
Rapid Systematic Review Health-Related Quality of Life in ...
35
Occupational Therapy Interventions for Improving Health-Related Quality of Life in Adults Post-Stroke: A Rapid Systematic Review Nicole Ellis, OTS, Claire Havala, OTS, Lauryn Johnson, OTS, Braegan Lyon, OTS, Maria Stiens, OTS Occupational therapy doctoral students at Indiana University; [email protected] This rapid systematic review of the literature examines 24 articles from the databases of Pubmed and CINAHL to determine the evidence and effectiveness of occupational therapy (OT) interventions in improving health-related quality of life (HRQOL) of adults post-stroke. Many adults report a decline in life satisfaction and occupational performance following a stroke due to various physical, cognitive, and emotional impairments. OT is a key component of stroke rehabilitation; therefore, there is a high need for effective and evidence-based occupational interventions for individuals post-stroke. Findings of this rapid systematic review reveal that the use of occupation-based activities has reasonable yet limited evidence to support its effectiveness in improving HRQOL for adults post-stroke. This review supports the premise that HRQOL, including physical wellbeing and occupational performance, can be positively affected through the use of several commonly used OT interventions. Specifically, there is strong evidence to support the use of robot-assisted therapy and bilateral upper extremity training for improving physical wellbeing. Additionally, there is strong evidence supporting the use of the Cognitive Orientation to daily Occupational Performance (CO-OP) approach for improving occupational performance. All other interventions included in this review ranged from low to moderate levels of evidence in improving HRQOL, therefore, future studies with larger sample sizes and equal treatment groups should be conducted to confirm the results of this rapid systematic review. Focused Clinical Question The purpose of this rapid systematic review was to search the literature, critically appraise, and analyze the applicable findings to address the following focused question: For 1 Indiana University Occupational Therapy
Transcript of Rapid Systematic Review Health-Related Quality of Life in ...

Occupational Therapy Interventions for ImprovingHealth-Related Quality of Life in Adults Post-Stroke: ARapid Systematic Review
Nicole Ellis, OTS, Claire Havala, OTS,Lauryn Johnson, OTS, Braegan Lyon, OTS,Maria Stiens, OTSOccupational therapy doctoral students at IndianaUniversity; [email protected]
This rapid systematic review of the literature examines 24articles from the databases of Pubmed and CINAHL todetermine the evidence and effectiveness of occupationaltherapy (OT) interventions in improving health-relatedquality of life (HRQOL) of adults post-stroke. Many adultsreport a decline in life satisfaction and occupationalperformance following a stroke due to various physical,cognitive, and emotional impairments. OT is a keycomponent of stroke rehabilitation; therefore, there is a highneed for effective and evidence-based occupationalinterventions for individuals post-stroke. Findings of thisrapid systematic review reveal that the use ofoccupation-based activities has reasonable yet limitedevidence to support its effectiveness in improving HRQOLfor adults post-stroke. This review supports the premise thatHRQOL, including physical wellbeing and occupationalperformance, can be positively affected through the use ofseveral commonly used OT interventions. Specifically, thereis strong evidence to support the use of robot-assistedtherapy and bilateral upper extremity training for improvingphysical wellbeing. Additionally, there is strong evidencesupporting the use of the Cognitive Orientation to dailyOccupational Performance (CO-OP) approach for improvingoccupational performance. All other interventions includedin this review ranged from low to moderate levels ofevidence in improving HRQOL, therefore, future studieswith larger sample sizes and equal treatment groups shouldbe conducted to confirm the results of this rapid systematicreview.
Focused Clinical Question
The purpose of this rapid systematic review was to searchthe literature, critically appraise, and analyze the applicablefindings to address the following focused question: For
1Indiana University Occupational Therapy

adults post-stroke, what is the effectiveness of occupationaltherapy for improving health-related quality of life?
Statement of Problem and Background
Stroke is the leading cause of disability in the United States,affecting 700,000 Americans every year (Almhdawi et al.,2016). Individuals living with long-term disabilitypost-stroke may experience decreased function in theiraffected side, resulting in limited ability to performmeaningful occupations and a decrease in overall quality oflife (Lewthwaite et al., 2018). Over 60% of individuals whoexperience a stroke require rehabilitation to regain functionin their daily lives and improve their quality of life, whichmeans that rehabilitation is a crucial part of post-strokerecovery. Despite this need for effective rehabilitationtechniques, research related to upper extremity recovery isstill limited (Almhdawi et al., 2016). Additionally, researchshows that occupational gaps are still widely present inindividuals post-stroke even after a full year of strokerehabilitation (Eriksson et al., 2015).
As mentioned previously, stroke is the leading cause ofdisability in the United States, which demands that OTinterventions for this population are evidence based andeffective. Despite this need, research states that there is stilllimited evidence to support many stroke-related OTinterventions and that many individuals still experienceoccupational gaps after a full year of intervention. Therefore,there is a need for evidence-based and effective OTinterventions for improving health-related quality of life inadults post-stroke.
Methods for Conducting theEvidence-Based Review
This rapid systematic review was conducted to identify OTinterventions that could be implemented to improve theHRQOL in adults post-stroke. This search topic was chosenby OT students who felt that HRQOL is one of the mostimportant outcomes for adults post-stroke. The articlesincluded in this review were gathered from the databases ofPubmed and CINAHL. This search was conducted by theaforementioned group of OT students with guidance fromlibrarians and professors from IUPUI’s School of Health &Human Sciences and Department of Occupational Therapy.Through this collaboration a relevant PICO question wasdeveloped, which led to the following search terms. Thesearches were filtered with the dates of 2010-2021.
Pubmed MESH Term Search:
(("Stroke"[Mesh]) AND ( "OccupationalTherapy"[Mesh] OR "Occupational TherapyDepartment, Hospital"[Mesh] )) AND "Adult"[Mesh]
CINAHL Search:stroke and OT and adult
This review utilized the levels of evidence criteria from thearticle titled “Evidence based medicine: What it is and whatit isn't” (Sacket et al.,1996) to determine the level ofevidence of each article. Articles that were level I, level II,and level III evidence were included in the study, whilearticles that were level IV and IV evidence were excluded.This rapid systematic review did not include meta-analyses,systematic reviews, descriptive studies, or case reports.Studies were initially excluded if they were not conducted inEnglish-speaking countries, but due to the limited number ofstudies, the search was expanded to include studies from allcountries. The inclusion and exclusion criteria were asfollows:
Inclusion criteria:● Participants were 18 years or older● Participants reported a history of one or more
strokes● Written in English● Method of intervention must be included within
the scope of OT● Outcomes included within the scope of HRQOL
Exclusion criteria:● Pilot studies● Studies published before 2010● Medication-only interventions
A total of 503 studies were imported into Covidence forscreening, with a total of 501 studies imported from Pubmedand CINAHL and 2 studies that were personally added dueto their high level of evidence and ability to meet theinclusion criteria. Each abstract was screened to determinerelevance and level of evidence, and articles required 2 votesfrom reviewers in order to be moved to the full-text review.Abstract screening resulted in 59 studies, which were movedto full-text review and assessed for eligibility. Each studyrequired 2 votes before being exported and used for the rapidsystematic review. A total of 25 articles were selected to beincluded, although one was dropped due to duplication,resulting in the final total of 24 studies (See Figure 1). Thearticles included in this rapid systematic review were brokeninto two main outcomes included within the scope of theoverall outcome of HRQOL.
2Indiana University Occupational Therapy

Outcome 1: Physical wellbeing● Included upper extremity function, muscular
strength, range of motion, hand prehension,motor recovery, visual functions, and sensoryfunction
Outcome 2: Occupational performance● Included performance in functional/daily
activities, transfer to untrained activities,community reintegration, participation inoccupations, functional use of the arm, quality oflife, depression, performance in IADL, personalmanagement, and independence
Figure 1: PRISMA diagram generated by Covidence
Results
Twenty-four studies were used in this systematic review thatfollowed inclusion and exclusion criteria. Twenty-one wereLevel I evidence, one was Level II evidence, and two wereLevel III evidence. From these studies, the authors identifiedthe following HRQOL outcome themes: Physical wellbeingand occupational performance.
Physical Wellbeing
Four level I randomized controlled trials compared robotactive assisted therapy to traditional occupational therapy(OT) (Orihuela-Espina et al., 2016; Xu et al., 2020; Sale etal., 2014; Lee et al., 2018). Three of the four studiesconcluded that the intervention of robot assisted therapyshowed significant physical improvements using the Wolf
Motor Function Test, Fugl-Meyer Score, and/or the BarthelIndex compared to the control group. One study reported nosignificant difference between the two groups after treatmentoverall (Xu et al., 2020).
A Level I two-group randomized comparison designstudy (Hayner et al., 2010) measured upper extremityfunction in constraint-induced movement therapy (CIMT)versus traditional bilateral upper extremity OT using theCanadian Occupational Performance Measure and the WolfMotor Function Test. The authors found significantimprovements in bilateral upper extremity function withinboth groups, and no significant differences between groups.
A Level I two-group randomized controlled trial (Lee etal., 2016) compared bilateral upper extremity training in avirtual reality environment and traditional bilateral upperextremity training. The authors found that the interventiongroup exhibited significant improvements in upper extremityfunction and muscle strength after the 6 week trainingprogram when compared to the control group.
A Level I randomized controlled trial (Jang et al., 2016)compared the effectiveness of Brain-ComputerInterface-Controlled Functional Electrical StimulationTraining (BCI-FES) paired with conventional OT tofunctional electrical stimulation (FES) on shouldersubluxation. The authors found that BCI-FES paired withconventional OT had the greatest impact on improvingshoulder flexion and abduction and reducing verticalsubluxation when compared to FES alone.
One Level I single-blind randomized trial (Winstein etal., 2016) randomized individuals into one of three groups.The intervention was completed within 16 weeks andinvolved accelerated skill acquisition program, monitoringonly and customary care UCC, and dose-equivalent usualpractice. Among participants with motor stroke andprimarily moderate upper extremity impairment, the use ofthe task-oriented program did not significantly improvemotor function. The findings do not support the superiorityof the ASAP intervention among patients with motor strokeand moderate upper extremity impairment.
One Level I randomized controlled trial (Pandian et al.,2011) compared Brunnstrom hand manipulation (BHM) anda motor relearning program (MRP) to determine theiroutcomes on chronic stroke patients. The authors concludedthat both interventions were effective in enhancing motorrecovery in the hand, however, there were statisticallysignificant results in favor of Brunnstrom movement therapy.Specifically, BHM was found to be better than MRP atimproving wrist and hand recovery, especially mass fingerflexion, extension, and grasp.
One Level I randomized controlled trial (Lin et al., 2010)compared the effects of bilateral arm training (BAT) totraditional OT in adults post-stroke. The authors reportedthat BAT showed better temporal and spatial efficiencyduring unilateral and bilateral tasks compared to standardOT, and the BAT group demonstrated significantly greater
3Indiana University Occupational Therapy

improvements in motor performance and motor impairment.A Level I three-armed randomized control trial
(Mödden et al., 2012) compared the effects of RestitutionTraining (RT) and Compensatory Training (CT) to OT. TheVisual Field Assessment, Testing Battery for AttentionPerformance, Behavioral Inattention Test, and ExtendedBarthel Index were used to assess visual field expansion forRT, visual search performance for CT, reading performancefor both treatments,The Barthel Index and Visualconjunction. Evidence from this study suggests that CTresulted in a better visual search performance compared toOT, and RT did not result in a larger expansion of the visualfield. CT improved all defined outcome parameters and RTseveral, whereas OT only improved one.
One Level I randomized control trial (Iwamoto et al.,2019) looked at 12 acute first time stroke patients that weredivided into two groups. Group one received combinationhybrid assistive limb (HAL-SJ) and OT, and group tworeceived just traditional OT. There were no significantdifferences seen in motor function severity defined by theoutcome measures between groups on day 14 after stroke.ADL limitations were not significantly different betweengroups either. Overall, there were no significant changesbetween group one and two after intervention.
Occupational Performance
Four Level I randomized controlled trials utilized theCognitive Orientation to daily Occupational Performance tocompare to other methods (Ahn et al., 2017; Song et al.,2019; McEwen et al., 2015; Wolf et al., 2016). All fourstudies reported the CO-OP approach to be beneficial, apositive therapeutic intervention, and highly significantcompared to the control groups.
One Level I randomized controlled trial (Mortensen etal., 2016) compared the use of combined transcranial directcurrent stimulation (tDCS) and home based OT. This studylooked at the ability to complete the Jebsen-Taylor Test(JTT) for activity and function, and also looked at the strokeimpact scale scores. There was a tendency for greaterimprovement in ADL performance in the anodal groupcompared with the sham group, and statistically significantimprovement in grip strength in the anodal group comparedto sham. Over time, both groups did improve in logJTT.
One Level I randomized controlled trial (Sackley et al.,2014) utilized a three-month long program of OT which wasdelivered by occupational therapists and assistants andinvolved patient centered goal setting, education, andadaptations to the environment. Scores on the Barthel Indexwere measured for ADLs at three months
post-randomization, along with 6 and 12 months. Betweenthe treatment arms, there was no significant difference. Theadjusted mean difference in Barthel index score at threemonths was .19 points higher in the intervention arm.
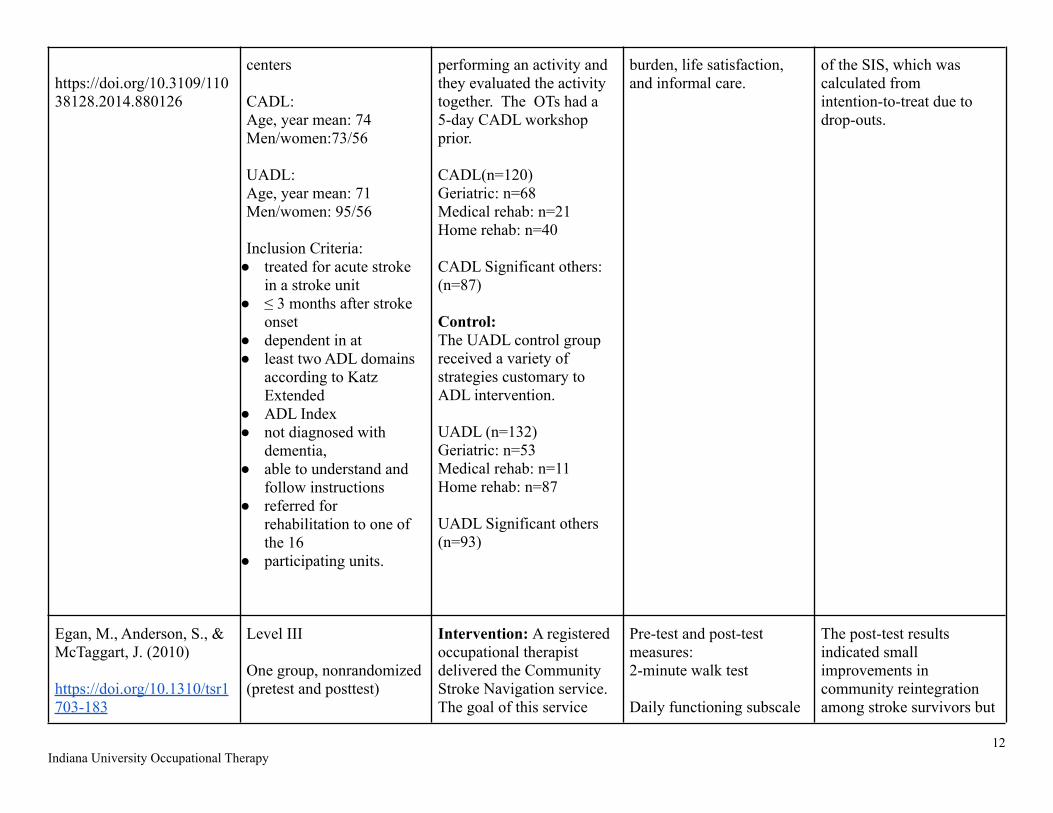
One Level III single group non-randomized pretest-posttest design (Egan et al., 2010) found that a CommunityStroke Navigation service that included case coordination,“just in time” education, coaching, family supportorganization, and accompaniment resulted in a smallimprovement in community reintegration among strokesurvivors and no significant changes among care partners.No changes in physical or emotional health were reported bystroke survivors or care partners.
One Level I cross-over randomized controlled trial(Almhdawi et al., 2016) provided evidence that a 6-weektask-oriented OT intervention that was individualized usingthe COPM produced statistically higher functional changescores than the control, which included significantimprovements in all functional measures including theCanadian Occupational Performance Measure (COPM),Motor Activity Log (MAL), and Wolf Motor Function Test(WMFT). The authors did not report significantimprovements over the control on any of the impairmentoutcomes including measures of active range of motion(AROM) and muscular strength.
One Level III single group repeated measures design(Henderson & Manns, 2012) found that group modifiedconstraint induced movement therapy (mCIMT) resulted instatistically and clinically significant improvements infunctional use of the arm and participation in meaningfuloccupations in thirteen stroke and two brain injuryparticipants. Significant improvements in motor recoverywere found as well.
One Level I randomized controlled trial (Linder et.al.,2015) compared the effectiveness of a home-based robotassisted rehabilitation program paired with a home exerciseprogram (HEP) to a HEP alone on improving the quality oflife and depression in adults post-stroke. The authorsreported that both interventions were similar in effectivenessproducing no superior results over another.
One Level II cohort study (Msengana et. al., 2019)assessed the effectiveness of a two-month conventional OTprogram on improving upper limb mobility and personalmanagement in adults post-stroke. The authors reported thatthere were significant improvements in all aspects of upperlimb function personal management, self-care, toileting, andmobility.
4Indiana University Occupational Therapy

One Level I randomized controlled trial (Bertilsson etal., 2014) compared the effects of client-centered ADL(CADL) OT to usual care OT including the ability to usehome-help service, independence in ADL, life satisfaction,perceived participation, and satisfaction with training. Intheir significant others, it looked at life satisfaction,caregiver burden, and informal care. The results indicate thatCADL does not appear to cause short-term differences inoutcomes. A part of the SIS was “emotion” which created asignificant effect, calculated from intention-to-treat due todrop-outs.
Implications for Practice and Research inOccupational Therapy
This rapid systematic review shows strong evidence that avariety of occupational therapy interventions are effective inimproving HRQOL in adults post-stroke. Specifically, thereis evidence that supports that OT interventions improvephysical wellbeing and occupational performance, which areboth major components of HRQOL. The review foundmoderate evidence to support the use of robot-assistedtherapy and constraint-induced movement therapy (CIMT)for improving both occupational performance and physicalwellbeing.
Overall significant physical improvements were noted fromrobot-assisted therapy, CIMT, bilateral upper extremitytraining, Brain-Computer Interface-Controlled FunctionalElectrical Stimulation Training with OT, Brunnstrom HandManipulation (BHM), motor relearning program, andcompensatory training. There was strong evidence to supportthe use of robot-assisted therapy and bilateral upperextremity training for improving physical wellbeing. Allother interventions with significant results had limitedevidence to support their clinical use.
Overall significant improvements in occupationalperformance were reported for CO-OP, task-oriented OT,combined transcranial direct current stimulation withhome-based OT, group mCIMT robot-assisted therapy withan HEP, HEP alone, and conventional OT. There was strongevidence to support the use of the CO-OP approach forimproving occupational performance. All other interventionswith significant results had limited evidence to support theirclinical use.
The results of this review can be used in practice as a meansto support the use of occupational therapy interventions forimproving HRQOL in adults post-stroke. This reviewindicates that robot-assisted therapy, bilateral upper
extremity training, CIMT and CO-OP are all beneficial inimproving aspects of HRQOL of adults post-stroke.Occupational therapists can adapt these interventions andimplement them with a stroke population to addresshealth-related quality of life including occupationalperformance and physical wellbeing.
The feasibility of implementation of the aforementionedinterventions may be affected by the financial costs andaccessibility to equipment. The need for training on certaintechniques and intervention strategies adds additionalbarriers to implementation.
This review found multiple significant gaps in the literature.First, there appears to be a significant lack in the number ofstudies on this topic that were conducted and published inthe United States. Due to the large variability in healthcaresystems used throughout the world, there is a need for morestudies exploring post-stroke OT interventions to beconducted within the United States. Additionally, many ofthe interventions explored in this review had limitednumbers of high level studies conducted on them. Therefore,there is a need for more research, especially randomizedcontrolled trials, to be conducted on OT stroke interventions.Lastly, there was a lack of feasibility studies conducted onthe OT interventions included in this review. Due to the widevariety in resources between healthcare facilities, additionalfeasibility studies should be conducted to determine thefeasibility of various stroke-related OT interventions.
Limitations
The majority of studies used in this review are Level Ievidence and published within the last eleven years. Despitethese strengths, there were still several limitations for thisreview. This review is a rapid systematic review, and not afull systematic review, which means that a limited number ofarticles were included in this review and that manypotentially relevant articles were excluded. An additionallimitation was the lack of access to articles. Because of thislack of access, several articles were excluded fromscreening. Other limitations include small sample sizes,unequal treatment between groups, use of self-reportingmeasures, unsuitable follow up times, drop outs due to death,and inadequately short treatment durations.
Conclusions
Overall, this review suggests that OT interventions arebeneficial in improving HRQOL in adults post-stroke. Thereviewed studies indicate that there is strong evidence for theeffectiveness of robot-assisted therapy and bilateral upperextremity training on physical wellbeing. Additionally,
5Indiana University Occupational Therapy

strong evidence was found for the use of CO-OP inimproving occupational performance. Lastly, there wasmoderate evidence that CIMT and robot-assisted therapyimproved both physical wellbeing and occupationalperformance in individuals post-stroke
It should be noted that some of the studies included in thisreview had conflicting results, potentially due tomethodological limitations and structure. Additionally, therewas limited evidence on the majority of the interventionsincluded in this review, therefore, there is a need for furtherinvestigation of post-stroke OT interventions to improveHRQOL. Future studies with larger sample sizes and equaltreatment groups are needed to confirm the results of thisrapid systematic review.
Acknowledgements
We would like to thank Rachel Hinrichs from the Ruth LillyMedical Library; and Rick Ralston, MSLIS; Anthony Chase,PhD and Terry Petrenchik, PhD, OTR/L; who providedguidance and assistance with this rapid systematic review.This review was completed for the Applied Research inOccupational Therapy course offered through theDepartment of Occupational Therapy at Indiana University.
References
Ahn, S.-nae, Yoo, E.-young, Jung, M.-ye, Park, H.-yean,Lee, J.-yeon, & Choi, Y.-im. (2017).Comparison of cognitive orientation to dailyoccupational performance and conventionaloccupational therapy on occupationalperformance in individuals with stroke: Arandomized controlled trial.NeuroRehabilitation.https://doi.org/10.3233/nre-161416
Almhdawi, K. A., Mathiowetz, V. G., White, M., &delMas, R. C. (2016). Efficacy of occupationaltherapy task-oriented approach in upperextremity post-stroke rehabilitation.Occupational Therapy International, 23(4),444-456. doi:10.1002/oti.144
Bertilsson, A. S., Ranner, M., von Koch, L., Eriksson,G., Johansson, U., Ytterberg, C., Guidetti, S., &Tham, K. (2014). A client-centred ADLintervention: three-month follow-up of arandomized controlled trial. Scandinavianjournal of occupational therapy, 21(5), 377–391.https://doi.org/10.3109/11038128.2014.880126
Egan, M., Anderson, S., & McTaggart J. (2010).
Community navigation for stroke survivors andtheir care partners: Description and evaluation.Topics in Stroke Rehabilitation, 17(3), 183-190.https://doi.org/10.1310/tsr1703-183
Eriksson, G., Aasnes, M., Tistad, M., Guidetti, S., & vonKoch, L. (2015). Occupational gaps in everydaylife one year after stroke and the associationwith life satisfaction and impact of stroke.Topics in Stroke Rehabilitation, 19(3), 244–255.https://doi.org/10.1310/tsr1903-244
Hayner, K., Gibson, G., & Giles, G. M. (2010).Comparison of constraint-induced movementtherapy and bilateral treatment of equal intensityin people with chronic upper-extremitydysfunction after cerebrovascular accident. TheAmerican journal of occupational therapy :official publication of the AmericanOccupational Therapy Association, 64(4),528–539. https://doi.org/1
Henderson, C. A. & Manns, P. J. (2012). Group modifiedconstraint-induced movement therapy (mCIMT)in a clinical setting. Disability & Rehabilitation,34(25), 2177-2183.https://doi.org/10.3109/09638288.2012.673686
Iwamoto, Y., Imura, T., Suzukawa, T., Fukuyama, H.,Ishii, T., Taki, S., Imada, N., Shibukawa, M.,Inagawa, T., Araki, H., & Araki, O. (2019)Combination of Exoskeletal Upper Limb Robotand Occupational Therapy Improve Activities ofDaily Living Function in Acute Stroke Patients.Journal of Stroke & Cerebrovascular Diseases,28(7).https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.03.006
Jang, Y. Y., Kim, T. H., & Lee, B. H. (2016) Effects ofBrain-Computer Interface-controlled FunctionalElectrical Stimulation Training on ShoulderSubluxation for Patients with Stroke: ARandomized Controlled Trial. Occup Ther Int,23(2), 175-185. doi:10.1002/oti.1422
Lee, M.-J., Lee, J.-H., & Lee, S.-M. (2018). Effects ofrobot-assisted therapy on upper extremityfunction and activities of daily living inhemiplegic patients: A single-blinded,randomized, controlled trial. Technology andHealth Care, 26(4), 659–666.https://doi.org/10.3233/thc-181336
Lee, S., Kim, Y., & Lee, B.-H. (2016). Effect of virtual6
Indiana University Occupational Therapy

reality-based bilateral upper extremity trainingon upper extremity function after stroke: Arandomized controlled clinical trial.Occupational Therapy International, 23(4),357–368. https://doi.org/10.1002/oti.1437
Lin, K.-C., Chen, Y.-A., Chen, C.-L., Wu, C.-Y., &Chang, Y.-F. (2010). The effects of bilateral armtraining on motor control and functionalperformance in chronic stroke: A randomizedcontrolled study. Neurorehabilitation and NeuralRepair, 24(1), 42-51.doi:10.1016/j.jbmt.2011.11.002
Linder, S. M., Rosenfeldt, A. B., Bay, R. C., Sahu, K.,Wolf, S. L., & Alberts, J. L. (2015) . Improvingquality of life and depression after strokethrough telerehabilitation. American Journal ofOccupational Therapy, 69, 6902290020.
http://dx.doi.org/10.5014/ajot.2015.014498
McEwen, S., Polatajko, H., Baum, C., Rios, J., Cirone,D., Doherty, M., & Wolf, T. (2015). CombinedCognitive-Strategy and Task-Specific TrainingImprove Transfer to Untrained Activities inSubacute Stroke: An Exploratory RandomizedControlled Trial. Neurorehabilitation and neuralrepair, 29(6), 526–536.https://doi.org/10.1177/1545968314558602
Mödden, C., Behrens, M., Damke, I., Eilers, N., Kastrup,A., & Hildebrandt, H. (2012). A randomizedcontrolled trial comparing 2 interventions forvisual field loss with standard occupationaltherapy during inpatient stroke rehabilitation.Neurorehabilitation and neural repair, 26(5),463–469.https://doi.org/10.1177/1545968311425927
Msengana, Z., De Witt, P., Owen, A., & Franzsen, D.(2019) Upper limb mobility and personalmanagement in patients with stroke attendingoccupational therapy at a tertiary hospital inGauteng. South African Journal of OccupationalTherapy, 49(3), 6-16.doi:10.17159/2310-3833/2019/vol49n3a3
Mortensen, J., Figlewski, K., & Andersen. H. (2016)Combined transcranial direct current stimulationand home-based occupational therapy for upperlimb motor impairment following intracerebralhemorrhage: a double-blind randomizedcontrolled trial. Disability and Rehabilitation,
38(7), 637-643.https://doi.org/10.3109/09638288.2015.1055379
Orihuela-Espina, F., Roldán, G. F.,Sánchez-Villavicencio, I., Palafox, L., Leder, R.,Sucar, L. E., & Hernández-Franco, J. (2016).Robot training for hand motor recovery insubacute stroke patients: A randomizedcontrolled trial. Journal of Hand Therapy, 29(1),51–57. https://doi.org/10.1016/j.jht.2015.11.006
Pandian, S., Arya, K. N., & Davidson, E. W. R. (2011).Comparison of Brunnstrom movement therapyand motor relearning program in rehabilitationof post-stroke hemiparetic hand: A randomizedtrial. Journal of Bodywork & MovementTherapies, 16(1), 330-337.doi:10.1016/j.jbmt.2011.11.002
Sackett, D. L., Rosenberg, W. M., Gray, J. A., Haynes,R. B., & Richardson, W. S. (1996). Evidencebased medicine: What it is and what it isn't. Bmj,312(7023), 71-72. doi:10.1136/bmj.312.7023.71
Sackley, C. M., Walker, M. F., Burton, C. R., Watkins, C.L., Mant, J., Roalfe, A. K., Wheatley, K.,Sheehan, B., Sharp, L., Stant, K. E.,Fletcher-Smith, J., Steel, K., Wilde, K., Irvine,L., Peryer, G., & OTCH trial investigators(2015). An occupational therapy intervention forresidents with stroke related disabilities in UKcare homes (OTCH): cluster randomisedcontrolled trial. BMJ (Clinical research ed.),350, h468. https://doi.org/10.1136/bmj.h468
Sale, P., Mazzoleni, S., Lombardi, V., Galafate, D.,Massimiani, P., Posteraro, F., Franceschini, M.(2014) Recovery of hand function withrobot-assisted therapy in acute stroke patients: arandomized-controlled trial. Int J Rehabil Res,37(3), 236-242.doi:10.1097/MRR.0000000000000059
Song, C. S., Lee, O. N., & Woo, H. S. (2019). Cognitivestrategy on upper extremity function for stroke:A randomized controlled trials. Restorativeneurology and neuroscience, 37(1), 61–70.https://doi.org/10.3233/RNN-1808
Winstein, C., Wolf, S., Dromerick, A. et al. Effect of aTask-Oriented Rehabilitation Program on UpperExtremity Recovery Following Motor Stroke:The ICARE Randomized Clinical Trial. JAMA.
7Indiana University Occupational Therapy

2016;315(6):571–581.doi:10.1001/jama.2016.0276
Wolf, T. J., Polatajko, H., Baum, C., Rios, J., Cirone, D.,Doherty, M., & McEwen, S. (2016). Combinedcognitive-strategy and task-specific trainingaffects cognition and upper-extremity function insubacute stroke: An exploratory randomizedcontrolled trial. American Journal ofOccupational Therapy, 70(2).https://doi.org/10.5014/ajot.2016.017293
Xu, Q., Li, C., Pan, Y., Li, W., Jia, T., Li, Z., Ma, D.,Pang, X., & Ji, L. (2020). Impact of smart forcefeedback rehabilitation robot training on upperlimb motor function in the subacute stage ofstroke. NeuroRehabilitation, 47(2), 209–215.https://doi.org/10.3233/NRE-203130
8Indiana University Occupational Therapy
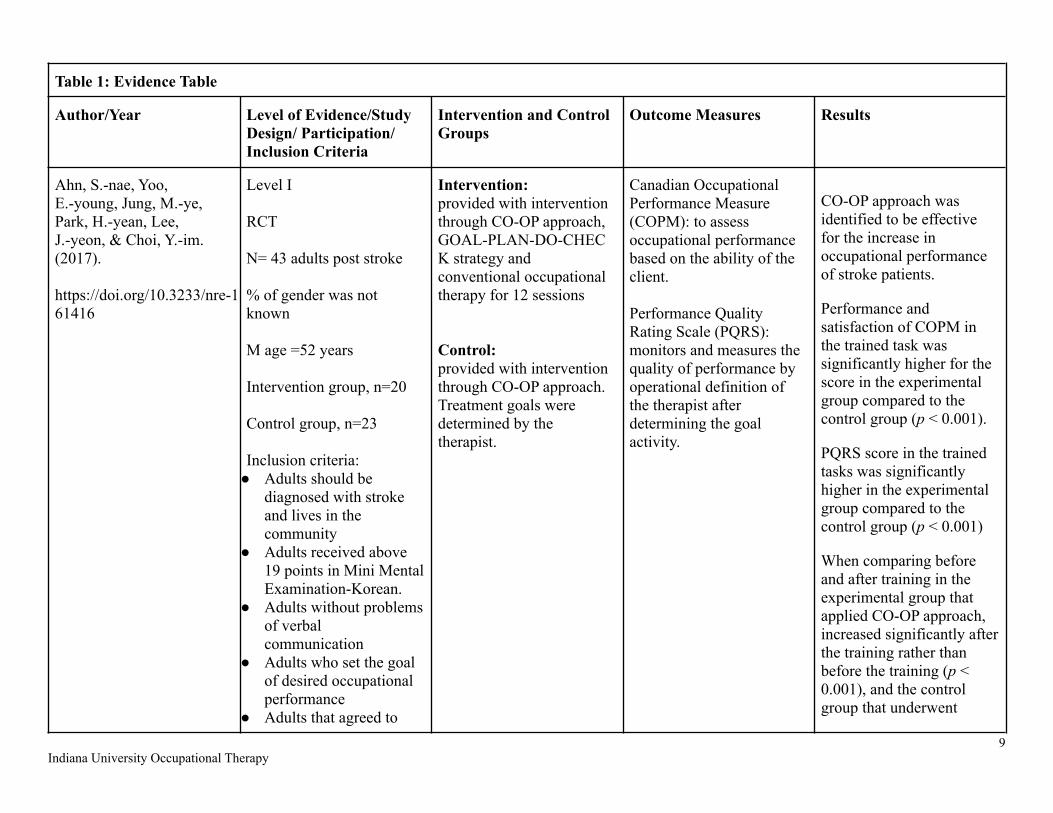
Table 1: Evidence Table
Author/Year Level of Evidence/StudyDesign/ Participation/Inclusion Criteria
Intervention and ControlGroups
Outcome Measures Results
Ahn, S.-nae, Yoo,E.-young, Jung, M.-ye,Park, H.-yean, Lee,J.-yeon, & Choi, Y.-im.(2017).
https://doi.org/10.3233/nre-161416
Level I
RCT
N= 43 adults post stroke
% of gender was notknown
M age =52 years
Intervention group, n=20
Control group, n=23
Inclusion criteria:● Adults should be
diagnosed with strokeand lives in thecommunity
● Adults received above19 points in Mini MentalExamination-Korean.
● Adults without problemsof verbalcommunication
● Adults who set the goalof desired occupationalperformance
● Adults that agreed to
Intervention:provided with interventionthrough CO-OP approach,GOAL-PLAN-DO-CHECK strategy andconventional occupationaltherapy for 12 sessions
Control:provided with interventionthrough CO-OP approach.Treatment goals weredetermined by thetherapist.
Canadian OccupationalPerformance Measure(COPM): to assessoccupational performancebased on the ability of theclient.
Performance QualityRating Scale (PQRS):monitors and measures thequality of performance byoperational definition ofthe therapist afterdetermining the goalactivity.
CO-OP approach wasidentified to be effectivefor the increase inoccupational performanceof stroke patients.
Performance andsatisfaction of COPM inthe trained task wassignificantly higher for thescore in the experimentalgroup compared to thecontrol group (p < 0.001).
PQRS score in the trainedtasks was significantlyhigher in the experimentalgroup compared to thecontrol group (p < 0.001)
When comparing beforeand after training in theexperimental group thatapplied CO-OP approach,increased significantly afterthe training rather thanbefore the training (p <0.001), and the controlgroup that underwent
9Indiana University Occupational Therapy

research conventional occupa- tionaltherapy also exhibited asignificant increase in theoccupational performanceafter training rather thanbefore training (p < 0.01)
Almhdawi, K. A.,Mathiowetz, V. G., White,M., & delMas, R. C.(2016).
doi:10.1002/oti.1447
Level I
RCT (cross-over)
N= 20 persons post-stroke
65% male35% female
M Age= 62.3 years old
Immediate interventiongroup, n= 10
Delayed interventiongroup, n= 10
Inclusion Criteria:●At least 3 months post-
onset of stroke●At least 10 degrees of
active anti-gravityshoulder abduction andflexion
●At least 10 degrees ofelbow flexion-extensionin the more affectedupper extremity
Immediate and delayedintervention groups wereused for this study. Theimmediate interventiongroup received 6 weeks ofintervention while thedelayed group received nointervention. After the 6weeks, the delayed groupthen received interventionwhile the immediateintervention group receivedno intervention.
Intervention: Participantsreceived task-orientedtherapy for two 1.5 hoursessions/week for 6 weeks.This approach is highlyclient-centered and basedupon motor learning andmotor control principles.Each participant’sintervention wasindividualized using theirCOPM results to identifythe functional activitiesthat were most important to
Outcome measures wereadministered at baseline(week 1 pretest), betweenthe two phases (week 7posttest 1), and after thesecond phase (week 12posttest 2).
COPM
Motor activity log (MAL)
Wolf motor function test(WMFT)
AROM (with goniometer)
Muscular strength(hand-held dynamometryand hand-gripdynamometry
The task-orientedintervention producedstatistically higherfunctional change scoresincluding performance andsatisfaction on the COPM,MAL scores, and WMFTscores.
10Indiana University Occupational Therapy

Exclusion●Persons with unstable
medical conditions●Persons with moderate
to severe cognitiveimpairments indicatedon the Mini-MentalStatus Test
●Persons withneurological disordersother than stroke thataffect upper extremityfunction
●Persons with severespasticity characterizedby a rigid affected upperextremity indicated bythe modified Ashworthscale
●Persons with severe painin affected upperextremity
them. Roughly 70% oftherapy time was used tointensively work on theidentified functionalactivities in the COPM,while the other 30% wasspent on supplementaryexercises includinggrasp-release training,strengthening, andspasticity management. Alogbook was kept forin-clinic and home-basedactivities for eachparticipant with thepurpose of graduallyincreasing the interventionchallenge and enhancingparticipant compliance. Noother professional upperextremity rehabilitationwas received duringintervention.
Control:Participants in the controlgroup did not receiveintervention for six weeks.
Bertilsson, A. S., Ranner,M., von Koch, L.,Eriksson, G., Johansson,U., Ytterberg, C., Guidetti,S., & Tham, K. (2014).
Level 1
RCT
N=280 people post-stroke,28 drop-outs from 16different rehabilitation
Intervention:The CADL interventiongroup includedclient-centered practice andusing the COPM forintervention. The OTobserved the client
Independence in ADL,perceived participation, lifesatisfaction, use ofhome-help service, andsatisfaction with trainingand, in their significantothers, regarding: caregiver
The results indicate thatCADL does not appear tobring about short-termdifferences in outcomes.There was a significanteffect on the outcome"emotion" which is a part
11Indiana University Occupational Therapy
https://doi.org/10.3109/11038128.2014.880126
centers
CADL:Age, year mean: 74Men/women:73/56
UADL:Age, year mean: 71Men/women: 95/56
Inclusion Criteria:● treated for acute stroke
in a stroke unit● ≤ 3 months after stroke
onset● dependent in at● least two ADL domains
according to KatzExtended
● ADL Index● not diagnosed with
dementia,● able to understand and
follow instructions● referred for
rehabilitation to one ofthe 16
● participating units.
performing an activity andthey evaluated the activitytogether. The OTs had a5-day CADL workshopprior.
CADL(n=120)Geriatric: n=68Medical rehab: n=21Home rehab: n=40
CADL Significant others:(n=87)
Control:The UADL control groupreceived a variety ofstrategies customary toADL intervention.
UADL (n=132)Geriatric: n=53Medical rehab: n=11Home rehab: n=87
UADL Significant others(n=93)
burden, life satisfaction,and informal care.
of the SIS, which wascalculated fromintention-to-treat due todrop-outs.
Egan, M., Anderson, S., &McTaggart, J. (2010)
https://doi.org/10.1310/tsr1703-183
Level III
One group, nonrandomized(pretest and posttest)
Intervention: A registeredoccupational therapistdelivered the CommunityStroke Navigation service.The goal of this service
Pre-test and post-testmeasures:2-minute walk test
Daily functioning subscale
The post-test resultsindicated smallimprovements incommunity reintegrationamong stroke survivors but
12Indiana University Occupational Therapy
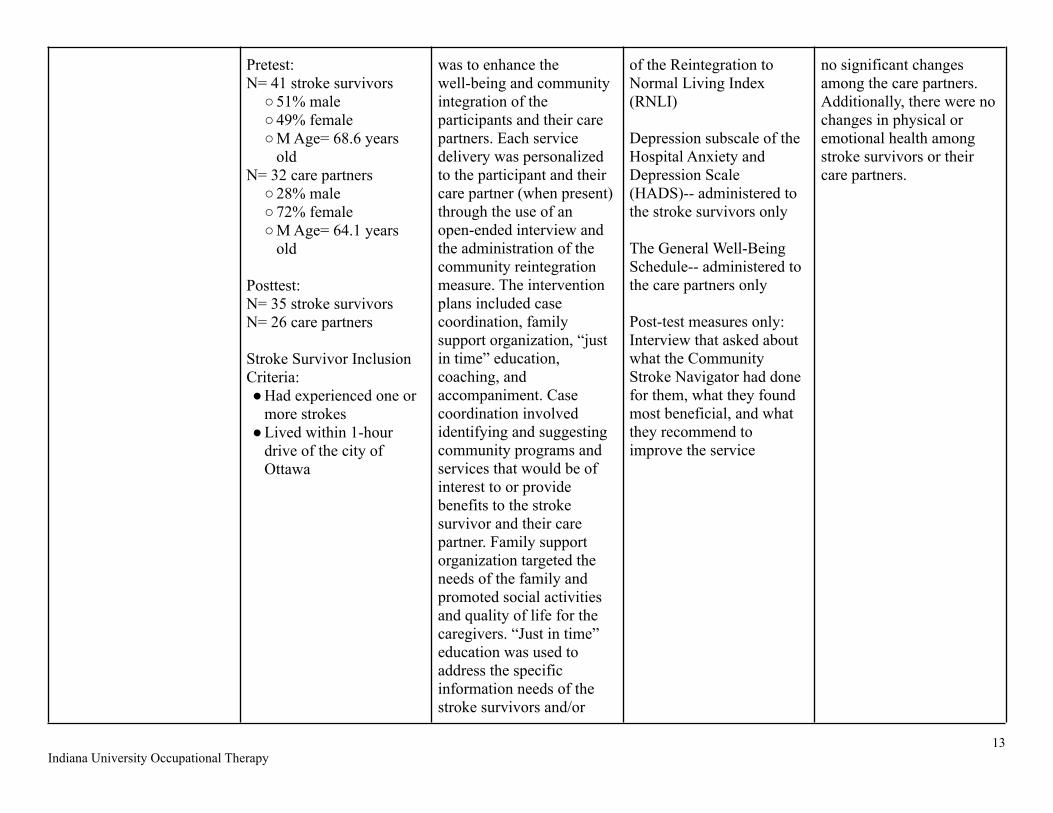
Pretest:N= 41 stroke survivors○51% male○49% female○M Age= 68.6 years
oldN= 32 care partners○28% male○72% female○M Age= 64.1 years
old
Posttest:N= 35 stroke survivorsN= 26 care partners
Stroke Survivor InclusionCriteria:●Had experienced one or
more strokes●Lived within 1-hour
drive of the city ofOttawa
was to enhance thewell-being and communityintegration of theparticipants and their carepartners. Each servicedelivery was personalizedto the participant and theircare partner (when present)through the use of anopen-ended interview andthe administration of thecommunity reintegrationmeasure. The interventionplans included casecoordination, familysupport organization, “justin time” education,coaching, andaccompaniment. Casecoordination involvedidentifying and suggestingcommunity programs andservices that would be ofinterest to or providebenefits to the strokesurvivor and their carepartner. Family supportorganization targeted theneeds of the family andpromoted social activitiesand quality of life for thecaregivers. “Just in time”education was used toaddress the specificinformation needs of thestroke survivors and/or
of the Reintegration toNormal Living Index(RNLI)
Depression subscale of theHospital Anxiety andDepression Scale(HADS)-- administered tothe stroke survivors only
The General Well-BeingSchedule-- administered tothe care partners only
Post-test measures only:Interview that asked aboutwhat the CommunityStroke Navigator had donefor them, what they foundmost beneficial, and whatthey recommend toimprove the service
no significant changesamong the care partners.Additionally, there were nochanges in physical oremotional health amongstroke survivors or theircare partners.
13Indiana University Occupational Therapy

care partners. Coachingwas utilized to coach strokesurvivors and care partnerson successful transitions byengaging their serviceproviders in conversationsfocused on theirinformation needs.Through accompaniment,stroke survivors wereaccompanied to newgroups/events by a trustedindividual who understoodtheir challenges and couldassist them whennecessary. Serviceprovision occurred for 4months, and strokesurvivors and their carepartners were visitedanywhere between 1-8times by the CommunityStroke Navigator duringthis period. TheCommunity StrokeNavigator also aided theparticipants and carepartners through writtencorrespondence, phonecalls, and visits tocommunity agencies.
Hayner, K., Gibson, G., &Giles, G. M. (2010).
https://doi.org/10.5014/ajot
Level 1
Two-group randomizedcomparison design study ,
Both groups had 6 hours ofOT for 10 consecutive daysplus varying amounts ofat-home therapy.
Wolf Motor Function Testand Canadian OccupationalPerformance Measure wereused to measure upper
The results indicated thatsignificant improvementswere found in WMFT andCOPM scores across time
14Indiana University Occupational Therapy
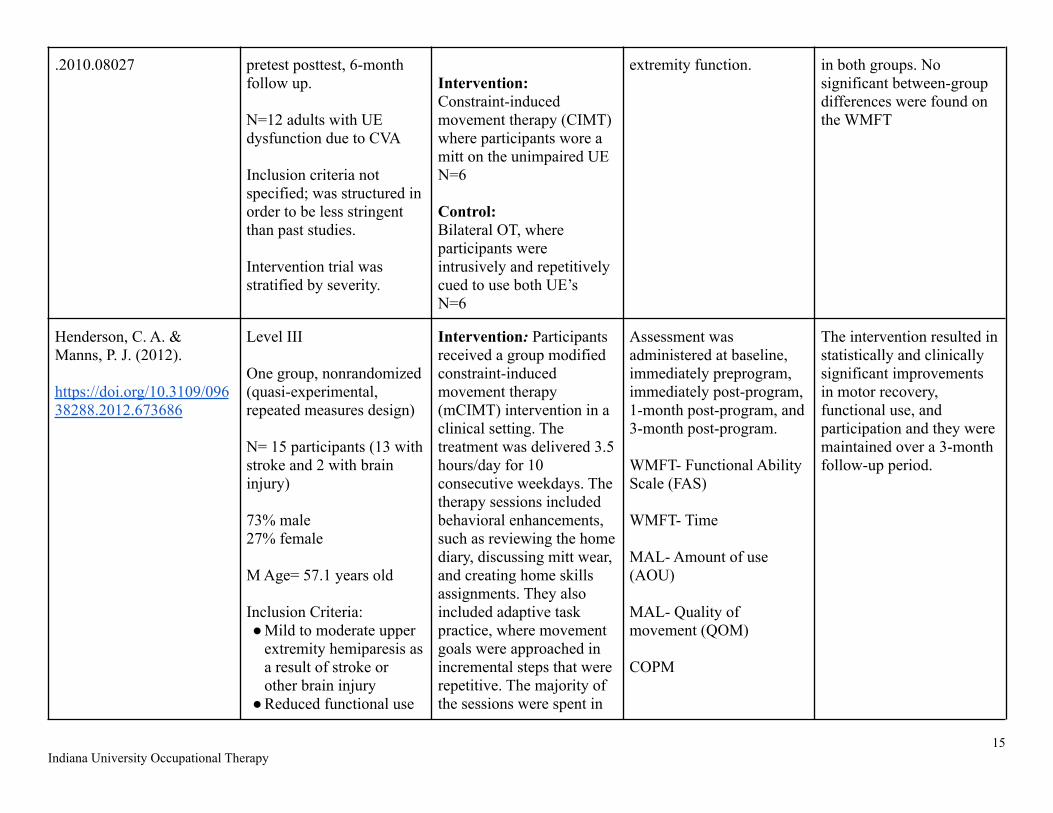
.2010.08027 pretest posttest, 6-monthfollow up.
N=12 adults with UEdysfunction due to CVA
Inclusion criteria notspecified; was structured inorder to be less stringentthan past studies.
Intervention trial wasstratified by severity.
Intervention:Constraint-inducedmovement therapy (CIMT)where participants wore amitt on the unimpaired UEN=6
Control:Bilateral OT, whereparticipants wereintrusively and repetitivelycued to use both UE’sN=6
extremity function. in both groups. Nosignificant between-groupdifferences were found onthe WMFT
Henderson, C. A. &Manns, P. J. (2012).
https://doi.org/10.3109/09638288.2012.673686
Level III
One group, nonrandomized(quasi-experimental,repeated measures design)
N= 15 participants (13 withstroke and 2 with braininjury)
73% male27% female
M Age= 57.1 years old
Inclusion Criteria:●Mild to moderate upper
extremity hemiparesis asa result of stroke orother brain injury
●Reduced functional use
Intervention: Participantsreceived a group modifiedconstraint-inducedmovement therapy(mCIMT) intervention in aclinical setting. Thetreatment was delivered 3.5hours/day for 10consecutive weekdays. Thetherapy sessions includedbehavioral enhancements,such as reviewing the homediary, discussing mitt wear,and creating home skillsassignments. They alsoincluded adaptive taskpractice, where movementgoals were approached inincremental steps that wererepetitive. The majority ofthe sessions were spent in
Assessment wasadministered at baseline,immediately preprogram,immediately post-program,1-month post-program, and3-month post-program.
WMFT- Functional AbilityScale (FAS)
WMFT- Time
MAL- Amount of use(AOU)
MAL- Quality ofmovement (QOM)
COPM
The intervention resulted instatistically and clinicallysignificant improvementsin motor recovery,functional use, andparticipation and they weremaintained over a 3-monthfollow-up period.
15Indiana University Occupational Therapy
of upper extremityindicated by the MAL-amount of use score
●At least 6 months postinjury
●Able to participate in 3.5hours of therapy daily,with short rest breaks asneeded
●Adequatecommunication,perceptual, andcognitive skills toparticipate in self-ratescales
●Medically stable,including no significantjoint or upper extremitypain
● Independent withactivities of daily living(including toileting andmedicationadministration)
●Not receiving BotulinumToxin A for upperextremity spasticityduring treatment periodor follow-up period
group functional taskpractice, including bothindividualized taks andcollaborative activities. Apadded safety mitt wasworn on the less involvedupper extremity throughouttherapy and wasencouraged to be worn90% of waking hoursoutside of therapy.
Iwamoto, Y., Imura, T.,Suzukawa, T., Fukuyama,H., Ishii, T., Taki, S.,Imada, N., Shibukawa, M.,Inagawa, T., Araki, H., &Araki, O. (2019)
Level I
RCT
N= 12 acute stroke patientsdivided into two groups.
Intervention:Patients receivedcombination hybridassistive limb (HAL-SJ)and occupational therapy
Recovery grade,hemiplegia
Br-stage
Motricity Index
No significant differencesseen in motor functionseverity defined byrecovery grade ofhemiplegia, Br-stage,motricity index grip
16Indiana University Occupational Therapy

https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.03.006
Inclusion Criteria:● First time stroke
Brunnstrom recoverystage II to IV
● Study participant within2 weeks after strokeonset
Excluded:● The surface electrode
could not be attached toskin due to cutaneousdisease
● Not able to followinstructions
Control:conventional occupationaltherapy
Grip strength of affectedhandModified Ashworth Scaleof biceps
Sensory function.
ADLS.
Measured on days 14, 19,24, 29, and 34 after strokeonset.
strength, modifiedashworth scale, or sensoryfunction between groupson day 14 after stroke.ADL limitations were notsignificantly differentbetween groups,mini-mental stateexamination score was notas well.
Jang, Y. Y., Kim, T. H., &Lee, B. H. (2016)
https://doi.org/10.1097/md.0000000000008023
Level I
RCT
N=23 adults post-stroke
Inclusion Criteria:● Onset within 6 months
post-stroke● Diagnosed with shoulder
subluxation by X-rayfinding
● Scored more than 24points on theMini-Mental StateExamination (MMSE)
● Had unimpaired visualand somatosensoryfunction.
Intervention:Brain-ComputerInterface-ControlledFunctional ElectricalStimulation Training andconventional occupationaltherapy (BCI-FES)
Control:Functional ElectricalStimulation (FES)
Vertical and horizontaldistance of subluxation
Visual analogue scale
Modified Ashworth Scale
Manual Function Test
The results showedstatistically significantchanges in vertical distanceof subluxation (p<0.001),horizontal distance ofsubluxation (p=0.002),visual analogue scale(p=0.009) and manualfunction test (p<0.001) forthe BCI-FES group andsignificant changes invertical distance ofsubluxation (p=0.034),visual analogue scale(p=0.003), and manualfunction test (p=0.007) forthe FES group
17Indiana University Occupational Therapy
Lee, M. J., Lee, J. H., &Lee, S. M. (2018).
https://doi.org/10.3233/thc-181336
Level I
RCT
N= 30 adults post stroke
63% male, 37% female
M age = 52 yrs
Intervention group, n= 15
Control group, n=15
Inclusion Criteria:● Patients were
diagnosed withstroke-inducedhemiplegia occurring atleast 6 months beforeenrollment
● Patients were capableof communicating ontheir own with a scoreof > 21 points on theKorean version of theMini-Mental StateExamination(MMSE-K)
● Patients had a muscletone of grade 2 orbelow on the ModifiedAshworth Scale in thehemiplegic upperextremity
● Patients had a
Intervention: Receivedgeneral occupationaltherapy consisting of five30-min sessions per weekfor 8 weeks. Theexperimental groupreceived an additional 30min of robot-assistedtherapy using theREJOYCE robot treatment.
Control:Received generaloccupational therapyconsisting of five 30-minsessions per week for 8weeks. The control groupreceived an additional 30min of generaloccupational therapy.General occupationaltherapy comprisedstretching exercises topromote flexibility. NDT topromote postural reaction,resistance exercise toimprove strength, and finemotor training.
The Fugl-MeyerAssessment (FMA)quantitatively assesses theupper limb’s motorfunction in hemiplegicpatients.
The modified BarthelIndex (MBI) examines thelevel of independence inADL.
There was no significantdifference between theexperimental and controlgroups with respect to pre-treatment FMA and MBIscores (p > 0.05). Both theexperimental and controlgroups showed astatistically significantincrease in post-treatmentFMA and MBI scores ascompared to thepre-treatment scores (p <0.05). Intergroupcomparisons showed astatistically significantincrease in scores for allassessments in theexperimental group ascompared to those for thecontrol group. Theexperimental group showeda significantly greaterimprovement inupper-extremity functionthan did the control group.The distal part of the handshowed improvement infunction based on FMAscores with respect to theability to grip paper, pen,cans, and balls.
18Indiana University Occupational Therapy

minimally functionalupper limb(Fugl-Meyer Score >35).
Lee, S., Kim, Y., & Lee,B.-H. (2016).
https://doi.org/10.1002/oti.1437
Level I
RCT
N= 18 adults post stroke
44% male, 56% female
M age =69 years
Intervention group, n= 10
Control group, n=8
Inclusion criteria:● Diagnosis of stroke at
least 6 months prior● Mini Mental State
Examination (MMSE)score of 24-30,
● Brunnstrom recoverystages 1-4
● Modified AshworthScale (MAS) score of anupper extremity of lessthan 2
Intervention:Subjects in the VRBTgroup performed bilateralupper extremity training ina VR environment for 30minutes per session, 3 daysa week, for 6 weeks.Conventional occupationaltherapy for 30 minutespersession, 5 days a week,for 6 weeks was alsocompleted.
The animation consisted offour training programmes,including symmetric upperextremity training,asymmetric upperextremity training, sym-metric upper extremitytraining at 0° and 45° in theVR environment, andasymmetric upperextremity training at 0° and45° in the VR environment.Each movement wasperformed for 4minutes,followed by 1 minute ofrest designed to minimizefatigue. During training,the subject grasped the
Upper extremity functionwas measured using:
Jebsen–Taylor HandFunction Test (JHFT)
Box and Block test (BBT)
Grooved Pegboard Test(GPT).
Compared with the BTgroup, the VRBT groupexhibited significantimprovements in upper ex-tremity function andmuscle strength (p < 0.05)after the 6-week trainingprogramme. The Box andBlock test results revealedthat upper extremityfunction and elbow flexionin hand strength weresignificantly improved interms of group, time andinteraction effect of groupby time. Furthermore, theVRBT group demonstratedsignif- icant improvementsin upper extremityfunction, as measured bythe Jebsen Hand FunctionTest and Grooved Pegboardtest, and in the handstrength test, as measuredby elbow extension, grip,palmar pinch, lateral pinchand tip pinch, in both timeand the interaction effect ofgroup by time.
19Indiana University Occupational Therapy

handles or the affectedhand was strapped to ahandle, depending on thesever- ity of the deficitsControl: Subjects in the BTgroup watched anirrelevant video in a VRenvironment with bilateralupper extremity trainingfor 30 minutes per session,3 days a week, for 6 weeks.Conventional occupationaltherapy for 30 minutes persession, 5 days a week, for6 weeks was alsocompleted.
Control:
The BT group underwentthe same four upper ex-tremity trainingprogrammes as did theVRBT group, whichconsisted of symmetricupper extremity training,asymmetric upperextremity training,symmetric upper extremitytraining at 0° and 45° in aVR environment andasymmetric upperextremity training at 0° and45° in a VR environment,while watching anirrelevant nature
20Indiana University Occupational Therapy
documentary
Lin, K.-C., Chen, Y.-A.,Chen, C.-L., Wu, C.-Y., &Chang, Y.-F. (2010).
https://doi.org/10.1177/1545968309345268
Level I
RCT
N= 33 stroke patients
Intervention group, n=16●62.5% male●37.5% female
Control group, n=17●52.9% male●47.1% female
M Age= 53.85 years old
Inclusion Criteria:●Clinical diagnosis of a
first or recurrentunilateral stroke
●Ability to reachBrunnstrom stage III orabove in the proximaland distal part of thearm
●No serious cognitivedeficits indicated by theMini-Mental StateExamination
●No excessive spasticityin the affected arm,including shoulder,elbow, wrist, and fingers
Intervention:The intervention groupreceived bilateral armtraining 2 hours/day, 5days/week for 3 weeks.Participants practiced avariety of functional tasksthat incorporated thesimultaneous movement ofthe affected and unaffectedupper extremities. Allactivities incorporatedsimultaneous movement ofboth hands such as lifting 2cups, folding 2 towels, ormanipulating 2 coinssimultaneously.
Control:The control group receivedstandard occupationaltherapy focused on upperextremity training 2hours/day, 5 days/week for3 weeks. The therapyincludedneurodevelopmentaltechniques, weight bearingby the affected arm, finemotor tasks, trunk-armcontrol, and compensatorystrategy practice for dailyactivities.
Outcome measures wereadministered within 7 daysbefore and after the 3-weekintervention
Kinematic analysis
Clinical assessment:
Upper extremity section ofthe FMA
FIM
MAL- amount of use(AOU)
MAL- quality ofmovement (QOM)
Compared to the controlgroup, the BAT groupshowed better temporal andspatial efficiency duringunilateral and bilateraltasks and less online errorcorrection only during thebilateral task. Additionally,the BAT group showedsignificantly greaterimprovement in the FMAthan the control, but nosignificant differences inthe FIM or MAL.
21Indiana University Occupational Therapy

that might preclude thefunctional movements;indicated by theModified AshworthScale
●No other neurologic,neuromuscular, ororthopedic disease
●Lack of participation inany experimentalrehabilitation or drugstudies
Exclusion Criteria:● Individuals who had a
stroke relapse or seizureattack during theintervention
Linder, S. M., Rosenfeldt,A. B., Bay, R. C., Sahu, K.,Wolf, S. L., & Alberts, J. L.(2015)
http://dx.doi.org/10.5014/ajot.2015.014498
Level I
RCT
N=99
Inclusion Criteria:
● Unilateral ischemic orhemorrhagic strokewithin the previous 6months
● 11–55 on theFugl-MeyerAssessment
● Limited access(logistical, financial,
Intervention:Home-based robot assistedrehabilitation (HandMentor Pro RoboticDevice) paired with a homeexercise program (HEP)
Control:Home exercise program(HEP)
Stroke Impact Scale (SIS)questionnaire assessedphysical strength, memory,feelings and emotions ormood, communication,ADLs and IADLs,mobility, hand function andmeaningful activities
Center for EpidemiologicStudies Depression Scale(CES-D) assesseddepressivesymptomatology afterstroke
This study comparedbaseline scores for the SISand CES-D to the end oftreatment (EOT) scores fora home-basedrobot-assistancerehabilitation programcoupled with a homeexercise program and ahome exercise programalone. Each groupimproved significantly inCES scores and SIS scoresexcept for mood andmemory.
22Indiana University Occupational Therapy

and geographicalbarriers) to other meansof organized strokerehabilitation programs
● Preserved cognitivefunction.
● All participants wererecruited fromCleveland, OH orAtlanta, GA.
Exclusion Criteria:● Individuals who lacked
independence prior totheir stroke
● Received anantispasticity injectionin the hemipareticupper limb since theonset of the stroke.
McEwen, S., Polatajko, H.,Baum, C., Rios, J., Cirone,D., Doherty, M., & Wolf, T.(2015).
https://doi.org/10.1177/1545968314558602
Level 1
RCT
N=26 adults 3 monthspost-stroke or less
Inclusion Criteria:● Patients who had
sustained an ischemicstroke (ICD-10 codesI63 and I64)
● Within 3 months or lesswhen starting outpatient
Intervention:CO-OPThe goal-plan-do-checkmethod was used as themain problem-solvingframework to facilitateactivity acquisition. 3 goalswere made to achieve andif they were not, the planwould be modified and theparticipant would breakdown the performance.This process would repeatuntil the goal was achieved
The primary outcome wasperformance of untrainedand trained self-selectedactivities, measured byPerformance QualityRating Scale (PQRS).
Other outcomes weremeasured by the CanadianOccupational PerformanceMeasure (COPM)
The Stroke Impact Scale
The results indicate thatthere was a large treatmenteffect on follow-upperformance onself-selected activities anddemonstrated transfer tountrained activities.CO-OP will most likelyhelp patients locally, but itis difficult to tell as therewas a small sample sizeand it cannot begeneralized withconfidence yet.
23Indiana University Occupational Therapy

rehabilitation were● Referred to outpatient
rehabilitation atSunnybrook–St John’sRehab in Toronto, ON,Canada, or TheRehabilitation Instituteof St Louis, MO
● Between March 2011and March 2013
Exclusion criteria:● Hemorrhagic stroke● Other neurological
diagnoses● Major psychiatric illness● Moderate or severe
aphasia (combinedscores of 6 or less onCanadian Institute ofHealth Information
and participant is satisfiedwith their performance onthe task at hand. Therapistswere trained in a 2-dayworkshop.
Control:Usual Care. A combinationof functional, task-basedtraining andcomponent-based training,as deemed necessary by thetreating therapists.
Participation Domain
Community ParticipationIndex
Self-Efficacy Gauge
compare the effect oflong-term activityperformance andparticipation when utilizingCognitive Orientation todaily OccupationalPerformance (CO-OP) incomparison to usualoccupational therapy
Mödden, C., Behrens, M.,Damke, I., Eilers, N.,Kastrup, A., &Hildebrandt, H. (2012).
https://doi.org/10.1177/1545968311425927
Level 1
Three-group RCT
N=45 stroke participantswith a visual field defectadmitted for inpatientrehabilitation
In addition to theinterventions, allparticipants also receivedstandard rehabilitationtreatment for inpatientrehab setting regardingphysiotherapy, speechtherapy, and healtheducation. Allinterventions werecompleted in the samelocation.Intervention:Restitution Training (RT)
Outcomes measuredinclude the primaryoutcome measures werevisual field expansion forRT, visual searchperformance for CT, andreading performance forboth treatments.Visual conjunction search,alertness, and the BarthelIndex were secondaryoutcomes. The TestingBattery for AttentionPerformance, Visual Field
Results indicate thatcompared with OT, CTresulted in a better visualsearch performance, andRT did not result in a largerexpansion of the visualfield. Intra-group pre–postcomparisons demonstratedthat CT improved alldefined outcomeparameters and RT several,whereas OT only improvedone.
24Indiana University Occupational Therapy

N=15Male/Female: 10/5A series of targets basedoff of exact measurementof visual field border werepresented on a screen andthe participants had torespond to each stimulustarget as soon as it wasperceived by pressing akey. Eye movements werenot allowed and controlledby an assistant.
Intervention:Compensatory Training(CT)N=15Male/Female: 9/6Participants followedbright stimuli on darkbackground and identifiedtargets by eye movementclustered in blind side. Theprogram had severaldifficulties.
Control:OTN=15Male/Female: 7/8After a standardizedassessment ofdaily living activities, thetherapy consisted of
Assessment, BehavioralInattention Test,andExtended Barthel Indexwere used.
25Indiana University Occupational Therapy

individuallyadapted stimulation ofdaily activity tasks tocompensatevia eye-, head-, and bodymovements. Thesecompensationstrategies included aspectsof spatial and bodyperception,searching or arrangingobjects, pen and papersearchingtask, reading maps ornewspapers, and self-careactivities.The participant wasinstructed to performsystematic eyemovements toward the lostvisual field.
Msengana, Z., De Witt, P.,Owen, A., & Franzsen, D.(2019)
http://dx.doi.org/10.17159/2310-3833/2019/vol49n3a3
Level II
Cohort Study
N=45
Inclusion Criteria:● Medically stable adults● Between the ages of 18
Conventional occupationaltherapy
The Fugl-Meyerassessment
The South African DataFunctional Medicine(SADFM) Beta Scale
The results showedsignificant improvementsin all aspects of upper limbfunction including personalmanagement, self-care,toileting, and mobility, atall four assessmentintervals.
26Indiana University Occupational Therapy

and 75 years old
Mortensen, Figlewski,Andersen (2016)
https://doi.org/10.3109/09638288.2015.1055379
Level I
Double-blind RCT
Stratified randomizationapproach was used
Inclusion Criteria:● 18-80 years old● >6 months and <5
years from theinitial ICH.
Exclusion Criteria:● Traumatic ICH● Epilepsy, metal
implants in the head● Other neurological
diseases● Cognitive
disabilities● Residence >100hm
away fromrehabilitationhospital.
Randomized to receive 5consecutive days ofoccupational therapy
Intervention:Combined with eitheranoda tDCS.
Control:Combined with shamtDCS.
Ability to complete theJebsen-taylor Test (activityand function)
Stroke Impact Scale.
Grip strength
Tendency for greaterimprovement in ADLperformance in the anodalgroup compared with thesham group; statisticallysignificant improvement ingrip strength in the anodalgroup compared with thesham; both groupsimproved in logJTT overtime.
Orihuela-Espina, F.,Roldán, G. F.,Sánchez-Villavicencio, I.,Palafox, L., Leder, R.,Sucar, L. E., &Hernández-Franco, J.(2016).
Level I
RCT
N= 17 adults post stroke
65% male, 35% female
Intervention:Attended therapy 5 times aweek until they completed40 sessions of treatment.The first 4 sessions wereshorter and lastedapproximately 40 minutes.Therapy sessions lasted 1
Sensorimotor recovery ofpatients was evaluated withthe Fugl-Meyer assessment(FMA) scale
The Motricity Index (MI)scale was used to assess themotor recovery rate of the
Statistically significantimprovement inperformance was found forthe FMA for roboticintervention control handFMA (WSR: p-value 1⁄40.097); for the roboticintervention group hand
27Indiana University Occupational Therapy

https://doi.org/10.1016/j.jht.2015.11.006
M age =55 years
Intervention group, n=9
Control group, n=8
Inclusion criteria:● Adult patients >30 with
a diagnosis ofhemorrhagic or ischemicstroke
● Experience severe upperextremity hemiparesis(estimated by theFugl-Meyer scale >8and <30)
hour with rest periods. Theintervention group wasadministered roboticassisted therapy involvedtwo stages; first passiveactivities (300 repetitions),followed with partialassistance or resistance(300 repetitions) whichprovides a variablechallenge for the patients.From the fourth ses- siononwards active movementswere included (100repetitions) for a total of700 repetitions per session.
Control:Received classicaloccupational therapy. Theywere treated with massageand conventionaloccupational exercises. Ineach session the patientsunderwent a stretchingstage involving passivemove- ments (300repetitions), a warming upstage with strengtheningexercises, and a finaltraining active stageensemble to promotepalmar grasps, andpersonalized activities withmarbles and screw for finepinching (lateral and pulp)
patients FMA (WSR: p < 0.001).However, the MI did notexhibit the same statisticaldifference. For control:prehension MI (WSR: p 1⁄40.097). For intervention:prehension MI (WSR: p 1⁄40.009). Differences for thehand, were as follows:Fugl- Meyer improvementsin the motor dexterity forthe hand ach- ieved withthe intervention therapywas significantly greaterthan improvement obtainedwith the control therapy,but the Motricity Index,despite the bigger effectsize induced by theintervention therapy, didnot show such significantdifference for prehension
28Indiana University Occupational Therapy

control.
Pandian, S., Arya, K. N., &Davidson, E. W. R. (2011).
https://doi.org/10.1016/j.jbmt.2011.11.002
Level I
RCT
N= 30 chronic strokepatients
Brunnstrom handmanipulation group, n= 15● M Age= 47.4 years old● 66.7% male● 33.3% female
Motor relearning programgroup, n=15●M Age= 51.67 years old●93.3% male●6.7% female
Inclusion Criteria:●Post-stroke patients●Between the age of
35-60● In stage 3 of Brunnstrom
recovery stage of thehand
● Intact cognition andperception
Exclusion Criteria:● Individuals with
cerebellar lesions● Individuals with painful
or subluxed shoulders
Intervention: Participantsreceived Brunnstrom handmanipulation (BHM) alongwith standard occupationaltherapy for upper andlower extremities(excluding the hand).BHM was focused onattaining mass grasp andrelease with the use ofreflexive, passive,synergistic and activemovements.
ComparisonIntervention: Participantsin this group received amotor relearning program(MRP) for their hand alongwith standard occupationaltherapy for upper andlower extremities(excluding the hand).Instruction was provided ina variety of ways includingverbally, visualdemonstration, manualguidance, feedback, andpractice of the task.Upper-extremity functionalskills were learned throughthe analysis of the taks,practice of the missingcomponent of the task and
Outcome measures wereadministered pre-test andpost-test
Brunnstrom recoverystages of hand (BRS-H)
Fugl-Meyer assessment--wrist and hand (FMA-WH)
BHM and MRP were botheffective in enhancing themotor recovery of thehand. However, there werestatistically significantresults in motor recovery ofthe hand in favor ofBrunnstrom movementtherapy indicating thatBHM is better than MRPfor the wrist and handrecovery, especially massfinger flexion, extension,and grasp.
29Indiana University Occupational Therapy

● Individuals with anycontracture or deformityof the upper extremity
● Individuals with nositting balance
practice of the entire task.
Sackley, Walker,Burton…;2014doi:10.1136/bmj.h468
Level I
RCT
N= 1042 care homeresidents with history ofstroke or transient ischemicattack, including those withlanguage and cognitiveimpairments, not receivingend of life care;randomized between May2010 and March 2012.
Intervention:Targeted three-monthprogram of OT, deliveredby OTs and assistants,involving patient centeredgoal setting, education ofcare home staff, andadaptations to theenvironment
Scores on the Barthel indexof ADLs at three monthspost randomization;
Barthel Index scores at 6and 12 monthspost-randomization
Rivermead Mobility Index
Geriatric Depression
Primary outcome did notdiffer significantly betweenthe treatment arms.Adjusted mean differencein Barthel index score atthree months was .19points higher in theintervention arm.Secondary outcomesshowed no significantdifferences at all timepoints.
Sale, P., Mazzoleni, S.,Lombardi, V., Galafate, D.,Massimiani, P., Posteraro,F., Franceschini, M. (2014)
doi:10.1097/MRR.0000000000000059
Level I
RCT
N=20
Inclusion Criteria:● First acute event of
cerebrovascular stroke● Unilateral paresis● Ability to understand
and follow simpleinstructions
● Ability to remain in asitting posture
● Mini Mental State
Intervention:Robot-assisted therapy
Control:Intensive Occupationaltherapy
Fugl-Meyer Scale
Medical Research CouncilScale for Muscle Strength
Motricity Index
Modified Ashworth Scale
Box and Block Test
Barthel Index
A Friedman test showed asignificant improvement inthe experimental group forthe Fugl-Meyer Scale(P=0.0039), the Box andBlock Test (P=0.0185),Motricity Index(P<0.0001), MedicalResearch Council Scale forMuscle Strength(P<0.0001), and ModifiedAshworth Scale(P=0.0025). The Friedmantest also showedstatistically improvementsin the control group for the
30Indiana University Occupational Therapy

examination score morethan 20
● Muscle strength in thefinger flexion andextension more that 2(movement withoutgravity) evaluated withMedical ResearchCouncil
● Absence of sensoryimpairment evaluatedusing a neurological test.
Fugl-Meyer Scale(P<0.0001), Box and BlockTest (P=0.0086), MotricityIndex (P-0.0303), andMedical Research CouncilScale for Muscle Strength(P=0.001).
Song, C. S., Lee, O. N., &Woo, H. S. (2019).
https://doi.org/10.3233/RNN-180853
Level I
N= 49 participants withchronic hemiparetic stroke.The pre-test wasadministered 1 day beforetraining and the post-testwas administered one dayafter the training.
Inclusion Criteria:● Patients were diagnosed
with the first onset ofunilateral hemisphericstroke due to anischemic or hemorrhagicattack 6 months prior tothe study
● Patients had sufficientcognitive ability to
Both groups underwentsessions 5 days a week, 30minutes a day, for 4 weeks.
Intervention:Cognitive Orientation toDaily OccupationalPerformance (CO-OP)N=25Male/Female: 16/9
There were two stages;cognitive strategy ofgoal-plan-do-check andmotor-based tasks in therepetitive action. Theparticipants, an OT, andpsychologist workedtogether to recognizeproblems and performancein self-selected activities.
Before and after training:
Box-and-block test (BBT)
Canadian occupationalperformance measure(COPM)
Community IntegrationQuestionnaire (CIQ)
Wolf motor functiontest-functional score(WMFT-F)
The results showedsignificant improvement inthe WMFT-F, COPM-P,COPM-S, BBT, and CIQscores after training in theCO-OP group, but onlyCOPM-S score wassignificantly improvedafter training in TUETgroup (p < 0.05). Thisstudy also found higherincreases in the meanWMFT-F, COPM-P,COPM-S and BBT scoresin the CO-OP group than inthe TUET group, but CIQscore did not have asignificantly higher
31Indiana University Occupational Therapy

understand and followsimple verbalinstructions, as indicatedby a mini-mental stateexamination score of 24or higher
● Patients were capable ofindependent walkingwithout any assistancefor a distance of at least10 meters
● Patients did not havevisuoperceptualimpairment
● Patients did not haveany orthopedicconditions that affect thetherapeutic effects
● Patients did not haveany other neurologicaldiseases other than thefirst stroke
Control:Task-Specific UpperExtremity Training(TUET)N=24Male/Female: 18/6
Goal-directed, repetitive,and self-selected activitiesrelated to upper extremitybased on the examinationof motor function andCOPM score. The OT andparticipant modified taskdemands based onlimitations and the patientreceived repetitive selectedtarget tasks, 10 repetitionswith a 1-minuterest period per task. Thepatient took a 3 minutebreakafter performing a task inorder to prevent fatigue.After completing 1 task,the patient moved to thenexttask on the self-selectedtarget task list.
increase between-groupafter training.
The results of the studysuggest that the CO-OPapproach resulted in apositive therapeutic effecton self-selectedoccupational performanceand daily and functionalactivities in individualswith chronic hemipareticstroke.
Winstein, C. J., Wolf, S. L.,Dromerick, A. W., Lane, C.
Level I
Single-blind RCT
Randomized into 1 of 3treatment groups.
Outcomes were clearlyspecified and included:body functions and
Among participants withmotor stroke and primarilymoderate upper extremity
32Indiana University Occupational Therapy

J., Nelsen, M. A.,Lewthwaite, R., … Azen,S. P. (2016).
https://doi.org/10.1001/jama.2016.0276
N= 361 participants
Inclusion Criteria:● Older than 21● Ischemic or hemorrhagic
stroke meeting Worldhealth Organizationcriteria
● Upper extremityhemiparesis
● Voluntary fingerextension
● No more than 6outpatient occupationaltherapy sessions
● Absence of traumatic ornonvascular brain injuryand subarachnoid orprimary intraventricularhemorrhage.
Intervention:Intervention was completedwithin 16 weeks ofrandomization. AcceleratedSkill Acquisition Program,monitoring only
Control:Customary care UCC, anddose-equivalent usual andcustomary practice(DEUCC). Task-orientedapproach.
structures, activities,patient-centeredness,participation, andhealth-related quality oflife.
impairment, use oftask-oriented program, didnot significantly improvemotor function. Findingsdo not support superiorityof the ASAP amongpatients with motor strokeand primarily moderateupper extremityimpairment
Wolf, T. J., Polatajko, H.,Baum, C., Rios, J., Cirone,D., Doherty, M., &McEwen, S. (2016).
https://doi.org/10.5014/ajot.2016.017293
Level I
RCT
N= 35 adults post stroke
63% male, 37% female
M age =57 years
Intervention group, n=19
Control group, n=16
Intervention:The participant used theproblem-solving strategyGoal–Plan– Do–Check toaddress and master eachgoal activity.
Control:Usual-care strokerehabilitation consisted of acombination of functional,task-based training, such aspracticing dressing, and
Delis-Kaplan ExecutiveFunction System(D-KEFS): cognitivefunction (executive)
Action Research Arm Test(ARAT): upper extremityfunction
Stroke Impact Scale (SIS):Health status
Canadian OccupationalPerformance Measure
At Time 2, CO–OP had alarge effect over usual carefor SIS Re- covery (d =0.8) and a medium effectover usual care for changesin the SIS Physicalsummary score (strength,hand function, mobility,and ADL/IADL scores),SIS Hand Function, and theD–KEFS Trail Makingsubtest (d = 0.5).
Data support a positive33
Indiana University Occupational Therapy
Inclusion Criteria:● Patients with ischemic
stroke● Referred for OP therapy
at either Sunnybrook-St. John’s Rehab or theRehabilitation Institute
component-based training,such as grasping objects,chosen by each individualtherapist to meet individualpatient needs.
(COPM): Self-reportedoccupational performance:trained and untrained goals
Performance QualityRating Scale (PQRS):Objective rating ofperformance of COPMgoals.
effect of CO–OP overusual occupational therapyon upper-extremityfunction, cognitiveflexibility, and perceivedbody functions, areas notdirectly targeted duringtreatment.
Xu, Quan, Li, Chong, Pan,Yu, Li, Wei, Jia, Tianyu;2020
DOI:10.3233/NRE-203130
Level I
RCT
N=45 stroke patientshospitalized from January2018 to June 2019 wererandomly divided
Inclusion Criteria:● Patients with the first
onset of cerebralinfarction or cerebralhemorrhagePatients withBrunnstrom stage withinstage II–V
● Patients with the courseof disease within one tosix months
● Patients aged between18 and 75 years
● Patients who cancoordinate therehabilitation treatment
Intervention:Received upper limb robotassistance on the basis oftraditional training, 20min/time, once/day, andfive days/week.
Control:Trained with traditionalexercises, 40 min/time,once/day, and fivedays/week. WMFT
WMFT assessment
Daily Life AbilityAssessment
Fugl-Meyer Assessment
No statistical significancein the Fugl-Meyer score,Wolf motor function test,modified Barthel indexscore between the twogroups before treatment.After treatment, the FMscore, WMFT score, andMBI score weresignificantly higher thanbefore treatment. Nosignificant significancebetween two groups aftertreatment.
34Indiana University Occupational Therapy

Patients who signed theinformed consent form.
35Indiana University Occupational Therapy


















