
Radiology of Fracture Principles Suzanne O’Hagan 18 May 2012.
73
Radiology of Fracture Principles Suzanne O’Hagan 18 May 2012
-
Upload
parker-parmentier -
Category
Documents
-
view
219 -
download
3
Transcript of Radiology of Fracture Principles Suzanne O’Hagan 18 May 2012.

Radiology of Fracture Principles
Suzanne O’Hagan18 May 2012

Radiographic Principles• When analysing and ordering x-rays you should remember the
rule of two’s:
• Two views. At 90 degrees, usually anterior-posterior and lateral.
• Two joints. The joints above and below.• Two occasions. Some fractures are not easily visible
immediately after trauma.• Two limbs. If required for comparison. • NB: In certain injuries, ‘special’ views are required. These
include Scaphoid views, Skyline views for the patello-femoral compartment of the knee and Mortise view at the ankle.

Recognizing an acute fracture
Disruption in the continuity of all or part of the cortex of a bone
Complete:cortex broken through and through, traversing the width of the bone
Incomplete: part of cortex fractured. Tend to occur in bones that are “softer” such as in children or in adults with bone-softening diseases such as osteomalacia or Paget’s disease
Examples of incomplete fracture in children are:-Greenstick fracture, involves only one part of the cortex- Buckle fracture, compression of cortex

Greenstick fracture
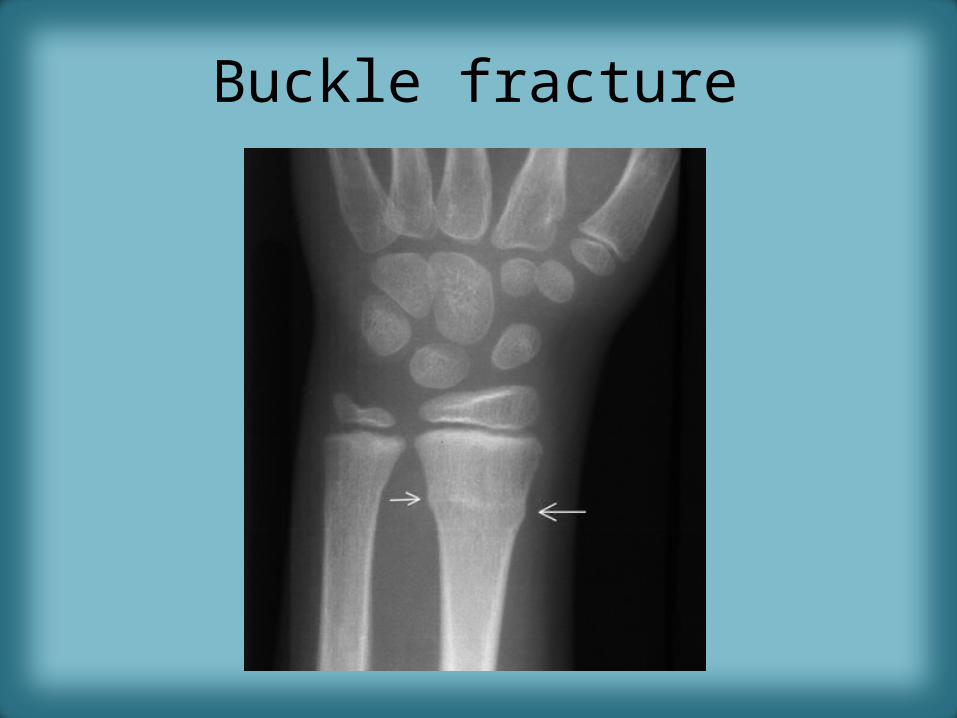
Buckle fracture

Fracture Lines
• More lucent than other lines normally found in bones such as nutrient canals
• Abrupt discontinuity of the cortex
• Straighter in their course yet more acute in their angulation than naturally occurring lines such as epiphyseal plates
• The edges tend to be jagged and rough

Pitfalls• Sesamoids
– Bones that form in a tendon as it passes over a joint. The patella is the largest.• Accessory ossicles
– These are accessory epiphyseal or apophyseal ossification centres that do not fuse with the parent bone
Unlike fractures these small bones are corticated and their edges are usually smooth
Sesamoids and accessory ossicles are usually bilateral and at anatomically predictable sites
• Old, unhealed fracture fragments– Can be confused with new fractures

Sesamoid bones at joints
Knee – the patella (within the quadriceps tendon)
Hand– two sesamoid bones commonly found in the distal portions of the first metacarpal bone (within the tendons of adductor pollicis and flexor pollicisbrevis); also distal portion of second metacarpal boneWrist– the pisiform within the flexor carpiulnaris tendon
Foot – first metatarsal bone has two sesamoids at its connection to the big toe, within the tendon of flexor hallucisbrevis (sometimes only a single sesamoid)

Accessory Ossicles• The process of ossification progresses from a primary ossification centre, until the bone is completely ossified.
Irregularly shaped bones such as the tarsal bones may develop a secondary centre and in some individuals complete ossification does not occur. The secondary centre remains separate from the rest of the bone, forming an accessory ossicle.
Os trigonum – the separated posterolateral tubercle of the talus.
Os tibiale externum (accessory navicular) – located posteromedial aspect of navicular where posterior tibialis tendon inserts

Accessory ossicles
• Os PeroneumIn peroneusbrevis tendon
• Os fabellaPosterior to the lateral condyle of the femur. It exists in the location of the lateral head of gastrocnemius tendon.
Many more…

Describing fractures
• 4 major parameters
– Number of fragments– Direction of fracture line– Relationship of fragments to each other– Communication of the fracture with the outside
atmosphere

Number of fracture fragments• 2 fragments = simple fracture• >2 = comminuted fracture
– Segmental fractureA portion of the shaft exists as an isolated fragment
– Butterfly fragmentCentral fragment has a triangular shape

Direction of fracture lines• Transverse: Fracture line perpendicular to long axis of
bone (perpendicular force)• Oblique: Fracture line diagonal relative to long axis
(force usually applied along same direction as long axis)• Spiral: Caused by a twisting force, usually unstable and
often associated with soft tissue injury

Relationship of Fragments to each other
1. Displacement2. Angulation3. Shortening4. Rotation
By convention, describe the relationship of the distal fragment relative to theproximal fragment

Displacement
• Amount by which the distal fragment is offset, front to back and side to side, from the proximal fragment
• Described in terms of percent or fractions (e.g. 50% the width of the shaft or ½ the width of the shaft of the proximal fragment)

Angulation
• Angle between the distal and proximal fragments
• Described in degrees and by position– State direction of distal bone• Superior, inferior, anterior, posterior, medial, lateral,
volar, dorsal
– State degree of angulation relative to proximal bone
– Medial (varus), Lateral (valgus)

Colles fractureTransverse fracture of distal radius2.5cm proximal to radiocarpal jointDorsal displacement and volar angulation

Shortening
• How much, if any, overlap there is of the ends of the fracture fragments
• How much shorter the fractured bone is than it would be had it not been fractured
• Shortening is described in centimetres

Midshaft femur fracture

Distraction and Impaction• Distraction– Increase in overall
bone length
•Impaction – Shortening with no loss of bone alignment

Rotation

Rotation• Unusual
• Almost always involving the long bones
• Describes the orientation of the joint at one end relative to the orientation of the joint at the other end of the fractured bone
• Eg proximal tibia oriented in frontal projection while distal tibia and ankle oriented laterally
• Both the joint above and below the fracture need to be included to appreciate rotation

Relationship of Fracture to Atmosphere
• Closed– More common– No communication
• Open/compound– Communication
Best diagnosed clinically
Avulsion fractures• Common mechanism of fracture production• Avulsed fragment is pulled from its parent bone by contraction of a
tendon or ligament• More common in young athletes• Derive many of their names from athletic activity e.g. dancer’s fracture,
skier’s fracture, sprinter’s fracture• Occur in anatomically predictable locations where tendons are known
to insert• May heal with exuberant callous formation• Some may resemble a neoplastic or infectious process• Some may have an aggressive appearance that may include areas of
mixed lysis and sclerosis• The appearance depends on whether acute, subacute or chronic

Avulsion fracture lesser trochanter
(iliopsoas)
Avulsion fracture ischialtuberosity
(hamstrings)
Avulsion Fractures: common in the pelvisIn the pelvis, the newly formed secondary centers of ossification, the apophyses, are most likely to avulse· Apophyses tend to form at the time of puberty = time of pelvic avulsions

Sites and Insertions

Dancer fracture

Don’t confuse with Jone’s Fracture
Jones fracture involves a fracture at the base of fifth metatarsal at metaphyseal-diaphyseal junction
A Jones fracture is located within 1.5 cm distal to tuberosity of 5th metatarsal
Avulsion fracture more common and affects the 5th metatarsal styloid process proximally.

Osgood Schlatter
• Caused by stress on the patellar tendon• Patellar tendon attaches the quadriceps muscle to the tibial tuberosity• Adolescent growth spurt, repeated stress from quadriceps contraction is transmitted through the tibial tuberosity• Causes multiple subacute avulsion fractures with inflammation along the tendon leading to excess bone grwoth in
the tuberosity

SALTER-HARRIS FRACTURESEpiphyseal plate fractures in children
• In growing bone, the hypertrophic zone in the growth plate (epiphyseal plate or physis) is most vulnerable to shearing injuries
• Account for as many as 30% of childhood fractures
• SH classification helps determine treatment and predict complications
• Represent a spectrum of accidental injuries in children
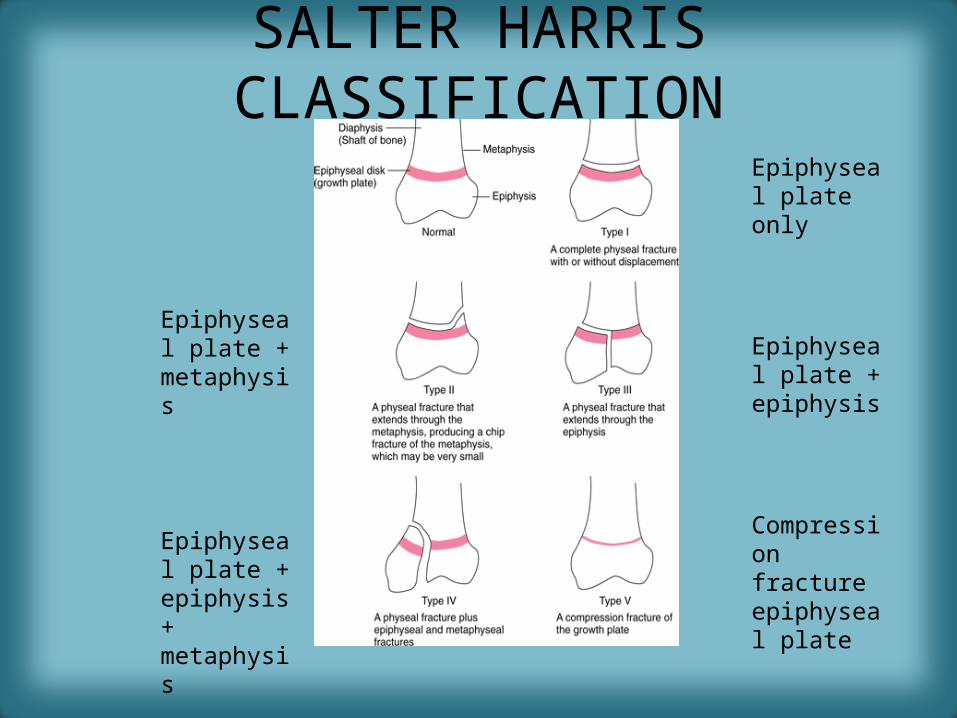
SALTER HARRIS CLASSIFICATION
Epiphyseal plate only
Epiphyseal plate + metaphysis
Epiphyseal plate + epiphysis
Compression fracture epiphyseal plate
Epiphyseal plate + epiphysis + metaphysis
Prognosis
• Types I and II heal well
• Type III fractures can develop arthritic changes or asymmetric growth plate fusion
• Types IV and V are more likely to develop early fusion of the growth plate with angular deformities and shortening of that bone

Type I: Fractures of the epiphyseal plate alone
• Difficult to detect without comparison views• SCFE is a manifestation of a SH I injury– Tall, heavy teenage boys– Bilateral in 25%– Can result in avascular necrosis due to interrupted
blood supply in 15%

Salter Harris I
“widening of the growth plate”
Slipped Capital Femoral Epiphysis

Salter Harris I

Type II: Fracture of the epiphyseal plate and fracture of metaphysis
• Most common (75%)
• Seen especially in the distal radius
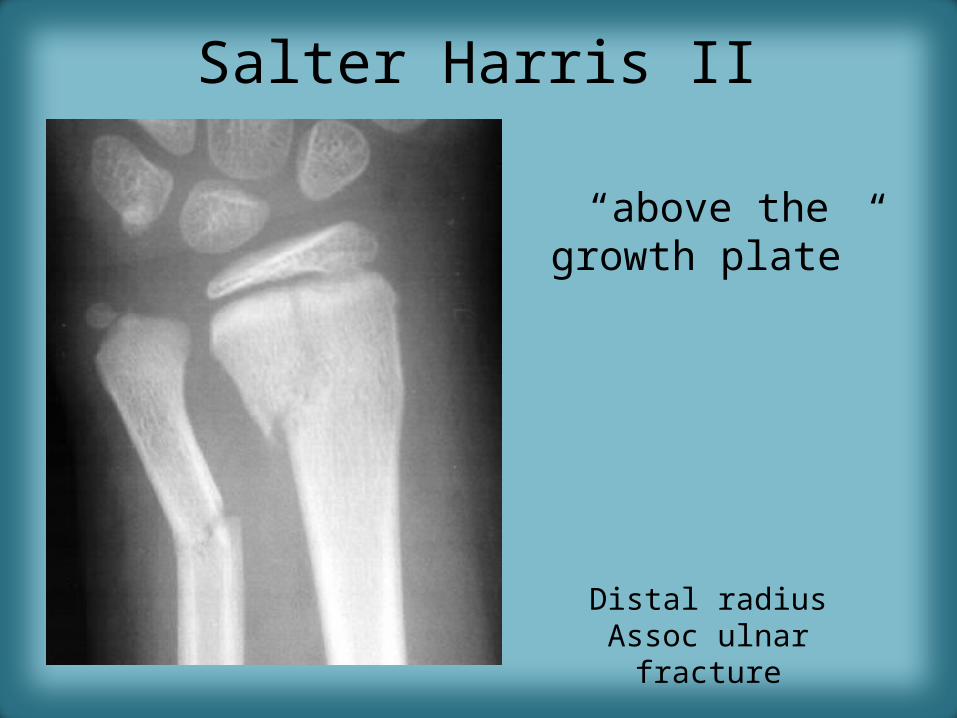
Salter Harris II
Distal radiusAssoc ulnar fracture
“above the growth plate”

Type III: Fracture of the epiphyseal plate and epiphsysis
• Longitudinal fracture through epiphysis itself; fracture invariably enters the joint space and fractures the articular cartilage
• Risk of osteoarthritis later in life
• Can result in premature and asymmetric fusion of the growth plate with subsequent deformity

Salter Harris III
“below the growth plate”

Type IV: Fracture of epiphysis and metaphysis through the epiphyseal plate
• Poorer prognosis – premature and possibly asymmetric closure of
growth plate
• May lead to differences in limb length, angular deformities and secondary OA
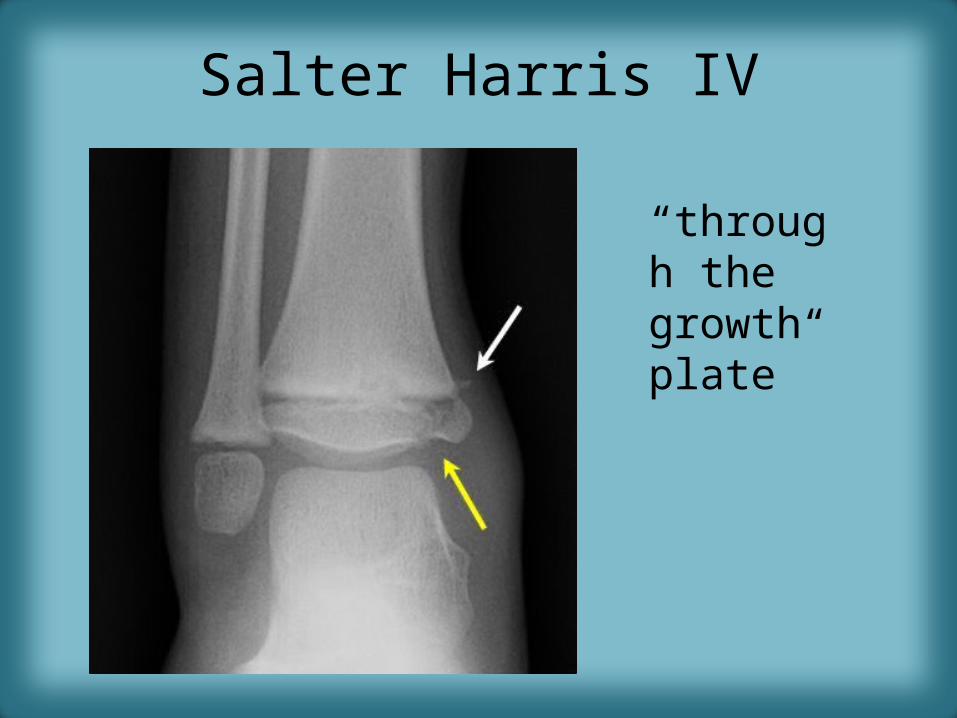
Salter Harris IV
“through the growth plate”

Salter Harris IV

Salter Harris V
• Rare• Associated with vascular injury• Almost always result in growth impairment
through early focal fusion of the growth plate• Most common in the distal femur, proximal
tibia and distal tibia• Difficult to diagnose on conventional
radiographs until later when they complicate

Salter Harris V
LeftRight

Non-accidental injury patterns
• Metaphyseal corner fractures• Rib fractures– Especially multiple and posterior
• Head injuries– Skull fractures tend to be bilateral, comminuted
and cross suture lines (associated subdurals, SAH, cerebral contusion)

CML: Classic Metaphyseal LesionVirtually pathognomonic of abuse
• series of microfractures across the metaphysis• the fracture line is oriented essentially parallel to the physis,
although it may not travel the entire width of the bone • precipitating force is a shearing injury across the bone end,
the result of horizontal motion across the metaphysis, therefore not a feature of falls or blunt trauma
• force is generated by manual to-and-fro manipulation of the extremities (eg, holding and shaking an infant by the feet or hands or shaking the infant while he is held around the chest)
• CML is seen almost exclusively in children less than 2 years of age

CML: Corner or Bucket Handle Fracture

Stress Fracture
• Bone subjected to repeated stretching and compressive forces
• Numerous microfractures• Conventional radiographs may initially appear normal
in up to 85%• Fracture may not be diagnosable until after periosteal
new bone formation or healing occurs• Bone scans or MRI will usually be positive earlier• Common locations include the shafts of long bones, the
calcaneus and the 2nd and 3rd metatarsals

Stress Fractures

5 MOST COMMON EPONYMS
• Colle’s• Smith’s• Jones• Boxer’s• March
3 in the hand, 2 in the foot

Colle’s Fracture
• Colles' fracture is a fracture of the distal metaphysis of the radius with dorsal displacement and volar angulation leading to a ’dinner fork deformity’.
• Colles fractures are seen more frequently with advancing age and in women with osteoporosis.
• Mostly an extraarticular, uncomplicated and stable fracture, but it can be intra-articular.

Smith’s FractureReversed Colle’sOccurs in younger patientsResults from high energy trauma on the volar flexed wristVolar displacement and dorsal angulationIntra-articular extension more common

Jone’s Fracture
• Transverse fracture of 5th metatarsal 1.5cm from its base
• Caused by plantar flexion of the foot and inversion of the ankle
• Less common than avulsion fracture

Boxer’s Fracture• Fracture of head of 5th metacarpal with palmar angulation• Usually results from punching a person or wall

March Fracture
• Type of stress fracture to the foot
• Usually shafts of 2nd or 3rd
metatarsals

EASILY MISSED FRACTURES
• Scaphoid fractures• Buckle fractures• Radial head fractures• Supracondylar fractures• Posterior disclocation of the shoulder• Hip fractures in the elderly

Scaphoid Fracture• Tenderness in anatomical snuff box after fall on outstretched hand• Hairline thin radiolucencies on scaphoid views (ulnar deviation of wrist)

Radial Head Fracture
• Common in adults• Look for a positive fat pad sign:– Posterior fat pad usually invisible– Crescenticlucency of fat along the posterior aspect
of the distal humerus is produced by normally invisible fat that is lifted away from the bone by swelling of the joint capsule due to haemarthrosis

Radial head fracture

Supracondylar Fracture
• Most common fracture of the elbow in a child• Most produce posterior displacement of the
humerus• True lateral, anterior humeral line should
bisect the middle third of the ossification centre of capitellum
• In most supracondylars, this line passes anterior to its normal location
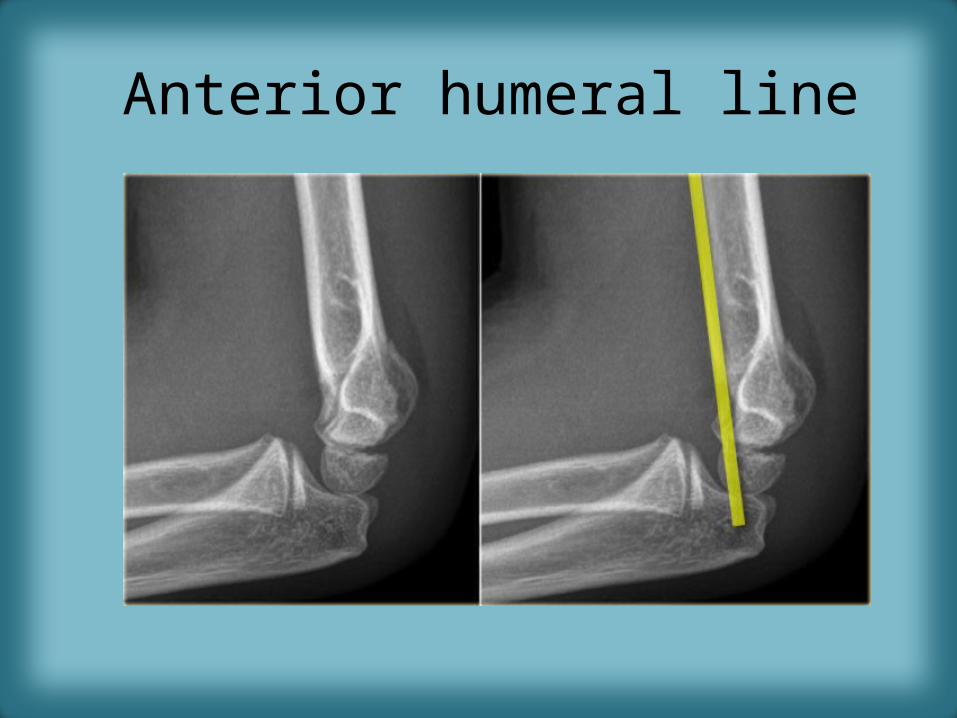
Anterior humeral line

Positive Fat Pad Sign

Posterior Dislocation of the Shoulder
“Y” view (oblique view of the shoulder), head will lie lateral to the glenoid in posterior dislocation
Frontal: Humeral head fixed in internal rotation, resembles a light bulb

Hip Fractures in the ElderlyFrequently related to osteoporosisTake x-rays with leg in internal rotation to display the neck in profileLook for angulation of the cortex and zones of increased density (impaction)Look for secondary signs MRI or bone scan will be required when indicated

Secondary signs of fractures
• Soft tissue swelling
• Disappearance of normal fat stripes
• Joint effusion
• Periosteal reaction (late)

FRACTURE HEALING
• Determined by many factors– Age of patient– Fracture site– Position of fracture fragments– Degree of immobilization– Blood supply– Mineralisation of bone– Medication

FRACTURE HEALING PROCESS
• Immediate: Haemorrhage into fracture site• First few weeks: Osteoclasts act to remove
diseased bone (fracture line may widen)• Next few weeks: New bone (callus) begins to
fill the fracture defect.• 8 – 12 weeks: Remodelling– Mechanical forces adjust bone back to its original
shape– Fast in children, slow in adults
COMPLICATIONS OF FRACTURE HEALING
• Delayed union– Fracture does not heal in expected time– Most will eventually heal if immobilisation extended
• Malunion– Healing occurs in a mechanically or cosmetically unacceptable
position• Non-union
– Implies that fracture healing will never occur– Smooth, sclerotic margins with distraction of the fracture fragments– Pseudarthrosis may form– Motion at the fracture site may be demonstrated on stress views or
with fluoroscopy

Fracture healing complications

Role of CT and MRI
• CT usually requested to obtain further detail for surgical planning especially in fractures of:– Tibial plateau– Acetabulum– Ankle (?trimalleolar)– Calcaneus– Cervical spine
• MRI usually cases of doubt to detect bone marrow oedema particularly in occult fractures of:– Hip– Scaphoid– Stress fractures eg tibia, metatarsal
Also gives additional information regarding the soft tissue components
Bone scan low specificity
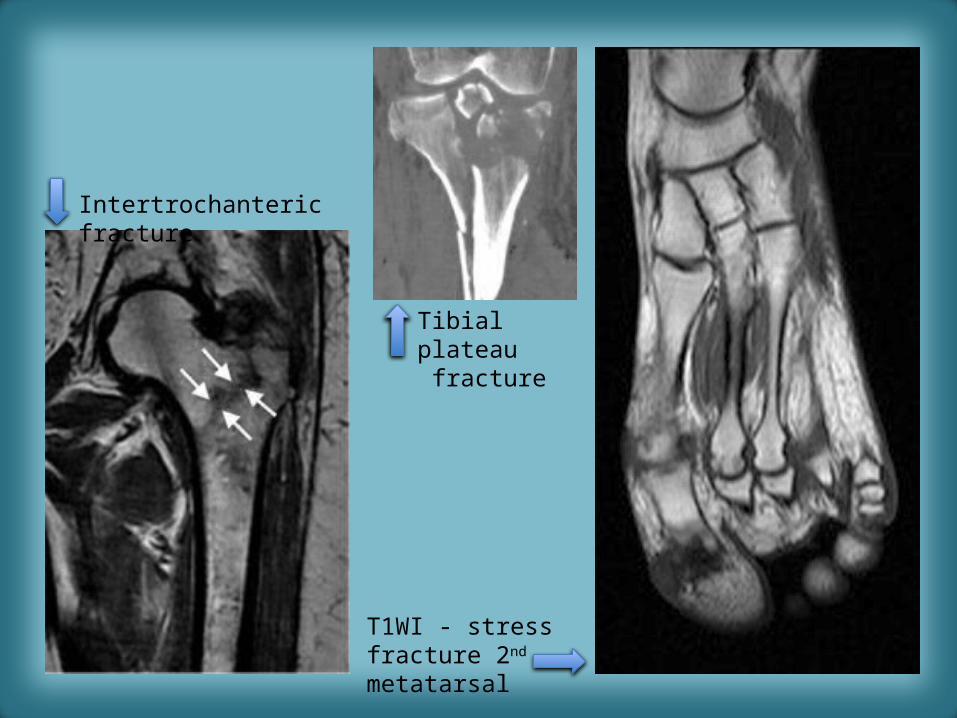
Intertrochanteric fracture
Tibial plateau fracture
T1WI - stress fracture 2nd metatarsal

Conclusion
• Radiological interpretation of fractures is a huge topic. Classifications are detailed and can sometimes be clumsy.
• A good starting point is to be able to describe a fracture correctly using the principles discussed in this lecture.

References
• Herring, W. Learning Radiology: Recognizing the Basics 2nd Ed 2012. p232.
• Greenspan, A. Orthopaedic Imaging: A Practical Approach. Chapter 4: Radiologic Evaluation of Trauma
• Thompson, JC. Netters Concise Orthopaedic Anatomy. 2010
• www.wheelessonline.com/ortho/trauma_fractures


















