Recent therapeutic advances in AL …nephro-necker.org/pdf/2013/20-Bridoux.pdf · Destabilise by...
39
Recent therapeutic advances in AL Recent therapeutic advances in AL amyloidosis amyloidosis and myeloma cast nephropathy and myeloma cast nephropathy Frank Bridoux 1 , Arnaud Jaccard 2 , Jean-Paul Fermand 3, Guy Touchard 1 Guy Touchard 1 CHU Poitiers, 2 CHU Limoges, 3 Hôpital Saint Louis, Paris, France Centre de référence des amyloses primitives et autres maladies de dépôts d’immunoglobulines monoclonales Actualités Néphrologiques Jean Hamburger Hôpital Necker 23 avril 2013
Transcript of Recent therapeutic advances in AL …nephro-necker.org/pdf/2013/20-Bridoux.pdf · Destabilise by...

Recent therapeutic advances in AL Recent therapeutic advances in AL amyloidosisamyloidosis and myeloma cast nephropathyand myeloma cast nephropathy
Frank Bridoux1, Arnaud Jaccard2, Jean-Paul Fermand3,
Guy Touchard1Guy Touchard1CHU Poitiers, 2CHU Limoges, 3Hôpital Saint Louis, Paris, France
Centre de référence des amyloses primitives et autres maladies de dépôts d’immunoglobulines monoclonales
Actualités Néphrologiques Jean HamburgerHôpital Necker23 avril 2013

Light chains filtered Light chains filtered (MW ~ 22 kDa)(MW ~ 22 kDa)
AL AL amyloidosisamyloidosisLCDDLCDD
TammTamm--HorsfallHorsfallproteinprotein
Cubilin Megalin
FanconiFanconisyndromesyndrome
mTALmTALMyelomaMyeloma castcastnephropathynephropathy


AL amyloidosisAL amyloidosis
Clonal plasma cells (MGUS/stage I myeloma)
Monoclonal light chains(lambda > kappa)
Amyloid fibrils
Amyloid deposits
Slow spontaneous tissue catabolism (SAP binding)
Progressive alteration of organ structure and function
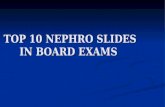
AL AL amyloidosisamyloidosis: : diagnosisdiagnosis
Anti-lambda x 200 Anti-kappa x 200

DNA screening in 350 patients DNA screening in 350 patients with apparent AL with apparent AL amyloidosisamyloidosis
34 (9.7%) had amyloidogenic mutations, confirmed to be the cause of their disease
18 Fibrinogen A alpha chain Val52613 Variants of TTR, including 4 new ones13 Variants of TTR, including 4 new ones2 Apolipoprotein A1 (Pro175 and Arg26)1 Lysozyme His67Of those, 8 had evidence of monoclonal
gammopathy…
Lachmann HJ et al., NEJM 2002;346:1786
Incomplete penetrance → family history sometimes lacking

Fibrinogen A Fibrinogen A αα--chain chain amyloidosisamyloidosis
Lachmann HJ et al., NEJM 2002;346:1786

Diagnosis of Diagnosis of amyloidosisamyloidosis
• Unsuccessful typing after IF/IHC?
– Molecular biology : amyloidogenic mutation?
• glomerular deposits only → AαFib
• Tubulo-interstitial deposits only → AapoA1 (Leu175Pro)
– Laser capture-microdissection and – Laser capture-microdissection (paraffin-embedded samples) and tandem mass spectrometry and proteomic analysis :
• sensitivity ~ 100%, specificity ?
– Immuno-electron microscopy :
→ correct typing in > 90% of cases
Sehti S et al. Kidney Int 2012
Arbustini E, et al. Amyloid 2002; 9:108
Herrera GA. Ultrastruct Pathol 2010; 34:161

100,0
1000,0
10000,0
100000,0
AL AL amyloidosisamyloidosis : prognostic markers: prognostic markers
Abnormal FLCs in 98% of AL patients
Kappa FLC mg/l
0,1
1,0
10,0
0,1 1,0 10,0 100,0 1000,0 10000,0 100000,0
Lachmann et al. Br J Haematol 2003; 348: 2583

Validation of response criteria in AL Validation of response criteria in AL amyloidosisamyloidosis
XII International Symposium on Amyloidosis, Rome, A pril 18-21, 2010Gertz MA, Merlini G. Amyloid 2010; 17(Suppl 1): 48-49
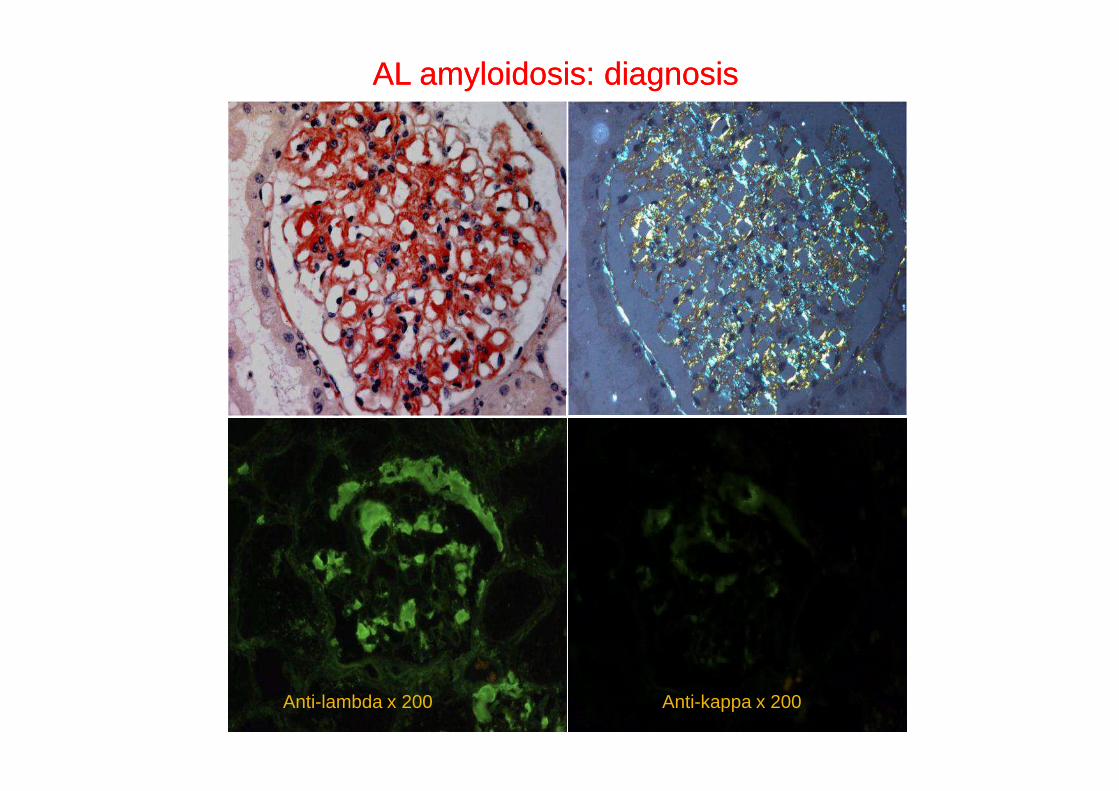
AL AL amyloidamyloid cardiomyopathycardiomyopathy
• Heart involvement : 60 % of patients at diagnosis
• Major prognostic factorMain causes of death :
conduction blocks /arrhythmia
Kyle RA N Engl J Med 1997; 336: 1202Kapoor P, et al. Am J Med 2011; 124: 1006
Median survival = 5 months

Serum markers of heart involvement Serum markers of heart involvement The Mayo Clinic staging systemThe Mayo Clinic staging system
Threshold values:• Troponin T (cTnT) : 0.035 mg/L• NT-proBNP : 332 ng/L
Stage 1 : 2 normal valuesStage 2 : 1 abnormal valueStage 3 : 2 abnormal valuesStage 3 : 2 abnormal values
High sensitive cTnT :
Threshold 50 ng/L?
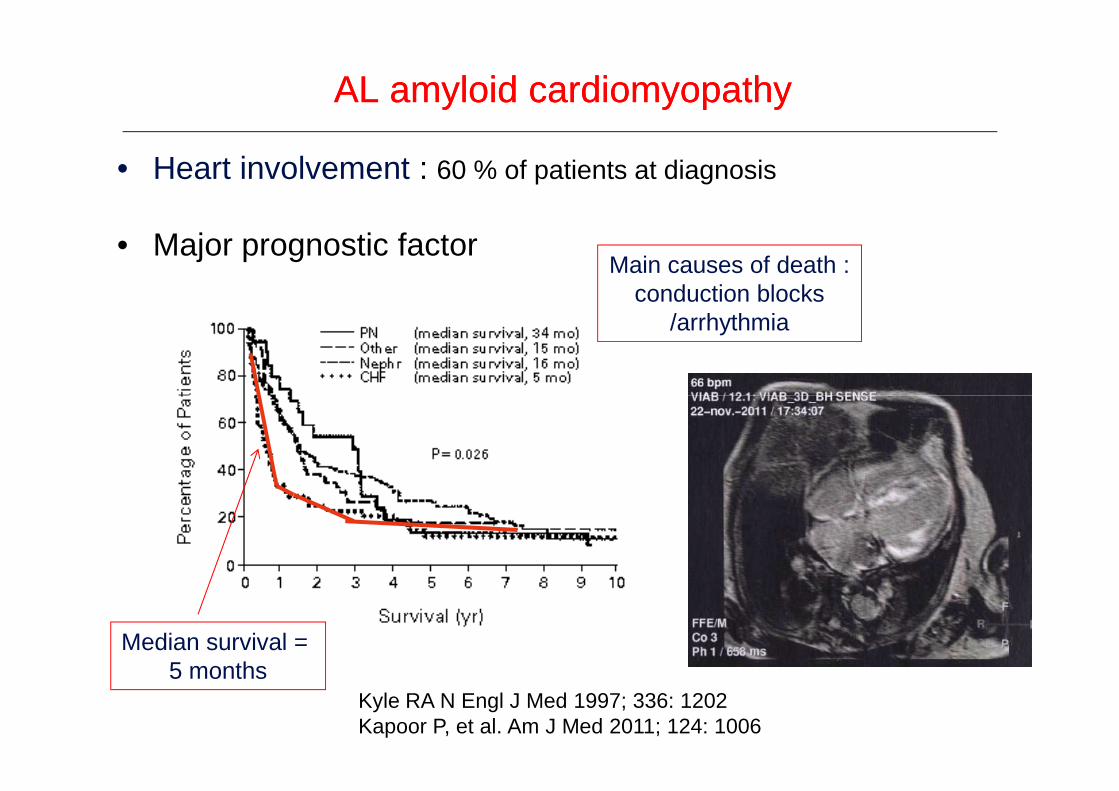
Native Native proteinprotein Amyloid depositsAmyloid deposits
FibrillogenesisFibrillogenesis
�Reversion to native fold
+
AmyloidosisAmyloidosis : treatment strategies: treatment strategies
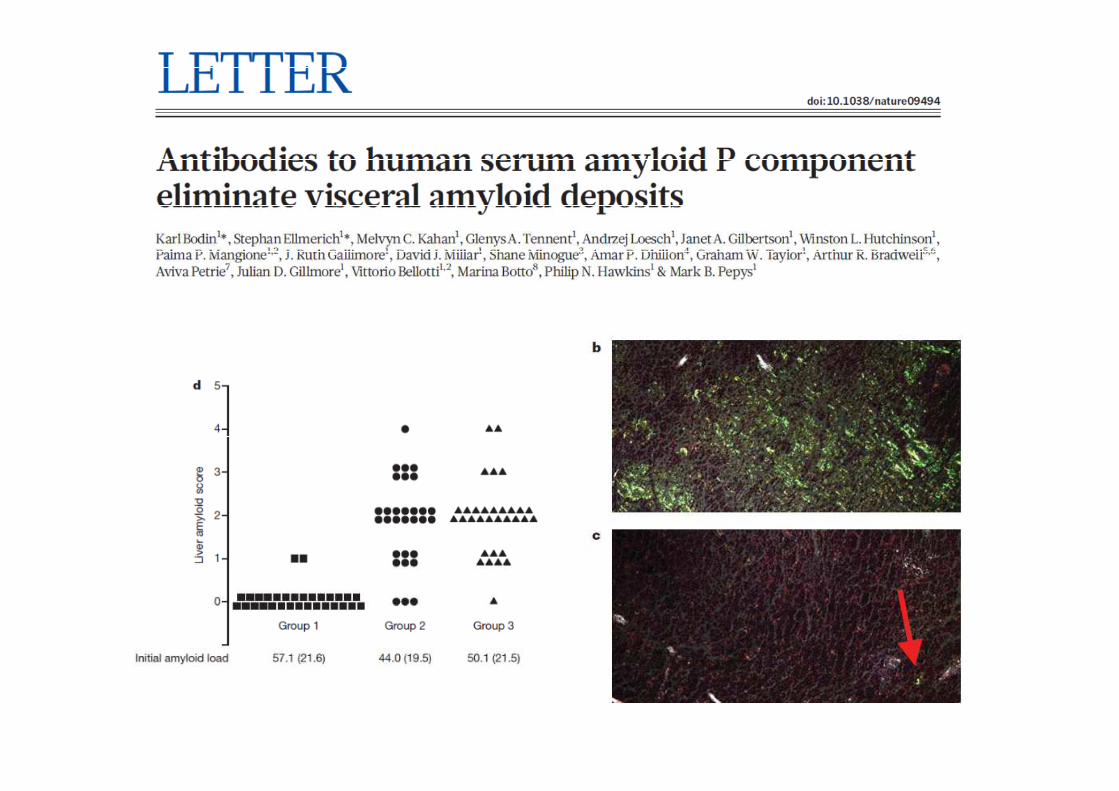
�Immunotherapy
�Destabilise by SAP depletion
�Reduce supply of amyloid
precursor protein
�Stabilise precursor ccccc proteins
�Inhibit GAG cccc binding
�β sheet breakers
-
--
Courtesy of PN Hawkins and JD Gillmore, National Amyloidosis Centre, London
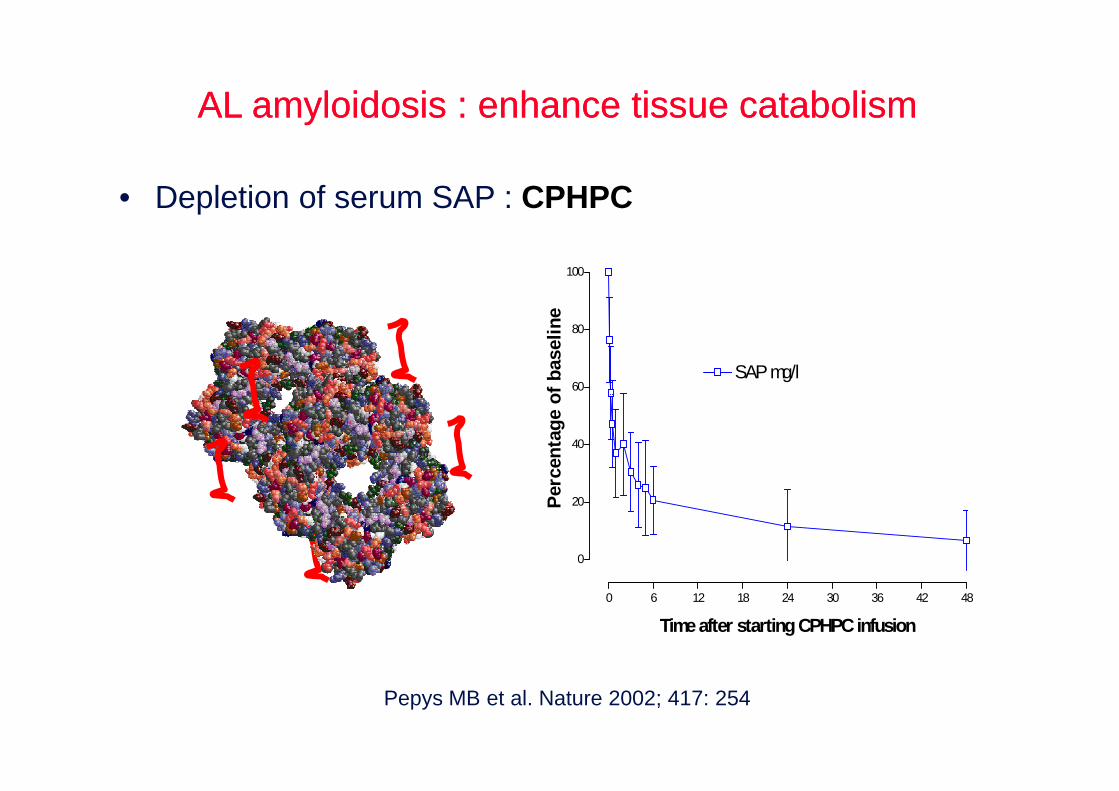
AL AL amyloidosisamyloidosis : : enhanceenhance tissue tissue catabolismcatabolism
• Depletion of serum SAP : CPHPC
60
80
100
SAP mg/l
Per
cent
age
of b
asel
ine
0 6 12 18 24 30 36 42 48
0
20
40
Time after starting CPHPC infusion
Per
cent
age
of b
asel
ine
Pepys MB et al. Nature 2002; 417: 254

• Oral Melphalan + Prednisone (MP):
- Median survival : 18 months
- Hematological response rate <30%
- Delayed response (6-12 mo)
→ insufficient in patients with
heart disease
Standard dose Standard dose chemotherapychemotherapy in AL in AL amyloidosisamyloidosis
heart disease
Kyle et al. N Engl J Med, 1997; 336: 1202
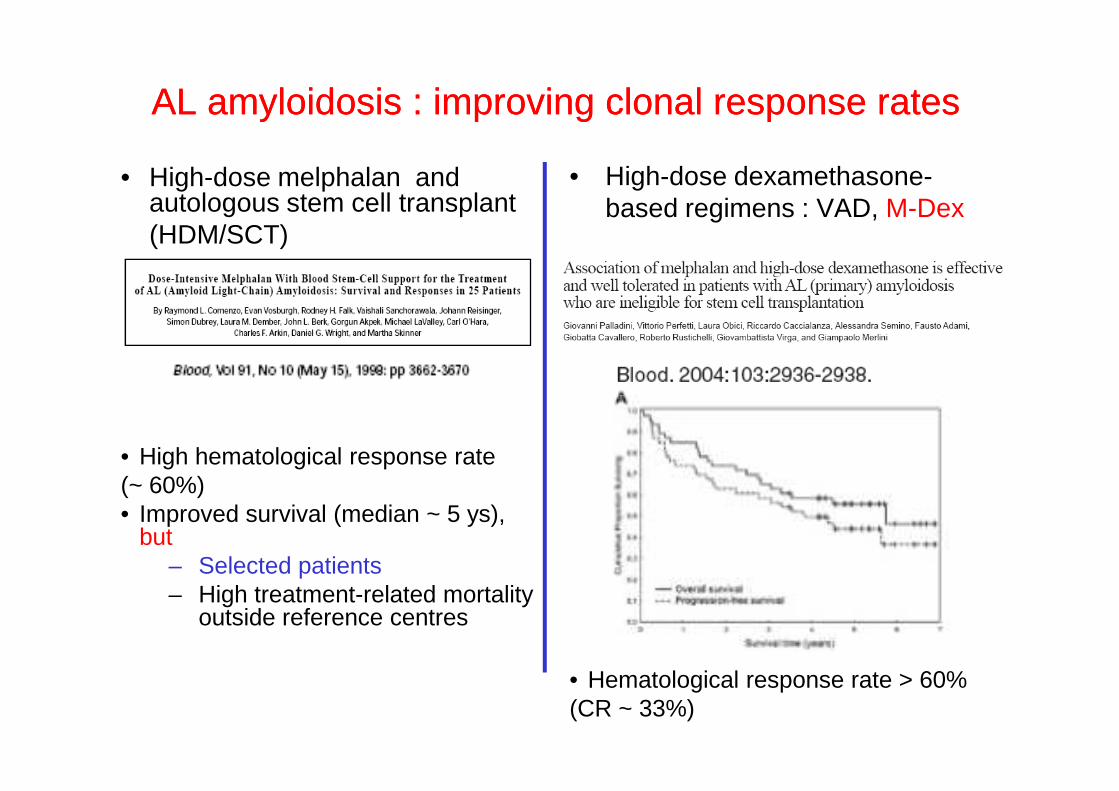
AL AL amyloidosisamyloidosis : improving : improving clonalclonal response ratesresponse rates
• High-dose melphalan and autologous stem cell transplant(HDM/SCT)
• High-dose dexamethasone-based regimens : VAD, M-Dex
• High hematological response rate (~ 60%) • Improved survival (median ~ 5 ys),
but – Selected patients – High treatment-related mortality
outside reference centres
• Hematological response rate > 60%(CR ~ 33%)
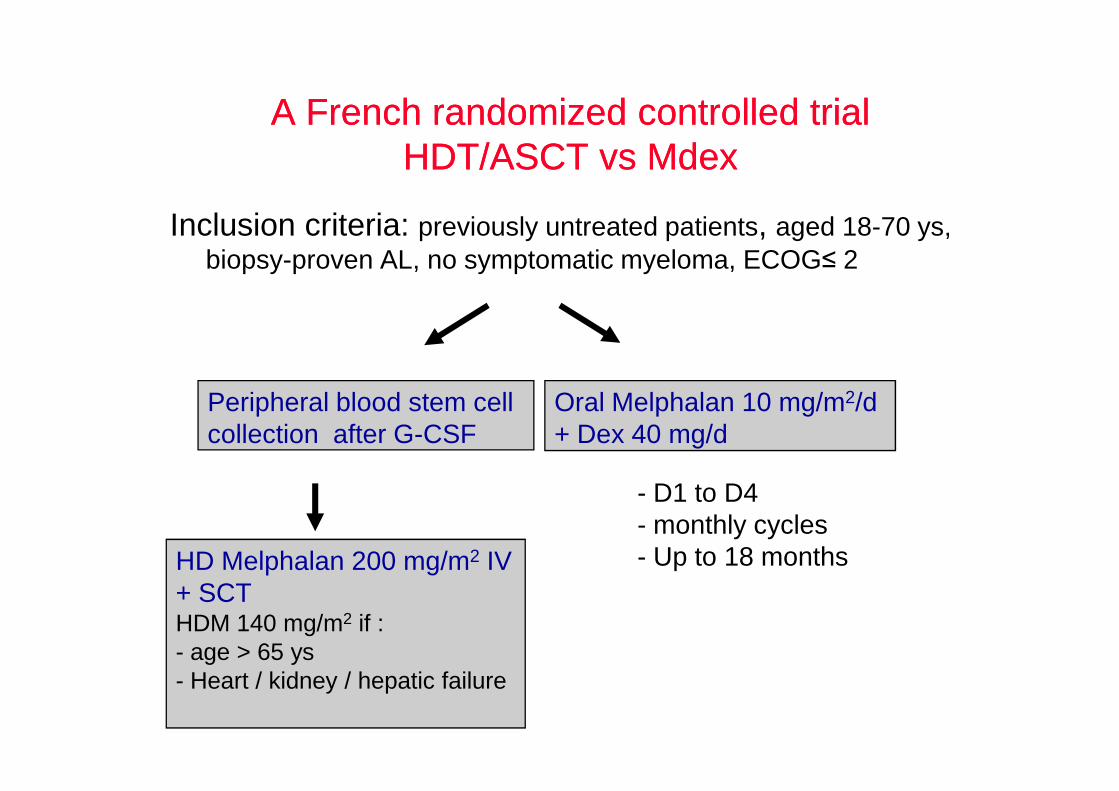
A French randomized controlled trialA French randomized controlled trialHDT/ASCT HDT/ASCT vsvs MdexMdex
Inclusion criteria: previously untreated patients, aged 18-70 ys, biopsy-proven AL, no symptomatic myeloma, ECOG≤ 2
Peripheral blood stem cell Oral Melphalan 10 mg/m2/d Peripheral blood stem cell collection after G-CSF
Oral Melphalan 10 mg/m2/d + Dex 40 mg/d
HD Melphalan 200 mg/m2 IV+ SCTHDM 140 mg/m2 if :- age > 65 ys- Heart / kidney / hepatic failure
- D1 to D4 - monthly cycles- Up to 18 months
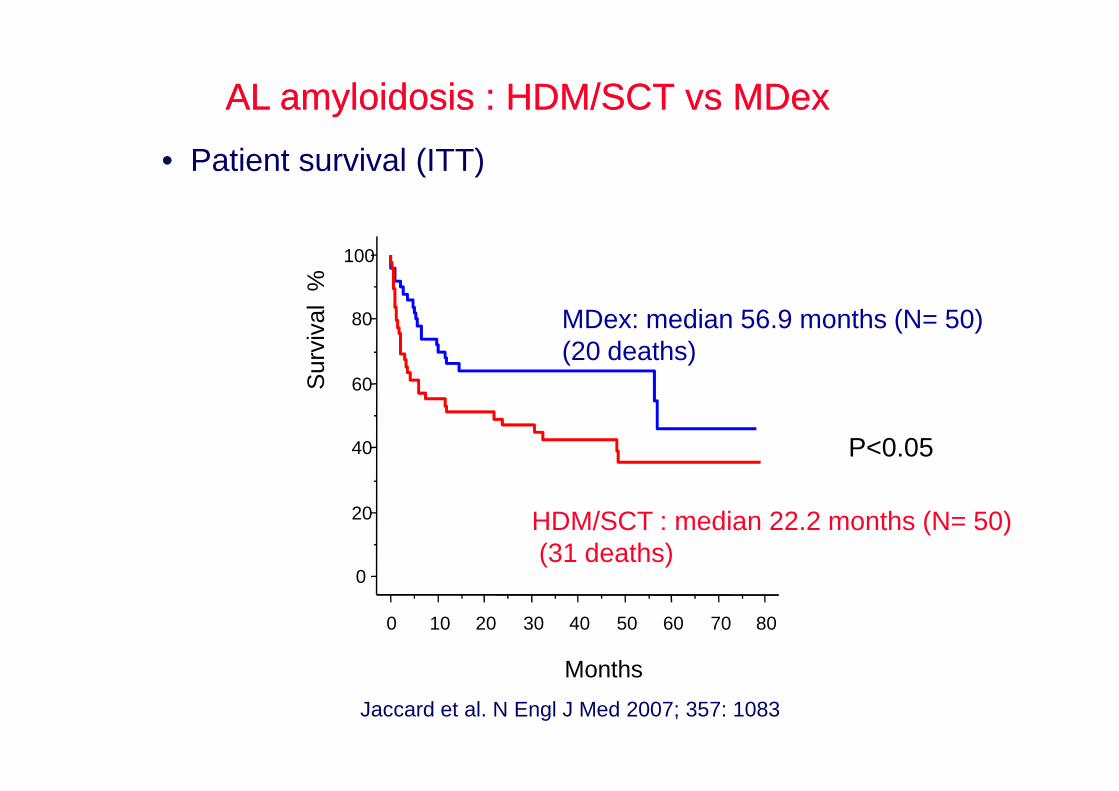
• Patient survival (ITT)
AL amyloidosis : HDM/SCT vs MDexAL amyloidosis : HDM/SCT vs MDex
60
80
100
MDex: median 56.9 months (N= 50)(20 deaths)
Sur
viva
l%
P<0.05
0
20
40
0 10 20 30 40 50 60 70 80
HDM/SCT : median 22.2 months (N= 50)(31 deaths)
Months
Jaccard et al. N Engl J Med 2007; 357: 1083

• Low risk versus high risk (Mayo Clinic criteria)Low risk: interventricular septum thickness ≤ 15 mm, LVEF > 55%, serum creatinine ≤ 2.0 mg/dL, total bilirubin ≤ 2.0 mg/dL
80
100
Sur
viva
l %
Low risk (N=60)
p = 0.13MDex
AL amyloidosis : HDM/SCT vs MDexAL amyloidosis : HDM/SCT vs MDex
0
20
40
60
80
Sur
viva
l %
0 10 20 30 40 50 60 70
Months
Low risk (N=60)HDM
High risk (N= 40)
p = 0.97MDex
HDM

HDM/SCT vs MDex : conclusionsHDM/SCT vs MDex : conclusions
• MDex > HDM/SCT:
– Most patients eligible, moderate toxicity, oral route– Similar response rates– Survival :– Survival :
• Similar in low-risk patients• Equally poor in high-risk patients
MdexMdex: first: first--line line therapytherapy in in mostmost EuropeanEuropean centerscenters sincesince 20072007
Jaccard et al. N Engl J Med 2007; 357: 1083

Other strategies required in :Other strategies required in :
,6
,8
1
Cum
. Sur
viva
l
,6
,8
1
Cum
. Sur
viva
l
0
,2
,4
0 10 20 30 40 50 60 70 80
Cum
.
0
,2
,4Cum
. Sur
viva
l
0 10 20 30 40 50 60 70 80
Months
High-risk patients(Mayo Clinic stage III)
Non-responders
Months

Novel antiNovel anti--myeloma agents in AL myeloma agents in AL amyloidosisamyloidosis
• Thalidomide• Lenalidomide (Revlimid®) + dexamethasone• Bortezomib (Velcade®)
• Combined with alkylating agents : melphalan, • Combined with alkylating agents : melphalan, cyclophosphamide
• In development:� Bendamustine� Pomalidomide� Novel proteasome inhibitors (carfilzomib)� Monoclonal antibodies targeting plasma cells (daratuzumab, elotuzumab)

StandardStandard--dose regimens including novel agents in ALdose regimens including novel agents in AL
-
-
-
-
-
-
50%
HRR(%)
Cyclo-Dex + Thalidomide
MDex MDex + Revlimid
MDex + Bortezomib
Bortezomib - Dex
ORR100%
-
-
-
-
-50% Revlimid
Moreau, Blood 2010
Zonder ASH, 2009
Kastritis, JCO 2010
CR 40%
Cy-Bor-D
Wechalekar, Blood 2009
Mickael, Blood 2012
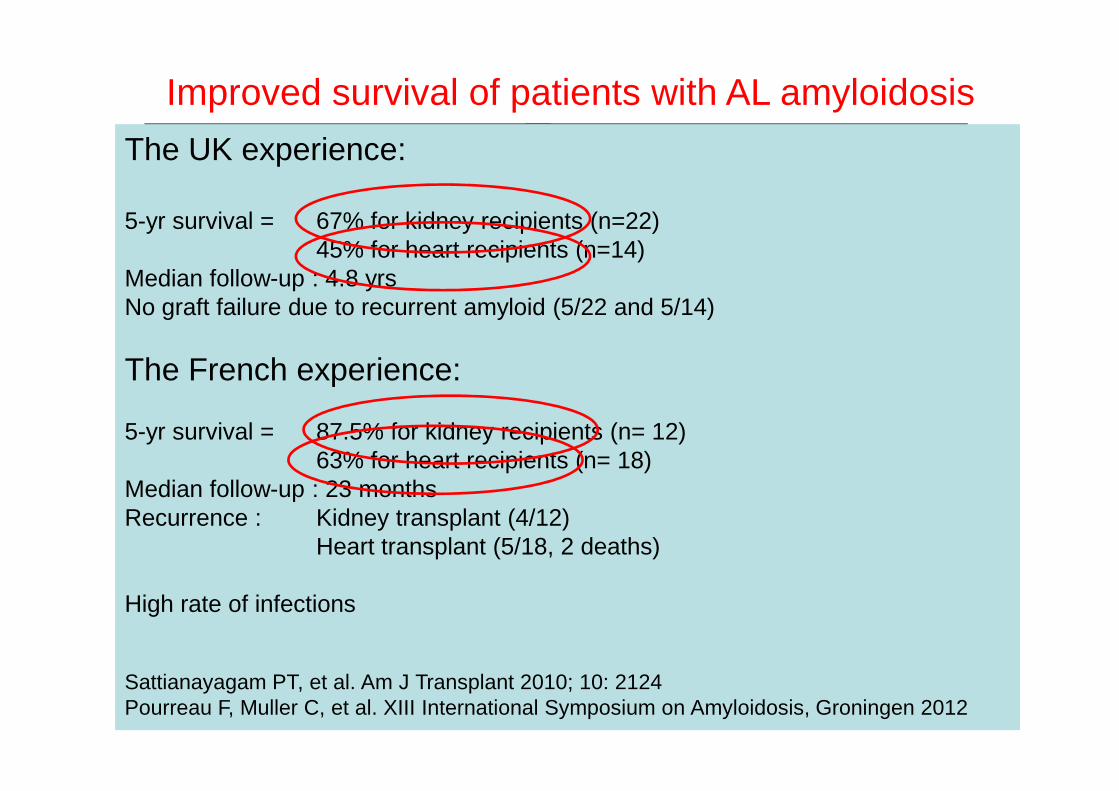
Improved survival of patients with AL amyloidosis
0.4
0.6
0.8
1.0Proportion surviving
1995-1999 (n=208)
2000-2004 (n=418)
2005-2008 (n=352)
p=0.016Solid organ transplantation = a valid option providing suppression of the underlying plasma cell clone
and limited disease extension
The UK experience:
5-yr survival = 67% for kidney recipients (n=22) 45% for heart recipients (n=14)
Median follow-up : 4.8 yrsNo graft failure due to recurrent amyloid (5/22 and 5/14)
The French experience:
Merlini et al. XIII Intl. Workshop on Myeloma, Paris, 2011
00.0
24 48 72 96 120 144 168
Time (mths)
0.2 1984-1994 (n=153)
5-yr survival = 87.5% for kidney recipients (n= 12)63% for heart recipients (n= 18)
Median follow-up : 23 monthsRecurrence : Kidney transplant (4/12)
Heart transplant (5/18, 2 deaths)
High rate of infections
Sattianayagam PT, et al. Am J Transplant 2010; 10: 2124Pourreau F, Muller C, et al. XIII International Symposium on Amyloidosis, Groningen 2012

ConclusionsConclusions
• M-Dex: current standard of care
• Already challenged by the novel anti-myeloma agents
to be introduced rapidly :- after 1 to 3 courses of M-Dex if no clonal response (Mayo stage 1-2)- VCD (CyBorD) as first-line if Mayo stage 3
• Early diagnosis of AL amyloidosis is crucial
• Chemotherapy guided by frequent assessment of FLC andcardiac biomarkers
International phase III trial M-Dex vs M-Dex + Bortezomib
• HDM/SCT ? limited to highly selected patients, experienced centers

Myeloma cast nephropathy Myeloma cast nephropathy
• Main cause of AKI in MM(30 to >80% in pathological studies)
• High mass MM (LC MM)• No LC over-representation• Predominant LC (> 70%) proteinuria• Precipitating factors• May be associated with other LC
nephropathies• Renal recovery : 50% (<20% if HD)

MCN : impact of ESRD on patient MCN : impact of ESRD on patient survivalsurvival
N = 85 patients with hematological response ≥ PR
Leung N, Bridoux F, Kumar S, et al. ASH 2011, abstract 3949
RR = free of RR = free of dialysisdialysisNR = on NR = on dialysisdialysis

Light chains filtered (MW ~ 22 kDa)
TammTamm--HorsfallHorsfallproteinprotein
Myeloma cast nephropathy : Myeloma cast nephropathy : pathophysiologypathophysiology
Excessive LC endocytosis in PT :→ Activation of redox pathways→ Increased expression of NFκκκκB and MAPK→ Transcription of IL-6, IL-8, CCL2, TGFββββ-1→ Morphological changesApoptosis, epithelial-mesenchymal transition→ Renal fibrosis
mTALMyelomaMyeloma castcastnephropathynephropathy
Sanders PW et al. J Clin Invest 1988Sengul S et al. Kidney Int 2002
LC interaction with THP :→ 9 amino-acid binding region of THP interacts with LC CDR3→ Increased by : dehydration, acidic urine pH, high Ca, infection
furosemide, NSAids, contrast media…→ Tubular obstruction→ Morphological changesTubular atrophy, interstitial inflammation, giant-cell reaction (tubulorrhexis)→ Renal fibrosis

Binding interaction between LCs and THP- Variable binding affinity depending on key amino-acids in CDR3
Myeloma cast nephropathy : Myeloma cast nephropathy : pathophysiologypathophysiology
Mutational analysis of the CDR3 sequence
Ying et al. J Clin Invest , 2012
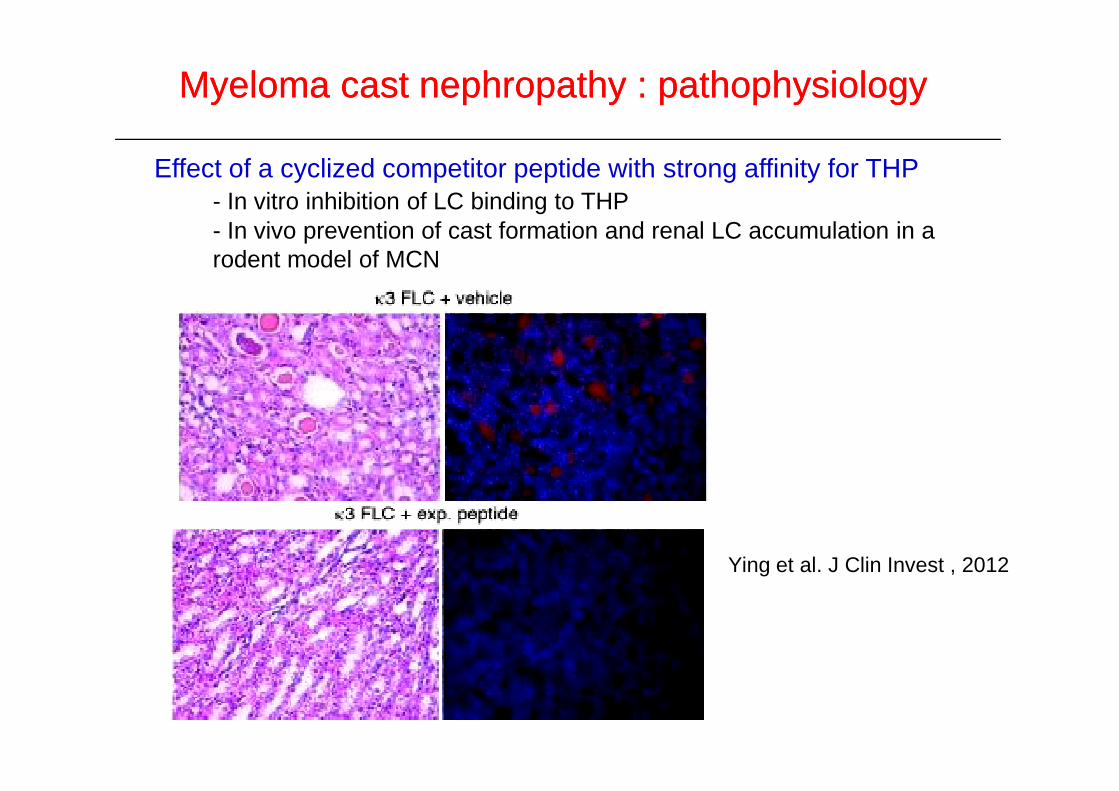
Effect of a cyclized competitor peptide with strong affinity for THP- In vitro inhibition of LC binding to THP- In vivo prevention of cast formation and renal LC accumulation in a rodent model of MCN
Myeloma cast nephropathy : Myeloma cast nephropathy : pathophysiologypathophysiology
Ying et al. J Clin Invest , 2012

Treatment of myeloma cast nephropathy :Treatment of myeloma cast nephropathy :Symptomatic measures Symptomatic measures
Urgent treatment required to reduce concentration and precipitation of urine FLCs
• Vigorous rehydration with saline and alkaline fluids
• Urine pH ≥ 7.0
• Correction of hypercalcemia : rehydration (avoid loop diuretics), bisphosphonates
• Stop NSAIDs, RAS blockers
• Treatment of concomitant infections with non-nephrotoxic antibiotics

Treatment of myeloma cast nephropathy :Treatment of myeloma cast nephropathy :Which chemotherapy? Which chemotherapy?
• High-dose steroids (HD-Dex)
• + Drugs which do not require dose adaptation to reduced GFR :
• Adriamycin
• Cyclophosphamide• Cyclophosphamide
• Bendamustine
• Thalidomide
• Bortezomib
~ ~ No randomized trial in myeloma patients with renal impairment No randomized trial in myeloma patients with renal impairment

• Bortezomib and renal response
TreatmentTreatment of MCN : of MCN : BortezomibBortezomib
N Regimen ≥ PR Renalresponse
Dialysis withdrawal
OS 2 yrs
Toxicity
Dimopoulos2009
46 BD ±various
59%(CR 30%)
2/9 Similar to pts without RI
Morabito2010
117 BD ±various
73% 41% 3/14 51% Similar to pts without RI
• Predicting factors of renal response :
− LC myeloma, absence of previous chemo., eGFR > 30 ml/min/1.73m2
Dimopoulos et al. Clin Lymphoma Myeloma 2009; 9: 302
− Baseline eGFR and hematological response
Ludwig et al. J Clin Oncol 2010; 28: 4635
2010 various without RI
Ludwig2010
68 BD + doxo.
66% 62% (CR 31%)
58% Similar to pts without RI

Treatment of myeloma cast nephropathy :Treatment of myeloma cast nephropathy :FLC removalFLC removal
• Is there a role for plasmapheresis ?
• Randomized prospective trial : 104 MM with AKI• 5 to 7 PE sessions (50 ml/kg) + VAD or MP
vs chemo. alonevs chemo. alone• No significant difference in the two arms for the primary study
end-point : death/need for dialysis/severe CKD with DFG < 30ml/min/1.73 m2
Clark WF, et al. Ann Intern Med 2005; 143: 777

Median number of PE = 8 (3-14)Renal response = 12/14 (86%)CR = 6/14 (43%)
Burnette, Leung & Rajkumar. N Engl J Med 2011; 364: 2365-6
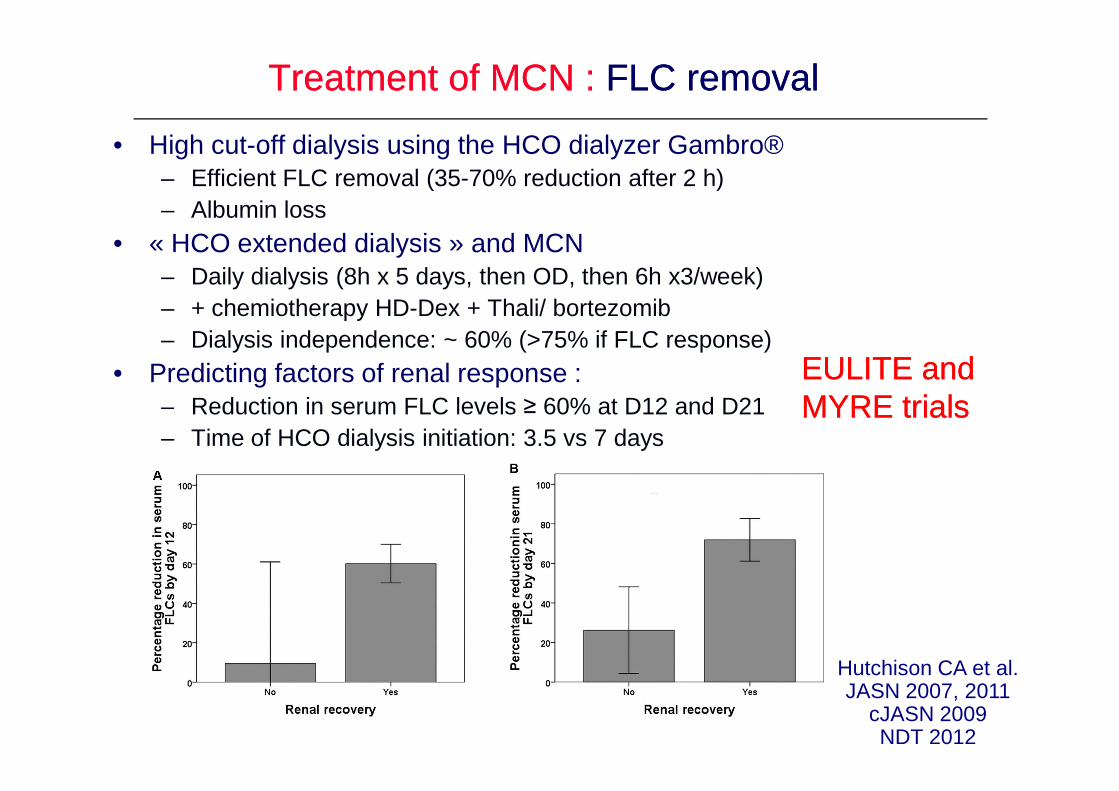
Treatment of MCN : Treatment of MCN : FLC removal FLC removal
• High cut-off dialysis using the HCO dialyzer Gambro®– Efficient FLC removal (35-70% reduction after 2 h)– Albumin loss
• « HCO extended dialysis » and MCN– Daily dialysis (8h x 5 days, then OD, then 6h x3/week)– + chemiotherapy HD-Dex + Thali/ bortezomib– Dialysis independence: ~ 60% (>75% if FLC response)
• Predicting factors of renal response : – Reduction in serum FLC levels ≥ 60% at D12 and D21
EULITE and EULITE and MYRE trialsMYRE trials– Reduction in serum FLC levels ≥ 60% at D12 and D21
– Time of HCO dialysis initiation: 3.5 vs 7 days
Hutchison CA et al. JASN 2007, 2011
cJASN 2009NDT 2012
MYRE trialsMYRE trials

Study objectives :1. EpidemiologyFrequency of MCN and other renal disorders in patients with monoclonal gammopathy and renal impairment
2. Treatment of MCN
AKI and multiple AKI and multiple myelomamyeloma ::
MYRE trial MYRE trial (NCT 01208818)
*Requiring dialysis = Bortezomib + Dex, comparaison of :
2 intensive hemodialysis regimens - high cut-off dialyzer (Gambro Theralite 2.1 m2)- conventional high-flux dialyzer
In patients with newly diagnosed MM and AKI secondary to MCN*Not requiring dialysis , comparison of :
– Bortezomib (Velcade®) + Dex (VD)– Bortezomib (Velcade®) + Dex + Cyclophosphamide (VCD)
2. Treatment of MCN

Acknowledgements
Services de Néphrologie et Pathologie, CHU PoitiersEstelle DesportCorinne Lacombe, Beatrice Fernandez, Nathalie Quellard, Jean-Michel Goujon
CNRS UMR7276, LimogesChristophe Sirac, Michel Cogné, Sébastien Bender, Claire Carrion
Centre de référence Amylose AL et autres maladies par dépôts d’Ig monoclonales
Department and Laboratory of Nephrology, UCL Medical School, BrusselsOlivier Devuyst, Sara Terryn, Claudia Raggi


![URINARY EXCRETION OF ALBUMIN - nephro-necker.org · urinary excretion of albumin ... tojo and endou [12], ... 105, 1353-1361 2000. renal albumin handling in megalin knock out mice](https://static.fdocuments.us/doc/165x107/5c4a0c7693f3c317653c31ff/urinary-excretion-of-albumin-nephro-urinary-excretion-of-albumin-tojo.jpg)