Rapid Phenotypic Antimicrobial Susceptibility...
45
Rapid Phenotypic Antimicrobial Susceptibility Testing Gunnar Kahlmeter Martin Sundquist, Emma Jonasson, EUROSTAR-gänget
Transcript of Rapid Phenotypic Antimicrobial Susceptibility...

Rapid Phenotypic Antimicrobial Susceptibility Testing
Gunnar Kahlmeter
Martin Sundquist, Emma Jonasson, EUROSTAR-gänget

Rapid phenotypic AST
• Direct susceptibility testing
– AST directly on sample (mostly Urine)
– AST directly from the blood culture bottle
Cuts 24 hours off the standard procedure
• Potential problems:
– Inoculum??
– Purity of culture??

Rapid phenotypic AST
• “Early Reading” susceptibility testing
– Reading disk diffusion, or gradient tests, or automated testing earlier than stipulated in the standard method.
Cuts 24 hours off the standard procedure
• Potential problems:
– Some resistance mechanisms may not have time to express themselves phenotypically in 6, 7 or 8 hours
– Not standardised, but could be standardised by EUCAST

Why rapid ID and rapid AST? To increase the chance of patient survival, save time and
limit costs.
• Species ID determines the course of treatment, not only choice of antibiotic, but of many non-antimicrobial decisions.
• Empiric antimicrobial therapy will fail more often as resistance increases.
• To improve antibiotic stewardship – fewer cocktails, fewer ”to be on the safe side”, fewer ”trials-and-errors”
• Saves time
• Saves cost (Garcia-Vazquez SJID 2013)
• Because now we can!

• Every hour is important in the treatment of sepsis (septic shock) (Kumar CCM 2006)
• Inappropriate AB therapy 2 days longer hospital stay (Shorr CCM 2011)
• More Rapid Species ID and AST improves AB-therapy (Kerremans JAC 2008)

The lives saving diagnostic chain in blood stream infections
• The 24/7 rapid transportation (2 h) of blood culture bottles from patient to cupboard (incubation).
• The 24/7 access to cupboards for incubation and growth detection.
• Laboratory staff action on positive signals.
• Rapid ID – direct MT on bottles within 60 minutes of positive signal.
• Direct inoculation of AST from blood culture bottles.
• Early reading of AST – 6 to 8 hours of positive signal.
• Immediate alert and transfer of result.

The lives saving diagnostic chain in blood stream infections
• The 24/7 rapid transportation (2 h) of blood culture bottles from patient to cupboard (incubation).
• The 24/7 access to cupboards for incubation and growth detection.
• Laboratory staff action on positive signals.
• Rapid ID – direct MT on bottles within 60 minutes of positive signal.
• Direct inoculation of AST from blood culture bottles.
• Early reading of AST – 6 to 8 hours of positive signal.
• Immediate alert and transfer of result.

No EUCAST recommendation on direct AST
• EUCAST does not recommend: – Direct inoculation of AST from blood culture bottles.
– Early reading of AST – 6 to 8 hours of positive signal.
Since the inoculum is not standardised and the standard method is validated for 16 – 20 h incubation.
Urine - cultures are mixed and the pH variability may affect antimicrobial activity.

EUCAST
…considers…
•validating ”direct inoculation from blood culture bottles” and ”early reading” of disk diffusion.
…will not consider…
•validating ”direct inoculation from urines”

Direct AST of urines Each laboratory needs to
• Validate - confirm with standard methods
• Restrict to certain agent/species combinations • E.coli, Klebsiella pneumoniae
• Primary UTI agents (Piv-MEC, NIT, CDR, TRI, CIP)
• Define when to repeat/confirm result.
• Only report if pure culture and acceptable inoculum.

Direct AST from blood culture bottles
• 22/26 Swedish labora-tories perform Direct AST from positive blood cultures
• Early reading (after 6-8h incubation) is perfomed by 10 of 22
– Disk diffusion
– Vitek2
Åkerlund A Läkartidningen 2015

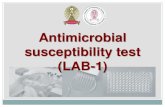
E.coli ATCC 25922 early reading
6h 18h

“Early reading – strategies”
1. Get it right – complete correlation - repeat testing not necessary.
2. Err on the side of caution – overcall resistance; use ECOFFs; repeat testing necessary
3. Identify “safe sensitive” – give the clinician a few safe alternatives; repeat testing necessary

EUROSTAR RAPID DISK
Metod
• EUCAST method with short incubation time
• 6h – E.coli
– K.pneumoniae
– Enterococci
• 8h – P.aeruginosa
– S.aureus
• 93% could be read after 6 or 8h
Lab
• Växjö – Manual reading
• Hvidovre – Manual reading
• AMC – Camera (Kiestra) with manual
adjustment. Reading every hour.

0
5
10
15
20
25
30
35
40
45
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
6 h
0
5
10
15
20
25
30
35
40
45
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
18 h
0
10
20
30
40
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
8h
E. coli vs. cefotaxime 5 μg
at 6, 8 and 18 h

E. coli vs. ciprofloxacin 5 μg
at 6, 8 and 18 h
0
5
10
15
20
25
30
35
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44
6 h
0
5
10
15
20
25
30
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44
18 h
0
5
10
15
20
25
30
6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44
8h

0
10
20
30
40
50
60
70
80
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
8h
0
10
20
30
40
50
60
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
18h
S. aureus vs. cefoxitin 30 μg

Disk diffusion – early reading
• After 6 – 8 hours
– Zone diameters for sensitive organisms are smaller than after 16-20 hours and
– Zone diameters for resistant organisms are bigger than after 16-20 hours
– The margin for errors shrink with 6-8h readings.

DIRECT AST DIRECTLY FROM URINE

DAST Urine
• Every day routine in many laboratories
• Increased usefulness with MALDI-TOF (direct?)
• Increased performance if pre-screening is performed?

DAST Urine
• ≥105 cfu/mL
• Singel species only
• 177 samples, 123 E.coli
• EUCAST CBP
• 855 tests
– 3 VME
– 5 ME
– 7mE
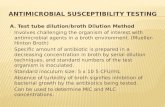
Sundqvist APMIS 2014
45
44 R I S
43
42 1
41
40 1
39 1 1 1
38 1 1 1 1
37 1 1 1
36 1 1 1 1 1 2
35 1 1 2 2
34 1 1 1 2 4 1 2 1 2 1
33 2 1 1 1 3
32 3 3 2 1 6 3 1 4 1
31 2 2 3 4 3 5 1 2 1 1 1
30 2 2 3 1 3 4 1 4 1
29 1 4 3 2 1 1
28 2 4 5 3 1 1 2
27 1 2 2 2 2 1 1
26 2 1 1 1
25 1 3 1
24 1 1 1 1
23 1 S
22 1
21
20 1 I
19 1
18 1 1
17 1 R
16
15
14
13
12
11 1 1
10 1 1
9
8
7
6 11
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45
Ciprofloxacin 5 µg
Inhibition zone diameter (mm). Standard AST
Inhib
itio
n z
one d
iam
ete
r (m
m).
DS
T-U
Ciprofloxacin

DAST urine, Routine Örebro University Hospital april 2013
• 470 prov
• 53% Neg
• Gram pos 9%
• 10% Mixed cultures
• DAST recorded on 25%
98 E.coli (87%)
• 2 ME (TRI och MEC)
• 2/2 ESBL were found
10 Proteus spp
• 1 mE
Other Enterobacteriaceae
• No errors
• Rapid Species ID important
Sundman 2013

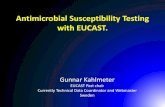
Antimicrobial Susceptibility Testing Directly from Urine
Samples – a Comparison between Standardised and
Direct Disk Diffusion Testing together with Direct
Species Identification using Matrix assisted laser
desorption/ionisation time of flight.
Jonas Olafsson
Klinisk mikrobiologi, Växjö
Linné-universitetet
Poster ECCMID 2014

44
43
42
41
40 1
39 1 1
38 1 1 1
37 1 1 1
36 1 1 2 1 1 2
35 1 1 2 2
34 1 1 1 2 4 1 2 1 2 1 1
33 2 1 1 1 3
32 3 3 2 1 5 3 1 4 1
31 1 2 3 4 3 5 1 2 1 1 1
30 2 2 2 3 4 1 4 1
29 1 4 3 2 1 1
28 2 3 5 3 1 1 2
27 1 2 2 2 2 1 1
26 2 1 1 1
25 1 2
24 1 1 1 1
23 1
22 1
21
20 1
19 1
18 1 1
17 1
16
15
14
13
12
11 1 1
10 1 1
9
8
7
6 10
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44
Inhibition zone diameter (mm)
EUCAST methodology
Inh
ibit
ion
zo
ne d
iam
ete
r (m
m)
D-A
ST
Ciprofloxacin 5 µg (n=188).

40
39
38
37
36
35
34
33 1
32
31 1 1 1 1
30 1 2 1 1 1 1
29 2 3 1 1
28 1 1 1 3 3 4 2 2
27 1 2 3 4 5 2 1 1 1
26 1 1 1 1 3 5 5 1
25 1 1 1 6 2 3 1
24 1 1 4 6 6 2 4 2
23 1 3 3 2
22 2 1 1 2 1 1
21 1 2 2
20 1 1 2 2
19 1
18
17 1 1 1
16 1
15 2 1
14
13
12
11 1
10 1
9 1
8
7
6 33
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Inhibition zone diameter (mm)
EUCAST methodology
Inh
ibit
ion
zo
ne
dia
met
er (
mm
)
D-A
ST
Trimethoprim 5 µg (n=188).
Errors for P. mirabilis are marked with black boxes.

40
39
38
37
36
35
34
33
32 1
31
30 1 1 2 1 1
29 4 2 2 4 1 2 1 1
28 1 1 1 3 3 1
27 1 1 5 6 3 2
26 1 1 4 7 6 4 1
25 2 2 2 3 7 2 1
24 2 2 1 3 3 2 2 1
23 1 2 1 1 2 2 1 3
22 1 2 3 2 1
21 2 1 2
20 2 1 2 1 1
19 2 2 1 2 1 1 1
18 1
17 1
16 2 1
15 1
14 1
13 1
12 1
11 1
10
9
8 1
7
6 5
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Inhibition zone diameter (mm)
EUCAST methodology
Inh
ibit
ion
zo
ne d
iam
ete
r (m
m)
D-A
ST
Mecillinam 10 µg
(E. coli, Klebsiella spp. and P. mirabilis, n=172).

40
39
38
37
36
35
34
33
32
31
30
29
28
27
26
25
24
23
22 2 1
21 1 3 4 1 3
20 1 4 13 2 7
19 8 7 16 5 2
18 1 1 4 7 15 8 4 3
17 2 8 5 3
16 2 1 3 6 3 1
15 1 3 1
14 1
13 1 1
12 1 1
11 1
10 1
9
8 1
7 1
6 16
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Inhibition zone diameter (mm)
EUCAST methodology
Inh
ibit
ion
zo
ne d
iam
ete
r (m
m)
D-A
ST
Cefadroxil 30 µg (n=188).

Direkt resistensbestämning på urinprover för andra gramnegativer än Escherichia coli och
Klebsiella pneumoniae
Nadia Vickius
Oskar Ekelund
Poster ECCMID 2015
Klinisk mikrobiologi för Kronoberg och Blekinge

Upplägg
Konsekutiva urinprover med signifikant bakteriuri med någon av följande arter: P. mirabilis (n=29)
Enterobacter spp. (n=17)
Citrobacter spp. (n=22)
K. oxytoca (n=29)
Serratia marcescens (n=3)
Totalt (n=100)
Studien utförs under perioden mars 2013 - augusti 2014 (18 månader). Provsättning och avläsning utförs av på urinavdelningen tjänstgörande BMA.

D-AST vs. EUCAST, endast P. mirabilis Mecillinam 10 µg
35 R S
34
33
32
31
30
29
28
27 1
26 1
25 1 1
24 1 1 1
23 1 1 1 3 2 1
22 1
DST-U 21 2 1
20 1 1
19 1
18
17 1 S
16 1
15
14
13
12 R
11
10
9
8
7
6 3 1
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
EUCAST
Felklassificeringar av P. mirabilis (3/29 = 10.3%)

D-AST vs. EUCAST, endast P. mirabilis
Trimetoprim 5 µg
35 R I S
34 1
33
32
31
30
29 1
28
27
26 1 1
25 1 1
24 1 1
23
22 1
DST-U 21 1
20 1 S
19 2
18 1 1
17 1
16 1 I
15 1
14
13
12 R
11
10
9
8
7
6 11
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
EUCAST
Felklassificering av P. mirabilis (5/29 = 17%)

D-AST vs. EUCAST, Gentamicin 10 µg
35 R I S
34
33
32
31
30
29
28
27 1
26 1 1
25 1 3 2 1
24 1 1 2 3 2 2 1
23 2 1 1 4 1 3 2
22 2 2 1 2 3 2
DST-U 21 1 3 2 4 4 2 1 1
20 1 1 1 4 4 3 1
19 2 2 2 1 1
18 1 2 1 2 1 S
17 1 1
16
15 1 I
14 1
13
12 R
11
10
9
8
7
6
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
EUCAST
Felklassificering av P. mirabilis
Felklassificering av K. oxytoca

Problems with DAST on Urine
• Errors probably not a major problem if restricted to E.coli and Klebsiella pneumoniae
– Other species need more validation
• High cost if performed on every sample
– Pre-screening ??
– On demand/request


IN PIPELINE

Resistance detection using MALDI-TOF
• Detection of resistant subtypes (i.e. subtyping)
– CfiA +/- B.fragilis (Wybo 2011, Johansson JMM 2014)
• Detection of specific peaks associated with resistance (i.e. subtypning)
– Porin loss in K.pneumonaie (Cai JCM 2012)
• Detection of degradation of antibitics (i.e. Beta-lactamase detection)
– TEM, ESBL, Carbapenemases (Sparbier JCM 2012)
– Carbapenemases (Hrabak 2011-2014)

Susceptibility testing using MALDI-TOF
• Detection of changes in mass-spektra in the presence of breakpoint concentrations of antibiotics (i.e. quantitative MALDI)
– Incubate in BHI-broth +/- antibiotics 1h
– Centrifugation steps and extraction with standard
– Load on MALDI-tray and cover with HCCA
– Analyse and compare AUC
– SIR can be predicted using Breakpoint concentrations
Lange JCM 2014

AST and MALDI (so far…)
Advantage
• Rapid
• Broth
• Not thorough validated (only one study)
• Might be useful for specific ”hard to test” bacteria
Drawback
• Laborious
• Not quantitative
• Not automated
• Breakpoint concentrations

Microcalorimetry
• Measurement of Isothermal Microcalorimetry
• Breakpoint concentrations, 6h
• Urine as medium
Braissant JCM 2014
E.coli resistant to ampicillin and
ciprofloxacin
Inhibition Index

Combined Broth Dilution and PCR (FAST)
• 5ml BC broth centrifuged
• Suspension in MH +/-ab
• Breakpoint concentrations
• Incubation 0-8h
• 16SrRNA qPCR
• Meltcurve species
• Good results
• 9h
• 50.7 vs 66.3h
Beuving PLoS One 2011.
EJCMID 2014

Combined Broth Dilution and using PadLock probes and RCA
• Short (0.5-2h) preincubation of urine in LB-broth +/- ab
• Breakpoint concentrations CIP and TRI
• Addition of species specific PadLock Probes
• RCA
• Differences in ”Growth curves” SIR
• Good correlation
Mezger JCM 2015

Schematic illustration of the method.
Anja Mezger et al. J. Clin. Microbiol. 2015;53:425-432

Future perspectives
• Molecular based detection from whole blood – Black box
– Random access
– Affordable
– If accomplished: preliminary report in 6-8h?
• Culture (usually positive within 20h)
– MALDI-TOF + rapid DD definitive report in <30h?

But, to be rapid we need ”Microbiologistics”:
• Blood culture cabinets (also decentralized) available 24/7/365
• Microbiology open 24/7/365
• Skilled staff 24/7/365
• Not to forget other samples from the critically ill patient
• Take control of the transport organization and the referrals!

Thanks to
Växjö
•Emma Jonasson
•Gunilla Cederbrandt
•Robert Smyth
•Stina Bengtsson
•Jonas Olafsson
•Liselott Byhlén
•Åsa Johansson
•Erika Matuscheck
•Gunnar Kahlmeter
Hvidovre
Pia Littauer
Jenny Dahl Knudsen
AMC
Caspar Hodiamont
Caroline Visser
Nijmegen
Johan Mouton
Örebro
Kristina Sundman
Theresa Ennefors
Kerstin Falkenström