Raine syndrome
4
Letter to the Editor Raine Syndrome To the Editor: In 1989, Raine et al. reported on a previously un- known disorder subsequently categorized as Raine syn- drome by Kan and Kozlowski [1992], which comprised severe craniofacial anomalies with microcephaly, de- formed hypoplastic nose, prominent exophthalmos, gum hypoplasia, low-set ears, and choanal atresia or stenosis. Radiographs showed diffuse osteosclerosis with periosteal thickenings of ribs, clavicles, and di- aphyses of long bones. Until now, 4 single cases have been described with, in addition to those of Raine et al. and Kan and Kozlowski, reports by Kingston et al. [1991] and by Al Mane et al. [1996], who established the ultrasound and computed tomographic demonstra- tion of intracranial calcification as a component of the syndrome. This last infant is the second of the three sibs discussed in the present report, the complete fam- *Correspondence to: Dr. Abdellatif Rejjal, Department of Pedi- atrics, King Faisal Specialist Hospital and Research Centre, PO Box 3354, MBC-58, Riyadh 11211, Kingdom of Saudi Arabia. Received 24 September 1997; Accepted 23 April 1998 Fig. 1. (a) Frontal and (b) lateral views of the face. Proptosis with deformed hypoplastic nose, bowed upper lip, and small mandible. An oro-pharyngeal airway is in place because of choanal obstruction. American Journal of Medical Genetics 78:382–385 (1998) © 1998 Wiley-Liss, Inc.
-
Upload
abdellatif -
Category
Documents
-
view
214 -
download
0
Transcript of Raine syndrome

Letter to the Editor
Raine Syndrome
To the Editor:
In 1989, Raine et al. reported on a previously un-known disorder subsequently categorized as Raine syn-drome by Kan and Kozlowski [1992], which comprisedsevere craniofacial anomalies with microcephaly, de-formed hypoplastic nose, prominent exophthalmos,gum hypoplasia, low-set ears, and choanal atresia orstenosis. Radiographs showed diffuse osteosclerosis
with periosteal thickenings of ribs, clavicles, and di-aphyses of long bones. Until now, 4 single cases havebeen described with, in addition to those of Raine et al.and Kan and Kozlowski, reports by Kingston et al.[1991] and by Al Mane et al. [1996], who establishedthe ultrasound and computed tomographic demonstra-tion of intracranial calcification as a component of thesyndrome. This last infant is the second of the threesibs discussed in the present report, the complete fam-
*Correspondence to: Dr. Abdellatif Rejjal, Department of Pedi-atrics, King Faisal Specialist Hospital and Research Centre, POBox 3354, MBC-58, Riyadh 11211, Kingdom of Saudi Arabia.
Received 24 September 1997; Accepted 23 April 1998
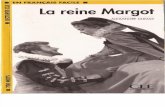
Fig. 1. (a) Frontal and (b) lateral views of the face. Proptosis with deformed hypoplastic nose, bowed upper lip, and small mandible. An oro-pharyngealairway is in place because of choanal obstruction.
American Journal of Medical Genetics 78:382–385 (1998)
© 1998 Wiley-Liss, Inc.

ily history coming to light only with the subsequentbirth of the third affected child.
The parents are first cousins and have had five chil-dren. The first and third children, a girl and a boyrespectively, are normal. The second child, a girl, wasborn at term elsewhere in Riyadh (at King Saud Uni-versity Hospital) and is described as having ‘‘micro-cephaly, bulging eyes, choanal atresia, and generalizedosteosclerosis’’ then interpreted as ‘‘osteopetrosis.’’ Shelived only a few days. Ultrasound and CT studies of thebrain showed prominent calcifications, and a brief re-port of the case was published [Patel et al., 1992]. Noradiographs of the skeleton were illustrated, and thesimilarity with the case reports of Raine et al. [1989]and Kingston et al. [1991] was not recognized; however,Al Mane et al. [1996] later suggested this patient mighthave had Raine syndrome.
The fourth child, a boy, was born at King Faisal Spe-cialist Hospital and Research Centre (KFSH & RC)with findings identical to those described in the previ-ously affected infant, and this is the patient reportedby Al Mane et al. [1996]. Birth weight was 2.8 kg. Hehad proptosis, depressed nose, low-set ears, and cleftpalate. The child was resuscitated and intubated. Re-spiratory distress due to the choanal atresia was notrelieved by conventional surgical treatment, and a tra-
cheostomy was performed. The parents requested thatfurther active treatment be discontinued and the childdied at 8 weeks of age. Radiographic study of the skel-eton showed diffuse osteosclerosis and widespreadperiosteal thickening of mandible, clavicles, scapulae,ribs, and long bones. Ultrasound and CT of the brainboth showed widespread focal cerebral calcifications in
Fig. 2. Cranial ultrasound study at age 1 day. Parasagittal image show-ing radiating linear hyperechoic appearance in the basal ganglia.
Fig. 3. a,b: Cranial CT, age 2 days. Unenhanced axial scan. Wide-spread focal calcifications in the periventricular white matter and in thecorpus callosum.
Letter to the Editor 383

the periventricular white matter and basal gangliawith some meningeal calcifications as well, and thesewere thought to correspond to the histologic calcifica-tions reported in the brain by Kan and Kozlowski. Themother became pregnant for a fifth time and was againseen at KFSH & RC. A prenatal ultrasound examina-tion identified craniofacial anomalies and, with knowl-edge of the previous history, the parents were informed
that this child was similarly affected. At birth, the in-fant was male with a birth weight of 2.8 kg, length of 47cm, and head circumference of 32.5 cm. Apgar scoreswere 3 and 8 at one and five minutes, respectively. Inappearance, this child (Fig. 1) was virtually identical tothe previous sib. The family requested no active inves-tigation or attempts at resuscitation. A minimalworkup was carried out to confirm the diagnosis with
Fig. 4. (a) Skull, (b) thorax, (c) left upper limb, and (d) lower limbs, age 2 days. (a) Dense bones of the cranial vault and base with wide sutures. Thefacial bones are small and sclerotic, the mandible irregular. (b, c, and d) Generalized osteosclerosis with impaired cortico-medullary differentiation andirregular periosteal thickenings of the ribs and long bones.
384 Rejjal

ultrasound (Fig. 2), CT (Fig. 3) examinations of thebrain, and radiographic skeletal survey (Fig. 4). Theseshowed characteristic intracranial calcifications andgeneralized osteosclerosis with irregular periostealthickening. Screening for congenital infections wasnegative, and blood count, renal, and hepatic profileswere all normal. The child was fed by oro-gastric tubebecause of the choanal atresia and died of respiratoryfailure on the third day. Autopsy was denied.
The fact that the parents of our three patients arefirst cousins, and that they have two normal children,supports the suggestions of the present and of previousauthors [Kingston et al, 1991; Kan & Kozlowski, 1992;Al Mane et al., 1996] of autosomal recessive inheri-tance.
In all six reported patients, the cause of death wasrespiratory failure, with survival after birth of between45 min [Kan & Kozlowski, 1992] and a few days (ourCase 1), except in our second patient who lived eightweeks, but with a tracheostomy and assisted ventila-tion. Respiratory insufficiency appears to relate to pul-
monary hypoplasia, an abnormal thoracic cage, andchoanal obstruction.
REFERENCES
Al Mane K, Coates RK, McDonald P (1996): Intracranial calcification inRaine syndrome. Pediatr Radiol 26:55–58.
Kan AE, Kozlowski K (1992): New distinct lethal osteosclerotic bone dys-plasia (Raine syndrome). Am J Med Genet 43:860–864.
Kingston HM, Freeman MB, Hall CM (1991): A new lethal sclerosing bonedysplasia. Skeletal Radiol 20:117–119.
Patel PJ, Kolawole TM, Al-Mofeda S, Malabarey TM, Hulailah A (1992):Osteopetrosis: brain ultrasound and computed tomography findings.Eur J Pediatr 151:827–828.
Raine J, Winger RM, Davey A, Tucker SM (1989): Unknown syndrome:microcephaly, hypoplastic nose, exophthalmos, gum hyperplasia, cleftpalate, low set ears and osteosclerosis. J Med Genet 26:786–788.
Abdellatif RejjalDepartment of PediatricsKing Faisal Specialist Hospital and Research CentreRiyadh, Kingdom of Saudi Arabia
Letter to the Editor 385