
Rapid detection of Candida albicans in oral exfoliative ...
7
541 Abstract: Loop-mediated isothermal amplification (LAMP) rapidly amplifies DNA under isothermal conditions. The aim of this study was to detect Candida albicans and compare the positivity rate in the LAMP reaction with that of conventional methods for oral exfoliative cytology (EC) samples. Sixty-eight EC samples from 53 patients were subjected to LAMP analysis. These patients had been clinically diagnosed with leukoplakia, squamous cell carcinoma, oral lichen planus (OLP), stomatitis, oral candidiasis, and other malignancies. LAMP reactions were defined as positive when the sample turbidity exceeded 0.1 (arbitrary unit). Periodic acid-Schiff (PAS) staining and microbial culture were also performed to detect Candida species in EC samples. The LAMP reaction detected C. albicans in 42.6% of EC samples. Candida species were detected in 32.4% of the same samples by culturing and in 29.4% of samples by PAS staining. C. albicans DNA was detected most frequently in samples from OLP patients. We conclude that, in comparison to conventional methods for detection of C. albicans, the LAMP method is highly sensitive and time- saving, and does not require expensive equipment or diagnostic technology. It may therefore be useful for on-site screening of C. albicans at dental clinics. Keywords: Candida albicans; exfoliative cytology; loop-mediated isothermal amplification. Introduction Fungal infections are the major cause of morbidity and mortality in debilitated or immunocompromised patients (1). Candida albicans (C. albicans) is the Candida species most frequently isolated from the oral cavity of both healthy and immunocompromised hosts. Recently, non-albicans species, including C. glabrata, C. tropi- calis, C. krusei, C. parapsilosis, and C. guilliermondii, have shown increased rates of isolation in patients with candidiasis (2). Apart from oral candidiasis, however, Candida species are associated with various diseases and can be the suspected causative agent. Such diseases include esophageal candidiasis, candida pneumonia, and invasive candidiasis (3,4). C. albicans is a commensal fungus but also an important pathogen responsible for the majority of superficial and systemic fungal infec- tions (5,6). The most common severe fungal infection is invasive candidiasis, which can lead to candidemia, the fourth most common bloodstream infection in intensive care units. Its mortality rate has been reported to range from 25% to 53% (5,7,8). The presence of Candida species is confirmed by blood culturing in up to 50% of Journal of Oral Science, Vol. 59, No. 4, 541-547, 2017 Original Rapid detection of Candida albicans in oral exfoliative cytology samples by loop-mediated isothermal amplification Hiroyasu Noguchi 1) , Takashi Iwase 2) , Daisuke Omagari 2) , Masatake Asano 2) , Ryota Nakamura 1) , Kosuke Ueki 1) , Keiji Shinozuka 3) , Tadayoshi Kaneko 3) , Morio Tonogi 3) , and Hiderou Ohki 3) 1) Division of Oral Structural and Functional Biology, Nihon University Graduate School of Dentistry, Tokyo, Japan 2) Department of Pathology, Nihon University School of Dentistry, Tokyo, Japan 3) Department of Oral and Maxillofacial Surgery, Nihon University School of Dentistry, Tokyo, Japan (Received October 11, 2016; Accepted December 19, 2016) Correspondence to Dr. Hiderou Ohki, Department of Oral and Maxillofacial Surgery, Nihon University School of Dentistry, 1-8-13 Kanda-Surugadai, Chiyoda-ku, Tokyo 101-8310, Japan Fax: +81-3-3219-8356 E-mail: [email protected] Color figures can be viewed in the online issue at J-STAGE. doi.org/10.2334/josnusd.16-0717 DN/JST.JSTAGE/josnusd/16-0717
Transcript of Rapid detection of Candida albicans in oral exfoliative ...

541
Abstract: Loop-mediated isothermal amplification (LAMP) rapidly amplifies DNA under isothermal conditions. The aim of this study was to detect Candida albicans and compare the positivity rate in the LAMP reaction with that of conventional methods for oral exfoliative cytology (EC) samples. Sixty-eight EC samples from 53 patients were subjected to LAMP analysis. These patients had been clinically diagnosed with leukoplakia, squamous cell carcinoma, oral lichen planus (OLP), stomatitis, oral candidiasis, and other malignancies. LAMP reactions were defined as positive when the sample turbidity exceeded 0.1 (arbitrary unit). Periodic acid-Schiff (PAS) staining and microbial culture were also performed to detect Candida species in EC samples. The LAMP reaction detected C. albicans in 42.6% of EC samples. Candida species were detected in 32.4% of the same samples by culturing and in 29.4% of samples by PAS staining. C. albicans DNA was detected most frequently in samples from OLP patients. We conclude that, in comparison to conventional methods for detection of C. albicans, the LAMP method is highly sensitive and time-
saving, and does not require expensive equipment or diagnostic technology. It may therefore be useful for on-site screening of C. albicans at dental clinics.
Keywords: Candida albicans; exfoliative cytology; loop-mediated isothermal amplification.
IntroductionFungal infections are the major cause of morbidity and mortality in debilitated or immunocompromised patients (1). Candida albicans (C. albicans) is the Candida species most frequently isolated from the oral cavity of both healthy and immunocompromised hosts. Recently, non-albicans species, including C. glabrata, C. tropi-calis, C. krusei, C. parapsilosis, and C. guilliermondii, have shown increased rates of isolation in patients with candidiasis (2). Apart from oral candidiasis, however, Candida species are associated with various diseases and can be the suspected causative agent. Such diseases include esophageal candidiasis, candida pneumonia, and invasive candidiasis (3,4). C. albicans is a commensal fungus but also an important pathogen responsible for the majority of superficial and systemic fungal infec-tions (5,6). The most common severe fungal infection is invasive candidiasis, which can lead to candidemia, the fourth most common bloodstream infection in intensive care units. Its mortality rate has been reported to range from 25% to 53% (5,7,8). The presence of Candida species is confirmed by blood culturing in up to 50% of
Journal of Oral Science, Vol. 59, No. 4, 541-547, 2017
Original
Rapid detection of Candida albicans in oral exfoliative cytology samples by loop-mediated isothermal amplification
Hiroyasu Noguchi1), Takashi Iwase2), Daisuke Omagari2), Masatake Asano2), Ryota Nakamura1), Kosuke Ueki1), Keiji Shinozuka3), Tadayoshi Kaneko3),
Morio Tonogi3), and Hiderou Ohki3)
1)Division of Oral Structural and Functional Biology, Nihon University Graduate School of Dentistry, Tokyo, Japan
2)Department of Pathology, Nihon University School of Dentistry, Tokyo, Japan3)Department of Oral and Maxillofacial Surgery, Nihon University School of Dentistry, Tokyo, Japan
(Received October 11, 2016; Accepted December 19, 2016)
Correspondence to Dr. Hiderou Ohki, Department of Oral and Maxillofacial Surgery, Nihon University School of Dentistry, 1-8-13 Kanda-Surugadai, Chiyoda-ku, Tokyo 101-8310, JapanFax: +81-3-3219-8356 E-mail: [email protected] figures can be viewed in the online issue at J-STAGE.doi.org/10.2334/josnusd.16-0717DN/JST.JSTAGE/josnusd/16-0717

542
cases of invasive candidiasis (3). Oral candidiasis is one of the most common opportunistic infections caused by Candida species in patients with impaired immunity or diabetes (9,10). C. albicans infection of the oral cavity presents as oral mucosal candidiasis, and is often associ-ated with a low level of host immune response, e.g., in children, elderly individuals, and immunocompromised individuals. Opportunistic C. albicans infections of the oral cavity are a known risk factor for aspiration pneu-monia (11).
Several detection methods for C. albicans are available, including microbial culture, microscopic examination (PAS staining, Grocott’s methenamine silver staining) and biochemical techniques (indirect hemagglutination, counterimmunoelectrophoresis), polymerase chain reaction (PCR), and real-time PCR (12-17). However, these methods require technical expertise and complex devices, and diagnosis using them is time-consuming and costly. A delay in diagnosis may lead to poor outcome in patients with systemic fungus disease. Typically, it takes several days to obtain the results of a fungal culture test for Candida species and therefore, in many cases, physi-cians initiate therapy before the test results are available. It is therefore imperative that a rapid and accurate test for Candida species be developed.
Loop-mediated isothermal amplification (LAMP) is a method for amplifying nucleic acid samples, facilitating the synthesis of large amounts of DNA with high speci-ficity in a short period of time (18). As the LAMP reaction progresses, pyrophosphate ions, the reaction by-product, bind to magnesium ions and form a white precipitate (magnesium pyrophosphate), which forms the basis of detection (19). LAMP is performed using a simple apparatus capable of measuring the turbidity of multiple samples simultaneously, in real-time, while maintaining a constant temperature (19). Real-time turbidity measure-ments of the LAMP reaction permit quantitative analyses of minute amounts of nucleic acid (19).
Exfoliative cytology (EC) is widely used to examine oral premalignancy and cancer. It is a quick, simple, relatively inexpensive, and non-invasive method (20). A cytobrush is employed for sample collection, as it permits easy sampling and ensures the quality of the sample (21). In addition, EC allows harvesting of cells over a wider area than selective tissue biopsy (22).
In this study, LAMP was used to detect C. albicans in EC samples. We aimed to detect Candida species and compare the positivity rate of the LAMP reaction in EC samples with that of conventional methods.
Materials and MethodsSamplesSixty-eight cytobrush samples obtained from 53 patients with various oral mucosal diseases who underwent EC examination were used in this study (Table 1). The mean age of the population was 58.7 (range 14-88) years. All of the subjects provided written informed consent and were treated at the Department of Oral and Maxillofacial Surgery, Nihon University School of Dentistry Dental Hospital (Tokyo, Japan), between 2013 and 2015. C. albi-cans strain ATCC 24433 was used as a positive control to evaluate the specificity of the LAMP method. The strain was purchased from the American Type Culture Collection (ATCC, Manassas, VA, USA). The study was conducted with the approval of the Ethics Committee of Nihon University School of Dentistry (EP2013-14) and in accordance with the Declaration of Helsinki.
Cytomorphometric analysesEC was performed on each lesion. Cells obtained by Cyto-brush Plus (CooperSurgical Inc., Trumbull, CT, USA) were smeared on Super Frost MAS Coated (Matsunami Glass Ind., Ltd., Osaka, Japan). The cells were immedi-ately fixed in 95% ethanol. Cytomorphometric analysis of the lesions was performed using Papanicolaou staining. These slides were routinely evaluated by skilled oral pathologists: M.A. and D.O. To evaluate the presence of Candida species, the slides were stained with peri-odic acid-Schiff (PAS) solution. Papanicolaou staining and PAS staining were performed in accordance with the conventional method (15,23). Cytomorphological features were classified according to the Papanicolaou classification (1960) as follows: Class I (normal): only normal cells observed; Class II (atypical): presence of minor atypia but no evidence of malignancy; Class III
Table 1 Exfoliative cytology samples used in this studySubjects Male Female TotalNumber of patients 28 25 53
Mean age 55.0 60.6 57.7Range 14-88 26-86 14-88
Clinical diagnosisLeukoplakia 12 9 21SCC1) 12 7 19Oral lichen planus 3 4 7Stomatitis 4 2 6Fibroma 2 2 4Oral candidiasis 1 2 3Papilloma 2 1 3Others2) 2 3 5
Values are given as numbers. 1)SCC: squamous cell carcinoma. 2)Others: xerostomia, black hairy tongue, bite wound, Fordyce spot, glossodynia.

543
(intermediate): intermediate cytology (the cells display a range of atypia that may be suggestive of malignancy but not clear-cut cancer, representing precancerous lesions or in situ carcinoma); Class IV (suggestive of cancer): a few epithelial cells with malignant characteristics or cells with borderline characteristics; Class V: positive cancer cells that are obviously malignant (21).
DNA extractionFor extraction of reference C. albicans DNA, the C. albi-cans ATCC 24433 strain was grown on Vitalmedia Color Candida Agar (Kyokuto Pharmaceutical Industrial Co., Tokyo, Japan) for 48 h at 37°C. The DNA of C. albicans was extracted from the pellet using the DNeasy Blood & Tissue Kit (Qiagen, Valencia, CA, USA) in accordance with the manufacturer’s instructions. The DNA concen-tration was measured by spectrophotometry using a NanoDrop 1000 (Thermo Fisher Scientific, Wilmington, DE, USA). DNA (1 ng/μL) was serially diluted (from 1 ng to 1 fg/μL) in sterilized double-distilled water, and used for DNA amplification. For the clinical samples, after the cytology slides had been prepared, the cytobrush was rinsed with 1.0 mL of phosphate-buffered saline (pH 6.0) and then centrifuged at 2,000×g for 10 min. The supernatant was discarded and the DNA was extracted from the pellet using a DNeasy Blood & Tissue Kit in accordance with the manufacturer’s instructions. DNA solutions were kept at −20°C until LAMP examination.
Culture and identification of C. albicans Vitalmedia Color Candida Agar was used for micro-biological identification of C. albicans. The principle of identification is based on differences in the oxidation-reduction ability for the substrate among Candida species. Different Candida species grow as differently colored colonies on this medium, as follows: C. albicans, green; C. glabrata, pale pink; C. tropicalis, dark blue, with a pink halo; C. krusei, pink and downy appearance; C. parapsilosis, pale pink to pink; C. guilliermondii,
pale pink to pink. Cytobrush rinse solutions (30 μL) were plated on the Vitalmedia Color Candida Agar and incubated for 48 h at 37°C.
LAMP reactionsFor LAMP analyses, the Loopamp Specified Micro-organism “Fungi Candida albicans” Detection Kit (Eiken Chemical Co., Tokyo, Japan) was used in accordance with the manufacturer’s instructions. Briefly, the primer mix (15 μL) and the template solutions (15 μL) were added to amplification reagent tubes. The tubes were then inverted for 3 min. The tubes were subsequently inverted five times and placed in a benchtop centrifuge to settle the reaction mixture. DNA amplification and real-time moni-toring of the sample turbidity were conducted using the Loopamp real-time turbidimeter (LA-200; TERAMECS Co. Ltd., Kyoto, Japan), for 60 min at 65°C. The turbidity threshold was defined as a Candida-positive sample >0.1 (arbitrary unit) within 60 min (19). A previous study reported that an increase in the quantity of initial template DNA will shorten the threshold time (19). The amplicons were then separated by electrophoresis in a 2% agarose gel, followed by ethidium bromide staining.
ResultsCytomorphometric analysis of samplesCytomorphometric analysis was performed using a five-stage classification system. Following cytomorphometric assessment, 54 EC specimens were designated as Class II, 10 as Class III, 3 as Class V, and 1 as Class I (Table 2).
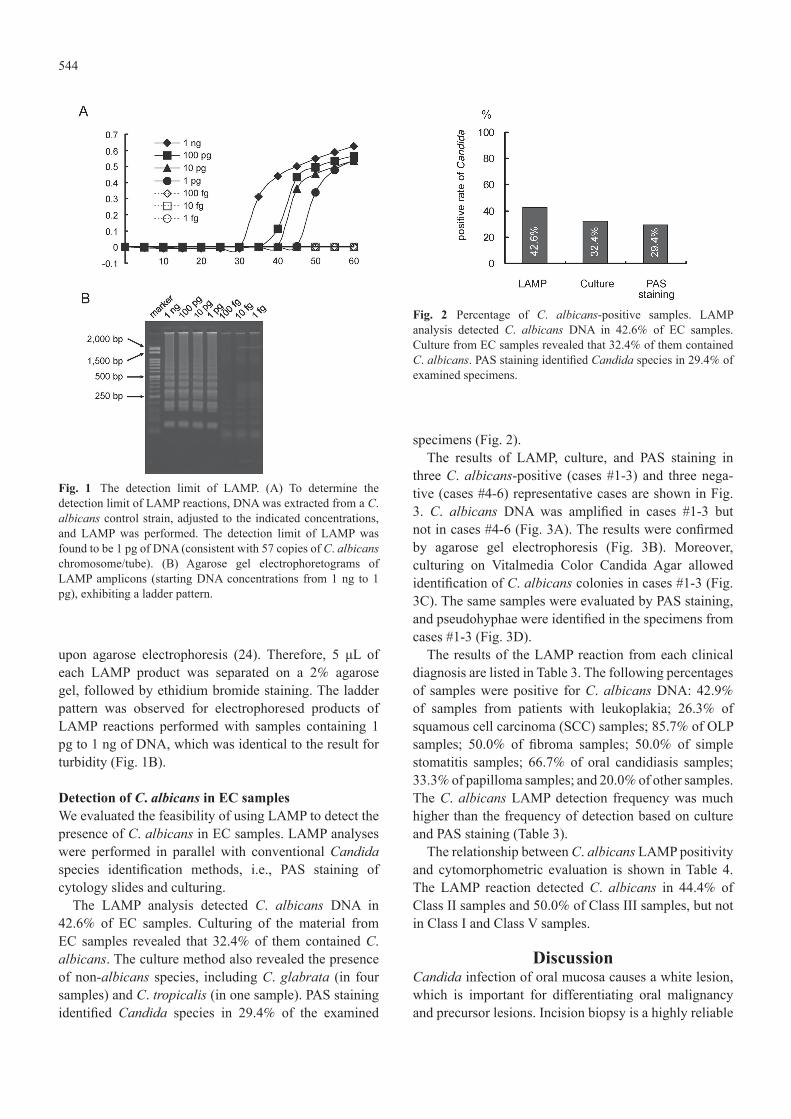
Sensitivity of the LAMP reaction for C. albicans The sensitivity of the LAMP reaction was examined using C. albicans DNA (1 fg, 10 fg, 100 fg, 1 pg, 10 pg, 100 pg, and 1 ng of DNA) isolated from strain ATCC 24433. The samples containing 1 pg to 1 ng exceeded a turbidity of 0.1 (arbitrary unit) within 60 min (Fig. 1A). When the LAMP reaction is performed successfully, the amplicons are detected as a characteristic ladder pattern
Table 2 Relationship between clinical diagnosis and cytomorphometric diagnoses of lesionsClinical diagnosis Class I Class II Class III Class IV Class V Leukoplakia (n = 21) 0 20 (95.2) 1 (4.8) 0 0 SCC (n = 19)1) 0 11 (57.9) 5 (26.3) 0 3 (15.8) Oral lichen planus (n = 7) 0 6 (85.7) 1 (14.3) 0 0 Stomatitis (n = 6) 0 6 (100.0) 0 0 0 Fibroma (n = 4) 0 3 (75.0) 1 (25.0) 0 0 Oral candidiasis (n = 3) 0 2 (66.7) 1 (33.3) 0 0 Papilloma (n = 3) 0 2 (66.7) 1 (33.3) 0 0 Others (n = 5)2) 1 (20.0) 4 (80.0) 0 0 0 Total (n = 68) 1 54 10 0 3Values are given as numbers (%). 1)SCC: squamous cell carcinoma. 2)Others: xerostomia, black hairy tongue, bite wound, Fordyce spot, glossodynia.
544
upon agarose electrophoresis (24). Therefore, 5 μL of each LAMP product was separated on a 2% agarose gel, followed by ethidium bromide staining. The ladder pattern was observed for electrophoresed products of LAMP reactions performed with samples containing 1 pg to 1 ng of DNA, which was identical to the result for turbidity (Fig. 1B).
Detection of C. albicans in EC samplesWe evaluated the feasibility of using LAMP to detect the presence of C. albicans in EC samples. LAMP analyses were performed in parallel with conventional Candida species identification methods, i.e., PAS staining of cytology slides and culturing.
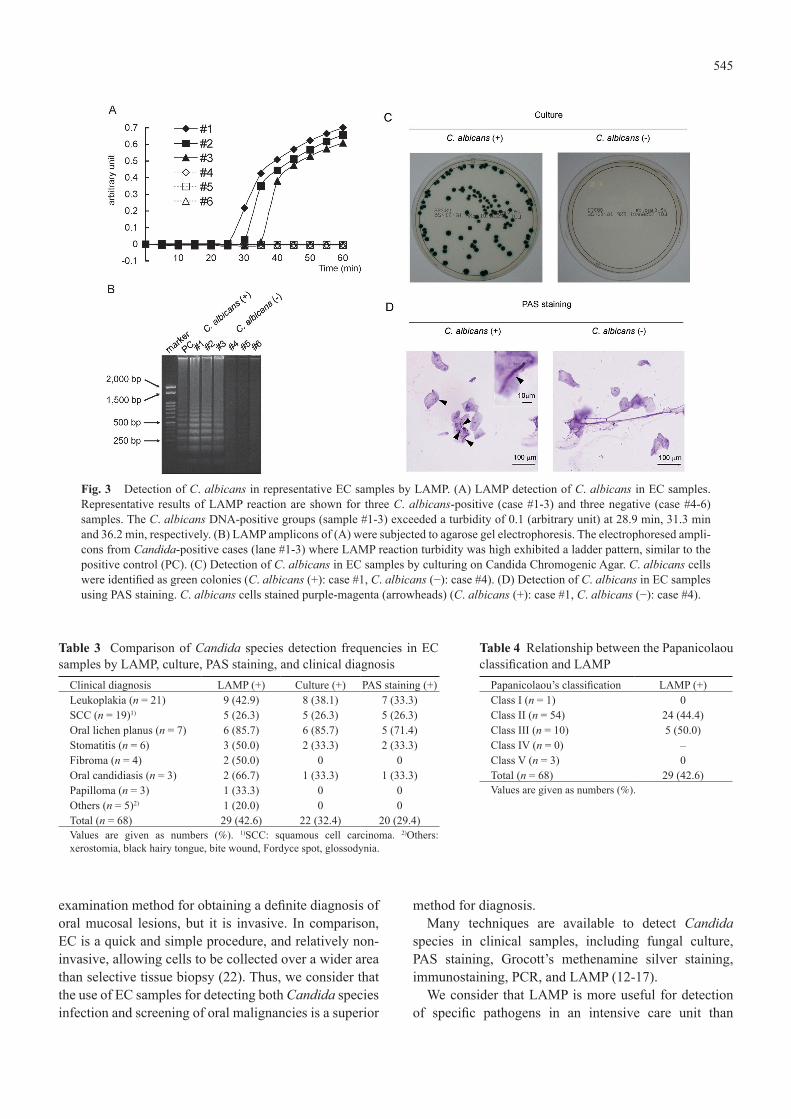
The LAMP analysis detected C. albicans DNA in 42.6% of EC samples. Culturing of the material from EC samples revealed that 32.4% of them contained C. albicans. The culture method also revealed the presence of non-albicans species, including C. glabrata (in four samples) and C. tropicalis (in one sample). PAS staining identified Candida species in 29.4% of the examined
specimens (Fig. 2).The results of LAMP, culture, and PAS staining in
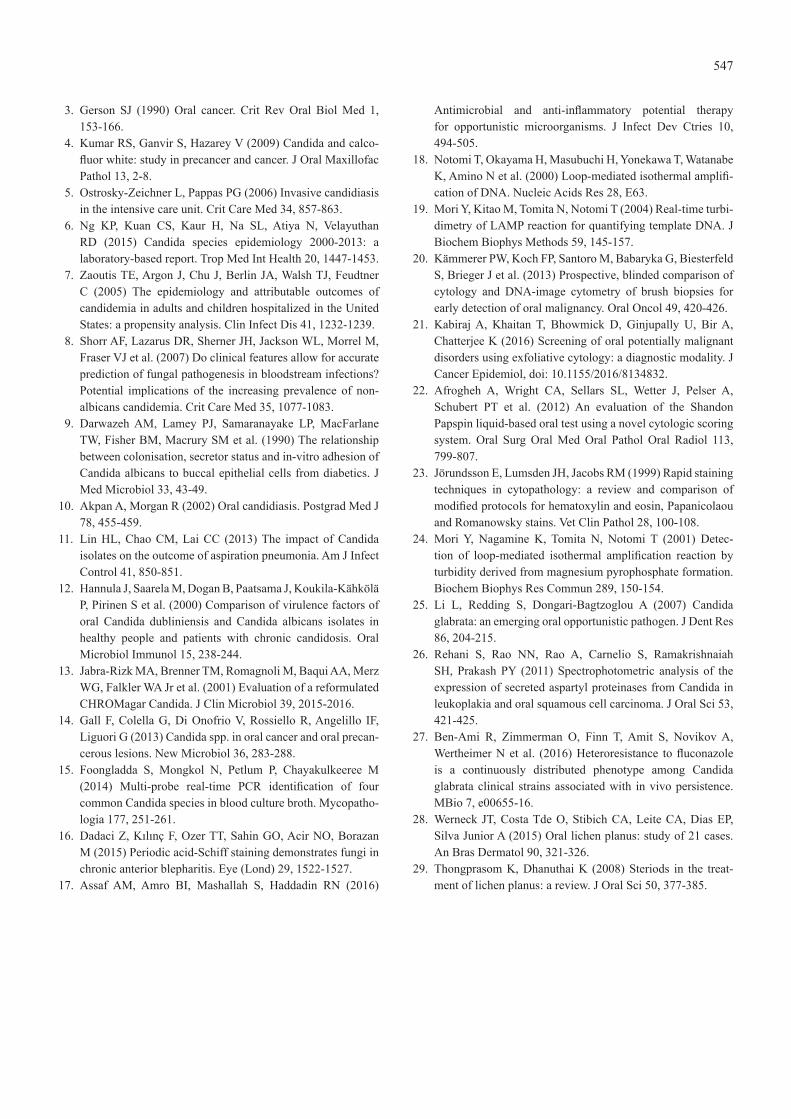
three C. albicans-positive (cases #1-3) and three nega-tive (cases #4-6) representative cases are shown in Fig. 3. C. albicans DNA was amplified in cases #1-3 but not in cases #4-6 (Fig. 3A). The results were confirmed by agarose gel electrophoresis (Fig. 3B). Moreover, culturing on Vitalmedia Color Candida Agar allowed identification of C. albicans colonies in cases #1-3 (Fig. 3C). The same samples were evaluated by PAS staining, and pseudohyphae were identified in the specimens from cases #1-3 (Fig. 3D).
The results of the LAMP reaction from each clinical diagnosis are listed in Table 3. The following percentages of samples were positive for C. albicans DNA: 42.9% of samples from patients with leukoplakia; 26.3% of squamous cell carcinoma (SCC) samples; 85.7% of OLP samples; 50.0% of fibroma samples; 50.0% of simple stomatitis samples; 66.7% of oral candidiasis samples; 33.3% of papilloma samples; and 20.0% of other samples. The C. albicans LAMP detection frequency was much higher than the frequency of detection based on culture and PAS staining (Table 3).
The relationship between C. albicans LAMP positivity and cytomorphometric evaluation is shown in Table 4. The LAMP reaction detected C. albicans in 44.4% of Class II samples and 50.0% of Class III samples, but not in Class I and Class V samples.
DiscussionCandida infection of oral mucosa causes a white lesion, which is important for differentiating oral malignancy and precursor lesions. Incision biopsy is a highly reliable
Fig. 1 The detection limit of LAMP. (A) To determine the detection limit of LAMP reactions, DNA was extracted from a C. albicans control strain, adjusted to the indicated concentrations, and LAMP was performed. The detection limit of LAMP was found to be 1 pg of DNA (consistent with 57 copies of C. albicans chromosome/tube). (B) Agarose gel electrophoretograms of LAMP amplicons (starting DNA concentrations from 1 ng to 1 pg), exhibiting a ladder pattern.
Fig. 2 Percentage of C. albicans-positive samples. LAMP analysis detected C. albicans DNA in 42.6% of EC samples. Culture from EC samples revealed that 32.4% of them contained C. albicans. PAS staining identified Candida species in 29.4% of examined specimens.
545
examination method for obtaining a definite diagnosis of oral mucosal lesions, but it is invasive. In comparison, EC is a quick and simple procedure, and relatively non-invasive, allowing cells to be collected over a wider area than selective tissue biopsy (22). Thus, we consider that the use of EC samples for detecting both Candida species infection and screening of oral malignancies is a superior
method for diagnosis.Many techniques are available to detect Candida
species in clinical samples, including fungal culture, PAS staining, Grocott’s methenamine silver staining, immunostaining, PCR, and LAMP (12-17).
We consider that LAMP is more useful for detection of specific pathogens in an intensive care unit than
Fig. 3 Detection of C. albicans in representative EC samples by LAMP. (A) LAMP detection of C. albicans in EC samples. Representative results of LAMP reaction are shown for three C. albicans-positive (case #1-3) and three negative (case #4-6) samples. The C. albicans DNA-positive groups (sample #1-3) exceeded a turbidity of 0.1 (arbitrary unit) at 28.9 min, 31.3 min and 36.2 min, respectively. (B) LAMP amplicons of (A) were subjected to agarose gel electrophoresis. The electrophoresed ampli-cons from Candida-positive cases (lane #1-3) where LAMP reaction turbidity was high exhibited a ladder pattern, similar to the positive control (PC). (C) Detection of C. albicans in EC samples by culturing on Candida Chromogenic Agar. C. albicans cells were identified as green colonies (C. albicans (+): case #1, C. albicans (−): case #4). (D) Detection of C. albicans in EC samples using PAS staining. C. albicans cells stained purple-magenta (arrowheads) (C. albicans (+): case #1, C. albicans (−): case #4).
Table 3 Comparison of Candida species detection frequencies in EC samples by LAMP, culture, PAS staining, and clinical diagnosis
Clinical diagnosis LAMP (+) Culture (+) PAS staining (+)Leukoplakia (n = 21) 9 (42.9) 8 (38.1) 7 (33.3)SCC (n = 19)1) 5 (26.3) 5 (26.3) 5 (26.3)Oral lichen planus (n = 7) 6 (85.7) 6 (85.7) 5 (71.4)Stomatitis (n = 6) 3 (50.0) 2 (33.3) 2 (33.3)Fibroma (n = 4) 2 (50.0) 0 0Oral candidiasis (n = 3) 2 (66.7) 1 (33.3) 1 (33.3)Papilloma (n = 3) 1 (33.3) 0 0Others (n = 5)2) 1 (20.0) 0 0Total (n = 68) 29 (42.6) 22 (32.4) 20 (29.4)Values are given as numbers (%). 1)SCC: squamous cell carcinoma. 2)Others: xerostomia, black hairy tongue, bite wound, Fordyce spot, glossodynia.
Table 4 Relationship between the Papanicolaou classification and LAMP
Papanicolaou’s classification LAMP (+)Class I (n = 1) 0Class II (n = 54) 24 (44.4)Class III (n = 10) 5 (50.0)Class IV (n = 0) –Class V (n = 3) 0Total (n = 68) 29 (42.6)Values are given as numbers (%).

546
other methods because of its shorter running time. Furthermore, the detection limit of the LAMP reaction is as low as 1 pg of DNA, equivalent to 57 copies of the C. albicans chromosome. In this study, the threshold time was prolonged along with template DNA dilution (28.8 min for a sample containing 1 ng; 39.3 min for 100 pg; 42.1 min for 10 pg; 47.3 min for 1 pg). The results were compatible with those of a previous study that had revealed the relationship between the template DNA concentration and threshold time (19).
In this study, LAMP evaluation of EC samples detected C. albicans in 42.6% of cases, which was higher than the detection rate for culturing (32.4%) and PAS staining (29.4%).
Vitalmedia Color Candida Agar is able to detect various Candida species, and not only C. albicans. In the present study, four samples contained C. glabrata, and one sample contained C. tropicalis. Identification of non-albicans species is an advantage of fungal culture; however, at least 2 days were required before the result could be obtained. Candida identification by the LAMP method is advantageous because of its rapid and specific amplification of C. albicans. Although the LAMP method used in this study is not able to detect non-albicans species, it is still clinically significant because of 1) rapid identification and 2) the predominance of C. albicans.
PAS staining of EC samples is a useful method of iden-tifying Candida species directly, under the microscope. However, it requires a complicated staining procedure and diagnostic capability, in contrast to LAMP. In this study, PAS staining detected Candida species in 29.4% of EC samples, which was lower than the rate for LAMP (42.6%) and culture (32.4%). These results indicate the difficulty of detecting Candida species by microscopic examination, even by a skilled pathologist.
Non-albicans fungi have been detected more frequently in recent years (5,25). In this study, the LAMP reaction and culture method detected C. albicans as the predominant species in EC samples. In vitro studies have shown that the adhesion of non-albicans species to buccal epithelial and vascular endothelial cells is weaker than that of C. albicans (26). C. glabrata, which is the second most frequently isolated fungus causing single infections or combined infections with C. albicans, causes persistent infections in patients treated with fluco-nazole and often acquires resistance to antifungal drugs (27). Because the sensitivity to antifungal drugs varies, identification of Candida species is important for treat-ment of candidiasis, allowing physicians to prescribe the appropriate antifungal drug.
Representative cases of C. albicans-positive and nega-
tive samples are shown in Fig. 3. The turbidity of three C. albicans DNA-positive samples exceeded 0.1 arbitrary units at 28.9 min, 31.3 min, and 36.2 min. However, the C. albicans DNA-negative samples showed no amplifica-tion (Fig. 3A). These data suggest that the LAMP method is reliable for clinical application to oral mucosal lesions.
The highest C. albicans positivity was observed for OLP samples (85.7%), which may suggest an appropriate treatment plan for these lesions using steroids. Similar results were reported in previous studies (28). The higher detection ratio of C. albicans in OLP might be associated with the use of steroids for treating these lesions (28,29). Unexpectedly, we found a relatively low fungal detection ratio in oral candidiasis samples. The detection ratio was also low in leukoplakia and SCC samples.
Although the Candida positivity rate was higher in Class II (44.4%) and III (50.0%) than in Class I (0.0%), and Class V (0.0%), the sample size was small in the Class I and V groups. Thus, more extensive investigations are required to verify the precise relationship between the Papanicolaou classification and the Candida positivity ratio.
The combination of EC and LAMP is considered to be a highly useful diagnostic system in areas where access to healthcare facilities is limited, because this system is non-invasive, requires less time for diagnosis, and does not require costly apparatus. These results suggest that rapid and accurate detection of C. albicans by the LAMP method could enable immediate initiation of treatment for oral candidiasis.
AcknowledgmentsWe would like to thank Prof. Kazuo Komiyama for technical advice and for reviewing the manuscript. This study was supported, in part, by Grants from Dental Research Center (2016), Sato Fund (2016), and Uemura Fund (2016), Nihon University School of Dentistry.
Conflict of interestThe authors have no conflict of interest to declare.
References 1. Wiesner SM, Bendel CM, Hess DJ, Erlandsen SL, Wells CL
(2002) Adherence of yeast and filamentous forms of Candida albicans to cultured enterocytes. Crit Care Med 30, 677-683.
2. Pfaller MA, Diekema DJ, Gibbs DL, Newell VA, Ellis D, Tullio V et al. (2010) Results from the ARTEMIS DISK global antifungal surveillance study, 1997 to 2007: a 10.5-year analysis of susceptibilities of Candida species to fluconazole and voriconazole as determined by CLSI standardized disk diffusion. J Clin Microbiol 48, 1366-1377.
547
3. Gerson SJ (1990) Oral cancer. Crit Rev Oral Biol Med 1, 153-166.
4. Kumar RS, Ganvir S, Hazarey V (2009) Candida and calco-fluor white: study in precancer and cancer. J Oral Maxillofac Pathol 13, 2-8.
5. Ostrosky-Zeichner L, Pappas PG (2006) Invasive candidiasis in the intensive care unit. Crit Care Med 34, 857-863.
6. Ng KP, Kuan CS, Kaur H, Na SL, Atiya N, Velayuthan RD (2015) Candida species epidemiology 2000-2013: a laboratory-based report. Trop Med Int Health 20, 1447-1453.
7. Zaoutis TE, Argon J, Chu J, Berlin JA, Walsh TJ, Feudtner C (2005) The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis 41, 1232-1239.
8. Shorr AF, Lazarus DR, Sherner JH, Jackson WL, Morrel M, Fraser VJ et al. (2007) Do clinical features allow for accurate prediction of fungal pathogenesis in bloodstream infections? Potential implications of the increasing prevalence of non-albicans candidemia. Crit Care Med 35, 1077-1083.
9. Darwazeh AM, Lamey PJ, Samaranayake LP, MacFarlane TW, Fisher BM, Macrury SM et al. (1990) The relationship between colonisation, secretor status and in-vitro adhesion of Candida albicans to buccal epithelial cells from diabetics. J Med Microbiol 33, 43-49.
10. Akpan A, Morgan R (2002) Oral candidiasis. Postgrad Med J 78, 455-459.
11. Lin HL, Chao CM, Lai CC (2013) The impact of Candida isolates on the outcome of aspiration pneumonia. Am J Infect Control 41, 850-851.
12. Hannula J, Saarela M, Dogan B, Paatsama J, Koukila-Kähkölä P, Pirinen S et al. (2000) Comparison of virulence factors of oral Candida dubliniensis and Candida albicans isolates in healthy people and patients with chronic candidosis. Oral Microbiol Immunol 15, 238-244.
13. Jabra-Rizk MA, Brenner TM, Romagnoli M, Baqui AA, Merz WG, Falkler WA Jr et al. (2001) Evaluation of a reformulated CHROMagar Candida. J Clin Microbiol 39, 2015-2016.
14. Gall F, Colella G, Di Onofrio V, Rossiello R, Angelillo IF, Liguori G (2013) Candida spp. in oral cancer and oral precan-cerous lesions. New Microbiol 36, 283-288.
15. Foongladda S, Mongkol N, Petlum P, Chayakulkeeree M (2014) Multi-probe real-time PCR identification of four common Candida species in blood culture broth. Mycopatho-logia 177, 251-261.
16. Dadaci Z, Kılınç F, Ozer TT, Sahin GO, Acir NO, Borazan M (2015) Periodic acid-Schiff staining demonstrates fungi in chronic anterior blepharitis. Eye (Lond) 29, 1522-1527.
17. Assaf AM, Amro BI, Mashallah S, Haddadin RN (2016)
Antimicrobial and anti-inflammatory potential therapy for opportunistic microorganisms. J Infect Dev Ctries 10, 494-505.
18. Notomi T, Okayama H, Masubuchi H, Yonekawa T, Watanabe K, Amino N et al. (2000) Loop-mediated isothermal amplifi-cation of DNA. Nucleic Acids Res 28, E63.
19. Mori Y, Kitao M, Tomita N, Notomi T (2004) Real-time turbi-dimetry of LAMP reaction for quantifying template DNA. J Biochem Biophys Methods 59, 145-157.
20. Kämmerer PW, Koch FP, Santoro M, Babaryka G, Biesterfeld S, Brieger J et al. (2013) Prospective, blinded comparison of cytology and DNA-image cytometry of brush biopsies for early detection of oral malignancy. Oral Oncol 49, 420-426.
21. Kabiraj A, Khaitan T, Bhowmick D, Ginjupally U, Bir A, Chatterjee K (2016) Screening of oral potentially malignant disorders using exfoliative cytology: a diagnostic modality. J Cancer Epidemiol, doi: 10.1155/2016/8134832.
22. Afrogheh A, Wright CA, Sellars SL, Wetter J, Pelser A, Schubert PT et al. (2012) An evaluation of the Shandon Papspin liquid-based oral test using a novel cytologic scoring system. Oral Surg Oral Med Oral Pathol Oral Radiol 113, 799-807.
23. Jörundsson E, Lumsden JH, Jacobs RM (1999) Rapid staining techniques in cytopathology: a review and comparison of modified protocols for hematoxylin and eosin, Papanicolaou and Romanowsky stains. Vet Clin Pathol 28, 100-108.
24. Mori Y, Nagamine K, Tomita N, Notomi T (2001) Detec-tion of loop-mediated isothermal amplification reaction by turbidity derived from magnesium pyrophosphate formation. Biochem Biophys Res Commun 289, 150-154.
25. Li L, Redding S, Dongari-Bagtzoglou A (2007) Candida glabrata: an emerging oral opportunistic pathogen. J Dent Res 86, 204-215.
26. Rehani S, Rao NN, Rao A, Carnelio S, Ramakrishnaiah SH, Prakash PY (2011) Spectrophotometric analysis of the expression of secreted aspartyl proteinases from Candida in leukoplakia and oral squamous cell carcinoma. J Oral Sci 53, 421-425.
27. Ben-Ami R, Zimmerman O, Finn T, Amit S, Novikov A, Wertheimer N et al. (2016) Heteroresistance to fluconazole is a continuously distributed phenotype among Candida glabrata clinical strains associated with in vivo persistence. MBio 7, e00655-16.
28. Werneck JT, Costa Tde O, Stibich CA, Leite CA, Dias EP, Silva Junior A (2015) Oral lichen planus: study of 21 cases. An Bras Dermatol 90, 321-326.
29. Thongprasom K, Dhanuthai K (2008) Steriods in the treat-ment of lichen planus: a review. J Oral Sci 50, 377-385.


















