carvalho F, Siqueira AC, Lordelo M, Rocha R, De Freitas LA. Nonalcoholic fatty liver and insulin resistance among
petrochemical workers. JAMA 2005; 294(13): 1618-20. [138] Xu Z, Chen L, Leung L, Yen TS, Lee C, Chan JY. Liver-specific
inactivation of the Nrf1 gene in adult mouse leads to nonalcoholic steatohepatitis and hepatic neoplasia. Proc Natl Acad Sci U S A
2005; 102(11): 4120-5. [139] Sookoian S, Rosselli MS, Gemma C, Burgueno AL, Fernandez
Gianotti T, Castano GO, et al. Epigenetic regulation of insulin re-sistance in nonalcoholic fatty liver disease: impact of liver methyla-
tion of the peroxisome proliferator-activated receptor gamma coac-tivator 1alpha promoter. Hepatology 2010; 52(6): 1992-2000.
[140] Webster BR, Lu Z, Sack MN, Scott I. The role of sirtuins in modu-lating redox stressors. Free Radic Biol Med 2012; 52(2): 281-90.
[141] Yang Y, Fu W, Chen J, et al. SIRT1 sumoylation regulates its deacetylase activity and cellular response to genotoxic stress. Nat
Cell Biol 2007; 9(11): 1253-62. [142] Purushotham A, Schug TT, Xu Q, Surapureddi S, Guo X, Li X.
Hepatocyte-specific deletion of SIRT1 alters fatty acid metabolism and results in hepatic steatosis and inflammation. Cell Metab 2009;
9(4): 327-38. [143] Gao Z, Zhang J, Kheterpal I, Kennedy N, Davis RJ, Ye J. SIRT1
degradation in response to persistent JNK1 activation contributes to hepatic steatosis in obesity. J Biol Chem 2011 May 3.
[144] Minocherhomji S, Tollefsbol TO, Singh KK. Mitochondrial regula-tion of epigenetics and its role in human diseases. Epigenetics
2012; 7(4). [145] Kim HS, Patel K, Muldoon-Jacobs K, et al. SIRT3 is a mitochon-
dria-localized tumor suppressor required for maintenance of mito-chondrial integrity and metabolism during stress. Cancer Cell 2010;
17(1): 41-52. [146] Scher MB, Vaquero A, Reinberg D. SirT3 is a nuclear NAD+-
dependent histone deacetylase that translocates to the mitochondria upon cellular stress. Genes Dev 2007; 21(8): 920-8.
[147] Shimazu T, Hirschey MD, Hua L, et al. SIRT3 deacetylates mito-chondrial 3-hydroxy-3-methylglutaryl CoA synthase 2 and regu-
lates ketone body production. Cell Metab 2010; 12(6): 654-61. [148] Hirschey MD, Shimazu T, Goetzman E, et al. SIRT3 regulates
mitochondrial fatty-acid oxidation by reversible enzyme deacetyla-tion. Nature 2010; 464(7285): 121-5.
[149] Hirschey MD, Shimazu T, Jing E, et al. SIRT3 deficiency and mitochondrial protein hyperacetylation accelerate the development
of the metabolic syndrome. Mol Cell 2011; 44(2): 177-90. [150] Hirschey MD, Shimazu T, Capra JA, Pollard KS, Verdin E. SIRT1
and SIRT3 deacetylate homologous substrates: AceCS1,2 and HMGCS1,2. Aging (Albany NY) 2011; 3(6): 635-42.
[151] Garinis GA, Fruci B, Mazza A, , et al. Metformin versus dietary treatment in nonalcoholic hepatic steatosis: a randomized study. Int
J Obes (Lond) 2010; 34(8): 1255-64.
[152] Nelson LE, Valentine RJ, Cacicedo JM, Gauthier MS, Ido Y, Rud-
erman NB. A novel inverse relationship between metformin-triggered AMPK-SIRT1 signaling and p53 protein abundance in
high glucose exposed HepG2 cells. Am J Physiol Cell Physiol 2010 Feb 29.
[153] Gavrilova O, Haluzik M, Matsusue K, et al. Liver peroxisome proliferator-activated receptor gamma contributes to hepatic steato-
sis, triglyceride clearance, and regulation of body fat mass. J Biol Chem 2003; 278(36): 34268-76.
[154] Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med 2010;
362(18): 1675-85. [155] Shen Z, Liang X, Rogers CQ, Rideout D, You M. Involvement of
adiponectin-SIRT1-AMPK signaling in the protective action of rosiglitazone against alcoholic fatty liver in mice. Am J Physiol
Gastrointest Liver Physiol 2011; 298(3): G364-74. [156] Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myo-
cardial infarction and death from cardiovascular causes. N Engl J Med 2007; 356(24): 2457-71.
[157] Ryder RE. Pioglitazone and bladder cancer. Lancet 2011; 378(9802): 1544; author reply -5.
[158] Zanchi A, Maillard M, Jornayvaz FR, et al. Effects of the perox-isome proliferator-activated receptor (PPAR)-gamma agonist pio-
glitazone on renal and hormonal responses to salt in diabetic and hypertensive individuals. Diabetologia 2010; 53(8): 1568-75.
[159] Anderson N, Borlak J. Molecular mechanisms and therapeutic targets in steatosis and steatohepatitis. Pharmacol Rev 2008; 60(3):
311-57. [160] Valdecantos MP, Perez-Matute P, Gonzalez-Muniesa P, Prieto-
Hontoria PL, Moreno-Aliaga MJ, Martinez JA. Lipoic Acid Im-proves Mitochondrial Function in Nonalcoholic Steatosis Through
the Stimulation of Sirtuin 1 and Sirtuin 3. Obesity (Silver Spring) 2012 Feb 13.
[161] Roth CL, Elfers CT, Figlewicz DP, et al. Vitamin D deficiency in obese rats exacerbates nonalcoholic fatty liver disease and in-
creases hepatic resistin and Toll-like receptor activation. Hepatol-ogy 2012; 55(4): 1103-11.
[162] Zelber-Sagi S, Ratziu V, Oren R. Nutrition and physical activity in NAFLD: an overview of the epidemiological evidence. World J
Gastroenterol 2011; 17(29): 3377-89. [163] Soory M. Relevance of nutritional antioxidants in metabolic syn-
drome, ageing and cancer: potential for therapeutic targeting. Infect Disord Drug Targets 2009; 9(4): 400-14.
[164] Cho SJ, Jung UJ, Choi MS. Differential effects of low-dose res-veratrol on adiposity and hepatic steatosis in diet-induced obese
mice. Br J Nutr 2012; 14: 1-10. [165] Gomez-Zorita S, Fernandez-Quintela A, Macarulla MT, et al. Res-
veratrol attenuates steatosis in obese Zucker rats by decreasing fatty acid availability and reducing oxidative stress. Br J Nutr 2012;
107(2): 202-10. [166] Bujanda L, Hijona E, Larzabal M, et al. Resveratrol inhibits nonal-
coholic fatty liver disease in rats. BMC Gastroenterol 2008; 8: 40.
Received: September 25, 2012 Accepted: October 17, 2012