Rapid Eradication of a Cluster ofSerratia marcescensin a Neonatal Intensive Care Unit: Use of...
6
Rapid Eradication of a Cluster of Serratia marcescens in a Neonatal Intensive Care Unit: Use of Epidemiologic Chromosome Profiling by Pulsed‐Field Gel Electrophoresis • Author(s): Kwan Kew Lai , DMD, MD; Stephen P. Baker , MSc, PH; Sally A. Fontecchio , RN, BSNsgED, CIC Source: Infection Control and Hospital Epidemiology, Vol. 25, No. 9 (September 2004), pp. 730- 734 Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiology of America Stable URL: http://www.jstor.org/stable/10.1086/502468 . Accessed: 15/05/2014 23:37 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. . The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaborating with JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology. http://www.jstor.org This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PM All use subject to JSTOR Terms and Conditions
Transcript of Rapid Eradication of a Cluster ofSerratia marcescensin a Neonatal Intensive Care Unit: Use of...

Rapid Eradication of a Cluster of Serratia marcescens in a Neonatal Intensive Care Unit: Use ofEpidemiologic Chromosome Profiling by Pulsed‐Field Gel Electrophoresis • Author(s): Kwan Kew Lai , DMD, MD; Stephen P. Baker , MSc, PH; Sally A. Fontecchio , RN,BSNsgED, CICSource: Infection Control and Hospital Epidemiology, Vol. 25, No. 9 (September 2004), pp. 730-734Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/502468 .
Accessed: 15/05/2014 23:37
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions

730 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY September 2004
RAPID ERADICATION OF A CLUSTER OF SERRATIAMARCESCENS IN A NEONATAL INTENSIVE CARE UNIT:
USE OF EPIDEMIOLOGIC CHROMOSOME PROFILING BY
PULSED-FIELD GEL ELECTROPHORESIS
Kwan Kew Lai, DMD, MD; Stephen P. Baker, MSc, PH; Sally A. Fontecchio, RN, BSNsgED, CIC
Serratia marcescens is ubiquitous and can be isolatedfrom soil and moist areas.1 It has been recognized to be an important cause of severe healthcare-associated infec-tions, particularly meningitis, pneumonia, and bloodstreaminfections.2 Most outbreaks of S. marcescens occur in inten-sive care units.3,4 Neonatal S. marcescens outbreaks havebeen associated with low birth weight, long-term hospital-ization, mechanical ventilation, invasive procedures, expo-sure to antibiotics and steroids, and contamination ofsolutions and devices.5-10 The predominant mode of trans-mission is via the hands.2 In June 2001, S. marcescens infec-tions were noted in two neonates in the neonatal intensivecare unit (NICU): one died of bloodstream infection andthe other recovered from a pulmonary infection. The pre-vious two clinical infections from S. marcescens in the NICUhad been recorded 2 months and more than 1 year earlier.An investigation was conducted and typing by pulsed-fieldgel electrophoresis (PFGE) was performed to determinewhether a single strain or multiple strains of S. marcescenscaused this increased incidence.
METHODS
Investigation of a Cluster of S. marcescensClinical infections with S. marcescens are unusual in
the NICU. In June 2001, two neonates in the NICU werefound to have clinical infections with S. marcescens andone died. Infection control surveillance data for the NICUfor the previous year were reviewed.
Surveillance and Environmental CulturesRectal and nasopharyngeal cultures of all patients
in the NICU were performed and then weekly there-after. Specimens for culture were also obtained fromsinks, soaps, lotions, shampoos, ointments, water fromhumidifiers, and disinfectant solutions. Sink 11 in pod 1(Fig. 1) historically had a problem with odors; it wasreplaced and the pipes were flushed with steam underpressure and hyperchlorinated. Routine bacteriologicidentification and antibiograms were performed with anautomated system (VITEK, bioMérieux, Hazelwood,MO).
The authors are from the UMass Memorial Medical Center, Worcester, Massachusetts. Dr. Lai and Mr. Baker are also from the University ofMassachusetts Medical School, Worcester, Massachusetts.
Address reprint requests to Kwan Kew Lai, DMD, MD, UMass Memorial Medical Center, 55 Lake Avenue North, Worcester, MA01655.
Presented in part at the 13th Annual Meeting of the Society for Healthcare Epidemiology of America; April 5-8, 2003; Arlington, VA.
OBJECTIVE: To investigate a cluster of patients infectedand colonized with Serratia marcescens in a neonatal intensivecare unit (NICU).
METHODS: In June 2001, two neonates in the NICU hadclinical infections with S. marcescens and one died. Infection controlsurveillance data for the NICU revealed that S. marcescens wasrarely isolated from clinical specimens. Surveillance and environ-mental cultures were performed and isolates were typed usingpulsed-field gel electrophoresis. Staff and neonates were cohortedand a waterless, alcohol-based handwashing agent was introduced.A case–control study was performed.
RESULTS: From June 2 through August 20, 2001, 11neonates with S. marcescens infection and colonization wereidentified. The incidence of S. marcescens infections increasedfrom 0.19 per 1,000 patient-days in 2000 to 0.52 per 1,000patient-days in 2001 (P < .0001). In the first 3 weeks of the inves-
tigation, there were 2 sets of patients and sinks with indistin-guishable strains; however, in subsequent weeks, all isolateswere of unique strains, signifying no further transmission of thetwo initial predominant strains. Neonates with S. marcescenswere more likely to have a lower gestational age and birthweight. There was no association between cases and healthcareworkers (HCWs).
CONCLUSIONS: A cluster of S. marcescens was quicklyterminated after the introduction of preventive measures includ-ing cohorting of infected and colonized neonates and HCWs, con-tact precautions, surveillance cultures, and a waterless, alcohol-based hand antiseptic. Chromosomal typing determined thatstrains with an indistinguishable pattern were no longer presentin the unit after control measures were implemented (InfectControl Hosp Epidemiol 2004;25:730-734).
ABSTRACT
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions

Vol. 25 No. 9 S. MARCESCENS OUTBREAK IN A NICU 731
Preventive MeasuresAt the outset of the investigation, cohorting of
neonates and staff was enforced and contact precautionswere instituted. Healthcare workers (HCWs) who workedin pod 1 during the week before the identification ofneonates infected and colonized with S. marcescens werecohorted to care for those who were already in pod 1 orhad been discharged from pod 1. Neonates who were laterfound to be colonized with S. marcescens were cared forby these HCWs. Ongoing staff education regarding theepidemiology of S. marcescens was conducted. Artificialfingernails, wraps, and tips were banned, and natural nailswere kept at an acceptable length. Hand cultures of per-sonnel were not done. During the first week of the inves-tigation, enhanced environmental cleaning was per-formed by the environmental service and sterile water forbathing and rewarming formula and breast milk was insti-tuted. A waterless, alcohol-based antiseptic foam(ALCARE antiseptic foamed alcohol, Steris Corp., St.Louis, MO) for hand hygiene was introduced during thefirst 2 weeks. The dispensers were conveniently locatednear the bassinets and outside the pods.
PFGEPFGE of whole-cell DNA digested by SpeI was used
as a marker of strain identity. Isolates were considered to
be the same strain if their PFGE patterns were identical,closely related if their PFGE patterns differed from thecluster pattern by two to three bands, possibly related iftheir PFGE patterns differed from the cluster pattern byfour to six bands, and distinct from the outbreak cluster iftheir PFGE patterns differed by seven or more bands.11
Case–Control StudyA case was defined as a neonate with infection or
colonization with S. marcescens. Two control-patientswere selected for each case-patient on the basis of havingbeen admitted to the NICU within 3 days of the case-patient. Demographic data, location, antibiotic use, inva-sive procedures, and HCW exposure were compared.
Statistical AnalysisStatistical analyses were performed using SPSS (ver-
sion 12; SPSS, Inc., Chicago, IL) and SAS (version 8e; SASInstitute, Inc., Cary, NC) software. Tests of the significanceof hypotheses about differences in proportions betweencase-patients and control-patients were evaluated usingFisher’s exact test.12 Differences between them on normal-ly distributed continuous variables were evaluated usingthe Student’s t test or the Welch–Aspin t test, depending onwhether homogeneity of variances was present as deter-mined by an F test of the ratio of variances. Differences indistribution for rank-order or non-normally distributed con-tinuous variables were evaluated using the Mann–Whitneytest.13 Relative prevalence was estimated by the commonodds ratio, and multivariate models were fit by logisticregression analysis to estimate relative prevalence for riskfactors after controlling for other risk factors. Statistical sig-nificance was defined as effects, difference, or associationsthat would be likely to occur by chance alone less than 5%of the time with repeated sampling.
RESULTS
Incidence and Patient CharacteristicsFrom June 2 through August 20, 2001, a total of 11
neonates with S. marcescens infection and colonizationwere identified. The incidence of S. marcescens infections
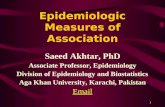
FIGURE 1. Floor plan of the neonatal intensive care unit. CCN = continu-ing care nursery.
FIGURE 2. Distribution of the Serratia marcescens cases.
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions

732 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY September 2004
increased from 0.19 per 1,000 patient-days in 2000 to 0.52per 1,000 patient-days in 2001 (Fig. 2), a 2.7-fold increase(P < .0001). The first two cases of S. marcescens that start-ed the investigation were from pod 1 (Fig. 2) and thesewere the infected patients: one died of bloodstream infec-tion and one had pneumonia but survived. The rest of thecases were identified from surveillance cultures and allwere colonized. Sixty-three percent of all S. marcescensfrom this period were from pod 1. All of these neonates
were premature and had a mean birth weight of 1,215 g.Prematurity was defined as birth before 37 weeks of gesta-tion. All had hyperbilirubinemia, 73% had received priorantibiotic therapy (receipt of antibiotics for at least 48 hours2 to 4 weeks prior to isolation of S. marcescens), and 91%had received an invasive device such as a ventilator, centralcatheter, or nasogastric tube. The median length of stay ofcase-patients from admission to the NICU until the firstpositive result was 15 days. The rest of the patient charac-teristics are listed in Table 1.
Environmental CulturesFive S. marcescens isolates were cultured from
sinks 1, 10, and 11 in the NICU (sinks 10 and 11 were inpod 1) and from sink 16 in the continuing care nursery.Two of the 5 isolates were from sink 1 before and after itwas cleaned. No S. marcescens was isolated from soaps,lotions, or other solutions.
PFGETen clinical and 5 environmental isolates were
available for typing. No infecting isolate was available foranalysis. Six of the 10 clinical isolates were unique. All 5of the environmental isolates were isolated from thesinks: two from sink 1 (before and after hyperchlorina-tion) and 1 each from sinks 10, 11, and 16. The 2 isolatesfrom sink 1 were the same strain and the isolates fromsinks 10 and 11 were closely related to each other, but theisolate from sink 16 was different from the other envi-ronmental isolates. In the first 3 weeks of the outbreak,there were 2 sets of patients and sinks with identicalstrains: set 1 included 3 patients (patients B, C, and F)and sink 1 (pattern II), and set 2 included 2 patients(patients D and E) and sink 16 (pattern III) (Figs. 3 and4; Table 2).
Case–Control StudyThe case–control study showed that neonates with
S. marcescens were more likely to have a lower gestation-al age and birth weight (P = .003 and P < .001, respective-ly) (Table 1). There was no association of cases witheither pod 1 or HCWs. However, several HCWs werenoted to have artificial nails, and these were banned at thebeginning of the outbreak. The contribution of nails to theoutbreak could not be entirely ruled out. Ongoing spreadof either of these two strains (patterns II and III) did notoccur after preventive measures were implemented. Atthe end of August, when PFGE showed no further person-to-person transmission because the S. marcescens isolateswere of different strains, cohorting of neonates and staffand other preventive measures were discontinued withthe exception of the alcohol handrub.
The last S. marcescens was isolated from a surveil-lance culture during the third week of August.Subsequent rectal and nasal surveillance through thenext 3 weeks did not reveal any further positive cultures.Surveillance cultures were discontinued, but microbiolo-gy laboratory surveillance for isolates of S. marcescens
TABLE 1PATIENT CHARACTERISTICS
Case- Control-Patients Patients
Characteristic (n = 11) (n = 22) P
Mean gestational age, 29 (24–34) 34 (25–44) .003wk (range)
GenderMale 6 (55%) 11 (50%) 1.0Female 5 (45%) 11 (50%)
Respiratory distress 9 (82%) 14 (64%) .430or apnea
Mean birth weight, 1,215 (705–1,760) 2,581 (885–4,160) < .001g (range)
DeliveryVaginal 6 (55%) 14 (64%) 1.0Cesarean section 5 (45%) 8 (36%)
Apgar score1 min 6 6 .6705 min 9 8 .555
Prematurity 11 (100%) 15 (68%) .067Site of Serratia
marcescens isolationBlood 1 N/ATracheal aspirate 1Nares 2Rectum 7
S. marcescens infections 1 (9%) N/AAntibiotic therapy 8 (73%) 16 (73%) 1.0Hyperbilirubinemia 11 (100%) 16 (73%) .077Invasive device
Ventilator 7 (64%) 16 (73%) 1.0Central catheter 4 (36%) 4 (18%) .391UVC 5 (45%) 14 (64%) .459UAC 4 (36%) 9 (41%) 1.0TPN 7 (64%) 10 (46%) .465Nasogastric tube 10 (91%) 13 (59%) .109
Breast milk 9 (82%) 15 (68%) .681Median length of stay, 67 (15–181) 21 (2–95) .019
d (range)Surgery 2 (18%) 3 (14%) 1.0Death 1 (9%) 1 (5%) 1.0
N/A = not applicable; UVC = umbilical vein catheterization; UAC = umbilical artery catheteriza-tion; TPN = total parenteral nutrition.
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions

Vol. 25 No. 9 S. MARCESCENS OUTBREAK IN A NICU 733
continued; this also failed to uncover any further isolatesuntil May 2003.
DISCUSSION
In previous outbreaks involving S. marcescens,14,15 theidentification of a reservoir was impossible despite exten-sive sampling of the environment and staff. In this cluster,we were able to sample environmental surfaces, solutions,
and lotions but not the staff. S. marcescens was isolated fromthe sinks. Two of the isolates from the sinks were associat-ed with the first two sets of neonates. However, despite theassociation, we were unable to state definitively whether thesinks were the cause of the outbreak or had been contami-nated as a result of it, given that most sinks would inevitablyhave some forms of organisms isolated from them.
FIGURE 3. Pulsed-field gel electrophoresis (PFGE) for set 1 Serratiamarcescens isolates from patients and the environment. Lanes 1, 8, and14 = references for computer analysis; lane 15 = lambda ladder DNAfragment size standard; lanes 2 and 5 = isolates from sink 1 (pattern II);lane 7 = isolate from sink 10 (pattern V); and lanes 12 and 13 = isolatesfrom nasal swab from patient A (pattern I). Isolates with PFGE pattern IIinclude those from 3 patients (B, C, and F in lanes 3, 4, and 6, respec-tively) and from sink 1 (lanes 2 and 5). Isolates with PFGE pattern IIIinclude those from 2 patients (D and E in lanes 10 and 11, respectively)and from sink 16 (lane 9).
FIGURE 4. Pulsed-field gel electrophoresis for set 2 Serratia marcescensisolates from patients and the environment. Lanes 1, 8, and 12 = refer-ence lanes; lane 13 = lambda ladder DNA fragment size standard; lane 11= comparison strain from University Hospital, San Antonio, Texas; lanes 4,6, and 7 = isolates from patients D, E (both are pattern III), and G (pat-tern VI); lanes 2, 9, and 10 = isolates from patients H (pattern VII), I (pat-tern VIII), and J (pattern IX) in late July and early August 2001; lane 3 =isolate from sink 11 (pattern IV); and lane 5 = isolate from sink 16 (pat-tern III).
TABLE 2CHARACTERISTICS OF SERRATIA MARCESCENS IN THE STUDY
Isolate Source of Isolate PFGENo. Gel Lane Patient Sink Isolate Date Pattern
1 1 12, 13 A (pod 1) Nasal swab 6/25/01 I2 1 3 B (pod 1) Nasal swab 6/25/01 II3 1 4 C (pod 1) Nasal swab 6/25/01 II4 1 10 D Nasal swab 6/29/01 III
2 65 1 11 E Endotracheal 7/5/01 III
2 7 aspirate6 2 3 11 (pod 1) 6/26/01 IV7 1 2 1 (pod 2) 7/11/01 II8 1 7 10 (pod 1) 7/11/01 V9 1 9 16 (CCN) 7/11/01 III
2 510 1 6 F Rectal swab 7/15/01 II11 1 5 1 (pod 2) 7/25/01 II12 2 4 G (pod 1) Rectal swab 7/3/01 VI13 2 2 H Rectal swab 7/24/01 VII14 2 9 I (pod 1) Rectal swab 8/6/01 VIII15 2 10 J (pod 1) Rectal swab 8/20/01 IX
PFGE = pulsed-field gel electrophoresis; CCN = continuing care nursery.
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions

734 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY September 2004
The contribution of artificial nails to this outbreakcould not be determined once HCWs were banned fromwearing them. Long nails, both natural and artificial, havebeen known to result in nosocomial colonization andinfection with pathogens.16 Moolenaar et al. reported aprolonged Pseudomonas aeruginosa outbreak associatedwith two nurses with long natural and artificial nails. Theyalso found that significantly more nurses with artificialnails had gram-negative rods than those with naturalnails, both before (36% vs 5%) and after (41% vs 9%) hand-washing. Therefore, long natural or artificial nails canclearly be a reservoir for pathogens. Schroeder et al.reported an outbreak of S. marcescens in a NICU17; one ofthe strains was traced to a nurse who had a persistentlyinfected thumbnail. Once the nurse was identified as col-onized with one of the epidemic strains, the number ofcases of S. marcescens diminished.
Miranda et al.14 suggested that the results of PFGEfacilitate a prompt evaluation of outbreaks and institutionof effective preventive measures. We were able to identifytwo sets of patients with genetically distinct strains of S.marcescens (patterns II and III; Table 2) that wereinvolved early in the cluster. Subsequent isolates with dif-ferent patterns were then observed, suggesting that therewas no longer persistent person-to-person transmission ofstrains with patterns II and III. This confirmed that thepreventive measures instituted were effective.
Waterless, alcohol-based hand antiseptic has beenshown to be more effective than antimicrobial soap in elim-inating pathogens from natural or artificial nails.18 McNeilet al. demonstrated that only 11% of HCWs with artificialnails who had pathogens at baseline effectively removedthe pathogens using soap compared with 38% using alco-hol-based gel. Of those HCWs who had natural nails andpathogens at baseline, 14% removed the pathogens usingsoap compared with 80% of those using an alcohol-basedantiseptic (P = .09). The introduction of the waterless, alco-hol-based hand antiseptic to the NICU effectively providedeasy access to another method of hand hygiene, whichmay have contributed to more frequent handwashingbetween patient contacts. However, we were not able toprove that this occurred because we did not monitor thefrequency of handwashing among HCWs.
Several infection control measures were introducedat the same time, including the waterless, alcohol-basedhand antiseptic; therefore, it is difficult to identify whichmeasures were responsible for controlling and eliminatingthe cluster. However, the timely application of epidemio-
logic chromosome profiling with PFGE helped us deter-mine that the preventive measures instituted were effec-tive early on, thus enabling us to discontinue their use.
REFERENCES1. Sartor C, Jacomo V, Duvivier C, Tissot-Dupont H, Sambuc R,
Drancourt M. Nosocomial Serratia marcescens infections associatedwith extrinsic contamination of a liquid nonmedicated soap. InfectControl Hosp Epidemiol 2000;21:196-199.
2. Yu VL. Serratia marcescens: historical perspective and clinical review.N Engl J Med 1979;300:887-893.
3. Manning ML, Archibald LK, Bell LM, Banerjee SN, Jarvis WR.Serratia marcescens transmission in a pediatric intensive care unit: amultifactorial occurrence. Am J Infect Control 2001;29:115-119.
4. Jones BL, Gorman LJ, Simpson J, et al. An outbreak of Serratiamarcescens in two neonatal intensive care units. J Hosp Infect 2000;46:314-319.
5. Berthelot P, Grattard F, Amerger C, et al. Investigation of a nosocomi-al outbreak due to Serratia marcescens in a maternity hospital. InfectControl Hosp Epidemiol 1999;20:233-236.
6. van Ogtrop ML, van Zoeren-Grobben D, Verbakel-Salomons EM, vanBoven CP. Serratia marcescens infections in neonatal departments: descrip-tion of an outbreak and review of the literature. J Hosp Infect 1997;36:95-103.
7. Stamm WE, Kolff CA, Dones EM, et al. A nursery outbreak caused bySerratia marcescens: scalp-vein needles as a portal of entry. J Pediatr1976;89:96-99.
8. Sanders CV Jr, Luby JP, Johanson WG Jr, Barnett JA, Sanford JP.Serratia marcescens infections from inhalation therapy medications:nosocomial outbreak. Ann Intern Med 1970;73:15-21.
9. Archibald LK, Corl A, Shah B, et al. Serratia marcescens outbreak asso-ciated with extrinsic contamination of 1% chlorxylenol soap. InfectControl Hosp Epidemiol 1997;18:704-709.
10. Sautter RL, Mattman LH, Legaspi RC. Serratia marcescens meningitisassociated with a contaminated benzalkonium chloride solution. InfectControl 1984;5:223-225.
11. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomalDNA restriction patterns produced by pulsed-field gel electrophore-sis: criteria for bacterial strain typing. J Clin Microbiol 1995;33:2233-2239.
12. Snedecor GW, Cochran WG. Statistical Methods. Ames, IA: Iowa StateUniversity Press; 1989.
13. Siegel S. Nonparametric Statistics for the Behavioral Sciences. NewYork: McGraw-Hill; 1956.
14. Miranda G, Kelly C, Solorzano F, Leanos B, Coria R, Patterson JE. Useof pulsed-field gel electrophoresis typing to study an outbreak of infec-tion due to Serratia marcescens in a neonatal intensive care unit. J ClinMicrobiol 1996;34:3138-3141.
15. Braver DJ, Hauser GJ, Berns L, Siegman-Igra Y, Muhlbauer B. Controlof a Serratia marcescens outbreak in a maternity hospital. J Hosp Infect1987;10:129-137.
16. Moolenaar RL, Crutcher JM, San Joaquin VH, et al. A prolonged out-break of Pseudomonas aeruginosa in a neonatal intensive care unit: didstaff fingernails play a role in disease transmission? Infect Control HospEpidemiol 2000;21:80-85.
17. Schroeder P, Kieffer P, Kilian C, et al. Outbreak of Serratia marcescensin a neonatal intensive care unit. Presented at the 28th Annual Meetingof the Association for Professionals in Infection Control andEpidemiology; June 10-14, 2001; Seattle, WA. Abstract 245.
18. McNeil SA, Foster CL, Hedderwick SA, Kauffman CA. Effect of handcleansing with antimicrobial soap or alcohol-based gel on microbialcolonization of artificial fingernails worn by health care workers. ClinInfect Dis 2001;32:367-372.
This content downloaded from 195.78.108.127 on Thu, 15 May 2014 23:37:42 PMAll use subject to JSTOR Terms and Conditions