
R EPRODUCTION Topics 6.6, 11.4. A SSESSMENT STATEMENTS 6.6.1 Draw and label diagrams of the adult...
50
REPRODUCTION Topics 6.6, 11.4
-
Upload
roderick-fox -
Category
Documents
-
view
214 -
download
0
Transcript of R EPRODUCTION Topics 6.6, 11.4. A SSESSMENT STATEMENTS 6.6.1 Draw and label diagrams of the adult...

REPRODUCTIONTopics 6.6, 11.4

ASSESSMENT STATEMENTS 6.6.1 Draw and label diagrams of the adult male and
female reproductive systems. 6.6.2 Outline the role of hormones in the menstrual
cycle, including FSH (follicle stimulating hormone), LH (luteinizing hormone), estrogen and progesterone.
6.6.3 Annotate a graph showing hormone levels in the menstrual cycle, illustrating the relationship between changes in hormone levels and ovulation, menstruation and thickening of the endometrium.
6.6.4 List three roles of testosterone in males. 6.6.5 Outline the process of in vitro fertilization (IVF). 6.6.6 Discuss the ethical issues associated with IVF.
HUMAN REPRODUCTION
Process includes a male gamete (sperm) fertilizing a female gamete (egg or ovum)
Union ensures that half of the genetic makeup of the resulting zygote is derived from each parent
Ensures genetic variation in the species

MALE REPRODUCTIVE SYSTEM

Roles of testosterone in males
Determines the development of male genitalia during embryonic development
Ensures development of secondary sex characteristics during puberty
Maintains the sex drive of males throughout their lifetime

FEMALE REPRODUCTIVE SYSTEM

MENSTRUAL CYCLE Begins at puberty in females Each complete cycle lasts about 28 days Purpose is to time the release of an egg or
ovum (ovulation) for possible fertilization and later implantation into the inner lining of the uterus
Implantation must occur when the uterine lining (endometrium) is rich with blood vessels
Vascularization is not maintained if there is no implantation
Breakdown of the blood vessels leads to the menstrual bleeding (menstruation) of a typical cycle
Sign that no pregnancy occurred

HORMONES FROM THE BRAIN
Hypothalamus produces gonadotrophin releasing hormone (GnRH)
Target tissue is the pituitary gland and it results in the pituitary gland producing and secreting two other hormones: follicle stimulating hormone (FSH) and luteinizing hormone (LH)
Target tissue for these hormones are the ovaries

HORMONAL SUMMARY OF THE MENSTRUAL CYCLE
EFFECTS OF FSH AND LH ON THE OVARIES
Increases the production and secretion of oestrogen Oestrogen enters the bloodstream and targets
the endometrium of the uterus Result is an increase in the blood vessels in the
endometrium of the uterus Production of structures within the ovaries
known as Graafian follicles

OVARY EVENTS DURING A SINGLE MENSTRUAL CYCLE

Spike in the level of FSH and LH leads to ovulation (release of the oocyte from the Graafian follicle)
Oocyte is accompanied by the inner ring of follicle cells and a glycoprotein membrane coat known as the zona pellucida
Entire structure is known as a follicle and typically enters the Fallopian tube soon after ovulation
Outer ring of follicle cells remains within the ovary and begin to produce/secrete progesterone
Cells of outer ring begin to divide and fill in the area left by ovulation (now known as corpus luteum)
Corpus luteum continues to produce progesterone for 10-12 days after ovulation
Progesterone maintains the thickened endometrium As long as progesterone is produced, endometrium
will not break down and an embryo will still be able to implant

High levels of oestrogen and progesterone are a negative feedback signal to the hypothalamus
Hypothalamus does not produce GnRH, so FSH and LH remain at levels not conducive to production of another Graafian follice during this time
Assuming there is no pregnancy, the corpus luteum breaks down and levels of progesterone and oestrogen drop
Capillaries and small blood vessels begin to rupture and menstruation begins
Hypothalamus begins producing GnRH and thus another menstrual cycle begins


FERTILIZATION
Natural fertilization typically occurs in one of a female’s Fallopian tubes 24-48 hours after ovulation
The resulting zygote begins to divide by mitosis and takes several more days to travel down the Fallopian tube to the endometrium of the uterus
The embryo will then implant in the highly vascular tissue of the endometrium

INFERTILITY
Some couples are unable to bear children for a wide variety of possible reasons, including: Males with low sperm counts Males with impotence (failure to achieve or
maintain an erection) Females who cannot ovulation normally Females with blocked Fallopian tubes
Reproductive technologies have been developed to help overcome these situations.
Most common of these new technologies is in-vitro fertilization

IN-VITRO FERTILIZATION (IVF) Woman is injected with FSH for about 10 days This will ensure the development of many Graafian
follicles within her ovaries Several eggs (oocytes) are then harvested surgically Man ejaculates into a container to obtain the sperm cells
that are needed for fertilization Harvested eggs are mixed with sperm cells in separate
culture dishes Microscopic observation reveals which ova are fertilized
and if the early development appears normal and healthy Usually two or three healthy embryos are introduced into
the woman’s uterus for implantation Very expensive Introducing more than one embryo increases the
likelihood that at least one will implant successfully

ETHICAL ISSUES CONCERNING IVF Arguments for IVF:
Enables couples to have a family Embryos that are visibly not healthy in early stages of
development can be eliminated from consideration Genetic screening is possible before implantation to eliminate
the chance of passing on genetic diseases Arguments against IVF:
Embryos produced, but not implanted are either frozen or destroyed
Legal issues concerning use of frozen embryos when couples split up
Genetic screening could lead to society choosing desirable characteristics
Bypasses natures way of decreasing genetic frequency of that reproductive problem
Multiple births and the problems associated with a multiple births are more likely with IVF than with natural conception
ASSESSMENT STATEMENTS 11.4.1 Annotate a light micrograph of testis tissue to show the location and function of interstitial
cells (Leydig cells), germinal epithelium cells, developing spermatozoa and Sertoli cells. 11.4.2 Outline the processes involved in spermatogenesis within the testis, including mitosis, cell
growth, the two divisions of meiosis and cell differentiation. 11.4.3 State the role of LH, testosterone and FSH in spermatogenesis. 11.4.4 Annotate a diagram of the ovary to show the location and function of germinal epithelium,
primary follicles, mature follicle and secondary oocyte. 11.4.5 Outline the processes involved in oogenesis within the ovary, including mitosis, cell growth,
the two divisions of meiosis, the unequal division of cytoplasm and the degeneration of polar body. 11.4.6 Draw and label a diagram of a mature sperm and egg. 11.4.7 Outline the role of the epididymis, seminal vesicle and prostate gland in the production of
semen. 11.4.8 Compare the processes of spermatogenesis and oogenesis, including the number of
gametes and the timing of the formation and release of gametes. 11.4.9 Describe the process of fertilization, including the acrosome reaction, penetration of the egg
membrane by a sperm and the cortical reaction. 11.4.10 Outline the role of HCG in early pregnancy. 11.4.11 Outline early embryo development up to the implantation of the blastocyst. 11.4.12 Explain how the structure and functions of the placenta, including its hormonal role in
secretion of estrogen and progesterone, maintain pregnancy. 11.4.13 State that the fetus is supported and protected by the amniotic sac and amniotic fluid. 11.4.14 State that materials are exchanged between the maternal and fetal blood in the placenta. 11.4.15 Outline the process of birth and its hormonal control, including the changes in
progesterone and oxytocin levels and positive feedback.

LIGHT MICROGRAPH OF TESTIS
(Leydig cells)
(germinal epithelium cells)

SPERMATOGENESIS: PRODUCTION OF MALE GAMETES BY MEIOSIS
Occurs within testes which are located outside of the human body to provide the cooler temp. necessary for production of sperm cells or spermatozoa
Occurs within seminiferous tubules of each testis
Near the outer wall of the seminiferous tubules lie germinal cells called spermatogonia
Each spermatogonium may be undergoing either mitosis or meiosis at any given time

MITOSIS
Spermatogonia undergo mitosis in order to replenish their numbers
Mitosis replaces the cells that have become spermatozoa
Sperm cells production begins at puberty and continues throughout life
Millions of sperm cells can be produced in a single day
1st replicate DNA within diploid cell Mitosis will result in two half-size cells,
capable of growing again for another cell division

MEIOSIS
Spermatogonia undergo meiosis to produce spermatozoa
Reduces the diploid number of chromosomes in spermatogonia to the haploid number in spermatozoa
In humans, 23 homologous pairs of chromosomes becomes 23 individual chromosomes
Meiosis will result in four spermatozoa, each containing a haploid number of chromosomes

SPERMATOGENESIS
Spermatagonia (2n) contain 23 homologous pairs of chromosomes (total of 46)
DNA replication occurs and each of the 46 chromosomes now exists as a pair of chromatids
Meiosis I occurs and two half-sized cells result, each with the haploid number of chromosomes (23) because homologous pairs have been separated
Each chromosome exists as a pair of chromatids, so then meiosis II must occur
During meiosis II, the chromatids separate 4 haploid cells, each containing 23
chromosomes are created


DIFFERENTIATION INTO SPERMATOZOON
After meiosis, cells stay within the interior of the seminiferous tubule while they form a flagellum for motility and an acrosome (enzyme needed for fertilization)
Developing cells stay attached to Sertoli cells which nourish them
Once spermatozoa have completed formation of flagella, they detach from Sertoli cells and are carried through the lumen with the movement of fluid
Each sperm cell is swept to the epididymis of the testis where it is stored

HORMONAL CONTROL OF SPERM PRODUCTION
Leutinizing hormone (LH) stimulates Lyedig cells to produce testosterone
Follicle stimulating hormone (FSH) and testosterone stimulate the meiotic divisions of spermatogonia into spermatozoa

ROLE OF THE EPIDIDYMIS, SEMINAL VESICLES, AND PROSTATE
Epididymis Sperm cells are stored and gain motility On sexual arousal, sperm move from the
epididymis into the vas deferens Seminal vesicles
Add large volume of fluid into vas deferens with sperm
Fluid contains fructose (provides energy for sperm cells)
Prostate gland Adds more fluid that is alkaline and helps the
spermatozoa survive the environment within the female’s vagina

OVARY
OOGENESIS
Produces female gametes by meiosis Only one of the four end products (cells) are
used as gametes Gamete is known as ovum; others are known
as polar bodies Within the ovaries of a female fetus, cells
called oogonia undergo mitosis repeatedly in order to build up the numbers of oogonia within the ovaries
Oogonia grow into larger cells called primary oocytes (diploid)
Primary oocytes begin meiosis, but stops during prophase I
Other cells called follicles repeatedly undergo mitosis
A single layer of these follicle cells surrounds each primary oocyte and the entire structure is then called a primary follicle
Females’ ovaries contain 400,000 primary follicles
Primary follicles remain unchanged until puberty and menstrual cycles begin

MENSTRUAL CYCLE During each menstrual cycle, a few primary follicles
finish meiosis I One cell is very large and is a secondary oocyte One cell is very small and is called 1st polar body (may
divide again; both degenerate) The single ring of follicle cells begin dividing and
forming a fluid Two rings of follicle cells are formed with a fluid-filled
cavity separating them Secondary oocyte begins meiosis II, but stops during
prophase II Entire structure is now called a Graafian follicle Increased fluid between layers creates a bulge on the
surface of the ovary and eventually leads to ovulation

Secondary oocyte with the inner ring of follicle cells is released from the ovary at ovulation
Meiosis II is not completed until fertilization Another polar body is created (degenerates) Fertilized secondary oocyte is now a zygote

MATURE SPERM AND OVA
Both gametes are haploid Spermatozoon is a very small cells with a
flagellum for motility and mitochondria to provide ATP for swimming
At its anterior end, each sperm cell contains an organelle called an acrosome which contains hydrolytic enzymes which help with the fertilization process

Egg is the largest cell in the body by volume Unequal division of cytoplasm ensures that
one cell would receive all of the cytoplasm, nutrients, and organelles
Nutrients are known as yolk Cytoplasm contains small vesicles called
cortical granules which release calcium and prevents other sperm from entering the egg
Just outside the plasma membrane is a layer of glycoproteins called the zona pellucida which disappears to permit implantation in the uterus

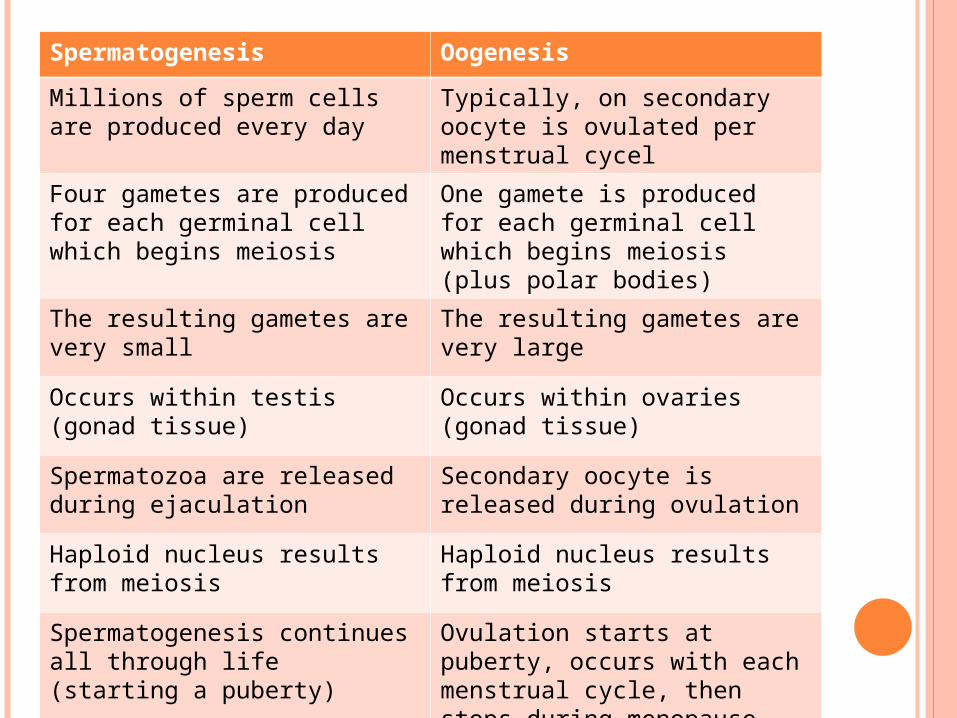
Spermatogenesis Oogenesis
Millions of sperm cells are produced every day
Typically, on secondary oocyte is ovulated per menstrual cycel
Four gametes are produced for each germinal cell which begins meiosis
One gamete is produced for each germinal cell which begins meiosis (plus polar bodies)
The resulting gametes are very small
The resulting gametes are very large
Occurs within testis (gonad tissue)
Occurs within ovaries (gonad tissue)
Spermatozoa are released during ejaculation
Secondary oocyte is released during ovulation
Haploid nucleus results from meiosis
Haploid nucleus results from meiosis
Spermatogenesis continues all through life (starting a puberty)
Ovulation starts at puberty, occurs with each menstrual cycle, then stops during menopause

FERTILIZATION
As a result of sexual intercourse, millions of sperm are ejaculated into a female’s vagina
Spermatozoa absorb fructose for their long journey
Some spermatozoa die immediately upon entering the female due to high acidity
Others find their way to the cervical opening and enter the uterus
Some of these enter the openings of the Fallopian tubes
If the female is near the middle of her menstrual cycle, there may be a secondary oocyte within one of the tubes

Many sperm cells are needed to push their way through the follicle cells surrounding the oocyte
Sperm cells gain access to the zona pellucida (glycoprotein gel layer) and release the hydrolytic enzymes contained in the acrosomes
One sperm cell reaches the plasma membrane of the secondary oocyte first
The plasma membranes of the two gametes fuse together initiating a series of events called the cortical reaction
Cortical granules within the secondary oocyte fuse with the oocyte’s membrane and release enzymes to the outside

A chemical change occurs in the zona pellucida making it impermeable to any more sperm cells
This reaction takes place within a few seconds and ensures that only one sperm cells actually fertilizes the oocyte
The secondary oocyte now completes meiosis II and produces another polar body
Resulting fertilized ovum is now referred to as a zygote

PREGNANCY
Fertilization triggers the zygote to begin a mitotic division which occurs 24 hours after fertilization
The early embryo continues to divide for about 5 days and moves within the Fallopian tube towards the uterus
By the time it reaches the uterus it is approximately 100 cells and is ready to implant itself into the endometrial wall
Ball of cells known as a blastocyst: Surrounding layer of cells called a trophoblast (helps
form placenta) Inner cell mass (becomes body) Fluid-filled cavity


ROLES OF HORMONES
Ovulation of the secondary oocyte left an outer ring of follicle cells within the ovary
This remainining layer (corpus luteum) divides mitotically and begins secreting estrogen and progesterone for about 14 days
These hormones maintain the thickened endometrium in case there has been fertilization
If no fertilization occurs, the corpus luteum ceases hormone production and the endometrium begins to break down
HUMAN CHORIONIC GONADOTROPHIN (HCG)
If fertilization occurs, the embryo enters the uterus and begins implantation about a week after fertilization
Corpus luteum is still active and therefore endometrium is still thick
Soon after implantation, the embryo begins to secrete HCG
HCG enters the mother’s bloodstream targeting the corpus luteum and maintaining its secretory function

ROLE OF THE PLACENTA
During the 1st two weeks, the cell divisions that occur create an embryo of 100 or more cells but the overall size is no larger than the original cell
The nutrients stored within the egg have been used for metabolism, not growth
Upon implantation, it is running out of yolk The embryo and maternal endometrium soon
begin to create a structure known as the placenta
Forms from the trophoblast layer of the blastocyst When fully formed, two fetal blood vessels within
the umbilical cord carry fetal blood to the placenta

Materials passed from fetus to mother within the placenta
Materials passed from mother to fetus within the placenta
Carbon dioxide Oxygen
Urea Nutrients (glucose, amino acids, etc.)
Water Water
Hormones (e.g. HCG) Hormones
Vitamins, minerals
Alcohol, many drugs, nicotine
Some viruses, such as German measles, HIV

At no time does the blood of the fetus and the blood of the mother actually mix
When the corpus luteum stops production of estrogen and progesterone, the placenta has already begun producing and secreting these hormones
ROLE OF AMNIOTIC FLUID Some of the tissue of a developing embryo is
used to create extraembryonic membranes, such as the amniotic sac
Amniotic sac extends all of the way around the fetus and is filled with amniotic fluid in which the fetus floats as it continues to grow and develop
Functions: Cushions fetus should a blunt force be applied to the
mother’s abdomen Provides an environment in which the fetus has free
movement and therefore well balanced exercise for all developing muscles and skeleton
Provides thermal stability Sampled during amniocentesis which can be
cultured for chromosome abnormalities

HORMANAL EVENTS ASSOCIATED WITH BIRTH
Physiological events associated with a woman’s body preparing for a birth are collectively called parturition
1. Major hormone changes Drop in progesterone Oxytocin released stimulating contractions
within uterus Contractions signal posterior lobe of pituitary to
produce more oxytocin which intensifies and increases frequency of contractions (positive feedback)
2. Opening of cervix to 10 cm3. Baby head-first, face down

4. Shoulders of baby (widest part) pass through the birth canal
5. Afterbirth (placenta) is expelled after birth6. Lactation (birth milk production) begins
after birth


















