Recommended management of vestibular causes of · PDF fileRecommended management of vestibular...
5
Click here to load reader
Transcript of Recommended management of vestibular causes of · PDF fileRecommended management of vestibular...

Dizziness or imbalance is experi-enced by 30 per cent of the UK
population before the age of 65 andbecomes the commonest reason fora visit to their GP for patientsbeyond 75 years of age. Recentlypublished proposals from theDepartment of Health stress theimportance of raising awareness ofthe prevalence of these disordersand the distress they can cause,while emphasising the role local bal-ance services in the community willplay in future care provision.
Medication is often useful, espe-cially in the acute phase, but as pro-longed drug therapy can slow orprevent recovery in certain vestibu-lar conditions and many nonphar-macological treatments are
available, cautious prescribing maybe required.
Vestibular causes of dizzinessWhen assessing a patient with avestibular disorder it is helpful clin-ically to consider three distinctgroups of patients, as treatment andprescribing will be different foreach: the acute episode, the recur-rent acute episode and chronicvestibular symptoms.
The acute vestibular episode Vestibular neuritis Acute vestibularneuritis (also referred to as vestibu-lar neuronitis or viral labyrinthitis)is common and presents with arapid onset of distressing rotational
vertigo associated with nausea andvomiting. There are no associatedneurologic or auditory symptoms.It can be terrifying and patientsoften believe they are having astroke. Persistent horizontal-tor-sional jerk nystagmus is observedusually towards the unaffected ear(a paralytic nystagmus). The severevertigo settles over days and mostpatients recover spontaneously overdays or weeks. Those who fail tocompensate are left with chronicvestibular symptoms.
Vestibular neuritis is believed toresult most commonly from a viralinflammation of the superior divi-sion of the vestibular nerve. It canoccur in clusters in the community(‘epidemic labyrinthitis’). As the
52 Prescriber 5 October 2010 www.prescriber.co.uk
Prescribing in practice
Recommended management ofvestibular causes of dizzinessPeter Rea MA, FRCS
Most patients with vestibular
causes of dizziness can now
be treated with either drug
therapy or vestibular physio-
therapy. Mr Peter Rea dis-
cusses the various causes of
dizziness and their appropri-
ate management.
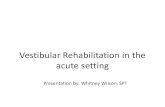
Figure 1. The inner ear showing a cross-sectional view of the cochlea
SP
L

nerve degenerates the end organ(the utricle) also degenerates: it isfrom here that the otoconia thatcause benign paroxysmal posi-tional vertigo (BPPV) are releasedand it is common for patients toreport symptoms of vestibular neu-ritis months or years before theonset of BPPV.
Labyrinthitis Symptoms oflabyrinthitis are those of vestibularneuritis but with additional acutehearing loss and tinnitus. Most casesare believed to be viral in origin andaffect the membranous vestibularlabyrinth and cochlea. Ischaemicevents, particularly in the older per-son, may have similar results.Hearing loss is often permanent.
In contrast suppurative (bacter-ial) labyrinthitis is a severe invasiveinfection often associated withacute otitis media and sometimesmeningitis. Hearing loss and vertigoare both severe.
Recurrent acute vertigo of vestibular originThere are four classical vestibulardisorders that cause recurrent ver-tiginous episodes, along with a hostof less common conditions.
Benign paroxysmal positional vertigoBPPV is the commonest cause ofrecurrent short-lasting vertigo. Over2 per cent of people experience itat some time and its incidenceincreases with age. Intense unpleas-ant spinning lasting up to a minuteis triggered by position change suchas looking up, lying down, gettingup from bed or rolling over in bed.It often occurs in clusters that areself-limiting. It may result from anyinner ear damage, the commonestbeing head injury, previous vestibu-lar neuritis and aging. Otolithsreleased from the injured utriclemigrate to the posterior semicircu-lar canal and their movement trig-gers vertigo. It is diagnosed on theHallpike test where upbeat, tor-
sional, geotropic nystagmus isobserved.
Vestibular migraine A controver-sial but increasingly recognisedcause of vertigo, vestibularmigraine may affect 1 per cent ofthe population. Headaches occurin only 25-50 per cent of cases. Thevertigo may last minutes, hours(usually) or even days. A family his-tory of migraine is helpful andmigraine aura diagnostic if present.Patients’ balance is good betweenattacks but a history of motion sick-ness is common.
Ménière’s disease has a prevalenceas high as 0.2-0.5 per cent. Classicalattacks are described as a build-upof unilateral tinnitus, aural fullnessand hearing loss followed by severevertigo associated with vomitingand diarrhoea lasting from 20 min-utes to 10 hours. Hearing recoversafter the attack to a variable degree.In practice Ménière’s can presentwith only one or two of the classicalsymptoms making diagnosis chal-lenging. Attacks occur in clustersand may be spaced over months oryears. The aetiology remainsobscure though some attacks seemto have an autoimmune basis.
Recurrent vestibular neuritisRecurrent vertigo attacks lastinghours or days are often very diffi-cult to diagnose as the patient hasno signs or symptoms when exam-ined. Reactivation of a latent neuro -tropic virus, particularly the herpessimplex virus, is thought to beresponsible for some cases. Thismight be similar to recurrent Bell’s
palsy or cold sores for example.Attacks seem to reduce in severitywith time.
Other causes of recurrent dizzinessThere is a wide range of less com-mon disorders. Enquiring about theseven ‘P’s’ of recurrent vertigo mayhelp distinguish between them (seeTable 1). Vestibular paroxysmia isan interesting condition thought toarise from irritability of the vestibu-lar nerve causing multiple very briefspins every day.
Chronic vestibular symptomsThe most common presentation ina balance clinic is of the chronicallydizzy patient. Symptoms are variedand summarised in Table 2. Suchsymptoms usually result from inad-equate central compensation to aperipheral vestibular deficit.Neurological and cardiovascular‘red flags’ should be sought andreferred appropriately. Exam -ination of other systems that maybe preventing recovery is helpful.In older people there may be mul-tiple contributors, hence the term‘multisystem balance disorder’ (seeFigure 2).
Pharmacological treatmentMedication in vestibular disordersis usually palliative rather thancurative, the exceptions beingintratympanic gentamicin forMénière’s disease and antibioticsfor suppurative labyrinthitis.Many drugs do, however, have avaluable role.
www.prescriber.co.uk Prescriber 5 October 2010 53
Prescribing in practice
Table 1. Key questions in recurrent acute dizziness: the seven P’s
1. Positional trigger BPPV2. Pressure induced perilymph fistula, superior canal
dehiscence syndrome3. Postural trigger postural hypotension 4. Phonophobia, photophobia migraine5. Psychological hyperventilation, panic attack6. Paroxysmia vestibular paroxysmia 7. Periodic perimenstrual symptoms

Treating the acute vestibular episode A combination of vestibular sup-pressant and antiemetic is requiredfor the distressing acute vestibularevent.
Vestibular suppressantsVestibular suppressants should beused only during the acute phase ofthe illness. Prolonged use may pre-vent central adaptation to a periph-eral vestibular lesion and result inchronic vestibular symptoms. Thebenzodiazipines are among themore potent vestibular suppressantsand diazepam is a good choice foran acute attack. As a gamma-aminobutyric acid (GABA;inhibitory neurotransmitter) ago-nist it is thought to have aninhibitory effect on the vestibularnuclei. Its anxiolytic action is anadditional help.
PromethazinePromethazine is an antihistaminicprothiazine and has significant anti-histaminic and anticholinergicproperties. It acts both as an effec-tive antiemetic and mild vestibularsedative.
CinnarizineCinnarizine is another usefulvestibular suppressant with antihis-taminic properties but also acts as acalcium-channel blocker and blocks5-HT receptors, reducing vestibularnuclei activity. Although promotedfor use in Ménière’s disease it alsohas a role in the days followingacute vestibular neuritis and in cer-tain chronic vestibular conditions.
DimenhydrinateDimenhydrinate is an antihistaminewith vestibular suppressant andmotion sickness suppression prop-erties. It is not used frequently onits own in the UK, but a combina-tion with cinnarizine (Arlevert) is apromising addition to our thera-
peutic options, particularly whenused in the first days or weeks fol-lowing an acute attack. It is popularin Europe.
Antiemetics Prochlorperazine is an antidopamin-ergic phenothiazine that acts byblocking the chemoreceptor triggerzone centrally. It is the most com-monly prescribed medication foracute vertiginous episodes in theUK. It is an effective antiemetic.
However, its prolonged use isdiscouraged for two reasons. Firstly,it may slow central adaptation to avestibular injury. Many patientsreferred to the balance centre aretaken off their prochlorperazineand it is only then that their vestibu-lar rehabilitation physiotherapy willbegin to work. Secondly, extrapyra-midal side-effects are often seenwith prolonged use.
Cyclizine (Valoid) is an antihista-mine with anticholinergic activityhelpful for acute vertigo. It also actson central chemoreceptor triggerzones and is effective in controllingnausea, vomiting and vertigo.
Steroids The use of steroids in themanagement of acute vestibularneuritis is probably beneficial. Astudy1 showed that a reducing doseof methylprednisolone (starting at100mg on day 1 and reducing to10mg by three weeks) produced asignificant reduction in persistentvestibular weakness. While potential
side-effects need to be discussedwith patients, on balance the evi-dence suggests this should be con-sidered for patients with acutevestibular neuritis. Antiviral medica-tion, in contrast, was of no benefit.
Antibiotics If acute otitis mediaoccurs in conjunction with vertigoantibiotics are required urgentlyand such patients should bereferred for specialist management.
Treating recurrent acutevertigo of vestibular originBPPV Medication plays no significant partin the management of BPPV as it isusually so easily treated with Epleymanoeuvres (see Figure 3).
Vestibular migraine Lifestyle and dietary alterations areoften adequate in treatingmigraine. For those more severelyaffected the side-effect profile ofthe available drugs needs to be dis-cussed with patients. For acuteattacks analgesics and antiemeticsare the mainstay of treatment, buttriptans can be both helpful thera-peutically and diagnostically if oneis uncertain as to the cause of recur-rent acute vertigo attacks.
Amitriptyline is often my first-linerecommendation, or nortriptylinewhich is less sedating. Treatmentstarts at 10mg nocte for the firstmonth working up in 10mg incre-ments at monthly intervals. Somepatients find it too sedating.
Propranolol is helpful, especiallywhere anxiety is also a problem;however, cardiovascular and respi-ratory interactions may limit its use.
Pizotifen is an antihistamine andserotonin antagonist. It is an effec-tive migraine prophylactic thoughweight gain can be a problem.
Verapamil is the most effective ofthe calcium-channel blockers forthe management of migraine.Although less effective than the tri-cyclics and beta-blockers, it has the
54 Prescriber 5 October 2010 www.prescriber.co.uk
Prescribing in practice
Table 2. The myriad symptoms of chronicvestibulopathy
cotton wool in headwalking on cotton wooleyes not keeping up with brain when turning head
forgetfulnessfatiguedrunken feelingmood changeneck acheheadache and facial pain

advantage of often being well toler-ated long term.
Acetazolamide, the carbonic anhy-drase inhibitor, is also reported onoccasion to be successful inmigraine prophylaxis. It sharessome features with topiramate (ananticonvulsant), which is more reg-ularly recommended.
Ménière’s diseaseLifestyle and dietary modificationsare also the first-line treatment forMénière’s, in particular a low saltdiet aiming for 2.5g of sodium perday. Although evidence in the liter-ature is not strong, this is often rec-ommended.
Betahistine is usually the firstdrug recommended in the UK. Itsmechanism of action is unclear, butit is felt to act as a vasodilator on thestria vascularis of the inner ear,which may reduce hydrops. It hassome vestibular sedative properties.It is extremely well tolerated. Whilemany patients report little benefit,
there is no doubt many feel a rapidreturn of symptoms if they stop it.
Bendroflumethiazide is usually thesecond-line therapy, especially if alow salt diet is difficult. It is thoughtto work by reducing the sodiumload and thus reducing hydrops inthe labyrinth. Again, evidence issparse. Other diuretics may also berecommended.
Diuretics are particularly helpfulfor women whose symptoms areexacerbated with their menstrualperiod, and I recommend ben-droflumethiazide for the five daysbefore their period to reduce thefluid load in the labyrinth.
Urea is an interesting medica-tion. It tastes absolutely foul andpatients are rather reluctant todrink ‘concentrated urine’ despiteassurances that it is entirely syn-thetic; 25mg dissolved in orangejuice and knocked back quickly isjust about bearable. It does have aplace, though, for Ménière’spatients: they are almost guaran-
teed 24 hours free from attacks aftertaking it as it dehydrates thelabyrinth. Consider it before impor-tant exams or weddings (and therecan be no greater confirmation ofdevotion). A test dose before thebig day is recommended.
Steroids have a place in the man-agement of both Ménière’s diseaseand autoimmune inner ear disease,the symptoms of which can overlap.They may be given orally as prophy-laxis but have gained popularitywhen given via a transtympanicroute with a spinal needle underlocal anaesthetic. The treatment isvery well tolerated (I have neverhad anyone not complete thecourse) and may give long periodsfree from attack. Dexamethasone ispreferred for injection.
Gentamicin, the aminoglycosideantibiotic, has revolutionised themanagement of severe Ménière’sdisease. It is selectively vestibulo-toxic and is also administered via atranstympanic route in clinic.
56 Prescriber 5 October 2010 www.prescriber.co.uk
Prescribing in practice
Figure 2. Systems that can affect balance
labyrinthine
musculoskeletal
medications Dizziness/imbalance
proprioceptive/peripheral nervous
system
psychiatric
genetic
autoimmune cardiovascular
haematological
endocrine
central and autonomic nervous
systems
visual/ocular

Reduction in vertigo is observed in96 per cent of patients and perma-nent abolition of vertigo in 80 percent; 5 per cent lose all the hearingin the treated ear (though this isoften very poor already), and asmall number experience imbal-ance for a while. This treatment hastransformed the lives of many of mypatients.
Cinnarizine or Arlevert is some-times prescribed to help patientsthrough clusters of attacks.
Recurrent vestibular neuritisAs this condition is thought to havea reactivated virus as its aetiologythere is a potential advantage inprescribing a short course of pred-nisolone and aciclovir at the onsetof symptoms. It is a treatment I useonly occasionally and the evidenceis in part theoretical.
Rare conditionsCarbamazepine, an anticonvulsant, isused to treat vestibular paroxysmiaas it appears to stabilise the irritablevestibular nerve.
Acetazolamide is particularly inter-esting as it can be a very effectivetreatment for familial episodicataxia type II – although perhapsmore cerebellar than vestibular, it isseen in the balance centre as itshares features with migraine andMénière’s and can be a rewardingcondition to diagnose and treat.
Treating chronic vestibularsymptomsMedication plays a much smallerrole in chronic vestibular symp-toms, in part for fear of preventingcentral adaptation.
Prochlorperazine has no signifi-cant place in the long-term manage-ment of chronic vestibular deficits.
Hyoscine hydrobromide is effectivein preventing motion sickness,though a recent Cochrane reviewwas unable to compare it to othermotion sickness medications such
as antihistamines. There is no goodevidence to support its use in estab-lished motion sickness syndromes.
Cinnarizine or Arlevert is some-times used to help patients throughexacerbations of their chronicsymptoms.
Many patients with chronicvestibulopathies have a significantemotional reaction to their illness –indeed this is almost universal. Ifanxiety and panic disorder areprominent and psychological inter-ventions are unsuccessful, I some-times use a short course of thebenzodiazepine clonazepam in verylow dose (this is off licence, how-ever, and careful explanation isrequired), which also helps settletheir sleep pattern and anxiety aswell as being a vestibular sedative.Lorazepam or diazepam might beconsidered too.
SSRIs such as citalopram areoften helpful but as an ENT sur-geon I do not feel it appropriate toprescribe these myself.
ConclusionA wide variety of drug classes havebeen discussed that may helppatients with vestibular disordersand all have their place. In many
cases, however, vestibular physio-therapy or particle repositioningmanouvres will be the mainstay oftreatment. In selected cases surgerycan be curative. With this combina-tion of therapies now available,most patients with vestibular disor-ders can be successfully managed.
Further readingBallantyne’s deafness. 7th ed. GrahamJ, Baguley D, eds. Ch 24. Disorders ofbalance. Rea P. Wiley-Blackwell, 2009.Methylprednisolone, valacyclovir orthe combination for vestibular neu-ritis. Strupp M, et al. NEJM 2004;351(4):354-61.Practical management of the dizzy patient.2nd ed. Goebel J, ed. LippincottWilliams and Wilkins, 2008.Provision of adult balance services, agood practice guide. 2009. (www.dh.gov.uk/publications).
Reference1. Strupp M, et al. NEJM 2004;351(4):354-61.
Mr Rea is consultant ENT surgeon atThe Leicester Royal Infirmary andlead clinician at The Leicester BalanceCentre and The Balance Clinic at TheLondon Road Clinic, Leicester
www.prescriber.co.uk Prescriber 5 October 2010 57
Prescribing in practice
Figure 3. The Epley manoeuvre is used to treat benign paroxysmal positional vertigo. Thehead is held in specific positions on the opposite side to that which elicits symptoms.