Recent advances in pain management
86
RECENT ADVANCES IN PAIN MANAGEMENT DR.K.KISHORE
-
Upload
krishna-kishore -
Category
Health & Medicine
-
view
24 -
download
2
Transcript of Recent advances in pain management
RECENT ADVANCES IN PAIN MANAGEMENT
DR.K.KISHORE

PAIN
• DEFINITION: “An unpleasant sensory and emotional
experience associated with actual or potential damage” .
• PAIN IS SUBJECTIVE REACTION TO AN OBJECTIVE STIMULUS.

DIFF. MODALITIES OF TREATMENT

Multimodal analgesia:
• Different classes of analgesics using different routes of administration such as iv and epidural are used to produce fewer side effects of sedation, nausea,vomiting, pruritis, constipation, and improved pain relief.
• Multimodal analgesia also can produce opioid sparing.
• Faster recovery, reduced hospital stay, and decreased length of convalescence can occur if multimodal analgesia is combined with a rehabilitation program that is multidisciplinary and multimodal.

PAIN MANAGEMENT
• PHARMACOLOGICAL : >90%
• NONPHARMACOLOGICAL : <10% INTERVENTIONAL NONINTERVENTIONAL

WHO LADDER

Pain
Step 1±Nonopioid± Adjuvant
Pain persisting or increasing
Step 2Opioid for mild to moderate pain
±Nonopioid ± Adjuvant
Pain persisting or increasing
Pain persisting or increasing
Step 3Opioid for moderate to severe pain
±Nonopioid ±Adjuvant
Invasive treatments
Opioid Delivery
Quality of Life
MODIFIED WHO ANALGESIC LADDER
Proposed 4th Step
The WHOLadder
Deer, et al., 1999


OPIOIDS• Opioid use worldwide is increasing; in many
countries opioid availability is limited by legislation or circumstances .
• Data on long-term benefits are limited except for highly selected patients, while risks of abuse, diversion and even mortality are high .
• Multiple new formulations, aimed at increased speed of onset or reduced risk of abuse and diversion, are or have been recently developed.
• A large number of deaths have been reported with these preparations if used inappropriately .
• Combinations with antagonists such as naloxone (in buprenorphine or oxycodone preparations) and naltrexone (in a morphine preparation) are also available or have been investigated .
• TAPENTADOL:• Centrally acting analgesic • Dual mode of action as an agonist at the μ-opioid
receptor and as a norepinephrine reuptake inhibitor.
• Used in the treatment of moderate to severe chronic pain that proves unresponsive to conventional non-narcotic medications.
• 18-fold affinity for the μ opioid receptor in as compared to morphine.
• 3 times less analgesic than morphine.• Improved GI tolerability when compared to
opioids.

• Dose adjustment for tapentadol is not needed in the presence of renal impairment.
• No Hepatoxicity. • Potency between Tramadol and Morphine.• Contraindicated in severe bronchial asthma,
paralytic ileus, and patients on MAOI (serotonin syndrome).
• Risk of death - lower than from conventional opioids
• It is similar to tramadol, but differs in not being a racemic mixture of two enantiomers with different pharmacological effects, has no active metabolites (which are relevant for tramadol’s mu opioid receptor agonism) and has only minimal serotonin effects .

• Transmucosal immediate-release formulations of fentanyl (TIRF) –
• Fentanyl -commonly used synthetic phenylpiperidine derivative.
• Initially developed for parenteral administration, with the oral route being of limited use due to high first pass metabolism.
• High lipophilicity and high potency make it suitable for both acute and chronic pain management .
• Oral transmucosal fentanyl citrate (OTFC) .
• Oral disintegrating tablets (ODT) of fentanyl:
• mixture of carrier particles coated with fentanyl .• These particles adhere to the oral mucosa through a
mucoadhesive agent aiming for rapid absorption and result in good control of breakthrough pain .
• Fentanyl buccal tablets (FBT):• an effervescent disintegrating tablet, which enhances
early systemic uptake by changing the mucosal pH to increase unionized fentanyl concentration in the area of absorption .
• Fentanyl buccal soluble films (FBSF).


• Patient-controlled intranasal analgesia (PCINA):
• Intranasal (IN) opioids in the form of a dry powder or water or saline solution, are delivered using a syringe, nasal spray or dropper, or nebulized inhaler.
• Needle-free administration • bypass the hepatic first-pass effect• excellent perfusion of the nasal mucosa• rapid absorption and rise in plasma
concentration.• PCINA is efficacious, safe, non-invasive, and easy
to administer, but there are limited studies evaluating this route of analgesic administration in the postoperative period .
• Patient-controlled transpulmonary analgesia AeroLEF™(aerosolized liposome-encapsulated Fentanyl):
• Inhalation formulation of free and liposome-encapsulated fentanyl .
• AeroLEF™ is in development for the treatment of moderate to severe pain, including cancer pain.
• AeroLEF™ has a simple and noninvasive route of administration,
• rapid onset of action, • sustained effect, and • self-titratable dosing for the treatment of acute
and breakthrough pain.

• Extended-release epidural morphine (EREM) called DepoDur:
• Single-dose• Works locally to give long-lasting pain relief at the
site of surgical focus.• Duration of action: 48 hrs • Long-lasting analgesia in the absence of large
systemic concentrations of opioids as well as better patient activity levels.
• For surgeries like- knee arthroplasty and cesarean section.
• Side effects of EREM-treated with opioid antagonists.
• Pruritis and respiratory depression common.• Elderly sensitive to EREM, so close peri-operative
monitoring required.

• Patient-controlled fentanyl hydrochloride iontophoretic transdermal system (fentanyl ITS):
• Fentanyl ITS is an innovative, needlefree, self-contained, pre-programmed drug delivery system that uses iontophoretic technology to deliver fentanyl through the skin by application of a low-intensity electrical field.
• Not approved by the U.S. FDA for current clinical use; • Demonstrated to have efficacy and safety equivalent
to morphine IV-PCA in four RCT, and a meta-analysis.

• Adverse events - similar to those with IV opioid administration, including nausea, vomiting, pruritis, headache, and mild-to moderate dizziness.
• Disadv: as with all transdermal systems, skin hypersensitivity, skin redness, and hyperpigmentation.
• Use with extreme caution for in-patients with severe hepatic dysfunction, head injuries, sleep apnea, and impending respiratory failure and in pts with increased ICP of any etiology.


Analgesic adjuvants• Adjuvants are compounds, which by
themselves have undesirable side effects or low potency, but in combination with opioids allow a reduction of narcotic dosing for postoperative pain control.
• Needed for postoperative pain management due to s/e of opioid analgesics, which hinder recovery.

NON OPIOID ANALGESICS
• Acetaminophen (paracetamol)-• One of the oldest and most used analgesics, the
debate on its mechanism of action continues. • Mediated centrally and may involve direct and
indirect inhibition of central cyclo-oxygenases, but also the activation of the endocannabinoid system and spinal serotonergic pathways .
• Perioperative administration reduces postoperative nausea and vomiting (PONV), in particular if given prophylactically at induction of anesthesia .
• In therapeutic doses below 4 g/day, hepatotoxicity is very unlikely to occur .
• Acetaminophen intake has been linked to increase INR with warfarin treatment .


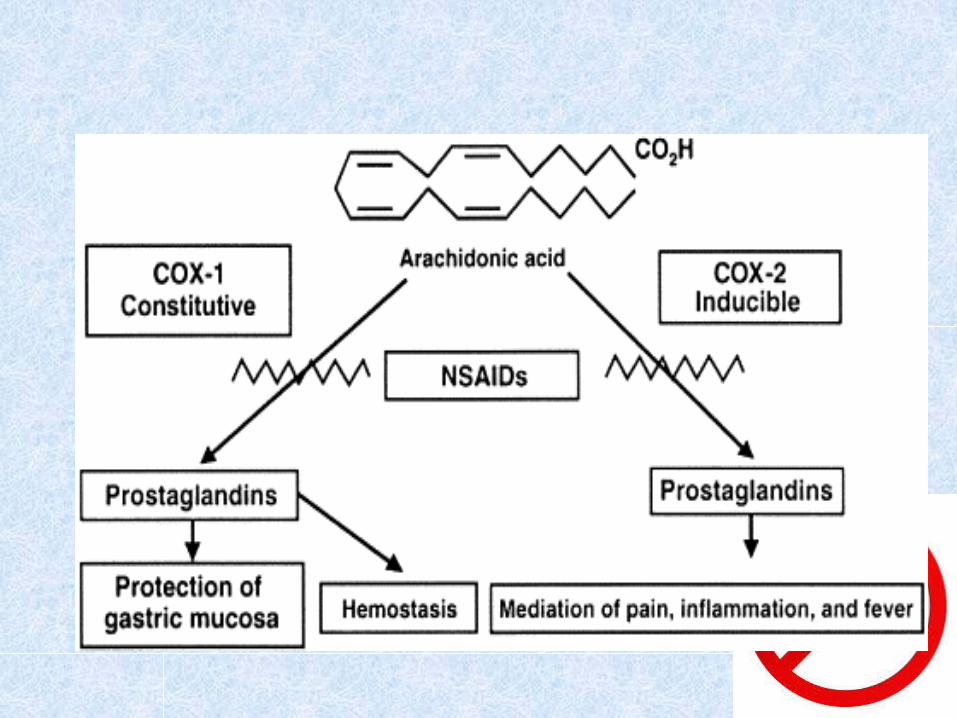
• Non-steroidal anti-inflammatory drugs (NSAIDs) –
• Fast-acting preparations provide better analgesia than slow-acting ones .
• There is no difference in analgesic efficacy between non-selective NSAIDs (nsNSAIDs) and COX-2 selective NSAIDs (Coxibs).
• With regard to gastrointestinal complications, in particular bleeds, coxibs carry a lower risk than nsNSAIDs .
• Coxibs are safe in patients with aspirin-sensitive asthma .
• In the perioperative setting, coxibs- do not impair platelet function , do not increase blood loss even after high-risk surgery such as total knee joint replacement ; this is in contrast to increased risk of bleeding with nNSAIDs .

• With regard to cardiovascular risk-with short-term use in the acute setting parecoxib/valdecoxib is
safe.• No recent new substances in this class of
analgesics. • Ketorolac as nasal spray, recently approved by
the FDA. • Other developments are preparations, which
permit use of lower doses of NSAIDs in an attempt to reduce adverse effects.
• Submicron particle NSAIDs (so called nano formulations); diclofenac as well as indomethacin have been tested in such formulations.
• A new formulation of injectable diclofenac sodium solubilized with hydroxypropyl-beta-cyclodextrin similarly showed efficacy at much reduced doses .
Alpha-2-delta modulators (gabapentin and pregabalin)
• Gabapentin :• Anti-epileptic drug • Analgesic effect in DM neuropathy, post-herpetic
neuralgia, and neuropathic pain. • Gabapentin does not bind to GABA A or GABA B
receptor but to the alpha-2 delta subunit of the presynaptic voltage gated-calcium channels responsible for the inhibition of the calcium influx.
• The inhibition of calcium release then prevents the release of excitatory neurotransmitters involved in the pain pathways.
• Potential for perioperative use as an analgesic adjuvant and anti-hyperalgesic agent when used in conjunction with opioids.
• Pregabalin: • Analgesic, Sedative, Anxiolytic, and Opioid-
sparing effect• Structural analog of GABA and a derivative of
gabapentin, used in various pain settings, including postoperative pain.
• Its MOA is similar to that of gabapentin . • Efficacy in neuropathic pain conditions such as
postherpetic neuralgia, painful diabetic neuropathy, central neuropathic pain, and fibromyalgia.

• Benefits-• reducing opioid requirements, • prevn and reduction of opioid tolerance, • improvement of the quality of opioid analgesia, • decreased respiratory depression, • relief of anxiety, and • gastric sparing.• Also used in certain specific operations such as
hysterectomy and laminectomy.• Currently no agreement on the ideal doses and
treatment duration for the indication of acute postoperative pain .

• Serotonin-norepinephrine reuptake inhibitors (SNRIs) :
• MOA- related to the inhibitory effects on norepinephrine and serotonin reuptake, thereby strengthening endogenous descending pathways of
pain control. • In the management of chronic pain, with tricyclic
antidepressants (TCAs), in particular amitriptyline, commonly being utilized in the treatment of neuropathic pain .
• For treatment of diabetic polyneuropathy, where both, duloxetine and venlafaxine, show better efficacy and a better benefit-risk balance than amitriptyline .
• Duloxetine and, to a lesser extent, milnacipran , are also effective in fibromyalgia .
• Also for conditions like chronic low back pain and osteoarthritis.

• Ketamine-• Originally introduced into clinical practice as a
dissociative anaesthetic in 1963 .• NMDA receptor antagonist.• iv, sc, epidural, transdermal, and intra-articular.• At low sub anesthetic doses (0.15–1 mg/kg),
ketamine exerts a specific NMDA blockade and, hence, modulates central sensitization.
• Ketamine appears to reduce the level of sensitisation by modulating the ‘wind up’ process.
• Ketamine also has a number of other sites of action including nicotinic, muscarinic, opioid, AMPA and Kainate receptors. It also inhibits serotonin and dopamine reuptake, and down regulates certain ion channels

• Use of sub-anesthetic doses of ketamine as an adjunct to provide postoperative pain relief in opioid-dependent patients
• Prevents opioid-induced hyperalgesia in patients receiving high doses of opioid for their postoperative pain relief.
• Adv effects- dizziness, blurred vision, nausea ,vomiting and hallucinations.
• After burns injury, it reduces wind-up and secondary hyperalgesia .

• CALCITONIN-• a polypeptide hormone produced naturally by the
para-follicular cells of the thyroid gland .• Uses-• CRPS later stages.• acute phantom limb pain after amputation.• pain caused by vertebral compression fractures.

• Cannabinoids:• Act upon the cannabinoid receptor• Receptor proteins include the endocannabinoids
such as anandamide, the phytocannabinoids and synthetic cannabinoids .
• Derivatives of the cannabis plant -used anecdotally to treat a variety of ailments such as anorexia, insomnia, pain and nausea .
• Primary active component is d-9-tetrahydrocannabinol (THC).
• At least another eighty-five different cannabinoids exist.

• CB1 receptors are found mainly within the brain, responsible for the analgesic, euphoric and anticonvulsive effects;
• they are however absent from the medulla oblongata, possibly explaining the lack of respiratory and cardiac depressive effects.
• CB2 receptors are found primarily within the immune system, modulate the cytokinin system and are believed to have anti-inflammatory and immunosuppressive effects.
• Dronabinol (a synthetic THC)-used as an antiemetic and as an appetite stimulant in AIDS related weight loss,
• Nabilone, a synthetic THC analogue- used for chemotherapy induced nausea and vomiting, with only minimal analgesic benefits in neuropathic pain.

Local anaesthetics• There are two approaches for prolongation of LA action: • One is the use of novel delivery techniques for existing
drugs. Liposome or polymer encapsulation of LA are being formulated.
• Second is the development of novel, extremely long-acting LA.
• Liposomes are microscopic phospholipid- bilayered vesicles that are biocompatible, biodegradable, and non-immumnogenic.
• Recently, new drug delivery systems utilizing nanoparticles, micro-particles composed of biodegradable polymers are developed.
• They have some advantages over liposomes in terms of stability both during storage and in vivo.

• Lidocaine plaster:• amide local anesthetic. • its effects are mediated by sodium channel
block • It has a potential to be a treatment for
neuropathic pain. • the development of a plaster for topical
administration of lidocaine has resulted in a new first-line treatment of localized neuropathic pain with minimal systemic adverse effects .

• Lidocaine plaster 5%, is a 10 cm × 14 cm patch containing around 700 mg lidocaine (50 mg/g of patch).
• The patch is placed directly over the painful area (intact skin only) for a period of 12 hrs f/b 12 hrs patch free time.
• Only around 3% of the lidocaine dose from the patch is absorbed.
• Used in diabetic neuropathy and post herpetic neuralgia
• Effective in the treatment of neuropathic pain and accompanying allodynia with fewer adverse events than pregabalin .

• Used in painful idiopathic sensory polyneuropathy, CRPS, carpal tunnel syndrome, postsurgical and posttraumatic pain.
• Also used in the elderly population and other high-risk groups.
• Most common adverse effects are skin irritation in the area of application.
• They can also be safely combined with systemic medications as part of a multimodal approach to pain management .

• Capsaicin:• 8-methyl-N-vanillyl-6-nonenamide• Non narcotic , acts peripherally.• TRPV-1 agonist . Capsaicin binds to the
transient receptor potential vanilloid 1 (TRPV1) subunits.
• TRPV1 is a receptor present on unmyelinated C fiber endings in the periphery. The activation of the TRPV receptors releases substance P

• While exposure to capsaicin results initially in a painful burning sensation due to substance P release, multiple administration of low concentration or single administration of high concentration capsaicin will finally lead to reduced sensitization or even complete desensitization.
• No effect on A delta and A alpha fibers and does not affect the temperature and touch sensations. Capsaicin cream contains capsaicin that is combined with narcotic analgesics and NSAIDS .
• Used for back pain, arthritic jointpains, and strains and sprains.
• Higher concentrations used for the treatment of the neuropathic pain of post herpetic neuralgia.
• It can be used in the elderly as an adjuvant, as it has opioid sparing effects.

• Injectable capsaicin is used for the control of post op pain, such as after TKR,THR, hernia repair , shoulder arthroscopy.
• Absolute contraind- Hypersensitivity.• Relative contraindications- age < 2 years, pts with elevated liver enzymes, pts on ACE inhibitors, and pts with signs of septic arthritis and joint
infections.

• Capsaicin in low concentrations (<1%) with repeat administration has been used for a long time in an attempt to treat neuropathic pain.
• High concentration (8%) capsaicin patch for single administration
• In postherpetic neuralgia and HIV-related neuropathy, low incidence of adverse effects.

• Dexmedetomidine :• highly selective central alpha2 agonist. • sedative, pro-anesthetic, and pro-analgesic effects
at 0.5-2 micrograms/kg iv.• Blunt the central sympathetic response .• Also minimizes opioid-induced muscle rigidity,
lessens postop shivering, causes minimal respiratory depression, and has hemodynamic stabilizing effects.
• When used as an adjunct, can reduce postoperative morphine consumption.
• Addition of dexmedetomidine to IV PCA morphine resulted in superior analgesia, significant morphine sparing, and less morphine-induced nausea, and devoid of additional sedation and untoward hemodynamic changes.

Botulinum toxin• ACTION-• Inhibition of ach release,• Inhibition of the release of glutamate, substanceP,
and CGRP• Reduced afferent input to the CNS through effects
of the toxins on muscle spindles• INDICATIONS-• Strabismus,• Blepharospasm, • Hemifacial spasm, • Cervical dystonia ,• Muskuloskeletal Pain

• SIDE EFFECTS- • Pain, muscle weakness, • Flulike syndrome• Autonomic side effects appear to be
commonly seen with type B toxin• CONTRAINDICATIONS –• Pregnancy (category C),• Concurrent use of aminoglycoside ,
Myasthenia gravis, Eaton–Lambert .• Known sensitivity to the toxins

NON PHARMACOLOGICAL• Because medical treatments have limited effects on patients
with chronic pain, patients are twice as likely to commit suicide and lifetime prevalence of suicide attempts is about 10%.
• Medication will likely affect not only the neural structures responsible for sustaining pain, but also other brain regions that can give rise to side-effects or render the interventions less effective.

NON INTERVENTIONAL• PHYSIOTHERAPY• ELECTROTHERAPY- COLD THERAPY, HEAT THERAPY, ULTRASOUND, TENS• MANIPULATIVE THERAPY- MASSAGE, SPINAL TRACTION, PASSIVE STRETCHING, ORTHOSES (CERVICAL COLLARS,
LUMBAR SUPPORTS) • HYDROTHERAPY

NON INTERVENTIONAL• MEDITATION,• HYPNOSIS, • BIOFEEDBACK, BEHAVIOURAL
THERAPY • POSTURE• PHYSICAL EXERCISES• DIET THERAPY

NON-INVASIVE BRAIN STIMULATION TECHNIQUES
• Brain stimulation is a technique that can guide brain plasticity and thus be suitable to treat chronic pain-a disorder that is associated with substantial reorganisation of CNS activity.
• Therefore, therapies that directly modulate brain activity in specific neural networks might be particularly suited to relieve chronic pain.
• Repetitive transcranial magnetic stimulation (TMS) and Transcranial direct current stimulation (tDCS), are particularly appealing as they can change
brain activity in a non-invasive, painless and safe way.

TMS-TRANS CRANIAL MAGNETIC STIMULATION
• Developed in 1985.• It is based on a time-varying magnetic field that
generates an electric current inside the skull, where it can be focused and restricted to small brain areas by appropriate stimulation coil geometry and size.
• This current, if applied repetitively, repetitive TMS (rTMS), induces a cortical modulation that lasts beyond the time of stimulation.

tDCS –TRANS DIRECT CRANIAL STIMULATION
• Induces similar modulatory effects.• tDCS is based on the application of a weak direct
current to the scalp that flows between two relatively large electrodes—anode and cathode electrodes.
• Some studies have shown that the efficacy of tDCS depends critically on parameters such as electrode position and current strength.
• Application of tDCS for 13 min to the motor cortex can modulate cortical excitability for several hours.
• This technique can also be used to obtain clinical gains in neuropsychiatric disorders such as stroke, epilepsy, and tinnitus.

1.high-frequency rTMS of the primary motor cortex . 2.low and high-frequency rTMS of dorsolateral prefrontal cortex

1. low-frequency rTMS of the secondary somatosensory cortex 2. anodal tDCS of the primary motor cortex

• At the beginning of the 1990s, a new and less invasive strategy of brain stimulation was developed, known as epidural motor cortex stimulation,
• It showed substantial pain improvement and brought new life to the concept of brain stimulation for the treatment of chronic pain.
• Epidural cortical stimulation not only decreased the neurosurgical risks of brain stimulation for chronic pain, but also invited the exploration of non-invasive brain stimulation techniques, tDCS and rTMS.

RESULTS
• FOR rTMS-• Right and Left secondary
somatosensory cortex stimulation with 1 Hz, 20 Hz.
• The results showed that 1 Hz (of left and right secondary somatosensory cortex) and right somatosensory cortex (with 1 and 20 Hz) stimulation led to a significant pain reduction.
RESULTS• FOR tDCS• Patients with chronic pain due to spinal cord
injury were randomised to receive active motor tDCS (2 mA for 20 min for five consecutive days).
• There was a significant pain improvement after active anodal stimulation of the motor cortex.
• tDCS has some advantages over rTMS-• it has longer-lasting modulatory effects of cortical
function.• is less expensive.• easy to administer.

INTERVENTIONAL1. SPINAL & EPIDURAL OPIOID & STEROID2. PNS,SCS & DBS3. NEUROLYSIS-Chemical neurolysis, Radiofrequency thermocoagulation Cryoanalgesia4.VERTEBROPLASTY & KYPHOPLASTY5.DRY NEEDLING,INFILTRATION,PROLOTHERAPY,TPI6.ACUPUNCTURE7.RADIOTHERAPY8.OZONETHERAPY9. CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY
(LYSIS OF ADHESIONS)10.PERCUTANEOUS MANAGEMENT OF
VISCERAL PAIN11.NEUROSURGICAL PROCEDURES
EQUIPMENTS USED ARE
• FLUOROSCOPIC GUIDED• ULTRASOUND GUIDED• CT GUIDED• MRI GUIDED
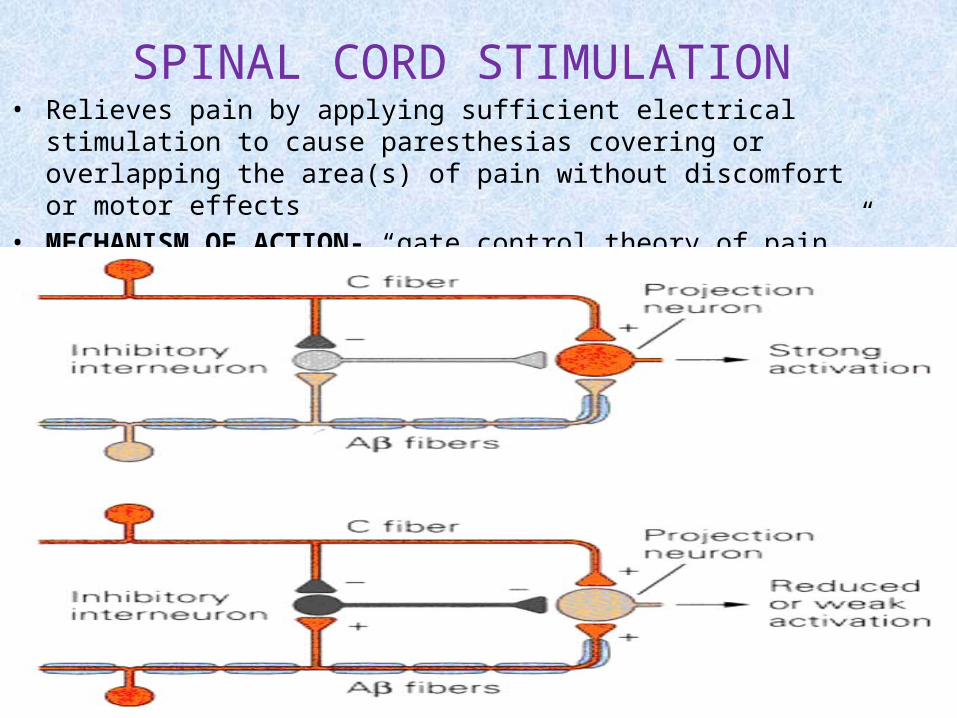
SPINAL CORD STIMULATION• Relieves pain by applying sufficient electrical stimulation to
cause paresthesias covering or overlapping the area(s) of pain without discomfort or motor effects
• MECHANISM OF ACTION- “gate control theory of pain,”

SPINAL CORD STIMULATION
• SCS is minimally invasive and reversible. • A typical SCS system has four components. 1. A neurostimulator that generates an electrical
pulse (or receives radio frequency pulses) – this is surgically implanted under the skin in the abdomen or in the buttock area.
2. An electrode(s) implanted near the spinal cord either surgically or percutaneously (the latter via puncture, rather than through an open surgical incision, of the skin).
3. A lead that connects the electrode(s) to the neurostimulator.
4. A remote controller that is used to turn the neurostimulator on or off and to adjust the level of stimulation.

SPINAL CORD STIMULATION

INDICATIONS-• Failed back surgery syndrome,• Ischemic pain of peripheral vascular disease • Postcordotomy dysesthesias, • Reflex sympathetic dystrophy • Phantom limb and stump pain.
CONTRAINDICATIONS-• Coagulopathy, Sepsis,• Serious drug behavior problems,• Inability to cooperate or to control the device• Demand cardiac pacemaker (without ECG monitoring
or changing the pacemaker mode to a fixed rate).

COMPLICATIONS-• Electrode fatigue fracture, Electrode
migration/malposition• Exposure to electromagnetic fields (eg,
diathermy,security systems)• Spinal cord or nerve injury, • CSF leak• Infection• Bleeding

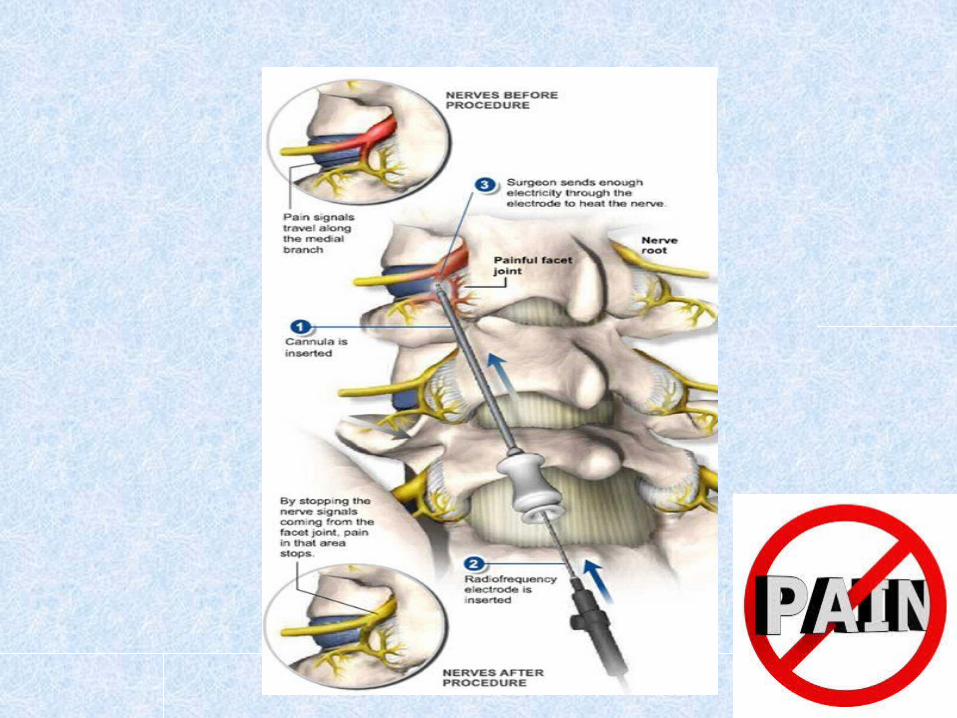
RADIOFREQUENCY ABLATION• ACTION-• Destruction of the nerves that signal pain • The effect of RF on tissue depends on the
temperature generated:• >45°C, irreversible tissue injury occurs;• Between 42 and 45°C, temporary neural blockade
occurs.
• INDICATIONS-• head and neck pain ,• spine pain ,• neuropathic pain

• COMPLICATIONS-• Neurologic deficits from the intended target or
nearby neural structures,• Deafferentation pain, • Neuritis,• Burn injury at breaks in the needle insulation,• Hematoma• Infection

CRYONEUROLYSIS• Temporarily destroys a nerve through the
application of extreme cold.• The extreme cold degenerates the nerve axons
without damaging surrounding connective tissue• Larger myelinated fibers cease conduction at
10°C,• At 0°C, all nerve fibers entrapped in the ice ball
stop conduction.• Can be cooled upto -70 degrees• Pain relief upto 3 months.

CRYONEUROLYSIS

CRYONEUROLYSIS
• INDICATIONS-• POSTTHORACOTOMY PAIN,
POSTHERNIORRHAPHY PAIN• INTERCOSTAL NEURALGIA, PAINFUL NEUROMA• CERVICAL AND LUMBAR FACET AND
INTERSPINOUS LIGAMENT PAIN• COCCYDYNIA, PERINEAL PAIN• ILIOINGUINAL, ILIOHYPOGASTRIC, AND
GENITOFEMORAL NEUROPATHIES• SUPERIOR GLUTEAL NERVE NEURALGIA• CRANIAL NEURALGIA, SUPRAORBITAL NERVE
NEURALGIA• INFRAORBITAL NEUROPATHY, MANDIBULAR
NEUROPATHY

VERTEBROPLASTY
L2
• Bone cement is injected percutaneously into a fractured vertebra with the goal of relieving back pain caused by vertebral compression fractures
• Recent research has demonstrated that percutaneous vertebroplasty can relieve pain from vertebral compression fractures for up to nearly three years following the procedure.

CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS)
Indications-• Failed back surgical• Disc disruption• Mets of spine compression fracture• Multilevel degenerative arthritis• Epidural scarring following infection or meningitis • Pain unresponsive to spinal cord stimulation• Pain unresponsive to spinal opioids
Contraindications-• Sepsis• Coagulopathy• Local infection at the site of the procedure• Patient refusal
CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS)
• Neuroplasty is done to repair nerve damage.• It is a procedure that is used to break up scar
tissue that has formed around the nerve in the epidural space of the spine, so medications such as the steroid can reach the affected nerve/nerves so pain and other symptoms will lessen or go away.
• The actual procedure is similar to a caudal steroid injection in that a thin catheter is inserted from very low in the spine and it runs up to the point where there is scarring.

CAUDAL EPIDURAL DECOMPRESSIVE NEUROPLASTY (LYSIS OF ADHESIONS)
• Immediate complications
• Bleeding in the epidural space
• Bending of the tip of the needle
• Penetration of the Dura• Subdural insertion of
the catheter • Shearing of the catheter• Hypotension
• Late complications
• Penetration of the Dura• Numbness in the
dermatomal distribution• Temporal anesthesia• Permanent paresthesias• Bowel and bladder
dysfunction• Sexual dysfunction• Headache• Infection at the site of
penetration• Epidural abscess• Arachnoiditis
COELIAC PLEXUS BLOCK• INDICATIONS-• To control pain of the epigastric viscera, especially due to
primary or metastatic upper abdominal cancers• chronic pancreatitis• for intraabdominal surgery.
• DRUGS UTILIZED-• For a sensory block-• 0.25% Bupivacaine with or without 1:200,000 epi.• For a neurolytic block-• 50% - 100% Alcohol diluted with sterile water or local
anesthetic.• Total volume - no more than 15-20 ml for each injection.• Overfilling the space may cause the alcohol to leak
and spread posteriorly, resulting in alcohol neuritis.

COELIAC PLEXUS BLOCK
• At the level of the T12 and L1 vertebrae• Ganglia lie on each side of L1 (aorta lying
posteriorly, pancreas anteriorly and inferior vena cava laterally).
• Receive sympathetic fibers from the greater, lesser, and least splanchnic nerves.
• Receives parasympathetic fibers from the vagus nerve.
• Retrocrural and Transcrural blocks-MOST COMMON
• Other techniques include- Transaortic approach Anterior approach Paramedian approach at T-12 Transdiscal approach

COELIAC PLEXUS BLOCK
PROCEDURE-• Prone position• Lines are drawn connecting the spine of T12 with
points 7-8 cm lateral at the edges of the 12th ribs• Performed with a 15-cm, 20-22 G needle• Advance the needle at a 45 angle from the
horizontal plane toward the body of T12 or L1 .• Bony contact should be made at an average
depth of 7-9 cm.• Withdraw the needle and reinsert it at an
increased angle of 5-10 degrees to allow the tip to slide off the vertebral body anterolaterally.
COELIAC PLEXUS BLOCK
• Complications• Related to needle insertion/technique Pneumothorax Needle placed too far cephalad Puncture of surrounding structures, mainly kidneys• Due to puncture of the aorta or vena cava- bleeding• Related to sympathetic block/neurolytic agent• Hypotension -MOST COMMON• Systemic toxicity• Transient mild diarrhea (lasting up to 2 weeks)• Paraplegia (rare but most serious) - related to use
of alcohol damaging the artery of Adamkiewicz

• HYPOGASTRIC PLEXUS BLOCK• Distal ureters, gonads, sigmoidcolon,
vagina, rectum, bladder, perineum, vulva, prostate, uterus, and the major pelvic blood vessels

OTHERS
• DRYNEEDLING,• INFILTRATION,• PROLOTHERAPY,• ACUPUNCTURE• RADIOTHERAPY• OZONETHERAPY
Neurosurgical Pain Therapies
Ablative•Neurectomy •Sympathectomy •Ganglionectomy •Rhizotomy •Spinal DREZ lesioning •Cordotomy •Myelotomy •Nucleus caudalis DREZ lesioning •Trigeminal tractotomy •Mesencephalotomy •Thalamotomy •Cingulotomy •Hypophysectomy
Augmentative•Peripheral nerve stimulation •Spinal cord stimulation •Thalamus (PVG-PAG) stimulation •Motor cortex/deep brain stimulation •Intrathecal/epidural drug infusion •Intraventricular drug infusion

Intrathecal Drug Delivery Systems
AKA: Pain pump
Mechanism of Action:
• Drug delivered directly to the intrathecal space
Drugs:• Morphine• Baclofen• Bupivacaine• Clonidine• Ketamine
http://www.medtronic.com/IN/images/intro_intrathecal1.gif
Intrathecal Drug Delivery Systems
PROS• Short reversible
trial• Delivery of drug
directly to the site of action
• 1mg IT Morphine = 300 gm oral Morphine
• Cancer Pain: pain, toxicity, survival 6mo
CONS• Short reversible
trial• opioid benefit
with time (40% failure with time)
• Contraindications to placement
• Complications (granuloma)

SUMMARY• Pharmacological management of pain will
continue to have to rely on a multimodal approach with old medications finding new uses and indications.
• Many factors must be considered before deciding on the type of pain therapy to be provided to the surgical patient

P atients
A re
I n
N eed