
Recommendations on the content of a survey protocol for€¦ · 37 SCHEDULE FOR THE PROPOSED...
126
Working document QAS/14.590 July 2014 Document for comment Recommendations on the content of a survey protocol for 1 surveys of the quality of medicines 1 2 (July 2014) 3 DRAFT FOR COMMENT 4 5 6 7 8 9 10 11 12 © World Health Organization 2014 13 All rights reserved. 14 This draft is intended for a restricted audience only, i.e. the individuals and organizations having received this draft. The draft 15 may not be reviewed, abstracted, quoted, reproduced, transmitted, distributed, translated or adapted, in part or in whole, in 16 any form or by any means outside these individuals and organizations (including the organizations' concerned staff and 17 member organizations) without the permission of the World Health Organization. The draft should not be displayed on any 18 website. 19 Please send any request for permission to: 20 Dr Sabine Kopp, Group Lead, Medicines Quality Assurance, Technologies, Standards and Norms, Department of Essential 21 Medicines and Health Products, World Health Organization, CH-1211 Geneva 27, Switzerland. Fax: (41-22) 791 4730; 22 email: [email protected]. 23 The designations employed and the presentation of the material in this draft do not imply the expression of any opinion 24 whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or 25 of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate 26 border lines for which there may not yet be full agreement. 27 The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or 28 recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors 29 and omissions excepted, the names of proprietary products are distinguished by initial capital letters. 30 All reasonable precautions have been taken by the World Health Organization to verify the information contained in this 31 draft. However, the printed material is being distributed without warranty of any kind, either expressed or implied. The 32 responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health 33 Organization be liable for damages arising from its use. 34 This draft does not necessarily represent the decisions or the stated policy of the World Health Organization. 35 36 1 This was previously working document QAS/12.510: Proposal for a procedure on sampling and market surveillance survey. Should you have any comments on the attached revision, please send these to Dr S. Kopp, Group Lead, Medicines Quality Assurance, Technologies, Standards and Norms ([email protected]) with a copy to Ms Marie Gaspard ([email protected]) by 30 August 2014. Our working documents will be sent out electronically only and will also be placed on the Medicines website for comment under “Current projects”. If you do not already receive our draft working documents please let us have your email address (to [email protected]) and we will add it to our electronic mailing list.
-
Upload
vuongquynh -
Category
Documents
-
view
215 -
download
1
Transcript of Recommendations on the content of a survey protocol for€¦ · 37 SCHEDULE FOR THE PROPOSED...
Working document QAS/14.590
July 2014
Document for comment
Recommendations on the content of a survey protocol for 1
surveys of the quality of medicines1 2
(July 2014) 3
DRAFT FOR COMMENT 4
5
6
7
8
9
10
11
12
© World Health Organization 2014 13
All rights reserved. 14
This draft is intended for a restricted audience only, i.e. the individuals and organizations having received this draft. The draft 15 may not be reviewed, abstracted, quoted, reproduced, transmitted, distributed, translated or adapted, in part or in whole, in 16 any form or by any means outside these individuals and organizations (including the organizations' concerned staff and 17 member organizations) without the permission of the World Health Organization. The draft should not be displayed on any 18 website. 19
Please send any request for permission to: 20
Dr Sabine Kopp, Group Lead, Medicines Quality Assurance, Technologies, Standards and Norms, Department of Essential 21 Medicines and Health Products, World Health Organization, CH-1211 Geneva 27, Switzerland. Fax: (41-22) 791 4730; 22 email: [email protected]. 23
The designations employed and the presentation of the material in this draft do not imply the expression of any opinion 24 whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or 25 of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate 26 border lines for which there may not yet be full agreement. 27
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or 28 recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors 29 and omissions excepted, the names of proprietary products are distinguished by initial capital letters. 30
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this 31 draft. However, the printed material is being distributed without warranty of any kind, either expressed or implied. The 32 responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health 33 Organization be liable for damages arising from its use. 34
This draft does not necessarily represent the decisions or the stated policy of the World Health Organization. 35
36
1
This was previously working document QAS/12.510: Proposal for a procedure on sampling and market
surveillance survey.
Should you have any comments on the attached revision, please send these to Dr S. Kopp, Group
Lead, Medicines Quality Assurance, Technologies, Standards and Norms ([email protected]) with a
copy to Ms Marie Gaspard ([email protected]) by 30 August 2014.
Our working documents will be sent out electronically only and will also be placed on the
Medicines website for comment under “Current projects”. If you do not already receive our
draft working documents please let us have your email address (to [email protected]) and we
will add it to our electronic mailing list.

Working document QAS/14.590
page 2
SCHEDULE FOR THE PROPOSED ADOPTION PROCESS OF DOCUMENT QAS/14.590: 37
Recommendations on the content of a survey protocol for 38
surveys of the quality of medicines 39
40
41
Survey and feedback from national organizations and
nongovernmental organizations
June–September 2011
Presentation to forty-sixth meeting of the WHO Expert
Committee on Specifications for Pharmaceutical
Preparations
9–12 October 2011
Expert Committee recommendation to develop sampling
procedure (WHO Technical Report Series, No. 970)
October 2011
Proposal for a procedure on sampling and market
surveillance
August 2012
Working document sent out for comment September 2012
Collation of comments September–October 2012
Presentation to forty-seventh meeting of the WHO Expert
Committee on Specifications for Pharmaceutical
Preparations
October 2012
Receipt of document on Recommendations on the
content of a Survey Protocol: Surveys of the quality of
essential medicines from Ms Patricia Tabernero,
Scientific Coordinator, Antimalarial Quality Module,
WorldWide Antimalarial Resistance Network, in close
collaboration with Ms Sue J. Lee, Ms Kasia Stepniewska
and Mr Paul N. Newton
June 2014
Working document sent out for comment July 2014
Collation of comments August–September 2014
Presentation to forty-ninth meeting of the WHO Expert
Committee on Specifications for Pharmaceutical
Preparations
October 2014
Any further action as necessary …

Working document QAS/14.590
page 3
42
43
Recommendations on the content of a survey protocol for 44
surveys of the quality of medicines 45
46
A survey protocol may follow chapters as suggested below or may be appropriately modified. 47
Explanatory notes are in italics. 48
49
BACKGROUND 50
Extract from the forty-eighth report of the WHO Expert Committee on Specifications for 51
Pharmaceutical Preparations: 52
8.2.2 Proposal for a procedure on sampling and market surveillance survey 53
Following the recommendation made by the Expert Committee at its forty-sixth 54
and forty-seventh meetings in 2011 and 2012 the Secretariat commissioned the 55
development of guidance for sampling procedures based on examples obtained 56
from many countries as feedback to the Secretariat's proposal for a procedure on 57
sampling and market surveillance and on a first proposal presented in 2012. This 58
first proposal was based on an existing survey protocol developed by the WHO 59
Prequalification Laboratory Programme, which had been extensively involved 60
in the establishment of survey protocols for major studies for antimalarial and 61
antituberculosis medicines. 62
The Expert Committee noted in 2012 that the document would be of 63
particular importance in monitoring and post-marketing surveillance and agreed 64
that it should be further developed as a general document to provide advice on 65
sampling for various groups of medicines. The Expert Committee also noted 66
the need for separate, specific guidance in relation to SFFC medical products. 67
A comprehensive draft working document, which would be prepared 68
for public consultation in due course, was presented to the Expert Committee 69
for comments. 70
The Expert Committee noted this information and thanked the Secretariat 71
for the draft working document. 72
73
This document is now being submitted as the first of two dealing with the monitoring and 74
postmarket surveillance of medicines and providing advice on survey protocols and sampling for 75
medicines. A second specific guidance is in preparation in relation to spurious/falsely-labelled/ 76
falsified/counterfeit (SFFC) medical products. 77
Working document QAS/14.590
page 4
CONTENTS 78
page 79
1. Acknowledgements .............................................................................................................................. 6 80
2. Glossary of terms and abbreviations ..................................................................................................... 7 81
3. Executive summary .............................................................................................................................. 8 82
4. Introduction and background ................................................................................................................ 8 83
5. Initial planning ................................................................................................................................... 13 84
5.1 What is already known about medicine quality? ........................................................... 13 85
5.2 What registered and unregistered medicines are available in the survey area? ............... 13 86
5.3 What is the distribution system or supply chain of the medicines? ................................ 14 87
5.4 Maps of pharmaceutical outlets .................................................................................... 15 88
5.5 Information on health-seeking behaviour for the target pharmaceuticals? ..................... 15 89
6. Objectives .......................................................................................................................................... 15 90
6.1 Are there poor-quality drugs in this area, border checkpoint, etc.? ................................ 16 91
6.2 What are the proportion of poor-quality medicines being sold and/or proportion 92
of outlets selling poor-quality medicines in a particular geographical area? ................................ 17 93
6.3 Do the proportion of poor-quality medicines or the proportion of outlets selling 94
poor-quality medicines exceed a predetermined level? ............................................................... 17 95
6.4 Has medicine quality changed for the better or worse in an area or for a 96
medicine or medicine group? ..................................................................................................... 18 97
6.5 Areas to be sampled ..................................................................................................... 18 98
6.6 Products to be surveyed ................................................................................................ 20 99
6.7 Medicine preparation type ............................................................................................ 22 100
6.8 Timing of the survey .................................................................................................... 22 101
6.9 Types of sample collection sites ................................................................................... 22 102
6.10 Definitions used to determine quality ........................................................................... 25 103
7. Survey management and time frame ................................................................................................... 25 104
8. Methodology ...................................................................................................................................... 26 105
8.1 Terminology ................................................................................................................. 27 106
8.2 Sampling designs (convenience, random, LQAS, sentinel) ........................................... 29 107
Convenience sampling ............................................................................................................... 29 108
Random sampling ...................................................................................................................... 30 109
Lot quality assurance sampling .................................................................................................. 31 110
Sentinel site monitoring ............................................................................................................. 32 111
8.3 Number of dosage units to be collected: ....................................................................... 33 112
8.4 Sampling techniques for the dosage units within medicine samples .............................. 38 113
9. Sample collection ............................................................................................................................... 40 114
Overt sampling versus mystery shopper methodology ................................................................ 40 115
Survey team and procedures for collection ................................................................................. 42 116
10. Ethical considerations on quality of medicines surveys ..................................................................... 44 117
General ethical issues................................................................................................................. 45 118
Risks to the survey team members? ........................................................................................... 47 119
Working document QAS/14.590
page 5
What is the risk to those surveyed? ............................................................................................ 47 120
Do medicine quality surveys require review by a research ethics committee? ............................. 48 121
Should outlet staff be told that they are being part of a study? .................................................... 50 122
What to do with the information once it has been gathered? ....................................................... 51 123
11. Storage and transport of samples ...................................................................................................... 52 124
12. Techniques to determine quality and laboratory facilities ................................................................. 53 125
Assays to be conducted .............................................................................................................. 54 126
Test methods and specifications ................................................................................................. 55 127
Receipt and testing of samples by a testing laboratory ................................................................ 56 128
13. Data management, reporting and publication.................................................................................... 56 129
14. Conclusions ..................................................................................................................................... 60 130
15. References: ...................................................................................................................................... 61 131
Annex 1. Sources of information of medicine quality 132
Annex 2. Methodology section 133
Annex 3. National sampling plan 134
Annex 4. Sample collection form 135
Annex 5. SOP for mystery shopper methodology 136
Annex 6. SOP for overt sampling methodology 137
Annex 7. Testing protocol 138
Annex 8. Content of the analytical test report 139
Appendix to survey protocol 140
Example based on WHO survey of the quality of antituberculosis medicines circulating in selected NIS of the former
Soviet Union:
1. Questionnaire
2. National sampling plan
3. Sample collection form
4. Testing protocol 5. Content of the analytical test report
141
142
Working document QAS/14.590
page 6
ACKNOWLEDGEMENTS 143
144
This document was prepared by: 145
Patricia Tabernero (WorldWide Antimalarial Resistance Network (WWARN), Centre for 146
Tropical Medicine, Nuffield Department of Medicine, University of Oxford, Oxford, United 147
Kingdom); Sue J. Lee (Mahidol Oxford Tropical Medicine Research Unit, Faculty of Tropical 148
Medicine, Mahidol University, Bangkok, Thailand, Centre for Tropical Medicine, Nuffield 149
Department of Medicine, University of Oxford, Oxford, United Kingdom); Kasia 150
Stepniewska (Worldwide Antimalarial Resistance Network (WWARN), Centre for Tropical 151
Medicine, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom); 152
Paul N. Newton (Worldwide Antimalarial Resistance Network (WWARN), Centre for 153
Tropical Medicine, Nuffield Department of Medicine, University of Oxford, Oxford, United 154
Kingdom). 155
156
We are very grateful to all those who have given advice and have helped in the completion of 157
this report: 158
Roger Bate, American Enterprise Institute, Washington, D.C., United States of America; 159
Facundo Fernández, Georgia Institute of Technology, Atlanta, Georgia, United States of 160
America; Michael Green, Division of Parasitic Diseases, CDC, Atlanta, Georgia, United 161
States of America; Philippe Guerin, WorldWide Antimalarial Resistance Network, Oxford 162
University, United Kingdom; Manuel Hetzel, Swiss Tropical and Public Health Institute, 163
Switzerland; Harparkash Kaur, London School of Hygiene and Tropical Medicine, United 164
Kingdom; Mayfong Mayxay, Laos–Oxford, Mahosot Hospital – Wellcome Trust Unit, 165
Vientiane, Lao People’s Democratic Republic; Michael Parker, Ethox Centre, Oxford 166
University, United Kingdom; Souly Phanouvong, United States Pharmacopeia, Rockville, 167
MD, United States of America; Raffaella Ravinetto, Institute of Tropical Medicine Antwerp, 168
Belgium; Shunmay Yeung, London School of Hygiene and Tropical Medicine, United 169
Kingdom. 170
171
Working document QAS/14.590
page 7
GLOSSARY OF TERMS AND ABBREVIATIONS 172
173
ACT artemisinin-based combination therapy 174
API active pharmaceutical ingredient 175
AQ antimalarial quality 176
BP British Pharmacopoeia 177
CODFIN Counterfeit Drug Forensic Investigation Network 178
FDC fixed-dose combination 179
GDP good distribution practices 180
GMP good manufacturing practices 181
INN International Nonproprietary Name 182
INTERPOL International Criminal Police Organization 183
LIC/MIC low- and middle-income countries 184
LQAS lot quality assurance sampling 185
MEDQUARG Medicine Quality Assessment Reporting Guidelines 186
NDRA national drug regulatory authority 187
NGO nongovernmental organization 188
OOS out-of-specification products 189
Ph.Int. The International Pharmacopoeia 190
QAMSA Survey of the Quality of Selected Antimalarial Medicines 191
QCL quality control laboratory 192
REC Research Ethics Committee 193
SSFFC substandard/spurious/falsely-labelled/falsified/counterfeit medical 194
products 195
UNODC United Nations Office on Drugs and Crime 196
USP United States Pharmacopeia 197
WHO World Health Organization 198
WWARN WorldWide Antimalarial Resistance Network 199
200
Working document QAS/14.590
page 8
EXECUTIVE SUMMARY 201
202
The quality of medicines and medical products has been a neglected factor in global attempts 203
to improve access to effective health care. Data on the quality of medicines, if properly 204
collected, interpreted and used, have much to contribute to improving the effectiveness of 205
interventions to improve the quality of medicines and medical products and advocacy for their 206
importance. The different methods by which data on the quality of medicines and medical 207
devices can be collected, and their potential pitfalls and advantages, are not yet common 208
knowledge among public health scientists, officials and pharmacy inspectors. 209
These guidelines set out the necessary steps to conduct medicine quality surveys with 210
discussion of statistically valid sampling methodologies, the different options to measure poor 211
quality medicine frequency and suggestions on how to assess and interpret the data obtained. 212
This report also discusses the advantages and disadvantages of each of the potential sampling 213
techniques and the ethical challenges to survey teams when collecting medicines in the field. 214
Accurate estimates of the frequency of poor-quality medicines in the market are urgently 215
needed as a requirement for valid comparisons between countries and regions and to measure 216
the impact of interventions. Convenience sampling is important and useful for detecting poor-217
quality medicines but cannot be used to give accurate estimates of frequency, for which some 218
form of random sampling is required. Transparent and consistent reporting can provide robust 219
evidence to assist in improving medicine quality by informing interventions. 220
221
INTRODUCTION AND BACKGROUND 222
223
In the last decade many studies have highlighted the public health impact of poor-quality 224
medicines and medical products, especially in low- and middle-income countries (LIC/MIC). 225
Poor-quality medicines, both falsified and substandard, of the majority of commonly used 226
medicines have recently been described (1–9). However, it is not a new problem with, for 227
example, reports of falsified Cinchona bark in the 1600s (10) and falsified quinine in the 228
1800s (11-13). Deaths from adulterated sulphonamide medicines in the United states of 229
America (USA) in the 1930s were responsible for the strengthening of the Food and Drug 230
Administration (14). Recent reports include falsified meningitis vaccines in Niger, where 231
Working document QAS/14.590
page 9
60 000 inoculated people were unprotected (15) and poor-quality paracetamol syrups 232
containing the antifreeze diethylene glycol, resulting in hundreds of children suffering kidney 233
failure and death in south Asia, central America and Africa (16). Such problems continue, for 234
example, in 2012, ~125 people died in Pakistan, after taking isosorbide mononitrate that 235
contained toxic amounts of the antimalarial drug pyrimethamine (17) and fakes of the 236
anticancer drug bevacizumab (Avastin) circulating in ~22 US states (18). Deliberate 237
falsification of medicines is widespread, but poor manufacturing and insufficient regulation, 238
without deliberate attempt to deceive, are linked to poor-quality substandard medicines 239
entering the supply chain. These medicines may go unnoticed because of lack of acute 240
toxicity or obvious treatment failure but they can still cause avoidable morbidity and mortality 241
as they often contain subtherapeutic amounts of active pharmaceutical ingredients (APIs). 242
Despite having been a significant long-standing public health problem, the quality of global 243
medicine supply has received remarkably little attention. Much effort and finance have been 244
expended on trying to optimize the treatment of diseases and improving access, but such 245
investment is lost if the medicines patients take are of poor quality. Medicines are 246
fundamental to strategies for effective reduction of mortality and morbidity and good quality 247
is essential for ensuring their efficacy and safety. Therefore, quality assurance and quality 248
control of medicines throughout the manufacturing and distribution system, from 249
manufacturing of pharmaceutical ingredients to medicines use by patients, is essential to 250
ensure optimal treatment. Unfortunately, according to the World Health Organization (WHO) 251
30% of the world´s national drug regulatory authorities (NDRAs) do not have functional 252
capacity (19) and in low-income countries (LICs) the NDRAs often lack sufficient financial 253
and human resources to carry out such controls in a stringent and comprehensive way. 254
There has been much discussion of the use of the term substandard/spurious/falsely-255
labelled/falsified/counterfeit (SSFFC) medicines in the Member State Mechanism (20, 21). 256
This term conflates medicines that are deliberately and fraudulently mislabelled 257
(spurious/falsely-labelled/falsified/counterfeit) with those that arise from errors and 258
negligence in factory production (substandard). Here we classify poor-quality medicines into 259
two main categories, falsified and substandard, based on earlier WHO definitions (Box 1, 260
WHO definitions). Falsified medicines are made with the intention to deceive patients and 261
health workers and are, by definition, the work of criminals. Public health should be the prime 262
consideration when defining poor-quality medicines and the term falsified has the advantage 263
Working document QAS/14.590
page 10
of being devoid of trademark and intellectual property considerations of the term counterfeit 264
(22, 23). In contrast, substandard drugs are medicines produced by registered manufacturers 265
that do not meet the quality specifications due to error and negligence and not deliberate fraud. 266
However, if the negligence was gross or systematic, depending on the legal system of the 267
country concerned, criminal negligence may – and should – be invoked. In addition, 268
inadequate post-production storage conditions may result in degradation leading to formation 269
of decomposition products and reduced APIs. Both generic and innovative medicines have 270
been falsified or produced as substandard products. 271
Poor-quality medicines have far-reaching consequences ranging from prolonged sickness, 272
treatment failure, side effects, economic hardship and death. In addition, public confidence on 273
medicines, health-care systems and manufacturers may be diminished as a result of using 274
poor-quality medicines, leading to societies suffering major economic losses. Medicines with 275
sub-therapeutic amounts of active ingredients may contribute to drug resistance hampering 276
disease control and harming patients (4). 277
278
Although there is evidence that a significant proportion of medicines consumed, especially in 279
LIC/middle-income countries (MICs), are of poor quality (4, 8, 24), the quality of the data 280
describing the epidemiology of poor-quality medicines is poor (9), in part because of diverse, 281
unstandardized methodologies followed when collecting medicines in the supply chain. 282
Accurate estimates of the prevalence of poor-quality medicines are sparse, making 283
comparison of the results through space and time very difficult, impeding evidence-based 284
policy decisions and evaluations. There are also very few data on the geographical 285
distribution of poor-quality medicines in relation to population density, borders, disease 286
epidemiology, public versus private health facilities, trade routes and socioeconomic status 287
(25). 288
289
There has been little discussion on the most appropriate sampling and reporting strategies (25, 290
26), in contrast to much progress in other branches of medical science (27). The majority of 291
objective evidence on medicine quality derives from surveys of antimalarial medicines. 292
However, we hope that this discussion will inform surveys to determine the quality of other 293
classes of essential medicines. 294
295
Working document QAS/14.590
page 11
Surveys providing information on the quality of medicines have been conducted by different 296
NDRAs, research groups, international organizations and nongovernmental organizations 297
(NGOs) (28–35). They are helpful to give us snapshots of the medicine quality situation but 298
have important limitations. The accuracy, reliability and generalizability of the data obtained 299
will depend on study design and especially whether the medicine collectors, consciously or 300
subconsciously, prefer to find (e.g. if it might result in a publication or additional funding), or 301
not find, poor-quality medicines (e.g. if it might cause embarrassment, panic, danger, or is 302
part of a larger criminal, political or economic agenda). Such factors may result in 303
underestimating or overestimating the frequency of outlets selling poor-quality medicines and 304
surveys may especially be prone to bias if inspectors are known by pharmacists or other 305
sellers. Adequate systems for management and supervision of field personnel are necessary 306
for data collection, which may not be available in rural areas. Funding is another limitation, 307
restricting the number of samples to be collected in the field, the techniques to be used for 308
analysis or the number of staff available to conduct the survey and analysis. The restriction of 309
the techniques to be used for analysis may further put the accuracy of the results at stake and 310
may result in overlooking important quality problems, e.g. poor bioavailability, presence of 311
impurities, cross-contamination or inter-batch variability. Furthermore, publication and 312
dissemination of the results appears to be relatively difficult despite its obvious and 313
immediate relevance to public health. 314
A summary of the necessary steps to conduct quality surveys is presented in this document, 315
with discussion of different statistically valid sampling techniques for market surveillance. 316
We discuss their advantages and disadvantages, how they can be performed and give 317
examples and standard operating procedures (SOPs) that can be adapted. Accurate estimates 318
of the frequency of poor-quality medicines in the market are urgently needed as a requirement 319
for valid comparisons between countries and regions and to understand time trends and the 320
efficacy of interventions. Transparent and consistent reporting will provide robust evidence to 321
assist in improving medicine quality by informing interventions. As highlighted in this report 322
there remain some uncertainties as to the correct techniques and more research is urgently 323
needed to inform optimum methodology. 324
325
326
Working document QAS/14.590
page 12
Box 1. WHO definition of medicine quality 327
(N.B. Consistent with a trend over the last two years we use the term falsified and not 328
counterfeit) 329
• Counterfeit medicines “A counterfeit medicine is one which is deliberately and fraudulently 330
mislabelled with respect to identity and/or source. Counterfeiting can apply to both branded 331
and generic products and counterfeit products may include products with the correct 332
ingredients, wrong ingredients, without active ingredients, with insufficient quantity of active 333
ingredient or with fake packaging.” 334
• Substandard medicines “Substandard medicines (also called out-of-specification (OOS) 335
products) are genuine medicines produced by manufacturers authorized by the NDRA which 336
do not meet quality specifications set for them by national standards. Normally each medicine 337
that a manufacturer produces has to comply with quality standards and specifications. These 338
are reviewed and assessed by the NMRA before the product is authorized for marketing.” 339
World Health Organization (2009) What are substandard medicines? Available at: 340
http://www.who.int/medicines/services/counterfeit/faqs/06/en/index.html 341
342
Working document QAS/14.590
page 13
INITIAL PLANNING 343
344
When it has been decided that more needs to be known about the quality of essential 345
medicines in a region (whether country, group of countries or area or community within a 346
country) the following should be considered. 347
348
5.1 What is already known about medicine quality? 349
350
Data on medicine quality are scattered and rarely available at one source. A list of sources and 351
websites of different organizations working on medicine quality is given in Annex 1. In 352
addition to searches in PubMed and Google Scholar, key sources are: 353
- WHO (http://www.who.int/medicines/services/counterfeit/en/index.html) 354
- USP MQDB database (http://www.usp.org/around-world/pqm-uspusaid/medicines-355
quality-database-mqdb) 356
- WWARN AQ Surveyor for antimalarials 357
(http://www.wwarn.org/resistance/surveyors/antimalarial-quality) 358
- ReMed (http://www.remed.org/) 359
- QUAMED (http://www.quamed.org/en/home.aspx) 360
- NDRAs and regional groupings of NDRAs (such as EU that may hold unpublished 361
data, http://ec.europa.eu/health/human-use/falsified_medicines/index_en.htm) 362
363
These data, along with any alerts of medicine quality or pharmacovigilance reports, will assist 364
deciding which medicines should be investigated. For much of the world and for most 365
medicines, there is very little information in the public domain and for these 366
regions/medicines discussions with pharmacists and NDRAs and those involved in treating 367
major public health problems may help prioritize surveys. 368
369
5.2 What registered and unregistered medicines are available in the survey area? 370
371
Working document QAS/14.590
page 14
Attempts should be made to obtain lists of registered medicines from the ministry of health 372
and NDRA in a particular country. A medicine is registered in the NDRA when it meets the 373
required standards of quality, safety and efficacy in product specific premarketing 374
assessments (good manufacturing practices (GMP) inspection and product’s dossier 375
assessment). However, in many countries this information can be hard to access. It can be 376
much harder to obtain lists of unregistered medicines as by definition these should not be 377
present. As these are outside the NDRA regulated system they may contain a higher 378
frequency of poor-quality medicines – hence it is vital to consider including them in the 379
survey. Information about unregistered medicines may be obtained from previous surveys 380
conducted in the same area of the study or during the survey. 381
382
5.3 What is the distribution system or supply chain of the medicines? 383
384
The supply chain of a pharmaceutical product is the system of organizations, activities and 385
resources involved in moving a medicine from manufacturers of raw materials, including the 386
API, to patients. A supply chain of one product can consist of multiple manufacturing sites, 387
market warehouses, distribution centres, national or international wholesalers, retailers and 388
public and private outlets. 389
In order to have a good market surveillance system in place it is important to understand how 390
medicines are supplied within the country of study and how they reach patients. There is little 391
information in the public domain about how distribution systems vary between countries (36, 392
37). For antimalarials the ACTWatch reports are an important source of information 393
(http://www.actwatch.info/) and have demonstrated great diversity in the distribution chains 394
between countries. 395
396
Working document QAS/14.590
page 15
5.4 Maps of pharmaceutical outlets 397
398
Pharmaceutical outlets, licensed and unlicensed, are defined as any point of sale or provision 399
of medicines for individual patients or other medicine providers. They are often the first 400
points of treatment seeking in LIC/MICs. 401
NDRAs, ministries of health, provincial health departments and health centres may be able to 402
provide lists of outlets of the area of study that will facilitate the planning of the survey. In 403
addition, international organizations such as ACTwatch (http://www.actwatch.info/) and 404
Population Services International (PSI) (http://www.psi.org/) are mapping and identifying the 405
exact location of health facilities, private clinics and pharmacies in many countries. For 406
example, the Thai Pharmaceutical System Research & Development Foundation (PhaRed) 407
(http://www.phared.org/home/index.php?lang=en) also has internet maps of pharmacies in 408
Thailand. The collection of medicines from unlicensed outlets may be linked to a preceding 409
shop census or household survey, especially when information on treatment-seeking 410
behaviour is investigated. 411
412
5.5 Information on health-seeking behaviour for the target pharmaceuticals? 413
414
In many countries the medicine market is heavily segmented with different markets for people 415
of different spending power and ethnicity. For example, the wealthier people may go to 416
pharmacies or private clinics, whilst the poorest go to grocery shops or street peddlers and 417
people of middle income may go to hospitals. There will also be brands of the same product at 418
different prices aimed at different market segments. It is therefore fundamental for the 419
accuracy and generalizability of the survey to understand where different categories of 420
patients tend to buy their medicines and what kind of product they buy. 421
Bearing the above information in mind, the key decision to inform the methodology of the 422
study is the main objective or question being asked. 423
424
OBJECTIVES 425
426

Working document QAS/14.590
page 16
It is essential to set detailed objectives at the start of planning because all the activities and 427
requirements for the survey are derived from the objectives. Clearly defined objectives are 428
essential for setting up conditions for sampling and testing, which are reflected in the protocol 429
of the survey. 430
431
In order to make clear objectives the question(s) to be addressed in the survey should be 432
clearly formulated. Examples of common questions that are asked are given below. 433
434
1.1 Are there poor quality drugs in this area, border checkpoint, etc.? 435
436
For example, one may be concerned that there may be a quality problem with medicine x in 437
area y or medicine x being imported through checkpoint y. This is both the simplest and most 438
complicated question to answer. Simple, because one could visit a variety of outlets or inspect 439
a variety of shipments looking for poor-quality medicines based on local intelligence or 440
“hunches”. Complicated, because it is difficult to interpret the results – if one finds a poor-441
quality medicine, is it common or rare and if one does not find a poor-quality medicine, is this 442
because one did not look in the correct place or at a sufficient number of samples? 443
444
However, such an approach is vital for NDRAs in order to take enforcement action against 445
falsified and substandard medicines, for alerting the public and pharmaceutical industry and 446
for prompting surveys. They are analogous to pharmacovigilance case reports of new adverse 447
effects of medicines. 448
449

Working document QAS/14.590
page 17
1.2 What are the proportion of poor-quality medicines being sold and/or proportion of 450
outlets selling poor-quality medicines in a particular geographical area? 451
452
For example, an alert may have been received from a customer or from the above Objective 453
(6.1) but the investigators would like to know how common these poor quality “medicines” 454
are. There are two main approaches – convenience and random surveys. In the convenience 455
sampling approach, samples are collected without specific guidance as to which outlets to 456
sample. Results are dependent on the collector´s choices, which are predisposed to bias and 457
cannot be associated with confidence intervals. In contrast, random sampling of sufficient 458
power is a more objective approach that provides accurate estimates of poor-quality 459
medicines or the proportion of outlets selling them in the study area, and confidence intervals 460
of this estimate. Random sampling requires larger sample sizes, greater complexity and hence 461
higher survey costs but should be the preferred methodology if resources allow. 462
When investigating the proportion of poor-quality medicines sold to patients, outlet sale 463
volumes should be considered to provide an accurate estimate of the prevalence. 464
465
1.3 Do the proportion of poor quality medicines or the proportion of outlets selling 466
poor-quality medicines exceed a predetermined level? 467
468
A major problem of conducting random surveys is their complexity and expense with large 469
sample sizes required. An alternative, simpler and less expensive approach, needing smaller 470
sample sizes than formal random sampling, uses lot quality assurance sampling (LQAS). 471
LQAS methodology is useful to determine whether a lot of goods meet desired predefined 472
specifications without having to inspect the entire lot. This cannot give an accurate estimate 473
of the prevalence of poor-quality medicines or outlets selling falsified medicines, but will 474
allow determination as to whether the proportion is below a certain percentage, e.g. 10%, in 475
the area sampled. 476
477

Working document QAS/14.590
page 18
1.4 Has medicine quality changed for the better or worse in an area or for a medicine 478
or medicine group? 479
480
Repeated random surveys and prospective sentinel monitoring sites may be able to estimate 481
changes in medicine quality through time and evaluate the impact of interventions. However, 482
such prospective studies require that the sampling design is consistent through time. Sentinel 483
surveys using the same sites every time, suffer the disadvantage that outlet staff and their 484
distributors may become aware of the survey being conducted and change their behaviour 485
accordingly. This is particularly important when inspectors are known by the pharmacists or 486
outlet providers. Convenience sampling cannot be used to answer this specific question as 487
results are not statistically comparable through space and time. 488
Other related questions include: 489
- what are the supply chains by which poor-quality medicines are distributed and the 490
market segments they serve? 491
- How does the proportion of poor-quality medicines vary at different levels of the 492
regulated and informal distribution chains? 493
- How does the proportion of poor-quality medicines vary by medicines produced 494
within country versus those imported from different countries? 495
- How does the proportion of poor-quality medicines vary by registered and non-496
registered products? 497
498
The detailed objectives for a quality survey should be formulated in a way which makes 499
possible to identify the following. 500
501
1.5 Areas to be sampled 502
503
Samples should not usually be collected only in the capital city as situations in rural and 504
suburban areas often differ. Different geographical areas should be sampled unless the survey 505
expressly justifiably targets one area. A distinction can be made between rural and urban 506
outlets but with the definitions of these two categories clearly stated. 507

Working document QAS/14.590
page 19
Medicines can also be collected in an area where the population is at risk of a disease (38). 508
Locations can be classified by variables such as incidence/prevalence of the disease for which 509
the medicines are produced for, or by population density or by degree of urbanization. For 510
example, malaria is endemic in Thailand only at international borders and antimalarials 511
should be collected in these targeted areas. 512
In the design of a survey with any sampling method it is assumed that the 513
prevalence/incidence of a disease/income level or other risk factors are homogenous across 514
the geographical area to be studied. Small surveys focused on particular areas using the same 515
methodology will obtain comparable results. 516
517
For example, the areas to be sampled in a survey can be stratified by: 518
- income level of the population to be sampled; 519
- areas within countries at high risk of the disease for which the target medication is 520
indicated; 521
- areas within countries at high risk of poor-quality medicines; 522
- rural or urban areas or stratified by this variable; 523
- areas stratified by different distribution systems; 524
- countries or groups of countries. Sampling a diversity of countries in a region, 525
according to the same survey protocol, gives broader pictures of quality of medicines 526
in the region and enables comparisons between countries, but tend to be very 527
expensive, difficult to manage and unlikely to be representative of the situation. 528
529
530
Countries with political instability may not allow the team to sample some areas and study 531
sponsors may disallow such research on safety grounds. 532
533

Working document QAS/14.590
page 20
1.6 Products to be surveyed 534
535
Public-health considerations and the potential public-health impact of different poor-quality 536
medicines should be key guides for which medicines to sample. In resource-poor settings 537
medicines sampled should be on the country’s essential medicine list or for key public-health 538
problems. The dosage form and strengths to be sampled should be prioritized using evidence 539
as to what patients frequently use, e.g. if patients overwhelmingly use doxycycline capsules 540
these should be prioritized rather than doxycycline tablets. The number of dosage units or 541
multidose packages of selected medicines to be collected should be agreed in advance to 542
allow: 543
- conducting the planned tests; 544
- confirmatory testing for those found to OOS; 545
- retention samples; 546
- forensic analysis if evidence of falsification is obtained. 547
548
It is reasonable to formulate the objectives and organize the survey in a way to focus on 549
medicines: 550
- for which inferior quality has documented actual or potential serious implications for 551
the health of patients, such as treatment failures; 552
- used in large volumes; 553
- susceptible to quality deterioration (unstable active ingredients, liquid dosage forms); 554
- for which quality problems have been described and more information on frequency, 555
distribution and time trends are required; 556
- for which resistance issues are pertinent. 557
558
As outlets may have more than one brand of a particular medicine available decisions should 559
be made before sampling as to which to request and, if a selection has to be made, this should 560
be done by random selection to avoid bias from seller or investigator. Mystery shoppers 561
requesting a very specific brand or product may alert sellers of the survey being conducted 562
and this should be taken into consideration. However, such an approach may be required if 563
evidence suggests that only one brand of an essential medicine is afflicted by falsification or 564
substandard production. If the objectives of the survey require a wide picture of the quality of 565

Working document QAS/14.590
page 21
medicines available on the market, samples produced by as many manufacturers as possible 566
should be collected. However, in order to collect samples from more manufacturers it may be 567
necessary to visit more sampling sites. 568
In general, not more than five different types of products (identified by active ingredient/s and 569
dosage form) should usually be included in one survey; otherwise the project would be 570
difficult to manage, unless the study is sufficiently funded and staffed to allow a larger 571
number of types of product. The number of different types of products to be collected should 572
also be a function of the number of different brands that can be expected, which might inflate 573
the number of samples to be tested (less diversity would be expected in public-health facilities 574
than in the private sector). 575
Collectors should be mindful of the stock of sampled products in outlets, and potential 576
difficulties of replenishment of sampled medicines through the supply chain, so as not to 577
jeopardize the availability of these medicines to patients. If there is risk of product shortage 578
after sampling replacement of the sampled amount should be arranged, immediately after the 579
survey, or, less desirably, collection of that particular product in that outlet omitted. 580
Different categories of products to be surveyed may include: 581
- by active ingredients (e.g. artemisinin-based combination therapy (ACTs), sulfadoxine/ 582
pyrimethamine); 583
- by classification of medicines into therapeutic groups; 584
- by formulation for the same drug (e.g. combination therapy sold in loose formulation, 585
blister pack, fixed dose); 586
- by target groups (e.g. paediatric patients); 587
- by stated manufacturer or distributor; 588
- by specific programme under which they are supplied (e.g. a Global Fund grant, national 589
disease control programme); 590
- as commonly used; 591
- registered vs non-registered medicines. 592
593
Information on commonly used drugs may be derived from household surveys with 594
investigation of treatment-seeking behaviour. Collaborating with other sectors, such as 595
national disease control programmes, may help to identify if such questions have been 596
previously included in other surveys. 597

Working document QAS/14.590
page 22
598
1.7 Medicine preparation type 599
600
Medicine quality surveys have especially focused on the quality of tablets/capsules 601
formulations and there is relatively little information about the quality of intravenous or 602
intramuscular dosage forms, syrups or fixed-dose combination therapies, such as for 603
tuberculosis and HIV. The study of diverse formulations is of great importance as different 604
dosage forms may be used according to the degree of severity of a disease or target groups, 605
such as children. For example, tablets are normally used for the treatment of uncomplicated 606
malaria whilst severe malaria is treated with parenteral formulations. There are very few data 607
on the quality of parenteral antimalarial formulations despite their extreme importance in the 608
treatment of severe malaria (9). 609
610
The dosage form of the medicines to be collected in a survey should be clearly specified in the 611
study plan. It is important to ensure that laboratory procedures for the different dosage forms 612
are available, especially for syrups, etc., which may be difficult to analyse. In addition, some 613
parenteral formulations and vaccines may require temperature-controlled storage and 614
transport conditions after collection. 615
616
1.8 Timing of the survey 617
618
It is important to take into consideration when the samples will be collected. There is no 619
information on seasonal changes in frequency of poor-quality medicines, but these may occur. 620
For example, it is possible that falsified antimalarials are more common during the malaria 621
season. Access to outlets in rural areas may be impaired in the rainy season due to factors 622
such as floods and landslides. 623
624
1.9 Types of sample collection sites 625
626
Outlets vary greatly in type both within and between countries, and may be classified by 627
NDRAs according to the countries’ medicine regulatory laws and by their mobility, number 628
Working document QAS/14.590
page 23
and training of staff. To allow comparison between regions/countries with different outlet 629
classification terminologies, outlets could be classed as suggested in the Methodology section, 630
point 8.1, Terminology. 631
Samples collected close to the point of sale to patients in the supply chain (see section 5.3) 632
may be influenced by distribution and storage conditions, such as high temperatures and being 633
sold past expiry date. However, these will be closest in terms of quality to the medicines that 634
patients actually take. There is remarkably little information on degradation of medicines in 635
supply chains of variable quality in terms of good pharmaceutical practices (GPP) (39). If 636
medicine quality problems suggestive of degradation are found in the distal parts of supply 637
chains, collection of additional samples of the same product at higher levels of the chain, e.g. 638
in central wholesalers and medical stores, may help shed light on the importance of poor 639
supply chain management. 640
641
Sampling may be performed at the most proximal parts of the distribution chain such as at 642
manufacturers, wholesalers, importers and central medical stores. There is great diversity in 643
the structure and function of such supply chains between and within countries and 644
understanding of this will be vital in planning surveys (36). Samples collected at proximal 645
points of entry to the market should be less affected by the environment they encounter in 646
distribution and storage, but are relatively removed from the actual quality of medicines that 647
patients will have access to and take. Sampling at this point of the supply chain has the 648
advantage of detecting quality issues before the products reach patients and corrective actions 649
may be more easily put in place if the results are quickly available. The sampling process in 650
countries where there are only a few distributors from which all outlets obtain medicines will 651
be very different from the process in countries with multiple independent distributors selling 652
directly to small outlets. 653
Lists of the locations of the target outlets, e.g. licensed and/or unlicensed outlets, in the 654
selected geographically defined areas are required. It may not be possible to map the “territory” 655
of itinerant medicine sellers but an estimate of what proportion of the total number of sellers 656
are itinerant could be used to generate a sensitivity analysis. Another option would be to 657
include a list of the market places where itinerant vendors are known to buy their medicines. 658
Furthermore, sampling just the public sector outlets for medicine X will be of little use in 659
assessing the public health impact of medicine quality if patients in this community most 660
Working document QAS/14.590
page 24
frequently obtain medicine X from private sector pharmacies or from informal mobile traders 661
(40). Sample collection in public health facilities would mean overt collection in almost all 662
the cases (see section 9). 663
NDRA personnel experienced in national distribution chain structure and function should be 664
asked to advise on sample distribution from the site, transport and storage conditions, 665
especially where quality deterioration could occur. 666
Procurement and treatment outlets in selected areas may be very diverse in terms of 667
regulatory status, size, stock, staffing and level within the distribution chain. The level of 668
sampling within the supply chain will determine the influence of distribution and storage 669
conditions on medicines’ quality which will be more important the more distal in the supply 670
chain is sampled. 671
Different types of collection sites may include: 672
- pharmacy outlets of different categories; 673
- public sector or public-health facilities (national) procurement centres, referral hospitals, 674
health centres or sub-health centres, district hospitals, health posts, community health 675
workers; 676
- private sector: private hospitals, clinics, polyclinics, cabinets, pharmacies; 677
- confessional health facilities or NGOs; 678
- informal providers: drug stores, general retailers, itinerant providers; 679
- wholesalers, at points of entry to the market; 680
- at a specific manufacturer. 681
682
Any type of sampling will suffer from biases especially when inspectors are known by 683
providers, for example, if: 684
- some of the locations to be sampled are not easily accessed by a normal shopper, i.e. 685
collection sites in the public sector, then buying medicines from such locations becomes 686
exceptional and may not be representative of the population; 687
- sampling from wholesalers or points of entry to the market; staff at these facilities may 688
have some knowledge about poor-quality medicines that may lead to bias; 689
- estimating the number of expired medicines in the market may only be possible if 690
medicines are collected using covert sampling methodology (see section 9). 691
Working document QAS/14.590
page 25
692
1.10 Definitions used to determine quality 693
694
Different countries use different definitions for poor-quality medicines, hampering 695
comparison of the results between countries (22, 23, 41). It is important to specify which 696
definitions will be used to determine quality at the start of the survey. 697
698
SURVEY MANAGEMENT AND TIME FRAME 699
700
Ideally each country involved (ministry of health/NDRA) should agree with the survey plans 701
before it commences. Responsibilities and tasks of persons having key roles in survey 702
organization (e.g. survey coordinator, focal persons in individual countries) should be 703
identified at the beginning of the survey and should include those with responsibility for 704
monitoring the conduct of the survey, for performing chemical and packaging analysis, 705
processing results and preparation of the final report. 706
Issues such as the utilization of results and their public availability should be clearly 707
understood by responsible authorities and all the parties involved in the survey from the 708
beginning. A publication plan including authorship of any papers to be submitted for peer-709
reviewed publication and a distribution list of those to whom the report will be disseminated 710
should be agreed at the beginning of the survey. 711
It is vital to organize a meeting with participation of focal persons involved in sample 712
collection to explain and discuss the project, survey protocol and provide detailed instructions. 713
The survey plan with key milestones and organizations/persons responsible for individual 714
parts should be predefined together with an estimated timeframe (Table 1). It is necessary to 715
plan the financial resources expected for the whole survey before beginning. It usually costs 716
more than anticipated! 717
Table 1. Timeframe and responsible officers for the survey (as an example) 718
Activity Timeframe Responsible officers
Selection of geographical area and medicines to
be surveyed
Working document QAS/14.590
page 26
Agreement with authority (ies)
Selection of testing laboratory (ies)
Preparation of testing protocol in agreement with
testing laboratory (ies)
Meeting held with focal points from the targeted
geographical area to discuss the survey protocol
Preparation of detailed national sampling plans
Preparation and pilot test of data collection tools
Training and supervision of personnel
Collection of samples and transport to testing
laboratory (ies)
Sample scanning and logging into databases
Testing of samples
Compilation of results
Data analysis
Report drafting
Meeting held with the participating countries to
discuss the results and the actions needed
Report finalization
Publication and distribution of the results
719
METHODOLOGY 720
721
The main purpose of statistically valid objective sampling is to collect samples of medicines 722
from outlets in various sectors to accurately reflect what consumers use in a given site and/or 723
geographic area (26). Objective sampling is important to draw inferences about the entire 724
"population", whether this refers to the "population of shops" or the "population of patients". 725
It is vital to clearly state the question or aim of the survey/study before designing the 726
methodology (see section 6). It is also critical to maintain the covert nature of the sampling, if 727
that has been decided as the methodology, in order to avoid bias when collecting the 728
medicines in the field. 729

Working document QAS/14.590
page 27
A detailed sampling plan should be prepared prior to the collection of dosage units and it 730
should specify the types of medicines, types of outlets, the area to be covered and who will 731
collect them and how. In order to conduct all the necessary quality assays the number of 732
samples per product to be collected and analysed should be agreed with the quality control 733
laboratory. If possible this should be drafted in cooperation with the respective NDRA(s). The 734
sampling plan will identify: 735
- sampling frame; 736
- sampling unit; 737
- sample size; 738
- outlets; 739
- sample or package; 740
- dosage unit. 741
742
In the following sections the terminology and details of sampling techniques for outlets and 743
sampling techniques for medicines are discussed. For discussion of further methodological 744
considerations not covered in this chapter please refer to Annex 2.4. 745
746
8.1 Terminology 747
748
• Sampling plan: a detailed outline of how many dosage units will be collected from how 749
many medicines, and from what outlets and in which region. Table 3 lists specific 750
elements to be addressed in the sampling plan. 751
752
[Note from the Secretariat: The authors have been contacted regarding the table as to 753
whether it is missing or whether the text refers to Table 6 on page 39.] 754
755
• Sampling frame: the up-to-date list of outlets where the dosage units will be obtained and 756
the set of medicines from which the dosage units are to be collected. The sampling frame 757
should coincide with the “population” of interest. There may be cases where the sampling 758
frame may differ from the actual “population” depending on the objectives of the survey, 759
e.g., if only registered outlets are sampled then unregistered outlets will not be represented. 760
Working document QAS/14.590
page 28
Results from surveys may not be comparable with other studies that sampled a different 761
population of interest. 762
763
• Sampling unit: the sampling units for analysis may be the outlets and/or the medicines 764
sold from them or both. The distinction is important as, for example, an area may have 765
one outlet selling 50% of the poor-quality medicine(s) or 10 outlets each selling 5% of the 766
poor-quality medicines. Weighting may be required based on the number of treatments 767
dispensed per outlet, which could be derived from household surveys or sales volumes 768
declared by the outlets. Surveys have usually estimated the proportion of poor-quality 769
medicines in outlets and not the proportion of shops selling poor-quality medicines. By 770
using the proportion of medicine outlets selling poor-quality essential medicines as the 771
unit of observation and a standardized, randomized sampling procedure of sufficient 772
sample size, it would be possible to map distribution of medicine quality and allow 773
comparisons through time. Such a procedure will require knowledge of the expected 774
underlying prevalence to calculate the sample size. If this knowledge is unavailable the 775
worst-case scenario must be assumed, necessitating larger sample size. Large sampling 776
sizes may alert providers to those procuring for the survey but samples of sufficient size 777
are vital to give reliable results. 778
779
• Sample size: the outlets selected from the sampling frame or the dosage units within the 780
medicines drawn from the population. A minimum sample size of outlets is needed with 781
medicines in stock to provide information of the changes in medicine quality. 782
783
• Outlets: a place where medicines are sold or distributed. Outlets vary greatly in type and 784
can be classed as public (government), registered private for profit (e.g. private 785
pharmacies, supermarkets), private not for profit (e.g. mission hospitals, NGOs) and 786
informal (e.g. kiosks, street vendors, grocery shops). Sampling should usually be 787
performed in both the public and private sectors as well as in the "informal market" (i.e. 788
outside the approved distribution chain), i.e include both licensed and unlicensed outlets. 789
790
• Sample: a sample means an individual medicine (active ingredient/s by International Non-791
Proprietary Names (INNs), dosage form, strength and brand) collected at one outlet. All 792
dosage units (or medicine units) of one sample must be of the same brand and batch – if 793
Working document QAS/14.590
page 29
they are the same medicine brand but from different batches they should be regarded as 794
multiple samples. 795
796
• Dosage unit: a single individual unit of a medicine (e.g. a single tablet or a single package 797
containing powder or a vial of medicine) that is the smallest dosage unit that can be 798
analysed. Dosage units come in diverse forms, including tablets, capsules, oral 799
solutions/suspensions, powder for oral solution/suspension and injections or powders for 800
injections. Tablets and capsules may come packaged in a box and be presented in blister 801
packs (with batch number, manufacturer and expiration date) or in unlabelled plastic 802
(locally repacked) bags coming from large-sized boxes. Vials may also be sold 803
individually sometimes without the appropriate leaflet instructions or paired diluent. 804
Surveys may sample nationally-registered medicines and should help to find the presence 805
of unregistered ones. The number of dosage units per sample to be collected should be 806
specified at the beginning of the survey. 807
808
8.2 Sampling designs (convenience, random, lot quality assurance sampling (LQAS), 809
sentinel) 810
Convenience sampling 811
Convenience surveys, in which samples are collected without specific guidance as to which 812
outlets to sample, have been the predominant techniques used and may provide evidence to 813
support legal action in police and NDRA investigations. As the name implies convenience 814
surveys are simple and relatively inexpensive and do not require complete lists of outlets in 815
defined areas, which may be difficult to obtain, especially for unlicensed or mobile outlets. 816
However, they are inherently prone to biases and are potentially misleading and should only 817
be considered if other sampling methods cannot be implemented. The results of convenience 818
sampling are crucially dependent on the collector’s choice of outlets and any derived 819
prevalence estimates cannot be generalized to other areas, even within the same country. If 820
those conducting sampling were particularly interested in finding poor-quality or quality 821
medicines, this may influence their selection of outlets to sample. Changes in the prevalence 822
of poor-quality medicines, and the outlets selling them, cannot be reliably interpreted over 823
time if obtained from convenience sampling as changes may simply represent sampling 824
artifact. Convenience sampling techniques are now avoided in medical research because of 825
these inherent disadvantages. Nevertheless convenience surveys may provide the initial signal 826
Working document QAS/14.590
page 30
of a pharmaceutical problem (analogous to case reports of adverse effects to a drug) and may 827
be useful during routine post-marketing medicine quality monitoring, particularly when 828
doubts are raised about the quality of a specific medicine in a particular area. Whenever 829
convenience sampling is used, how the sites were identified and the proportion of the outlets 830
this represents should be reported. If convenience sampling does indicate a drug quality 831
problem, more objective methods should be used in subsequent surveys. If convenience 832
surveys do not demonstrate a problem one should bear in mind that this may be a false 833
negative result. It is important to emphasize the limitations of this technique in reports and 834
scientific papers and when discussing with journalists. 835
836
Examples of convenience sampling include surveys conducted in Africa (24, 34, 42) 837
and South-East Asia (28, 43). 838
839
Random sampling 840
Random sampling is an objective technique that, with sufficient sample size, will give reliable 841
estimates of the prevalence of outlets selling poor-quality medicines with confidence intervals. 842
Stratified sampling to adjust for potential differences in income levels of the population of 843
interest or sales size of each location should be considered. It can also include geographical, 844
trade and socioeconomic variables, such as rural versus urban, private versus public outlets 845
and one geographic area versus another. Stratification requires adjustment of the sample size 846
calculation (see Annex 2.4 for more on further statistical issues related to methodology). 847
Sampling proportional to population size (or number of medicine outlets) will be more 848
efficient compared to simple random sampling. It is important that the randomization 849
procedure uses formal random number tables or simple statistical software and not 850
pseudorandom techniques. Comparisons with subsequent estimates using the sampling design 851
should be valid and will allow the evaluation of interventions. The disadvantages of random 852
sampling are the large sample sizes needed and the additional costs in labour and time. In 853
addition, it is important to recognize that a random survey will only produce reliable and 854
useful information if the sampling frame and actual within-outlet sampling is in concordance 855
with the primary aims of the study. For example, a random survey of the quality of medicine 856
in the private sector when most patients obtain this medicine in the public sector would not be 857
useful, nor would a random survey using overt shoppers for a medicine that the outlet staff 858
know they should not be selling. 859

Working document QAS/14.590
page 31
An example of this technique is described in a stratified random sample of the quality of 860
antimalarial medicines in the Lao People’s Democratic Republic (44). The random sampling 861
of medicine outlets was accomplished by the collectors in the field making numbered lists of 862
outlets and telephoning a central location giving the total number of outlets found. The central 863
location staff then used random number tables to tell the field team which outlets to sample. 864
865
Other examples of random surveys are from Nigeria, Uganda and the United Republic of 866
Tanzania (29, 31, 32, 45). 867
868
Lot quality assurance sampling 869
LQAS can be used to determine whether the prevalence of outlets selling poor-quality 870
medicines exceeds a certain threshold and may be a useful methodology to be used in routine 871
surveillance. There has been almost no discussion as to what proportion of outlets selling 872
poor-quality medicines should be regarded as unacceptable (25). Ideally there should be zero-873
tolerance for outlets selling poor-quality medicines, as even a 1% prevalence of such 874
medicines for potentially fatal diseases, such as malaria, tuberculosis and HIV, is disastrous 875
for individual patients. 876
LQAS is designed to allow determination as to whether a batch, or lot, of goods meet desired 877
specifications without having to inspect the entire lot. Thus, the sample size in LQAS is 878
defined as the number of outlets (“goods”) that are selected for each site (“lot”) and the only 879
outcome is that the site is “acceptable” or “unacceptable”. Setting the level of risk taken by 880
not inspecting each and every item enables the investigator to accept or reject an entire lot 881
after inspecting a randomly selected sample of items. Therefore, the sample size in LQAS is 882
based on defined threshhold values that classify good and bad outcomes and the probability of 883
error that the investigators are willing to tolerate. For example, an area in which 10% or more 884
of the outlets sell poor-quality medicines may be considered a “bad” situation since the risk of 885
buying poor-quality medicines will be high, whereas 5% or less may be considered a “good” 886
situation since the risk of buying poor-quality medicines will be lower (25, 46). 887
Acceptable probabilities of error must be specified; the risk of accepting a “bad” lot 888
(“consumer risk”) and the risk of not accepting a “good” lot (“provider risk”). These risks are 889
commonly referred to as Type I (alpha) and Type II (beta) errors, respectively. The former is 890

Working document QAS/14.590
page 32
often set to 0.05. This means that if the null hypothesis (that the site has fewer outlets selling 891
poor-quality medicines than the specified value) is true, there is a 5% chance that a site with 892
an unacceptable proportion of outlets selling poor-quality medicines will be “accepted” or go 893
undetected. In general, Type 1 risk is set lower than the Type 2 risk. 894
Once the threshold values and probabilities of error have been considered a sample size and 895
decision value can be obtained. The decision value is the number of outlets selling poor-896
quality medicines that need to be found before an area is considered unacceptable. LQAS still 897
requires random sampling and has the disadvantage that it does not estimate an exact 898
prevalence but the advantage of requiring smaller sample sizes (see example in Annex 2.1b). 899
Sampling can stop once the number of outlets selling poor-quality medicine is exceeded, 900
greatly reducing sampling time and costs (47). 901
Random-sampling LQAS is probably the most efficient and accurate initial sampling 902
procedure. As LQAS will only provide a binary result formal random sampling will be 903
required to examine longitudinal changes in the prevalence of poor-quality medicines 904
accurately. It can also be useful when the exact prevalence of poor-quality medicines is 905
known as a way to monitor the situation. There is only one published LQAS medicine 906
quality survey (46). More experience is needed so that comparisons of costs and human effort 907
needed against formal random sampling can be made. A LQAS toolkit is available from the 908
Liverpool School of Tropical Medicine (48). Other references for this topic are (49–52). 909
910
Sentinel site monitoring 911
Sentinel site monitoring, in which the quality of medicines in a particular locality is followed 912
through time, is used in many countries (53). There has been no consensus as to whether these 913
sites should be chosen on the basis of potentially important variables such as rural versus 914
urban and private versus public outlets, or using what sampling methodology (i.e. 915
convenience or random samples or LQAS). Although the power of sentinel site monitoring 916
resides in allowing longitudinal changes to be followed in one place, it suffers from the 917
disadvantage that shop owners may soon realize that they are being sampled, change their 918
behaviour accordingly and thus are no longer representative of the population. 919
Each sentinel site should arrange an appropriate schedule that takes into account the logistics 920
and availability of resources (26). 921

Working document QAS/14.590
page 33
For examples of sample size calculation with LQAS and random sampling see Annex 2.1. 922
923
8.3 Number of dosage units to be collected 924
925
A problematic and unresolved issue is the number of dosage units that should be collected. 926
The uniformity of dosage units’ assay measures the individual content of the active ingredient 927
in each capsule or tablet and compares it with the amount of active ingredient claimed on the 928
label of the medicine. 929
Current recommendations from pharmacopoeias 930
- The United States Pharmacopeia (USP) recommends that 30 units of each medicine 931
should be collected. Unless otherwise specified in the individual monograph the 932
requirements for dosage uniformity are met if the amount of API in each of the 10 dosage 933
units as determined from their weight variation or their content uniformity method lies 934
within the range of 85.0% to 115.0% of the label claim and the relative standard deviation 935
is less than or equal to 6.0%. If one unit is outside the range of 85.0% to 115.0% of label 936
claim and no unit is outside the range of 75.0% to 125.0% of label claim, or if the relative 937
standard deviation is greater than 6.0%, or if both conditions prevail, USP recommends 938
testing 20 additional units. The requirements are then met if not more than one unit of the 939
30 is outside the range of 85.0% to 115.0% of label claim and no unit is outside the range 940
of 75.0% to 125.0% of label claim and the relative standard deviation of the 30 dosage 941
units does not exceed 7.8% (54). 942
943
- The procedures of The International Pharmacopoeia (Ph.Int.) (2006) recommend 944
determining the amount of API in each of 10 units using the analytical method specified 945
in the individual monograph. For uniformity of content for single-dose preparations assay 946
the Ph.Int. states: “This test is only to be applied where the declared quantity of active 947
ingredient is 5% or less of the total formulation. For tablets and powders for injection: 948
each single unit should contain within ±15% of the average amount of active ingredient. 949
However if one individual unit deviates by more than ±15% but is within ±25% of the 950
average amount of the active ingredient, examine further 20 units drawn from the same 951
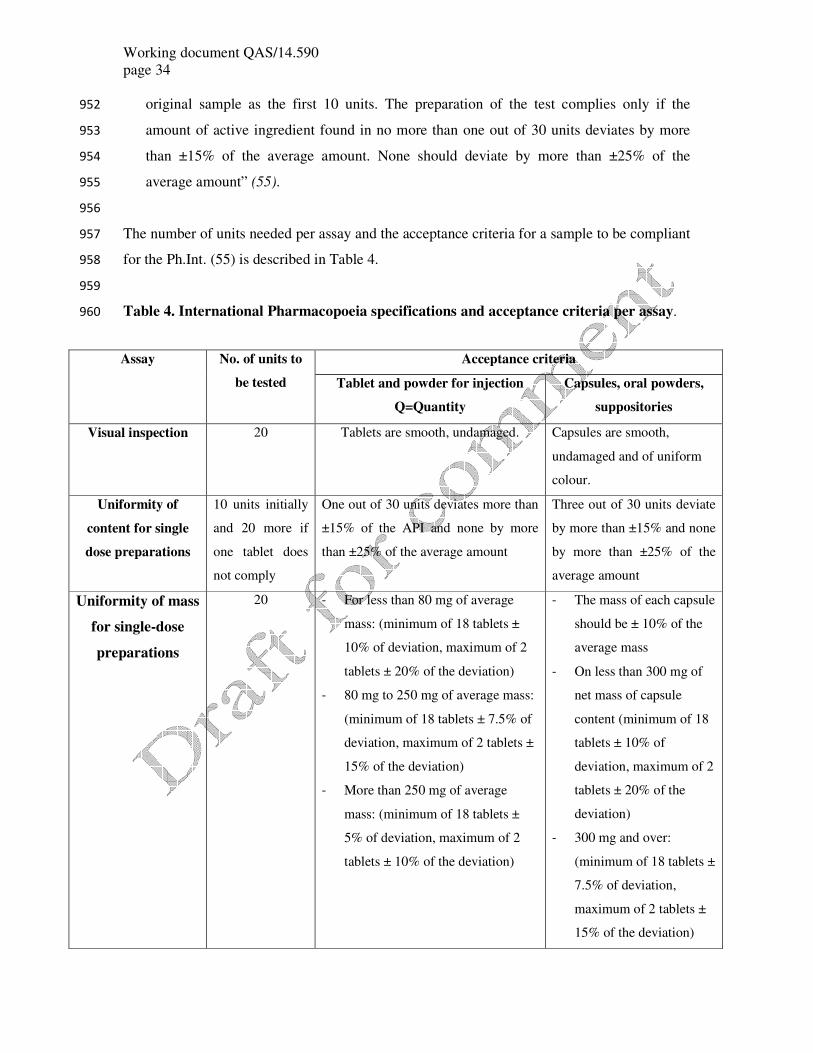
Working document QAS/14.590
page 34
original sample as the first 10 units. The preparation of the test complies only if the 952
amount of active ingredient found in no more than one out of 30 units deviates by more 953
than ±15% of the average amount. None should deviate by more than ±25% of the 954
average amount” (55). 955
956
The number of units needed per assay and the acceptance criteria for a sample to be compliant 957
for the Ph.Int. (55) is described in Table 4. 958
959
Table 4. International Pharmacopoeia specifications and acceptance criteria per assay. 960
Assay No. of units to
be tested
Acceptance criteria
Tablet and powder for injection
Q=Quantity
Capsules, oral powders,
suppositories
Visual inspection 20 Tablets are smooth, undamaged. Capsules are smooth,
undamaged and of uniform
colour.
Uniformity of
content for single
dose preparations
10 units initially
and 20 more if
one tablet does
not comply
One out of 30 units deviates more than
±15% of the API and none by more
than ±25% of the average amount
Three out of 30 units deviate
by more than ±15% and none
by more than ±25% of the
average amount
Uniformity of mass
for single-dose
preparations
20 - For less than 80 mg of average
mass: (minimum of 18 tablets ±
10% of deviation, maximum of 2
tablets ± 20% of the deviation)
- 80 mg to 250 mg of average mass:
(minimum of 18 tablets ± 7.5% of
deviation, maximum of 2 tablets ±
15% of the deviation)
- More than 250 mg of average
mass: (minimum of 18 tablets ±
5% of deviation, maximum of 2
tablets ± 10% of the deviation)
- The mass of each capsule
should be ± 10% of the
average mass
- On less than 300 mg of
net mass of capsule
content (minimum of 18
tablets ± 10% of
deviation, maximum of 2
tablets ± 20% of the
deviation)
- 300 mg and over:
(minimum of 18 tablets ±
7.5% of deviation,
maximum of 2 tablets ±
15% of the deviation)

Working document QAS/14.590
page 35
961
Such a sample sizes gives enough dosage units to determine identity and accurate estimates of 962
content of active ingredients, dissolution and degradation. However, many outlets in the rural 963
tropics do not have 30 dosage units of a particular medicine (25), especially expensive brands, 964
and so a request for such a large quantity is likely to suggest to the outlet owner that the buyer 965
is not an ordinary shopper (56). In addition, outlet staff may dispense units of the same 966
medicine with different batch numbers, expired dates, fewer number of units or in a different 967
container to the original packaging. Ideally unopened packages should be collected. An 968
alternative would be to sample key medicines at the level of the wholesaler where requests for 969
large quantities would be routine. USP guidelines on dosage-unit sampling are designed for 970
analyses that would withstand examination in a court of law, such as would be needed by a 971
NDRA to press legal charges. However, scientific research studies have not included legal 972
chain of custody procedures and hence cannot usually be used as evidence, but may 973
precipitate NDRA legal investigations with appropriate protocols (57). 974
For mystery shopper surveys in which samples failing analysis would prompt NDRA 975
investigations smaller sample size of dosage units may be appropriate. Mystery shoppers 976
could normally collect one or two full treatment courses without raising too much attention 977
from shop keepers. Thirty units for tablet or capsule forms of single drug preparation would 978
allow assessment of identity, content of active ingredients, dissolution and degradation. When 979
fewer units are found (i.e. informal sector) samples with less than 30 units may be included 980
(Table 5). Newly deployed non-destructive techniques such as high throughput mass 981
Disintegration 6 - All six tablets should disintegrate
to pass the test
- All six capsules should
disintegrate to pass the
test
Dissolution 6 units initially
and 18 more if
one unit does not
comply
- 6 tablets tested and each unit is not
less than Q +5%
- Average of 12 units is equal to or
greater than Q and no unit is less
than Q-15%
- Average of 24 units is equal to or
greater than Q; not more than 2
units are less than Q-15%; no unit
is less than Q-25%

Working document QAS/14.590
page 36
spectrometry, Raman and IR spectroscopy can perform assays for identity and active 982
ingredient content, followed by assays for disintegration and dissolution, allowing for smaller 983
sample sizes. 984
The amount of work in collecting and analysing medicine quality surveys is frequently 985
underestimated and discussions of what is realistic given human and financial resources and 986
the intrinsic difficulties of studies (e.g. remote travel, sample transport) are essential. The 987
maximum number of samples to be collected should be set before sample collection starts (see 988
Annex 2.3). If more countries are involved maximum number of samples should be set for 989
each country. 990
The following general rules can be used, if not justified otherwise. 991
992
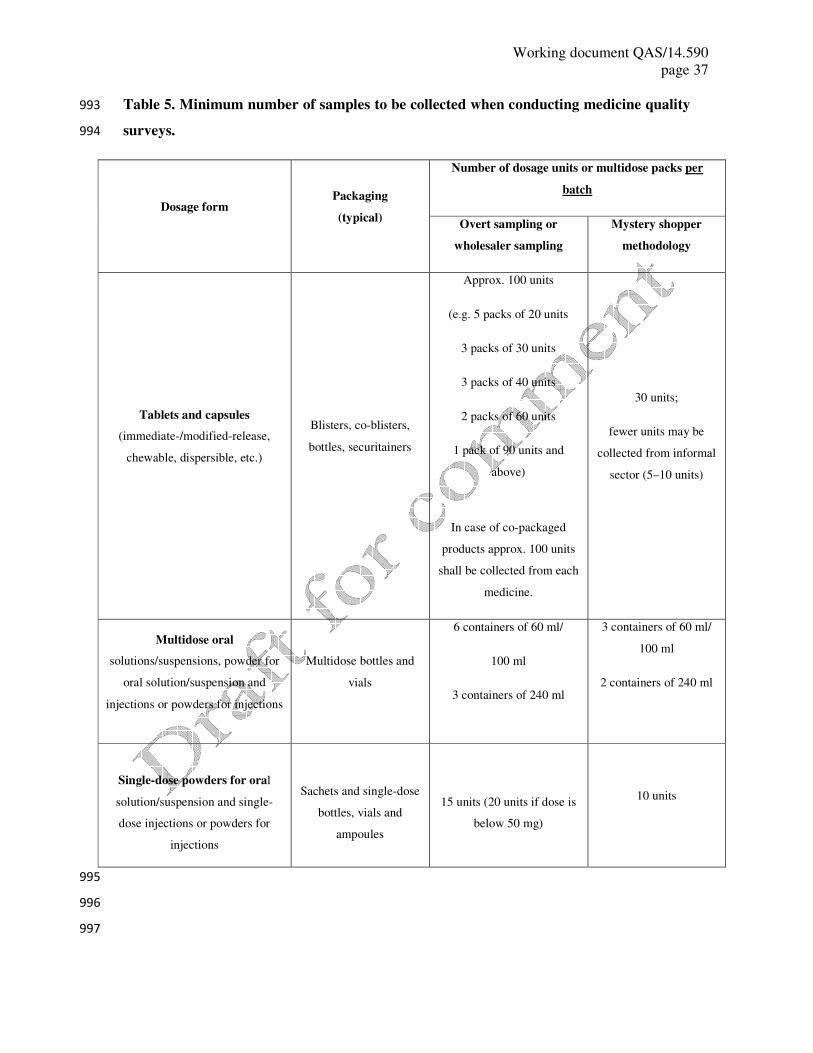
Working document QAS/14.590
page 37
Table 5. Minimum number of samples to be collected when conducting medicine quality 993
surveys. 994
Dosage form Packaging
(typical)
Number of dosage units or multidose packs per
batch
Overt sampling or
wholesaler sampling
Mystery shopper
methodology
Tablets and capsules
(immediate-/modified-release,
chewable, dispersible, etc.)
Blisters, co-blisters,
bottles, securitainers
Approx. 100 units
(e.g. 5 packs of 20 units
3 packs of 30 units
3 packs of 40 units
2 packs of 60 units
1 pack of 90 units and
above)
In case of co-packaged
products approx. 100 units
shall be collected from each
medicine.
30 units;
fewer units may be
collected from informal
sector (5–10 units)
Multidose oral
solutions/suspensions, powder for
oral solution/suspension and
injections or powders for injections
Multidose bottles and
vials
6 containers of 60 ml/
100 ml
3 containers of 240 ml
3 containers of 60 ml/
100 ml
2 containers of 240 ml
Single-dose powders for oral
solution/suspension and single-
dose injections or powders for
injections
Sachets and single-dose
bottles, vials and
ampoules
15 units (20 units if dose is
below 50 mg)
10 units
995
996
997

Working document QAS/14.590
page 38
8.4 Sampling techniques for the dosage units within medicine samples 998
999
How many dosage units within a medicine sample need to be analysed is difficult and 1000
contentious with few data to inform discussions. There is very little evidence on the 1001
interdosage unit % API or dissolution variability within a sample of poor-quality medicines 1002
with only one publication, that we are aware of, that discusses this issue (58). We suggest 1003
that sampling strategies should assume that variability is high but more research is urgently 1004
needed to inform this question. 1005
The aim of sampling dosage units is to estimate the proportion of poor quality drugs in a 1006
specific outlet based on a relatively small subset of units being tested. The outlet is assessed 1007
based on sampling of dosage units from that outlet. Usually the package of units is obtained 1008
and then a number of units from that package are tested and a conclusion is drawn regarding 1009
the package and therefore the outlet. 1010
The assumption behind this approach is that a fixed but unknown proportion of the population 1011
(sampling frame) contains poor-quality drugs. Therefore the proportion of poor-quality units 1012
in a sample (a subset of units from the population) can estimate the proportion of poor-quality 1013
medicines for the whole population. 1014
The actual proportion of poor-quality medicines will vary between samples but is determined 1015
by a discrete probability distribution that can be used to calculate the size of the sample to be 1016
drawn so that meaningful inferences can be made about the whole population. The two 1017
distributions which describe a number of positive (poor-quality) units in a randomly drawn 1018
sample are the binomial and hypergeometric distributions and they are described in more 1019
detail in Annex 2.2 and 2.3. 1020
Other resources describing the representative medicine sampling can be found (59–61). 1021
A national sampling plan is included in Annex 3. 1022
1023
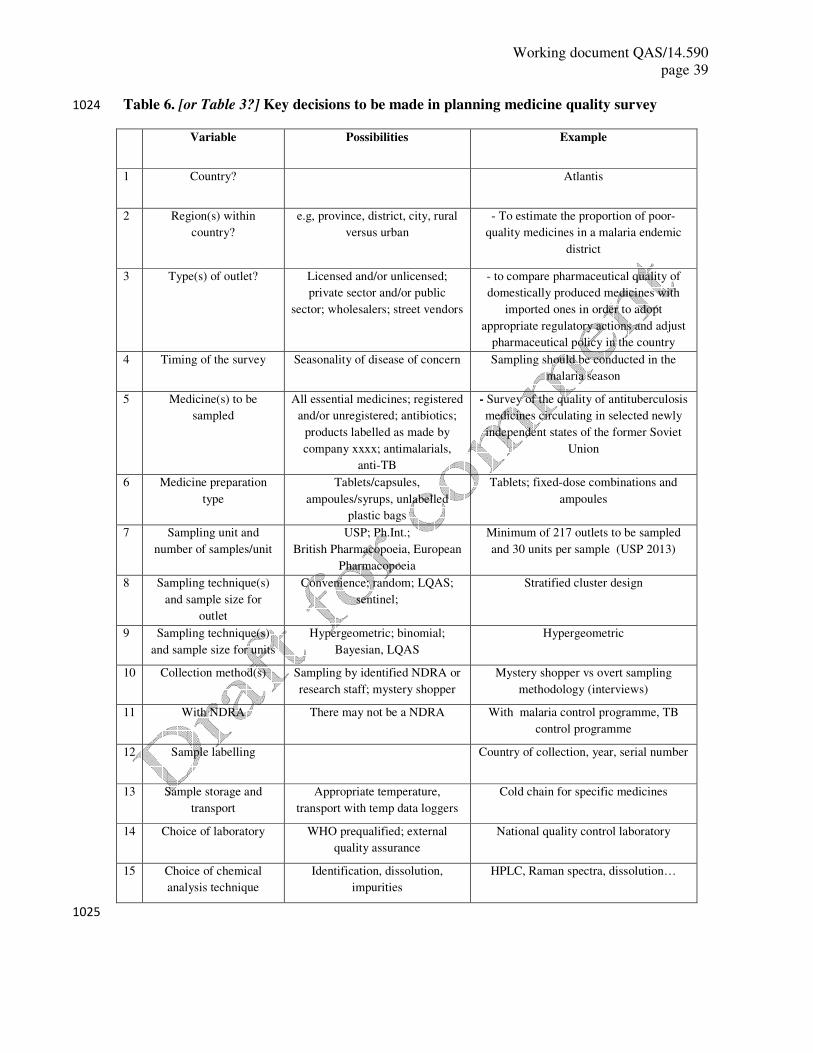
Working document QAS/14.590
page 39
Table 6. [or Table 3?] Key decisions to be made in planning medicine quality survey 1024
Variable Possibilities Example
1 Country? Atlantis
2 Region(s) within
country?
e.g, province, district, city, rural
versus urban
- To estimate the proportion of poor-
quality medicines in a malaria endemic
district
3 Type(s) of outlet? Licensed and/or unlicensed;
private sector and/or public
sector; wholesalers; street vendors
- to compare pharmaceutical quality of
domestically produced medicines with
imported ones in order to adopt
appropriate regulatory actions and adjust
pharmaceutical policy in the country
4 Timing of the survey Seasonality of disease of concern Sampling should be conducted in the
malaria season
5 Medicine(s) to be
sampled
All essential medicines; registered
and/or unregistered; antibiotics;
products labelled as made by
company xxxx; antimalarials,
anti-TB
- Survey of the quality of antituberculosis
medicines circulating in selected newly
independent states of the former Soviet
Union
6 Medicine preparation
type
Tablets/capsules,
ampoules/syrups, unlabelled
plastic bags
Tablets; fixed-dose combinations and
ampoules
7 Sampling unit and
number of samples/unit
USP; Ph.Int.;
British Pharmacopoeia, European
Pharmacopoeia
Minimum of 217 outlets to be sampled
and 30 units per sample (USP 2013)
8 Sampling technique(s)
and sample size for
outlet
Convenience; random; LQAS;
sentinel;
Stratified cluster design
9 Sampling technique(s)
and sample size for units
Hypergeometric; binomial;
Bayesian, LQAS
Hypergeometric
10 Collection method(s) Sampling by identified NDRA or
research staff; mystery shopper
Mystery shopper vs overt sampling
methodology (interviews)
11 With NDRA There may not be a NDRA With malaria control programme, TB
control programme
12 Sample labelling Country of collection, year, serial number
13 Sample storage and
transport
Appropriate temperature,
transport with temp data loggers
Cold chain for specific medicines
14 Choice of laboratory WHO prequalified; external
quality assurance
National quality control laboratory
15 Choice of chemical
analysis technique
Identification, dissolution,
impurities
HPLC, Raman spectra, dissolution…
1025
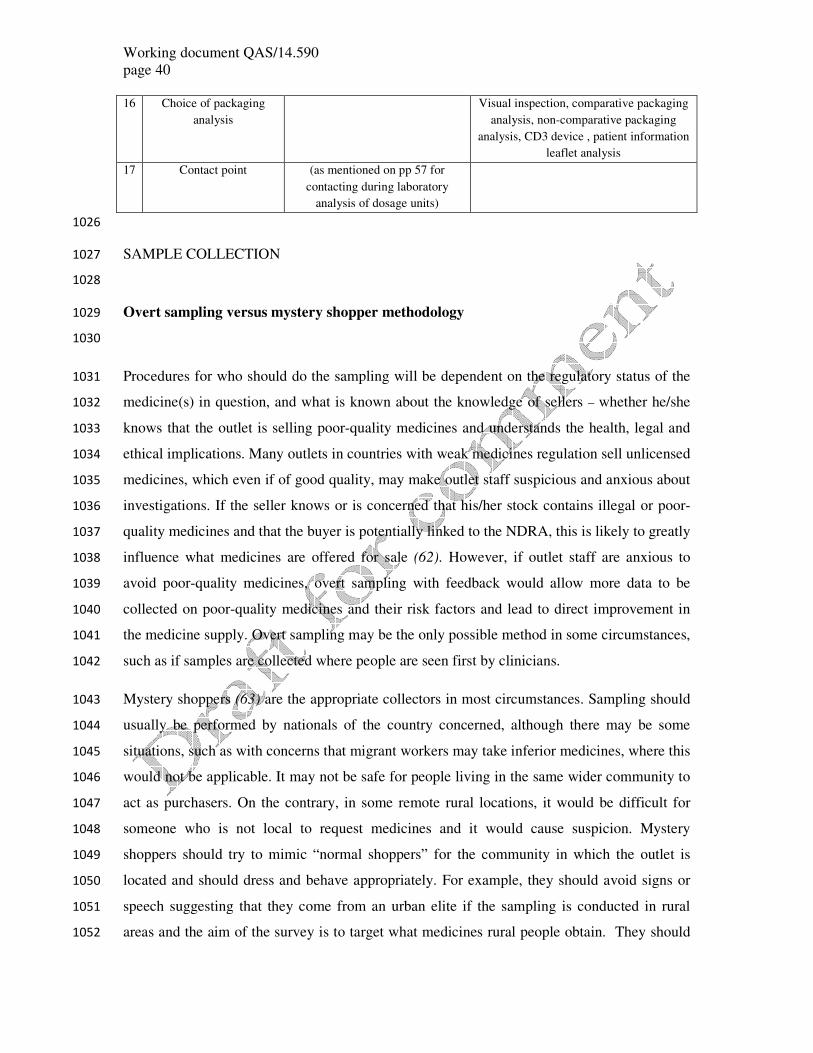
Working document QAS/14.590
page 40
16 Choice of packaging
analysis
Visual inspection, comparative packaging
analysis, non-comparative packaging
analysis, CD3 device , patient information
leaflet analysis
17 Contact point (as mentioned on pp 57 for
contacting during laboratory
analysis of dosage units)
1026
SAMPLE COLLECTION 1027
1028
Overt sampling versus mystery shopper methodology 1029
1030
Procedures for who should do the sampling will be dependent on the regulatory status of the 1031
medicine(s) in question, and what is known about the knowledge of sellers – whether he/she 1032
knows that the outlet is selling poor-quality medicines and understands the health, legal and 1033
ethical implications. Many outlets in countries with weak medicines regulation sell unlicensed 1034
medicines, which even if of good quality, may make outlet staff suspicious and anxious about 1035
investigations. If the seller knows or is concerned that his/her stock contains illegal or poor-1036
quality medicines and that the buyer is potentially linked to the NDRA, this is likely to greatly 1037
influence what medicines are offered for sale (62). However, if outlet staff are anxious to 1038
avoid poor-quality medicines, overt sampling with feedback would allow more data to be 1039
collected on poor-quality medicines and their risk factors and lead to direct improvement in 1040
the medicine supply. Overt sampling may be the only possible method in some circumstances, 1041
such as if samples are collected where people are seen first by clinicians. 1042
Mystery shoppers (63) are the appropriate collectors in most circumstances. Sampling should 1043
usually be performed by nationals of the country concerned, although there may be some 1044
situations, such as with concerns that migrant workers may take inferior medicines, where this 1045
would not be applicable. It may not be safe for people living in the same wider community to 1046
act as purchasers. On the contrary, in some remote rural locations, it would be difficult for 1047
someone who is not local to request medicines and it would cause suspicion. Mystery 1048
shoppers should try to mimic “normal shoppers” for the community in which the outlet is 1049
located and should dress and behave appropriately. For example, they should avoid signs or 1050
speech suggesting that they come from an urban elite if the sampling is conducted in rural 1051
areas and the aim of the survey is to target what medicines rural people obtain. They should 1052

Working document QAS/14.590
page 41
use a standard scenario, stating, for example, that they are visiting from another part of the 1053
country and would like some medicines for disease X for reason Y for a stereotyped patient Z. 1054
If many dosage units of a large number of medicines are requested the seller may become 1055
suspicious and the medicines collected may not reflect what is actually available at those 1056
outlets (62). 1057
An additional concern is that in many resource-poor countries the medicine market is heavily 1058
segmented with different markets for people of different spending power and ethnicity. For 1059
example, the least poor may go to pharmacies or private clinics, whilst the poorest go to 1060
grocery shops or street peddlers and people of middle income may go to hospitals. Even 1061
within a single outlet there will often be several different brands of the same product at 1062
different prices aimed at different market segments with, for example, a “local” brand (least 1063
expensive), a non-local and non-European (middling expensive) and a “Western” brand 1064
(expensive). Therefore, what the mystery shopper will collect may depend partly on how 1065
wealthy the shopkeeper thinks the shopper is. This also emphasizes the importance of 1066
sampling guided by the volume consumed rather than that displayed. Any weighting that 1067
requires sales volumes cannot be done if mystery shoppers are used, unless these are preceded 1068
or followed by an outlet census. Expired drugs may be more likely to be sold to mystery 1069
shoppers than overt buyers. 1070
In overt sampling methodology data should be collected using a structured questionnaire and 1071
the location of each outlet recorded with a hand-held global positioning system (GPS) unit. 1072
The questionnaire should collect data on outlet identification, outlet characteristics such as 1073
their supply chains, provider knowledge, availability of medicines and stock outs. Opinions 1074
and sell-reported practice with regards to medicines or falsified medication should also be 1075
included. A standard reporting form should be used to record details of the medicines such as 1076
collection date and site, cost and type, location and type and size of outlet (Annex 4). 1077
Data collection tools should be translated in the language of the collectors, back-translated to 1078
English, piloted and revised before implementing the final version. 1079
If the samples are collected through the mystery shopper methodology, the interaction 1080
between the mystery shopper and outlet staff should be documented on a debriefing form. 1081
When the mystery shopper returns from each outlet the study coordinator should perform a 1082
debriefing and transcribe the reported interaction with translation as appropriate. Translations 1083
should use a meaning-based translation method rather than a literal or interpretative approach. 1084

Working document QAS/14.590
page 42
The original text will remain in the document with the translation made beneath each section. 1085
Sections of text will be double-checked for accuracy of translation by other members of the 1086
field team. This part of the work may need to be conducted in collaboration with social 1087
scientists. 1088
Standard operating procedures (SOP) documents should be created for the methodology 1089
followed. An example of the SOPs for overt sampling and mystery shopper methodology can 1090
be found in Annex 5 and Annex 6, respectively. 1091
Examples of overt sampling include (35) and examples of mystery-shopper methodology 1092
include (44). 1093
1094
Survey team and procedures for collection 1095
1096
Ideally the survey team should be composed of a survey coordinator, inspectors or staff 1097
trained for collection of medicines, assistants and, if necessary, a driver. Cooperation with the 1098
WHO country office staff in the respective country may be useful. The focal person for each 1099
country will arrange for training of collectors to be familiar with the project, survey protocol, 1100
national sampling plan and instructions for collection of samples. Staff from the NDRA and 1101
the different national control programmes, such as the malaria or tuberculosis control 1102
programmes, may provide a useful insight into the survey planning. However, if the NDRA is 1103
highly politicized involving them may bias the entire process, since they may not accept a 1104
“bad” result from any sampling. 1105
The following specifications for sample collection should be included/adhered to: 1106
- the number of units per sample and number of batches to be collected from each 1107
collection site for each selected medicine as indicated in the sampling plan; 1108
- there should not be a mixed batch collection per sample; all units of one sample must 1109
be of the same batch number; 1110
- the medicine samples should not be taken out of the original primary packaging and 1111
outer containers (though removal from large secondary packs is appropriate). 1112
Containers such as bottles and vials should not be opened; 1113
Working document QAS/14.590
page 43
- samples collected should have at least six months remaining to expiry to allow time 1114
for chemical analysis; 1115
- the medicine labels and package leaflets should not be removed or damaged; 1116
- individual samples should be recorded using the sample collection form for each 1117
sample (example in Annex 4). Whenever the required information is not available it 1118
should be indicated in the appropriate space on the sample collection form, where any 1119
abnormalities should also be recorded; 1120
- each sample will be identified by a unique sample code, defined on the sample 1121
collection form template and specified on all the original packages belonging to the 1122
respective sample. The sample collection form and all packages belonging to one 1123
sample will be kept together (e.g. blisters inserted in a dedicated zip log plastic bag 1124
marked with the appropriate sample code and trade name of the product); 1125
- manufacturer’s batch certificates of analysis will be collected with samples, if 1126
available, and kept with the sample collection form; 1127
- the samples should be collected and kept under controlled conditions. Samples should 1128
be stored in in zip lock plastic bags labelled with their unique identification codes 1129
marked with permanent markers. For large surveys bar-code systems would be very 1130
helpful and reduce errors. Samples should be kept in foam boxes or closed containers, 1131
protected from light, excessive moisture or dryness. Prepacked desiccants may be used 1132
for sample conservation. Storage temperatures should be 15 °C to 25 °C, unless 1133
otherwise indicated on the sample packaging. Samples should not be subjected to 1134
temperatures above 30 °C or frozen. Certain heat-sensitive medicines should be kept 1135
in between 4 °C and 8 °C (64); 1136
1137
- the time period, within which samples should be collected in the countries and the 1138
deadline for sending the last sample to the testing laboratory, should be clearly 1139
indicated and followed. 1140
1141
Working document QAS/14.590
page 44
ETHICAL CONSIDERATIONS ON QUALITY OF MEDICINES SURVEYS 1142
1143
There are important ethical considerations in investigating medicine/medical product quality, 1144
usually important in other branches of medical research, which have received scant attention. 1145
We are aware of no specific opinion or consensus guidance (Tabernero et al (in preparation)). 1146
The production and trade in falsified medicines is a criminal activity with the details and 1147
penalties of the offence depending on the laws and regulations of the country concerned. The 1148
production and trade in substandard medicines may also be an offence, usually against 1149
national medicine regulatory legislation and may, in some jurisdictions, be criminal 1150
negligence, i.e. allowing otherwise avoidable poor-quality medicines to be accessible to 1151
patients due to negligence. In addition to the law we are also informally regulated by moral 1152
obligations as members of the community as well as by our profession (65, 66). Criminality 1153
and negligence are thankfully rarely the subjects of medical research, but they may arise in 1154
different research studies and thus raise important issues when they emerge, for legal and 1155
ethical codes. 1156
Here we raise some of the issues that those involved in collecting medicines for quality 1157
testing should consider. 1158
The World Medical Association developed the Declaration of Helsinki as a statement of 1159
ethical principles in medical research involving human subjects. The document has been 1160
revised a number of times since its first publication in 1964; at the time of writing the most 1161
recent revision was in October 2013 (67). Other important information on medical research 1162
ethics can be found in Nuffield Council on Bioethics (68); Belmont Report (69); CIOMS 1163
Guidelines (70); report from the UNICEF/UNDP/World Bank/WHO Special Programme for 1164
Research and Training in Tropical Diseases (TDR) (71); Emanuel et al. 2004 (72), the 1165
American Anthropological Association (66) and the American Sociological Association (65) 1166
websites. In addition, WHO good clinical practices (GCP) (73) and the International 1167
conference on Harmonisation (ICH) (74) translate such ethical principles in methodological 1168
good practices for clinical and medical research. These guidelines are inclusive to subjects 1169
working on data management that have direct impact on data quality and reliability of the 1170
results. Even if quality surveys do not involve the participation of human subjects in medical 1171
experiments their results may inform national policies and have a direct impact on individuals 1172
Working document QAS/14.590
page 45
and their public health. Therefore, it is of paramount importance that the people involved in 1173
such studies comply with appropriate methodological and ethical standards. 1174
Medicines may be collected by diverse groups of investigators, from NDRA inspectors, 1175
agents of pharmaceutical companies, journalists and international organizations, to scientists 1176
from higher education institutes. All such groups should behave ethically and consider the 1177
ethical obligations and consequences of their work, especially towards the risk to those 1178
surveyed, those surveying and the public health of the population. This discussion focuses on 1179
academics conducting research but the principles also apply to other groups. 1180
1181
General ethical issues 1182
1183
The ethical issues related to medicine collection for quality testing will depend on the context 1184
and country in which they are to be carried out. It is important to carefully consider ethical 1185
issues in favour of carrying out the surveys as well as at the ethical “challenges”. The issues 1186
in favour of such work include: 1187
- individuals and communities are harmed by taking medicines that are ineffective or toxic, 1188
or both; 1189
- there are important public health benefits to be gained from having accurate information 1190
about the frequency of poor-quality medicines on the market in particular locations; 1191
- provision of information to NDRAs that will help identify those who sell and/or 1192
manufacture falsified medicines in subsequent NDRA/police investigations; 1193
- provide information on medicine quality problems that will alert NDRAs and 1194
manufacturers to problems and facilitate technical support for improvements or corrective 1195
actions in manufacturing medicine/medicinal product quality; 1196
- the benefits to communities and health professionals of raising awareness about poor-1197
quality medication/medical products and how to reduce their risk, in particular by 1198
allowing their identification and corrective actions before they reach the patients; 1199
- the prevention and/or reduction of the already scarce financial resources that would have 1200
been spent on poor-quality medicines to be used for other health-care benefits. 1201
1202
Working document QAS/14.590
page 46
Nonetheless, despite the benefits the carrying out of such surveys can also present a number 1203
of important ethical challenges and risks. Risks to surveyors and the surveyed are discussed 1204
below. Another neglected issue is that if investigators, at small, remoter outlets, sample the 1205
entire stock of a particular medicine, the accessibility of medicines to patiemts may be 1206
reduced, e.g. if a survey removed all antimalarials in a malarious area in a distal limb of the 1207
supply chain this would be unethical. If this is likely, as a way of addressing this risk, the 1208
survey team should provide quality-assured medicines in exchange at the time of overt 1209
purchase or return soon after mystery-shopper sampling to provide these. Furthermore, health 1210
providers in the government sector may not be willing to give medicines to the survey team 1211
because their drugs are only used for the patients with evidence of having a certain disease 1212
(i.e. positive malaria blood smear) otherwise they may be in trouble if they are audited. 1213
In addition, the survey methodology and/or conduct may pose important ethical challenges 1214
due to insufficient sample size, incorrect sampling or the analysis of a partial set of samples. 1215
This may lead to inaccurate results and policy recommendations and eventually harm the 1216
community. Just as in other branches of medical research, scientific and methodological 1217
soundness is a fundamental prerequisite for the ethical soundness of medicine quality surveys. 1218
Careful methodological and ethical considerations should therefore guide the preparation, the 1219
conduct and the dissemination of results of each survey. 1220
If a survey identifies manufacturers/suppliers as sources of poor-quality medicines to the 1221
outlets, caution should be taken when disseminating this information publicly. On the one 1222
hand, the information may expose the research team to legal action from the concerned 1223
company(ies), whilst not going public will result in not protecting the community from 1224
preventable harm. Such difficulties may be especially difficult if sources are government or 1225
international agencies (5). Legal advice should be sought but the default position should be to 1226
release public health information. These potential situations should be envisaged in the initial 1227
protocol and strategies predefined in advance, when possible in strict collaboration with the 1228
NDRAs, other relevant national stakeholders (e.g. national malaria programme). 1229
1230
1231
Working document QAS/14.590
page 47
Risks to the survey team members? 1232
1233
The production of and trade in falsified medicines is a criminal activity. Hence, the safety of 1234
those acting as mystery shoppers or involved in surveys of medicine quality must be 1235
considered. There are only a few examples in the public domain of people working on 1236
medicine quality being attacked or threatened. The most extreme was the apparent attempted 1237
murder of the head of the Nigerian Food and Drug Aministration, presumably related to her 1238
work (75). Formal overt inspection of the outlets by NDRA inspectors is likely to be the best 1239
option when the risk to the mystery shoppers is thought to be too significant. However, if the 1240
NDRA is poorly functioning or corrupt this will not be possible (76). 1241
The level of risk acceptable by the survey team, the responsibilities of institutions and 1242
supervisors and adequate training and support should be discussed with the NDRA, police and 1243
the collection team members and their institutions and a risk assessment performed. If 1244
mystery shoppers are members of the community this may present particular problems if they 1245
are recognized as participating in the survey. Therefore, appropriate risk assessments and 1246
discussion of training, confidentiality, security and insurance should be considered. Clear 1247
guidelines appropriate to local conditions need be developed and clearly explained to all those 1248
involved in this work. 1249
More widely, safety concerns of the research team will have to be addressed if it becomes 1250
known that surveys are being carried out by particular institutions or individuals – this 1251
information may be accessed within a few minutes on the internet. The publication of results 1252
may lead to reputational damages to specific individuals or groups (e.g. losing confidence in 1253
all the manufacturers from a given country, because poor-quality medicines from that given 1254
country have been found). Care should be taken in avoiding the identification of mystery 1255
shoppers in survey reports and publications. 1256
1257
What is the risk to those surveyed? 1258
1259
There is very little information as to what proportion of medicine providers sell poor-quality 1260
medicines, at different levels of the health-care system and how many know that the 1261
medicines that they are selling are poor quality (56, 77). Clearly they have a moral and 1262
Working document QAS/14.590
page 48
ethical responsibility to ensure that what they sell is good quality in cases where they are able 1263
to assess the reliability of supply channels and tell the differences between a genuine and a 1264
falsified medicine. Unfortunately, in much of the world they do not have the training or 1265
facilities to allow this. Risks include: 1266
- if overt, especially NDRA/police, inspections are noted in the community and raise 1267
suspicions of the quality of medicines sold in an outlet; the outlets may lose income by the 1268
community shopping elsewhere even though the medicines supplied are good quality; 1269
- innocent outlet staff and owners selling poor-quality medicines (e.g. those who bought 1270
drugs in good faith from suppliers of poor-quality medicines) may risk harm. Suppliers, 1271
irrespective of their knowledge of the quality of their products, may be at risk of losing 1272
income (possibly losing the business and bankruptcy) and perhaps being attacked or their 1273
medicines being seized by the community, as has been described (78); 1274
- if staff in outlets selling falsified medicines inform or are thought to have informed on 1275
those trading in such medicines, to NDRA or research staff, they may be at risk. 1276
1277
For these reasons, data and samples in a research study should be anonymized when sent for 1278
analysis, devoid of linkage to named outlets until results are obtained and, after appropriate 1279
risk assessments, discussed with the NDRA. Caution should be exercised if there is suspicion 1280
of corruption and poor supervision of the supply chain. Ethical challenges should be discussed 1281
with the ethical committee concerned and, if appropriate, with local pharmacy associations. 1282
1283
Do medicine quality surveys require review by a research ethics committee? 1284
1285
There is no consensus as to whether ethical approval is required for surveys and different 1286
bodies have different opinions. The scope of the WHO Standards and Operational Guidance 1287
for Ethics Review of Health-Related Research with Human Participants (79) includes that “all 1288
health-related research ethics committees, whether they review biomedical, social science, 1289
epidemiological, operational, or health systems research”. This is consistent with the position 1290
that medicine quality surveys should be subject to careful ethical scrutiny, but does not state 1291
this. Where possible and realistic those who are conducting such work should have access to 1292
ethics support and training. 1293

Working document QAS/14.590
page 49
It should also be noted that regulatory requirements for ethical clearance vary between 1294
different countries and that they must be carefully checked by the research team before 1295
planning each specific survey. 1296
The aim of the survey can be primarily an essential element of good public health practice, to 1297
improve programmes, reduce harm to patients and enforce drug quality standards or to 1298
generate new scientific knowledge. It may therefore represent routine surveillance and not 1299
research. We suggest that ethical scrutiny should be considered if (a) the survey goes beyond 1300
routine surveillance, (b) and/or if risk assessment suggests that there are significant risks to 1301
either surveyors or the surveyed. The advice of an independent medical ethicist may be 1302
valuable. The following steps should be considered: 1303
- ethical review should be considered before the survey, either with discussion of the need 1304
for ethical review with the Research Ethics Committees or a formal submission in the 1305
study country(ies) (80). Periodical and final study reports, should be submitted according 1306
to Research Ethics Committee requirements; 1307
1308
- there may be circumstances in which ethical review would not be appropriate, for example, 1309
if the Research Ethics Committees might be compromised or might feel that embarrassing 1310
data on poor-quality medicines should be suppressed. Should this be the case, the choice 1311
to proceed without ethical review should be documented and justified; 1312
- given the field nature of the surveys, they will usually be carried out in cooperation with 1313
the concerned NDRA(s). Should this not be appropriate (76) or possible, the decision to 1314
proceed without NDRAs involvement and approval should be documented and justified. 1315
1316
If risk assessment suggests that there are significant risks to either surveyors or the surveyed 1317
and/or if the results of the study are expected to be potentially sensitive, it is recommended 1318
that in addition to discussing the need, or otherwise, of applying for ethical clearance with the 1319
concerned Research Ethics Committee(s) in the country(ies) of study, a specially established 1320
independent ethics and legal advisory board where all the pertinent skills and expertise would 1321
be represented (e.g. analytical, legal, ethical, anthropological …) may be appointed to advise 1322
on the survey design and conduct, the communication of results and the management of any 1323
problems/incidents occurring at any stage of the research. The board should be selected with 1324
due consideration for expertise and for potential conflicts of interest/full independence, e.g. 1325

Working document QAS/14.590
page 50
none of the members should feel that embarrassing data on poor-quality medicines should be 1326
suppressed and that public health should be the prime guide to decision making. 1327
Those conducting the work should have access to ethical support and training in research 1328
ethics. If resources are limited this should focus at least on skills required for specific tasks 1329
(e.g. privacy and confidentiality issues for those collecting the information). If the country has 1330
no available ethics committee, the Science and Ethical Review Group (SERG) at WHO (81, 1331
82) has developed guidelines for the establishment of scientific and ethical review bodies. 1332
1333
Should outlet staff be told that they are being part of a study? 1334
1335
There is no consensus as to whether it is necessary to tell outlet staff that they are being 1336
sampled or whether a covert, mystery-shopper, approach is more appropriate. On the one 1337
hand an overt approach may allow the investigator to learn more about the product sample, 1338
distribution systems for medicines and what the outlet staff knows. This might be appropriate 1339
if the survey is carried out as routine surveillance. If it is decided that outlet staff should be 1340
informed the aims, methods and source of funding of the research should be explained and 1341
consent requested. This is important as participants should understand the implications for 1342
enrolment in the study and the right to abstain and withdraw. This consent-seeking process 1343
should take into consideration the cultural context and community consultation or 1344
engagement prior to the course of the research. The researchers should also establish 1345
appropriate measures to ensure confidentiality of outlet staff. 1346
On the other hand, a mystery-shopper approach increases the probability that the samples 1347
obtained will represent what such a shopper would be sold in real life. This is clearly 1348
appropriate for NDRA investigations and should also be aimed for during research surveys, 1349
especially for unregistered medicines that may otherwise be concealed. If the seller knows or 1350
is concerned that his/her stock contains illegal or poor-quality medicines and that the buyer is 1351
potentially linked to the NDRA or a medicine quality survey, this may falsely improve the 1352
quality of the medicines offered for sale (63). However, if outlet staff is aware and anxious to 1353
avoid falsified medicines, open sampling with feedback would allow more data to be 1354
collected on the risk factors and facilitate direct improvement in the medicine supply by 1355
positively engaging with pharmaceutical retailers. 1356

Working document QAS/14.590
page 51
A third compromise strategy is for outlets to be sampled by mystery shoppers after being 1357
informed on a prior visit that the survey will happen at some point in the future and requesting 1358
consent for this future undisclosed visit. However, this may influence the seller´s medicine 1359
selling behaviour, resulting in an inaccurate picture of the situation. Further research to 1360
examine the various methods for addressing these issues and to inform the development of 1361
models of good practice is needed. 1362
1363
What to do with the information once it has been gathered? 1364
1365
It is unethical for the details of the stated manufacturer and other sample details of poor-1366
quality medicines not to be reported to the NDRA and the WHO Rapid Alert System (83). 1367
There is no point in performing the survey if this is not done. We recommend that poor-1368
quality samples are reported in a timely manner to the NDRA for administrative and/or 1369
enforcement actions and should also be made available in the public domain, e.g. in an open 1370
access, peer-reviewed scientific paper and NDRA website. 1371
1372
There is no consensus on what should be done, how and when, in terms of release of public 1373
information if suspicious medicines/medical products are found. Clearly public health should 1374
be the primary priority, but there remains tension between commercial interests, the need to 1375
investigate (and investigator safety) and the need to act quickly to safeguard public health. It 1376
will also be important to ensure that public engagement is performed in a way to reduce the 1377
risk that patients stop taking genuine medicines and to reduce the risk of public loss of faith in 1378
medicines or the health-care system (Newton et al, submitted). 1379
1380
Results and findings should also be used for advocacy and educational purposes. When there 1381
is evidence of international illicit trade in poor-quality medicines, the WHO Rapid Alert 1382
System and INTERPOL are able to link countries NDRAs and police forces. 1383
1384
The antimalarial quality group at the WorldWide Antimalarial Resistance Network has been 1385
compiling reports of antimalarial quality globally and developed the antimalarial quality 1386
surveyor, an online visualization tool to try to understand the epidemiology of poor quality 1387
medicines (9, 84). 1388
Working document QAS/14.590
page 52
Samples should be described with the term “stated” before the manufacturer’s name and 1389
address, etc., as for falsified medicines they, by definition, do not originate from the 1390
manufacturer stated on the packet. It would be important not to falsely accuse a genuine 1391
manufacturer, making good quality of products that has been targeted by counterfeiters, of 1392
counterfeiting. Investigators may need to request legal advice to ensure that samples are 1393
appropriately described. 1394
1395
STORAGE AND TRANSPORT OF SAMPLES 1396
1397
Storage and transport of the sample should be done according to the requirements set out in 1398
paragraph 2.3 of WHO Guidelines for Sampling of Pharmaceutical Products and related 1399
materials (85): 1400
- the samples should be kept in original packaging and under storage conditions as 1401
specified on the sample label; 1402
- for transport all samples should be packaged adequately and transported in such a way as 1403
to avoid breakage and contamination during transport. Any residual space in the 1404
container should be filled with a suitable material. Where required the cold chain should 1405
be retained during storage and transport; 1406
- data temperature loggers should be included within shipments to document adequate 1407
temperature in prolonged transit after data download; 1408
- a covering letter, the copies of a sample collection form and, if available, copies of the 1409
manufacturer’s batch certificate of analysis should accompany the samples; 1410
- samples with the accompanying documents should be sent to the assigned testing 1411
laboratory by a courier service. For each shipment it should be clearly indicated that 1412
samples are sent for laboratory testing purposes only, will not be used on humans or 1413
animals, have no commercial value and will not be placed on the market. The NDRA of 1414
the country of the laboratory may be able to assist with permissions for importation; 1415
- the laboratory should be informed of the shipment, with the tracking number as provided 1416
by the courier service, to be able to follow the shipment and collection as soon as 1417
possible; 1418
Working document QAS/14.590
page 53
- copies of sample collection forms and, if available, copies of manufacturer’s batch 1419
certificates of analysis should also be sent to the survey coordinator/person preparing the 1420
report on the survey. 1421
1422
The USP developed the Rapid Assessment tool as a guideline for “Rapid Assessment of 1423
Medicines Quality Assurance and Medicines Quality Control” (86). 1424
1425
1426
TECHNIQUES TO DETERMINE QUALITY AND LABORATORY FACILITIES 1427
1428
An appropriate laboratory has to be selected for testing. Preferably a prequalified laboratory 1429
should be used (see the list of WHO-prequalified laboratories at www.who.int/prequal). 1430
Should such a laboratory not be available or should it not have sufficient capacity then 1431
another laboratory, for which evidence of reliability is available, should be chosen and the 1432
choice should be explained/justified in the study protocol, ethical/regulatory submissions, 1433
reports and publications (87). Many countries do not have a fully functioning quality control 1434
laboratory and should consider making arrangements with a laboratory abroad. 1435
The appropriate arrangement with the laboratory has to be made in advance, both to plan 1436
together that enough units and financial resources are available for carrying out all the tests 1437
needed to obtain meaningful and reliable results, and to give the laboratory time to be ready 1438
for testing (find the appropriate time slots, purchase necessary materials and standards …). 1439
The request for testing should be in line with WHO guideline Considerations for requesting 1440
analysis of drug samples (88), and no sample should be sent before such an arrangement is 1441
made. A contract with the laboratory should be concluded in advance to allow the laboratory 1442
to prepare for testing. 1443
A detailed address of the laboratory selected for the survey should be provided to the 1444
sampling organization. If there is more than one laboratory involved, clearly specify products 1445
which should be sent to each laboratory, for what assays and provide evidence that the 1446
laboratories will work according to the same standards, to make results comparable across 1447
different laboratories, products and countries. 1448
The laboratory will normally start testing only when all the samples are received. Therefore it 1449
is important to set and adhere to the deadline for sending to the testing laboratory. 1450
Working document QAS/14.590
page 54
1451
Assays to be conducted 1452
1453
Laboratory testing of all collected samples will be performed according to the testing protocol, 1454
which is a part of the survey protocol and has to be agreed with the testing laboratory(ies) 1455
according to the pharmacopoeial monograph and specifications. Tests to be conducted depend 1456
on the objectives of the survey. For example of testing protocol see Annex 7. 1457
In principle, the following tests should be included in quality surveys of products on the 1458
market: 1459
• appearance; 1460
• identity; 1461
• assay; 1462
• related substances test; 1463
• dissolution or disintegration and uniformity of mass for (solid dosage forms, e.g. tablets, 1464
capsules); 1465
• pH value for liquid dosage forms (e.g. oral solutions, injections, powders for injection) 1466
• sterility of injectables; 1467
• packaging analysis of all packaging and labelling. 1468
1469
Some tests for injectable samples, such as for uniformity of content for single-dose dosage 1470
forms or sterility, are not normally included in quality surveys but we suggest that they should, 1471
being costly. The recent catastrophic fungal contamination of injectable methylprednisolone 1472
emphasizes the importance of being alert to this problem (2, 89). 1473
Screening methods do not provide a full picture of the quality of medicines and, as shown in 1474
Survey of the Quality of Selected Antimalarial Medicines study (QAMSA) (24), often 1475
underestimate non-compliant findings in comparison with laboratory testing. It is 1476
recommended to perform testing in a quality control laboratory, at the very least, for a random 1477
selection of those samples that pass screening assays and all those that fail. Simple screening 1478
methods are more suitable for screening of large number of samples in the field, e.g. to search 1479
for falsified medicines, but should always be validated by reference assays. Laboratory 1480

Working document QAS/14.590
page 55
procedures should be blinded, i.e. packaging and labelling assessment should not be 1481
conducted by the same person who carries out the chemical tests. 1482
1483
Test methods and specifications 1484
1485
Test methods and specifications are in general selected according to the following rules: 1486
- preferably Ph.Int. monographs should be used, if available; 1487
- if no monograph exists in the Ph.Int. then BP or USP can be used; 1488
- if there is no pharmacopoeial monograph or the existing monographs do not provide for 1489
desired tests, a validated method of the laboratory or manufacturer's method, if available, 1490
should be used; 1491
- wherever possible the laboratory should perform internal and external quality assurance for 1492
the assays used 1493
1494
For the example of testing protocol used in the QAMSA study (24) for artemisinin-based 1495
combination therapy and sulfadoxine/pyrimethamine see Annex 7. 1496
When samples from different manufacturers are collected within a quality survey all samples 1497
containing the same combination of active ingredients are tested according to the same 1498
specification to enable comparison of samples from different manufacturers. This 1499
specification is then used to decide on compliance or non-compliance of tested samples for 1500
the purposes of this survey. It should be noted that individual manufacturers may use different 1501
specifications and different methods for testing of their products and these specifications and 1502
methods may be approved by regulatory authorities in different countries. Non-compliance 1503
with the specification selected for the survey does not necessarily imply non-compliance with 1504
the specifications approved in the country. But it indicates the need to look at the product and 1505
conditions of regulatory approval more closely and further actions should be considered by 1506
the respective NDRA. 1507
Medicine quality evaluation laboratories should have decision trees and flow diagrams for 1508
samples and those developed as part of the Counterfeit Drug Forensic Investigation Network 1509
project are available (90, 91). 1510
Working document QAS/14.590
page 56
1511
Receipt and testing of samples by a testing laboratory 1512
1513
When samples are received, the testing laboratory will: 1514
- inspect each sample to ensure that the labelling is in conformance with the information 1515
contained in the sample collection form or test request; 1516
- store the samples according to the respective medicine requirement, including compliance 1517
with any cold chain requirements; 1518
- conduct quality testing in line with the testing protocol and in compliance with WHO 1519
standards recommended for quality control laboratories; 1520
- complete an analytical test report (Annex 8). If non-compliant results are found and 1521
confirmed after application of a laboratory OOS procedure, they have to be reported 1522
immediately to the study team or the contact point. The contact point should be specified in 1523
the sampling plan; 1524
- keep records of each sample, accompanying document/s and retention samples for at least 1525
5 five years with the analytical test requirements; 1526
- an electronic databank (e.g. scanned pictures or photographs of the medicines, such as of 1527
the tablets, packaging, and package leaflet) is recommended. 1528
1529
DATA MANAGEMENT, REPORTING AND PUBLICATION 1530
1531
Data obtained from the different collection tools such as sample forms, mystery-shopper 1532
debriefing forms or open sampling questionnaires should be double entered into a predesigned 1533
data entry database. Diverse software is available for data entry when conducting 1534
epidemiological studies e.g. Epiinfo (http://wwwn.cdc.gov/epiinfo/) or Epidata 1535
(http://www.epidata.dk/) are freely available from the internet, and should be preferred to 1536
Excel which is not a software specifically designed for data management. Preferably, and 1537
especially if the survey’s results may be sensitive, a password-controlled database with audit 1538
trail should be chosen. The information entered in the database should link the sample with 1539
subsequent analysis and interpretation data using the unique ID code. The database should be 1540
checked for coding errors and consistency. Two double-entry datasets should be compared 1541
Working document QAS/14.590
page 57
and differences checked against the original data form. Data management and statistical 1542
analysis of the results can be conducted with, for example, STATA®
, (Stata Corp., College 1543
Station, TX, USA) or SPSS programmes. Personal identification of individuals who 1544
participated in the survey (buyers, sellers, etc.) should not be entered in the database with the 1545
use of codes only. 1546
The concerned NDRAs should be informed of any non-compliant results as soon as possible 1547
and investigations pursued, in line with regulatory practice and legislation, with the stated 1548
manufacturer. In addition the WHO Rapid Alert System should be informed (83) and if 1549
applicable batch recall procedures should be started. 1550
The analytical test reports of the testing laboratory(ies) will be provided to all NDRAs 1551
involved in the project. The outcomes of the project will be discussed by national authorities 1552
in a meeting and corrective actions, if necessary, will be recommended. Relevant regulatory 1553
measures in the different countries lie within the responsibility of the NDRA in collaboration 1554
with the police when applicable (falsified medicines or criminal negligence). Agreed 1555
outcomes and the report from the survey should be reviewed by the investigation team first to 1556
make it available for publication by WHO. The WHO alert system and INTERPOL (when 1557
applicable) should be informed when results are considered a public health emergency. The 1558
Medicine Quality Assessment Reporting Guidelines published in 2009 (25) provide an 1559
example checklist of items that should be included in reports of medicine quality (Table 7). 1560
1561
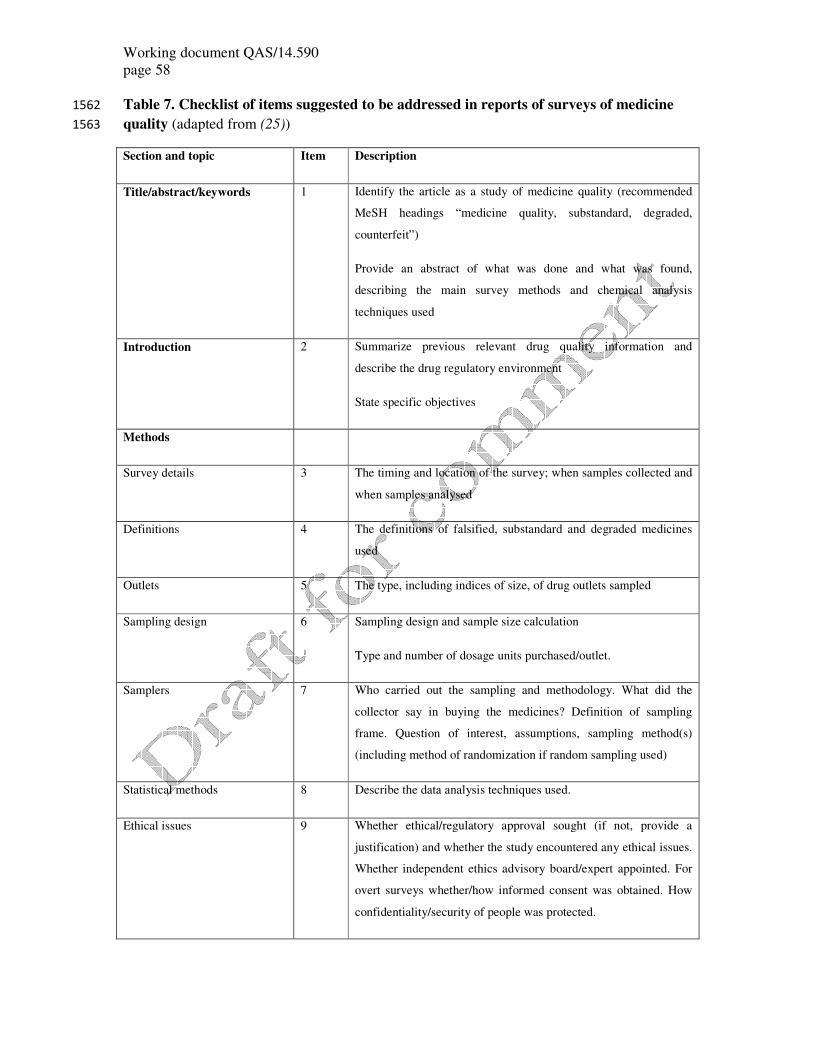
Working document QAS/14.590
page 58
Table 7. Checklist of items suggested to be addressed in reports of surveys of medicine 1562
quality (adapted from (25)) 1563
Section and topic Item Description
Title/abstract/keywords 1 Identify the article as a study of medicine quality (recommended
MeSH headings “medicine quality, substandard, degraded,
counterfeit”)
Provide an abstract of what was done and what was found,
describing the main survey methods and chemical analysis
techniques used
Introduction 2 Summarize previous relevant drug quality information and
describe the drug regulatory environment
State specific objectives
Methods
Survey details 3 The timing and location of the survey; when samples collected and
when samples analysed
Definitions 4 The definitions of falsified, substandard and degraded medicines
used
Outlets 5 The type, including indices of size, of drug outlets sampled
Sampling design 6 Sampling design and sample size calculation
Type and number of dosage units purchased/outlet.
Samplers 7 Who carried out the sampling and methodology. What did the
collector say in buying the medicines? Definition of sampling
frame. Question of interest, assumptions, sampling method(s)
(including method of randomization if random sampling used)
Statistical methods 8 Describe the data analysis techniques used.
Ethical issues 9 Whether ethical/regulatory approval sought (if not, provide a
justification) and whether the study encountered any ethical issues.
Whether independent ethics advisory board/expert appointed. For
overt surveys whether/how informed consent was obtained. How
confidentiality/security of people was protected.
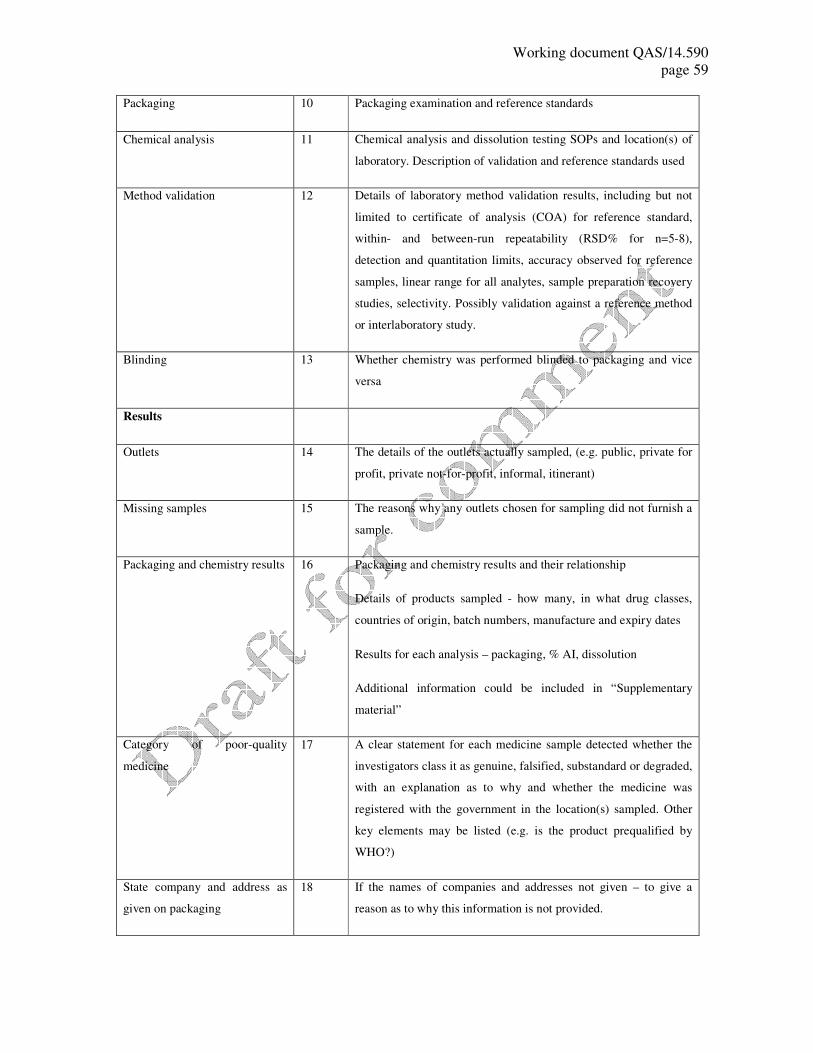
Working document QAS/14.590
page 59
Packaging 10 Packaging examination and reference standards
Chemical analysis 11 Chemical analysis and dissolution testing SOPs and location(s) of
laboratory. Description of validation and reference standards used
Method validation 12 Details of laboratory method validation results, including but not
limited to certificate of analysis (COA) for reference standard,
within- and between-run repeatability (RSD% for n=5-8),
detection and quantitation limits, accuracy observed for reference
samples, linear range for all analytes, sample preparation recovery
studies, selectivity. Possibly validation against a reference method
or interlaboratory study.
Blinding 13 Whether chemistry was performed blinded to packaging and vice
versa
Results
Outlets 14 The details of the outlets actually sampled, (e.g. public, private for
profit, private not-for-profit, informal, itinerant)
Missing samples 15 The reasons why any outlets chosen for sampling did not furnish a
sample.
Packaging and chemistry results 16 Packaging and chemistry results and their relationship
Details of products sampled - how many, in what drug classes,
countries of origin, batch numbers, manufacture and expiry dates
Results for each analysis – packaging, % AI, dissolution
Additional information could be included in “Supplementary
material”
Category of poor-quality
medicine
17 A clear statement for each medicine sample detected whether the
investigators class it as genuine, falsified, substandard or degraded,
with an explanation as to why and whether the medicine was
registered with the government in the location(s) sampled. Other
key elements may be listed (e.g. is the product prequalified by
WHO?)
State company and address as
given on packaging
18 If the names of companies and addresses not given – to give a
reason as to why this information is not provided.
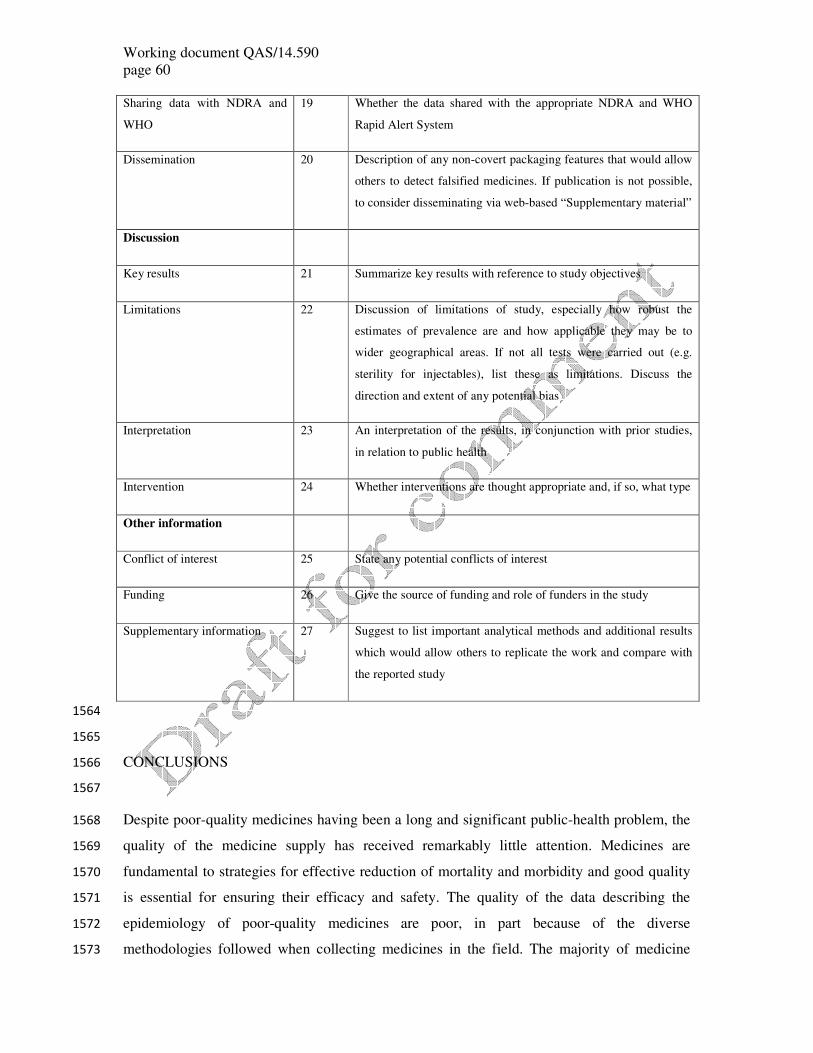
Working document QAS/14.590
page 60
Sharing data with NDRA and
WHO
19 Whether the data shared with the appropriate NDRA and WHO
Rapid Alert System
Dissemination 20 Description of any non-covert packaging features that would allow
others to detect falsified medicines. If publication is not possible,
to consider disseminating via web-based “Supplementary material”
Discussion
Key results 21 Summarize key results with reference to study objectives
Limitations 22 Discussion of limitations of study, especially how robust the
estimates of prevalence are and how applicable they may be to
wider geographical areas. If not all tests were carried out (e.g.
sterility for injectables), list these as limitations. Discuss the
direction and extent of any potential bias
Interpretation 23 An interpretation of the results, in conjunction with prior studies,
in relation to public health
Intervention 24 Whether interventions are thought appropriate and, if so, what type
Other information
Conflict of interest 25 State any potential conflicts of interest
Funding 26 Give the source of funding and role of funders in the study
Supplementary information 27 Suggest to list important analytical methods and additional results
which would allow others to replicate the work and compare with
the reported study
1564
1565
CONCLUSIONS 1566
1567
Despite poor-quality medicines having been a long and significant public-health problem, the 1568
quality of the medicine supply has received remarkably little attention. Medicines are 1569
fundamental to strategies for effective reduction of mortality and morbidity and good quality 1570
is essential for ensuring their efficacy and safety. The quality of the data describing the 1571
epidemiology of poor-quality medicines are poor, in part because of the diverse 1572
methodologies followed when collecting medicines in the field. The majority of medicine 1573

Working document QAS/14.590
page 61
quality surveys performed have not used rigorous sampling methods. Any sampling 1574
methodology is inherently prone to bias if it is conducted in such a way that it is different 1575
from the population of interest, i.e. in cases where the location of sample collection is not the 1576
normal access to treatment or if collectors are known in the area. Convenience sampling of 1577
outlets is unlikely to accurately reflect the quality of medicines that consumers actually use in 1578
a defined area, but it can give reports of the presence of poor-quality medicines and provide 1579
an approximate estimate of frequency, without confidence intervals, of unknown accuracy. 1580
All sampling techniques, except convenience sampling, require a sampling frame from which 1581
the samples are drawn. This sampling frame should be representative of the population to 1582
which the investigators wish to be able to generalize the results. Even though randomization 1583
has been considered the “gold standard” sampling technique it will not deal with problems of 1584
inspectors known to pharmacists or any internal knowledge by staff about poor-quality 1585
medicines at the facilities. Therefore it is critical to maintain the covert nature of sampling. 1586
Large sampling sizes or a very high number of dosage units collected will alert sellers to the 1587
aims of those collecting samples as well as asking for a specific brand or medicine for 1588
collection. Communication lines and methods should be agreed well in advance prior the 1589
survey and a plan for publication and dissemination should be developed and agreed at the 1590
planning stage of the survey. Accurate estimates of the frequency of poor-quality medicines in 1591
the market are urgently needed as a requirement for valid comparisons between countries and 1592
regions. Further discussion and consensus-building on the ethics of medicine quality surveys 1593
is required. 1594
REFERENCES 1595
1596
1. Newton, P.N., et al., Counterfeit anti-infective drugs. The Lancet Infectious Diseases, 1597
2006. 6(9): p. 602-613. 1598
2. Caudron, J.M., et al., Substandard medicines in resource-poor settings: a problem that 1599
can no longer be ignored. Tropical Medicine & International Health, 2008. 13(8): p. 1600
1062-1072. 1601
3. IOM, Countering the Problem of Falsified and Substandard Drugs, in National 1602
Academy of Sciences, L. Gostin, Editor. 2013, Institute of Medicine of the National 1603
Academies: http://www.iom.edu/Reports/2013/Countering-the-Problem-of-Falsified-1604
and-Substandard-Drugs.aspx. 1605
4. Newton, P., et al., Poor quality vital anti-malarials in Africa - an urgent neglected 1606
public health priority. Malaria Journal, 2011. 10(1): p. 352. 1607
5. Dorlo, T.P.C., et al., A Poor-Quality Generic Drug for the Treatment of Visceral 1608
Leishmaniasis: A Case Report and Appeal. PLoS Negl Trop Dis, 2012. 6(5): p. e1544. 1609
6. Keoluangkhot, V., et al., Impaired Clinical Response in a Patient with Uncomplicated 1610
Falciparum Malaria Who Received Poor-Quality and Underdosed Intramuscular 1611
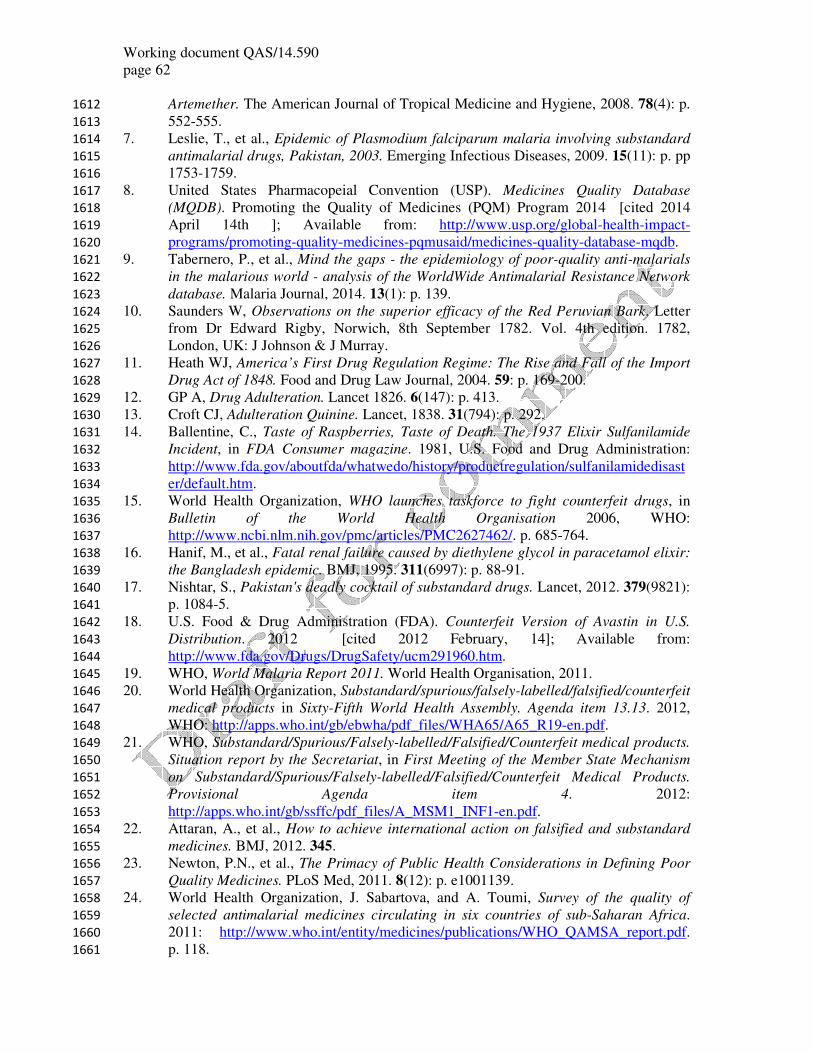
Working document QAS/14.590
page 62
Artemether. The American Journal of Tropical Medicine and Hygiene, 2008. 78(4): p. 1612
552-555. 1613
7. Leslie, T., et al., Epidemic of Plasmodium falciparum malaria involving substandard 1614
antimalarial drugs, Pakistan, 2003. Emerging Infectious Diseases, 2009. 15(11): p. pp 1615
1753-1759. 1616
8. United States Pharmacopeial Convention (USP). Medicines Quality Database 1617
(MQDB). Promoting the Quality of Medicines (PQM) Program 2014 [cited 2014 1618
April 14th ]; Available from: http://www.usp.org/global-health-impact-1619
programs/promoting-quality-medicines-pqmusaid/medicines-quality-database-mqdb. 1620
9. Tabernero, P., et al., Mind the gaps - the epidemiology of poor-quality anti-malarials 1621
in the malarious world - analysis of the WorldWide Antimalarial Resistance Network 1622
database. Malaria Journal, 2014. 13(1): p. 139. 1623
10. Saunders W, Observations on the superior efficacy of the Red Peruvian Bark. Letter 1624
from Dr Edward Rigby, Norwich, 8th September 1782. Vol. 4th edition. 1782, 1625
London, UK: J Johnson & J Murray. 1626
11. Heath WJ, America’s First Drug Regulation Regime: The Rise and Fall of the Import 1627
Drug Act of 1848. Food and Drug Law Journal, 2004. 59: p. 169-200. 1628
12. GP A, Drug Adulteration. Lancet 1826. 6(147): p. 413. 1629
13. Croft CJ, Adulteration Quinine. Lancet, 1838. 31(794): p. 292. 1630
14. Ballentine, C., Taste of Raspberries, Taste of Death. The 1937 Elixir Sulfanilamide 1631
Incident, in FDA Consumer magazine. 1981, U.S. Food and Drug Administration: 1632
http://www.fda.gov/aboutfda/whatwedo/history/productregulation/sulfanilamidedisast1633
er/default.htm. 1634
15. World Health Organization, WHO launches taskforce to fight counterfeit drugs, in 1635
Bulletin of the World Health Organisation 2006, WHO: 1636
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2627462/. p. 685-764. 1637
16. Hanif, M., et al., Fatal renal failure caused by diethylene glycol in paracetamol elixir: 1638
the Bangladesh epidemic. BMJ, 1995. 311(6997): p. 88-91. 1639
17. Nishtar, S., Pakistan's deadly cocktail of substandard drugs. Lancet, 2012. 379(9821): 1640
p. 1084-5. 1641
18. U.S. Food & Drug Administration (FDA). Counterfeit Version of Avastin in U.S. 1642
Distribution. 2012 [cited 2012 February, 14]; Available from: 1643
http://www.fda.gov/Drugs/DrugSafety/ucm291960.htm. 1644
19. WHO, World Malaria Report 2011. World Health Organisation, 2011. 1645
20. World Health Organization, Substandard/spurious/falsely-labelled/falsified/counterfeit 1646
medical products in Sixty-Fifth World Health Assembly. Agenda item 13.13. 2012, 1647
WHO: http://apps.who.int/gb/ebwha/pdf_files/WHA65/A65_R19-en.pdf. 1648
21. WHO, Substandard/Spurious/Falsely-labelled/Falsified/Counterfeit medical products. 1649
Situation report by the Secretariat, in First Meeting of the Member State Mechanism 1650
on Substandard/Spurious/Falsely-labelled/Falsified/Counterfeit Medical Products. 1651
Provisional Agenda item 4. 2012: 1652
http://apps.who.int/gb/ssffc/pdf_files/A_MSM1_INF1-en.pdf. 1653
22. Attaran, A., et al., How to achieve international action on falsified and substandard 1654
medicines. BMJ, 2012. 345. 1655
23. Newton, P.N., et al., The Primacy of Public Health Considerations in Defining Poor 1656
Quality Medicines. PLoS Med, 2011. 8(12): p. e1001139. 1657
24. World Health Organization, J. Sabartova, and A. Toumi, Survey of the quality of 1658
selected antimalarial medicines circulating in six countries of sub-Saharan Africa. 1659
2011: http://www.who.int/entity/medicines/publications/WHO_QAMSA_report.pdf. 1660
p. 118. 1661
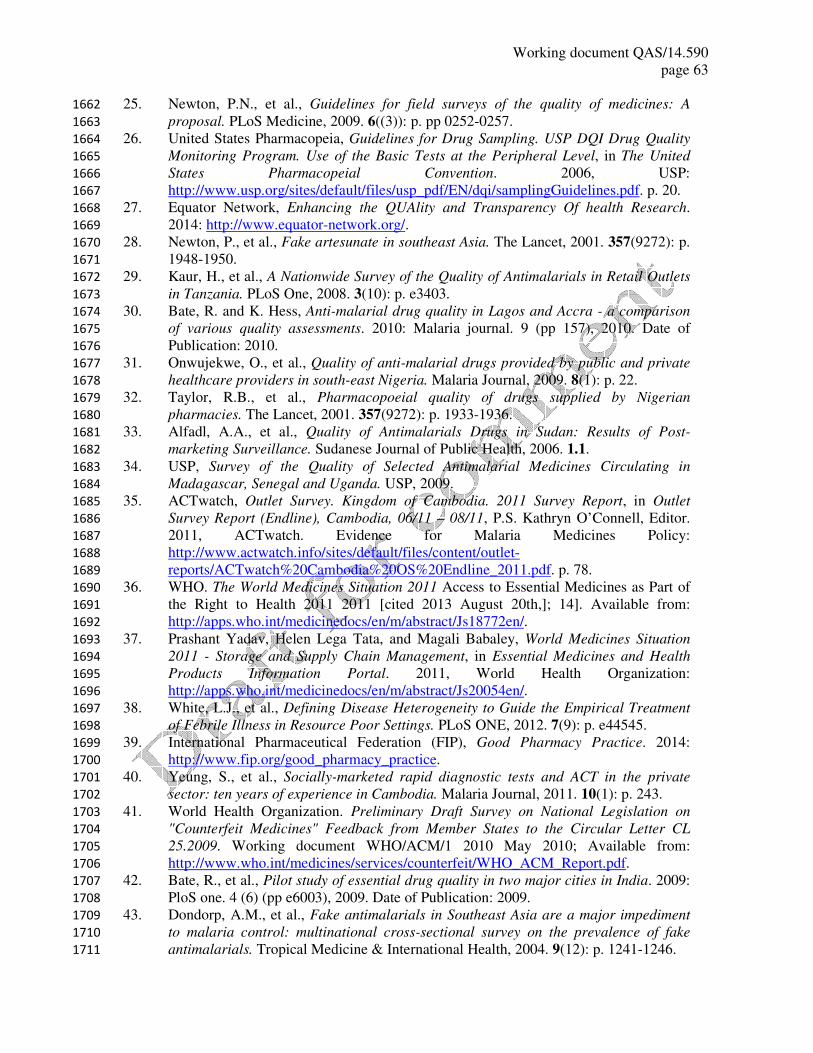
Working document QAS/14.590
page 63
25. Newton, P.N., et al., Guidelines for field surveys of the quality of medicines: A 1662
proposal. PLoS Medicine, 2009. 6((3)): p. pp 0252-0257. 1663
26. United States Pharmacopeia, Guidelines for Drug Sampling. USP DQI Drug Quality 1664
Monitoring Program. Use of the Basic Tests at the Peripheral Level, in The United 1665
States Pharmacopeial Convention. 2006, USP: 1666
http://www.usp.org/sites/default/files/usp_pdf/EN/dqi/samplingGuidelines.pdf. p. 20. 1667
27. Equator Network, Enhancing the QUAlity and Transparency Of health Research. 1668
2014: http://www.equator-network.org/. 1669
28. Newton, P., et al., Fake artesunate in southeast Asia. The Lancet, 2001. 357(9272): p. 1670
1948-1950. 1671
29. Kaur, H., et al., A Nationwide Survey of the Quality of Antimalarials in Retail Outlets 1672
in Tanzania. PLoS One, 2008. 3(10): p. e3403. 1673
30. Bate, R. and K. Hess, Anti-malarial drug quality in Lagos and Accra - a comparison 1674
of various quality assessments. 2010: Malaria journal. 9 (pp 157), 2010. Date of 1675
Publication: 2010. 1676
31. Onwujekwe, O., et al., Quality of anti-malarial drugs provided by public and private 1677
healthcare providers in south-east Nigeria. Malaria Journal, 2009. 8(1): p. 22. 1678
32. Taylor, R.B., et al., Pharmacopoeial quality of drugs supplied by Nigerian 1679
pharmacies. The Lancet, 2001. 357(9272): p. 1933-1936. 1680
33. Alfadl, A.A., et al., Quality of Antimalarials Drugs in Sudan: Results of Post-1681
marketing Surveillance. Sudanese Journal of Public Health, 2006. 1.1. 1682
34. USP, Survey of the Quality of Selected Antimalarial Medicines Circulating in 1683
Madagascar, Senegal and Uganda. USP, 2009. 1684
35. ACTwatch, Outlet Survey. Kingdom of Cambodia. 2011 Survey Report, in Outlet 1685
Survey Report (Endline), Cambodia, 06/11 – 08/11, P.S. Kathryn O’Connell, Editor. 1686
2011, ACTwatch. Evidence for Malaria Medicines Policy: 1687
http://www.actwatch.info/sites/default/files/content/outlet-1688
reports/ACTwatch%20Cambodia%20OS%20Endline_2011.pdf. p. 78. 1689
36. WHO. The World Medicines Situation 2011 Access to Essential Medicines as Part of 1690
the Right to Health 2011 2011 [cited 2013 August 20th,]; 14]. Available from: 1691
http://apps.who.int/medicinedocs/en/m/abstract/Js18772en/. 1692
37. Prashant Yadav, Helen Lega Tata, and Magali Babaley, World Medicines Situation 1693
2011 - Storage and Supply Chain Management, in Essential Medicines and Health 1694
Products Information Portal. 2011, World Health Organization: 1695
http://apps.who.int/medicinedocs/en/m/abstract/Js20054en/. 1696
38. White, L.J., et al., Defining Disease Heterogeneity to Guide the Empirical Treatment 1697
of Febrile Illness in Resource Poor Settings. PLoS ONE, 2012. 7(9): p. e44545. 1698
39. International Pharmaceutical Federation (FIP), Good Pharmacy Practice. 2014: 1699
http://www.fip.org/good_pharmacy_practice. 1700
40. Yeung, S., et al., Socially-marketed rapid diagnostic tests and ACT in the private 1701
sector: ten years of experience in Cambodia. Malaria Journal, 2011. 10(1): p. 243. 1702
41. World Health Organization. Preliminary Draft Survey on National Legislation on 1703
"Counterfeit Medicines" Feedback from Member States to the Circular Letter CL 1704
25.2009. Working document WHO/ACM/1 2010 May 2010; Available from: 1705
http://www.who.int/medicines/services/counterfeit/WHO_ACM_Report.pdf. 1706
42. Bate, R., et al., Pilot study of essential drug quality in two major cities in India. 2009: 1707
PloS one. 4 (6) (pp e6003), 2009. Date of Publication: 2009. 1708
43. Dondorp, A.M., et al., Fake antimalarials in Southeast Asia are a major impediment 1709
to malaria control: multinational cross-sectional survey on the prevalence of fake 1710
antimalarials. Tropical Medicine & International Health, 2004. 9(12): p. 1241-1246. 1711

Working document QAS/14.590
page 64
44. Sengaloundeth, S., et al., A stratified random survey of the proportion of poor quality 1712
oral artesunate sold at medicine outlets in the Lao PDR - implications for therapeutic 1713
failure and drug resistance. Malaria Journal, 2009. 1714
45. Ogwal-Okeng, J.W., D.O. Okello, and O. Odyek, Quality of oral and parenteral 1715
chloroquine in Kampala. 1998: East African medical journal. 75 (12) (pp 692-694), 1716
1998. Date of Publication: Dec 1998. 1717
46. Hani M. J. Khojah, et al., Adherence of Community Pharmacies in Riyadh, Saudi 1718
Arabia, to Optimal Conditions for Keeping and Selling Good-Quality Medicines. 1719
Pharmacology & Pharmacy, 2013. 4(5): p. 431. 1720
47. Lemeshow, S. and S. Taber, Lot quality assurance sampling: single- and double-1721
sampling plans. World Health Stat Q, 1991. 44(3): p. 115-32. 1722
48. Liverpool School of Tropical Medicine LSTM, The LQAS Generic Toolkit. 2014: 1723
http://www.lstmliverpool.ac.uk/research/departments/international-public-1724
health/metre/lqas-generic-toolkit/. 1725
49. Reinke, W.A., Applicability of Industrial Sampling Techniques to Epidemiologic 1726
Investigations: Examination of an Underutilized Resource. American Journal of 1727
Epidemiology, 1991. 134(10): p. 1222-1232. 1728
50. Lanata, C.F. and R.E. Black, Lot quality assurance sampling techniques in health 1729
surveys in developing countries: advantages and current constraints. World Health 1730
Stat Q, 1991. 44(3): p. 133-9. 1731
51. Robertson, S.E., et al., The lot quality technique: a global review of applications in the 1732
assessment of health services and disease surveillance. World Health Stat Q, 1997. 1733
50(3-4): p. 199-209. 1734
52. Valadez, J.J., A Trainer’s Guide. Using LQAS for Baseline Surveys and Regular 1735
Monitoring, in Assessing Community Health Programs. 2003, Teaching-aids At Low 1736
Cost (TALC), London Illustrations by The Hesperian Foundation: 1737
http://www.coregroup.org/storage/documents/LQAS/Intro.pdf. 1738
53. Phanouvong, S., Mekong Malaria Initiative, Antimalarial Drug Quality Monitoring 1739
and Evaluation. Indicators, in USP. 2004: 1740
http://pdf.usaid.gov/pdf_docs/pnadh147.pdf. 1741
54. Pharmacopeia, U.S. Uniformity of dosage units. Chapter 905. Stage 6 Harmonization 1742
2011 [cited 2014 February 27th, ]; Available from: 1743
http://www.pharmacopeia.cn/v29240/usp29nf24s0_c905.html. 1744
55. WHO. The International Pharmacopeia Fourth Edition. Volume 2 2006; Available 1745
from: http://apps.who.int/phint/en/p/docf/. 1746
56. Syhakhang, L., et al., Knowledge and perceptions of drug quality among drug sellers 1747
and consumers in Lao PDR. Health Policy and Planning, 2004. 19((6)): p. 391-401. 1748
57. Newton, P.N., et al., A collaborative epidemiological investigation into the criminal 1749
fake artesunate trade in South East Asia. 2008: PLoS medicine. 5 (2) (pp e32), 2008. 1750
Date of Publication: Feb 2008. 1751
58. Venhuis, B.J., et al., Dose-to-dose variations with single packages of counterfeit 1752
medicines and adulterated dietary supplements as a potential source of false negatives 1753
and inaccurate health risk assessments. Journal of Pharmaceutical and Biomedical 1754
Analysis, 2014. 89(0): p. 158-165. 1755
59. United Nations Office on Drugs and Crime, Guidelines on Representative Drug 1756
Sampling, Laboratory and Scientific Section, Editor. 2009: 1757
http://www.unodc.org/documents/scientific/Drug_Sampling.pdf. 1758
60. Administration, U.S.D.o.J.D.E., Scientific working group for the analysis of seized 1759
drugs (SWGDRUG) Recommendations,. 2011: 1760
http://www.swgdrug.org/Documents/SWGDRUG%20Recommendations%206.pdf. 1761

Working document QAS/14.590
page 65
61. Frank, R., C. Hoffman, and S. Hinkley, Representative Sampling of Drug Seizures in 1762
Multiple Containers. ASTM International, 1991. 36(2). 1763
62. SEARPharm and S.E.A.F.-W.F.o.P. Associations, Extent of Spurious (Counterfeit) 1764
Medicines in India. South East ASian FIP-WHO Forum of Pharmaceutical 1765
Associations, 2007. 1766
63. Madden, J.M., et al., Undercover careseekers: Simulated clients in the study of health 1767
provider behavior in developing countries. Social Science & Medicine, 1997. 45(10): 1768
p. 1465-1482. 1769
64. Pharmacopeia, U.S., Ensuring the Quality of Medicines in Resource-Limited 1770
Countries: An Operational Guide, in Drug Quality and Information Program. 2007, 1771
United States Pharmacopeial Convention: 1772
http://apps.who.int/medicinedocs/documents/s18424en/s18424en.pdf. 1773
65. American Sociological Association. ASA Code of Ethics. Ethics and the Code of 1774
Ethics [cited 2014 February 25th]. 1775
66. The American Anthropological Association (AAA). Code of Ethics of the American 1776
Anthropological Association. 1998 [cited 2014 February 25th]. 1777
67. The World Medical Association (WMA), WMA Declaration of Helsinki - Ethical 1778
Principles for Medical Research Involving Human Subjects. 2013: 1779
http://www.wma.net/en/30publications/10policies/b3/index.html. 1780
68. Nuffield Foundation. The Nuffield Council on Bioethics,. 1991 [cited 2014 February 1781
24]. 1782
69. The National Commission for the Protection of Human Subjects of Biomedical and 1783
Behavioral Research, The Belmont Report, in Ethical Principles and Guidelines for 1784
the Protection of Human Subjects of Research. 1979, Department of Health, 1785
Education, and Welfare: 1786
http://videocast.nih.gov/pdf/ohrp_appendix_belmont_report_vol_2.pdf. 1787
70. Council for International Organizations of Medical Sciences (CIOMS) in 1788
collaboration with the World Health Organization (WHO), International Ethical 1789
Guidelines for Biomedical Research Involving Human Subjects. 2002: 1790
http://www.cioms.ch/publications/layout_guide2002.pdf. 1791
71. World Health Organization, Ethical challenges in study design and informed consent 1792
for health research in resource-poor settings in TDR/SDR/SEB/ST/07.1 SPECIAL 1793
TOPICS No.5, Special Programme for Research & Training in Tropical Diseases 1794
(TDR) sponsored by UNICEF/ UNDP/ World Bank/ WHO, Editor.: 1795
http://whqlibdoc.who.int/publications/2007/9789241563383_eng.pdf. 1796
72. Emanuel, E.J., et al., What Makes Clinical Research in Developing Countries Ethical? 1797
The Benchmarks of Ethical Research. Journal of Infectious Diseases, 2004. 189(5): p. 1798
930-937. 1799
73. World Health Organization, Guidelines for good clinical practice (GCP) for trials on 1800
pharmaceutical products,, in WHO Technical Report Series. 1995: 1801
http://apps.who.int/medicinedocs/pdf/whozip13e/whozip13e.pdf. 1802
74. ICH, Guideline for good clinical practice in INTERNATIONAL CONFERENCE ON 1803
HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF 1804
PHARMACEUTICALS FOR HUMAN USE 1996: 1805
http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E61806
_R1/Step4/E6_R1__Guideline.pdf. 1807
75. Aldhous, P., Counterfeit pharmaceuticals: Murder by medicine. Nature, 2005. 1808
434(7030): p. 132-136. 1809
76. Francis PA, THE TIP OF AN ICEBERG. 2003, Pharmabiz.com: 1810
http://www.pharmabiz.com/article/detnews.asp?articleid=15677§ionid=47. 1811

Working document QAS/14.590
page 66
77. Khan, M., et al., Perceptions and practices of pharmaceutical wholesalers 1812
surrounding counterfeit medicines in a developing country: a baseline survey. BMC 1813
Health Services Research, 2011. 11(1): p. 306. 1814
78. Newton, P.N., et al., Manslaughter by Fake Artesunate in Asia-Will Africa Be Next? 1815
PLoS Med, 2006. 3(6): p. e197. 1816
79. WHO, Standards and Operational Guidance for Ethics Review of Health-Related 1817
Research with Human Participants. 2011: 1818
http://whqlibdoc.who.int/publications/2011/9789241502948_eng.pdf. 1819
80. Ravinetto, R., et al., Double ethical review of North–South collaborative clinical 1820
research: hidden paternalism or real partnership? Tropical Medicine & International 1821
Health, 2011. 16(4): p. 527-530. 1822
81. WHO, Ethical issues in patient safety research: interpreting existing guidance. 2013: 1823
http://apps.who.int/iris/bitstream/10665/85371/1/9789241505475_eng.pdf. 1824
82. WHO, Quality practices in basic biomedical research in Prepared for TDR by the 1825
Scientific Working Group on Quality Practices in Basic Biomedical Research, 1826
S.P.f.R.T.i.T.D.T.s.b.U.U.W.B. WHO, Editor.: 1827
http://www.who.int/tdr/publications/documents/quality_practices.pdf. 1828
83. WHO, WHO project for the surveillance and monitoring of SSFFC medical products, 1829
in WHO Drug Information. Quality and Safety of Medicines. 2013: 1830
http://www.who.int/medicines/publications/druginformation/issues/DrugInformation21831
013_Vol27-2/en/index.html. p. 115. 1832
84. Tabernero, P. and P.N. Newton, The WWARN Antimalarial Quality Surveyor. 1833
Pathogens and Global Health, 2012. 106(2): p. 77-78. 1834
85. World Health Organization, WHO guidelines for sampling of pharmaceutical products 1835
and related materials, in WHO Technical Report Series. 2005: 1836
http://apps.who.int/prequal/info_general/documents/TRS929/WHO_TRS_929-1837
Annex4.pdf. 1838
86. United States Pharmacopeia, Rapid Assessment of Medicines Quality Assurance and 1839
Medicines Quality Control. 2007, USP: 1840
http://www.usp.org/sites/default/files/usp_pdf/EN/dqi/rapidAssessmentTool.pdf. 1841
87. World Health Organization, WHO good practices for pharmaceutical quality control 1842
laboratories, in WHO Technical Report Series. 2010: 1843
http://apps.who.int/prequal/info_general/documents/TRS957/GPCL_TRS957_Annex11844
.pdf. 1845
88. Organization, W.H., Considerations for requesting analysis of drug samples, in WHO 1846
Technical Report Series,. 2002: 1847
http://apps.who.int/prequal/info_general/documents/TRS902/WHO_TRS_902-1848
Annex4.pdf. 1849
89. Smith, R.M., et al., Fungal Infections Associated with Contaminated 1850
Methylprednisolone Injections. New England Journal of Medicine, 2013. 369(17): p. 1851
1598-1609. 1852
90. Fernandez, F.M., et al., Poor quality drugs: grand challenges in high throughput 1853
detection, countrywide sampling, and forensics in developing countries. Analyst, 1854
2011. 136(15): p. 3073-82. 1855
91. Kovacs, S., et al., Technologies for Detecting Falsified and Substandard Drugs in Low 1856
and Middle-Income Countries. PLoS ONE, 2014. 9(3): p. e90601. 1857
1858
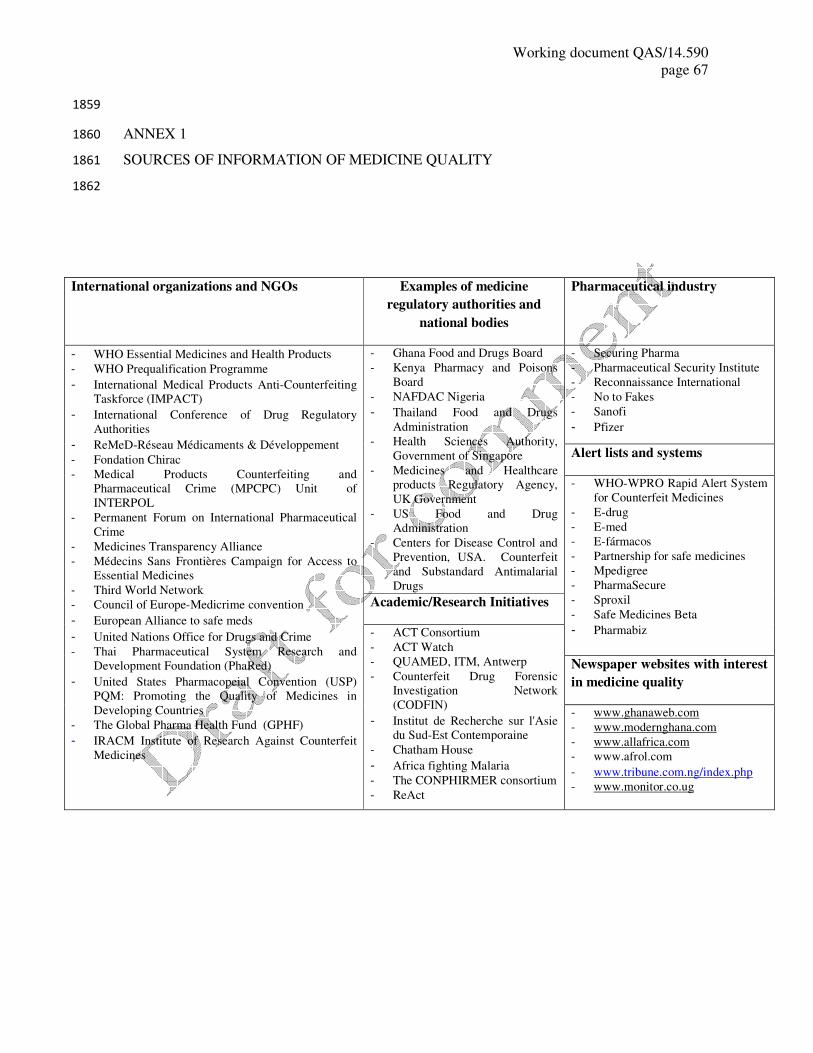
Working document QAS/14.590
page 67
1859
ANNEX 1 1860
SOURCES OF INFORMATION OF MEDICINE QUALITY 1861
1862
International organizations and NGOs Examples of medicine
regulatory authorities and
national bodies
Pharmaceutical industry
- WHO Essential Medicines and Health Products - WHO Prequalification Programme
- International Medical Products Anti-Counterfeiting
Taskforce (IMPACT)
- International Conference of Drug Regulatory
Authorities
- ReMeD-Réseau Médicaments & Développement - Fondation Chirac
- Medical Products Counterfeiting and
Pharmaceutical Crime (MPCPC) Unit of
INTERPOL
- Permanent Forum on International Pharmaceutical
Crime
- Medicines Transparency Alliance
- Médecins Sans Frontières Campaign for Access to
Essential Medicines
- Third World Network
- Council of Europe-Medicrime convention
- European Alliance to safe meds
- United Nations Office for Drugs and Crime - Thai Pharmaceutical System Research and
Development Foundation (PhaRed)
- United States Pharmacopeial Convention (USP)
PQM: Promoting the Quality of Medicines in
Developing Countries - The Global Pharma Health Fund (GPHF)
- IRACM Institute of Research Against Counterfeit
Medicines
- Ghana Food and Drugs Board
- Kenya Pharmacy and Poisons
Board
- NAFDAC Nigeria
- Thailand Food and Drugs
Administration - Health Sciences Authority,
Government of Singapore
- Medicines and Healthcare
products Regulatory Agency,
UK Government
- US Food and Drug
Administration
- Centers for Disease Control and
Prevention, USA. Counterfeit
and Substandard Antimalarial
Drugs
- Securing Pharma
- Pharmaceutical Security Institute
- Reconnaissance International
- No to Fakes
- Sanofi
- Pfizer
Alert lists and systems
- WHO-WPRO Rapid Alert System
for Counterfeit Medicines
- E-drug
- E-med
- E-fármacos
- Partnership for safe medicines
- Mpedigree
- PharmaSecure
- Sproxil
- Safe Medicines Beta
- Pharmabiz
Academic/Research Initiatives
- ACT Consortium
- ACT Watch
- QUAMED, ITM, Antwerp
- Counterfeit Drug Forensic
Investigation Network
(CODFIN)
- Institut de Recherche sur l'Asie
du Sud-Est Contemporaine - Chatham House
- Africa fighting Malaria - The CONPHIRMER consortium
- ReAct
Newspaper websites with interest
in medicine quality
- www.ghanaweb.com
- www.modernghana.com
- www.allafrica.com
- www.afrol.com
- www.tribune.com.ng/index.php
- www.monitor.co.ug
Working document QAS/14.590
page 68
ANNEX 2 1863
METHODOLOGY SECTION 1864
2.1 Random sampling and LQAS examples 1865
1866
(a) Random sampling 1867
For example, the investigators would like to determine the prevalence of outlets selling poor-1868
quality medicine of INN X in area Y. 1869
1870
We can estimate a sample size assuming a prevalence of poor-quality medicines of 50% (or p 1871
= 0.5). This choice of estimated prevalence will give us the most conservative (i.e. largest) 1872
sample size needed. To determine the actual prevalence of outlets selling falsified medicines 1873
with a precision of 5% (i.e. to within ±0.05; precision = 0.05 × 2 = 0.1) with 95% confidence 1874
intervals (z = 1.96) we would need a random sample size (n) of ~390 (n = 1875
4p(1−p)z2/precision2 = 4 × 0.5(1−0.5 ×(1.96)2/(0.1)2) (1). This means that purchases from 1876
390 different outlets selling medicine X would be required to obtain an objective estimate of 1877
the prevalence of those selling poor-quality medicine X at one time point in one area. Within 1878
each outlet the sampling of medicine units should follow one of strategies described in section 1879
8 and Annex 2.2 below. 1880
1881
Yamane (1967) (2) provides a simplified formula for random sampling that assumes a 95% 1882
confidence level and a prevalence of 50%: 1883
sample size = N/ (1+N (precision) 2
) 1884
where N = the total number of outlets selling medicine. 1885
1886
(b) LQAS 1887
For example, the investigators would like to determine whether the prevalence of outlets 1888
selling poor-quality medicine of INN X is less than 80% in area Y. 1889
1890
For LQAS sampling we may set our upper threshold to 95% and the lower threshold to 80%. 1891
This means that it is acceptable for 95% of outlets selling medicine X (the unit) in one district 1892
(the lot) in location Y to have good-quality medicines and unacceptable for less than 80% to 1893
have good-quality medicines. If we set the Type I error to 0.05 (i.e. there is a 5 in 100 chance 1894
that a district with 80% or fewer of the outlets selling good-quality drugs will go undetected) 1895

Working document QAS/14.590
page 69
and the Type II risk to 0.10 (i.e. there is a 10 in 100 chance that we will inappropriately direct 1896
resources to a district in which 95% or more of the outlets are in fact selling good-quality 1897
drugs). Our sample size would be 38 randomly selected outlets and the district would be 1898
considered unacceptable if more than four outlets had poor-quality medicine X (calculated 1899
using sample LQ (3, 4)). In other words, the null hypothesis that the district has at least 80% 1900
of its outlets selling good medicine X would be rejected if more than four out of 38 outlets 1901
sold poor-quality medicine X in area Y. 1902
2.2 Sampling techniques for the dosage units within medicine samples 1903
A binomial distribution assumes that the probability of selecting a positive unit does not 1904
change during the sampling process; in other words, the proportion of poor-quality samples in 1905
the population remains constant. This certainly would not be true when a sample would be 1906
selected from a small population. For example, for a population of 10 units with 5 poor-1907
quality units, the initial probability of selecting a poor-quality unit is 5/10 but changes to 4/9, 1908
3/8, etc., after one, two, three poor-quality units are drawn. For the probability to remain 1909
constant, the drawn unit would need to be returned to the population before the next draw – 1910
this type of drawing is called “sampling with replacement” and may only be relevant to very 1911
large populations when removing a few units from the population will change the proportion 1912
of positive units only negligibly. The hypergeometric distribution, in contrast, describes 1913
sampling without replacement and takes into account that the proportion of positive units 1914
change throughout the sampling process, so can be used for any population. The binomial 1915
distribution is a good approximation to the hypergeometric when the relative size of the 1916
drawn sample is small compared to the population. In practice, for samples <50 units the 1917
hypergeometric distribution should always be used. 1918
Assuming that the population of N units consists of N1 positive units and N2 negative units, 1919
the probability distribution allows estimation of the probability α of observing x positive (in 1920
this case poor-quality medicine) units in a random sample of size n if the proportion of poor-1921
quality units in the whole population of size N is k = N1/N. A sample size of n units that have 1922
to be analysed can be calculated such that if all units in that sample are poor quality (x=1) we 1923
can conclude with (1−α) 100% confidence that overall at least k100% of the units are positive, 1924
i.e. are poor-quality medicines, using the relationship between α, x, n, k and N defined by the 1925
distribution function. Similarly, the calculation can be done when it is expected that one or 1926
two units in the sample will be negatives (i.e. do not contain poor-quality medicines). In this 1927
Working document QAS/14.590
page 70
case, the number of units to be sampled will be significantly higher. To show that the 1928
population contains >5% of poor-quality units with 95% confidence, 3–5 units will need to be 1929
analysed for a population size 10–10 000, assuming they all test positive, while for >90% the 1930
required numbers of units to be sampled will vary between 8–29. When analysing essential 1931
medicines, if no poor-quality medicines are found it would be desirable to conclude that the 1932
proportion of poor antimalarials is sufficiently low, say below 1%. See calculation below. 1933
1934
Tables with the required number of samples to be tested for different scenarios and baset 1935
European Network of Forensic Sciences Institutes (ENFSI), for examples, see Appendix 2.6. 1936
The calculator for qualitative sampling of seize drugs is available at: 1937
http://www.enfsi.eu/documents/enfsi-dwg-calculator-qualitative-sampling-seized-drugs-2012 1938
1939
The choice of the numbers for α and k depend on laboratory guidelines, costs, legal 1940
requirements and the specific situation. The assumption that all sampled units contain poor- 1941
(or good-) quality medicines is often made based on previous surveys or experience in the 1942
field. 1943
1944
The LQAS methodology, which was described in the context of outlets sampling, can also be 1945
employed for dosage-unit sampling. The number of units to be sampled and analysed can be 1946
calculated in populations with a specified ≥ k100% poor-quality medicines with significance 1947
level α. This method ensures that populations with ≤ m100% will not be wrongly classified as 1948
populations with a high proportion of poor-quality medicines, with 80% power. 1949
1950
Rather than using a probability distribution to calculate the required number of units to be 1951
sampled a Bayesian approach may be used. The assumption of this approach is that the 1952
proportion of poor-quality medicines in a random sample is known and fixed but the 1953
proportion in the population is not known. A distinction can be made between sampling with 1954
replacement and sampling without replacement, as for the frequentist approach. Sampling 1955
with replacement is easier and can be used as an approximation for situations where the 1956
population size is at least 50 and the sample drawn is relatively small. Here an overestimate is 1957
not such a problem as with the binomial distribution. 1958
1959
Working document QAS/14.590
page 71
In the Bayesian approach, although the population proportion is not known, there may be 1960
some ideas about the size of this proportion. These ideas are represented by a probability 1961
distribution p (θ), the so-called “prior distribution” which expresses the uncertainty about the 1962
exact value of the proportion or our belief about what the size of the proportion may be 1963
(which may be based on previous studies). This uncertain knowledge is combined with the 1964
information provided by the sample and a so-called “posterior distribution” of the proportions 1965
is provided. With this posterior distribution it is possible to calculate directly the probability 1966
that the proportion of bad-quality drugs is at least k (given the sample results) without using 1967
tests or confidence intervals. With this approach it is possible to incorporate some knowledge 1968
about the total sample that you may possibly have. Sample size calculations can be conducted 1969
for more than 50 samples or less than 50 samples. 1970
1971
2.3 Sample size calculation for the dosage units within medicine samples 1972
The sample size n to be selected from a population of size N is calculated by testing the null-1973
hypothesis that the number of positives in the population, N1 is less than K against the 1974
alternative hypothesis that the number of positives is at least K: 1975
1976
Null hypothesis H0 : N1 < K 1977
Alternative hypothesis H1 : N1 ≥ K. 1978
1979
The null-hypothesis will be rejected when the number of positives in the sample selected is 1980
larger than a certain number. If this number is taken as the number of positives expected in 1981
the sample x then n should be selected such that the probability of observing more than x 1982
positives in that sample under the assumption of N1 positives in the whole population is very 1983
low, i.e. 1984
P(X ≥ x | N1 <K) ≤ α (1) 1985
Where α is the probability that the null-hypothesis is rejected when it is actually true and it is 1986
usually selected as 0.05 or 0.01. 1987
1988
Inequality (1) can be expressed as: 1989
∑ P�X = �|�� � − 1,�, �) ≤ α 1990
and solved for n using an appropriate formula for the probability P(X=i| K-1,N,n) that a 1991
sample of a given size contains a prespecified number of positives. Two such formulas are 1992

Working document QAS/14.590
page 72
listed below: for the hypergeometric distribution, which should be used for sampling with 1993
replacement, and the binomial distribution, for sampling without replacement. 1994
The number of units to be tested n can be derived for different values of N, K and α and these 1995
are shown in tables in section 2.5 below. 1996
Hypergeometric distribution 1997
The probability that a sample of size n contains X positives (units containing poor-quality 1998
drugs), given that the population of size N contains N1 positives, is calculated as: 1999
��� = �|��, �, �) = ���� ��
������� �
����
Where ���� =�!
����)!�! and is equal to the number of ways of selecting b units from a 2000
population of a units. 2001
Binomial distribution 2002
The probability that a sample of size n contains X positives (units containing bad quality 2003
drugs), given that the population of size N contains a proportion of θ =N1/N poor quality drugs, 2004
is calculated as: 2005
2006
��� = �|��, �, �) = ��! θ��1 − θ)���
Where ��! = �!����)!�! as before. 2007
2008
Working document QAS/14.590
page 73
2.4 Further statistical considerations 2009
2010
Data can be weighted at the analysis stage and survey settings can be incorporated to account 2011
for clustering of the outlets within the districts, provinces, regions. 2012
a) Booster sample: oversampling to ensure adequate representation of relatively rare but 2013
important outlet types (i.e. public health facilities operating in the district of the sampled 2014
area). 2015
b) Sampling weights: sample weights can be calculated for an outlet survey data to 2016
allow for: 2017
- differences in sampling probabilities due to variation in the size of strata; 2018
- the oversampling of the booster sample; 2019
c) the sampling strategy which involved a census of outlets in populations of varying 2020
size selected with probability proportional to size (PPS). Weights can be based on 2021
sampling probabilities (2). 2022
d) Clustering: sample can be clustered at the level of the district/province or communities. 2023
The calculation of standard errors takes this clustering into account because outlets in a 2024
given cluster are likely to be more similar to each other than to outlets in other clusters (5, 2025
6), i.e. sampling can be conducted using a one-stage probability proportion size (PPS) 2026
cluster design, with the measure of size being the relative commune population. Different 2027
zones can be calculated as different strata with approximately 10 000–15 000 inhabitants 2028
(7). 2029
e) Stratification: communities can be sampled separately in each stratum and this can also 2030
be adjusted for in the calculation of the standard error terms during analysis. The 2031
stratification of the sampling units by geographical, trade and socioeconomic variables 2032
can be conducted before the sample selection is conducted. Outlets vary greatly in type 2033
whether sampling should stratify the outlets in this way for analysis should be discussed 2034
during the survey planning. 2035
f) Lots: it may be necessary to specify lots (or defined areas) using predefined geographical 2036
boundaries (e.g. districts, provinces, communities, rural vs urban, etc.) and to vary 2037
thresholds to classify good and bad outcomes by area. While exact longitudinal changes 2038
in prevalence cannot be calculated strict thresholds may be useful for identifying areas 2039
with acceptable levels of good-quality medicines. 2040
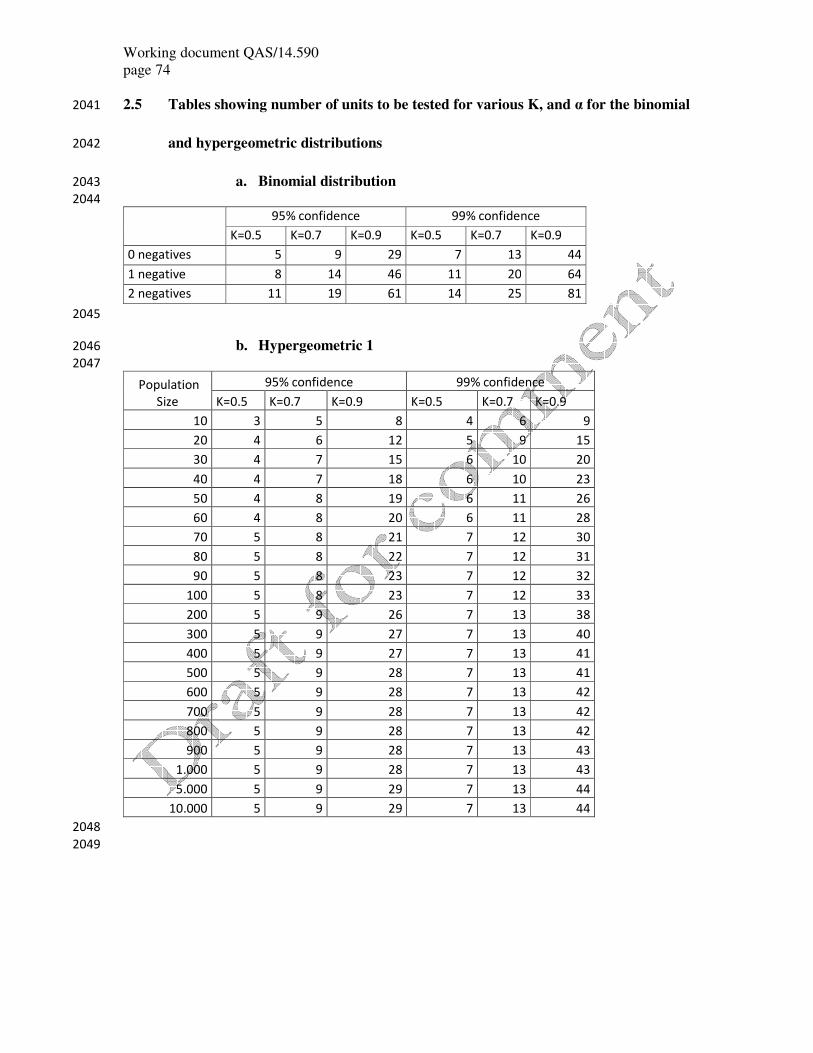
Working document QAS/14.590
page 74
2.5 Tables showing number of units to be tested for various K, and α for the binomial 2041
and hypergeometric distributions 2042
a. Binomial distribution 2043
2044
95% confidence 99% confidence
K=0.5 K=0.7 K=0.9 K=0.5 K=0.7 K=0.9
0 negatives 5 9 29 7 13 44
1 negative 8 14 46 11 20 64
2 negatives 11 19 61 14 25 81
2045
b. Hypergeometric 1 2046
2047
Population
Size
95% confidence 99% confidence
K=0.5 K=0.7 K=0.9 K=0.5 K=0.7 K=0.9
10 3 5 8 4 6 9
20 4 6 12 5 9 15
30 4 7 15 6 10 20
40 4 7 18 6 10 23
50 4 8 19 6 11 26
60 4 8 20 6 11 28
70 5 8 21 7 12 30
80 5 8 22 7 12 31
90 5 8 23 7 12 32
100 5 8 23 7 12 33
200 5 9 26 7 13 38
300 5 9 27 7 13 40
400 5 9 27 7 13 41
500 5 9 28 7 13 41
600 5 9 28 7 13 42
700 5 9 28 7 13 42
800 5 9 28 7 13 42
900 5 9 28 7 13 43
1.000 5 9 28 7 13 43
5.000 5 9 29 7 13 44
10.000 5 9 29 7 13 44
2048
2049

Working document QAS/14.590
page 75
2050
c. Hypergeometric 2 2051
2052
Population
Size
95% confidence 99% confidence
K=0.5 K=0.7 K=0.9 K=0.5 K=0.7 K=0.9
1 neg 2 neg 1 neg 2 neg 1 neg 2 neg 1 neg 2 neg 1 neg 2 neg 1 neg 2 neg
10 5 7 7 9 10 – 6 7 8 9 10 –
20 6 8 10 13 17 20 8 10 12 14 19 20
30 7 9 11 14 22 27 8 11 14 17 25 29
40 7 9 12 15 26 32 9 11 15 18 30 35
50 7 10 12 16 29 36 9 12 16 20 34 41
60 7 10 12 16 31 39 9 12 16 20 38 45
70 7 10 13 17 32 41 10 12 17 21 40 48
80 7 10 13 17 34 43 10 12 17 21 42 51
90 7 10 13 17 35 45 10 13 17 21 44 54
100 7 10 13 17 36 46 10 13 17 22 46 56
200 8 10 14 18 40 53 10 13 18 24 54 67
300 8 10 14 19 42 55 10 13 19 24 57 71
400 8 11 14 19 43 57 10 13 19 24 58 74
500 8 11 14 19 44 58 10 14 19 24 59 75
600 8 11 14 19 44 58 10 14 19 25 60 76
700 8 11 14 19 44 59 11 14 19 25 61 77
800 8 11 14 19 44 59 11 14 19 25 61 77
900 8 11 14 19 45 59 11 14 19 25 61 78
1.000 8 11 14 19 45 59 11 14 19 25 62 78
5.000 8 11 14 19 46 61 11 14 20 25 64 81
10.000 8 11 14 19 46 61 11 14 20 25 64 81
2053
2054
2055
2.6 Calculator for qualitative sampling of seized drugs. Developed by The European 2056
Network of Forensic Sciences Institutes (ENFSI) and available at: 2057
http://www.enfsi.eu/documents/enfsi-dwg-calculator-qualitative-sampling-seized-drugs-2012 2058
2059
Working document QAS/14.590
page 76
Software instructions
The software is a Microsoft Excel 2000 application. You will need to have the “Analysis
ToolPak” add-in installed (select: Tools/Add ins…/Analysis ToolPak). The “protection”
option (without a password) is enabled so that users may only enter data in specific required
cells. This protection option can be disabled if you wish to experiment with the package.
Older versions of Excel can only handle numbers up to about 1E+308. In such cases if a
number (either in a result or an intermediate calculation) exceeds this value then an overflow
error occurs and a “#NUM” error result is returned. Users must be aware of this when dealing
with large numbers. For example: (Excel 2000 version) 100 000 tablets, 0.99 confidence, k =
0.99, expected negatives = 2 will give an invalid result for the sample size. No laboratory
would ever use such unrealistic levels. However users should be aware of the limitations of
the software.
The graph is for display purposes only. The sample size scale is set from 1 to 100 as this
range will cover most results.
Hypergeometric sampling
1. The Excel sheet has five tabs at the bottom (Instructions, Hypergeometric, Bayesian,
Binomial and Estimation of Weight).
2. Select the Hypergeometric tab.
3. Enter the desired values for steps 1,2,3 & 4.
4. The required sample size will be given at step 5 (cell B5).
The Excel hypergeometric distribution function is used here as follows:
P = HYPGEOMDIST ((n-r), n, (N*k)-1, N)
This gives the probability of finding n-r positives in a sample of size n taken from a
population N containing (N*k)-1 positives.
In the case of 0 negatives expected (r = 0):
Working document QAS/14.590
page 77
If P gives the probability of finding n positives, then 1-P gives the probability of not finding
this number of positives.
In other words 1-P gives the probability of finding at least one negative. A sample size n is
chosen to give a value for 1-P which exceeds the desired confidence level (1-a).
NOTE 1
It may happen that a number of samples have been taken, assuming that there would be zero
negatives; however, upon analysis one of the samples appeared to be negative. What can then
be said about the proportion of the seizure that is positive for drugs? The macro can also
calculate this proportion. (Note: depending on the setting of your Excel program, points or
commas must be used for decimals)
Scenario:
Seizure of 1000 tablets
Proportion of positives = 0.9
Expected negatives = 0
Confidence level = 0.95
This requires a sample size of 28.
Suppose you have analysed these 28 tablets and found one negative. What proportion of the
seizure can you still be 0.95
confident to contain positives?
Step 1: Start at the begin position. Scroll down until sample size 28 is visible on the screen
(this has a current probability value of 0.951419384)
Step 2: Change the “expected negatives” value from 0 to 1.
(this will reduce the probability value for sample size 28 to 0.793866654)
Step 3: Reduce the value for “proportion of positives” continuously until the probability for
sample size 28 reaches
or exceeds 0.95 again (this happens when k=0.84)
Therefore we can be 95% confident that 84 % of the seizure contains positives.
Working document QAS/14.590
page 78
NOTE 2
The HPD calculations are based on whole numbers only. Therefore, if certain entries (or the
result of some intermediate calculations) are not whole numbers the software will round the
values down to the nearest whole number. This may produce some anomalies in sample size,
especially with low population numbers.
e.g. for a small population of, say 12 tablets (with k = 0.5 and 1-α = 0.99), the calculated
sample size is 5 whereas if the population increases to 13, the sample size reduces to 4. In the
latter case (with k = 0.5) the number of positives in the population is calculated by the
software to be 13 * 0.5 = 6.5 tablets. Obviously HPD cannot use the value of 6.5 tablets in its
calculations and therefore the value is rounded down to 6. This is why the sample size is
reduced here because HPD is calculating the probability of finding at least one negative when
there are only 6 positive tablets (instead of 6.5) in a population of 13 (in reality the rounding
process in this case has changed the value of k from 0.5 to 0.46).
Bayesian sampling
1. Select the Bayesian tab.
2. Enter the desired values for steps 1, 2, 3, 4, 5 and 6.
Note 1: Although population size is not used in the calculations for the beta distribution, it
is necessary to enter
the population size so that the software can decide whether to use beta or beta-binomial
distribution in the calculations.
Note 2: The values selected for steps 2 and 3 (a & b values) will depend on the analyst’s
prior knowledge or assumptions about θ.
3. The required sample size will be given at step 7 (cell B7).
N >= 50
The Excel beta distribution function is used here as follows:
P(θ>k)=BETADIST (k, a+(n-r), b+r, lower limit for k, upper limit for k).
N <50

Working document QAS/14.590
page 79
The Γ(x) function can be calculated in Excel by using a combination of the EXP and
GAMMALN worksheet
functions as follows:
GAMMALN(x) = LN(Γ(x))
The EXP function is the inverse of the LN function therefore:
EXP(GAMMALN(x)) = Γ(x)
This function is incorporated into the beta-binomial distribution equation as follows:
P(Y>=y)=
( EXP(GAMMALN(n+a+b))*COMBIN(N-n,y) * EXP(GAMMALN(y+x+a)) *
EXP(GAMMALN(N-x-y+b) )
/ ( EXP(GAMMALN(x+a) * EXP(GAMMALN(n-x+b)) * EXP(GAMMALN(N+a+b) )
Binomial sampling
1. Select the Binomial tab.
2. Enter the desired values for steps 1,2 &3.
3. The required sample size will be given at step 4 (cell B4).
The Excel binomial distribution function is used here as follows:
P = BINOMDIST (n-r, n, k, FALSE)
Estimation of weights
1. Select the Estimation of Weight tab.
2. Enter the required values for steps 1 to 6.
3. The confidence interval is given in cells B12: D12
The confidence interval is calculated as follows:
C.I. = mean weight ± t*s/ √(n-r)
Working document QAS/14.590
page 80
In the event of any negatives being detected in the samples, a correction factor (n-r)/n is
applied as follows:
C.I. = (mean weight) * (n-r)/n ± (t*s/ √(n-r)) * (n-r)/n
For smaller populations where n/N > 0.1 a further correction factor √((N-n)/N) is
applied giving:
C.I. = (mean weight) * (n-r)/n ± (t*s/ √n-r) * (n-r)/n* √((N-n)/N)
Estimation of tablet numbers
1. Select the Estimation of Tablets tab.
2. Enter the required values for steps 1 to 5.
3. The estimated number of tablets is given in cell B9
2060
2061
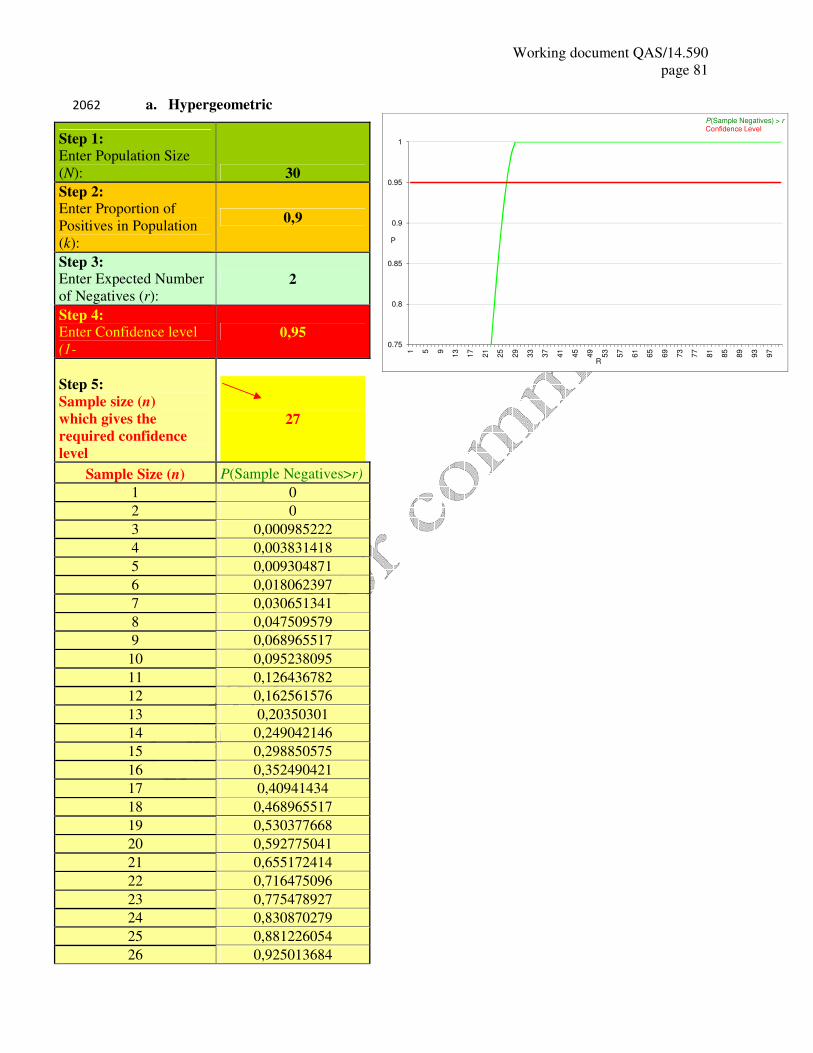
Working document QAS/14.590
page 81
a. Hypergeometric 2062
Step 1: Enter Population Size
(N): 30
Step 2: Enter Proportion of
Positives in Population
(k):
0,9
Step 3: Enter Expected Number
of Negatives (r): 2
Step 4: Enter Confidence level
(1-�� 0,95
Step 5:
Sample size (n)
which gives the
required confidence
level
27
Sample Size (n) P(Sample Negatives>r)
1 0
2 0 3 0,000985222
4 0,003831418
5 0,009304871
6 0,018062397
7 0,030651341 8 0,047509579
9 0,068965517
10 0,095238095
11 0,126436782
12 0,162561576 13 0,20350301
14 0,249042146
15 0,298850575
16 0,352490421
17 0,40941434 18 0,468965517
19 0,530377668
20 0,592775041
21 0,655172414
22 0,716475096 23 0,775478927
24 0,830870279
25 0,881226054
26 0,925013684
0.75
0.8
0.85
0.9
0.95
1
1 5 9
13
17
21
25
29
33
37
41
45
49
53
57
61
65
69
73
77
81
85
89
93
97
P
R
P(Sample Negatives) > r
Confidence Level
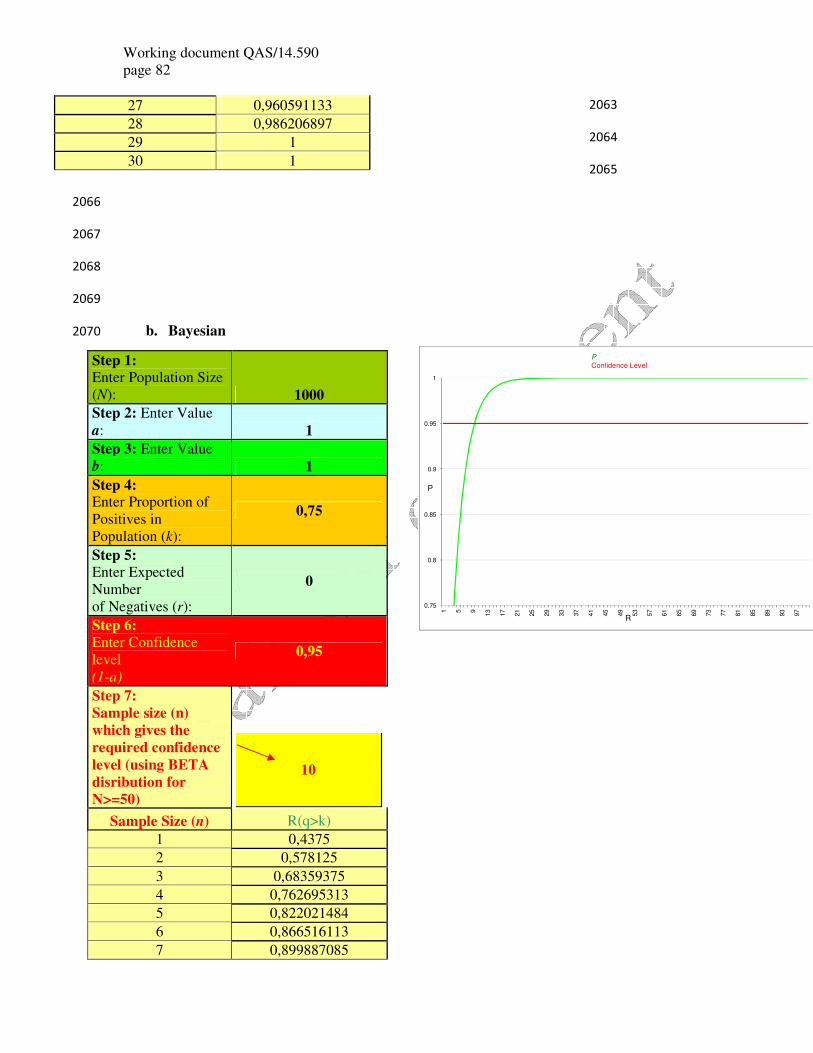
Working document QAS/14.590
page 82
2063
2064
2065
2066
2067
2068
2069
b. Bayesian 2070
Step 1: Enter Population Size
(N): 1000
Step 2: Enter Value
a: 1
Step 3: Enter Value
b: 1 Step 4:
Enter Proportion of
Positives in
Population (k):
0,75
Step 5: Enter Expected
Number
of Negatives (r):
0
Step 6: Enter Confidence
level
(1-a)
0,95
Step 7:
Sample size (n)
which gives the
required confidence
level (using BETA
disribution for
N>=50)
10
Sample Size (n) R(q>k) 1 0,4375
2 0,578125
3 0,68359375
4 0,762695313
5 0,822021484 6 0,866516113
7 0,899887085
27 0,960591133
28 0,986206897 29 1
30 1
0.75
0.8
0.85
0.9
0.95
1
1 5 9
13
17
21
25
29
33
37
41
45
49
53
57
61
65
69
73
77
81
85
89
93
97
P
R
P
Confidence Level
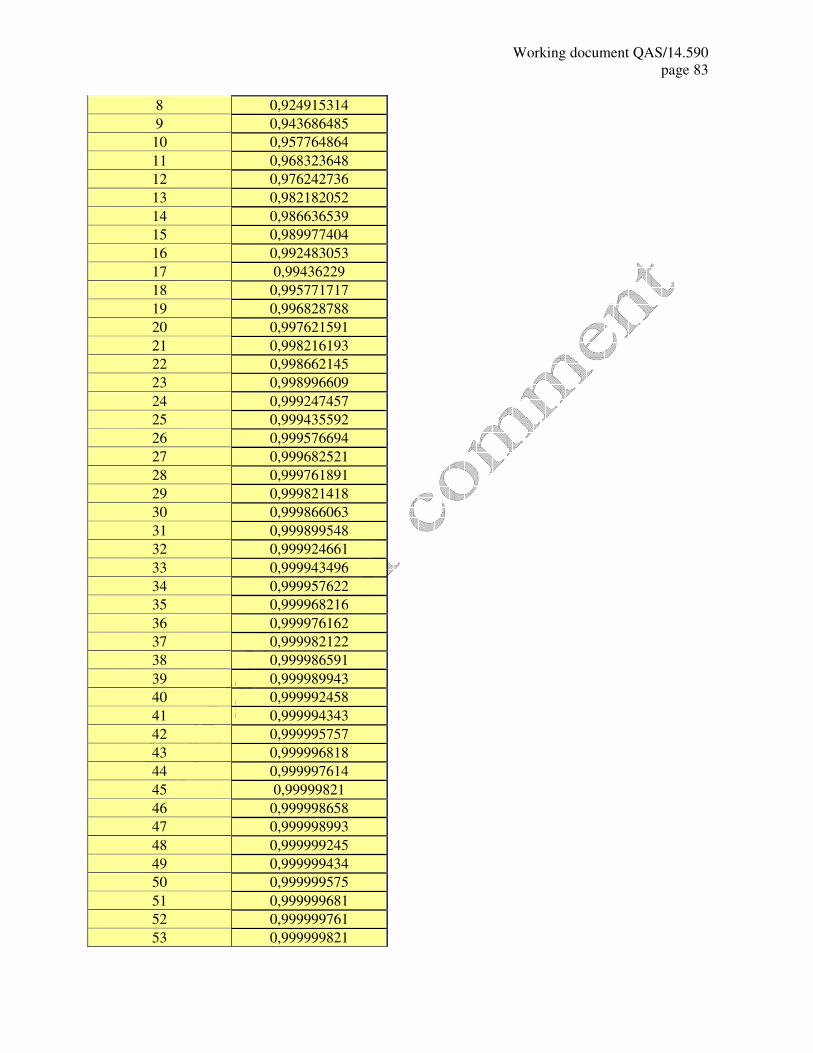
Working document QAS/14.590
page 83
8 0,924915314
9 0,943686485
10 0,957764864 11 0,968323648
12 0,976242736
13 0,982182052
14 0,986636539
15 0,989977404 16 0,992483053
17 0,99436229
18 0,995771717
19 0,996828788
20 0,997621591 21 0,998216193
22 0,998662145
23 0,998996609
24 0,999247457
25 0,999435592 26 0,999576694
27 0,999682521
28 0,999761891
29 0,999821418
30 0,999866063 31 0,999899548
32 0,999924661
33 0,999943496
34 0,999957622
35 0,999968216 36 0,999976162
37 0,999982122
38 0,999986591
39 0,999989943
40 0,999992458 41 0,999994343
42 0,999995757
43 0,999996818
44 0,999997614
45 0,99999821 46 0,999998658
47 0,999998993
48 0,999999245
49 0,999999434
50 0,999999575 51 0,999999681
52 0,999999761
53 0,999999821
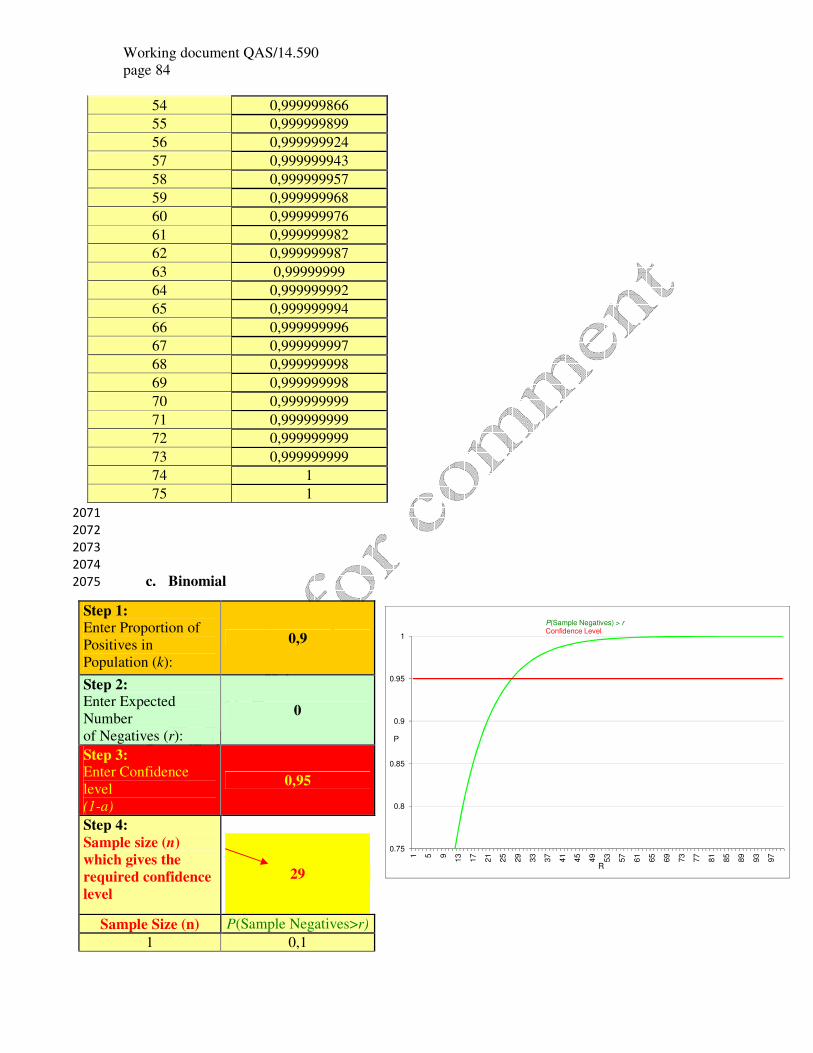
Working document QAS/14.590
page 84
54 0,999999866
55 0,999999899 56 0,999999924
57 0,999999943
58 0,999999957
59 0,999999968
60 0,999999976 61 0,999999982
62 0,999999987
63 0,99999999
64 0,999999992
65 0,999999994 66 0,999999996
67 0,999999997
68 0,999999998
69 0,999999998
70 0,999999999 71 0,999999999
72 0,999999999
73 0,999999999
74 1
75 1 2071
2072
2073
2074
c. Binomial 2075
Step 1: Enter Proportion of
Positives in
Population (k):
0,9
Step 2: Enter Expected
Number
of Negatives (r):
0
Step 3: Enter Confidence
level
(1-a)
0,95
Step 4:
Sample size (n)
which gives the
required confidence
level
29
Sample Size (n) P(Sample Negatives>r)
1 0,1
0.75
0.8
0.85
0.9
0.95
1
1 5 9
13
17
21
25
29
33
37
41
45
49
53
57
61
65
69
73
77
81
85
89
93
97
P
R
P(Sample Negatives) > rConfidence Level

Working document QAS/14.590
page 85
2 0,19
3 0,271
4 0,3439 5 0,40951
6 0,468559
7 0,5217031
8 0,56953279
9 0,612579511
10 0,65132156 11 0,686189404 12 0,717570464
13 0,745813417
14 0,771232075
15 0,794108868
16 0,814697981
17 0,833228183 18 0,849905365
19 0,864914828
20 0,878423345
21 0,890581011
22 0,90152291
23 0,911370619
24 0,920233557 25 0,928210201
26 0,935389181
27 0,941850263
28 0,947665237
29 0,952898713
30 0,957608842 31 0,961847958 32 0,965663162
33 0,969096846
34 0,972187161
35 0,974968445
36 0,9774716
37 0,97972444 38 0,981751996 39 0,983576797
40 0,985219117
41 0,986697205
42 0,988027485
43 0,989224736
44 0,990302263 45 0,991272036
46 0,992144833
47 0,99293035
48 0,993637315
49 0,994273583
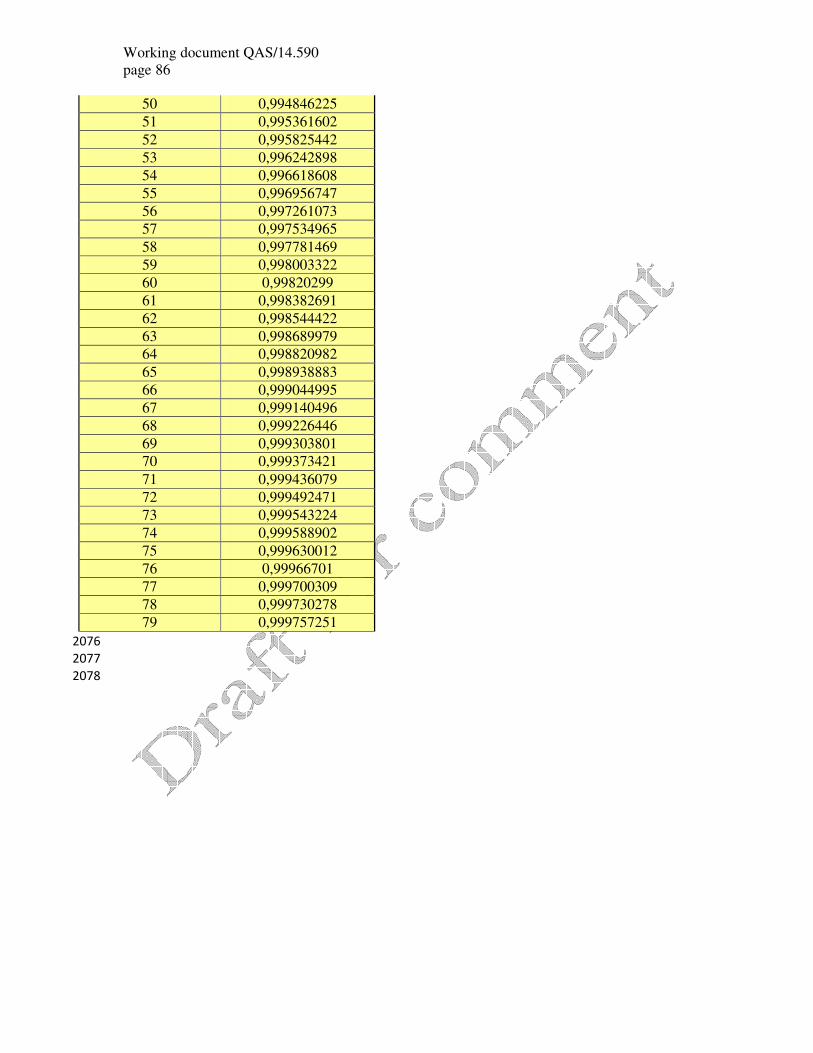
Working document QAS/14.590
page 86
50 0,994846225
51 0,995361602
52 0,995825442 53 0,996242898
54 0,996618608
55 0,996956747
56 0,997261073
57 0,997534965
58 0,997781469 59 0,998003322 60 0,99820299
61 0,998382691
62 0,998544422
63 0,998689979
64 0,998820982
65 0,998938883 66 0,999044995
67 0,999140496
68 0,999226446
69 0,999303801
70 0,999373421
71 0,999436079
72 0,999492471 73 0,999543224
74 0,999588902
75 0,999630012
76 0,99966701
77 0,999700309
78 0,999730278 79 0,999757251 2076
2077
2078

Working document QAS/14.590
page 87
2079
d. Estimation of weight 2080
Step 1: Enter Confidence level (1-a) 0,95 a= 0,05
Step 2: Enter Population (N) 100 t= 2,086
Step 3: Enter Sample Size (n) 23 n/N= 0,230
Step 4: Enter Mean Weight (x-bar) 0,265 Q= 0,877
Step 5: Enter Sample Standard
Deviation (s) 0,023 rsd(%) = 8,7
Step 6: Enter Number of Negative
Results in Sample ( r ) 2 P= 0,913043478
Confidence Interval = 0,24196 ± 0,008
Estimate of Weight = 24,196 ± 0,839
2081
2082
e. Estimation of tablets 2083
Step 1: Enter Total Weight of Tablets
(grams): 1027,1
Step 2: Enter Number of Individual
Weighings (n): 10
Step 3: Enter the Number of Tablets per
Individual Weighing: 50
Step 4: Enter Mean Weight
of Individual Weighings (grams): 14,772
Estimated Number of Tablets = 3476 Tablets
2084
2085
Working document QAS/14.590
page 88
REFERENCES 2086
2087
1. Machin David, et al., Sample Size Tables for Clinical Studies, Second Edition. 1997: 2088
Blackwell Science, Oxford, UK. 2089
2. Phanouvong, S., The Quality of Antimalarial Medicines in Western Cambodia: A Case 2090
Study Along the Thai-Cambodian Border Southeast Asian J Trop Med Public Health, 2091
2013. 44(3): p. 349-362. 2092
3. Brixton Health, Sample LQ. 2008: http://www.brixtonhealth.com/samplelq.html. 2093
4. Valadez, J.J., Assessing child survival programs in developing countries : testing lot 2094
quality assurance sampling, Population and International Health Harvard School of 2095
Public Health, Editor. 1991, Harvard University Press,: 2096
http://trove.nla.gov.au/work/34476731?selectedversion=NBD8721131. 2097
5. North Carolina Center for Public Health Preparedness, Two-Stage Cluster Sampling: 2098
General Guidance for Use in Public Heath Assessments, in Introduction to Cluster 2099
Sampling, P.H.R.S.T. 5, Editor.: http://nciph.sph.unc.edu/cha-learning-2100
congress/TwoStageClusterSampling.pdf. 2101
6. World Health Organization, Cluster sampling to assess immunization coverage: a 2102
review of experience with a simplified sampling method, in Bulletin of the World 2103
Health Organization. 1982: http://whqlibdoc.who.int/bulletin/1982/Vol60-2104
No2/bulletin_1982_60%282%29_253-260.pdf. p. 25-260. 2105
7. ACTwatch, Outlet Survey. Kingdom of Cambodia. 2011 Survey Report, in Outlet 2106
Survey Report (Endline), Cambodia, 06/11 – 08/11, P.S. Kathryn O’Connell, Editor. 2107
2011, ACTwatch. Evidence for Malaria Medicines Policy: 2108
http://www.actwatch.info/sites/default/files/content/outlet-2109
reports/ACTwatch%20Cambodia%20OS%20Endline_2011.pdf. p. 78. 2110
2111
2112
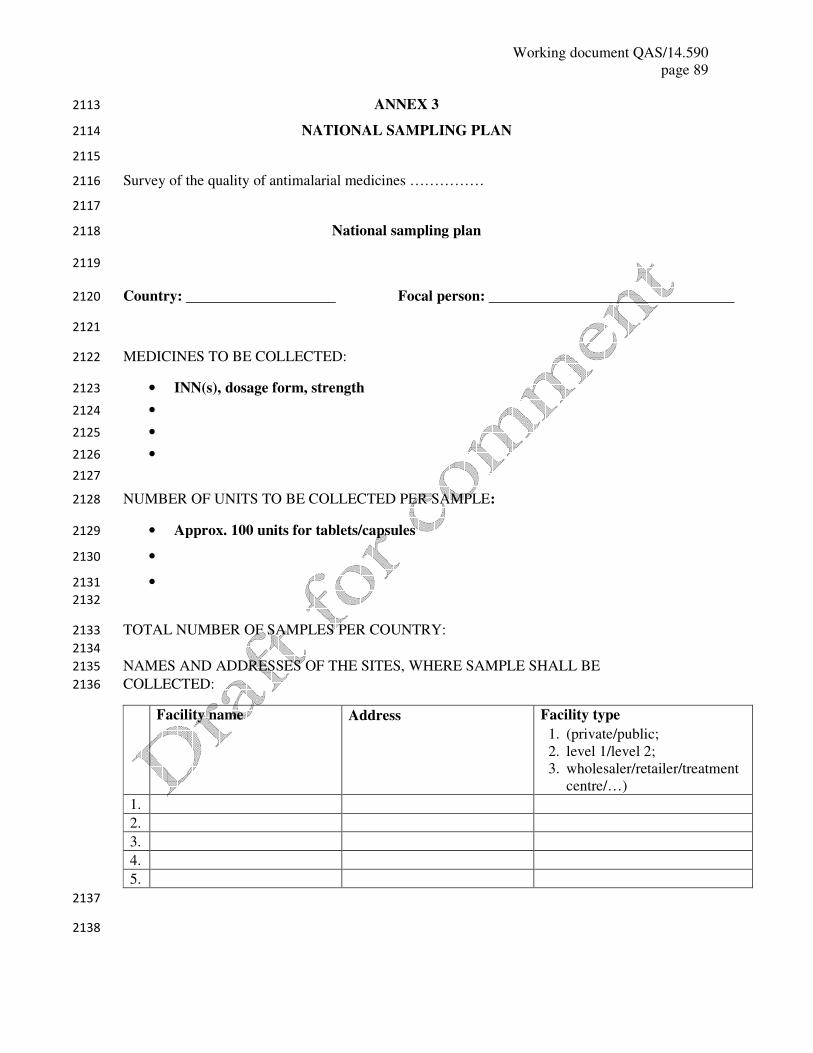
Working document QAS/14.590
page 89
ANNEX 3 2113
NATIONAL SAMPLING PLAN 2114
2115
Survey of the quality of antimalarial medicines …………… 2116
2117
National sampling plan 2118
2119
Country: Focal person: 2120
2121
MEDICINES TO BE COLLECTED: 2122
• INN(s), dosage form, strength 2123
• 2124
• 2125
• 2126
2127
NUMBER OF UNITS TO BE COLLECTED PER SAMPLE: 2128
• Approx. 100 units for tablets/capsules 2129
• 2130
• 2131
2132
TOTAL NUMBER OF SAMPLES PER COUNTRY: 2133
2134
NAMES AND ADDRESSES OF THE SITES, WHERE SAMPLE SHALL BE 2135
COLLECTED: 2136
Facility name Address Facility type
1. (private/public;
2. level 1/level 2;
3. wholesaler/retailer/treatment
centre/…)
1.
2.
3.
4.
5.
2137
2138
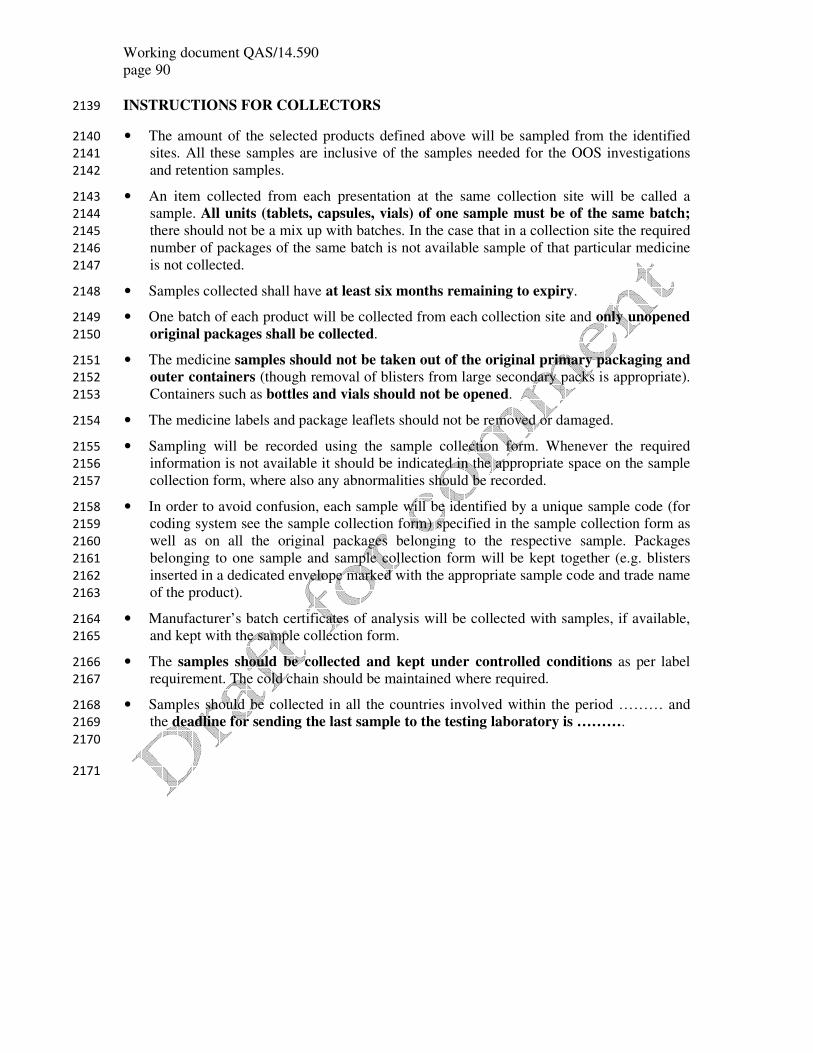
Working document QAS/14.590
page 90
INSTRUCTIONS FOR COLLECTORS 2139
• The amount of the selected products defined above will be sampled from the identified 2140
sites. All these samples are inclusive of the samples needed for the OOS investigations 2141
and retention samples. 2142
• An item collected from each presentation at the same collection site will be called a 2143
sample. All units (tablets, capsules, vials) of one sample must be of the same batch; 2144
there should not be a mix up with batches. In the case that in a collection site the required 2145
number of packages of the same batch is not available sample of that particular medicine 2146
is not collected. 2147
• Samples collected shall have at least six months remaining to expiry. 2148
• One batch of each product will be collected from each collection site and only unopened 2149
original packages shall be collected. 2150
• The medicine samples should not be taken out of the original primary packaging and 2151
outer containers (though removal of blisters from large secondary packs is appropriate). 2152
Containers such as bottles and vials should not be opened. 2153
• The medicine labels and package leaflets should not be removed or damaged. 2154
• Sampling will be recorded using the sample collection form. Whenever the required 2155
information is not available it should be indicated in the appropriate space on the sample 2156
collection form, where also any abnormalities should be recorded. 2157
• In order to avoid confusion, each sample will be identified by a unique sample code (for 2158
coding system see the sample collection form) specified in the sample collection form as 2159
well as on all the original packages belonging to the respective sample. Packages 2160
belonging to one sample and sample collection form will be kept together (e.g. blisters 2161
inserted in a dedicated envelope marked with the appropriate sample code and trade name 2162
of the product). 2163
• Manufacturer’s batch certificates of analysis will be collected with samples, if available, 2164
and kept with the sample collection form. 2165
• The samples should be collected and kept under controlled conditions as per label 2166
requirement. The cold chain should be maintained where required. 2167
• Samples should be collected in all the countries involved within the period ……… and 2168
the deadline for sending the last sample to the testing laboratory is ………. 2169
2170
2171

Working document QAS/14.590
page 91
ANNEX 4 2172
SAMPLE COLLECTION FORM 2173
2174
Survey of the quality of medicines …………… 2175
Sample collection form* 2176
Country: Sample code: 2177
(Country code/product abbreviation/sequence 2178
number/sampling date ddmmyy)** 2179
Name of location/place where sample was taken: 2180
2181
Address (with telephone, fax number and email address, if applicable): 2182
2183
2184
Organization and names of people who took samples: 2185
1. 2186
2. 2187
Product name of the sample: 2188
Name of active pharmaceutical ingredient(s) (INN) with strength: 2189
2190
Dosage form (tablet, capsule, powder for injection, etc.): 2191
Package size, type and packaging material of the container: 2192
2193
Batch/lot number: 2194
Date of manufacture: Expiry date: 2195
Regulatory status in the country, registration number, if applicable: 2196
2197
Name and address of the manufacturer: 2198
2199
* This sample collection form should always be kept with the sample collected. Proper sampling procedures
should be followed.
** Product abbreviations: …….. . Sample code system can be extended to be appropriate for a particular country
collection system.
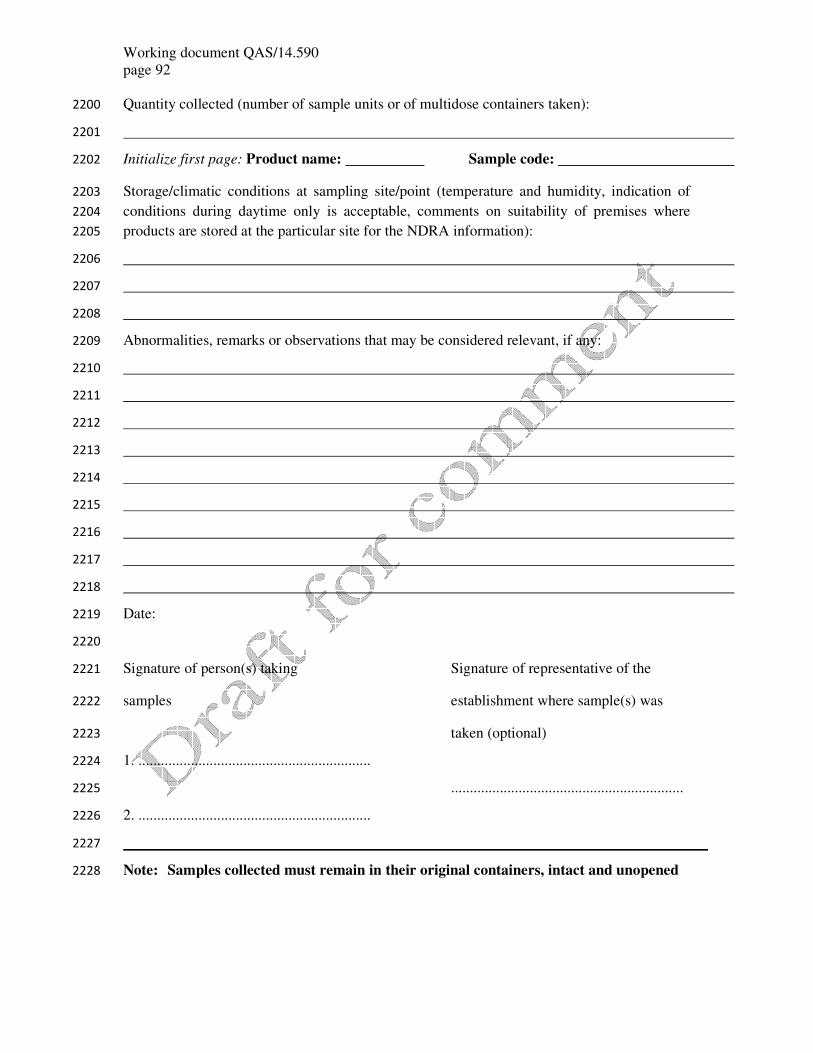
Working document QAS/14.590
page 92
Quantity collected (number of sample units or of multidose containers taken): 2200
2201
Initialize first page: Product name: Sample code: 2202
Storage/climatic conditions at sampling site/point (temperature and humidity, indication of 2203
conditions during daytime only is acceptable, comments on suitability of premises where 2204
products are stored at the particular site for the NDRA information): 2205
2206
2207
2208
Abnormalities, remarks or observations that may be considered relevant, if any: 2209
2210
2211
2212
2213
2214
2215
2216
2217
2218
Date: 2219
2220
Signature of person(s) taking Signature of representative of the 2221
samples establishment where sample(s) was 2222
taken (optional) 2223
1. .............................................................. 2224
.............................................................. 2225
2. .............................................................. 2226
2227
Note: Samples collected must remain in their original containers, intact and unopened 2228

Working document QAS/14.590
page 93
ANNEX 5 2229
SOP FOR MYSTERY SHOPPER METHODOLOGY 2230
2231
SOP. No. 1 Mystery shopper
Date of issue
Prepared by: Review by: Approved by:
Version no.
2232
I. Objective 2233
Investigate the quality of medicines……………………………………. in the private and/or public sectors in 2234
location …………………………sold to patients. 2235
2236
Key outcomes will be: 2237
1. What medicines were offered to mystery shoppers at registered and unregistered outlets? 2238
2. Proportion of outlets selling monotherapy? 2239
3. What is the chemical quality of these medicines? 2240
4. Has the prevalence of counterfeit and substandard medicines changed since the …………. year survey? 2241
2242
II. Rationale 2243
The study ……………………. funded quality study is planned to be conducted 2244
in ……………………………………..provinces in the country……………………………..starting 2245
on ………………………………... One urban and one rural district will be selected by random number tables in 2246
each of the ………………………..study provinces. Collection of medicines will be conducted through separate 2247
mystery-shopper (MS) methodology. 2248
2249
III. Requirements 2250
Equipments Consumables Documents/ register
- Phone
- one laptop computer with
- Microsoft Office and Epidata
- Hard boxes to keep the drugs
- Safe box for field money
- Fuel
- Phone credit
- Zip bags to collect
drugs
- Notebook
- Pens
- Marker pen
- Provincial health
Department
- Diary/scheduling
sheet
- Printed SOPs
2251
2252

Working document QAS/14.590
page 94
IV. Procedure 2253
The team will be composed of a coordinator, ………………senior staff, ………………….. assistant 2254
and ………………… driver. The assistants will purchase the anti-infective medicines from all outlets identified 2255
in the selected districts. Lists of pharmacies and shops in the selected areas will be provided by government 2256
authorities. Provincial and district staff will assist with updating the lists of pharmacies and shops that sold 2257
medicines. 2258
Mystery shopper 2259 2260
A MS, dressed as a worker, will visit the outlets. He/she will state: “I would like to buy some drugs for my 2261
friend – we are travelling and work in construction – may I see which ones you have so I can choose?” 2262
When the MS is offered medicine(s), the MS will ask “Do you have any other makes, please ?” 2263
Twenty tablets of each preparation and five vials of parenteral medicines will be requested. After visiting each 2264
outlet the research coordinator will debrief the MS, using a debriefing form including feedback about his/her 2265
experience and challenges with the study methodology and how these were overcome and could be improved. 2266
List of medicines 2267
Artemether-lumefantrine (tabs) 2268
Artesunate (tabs) 2269
Artesunate (iv/im) 2270
Artemether (im) 2271
Chloroquine (tablet or capsule, syrup) 2272
Chloroquine (im) 2273
Mefloquine (tabs) 2274
Quinine (tablet or capsule) 2275
Quinine (iv/im) 2276
Sulphadoxine-pyrimethamine (tabs) 2277
Dihydroartemisinin-piperaquine (tabs) 2278
2279
V. Sample labelling 2280
Samples will stored in zip lock plastic bags and labelled with the date of collection, the place of collection 2281
(provider/outlet identified by a unified ID code) and the name of the collector. Samples will be kept in a foam 2282
box and sent to ………………………………as early as possible for storage at + 4C in a refrigerator. 2283
2284
VI. Data analysis 2285
All information will be double entered in a pre-established Epi-Data database. It will be analysed in Stata. 2286
2287
VII. Conducting MS 2288
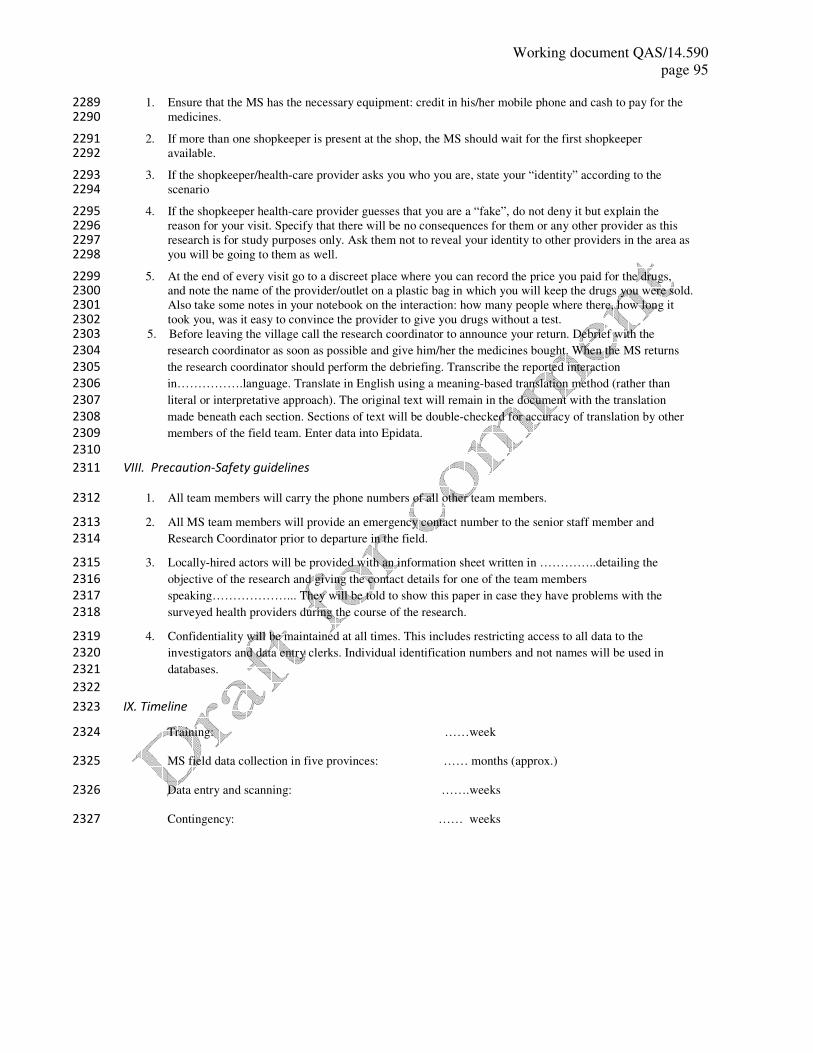
Working document QAS/14.590
page 95
1. Ensure that the MS has the necessary equipment: credit in his/her mobile phone and cash to pay for the 2289 medicines. 2290
2. If more than one shopkeeper is present at the shop, the MS should wait for the first shopkeeper 2291 available. 2292
3. If the shopkeeper/health-care provider asks you who you are, state your “identity” according to the 2293 scenario 2294
4. If the shopkeeper health-care provider guesses that you are a “fake”, do not deny it but explain the 2295 reason for your visit. Specify that there will be no consequences for them or any other provider as this 2296 research is for study purposes only. Ask them not to reveal your identity to other providers in the area as 2297 you will be going to them as well. 2298
5. At the end of every visit go to a discreet place where you can record the price you paid for the drugs, 2299 and note the name of the provider/outlet on a plastic bag in which you will keep the drugs you were sold. 2300 Also take some notes in your notebook on the interaction: how many people where there, how long it 2301 took you, was it easy to convince the provider to give you drugs without a test. 2302
5. Before leaving the village call the research coordinator to announce your return. Debrief with the 2303
research coordinator as soon as possible and give him/her the medicines bought. When the MS returns 2304
the research coordinator should perform the debriefing. Transcribe the reported interaction 2305
in…………….language. Translate in English using a meaning-based translation method (rather than 2306
literal or interpretative approach). The original text will remain in the document with the translation 2307
made beneath each section. Sections of text will be double-checked for accuracy of translation by other 2308
members of the field team. Enter data into Epidata. 2309
2310
VIII. Precaution-Safety guidelines 2311
1. All team members will carry the phone numbers of all other team members. 2312
2. All MS team members will provide an emergency contact number to the senior staff member and 2313
Research Coordinator prior to departure in the field. 2314
3. Locally-hired actors will be provided with an information sheet written in …………..detailing the 2315
objective of the research and giving the contact details for one of the team members 2316
speaking………………... They will be told to show this paper in case they have problems with the 2317
surveyed health providers during the course of the research. 2318
4. Confidentiality will be maintained at all times. This includes restricting access to all data to the 2319
investigators and data entry clerks. Individual identification numbers and not names will be used in 2320
databases. 2321
2322
IX. Timeline 2323
Training: ……week 2324
MS field data collection in five provinces: …… months (approx.) 2325
Data entry and scanning: …….weeks 2326
Contingency: …… weeks 2327
Working document QAS/14.590
page 96
ANNEX 6 2328
SOP FOR OVERT SAMPLING METHODOLOGY 2329
2330
SOP. No. 2 Overt sampling
Date of issue:
Prepared by: Review by: Approved by:
Version no.
2331
I. Objective 2332
To undertake ………………..medicine sampling in all private providers of the ………………study site 2333
in ……………………country 2334
The overt medicine survey will cover all private providers of medicines within the study catchment areas, 2335
including registered providers in …………..district and ……………………..town, village health volunteers 2336
in………………district villages and unregistered outlets. This will include private clinics, pharmacies, general 2337
shops, drug sellers and mobile providers, excluding providers using only traditional drugs and diagnostics. 2338
Key outcomes will be: 2339
1. What medicines are offered to overt collectors at registered, unregistered outlets and by VHV? 2340 2. Proportion of outlets selling monotherapy. 2341 3. What is the chemical quality of these antimalarials? 2342
2343
II. Rationale 2344
2345
The purpose of this study is to investigate the quality of ……………………………………. in 2346
the ………………..study sites in country…………………………... 2347
The study will be conducted in one phase were an overt sampling will be conducted in the providers of the study 2348
area. 2349
III. Requirements 2350
2351
Equipment Consumables Documents/register
- GPS
- Car
- Phone
- Identification badge
- Bag for documents
- Watch or clock
- Fuel
- Phone credit
- Notebook
- Pens/Pencil
- Clipboard
- Batteries for GPS
- Ziplock bag
- Labels
- Information letter for
VHV
- Diary/scheduling sheet
- 25 copies of overt
sampling forms and
SOPS
- Information sheets and
consent form
2352
Working document QAS/14.590
page 97
IV. Procedure 2353
2354
1. Outlet survey. This section is designed to identify the type of each outlet in the survey. Doing so will 2355
provide an assessment of the numbers and types of outlet in which people procure antimalarials. 2356
2. Obtaining consent form. This section ensures that providers understand the purpose of this study and 2357
their role in it, should they voluntarily consent to be part of the study. It also screens outlets that are not 2358
eligible to be surveyed out. 2359
2360
V. Inclusion criteria 2361
2362
Providers selling ……………………………….drugs in ………………………… or …………………………. 2363
town. 2364
2365
VI. Data collection tools 2366
2367
Data collection will be done using the …………………….. form 2368
2369
VII. Data entry 2370
2371
Data will be double entered into a predesigned database that will be linked to subsequent data using the unique 2372
ID code. 2373
2374
VIII. Conducting private providers census 2375
2376
1. The primary sampling unit is ……………………. town and …………………… province. Prepare a 2377
scheduling sheet where survey will take place. 2378
2. Obtain list of known outlets. This will be supplemented by additional information when you are in the 2379
field. 2380
3. Ensure you have necessary equipment, consumables and documents. 2381
4. Coordinator and supervisors should identify a number of potential key informants who can guide them 2382
to the other unregistered and mobile providers, including local health officials, community leaders, 2383
villagers and other key informants. 2384
5. Through discussion with these key informants, the supervisor should write a full list of potential 2385
medicine providers in their area. 2386
6. Each member of the study team should then be allocated an area for sampling. 2387
2388
2389
Working document QAS/14.590
page 98
Conducting the census 2390
1. Before going to each first shop, fill in the details in Section A. The first outlet code should be “01” , the 2391
next one “02”, etc. Remember to fill in the ID code at the top of the form. 2392
2. Start walking! 2393
3. At the shop the surveyor should him/ herself, followed by a brief summary of what the project is all 2394
about and why the private provider is asked to participate in the study. Explain that you are involved in 2395
the ……………………………… project which is about improving the usage ……………… in private 2396
providers in ………………………. Explain that you are collecting information from all private 2397
providers in that area. Ask the screening questions. 2398
4. If there is more than one person in the shop introduce yourself to the one who serves customers first and 2399
then ask for the owner or any other person selling medicines. 2400
5. If the shop is eligible for inclusion give the information sheet and ask for consent and begin the 2401
questionnaire. 2402
6. Also ask about other private providers in the vicinity to identify any health facilities that are not on the 2403
original list. This is called a snowball sampling method and will be particularly useful for identifying 2404
other private providers. 2405
7. Record information of closed outlets. If outlets are not permanently “closed down” interviewers will try 2406
to make call-backs to these outlets 2407
8. If the informants work both in a health centre and a private outlet conduct the interview in the private 2408
outlet. 2409
9. At the end of every visit fieldworkers will position every outlet using a global positioning system (GPS). 2410
One longitudinal and latitudinal reading will be taken. Turn on the GPS and check it is showing 2411
coordinates. Record GPS coordinates and altitude of the facility in the census form. Turn off the GPS. 2412
10. Move to the next provider and repeat steps 1–10. 2413
11. Participants will be able to drop out at any time during the survey and do not have to reply to questions 2414
if they do not wish to. Reasons for not participating or not answering questions will be obtained. 2415
12. Ensure that all the information collected is input into the database. 2416
2417
IX. Precaution-Safety guidelines 2418
2419
1. Check GPS battery to ensure it is fully charged before taking off 2420
2. Choose a suitable position to ensure that GPS has a high resolution. Ideally it must be in an 2421
open space away from trees and any roof. 2422
3. Do not dispose of used batteries into fire or near fire because of risk of explosion. 2423
4. Always carry an extra pack of batteries 2424
2425

Working document QAS/14.590
page 99
X. Quality assurance 2426
2427
1. Appropriate and rigorous selection and training of fieldworkers. 2428
2. Daily supervision of data collection in the field for the survey, checking completed census 2429
forms, ensuring that all potentially eligible outlets are visited. 2430
3. Confidentiality will be maintained at all times. This includes restricting access to all data to 2431
the investigators and data-entry clerks when needed, as well as using individual identification 2432
numbers on software programs for data analysis. 2433
4. Spot check of a random sample of 5% of outlets censused which met the screening criteria and 2434
5% that did not. For those meeting the screening criteria this does not need to entail a full 2435
repeat of the questionnaire, but rather is a quality control visit to assess whether the interview 2436
was completed, whether a few key questions were answered appropriately. For those not 2437
meeting the screening criteria the spot check should verify that the screening criteria where 2438
appropriate were completed. This is to ensure that interviewers do not report “No” to these 2439
questions just to skip the outlet and reduce their workload. 2440
2441
XI. Limitation of the procedure 2442
2443
1. Cloud cover may affect the resolution of the GPS. 2444
2. Some attendants may not give contact information in the absence of their chief. 2445
3. Some people may not accept to be part of the study. 2446
4. Some private providers who work in a health centre might refuse to receive the team in their 2447
private clinic 2448
2449
XII. Additional notes 2450
2451
1. All survey team members should be polite and friendly, carry your authorization documents, 2452
put on identification badges and work according to procedure stipulated in SOP. 2453
2. Before inviting participants all survey team members must make sure they meet the eligibility 2454
criteria set out in the study protocol for each target group. 2455
3. Thank the participant at the end of every visit. 2456
4. No payment or gift will be given to providers who participate to this study. 2457
2458
2459
Working document QAS/14.590
page 100
ANNEX 7 2460
TESTING PROTOCOL 2461
2462
Survey of the quality of antimalarial medicines …………… 2463
2464
TESTING PROTOCOL 2465
2466
Product Tests to be performed and specifications for testing
Artemether/
Lumefantrine tablets
FDC
International Pharmacopoeia monograph
• Appearance - general requirements of Ph.Int. for tablets
• Uniformity of mass – Ph.Int.
• Identity – HPLC as for assay
• Assay – Ph.Int. – HPLC
• Artemether related substances – Ph.Int. – TLC
• Dissolution – laboratory-validated method similar to the method used for
Lumefantrine and Artemether tablets in USP Non–US Monograph (authorized
1.3.2009);
Requirements: lumefantrine – not less than 60% (Q) in 45 min; artemether –
not less than 40% (Q) in 1 hour and not less than 60% (Q) in 3 hours.
Artesunate /
Amodiaquine tablets
Co-blistered
Artesunate tablets:
International Pharmacopoeia monograph
• Appearance – general requirements of Ph.Int. for tablets
• Uniformity of mass – Ph.Int.
• Identity – HPLC as for assay
• Assay – Ph.Int. – HPLC
• Artesunate related substances – Ph.Int. – HPLC
• Dissolution – Ph.Int.
Amodiaquine tablets:
US Pharmacopeia monograph
• Appearance – - general requirements of Ph.Int. for tablets
• Uniformity of mass – PhInt
• Identity – USP
• Assay – USP – UV spectrophotometry
• Dissolution – USP
Artesunate /
Amodiaquine tablets
FDC
Laboratory-validated methods
• Appearance – general requirements of Ph.Int. for tablets
• Uniformity of mass – Ph.Int.
• Identity – HPLC as for assay
• Assay – HPLC; 90–110%
• Artesunate-related substances – tested without specifications
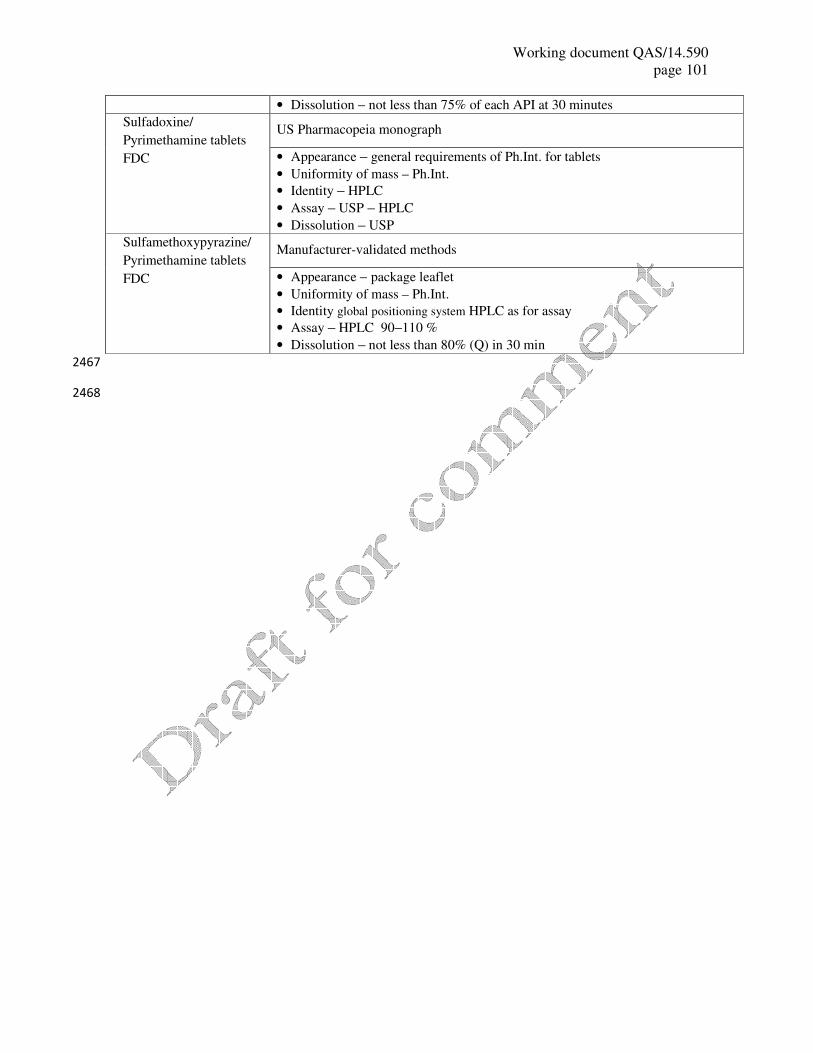
Working document QAS/14.590
page 101
• Dissolution – not less than 75% of each API at 30 minutes
Sulfadoxine/
Pyrimethamine tablets
FDC
US Pharmacopeia monograph
• Appearance – general requirements of Ph.Int. for tablets
• Uniformity of mass – Ph.Int.
• Identity – HPLC
• Assay – USP – HPLC
• Dissolution – USP
Sulfamethoxypyrazine/
Pyrimethamine tablets
FDC
Manufacturer-validated methods
• Appearance – package leaflet
• Uniformity of mass – Ph.Int.
• Identity global positioning system HPLC as for assay
• Assay – HPLC 90–110 %
• Dissolution – not less than 80% (Q) in 30 min
2467
2468
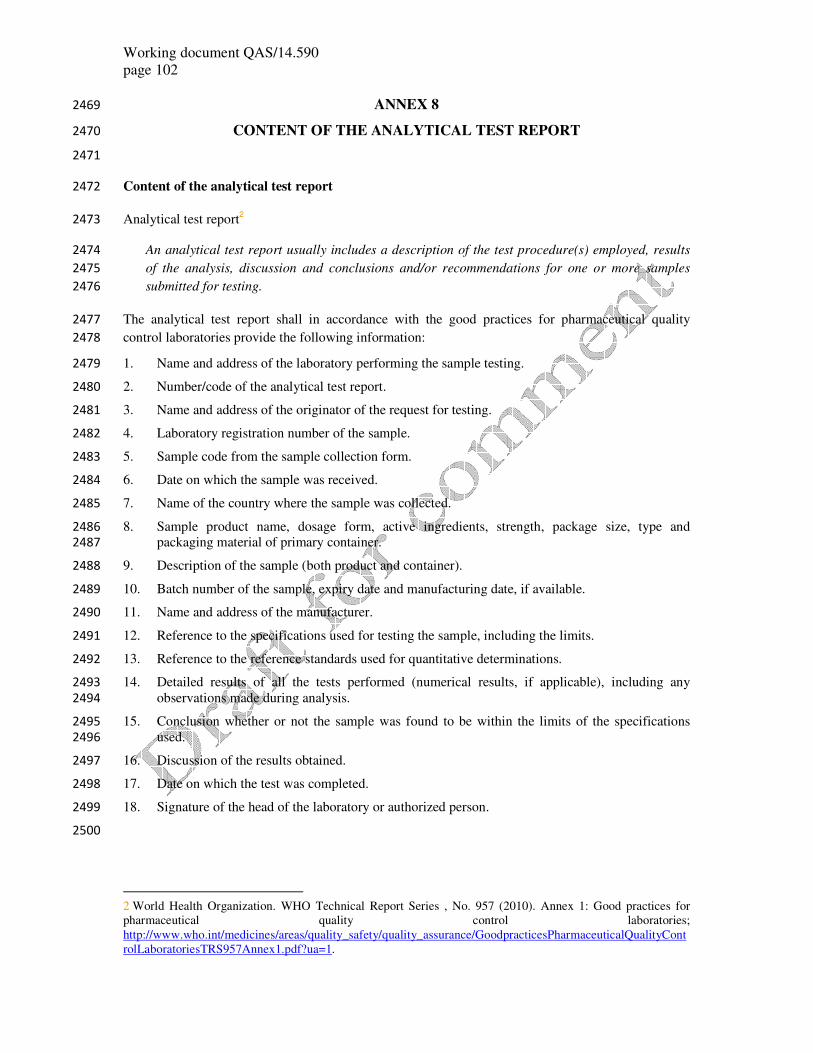
Working document QAS/14.590
page 102
ANNEX 8 2469
CONTENT OF THE ANALYTICAL TEST REPORT 2470
2471
Content of the analytical test report 2472
Analytical test report2 2473
An analytical test report usually includes a description of the test procedure(s) employed, results 2474
of the analysis, discussion and conclusions and/or recommendations for one or more samples 2475
submitted for testing. 2476
The analytical test report shall in accordance with the good practices for pharmaceutical quality 2477
control laboratories provide the following information: 2478
1. Name and address of the laboratory performing the sample testing. 2479
2. Number/code of the analytical test report. 2480
3. Name and address of the originator of the request for testing. 2481
4. Laboratory registration number of the sample. 2482
5. Sample code from the sample collection form. 2483
6. Date on which the sample was received. 2484
7. Name of the country where the sample was collected. 2485
8. Sample product name, dosage form, active ingredients, strength, package size, type and 2486
packaging material of primary container. 2487
9. Description of the sample (both product and container). 2488
10. Batch number of the sample, expiry date and manufacturing date, if available. 2489
11. Name and address of the manufacturer. 2490
12. Reference to the specifications used for testing the sample, including the limits. 2491
13. Reference to the reference standards used for quantitative determinations. 2492
14. Detailed results of all the tests performed (numerical results, if applicable), including any 2493
observations made during analysis. 2494
15. Conclusion whether or not the sample was found to be within the limits of the specifications 2495
used. 2496
16. Discussion of the results obtained. 2497
17. Date on which the test was completed. 2498
18. Signature of the head of the laboratory or authorized person. 2499
2500
2 World Health Organization. WHO Technical Report Series , No. 957 (2010). Annex 1: Good practices for
pharmaceutical quality control laboratories;
http://www.who.int/medicines/areas/quality_safety/quality_assurance/GoodpracticesPharmaceuticalQualityCont
rolLaboratoriesTRS957Annex1.pdf?ua=1.
Working document QAS/14.590
page 103
EXAMPLE OF SURVEY PROTOCOL 2501
based on 2502
WHO survey of the quality of antituberculosis medicines circulating in selected newly 2503
independent states of the former Soviet Union 2504
Version: Final (May 2009) 2505
1. GENERAL OUTLINE 2506
1. Introduction 2507
WHO estimates that nearly half a million multidrug-resistant tuberculosis (MDR-TB)3 cases emerge 2508
each year, as a result of inadequate or poorly-administered treatment regimens, insufficient supply or 2509
quality of anti-TB medicine, and transmission of drug-resistant strains. Newly independent states of 2510
the former Soviet Union (NIS) have some of the highest prevalence rates of MDR-TB, with 2511
proportions of MDR-TB among new and previously treated TB cases have been reported as high as 2512
28.3% and 61.6%, respectively.4 2513
It has been hypothesized that one of the most important factors for the resurgence of TB, and the high 2514
rates of MDR-TB, in the NIS was the socioeconomic crisis that followed the disintegration of the 2515
Soviet Union in 1991.5,6,7
This crisis resulted in interruptions in medicines supply and overall 2516
deterioration of the health sector, which had an impact on the transmission of and susceptibility to TB 2517
and MDR-TB. The lack of standardized treatment regimens in many countries is also likely to have 2518
contributed to the development of drug resistance. 2519
Limited research has been conducted into the factors contributing to drug resistance in this region and 2520
to the marked regional and national differences in drug resistance rates. In particular there has been 2521
little consideration of the extent to which substandard, spurious, falsely-labelled, falsified and 2522
counterfeit (SSFFC) anti-TB medicines might circulate in this region. This survey aims to investigate 2523
the quality of anti-TB medicines in use in selected NIS. 2524
2525
3 MDR-TB is defined as resistance to at least rifampicin and isoniazid, the two most powerful anti-TB
medicines.
4 WHO/IUATLD Global Project on Anti-tuberculosis Drug Resistance Surveillance. Anti-tuberculosis drug
resistance in the world: fourth global report. Geneva, World Health Organization, 2008.
5 Raviglione MC et al. Tuberculosis trends in eastern Europe and the former USSR. Tubercle and Lung
Disease, 1994 Dec, 75(6):400-16.
6 Shilova MV, Dye C. The resurgence of tuberculosis in Russia. Philosophical Transactions of the Royal
Society London B: Biological Sciences, 2001 Jul 29, 356(1411):1069-75.
7 Global tuberculosis control: a short update to the 2009 report. Geneva, World Health Organization, 2009
(available at: http://whqlibdoc.who.int/publications/2009/9789241598866_eng.pdf, accessed 23 June 2011).
Working document QAS/14.590
page 104
2. Definitions 2526
Country code for the purposes of this project means a 2-digit code used for the country in an 2527
email address. 2528
Delivery centre for the purpose of this project means a point, where a medicine enters the 2529
country, central stores and stores, where a medicine is kept during the in-2530
country distribution. 2531
Product abbreviations (for the purposes of coding samples): 2532
Isoniazid = H 2533
Rifampicin = R 2534
Isoniazid + rifampicin = H-R 2535
Kanamycin = Km 2536
Ofloxacin = Ofx 2537
Sample for the purposes of this project means an item collected from each 2538
presentation at the same collection site. That means that a product of the same 2539
name, content of APIs, the same dosage form, strength, batch and from the 2540
same manufacturer collected in two different sites represents two samples. 2541
Treatment centre for the purpose of this project means the final site, where a medicine is 2542
delivered and where it is provided to a patient. 2543
3. Objectives 2544
The WHO Stop TB and Essential Medicines and Health Products Departments, and counterparts in the 2545
WHO Regional Office for Europe, are collaborating with NMRAs to study the quality of first- and 2546
second-line anti-TB medicines circulating in the countries with the highest MDR-TB and XDR-TB 2547
rates. The project will commence in countries of Eastern Europe and the NIS as indicated in this study 2548
protocol and will subsequently expand to China and India. 2549
The aim of this project is therefore to evaluate the pharmaceutical quality of widely used anti-TB 2550
medicines (first- and second-line) obtained at public and private sector procurement and treatment 2551
centres in selected countries of Eastern Europe and the NIS. The following questions will be addressed: 2552
• Which anti-TB medicines are mostly used? 2553
• What proportion of anti-TB medicines samples, including fixed-dose combination (FDC) 2554
products, collected at approved procurement and treatment centres fail quality testing? 2555
• Which specific quality tests do the samples fail, if any? 2556
• Are any of the deficiencies critical, i.e. could most likely affect treatment efficacy and/or 2557
cause harm to the patient? 2558
The results of this study are expected to assist responsible authorities in the countries surveyed to 2559
adopt regulatory actions, if necessary, and to develop appropriate quality assurance strategies for anti-2560
TB medicines. They will also provide information for WHO to adapt its prequalification procedures. 2561
Finally, they will be of use in awareness and advocacy programmes on quality issues in anti-TB 2562
medicines in general. 2563
Working document QAS/14.590
page 105
Limitations of the study 2564
This quality survey cannot completely solve the problem of bioavailability which may be of special 2565
relevance in case of rifampicin. 2566
Appropriate bioavailability must be assured by complex regulatory measures which include 2567
compliance of manufacture with GMP standards, appropriate quality specifications for both active 2568
ingredients and finished product and proof of bioequivalence with proper comparator. These 2569
parameters should be assessed during registration and followed up in the post-registration period. 2570
From anti-TB medicines included in this survey only rifampicin strictly requires bioequivalence 2571
testing in vivo, for other appropriate bioavailability may be judged upon based on in vitro testing. 2572
However, organization of bioequivalence studies for rifampicin-containing products cannot be applied 2573
as a quality control method without proper understanding of GMP compliance and registration 2574
conditions and as a control method for the given purpose is considered unethical. Instead of that 2575
comparative dissolution is performed to respond at least partially to the issue of bioavailability. 2576
It is obvious that study findings are relevant only to tested samples and extrapolation to individual 2577
batches and products is limited. 2578
4. Methodology 2579
4.1 Participating countries 2580
The study should involve some six countries where anti-TB medicines are not produced or are 2581
produced on a small scale. 2582
The following nine countries were approached before the selection of countries was made: 2583
• Armenia 2584
• Azerbaijan 2585
• Belarus 2586
• Estonia 2587
• Kazakhstan 2588
• Latvia 2589
• Moldova 2590
• Ukraine 2591
• Uzbekistan 2592
The countries where samples should be collected were selected as below. 2593
1. A questionnaire (Annex 1) was sent to the NMRA in the nine above-mentioned countries. The 2594
questionnaire asked for first- and second-line anti-TB medicines, including FDCs, that were in 2595
2008 used in the country in both public and private sectors, the volumes used, the 2596
manufacturers of these medicines and also which institutions were involved in importation and 2597
distribution of these medicines (to identify sampling locations). 2598
2. Following the compilation of the results of the questionnaire six relevant countries were 2599
selected, focusing on those where the widest choice of medicines selected for this study was in 2600
use. 2601
Working document QAS/14.590
page 106
3. A certain amount of medicines is procured through the Global Drug Facility (GDF), including 2602
the Green Light Committee. These medicines should also be tested. However, it is important 2603
to select countries using other sources than GDF. 2604
4. An official WHO letter was sent to the ministries of health of the six selected countries. The 2605
letter described the project and asked for the willingness of the ministry of health to 2606
collaborate on this project. Without the consent of the ministry of health the country was not 2607
included in the project. 2608
Based on the results of the questionnaire and taking into account the above mentioned aspects the 2609
following countries were selected for sampling: 2610
• Armenia 2611
• Azerbaijan 2612
• Belarus 2613
• Kazakhstan 2614
• Uzbekistan 2615
• Ukraine 2616
The ministries of health of the above-mentioned six countries also nominated focal persons for this 2617
project. 2618
4.2 Anti-tuberculosis medicines surveyed 2619
Based on the information on medicines used in individual countries the final medicines selection was 2620
made. Apart from availability volumes and sources of medicines used in individual countries, the 2621
susceptibility of medicines to quality deterioration such as low stability was taken into account. 2622
Based on these considerations the following medicines were selected to be surveyed: 2623
• Isoniazid tablets 300 mg, 100 mg, injection 10% (5 mL) 2624
• Rifampicin capsules 300 mg, 150 mg 2625
• Isoniazid/rifampicin tablets 150 mg/300 mg, 150/150 mg, 75/150 mg, 60/60 mg, 30/60 mg 2626
• Kanamycin powder for injection 1 g 2627
• Ofloxacin tablets/capsules 200 mg, 400 mg, solution for injection 0.2% (200 mL) 2628
2629
4.3 Study period 2630
The study period should last from summer 2008 to beginning 2010 and as indicated in Table 2. 2631
Table 2. Timeframe and responsible officers for the survey of the quality of anti-TB medicines 2632
circulating in selected countries of Eastern Europe and the NIS. 2633
Activity Timeframe Responsible officers
Anti-TB medicines quality survey
questionnaire sent to the nine countries
June 2008 EURO Pharmaceutical
Programme
Compilation of results of the questionnaire October 2008 EURO Pharmaceutical
Programme
Selection of countries and anti-TB
medicines to be surveyed
November 2008 EURO Pharmaceutical
Programme and HQ TB and
EMP/QMS departments
Letters sent to ministers of health of six December 2008 EURO Pharmaceutical
Working document QAS/14.590
page 107
countries for collaboration in this project Programme
Laboratory(ies) selected for the
performance of the tests
January 2009 HQ EMP/QMS
Preparations of contracts with NMRA to
cover for national expenditures
May 2009 EURO Pharmaceutical
Programme and HQ TB and
EMP/QMS departments
Meeting held with selected countries and
pharmaceutical experts
May 2009 EURO Pharmaceutical
Programme and HQ EMP/QMS
Collection of samples by NMRAs June–September
2009
NMRAs in close collaboration
with WHO country, region and
HQ staff
Analysis of medicines quality by selected
laboratories
October 2009–April
2010
HQ EMP/QMS
Compilation of results April–June 2010 EURO Pharmaceutical
Programme and HQ TB and
EMP/QMS
Meeting held with the participating
countries (ministries of health and NMRA
staff) and WHO pharmaceutical and TB
experts to discuss the final results and the
actions needed
June 2010 EURO Pharmaceutical
Programme and HQ TB and
EMP/QMS departments
2634
4.4 Selection of sample collection sites 2635
Samples should be collected from the following levels of distribution chain: 2636
• level 1 – delivery centres (private and/or public); as the aim of the survey is to assess the 2637
quality of medicines available to patients samples should be collected at the manufacturing 2638
sites only in cases where it is not possible to collect appropriate samples at the other sites; 2639
• level 2 – wholesalers, regulated retailers including dispensing facilities and treatment centres, 2640
in both private and public sectors. 2641
A meeting should be held with participation of focal persons from individual countries and WHO 2642
representatives from the EURO Pharmaceutical Programme and HQ TB and EMP/QMS Departments 2643
to explain the project, to provide detailed instructions and to identify names and addresses of sample 2644
collection sites in each country involved. 2645
Samples will be collected by the staff of the NMRAs in cooperation with the WHO country offices’ 2646
staff in the respective country and with backup support from the EURO Pharmaceutical Programme 2647
and HQ EMP/QMS Department. 2648
4.5 Sample collection 2649
For the purposes of this project a sample means an item collected from each presentation at the same 2650
collection site. That means that a product of the same name, content of APIs, the same dosage form, 2651
strength, batch and from the same manufacturer collected in two different sites represents two samples. 2652
Working document QAS/14.590
page 108
A detailed national sampling plan will be prepared for each country by the focal person in the NMRA 2653
in cooperation with WHO pharmaceutical experts (Annex 2). The focal person in each country will 2654
arrange for training of collectors to be familiar with the national sampling plan and instructions. 2655
In general the following information shall be included in the national sampling plan: 2656
• identification of the country and the person responsible for sampling; 2657
• names and addresses of the sites, where samples shall be collected; 2658
• identification of medicines to be collected (active ingredients by INNs, dosage form, 2659
strength, manufacturer, number of batches to be collected in each site and number of units 2660
to be collected per batch of each medicine); 2661
• maximum number of samples collected per country; 2662
• detailed instructions for collecting samples (see below). 2663
2664
Number of dosage units or multidose packages of selected medicines to be collected should allow for: 2665
• conducting the agreed tests; 2666
• possible confirmative testing due to OOS investigations; 2667
• retention samples. 2668
The following general rules are used, if not justified otherwise: 2669
Dosage form Packaging
(typical)
Number of dosage units or
multidose packs per batch
Tablets and capsules
(immediate-/modified-release,
chewable, dispersible, etc. )
Blisters, co-blisters,
bottles, securitainers
Approx.100 units
(e.g. 5 packs of 20 units
3 packs of 30 units
3 packs of 40 units
2 packs of 60 units
1 pack of 90 units and above)
In case of co-packaged FPPs
approx.100 units shall be collected
from each medicine.
Multidose oral
solutions/suspensions, powder for
oral solution/suspension and
injections or powders for injections
Multidose bottles and
vials
6 containers of 60 mL /100 mL
3 containers of 240 mL
Single-dose powders for oral
solution/suspension and single-dose
injections or powders for injections
Sachets and single-dose
bottles, vials and
ampoules
Unless otherwise specified, 15 units
(20 units if dose is below 50 mg)
2670
Working document QAS/14.590
page 109
Instructions for sample collection: 2671
• the time period, within which samples should be collected in the countries and the deadline for 2672
sending the last sample to the testing laboratory, should be clearly indicated and followed; 2673
• the minimum quantity of sample per batch and number of batches to be collected from each 2674
collection site for each selected medicine as indicated in the sampling plan shall be followed. 2675
Note that there should not be a mix up with batches, all units of one sample must be of the same 2676
batch. In the case that in a collection site the required number of packages of the same batch is 2677
not available, sample of that particular medicine is not collected; 2678
• samples collected should have at least six months remaining to expiry; 2679
• only unopened original packages shall be collected; 2680
• the medicine samples should not be taken out of the original primary packaging and outer 2681
containers (though removal from large secondary packs is appropriate). Containers such as bottles 2682
and vials should not be opened; 2683
• the medicine labels and package leaflets should not be removed or damaged; 2684
• sampling will be recorded using the sample collection form (Annex 3). Whenever the required 2685
information is not available, it should be indicated in the appropriate space on the sample 2686
collection form where also any abnormalities should be recorded; 2687
• in order to avoid confusion each sample will be identified by a unique sample code (for coding 2688
system see the sample collection form, Annex 3) specified in the sample collection form as well 2689
as on all the original packages belonging to the respective sample. Packages belonging to one 2690
sample and the sample collection form will be kept together (e.g. blisters inserted in a dedicated 2691
envelope marked with the appropriate sample code and trade name of the product); 2692
• manufacturer’s batch certificates of analysis will be collected with samples, if available, and kept 2693
with the sample collection form; 2694
• the samples should be collected and kept under controlled conditions, as per label requirement. 2695
The cold chain should be maintained, where required. 2696
If needed, the appropriate arrangements shall be made with treatment centres to ensure that there is no 2697
shortage due to collection of samples (e.g. requesting for replacements of medicines). 2698
4.6 Storage and dispatch of samples 2699
Storage and transport of the sample should be done according to the requirements set out in paragraph 2700
2.3 of WHO’s Guidelines for Sampling of Pharmaceutical Products and related materials:8 2701
• the samples should be kept in original packaging and under storage conditions specified on 2702
the label; 2703
• for transport all samples should be packaged adequately and transported in such a way as to 2704
avoid breakage and contamination during transport. Any residual space in the container 2705
should be filled with a suitable material. Where required the cold chain should be retained 2706
during storage and transport; 2707
• a covering letter, the copy sample collection form and, if available, copy of manufacturer’s 2708
batch certificates of analysis should accompany the samples; 2709
8 WHO guidelines for sampling of pharmaceutical products and related materials. In: WHO Expert Committee
on Specifications for Pharmaceutical Preparations. Thirty-ninth report. Geneva, World Health Organization,
2005, Annex 4 (WHO Technical Report Series, No.929).
http://whqlibdoc.who.int/trs/WHO_TRS_929_eng.pdf#page68
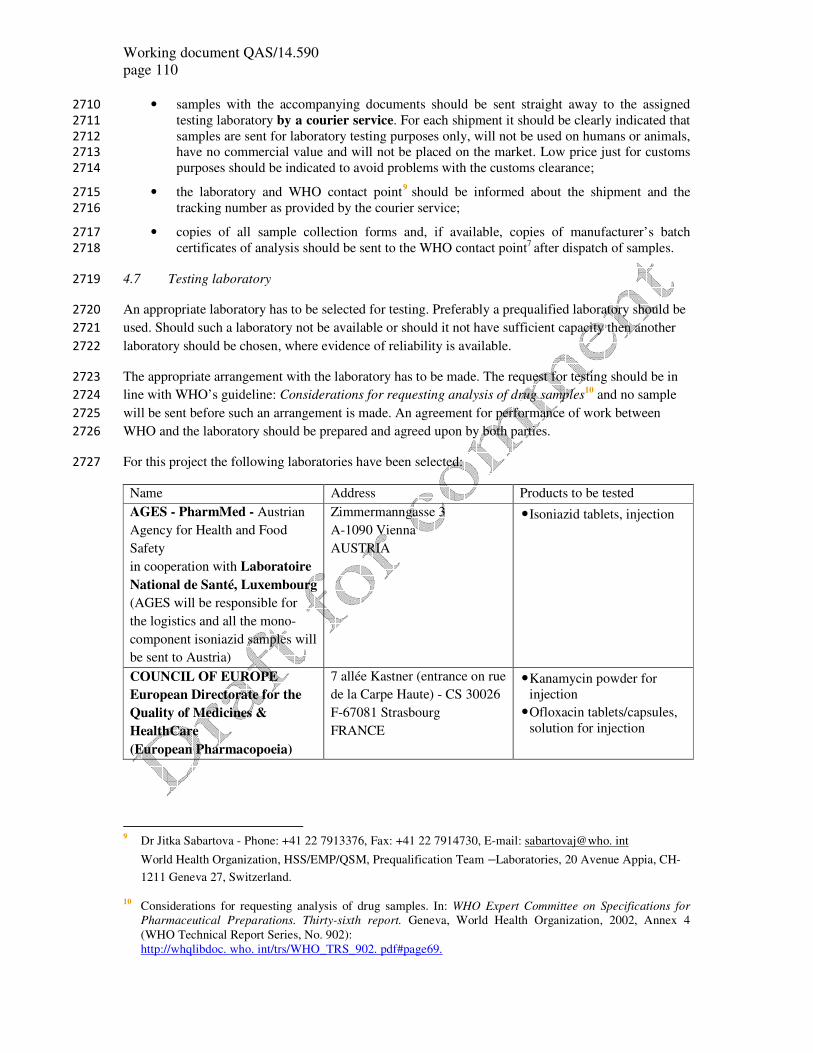
Working document QAS/14.590
page 110
• samples with the accompanying documents should be sent straight away to the assigned 2710
testing laboratory by a courier service. For each shipment it should be clearly indicated that 2711
samples are sent for laboratory testing purposes only, will not be used on humans or animals, 2712
have no commercial value and will not be placed on the market. Low price just for customs 2713
purposes should be indicated to avoid problems with the customs clearance; 2714
• the laboratory and WHO contact point9 should be informed about the shipment and the 2715
tracking number as provided by the courier service; 2716
• copies of all sample collection forms and, if available, copies of manufacturer’s batch 2717
certificates of analysis should be sent to the WHO contact point7 after dispatch of samples. 2718
4.7 Testing laboratory 2719
An appropriate laboratory has to be selected for testing. Preferably a prequalified laboratory should be 2720
used. Should such a laboratory not be available or should it not have sufficient capacity then another 2721
laboratory should be chosen, where evidence of reliability is available. 2722
The appropriate arrangement with the laboratory has to be made. The request for testing should be in 2723
line with WHO’s guideline: Considerations for requesting analysis of drug samples10
and no sample 2724
will be sent before such an arrangement is made. An agreement for performance of work between 2725
WHO and the laboratory should be prepared and agreed upon by both parties. 2726
For this project the following laboratories have been selected: 2727
Name Address Products to be tested
AGES - PharmMed - Austrian
Agency for Health and Food
Safety
in cooperation with Laboratoire
National de Santé, Luxembourg
(AGES will be responsible for
the logistics and all the mono-
component isoniazid samples will
be sent to Austria)
Zimmermanngasse 3
A-1090 Vienna
AUSTRIA
• Isoniazid tablets, injection
COUNCIL OF EUROPE
European Directorate for the
Quality of Medicines &
HealthCare
(European Pharmacopoeia)
7 allée Kastner (entrance on rue
de la Carpe Haute) - CS 30026
F-67081 Strasbourg
FRANCE
• Kanamycin powder for
injection
• Ofloxacin tablets/capsules,
solution for injection
9 Dr Jitka Sabartova - Phone: +41 22 7913376, Fax: +41 22 7914730, E-mail: sabartovaj@who. int
World Health Organization, HSS/EMP/QSM, Prequalification Team –Laboratories, 20 Avenue Appia, CH-
1211 Geneva 27, Switzerland.
10 Considerations for requesting analysis of drug samples. In: WHO Expert Committee on Specifications for
Pharmaceutical Preparations. Thirty-sixth report. Geneva, World Health Organization, 2002, Annex 4
(WHO Technical Report Series, No. 902):
http://whqlibdoc. who. int/trs/WHO_TRS_902. pdf#page69.
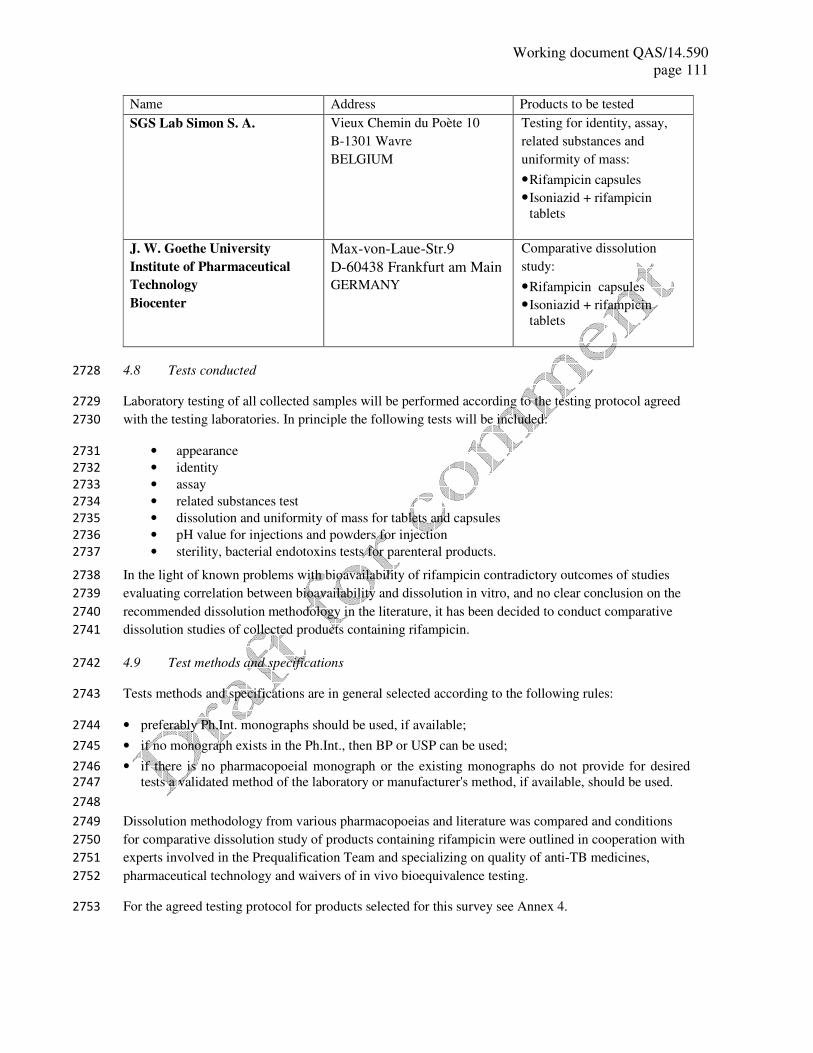
Working document QAS/14.590
page 111
Name Address Products to be tested
SGS Lab Simon S. A. Vieux Chemin du Poète 10
B-1301 Wavre
BELGIUM
Testing for identity, assay,
related substances and
uniformity of mass:
• Rifampicin capsules
• Isoniazid + rifampicin
tablets
J. W. Goethe University
Institute of Pharmaceutical
Technology
Biocenter
Max-von-Laue-Str.9
D-60438 Frankfurt am Main
GERMANY
Comparative dissolution
study:
• Rifampicin capsules
• Isoniazid + rifampicin
tablets
4.8 Tests conducted 2728
Laboratory testing of all collected samples will be performed according to the testing protocol agreed 2729
with the testing laboratories. In principle the following tests will be included: 2730
• appearance 2731
• identity 2732
• assay 2733
• related substances test 2734
• dissolution and uniformity of mass for tablets and capsules 2735
• pH value for injections and powders for injection 2736
• sterility, bacterial endotoxins tests for parenteral products. 2737
In the light of known problems with bioavailability of rifampicin contradictory outcomes of studies 2738
evaluating correlation between bioavailability and dissolution in vitro, and no clear conclusion on the 2739
recommended dissolution methodology in the literature, it has been decided to conduct comparative 2740
dissolution studies of collected products containing rifampicin. 2741
4.9 Test methods and specifications 2742
Tests methods and specifications are in general selected according to the following rules: 2743
• preferably Ph.Int. monographs should be used, if available; 2744
• if no monograph exists in the Ph.Int., then BP or USP can be used; 2745
• if there is no pharmacopoeial monograph or the existing monographs do not provide for desired 2746
tests a validated method of the laboratory or manufacturer's method, if available, should be used. 2747
2748
Dissolution methodology from various pharmacopoeias and literature was compared and conditions 2749
for comparative dissolution study of products containing rifampicin were outlined in cooperation with 2750
experts involved in the Prequalification Team and specializing on quality of anti-TB medicines, 2751
pharmaceutical technology and waivers of in vivo bioequivalence testing. 2752
For the agreed testing protocol for products selected for this survey see Annex 4. 2753

Working document QAS/14.590
page 112
4.10 Receipt and testing of samples by a testing laboratory 2754
• Inspect each sample to ensure that the labelling is in conformance with the information 2755
contained in the sample collection form or test request. 2756
• Store the samples according to the respective medicine requirements. If appropriate ensure 2757
compliance with the cold chain. 2758
• Conduct quality testing in line with this protocol and in compliance with WHO standards 2759
recommended for quality control laboratories.11
2760
• Complete an Analytical Test Report (Annex 5). In the case that non-compliant results are 2761
found and confirmed after application of a laboratory out-of-specification procedure, report 2762
them immediately to WHO contact point7. 2763
• Keep records of each sample, accompanying document/s and retention samples for at least 2764
six months if the sample complied with the analytical test requirements, or for at least one 2765
year or until the expiry date (whichever is longer) if it did not comply. 2766
• An electronic databank (e.g. photos of medicine such as tablets, packaging, package leaflet) 2767
is recommended. 2768
5. Data management, analysis and publication 2769
Any non-compliant result found in the survey will be investigated with the respective manufacturer 2770
and NMRA. 2771
A data analyst/statistician will be hired to compile and analyse the laboratory test results. 2772
The analytical test reports of the testing laboratories will be provided to all NMRA involved in the 2773
project. The outcomes of the project will be discussed by national authorities and WHO in a meeting, 2774
and corrective actions, if necessary, will be recommended. To take the relevant measures in countries 2775
lies within the responsibility of the NMRA. 2776
Agreed outcomes and the report from the project will be published by WHO. 2777
11
World Health Organization. WHO Technical Report Series , No. 957 (2010). Annex 1: Good practices for
pharmaceutical quality control laboratories;
http://www.who.int/medicines/areas/quality_safety/quality_assurance/GoodpracticesPharmaceuticalQualityC
ontrolLaboratoriesTRS957Annex1.pdf?ua=1.

Working document QAS/14.590
page 113
EXAMPLE OF SURVEY PROTOCOL
based on
WHO survey of the quality of anti-tuberculosis medicines circulating in selected NIS of the former Soviet Union
2. QUESTIONNAIRE
please fill in ONLY for products which are actually available in July 2008
Name and address of the site
Responsible person(s) and contact details
(phone, mobile, e-mail)
Type of site
what organization is best to approach for sampling, i.e. which one
has the longest list of TB products available.
Hospital
pharmacy
Warehouse Retail
pharmacy
Please mark with X in the box under the correct answer
Finished pharmaceutical product and
dosage form
Strength Quantity
(packs)
Manufacturer name
and manufacturing site
address
Country
of origin
Not used in
the country
Single ingredient first-line antituberculosis medicines
Ethambutol, tablet 400 mg
Isoniazid, tablet 300 mg
Pyrazinamide, tablet 400 mg
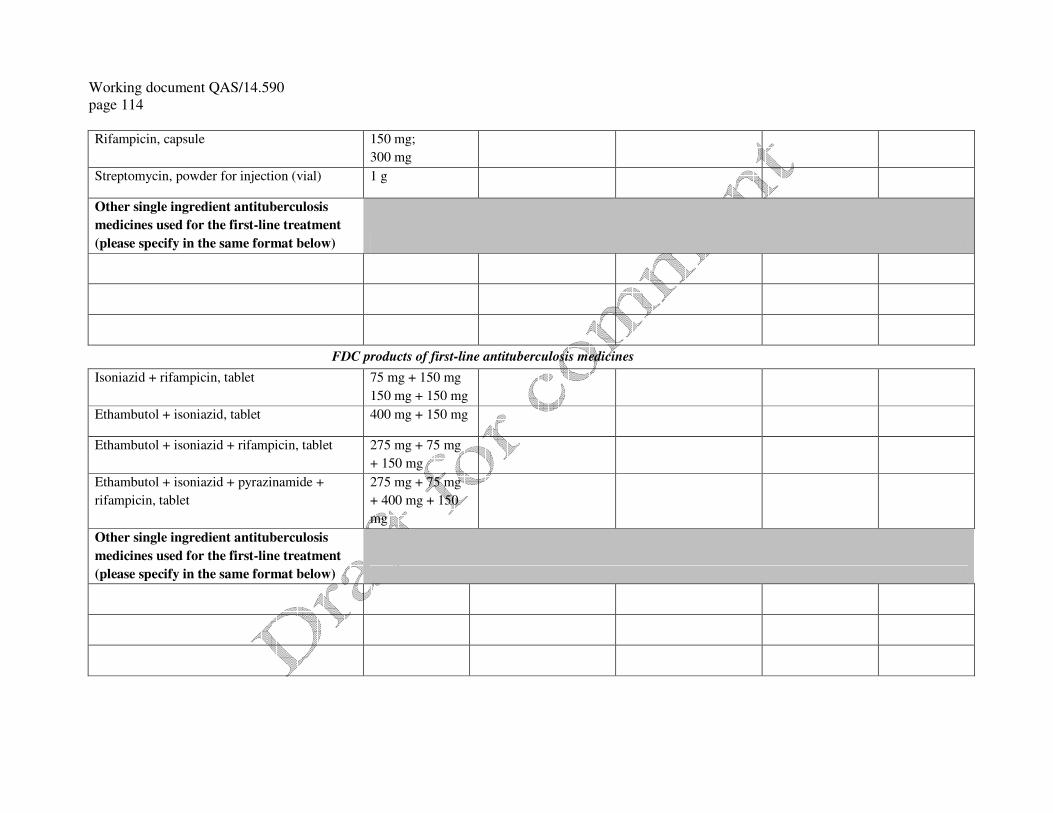
Working document QAS/14.590
page 114
Rifampicin, capsule 150 mg;
300 mg
Streptomycin, powder for injection (vial) 1 g
Other single ingredient antituberculosis
medicines used for the first-line treatment
(please specify in the same format below)
FDC products of first-line antituberculosis medicines
Isoniazid + rifampicin, tablet 75 mg + 150 mg
150 mg + 150 mg
Ethambutol + isoniazid, tablet 400 mg + 150 mg
Ethambutol + isoniazid + rifampicin, tablet 275 mg + 75 mg
+ 150 mg
Ethambutol + isoniazid + pyrazinamide +
rifampicin, tablet
275 mg + 75 mg
+ 400 mg + 150
mg
Other single ingredient antituberculosis
medicines used for the first-line treatment
(please specify in the same format below)
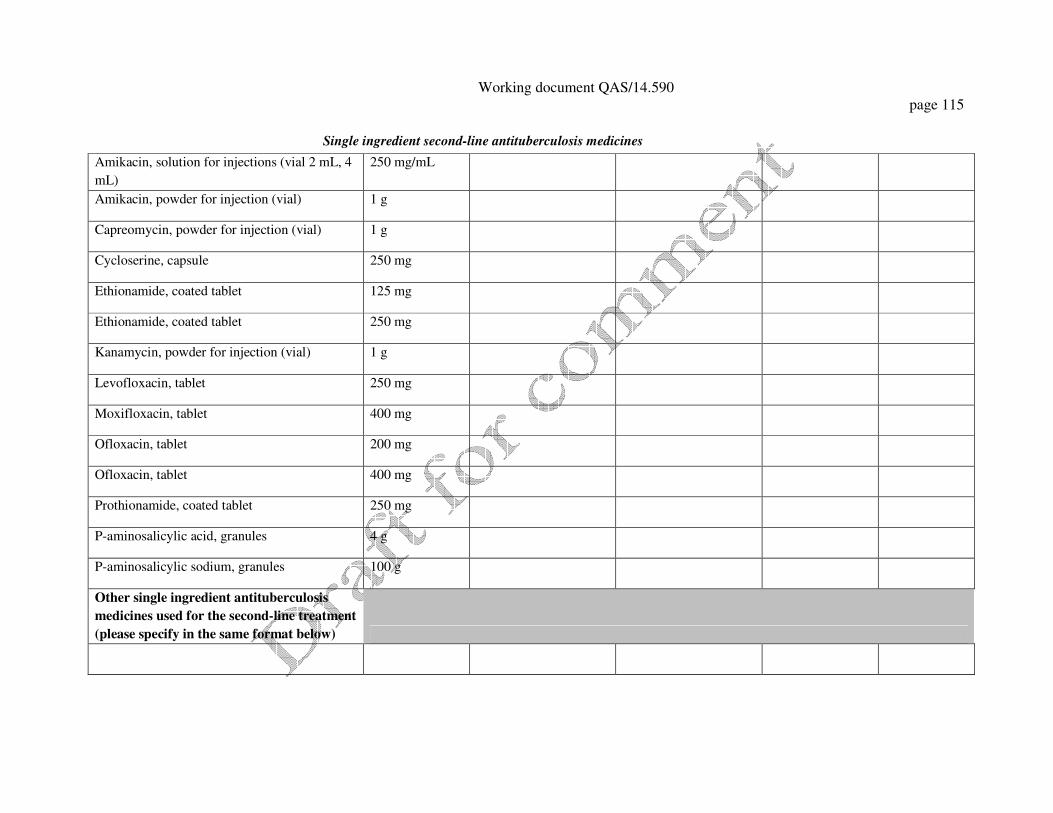
Working document QAS/14.590
page 115
Single ingredient second-line antituberculosis medicines
Amikacin, solution for injections (vial 2 mL, 4
mL)
250 mg/mL
Amikacin, powder for injection (vial) 1 g
Capreomycin, powder for injection (vial) 1 g
Cycloserine, capsule 250 mg
Ethionamide, coated tablet 125 mg
Ethionamide, coated tablet 250 mg
Kanamycin, powder for injection (vial) 1 g
Levofloxacin, tablet 250 mg
Moxifloxacin, tablet 400 mg
Ofloxacin, tablet 200 mg
Ofloxacin, tablet 400 mg
Prothionamide, coated tablet 250 mg
P-aminosalicylic acid, granules 4 g
P-aminosalicylic sodium, granules 100 g
Other single ingredient antituberculosis
medicines used for the second-line treatment
(please specify in the same format below)

Working document QAS/14.590
page 116
Scored solid dosage formulations for children, preferably dispersible
Ethambutol, tablet 100 mg
Isoniazid, tablet 50 mg
Isoniazid, tablet 100 mg
Isoniazid + rifampicin, tablet 60 mg + 60 mg
Isoniazid + rifampicin, tablet 30 mg + 60 mg
Isoniazid + pyrazinamide + rifampicin, tablet 30 mg + 150 mg
+ 60 mg
Pyrazinamide, tablet 150 mg
Other scored solid dosage formulations for
children, preferably dispersible, used for TB
treatment (please specify in the same format
below)

Working document QAS/14.590
page 117
Instructions to fill the questionnaire
1. Before completion of the questionnaire please select the SITES which will have products actually available for sampling in July 2008. The site must have
the longest list of the medicines and amounts available for sampling.
2. Complete the form only for PRODUCTS that would be available at the selected sites for sampling in July 2008.
2. If the site has more that one product in the line, e.g. Ethambutol, tablet, 400mg, please insert the row below the specified product name and complete it
with all requested information.
4. Please complete the form in electronic format (as it is in MS Excel file) and send it by email to Olexandr Polishchuk, WHO/EURO at [email protected]
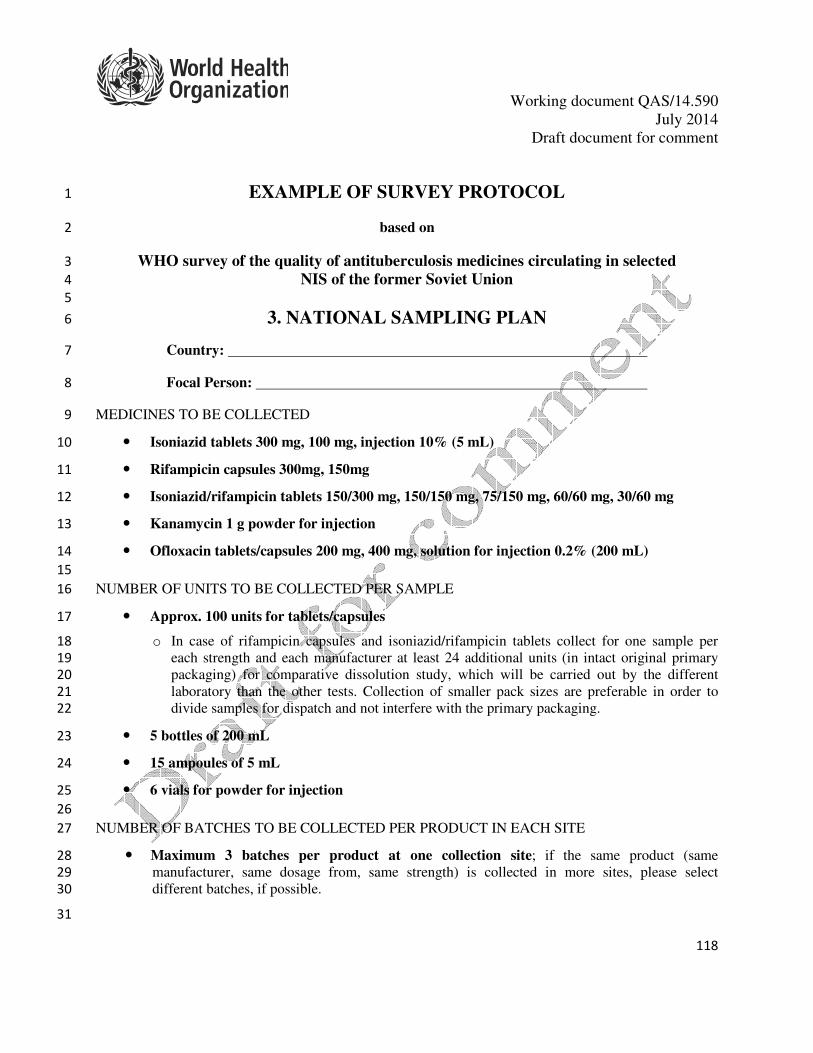
Working document QAS/14.590
July 2014
Draft document for comment
118
EXAMPLE OF SURVEY PROTOCOL 1
based on 2
WHO survey of the quality of antituberculosis medicines circulating in selected 3
NIS of the former Soviet Union 4
5
3. NATIONAL SAMPLING PLAN 6
Country: 7
Focal Person: 8
MEDICINES TO BE COLLECTED 9
• Isoniazid tablets 300 mg, 100 mg, injection 10% (5 mL) 10
• Rifampicin capsules 300mg, 150mg 11
• Isoniazid/rifampicin tablets 150/300 mg, 150/150 mg, 75/150 mg, 60/60 mg, 30/60 mg 12
• Kanamycin 1 g powder for injection 13
• Ofloxacin tablets/capsules 200 mg, 400 mg, solution for injection 0.2% (200 mL) 14
15
NUMBER OF UNITS TO BE COLLECTED PER SAMPLE 16
• Approx. 100 units for tablets/capsules 17
o In case of rifampicin capsules and isoniazid/rifampicin tablets collect for one sample per 18
each strength and each manufacturer at least 24 additional units (in intact original primary 19
packaging) for comparative dissolution study, which will be carried out by the different 20
laboratory than the other tests. Collection of smaller pack sizes are preferable in order to 21
divide samples for dispatch and not interfere with the primary packaging. 22
• 5 bottles of 200 mL 23
• 15 ampoules of 5 mL 24
• 6 vials for powder for injection 25
26
NUMBER OF BATCHES TO BE COLLECTED PER PRODUCT IN EACH SITE 27
• Maximum 3 batches per product at one collection site; if the same product (same 28
manufacturer, same dosage from, same strength) is collected in more sites, please select 29
different batches, if possible. 30
31
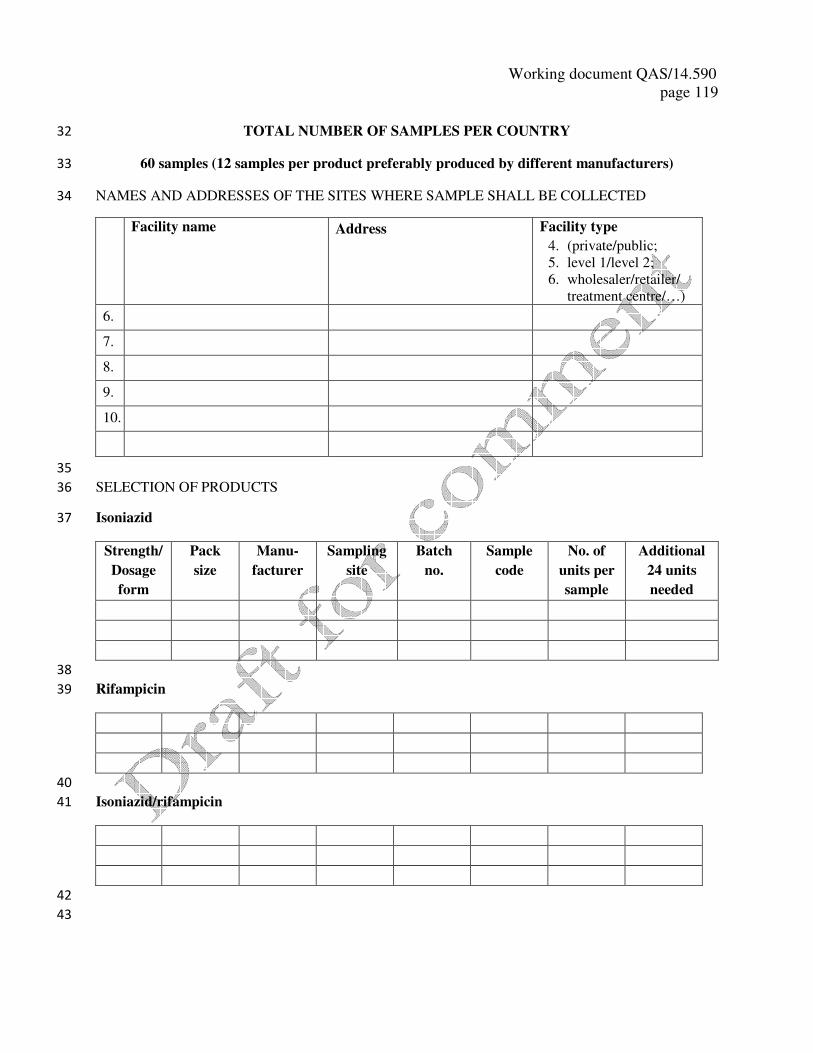
Working document QAS/14.590
page 119
TOTAL NUMBER OF SAMPLES PER COUNTRY 32
60 samples (12 samples per product preferably produced by different manufacturers) 33
NAMES AND ADDRESSES OF THE SITES WHERE SAMPLE SHALL BE COLLECTED 34
Facility name Address Facility type
4. (private/public;
5. level 1/level 2;
6. wholesaler/retailer/
treatment centre/…)
6.
7.
8.
9.
10.
35
SELECTION OF PRODUCTS 36
Isoniazid 37
Strength/
Dosage
form
Pack
size
Manu-
facturer
Sampling
site
Batch
no.
Sample
code
No. of
units per
sample
Additional
24 units
needed
38
Rifampicin 39
40
Isoniazid/rifampicin 41
42
43

Working document QAS/14.590
page 120
120
Kanamycin 44
Ofloxacin 45
46
INSTRUCTIONS FOR COLLECTORS 47
• The amount of the selected products defined above will be sampled from the identified sites. All 48
these samples are inclusive of the samples needed for the OOS investigations and retention samples. 49
• An item collected from each presentation at the same collection site will be called a sample. All units 50
(tablets, capsules, vials) of one sample must be of the same batch, there should not be a mix up 51
with batches. In the case that in a collection site the required number of packages of the same batch 52
is not available a sample of that particular medicine is not collected. 53
• Samples collected shall have at least six months remaining to expiry. Products with a shorter 54
period remaining to expiry date are not collected. 55
• One batch of each product will be collected from each collection site and only unopened original 56
packages shall be collected. 57
• The medicine samples should not be taken out of the original primary packaging and outer 58
containers (though removal of blisters from large secondary packs is appropriate). Containers such 59
as bottles and vials should not be opened. 60
• The medicine labels and package leaflets should not be removed or damaged. 61
• Sampling will be recorded using the sample collection form (Annex 3). Whenever the required 62
information is not available it should be indicated in the appropriate space on the sample collection 63
form, where also any abnormalities should be recorded. 64
• In order to avoid confusion each sample will be identified by a unique sample code (for coding 65
system see the sample collection form, Annex 3) specified in the sample collection form as well as 66
on all the original packages belonging to the respective sample. Packages belonging to one sample 67
and sample collection form will be kept together (e.g. blisters inserted in a dedicated envelope 68
marked with the appropriate sample code and trade name of the product). 69
• Manufacturer’s batch certificates of analysis will be collected with samples, if available, and kept 70
with the sample collection form. 71
• The samples should be collected and kept under controlled conditions as per label requirement. 72
The cold chain should be maintained where required. 73
• Samples should be collected in all the countries involved during XXX and the deadline for 74
sending the last sample to the testing laboratory is XXX 75
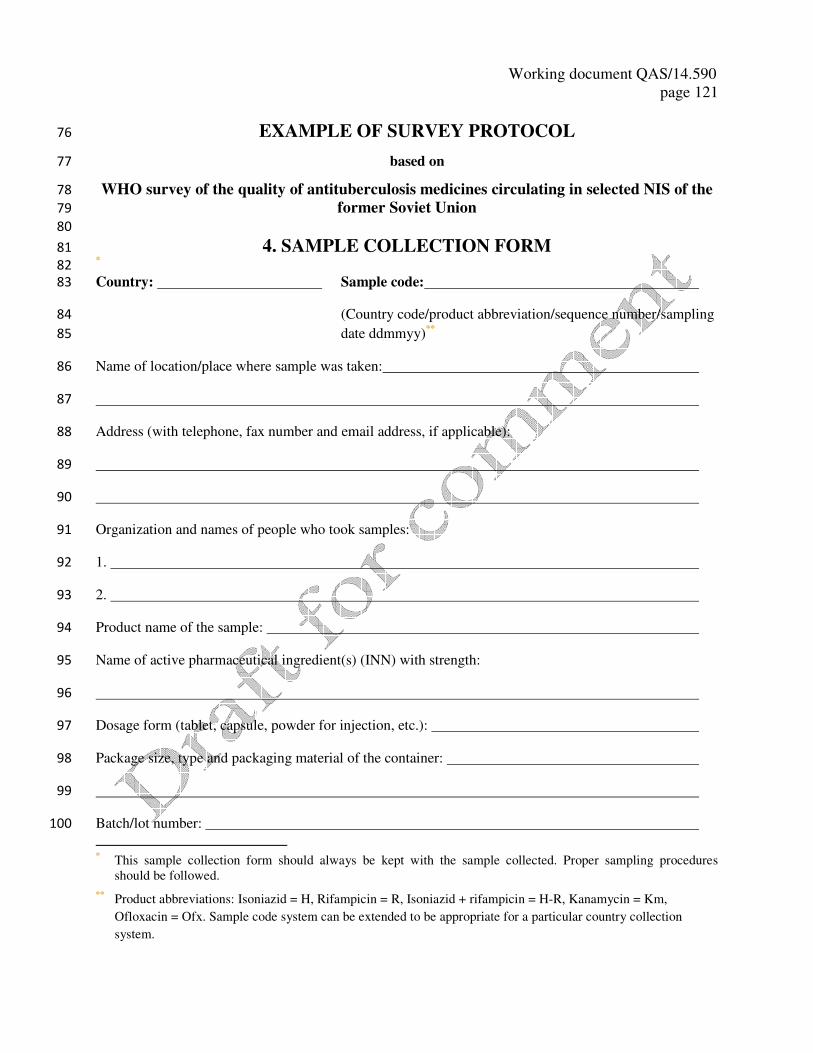
Working document QAS/14.590
page 121
EXAMPLE OF SURVEY PROTOCOL 76
based on 77
WHO survey of the quality of antituberculosis medicines circulating in selected NIS of the 78
former Soviet Union 79
80
4. SAMPLE COLLECTION FORM 81 * 82
Country: Sample code: 83
(Country code/product abbreviation/sequence number/sampling 84
date ddmmyy)**
85
Name of location/place where sample was taken: 86
87
Address (with telephone, fax number and email address, if applicable): 88
89
90
Organization and names of people who took samples: 91
1. 92
2. 93
Product name of the sample: 94
Name of active pharmaceutical ingredient(s) (INN) with strength: 95
96
Dosage form (tablet, capsule, powder for injection, etc.): 97
Package size, type and packaging material of the container: 98
99
Batch/lot number: 100
* This sample collection form should always be kept with the sample collected. Proper sampling procedures
should be followed.
** Product abbreviations: Isoniazid = H, Rifampicin = R, Isoniazid + rifampicin = H-R, Kanamycin = Km,
Ofloxacin = Ofx. Sample code system can be extended to be appropriate for a particular country collection
system.

Working document QAS/14.590
page 122
122
Date of manufacture: Expiry date: 101
Regulatory status in the country, registration number, if applicable: 102
103
Name and address of the manufacturer: 104
105
Quantity collected (number of sample units or of multidose containers taken): 106
107
Initialize first page 108
Product name: Sample code: 109
Storage/climatic conditions at sampling site/point (temperature and humidity, indication of conditions 110
during daytime only is acceptable, comments on suitability of premises where products are stored at the 111
particular site for the NMRA information): 112
113
114
115
Abnormalities, remarks or observations that may be considered relevant, if any: 116
117
118
119
120
121
122
Date: 123
Signature of person(s) taking Signature of representative of the 124
samples establishment where sample(s) was 125
taken (optional) 126
Working document QAS/14.590
page 123
1. .............................................................................................................................................................. 127
128
2. ............................................................................................................................................................. 129
130
Note: Samples collected must remain in their original containers, intact and unopened. 131
132

Working document QAS/14.590
page 124
124
EXAMPLE OF SURVEY PROTOCOL 133
based on 134
WHO survey of the quality of antituberculosis medicines circulating in selected NIS of the 135
former Soviet Union 136
137
5. TESTING PROTOCOL 138
139
Product Tests to be performed and specifications for
testing
Reference substances
1. Isoniazid tablets
100 mg, 300 mg
USP
• Appearance – package leaflet
• Identity – HPLC as for assay
• Uniformity of mass
• Assay – HPLC
• Dissolution – UV
USP:
Isoniazid – 1349706, 200 mg
2. Isoniazid injection
10% (5 mL)
USP
• Appearance – package leaflet
• Visual inspection – clear and free from visible
particulate matter
• Volume in container/Extractable volume
• Identity – HPLC as for assay
• Assay – HPLC
• pH – 6.0 – 7.0
• Sterility (to be performed for one sample per
batch/manufacturer)
USP:
Isoniazid – 1349706, 200 mg
3. Rifampicin capsules
150 mg, 300 mg
Ph.Int.
• Appearance – package leaflet
• Identity – HPLC as for assay
• Uniformity of mass
• Assay – HPLC
• Related substances – HPLC
• Comparative dissolution study – 2 sets of
comparison – 1 using Ph.Int. conditions, the
other USP/BP conditions, 7 points up to 60
min
Ph.Int. :
9930409 – Rifampicin, 300 mg
9930410 – Rifampicin quinine,
200 mg
BP:
627 – 3-formylrifamycin, 25 mg
4. Isoniazid/rifampicin
tablets
150/300 mg, 150/150
mg, 75/150 mg, 60/60
mg, 30/60 mg
Ph.Int.
• Appearance – package leaflet
• Identity – HPLC as for assay
• Uniformity of mass
• Assay – 2x HPLC
• Related substances – for rifampicin only –
HPLC
• Comparative dissolution study – 1 set of
Ph.Int. :
9930331 – Isoniazid, 100 mg
9930409 – Rifampicin, 300 mg
9930410 – Rifampicin quinone,
200 mg
BP:
627 – 3-formylrifamycin, 25 mg
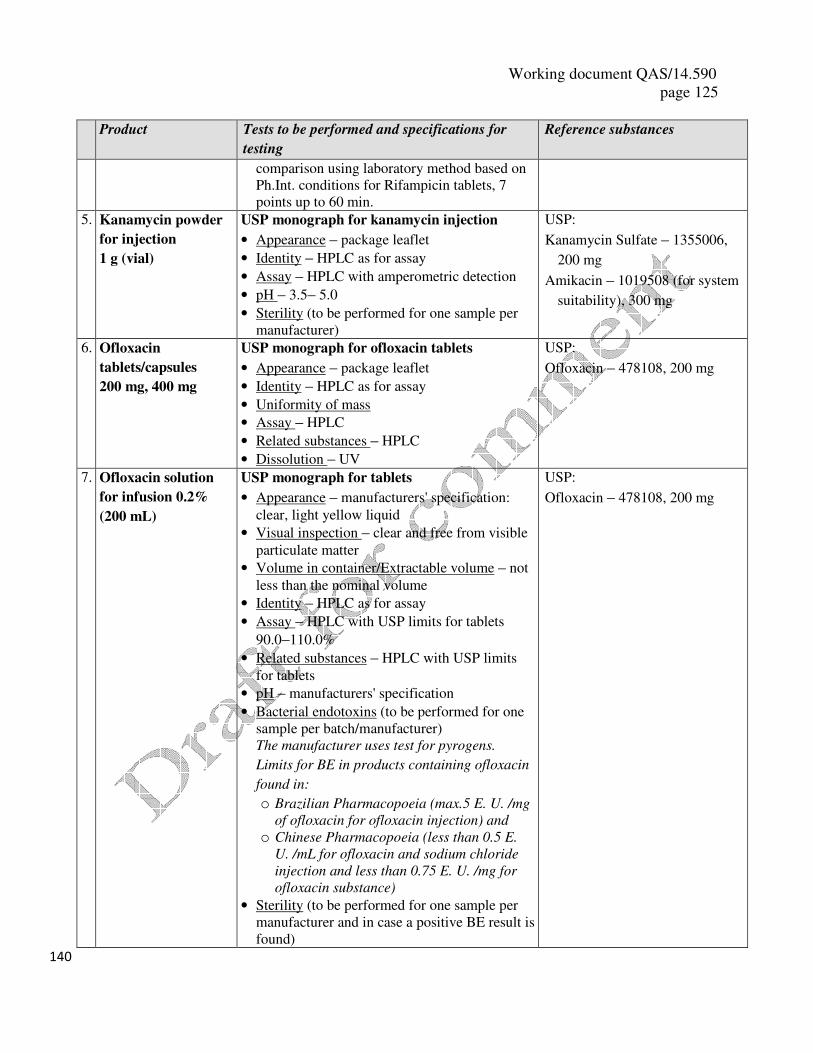
Working document QAS/14.590
page 125
Product Tests to be performed and specifications for
testing
Reference substances
comparison using laboratory method based on
Ph.Int. conditions for Rifampicin tablets, 7
points up to 60 min.
5. Kanamycin powder
for injection
1 g (vial)
USP monograph for kanamycin injection
• Appearance – package leaflet
• Identity – HPLC as for assay
• Assay – HPLC with amperometric detection
• pH – 3.5– 5.0
• Sterility (to be performed for one sample per
manufacturer)
USP:
Kanamycin Sulfate – 1355006,
200 mg
Amikacin – 1019508 (for system
suitability), 300 mg
6. Ofloxacin
tablets/capsules
200 mg, 400 mg
USP monograph for ofloxacin tablets
• Appearance – package leaflet
• Identity – HPLC as for assay
• Uniformity of mass
• Assay – HPLC
• Related substances – HPLC
• Dissolution – UV
USP:
Ofloxacin – 478108, 200 mg
7. Ofloxacin solution
for infusion 0.2%
(200 mL)
USP monograph for tablets
• Appearance – manufacturers' specification:
clear, light yellow liquid
• Visual inspection – clear and free from visible
particulate matter
• Volume in container/Extractable volume – not
less than the nominal volume
• Identity – HPLC as for assay
• Assay – HPLC with USP limits for tablets
90.0–110.0%
• Related substances – HPLC with USP limits
for tablets
• pH – manufacturers' specification
• Bacterial endotoxins (to be performed for one
sample per batch/manufacturer)
The manufacturer uses test for pyrogens.
Limits for BE in products containing ofloxacin
found in:
o Brazilian Pharmacopoeia (max.5 E. U. /mg
of ofloxacin for ofloxacin injection) and
o Chinese Pharmacopoeia (less than 0.5 E.
U. /mL for ofloxacin and sodium chloride
injection and less than 0.75 E. U. /mg for
ofloxacin substance)
• Sterility (to be performed for one sample per
manufacturer and in case a positive BE result is
found)
USP:
Ofloxacin – 478108, 200 mg
140
Working document QAS/14.590
page 126
126
EXAMPLE OF SURVEY PROTOCOL 141
6. CONTENT OF THE ANALYTICAL TEST REPORT 142
143
Analytical test report 144
The report of the results, including the final conclusion of the analysis of a sample which has been 145
submitted by a laboratory in another country or in the field not having appropriate facilities to 146
perform certain tests, and issued by the official pharmaceutical control laboratory that performed the 147
test. This is often in the same style as a certificate of analysis. 148
The analytical test report shall in accordance with the good practices for national pharmaceutical control 149
laboratories provide the following information: 150
7. name and address of the laboratory performing the sample testing; 151
8. number/code of the analytical test report; 152
9. name and address of the originator of the request for testing; 153
10. sample code from the sample collection form; 154
11. date on which the sample was received; 155
12. name of the country where the sample was collected; 156
13. sample product name, dosage form, active ingredients, strength, package size, type and packaging 157
material of primary container; 158
14. description of the sample (both product and container); 159
15. batch number of the sample, expiry date and manufacturing date, if available; 160
16. name and address of the manufacturer; 161
17. reference to the specifications used for testing the sample, including the limits; 162
18. reference to the reference standards used for quantitative determinations; 163
19. results of all the tests performed (numerical results, if applicable); 164
20. conclusion whether or not the sample was found to be within the limits of the specifications used; 165
21. date on which the test was performed; 166
22. signature of the head of the laboratory or authorized person. 167
168
*** 169
170
171


















