Rapid and Massive Virus-Specific Plasmablast Responses ...
9
Rapid and Massive Virus-Specific Plasmablast Responses during Acute Dengue Virus Infection in Humans Jens Wrammert, Emory University Nattawat Onlamoon, Mahidol University Rama Akondy, Emory University Guey Chuen 'Oscar' Perng, Emory University Korakot Polsrila, Mahidol University Anmol Chandele, Emory University Marcin Kwissa, Emory University Bali Pulendran, Emory University Patrick C. Wilson, University of Chicago Orasri Wittawatmongkol, Mahidol University Only first 10 authors above; see publication for full author list. Journal Title: Journal of Virology Volume: Volume 86, Number 6 Publisher: American Society for Microbiology | 2012-03, Pages 2911-2918 Type of Work: Article | Final Publisher PDF Publisher DOI: 10.1128/JVI.06075-11 Permanent URL: http://pid.emory.edu/ark:/25593/cx6cc Final published version: http://dx.doi.org/10.1128%2FJVI.06075-11 Copyright information: © 2012, American Society for Microbiology. All Rights Reserved. Accessed October 4, 2021 12:14 AM EDT
Transcript of Rapid and Massive Virus-Specific Plasmablast Responses ...

Rapid and Massive Virus-Specific PlasmablastResponses during Acute Dengue Virus Infection inHumansJens Wrammert, Emory UniversityNattawat Onlamoon, Mahidol UniversityRama Akondy, Emory UniversityGuey Chuen 'Oscar' Perng, Emory UniversityKorakot Polsrila, Mahidol UniversityAnmol Chandele, Emory UniversityMarcin Kwissa, Emory UniversityBali Pulendran, Emory UniversityPatrick C. Wilson, University of ChicagoOrasri Wittawatmongkol, Mahidol University
Only first 10 authors above; see publication for full author list.
Journal Title: Journal of VirologyVolume: Volume 86, Number 6Publisher: American Society for Microbiology | 2012-03, Pages 2911-2918Type of Work: Article | Final Publisher PDFPublisher DOI: 10.1128/JVI.06075-11Permanent URL: http://pid.emory.edu/ark:/25593/cx6cc
Final published version: http://dx.doi.org/10.1128%2FJVI.06075-11
Copyright information:© 2012, American Society for Microbiology. All Rights Reserved.
Accessed October 4, 2021 12:14 AM EDT

Rapid and Massive Virus-Specific Plasmablast Responses during AcuteDengue Virus Infection in Humans
Jens Wrammert,a,b Nattawat Onlamoon,c,f Rama S. Akondy,a,b Guey C. Perng,a Korakot Polsrila,c Anmol Chandele,a Marcin Kwissa,a
Bali Pulendran,a Patrick C. Wilson,d Orasri Wittawatmongkol,e Sutee Yoksan,f,g Nasikarn Angkasekwinai,h Kovit Pattanapanyasat,c,f
Kulkanya Chokephaibulkit,e and Rafi Ahmeda,b
Emory Vaccine Center, School of Medicine, Emory University, Atlanta, Georgia, USAa; Department of Microbiology and Immunology, School of Medicine, Emory University,Atlanta, Georgia, USAb; Office for Research and Development, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailandc; Department of Medicine,Section of Rheumatology, The Committee on Immunology, The Knapp Center for Lupus and Immunology Research, University of Chicago, Chicago, Illinois, USAd;Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailande; Center for Emerging and Neglected Infectious Diseasesf andInstitute of Molecular Biosciences,g Mahidol University, Nakhon Pathom, Thailand; and Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University,Bangkok, Thailandh
Humoral immune responses are thought to play a major role in dengue virus-induced immunopathology; however, little isknown about the plasmablasts producing these antibodies during an ongoing infection. Herein we present an analysis of plas-mablast responses in patients with acute dengue virus infection. We found very potent plasmablast responses that often in-creased more than 1,000-fold over the baseline levels in healthy volunteers. In many patients, these responses made up as much30% of the peripheral lymphocyte population. These responses were largely dengue virus specific and almost entirely made up ofIgG-secreting cells, and plasmablasts reached very high numbers at a time after fever onset that generally coincided with the win-dow where the most serious dengue virus-induced pathology is observed. The presence of these large, rapid, and virus-specificplasmablast responses raises the question as to whether these cells might have a role in dengue immunopathology during theongoing infection. These findings clearly illustrate the need for a detailed understanding of the repertoire and specificity of theantibodies that these plasmablasts produce.
Dengue virus causes an infection with symptoms ranging froma mild fever to severe hemorrhagic fever with vascular leakage
that ranges in severity from minor subcutaneous bleeding to se-vere gastrointestinal bleeding (5, 28, 34). A striking epidemiolog-ical and immunological characteristic of dengue fever (DF) is thatthe severe immunopathology is more likely to occur in individualswho have previously been infected with a heterologous denguevirus serotype (8, 29, 32). While the exact mechanism of this phe-nomenon remains to be fully elucidated, several hypotheses havebeen developed over the last few decades to explain the reason forthe exacerbated pathology observed in these patients. One of themain hypotheses revolves around a mechanism referred to asantibody-dependent enhancement (ADE) (14). This hypothesissuggests that during a secondary infection, cross-reactive yetpoorly cross-neutralizing antibodies produced against a previ-ously encountered serotype will mediate an increased infectivity,in addition to altering the host range of target cells. This mecha-nism has been extensively studied in vitro (6, 17, 20), and its im-portance in vivo is beginning to be elucidated (2, 10, 27). Anotherproposed hypothesis (22, 23) suggests that an enhanced infectiontogether with a potent T cell-mediated recall response producesmassive amounts of effector mediators (4, 11–13, 15, 16, 25), aso-called cytokine storm, that is responsible for the observed im-munopathology. These two mechanisms are not mutually exclu-sive and may in fact work in concert to cause the immunopathol-ogy of dengue disease.
While human T cell responses during acute dengue virus in-fection have been studied in some detail, much less is knownabout the B cell responses. Early studies in dengue patients showedthat increases in immunoglobulin-containing cells could be ob-served during infection and that these cells reached maximal
numbers near the time of subsidence of fever (7). It has also beenshown that total CD19� B cells increase during dengue virus in-fection and that these increases correlate with the presence of so-called atypical lymphocytes (19). In addition, a more recent studyof the global gene expression patterns in peripheral blood mono-nuclear cells (PBMCs) isolated from dengue hemorrhagic fever(DHF) patients showed an enrichment of plasmablast signaturesthat was accompanied by an increase of plasmablasts by flow cy-tometric analysis (30).
Here, we have analyzed the magnitude, kinetics, antigen spec-ificity, and isotype usage of the plasmablast responses induced inpediatric and adult patients with acute dengue virus infection. Wefound during the acute phase of the infection a very potent andrapid induction of virus-specific plasmablasts, which in somecases made up as much as 30% of total lymphocytes. The rapidexpansion of plasmablasts was observed in the infected patients ata time point that generally coincides with the subsidence of feverand the most serious symptoms. These findings suggest that thesecells and the antibodies that they produce might be involved indengue immunopathology. However, while suggestive, these find-ings also clearly illustrate the need for more detailed analyses ofthe plasmablasts and the antibodies that they produce during the
Received 20 August 2011 Accepted 23 December 2011
Published ahead of print 11 January 2012
Address correspondence to Jens Wrammert, [email protected].
Supplemental material for this article may be found at http://jvi.asm.org/.
Copyright © 2012, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JVI.06075-11
0022-538X/12/$12.00 Journal of Virology p. 2911–2918 jvi.asm.org 2911

acute phase of dengue virus infection to clearly define their poten-tial role in dengue immunopathology.
MATERIALS AND METHODSDengue patient cohort. Patients enrolled in this study were clinicallydiagnosed with dengue virus infection upon admission to Siriraj Hospitalin Bangkok, Thailand. The dengue virus infection was confirmed by aserotype-specific reverse transcription-PCR (RT-PCR) as well as severalother diagnostic tests (NS1 test, dengue-specific IgG and IgM test[enzyme-linked immunosorbent assay {ELISA}, or dipstick tests]). Rou-tine laboratory measurements (complete blood count [CBC], urine andblood chemistry) and clinical manifestations of dengue virus infectionwere recorded. A final diagnosis and severity classification were done atthe conclusion of the trial with a full review of all the clinical and labora-tory data. Information about the patient cohort is detailed in Table 1 andin Table S1 in the supplemental material. All studies were preapproved bythe Faculty of Medicine at Siriraj Hospital and the Emory institutionalreview boards.
PBMC and plasma isolation. PBMCs and plasma were isolated essen-tially as previously described (35). Briefly, blood samples were collected inVacutainer CPT tubes (Becton Dickinson [BD]). Plasma samples wereisolated from the CPT tubes and preserved at �80°C. The PBMCs werecollected, washed extensively, and resuspended in phosphate-buffered sa-line (PBS) with 2% fetal calf serum (FCS) for immediate use or frozen inliquid nitrogen in FCS with 10% dimethyl sulfoxide for subsequent anal-ysis.
Serological determination of primary or secondary dengue virus in-fection. Dengue IgM and IgG antibodies were detected by a modifiedELISA as described by Innis et al. (18). Briefly, microtiter plates (Nunc)were coated with 100 �l of goat antihuman IgM or IgG and stored at 4°C.Serum specimens were diluted at 1:100 (0.05% PBS–Tween [PBS-T], 3%skim milk), added to the plates, and incubated for 1 h at 37°C. Afterwashing, 50 �l of pooled dengue virus antigens diluted at 1:3 (0.05%PBS-T, 2% lipid-extracted normal human serum, 3% skim milk) was putinto each tested well, and the plate was incubated for 1 h at 37°C andwashed before adding 50 �l of anti-dengue virus complex (2H2) mono-clonal antibody diluted at 1:10,000. After 1 h at 37°C, plates were washedbefore adding 50 �l of the goat antimouse conjugate. Plates were read at492 nm using an ELISA reader (Powerwave 340; BioTek), and sampleswere considered positive at a 0.500 optical density (OD) absorbance.
Identification of dengue virus serotype. Dengue virus RNA was ex-tracted from patient plasma using a QIAamp viral RNA extraction kit(Qiagen, Hilden, Germany) according to the manufacturer’s instruction.Dengue virus serotype was determined by a multiplex nested PCR methodas previously described (36) with some modification. Briefly, RNA wassubjected to reverse transcription (RT) with primer DEUR (5=-GCTGTGTCACCCAGAATGGCCAT-3=), and a multiplex nested PCR with fourprimer pairs specific for the E region of each dengue virus serotype wasperformed. Four pairs of serotype-specific primers were used, includ-ing D1L (5=-GGGGCTTCAACATCCCAAGAG-3=) and D1R (5=-GCTTAGTTTCAAAGCTTTTTCAC-3=) for dengue virus serotype 1 (DENV-1), D2L (5=-ATCCAGATGTCATCAGGAAAC-3=) and D2R (5=-CCGGCTCTACTCCTATGATG-3=) for DENV-2, D3L (5=-CAATGTGCTTGAATACCTTTGT-3=) and D3R (5=-GGACAGGCTCCTCCTTCTTG-3=) forDENV-3, and D4L (5=-GGACAACAGTGGTGAAAGTCA-3=) and D4R(5=-GGTTACACTGTTGGTATTCTCA-3=) for DENV-4. The expectedsizes of the nested PCR products for DENV-1, DENV-2, DENV-3, andDENV-4 were 504 bp, 346 bp, 196 bp, and 143 bp, respectively.
Viral antigen. Purified DENV-2 particles were purchased from Mi-crobix Biosystems Inc. (catalog no. EL-22-02; Canada). According to themanufacturer, this preparation contains virus particles (DENV-2 strain16681) concentrated from tissue culture supernatants by precipitationand ultracentrifugation. The antigen is then purified by sucrose densitygradient centrifugation. Virus particles are separated from the sucrose-containing buffer by ultracentrifugation, and the antigen is resuspendedin medium 199, followed by inactivation at room temperature with form-aldehyde. For the final product formulation, the formaldehyde is neutral-ized by the addition of sodium bisulfite.
Analytical flow cytometry. Staining for analytical flow cytometry ofplasmablasts was performed on whole blood as previously described(35). Briefly, cells were stained with the appropriately titrated antibod-ies, followed by lysis of erythrocytes (catalog no. 349202; BD FACSlysing solution; Pharmingen) and fixation in 2% phosphonoformicacid. All antibodies were purchased from Pharmingen (CD19-fluorescein isothiocyanate [555412], CD38-phycoerythrin [555460],CD3-peridinin chlorophyll protein [PerCP; 340663], CD20-PerCP[347674]), except anti-CD27-allophycocyanin (17-0279-73), whichwas purchased from eBiosciences. Plasmablasts were defined herein asCD19� CD3� CD20�/low CD27high CD38high cells gated on an ex-tended lymphocyte gate to include blasting cells. Flow cytometry datawere analyzed using FlowJo software. Absolute cell numbers per vol-ume blood were calculated using the BD Trucount Tubes bead system(catalog no. 340334BD; eBiosciences) according to the manufacturer’sprotocol.
ELISPOT assay. Direct enzyme-linked immunosorbent spot(ELISPOT) assay to enumerate either dengue virus-specific or total IgG-,IgM-, and IgA-secreting plasmablasts present in the PBMC samples wasperformed as previously described (9, 35). Briefly, 96-well ELISPOT assayfilter plates (MAHA N4510; Millipore) were coated overnight either withthe optimized amounts of purified dengue virions as described above (10�g/ml) or with polyvalent goat anti-human immunoglobulins (10 �g/ml;catalog no. 109-005-064; Jackson ImmunoResearch) in PBS. Plates werewashed and blocked by incubation with RPMI containing 10% FCS at37°C for 2 h. Purified and extensively washed PBMCs were added to theplates in dilution series starting at 10 � 105, diluted 3- to 5-fold down theplate, and incubated overnight. Plates were washed with PBS, followed byPBS containing 0.05% Tween, and then incubated with either a biotinyl-ated anti-human IgG antibody (catalog no. H10015; Invitrogen), anti-human IgA (catalog no. H14015; Invitrogen), or anti-human IgM (cata-log no. H15015; Invitrogen) for 1.5 h at room temperature. After washing,the plates were incubated with an avidin D-horseradish peroxidase con-jugate (catalog no. A-2004; Vector Laboratories) and finally developedusing 3-amino-9-ethyl-carbazole (AEC) substrate (Sigma). Developedplates were scanned and analyzed using an automated ELISPOT counter(CTL, Cellular Technologies Ltd.).
TABLE 1 Summary of dengue patients enrolled in the studya
Characteristic DF DHFb
Total no. of patients 28 18No. of males/no. of females 20/8 10/8Age (yr)c 17 (1–50) 20 (7–40)Fever day of sampled 6 (2–8) 6 (3–8)No. of patients infected with dengue
virus serotypee:1 8 72 10 43 7 64 0 0
a Patients were diagnosed on the basis of serology (dengue virus-specific RT-PCR, NS1test, dengue virus-specific IgG/IgM test, clinical measurements [CBC, urine and bloodchemistry]) and clinical manifestations of dengue virus infection.b One of the 18 DHF cases was classified as DSS (DHF class III).c Median age is shown with the range in parentheses.d Median day after fever onset on which the blood sample was obtained. Ranges are inparentheses.e Serotype determination by RT-PCR. Four patients were negative by this assay butclassified as having dengue on the basis of other clinical measurements, determined asdescribed in footnote a.
Wrammert et al.
2912 jvi.asm.org Journal of Virology

ELISA. Direct ELISA was performed by coating ELISA plates over-night with either anti-human Ig (catalog no. 109-005-064; Jackson Im-munoResearch) or dengue virus antigen (as described above) at 10 mg/ml. Plates were washed with PBS with 0.5% Tween and blocked in PBSwith 10% FCS and 0.2% Tween. Serially diluted serum samples were thenadded to the plates, followed by incubation with a peroxidase-conjugatedanti-human IgG antibody (catalog no. H10015; Invitrogen), and werefinally developed using o-phenylenediamine substrate. Serum dilutionwas plotted versus the OD value at 492 nm, and the midpoint dilutionvalues were determined.
Statistical analysis. Data were collected and graphed using MS Exceland GraphPad Prism software. Data for each individual subject are pre-sented as a circle dot with a bar that represents the median of each group.An unpaired, two-tailed t test was used to determine the statistical signif-icance of the difference observed between groups. Spearman’s correlationcoefficient test was used to analyze the correlation observed between dif-ferent parameters.
RESULTS
The patient cohort in this study was comprised of individualsdiagnosed with dengue virus infection at Siriraj Hospital, Bang-kok, Thailand, from 2009 to 2011. Single blood samples were ob-tained 2 to 8 days after symptom onset and for some of the donorsalso at a convalescent-phase time point 1 month or later afterdischarge. Of 56 patients diagnosed clinically, 46 were confirmedto be infected with dengue virus (Table 1; see Table S1 in thesupplemental material), while 10 were found to have some other,nondengue, febrile illness. Those testing positive for dengue wereinfected with dengue virus serotype 1, 2, or 3, while none wereinfected with a dengue virus serotype 4 strain. This result is inconcordance with previous studies demonstrating the low preva-lence of DENV-4 in the area (21). Of the 46 confirmed denguecases, 28 were classified as having DF, 17 were classified as havingDHF class I and II, and 1 patient had dengue shock syndrome(DSS; DHF class III), according to the WHO criteria (34). Threeadditional patients were also enrolled in 2011, and we obtainedtwo consecutive blood samples during hospitalization. Serologicalanalyses showed that of the 46 dengue patients, only 4 weremounting primary responses, based on an IgM/IgG ratio lowerthan 1.7 (18) (see Table S1 in the supplemental material). Thus,the majority of the patients enrolled in the study had had previousexposure to dengue virus and were mounting secondary immuneresponses.
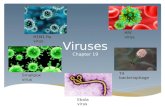
Potent and rapid plasmablast responses induced by denguevirus infection. Antibodies are thought to play a central role in thedevelopment of dengue immunopathology (2, 6, 10, 20). How-ever, relatively little is known about the magnitude or kinetics ofthe B cell responses induced during the acute phase of denguevirus infection. Figure 1A shows representative examples of theflow cytometric analysis of plasmablasts during the acute infec-tion. These patients demonstrated a massive induction of periph-eral plasmablasts, in some cases corresponding to as much as 30%of peripheral lymphocytes. Analysis of the overall set of patientsshowed that the majority had very high numbers of plasmablasts(Fig. 1B), averaging 47% of the peripheral B cells. At convalescentphase, 1 month after discharge, the numbers of peripheral plas-mablasts had returned to baseline levels, similar to those found inhealthy adults.
The magnitude of this response is striking, particularly com-pared with the immune responses to influenza booster vaccina-tion (peak, day 7; historical data from reference 35) or primary
infection (peak, days 11 to 14) with the live attenuated yellow fevervirus vaccine. While these results are derived from clinical studiesperformed in the United States (1, 24, 35) and therefore in differ-ent cohorts and settings, it is clear that the already sizeable plas-mablast responses observed in both these systems (Fig. 1D) aresignificantly smaller in magnitude than the responses observedduring dengue virus infection.
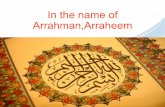
In terms of absolute numbers, several dengue patients carriedmore than 1 � 106 plasmablasts per ml of blood (median, 3.7 �105; Fig. 1C and 2A), which is a 1,000-fold increase over what isnormally observed in healthy individuals. Not surprisingly, theseresponses are of a similar magnitude regardless of what serotype ofdengue virus the patients were infected with (Fig. 1C). Althoughthis trial was not designed to be a detailed kinetic analysis, thetiming of collection of the samples that we analyzed providedinteresting information about the kinetics of this response. Sam-ples obtained on day 2 or 3 generally displayed relatively low num-bers of plasmablasts, often indistinguishable from the numbers insamples taken from healthy adults. However, as shown in Fig. 2A,the samples obtained from patients later after symptom onsetshowed a steady and dramatic increase of plasmablasts, reachingpeak numbers by day 6 or 7. This finding is substantiated by theanalysis of a small number of additional donors in a separate trial,where we found similar increases in consecutive blood samplestaken from the same donor. Thus, Fig. 2B shows an analysis ofthree donors from whom consecutive blood samples were ob-tained 2 days apart, where we saw a significant increase of plas-mablasts when comparing the earlier time point to the later one.The clinical diagnosis of DF or DHF did not correlate with themagnitude or kinetics of the plasmablast response (Fig. 2A), al-though this might have been confounded by the fact that all pa-tients were unwell enough to require hospital admission. Finally,the responses observed in the four donors who mounted primaryresponses (based on serological analyses) were similar to thoseobserved in the secondary responders (see Fig. S1 in the supple-mental material).
We conclude from these analyses that dengue virus infectioninduces a massive plasmablast response, often leading to increasesof more than 1,000-fold over the number observed in healthydonors. This increase occurs rapidly over several days after feveronset, with very high numbers reached at about day 6 or 7, in somecases generating a plasmablast pool that makes up as much as athird of all peripheral blood lymphocytes.
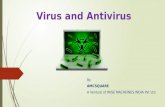
The majority of the plasmablast response during the acutephase of dengue virus infection is dengue virus specific. It hasbeen proposed not only that infection can lead to activation ofantigen-specific cells but also that the proinflammatory environ-ment could lead to the activation of both B and T cells in a non-specific manner, i.e., bystander activation (3, 31, 33). To deter-mine the extent to which the dengue virus infection-inducedplasmablast response was the result of antigen-specific or nonspe-cific bystander activation, we examined the specificity and isotypeusage of the antibodies that they produced using a dengue virus-specific ELISPOT assay (Fig. 3A). This analysis showed that theresponse was dominated by dengue virus-specific IgG-secretingcells, with several donors showing more than 105 dengue virus-specific IgG-secreting cells per 106 PBMCs. We also observed den-gue virus-specific IgA-secreting cells in most donors but at abouta 100-fold lower frequency. Finally, a small number of the donorshad detectable IgM-secreting plasmablast responses. Importantly,
Plasmablast Responses to Dengue Virus Infection
March 2012 Volume 86 Number 6 jvi.asm.org 2913

none of these were IgM only, and only one (donor Den01-066)had an IgM response that was larger than the IgG response in thesame donor. It is interesting to note that of the four donors iden-tified to be primary responders, all had detectable IgM responsesby ELISPOT assay. Of these, donor Den01-066 mentioned abovehad a very high serum IgM/IgG ratio (see Table S1 in the supple-mental material) and also showed the highest IgM response byELISPOT assay.
Comparing the number of specific and total IgG-secretingplasmablasts, we found that the majority of the IgG response wasindeed dengue virus specific, often with 70% or more of the IgG-secreting cells being specific for the virus (Fig. 3B and C). Thisfrequency is likely an underestimation, as these assays were per-formed using formalin-inactivated purified DENV-2. A large pro-portion of these responses are likely directed against proteins or
epitopes shared between the dengue virus serotypes, as no signif-icant difference in the frequency of virus-specific cells was seenbetween patients infected with DENV-2 and those with DENV-1or DENV-3 infections (see Fig. S2 in the supplemental material).The current study was aimed at understanding the overall im-mune responses induced by dengue virus infection, but futurestudies will be aimed at understanding the serotype-specific re-sponses and their functional properties. Figure 3B also shows re-sults for two patients, one with acute hepatitis A virus infectionand one with an unidentified febrile illness. Both patients showedsubstantial plasmablast responses; however, none of the inducedcells were dengue virus specific. When samples from patients re-turning 1 month after hospital discharge were analyzed, plasma-blast numbers had returned to baseline. This illustrates that theseresponses are transient in peripheral blood, likely reflecting sub-
FIG 1 Potent plasmablast responses induced during acute dengue virus infection. Plasmablast responses in peripheral blood of healthy controls or patientsdiagnosed with dengue fever (retrospectively confirmed to be dengue) were measured by flow cytometry. A subset of the patients came back for testing of afollow-up blood sample 1 month after discharge. (A) Representative flow cytometric analysis of the plasmablast frequency in four patients during ongoingdengue virus infection and 1 month after resolution. Plasmablasts are defined herein as CD19� CD3� CD20�/low CD38hi CD27hi cells. All plots shown are gatedon CD3� CD20�/low lymphocytes, including blasting cells. The numbers in the plots represent the percentage of that gate, while numbers in parentheses are thepercentage of all lymphocytes. (B) Summary of the frequency of plasmablasts, as a fraction of total CD19� B cells, in samples obtained from healthy adults,patients with ongoing dengue virus infection, and dengue patients returning after at least 1 month after clearance of infection. Statistical analysis was performedusing an unpaired, two-tailed t test. (C) Magnitude of the plasmablast response as absolute numbers in patients infected with different dengue viral serotypes.Statistical analysis was done using an unpaired, two-tailed t test. ND, not detected; ns, not significant. (D) Comparison of the magnitude of the dengue virusinfection-induced plasmablast responses to that observed after vaccination with either the inactivated influenza virus vaccine (which induces a recall responsethat peaks at 7 days after vaccination [35]) or the live attenuated yellow fever virus (YFV) vaccine (which induces a primary response that peaks at day 11/14 aftervaccination). Statistical analysis was done using an unpaired, two-tailed t test.
Wrammert et al.
2914 jvi.asm.org Journal of Virology

stantial cell death as well as migration to tissues capable of long-term maintenance of plasma cells, such as the bone marrow.
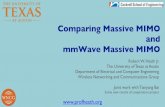
Analyzing the serological responses induced at the same timepoint as the plasmablast analyses showed that there were hightiters of dengue virus-specific IgG present during the acute phaseof the infection (Fig. 4A). All the infected patients had very highlevels of dengue virus-specific antibody, but there was a wide vari-ability between individuals. Of interest, the two patients with pri-
mary infection (based on the IgG/IgM ratios) showed very lowoverall titers at this time point. Furthermore, as expected, amongthe healthy adult controls from Thailand, 2/3 had detectable titers,whereas the healthy controls from the United States were sero-negative. Finally, comparing the dengue virus-specific serologicalresponses to the plasmablast responses, we found that they corre-lated well, as shown in Fig. 4B and C.
Given the size and isotype of the plasmablast response, it mightbe expected that these patients show evidence of hypergam-maglobulinemia. To this end, we also measured the total IgG inthese patients and healthy controls. However, no significant dif-ferences were observed (data not shown) between the patients andthe healthy controls.
Collectively, this study shows that dengue virus infection in-duced a very potent virus-specific plasmablast response in nearlyall of the patients (93%). These responses are dominated by IgG-secreting cells and increased as much as 1,000-fold in magnitude,reaching maximal numbers by day 6 or 7 after fever onset. Thesefindings regarding the magnitude and specificity of the plasma-blast responses during the acute phase of dengue virus infectionprompt more in-depth analyses of plasmablast responses with re-gard to the repertoire breadth and fine specificity of the antibodiesthat they produce, as well as their possible involvement in dengue-induced immunopathology.
DISCUSSION
In an effort to analyze the plasmablast responses induced duringthe acute phase of dengue virus infection, we have examined acohort of patients from both pediatric and adult clinics identifiedat Siriraj Hospital in Bangkok. This patient group contained bothpatients with mild symptoms (DF) and patients with more severesymptoms (DHF). We found very potent plasmablast responsesinduced in almost all of the dengue virus-infected donors. Inmany cases, these responses completely dominated the B cell com-partment (often as much as 80% of the CD19� B cells were plas-mablasts), making up as much as 30% of the total peripheral lym-phocytes. In contrast, by way of comparison to U.S. volunteersreceiving the influenza vaccine (35) or a primary vaccination withthe yellow fever vaccine, we find much smaller responses, on theorder of 2 to 3% of the total CD19� B cells. The magnitude of theplasmablast response during dengue virus infection correlatedwith the time following the onset of febrile symptoms. Thus, mostsamples taken 2 to 3 days after fever onset showed a barely detect-able response, but over time the response increased to the massiveresponses observed in samples obtained on day 6 or 7. These find-ings were substantiated by additional analysis of three donorsfrom whom two samples were obtained 2 days apart, whichshowed a similar increase with time.
Importantly, ELISPOT assay analysis showed that the major-ity, often 80% or more, of the dengue virus-induced plasmablastswere secreting dengue virus-specific IgG. This suggests that thesecells were induced by interaction with their cognate antigen andwere not the result of nonspecific, bystander mechanisms. Inter-estingly, even though we used a DENV-2 clone for detection ofantigen-specific cells in the ELISPOT assay, there was little differ-ence in the relative frequency of antigen-specific cells over totalIgG-secreting cells in patients infected with DENV-1 or -3 com-pared to patients infected with DENV-2 (see Fig. S2 in the supple-mental material). This indicates that most of the plasmablast cellsinduced by infection are specific for proteins or epitopes present
FIG 2 Rapid expansion of plasmablast responses during acute dengue virusinfection. (A) Absolute plasmablast numbers per ml blood (calculated using abead-based [TruCount; BD] system) for all the donors analyzed as a functionof number of days after fever onset. Spearman’s correlation coefficient test wasused to analyze the correlation observed between different parameters for allthe data points. Similar results were obtained when each subgroup was ana-lyzed individually. (B) Plasmablast responses in peripheral blood in three pa-tients diagnosed with and confirmed to have dengue fever infection were mea-sured by flow cytometry at two consecutive time points with 2 days betweensample collections. Plots show cells gated for CD3� CD20�/low cells with theCD27hi CD38hi plasmablasts marked by a box. The frequency of these plas-mablasts is shown next to the box, and the frequency of total lymphocytes isshown in parentheses.
Plasmablast Responses to Dengue Virus Infection
March 2012 Volume 86 Number 6 jvi.asm.org 2915

in multiple serotypes. Future studies, on a monoclonal level, areneeded to identify what protein/epitope these responses target,what proportion of these responses are functionally active, andhow this activity correlates with serotype specificity.
Patients returning to the hospital for a follow-up visit about 1month after discharge showed essentially baseline numbers ofplasmablasts by flow cytometry with no dengue virus-specific cellsby ELISPOT assay. This demonstrates that these cells are present
in the peripheral circulation only for a relatively short time, likelyrepresenting either contraction through extensive cell death ormigration of at least a subset of these cells to tissues where long-term antibody production can be sustained, such as bone marrowor secondary lymphoid tissues. Furthermore, while patients suf-fering from other febrile illnesses often showed sizeable numbersof plasmablasts in the periphery, these cells were not dengue virusspecific by the ELISPOT assay.
FIG 3 The majority of the plasmablasts induced by dengue virus infection are virus specific. Plasmablast responses in peripheral blood were measured byELISPOT analysis during infection and 1 month after discharge. (A) Graphs showing the number of IgG-, IgA-, or IgM-secreting dengue virus-specificplasmablasts per million PBMCs. ELISPOT assay plates were coated with purified 16681 DENV-2 antigen. (B) Representative IgG-specific ELISPOT analysis oftwo dengue virus-infected patients, two patients with other acute febrile illnesses, a dengue patient returning for a 1-month follow-up, and a healthy control.Upper row, dengue virus-specific IgG spots; lower row, total IgG-secreting cells. From left to right, the numbers of cells plated was 823, 823, 2,489, 7,407, 66,000,and 66,000 PBMCs. The number given below each well is the spot count for that well. Relative frequency (percent) of dengue virus-specific IgG-secretingplasmablasts over total IgG secreting plasmablasts is also shown. (C) Summary of the number of total IgG-secreting cells and dengue virus-specific IgG-secretingcells for all the donors analyzed. The entire bar (black and white together) represents the total number of IgG-secreting cells per million PBMCs, while thenumbers of dengue virus-specific IgG-secreting cells are marked in black only. Shown above each bar is the percentage of dengue virus-specific cells over totalIgG-secreting cells.
Wrammert et al.
2916 jvi.asm.org Journal of Virology

The patient cohort studied here almost exclusively representedsecondary exposures to dengue virus, based on serological analy-ses (see Table S1 in the supplemental material) as well as the factthat the virus is endemic in this area. In fact, the vast majority ofthe population in this region seroconverts very early in life (8).Although the few primary cases identified in the current cohortshowed responses similar to those of the overall cohort, they weretoo few to be able to reach a solid conclusion regarding differencesbetween the responses induced in primary versus secondary re-sponses. Ongoing studies of primary dengue virus infection inareas where the virus is not endemic will determine how these datacompare to primary immune responses in terms of magnitude,kinetics, and isotype distribution in the plasmablast response.
Acute infection with dengue virus results in symptoms rangingfrom a mild fever to severe vascular leakage and massive internalbleeding. Interestingly, epidemiological studies suggest that theimmunological history might be important for the outcome ofinfection, such that while a primary exposure to this virus gener-ally leads to a mild disease and lifelong protection against thatserotype, a subsequent exposure to a heterologous strain cansometimes lead to the more severe form of dengue, with the ac-companying hemorrhagic symptoms described above. Both T and
B cell-mediated mechanisms have been implicated in dengue-induced immunopathogenesis, but the importance of either ofthese mechanisms has not been fully characterized in vivo (23).Recently, two papers have also described dengue virus-specificmemory B cells at convalescent-phase time points and character-ized the antibodies that the memory B cells produce (2, 10). How-ever, studies describing the antibodies produced by respondingplasmablasts during the acute phase of the infection have not beenreported. Ongoing studies to clearly define the repertoire breadthof the infection-induced plasmablasts, the epitopes that they rec-ognize, and their ability to cause immunopathology by ADE-likeresponses at a monoclonal level will provide further insight intothe role of these cells.
In addition to their role in binding antigen, antibodies are ableto regulate immune responses through interaction with severaldifferent Fc receptors, a function that is directly dependent ontheir Fc-region glycosylation pattern. Recent studies (reviewed inreference 26) have clearly shown that glycosylation patterns regu-lated on IgG can mediate pro- or anti-inflammatory functions.These findings suggest a mechanism for ensuring that steady-stateserum IgG maintains an anti-inflammatory state, while, in con-trast, upon antigenic challenge by a pathogen, the antigen-specific
FIG 4 Dengue virus-specific serum antibody correlates with the observed plasmablast responses. ELISA analysis of serum samples obtained from the acutelyinfected dengue patients as well as healthy control samples. This group of samples was from 17 cases of secondary infection, 2 primary cases (based on IgG/IgMratios, as described in the text), and 3 healthy Thai and 2 healthy U.S. volunteers. Dengue virus-specific IgG was measured by direct ELISA using the same denguevirus antigen used for the ELISPOT analysis of the cellular responses described in the legend to Fig. 3. (A) ELISA measurement of total dengue virus-specific IgG.Midpoint dilution values were determined as the intersection of the dotted line at 50% of the OD value and the ELISA binding curves. (B and C) Correlation ofthe serological responses (as determined by the midpoint dilution value determined in panel A) and the plasmablast response by absolute plasmablasts in blood(flow cytometry) (B) and dengue virus-specific plasmablasts by ELISPOT assay (C).
Plasmablast Responses to Dengue Virus Infection
March 2012 Volume 86 Number 6 jvi.asm.org 2917

IgG antibodies produced can mediate a more proinflammatorystate. Given the large antibody-secreting cell responses that wehave observed in dengue patients, it is possible that the IgG pro-duced by the plasmablasts is also contributing to pathology byexacerbating the proinflammatory state in these patients. How-ever, while the dengue virus-infected patients showed very hightiters of dengue virus-specific antibody that were proportional tothe magnitude of the plasmablast response (Fig. 4), no overallincreases of total IgG were found in these patients (data notshown). Given the massive numbers of plasmablasts present inthese patients during the acute phase of infection, this would in-dicate that only a smaller number of them are able to survive longterm as long-lived plasma cells. It is unclear if this is due to the factthat the bone marrow can sustain only a smaller number of plasmacells or if the majority of the induced plasmablasts are predestinedto a short life span.
In conclusion, human dengue virus infection induces a veryrapid and potent plasmablast response, often dominating the Bcell compartment of these patients. We show that these responsesare largely dengue virus specific and almost entirely made up ofIgG-secreting cells and that they reach very large numbers at atime after fever onset that generally coincides with the windowwhere the most serious dengue virus-induced pathology is ob-served. The findings are suggestive of a role for these cells in den-gue immunopathogenesis. However, more detailed analyses of thefine specificity and functional properties of the antibodies thatthey produce would be needed to truly address this importantquestion.
ACKNOWLEDGMENTS
We thank Chris Chiu, Carl Davis, and Megan McCausland for criticalreading of the manuscript and S. Kongprasit, K. Intalapaporn, A. Malee-satharn, N. Kongstan, C. Utenpitak, and R. Arjwong for excellent techni-cal and clinical support.
This work was funded by National Institutes of Health (NIH)/Na-tional Institute of Allergy and Infectious Diseases (NIAID) grant U19-AI057266 and by the Office of the Higher Education Commission andMahidol University under the Thai National Research Universities Initia-tive. N.O. is supported by a Chalermphrakiat grant from the Faculty ofMedicine, Siriraj Hospital, Mahidol University. K.P. is a Thailand Re-search Fund Senior Research Scholar.
REFERENCES1. Akondy RS, et al. 2009. The yellow fever virus vaccine induces a broad
and polyfunctional human memory CD8� T cell response. J. Immunol.183:7919 –7930.
2. Beltramello M, et al. 2010. The human immune response to dengue virusis dominated by highly cross-reactive antibodies endowed with neutraliz-ing and enhancing activity. Cell Host Microbe 8:271–283.
3. Bernasconi NL, Traggiai E, Lanzavecchia A. 2002. Maintenance of sero-logical memory by polyclonal activation of human memory B cells. Sci-ence 298:2199 –2202.
4. Bethell DB, et al. 1998. Pathophysiologic and prognostic role of cytokinesin dengue hemorrhagic fever. J. Infect. Dis. 177:778 –782.
5. Bhamarapravati N, Tuchinda P, Boonyapaknavik V. 1967. Pathology ofThailand haemorrhagic fever: a study of 100 autopsy cases. Ann. Trop.Med. Parasitol. 61:500 –510.
6. Blackley S, et al. 2007. Primary human splenic macrophages, but not T orB cells, are the principal target cells for dengue virus infection in vitro. J.Virol. 81:13325–13334.
7. Boonpucknavig S, Lohachitranond C, Nimmanitya S. 1979. The patternand nature of the lymphocyte population response in dengue hemor-rhagic fever. Am. J. Trop. Med. Hyg. 28:885– 889.
8. Burke DS, Nisalak A, Johnson DE, Scott RM. 1988. A prospective studyof dengue infections in Bangkok. Am. J. Trop. Med. Hyg. 38:172–180.
9. Crotty S, Aubert RD, Glidewell J, Ahmed R. 2004. Tracking humanantigen-specific memory B cells: a sensitive and generalized ELISPOT sys-tem. J. Immunol. Methods 286:111–122.
10. Dejnirattisai W, et al. 2010. Cross-reacting antibodies enhance denguevirus infection in humans. Science 328:745–748.
11. Dung NT, et al. 2010. Timing of CD8� T cell responses in relation tocommencement of capillary leakage in children with dengue. J. Immunol.184:7281–7287.
12. Green S, et al. 1999. Early immune activation in acute dengue illness isrelated to development of plasma leakage and disease severity. J. Infect.Dis. 179:755–762.
13. Green S, et al. 1999. Elevated plasma interleukin-10 levels in acute denguecorrelate with disease severity. J. Med. Virol. 59:329 –334.
14. Halstead SB, O’Rourke EJ. 1977. Antibody-enhanced dengue virus in-fection in primate leukocytes. Nature 265:739 –741.
15. Hober D, Delannoy AS, Benyoucef S, De Groote D, Wattre P. 1996.High levels of sTNFR p75 and TNF alpha in dengue-infected patients.Microbiol. Immunol. 40:569 –573.
16. Hober D, et al. 1993. Serum levels of tumor necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), and interleukin-1 beta (IL-1 beta) in dengue-infected patients. Am. J. Trop. Med. Hyg. 48:324 –331.
17. Huang KJ, et al. 2006. The dual-specific binding of dengue virus andtarget cells for the antibody-dependent enhancement of dengue virus in-fection. J. Immunol. 176:2825–2832.
18. Innis BL, et al. 1989. An enzyme-linked immunosorbent assay to char-acterize dengue infections where dengue and Japanese encephalitis co-circulate. Am. J. Trop. Med. Hyg. 40:418 – 427.
19. Jampangern W, et al. 2007. Characterization of atypical lymphocytes andimmunophenotypes of lymphocytes in patients with dengue virus infec-tion. Asian Pac. J. Allergy Immunol. 25:27–36.
20. Kliks SC, Nisalak A, Brandt WE, Wahl L, Burke DS. 1989. Antibody-dependent enhancement of dengue virus growth in human monocytes asa risk factor for dengue hemorrhagic fever. Am. J. Trop. Med. Hyg. 40:444 – 451.
21. Klungthong C, Zhang C, Mammen MP, Jr, Ubol S, Holmes EC. 2004.The molecular epidemiology of dengue virus serotype 4 in Bangkok, Thai-land. Virology 329:168 –179.
22. Kurane I, et al. 1994. Immunopathologic mechanisms of dengue hem-orrhagic fever and dengue shock syndrome. Arch. Virol. Suppl. 9:59 – 64.
23. Mathew A, Rothman AL. 2008. Understanding the contribution of cellularimmunity to dengue disease pathogenesis. Immunol. Rev. 225:300–313.
24. Miller JD, et al. 2008. Human effector and memory CD8� T cell re-sponses to smallpox and yellow fever vaccines. Immunity 28:710 –722.
25. Mustafa AS, Elbishbishi EA, Agarwal R, Chaturvedi UC. 2001. Elevatedlevels of interleukin-13 and IL-18 in patients with dengue hemorrhagicfever. FEMS Immunol. Med. Microbiol. 30:229 –233.
26. Nimmerjahn F, Ravetch JV. 2010. Antibody-mediated modulation ofimmune responses. Immunol. Rev. 236:265–275.
27. Onlamoon N, et al. 2010. Dengue virus-induced hemorrhage in a non-human primate model. Blood 115:1823–1834.
28. Piyaratn P. 1961. Pathology of Thailand epidemic hemorrhagic fever.Am. J. Trop. Med. Hyg. 10:767–772.
29. Sangkawibha N, et al. 1984. Risk factors in dengue shock syndrome: aprospective epidemiologic study in Rayong, Thailand. I. The 1980 out-break. Am. J. Epidemiol. 120:653– 669.
30. Simmons CP, et al. 2007. Patterns of host genome-wide gene transcriptabundance in the peripheral blood of patients with acute dengue hemor-rhagic fever. J. Infect. Dis. 195:1097–1107.
31. Suwannasaen D, Romphruk A, Leelayuwat C, Lertmemongkolchai G.2010. Bystander T cells in human immune responses to dengue antigens.BMC Immunol. 11:47.
32. Thein S, et al. 1997. Risk factors in dengue shock syndrome. Am. J. Trop.Med. Hyg. 56:566 –572.
33. Tough DF, Borrow P, Sprent J. 1996. Induction of bystander T cell prolif-eration by viruses and type I interferon in vivo. Science 272:1947–1950.
34. World Health Organization. 1997. Dengue haemorrhagic fever: diagno-sis, treatment, prevention and control. World Health Organization, Ge-neva, Switzerland.
35. Wrammert J, et al. 2008. Rapid cloning of high-affinity human mono-clonal antibodies against influenza virus. Nature 453:667– 671.
36. Yenchitsomanus PT, et al. 1996. Rapid detection and identification ofdengue viruses by polymerase chain reaction (PCR). Southeast Asian J.Trop. Med. Public Health 27:228 –236.
Wrammert et al.
2918 jvi.asm.org Journal of Virology