Forlini artificial iris for large post traumatic iris coloboma pediatric
Upload
peter-goodwinCategory
view
214download
2
Ranibizumab for coloboma-related choroidalneovascular membrane in a childPeter Goodwin, MD,a Carol L. Shields, MD,a Aparna Ramasubramanian, MD,a Gary C. Brown, MD,b
and Jerry A. Shields, MDa
Optic nerve and retinochoroidal coloboma are caused by incom-plete closure of the embryonic fissure during fetal development.1 Af-fected patients carry a risk for retinal detachment and less so forchoroidal neovascular membranes (CNVM) secondary to the alteredanatomy. Because of the rarity of this condition and the even moreunusual occurrence of such complications, there are only a few casereports on the treatment of coloboma-related CNVM. Herein we re-port the results of ranibizumab and laser photocoagulation for colo-boma-related CNVM in a child.
Case Report
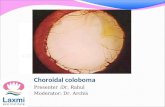
A3-month-old white male infant with left esotropiawas found to have bilateral symmetrical retino-choroidal coloboma involving the optic nerve
(Figure 1A). There was no retinal detachment. The childfixed and followed with both eyes and had normal papillaryreactions. At 19 months of age, the right fundus revealedsubtle subretinal hemorrhage at the temporal colobomamargin associated with an area of retinal pigment epithelialhyperplasia and subretinal fluid (Figure 1B). Fluoresceinangiography demonstrated choroidal neovascular mem-brane (CNVM) approximately 1 mm from the foveola(Figure 1C). Intravitreal ranibizumab 0.25 mg/0.025 mLwas injected due to the proximity of the CNVM to the fo-veola. At 8 weeks follow-up, resolution of the hemorrhageand subretinal fluid with reduction in the CNVM wasnoted. The patient did not undergo repeat fluorescein an-giography due to previous allergic reaction. A repeat injec-tion of ranibizumab 0.25 mg/0.025 mL was administeredcoupled with minimal ablative argon laser photocoagula-tion (200 mw power, 35 spots) to the regressed CNVMsparing the foveola. One year after initial therapy, theCNVM was regressed clinically, with no evidence of subre-tinal fluid or hemorrhage. There was no evidence of recur-
Author affiliations: aOcular Oncology and bRetina Service, Wills Eye Institute, ThomasJefferson University, Philadelphia, Pennsylvania
Support provided by the Retina Research Foundation of the Retina Society in CapeTown, South Africa (CLS), the Eye Tumor Research Foundation, Philadelphia, PA (CLS,JAS), Mellon Charitable Giving from the Martha W. Rogers Charitable Trust (CLS), thePaul Kayser International Award of Merit in Retina Research, Houston TX (JAS), andthe LuEsther Mertz Retina Research Foundation (CLS).
Submitted July 23, 2009.Revision accepted September 16, 2009.Reprint requests: Carol L. Shields, MD, Ocular Oncology Service, Suite 1440, Wills Eye
Institute, 840 Walnut Street, Philadelphia, PA 19107 (email: [email protected]).J AAPOS 2009;13:616-617.
Copyright � 2009 by the American Association for Pediatric Ophthalmology andStrabismus.
1091-8531/2009/$36.00 1 0doi:10.1016/j.jaapos.2009.09.009
616
rence and hence no further treatment was required(Figure 1D). During the entire course of treatment, theleft eye remained stable.
Discussion
CNVM is a well-documented complication of retinochor-oidal coloboma in both adults and infants. The CNVM isclassically found at the margin of the coloboma.1 It is pos-tulated that disruption of Bruch’s membrane at the marginof the coloboma provides a space into which choroidal ves-sels can proliferate. The subsequent leakage of serous fluidand hemorrhage is detectable on either clinical examina-tion or fluorescein angiography. The natural history ofCNVM ranges from spontaneous resolution to cata-strophic visual loss.2-4 Takenaka and colleagues2 reportedthe case of a 44-year-old woman who had spontaneous res-olution of CNVM arising at the margin of a coloboma.Gupta and colleagues4 reported the occurrence of a large(3 disk diameters) subfoveal CNVM in the only seeingeye of a 20-year-old man with coloboma who ultimatelyhad poor final visual outcome.
There have been several methods of treating coloboma-related CNVM, including focal laser photocoagulation,photodynamic therapy, and surgical removal. Anatomicsuccess with 1 or 2 sessions of ablative focal laser photoco-agulation has been reported and visual acuity outcomesrange from slight improvement to vision loss.5-7 The abilityto photocoagulate such CNVM is limited by its proximity tothe foveola. Photodynamic therapy was reported to be suc-cessful in 1 case of a 5-year-old girl with subfoveal CNVM.8
One publication of surgical removal of subfoveal coloboma-related CNVM did not report visual acuity outcome.9
The decision to use ranibizumab, an antivascular endo-thelial growth factor (VEGF), was based on several find-ings including presence of subretinal fluid and theCNVM location near the foveola, in an effort to minimizelong-term damage. In this case, the CNVM was located onthe temporal coloboma margin, approximately 1 mm fromthe undefined foveola. Laser photocoagulation was initiallyavoided due to the size of the CNVM, proximity to the fo-veola, and power needed to treat through subretinal fluid.After ranibizumab reduction in the CNVM and resolutionof fluid, minor laser power and spots were necessary. Othertreatments, such as photodynamic therapy, would havebeen impractical in a 19-month-old child and surgicalremoval might have involved visually threatening risks.
The successful use of anti-VEGF therapies in youngerpatients, most notably in neonates with retinopathy of pre-maturity,10 has allowed for application of this treatment to
Journal of AAPOS

FIG 1. A, Congenital retinochoroidal coloboma of the right eye in a 13-month-old child. No visible signs of choroidal neovascular membrane (CNVM)are seen. B, At 19 months of age, the retinal pigment epithelial (RPE) hyperplasia at the temporal coloboma margin was increased and focal shallowsubretinal fluid extending for 4 mm (arrow point) and subtle hemorrhage within the coloboma were noted. C, At 19 months of age, fluorescein an-giography showed leakage at the temporal margin of the coloboma, suggestive of CNVM. The patient was treated with 2 intravitreal ranibizumabinjections (0.25 mg/0.025 mL) followed by minimal focal laser photocoagulation. D, At 25 months, the CNVM, subretinal fluid, and hemorrhageremained resolved with preservation of the undefined fovea.
Volume 13 Number 6 / December 2009 Goodwin et al 617
other pediatric conditions. Cakir and colleagues11,12
reported 2 children with choroidal neovascular membranethat regressed following treatment with bevacizumab withdocumented improvement in visual acuity. Avery,13 in hiseditorial on anti-VEGF therapy, discussed the potentialuses of anti-VEGF in pediatric diseases. He also raisedconcern and demanded caution in the use of these powerfulagents, especially bevacizumab, which has a long systemichalf-life. In our case, anti-VEGF for coloboma-relatedCNVM was beneficial and allowed for minimal damageto the foveola.
References
1. Brown GC, Tasman WS. Congenital anomalies of the optic disc. NewYork: Grune and Stratton;1983:159-61.
2. Takenaka J, Yamane K, Minamoto A, Mishima HK, Hayashida H.Subretinal neovascularization associated with retinochoroidal colo-boma. Eur J Ophthalmol 2005;15:815-17.
3. Leff SR, Britton WA, Brown GC, Lucier AC, Brown JF. Retinochor-oidal coloboma associated with subretinal neovascularization. Retina1985;5:154-6.
4. Gupta V, Gupta A, Dogra MR. Subretinal neovascularization associ-ated with retinochoroidal coloboma. Indian J Ophthalmol 1997;45:116-17.
Journal of AAPOS
5. Spitzer M, Grisanti S, Bartz-Schmidt KU, Gelisken F. Choroidalneovascularization in retinochoroidal coloboma: Thermal laser treat-ment achieves long-term stabilization of visual acuity. Eye 2006;20:969-72.
6. Guirgis MF, Lueder GT. Choroidal neovascular membrane associ-ated with optic nerve coloboma in a patient with CHARGE associa-tion. Am J Ophthalmol 2003;135:919-20.
7. Yedavally S, Frank RN. Peripapillary subretinal neovascularizationassociated with coloboma of the optic nerve. Arch Ophthalmol1993;111:552-3.
8. von Eiken J, Hoh H, Rehfeldt K. Photodynamic therapy for choroidalneovascularization due to choroidal coloboma in a 51⁄2 -year-old child.Klin Monatsbl Augenheilkd 2007;22:140-45.
9. Uemura A, Thomas MA. Visual outcome after surgical removal ofchoroidal neovascularization in pediatric patients. Arch Ophthalmol2000;118:1373-8.
10. Mintz-Hittner HA, Kuffel RR Jr. Intravitreal injection of bevacizu-mab (avastin) for treatment of stage 3 retinopathy of prematurity inzone I or posterior zone II. Retina 2008;28:831-8.
11. Cakir M, Cekic O, Yilmaz OF. Intravitreal bevacizumab for idio-pathic choroidal neovascularization. J AAPOS 2009;13:296-8.
12. Cakir M, Cekic O, Yilmaz OF. Intravitreal bevacizumab and triam-cinolone treatment for choroidal neovascularization in Best disease.J AAPOS 2009;13:94-6.
13. Avery RL. Extrapolating anti-vascular endothelial growth factor ther-apy into pediatric ophthalmology: Promise and concern. J AAPOS2009;13:329-31.