Radiology Business Journal Jan/Feb 2009
52
FOR LEADERS IN MEDICAL IMAGING SERVICES February/March 2009 FEATURED IN THIS ISSUE Imaging Executives Crunch the Numbers | page 28 Mining the RSNA Landscape | page 34 Teleradiology Permeates the Specialty | page 40 www.radbizjournal.com Coding | Reimbursement | Operations PAGE 18 The CCTA Playbook The CCTA Playbook
-
Upload
imagingbiz -
Category
Documents
-
view
294 -
download
5
description
Welcome to Radiology Business Journal, a bi-monthly print journal published by ImagingBiz. This next-generation economics journal is published by the team that founded and developed Decisions in Imaging Economics, Curtis Kauffman-Pickelle and Cheryl Proval. We published our first quarterly issue in April 2008 and went to a bi-monthly frequency in 2009. The challenges ahead for health care, and, more specifically, for radiology, will require vision, strong leadership, and masterful business skills. Radiology Business Journal’s mission is to feed all of those competencies with insightful articles written by expert authors.
Transcript of Radiology Business Journal Jan/Feb 2009

FOR LEADERS IN MEDICAL IMAGING SERVICES
February/March 2009
FEATURED IN THIS ISSUE
Imaging ExecutivesCrunch the Numbers | page 28
Mining the RSNALandscape | page 34
Teleradiology Permeatesthe Specialty | page 40
www.radbiz journal .com
Coding | Reimbursement | Operations
PAGE 18
The CCTAPlaybookThe CCTAPlaybook

Oasis is the Right MR for Every PatientThe unobstructed view puts even difficult patients at ease. And in every type of scan. The trulyopen Oasis can make a difference in the way patients and referring clinicians view your services.
And With Every Clinical CapabilityFrom advanced Neuro and Vascular imaging to comprehensive Body and Ortho applications,you get the image resolution and clinical flexibility of high-field strength imaging.
This is Your OASIS – Look into the High-Field MR with Advantages for Everyone.
Everything Improves with a Comfortable Patient
THE PATIENT MAGNET
Hitachi Medical Systems America
Hi tach iMed .com • 800 .800 .3106
Oasis.multi-people ad:Layout 1 8/15/08 2:18 PM Page 1

Oasis is the Right MR for Every PatientThe unobstructed view puts even difficult patients at ease. And in every type of scan. The trulyopen Oasis can make a difference in the way patients and referring clinicians view your services.
And With Every Clinical CapabilityFrom advanced Neuro and Vascular imaging to comprehensive Body and Ortho applications,you get the image resolution and clinical flexibility of high-field strength imaging.
This is Your OASIS – Look into the High-Field MR with Advantages for Everyone.
Everything Improves with a Comfortable Patient
THE PATIENT MAGNET
Hitachi Medical Systems America
Hi tach iMed .com • 800 .800 .3106
Oasis.multi-people ad:Layout 1 8/15/08 2:18 PM Page 1

4 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.comwww.fujimed.com©2008 FUJIFILM Medical Systems USA, Inc.
Synapse brings all the domains, modalities, tools – everything together in one place. No more logging on and off different systems with different interfaces and different tools. Now Radiology,Cardiology, Mammography, Oncology, Ophthalmology, Endoscopy and more are all in one system. Andsince it’s Synapse, you can work anywhere you want: at the hospital, at home, wherever. Synapse medicalimaging informatics gives it all to you – in one brilliant package. With over 1500 sites and more than tenmillion studies, Synapse has helped thousands of radiologists be more productive, be more efficient anddeliver a higher level of care. There’s a whole lot going on inside Synapse, so you can feel a little lessstressed. Call 1-866-879-0006 or visit www.fujimed.com.
There’s a whole lot going on inside Synapse®.
913_Synapse_AR.qxd:Layout 1 11/11/08 3:16 PM Page 1
FEATURES18 THE CCTA PLAYBOOK:
A GUIDE TO CODING, REIMBURSEMENT, AND OPERATIONS
By Jonathan Berlin, MD, MBAA compendium of the business intelligencerequired to launch a CCTA service.
24 MASTERS OF MANIPULATION
By Cat VaskoRadiologists and vendors race to grasp and improvethe tools of advanced visualization as imagingmodalities churn out ever more information.
28 DATA MINING: IMAGING EXECUTIVES CRUNCH THE NUMBERS
By George WileyRIS data, keyed to billing, can be analyzed to improvecompetitive capability and pare inefficiency to the nub.
34 RSNA 2008: MINING THE LANDSCAPE, ASSESSING THE EXHIBITS
By Lisa Bielamowicz, MDIn assessing the imaging technologies on display at RSNA,an observer provides tools for making criticaldecisions regarding your capital budget for 2009.
40 DAY FOR NIGHT, EAST FOR WEST
By Greg ThompsonTeleradiology permeates the specialty as practices crossstate, regional, and global boundaries to purchaseand practice radiology.
DEPARTMENTS8 ADVIEW
Prove ItBy Cheryl Proval
10 THE BOTTOM LINE
Radiology: Ancillary No MoreBy Howard Fleishon, MD
F E B R U A R Y / M A R C H 2 0 0 9 | VOLUME 2 , NUMBER 1
C O N T E N T S
18
24
28
40

www.fujimed.com©2008 FUJIFILM Medical Systems USA, Inc.
Synapse brings all the domains, modalities, tools – everything together in one place. No more logging on and off different systems with different interfaces and different tools. Now Radiology,Cardiology, Mammography, Oncology, Ophthalmology, Endoscopy and more are all in one system. Andsince it’s Synapse, you can work anywhere you want: at the hospital, at home, wherever. Synapse medicalimaging informatics gives it all to you – in one brilliant package. With over 1500 sites and more than tenmillion studies, Synapse has helped thousands of radiologists be more productive, be more efficient anddeliver a higher level of care. There’s a whole lot going on inside Synapse, so you can feel a little lessstressed. Call 1-866-879-0006 or visit www.fujimed.com.
There’s a whole lot going on inside Synapse®.
913_Synapse_AR.qxd:Layout 1 11/11/08 3:16 PM Page 1

6 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
C O N T E N T SF E B R U A R Y / M A R C H 2 0 0 9 | VOLUME 2 , NUMBER 1
46
12
48
PUBLISHERCurtis Kauffman-Pickelle
EDITORCheryl Proval
ART DIRECTOR Patrick R. Walling
TECHNICAL EDITORKris Kyes
CONTRIBUTING WRITERSJonathan Berlin, MD, MBA
Lisa Bielamowicz, MDHoward B. Fleishon, MD, MMM
Daniel McLaughlinGreg Thompson
Cat VaskoGeorge Wiley
ADVERTISING DIRECTORSharon Fitzgerald
PRODUCTION COORDINATORMegan Runyon
CORPORATE OFFICEImaging Center Institute
17291 Irvine Blvd., Suite 406Tustin, CA 92780(714) 832-6400
www.ImagingCenterInstitute.com
PRESIDENT/CEOCurtis Kauffman-Pickelle
VP, PUBLISHINGCheryl Proval
VP, CLIENT SERVICESSteve Smith
VP, ADMINISTRATIONMary Kauffman
BPA Worldwide membership applied forFebruary, 2009
Radiology Business Journal is published bimonthly by theImaging Center Institute, 17291 Irvine Blvd., Suite 406,Tustin, CA 92780. US Postage Paid at Lebanon Junction, KY40150. February/March 2009, Vol 2, No 1 © 2009 ImagingCenter Institute. All rights reserved. No part of this publica-tion may be reproduced in any form without written permis-sion from the publisher. POSTMASTER: Send address changesto Imaging Center Institute, 17291 Irvine Blvd., Suite 406,Tustin, CA 92780. While the publishers have made everyeffort to ensure the accuracy of the materials presented inRadiology Business Journal, they are not responsible for thecorrectness of the information and/or opinions expressed.
48
DEPARTMENTS (continued)
12 PRIORS
12 HEALTH POLICY | Further TC Cuts Ahead?
14 UTILIZATION | Under the Influence of RBMs
15 STRATEGIC PLANNING | Thoughtful Management for Hard Times
46 MARKETPLACE
48 ADVERTISER INDEX
50 FINAL READ
Highly Functional ImagingBy Curtis Kauffman-Pickelle
The Achieva 3.0T TX automatically adjusts to each patient’s unique anatomy. Proprietary
parallel RF transmission technology tailors signals for enhanced image uniformity, reduced
scan times and improved throughput across a broad
range of clinical applications. Fast, robust and versatile.
It just makes clinical and economic sense. Learn more
at www.philips.com/healthcare.
because no two patients are alike,we designedan MR unlikeany other.
MR unlike any other_206x276.indd 1 09-02-2009 14:31:49

The Achieva 3.0T TX automatically adjusts to each patient’s unique anatomy. Proprietary
parallel RF transmission technology tailors signals for enhanced image uniformity, reduced
scan times and improved throughput across a broad
range of clinical applications. Fast, robust and versatile.
It just makes clinical and economic sense. Learn more
at www.philips.com/healthcare.
because no two patients are alike,we designedan MR unlikeany other.
MR unlike any other_206x276.indd 1 09-02-2009 14:31:49

8 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
AdView
It is time for the specialty to take a proactiverole in evidence-based radiology
If you have any doubt that imagingremains a target for further cuts, you willfind an article within a section on imag-ing1 in the November–December 2008
issue of Health Affairs enlightening—if not toyour liking. The authors are analysts for theMedicare Payment Advisory Commission(MedPAC), and they are urging CMS to take ascalpel, instead of a hatchet—as in theDRA—to the technical reimbursement forimaging. In the end, the cuts would be likelyto exact a similarly painful pound of cure.
You decide whether the fixes proposed byWinter and Ray (summarized on page 12) wouldrender a more accurate payment methodologyfor practice expenses in this era of dwindlingresources. My point is this: Payors, regulators,and, now, health policy experts perceive imag-ing as a problem, not a solution. What is radiol-ogy going to do about that?
The price of medical technology is thetheme of the Health Affairs issue in which theabove article appeared. The first five articlesare devoted to medical imaging and arerequired reading for anyone who cares aboutthe specialty, how it is perceived, and what isrequired to demonstrate its usefulness.
A group from Stanford University,Stanford, Calif, led by Baker, wrote the firstarticle in the section. Using an equipmentcensus and Medicare claims data, the teamdocuments a direct relationship between thegrowth in the availability of high-tech imag-ing technology between 1995 and 2004 andthe growth of the total number of proceduresperformed on Medicare beneficiaries. Theteam acknowledges the difficulty of deter-mining whether the increased expendituresprovided an equivalent benefit to society, butit does offer an approach to developing pop-ulation-level evidence to begin to answerthat question, using the diagnosis of abdom-inal aortic aneurysm as an example.
Winter and Ray’s article appears second inthe section; a third article is provided bySmith-Bindman (a University of California–SanFrancisco radiologist) and two researchersassociated with the Group HealthCooperative, Seattle, a nonprofit, mixed-model integrated care system coveringapproximately 10% of Washington state resi-dents through its own facilities.
Studying the imaging patterns of 377,048patients between 1997 and 2006, the authorscalculate the number of imaging tests per yearby anatomic area, modality, and year withinage groups (including elderly enrollees), witha focus on repeat imaging and cost. The GroupHealth Cooperative data describe patterns inits managed care environment that are verysimilar to those growth patterns reported byMedPAC in the Medicare population, leadingthe authors to surmise that disincentives inthe managed care model may not suffice tochange the impulses toward increased use ofimaging in the fee-for-service population.
The fourth article in the section comesfrom a team of researchers led by Pearson atthe Institute of Clinical and Economic Reviewat Massachusetts General Hospital’s Institutefor Technology Assessment (ITA), Boston,which is directed by Gazelle (a radiologistwho is also one of the article’s authors).Stating that new medical tests and treat-ments frequently become widely used priorto definitive evidence of their effectiveness,the authors assert that medical imaging isprime for clinical effectiveness studies.
After describing the challenges of perform-ing those analyses—and they are consider-able—the authors describe a technique calleddecision-analytic modeling that can accommo-date information gaps. The authors demon-strate the method in a case study to assess thecomparative effectiveness of CT colonography.
In the last of the five articles, a USA Todayreporter offers an account of the CMSattempt to roll back reimbursement for car-diac CT angiography (CTA) and the successfulefforts of cardiology and radiology to over-turn that decision.
EXHILARATING AND TROUBLINGThroughout this section, some familiar
and new ideas emerge, both exhilarating andtroubling. The work done by Smith-Bindmanet al in this population is not their first, andwe are likely to see the authors continue tomine this rich vein of information over time asthey study the impact of coverage decisionsand new technologies. They have laid thegroundwork for collecting the evidence thatis expected to become even more importantto health care decision-making.
In the next article, Pearson et aladdress the problem of new technologiesand procedures adding an extra layer ofcost to the system by failing to replaceolder, less effective ones. The work doneat ITA; at Johns Hopkins University,Baltimore; and at the PermanenteFoundation, Oakland, Calif, to assess thecomparative effectiveness of CT colonog-raphy represents a refreshing advancebeyond the dithering about the challengesof obtaining outcomes data for radiology.
Yes, it is difficult, but this team plots apath around the hurdles. The methoddescribed in this article requires theinput of a great number of people to pre-serve the integrity of the results, but inthe absence of the gold standard oflarge, prospective studies, it providesmuch-needed, well-vetted informationon which to base decisions.
Here’s the troubling part. In introduc-ing the imaging section, the editor ofHealth Affairs draws parallels betweenthe boom brought about by subprimemortgage lending and unbridled securiti-zation and the rapid increases in medicalimaging. Also disturbing is the reporter’scynical summation of the struggle toretain reimbursement for cardiac CTA,which is characterized as a money grabby cardiology and radiology.
Clearly, radiology has a perceptionproblem. The specialty can reverse thisperception by taking a proactive role inproving the value of imaging, but it can’tbe done in the absence of the compara-tive effectiveness studies on new tech-nologies and techniques that arerequired to address the issue of spiralinghealth care costs. A new era in medicinehas dawned: Prove it or lose it.
Cheryl Proval is the editor ofRadiology Business Journal and vicepresident, publishing, The ImagingCenter Institute, Tustin, Calif;[email protected].
Reference1. The imaging boom. Health Aff(Millwood). 2008;27:1466-1521.
Prove It
By Cheryl Proval


10 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
Radiology: Ancillary No More
THE BOTTOM LINE
BY HOWARD B. FLEISHON, MD, MMM
Under the 1989 Stark legislation,radiology services, both diagnos-tic and therapeutic, were classi-fied by Medicare as ancillary.
Medical imaging and radiation therapy werecategorized as comparable to laboratoryservices, physical therapy, occupational ther-apy, speech/language pathology, durablemedical equipment and supplies, nutritionaltherapy, prosthetics, home health services,and similar fields.
The word ancillary is derived from the Latinancilla, which means maid. As an adjective,ancillary is defined as subordinate, auxiliary, orsecondary. The context of the term’s use, with-in the Stark legislation, was the intent toaddress self-referral abuses within those serv-ices that were considered extensions of physi-cian-office visits. These services included testslike chest radiographs, or even ultrasoundexams in obstetrician/gynecologists’ offices.Such services, arguably, serve as extensions ofthe stethoscope in the new age of technology.
As we all know, modern radiology is by nomeans ancillary. Studies, particularly thoseacquired on high-tech equipment, are usual-ly scheduled and performed at separate vis-its, and commonly at different locations thanthose of the originating office visits. Theseare not incidental exams, and they should nolonger be classified as ancillary. The ACR cur-rently is presenting this argument to CMS inan attempt to address the in-office exemp-tion loophole on which most self-referralmodels rely for their justification.
Radiologists (and many referring physi-cians) realize that medical imaging is vital toevidence-based medical care. The boomingrate of utilization for imaging tests is a testi-mony to the importance of radiology as adiagnostic imperative. For example, up to75% of all emergency-department patientsreceive some sort of medical imaging.
The perception that radiology is some-thing less than real medicine, however,somehow persists in many circles—includingamong some physicians, the public, and,unfortunately, politicians and regulators. On
November 17, 2008, in the South Florida Sun-Sentinel, Ted Epperly, MD, president of theAmerican Academy of Family Physicians, wasquoted as saying, “America won’t be caredfor properly by having a million radiologistsand dermatologists. We’re producing thewrong doctor work force for America.” Duringthe 2008 ACR branding campaign, it wasdetermined that only about 50% of the pub-lic was aware that radiologists are doctors.
We also are contributing to this mispercep-tion. Our business models have emphasizedincreased productivity in order to make up fordecreasing reimbursement. Some conse-quences of these new priorities includedecreasing communication and contact withthose we serve. The diffusion of PACS and tel-eradiology into our practices and hospitals hassignificantly reduced our direct interactionswith referring physicians. Night-coverage serv-ices have led others to conclude that radiologycan be commoditized. Put the CT data into ablack box and an interpretation will appear.
Take a look at modern ECG machines. Acomputer-aided detection program types outthe preliminary report before any physiciantouches the study. Automation is challengingthe value proposition of some physicians’professional services, including ours.
ADDED VALUEThe problem with this path is that it dis-
counts the added value that we, as physi-cians, bring to the health care enterprise.Radiologists are the experts in image inter-pretation, but we do much more. We care forthe patient, assume the responsibility forcommunication and follow-up, attend to con-trast reactions, determine appropriateness,maintain protocols, monitor radiation safety,administer conscious sedation, and serve asmedical directors for our hospitals andoffices. Those reading this article could addmany more responsibilities.
We also add value, in the business ofmedicine. We have established practice mod-els that can handle large volumes of encoun-ters. Radiology groups have developed orga-
nizational structures that have served tomanage large numbers of physicians.
Radiologists must re-establish their rolesas physicians integral to the health careenterprise. We are, first and foremost, physi-cians. We all went to medical school beforewe went into radiology. Our focus is on takingcare of patients.
There are numerous opportunities, everyday, for us to promote ourselves and the spe-cialty. Talk to patients, introduce yourself tothe patient as his or her radiologist, call refer-ring physicians with important results, makeyourself available for consultations, contributeto community functions, become a member ofhospital staff committees, be active in medicalsocieties, and coordinate facility visits for yourlocal, state, and federal politicians.
Radiology has been blessed over the pastfew decades. Radiologists have been remu-nerated well while enjoying professional sat-isfaction. We must not fall victim, however, toour own success through apathy. We all havea responsibility to raise the profile of our spe-cialty. Residency directors can indoctrinatethe next generation of radiologists by priori-tizing patient interaction and communicationin their training programs.
The importance of medical imaging, andthe promise of its future, secure its claim inany paradigm to be considered in the healthcare reform debate. Our relevance as radiolo-gists, however, depends on the value that weadd to our machines and methods. Our chal-lenge is to communicate that, as physicians,our imaging services are vital to medicine,patient care, and the health care enterprise.
Radiology has a great story. Let’s go outand tell it.
Howard B. Fleishon, MD, MMM, is a diag-nostic radiologist; past president of ValleyRadiologists, Phoenix; and cofounder ofSouthwest Diagnostic Imaging Ltd, Phoenix.He is a member of North Mountain RadiologyGroup, Phoenix, a hospital-based practice,and he serves on the ACR Council SteeringCommittee.
Radiologists must counteract practice developmentsthat can result in trivializing their specialty’s contributions to medicine


Due to inequities in paymentmethodology, are providers ofimaging services overpaid?
That question is raised, along with oth-ers, in a provocative article by Winter andRay,1 two analysts for the MedicarePayment Advisory Commission(MedPAC), that was published in a recentissue of Health Affairs. In examining thegrowth in imaging and Medicare’s methodof paying for imaging, the authors identifyseveral weaknesses in the paymentmethodology that may lead to inaccuraterates, and they suggest some options toimprove the system. While much of theinformation in the report had been previ-ously published, the MedPAC analyststake this opportunity to reply in the affir-mative to the above question.
The authors first review the now-famil-iar data charting the outlier growth of imag-ing (61%), compared with all physicianservices (31%), between 2000 and 2005, aspaid under the Medicare Physician FeeSchedule (MPFS). In fact, Medicare spend-ing on imaging paid under the MPFS prac-tically doubled between 2000 and 2005,from $6.4 billion to $12.3 billion.
After describing the mechanics ofphysician reimbursement under theMPFS, the authors identify what theycharacterize as inaccuracies in the distri-bution of payments among all physicians,even after accounting for the DRA cuts,the discount for contiguous body parts,and impending declines in payment thatwill accrue through 2010 due to a recentrevision to the methodology CMS uses tocalculate practice-expense RVUs.
12 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
PR IO RS{PR IO RS}
Until 2007, payment for practiceexpenses not involving physician work—including imaging services—was based onphysician charges from 1998. CMS beganphasing in new methodology in 2007;when it is fully implemented in 2010, thiswill result in an estimated 9% decline inpractice-expense RVUs for all imagingservices. This decline notwithstanding,practice-expense RVUs for imaging servic-es may still be overvalued due to the fol-lowing shortcomings, the authors contend.
THREE SYSTEM WEAKNESSESOne weakness in the system, the
authors believe, is the overstatement ofequipment costs. Due to the expensivenature of high-end imaging technology,
equipment costs account for a large per-centage of practice expenses. The authorsoffer the example of an MRI of the brain,for which equipment costs account for90% of the total direct cost of the proce-dure. For a chest radiograph, equipmentcosts account for just slightly more thanhalf of the direct cost of such a procedure.
The per-unit cost of a procedure isbased on the number of minutes that theequipment is used multiplied by its costper minute. The authors posit that recentadvances in imaging technology that haveresulted in shorter scanning times, such as64-slice CT and 3T MRI, mean that thetimes per scan generated in 2002 and2003 by the AMA’s RVU UpdateCommittee (RUC) may result in an over-valuing of the practice expense for someprocedures.
They also point out that CMS uses aformula that spreads the cost of the tech-nology over the number of minutes thatthe scanner is expected to be operatingduring its useful lifetime to derive theequipment cost per minute. Another fun-damental assumption used by CMS is thatthe equipment is in operation 50% of thetime that the site is open for business.
The authors report that a MedPAC-sponsored survey in six markets foundthat MRI scanners are used during 91%of operating hours and CT scanners areused during 73% of operating hours(MedPAC recently voted to recommendthat the secretary of HHS increase theequipment-use standard to 90% for MRI,CT, and PET scanners). The authorsbelieve that CMS would be encouraging
H E A L T H P O L I C Y
feb_9-09_08.indd 1 2/4/09 1:32:55 PM
Further TC Cuts Ahead?

S
feb_9-09_08.indd 1 2/4/09 1:32:55 PM

14 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
the efficient use of high-tech equipmentwith a 90% use rate.
A second inequity of the system thatfavors higher costs for imaging services isthe fact that CMS began using new prac-tice-expense data in 2007 for the eightspecialties that responded to CMS’ invita-tion to submit new data. The authorsbelieve that this has resulted in all of thoseeight specialties, including radiology andcardiology, receiving a higher value forpractice expenses than those specialtiesthat did not submit new data.
Cardiology’s hourly practice costs, forinstance, more than doubled, from $82per hour to $184 per hour. The authorsbelieve that, had radiology not submit-ted new practice-expense data, imagingpractice-expense RVUs would havedeclined by 20% instead of 9% by 2010.The authors believe that CMS needs cur-rent practice expense data from all spe-cialties in order to achieve an equitablesolution.
The third point made by the authorsrelates to the three separate geographicpractice-cost indices (GPCIs) used toaccount for differences in price inputs forphysician costs. The authors point out that
the GPCI does not recognize that individ-ual services have different shares of inputsfor which prices vary geographically (suchas nonphysician staff and office space) andfor which prices are uniform (such asequipment and supplies).
Therefore, for services with above-average costs for equipment, such asimaging, the index adjusts too large aportion of the practice-expense payment;for services with low equipment costs,the index adjusts too little of the cost.The average share of practice expensesrelated to equipment for all physicianservices is 14.6%, but equipment andsupplies account for 60% of the practiceexpenses associated with MRI of thebrain. In assuming that 14.6% (ratherthan 60%) of the practice expense of anMRI is related to equipment, the GPCIallows too much of this payment to varygeographically.
The authors believe that this may resultin overpayment for imaging in high-costareas and underpayment for imaging inlow-cost areas. On the other hand, equip-ment accounts for just 7.5% of an officevisit, so the index allows too small a shareof the practice-expense payment for an
office visit to vary geographically. Theauthors suggest that this may result infewer office visits and excessive imaging inareas with high input costs. MedPAC hasdiscussed an alternative practice-expenseGPCI that would exclude equipment andsupplies, at least for those services withhigh equipment costs, such as high-techimaging.
OPTIONS FOR ACHIEVING EQUITYThe authors conclude that inaccuracies
in how Medicare pays for the practice-expense portion of physician services maybe driving the overutilization of imaging.They ask CMS to request a review of CTand MRI codes by the RUC, to ensureaccuracy; to acquire more current prac-tice-cost data for all specialties; and toconsider using an alternative GPCI thatwould recognize that different serviceshave larger portions of costs that do notvary geographically.
—C. Proval
Reference1. Winter A, Ray N. Paying accurately forimaging services in Medicare. Health Aff(Millwood). 2008;6:1479-1490.
It’s no secret that utilization control hasemerged as the method of choice forprivate payors focused on reining inimaging costs. What is surprising is
the speed with which radiology benefitmanagement (RBM) companies havebrought the commercial-payor marketunder the influence of precertification. Atthe end of 2005, RBMs covered approxi-mately 25% of all lives in the commercial-payor market, but by the end of 2008,market penetration surpassed 60%, ShayPratt, practice manager, The AdvisoryBoard, Washington, DC, believes.
Pratt addressed Advisory Board mem-bers in his Outlook for Imaging Paymenton December 3, 2008, at the University ofChicago’s Gleacher Center. “For 2009, wecan probably expect a bit of a slowdownfor further precertification adoption, butwe are approaching 70% of the commer-cial market covered by precertification,”
he notes. “These programs are here to stay;they are entrenched.”
Precertification loomed large in Pratt’soutlook, due in part to the growing influ-ence of RBMs and their impact on volume.The top five companies—NationalImaging Associates, CareCore, AmericanImaging Management, MedSolutions, andHealthHelp—together cover an estimated130 million lives.
Based on the premise that RBMs aredenying an average of 15% of referrals inthe outpatient imaging market, Pratt esti-mates that precertification blocked morethan 2.5 million CTs and 1.5 million MRIsfrom getting to outpatient scanners.
Just how great an effect precertificationis having is best understood when thoselosses are translated into dollars.Precertification eliminated more than $1billion in CT and MRI revenue in 2008alone. The Advisory Board based these
estimates on rates of 150% of Medicarepayment levels.
THE MODELSIn formulating his overall outlook for
imaging, Pratt took into account three fac-tors: volume, price, and provider supply.Even here, however, RBMs and precertifi-cation figured largely. “With volume, oneof the most important questions is this:Will private payors still cling to precertifi-cations, or are there any alternatives thatare emerging that might give providerssome relief?” he asks.
“Precertification is having a very realeffect on hospital bottom line,” Pratt notes.In modeling annual procedure volumes tocalculate how much volume and revenuehospitals are losing to precertification,Pratt estimates that a radiology depart-ment doing 30,000 CTs annually is losing1,942 exams, or $1.08 million in revenue.
Under the Influence of RBMs

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 15
Hospitals with an annual MRI volume of13,500 would lose an estimated 1,014MRI procedures to precertification, or$806,117.
Because RBMs require referring physi-cians to obtain the precertification, hospi-tals often find themselves in the difficultposition of either withholding imagingprocedures or absorbing the cost if thepaperwork is not in order. “Hospitals arebeing held accountable financially forreferring physicians getting this right, butat the same time, we are barred, technical-ly, from participating in this process,” Prattexplains. “There is a lot of experimentationacross the country, with hospitals as wellas imaging centers trying to take a moreactive role in the process.” Pratt outlinesfour models that The Advisory Board hasobserved providers using to obtain precer-tification for imaging examinations.
The first is the precertification-initia-tion process. The provider’s staff contactsthe RBM or payor to initiate the precertifi-cation process on behalf of the referringphysician. The referring physician mustconclude the process with each request.
The second model is a precertification-acquisition service. The provider’s staffcontacts the RBM or payor for the referringphysician and acquires the precertificationnumber for the referring physician.
The third is an external precertificationoffice. The provider establishes an inde-
pendent office to acquire precertificationsfor referrers, and referrers pay a fee, at fairmarket value, per order.
The fourth model is outsourced precer-tification acquisition. A third-party entitywith no financial relationship to the imag-ing provider or referring physician obtainsthe precertification on a fee-per-order basis.
Pratt warns providers to proceed withcaution in participating in the precertifica-tion process, as RBMs have been inconsis-tent in their acceptance of these models, andsome may cause hospitals to run afoul ofanti-kickback regulations. “The waters arebeing muddied here in terms of what isallowable, what is not,” Pratt notes, addingthat a recent OIG opinion appeared toapprove of the outsourced precertificationmodel. “We have yet to see a case go to courton this, so right now, it is a bit of a free-for-all,” Pratt adds.
THE OUTLOOKWhile Pratt believes that precertification
is here to stay, he also sees signs that thedoor is opening to decision support. BlueCross of Massachusetts has three types ofprograms for radiology ordering, includingan alternative radiology-management pro-gram that excuses physicians from the reg-ular precertification process if they runtheir orders through a decision-supporttool, Pratt reports. He also cites a programin Minnesota that permits referring physi-
cians to order outpatientimaging procedures usingdecision support in lieu ofprecertification.
“The overall messagethat decision support maybe a viable option in thefuture is encouraging, evenif it does potentially requiresome investment on yourpart,” he says. “Playing amore active role in theappropriateness of imagingis going to be increasinglyimportant in relationshipswith payors, and also indemonstrating overall qual-ity: right scan, right patient,and right time.”
Despite the obstacles,Pratt’s outlook is fairly san-guine for imaging providers.Imaging volumes continue to grow, andradiologic procedures continue to con-tribute the lion’s share of profit amonghospital-based outpatient services. “Forhospitals, especially, it is still key toremember how important imaging is tooverall financial health,” Pratt notes. “Ithink we are still in that golden period ofphysicians learning what imaging can dofor them, particularly on the advancedimaging side.”
—C. Proval
UT
ILIZ
AT
ION
{PR
IOR
S}
Thoughtful Management for Hard TimesBY DANIEL McLAUGHLIN
Historically, financial downturns have notaffected the health care industry, but it is notso this time. Patients are deferring care oravoiding treatment completely; uncompensat-
ed care and bad debt are rising; and the impact is beingfelt by all provider organizations, both large and small.
Out of necessity, practices are responding. Some of thesereactions are thoughtful, but unfortunately, many appear tofocus on short-term, bottom-line fixes. This is very signifi-cant, as many gains in long-term quality improvements andcost management achieved during recent years may be lostthrough poor decisions being made today.
Industries outside health care have a more robust history of coping with mar-ket swings. Therefore, it is useful to learn from their experiences and understandhow they have preserved the core values of their organizations as they have navi-gated tough times.
S T R A T E G I C P L A N N I N G
Daniel McLaughlinDaniel McLaughlin

16 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
Be open with employees about the businessproblems you face and invite them to be partof the solution, while encouraging them tomeet critical needs in other parts of theirlives. Do this correctly and you’ll reducestress, decrease wasted time, boost trust,build resilience, and improve productivity.
Acknowledging the pressure thatemployees feel during downturns andpaying attention to employees’ livesbeyond work shows concern for the wholeperson and will be rewarded with loyaltyand extraordinary effort.
THE WISDOMOF CROWDS
Erickson3 suggests that, during toughtimes, executive instinct drives greatercontrol; executives review costs, tightenapproval criteria, redirect key decisions tohigher levels, ensure that everyone is asbusy as possible, narrow the scope of thebusiness, and so on. Small teams of exec-utives attend secret retreats to reviewoptions, even as meetings that wouldbring all the troops together are canceled.As a result, authority becomes centralized.
What leaders frequently forget, in theheat of crisis, is that the wisdom of crowdsapplies within their own companies.Instead of hogging the ball during a down-turn, they ought to tap the ideas and theenergy of the entire organization.
ADAPTIVE LEADERSHIPAn extension of all of these recommenda-
tions is another very useful approach tochange that is used by many industries:adaptive leadership. Heifetz4 developed thismodel at Harvard, and it focuses on success-ful change management.
Change can take two forms. Technicalchange uses existing knowledge and skills;an example would be expanding a clinic’sspace, but using existing staff and proce-dures to operate the new space. In con-trast, adaptive change requires individualsand groups to generate new knowledge,skills, and behaviors. An example of adap-tive change would be the installation ofnew software that changes work processesand roles within a clinic.
Conflict and ineffective change occurwhen a technical fix is applied to an adap-tive problem. This phenomenon is particu-larly widespread in health care due to itstechnical and scientific base. Adaptive prob-lems usually cannot be successfully solvedby someone who provides answers based
The December 2008 issue of HarvardBusiness Review provides a useful focus onthis topic: Staying Calm at the Center ofa Storm. Health care leaders can learnuseful approaches from these well-respected industry leaders and consult-ants. Three articles from this issue will beparticularly helpful to the strugglinghealth care leader.
STRATEGIC BUDGETINGKaplan and Norton1 (inventors of the
balanced scorecard) suggest that challeng-ing financial times providethe motivation to focus onproductivity improve-ments. They also cautionreaders that cost reduc-tions can sometimes sacri-fice strategic initiativesthat will build capabilitiesfor long-term strategicmanagement.
To avoid this dilemma,they recommend thatorganizations maintain andmanage a separate budgetfor strategic expenditures.To avoid the easy financialreflex of deferring theseexpenses, successful organ-izations specifically inden-tify each strategic initiativewith a budgeted amountand assign it to an existingmanager.
LOWER THE HEATFriedman2 cautions
against turning up the pres-sure and making employ-ees work harder. He advo-cates a smarter approach:
ST
RA
TE
GIC
PL
AN
NIN
G{P
RIO
RS}
on authority structures. To the contrary,adaptive work creates and demands bothindependence and interdependence of indi-viduals and teams.
Heifetz provides a number of strategiesfor successfully confronting adaptive chal-lenges. Find partners in the change, andbe sure to inform and involve even thosewho are opposed to change. As people’roles are revised, acknowledge the difficul-ty of change and accept their loss.
It is also very helpful to create a holdingenvironment. This could include an out-side facilitator to manage team meetings.An off-site retreat is helpful for examiningand planning adaptive changes whileacknowledging shared language and histo-ry. The pace of change must be carefullycontrolled, and if resistance to adaptivechange is increasing, a focus on technicalissues can help keep a major project ontrack. After the technical issues areresolved, the team can return to the adap-tive problem. Keeping the desired futurestate in front of the team is also necessary.
The most important aspect of successful-ly executing an adaptive change is giving thework back to the people. This is very diffi-cult for managers who pride themselves onbeing problem solvers who act decisively.Having the team itself devise new processesand roles for an adaptive challenge, howev-er, will provide robust and long-lastingchange for the successful organization.
Tough times can be stressful, and poordecisions can be made to solve immediateproblems. The wise manager, nonetheless,will use this time to reset, refocus, andstructure the organization for many futureyears of success.
Daniel McLaughlin is the director of theCenter for Health and Medical Affairs at theUniversity of St. Thomas, Minneapolis. He isthe author of Healthcare Operations Manage-ment and was formerly the CEO of HennepinCounty Medical Center, Minneapolis.
References1. Kaplan RS, Norton DP. Protect strategicexpenditures. Harv Bus Rev. 2008;86:28.2. Friedman SD. Dial down the stresslevel. Harv Bus Rev. 2008;86:28.3. Erickson TJ. Give me the ball! is thewrong call. Harv Bus Rev. 2008;86:30. 4. Heifetz RA. Leadership Without EasyAnswers. Cambridge, Mass: HarvardUniversity Press; 2003.


The CCTA Playbook:CCTA SERVICE | A Guide
By Jonathan Berlin, MD, MBA
In the United States, unspecified chestpain is the second most common rea-son for an emergency-departmentvisit. Each year, 5 million to 8 million
patients present to the emergency depart-ment with chest pain; in 2004, more than6 million patients presented to US emer-gency departments with acute chest pain.Of these patients, 4% to 5% have a coro-nary event that is not properly diagnosed,resulting in an erroneous discharge fromthe emergency department.
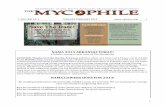
Approximately 40% of elective stresstests will yield false-positive results, butonly about 13% of coronary CT angiogra-phy (CCTA) exams (see Figures 1 through4) will have potentially false-positiveresults. The lower false-positive rate shouldmean better patient care and cost savings,which should be important to payors.
Market ForcesIn an acute situation, CCTA could
result in cost savings and better patientcare by decreasing unnecessary hospitaladmissions for chest pain. In addition, itsuse could decrease the incidence ofpatients being discharged from the hospi-tal if they have true disease.
In a 2007 study,1 54 low-risk patientswith chest pain who showed no acuteischemia on ECG then underwent CCTA.None of the 46 (85%) patients who weredischarged following negative CCTAresults experienced any coronary compli-cations within the 30-day follow-up peri-od. These findings support the conclusionthat CCTA may safely allow rapid dis-charge of patients with negative studies.
Given the well-documented sensitivityand specificity of CCTA, why is there hes-itation to reimburse for this exam on auniform national level? For a potentially
heavily utilized study, payors want out-comes data before approving reimburse-ment for new technologies. In the case ofimaging, that information can be extreme-ly difficult to obtain. Drugs and medicaldevices may have measurable effects onpatient outcomes, but diagnostic tech-nologies have a less direct connection with
patient outcomes because outcomes aremore likely to be altered by treatmentdecisions and patient compliance, amongother nonimaging factors.
It is clear, however, that utilization ofradiology services is increasing. Diagnosticimaging services paid for under Medicare’sphysician fee schedule grew more rapidlythan any other type of physician servicebetween 1999 and 2003. During the sameperiod, the average growth in physicianservices was 22%, but for imaging, it was45%. Imaging costs are growing at twicethe rate of prescription-drug costs, and maycontinue to grow at an accelerated rate.
These figures make imaging a target forcost cutting, even in areas where imaginghas great potential to reduce the total costof care. In 2007, for example, CMS pro-posed a restrictive national coverage deter-mination that would have required cover-age with evidence development, effective-ly restricting CCTA to research settings.
In January 2008, six professional soci-eties informed CMS that, if implemented,this policy would have a profoundly nega-tive effect on Medicare beneficiaries bylimiting needed access to CCTA for clini-cally appropriate indications. In responseto this and other public commentary, CMSwithdrew its proposal in March 2008,allowing Medicare carriers to retain theirown local coverage determinations. Untilpayors become convinced by furtherresearch that CCTA replaces other tests(instead of being added to them), a nation-al coverage decision resulting in the cre-ation of category-I CPT® codes for CCTA isunlikely to be made.
CodingThere are eight current CPT codes in
category III that are applicable to CCTA.
18 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
A compendium of the business intelligencerequired to launch a CCTA service
A Guide to Coding, Reimbursement, and Operations
Figure 1. Patient referred to cardiac CTangiography to rule out obstructivecoronary-artery disease was scannedon a Philips 256-slice Brilliance iCTscanner with a low-dose, prospectivelygated protocol, demonstrating a nonob-structive mixed (calcified and noncalci-fied) lesion in the left main artery. Im
age
cour
tesy
of M
artin
HK
Hoffm
ann,
MD,
unive
rsity
Hos
pita
l,Ul
m,G
erm
any.


20 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
CCTA SERVICE | A Guide
They are:• 0144T, for CT of the heart withoutcontrast material, including imagepostprocessing and quantitative evalua-tion of coronary calcium;• 0145T, for cardiac structure and mor-phology, CT of the heart before andafter contrast administration and fur-ther sections, including cardiac gatingand 3D image postprocessing;• 0146T, for CTA of the coronary arter-ies (including native and anomalouscoronaries and bypass grafts) withoutevaluation of calcium;• 0147T, for CTA of the coronary arter-ies with evaluation of coronary-arterycalcium;• 0148T, for cardiac structure and mor-phology with CTA of the coronariesand without coronary calcium scoring;• 0149T, for cardiac structure and mor-phology with CTA of the coronarieswith coronary calcium scoring;
Turf questions have always sur-rounded the provision and inter-pretation of coronary CT angiogra-phy (CCTA) studies. Who should
read these studies? Cardiologists and radi-ologists are unlikely to exclude each otherfrom interpreting these studies, but theapplication of standards may help bothspecialties ensure an emphasis on appro-priate training and experience as indica-tors of probable interpretation quality.
Professional standards are becomingincreasingly important as part of thereimbursement process as well. Forexample, Medicare carriers may requirecompliance with the specified levels ofcompetence for the professional andtechnical components of CCTA, as definedby the two guidelines issued by the ACR1
and the American College of CardiologyFoundation/American Heart Association(ACCF/AHA).2 For political reasons, twocompeting guidelines exist for cardiac CT;at this time, neither set of guidelines isuniversally accepted or endorsed.
Cardiology and Radiology Standards
The ACCF/AHA guidelines for qualify-ing to perform and interpret CCTA, issued
in 2005, were based on the contributions ofthe ACCF, the AHA, the American Society ofEchocardiography, the American Society ofNuclear Cardiology, and the Society ofAtherosclerosis Imaging, and they wereendorsed by the Society of CardiovascularComputed Tomography (SCCT). They speci-fy three levels of competence; in order tointerpret CCTA unsupervised, the physicianmust reach level 2 (contrast cardiac CT).
This level requires eight weeks of train-ing, the performance of 50 mentoredexams, and the interpretation of 150 men-tored exams (with the use of textbook andteaching-file reviews permitted). In addi-tion, the candidate must have completed20 hours of lecture instruction in general CTor cardiac CT. Continuing experience of 50contrast cardiac CT exams conducted andinterpreted per year is also required.
The ACR guidelines have separate criteriafor physicians with and without prior qualifi-cation in CT interpretation. Physicians whohave prior qualification in CT interpretationshould meet one of two requirements. Thefirst calls for the completion of at least 30hours of CME training in cardiac anatomy,physiology, and pathology and in cardiac CTimaging. The second calls for interpretation,reporting, and/or supervised review of at
least 50 cardiac CT examinations in thepreceding 36 months; coronary-artery cal-cium scoring does not qualify for inclusionin meeting these requirements.
For physicians without prior qualifica-tion in CT interpretation, the ACR guide-lines require completion, within the spe-cialty practiced by the physician, of atraining program approved by theAccreditation Council for GraduateMedical Education, plus 200 category-1CME credits in the performance/interpre-tation of CT exams. In addition, the physi-cian must have completed, under super-vision, during the preceding 36 months,the supervision, interpretation, andreporting of 500 cases, at least 100 ofwhich must be thoracic CT or thoracic CTA(with coronary-artery calcium scoringbeing exempt).
The candidate must also complete 30hours of category-1 CME in cardiac imag-ing and interpretation, as well as thereporting and/or supervised review of atleast 50 cardiac CT exams in the previous36 months. Again, coronary-artery calci-um scoring is not counted toward thistotal. The ACR has an additional practiceguideline for CCTA that advocates inter-preting physicians having a knowledge of
CCTA STANDARDS AND TURF
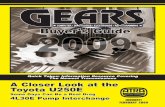
Figure 2. Cardiac CT angiography showing left anterior descending arterystent, acquired using a prospective scan protocol with the time frame of oneheartbeat on Toshiba’s Aquilion ONE.
Imag
e co
urte
sy o
f Tos
hiba
Am
erica
s M
edica
l Sys
tem
s,Tu
stin
,Cal
if.

Can cardiologists learn to describethese findings? Probably; with propertraining, there is no reason to believe thatcardiologists cannot learn how to inter-pret the noncardiac portions of a chestCT. As such, the requirement that inter-preting physicians also read the chestportion of the exam probably does notshield radiologists from turf incursions.There is, however, another question thatit is important to ask in this context: Willphysicians want to interpret these examsif they are reimbursed only at a low level?
—Jonathan Berlin, MD, MBA
References1. Weinreb JC, Larson PA, Woodard PK, etal. ACR clinical statement on noninvasivecardiac imaging. J Am Coll Radiol.2005;2:471-477.2. ACCF/AHA clinical competence state-ment on cardiac imaging with computedtomography and magnetic resonance.Circulation. 2005;112:598-617.3. Gil BN, Ran K, Tamar G, Shmuell F, Eli A.Prevalence of significant noncardiac find-ings on coronary multidetector comput-ed tomography angiography in asympto-matic patients. J Comput Assist Tomogr.2007;31:1-4.
the entire chest, as well as a knowledgeof the administration of contrast media.
Outside the HeartRadiologists cannot assume that
CCTA technology will be their soledomain. Cardiologists, like radiologists,are already involved. They conduct andattend CME courses on CCTA that aregeared for cardiologists.
They are also instrumental in the SCCT;founded in 2005, it already has more than3,900 members, many of whom are cardi-ologists (as are 12 of its 16 board mem-bers). As its advocacy mission, the SCCTis dedicated to ensuring that competent,skilled physicians—regardless of special-ty—can perform (and be reimbursed for)cardiovascular CT procedures.
The turf questions involved in per-forming and interpreting CCTA are compli-cated by the fact that extracardiac find-ings are common in patients who under-go CCTA. For example, of 258 consecutiveCCTA patients in a 2007 study,3 56.2%had significant noncardiac abnormalitiesseen on CCTA. These included lung andpericardial abnormalities, liver disease,adrenal masses, and bone lesions in adja-cent ribs or vertebral bodies.
www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 21
• 0150T, for cardiac structure andmorphology in congenital heart dis-ease; and• +0151T, an add-on code for func-tion evaluation (left and right ventric-ular function, ejection fraction, andsegmental wall motion).In general, codes that specify structure
and morphology are for use with pre-electrophysiology CT studies. These maybe ablations, in which the atria and pul-monary veins are being evaluated by CT,
or may be evaluations of the cardiacvenous system in anticipation of biven-tricular pacemaker placement. There are,at present, two separate category-I codesfor 3D rendering, but they should not beused for CCTA because 3D imaging isalready included in the T codes.
The triple–rule-out CCTA study(Figure 3, page 22) is often ordered toevaluate the patient for coronary-arterystenosis, aortic dissection, and pulmonaryembolism. For this study, it is possible to
use two codes: 71275 (conventional CTAevaluation of the aorta and pulmonaryvessels) and 0146T (CTA of the coronaryarteries). Billing for both codes mightrequire advance beneficiary notice for theT code plus a modifier of reduced profes-sional service for one of the codes (a 52modifier); this may be difficult if thepatient is in acute distress. For this reason,it may be preferable to bill for the catego-ry-I code (71275) and write off the cardiacportion of the exam.
ICD-9 codes supporting medicalnecessity for 0146T and 0147T (CTA) are413.0, 413.1, and 413.9 (angina pectoris,decubitus, Prinzmetal, and unspecifiedangina); 427.31 and 427.32 (atrial fibrilla-tion/flutter); 786.50, 786.51, and 786.59(chest pain: unspecified, precordial, andother chest pain); 747.41 and 747.42(total/partial anomalous pulmonaryvenous return); 786.05 (shortness ofbreath); 414.8, 425.4, and 746.85 (chron-ic ischemic heart disease, cardiomyopathy,and congenital heart anomalies); 428.0(congestive heart failure, unspecified);and 794.30 (cardiovascular, abnormalfunction study, unspecified).
ICD-9 codes supporting medicalnecessity for cardiac structure and mor-phology codes 0145T, 0148T, and 0149Tinclude 427.31/427.32 (atrial fibrilla-tion/atrial flutter); 428.0 (congestiveheart failure, unspecified); and 425.4(other primary cardiomyopathies).
ReimbursementAt this time, and in all cases, the pro-
fessional component for CCTA reim-bursement is carrier priced (locally deter-mined). When CCTA is performed in anoutpatient imaging center, the technicalcomponent is carrier priced. Each carrierissues its own policy (local coverage deter-mination) regarding category-III codes.These determinations state whether thecode will be reimbursable and what crite-ria must be met for reimbursement. All 50states have local coverage determinationsin place for CCTA, and many are based oncommon language taken from a modeloriginally submitted by the ACR andother professional societies.
In one example of a carrier’s local coverage determination on CCTA
Jonathan Berlin, MD, MBA
At this time, and in all cases, the professional component for CCTA reimbursement is carrierpriced (locally determined).

22 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
CCTA SERVICE | A Guide
reimbursement, Wisconsin PhysicianServices (the local Medicare carrier forWisconsin, Illinois, Michigan, andMinnesota) specifies the four main cate-gories of indications for which CCTA willbe reimbursable. The first category isCCTA used as an alternative to invasiveangiography following an equivocal stresstest or one that is suspected to be inaccu-rate. CCTA, in this case, could provide aseparate method of assessing coronaryarteries (different from a stress test) andlimit the number of normal invasive coro-nary angiograms. CCTA may also help cli-nicians avoid missing coronary-artery dis-ease in patients suspected of having under-gone inaccurate stress tests.
The second indication category isevaluation of acute pain in the emergencydepartment. The exam can be used totriage patients quickly in the emergencydepartment and limit resource use inchest-pain patients who do not havecoronary-artery disease.
The third category is assessment ofcoronary or pulmonary venous anatomy.This includes presurgical planning prior topacemaker placement or pulmonary veincatheter ablation to eliminate recurrentatrial fibrillation.
The fourth category is assessment ofsuspected congenital anomalies of coro-nary circulation. Here, CCTA allows fur-
ther characterization of the presence of(and possible harm from) congenitalabnormalities; it may also be useful forsurgical planning in such cases.
Wisconsin Physician Services alsoimposes six exclusion criteria that may betypical of those found elsewhere. First, thetest is never covered for screening inasymptomatic patients. Second, the testmay be denied on postpayment review ifthere is sufficient pretest knowledge ofextensive calcification of the coronary seg-ment that would diminish interpretivevalue. Third, the multidetector CT usedmust have at least 64 slices per rotationand high-resolution slices of 1 mm or less.
Fourth, all studies must be ordered by aphysician or a qualified nonphysician prac-titioner. Fifth, when contrast is given, aphysician must be present for direct super-vision during testing. Sixth, atrial fibrilla-tion, by itself, is not an indication, but atrialfibrillation with planned ablation is allowed.
It should be noted that CCTA codesinclude the administration of beta blockersand the monitoring of the patient during theexam by a physician who is experienced inthe use of cardiovascular drugs, so these arenot separately payable services. Likewise,the administration of sublingual nitroglyc-erin is unlikely to be separately payable,although it may improve results by dilatingthe coronary arteries before scanning.
Medicare coverage for repeat CCTAexaminations is also determined by indi-vidual carriers, but reimbursement for fre-quent CCTA repetition is probably unlike-ly. The frequency of the studies must bereasonable and justified by the course ofthe patient’s illness, according to some car-riers’ utilization guidelines; this means thatreimbursement may be denied for repeattests for the same patient. In California,one Medicare carrier, National HeritageInsurance Co, has stated that it is not nor-mally reasonable to repeat CCTA in lessthan five years if the patient’s calciumscore is less than 10 (or the equivalent) onthe initial study; when the score is higherthan 10, it is not usually necessary torepeat the study in less than three years.
Empire Medicare, a carrier for NewYork and New Jersey, stresses the need forCCTA to produce usable information. Itstates that the selection of the test shouldbe made within the context of other testingmodalities, such as stress myocardial per-fusion images or cardiac ultrasoundresults, so that the resulting informationfacilitates the management decision insteadof merely adding a new layer of testing.
Planning for CCTABecause of variations in local carriers’
policies and general uncertainty, it is diffi-cult to predict the reimbursement level
Figure 3. Reconstruction of the thorax acquired in 0.8 secondson Siemens’ SOMATOM Definition Flash.
Figure 4. A 3D view of the coronary tree showing a stent, reconstructed using Vitrea Web.
Imag
eco
urte
syof
Siem
ens
Heal
thca
re,M
alve
rn,P
a.
Imag
eco
urte
syof
Vita
lIm
ages
,Min
neto
nka,
Min
n.

have already begun to fill this niche; forexample, they may offer processing andpreliminary interpretation of CCTA and oftriple–rule-out CTA as needed, around theclock. They may also provide images of allthe major coronary arteries and a prelimi-nary reading that indicates disease in anyof those vessels.
Those practices intending to offer CCTAexams must determine carefully whetherthis kind of external after-hours service isnecessary, as well as whether the practicecan afford it—and whether it is wise topurchase such services. Will outsourcingonly commoditize radiologists’ services?
Some practices may consider havingthe CCTA source images sent to the hometeleradiology units of their radiologists forafter-hours interpretation. Because thereis the potential for data overload, however,they should consider four questions. First,how long will it take to send all the axialimages to a radiologist’s home unit?Second, can the radiologists involved per-form reconstruction or volume renderingat home? Third, if they can, how long willthat take? Fourth, are reconstruction andvolume rendering necessary in all cases?The provision of CCTA studies may neces-sitate rethinking the need for 24-hour in-house attending coverage.
—Jonathan Berlin, MD, MBA
Radiology practices and depart-ments that intend to offer coronaryCT angiography (CCTA) need to con-sider how the additional exam vol-
ume and time commitments created by CCTAstudies will affect their operations and theirstaffing models. Will they need to hire addi-tional radiologists, nurses, and/or technolo-gists to manage the extra workload? Who willperform the necessary volume renderingsand reconstructions, and how long will it taketo perform them?
Some radiologists who interpret theseexams may insist on performing their ownreconstructions before interpreting the stud-ies. If so, how much of their time will thisrequire? Informal surveys indicate that thisstep could call for as few as 10 extra minutesper case—or as long as an hour. That hourmight be difficult to justify, and this possibili-ty of extreme variation in time requirements,in many cases, makes accurate operationalplanning difficult.
If additional personnel must be hired tointerpret CCTA exams and/or to performreconstructions, this will obviously increaseoverhead costs significantly, and any suchincreases should be factored into the prac-tice’s financial analysis of the merits of offer-ing CCTA services. This additional overheadexpense could mean that the practice willhave to accept lower margins for CCTA on aper-case basis.
In addition to evaluating overall changesin staffing needs that might be made neces-sary by CCTA, practices must should considerhow to provide after-hours coverage forthese studies. Since patients who present tothe emergency department with chest painare common candidates for CCTA, it is unlike-ly, in many settings, that the performance ofthese exams can be limited to the hours ofthe day shift.
Who will perform these studies at night?Who will perform the reconstructions afterhours? If your practice is based at an aca-demic hospital, it is important to determinewhether residents or fellows will have time toperform reconstructions and interpret examsat night as part of your decision to evaluatestaffing needs.
For private radiology practices, it is neces-sary to decide whether external after-hoursservices or local night-coverage staff will per-form reconstructions for CCTA. Companiesspecializing in after-hours radiology coverage
CCTA STAFFING AND COVERAGE
www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 23
that CCTA will eventually reach. Localcarriers and private insurers do reimbursefor CCTA, but it is important to ask atwhat payment rate they do so. Some car-riers have published the applicable rates,but these can’t be used to predict theeventual category-I reimbursement level.Accurate prediction isn’t possible becausethe data now being collected by the AMAon the utilization frequency of the eightcategory-III codes will influence which ofthese codes will survive the migration tocategory I, as well as whether some of thecodes will be eliminated or augmented.
It seems safe to predict, however, thattotal Medicare payments for CCTA willcontinue to rise. In 2006, Medicare paidfor roughly 70,000 CCTA exams at a costof $40 million to $50 million. As morefacilities perform CCTA, this amount willincrease. To limit overall expenditures,local rates could change (perhaps nega-tively) over time.
If it isn’t possible to predict rates, howcan providers approach planning forCCTA provision? Today, the bestapproach is to examine the nonfinancialfactors carefully, in addition to speakingto carriers individually about their poli-cies concerning the CCTA codes. Use ofthe self-pay system may also be feasiblefor patients who are not eligible for third-party reimbursement.
Jonathan Berlin, MD, MBA, is associateprofessor of radiology, NorthShoreUniversity HealthSystem, NorthwesternUniversity Feinberg School of Medicine,Evanston, Ill. This article has been adaptedfrom Business Issues Associated WithCardiac CTA: Coding, Reimbursement, Turf,and Operations, which he presented at theEconomics of Diagnostic Imaging 2008:National Symposium on October 23, 2008,in Arlington, Va.
Reference1. Hollander JE, Litt HI, Chase M, BrownAM, Kim W, Baxt WG. Computed tomog-raphy coronary angiography for rapid dis-position of low-risk emergency depart-ment patients with chest pain syndromes.Acad Emerg Med. 2007;14:112-116.

Masters ofManipulation
ADVANCED VISUALIZATION | Optimization
By Cat Vasko
Radiology stands on the cusp ofthe golden age of advanced visu-alization, with the two mostcommonly used high-tech
modalities, CT and MRI, increasinglyreliant on 3D reconstructions and 4Danalysis for examination interpretation. Asadvanced visualization for CT and MRIcomes of age—bolstered by augmentedprocessing power and ever-increasingtransmission speeds—how can radiolo-gists optimize the tools at their disposal forthe most rapid and accurate diagnoses?
Jeffrey C. Hellinger, MD, director of car-diovascular imaging and director of the 3DMedical Imaging Laboratory at TheChildren’s Hospital of Philadelphia, advo-cates an all-inclusive approach. Wheninterpreting cardiac CT angiography (CTA)exams, Hellinger uses a combination of alltools. “The tools have strengths and weak-nesses, advantages and disadvantages,” hesays. “I interact freely among volume ren-dering, maximum-intensity projection(MIP), multiplanar reconstruction (MPR),and curved planar reconstruction.”
Gary Wendt, MD, associate professor ofneuroradiology at the University ofWisconsin–Madison, finds that the limita-tions of advanced visualization for MRangiography (MRA) are more infrastruc-ture based. “One of the biggest problemsin advanced visualization, in general, isthe lack of universal accessibility,” he says.“The Web-based products are getting bet-ter, but they still have their flaws.”
Each subspecialty uses a differenttoolset, but they all have one commongoal: making interpretation as efficient aspossible. As MRI resolution improves and64-slice CT scanners gradually replaceolder 16-slice units, that goal is both clos-er and more remote than ever before.
Multislice CTThe evolution of CT scanners from 16
to 64 slices or more has meant an order-of-magnitude explosion in the number ofimages that compose a single study. Whilethis exponential increase takes its toll onnetworks and IT infrastructure, it alsoopens new doors, allowing more detailedvisualization of the heart than has everbeen possible.
“As the technology continues toadvance, it’s more important than ever thattrainees (from residents to fellows toattending radiologists from academic set-tings and private practice) learn to use aworkstation,” Hellinger says. “You’re notgoing to view each dataset with each tool,
but on the fly, in real time, it’s important toknow instinctively whether somethingwill be better with volume rendering, MIP,MPR, or curved planar reconstruction. Allthe tools have to be used in collaboration.”
C. Dan Johnson, MD, chair of thedepartment of radiology at the MayoClinic, Scottsdale, Ariz, specializes in CTcolonography. He emphasizes the impor-tance of learning the ins and outs of eachtool. “They all have their advantages anddisadvantages,” he says, “and they can allbe useful in complete analysis of thecolon.”
Johnson recommends striking a bal-ance between 2D and 3D visualization,stressing that both have roles to play incomprehensive interpretation. “With 2D
images, you have to put the image togeth-er in your mind, so sometimes it takes alittle problem solving to determine ifthere’s a polyp,” he notes, “but the 3D datamake discrimination of stool or residualbarium from polyps more difficult. Thevery best interpretation includes a primary
24 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
Radiologists and vendors race to grasp and improve the tools of advanced visualization as imaging modalities churn out ever more information
Jeffrey C. Hellinger, MD
You’re not going to view each datasetwith each tool, but on the fly, in real time,it’s important to know instinctively whethersomething will be better with volume rendering, MIP, MPR, or curved planarreconstruction.

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 25
2D review of the axial images, as well asthe 3D review.”
Hellinger’s most common cardiovas-cular CTA applications include pediatricand adult congenital heart disease andcongenital and acquired pediatric vascu-lar disease. He uses volume renderingand MIP for angiographic analysis andMPR as the principal tool for diagnosis.Johnson focuses on polyp detection and
finds simulated 3D flythrough and virtu-al dissection to be the most valuabletools in his arsenal. Both Hellinger andJohnson stress, however, that these toolsmust be used according to their strengthsand weaknesses for the best, most effi-cient interpretation.
“I always tell people to be flexible andapply every tool when appropriate,”Hellinger says. “If you’re not, then there’sno advantage of 3D imaging beyond thesource images. We can do everythingimaginable to make treatment planningefficient, but it’s really up to the end user.Radiologists have to know the principles of3D imaging. If they approach it in an edu-cated way, then everything’s in place forefficient interpretation and patient care.”
MRI’s Midlife CrisisAt 30 years old, MRI technology is
reaching middle age, with higher-resolu-tion 3T units dethroning their 1.5T prede-cessors. David Bluemke, MD, PhD, direc-tor of radiology and imaging sciences atthe US National Institutes of Health,Bethesda, Md, notes that the modality stillhas its limitations. “With cardiac MRA,we’re almost always looking for narrowingor stenosis. We use fairly straightforwardMIP tools, and the reason for that is it’svery quick—it can be done on the work-station or the PACS, and requires lesssophisticated processing than CT. Tools arebecoming available for automated detec-
Wendt concurs. “We’re a multiple-enterprise organization,” he says. “Weserve multiple hospitals and we have onePACS. We need a unified, single log-onfor advanced image processing, and itneeds to be tightly integrated with ourPACS. Otherwise, if you try to runadvanced image-processing tools in a tra-ditional manner, it becomes challenging.”
PACS IntegrationThe need for tighter PACS integration
isn’t limited to radiologists specializing inMRI. Johnson also cites workstation-based advanced visualization as a barrierto more efficient workflow. “Right now, Ido interpretation on separate, high-endworkstations, where the data are import-ed to the workstation for evaluation,” hesays. “It would be very helpful if thesetools were integrated into PACS. It prob-ably wouldn’t speed up my evaluationtime, but it would increase productivity ifyou didn’t have to leave your PACS andgo to a workstation to load up a study.”
Bluemke also sees the potential formore timely interpretation. “The ability todo rapid multiplanar imaging at the sametime as MIP is probably what’s mostimportant now,” he says. “Radiologistshave all those images on their PACS. It’shighly desirable not to have to go to aseparate workstation.”
Wendt looks forward to the wide-rang-ing operational efficiencies that could beachieved via full multiple-enterprise PACSintegration. “Then, you won’t need a wholeseparate deployment or a whole separatemethod for managing image flow,” he says.“When you’re trying to figure out howimages flow through multiple organiza-tions, you have to deal with managing flowacross multiple RIS and hospital informa-tion systems. If you have to deploy not onlyPACS, but also multiple advanced visuali-zation platforms, it gets impossible prettyquickly. How do you manage security, useraccess, and audit trails?”
Describing his vendor’s process, hesays that the company has had a thinclient for years. Now, he adds, “It’s inte-grating its thick client and thin client withthe integrated workstation thick client.It’s all four platforms converging onto oneback end.”
tion of stenoses, but so far, they haven’tcaught on,” he says. The principal issue isreliability; as he explains, “You need high-quality MRA studies, which are becomingmore commonplace, but can still be diffi-cult to get.”
Wendt, who specializes in neurologi-cal MRA, echoes Bluemke. “Doing thingslike stenosis quantification in MRI isimpossible. Advanced visualization tools
like automated stenosis measurement aremore applicable to CTA, where you canaccurately define a lumen. With MRA, it’smore about getting a quick, easy, targetedMIP,” he says.
Because much of the image’s back-ground information is suppressed withMRA, Wendt describes the visualizationand interpretation process as a quick-and-dirty approach. “It’s a technical limitationof the modality,” he says. “It’s nowherenear being as precise as CTA. MRA is allabout how fast you can get at it—how fastyou can generate the images.”
For Bluemke, the most interesting newadvanced visualization tools for MRI effec-tively leave behind the realm of 3D imag-ing to visualize flow. “These tools are new,and we don’t have a routine clinical appli-cation for them,” he says, “but 3D pointtracking of flow could be used to look atthe effect of flow on the vessel wall. They’reactually more 4D, because they’re timeresolved. You can look at the wall’s shearstress in 3D throughout the cardiac cycle.”
When it comes to incidental findings—including renal cancers, fistulae, or unsus-pected aneurysms—Bluemke turns to hisPACS for the right tools, such as thin-slid-ing MIP. “The most useful tools are thosethat are integrated into the PACS,” he says.“We’ve had very good software for sometime, but on very specialized and expensiveequipment. Integration is the key to gettingthe readings done quickly and accurately.”
These tools are new, and we don’t have a routine clinical application forthem, but 3D point tracking of flow couldbe used to look at the effect of flow on the vessel wall.
David Bluemke, MD, PhD

26 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
ADVANCED VISUALIZATION | Optimization
Hellinger looks forward to advancedvisualization integration not only withPACS, but also for reporting packages anddictation systems. “I think, in the next yearor so, we’ll begin to see deeper integrationwith all health IT,” he says, “and as weadvance the technology, education on 3Dimaging is more important than ever before.”
Choosing ClientsThe most daunting issue in advanced
visualization has nothing to do with thesoftware toolset, according to Wendt.Accessibility and cost are his concerns.“With the stand-alone workstations, whenyou have 15 to 20 of them, every time youdo an upgrade, you’re looking at a couplemillion bucks,” he says. “That’s pretty out-rageous. They have more functionalitythan thin clients, but the pricing gets outof hand really fast. Likewise, I think thereare vendors who oversell their thin clients.They claim to be 100% Web based, butwhen you hold their feet to the fire, itturns out that you do need to install soft-ware. I don’t know of any vendor that’struly 100% Web based right now.”
Bluemke takes a similarly measuredview of the thin-client technology current-ly available. “We’re not viewing in native
3D yet,” he notes. “The images are inher-ently 3D when they’re generated, butwe’re not routinely viewing them in 3D(Figure 1).” As advanced visualizationsolutions are incorporated into standardPACS and standard PC systems, however,Bluemke expects to see robust thin-clientvisualization systems proliferate.
Hellinger is more optimistic about thedirection in which the technology is head-ing. “First, you had thick clients; then,thin clients; and now, Web clients,” hesays. “The technology will only becomemore robust. Ten years ago, people werereally skeptical about the concept of thinclients. Now, they are the standard forimaging. I think the new standard will beWeb clients—no software, just an Internetbrowser where you log into a server toview and interpret studies (Figure 2).”
How is this possible? Wendt says thatwe have the Xbox 360® and SonyPlayStation 3®—among other gamingplatforms—to thank for coming advancesin the field. “The power that’s going intothe new graphics cards is going up expo-nentially, and it’s driven by factors wayoutside the medical industry,” he notes.“If you want cutting edge, check out theXbox. The amount of advanced graphics
processing that goes on in one game ismore than we do in two years.”
What’s NextAdvanced visualization evolves along-
side emerging clinical applications in radi-ology. What’s the next frontier in high-techimaging? For Johnson, computer-assisteddetection could mean a big improvementin productivity.
“Computer-assisted detection has yet tobe integrated in all of the commercialproducts yet, and I think it would be veryhelpful,” he says. “It may well be able toreduce the time on 3D review. If radiolo-gists just did the 2D review and looked forother detections on 3D with computer-assisted detection, it could reduce the 3Dinterpretation time and improve overallexam performance.”
Hellinger also looks for computer-assisted detection integration, and that’snot all. “I think there will be more of abridge between molecular imaging and 3Dimaging,” he says. “When you’re imagingat the genomic level with MRI and a radio-tracer, being able to diagnose, plan treat-ment, and guide treatment with greaterconfidence will be valuable.”
Meanwhile, Bluemke is most interestedin the potential for strain imaging of vesselwalls. “We could quantify what’s causingthe strain and the change in wall strainover time. That may relate to the progno-sis for aneurysm expansion and impend-ing dissection. It will probably be donefirst with echocardiography and vascularultrasound; I’d say it’s at least two to fiveyears away,” he says.
Further down the line, Hellinger expectsthe kind of anytime, anywhere interpreta-tive flexibility that’s becoming common-place in other areas of radiology. “The futureis being able to access a workstationremotely anywhere, anytime—in the hospi-tal, out of the hospital, or even from yourhandheld—with all these advanced tools,”he says. “There’s still a lot of innovation tobe done with 3D and 4D visualization, andthe success, over the years, has really beenthrough improvements in computers andtechnology. It will only get better.”
Cat Vasko is a contributing writer forRadiology Business Journal and the editorof ImagingBiz.com.
Figure 2. A sagittal oblique 3D MR angiogra-phy volume-rendered reconstruction throughthe thoracic aorta demonstrates high-gradejuxtaductal coarctation (long arrow). Note therobust collateral network that has developedto restore aortic flow below the coarctation.The network includes aortic-arch branch arter-ies, intercostal arteries, and a dominant postcoarctation collateral artery (short arrow).
Imag
e co
urte
sy o
f Dav
id A
.Blu
emke
,MD,
PhD.
Figure 1. The figure shows a volume-renderedimage of a coronary MR angiogram. The leftcoronary artery and its branches (largearrow) and right coronary artery (smallarrow) are shown.
Imag
e co
urte
sy o
f Jef
frey
C.He
llinge
r,M
D.
Kids aren’t the onlyones who have questionsWhen it comes to children’s CT scans, parents can have a lot of questions.
That’s why the image gently™ campaign has made parent education tools available to help clinicians answer these
questions and provide more information about radiation safety.
When parents ask about imaging precautions, direct them towww.imagegently.org for downloadable brochures and an
imaging record card to keep track of their child’s exams.
You’ll be empowering parents and yourselves to make better healthcare decisions.
Brought to you by the Alliance for Radiation Safety in Pediatric Imaging.
Proudly supported by GE Healthcare.
2389_KidsQuestionsAd_final.indd 1 2/4/09 3:08:57 PM

Kids aren’t the onlyones who have questionsWhen it comes to children’s CT scans, parents can have a lot of questions.
That’s why the image gently™ campaign has made parent education tools available to help clinicians answer these
questions and provide more information about radiation safety.
When parents ask about imaging precautions, direct them towww.imagegently.org for downloadable brochures and an
imaging record card to keep track of their child’s exams.
You’ll be empowering parents and yourselves to make better healthcare decisions.
Brought to you by the Alliance for Radiation Safety in Pediatric Imaging.
Proudly supported by GE Healthcare.
2389_KidsQuestionsAd_final.indd 1 2/4/09 3:08:57 PM

Data Mining:
DATA | Analytics
By George Wiley
Physicians and executives are simi-lar to scientists; they like data toassist them in making decisions,”Rob Cercek says. Cercek, vice
president of ambulatory services atRochester General Hospital (RGH),Rochester, NY, adds, “If you can put credibledata in front of people, discussions betweenhospitals and physicians become more
meaningful.” He is talking about arming hisdepartment representatives with data whenthey go out to solicit radiology businessfrom referring physicians, but he could justas easily be describing radiologists them-selves. Like physicians in any practice, radi-ologists are indebted to numbers foranswers to their operational questions: Arepractice RVUs stacking up in a positive way?Are imaging rooms and equipment beingused maximally? Are there too many (or toofew) technologists on staff?
Radiology managers and executiveslike Cercek are working diligently to cre-ate useful reports to guide themselves—
and their practices’ physicians—as theymake many types of decisions. Should anew clinic be opened? Should certain pro-cedures be marketed, or should they bequietly left to decline? Should productivi-ty be demanded, or will quality suffer iftoo much pressure is brought to bear?
Cercek says that some of the most help-ful reports have been those showing pat-
terns in physician referrals to the radiologydepartment at RGH. By comparing referralsfrom doctors on the hospital staff with thosefrom referrers outside the hospital, Cerceksays that he can gauge when a referringphysician is falling short of sending thenumber of cases that might be expected.The department representatives can then bedeployed to seek, politely, that missing busi-ness. Cercek says, “The people who usethese reports feel they are invaluable,” espe-cially for making it possible “to walk into thephysician’s office knowing the pattern—knowing what the referral rate should be—and getting them to turn in your direction.”
At RGH, which is licensed for 585 bedsand conducts about 175,000 radiologyexams per year, the RIS is at the heart ofthe data-gathering effort. The RIS, fromthe same vendor as the hospital’s PACS,collects patients’ demographic data fromthe hospital information system (HIS) andcorrelates them with radiology data fromthe PACS, such as exam types, exam times,and modalities used. When a radiologyreport is signed, the RIS also triggers thebilling cycle. All these data—exams, refer-ring doctors, technologist times, patientdemographics, billing codes, and muchmore—can be mined from the RIS in theform of either preprogrammed reports or,more pointedly, as customized reports pre-pared by the RGH staff.
Reports like those being done at RGHcan be used to shape (or reshape) a radiol-ogy practice. Moreover, the cost of thesoftware needed to issue reports is modest,by hospital standards. The return oninvestment for data-analysis software is sorapid (a matter of months) that many don’tbother to track it. At RGH, the work ofturning out most reports falls to PamMoseley, radiology informatics director.
A Data Gold MineWhen RGH installed its RIS, Moseley
says, the radiology department took overits own billing because the RIS could drivethat process. Now, when an exam is com-pleted, the patient data and radiology
28 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
RIS data, keyed to billing, can be analyzed to improve competitive capability and pare inefficiency to the nub
Imaging Executives Crunch the Numbers
If you can put credible data
in front of people, discussions
between hospitals and physicians
become more meaningful.Rob Cercek

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 29
data, including CPT® code and pricing,are automatically entered into the billingsystem via RIS. Billers in radiology makesure that all the data match, then send thebill to the hospital’s master billing systemfor the technical component and to thephysician’s billing system for the profes-sional component, Moseley says.
“Prior to this, everything was on paperand medical records was billing,” sheadds. “They’re not familiar with radiologyexams and functions; thus, there were alot of charges that weren’t being billed.”Since initiating semiautomated RIS-driv-en billing, Moseley says, the radiologydepartment’s receivables have shown a30% to 40% improvement. This hasadded up to hundreds of thousands ofdollars in recovered income. Moreover,billing time has dropped from more thantwo days to a day or less, she adds.
Moseley says that the RIS softwareturns out a number of automated reports,including patterns for the hospital’s top20 referrers, although this particular taskrequired special programming by the RISmanufacturer. Most of the reports thatMoseley submits to Cercek and others arecustom reports that she has completedherself, however. Custom reports of thiskind provide the real payoff when a hos-pital or practice wants to make immedi-ate adjustments to workflow, finances, orstaffing efficiency. At RGH, Moseley hasinitiated reports on staff productivity,
Moseley is now tracking patient-transport times via RIS in an attempt tojustify using radiology staff to transportpatients in beds or wheelchairs, insteadof a relying on the hospital’s centralizedtransport service. She says that toomuch downtime occurs when centraltransport is called; sometimes, its per-sonnel fail to bring patients on schedule,resulting in a schedule backlog, eventhough this is the favored approach ofhospital administrators.
According to Cercek, RIS data mininghas been especially useful for quick mar-keting response to changes in referral pat-terns. Efficiency inside the departmenthas also made the hospital more attractiveto referrers, he adds. He notes that a thirdof patients admitted to RGH comethrough the emergency department.Those emergency patients who needimaging are now entered into the RIS ona fast track.
“We were looking at a three-hourvisit in our emergency department forfast-track patients, and our competitorswere at 90 minutes. Of that three-hourvisit, 52 minutes were spent in theimaging department,” Cercek says.“Now, we have a target of less than 30minutes to perform imaging on fast-track patients to hit a visit time of 90minutes or less.” RGH now averages 28minutes for imaging studies in theemergency department. The order
room utilization, and even exam appro-priateness (based on initial indication).
“We get a lot of MRI orders from theemergency department,” she says, “butdoes the indication merit MRI? We haveto educate our physicians.” Moseley saysthat the custom reports that she com-pletes aren’t necessarily difficult,although some can get complicated (seesidebar, page 32). She says that herreports have affected staffing, modalityefficiency, and scheduling, as well as therecovery of lost billings. She notes thatthe RIS data can influence purchasingdecisions or reveal when imaging equip-ment is approaching the end of itsexpected lifetime, which is a key factor ina certificate-of-need state such as NewYork, where major equipment purchasesmust be justified to regulators.
“We’ve also adjusted staffing pat-terns—hours, lunches, and breaktimes,” Moseley adds. “The hospitalthought that we were overstaffed inradiology, but in actuality, we’re not.Report data are based on user input; inour case, the technologists were puttingin the incorrect time for how long ittook an exam to get done. They thoughtit was scan time, but it should havebeen time with the patient. Once thestaff was re-educated, a true cycle timewas reflected. Overall, our throughput-cycle time has shown an 80% improve-ment since we went to the RIS.”
Once the staff was re-educated, a true cycle time was reflected. Overall, our throughput-cycle time has shown an 80% improvement since we went to the RIS.
Pam Moseley

30 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
DATA | Analytics
issued for imaging triggers a time clock.Cercek says, “Before, we really didn’tknow how to hit that time. Now, we canput a time stamp on how long thosepatients are in radiology.”
Both Cercek and Moseley note thatRIS capabilities also play into the hospi-tal’s larger recordkeeping effort, alongwith the HIS data and the lab reports, allof which appear in the patient’s electron-ic medical record. Moseley notes that thecity itself is forming a regional healthinformation organization (RHIO) as acentral base for shared knowledge.When the RHIO is finished, the radiolo-gy reports will be available there “so thatthe whole city will be connected,”Moseley says.
Cercek agrees that some skepticismneeds to be applied to the reports that flowout of data repositories. “Whenever youreceive a report to review, you have togauge what it’s really telling you,” he says.“The RIS will never describe the benefitsor nuances of a 64-slice CT study versusan interventional procedure. You have tofinish the story.”
King’s Daughters HospitalA midsize hospital such as RGH is an
obvious fit for RIS data mining because itgenerates so much information, but evena small hospital can make profitable useof the technology. King’s DaughtersHospital (KDH) in Yazoo City, Miss, hassix doctors on staff and 25 acute carebeds. Stefanie Dendy, a former mammog-raphy supervisor at the University ofMississippi Medical Center in Jackson, isthe KDH director of radiology. Comingback to KDH five years ago was a home-coming for Dendy in the most basic sense;she was born at the hospital.
The radiology department at KDHincludes diagnostic radiography, nuclearmedicine, fluoroscopy, ultrasound, andCT. A mobile MRI unit appears on a regu-lar schedule. The department installed aPACS in 2006 and a companion RIS fromthe same vendor a year later. There are noradiologists resident at KDH; the singleradiologist on staff reads from a site inLouisiana. He was hired when the hospitalinstalled its RIS. Dendy says that KDHcompletes about 15,000 exams per year,
and that single radiologist reads them all.“No radiologist will come to our small
hospital anymore,” Dendy says.Nonetheless, she adds, competition is stiffamong outside providers. “Now, withPACS, everybody wants your business,”she says. At night, if the contracted radiol-ogist can’t be reached, the hospital willsend exams (CT only) to an after-hoursteleradiology service for preliminary read-ings, Dendy adds. She credits thePACS/RIS not only with making this pos-sible, but for making it quite workable.
“He’s been a great find for us,” she saysof the contracted radiologist. “We contacthim all day long, and he even calls theemergency department with critical results.He hasn’t been sick, he works holidays,and he has his laptop with him. He cangive us preliminary readings from that, andwhen he gets back to the PACS monitor, hewill dictate the final interpretation. Thatsatisfies the doctors on our medical staff.”
Despite the comparative simplicity ofthe KDH radiology department, Dendysays that she routinely pulls data from theRIS and creates her own custom reports to
Completing a customized reportusing RIS data-mining software(or some other system) is simplya matter of learning a little tech-
nology. For Stefanie Dendy, director of radi-ology at King’s Daughters Hospital in YazooCity, Miss, it can be as easy as changing thestart-date and end-date fields for the infor-mation that you want to correlate.
Dendy is talking about customizing tem-plates or automatic reports done by the RISby changing the dates to bracket a particu-lar segment of data. She can do the samething by changing fields for facilities ormodalities, which is mostly enough for herpurposes, she says. What she wants next isfor her hospital to activate a billing functionalready present in the RIS. This would lether study the financial bottom line for eachmodality, she says, but King’s Daughters,for now, is sticking with its old hospital-widebilling system. “We had an interface prob-lem because we use a hospital code insteadof a CPT® code,” Dendy says.
IS CUSTOM REPORTING DIFFICULT?At Rochester General Hospital, Rochester,
NY, Pamela Moseley, RIS/PACS director, saysthat she had to learn a reporting-softwareapplication, as well as the reporting featuresof her RIS, in order to create custom reports.Other than that, she says, it’s been a matterof perseverance.
“Cycle time per shiftand per modality—thattakes me a long time,”she says. “The clock is inmilitary time, and youhave to create two reportsand add them together”to cover a shift that theclock divides at midnight.
Sometimes, she adds, she will be asked forreports by modality by room, and she is asked todetermine “the number of exams ordered perhour, per month, and per shift, based on patienttype—emergency, inpatient, or outpatient.”
At Strategic Administrative andReimbursement Services in Grand Rapids,Mich, CFO Bill Ziemke and his team of finan-
cial analysts have been able to use theirdata warehouse and business-intelligencereporting software to provide useful infor-mation for making business decisions.
At Infinity Management in Nashville,Tenn, CEO J. Keith Radecic says that creatinga custom report is generally a point-and-click affair. “I choose the data, and I havemanual control over building that report,” hesays. “Today, a client wanted a report builtfor a specific payor and all claims outstand-ing for that payor for all of 2007: the charge,the amount paid, and the current balance. Iran that report and created it in about 35minutes. You have to run on the fly so thateverything is used in a timely fashion.”
Radecic says that the benefits ofreporting systems are undeniable. “Whynot invest in a better reporting tool?” heasks. “For medium-sized to larger groups,the benefits far outweigh the costs. Theexcuse that we can’t get to the data shouldnot be acceptable.”
—G. Wiley
Stefanie Dendy
2009ANNUAL MEETING
For program and registration information: www.siimweb.org/siim2009.
June 4–7, 2009Charlotte, North Carolina
Charlotte Convention Center
The Society for Imaging Informatics in Medicine
SIIM 2009 OFFERS9 LEARNING TRACKS: Basics of Imaging Informatics
Communicating Results
Image Acquisition & Management
Advanced Visualization
Enterprise Imaging
PACS Operations
Breast Imaging Informatics
Imaging Center PACS
Interoperability & Integration
NEW Features!The SIIM Annual Meeting
has been restructured and updated to provide the best
learning environment and instruction for imaging
informatics professionals (IIPs).
Diag Imag8.125x10.875.indd 1 1/20/09 1:29:19 PM

2009ANNUAL MEETING
For program and registration information: www.siimweb.org/siim2009.
June 4–7, 2009Charlotte, North Carolina
Charlotte Convention Center
The Society for Imaging Informatics in Medicine
SIIM 2009 OFFERS9 LEARNING TRACKS: Basics of Imaging Informatics
Communicating Results
Image Acquisition & Management
Advanced Visualization
Enterprise Imaging
PACS Operations
Breast Imaging Informatics
Imaging Center PACS
Interoperability & Integration
NEW Features!The SIIM Annual Meeting
has been restructured and updated to provide the best
learning environment and instruction for imaging
informatics professionals (IIPs).
Diag Imag8.125x10.875.indd 1 1/20/09 1:29:19 PM

32 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
DATA | Analytics
guide operational and strategic decisions.The RIS will track workflow averages andgenerates stalled-procedure reports.
“The workflow averages help me; theytell me where the breakdowns are,” Dendysays. Is the problem in registration or else-where in the exam cycle? Dendy says thatthe RIS reports answer that question andmore. She can look at RIS reports to seewhere exams are stalling and then respondto physicians who ask why a report is notshowing up in the patient’s chart. Is thedelay being caused by the radiologist, thetranscriptionist, or the clerk?
“The nurses blame radiology, and radi-ology blames the nurses,” Dendy says.“That’s another advantage of the RIS: If thereport is not in the chart, the clerk can calland print one. On the units, they haveaccess to the reports.” The RIS also allowsDendy to track and respond to modality-use patterns, on which she reports month-ly. After studying these trends, she canmake adjustments. She uses the example ofa bone-density scanner. “We got thatmachine at the request of medical staff, butall of a sudden, nobody was ordering thetest anymore,” she explains. In such cases,if use of a modality is unusually low forthree months, she can remind the medicalstaff that the hospital has this capability.“The doctors do go through cycles,” Dendysays. “Sometimes, all it takes is a reminder.”
Dendy has also used RIS data to trackthe referral sources of patients who don’tshow up for appointments. No-showscompromise patient flow by tying upschedules, she notes. Most of the KDH no-shows turned out to be coming from clin-ics with high volumes of indigent patients.KDH then worked with those clinics. “Wesaid, ‘Talk to your patients,’ and we actual-ly have cut no-shows,” Dendy says.
She also relies on RIS data in a waythat may be unusual: She creates the con-tract radiologist’s monthly invoice. Theinvoice lists patient names and the codefor each procedure that the radiologistinterpreted. “I break it down by modality,and by how many studies (and whattypes) he read most,” Dendy says. Whatshe is doing is creating the radiologist’sbill. She sends it to him, and then heapproves it. “It is backwards, but it’s blackand white,” she says.
Large-practice ModelsData mining, as a management tool, can
be even more useful when applied to alarge radiology practice. J. Keith Radecic isCEO of Infinity Management, LLC, themanagement arm of Radiology Alliance,PC, in Nashville, Tenn. Radiology Alliance,with 48 radiologists, is the largest privateradiology practice in Tennessee. Its clientsinclude three hospitals and more than halfa dozen outpatient imaging centers.
The RIS used by Alliance is interfacedwith the HIS and PACS at Alliance’s vari-ous clients, and an IT staff of four atInfinity makes sure that those interfacesare performing, Radecic says. For analyti-cal purposes, he relies primarily on a RISreporting tool that assembles the financialdata in conjunction with the imaging anddemographic data that flow to the RIS.
While customized reports get a lot ofattention because they can focus on specif-ic patterns or details, Radecic emphasizesthe importance of the template-basedreports that the RIS generates automatical-ly. He has more than 150 of them that hecan choose from monthly.
A particularly important templatereport, he says, is the aged trial balance.This report tracks accounts receivable,showing delinquent payments, where thereceivables are with each payor, and whatthe payment cycles have been. Radecicadds that studying receivables has allowedthe practice to lower its turnaround timefor receipts from payors from the 50-dayrange to the mid 40s. “Our goal is the high30s for 2009,” he says. He also notes thatthe receivables data, because they can betracked to the line-item level, have made iteasier to prove to insurance carriers thatsome payments should be given immedi-ate approval, rather than having to gothrough an appeals process.
Other template reports from the RISreveal specific modality patterns or CPT
codes in the aggregate, Radecic says.Among other things, these can be used toassess work RVUs and other efficiencies.“There are such powerful tools in today’smarket from the various vendors,” he adds.
Like others, Radecic tracks referralpatterns. “They go a long way in tellingus where our procedures come from,” hesays, but the gross figures for a referrerdon’t tell the whole story. He drills downto understand why the numbers showwhat they do. “Do all of a physician’sreferrals come from Medicaid? Is he orshe giving us all the low reimbursables?We’ll take any patient, but we need tomanage our practice. If all we get isMedicaid or self-pay, we’ll go to thatphysician and say, ‘We’re happy, but allyou’re giving us is self-pay. We want allyour business.’ We try to convince thatphysician that if we’re good for some ofhis or her business, we’re good for all ofit,” Radecic explains.
He adds that Infinity tracks referrals byZIP code to see whether new centersshould be opened or a joint venture with ahospital should be initiated. “These aredecision-driving models,” he says. InfinityManagement also works with its RIS ven-dor to turn regularly needed reports fromthe custom variety into those that the RISdoes automatically or nearly automatically.Radecic uses the example of a report thatcombines charge counts, charge dollars,work RVUs, and actual cash receipts.
“I used to have to run four reports,coordinate them with one giant spread-sheet based on the physicians’ work atmultiple locations, and then calculate theiraverage productivity per day. Now, I havea single reporting tool that gives me allthat I need to run that report. I can run, in25 to 30 minutes, a report that took daysbefore,” Radecic says.
There are, of course, some reports thatRadecic can get only by creating the data-analysis parameters himself. At present,he says, Infinity is trying to cut down onthe after-hours readings that its doctorsmust perform. While Alliance Radiologyuses a night-coverage service from 11 PMto 7 AM, the evening hours before 11 areunpopular with radiologists. “We knowthat on a typical day, we need 31 doctors tomanage the business, but of those, should

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 33
we schedule two or four in the eveningand 29 or 27 in the day?” Radecic asks.
He’s using RIS data to find the mostefficient evening staffing pattern that alsorequires the fewest radiologists. Thisreport, he says, will answer a quality-of-life question that will fit into largerstaffing puzzles when doctors want vary-ing workloads and schedules. Anotherarea that Radecic continually investigatesis the profitability of certain procedures,including radiofrequency ablation anduterine-artery embolization. “We knowthat uterine-artery embolization is a goodservice that generates revenue becausewe’ve run the numbers,” he says. “If youcan’t measure it, you can’t manage it.”
External ManagementNot every data-mining effort is based
directly on billing or RIS-driven data. AtAdvanced Radiology Services (ARS) inGrand Rapids, Mich, data from seven dif-ferent health systems are pulled from theRIS, HIS, and PACS at client facilities.From there, the data flow to servers at thepractice’s management service, StrategicAdministrative and ReimbursementServices (STARS), LLC, Grand Rapids,Mich, where they are analyzed usingbusiness-intelligence reporting software.
ARS is the outgrowth of several radiol-ogy practice mergers in the GrandRapids/Kalamazoo area. Representing115 radiologists, it is one of the largestradiology practices in the country. STARShandles billing and management for ARS.
Bill Ziemke, JD, LLM, MBA, CPA, isCFO at STARS. According to Ziemke,incoming medical reports are enteredinto coding software, where the reportsare coded either manually or using elec-tronic intelligence and entered into abilling system. All interventional radiolo-gy procedures are manually coded,whereas some of the diagnostic reports
are coded using electronic intelligence. Since the billing system itself has limit-
ed template-reporting capacity, STARSroutes the data from the billing system intoa data warehouse. “There is a nightlyextract of data fields from the billing sys-tem, which are transferred into a datawarehouse. The data warehouse can thenbe used for reporting purposes using busi-ness-intelligence reporting software,”Ziemke says.
Financial analysts further segment thedata, organizing subsets—for example,daily patient, location, physician, andbilling figures—into smaller, more man-ageable data cubes. Cubes, he says, allowdata to be analyzed more quickly than ifthey had to be pulled off the master file.“When the data warehouse is updated,the cubes are also updated,” he explains.
Ziemke says that almost all STARSreports are customized. They aredesigned, created, and updated by finan-cial analysts on staff. Currently, analystsare evaluating the costs of having radiolo-gists on-site after hours.
Among data-analysis successes,Ziemke lists stepped-up productivity inthe billing department. “We used cost-accounting principles to measure produc-tivity for each area,” he says. “By trackingproductivity, we were able to reducestaffing by 10%.” The study took morethan number crunching. “We had a costaccountant sit down with the staff doingthe work, watch them to measure whatthey were doing, and discuss outliers to
the standard measures with the staff per-forming the work,” Ziemke says. “Then,we set the productivity standard, which isconstantly being reviewed.”
The analysts are also searching for inno-vative ways to measure physician produc-tivity. Simply applying RVUs to radiologists’output is too imprecise, so ARS is lookingat numerous items. Other factors that needto be considered are the amount of admin-istrative responsibility a physician has;where the interpretation is being per-formed (home, hospital, or off-site loca-tion); the modality being interpreted; andthe degree of acute need for the studiesbeing interpreted. Another factor that ARSis measuring is the quality of the work.“Our doctors are committed to quality,”Ziemke says, noting that an electronic peer-review system has been implemented togive feedback on quality. “All of these fac-tors need to be considered when looking atand evaluating physician productivity.”
Drowning in DataThere are so many benefits of data
mining that it’s hard to notice the pitfalls,but they exist. In drilling down, there isalways the fear of suffocating on data.“You research yourself into a hole,”Radecic says.
For example, a practice can study thenumbers on a projected service expan-sion, he says, but until the move is actu-ally made, nobody can answer the mostimportant question: Are the physicians inthe new neighborhood going to give thepractice referrals? “Excess data make youwant to analyze down to the minute level,but you can stymie a business decisionbecause you get so minute you never act.You overanalyze yourself out of projects,”Radecic says.
George Wiley is a contributing writer forRadiology Business Journal.
We used cost-accounting principles tomeasure productivity for each area. By tracking productivity, we were able to reduce staffing by 10%.
Bill Ziemke, JD, LLM, MBA, CPA

RSNA 2008:RSNA 2008 | Exhibits Assessment
By Lisa Bielamowicz, MD
Despite reports that capital equip-ment budgets are frozen atsome hospitals, buyers were outin force at the 2008 meeting of
the RSNA in Chicago. Nonetheless, pro-fessional attendance did not reach lastyear’s level, and exhibit square footagepurchased and vendor attendance alsowere down, reportedly.
Clearly, the global economic crisis ishaving an impact, and both vendors andhealth care providers are feeling pressureon the capital side. Our financial analystsbelieve that from a capital-purchase stand-point, vendors will feel the greatest effectin the middle of 2009. For providers withtechnology decisions to make, it is moreimportant than ever to make every dollarcount, and we predict that there are stillsome great market opportunities.
Providers also need to maximize theequipment that they currently own; 64-slice (and beyond) CT is a great example.Scanners capable of doing cardiac imagingare located on every corner in most cities,but we have yet to see a market where oneprovider has risen to the top as the cardiacimaging provider of excellence. The tech-nology is there, but in almost all areas, thecardiac imaging program for which it waspurchased has not developed. The marketis wide open, with no new technologypurchase necessary.
One positive consequence of thesechanges is that hospitals, imaging centers,
and now vendors are placing a renewedfocus on efficiency. Surveying the offeringson the show floor makes the priorities ofevery vendor clear: increasing the efficien-cy of all departments across modalitiesand decreasing scheduling blocks toincrease revenue from one unit dramati-cally. With digital mammography, forinstance, halving the scanning block canmore than double revenue.
Top Five TrendsWe identified five top trends on the
show floor. First, focus on superpremiumtechnologies was diminished. We didn’tsee a big-splash technology, making thisone of the more sedate RSNAs in recenthistory. The other side of this is that we’veseen many vendors focusing on developingbudget lines: a 1.5T MRI scanner for lessthan $1 million and a workhorse 16-sliceCT scanner costing less than $500,000.The four major manufacturers have allintroduced budget CT and MRI units.
Second, the focus on women’s imagingcontinued. This is seen not only with dig-ital mammography and the excitementaround tomosynthesis, but in a huge arrayof offerings in the second-line imagingspace for treatment planning and diagno-sis. Subject to the economy, mammogra-phy volumes may decline, but vendorsperceive providers as likely to purchase.
Third, interest continues to grow inbreast tomosynthesis. We predict that it is
the one truly disruptive technology that willbe introduced in the next few years. Fourth,further advances in ultrasound generatedconsiderable excitement, as vendors con-tinue to add functionality. Increased atten-tion to radiation dose in 2008 has also refo-cused interest on ultrasound.
Fifth, we are starting to see the addi-tional development of niche offerings,with new market entrants such as special-ty, head-only PET/CT scanners and newdedicated breast MRI offerings. There isreal interest in developing market-specificplatforms for specific patient populations,although, as capital dollars become scarce,these niche scanners are increasingly diffi-cult to justify over a workhorse platform.
CTDuring the past 12 to 18 months, 64-
slice CT has become the technology ofchoice for hospitals interested in purchas-ing a workhorse CT scanner. While a 64-slice CT scanner is not required to per-form the vast majority of studies, priceshave fallen so precipitously that 64-sliceCT can now be purchased for less than $1million (without the cardiac package). It isa justifiable purchase today if there is apossibility that coronary-artery imagingwill ever be performed during the life ofthat scanner.
Is 64-slice CT good enough for coro-nary-artery imaging? Evidence demon-strates that 64-slice CT is the standard of
34 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
In assessing the imaging technologies on display at RSNA, an observer provides tools for making critical decisions regarding your capital budget for 2009
Mining the Landscape, Assessing the Exhibits

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 35
care for coronary CT angiography (CCTA)for most patients (see table), but one seri-ous concern is radiation dose. Dose-reduc-tion protocols exist, but if they are notused, 64-slice CCTA is associated with ahefty radiation dose. Dose-reduction pack-ages are very important for sites planningto offer CCTA in a programmatic way.
Nonetheless, 16-slice CT remains thestandard of care for nearly every examapart from CCTA—more than 90% ofdiagnostic CT exams performed today. In2007, it looked as though vendors hadcompletely abandoned 16-slice CT, andsome talked about discontinuing their16-slice CT scanners for the US market.In 2008, however, one major vendorbrought out a bare-bones (but good) 16-slice CT with a planned list price of$400,000. It is not necessary to have fivesuperpremium scanners in a hospital.
technology to the CFO, but most sitesdon’t end up doing the upgrade.
Acute stroke imaging is likely to be thenext place where superpremium CT isgoing to have a large clinical impact. Ourinstinct is that 64-slice CT is probably notgoing to be the prime technology. A bene-fit of a large single 256- or 320-detectorarray is that it allows capture of the entirebrain or heart in one rotation, offeringgreat perfusion images. This will allowrapid assessment of the extent of a strokeand, it is hoped, lead to expedited triage ofpatients to interventions. Combined withangiography, it creates the true optimalcardiac exam, visualizing the clot withCCTA and then seeing, downstream, theblood-flow data that would have comefrom nuclear medicine in the past.
In post–64-slice technology, theoptions available are staggering, with
During the past year, each vendor hassolidified its post–64-slice CT offerings,and all are in production today, with listprices holding steady around $2 million.Vendors are backtracking and filling inthe gaps; one introduced a reasonablysuccessful 256-slice scanner in 2007, butalso offered a 128-slice scanner (upgrad-able to 256 slices) at RSNA 2008.
The vendor that introduced dual-source CT rolled out a single-generator128-slice scanner available in 20-, 40-,64-, and 128-slice configurations. The20-slice unit can be upgraded to 128slices with as little as eight hours ofdowntime. While that is the best flexibil-ity we’ve ever seen, we haven’t seen theseupgrades really pay off; the option islargely an insurance policy, allowingaccess to premium technology asrequired. It may help sell the high-end
Category Laggards Late Majority Early Majority Early Adopters First Movers
Typical Rural hospitals Community hospitals Community hospitals Regional academic Top radiologyInstitutions in noncompetitive in average in competitive centers and community departments
markets markets markets hospitals in highly serving as testcompetitive markets sites for cutting-
edge multisliceCT technology
Slice Count Single 2 4 8 16 32 64 Next Generation
GeneralImaging
Trauma
3D Imaging
VirtualColonoscopy
Peripheral CTA
Coronary CTA
Next-generation CT technnologiesinclude 256-slice, 320-slice,
high-definition, and dual-source models
Substandard Standard of Care IdealKEY
Source: Technology Insights interviews and analysis, The Advisory Board Co.
CT Adoption and Application Profile, 2008

36 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
RSNA 2008 | Exhibits Assessment
each vendor offering a drastically differentscanner architecture. It is still difficult toassess which design offers the best long-term clinical bet.
CCTA and CT ColonoscopyThe slower-than-anticipated develop-
ment of CCTA has been frustrating.Clinical evidence has mounted that CCTAis a good way to evaluate symptomatic,low-risk chest-pain patients in an outpa-tient environment or emergency depart-ment. Evidence supports 64-slice CT inthis role, and operationally (and perhapseconomically), CCTA makes sense. Sincechest-pain patients account for 5% to 10%of emergency-department admissions,CCTA will be an operational boost—espe-cially for crowded emergency departmentsand telemetry units—by allowing properrouting of low-risk patients who are prob-ably not having myocardial infarctions.
Despite the promise, reimbursementand operational hurdles have been road-blocks for fully implementing CCTA pro-grams. Private payors would have fol-lowed CMS, had it moved forward with amore positive coverage decision, but CMShas given them reason to sit back as well.Getting the number of physicians (fromradiology, cardiology, or both) necessary toprovide the service around the clock isdaunting; no US emergency departmentappears, so far, to be able to offer 24/7CCTA on its own.
CCTA also was the catalyst for thebiggest imaging issue of the year: theresponse to radiation dose. If the 2007study1 estimating that 1.5% to 2% of allUS cancers could be due to medical radia-tion is to be believed, this is a significantproblem. There is a large risk for theyoung, and especially for females, from asingle CCTA exam, without a dose-reduc-tion strategy.
Media interest guarantees that patientswill ask whether they need the study andwhether the provider is doing somethingto make it safer. Providers need to be readyto answer those questions; must havetechnology in place, where appropriate, toreduce dose; and must ensure that front-line staff is prepared.
CT colonoscopy (CTC) has been slowto take off in recent years, but the publica-
tion of the ACRIN trial led many to believethat coverage was imminent. The ACRINstudy provided the first large data sample(5,000 patients) to show that virtualcolonoscopy stands up well as a screeningprocedure next to standard opticalcolonoscopy. Nonetheless, those hopeswere dashed when CMS declined to coverscreening CTC in its proposed nationalcoverage decision released in February.
A few caveats: First, this may be themost operator-dependent exam in imag-ing today, and physicians who are verywell trained are needed to replicate theACRIN results. Second, there is still somepatient misalignment here as to the need-ed prep and experience of a CTC exam,and distributing that knowledge is impor-tant. Third, providers should assess whatvirtual colonoscopy will do to scannercapacity. No volume onslaught is expect-ed, even if CMS coverage comes through,but as volumes start to mount, it willbecome troublesome that these examstake longer than standard diagnostic CT.Reimbursement is not going to make upfor losing the time to perform three or fourmore diagnostic scans for each CTC study.
For portable CT, resurgence is beingseen both in hospitals’ interest and in ven-dors’ consideration of offering technology.Our Technology Insights group has seenan upswing in hospitals looking forportable CT, whether for the operatingroom or, more commonly, for the ICU.There have been few offerings; a head-onlyportable CT unit has seen reasonable suc-
cess in the ICU environment, and installa-tions are increasing. A unit from the 1990scommands good money on the used mar-ket, and there is a CT suite available forthe operating room, but at more than $1million, its cost is comparable to that of anintraoperative MRI unit.
A potentially exciting development is awork in progress: a full-body portable unitthat could be the most versatile portableCT scanner available is anticipated within18 months.
3T MRIMRI is the modality hit most acutely by
the DRA, combining deep cuts in reim-bursement and volumes important to imag-ing centers and physician offices. Due tohigh costs and longer replacement cycles,MRI is also expected to be hardest hit byany upcoming capital crunch. Therefore,vendors are focusing on efficiency, work-flow, and increasing user friendliness.Continued upgrades in coil technologyacross vendors are allowing multiple scanswith fewer coil switch-outs. One vendornow offers a scanner with switch-out tables,so that the patient can be prepped outsidethe scanning suite and wheeled in while theother patient is being wheeled out, poten-tially increasing throughput.
Again, there is pressure on vendors todevelop lower-cost workhorse units.Several vendors showed a bare-bones 1.5Tunit priced at less than $1 million (a mile-stone). Another offered a reasonableupgrade package with which paying
Head/Brain Chest/Cardiac1%
Bone/Joint
Abdominal5%
Spine
Breast3%
Other1%
29%
25%
36%
Figure 1. 2007 MRI volumes by anatomic site. Source: GE Healthcare; SiemensHealthcare; and Technology Insights interviews and analysis, The Advisory Board Co.

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 37
slightly more for a 1.5T unit that is basi-cally a tuned-down 3T unit buys future3T capability with just two days of down-time, at a modest cost.
The pinch on MRI dollars has not soft-ened demand for 3T scanners. Vendorsare seeing a higher percentage of purchas-es involving 3T scanners. It took 10years, but it is finally prime time for 3T.Nonetheless, this is not a required pur-chase, as 1.5T remains the standard ofcare for all but the most advanced neu-roimaging. There is a clear benefit for allneurological imaging, but more and moreother areas (such as pediatric, abdominal,and prostate imaging) also show a clearclinical advantage for 3T over 1.5T.
Breast imaging, which currentlyaccounts for 3% of all MRI procedures(Figure 1, page 40), may be the next areawhere it is important to have 3T. Thismay not happens in the next year or two,but early studies3 are showing that 3TMRI has better specificity (the Achillesheel of breast MRI). Even in cardiac imag-ing, some data are being developed show-ing some benefits at 3T. More important,the floor has risen: the full portfolio ofexams can be done on 3T MRI, and it canbe a workhorse scanner in a stand-aloneenvironment, although issues in spineimaging are still being seen. Vendors areexpanding their options in 3T, increasingbore size, making a more patient-friendlyplatform; prices have also reached aplateau at slightly less than $2 million.
Looking hard at high-field open scan-ners that give 1.5T-quality images with amore open platform is also recommend-ed. Not only do these scanners provide amore comfortable patient experience, theyallow better access for procedures and forpediatric patients. A number of hospitalshave been able to reduce the number of
pediatric patients requiring sedation.Open units also have higher table weights,allowing improved access for obesepatients. Patients like the experience of anopen scanner, and the high-field openscanners give physicians the images theywant as well; they are one of the fewpatient-marketable purchases in MRI.
Media attention to nephrogenic sys-temic fibrosis and MRI contrast over thepast year has been significant. Althoughthe number of reported cases seems tohave diminished, there is a clear need toreduce the amount of contrast used, espe-cially for angiography, where three or fourtimes the recommended dose was com-monly used. Vendors are working todevelop noncontrast angiography.
Some niche MRI scanners also deserverecognition. For hospitals, it makes senseto own a scanner with the biggest bangfor the buck. Some breast centers canmake a case for dedicated breast MRI ifthey have enough volume, but data forother niche scanners like upright MRI arereally equivocal.
PET/CTPET/CT is the standard of care for
oncology imaging, particularly for stagingof a large majority of cancers; tumor imag-ing accounted for 93% of all PET/CT in2007 (Figure 2). The National OncologicPET Registry shared data early in 2008that showed a change in clinical manage-ment after PET imaging for 38% of cases.An Australian registry has replicated thoseresults. Other work showed that PET/CTdoes a much better job than thoracic CTof detecting lung lesions. The data arethere: you need access to PET/CT if youwant to have an oncology program.Despite the development of cardiac andneurological PET, oncology is going tocontinue to account for 90% or more ofall studies performed using PET/CT overthe next decade.
PET/CT, however, is an area wherereimbursement has been precarious. CMScontinued to chip away at coverage for2009. Reimbursement for oncology stud-ies went down by about $20 per scan.Cardiac PET coverage has seesawed likeno other exam has during the past fouryears, and it went down about another20% for 2009. Because it is necessary tocover the $30,000-plus monthly cost ofan on-site rubidium generator, myocardialPET remains an expensive business.
Development in PET/CT technologyhas been somewhat stagnant, with oneinteresting exception: a new entry thatpurports to decrease PET scanning timesignificantly. People have long discussed
The pinch on MRI dollars has not softened demand for 3T scanners.Vendors are seeing a higher percentageof purchases involving 3T scanners.
Tumor Imaging
Myocardial Imaging
BrainImaging2%
5%93%
Lisa Bielamowicz, MD
Figure 2. Oncology continues to dominate total PET/CT volume, 2007. Source: Technology Insights interviews and analysis.

38 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
RSNA 2008 | Exhibits Assessment
using the excess downtime on PET/CTunits to perform diagnostic CT scans, butoperationally, it’s not simple. This newplatform reportedly completes a whole-body oncology survey in five minutes. Ifthat is true, then it will actually be possibleto integrate PET and CT workflows. Thescanner is available in 40-, 64-, and 128-slice configurations, so a site with a verylow CT-slice capability could bring this inas PET/CT, but also as high-end CT withcardiac capabilities.
Hybrid SPECT/CT systems have laggedbehind PET/CT in development.Nonetheless, new SPECT and SPECT/CTsystems were on display, with greater focuson noncardiac applications. SPECT/CTmay be solidifying its role in the evaluationof some bone and infectious lesions, andother oncology-based applications aredeveloping as well, though this terrainmay be largely occupied by PET/CT overthe next decade.
SPECT/CT remains a nice-to-have, notmust-have, platform. What it needs is ahigh-volume exam where it makes a sub-stantial clinical impact over standardnuclear imaging, as PET/CT did for oncolo-gy imaging. SPECT/CT is still searching forthe study that makes it a necessity.
RSNA 2008 did not bring MRI/PET anycloser to commercial readiness. Althoughclinicians are able to fuse MRI and PETperformed separately, commercially avail-able clinical PET/MRI (still only discussedas a head-only unit) remains three to five
years away. Architectural issues associatedwith incorporating a PET ring into an MRImagnet historically have confoundeddevelopment. One vendor introduced aprototype scanner that is currently usedexclusively for investigational purposes.
Women’s ImagingNow considered the gold standard for
breast imaging, digital mammography maybe eclipsed by breast tomosynthesis in justa few years. Currently, digital mammogra-phy is at the forefront of replacement dis-cussions as institutions decide whether topursue replacement of analog systems withfull-field digital mammography (FFDM)scanners or to get lower-cost access to dig-ital exams with CR mammography tech-nology (Figure 3).
At RSNA 2008, vendors showcasedtheir flagship FFDM systems, includingnew platforms that will serve as the basisfor future breast tomosynthesis upgrades.Indeed, as institutions consider additionaldigital mammography units, more are con-sidering the market timing of future tech-nological developments, particularly breasttomosynthesis, which provides multipleslice-like views of the breast, allowing bet-ter visualization of many breast lesions.
The first commercially available prod-uct is expected to receive FDA approval inearly to mid-2009. An early clinical study4
indicates that tomosynthesis demonstratessuperior sensitivity, compared with con-ventional 2D mammography, and it is also
associated with a decreased recall rate.While vendors are promising that top-of-the-line FFDM units will be upgradablefor tomosynthesis, this upgrade will prob-ably still require a full-unit switch-out, orforklift upgrade.
CR mammography remains an attrac-tive alternative, allowing hospitals accessto digital technology for around half of thecost of a DR system. In April 2008, theFDA approved computer-assisted detec-tion for CR systems, resulting in a salesboost for the one approved system. Thisvendor hopes to capitalize on the successof its CR platform by developing a DRFFDM solution as well, which could resultin further price erosion.
Second-line breast imaging exams likebreast MRI and ultrasound have a well-established presence, and with recent com-petition from positron-emission mammog-raphy (PEM) and breast-specific gammaimaging (BSGI), the field promises tobecome even more diverse. PEM uses con-trast enhancement with radioactive FDG toassist in the detection of lesions of less than1 cm in diameter, and is especially effectivein the detection of ductal carcinoma in situand atypical ductal hyperplasia.
BSGI is capable of detecting early-stagetumors and offers differentiation of can-cerous versus benign tumors. Two vendorsof PEM and BSGI displayed mobile ver-sions of their technologies. The majorPEM vendor recently received 510(k)clearance for PET-guided biopsy on the
FFDM: 27%
Non-FFDM: 73%
FFDM: 44%
Non-FFDM: 56%
As of November 1, 2007 As of November 1, 2008
3,644
9,946
5,913
7,447
62% increaseversus 2007
Figure 3. Accredited mammography units in the United States. Source: FDA

www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 39
PEM platform, adding further versatilityto the modality and eliminating a key dis-advantage of the unit.
Automated breast ultrasound (ABUS)is not yet gaining momentum. Unlikeconventional handheld ultrasound, ABUSstandardizes image acquisition and limitsvariability among operators. Such auto-mated protocols consistently acquire aspecific set of 3D volumetric representa-tion, minimizing user error and maintain-ing quality standards across time andpatients. While early results indicate per-formance equivalent to that of handheldultrasound, further research will berequired to demonstrate (potentially)superior performance. The leading ven-dor of ABUS has had market exclusivity todate, but one major multimodality vendorintroduced a system at RSNA 2008,though its FDA clearance is still pending.
UltrasoundUltrasound introductions added to
rejuvenation of this modality, although itis necessary to spend $600,000 to obtainall of the features that enable the modali-ty to compete more effectively with CTand MRI.
Vendors continued to update 3D and4D models at RSNA 2008; 3D ultrasoundand volumetric imaging offer completeassessment of morphology by stacking 2Dcross-sections of the volume of interest.Currently, 3D ultrasound is best suited forobstetric and echocardiography studies,but increasing demand to view anatomicalstructures clearly, with more measure-ment parameters, is driving a continualshift away from 2D ultrasound toward 3Dand volumetric imaging for other applica-tions. Postprocessing software enhance-ments are allowing more detailed tissuecharacterization while simultaneouslyreducing operator dependence.
DRDigital imaging remains the primary
focus for vendors of radiography andradiography/fluoroscopy systems, andportability is also becoming an area ofinterest. Several vendors are developingnew portable plates that are lightweightand durable enough to sustain routinedaily use in high-volume settings.
Moreover, vendors are introducing morecomprehensive and versatile DR roomsolutions that combine multiple radi-ographic modalities.
DR vendors also are focusing onimproving workflow and reducing thesteps that technologists need to take toacquire images and position patients.Auto-alignment, auto-image stitching, andtracking software are now becoming rou-tine, as are user-friendly interfaces that aredesigned to enable hospitals with oldersystems to improve workflow by replacingone or two rooms with one new system.
Two technologies on display this year,DR tomosynthesis and lung computer-aided detection, show promise in theirability potentially to improve the detec-tion of lung cancer and lower the cost ofdetection. Tomosynthesis acquires 3Dimages using DR technology, and recentwork suggests that tomosynthesis is farsuperior to DR alone and significantly lesscostly than multislice CT for the detec-tion of pulmonary nodules. In addition,computer-aided detection with CT hasthe ability to detect nodules and reducereader variation (a problem area in CTdetection of lesions), even in a low-dosesetting. These developments could have apotentially large impact on the way thatpulmonary nodules are detected and onradiation dose, as well as reducing thecost of lung-cancer detection.
Outlook for 2009While molecular imaging is expected to
play a significant future role, its near-termclinical adoption is not expected withinthe decade. That said, future applicationsinclude improved lesion detection and theability to deliver targeted therapeutics.
First, for 2009, expect continued priceerosion across modalities. As next-gener-ation products come to market and asbroader economic issues continue to con-strain capital budgets, acquisition priceswill continue to erode. Second, breasttomosynthesis will become a commercialreality. With the ability to improve uponconventional mammography, tomosyn-thesis could prove to be a disruptive tech-nology, and centers intending to acquiredigital mammography platforms shouldconsider their path to tomosynthesis as
they make this purchaseThird, look for the continued refine-
ment—and growing adoption—ofadvanced CCTA applications. As clinicaldata continue to solidify the role of theexam, more institutions are expected todeploy CCTA in the emergency depart-ment, despite the low likelihood of broad-er Medicare coverage this year. Fourth, 3TMRI will further approach workhorse sta-tus through increased versatility, althoughthe attractive prices for 1.5T scannersmake it a hard sell this year.
Fifth, moving forward, increasing effi-ciency and getting more patients througheach scanner will be paramount. MRI willrepresent one of the primary targets ofthese efforts, bolstered by increasedautomation in each vendor’s MRI plat-form. Sixth, look for portable CT offer-ings—now catering to specific applica-tions such as neuroimaging—to increasethe versatility of their platforms withwhole-body units.
Lisa Bielamowicz, MD, is the nationalimaging practice leader, The Advisory BoardCo, Washington, DC. For more informationabout the company’s Imaging PerformancePartnership program and technology assess-ment services for member hospitals, contacther at [email protected].
References1. Brenner DJ, Hall EJ. Computed tomog-raphy—an increasing source of radiationexposure. N Engl J Med. 2007;357:2277-2284.2. Johnson CD, Chen MH, Toledano AY,et al. Accuracy of CT colonography fordetection of large adenomas and cancers.N Engl J Med. 2008;359:1207-1217.3. Bogner W, Pinker K, Gruber S, et al.High-field diffusion-weighted imaging forimproved differentiation of benign andmalignant breast lesions. Paper presentedat: 94th Scientific Assembly and AnnualMeeting of the Radiological Society of NorthAmerica; December 4, 2008; Chicago.4. Kopans DB, Moore RH, Gavenonis SC.Calcification in breast tomosynthesis.Paper presented at: 94th ScientificAssembly and Annual Meeting of theRadiological Society of North America;December 2, 2008; Chicago.

Day forNight,East forWest
TELERADIOLOGY | Crossing Boundaries
How did a 2000 lecture tour inChina spawn a teleradiologyrevolution? For William G.Bradley, MD, PhD, FACR, the
idea for an international business evolvedfrom a reading that he did nine years agoin the Far East. Thanks to PACS and theWeb, Bradley, who is now chair of theradiology department at the University ofCalifornia, San Diego (UCSD) MedicalCenter, interpreted an MRI of the brain inChina and then called the neurosurgeon inthe United States.
“It was the middle of the night back inLong Beach, Calif, and the middle of theafternoon in China,” Bradley recalls. “Atthat point, it occurred to me that with PACSand the Internet, you don’t have to be up atnight anymore—which is the worst thingabout being a radiologist.” That, he adds,was the genesis of the first after-hours tel-eradiology coverage provider.
After returning from Asia, Bradleymentioned the idea to friend and col-league Paul Berger, MD. With PACS,increased Internet bandwidth, and losslessimages fueling the digital transformation,
When taking on a new hospital client,many radiology groups, such as RadiologyConsultants of Iowa (RCI) in CedarRapids, keep a close eye on the windshieldfactor, preferring to contract only withhospitals no farther away than a two-hourdrive. Kathryn Epley, RCI’s chief adminis-trative officer, presides over the 27-radiol-ogist RCI group and takes pride in thecompany’s ability to offer both distancereadings and on-site services with a per-sonal touch.
With the continuing rise of subspecial-ization, high-end MRI, and interventionalprocedures, Epley points out, it is toughfor small, rural hospitals to retain enoughradiologists with all the necessary creden-tials and skills. The highly dispersed pop-ulation centers of Iowa mean that RCI pri-marily deals with critical-access hospitals(of 25 or fewer beds) outside its urbanhome base.
When Epley arrived four years ago,most of those hospitals still had film-basedradiology services, and turnaround forroutine studies could take days. To makematters worse, radiologists had to spend
40 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
Teleradiology permeatesthe specialty as practices
cross state, regional, andglobal boundaries to
purchase and practice radiology
By Greg Thompson
the idea took hold. Berger nurtured theconcept, eventually starting a companywith a name that became generic in theindustry and synonymous with nocturnalradiology.
“What we started was simple,” Bradleysays. “You moved to Sydney. You moved toZurich—and you worked during the day.”At present, he reports, 26% of US hospi-tals are covered by the original company,and 55% of hospitals are covered by oneof its 40 competitors.
Over time, and through the adoption ofPACS, many traditional radiology practiceshave embraced teleradiology, not just ascustomers, but as providers of daytimecoverage for contracted hospitals and long-distance and after-hours coverage for ruralhospitals and small radiology practices.
Today, for example, UCSD is not only aclient of the original after-hours coverageprovider, but is also a purveyor of subspe-cialty teleradiology services. Each day,UCSD radiologists perform 50 to morethan 100 teleradiology interpretations;Bradley expects this service line to gener-ate revenues of $1.5 million in 2009.


42 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
TELERADIOLOGY | Crossing Boundaries
time traveling to those hospitals to pro-vide on-site coverage, even for studiesthat could have been interpreted viaPACS (if it had been available).
With the help of an IT committee offour radiologists and a new CIO, JoeMoore, RCI selected a PACS in 2005 andbegan visiting outreach hospitals. “Themost precious resource we have is thedoctors’ time,” Epley says. “For them tobe driving to outreach sites is a poor useof their time if they can do that samework in a remote reading room.”
Realizing the dream of providing net-worked, real-time radiology service for allof the contracted outreach hospitals wasnot easy, but Epley and her staff madesteady progress. “Our vision required thatthose hospitals develop a stronger rela-tionship with us, in terms of trusting usto purchase their PACS through us,which was a real leap of faith,” Epley says.“Since that time in 2005, every one of our10 outreach hospitals has come ontowhat we call RCI Net. We provide a com-pletely turnkey digital system becausemost of these hospitals don’t have the ITinfrastructure necessary for PACS. Wealso provide 24/7 reading within ourgroup because we have radiologistsworking all three shifts.”
With those pieces in place, multisliceCT, MRI, digital mammography, andmore all became portable. From signedcontract to go-live date typically takesabout 90 days for RCI, in a feat that it hasbeen able to duplicate many times. Whensmall hospitals did not have the RIS inplace to place electronic orders properly,the RCI IT committee worked with a pro-grammer to write a mini RIS that fits thebill. Using voice-recognition software(with the vast majority of reports editedby the radiologists), turnaround time has
radiologist sitting somewhere.” In a change of attitude that is further
opening the door to remote practice,Racanelli says that he increasingly is see-ing a willingness on the part of cliniciansto talk with radiologists by telephone.“We’re at the point where the referringclinicians who used to walk in the doorand go over cases are getting comfortablewith calling and going over the cases,”Racanelli explains. “I get phone calls allthe time asking me to look at a case. Thecaller is in one place and I’m in another—and it really doesn’t matter where we are,because we can both bring up the case atthe same time. That used to be the bigthing: somebody had to sit there whenthe doctors came by, but now, that’s not somuch the case.”
Regulatory BarriersOne other limitation on expansion is
state licensing. The good news is thatgaining another license is usually just amatter of turning in the paperwork, pay-ing the fee, and waiting the required sixto nine months. Beyond marketing serv-ices to other areas, gaining the first out-of-state teleradiology client is often a mat-ter of mining old contacts. “The way itworks is that you may have a friend fromresidency in Texas who says that he hassome extra work,” Racanelli says. “Eventhough you may be far away, he may askif you want to do it, rather than havingthe hospital two counties away do theextra work.”
At RCI, tailoring services to fit each sit-uation is largely a function of geographyand mission. In keeping with its stricttwo-hour–drive policy, RCI provides amedical director for every hospital’s radi-ology department, and that directorattends all the medical staff’s meetings.“There is a lot of teleradiology out there,but those people are distant, and theyrarely come on site,” Epley says. “Thelocal physicians don’t know them, andthat makes a difference. Our physiciansattend the meetings, and they are therewith the local referring doctors to answerquestions. If we start expanding outsideof more than about a two-hour–driveradius, we are going to lose the ability todo that.”
been dramatically reduced—to minutes,in most cases.
So far, Epley has no plans to expandoutside Iowa. While she has not specifi-cally avoided crossing the border, shesays that there is still plenty to be donewithin the state.
Joseph Racanelli, MD, is president ofRadiologic Associates, New Windsor, NY,a 16-radiologist group that covers fourhospitals and four imaging centers in NewYork. Like UCSD, Racanelli’s group usesteleradiology to fill its own gaps while alsoproviding teleradiology services for oth-ers. For example, Racanelli contracts witha New York-based after-hours service tohandle his group’s overnight readings. “Inthe beginning, we had to use more radiol-ogists than we needed because we did notuse teleradiology,” he says. “That was thebig problem in staffing. Some placeswould be dead quiet and others were get-ting killed, and having radiologists drivingaround is not economical.”
Radiologic Associates currently offersteleradiology services in the surroundingcounty up to 35 miles away, under a limi-tation that is largely in place due to hospi-tal desires. “Most every hospital wants abody on the ground,” Racanelli says. “Theylike to have somebody sitting there for facetime to work with the technologists, butinstead of having two or three radiologiststhere, we send one. The overflow is han-dled via PACS and teleradiology.”
If Racanelli found a potential clientthat did not require the on-site presenceof a radiologist, offering teleradiologyservices in other states would definitelybe a realistic option for the practice. “Itwould not surprise me if we ended upjumping state lines,” Racanelli says.“More of our business will be handledover the computer, rather than having a
The mostpreciousresource wehave is thedoctors’time.
Kathryn Epley
Mostevery hospitalwants abody on theground.
Joseph Racanelli, MD


44 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
TELERADIOLOGY | Crossing Boundaries
Epley foresees a day when RCI couldpartner with other radiology groups, pro-viding them with the technology that herteam has developed and starting a joint ven-ture. She is quick to point out, however, thatany such move would have to be nonpreda-tory. “We don’t want to go into hospitals to
boot out the radiologists who are there,” sheexplains. “That’s not our design. We couldprovide some top-quality service that theymay not be able to provide because we have27 doctors, the technology, and the culturethat makes it all work well.”
Pushing the BoundariesWhile US-trained physicians residing
abroad currently perform readings for casesoriginating in the United States at night, itis still uncommon for US radiologists tointerpret exams that originate outside thecountry. The barrier is mostly reimburse-ment. Bradley explains that while Europeanradiologists complete training similar tothat of US radiologists, they only garnerabout half of what US doctors would bepaid for a typical night reading.
Indian physicians get approximately 10%of what US radiologists earn. “It does notreally pencil out for us to read for anyoneother than the US practices, because theyjust don’t pay enough,” Bradley says. “Otherradiologists around the world are not paid asmuch as US radiologists, so there is noincentive for us to read at night for them.”
Subspecialty daytime teleradiology isanother matter. According to Bradley,world-renowned UCSD musculoskeletalradiologist Donald Resnick, MD, getsenough per case from Portugal to make itworthwhile. “I have been doing MRI telera-diology since 1984,” Bradley says. “Initially,it was all MRI. After I moved to UCSD,where everything is subspecialized, I limit-ed my teleradiology to neuroradiology.”
Bradley points out that another reason
that radiologists trained abroad do notread for US providers is that they do nottake the US boards, leaving doubt thatthey are trained to the same standards.Some countries try to get around suchprohibitions through the practice of ghostreading, Bradley says.
He explains, “There is a risk, usuallyaddressed to India, that you will have oneUS-trained radiologist surrounding him-self with 10 Indian-trained radiologists,cranking through cases at hundreds anhour” that are actually being read by radi-ologists without US training or board cer-tification; the cases are then signed by theUS-trained radiologist. “The Indian-trained radiologists could be in the UnitedStates or in India. That’s called ghost read-ing, which is illegal. It’s a possibility, andthat is one of the inherent risks of teleradi-ology,” Bradley says.
Bradley believes that a dozen US telera-diology entities have sent radiologists tothe United Kingdom, France, India, Israel,and Australia. Because final readings forMedicare cases cannot be performed out-side the United States, coverage providersoutside the country provide so-called wetreadings in the middle of the night, and alocal radiologist does the final interpreta-tions the following morning.
“There is an inherent double reading ofevery case, which is an opportunity forquality assurance,” Bradley says. “The nextmorning, the local doctors are rested. They
have all the films, including films not sentin the middle of the night (because we’reonly concerned with emergency findings).We compare the night reading to the finalreading. At UCSD, we have been doing thissince we started with night-coverage serv-ice. If there is a discrepancy, half the time,the coverage provider is right, and half thetime, we are right.”
Most radiology groups that use after-hours services have fewer than 10 radiolo-gists, and therefore are not subspecialized.“If they are going to see one pulmonaryembolism a month, they might miss it,”Bradley says. “Ideally, the local radiologistwould read the case without seeing thewet reading and would then compare hisor her reading to the night interpretation.In fact, the local radiologists often knowwhat night service said, so it is not a truecomparison of reading capability, but itcould be set up that way.”
Thanks to several different coverageservices throughout the country, the idea ofnighttime subspecialty teleradiology cover-age has spread rapidly. In Bradley’s opin-ion, the after-hours market is just aboutsaturated, but there is still opportunity tobe found in daytime subspecialty readings.The advantage of daytime readings, hesays, is that they can be based in the UnitedStates and, therefore, can be final readings.
Bradley describes daytime readings asthe focus of the new push. He says,“Nighttime is pretty much saturated.There are too many companies competingfor the business, and the price is dropping,but if you can get a good subspecialistradiologist to read, you can save yourself.Let’s say that a group needs half of a boneradiologist. Rather than hiring someonelike that, who would rather be doing100% bone radiology, it can hire a subspe-cialty-coverage company.”
Bradley continues, “It will then do thesubspecialty readings with fellowship-trained radiologists. I also see this, really,as an opportunity for academic radiolo-gists to get more business—and we canuse teleradiology to help train our fellows.We can use it to supplement the cases thatour fellows see, so it is a win–win allaround.”
Greg Thompson is a contributing writerfor Radiology Business Journal.
Let’s say a group needs half a boneradiologist. Rather than hiring someonelike that who would rather be doing100% bone radiology, it can hire a subspecialty-coverage company.
William J. Bradley, MD, PhD, FACR
www.franklin-seidelmann.com866-4FSRADS
Experience in Millions of Subspecialty Interpretations• Neuroradiology• Musculoskeletal (MSK)• Body• Cardiac CTA• Oncological• Breast MR• Pediatric• Advanced Training in MRI, MDCT
and PET/CT
Clients everywhere trust Franklin & Seidelmann SubspecialtyRadiology (F&S) for high quality, clinically specific reports and proactive consultative services.
F&S, the largest final report teleradiology provider, gives youaccess to a large, experienced team of radiologists that includesnationally recognized subspecialty experts and academic leaders. Our unique blend of high quality reports, collaborativeconsultations with physicians and fast turnaround enables ourclients to improve referring clinician satisfaction, increase
referrals and revenues and optimize staffing costs.
Rely on Franklin & Seidelmann to be your single teleradiology resource for subspecialty, general, daytime, nighttime/ED and overflow coverage.
Visit www.franklin-seidelmann.com to view our report samples and radiologists’ biographies.
Full-Service Teleradiology
The Largest SubspecialtyTeleradiology Network
Visit us online for our “Final Reports for Radiology Groups” white paper – www.fs-rad.com/radgroups
Final, Preliminary, and SubspecialtyReports – Day or Night
RBJ:RBJ 9/8/08 7:30 AM Page 1

www.franklin-seidelmann.com866-4FSRADS
Experience in Millions of Subspecialty Interpretations• Neuroradiology• Musculoskeletal (MSK)• Body• Cardiac CTA• Oncological• Breast MR• Pediatric• Advanced Training in MRI, MDCT
and PET/CT
Clients everywhere trust Franklin & Seidelmann SubspecialtyRadiology (F&S) for high quality, clinically specific reports and proactive consultative services.
F&S, the largest final report teleradiology provider, gives youaccess to a large, experienced team of radiologists that includesnationally recognized subspecialty experts and academic leaders. Our unique blend of high quality reports, collaborativeconsultations with physicians and fast turnaround enables ourclients to improve referring clinician satisfaction, increase
referrals and revenues and optimize staffing costs.
Rely on Franklin & Seidelmann to be your single teleradiology resource for subspecialty, general, daytime, nighttime/ED and overflow coverage.
Visit www.franklin-seidelmann.com to view our report samples and radiologists’ biographies.
Full-Service Teleradiology
The Largest SubspecialtyTeleradiology Network
Visit us online for our “Final Reports for Radiology Groups” white paper – www.fs-rad.com/radgroups
Final, Preliminary, and SubspecialtyReports – Day or Night
RBJ:RBJ 9/8/08 7:30 AM Page 1

{MA RKE Tplace}
Women’s Imaging Ultrasound SystemRoyal Philips Electronics, Andover, Mass, has launched anew ultrasound system designed to deliver high-qualityimaging for a full range of women’s health needs, includ-ing obstetrics, gynecology, and breast imaging. The HD9system’s features include iSlice (which enables cliniciansto focus on specific areas of interest within a volume);spatiotemporal image correlation, for the evaluation offetal heart anatomy and function; tissue-specific imagingtechnology (which permits the system to be optimized fora specific patient or exam type); and tissue aberrationcorrection (which compensates for noise in difficult-to-image patients).www.philips.com/HD9
Handheld Finger-prickCreatinine TestStatSensorTM from ACIST Medical Systems, Eden Prairie, Minn, a Bracco Groupcompany, Princeton, NJ, is a point-of-care, handheld device that analyzes a finger-prick sample of blood for creatinine level (an important indicator of a patient’srenal function). Evaluating a patient’s kidney function can help determine his orher ability to receive IV contrast safely prior to CT and MRI exams. This is animportant precaution, especially for patients with risk factors such as diabetes,known kidney impairment, or advanced age.www.acist.com/radiology/stat.asp
Web-based ImagingWorkflow ResourceElsevier, Amsterdam, Netherlands, has releasedMosby’s Imaging Suite, a fully integrated, Web-based solution for the imaging department orcenter, designed to enhance quality and produc-tivity. The tool brings together reference, educa-tion, and communications capability in one plat-form for radiologic technologists, managers, andadministrators. An online, searchable edition ofMerrill’s Atlas of Radiographic Positioning andProcedures is at the core of the suite, which givestechnologists access to 70 hours of category-ACE credits, checklists to build competence, and aplatform that allows enhanced communicationsbetween department management and staff.www.mosbysimagingsuite.com
46 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com

{MA RKE Tplace}
www.radbizjournal.com | February/March 2009 | RADIOLOGY BUSINESS JOURNAL 47
Expanded Imaging Informatics ServicesFUJIFILM Medical Systems USA, Stamford, Conn, hasexpanded its Synapse Managed Services offerings toinclude RIS hosting and tele-RIS capabilities. The compa-ny’s Managed Services arm was originally designed to pro-vide Synapse customers with turnkey, high-reliability solu-tions that include software, system management, PACShosting, and other disaster-recovery services. Through thecompany’s expanded partnership with Evolved DigitalSolutions, Brentwood, Tenn, and through the use of virtual-ization technology, the program now includes RIS hostingand tele-RIS functionality, enabling radiology groups thatread for multiple facilities to read from a single worklist.www.fujimed.com
FDA-approved Brain-perfusion ApplicationZiosoft, Redwood City, Calif, has received FDA510(k) clearance for a brain-perfusion applica-tion available using its thin-client system,Ziostation®. The brain-perfusion application isa powerful analysis tool that provides brain-perfusion functionality as a thin-client applica-tion using standard commercial hardware. Thesoftware option aids in stroke assessment byproviding a color map of cerebral blood flowand other perfusion-related parameters fromCT of the brain.www.ziosoftinc.com
Low-dose, Rapid CT ScannerSiemens Healthcare, Malvern, Pa, has introduced theSOMATOM Definition Flash, a swift new dual-source CTscanner with a scan speed of 43 cm per second and a tem-poral resolution of 75 milliseconds, allowing a completescan of the chest region in 0.6 seconds. The scanner’sspeed also permits a dramatically reduced radiation dose;a spiral heart scan can be performed at a dose of less than1 mSv. Due to the high scanning speed, it is now possibleto acquire scans of the thorax, heart, or both in a fractionof a second, eliminating the need for patients to hold theirbreaths during the scan.www.siemens.com/healthcare

{MA RKE Tplace}
48 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
Affiliated Professional Services(800) 841-5200www.affilprof.net ....................................11
American College of Radiology(703) 648-8936www.acr.org ..........................................27
AMICAS(800) 490-8465www.amicas.com ......................................3
Codonics(800) 444-1198www.codonics.com ..................................17
Compressus(202) 742-4297www.compressus.com ..............................19
Franklin & Seidelmann(866) 437-7237www.franklin-seidelmann.com ..................45
FUJIFILM Medical Systems(800) 431-1850www.fujimed.com ....................................5
GE Healthcare(800) 886-0815www.gehealthcare.com ............................52
Hitachi Medical Systems America(800) 800-3106www.hitachimed.com ................................2
Imaging Center Institute(714) 832-6400www.imagingcenterinstitute.com ..............49
Imaging On Call(888) 647-5979www.imagingoncall.net............................41
Medical Imaging Specialists(800) 510-0680www.medicalimagingspecialists.com............9
NightHawk Radiology Services(866) 400-4295www.nighthawkrad.net ............................51
Philips Healthcarewww.philips.com/healthcare ......................7
SIIM(703) 723-0432www.siimweb.org ....................................31
Telerays(866) 972-9362www.telerays.com ..................................43
Visage Imaging(888) 338-4724www.visageimaging.com ..........................13
{ADVE RT I S E R Index}1.5T Magnet With Powerful Gradients
GE Healthcare, Waukesha, Wis, received FDA clear-ance for its new 1.5T MRI scanner, the DiscoveryTM
MR450. Built on the company’s short-bore supercon-ducting 1.5T magnet, the new platform features anewly designed digital receiver that extends thedynamic range by four times (compared with the com-pany’s previous 1.5T systems), as well as onboardoptical data architecture that boosts the signal-to-
noise ratio by 27%. The system also features a new parallel imaging technique that uses afull 3D data kernel for more accurate reconstruction, in addition to several new, advancedapplications: SWAN (T2 star-weighted angiography) and a new suite for non–contrast-enhanced MR angiography, Inhance.www.gehealthcare.com
Women’s UltrasoundImaging Applications andTransducerToshiba America Medical Systems, Tustin, Calif, demon-strated a new proprietary ultrasound technique at RSNAcalled MicroPureTM, which helps physicians detect breastlesions and microcalcifications more easily. The companyalso showcased its new 18-MHz, high-resolution DynamicMicro Slice transducer for imaging superficial structuresand identifying lesions; its spatiotemporal image correla-tion gating technique for fetal heart assessment; andElastoQ, a work in progress that evaluates tumors basedon their stiffness or elasticity.www.medical.toshiba.com
Web-based Advanced Visualization ApplicationsVital Images, Inc, Minneapolis, hasreleased Vitrea® Web, a new solution thatprovides distributed access to all of Vital’sadvanced clinical applications via Web andis available exclusively to ViTAL Enterprisecustomers. Advanced applications, includ-ing tools for measuring coronary plaque,probing a lung nodule, and evaluatingbrain perfusion on CT, are all accessiblethrough the new release. Vitrea Web sup-ports integration with PACS and the elec-tronic medical record through a standardURL interface and is optimized for low-bandwidth connectionsso that it will perform well when accessed remotely from home.www.vitalimages.com

the radiologistRichard A. Jensen, MD
Wwhy i read radiology business journal
you too can receive radiology business journalsubscribe online today at www.radbizjournal.com
I R
“I think a publication like Radiology Business Journal is long overdue—and timely. It brings a new level of analysis of the economic issues andmarket forces facing our profession, together with a depth of coverageof important events, both of which were often lacking in the past.
“In my opinion, it’s now the single best resource for the business ofradiology, and if anyone wants to get up to speed on the problems andopportunities facing us, I can think of no better place to start than theRadiology Business Journal.”
• Immediate Past President and Partner since 1998, Radiology Associates of TarrantCounty, a 57-person practice in Fort Worth, Texas
• BS Chemistry, Baylor University, Waco, Texas,Magna Cum Laude, 1984
• MD, University of Texas SouthwesternMedical School, Dallas, 1992
• Radiology Residency, Parkland Hospital,Dallas, 1993
• MRI Fellowship, Baylor University Medical Center
• Affiliations: ACR, Texas Medical Association,Tarrant County Medical Association, Society of Magnetic Resonance Imaging
• Honors: Phi Beta Kappa, National Merit Scholar
• Personal Fact: Father of four daughters, two in college, one in high school, and one in middle school

50 RADIOLOGY BUSINESS JOURNAL | February/March 2009 | www.radbizjournal.com
FinalREAD
Irecently facilitated an all-day retreat forthe management staff of a large hospitaloutpatient division that is part of a well-respected academic medical center. As I
have done on many similar occasions, Iasked the group’s members, prior to themeeting, to outline their respective issuesand concerns so that we might spend the dayworking toward alignment around a commonvision for future success. It is always a reveal-ing process.
One thing that became very clear early inthe group discussion, in this particular case,was the need to work through the fact thatmost large integrated health care systems(this one included) have evolved along func-tional lines in the delivery of care. That is,each department within the typical organiza-tion becomes its own functional silo.
Critical to the alignment of these silos isthe building of cross-functional teamworkaround a common purpose. It’s often easiersaid than done, and that’s why many organ-izations opt to have someone help themidentify methods of communication thatcan transcend parochial interests, lest theybecome codified into protected turf andisolated cultures.
Building a common culture based onmutual understanding of the vision and mis-sion is one area in today’s medical imagingpractices, departments, and centers where Ibelieve that I can help the enterprise competemore effectively in an unforgiving market. The
creation of a corporate culture based onaccountability, mutual respect, accessibility,service, trust, and communication is perhapsthe most significant accomplishment forwhich any leader can strive. This is especiallytrue in today’s medical imaging profession.
As we worked through the discussion atthe retreat, I was fascinated, as I always am,at the assembled group’s ability to grasp theurgent need to find new ways of developing asense of community and teamwork. In these
types of settings, the best and the brightestreach out to other departments and seg-ments of the organization as a means of con-necting and rising above traditional roles andpreconceptions.
The technical staff often feels isolatedand disconnected from the business officeand administrative staff. The radiologists typ-ically don’t connect with the line staff to helpthem understand the necessity of the clinicalprotocols that they develop. Marketers areoften at odds with the operations staff andfeel that hard-earned referrals are taken forgranted and service issues are not taken seri-ously. Likewise, the operations staff fre-quently thinks that marketers are constantlymaking them look bad by bringing bad newsfrom the referring physicians’ offices.
Linking these functional departmentsthrough leadership is not easy, but I believethat it will be among the most important ele-ments of a manager’s job description in thefuture. Whether that manager is running a
private-practice radiology group, a hospitalradiology department, an imaging center, ora group of centers, the challenges will be sim-ilar in each setting.
The ability to bring this disparate (andoften suspicious) group of department headstogether frequently—teaching them to com-municate more effectively and helping themfocus on the battles that need to be foughtoutside the organization (with competitors,regulators, payors, and others)—is the betterpart of leadership that will separate tomor-row’s winning imaging organizations fromthose that will continue to struggle, or willeven disappear.
I remain encouraged by the talent, com-mitment, and level of understanding amongthe majority of our profession’s front-linemanagers and leaders. Ours is a professionunder siege: a part of the health care deliverysystem that is fast becoming the bad guy inthe eyes and minds of legislators and regula-tors. The competitive landscape is brutal, andthe demands for accountability and efficacyare unrelenting. It is not a profession for thefaint of heart. Nevertheless, I see pockets ofexcellence and examples of leadership thatare redefining medical imaging leadershipunfolding each day around the country.
As with this most recent day spent witha talented group, it is gratifying for me to bea part of shaping the model that will consti-tute tomorrow’s successful medical imag-ing practice, and to nurture leadershipfocused on good, solid business practicesthat are built on community and throughcommunication.
Curtis Kauffman-Pickelle is the publisherof Radiology Business Journal and is the CEOof The Imaging Center Institute, Tustin, Calif;[email protected].
The competitive landscape is brutal, and the demandsfor accountability and efficacy are unrelenting. It is nota profession for the faint of heart.
Highly Functional ImagingGreat leadership will distinguish winning imaging organizations from those that struggle
By Curtis Kauffman-Pickelle

Discover the Di!erence "exibility can mean to
your practice.
Digital FTE™FinalsPLUS™ Digital Locums™Traditional Finals
Whether you’re looking for a long term !nals partner, sub-specialty expertise, or vacation coverage, NightHawk will bend over backwards
to accommodate your needs.
[email protected] www.nighthawkrad.net
Flexible Final Interpretation Services:
866-400-HAWK (4295)NightHawk Radiology Services © 2009