Readmissions Experience Hunterdon Medical Center CMO Roundtable October 2014.
30
Readmissions Experience Hunterdon Medical Center CMO Roundtable October 2014
-
Upload
colin-wilson -
Category
Documents
-
view
213 -
download
0
Transcript of Readmissions Experience Hunterdon Medical Center CMO Roundtable October 2014.
Readmissions Experience Hunterdon Medical Center
CMO Roundtable
October 2014
Background
• Hunterdon Medical Center is a 176 bed hospital in west-central New Jersey
• It is part of Hunterdon Healthcare, which also includes Hunterdon Regional Community Health (home care, visiting nurse, and hospice) and Mid-Jersey (for profit arm)
• Hunterdon Healthcare partnered with the Hunterdon Physician Practice Association, an IPA, to form Hunterdon HealthCare Partners
Background
• Readmissions Committee work began in 2011 in anticipation of CMS penalties to begin in fiscal 2012
• Focused on CHF first as we had the highest rate out of the three
• First looked at patient education
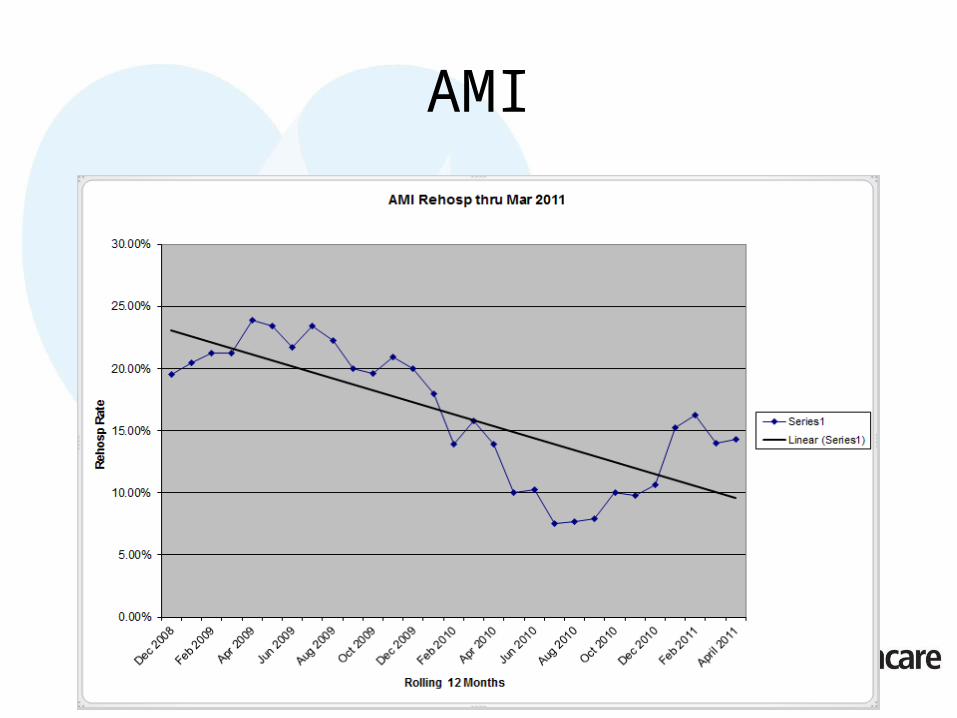
AMI
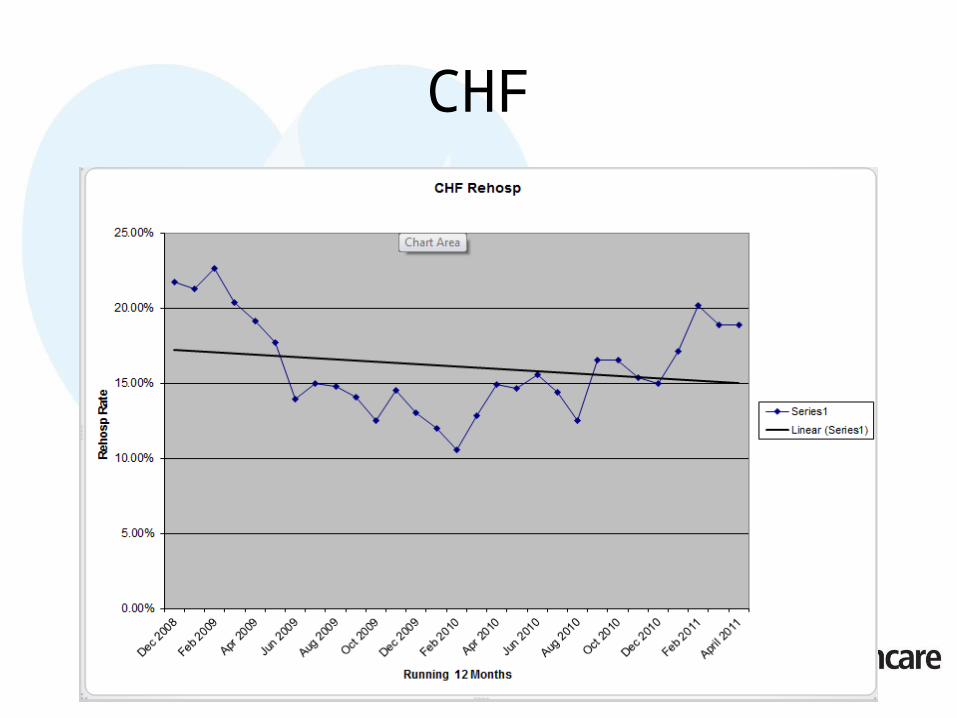
CHF
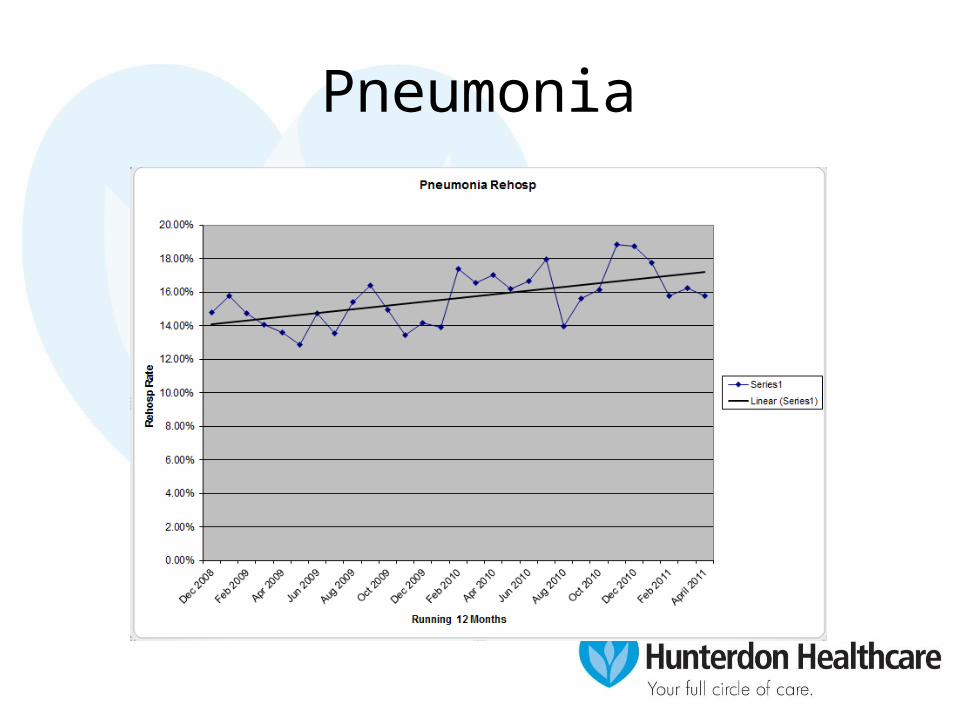
Pneumonia
Patient Education
• Created forms for nursing to document education during the inpatient stay
• Used a “stop light” system for patient self-assessment after discharge
• Tried to institute a discharge “test” for teach-back
Why Are Patients Readmitted
• We had our patient care managers complete a short questionnaire with readmitted patients
• Did the questionnaire with 50 patients
• Did not see any real trends
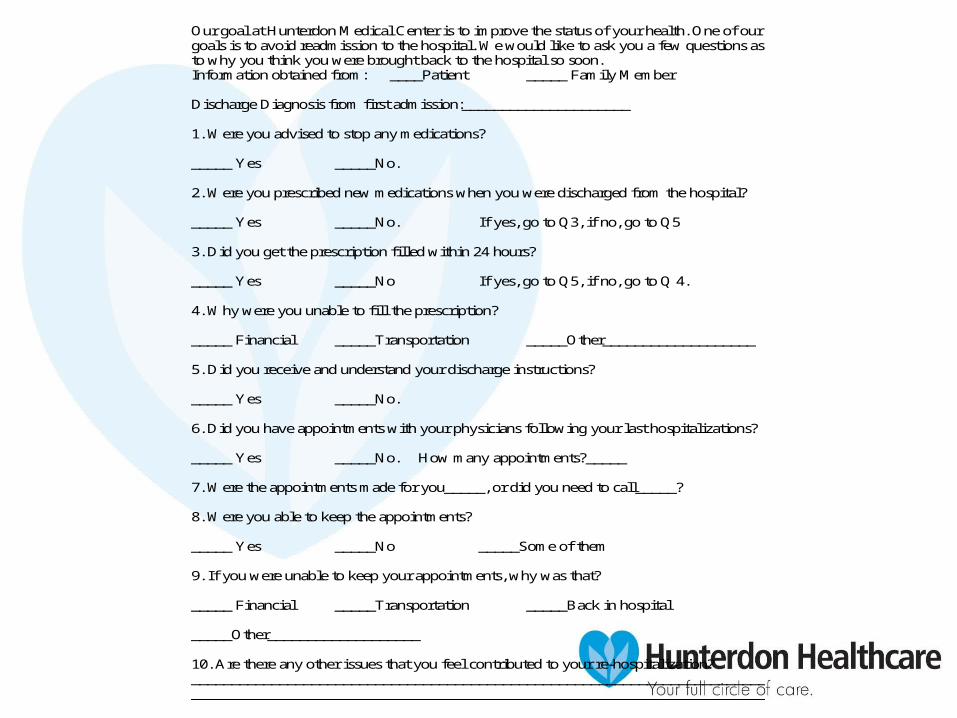
Our goal at Hunterdon Medical Center is to improve the status of your health. One of our goals is to avoid readmission to the hospital. We would like to ask you a few questions as to why you think you were brought back to the hospital so soon. Information obtained from: ____Patient _____ Family Member Discharge Diagnosis from first admission:_____________________ 1. Were you advised to stop any medications? _____ Yes _____No. 2. Were you prescribed new medications when you were discharged from the hospital? _____ Yes _____No. If yes, go to Q3, if no, go to Q5 3. Did you get the prescription filled within 24 hours? _____ Yes _____No If yes, go to Q5, if no, go to Q 4. 4. Why were you unable to fill the prescription? _____ Financial _____Transportation _____Other___________________ 5. Did you receive and understand your discharge instructions? _____ Yes _____No. 6. Did you have appointments with your physicians following your last hospitalizations? _____ Yes _____No. How many appointments?_____ 7. Were the appointments made for you_____, or did you need to call_____? 8. Were you able to keep the appointments? _____ Yes _____No _____Some of them 9. If you were unable to keep your appointments, why was that? _____ Financial _____Transportation _____Back in hospital _____Other___________________ 10. Are there any other issues that you feel contributed to your re-hospitalization? ________________________________________________________________________________________________________________________________________________
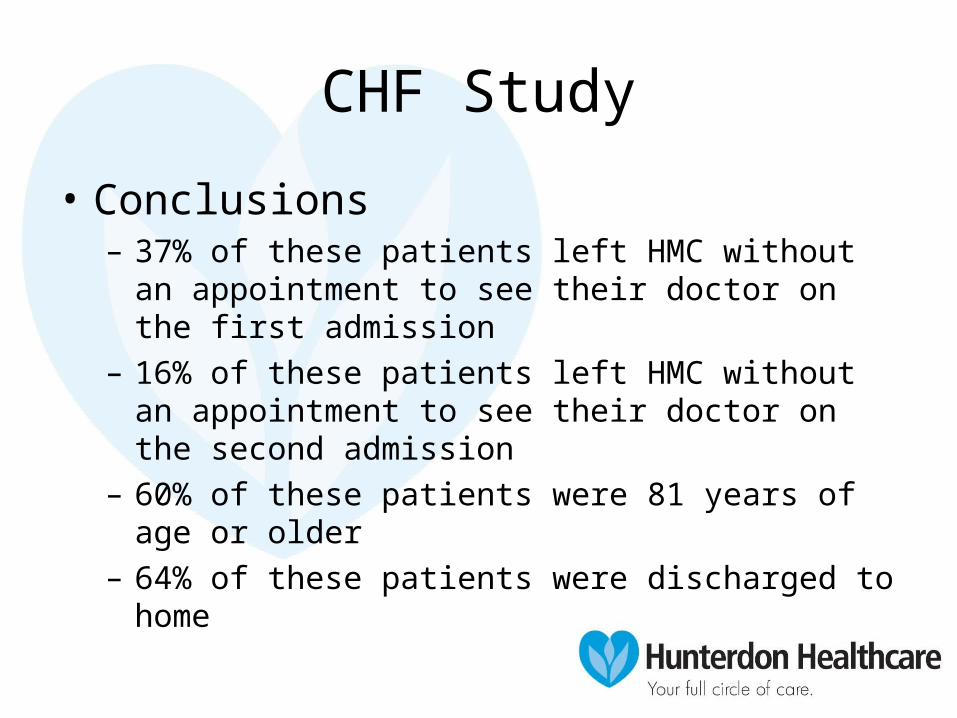
CHF Study
• Conclusions– 37% of these patients left HMC without an
appointment to see their doctor on the first admission– 16% of these patients left HMC without an
appointment to see their doctor on the second admission
– 60% of these patients were 81 years of age or older– 64% of these patients were discharged to home
Partnering with Post-Acute Providers
• Post Acute Providers were added to the Committee
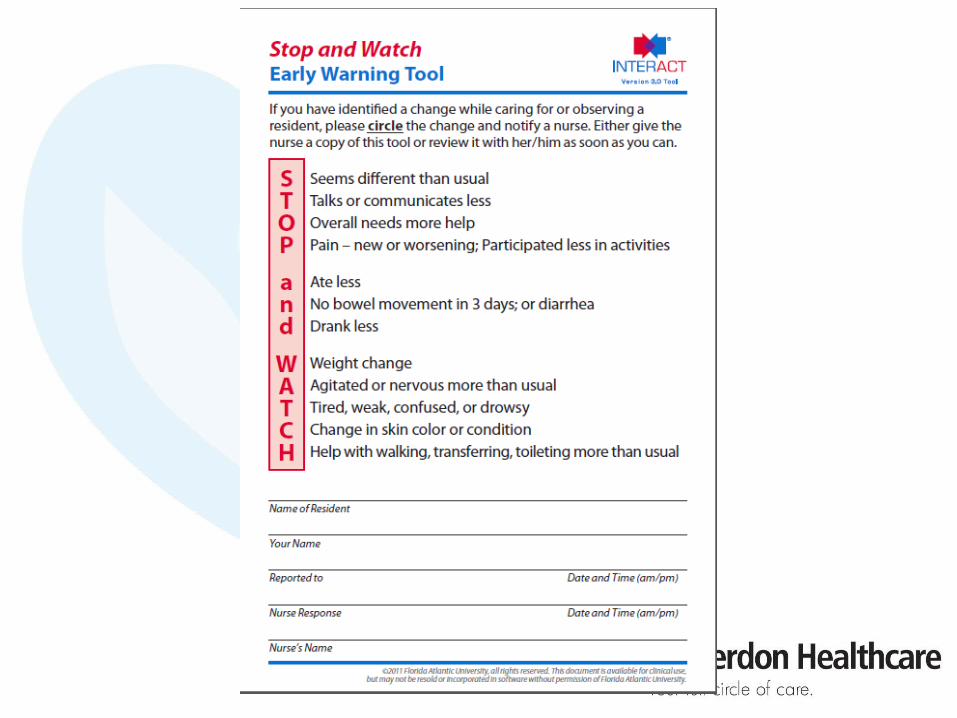
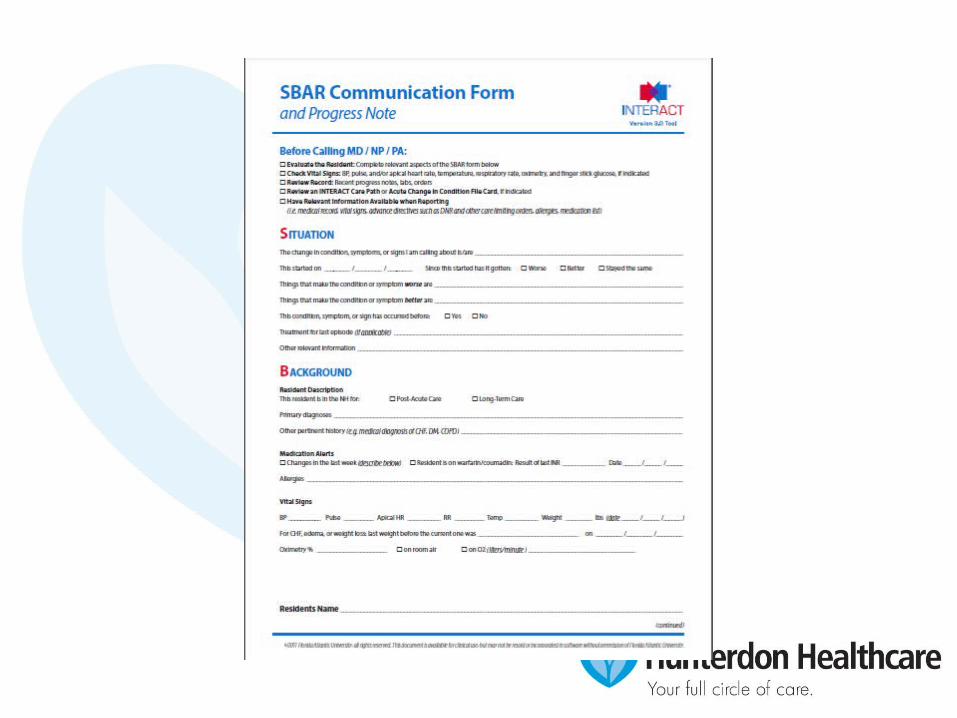
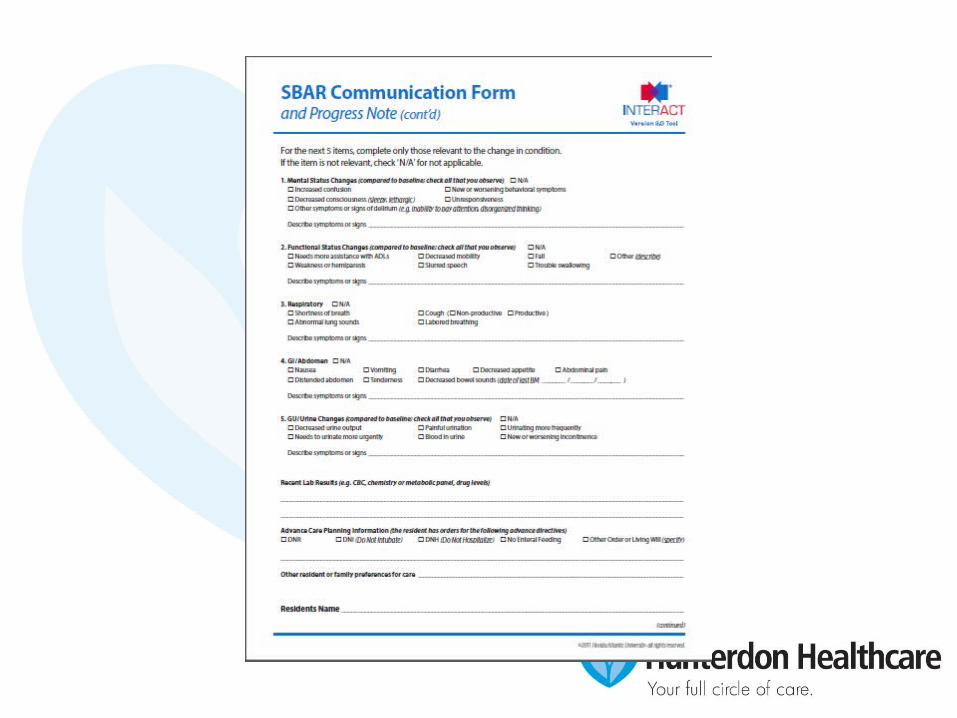
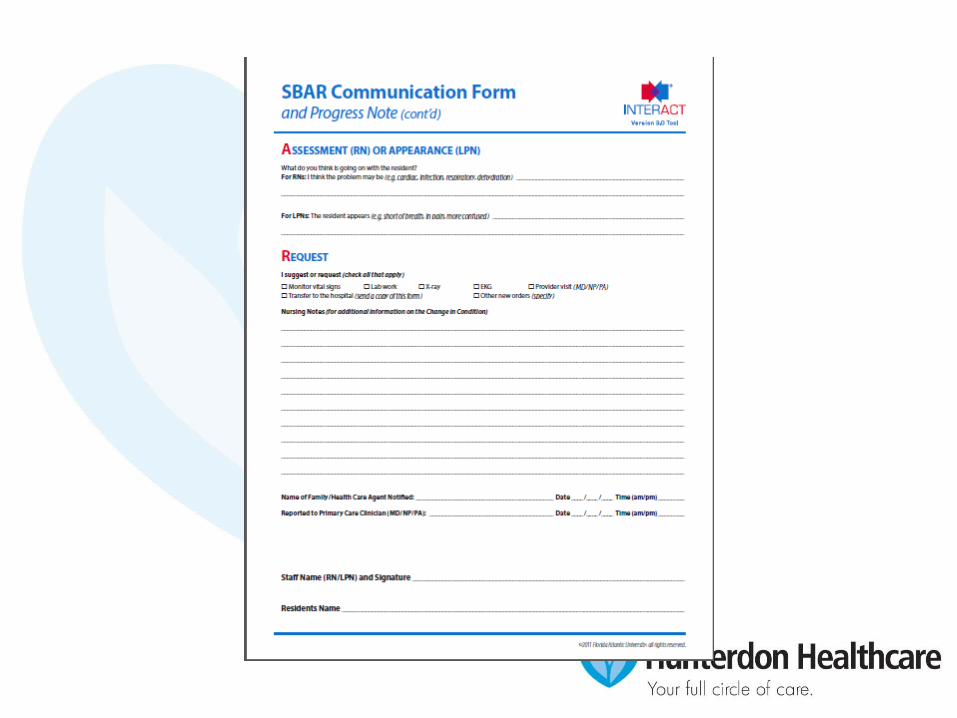
• INTERACT II (Interventions to Reduce Acute Care Transfers) Program introduced at one nursing home– Program to identify early changes in resident
status that could lead to hospitalization– Tools available through http://interact2.net/
Expansion of the Committee Role
• In September 2012, the Committee decided to look globally at readmissions and to look at processes around readmissions including:– Discharge checklists– Transfer of Information– Medication Reconciliation
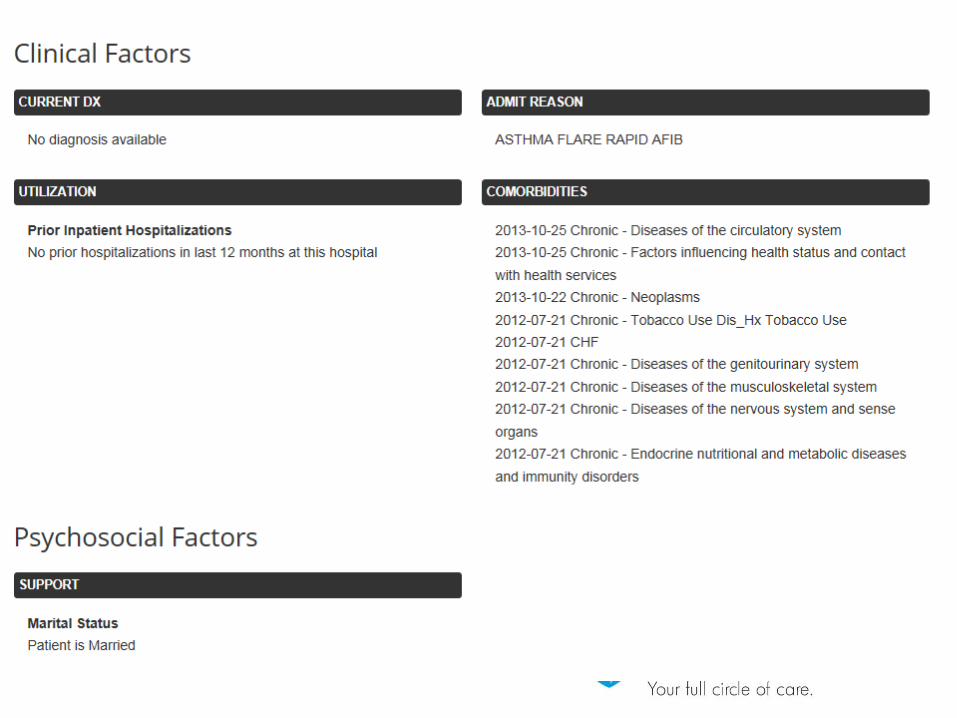
Risk Stratification
• We beta tested a program called Crimson RealTime from the Advisory Board Company
• Using historical billing data, the software was designed to:– Identify patients at high risk via a proprietary
algorithm– Identify CHF, Pneumonia, MI patients
Care Co-ordination Across the Continuum
• Set up a meeting with our inpatient Patient Care Managers and our Care Coordinators in the primary care offices
• Had them exchange phone numbers
• The Care Coordinators are informed when a high risk patient is admitted and when they are discharged
Exchange of Information
• At discharge, the unit coordinator will fax (don’t judge me) the discharge medication reconciliation and the discharge instructions to the PCP office (we are looking into a scan/e-mail system)
• It is an expectation that discharge summaries are dictated at the time of discharge—our hospitalists have this built into their bonus calculation
Follow-up
• Through our IDS, we created an expectation that high risk patients have a follow up appointment within 3 business days and moderate risk patients within one week
• We have not been universally successful in getting f/u appointments made prior to the patient leaving the building
Follow-up
• Our Clinical Nurse Leaders make phone calls 1-2 days after discharge and ask whether patients have their post-acute appointments made and whether they have filled their discharge prescriptions
• Care Coordinators will also reach out in a similar manner
Other Factors
• Our Home Health Company has invested in 20 telehealth monitors for CHF patients
• We have had our word processing department “push” discharge summaries out to the PCP of record
Next Steps
• Getting our inpatient EHR (Quadramed QCPR) to talk to our outpatient system (NextGen), especially regarding medications, and medical documentation
• Continue to improve our patient education functions• Continue to improve communication between Hospitalist
and PCP• Filling discharge prescriptions in outpatient pharmacy• Greater acceptance of Palliative Care and Hospice
services by both physicians and families
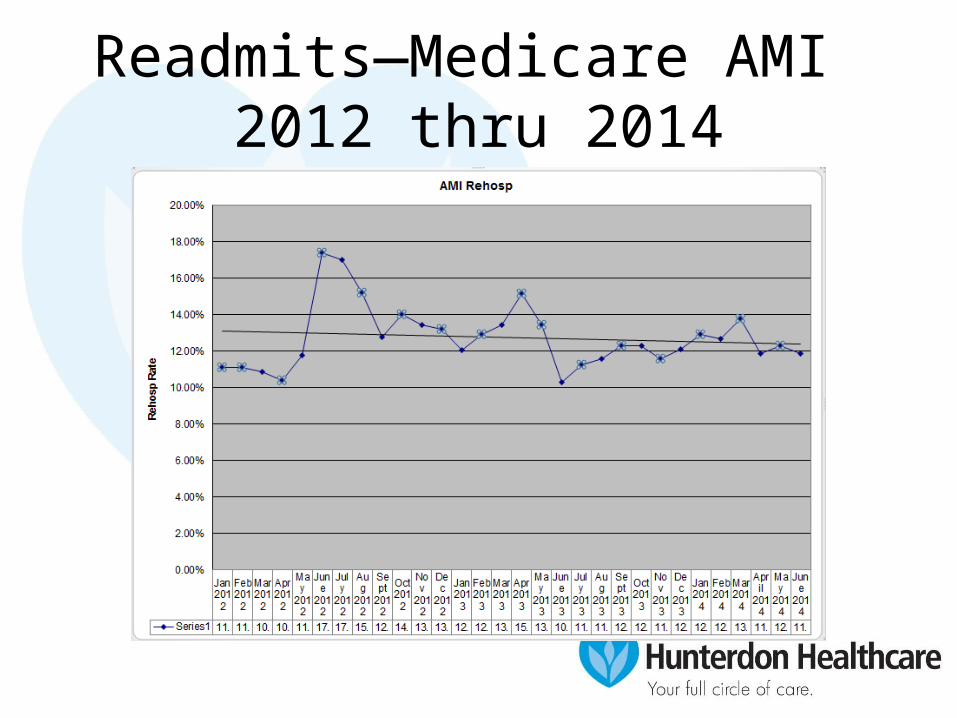
Readmits—Medicare AMI 2012 thru 2014
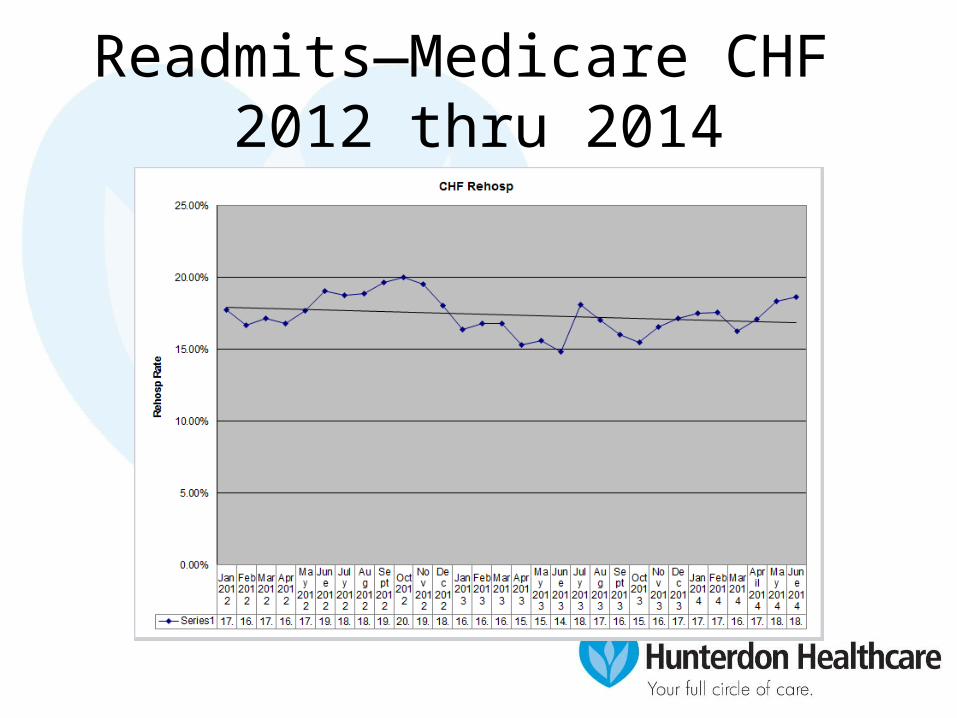
Readmits—Medicare CHF 2012 thru 2014
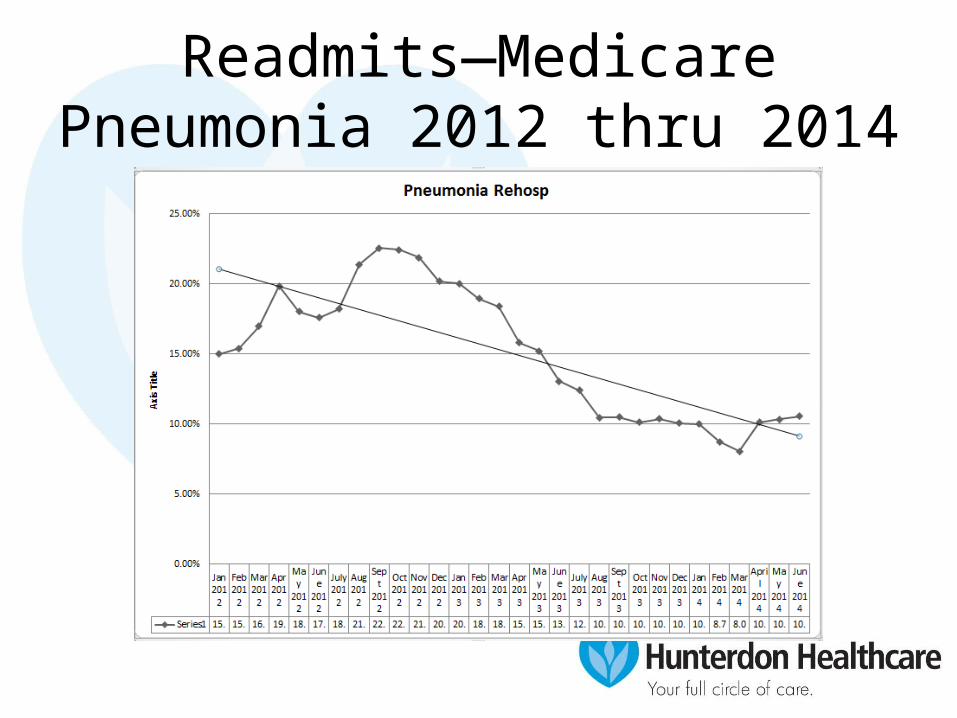
Readmits—Medicare Pneumonia 2012 thru 2014
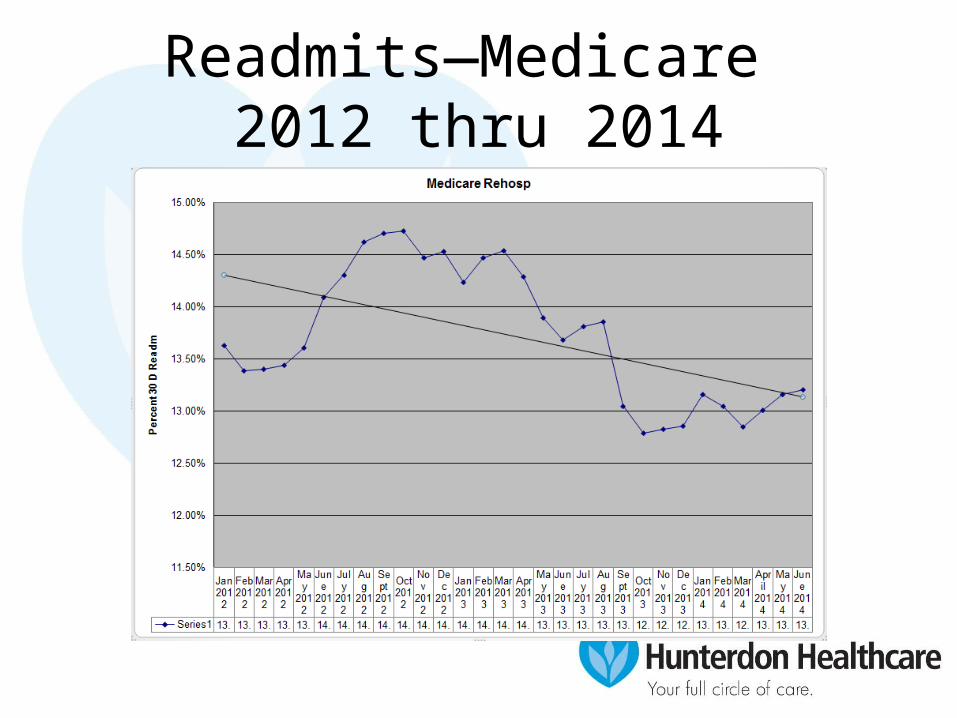
Readmits—Medicare 2012 thru 2014
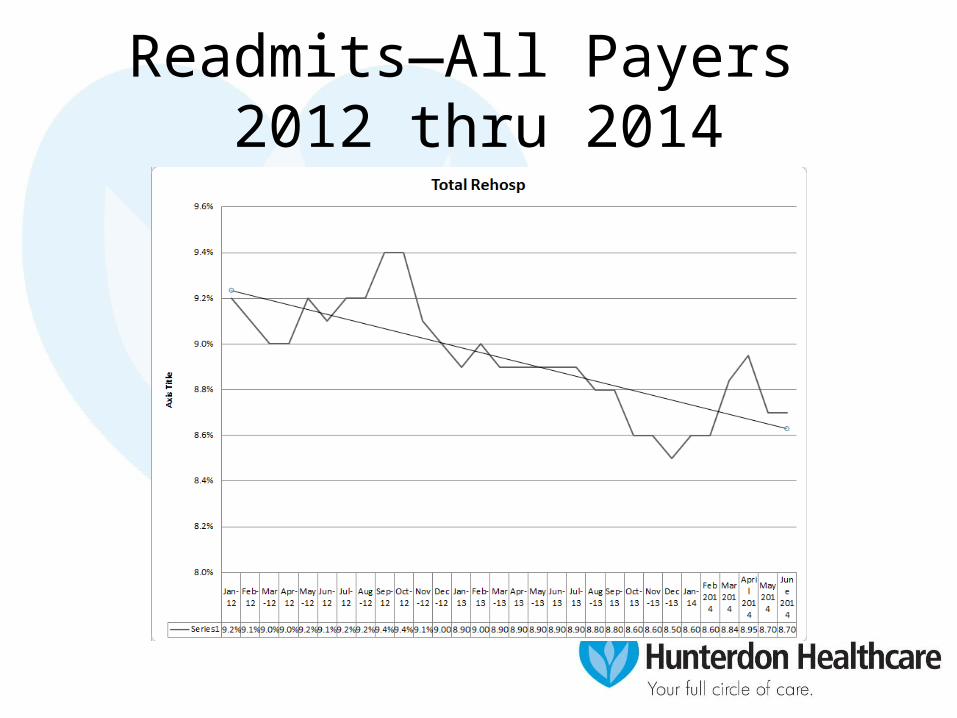
Readmits—All Payers 2012 thru 2014