Recent Advances in Migraine therapy
58
RECENT ADVANCES IN MIGRAINE THERAPY 1 Dr. Abialbon Paul M.D. Pharmacology, Junior Resident
-
Upload
abialbon-paul -
Category
Documents
-
view
153 -
download
2
Transcript of Recent Advances in Migraine therapy

RECENT ADVANCES IN MIGRAINE THERAPY
1
Dr. Abialbon Paul
M.D. Pharmacology, Junior Resident

Migraine, just a headache
2

“ Each day that I have a migraine,
it is a struggle to work, to move, sometimes even to breath.
That day, it began with stiffness in my neck and
an ache around my temples and brow bone.
I found it difficult to focus on the screen or on the words that
I was hearing. I began to see spots in front of my eyes.
I staggered across the hall to my room, not knowing whether
I would make it to my bed. In my room, I shut out all the light,
closed my laptop and hid myself under the covers. Even the
whirring of my laptop caused an annoying resonance in my
ears. I covered my head with my pillow and soon I found the
relief of sleep. I slept for the next fifteen hours, waking up
refreshed and new the next morning.”
3A day in the life of a migraineur

Migraine, just another headache?
• Yawning• Low mood• Irritability• Fatigue• Anorexia• Nausea & Vomiting• Throbbing headache• Photophobia & phonophobia• Hemiplegia• Blindness• Migranous infarction• Death
4

Phases of migraine
• Prodrome
• Aura
• Headache
• Postdrome
• Resolution 5

Outline
• Introduction• Current understanding of migraine pathogenesis• Newer neuronal targets• Newer approaches to old drugs• Need for prophylaxis• Newer drugs for prophylaxis• Migraine genetics• Conclusion
6

Introduction• Migraine is a complex heterogeneous neurovascular
disease
• Affects 15% general population, 3 times more common in females
• Varied clinical manifestations
• Lack of awareness among physicians as well as patients
• Changing paradigms in understanding of migraine pathophysiology
7

Migraine with aura
8
Diagnostic criteria:• A. At least 2 attacks fulfilling criteria B–D• B. Aura consisting of at least one of the
following, but no motor weakness:• 1. fully reversible visual symptoms including positive
features (eg, flickering lights, spots or lines) and/or negative features (ie, loss of vision)
• 2. fully reversible sensory symptoms including positive features (ie, pins and needles) and/or negative features (ie, numbness)
• 3. fully reversible dysphasic speech disturbance

• C. At least two of the following:• 1. homonymous visual symptoms and/or unilateral
sensory symptoms• 2. at least one aura symptom develops gradually
over ≥5 minutes and/or different aura symptoms occur in succession over ≥5 minutes
• 3. each symptom lasts ≥5 and <60 minutes
• D. Headache fulfilling criteria B–D for Migraine without aura begins during the aura or follows aura within 60 minutes
• E. Not attributed to another disorder. 9

Migraine without aura
10
• Diagnostic criteria:• A. At least 5 attacks fulfilling criteria B–D• B. Headache attacks lasting 4–72 hours • C. Headache has at least two of the following
characteristics:• 1. unilateral location• 2. pulsating quality• 3. moderate or severe pain intensity• 4. aggravation by or causing avoidance of routine physical
activity (eg, walking or climbing stairs)
• D. During headache at least one of the following:• 1. nausea and/or vomiting• 2. photophobia and phonophobia
• E. Not attributed to another disorder

Migraine pathogenesis
• Cortical Spreading Depression (CSD)• Trigeminovascular System (TGVS)• Peripheral & Central sensory dysmodulation
11

12
Figure1. Pathogenesis of migraine
Cortical Spreading Depression
TGVS
Central sensory areas

Current therapies
Specific migraine treatment• Triptans
Sumatriptan
Rizatriptan
Naratriptan
Zolmitriptan
Eletriptan
Almotriptan
Frovatriptan• Ergot and its derivatives
Ergotamine + caffeine
Dihydroergotamine13

Current therapies
• . Nonspecific pharmacological treatment• Anti-emetics (metoclopramide)• NSAIDs and nonnarcotic analgesics• Narcotics – Opiate analgesics
• Miscellaneous medications:• Steroids, isometheptene, intranasal lidocaine
Valproic acid IV• Non-pharmacological treatment
14

Limitation of current therapies
• Pharmacokinetics – Variable oral bioavailability• Nausea & vomiting of migraine• Less effective after initiation of headache phase of
the attack• 50-70% efficacy in terminating acute attacks• Side effect profile, concern on ischemic adverse
events• Contraindication in vascular diseases• Medication overuse headache and chronicization of
migraine 15

Newer neuronal targets
16

CGRP receptor antagonists
• Calcitonin Gene Related Peptide• Alternative splicing of calcitonin gene in ch11• αCGRP & βCGRP• Potent vasodilator & neurotransmitter in
nociceptive pathways
17

Why CGRP receptor antagonists?
18
• Location of receptors• Levels of CGRP were found elevated in the
external jugular vein in migraineurs during an acute attack
• CGRP levels normalised after treatment of the acute migraine attack.
• Infusion of human CGRP precipitated migraine attacks in susceptible individuals.

• Olcegepant - first CGPR receptor antagonist to be studied.
• Found effective in phase II trails.• Intravenous administration • Telcagepant, a potent orally active CGRP
receptor antagonist • Phase III• Similar efficacy to sumatriptan with better
tolerability19

Telcagepant
• Phase II trial studying Telcagepant in migraine prophylaxis resulted in elevation of liver enzymes after 300 mg twice a day for 3 months
• Off-target effect or CGRP antagonism??
20

21
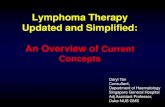
Figure 2. Efficacy and adverse effect profile of triptans and telcagepant in different RCTs (8)
Dose strengths are plotted along X-axis and %efficacy/ADR events in Y-axis

Newer drugs in the pipeline
22
• BMS-927711 – Phase I
• BI 44370 TA - Phase II
• “gepants” will be of major use in treating migraine patients with contraindications for triptans & those not tolerating triptans

5HT1F receptor agonists
• 5HT1F receptors activation inhibits the trigeminal nucleus fos activation which is a marker for neuronal activation and firing
• Triptans also have agonist action on the 5HT1F
23

• LY-334370, a potent 5HT1F agonist was found to be effective but with adverse actions on the central nervous system unrelated to its anti-migraine action.
• COL-144, another 5HT1F agonist has been found to be effective in phase II trial and is under further investigations.
24

Glutamate receptor antagonists
• Glutamate is one of the important excitatory neurotransmitters in the central nervous system involved in sensory and nociceptive pathways
• Ionotropic glutamate receptors (comprises of NMDA, AMPA & Kainate receptors)
• G protein coupled metabotropic receptors
25

• Central nociceptive dysmodulation may involve aberrant glutaminergic transmission
• Glutamate neurons in the trigeminal ganglia mostly
express 5-HT1B/1D/1F receptors, which have been proposed to modulate glutamate release.
• Glutamate is also implicated in trigeminovascular activation and cortical spreading depression
26

• Currently three drugs are in phase II clinical trials:• BGG492 - AMPA receptor antagonist • Tezampanel (LY-293558) - AMPA and kainate
receptor antagonist• LY466195a - GLUK5 and kainate receptor
antagonist
27

Transient receptor potential vanilloid (TRPV1) receptor antagonists
• TRPV1 receptors are cation channels activated by capsaicin and are present in nociceptive neurons of the central and peripheral nervous system.
• These receptors are present in the human trigeminal neurons with a sub group being co-localised along with the CGRP receptors.
• Sumatriptan is also known to block these receptors
• SB-705498 is a TRPV1 receptor antagonist and is in Phase II of clinical testing.
28

Nitric oxide synthesis inhibition
• Glyceryl trinitrate infusion causes an acute attack of migraine. The vasodilation of cranial vessels were implicated in the trigger of migraine attacks
• Magnetic Angiography studies revealed that vasodilation caused by glyceryl trinitrate resolved before the attack of headache
• NO has been proposed to activate trigeminovascular fibres and thus release CGRP
29

• NXN-188, a nNOS inhibitor with additional 5HT1B/1D
agonist activity is currently in phase II trials.
• GW274150 is an inducible NOS inhibitor in phase II of clinical trials.
30

Prostanoid receptor antagonists
• Prostaglandin E2 is one of the important mediators of inflammation and pain.
• EP1 and EP3 mediate smooth muscle contraction
• EP2 and EP4 induce smooth muscle relaxation.
• EP4 are present on the cerebral vasculature and are thought to mediate anti-nociceptive action
• Currently BGC20-1531, a prostaglandin EP4 competitive antagonist is in clinical trials 31

32
Table1: Drugs for acute management in clinical trials

Newer approach to older drugs
• Orally inhaled dihydroergotamine • Phase III clinical trial (FREEDOM-301) has been
completed and it is currently undergoing FDA review• rapidly and completely absorbed and reaches
Cmax in 12 minutes
• provide a quicker relief
33

• Novel iontophoretic sumatriptan transdermal patch
34
Figure 3. Mechanism of drug delivery of a sumatriptan transdermal system

FDA approved formulations
• A needle-free injection of sumatriptan - SUMAVEL®
• An epipen-type needle injection of sumatriptan - ALSUMA
• Rapid-dissolution oral tablets of sumatriptan - IMITREX® RT,
• Soluble oral diclofenac under trade name - CAMBIA™
• Intranasal ketorolac SPRIX®
35

Need for prophylactic Rx
• Limitation of dosage allowance per week to prevent toxicity
• The efficacy of these drugs decreases when administered after the onset of the headache
• Physiological changes, non-specific disabling symptoms may occur during the migraine free periods in chronic migraine.
• Long term frequent use of acute abortive treatment may transform the migraine to Medication overuse headache (MOH)
36

Criteria for prophylaxis
37

Limitations of the current drugs
• Side effects • Limited efficacy• The mechanism of action of most of the prophylactic
drugs is unknown or poorly understood. These drugs are used based on their effectiveness as shown by the various clinical trials
38

Table 3. Drugs for migraine prophylaxis. Current levels of evidence
Grade A evidence: Multiple randomized clinical trials with consistent findings to support efficacydivalproex, topiramate, propranolol, timolol, pizotifen (not approved in the United States)amitriptyline
Grade B evidence: Few randomized trials with some evidence supported by recommendation, suboptimal scientific supportGabapentin, atenolol, metoprolol, nadolol, nimodipine, verapamil (cyclandelate and flunarizine not approved in the United States), botulinum toxin type A, aspirin, fenoprofen, flurbiprofen, ketoprofen, mefenamic acid, naproxen, fluoxetine, estradiol, feverfew, magnesium, vitamin B2
Grade C evidence: US Headache Consortium consensus (published in 2000) in the absence of relevant controlled clinical trialsDiltiazem, bupropion, mirtazapine, phenelzine, trazodone, venlafaxine, ibuprofen, cyproheptadine, fluvoxamine, paroxetine, sertraline, doxepin, imipramine, nortriptyline, protriptyline 39

40

Topiramate
• Topiramate acts by• Inhibition of voltage-gated sodium channels• Inhibition of high voltage-activity (L-type) calcium
channels• Facilitates neuronal potassium conductance• Augments the inhibitory chloride ion flux caused
by GABA
• Recent evidence favours use of topiramate as the first line choice for migraine prophylaxis
41

• A randomised, double-blind, multicentre trial comparing two doses of topiramate (100mg & 200mg) with placebo and propranolol as active control concluded that 100mg of topiramate was effective than the placebo and had similar efficacy of propranolol.
A recent RCT of 38 patients which compared
topiramate monotherapy vs. topiramate + nortriptyline
37% 78.3%
had at least 50% reduction in headache
42

Side effects
• Frequent• paraesthesia• fatigue• loss of weight• mild nausea
• Rare side effects • CNS slowing or word finding difficulties• renal stones• secondary angle closure glaucoma
43

Gap junctions
Figure 4: structure of gap junctions44

Tonabersat
• Gap junctions connect the protoplasm of two adjacent cells aiding in cellular transfer and communication.
• A gap junction between two cells is formed by the fusion of two hemichannels from adjacent cells.
• Play a role in propagation of calcium waves. • Calcium waves are intracellular increases in the
calcium concentration which spreads to the adjacent cells propagating the hyperactivity of the neurons
• Tonabersat has completed phase II clinical trials 45

OnabotulinumtoxinA
• OnabotulinumtoxinA functions to inhibit the release of excitatory mediators by preventing the fusion of intracellular vesicles
• Injection of onabotulinumtoxinA at the designated therapeutic sites in the head, neck, and shoulders would result in internalization of the neurotoxin into nearby motor or sensory neurons
46

• OnabotuliunumtoxinA in motor neurons inhibits the release of acetylcholine, resulting in muscle paralysis.
• Internalization of the neurotoxin in sensory neurons that innervate the skin and muscles could potentially inhibit the release of proinflammatory mediators at several sites within the sensory neuron.
• It also supresses the second order sensory neurons and the glial cells which are involved in sensitization of central nociception
• Approved for chronic migraine prophylaxis47

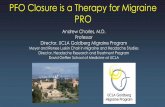
48Figure 5: Mutations implicated in migraine pathogenesis

Another gene KCNK18 which encodes for TRESK is implicated in migraine with aura.
TRESK is a neuronal potassium channel
Targeting TRESK is a viable pharmacological target for migraine pathogenesis
49

Conclusion
• Migraine is a complex multigenic clinically heterogenous neuronal disorder
• The cascade of events is migraine pathogenesis is not well understood.
• The newer neuronal targets promise better acute abortive treatment options.
• It could be well hypothesized that different targets may have varying levels of importance in different patients. There are no studies to show treatment response to newer drugs on older drug non-responders.
50

• Further identifying genetic mutations can identify subgroup of patients who would respond better to specific therapeutic targets.
51

52

Future of migraine…
“I began to experience some stiffness in my neck and an ache around my temples. I knew it was an attack of
migraine. I took my inhaler from my bag and took a puff. In 10 minutes I was relieved of the pain. Then I went to the
cinema with my friends and enjoyed the whole day”
53

References1. Katsarava Z, Buse DC, Manack AN, Lipton RB. Defining the differences between episodic migraine and chronic migraine. Curr Pain Headache Rep. 2012 Feb;16(1):86–92.
2. Kalra AA, Elliott D. Acute migraine: Current treatment and emerging therapies. Ther Clin Risk Manag. 2007 Jun;3(3):449–59.
3. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Headache Classification Committee of the International Headache Society. Cephalalgia. 1988;8 Suppl 7:1–96.
4. Mehrotra S, Gupta S, Chan KY, Villalón CM, Centurión D, Saxena PR, et al. Current and prospective pharmacological targets in relation to antimigraine action. Naunyn Schmiedebergs Arch Pharmacol. 2008 Oct;378(4):371–94.
5. Gupta VK. Cortical-spreading depression: at the razor’s edge of scientific logic. J Headache Pain. 2011 Feb;12(1):45–6.
6. Weir GA, Cader MZ. New directions in migraine. BMC Med. 2011;9:116.
7. Ferrari A, Tiraferri I, Neri L, Sternieri E. Why pharmacokinetic differences among oral triptans have little clinical importance: a comment. J Headache Pain. 2011 Feb;12(1):5–12. not? J Headache Pain. 2011 Dec;12(6):593–601.
54

8. Tfelt-Hansen P. Optimal balance of efficacy and tolerability of oral triptans and telcagepant: a review and a clinical comment. J Headache Pain. 2011 Jun;12(3):275–80.
9. Gilmore B, Michael M. Treatment of acute migraine headache. Am Fam Physician. 2011 Feb 1;83(3):271–80.
10. Negro A, Martelletti P. Chronic migraine plus medication overuse headache: two entities or not? J Headache Pain. 2011 Dec;12(6):593–601.
11. Durham PL, Vause CV. Calcitonin gene-related peptide (CGRP) receptor antagonists in the treatment of migraine. CNS Drugs. 2010 Jul;24(7):539–48.
12. Negro A, Lionetto L, Simmaco M, Martelletti P. CGRP receptor antagonists: an expanding drug class for acute migraine? Expert Opin Investig Drugs. 2012 Jun;21(6):807–18.
13. Monteith TS, Goadsby PJ. Acute migraine therapy: new drugs and new approaches. Curr Treat Options Neurol. 2011 Feb;13(1):1–14.
14. Evans MS, Cheng X, Jeffry JA, Disney KE, Premkumar LS. Sumatriptan Inhibits TRPV1 Channels in Trigeminal Neurons. Headache. 2012 May;52(5):773–84.
15. Olivia J. Phung P. Orally inhaled dihydroergotamine: A novel ergot delivery method for the treatment of migraine [Internet]. Formulary. 2012 [cited 2012 Jun 20]. Available from: http://formularyjournal.modernmedicine.com/formulary/Modern+Medicine+Now/Orally-inhaled-dihydroergotamine-A-novel-ergot-del/ArticleStandard/Article/detail/758883
55

16. Tepper SJ, Stillman MJ. What is the best drug-delivery approach for the acute treatment of migraine? Expert Rev Neurother. 2012 Mar;12(3):253–5.
17. Mannix LK. Clinical advances in the preventive treatment of migraine. Acta Neurol Taiwan. 2004 Dec;13(4):158–69.
18. Modi S, Lowder DM. Medications for migraine prophylaxis. Am Fam Physician. 2006 Jan 1;73(1):72–8.
19. Loj J, Solomon GD. Migraine prophylaxis: who, why, and how. Cleve Clin J Med. 2006 Sep;73(9):793–794, 797, 800–801 passim.
20. Krymchantowski AV, da Cunha Jevoux C, Bigal ME. Topiramate plus nortriptyline in the preventive treatment of migraine: a controlled study for nonresponders. J Headache Pain. 2012 Jan;13(1):53–9.
21. Durham PL, Garrett FG. Neurological mechanisms of migraine: potential of the gap-junction modulator tonabersat in prevention of migraine. Cephalalgia. 2009 Nov;29 Suppl 2:1–6.
22. Durham PL, Cady R. Insights into the mechanism of onabotulinumtoxinA in chronic migraine. Headache. 2011 Dec;51(10):1573–7.
23. Bigal ME, Rapoport AM, Sheftell FD, Tepper SJ. New migraine preventive options: an update with pathophysiological considerations. Rev Hosp Clin Fac Med Sao Paulo. 2002 Dec;57(6):293–8.
24. Barbanti P, Aurilia C, Egeo G, Fofi L. Future trends in drugs for migraine prophylaxis. Neurol Sci. 2012 May;33 Suppl 1:137–40.
25. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalso J. Harrison's principles of internal medicine. 18th Edition The McGraw-Hill Companies, Inc. 2012.
56

Queries
57

58
Thank You